
2 AM. 4 AM. Every single night.
Your family hasn't slept through in longer than you can remember. The exhaustion is bone-deep — and the worst part? You don't know why they keep waking, or how to help them stay asleep on their own.
D-447 | Sleep Independence
Age 2–12 | OT / ABA / NeuroDev

9 Materials That Help With Night Waking
Scientific. Practical. Home-executable tonight.
🌙 Recognize
Understand what's really happening
🧠 Science
The neuroscience behind night waking
🛒 Materials
9 evidence-backed tools
📋 Protocol
Step-by-step nightly system
📈 Progress
What to expect week by week
"You are not failing. Your child's nervous system is speaking — and there are evidence-based tools that answer it." — Pinnacle Blooms Consortium®
🏥 Pinnacle Blooms Consortium® | Age: 2–12 yrs | Domain: Sleep / OT / Behavioral Regulation | Series D-447 | WHO Nurturing Care Framework (2018): Parental awareness and responsive caregiving directly impact developmental outcomes.

Your child is not the only one awake tonight.
50–80%
ASD Sleep Disturbance
of children with autism experience significant sleep disturbances including night waking
1 in 3
Typically Developing
toddlers aged 1–3 still experience night waking requiring parental support
2–3×
Sensory Differences
higher rate of chronic sleep problems in children with sensory processing differences vs. neurotypical peers
📊 Research confirms: Children with autism are 5× more likely to have clinically significant sleep problems compared to neurotypical children, with night waking being the most reported challenge.
In India alone, with an estimated 18 million children on the autism spectrum and millions more with sensory processing differences, chronic night waking affects tens of millions of families. You are not failing. This is biology calling for support.
Sources: PMC11506176 | PRISMA Systematic Review (2024) · PMC10955541 | World J Clin Cases Meta-analysis (2024) · DOI: 10.12998/wjcc.v12.i7.1260

This isn't willfulness. This is neuroscience.
Sleep Cycle Architecture
All humans cycle through sleep stages every 60–90 minutes. Children have shorter cycles and spend more time in light sleep (Stage 1–2 NREM), creating more natural arousal points per night than adults.
The Arousal Threshold Difference
In neurotypical sleepers, brief arousals between cycles are sub-conscious. In children with sensory processing differences, ADHD, autism, or anxiety, the arousal threshold is lower — meaning environmental stimuli that most people sleep through become full conscious wake triggers.
Brain Regions Involved
- Reticular Activating System (RAS): Overactive in sensory-sensitive children — more easily triggered
- Amygdala: Heightened threat detection — increases anxiety-based awakenings
- Hypothalamus (SCN): Circadian clock — disrupted by light intrusion and irregular schedules
- Somatosensory Cortex: Processes touch and proprioception — lack of organizing input overnight disrupts regulated sleep

Sleep independence is a developmental skill — and it can be taught.
0–6 months
Multiple night feedings; frequent arousals are normal
6–18 months
Begin consolidating nighttime feeds; night waking challenge zone begins
18m–3 yrs
Most typically developing children begin weaning from parent presence overnight
3–6 yrs
Sleep through night with occasional brief arousals; self-managed for most
6–12 yrs
Sleep through night consistently; full independence expected
For children with sensory differences, autism, ADHD, or anxiety, the transition to independent night sleep takes longer and requires intentional scaffolding. This is not developmental failure — it is the intersection of neurodevelopmental difference with an immature self-regulation system.
What Commonly Co-Occurs
Sensory Processing Differences
Tactile, auditory, proprioceptive
Anxiety / Separation Anxiety
Anxiety disorders driving night waking
ADHD
Sleep architecture disruption
Autism Spectrum
Higher rates across all sleep parameters
Circadian Differences
Delayed melatonin onset
Sources: PMC9978394 | WHO/UNICEF Care for Child Development (2023) · WHO Developmental Milestones (2022)

Clinically validated. Home-applicable. Parent-proven.
🛡️ Environmental Optimization — Level I
Consistent, dark, quiet sleep environments reduce arousal triggers and support sleep continuity. Evidence: Cochrane reviews on pediatric sleep hygiene + multiple RCTs.
🛡️ Deep Pressure for Sleep — Level II
Weighted blankets activate the parasympathetic nervous system and reduce cortisol levels. Ball et al. (2020) — significant improvement in sleep onset and maintenance in ASD population.
🛡️ Behavioral Interventions — Level I STRONG
Graduated extinction, sleep restriction, and scheduled awakenings classified as evidence-based by the American Academy of Sleep Medicine. NCAEP (2020) confirms for autism.
🛡️ Visual Supports — Level II
OK-to-wake clocks and visual routine charts reduce nighttime parental calls and improve sleep independence. Evidence: Multiple clinical trials in pediatric behavioral sleep literature.
📖Systematic Review (Children, 2024) — PMC11506176: 16 studies (2013–2023) confirm sensory integration intervention meets evidence-based practice criteria for children with ASD across sleep and regulation domains.
Sources: PMC11506176 · PMC10955541 · PMC9978394 · NCAEP Evidence-Based Practices Report (2020) · Padmanabha et al., Indian J Pediatr (2019) | DOI: 10.1007/s12098-018-2747-4

The Night Waking Toolkit — What It Is
D-447
Sleep Independence
Sensory Processing
Behavioral Regulation
Formal Name: Sleep Environment Optimization & Self-Soothing Material Protocol for Night Waking
Parent-Friendly Name:The Night Waking Toolkit
Series ID: D-447 | Toileting & Self-Care Independence — Episode 447
Parent-Friendly Name:The Night Waking Toolkit
Series ID: D-447 | Toileting & Self-Care Independence — Episode 447
Night waking refers to fully waking during normal sleep cycle transitions (every 60–90 minutes) and being unable to return to sleep independently. This protocol addresses night waking through a three-pronged approach:
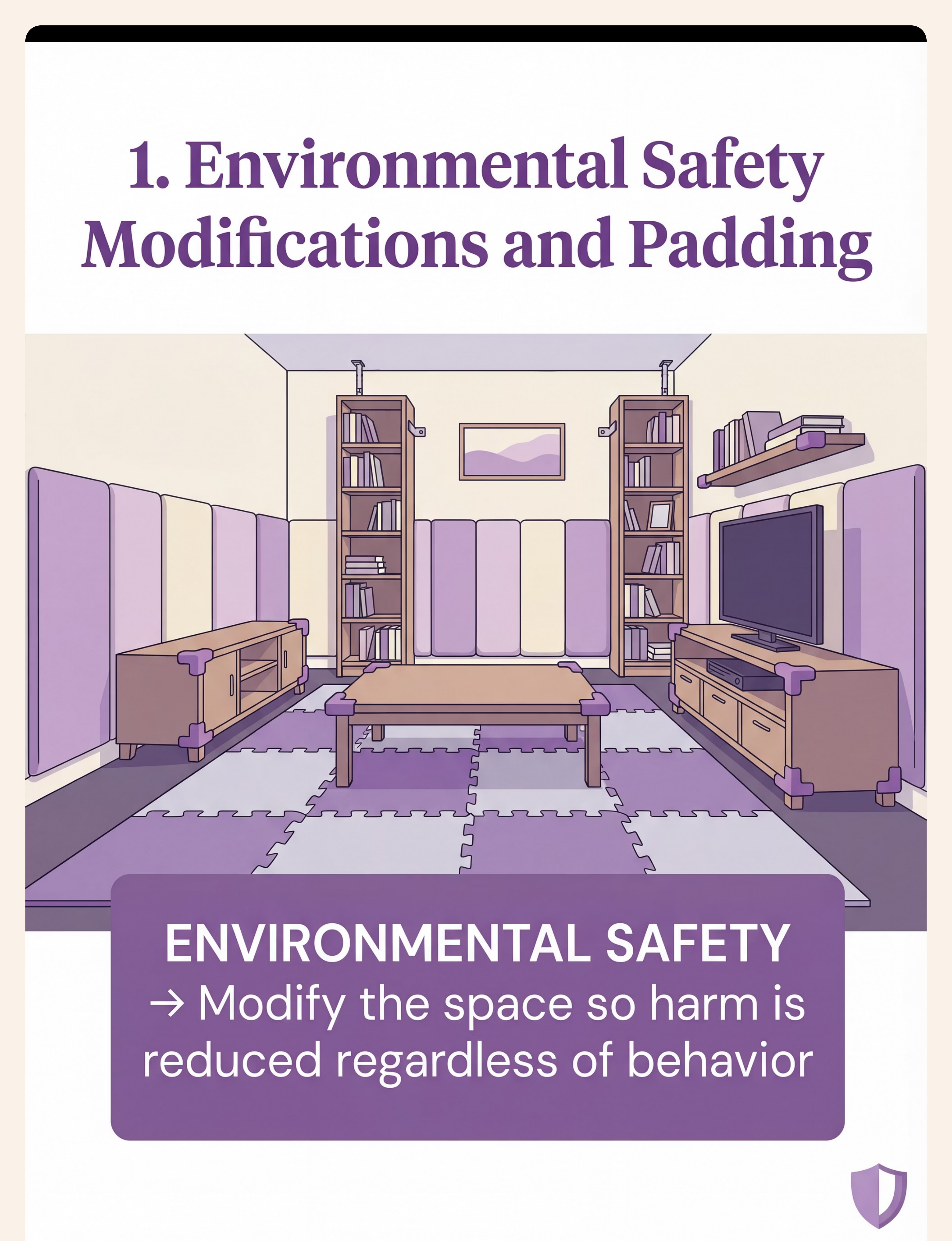
Environmental Modification
Removing sensory triggers that cause full awakening — light, sound, temperature disruptions that set off the arousal alarm.
Sensory Regulation Support
Providing calming proprioceptive and tactile input throughout the night — weighted blankets, compression sleepwear — keeping the nervous system settled.
Self-Soothing Skill Building
Equipping the child with tools and strategies to return to sleep independently — so the alarm turns itself off without parental intervention.
Age | Setting | Frequency | Duration | Discipline Lead | |
2–12 years | Home (bedroom) | Nightly — ongoing | Embedded in sleep environment | OT primary, ABA secondary |

Your child's sleep is a multi-disciplinary challenge — solved by a multi-disciplinary team.
Occupational Therapist (OT) — Primary Lead
Assesses sensory processing profile, prescribes weighted blankets and compression sleepwear, conducts formal Sensory Profile assessment, and leads the environmental and proprioceptive intervention layer.
ABA / BCBA — Secondary Lead
Designs behavioral sleep protocols — graduated response fading, reinforcement schedules for staying in bed, OK-to-wake clock implementation, and token economies. Tracks waking data.
NeuroDev Pediatrician
Rules out underlying sleep disorders (sleep apnea, restless legs, parasomnias), assesses melatonin production, evaluates medication interactions, determines when specialist referral is needed.
Special Educator (SpEd)
Designs visual supports — bedtime routine charts, self-soothing strategy cards, and social stories about nighttime. Ensures comprehension for children with cognitive or communication differences.
At Pinnacle centers, FusionModule™ coordinates all four disciplines under one GPT-OS® governed plan — so every therapist's approach to sleep reinforces every other's.

Precision therapy. Targeted developmental tools.
🎯 Primary Target
Sleep Continuity & Night Waking Reduction
Fewer wakings per night · Time to return to sleep decreasing · Increasing nights of full sleep through
Fewer wakings per night · Time to return to sleep decreasing · Increasing nights of full sleep through
🔵 Secondary Targets
Self-Soothing Capacity — child attempts strategies before calling parent
Arousal Regulation — nervous system stays calm longer, reduced startle responses
Arousal Regulation — nervous system stays calm longer, reduced startle responses
⚪ Tertiary Targets
Circadian rhythm stabilization · Daytime behavior improvement · Family system wellbeing · Sleep independence generalization to new environments
This technique is tracked under the Sleep Independence Readiness Index, the Self-Regulation Readiness Index, and the Sensory Processing Readiness Index within GPT-OS®.
PMC10955541 | Meta-analysis (World J Clin Cases, 2024): Sleep and behavioral regulation show measurable improvement across 24 studies using sensory and behavioral approaches.

9 Materials. Science behind every one.

1. Weighted Blanket
Sensory Regulation — Proprioceptive Input
Deep pressure touch activates the parasympathetic nervous system, suppressing cortisol and supporting melatonin maintenance. Weight guide: 10% of child's body weight. Price: ₹2,000–6,000

2. White Noise Machine
Auditory Environment Tools
Creates a consistent acoustic blanket masking intermittent sounds that trigger arousal. Spec: Continuous play, no auto-off. Volume 50–65 dB. Position across room, not near head. Price: ₹500–2,500
3. Red / Amber Night Light
Visual Environment Tools
Red/amber wavelengths (620–750 nm) do NOT suppress melatonin. Provides orientation when child briefly arouses without triggering the alerting response. Must be specifically RED or AMBER LED. Price: ₹200–800

4. OK-to-Wake Clock
Visual Supports / Behavioral Cue Tools
Gives children a concrete answer to "Is it still sleep time?" without requiring parent confirmation. Active Pinnacle Product: Smartivity DIY Interactive Clock | ₹673 | Buy on Amazon.in. Dedicated clocks: ₹1,000–3,000

5. Comfort Object with Parent Scent
Transition Objects / Comfort Items
Scent connects directly to the amygdala (emotional center) and hippocampus (memory) — activating safety neurochemistry without physical parent presence. Active Pinnacle Product: Animal Soft Toy | ₹425 | Buy on Amazon.in
6. Blackout Curtains
Environmental Modification — Light Control
Even 10 lux (streetlight level) can reduce melatonin by 25%. Complete darkness maintains melatonin through the full sleep period. Spec: True blackout — test in daylight. Price: ₹800–3,000


7. Visual Bedtime Routine Chart
Visual Supports / Predictability Tools
Predictable bedtime routines reduce pre-sleep anxiety by signaling the brain that sleep is approaching. Can include a "what to do if you wake up" step. Spec: Laminated, picture-based (photos of your child), sequential. Price: ₹100–500

8. Compression Sleepwear
Sensory Regulation — Proprioceptive Input (wearable)
Provides continuous deep pressure input without the weight of a blanket — cannot be kicked off. Particularly effective for sensory-seeking children. Spec: Snug but not restrictive. Breathable fabric. Price: ₹500–2,000

9. Self-Soothing Strategy Cards
Behavioral Skill Tools / Visual Supports
Provides explicit visual instructions for alternatives when waking: "Hug your teddy," "Take 5 deep breaths," "Check your clock." Over time, builds genuine self-soothing capacity. Spec: Laminated, pictorial, 3–5 strategies max, within reach of bed. Price: ₹50–300
🚀Begin with these 3: White noise machine + Blackout curtains + OK-to-wake clock. These address the most common environmental night waking triggers first. Total cost: ₹1,500–6,500 | Can be DIY'd for under ₹300
Every family can do this. No purchase required to start tonight.
This page follows the WHO Nurturing Care Framework principle that interventions must be accessible regardless of economic status. Every material above has a ₹0 household equivalent.
Material | Clinical Version | ₹0 Household Version | Same Principle | |
Weighted blanket | Commercial weighted blanket ₹2,000–6,000 | Extra quilt or 2 heavy blankets layered | Deep pressure = deep pressure | |
White noise | Dedicated machine ₹500–2,500 | Table fan on low, or free app on silent phone | Acoustic masking = acoustic masking | |
Red/amber light | Red LED night light ₹200–800 | Himalayan salt lamp ₹300, or candle in safe holder | Warm wavelength = warm wavelength | |
OK-to-wake clock | Dedicated clock ₹1,000–3,000 | Alarm clock + colored sticky note on clock face | Visual cue = visual cue | |
Comfort object | New soft toy ₹425 | Any existing soft toy with parent's worn t-shirt wrapped around it | Scent transfer = scent transfer | |
Blackout curtains | Commercial blackout ₹800–3,000 | Heavy blanket pinned over window, black bin bags taped to frame | Light blocking = light blocking | |
Routine chart | Printed laminated set ₹100–500 | Hand-drawn pictures on cardboard pinned to wall | Visual sequence = visual sequence | |
Compression sleepwear | Specialized compression ₹500–2,000 | Snug-fitting existing cotton full-body pajamas | Proprioceptive input = proprioceptive input | |
Strategy cards | Printed laminated set ₹50–300 | Small notepad with drawn pictures by child's bed | Visual prompt = visual prompt |
⚠️When clinical-grade is non-negotiable: The weighted blanket weight MUST be calibrated (10% of body weight). An unweighted blanket does NOT provide the same therapeutic effect. Verify weight with a kitchen scale before placing on child.

Safety is not a footnote. Read this before tonight.
🔴 RED — Do NOT Use If:
- Child is under 2 years old → Weighted blanket is CONTRAINDICATED. Risk of suffocation.
- Child cannot independently remove the weighted blanket
- Child has respiratory conditions, asthma, skin hypersensitivity, or circulatory issues → Consult pediatrician first
- Child is unwell, feverish, or post-meltdown → Postpone new material introduction
- Never use white or blue-tinted lights during sleep — suppresses melatonin
🟡 AMBER — Modify If:
- Sensory response to new materials is unknown → Introduce one material at a time, observe 3–5 nights
- Child has severe claustrophobia or tactile aversion → Start with compression sleepwear first
- Child has strong reactions to scent → Skip scented comfort object or use very mild scent
- OK-to-wake clock glowing bothers child → Choose dim or off-display model
- Child is pre-verbal → Use picture-only strategy cards; practice extensively during daytime
🟢 GREEN — Proceed When:
- Child is in a regulated baseline state (not post-meltdown, not unwell)
- Spaces between new material introductions (1 per week or per therapist guidance)
- All materials are age-appropriate and weight-calibrated
- Parent has read this card fully and discussed with OT if using weighted blanket for first time
Stop Immediately If: Child attempts to remove weighted blanket but cannot · Increased distress or panic with any material · Any breathing difficulty · Adverse reaction to comfort object
Medical Disclaimer: This information is educational. Persistent night waking may indicate underlying sleep disorders, sleep apnea, nocturnal seizures, or other medical conditions requiring professional evaluation. Consult your pediatrician if night waking is severe (4+ wakings/night consistently), sudden-onset, or accompanied by unusual behaviors.
📞9100 181 181 — FREE. 24×7. 16+ languages. Call before starting if you have any safety concerns.
The right room makes the technique work. Set this up this evening.
Room Setup Checklist
- ✅ Blackout curtains installed, all gaps sealed
- ✅ White noise machine across the room (NOT next to head), continuous play
- ✅ Red/amber night light in corner — ambient glow, not direct light
- ✅ OK-to-wake clock visible from bed, wake time set
- ✅ Weighted blanket on bed (calibrated weight)
- ✅ Comfort object with parent scent in bed
- ✅ Strategy cards in small basket or on bedside (within reach)
- ✅ Visual routine chart at child's eye level near bed
- ✅ All electronics with standby lights covered with black tape
- ✅ Room temperature: 18–22°C
- ✅ All daytime-stimulating toys removed or covered
Material Placement Rules
White Noise
ACROSS the room — 1–1.5 metres from bed. Never directly next to head (hearing safety).
Night Light
Corner or low on wall. Not visible directly from bed (ambient only).
Weighted Blanket
Ready on bed — child ALWAYS chooses to use it. Never forced.
Strategy Cards
Within reach without leaving bed — basket or key ring on bedside.

60 seconds before bedtime. Is tonight the night to introduce new materials?
Physical State
- Child is well-rested from the day (not overtired — overtiredness INCREASES night waking)
- Child has eaten a satisfying dinner (not hungry)
- Child has not had screen exposure in the last 60 minutes
- Child is not unwell or feverish
Emotional State
- Child is in calm-to-regulated state (not post-meltdown)
- No major schedule disruptions today that heightened anxiety
- Child has had positive interactions with parent today (connection is full)
Environment State
- Room setup complete (Card 12 checklist done)
- New material being introduced has been seen/touched during daytime (not first introduction at night)
8–9 ✅ → GO
Introduce new material tonight as planned
5–7 ✅ → MODIFY
Proceed with existing sleep environment only. No new materials tonight.
Under 5 ✅ → POSTPONE
Use normal routine without changes. Note what prevented readiness. Try again tomorrow.
"The best session is one that starts right. A postponed introduction is not failure — it is clinical wisdom. Introducing a new material into a dysregulated nervous system can create negative associations that set progress back weeks."

Step 1 — The Invitation
30–60 seconds
"It's getting close to sleep time. I have something special for you tonight. [Show material]. This is your [name of material]. It's going to help your body feel cozy and safe all night long. Would you like to hold it / try it / put it on?"
Body Language Guidance
- Get at child's eye level (sit on bed edge)
- Calm, slow voice — 30% quieter than daytime speaking
- No urgency, no demand framing
- Present material casually — in open hands, not thrust forward
Acceptance Cues ✅
- Reaches for or looks at material
- Relaxed shoulders, soft expression
- Touches or holds material voluntarily
Resistance Cues — Modify If You See:
- Turning away or backing up
- Vocalizing "no" or distress sound
- Covering eyes or batting away
If resistance → DO NOT FORCE. Place material visibly in room without applying or requiring. Try again tomorrow. Forced sensory introduction creates lasting aversion.
ABA Pairing Procedures: Establishing motivating operations before demand placement. OT "Just-Right Challenge" principle: task demand matched to child's current capacity.

Step 2 — The Engagement
1–3 minutes
Child has accepted the material. Now deepen engagement through agency — because ownership drives buy-in.
Let Child Lead
Let child handle, examine, and arrange the material freely. Agency = buy-in. Never rush this.
Weighted Blanket
Let child pull it over themselves or onto their legs first — their pace, their choice.
Comfort Object
Let child choose exactly where it sits in bed. Their room, their rules.
Strategy Cards
Go through each card together: "What does this one say? Deep breaths — can we practice?"
OK-to-Wake Clock
Show child the color change: "When it's red, your body is still sleeping. When it turns green, morning has come."
Reinforcement cue within 3 seconds of positive engagement: "Yes! You're doing that so well. Your body knows what to do."
Engagement ✅
Exploring, adjusting, asking questions — positive sign
Tolerance ✅
Using material without enthusiasm — also acceptable
Avoidance ⚠️
Pushing material away after initial acceptance → Stop, remove, note for OT

Step 3 — The Therapeutic Night
Ongoing — All Night
The materials are now in place. The therapeutic action is the sustained environmental and sensory condition throughout the night. Here, the environment itself delivers the intervention.
Environmental Layer (passive — works automatically)
- White noise runs all night → Acoustic masking of arousal triggers
- Blackout curtains sealed → Light-triggered arousal eliminated
- Red/amber night light on → Orientation without melatonin suppression
Sensory Regulation Layer (passive — works automatically)
- Weighted blanket in place → Continuous deep pressure throughout sleep cycles
- OR Compression sleepwear → Proprioceptive input without blanket
- Comfort object in arms → Olfactory safety signal present
Behavioral Layer (active when child wakes)
- OK-to-wake clock visible → Answers "is it still night?" without parent
- Strategy cards reachable → Gives child a plan before calling out
Parent's nighttime role (first 2 weeks): If child wakes and calls out, respond once with a brief, low-stimulation check. Enter quietly, minimal interaction. Prompt: "It's still sleep time. What does your clock say? Can you try your cards?" Exit within 60–90 seconds. Do NOT turn on bright lights, begin extended conversation, bring child to parent's bed, or respond with frustration.
Step 4 — The Nightly Protocol
7–14 Nights to Establish
Sleep interventions require nightly consistency for a minimum of 14 consecutive nights before meaningful pattern change occurs. This is not a 3-night experiment.
Week 1 (Nights 1–7)
Environmental Optimization Only. Run: White noise + Blackout + Night light. Introduce ONE sensory material only (weighted blanket OR compression sleepwear — not both). Observe and record.
Week 2 (Nights 8–14)
Add Behavioral Layer. Add: OK-to-wake clock + Comfort object. Begin strategy card introduction via daytime rehearsal first. Continue consistent environmental layer.
Week 3+ (Nights 15+)
Full Protocol. All 9 materials in place. Graduated reduction of parent response. Begin reinforcing morning: "You used your strategies last night! Here's your token."
Variation Options
- Child rejects weighted blanket → Substitute compression sleepwear — same proprioceptive principle
- Child not ready for OK-to-wake clock → Visual tape on existing clock face (red for night, green for morning)
- Strategy cards too complex → Simplify to one picture: "Hug teddy"
SI therapy dosage research: 8–12 week consistent implementation is standard protocol. PMC11506176 + Pinnacle clinical norms.

Step 5 — The Morning Reinforcement
Next Morning — Never at 3 AM
🥇The Golden Rule: Reinforcement happens NEXT MORNING, not at 3 AM. Never reinforce waking with attention, excitement, or rewards in the middle of the night. Reserve all positive attention for morning.
No calling out (even with wakings)
"I noticed you tried to go back to sleep on your own last night. I am SO proud of you. Your body is learning to sleep! Let's put a sticker on our chart."
Child used strategy before calling
"You tried your cards before you called me? That was amazing. Your brain is getting so strong at sleep."
Improvement over last night
"You only called once tonight instead of three times. That's real progress. Your body is learning."
A difficult night (no progress)
"Tonight was hard. That's okay. We try again tonight. I'm proud of you for being in your own bed."
Token Economy Framework
1 Token
Staying in bed all night (even with awakenings)
2 Tokens
Self-soothing back to sleep (no parent call)
3 Tokens
Full night's sleep through
5 Tokens
Redeem for preferred activity, outing, or special choice
Step 6 — The Bedtime Close
Last 5–10 Minutes Before Sleep
Cue 1 — The 5-Minute Warning
"Five more minutes. We're getting sleepy." Quiet voice. White noise already running. Lights already dimmed to night light only.
Cue 2 — Material Check-In
"Let's get your [blanket/comfort object/strategy cards] ready. Everything you need is right here."
Cue 3 — Night Waking Rehearsal
"If you wake up and it feels like nighttime, check your clock. If it's red, it's still sleep time. Hug [comfort object] and try your breathing card. I will be here. Your room is safe."
Cue 4 — The Final Statement
"I love you. Good night. Your body knows how to sleep."
Parent Exit: Leave while child is drowsy but not fully asleep — this supports independent sleep onset. Brief, calm exit — no extended lingering. If child protests: validate once, ONE return maximum. Each night, try to extend the time before return.

60 seconds of data this morning saves hours of guessing later.
3
Data Points Daily
Waking Count · Self-Soothing Attempt · Parent Response Required — nothing more
14
Days to Baseline
Minimum 14 nights of tracking before evaluating effectiveness or making protocol changes
60s
Morning Log Time
Record immediately in the morning while the night is fresh in memory
Date | Wakings | Self-soothe attempt | Parent response needed | |
Night 1 | 3 | No | Yes | |
Night 3 | 2 | No | Yes | |
Night 7 | 2 | Yes (once) | Yes | |
Night 10 | 1 | Yes | No | |
Night 14 | 0 | — | No |
What the data tells you: Trend toward fewer wakings per week = technique working · No change after 14 nights = consult OT, adjust materials · Sudden spike after improvement = check for new environmental factor or stress event

Session abandonment is not failure. It is data.
❓ Child rejected the weighted blanket completely
Why: May have tactile defensiveness, wrong weight, or not yet ready.
Fix: Start with compression sleepwear (same deep pressure, less intrusive). Or use blanket on legs only. Consult OT for formal sensory profile assessment.
Fix: Start with compression sleepwear (same deep pressure, less intrusive). Or use blanket on legs only. Consult OT for formal sensory profile assessment.
❓ Child is MORE awake after introducing white noise
Why: Wrong noise type, volume too high, or machine too close.
Fix: Try pink noise, brown noise, or rain. Move machine further away. Reduce volume to just above awareness level.
Fix: Try pink noise, brown noise, or rain. Move machine further away. Reduce volume to just above awareness level.
❓ OK-to-wake clock causing MORE tantrums
Why: Clock is creating anxiety rather than reducing it; child may not have the concept yet.
Fix: Remove clock for 2 weeks. Focus on comfort object + strategy cards. Reintroduce when concept is clearer.
Fix: Remove clock for 2 weeks. Focus on comfort object + strategy cards. Reintroduce when concept is clearer.
❓ Child is scared even with night light
Why: Red/amber light too dim, or new darkness from blackout curtains is unfamiliar.
Fix: Temporarily increase night light. Spend daytime time playing in room with curtains drawn. Transition gradually to full blackout.
Fix: Temporarily increase night light. Spend daytime time playing in room with curtains drawn. Transition gradually to full blackout.
❓ Child still waking 3–4+ times after 3 weeks
Why: May be medical/physiological factor, not behavioral/sensory.
Fix: Consult pediatrician to rule out sleep apnea, reflux, or neurological factor. Contact Pinnacle for OT assessment. Call 9100 181 181.
Fix: Consult pediatrician to rule out sleep apnea, reflux, or neurological factor. Contact Pinnacle for OT assessment. Call 9100 181 181.
❓ Strategy cards not being used at night
Why: Night is not the time to learn a new skill — child hasn't practiced enough during the day.
Fix: 5-minute daytime strategy card rehearsal every day for 2 weeks before expecting nighttime use. Make it a game.
Fix: 5-minute daytime strategy card rehearsal every day for 2 weeks before expecting nighttime use. Make it a game.

No two children sleep alike. Adapt this to your child's exact profile.
Sensory Seeking
Craves input — constant movement, tight hugs, heavy activities
Best starting materials: Weighted blanket (heavier end) + Compression sleepwear. May need BOTH for adequate input. Add proprioceptive pre-sleep activities: 10 minutes of heavy work before bed (carrying laundry, bear hugs, wall push-ups).
Sensory Avoiding
Overwhelmed by stimulation — sensitive to sounds, textures, lights
Best starting materials: White noise + Blackout curtains + Very light weighted blanket (start at 8% body weight). Introduce materials one at a time with 1-week gap between introductions. Compression may be too intense — start with snug cotton pajamas.
Anxiety-Based Waking
Wakes with fear, calling for parent, separation distress
Best starting materials: Comfort object with parent scent + Red/amber night light + Strategy cards. Social stories about nighttime safety. Create a "safety photo album" for beside the bed. Predictable parent response protocol every time.
Cognitive / Communication Differences
Visual routine chart and strategy cards must match child's comprehension level. Pre-verbal children: picture-only cards, practice every day. Limited understanding: simplify strategy cards to 1–2 items maximum.
Age Modifications
Ages 2–4
Visual chart + comfort object + night light (essential). Weighted blanket ONLY with OT guidance.
Ages 5–8
Full 9-material protocol. OK-to-wake clock + strategy cards highly effective.
Ages 9–12
Strategy cards in self-management format. Child creates their own sleep kit. Increasing autonomy in protocol design.

Nights 1–14: The nervous system is learning. Not changing yet — learning.
Week 1–2
Progress: 15%
Progress So Far
Early-stage. Tolerance and participation are the primary goals right now.
Better Night Signal
One notably better night in 7 is the system working — not luck
Duration Reduction
Waking duration may begin to shorten even before waking frequency drops
✅ What You Will Likely See
- Child tolerates new material (even reluctantly) — this IS progress
- Waking frequency stays same BUT duration of each waking may reduce slightly
- One night in 7 may be noticeably better
- Child begins to recognize materials as part of routine
❌ What You Will NOT See Yet (and that's normal)
- Consistent full nights through — too early
- Child self-soothing independently — skill still being built
- Dramatic reduction in waking frequency — the association is forming
Week 1–2 often feels like nothing is working. This is the most vulnerable period for abandoning the protocol. The evidence says: maintain consistency through weeks 1–2 and measurable change begins in weeks 3–4. "If your child tolerates the weighted blanket for 20 minutes of sleep before removing it — that's real progress."
Weeks 3–4: The neural pathways are forming. Watch for these signs.
Week 3–4
Progress: 40%
Behavioral Consolidation
- ✅ Child shows less resistance at bedtime (routine feels familiar now)
- ✅ Child reaches for comfort object without being prompted
- ✅ Waking frequency decreasing by 1–2 nights per week on average
- ✅ Child sometimes returns to sleep within 10 minutes (vs. 30+ in Week 1)
Neural Pathway Signals
- ✅ Child begins to self-settle occasionally without full parent intervention
- ✅ Strategy cards being noticed (even if not used independently yet)
- ✅ OK-to-wake clock understood — child checking it before calling out
Spontaneous Integration Signs
- ✅ Child asks for the weighted blanket at bedtime (positive association formed)
- ✅ Grabbing comfort object when drowsy (natural integration)
- ✅ Showing less anxiety at bedtime overall
"You may notice you're sleeping slightly better too. Your nervous system is learning that not every night will be broken. This is co-regulation — your calm is contagious."
Weeks 5–8: Your child is becoming a self-sufficient sleeper.
Week 5–8
Progress: 75%
🏆 Sleep Independence Mastery
Unlock when ALL 3 are present for 2+ consecutive weeks:
- Child sleeps through without calling for parent on 5+ of 7 nights
- When waking DOES occur, child uses at least one self-soothing strategy before calling
- Child independently settles within 15 minutes on waking nights
🌟 Generalization Indicators
Skill is truly internalized when:
- ✅ Sleep pattern maintained at grandparents'/relatives' home
- ✅ Sleep maintained during mild illness (not just perfect-condition nights)
- ✅ Child verbalizes their sleep strategies to others
- ✅ Child adapts their own kit (adds preferred items, removes others)
Full Generalization Mastery: Can the child sleep through in a hotel or unfamiliar room? This is the gold standard. If mastery is achieved at Week 8, the child is ready for Technique D-448 (Early Morning Waking) or D-449 (Nightmares and Night Terrors).
PMC10955541 | BACB mastery criteria standards: Mastery = criterion performance for defined number of consecutive sessions.

🎉 You did this. Your child sleeps because of your commitment.
Over the past 5–8 weeks you have set up a scientifically optimized sleep environment every single night, introduced sensory regulation tools with patience and consistency, held a calm supportive response protocol through broken nights, taught your child explicit self-soothing skills they will carry for life, and tracked data that proves measurable change.
"The nights you got up at 2 AM and didn't yell. The consistency you held when it would have been easier to give up. The love that made you keep trying. This result exists because of you."
📸 Mark the Moment
Take a photo of your child's sleep setup — their sleep sanctuary that you built together.
📓 Write it Down
"On [date], [child's name] slept through the night independently for the first time."
🌟 Tell Your Child
"Your body learned something amazing. You are so strong."

Progress is the goal. Safety is non-negotiable. Know when to pause.
🔴 Medical Red Flags — Pause & Consult Immediately
- Loud snoring, gasping, or observed breathing pauses → Possible sleep apnea
- Unusual repetitive movements during sleep (jerking, kicking, cycling legs) → Possible neurological factor
- Inconsolable screaming lasting 10–20+ minutes with child "not present" → Possible night terrors (different intervention required)
- Sudden onset of night waking that was NOT previously a problem → Rule out medical cause
- No improvement after 6 weeks of consistent implementation → Professional evaluation needed
🔴 Sensory/Behavioral Red Flags — Consult OT/Behavioral Therapist
- Weighted blanket causing visible distress every night after 2+ weeks → Wrong weight; formal sensory assessment needed
- Child's overall anxiety INCREASING over the protocol period → May need anxiety-specific intervention first
- Self-injurious behavior increasing around bedtime → Behavioral specialist immediately
"You know your child. If something feels genuinely wrong — not just 'this is hard' but truly wrong — pause and ask. That instinct is information."
📞9100 181 181 — FREE. 24×7. 16+ languages. | → Find a Pinnacle center near you
You are here. Here is where your journey continues.
D-445
Sleep Routine Establishment
D-446
Falling Asleep Independently
D-447 ← YOU ARE HERE
Night Waking — Full 9-Material Protocol
D-448
Early Morning Waking
D-449 / D-450
Nightmares & Night Terrors / Bedtime Resistance
Prerequisite Techniques
- D-445: Sleep Routine Establishment — consistent bedtime routine is prerequisite for night waking intervention
- D-446: Falling Asleep Independently — child who can't fall asleep independently also won't sleep through
Next-Level Options (choose based on remaining challenge)
- → D-448: Child now sleeps through but wakes early (5–6 AM)
- → D-449: Frightening nighttime episodes — different intervention required
- → D-450: Bedtime resistance is now the primary challenge
Long-Term Goal: Consistent, independent sleep through the night → daily readiness → improved therapy participation → accelerated developmental progress across all domains.

Explore the full Sleep Independence cluster.
You already own materials for several of these techniques from your D-447 toolkit — a significant investment in your child's complete sleep independence journey.
Technique | Code | Difficulty | Materials You Already Own | |
Sleep Routine Establishment | D-445 | 🟢 Intro | Visual chart (already created) | |
Falling Asleep Independently | D-446 | 🟡 Core | Comfort object + strategy cards | |
Night Waking (you are here) | D-447 | 🟡 Core | Full kit | |
Early Morning Waking | D-448 | 🟡 Core | OK-to-wake clock + blackout | |
Nightmares & Night Terrors | D-449 | 🔴 Advanced | Night light + comfort object | |
Bedtime Resistance | D-450 | 🟡 Core | Visual routine chart |
If you've built the D-447 toolkit, you already have materials for D-446, D-448, D-449, and D-450 — a major investment in the full Sleep Independence cluster already complete.
Night waking is one signal in a whole developmental symphony. See the full picture.
This Technique Feeds Into:
- Domain C (Behavioral Regulation): Better sleep = better emotional regulation = fewer behavioral challenges during the day
- Domain A (Sensory Processing): Night waking intervention often reveals sensory processing profile needing broader OT attention
- Domain K (Social-Emotional): Sleep-deprived children show reduced social engagement and emotional resilience
The GPT-OS® Whole-Child View
Every technique page in the Pinnacle system connects to the child's GPT-OS® developmental profile. Sleep Independence Readiness Index gains here unlock progress in multiple other domains simultaneously.
Real families. Real nights. Real change.
Priya, Hyderabad — Week 10
Before: 6-year-old son waking 3–4 times every night. By 4 AM he was in our bed. 18 months of broken sleep.
After: "Night 47 was the first night he didn't come to our room. By week 10, he was sleeping through 6 of 7 nights. The weighted blanket was the key — it was like the weight told his body it was safe. Our whole family is a different version of itself now."
After: "Night 47 was the first night he didn't come to our room. By week 10, he was sleeping through 6 of 7 nights. The weighted blanket was the key — it was like the weight told his body it was safe. Our whole family is a different version of itself now."
Santhosh, Bangalore — Week 6
Before: 4-year-old daughter, ASD diagnosis. Woke at 2 AM every night — needed parent lying with her for 45 minutes.
After: "She started reaching for the teddy before calling me. By week 6, I watched her check her strategy cards at 2:30 AM — and then put herself back to sleep. I cried."
After: "She started reaching for the teddy before calling me. By week 6, I watched her check her strategy cards at 2:30 AM — and then put herself back to sleep. I cried."
Rashida, Pune — Week 12
Before: 8-year-old still waking twice a night. Told by multiple doctors to "just accept it."
After: "Nobody had done a sensory profile before Pinnacle. White noise + blackout + compression sleepwear addressed environmental triggers we didn't even know existed. He now sleeps through 7 of 7 nights. He's a calmer, happier child during the day too."
After: "Nobody had done a sensory profile before Pinnacle. White noise + blackout + compression sleepwear addressed environmental triggers we didn't even know existed. He now sleeps through 7 of 7 nights. He's a calmer, happier child during the day too."
Individual results may vary. Outcomes represent aggregate clinical experience from Pinnacle Network. Statistics available at pinnacleblooms.org/outcomes

You shouldn't navigate this alone. 10,000+ parents are in this with you.
WhatsApp Community
10,000+ parents navigating night waking and sleep challenges in children with developmental differences. → Join Sleep Independence Parent Group
Online Discussion Forum
Post questions, share progress, and learn from parents who are 6 weeks ahead of you. → Pinnacle Parent Forums
Local Parent Meetups
Monthly parent meetups at 70+ Pinnacle centers across India. → Find a meetup near you
Peer Mentoring
Connect with an experienced sleep parent mentor — someone who has been exactly where you are and arrived where you want to be. → Connect with a mentor
"Your experience — your data, your breakthroughs, your hard-won knowledge — helps the next family. Consider sharing your journey. You may be the story that keeps someone going at 3 AM."
Home-based intervention works best when backed by professional expertise.
Service | Lead Discipline | What They Do for D-447 | |
Sensory Profile Assessment | Occupational Therapist | Identifies exact sensory triggers driving night waking; prescribes weight and material specifications | |
Behavioral Sleep Protocol | ABA / BCBA | Designs graduated extinction or bedtime pass; token economy architecture | |
NeuroDev Evaluation | Pediatric Neurologist | Rules out sleep apnea, parasomnias, neurological factors; melatonin assessment | |
AbilityScore® Assessment | GPT-OS® Clinical Team | Full developmental profile; Sleep Independence Readiness Index baseline |
📍 Find Your Center
📱 Teleconsultation
Book a teleconsultation — available 8:30 AM to 7:00 PM
Available in 16+ languages. No travel required.
Available in 16+ languages. No travel required.
FREE Helpline
📞9100 181 181
FREE · 24×7 · 16+ languages
"Home + clinic = maximum impact." The protocol works faster and more precisely when guided by an OT who has assessed your child's specific profile.
The science behind every material on this page.
Level I — Systematic Reviews
📖PMC11506176 | Children (2024): 16 studies confirm sensory integration intervention meets evidence-based practice criteria for children with ASD across sensory, behavioral, and sleep regulation domains. Read on PubMed
📖PMC10955541 | World J Clin Cases (2024): Meta-analysis of 24 studies — sensory integration therapy effectively promotes adaptive behavior, sensory processing, and regulation outcomes. Read on PubMed
Level II — Controlled Studies
📖Padmanabha et al. | Indian Journal of Pediatrics (2019): Home-based sensory interventions with parent administration demonstrate significant outcomes in Indian pediatric population. DOI: 10.1007/s12098-018-2747-4
📖PMC9978394 | WHO/UNICEF CCD Package (2023): Multi-caregiver implementation of environmental and sensory interventions in LMIC settings demonstrates equity-accessible outcomes. Read Study
Level II — Evidence-Based Practice Classification
📖NCAEP Evidence-Based Practices Report (2020): Behavioral sleep interventions, visual supports, and extinction-based approaches classified as evidence-based for autism. View Report
📖Frontiers in Integrative Neuroscience (2020): Neurological basis for sensory processing and sleep interaction in ASD. DOI: 10.3389/fnint.2020.556660
International Bodies
WHO Nurturing Care Framework · UNICEF Early Childhood Development · AOTA — American Occupational Therapy Association · American Academy of Sleep Medicine (AASM) Pediatric Sleep Guidelines
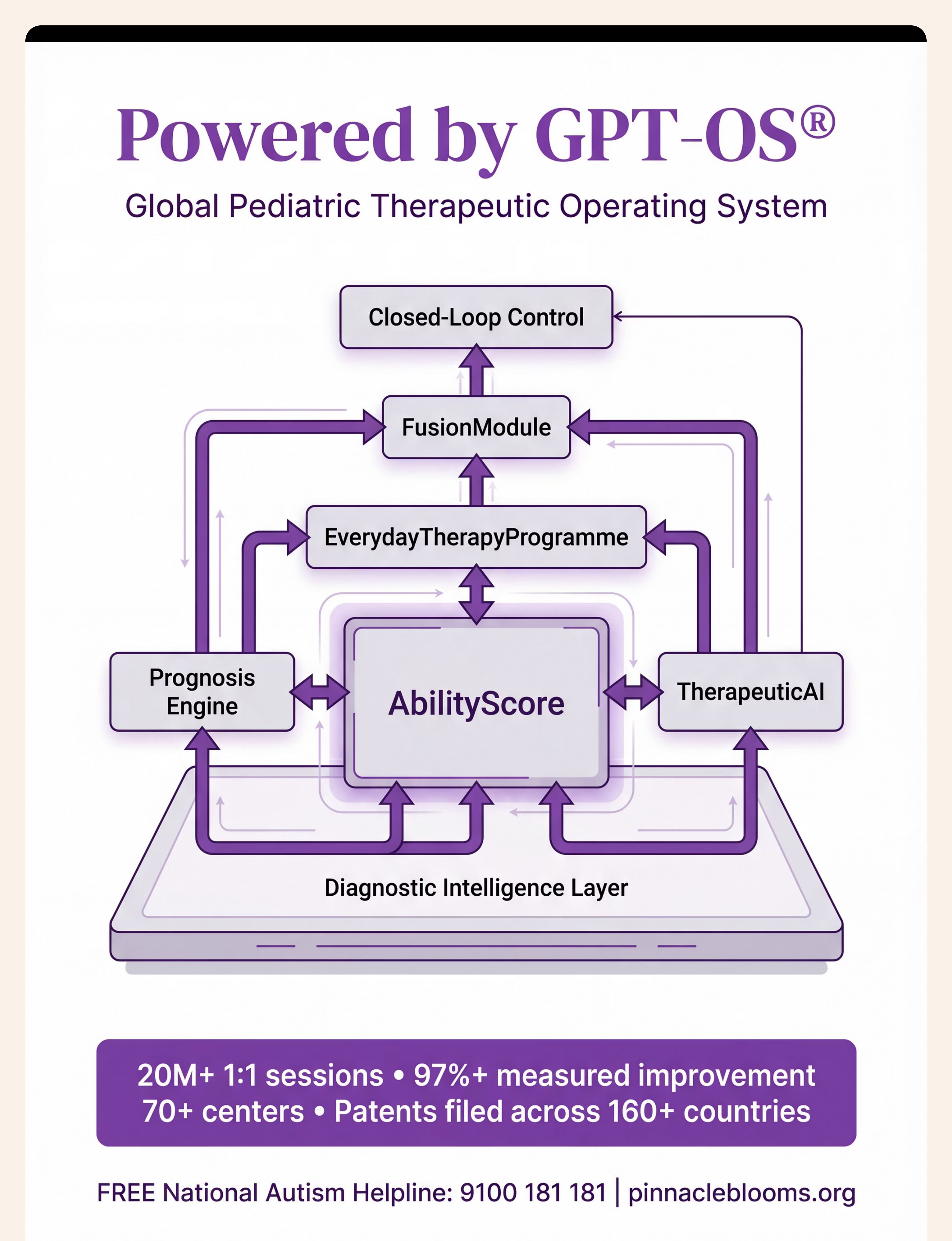
This is not software. This is therapeutic infrastructure.
Powered by GPT-OS®
What GPT-OS® Learns from Your Data
- Which material combination works for children with your child's sensory profile
- At what week improvements typically appear (to set your expectations accurately)
- When to escalate to professional intervention vs. continue home protocol
- How your child's sleep trajectory compares to 20M+ other children
Privacy Assurance
- All data is anonymized and encrypted
- No personally identifying information shared
- Population-level insights only in research outputs
- DPIIT DIPP8651 compliant data practices
"Your child's data — anonymized and protected — contributes to the most comprehensive pediatric sleep intervention dataset in India."
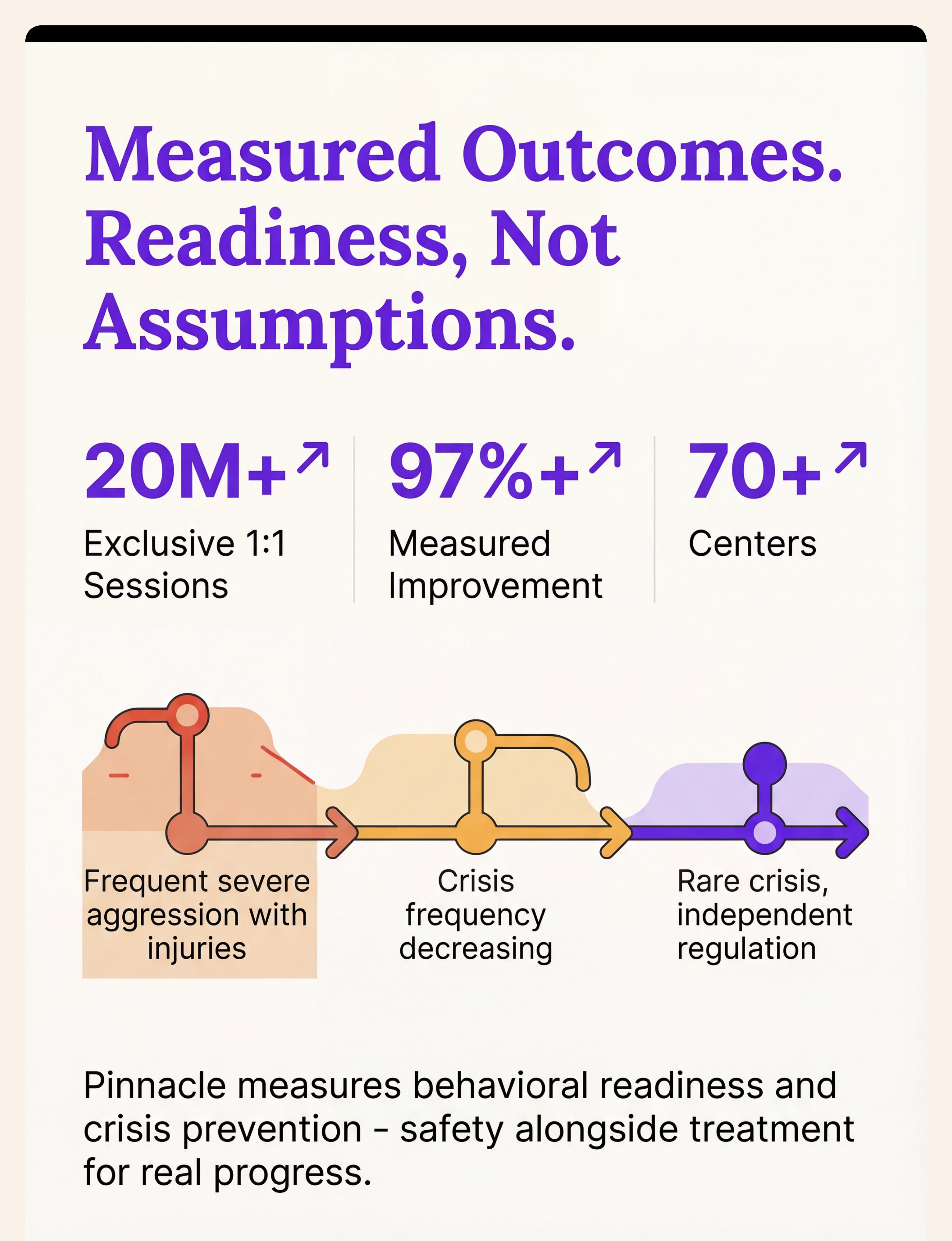
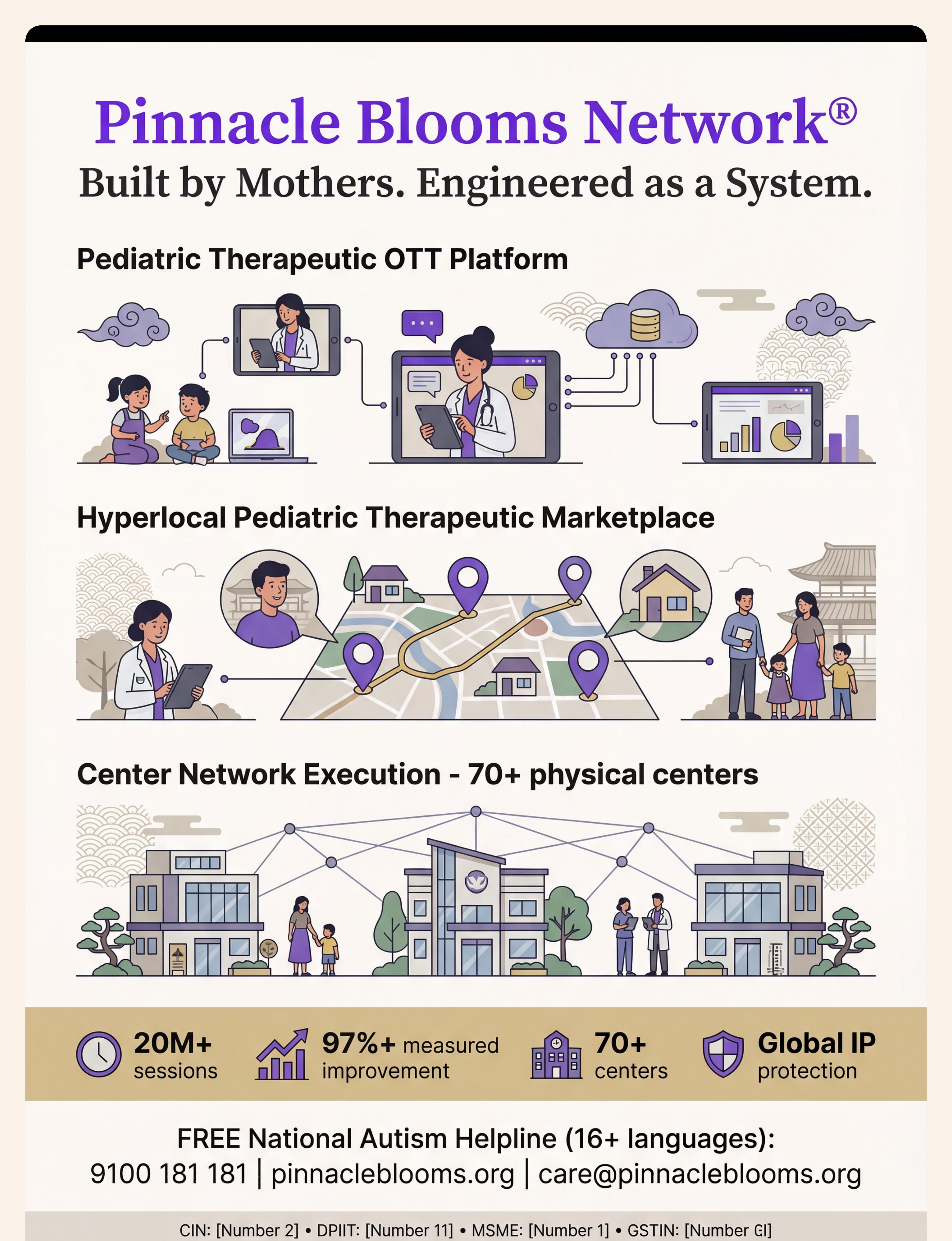
20M+
Exclusive 1:1 Sessions
97%+
Measured Improvement
70+
Centers Across India
160+
Countries — Patents Filed
Everything families ask. Answered by the consortium.
❓ How heavy should the weighted blanket be?
The clinical guideline is 10% of the child's body weight — for a 20 kg child, that's 2 kg. Never exceed 10% + 1 kg. Always verify weight on a kitchen scale. The blanket must be sized to cover the body only — not hang off the bed edges.
❓ My child is 3 — is a weighted blanket safe?
Hard age cutoff: NEVER under 2 years. For ages 2–4, consult your OT first. The child MUST be able to remove the blanket independently. Many OTs recommend compression sleepwear as the safer first choice for under-5s.
❓ How long until we see results?
Environmental improvements (white noise, blackout) often show effect within week 1. Weighted blanket typically shows measurable change at 3–4 weeks. Behavioral self-soothing (strategy cards, OK-to-wake clock) shows meaningful independence at 5–8 weeks. Commit to 8 weeks before evaluating overall effectiveness.
❓ My child falls asleep fine — they just can't STAY asleep. Are these materials still relevant?
Yes — directly. Night waking is specifically about what happens at natural sleep cycle transitions (every 60–90 minutes), not sleep onset. If your child falls asleep but can't stay asleep or self-soothe back, all 9 materials on this page are specifically designed for this pattern.
❓ We tried white noise before and it didn't help. Should we try again?
Most common failure reasons: (1) it was on a timer and turned off mid-night, (2) volume too low, (3) wrong noise type. True white noise must run all night at consistent volume (50–65 dB), positioned across the room. A new trial with these specifics is warranted.
❓ Can I use all 9 materials at once?
We recommend phased introduction: Start with 3-material environmental core (white noise + blackout + night light) for 1 week. Add 1–2 sensory materials in Week 2. Add behavioral tools in Week 3. Introducing everything simultaneously makes it impossible to know what's working — and can overwhelm a sensory-sensitive child.
❓ When do I call a professional instead of continuing home protocol?
Call 9100 181 181 or book a teleconsultation if: (1) No improvement after 6 weeks of consistent implementation, (2) You observe snoring, gasping, or unusual movements during sleep, (3) Night waking suddenly started or significantly worsened, (4) Child is showing signs of significant daytime impairment or behavioral regression.
Preview of 9 materials that help with night waking Therapy Material
Below is a visual preview of 9 materials that help with night waking therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.








Link copied!

Your child can sleep through the night.
The science is clear. The tools are ready. The only step left is yours.
🚀 Start This Technique Today
Launch GPT-OS® guided D-447 session — your personalized night waking protocol begins now.
📞 Book a Consultation
Speak with a Pinnacle OT or BCBA about your child's specific sleep profile. First session from ₹0 with Helpline.
→ Next: D-448 Early Morning Waking
Sleeping through — but waking at 5 AM? The next technique is ready.
📞FREE National Helpline: 9100 181 181 — 24×7 | 16+ languages | No appointment needed | India's most trusted pediatric developmental support line
🏛️Validated by the Pinnacle Blooms Consortium® | OT • SLP • ABA/BCBA • SpEd • NeuroDev Pediatrics • CRO | Multi-disciplinary review. Evidence-graded. Parent-tested.
Pinnacle Blooms Network® | "From fear to mastery. One technique at a time." | 70+ centers · 20M+ sessions · 97%+ measured improvement · 70 countries served
Medical Disclaimer: This content is educational and does not replace individualized assessment with licensed occupational therapists, behavioral specialists, and healthcare professionals. Persistent night waking may indicate underlying sleep disorders requiring professional evaluation. Individual results may vary. If your child is in distress or you are concerned about safety, contact your pediatrician or emergency services.
CIN U74999TG2016PTC113063 | DPIIT DIPP8651 | MSME TS20F0009606 | GSTIN 36AAGCB9722P1Z2 | © 2025–2026 Pinnacle Blooms Network®, a unit of Bharath Healthcare Laboratories Pvt. Ltd. | Technique D-447 | care@pinnacleblooms.org | pinnacleblooms.org