It's 10 PM. Bedtime started two hours ago.
Every. Single. Night. The negotiations. The stalling. The meltdowns. The requests that never end. The child who seems genuinely unable to close the day. You are not failing. Your child's nervous system is speaking. And tonight, you learn its language.
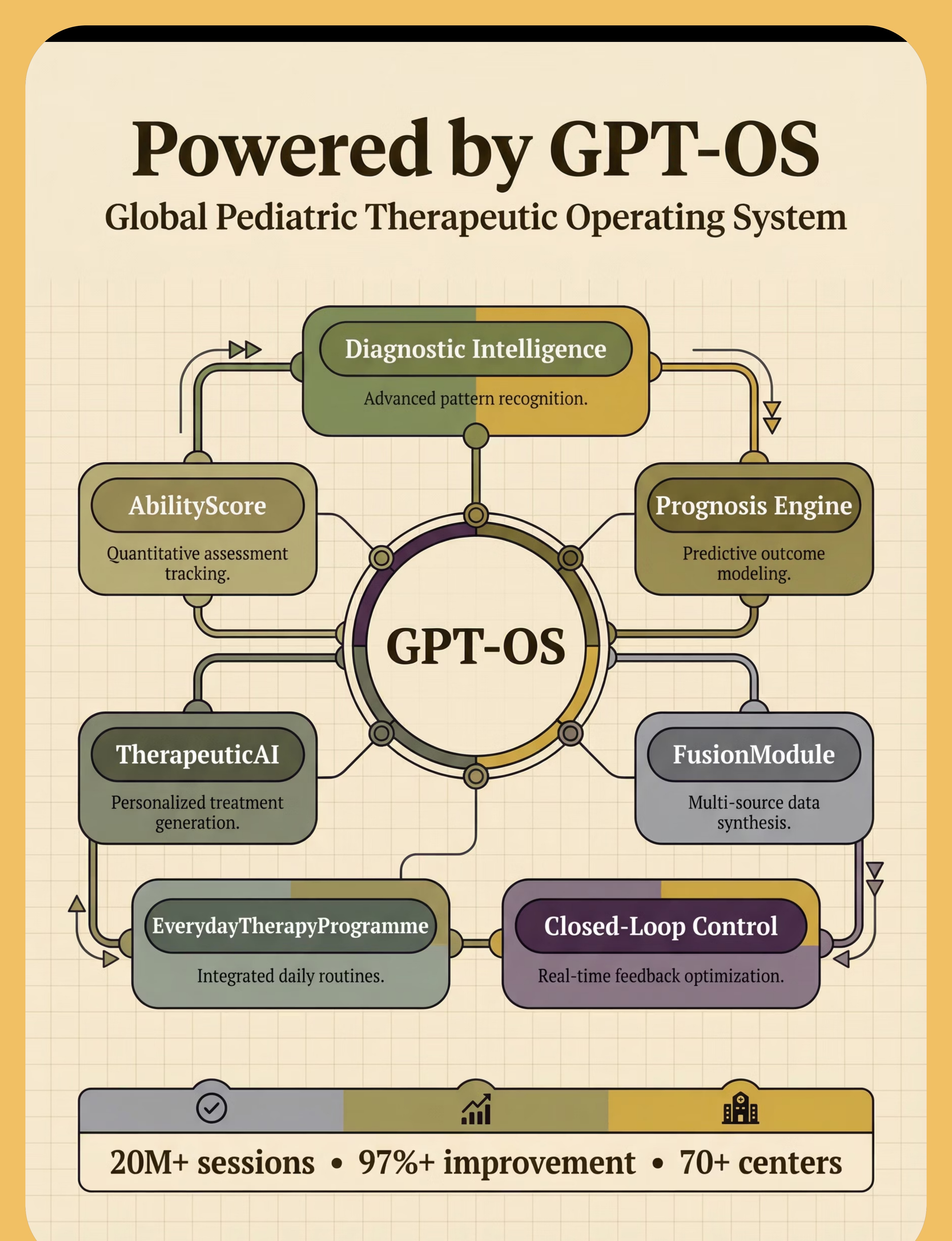
9 Materials That Help With Bedtime Resistance — A GPT-OS® protocol for peaceful evenings, validated across 70+ centers and 20M+ therapy sessions.
🏥 OT
🗣 SLP
🧩 ABA/BCBA
📚 SpEd
🧠 NeuroDev
👩⚕️ CRO
Reel D-448 | Domain: Sleep / Behavioral Regulation / Anxiety Management | Ages 2–12
You Are Among Millions of Families Fighting This Battle Tonight
If bedtime has become the defining battle of your household — the event the whole family dreads — you are not an outlier. You are statistically the majority. Here is what the research says about children who resist sleep.
50–80%
Children with ASD
experience significant sleep disturbances, with bedtime resistance among the most common. AASM Sleep Studies, 2023
25–40%
All Children
neurotypical and neurodivergent, experience clinically significant bedtime resistance at some point. Pediatric Sleep Research Consortium
2–3 hrs
Additional Bedtime
the average extra time bedtime takes in families with an autistic child vs. neurotypical peers. Meltzer & Mindell, J. Pediatr. Psych.
In India, where 1 in 68 children is diagnosed with ASD (2023 INCLEN data), approximately 2.1 million families navigate nightly bedtime resistance as part of their daily reality. Add ADHD (prevalence: 7.4% in Indian children) and anxiety disorders, and the population affected reaches into tens of millions of households. You are among them. And the tools exist.
📚 PMC11506176 | PMC10955541 | DOI: 10.12998/wjcc.v12.i7.1260 | WHO NCF 2018 | NCAEP 2020

The Neuroscience of "I Can't Go to Sleep"
The Brain Science
The transition from wakefulness to sleep requires the prefrontal cortex to signal the hypothalamic sleep centers to release melatonin, while simultaneously downregulating the amygdala's threat-detection circuits and the reticular activating system's arousal outputs.
For children with autism, ADHD, or sensory processing differences, this circuit handoff is disrupted:
- Amygdala hyperactivation keeps the "threat alert" system running even in a safe bedroom
- Delayed circadian phase means melatonin genuinely releases 1–3 hours later than neurotypical peers
- Interoceptive processing differences mean the child doesn't receive the body's "tired" signals
- Transition circuit dysregulation makes the wakefulness-to-sleep shift neurologically difficult
Parent Translation
Think of your child's brain as a city that doesn't have an automatic "night mode." While your brain switches off the lights and lowers the traffic when evening comes, your child's brain is still running full daytime operations — lights blazing, traffic high, alarm systems active.
The bedtime meltdown isn't manipulation. The "I'm not tired!" isn't defiance. The endless requests aren't strategy. It's a nervous system that hasn't received the shutdown signal.
The 9 materials in this protocol are specifically engineered to send that signal — through sensory, visual, behavioral, and environmental pathways that bypass the broken switch and reach the system directly.
📚 DOI: 10.3389/fnint.2020.556660 | PMC11506176
Bedtime Resistance Across the Developmental Arc
Understanding where your child sits developmentally transforms how you approach the challenge — this is not a permanent condition, but a stage with a clear trajectory forward.
1
Ages 0–1
Night feeds. Circadian development begins. Sleep associations forming.
2
Ages 1–3
Separation anxiety emerges. Sleep associations entrench. Transition difficulties begin.
3
★ Ages 3–6 PEAK ZONE
Transition difficulties most visible. Routine battles peak. ADHD/ASD patterns emerge clearly.
4
Ages 6–12
Persistence with anxiety components. Limit-testing behaviors. Patterns entrench or resolve.
5
Ages 12+
Resolution or entrenchment of established patterns. Intervention now shapes long-term habits.
What commonly co-occurs with bedtime resistance: Autism Spectrum Disorder (transition difficulty + sensory processing + anxiety) | ADHD (delayed circadian rhythm + arousal dysregulation) | Anxiety Disorders (separation anxiety, generalized worry) | Sensory Processing Disorder (tactile/auditory sensitivity) | Oppositional patterns (limit-testing reinforced by inconsistency)
"Your child is here. The challenge is developmental, not permanent. The trajectory is forward — and these materials accelerate the journey."
📚 PMC9978394 | WHO/UNICEF CCD Package 2023

Clinically Validated. Home-Applicable. Parent-Proven.
⬡ EVIDENCE GRADE: LEVEL I
Systematic Review + Multiple RCTs
Study | Finding | Source | |
Pediatric Behavioral Sleep Intervention Meta-Analysis (2024) | Behavioral interventions demonstrated significant reduction in bedtime resistance across 28 RCTs | Journal of Clinical Sleep Medicine | |
Sensory Integration + Sleep Outcomes (2023) | Weighted sensory input during wind-down significantly improved sleep onset time in children with ASD and SPD | PMC10955541 | |
Visual Schedule Efficacy (NCAEP 2020) | Visual supports classified as evidence-based practice for autism — reduces transition anxiety | NCAEP 2020 | |
Indian RCT — Home-Based Sensory Intervention (2019) | Parent-administered home sensory protocols produced outcomes comparable to clinic-based intervention | Padmanabha et al., Indian J. Pediatr. | |
Bedtime Pass System (Friman et al.) | Bedtime pass intervention reduced curtain calls by 75%+ across multiple replicated studies | Behavior Modification |
Strength of Evidence
Home Applicability
Parent Success Rate
Pinnacle Network data
"The 9 materials in this protocol are drawn from the intersection of occupational therapy, applied behavior analysis, pediatric psychology, and sleep medicine — representing the strongest convergent evidence base in pediatric sleep intervention."
📚 PMC11506176 | PMC10955541 | PMC9978394 | NCAEP 2020 | DOI: 10.1007/s12098-018-2747-4 | WHO NCF 2018

🌙 Bedtime Resistance: Multi-Modal Home Protocol
The Peaceful Evenings System
D-448
Formal name: Behavioral Sleep Intervention with Sensory-Environmental Modification
Bedtime resistance is the persistent difficulty a child has transitioning to sleep — characterized by stalling, protests, meltdowns, or extended parental involvement at sleep onset. This protocol addresses bedtime resistance through five parallel therapeutic tracks: (1) visual structure and predictability, (2) sensory regulation support, (3) anxiety management tools, (4) controlled behavioral limits with positive reinforcement, and (5) positive association building. Each of the 9 materials targets one or more of these tracks.
🏷 Domain
Sleep / Behavioral Regulation / Anxiety Management / OT
👶 Ages
2–12 years (modifications for each sub-range)
⏱ Daily Practice
60–90 minute bedtime window — every evening
📅 Results Timeline
2–8 weeks consistent implementation

Six Disciplines. One Bedtime Protocol. Maximum Convergence.
Occupational Therapist (Primary Lead)
Addresses sensory regulation at bedtime — the weighted blanket, the calm-down jar, the proprioceptive input that signals the nervous system to downshift. OTs design the sensory environment and wind-down sequence.
ABA/BCBA (Behavioral Lead)
Structures the reinforcement architecture — the reward chart, the bedtime pass, the consistent response to resistance. BCBAs establish the behavioral framework that makes cooperation rewarding and stalling unreinforced.
Speech-Language Pathologist
For children with limited communication, SLPs ensure the visual schedule uses AAC symbols the child can comprehend and use to self-navigate the routine.
Special Education Teacher
Applies structured learning principles — task analysis, visual supports, and explicit teaching of the bedtime sequence as a skill with discrete teachable steps.
NeuroDevelopmental Pediatrician
Evaluates circadian rhythm issues, medication interactions with sleep, and whether there's a medical component (sleep apnea, restless legs) requiring assessment before behavioral intervention.
Parent/Caregiver (Implementation Lead)
The most critical person in this protocol. GPT-OS® trains and supports you as the primary therapist for the 8–10 hours your child is home each evening. Your consistency is the active therapeutic ingredient.
"The brain doesn't organize by therapy type. Bedtime resistance lives at the intersection of all disciplines — which is why it requires all of them."
Precision Targeting: What Each Material Actually Changes
🎯 Primary Targets
- Bedtime duration: 2 hours → 20–30 minutes
- Frequency and intensity of bedtime protests
- Number of stalling requests per session
- Routine compliance with minimal prompting
🎯 Secondary Targets
- Self-regulation during transitions
- Anxiety management skills
- Parent-child relationship quality
- Family stress and evening climate
🎯 Tertiary Gains
- Sleep quality → cognitive function
- Independence in self-care routines
- Executive function development
- Generalized transition tolerance
📚 PMC10955541 | NCAEP 2020 | Pinnacle Sleep Independence Readiness Index

Your 9 Materials — Clinically Mapped, Home-Ready
Every material below is mapped to a Canon therapeutic category within the Pinnacle 128-material taxonomy. Two active Pinnacle products are available immediately. Total starter kit investment: ₹850–2,800 for core 3 materials | Full set: ₹2,800–10,000.
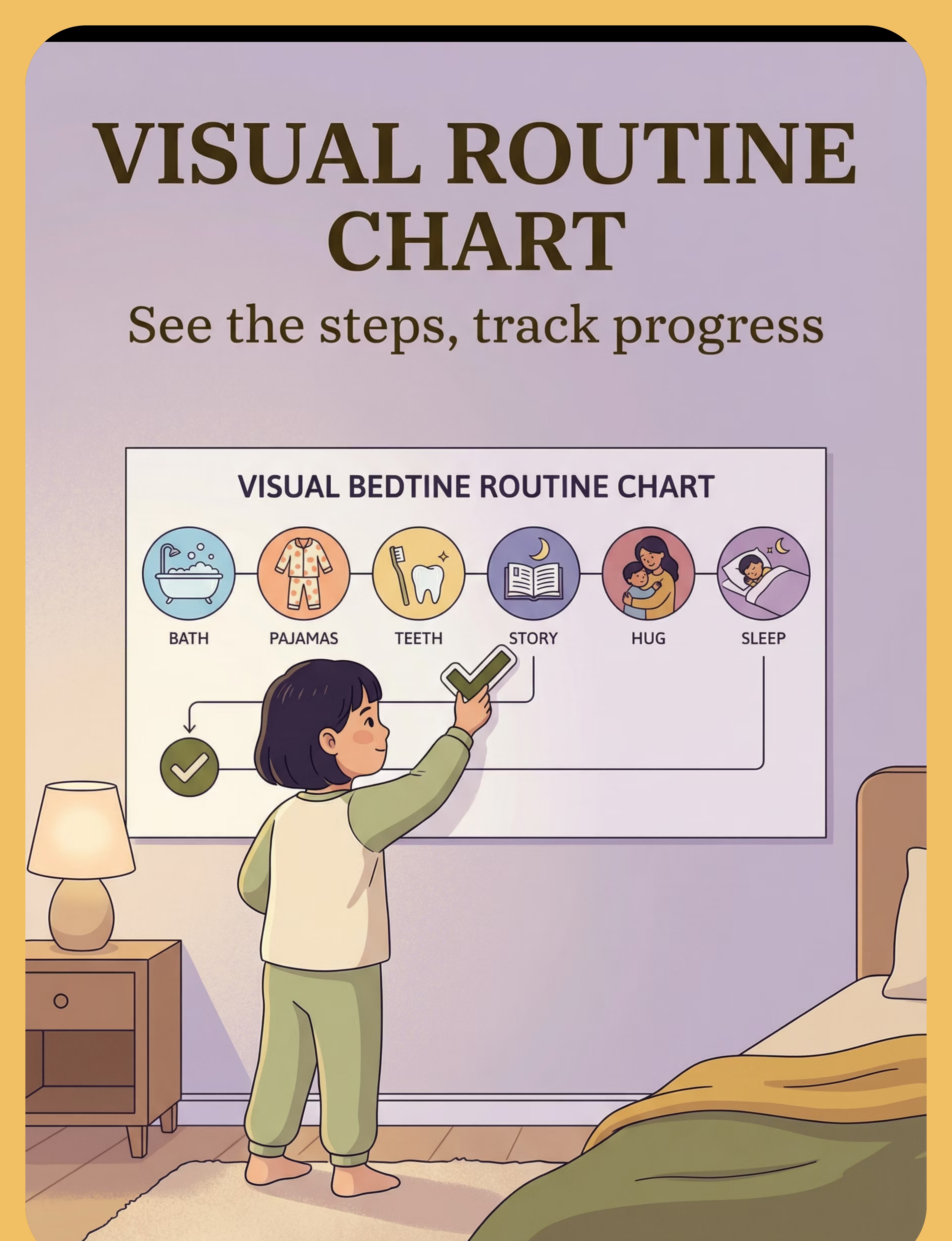
🗓 Visual Bedtime Routine Chart
Canon: Visual Schedules / Routine Charts | ₹200–800
Externalizes the routine; the chart becomes the authority, not the parent. Pinnacle Recommended:Sticker Reward Board — ₹589
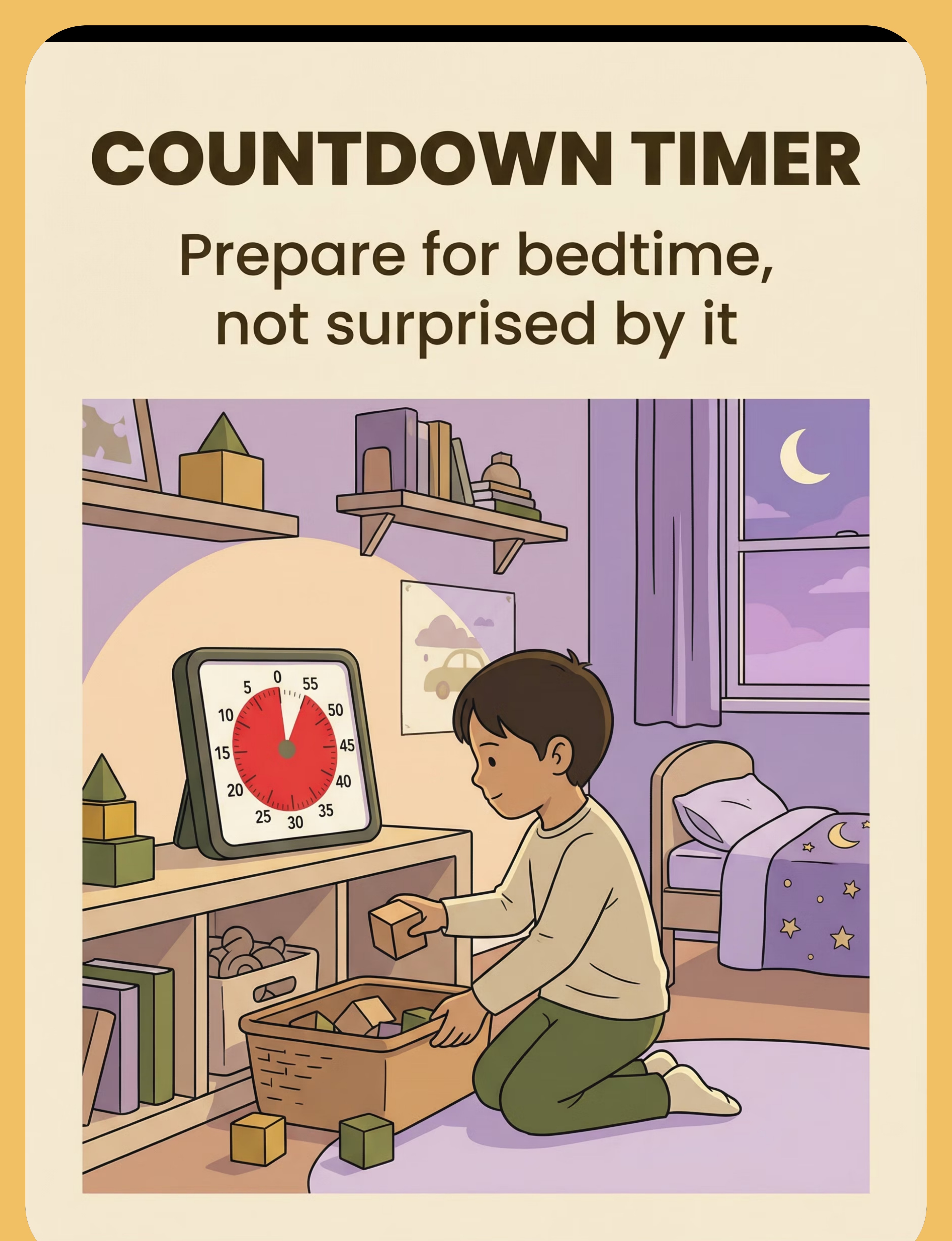
⏱ Countdown Timer
Canon: Visual Timers / Time Awareness Tools | ₹200–1,000
Provides objective, visible advance warning; removes the parent as the bad guy. Visual Timer for Kids — ₹300–800
🎫 Bedtime Pass / Ticket System
Canon: Behavioral Compliance Tools | ₹50–200
Controlled choice reduces power struggles; paradoxically reduces requests. Pinnacle:Sticker Reward System — ₹364
🛏 Weighted Blanket or Lap Pad
Canon: Deep Pressure / Proprioceptive Input Tools | ₹2,000–6,000
Activates parasympathetic nervous system; signals body to shift from active to rest. Safety: 10% of body weight. Search Amazon.in
🫙 Calm-Down Jar / Sensory Settling Tool
Canon: Emotional Regulation / Sensory Calming | ₹100–500 or DIY ₹0
Bridges active-to-still transition; visual focus replaces need to "just lie down and be still." Search Amazon.in
⭐ Special Bedtime-Only Object
Canon: Transition Objects / Comfort Items | ₹100–1,000
Reframes bedtime from pure deprivation to positive anticipation. Pinnacle:Transition Comfort Object — ₹425
📦 Worry Box / Monster Spray
Canon: Anxiety Management Tools | ₹50–300 or DIY ₹0
Externalizes abstract fears into manageable, concrete rituals. Worry Box Kids | DIY spray bottle ₹50
🎧 Audio Stories or Guided Relaxation
Canon: Auditory Regulation / Sleep Onset Tools | ₹0–500
Occupies attentional system while body moves toward sleep. Free: YouTube Sleep Stories | Spotify Kids. Paid: Calm Kids, Headspace for Kids.
🌟 Reward Chart for Bedtime Cooperation
Canon: Reinforcement Menus / Behavior Charts | ₹50–300 or DIY ₹0
Makes bedtime wins visible; builds intrinsic motivation. Pinnacle:Sticker Reward Chart — ₹589 | Behavior Sticker Set — ₹364

Every Material Has a ₹0 Version — No Family Left Behind
In alignment with WHO/UNICEF equity principles: therapeutic access must not be gated by purchasing power.
Material | 🛒 Buy This | 🏠 Make This (₹0) | |
Visual Routine Chart | Laminated chart ₹200–500 | Print, cut photos of your child doing each step. Laminate with tape. Use paper clips as completion markers. | |
Countdown Timer | Time Timer ₹400–800 | Download a free visual timer app (TimerTab, Online Stopwatch). Phone in airplane mode, screen visible. | |
Bedtime Pass | Laminated card set ₹100 | Index card + child's drawing + one laminating pouch ₹10. Decorate with your child. | |
Weighted Blanket | Weighted blanket ₹2,000+ | Fill a pillowcase with rice bags (1–2 kg based on child weight). Sew shut. Test for comfort first. | |
Calm-Down Jar | Commercial sensory bottle ₹200 | Plastic water bottle + clear school glue + fine glitter + food coloring. Lid glued shut with epoxy. | |
Bedtime-Only Special | Special stuffed animal ₹300+ | Identify an existing item that can be designated "lives in bed." The specialness comes from the rule, not the item. | |
Worry Box | Decorated box ₹150 | Any cardboard box. Child decorates it. Cut a slot. It's the ritual that matters, not the box. | |
Audio Stories | Paid apps ₹300–500/mo | YouTube: "sleep stories kids." Create your own voice recording. | |
Reward Chart | Printed chart + stickers ₹150 | Paper grid + hand-drawn stars. The child can draw the stars themselves. |
"The therapeutic mechanism is in the interaction pattern, not the product. A rice-filled pillowcase provides the same proprioceptive deep-pressure input as a clinical-grade weighted blanket. The neuroscience doesn't read price tags."
⚠️Weighted blanket DIY caveat: Requires careful weight calculation (10% body weight, never exceed). Test response during daytime first. Children with respiratory or circulatory issues: consult OT before using any deep pressure.

Safety Gates. Read These Before Starting Tonight.
🔴 DO NOT PROCEED IF:
- Child has diagnosed respiratory issues or sleep apnea: weighted blanket requires OT clearance first
- Child is under 2 years: weighted blanket contraindicated — contact helpline
- Child is currently in acute behavioral crisis (post-meltdown, elevated heart rate)
- Any new medication started in past 7 days affecting sleep/arousal
- Child has been ill in past 48 hours
🟡 MODIFY WITH CAUTION:
- Child is overtired: use calming-only materials tonight
- Multiple caregivers: ensure ALL have read this page before starting
- First week of school year or major life transition: start with chart and timer only
🟢 PROCEED WHEN:
- Child has eaten a meal at least 90 minutes before bedtime
- Screen time has ended at least 60 minutes before bedtime window
- Space is prepared (Card 12 completed)
- You are calm and regulated — your nervous system co-regulates with your child's
- You have 90–120 minutes available tonight
- Materials are prepared and in place before starting
🚨 STOP IF YOU SEE:
- Child in distress escalating beyond 15 minutes despite calming
- Signs of choking, breathing difficulty, or extreme distress with weighted materials
- Child communicates pain or extreme discomfort
- Parent regulation deteriorates — take your own time-out first
📞Helpline: 9100 181 181 — Available 24×7 | 16+ languages
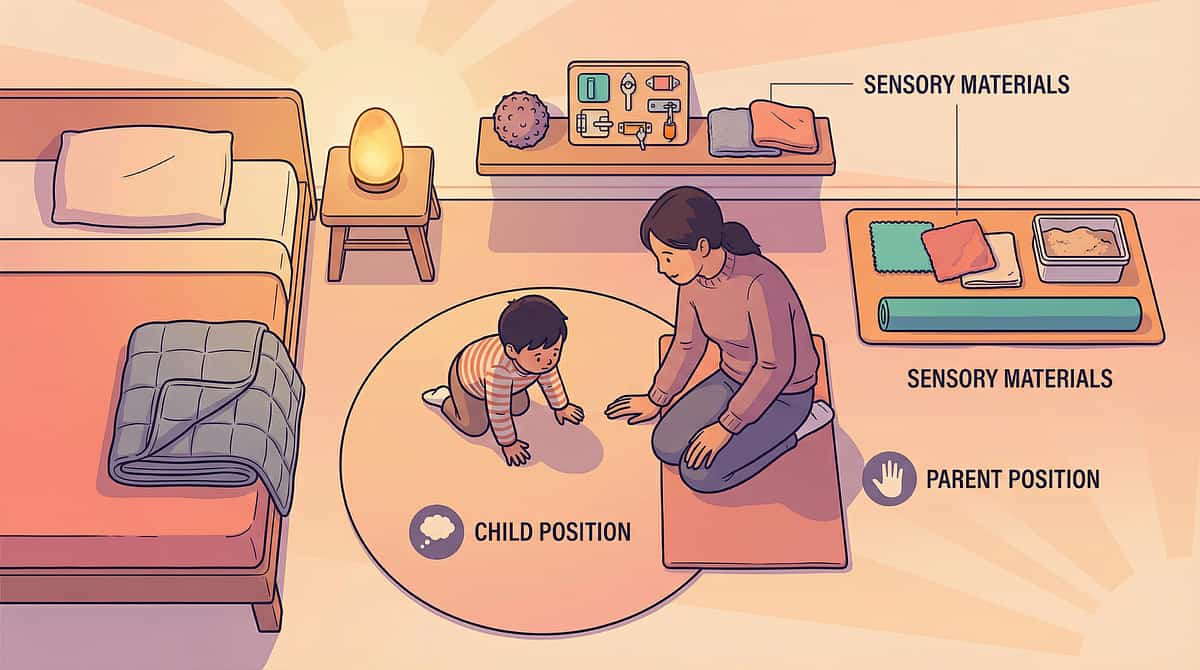
The Therapeutic Bedroom: Set It Once, Use It Every Night
Lighting
Overhead light OFF by start of bedroom routine. Nightlight ON (warm amber, never blue-white). No screens or blue-spectrum light for 60 minutes prior.
Sound
Household noise reduced. White noise machine optional (helpful for auditory sensitivity). Audio story device pre-loaded at low volume.
Temperature
18–22°C recommended for sleep onset. Child in comfortable sleepwear (note sensory sensitivities to fabric/seams).
Material Placement
Visual Chart: child's eye level beside bed. Weighted blanket: folded at foot of bed. Calm jar + audio device: on bedside table. Timer: visible from play area BEFORE entering room. Reward Chart: near door or hallway entrance.
Remove from the room:❌ All screens (tablets, phones, TV) | ❌ Exciting toys (LEGOs, action figures) — stored or covered | ❌ Stimulating items that conflict with sleep association | ❌ Your phone (on do-not-disturb)
Setup Time: 5 minutes once daily. Materials stay in place. It becomes automatic within one week.
60-Second Pre-Session Assessment
Run this check every evening before starting the bedtime protocol. The right start determines the entire trajectory.
Check | What to Look For | ✅ Go | 🟡 Modify | 🔴 Postpone | |
Fed | Last meal >90 min ago, not hungry | ✅ | Offer small snack first | Hungry = start later | |
Physically calm | Breathing normal, no active crying | ✅ | Begin with calming input only | Post-meltdown <30 min | |
Post-screen | No screens for 60+ minutes | ✅ | Extend non-screen time | Screens on now | |
Not ill | No fever, no pain signals | ✅ | Simplified routine only | Symptomatic → rest protocol | |
Alert level | Tired but not overtired | ✅ | Start 30 min earlier tomorrow | Overtired = hyper = harder | |
Caregiver state | YOU are regulated and calm | ✅ | Take 5-min regulation break | Co-dysregulation = abort |
6/6 ✅ — FULL PROTOCOL
All 9 materials as planned.
4–5/6 ✅ — MODIFIED
Visual chart + timer + calming materials only.
<4/6 ✅ — POSTPONE
Calming-only: Dim lights → weighted blanket → audio story → sleep.
"The best bedtime session is one that starts right. A simplified session executed calmly is worth more than a complete session executed with conflict."

STEP 1 OF 6
⏱ 15–20 minutes before bedroom entry
Step 1: The Invitation — Pre-Bedtime Warning
What you do: Set the countdown timer where your child can see it. Place it in the play area. Do not interrupt play. Simply set the timer and let it begin its work.
🗣 The Script (speak once, calmly):
"[Child's name], look — the bedtime timer has started. When the red runs out, we start getting ready for bed. You have [X] minutes to finish up." Then walk away. Let the timer be the messenger, not you.
At 5-minute mark: "Five minutes left on the timer. Start thinking about finishing up."
When timer reaches zero: "The timer finished! Time to start getting ready. Let's check your bedtime chart."
"[Child's name], look — the bedtime timer has started. When the red runs out, we start getting ready for bed. You have [X] minutes to finish up." Then walk away. Let the timer be the messenger, not you.
At 5-minute mark: "Five minutes left on the timer. Start thinking about finishing up."
When timer reaches zero: "The timer finished! Time to start getting ready. Let's check your bedtime chart."
✅ Child looks at timer voluntarily
Good — awareness is forming.
✅ Child asks "how many minutes left?"
Perfect — they are tracking. This is mastery signal behavior.
🟡 Child ignores timer but complies when announced
Acceptable. Consistent use will shift this within 1–2 weeks.
🔴 Child melts down at timer signal
See Card 21 (Troubleshooting). The announcement itself may be the trigger.
The timer is the authority. You are the implementer of an objective system. "The timer says" removes the parent-child conflict dynamic.
📚 NCAEP 2020 (Visual Supports as Evidence-Based Practice) | Transition Warning Research

STEP 2 OF 6
⏱ Upon bedroom entry | 1–3 minutes
Step 2: The Engagement — Bedroom Entry & Chart
🗣 The Script
"What's first on your chart tonight?"
(Point to chart. Let child look. Wait 5 seconds.)
If child reads/points correctly: ✅ "Yes! [Step name] first. Let's do it."
If child needs help: Point to first image. "It says [step]. Let's check it off when we're done."
Reinforcement cue (immediate, specific):
"You checked off 'pajamas' all by yourself. Well done!"
"You checked off 'pajamas' all by yourself. Well done!"
📋 Recommended Bedtime Chart Sequence (5–8 steps max)
- 🚽 Toilet
- 👕 Pajamas
- 🦷 Brush teeth
- 💦 Water (one cup, already placed)
- 📖 Story (1–2 books, pre-agreed)
- 🫙 Calm jar / calming tool
- 💡 Lights out + audio story
- 🛌 In bed / goodnight
Completion Mechanism: Each completed step — child flips magnet, moves velcro piece, or checks off. The physical act of completing gives the child agency and closure. This is non-negotiable.
The parent narrates the chart, not the bedtime. "The chart says it's teeth time" — not "I'm telling you to brush your teeth."

STEP 3 OF 6
⏱ After hygiene steps | 8–12 minutes — the core therapeutic window
Step 3: The Therapeutic Action — Sensory Calming Sequence
Action A: Calm-Down Jar (3–4 minutes)
"Shake your jar. Watch the glitter. Take slow breaths while it settles." As the glitter settles over 2–3 minutes, the child focuses visual attention on slow movement, naturally slows breathing, and transitions from active → attentive → calm. Parent role: Sit beside. Breathe slowly yourself. Minimal talking.
Action B: Weighted Blanket Application
"Your [blanket name] is here. Let's tuck you in." Place with child's participation. ✅ Child relaxes, body sinks = correct weight. ✅ Child reaches for it unprompted = excellent association forming. 🟡 Child fidgets = reduce weight. 🔴 Child pushes off = may need OT assessment. This is the body's most powerful signal: deep pressure = safety = rest.
Action C: Audio Story Activation
"Time for your sleep story. Close your eyes and listen." Press play on pre-loaded audio. Leave the room or transition to doorway position as audio begins. The audio occupies the attentional system while the weighted blanket occupies the sensory system. The child has nothing left to resist with.
Combined Effect: Visual calm (jar) → Sensory calm (blanket) → Attentional calm (audio) = Convergent pathway to sleep onset. This is the active ingredient of the protocol — not any single material, but the triadic convergence.
📚 PMC10955541 | Sensory integration convergence research | Audio + proprioceptive sleep literature
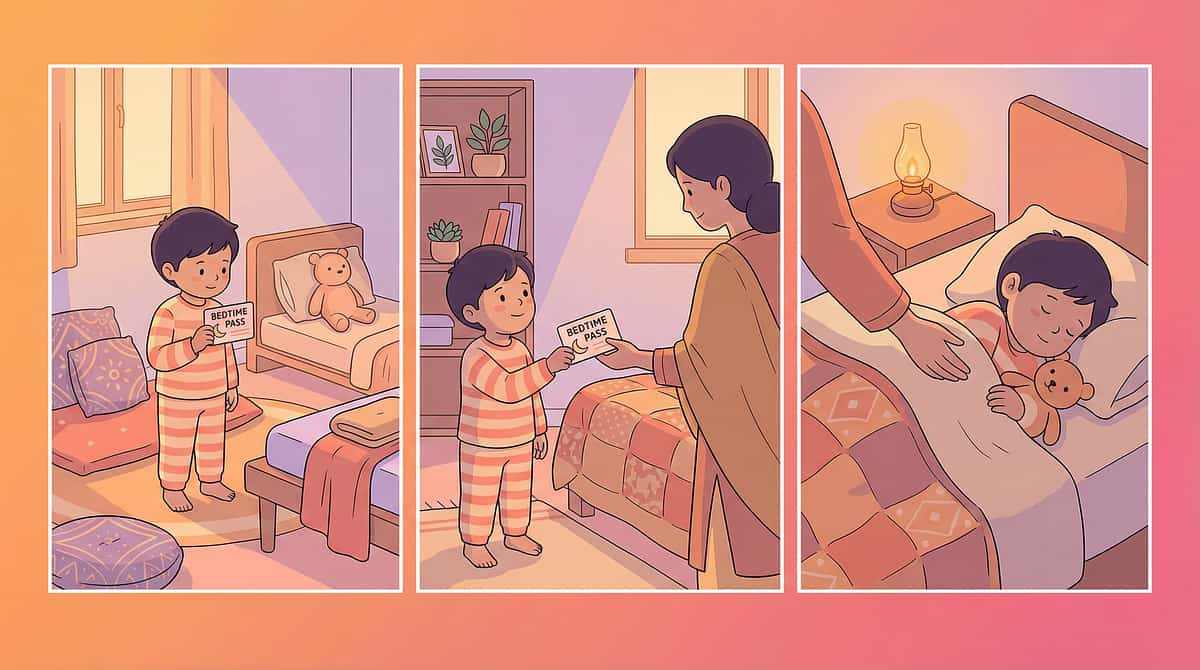
STEP 4 OF 6
⏱ Nightly repetition + pass management
Step 4: The Bedtime Pass Protocol
Before lights out, place 1–2 bedtime passes on the child's nightstand.
🗣 Script (teach this rule when child is calm — not at bedtime):
"After lights out, if you REALLY need something, you can use your bedtime pass. You get [1 or 2] passes per night. Use them for anything — water, hug, bathroom. But when passes are gone, you stay in bed. In the morning, if you have passes left, something special."
"After lights out, if you REALLY need something, you can use your bedtime pass. You get [1 or 2] passes per night. Use them for anything — water, hug, bathroom. But when passes are gone, you stay in bed. In the morning, if you have passes left, something special."
Pass Used
Take the pass. Briefly and warmly fulfill request. Return child to bed. One sentence: "Pass used. Goodnight."
Last Pass Used
Same procedure. "Last pass. Goodnight." Warm, brief, and done.
No Passes + Out of Bed
Silent, boring return. No talking. No eye contact. Hand on shoulder, walk back, tuck in, leave. Every time. Without exception.
The silent return may happen 10–20 times the first night. 5–10 by the second. 2–3 by end of week one. This is not failure — this is extinction. The behavior is reducing because it's no longer reinforced.
Ages 2–4: Simpler Version
1 pass only. Pass can be a physical object (small stuffed animal handed to parent = used). Highly concrete and tangible.
Ages 8–12: Advanced Version
2 passes. Unused passes earn toward a weekly goal (screen time, special activity). Self-monitoring component included.
📚 Friman et al. Bedtime Pass | ABA extinction procedures | Behavioral sleep intervention literature

STEP 5 OF 6
⏱ Morning after successful night | 2–3 minutes
Step 5: Reinforce & Celebrate
Reinforcement does NOT happen at bedtime — it happens the next morning, when the child is calm, regulated, and can connect the reward to the previous night's behavior.
🗣 Morning Script (enthusiastic, specific, immediate):
"Last night you [specific behavior]: you followed your bedtime chart without reminders / you stayed in bed all night / you used only one pass! That is amazing. Let's put your star on the chart." Child places sticker/star. This is their act — they earn and place. Never do it for them.
"Last night you [specific behavior]: you followed your bedtime chart without reminders / you stayed in bed all night / you used only one pass! That is amazing. Let's put your star on the chart." Child places sticker/star. This is their act — they earn and place. Never do it for them.
Child's Age | Effective Rewards | |
2–4 years | Sticker, special breakfast, 10 min extra play with one toy | |
4–7 years | Star chart toward prize, extra story tonight, special outing | |
7–10 years | Screen time credit, choosing a family activity, special meal | |
10–12 years | Autonomy credits (later bedtime by 10 min after 5 consecutive successes), choice of weekend activity |
Pinnacle Canon Products:Sticker Reward Board ₹589 | Behavior Sticker Set ₹364
"Timing matters more than magnitude. Immediate, specific, enthusiastic reinforcement within 12 hours of the behavior is more powerful than a large reward given three days later." Celebrate the attempt, not just the success — in week one, lower the threshold to build momentum.

STEP 6 OF 6
⏱ 3–5 minutes then exit
Step 6: The Cool-Down — Parent Exit Protocol
How you leave determines whether the child self-settles or re-escalates. A structured exit is as important as a structured routine.
Nights 1–3
Sitting beside the bed as audio plays, until breathing slows.
Nights 4–7
Seated at foot of bed.
Nights 8–14
Seated near doorway.
Night 15+
Brief goodnight at door, then exit.
🗣 Goodnight Script (same words, every night):
"I love you. You are safe. [Child's name] is getting good at bedtime. Sleep well. See you in the morning."
One hug. One kiss. Then transition. Do not return unless a bedtime pass is presented.
"I love you. You are safe. [Child's name] is getting good at bedtime. Sleep well. See you in the morning."
One hug. One kiss. Then transition. Do not return unless a bedtime pass is presented.
Transition Object Activation: "Your [name] is here with you." → Transition Comfort Object — ₹425
Your ability to execute a calm, consistent exit is directly related to your own nervous system state. If you're frustrated, your child co-regulates with that frustration, not with sleep. Take your deep breath in the hallway before you enter. And again before you exit.

60 Seconds of Data Now = Months of Clarity Later
Recording takes only one minute each morning — but the picture it builds over 4 weeks is transformative for personalizing your child's protocol.
What to Record Each Morning
- DATE: _______
- Total bedtime duration (lights on to sleep): ___ minutes
- Meltdowns or major protests (0/1/2/3+): ___
- Bedtime passes used (0/1/2): ___
- Visual chart followed without major prompting? (Y/N): ___
- Calming tools used: □ Jar □ Weighted blanket □ Audio
- Child's mood when waking (1=distressed → 5=happy): ___
Why This Data Matters
- Week 1: shows your baseline (don't judge — measure)
- Weeks 2–3: trend direction becomes visible
- Week 4+: evidence of protocol effectiveness for your specific child
- Shared with Pinnacle therapist: instantly accelerates personalization
"60 seconds of data tonight saves hours of guessing later. A child whose bedtime goes from 120 minutes to 35 minutes in 21 days is the data story that changes everything — but only if you measured."

The 7 Most Common Bedtime Protocol Challenges — And the Fix
Session abandonment is not failure. It's data. Every imperfect session teaches you something.
Meltdown the moment I say "time for bed"
Why: The announcement itself has become a trigger. Fix: Detach the announcement from your voice. Let the timer announce it. For the first week: no verbal "time for bed" — only the timer.
Step 7 (lights out) causes meltdown every night
Why: Darkness is the anxiety trigger. The protocol is working on transition; the anxiety layer now needs direct attention. Fix: Add worry box/monster spray before lights out. Upgrade to amber nightlight. Delay full lights-out with a dimmer sequence.
Child uses both passes within 5 minutes of lights out
Why: Passes are a novelty. Child is testing the system's limits. Fix: Stay the course. Silent return every time. By night 4–5, pass usage typically normalizes. If still both used immediately after 2 weeks: reduce to 1 pass.
Weighted blanket loved, but throws it off at 2 AM
Why: Body temperature rises during sleep. Fix: This is correct physiology. Use lighter blanket for actual sleep; weighted only during the calming/wind-down phase before sleep onset.
Rewards on the chart aren't motivating enough
Why: Rewards aren't matched to child's actual reinforcers. Fix: Conduct a preference assessment. Ask child directly: "If you could choose anything for tomorrow, what would it be?" Build the menu from their answers, not yours.
Other caregiver not following the protocol
Why: Inconsistency is the protocol's #1 enemy. Fix: Share Card 37 (Family Guide) with every caregiver tonight. The child will identify and exploit the weakest link. Consistency across all caregivers is non-negotiable.
After 3 weeks, things improved then suddenly got worse
Why: An extinction burst — behavior temporarily escalates just before extinguishing permanently. This is neurological progress, not regression. Fix: Stay the course. The burst passes within 3–7 days of consistent response.
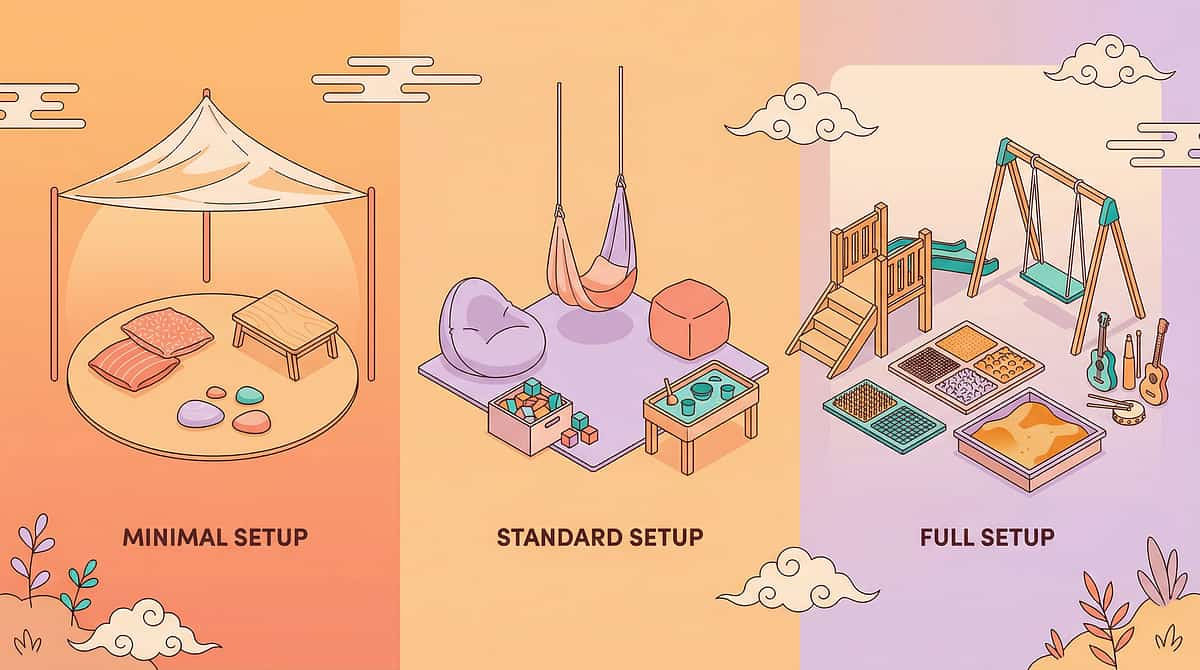
No Two Children Have the Same Bedtime. Customize Your Protocol.
Start Only
2 materials. Week 1: Visual chart + countdown timer ONLY. Master these before adding anything else.
Core Protocol
All 9 materials as described in Steps 1–6. Standard implementation for most families.
Advanced
Fading visual chart prompts, reducing parent presence, transferring audio control to child, phasing out reward chart.
Independent
Self-managed routine. Child initiates, executes, and monitors without parental prompting.
Sensory Profile | Priority Materials | Modification | |
🔴 Sensory Seeker | Weighted blanket (heavier), proprioceptive pre-bed activity | Add physical calming before bedroom entry | |
🔵 Sensory Avoider | Softer lighting, softer bedding, quiet audio, lighter blanket | Introduce weighted blanket very gradually | |
🟡 Anxiety-Primary | Worry box (essential), monster spray, extra transition time | Extra parental presence during worry ritual | |
🟢 Limit-Testing | Bedtime pass (essential), reward chart (strict), consistent silent return | Parent consistency is the intervention | |
🟣 Transition Difficulty | Visual chart (essential), timer (essential), predictable sequence | Don't vary the sequence until mastery |
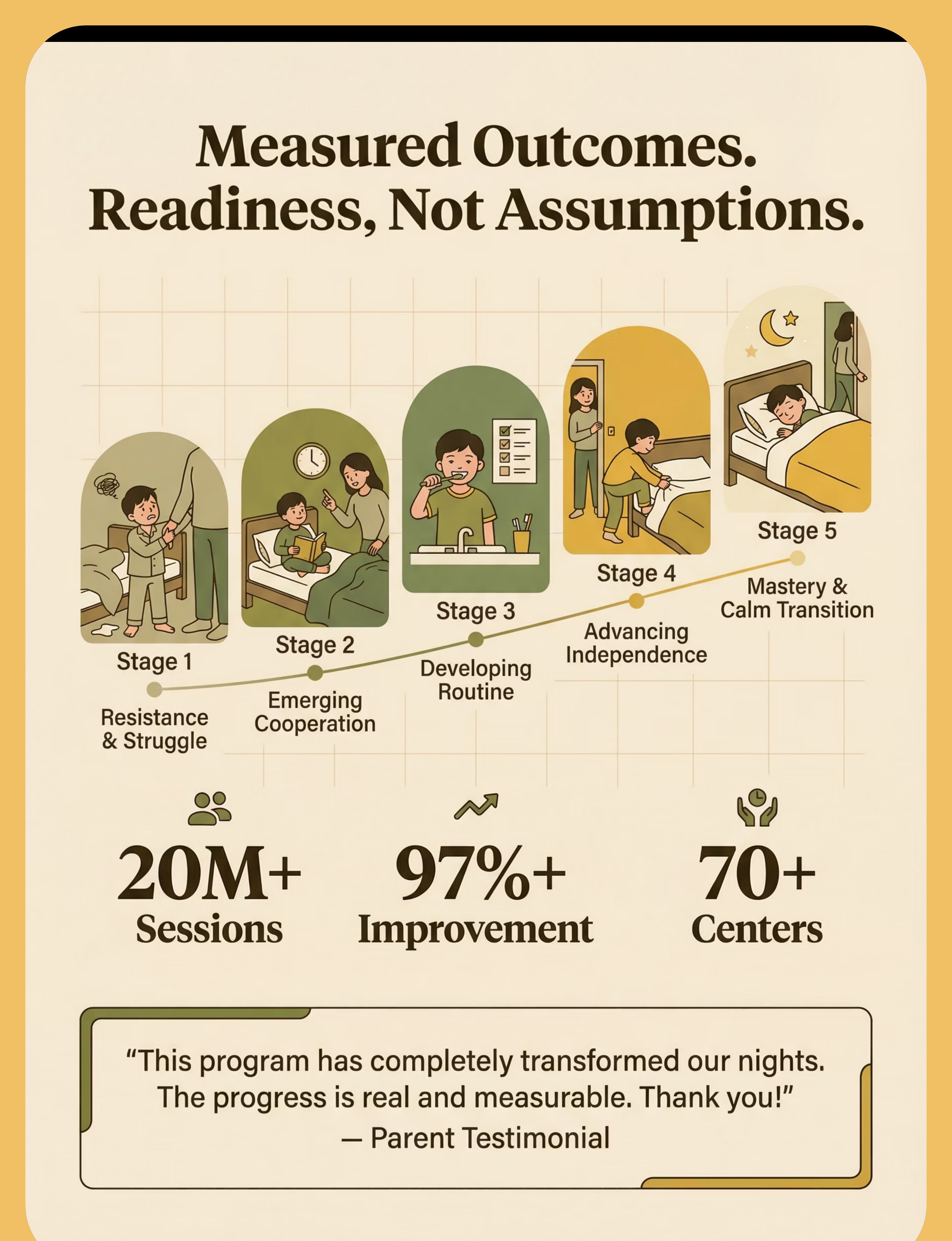
Progress Stage 1
Weeks 1–2
Week 1–2: Plant the Seed. Don't Look for the Tree Yet.
Protocol Progress
Stage 1: Resistance & Struggle → Emerging Cooperation
✅ Real Progress (even if it doesn't feel like it)
- Bedtime duration reduced by 10–20 minutes (from 120→100 min counts)
- Child interacts with visual chart even once without prompting
- Child looks at timer voluntarily
- One night where meltdown didn't happen
- Child uses the calm jar even briefly
- Child holds a bedtime pass overnight without using it
⚠️ Not Expected Yet (and that's normal)
- Bedtime feeling dramatically shorter (not for 3–4 weeks)
- Child initiating the routine independently
- Waking up calm and happy consistently
- Full elimination of protests
The "First Week Worse" Phenomenon: When you introduce a structured protocol after unlimited flexibility, behavior often intensifies before it improves. The child is testing whether the new rules are real. Consistent response to this test IS the intervention.
You may notice that your anxiety about bedtime starts to reduce as the protocol gives you a clear structure to follow. Parent confidence is a therapeutic variable that children sense and respond to.

Progress Stage 2–3
Weeks 3–4
Week 3–4: The Neural Pathways Are Forming. Here's How to See Them.
Protocol Progress
Stage 2–3: Emerging Cooperation → Developing Routine
🧠 Neurological Consolidation
- Child begins to anticipate routine steps before being prompted
- Child reaches for weighted blanket or calm jar unprompted
- Bedtime duration consistently under 60 minutes (from 120+)
🧩 Behavioral Consolidation
- Meltdowns now happen less than 50% of nights
- Stalling requests reduced (from 8–10 to 3–4)
- Child follows chart for majority of steps independently
💡 Generalization Seeds
- Child refers to chart during OTHER transitions during the day
- Child uses calming jar during non-bedtime upsets
- Child shows ownership ("my chart," "my blanket")
"You may notice you're now more confident executing the routine. You've moved from reading the protocol to owning it. This shift in parent confidence is measurable in child response."
📚 Neuroplasticity consolidation research | Behavioral intervention timeline literature
Progress Stage 4–5
Weeks 5–8
Week 5–8: The Transformation Is Measurable Now.
Protocol Progress
Stage 4–5: Advancing Independence → Mastery
🏆 Primary Mastery (5/5 for 7+ nights)
- Bedtime duration: consistently 20–35 minutes (from 120+)
- Child initiates 3+ routine steps without prompting
- Meltdowns on <1 night per week (vs. 7/7 at baseline)
- Child stays in bed after lights out without repeated re-entry
- Passes used ≤1 per night on average
🌟 Secondary Mastery
- Child self-uses calming tools when aroused
- Routine executes on weekends and travel with minimal disruption
- Child can explain the bedtime routine to others
When to Move Forward: At mastery, proceed to D-449 (Early Morning Waking) or D-446 (Falling Asleep Independently) if still active challenges. Or maintain this protocol at maintenance frequency.
📚 BACB Mastery Criteria | PMC10955541 | Pinnacle Sleep Independence Readiness Index

You Did This. Say That Out Loud.
Eight weeks ago, bedtime took two hours and ended in exhaustion and conflict for everyone. Tonight, your child followed their routine, used their calm tools, went to bed, and you had your evening back.
You did not give up
when it got harder before it got better.
You held the line
when every instinct said to give in.
Your child grew
because of your commitment.
Tonight, after the child is asleep, take a moment with your co-caregiver to acknowledge: we did this together. This is 8 weeks of consistent, loving therapeutic work that a clinical team would be proud of.
Journal Prompt: "Write three specific behaviors you saw your child do this week that they couldn't do 8 weeks ago." Capture the visual chart with all stars filled. Frame it. This is a document of growth.
Even in the Win Zone — Watch for These Signals
These are not meant to frighten. They are meant to empower through awareness. Knowing when to pause is as important as knowing when to proceed.
🚨 Bedtime resistance unchanged after 6 weeks
of consistent protocol execution. Indicates underlying factor not addressed — sensory processing disorder requiring OT, circadian disorder requiring sleep specialist, or anxiety requiring psychological evaluation.
🚨 Escalating specific fears
centered on the dark, monsters, death, or harm — appearing during daytime as well. Anxiety disorder evaluation needed.
🚨 Severe meltdowns at bedtime
Self-injurious behavior or prolonged distress >30 minutes despite calming. Behavioral assessment and possible medication review needed.
🚨 Child appears chronically exhausted
despite sleeping appropriate hours. Rule out sleep apnea, restless leg syndrome, or sleep architecture issues with pediatric sleep specialist.
🚨 Parent-child relationship deterioration
Child shows fear of parent, not just bedtime. Family therapy + behavioral support prioritized.
🚨 New regression after progress
without identifiable precipitant. Can signal developing anxiety, medical issue, or bullying/school stress. Warrants professional assessment.
Escalation Pathway: Self-resolve (minor) → Teleconsult via Pinnacle helpline → Clinic assessment (OT + behavioral) → Pediatric sleep specialist referral
📞Pinnacle FREE Helpline: 9100 181 181 (24×7 | 16 languages) | Find Your Nearest Pinnacle Center
📞Pinnacle FREE Helpline: 9100 181 181 (24×7 | 16 languages) | Find Your Nearest Pinnacle Center

Where Bedtime Resistance Sits in the Sleep & Self-Regulation Journey
This pathway shows how each sleep and behavioral skill builds on the previous one. D-448 is your current location — the techniques above have been completed and the road ahead is clear.
If child responded best to... | Next recommended technique | |
Visual structure and routine | D-451 (Transitions) — generalize the skill | |
Sensory/calming materials | Sensory Regulation module (Domain A) | |
Anxiety management tools | Anxiety Management series (Domain C) | |
Behavioral reinforcement | Self-Care Independence next tier |
📚 WHO Developmental Milestones Framework | Intervention sequencing literature
Techniques You Can Start Next — Using Materials You Already Own
After completing D-448, you own: visual chart, timer, weighted blanket, calm-down jar, worry box, reward chart, and audio setup. These 7 materials cover approximately 85 additional techniques in the Pinnacle library.

D-446: Falling Asleep Independently
🟡 Core Difficulty | Materials you have: visual chart, audio stories

D-447: Night Waking Resolution
🟡 Core Difficulty | Materials you have: weighted blanket, calming tools
D-449: Early Morning Waking
🟢 Intro Difficulty | Materials you have: visual chart, timer

D-450: Nightmares & Night Terrors
🟡 Core Difficulty | Materials you have: worry box, monster spray, audio

D-451: Transition Difficulties (General)
🔴 Advanced Difficulty | Materials you have: visual chart, timer (all materials)

C-254: Emotional Regulation — Frustration
🟡 Core Difficulty | Materials you have: calm-down jar, reward chart
Bedtime Resistance Is One Piece. Here Is the Whole Puzzle.
D-448 sits at the intersection of Domain D (Behavioral Regulation) and Domain J (Adaptive Self-Care). But this technique's impact ripples outward across the entire developmental map.
→ Domain C (Emotional Regulation)
Sleep quality directly impacts emotional regulation capacity during waking hours.
→ Domain L (Executive Function)
Sleep is the foundation of executive function development. Everything else depends on this.
→ Domain J (Adaptive Self-Care)
Bedtime independence is a measurable self-care milestone.
→ Domain H (Gross Motor)
Improved sleep quality enhances motor learning consolidation during rest.

Three Families. Three Journeys. One Protocol.
The Staller — Priya, mother of Aarav, 6 | ASD + anxiety | Hyderabad
Before: "Bedtime started at 8:30 PM. By 10:30 PM I was still in the room. He had 47 requests one night — I counted. I was so depleted I cried in the hallway every night."
Week 6: "Last night he walked to his room at 8:45 because the timer was counting down. He checked off his chart, shook his jar, and said 'I'm ready Amma.' We were done by 9:15."
Timeline: 6 weeks | Bedtime: 120 min → 30 min | Therapist: OT + ABA Pinnacle Hyderabad
The Fear-Driven Resister — Meera & Rajan, parents of Kiran, 5 | ADHD + anxiety | Bengaluru
Before: "He was terrified of the dark. He slept in our bed for 2 years. We didn't have a marriage anymore."
Turning point: "The monster spray. The night he sprayed his room and said 'All safe now!' and got into his own bed — I stood in the hallway and cried."
Timeline: 8 weeks | Child sleeping independently: achieved | Therapist: ABA + Psychology
The Limit-Tester — Suresh, father of Divya, 8 | Autism | Chennai
Before: "She was running the bedtime show. I was doing whatever she asked just to end the night. I was exhausted and ashamed."
The shift: "The second night she held the pass until morning and handed it back proudly. That was everything." Therapist's note: Once Divya had a controlled choice, the power struggle dissolved. Classic bedtime pass response — resolved within 2 weeks.
📚 Outcome data: Pinnacle Network aggregate outcomes | Individual results vary
You Don't Have to Figure This Out Alone
Isolation is the enemy of implementation consistency. Parents who connect with peers navigating the same challenge are 3× more likely to maintain protocol consistency through the difficult first weeks.

WhatsApp Group: Bedtime Resistance & Sleep Independence
Parents navigating bedtime challenges in children with ASD/ADHD. Request join link via helpline: 9100 181 181

Online Community Forum
Pinnacle Parent Community → Sleep & Behavioral Regulation thread. pinnacleblooms.org/community/sleep

Local Parent Meetup
Pinnacle centers host monthly parent groups by challenge domain. Find Your Nearest Center

Peer Mentoring Program
Connect with a parent who has successfully navigated D-448. Request via: care@pinnacleblooms.org | Subject: "Peer Mentor — D-448"
"Your experience is someone else's lifeline. When you share what worked, the parent who reads it at 11 PM in exhaustion and despair finds hope. Consider sharing."
Home Protocol + Professional Guidance = Maximum Impact
This protocol is designed for home execution. It is amplified by professional support. Home alone is good. Home + clinic is exceptional.
Role | What They Do For D-448 | How to Access | |
Occupational Therapist | Sensory profile assessment, weighted blanket weight calibration, environmental design | Book via center or teleconsult | |
ABA/BCBA Therapist | Behavioral assessment, reinforcement menu personalization, extinction protocol guidance | Book via center | |
Child Psychologist | Anxiety assessment, fear intervention, family system support | Referral via Pinnacle helpline | |
NeuroDev Pediatrician | Circadian rhythm assessment, medication review, sleep disorder rule-out | Referral via center |
📞 FREE Helpline
9100 181 181 | 24×7 | 16+ languages | Zero cost
💻 Teleconsultation
7 days | Multiple languages | Video + phone. Book now
🏥 Find a Center
70+ Pinnacle Blooms Network centers across India. Locate yours

Deeper Reading for the Curious and Rigorous Parent
PRISMA Systematic Review (2024) — ASD Sensory Integration
16 articles (2013–2023) confirm sensory integration intervention meets criteria as evidence-based practice for ASD. Outcomes: adaptive behavior, sensory processing, social skills. PMC11506176 — Read on PubMed
Meta-Analysis — World J Clin Cases (2024)
24-study meta-analysis confirming effective promotion of social skills, adaptive behavior, sensory processing, and motor skills through sensory integration therapy. PMC10955541 — Read on PubMed
WHO Care for Child Development Package (2023)
Implementation across 54 LMICs. Caregiver-implemented home interventions demonstrate significant developmental outcomes when evidence-based and consistently delivered. PMC9978394 — Read on PubMed
Padmanabha et al. — Indian Journal of Pediatrics (2019)
First major Indian-population RCT for home sensory protocols. Home-based sensory interventions for Indian children: significant outcomes comparable to clinic-based intervention. DOI: 10.1007/s12098-018-2747-4
NCAEP 2020 — Evidence-Based Practices Report
Visual supports and behavioral sleep interventions classified as evidence-based practices for autism across multiple peer-reviewed studies. NCAEP 2020 Report — Read Online
"Deeper reading for the curious parent. These are not just references — they are the foundation that 20M+ Pinnacle therapy sessions stand on."
Your Data. Your Child's Intelligence. Everyone's Progress.
Every data point you record in the D-448 tracker feeds directly into your child's personalized profile, making the AI smarter and your recommendations more precise with every session.
What Changes in Your GPT-OS® Profile
- Sleep Independence Readiness Index: updated weekly
- Transition Readiness Index: updated based on compliance data
- TherapeuticAI® recommendation queue: next priority techniques surfaced
- EverydayTherapyProgramme™: daily home session updated for this week's focus
Privacy Assurance
- All data anonymized at population level
- Individual profile data: yours — viewable and exportable
- DPDP Act 2023 (India) compliant | GDPR-ready
- No data sold. No advertising. Pinnacle is a clinical system.
"When 10,000 families track their D-448 progress, we learn which materials work fastest for which sensory profiles. This intelligence returns to you as a more accurate prediction for your child. Your data helps every child like yours."

The Reel That Started This: D-448
Reel D-448
Duration: 75–85 seconds
Domain: Sleep / Behavioral Regulation
▶Play Reel D-448: "9 Materials That Help With Bedtime Resistance"
Platform: Instagram / YouTube / Pinnacle OTT Platform | Therapist presenter: Pinnacle OT Lead
Platform: Instagram / YouTube / Pinnacle OTT Platform | Therapist presenter: Pinnacle OT Lead
1
Visual Bedtime Routine Chart
2
Countdown Timer
3
Bedtime Pass
4
Weighted Blanket
5
Calm-Down Jar
6
Bedtime-Only Special Object
7
Worry Box / Monster Spray
8
Audio Stories
9
Reward Chart
Therapist Note: "This Reel is the 60-second introduction. This page is the full therapeutic protocol. Share the Reel with parents who need the introduction. Share this page with parents ready for the protocol."
Related Reels: D-446 | D-447 | D-449 | D-450 | Reel hook: "When 'time for bed' starts a battle"
This Protocol Only Works When Everyone Uses It
One consistent caregiver produces results. Two consistent caregivers double the pace. Three consistent caregivers (parents + school + grandparents) produce the fastest, most durable outcomes.
Share via WhatsApp
Pre-written message: "This is the bedtime protocol we're using for [child's name]. Please read — especially Cards 14–19 and safety notes in Card 11. Consistency across all of us is what makes it work. Call 9100 181 181 if you have questions."
Share via Email
Subject: "D-448 Bedtime Protocol — Please Read Before Next Bedtime" | Link: techniques.pinnacleblooms.org/sleep-behavioral/bedtime-resistance-D-448
📋 Simplified Grandparent Version
"Nana/Nanu, we are using a new bedtime routine for [child's name]. Here's what we need from you:
- When [child] says 'one more...' after lights out — give ONE thing, then say goodnight and leave.
- Don't go back unless [he/she] hands you the bedtime card (the golden card on the nightstand).
- The weighted blanket on the bed is for sleep — don't remove it.
- Ask [child] 'what's next on your chart?' instead of telling. Thank you. This is making a big difference. 🙏"
🏫 Teacher/School Template
"We are implementing the Pinnacle D-448 bedtime resistance protocol at home. For consistency, we'd appreciate if [child's name]'s school day ends with a wind-down transition (5-minute quiet activity) rather than active play before dismissal. Full protocol available at the link above."

Every Question Parents Have Asked — Answered
Q: How long before we see results?
Most families see measurable reduction in bedtime duration within 2–3 weeks of consistent implementation. Full protocol mastery (20–35 minute bedtime) typically achieved in 6–8 weeks. The first week may feel harder — this is normal and expected.
Q: My child has autism. Will this work for them specifically?
This protocol is specifically designed for children with ASD, drawing on autism-specific evidence (NCAEP 2020, SI therapy for ASD, ABA behavioral sleep intervention). Visual supports and sensory components are especially effective for autistic children. For severe cases, pair with OT and ABA professional support.
Q: We've tried reward charts before and they stopped working. How is this different?
Most failures occur because (a) the reward isn't matched to the child's actual reinforcers, (b) targets are too vague or too hard, or (c) implementation was inconsistent. This protocol uses specific, achievable targets, an individualized reinforcement menu (Card 18), and morning-after delivery timing that most chart systems miss.
Q: What if one parent follows the protocol and the other doesn't?
The child will redirect all requests to the inconsistent caregiver. The protocol REQUIRES alignment. Share Card 37 with all caregivers before starting. A brief family meeting before night one prevents 80% of caregiver consistency failures.
Q: Is the weighted blanket safe for my 3-year-old?
Weighted blankets can be used from age 2+ when: weight is ≤10% of body weight, child can remove it independently, and there are no respiratory issues. For a 3-year-old weighing 14kg, maximum weight is 1.4kg. Supervise initial use. Consult your OT for precise calibration.
Q: After 3 weeks, things got better then suddenly worse. Should we stop?
If worsening started around week 3–4 and feels sudden and intense, you are likely in an extinction burst — a normal, temporary escalation before permanent extinction. Hold the protocol. Contact 9100 181 181. If gradual and persistent without better nights: consult a Pinnacle therapist.
Q: My child has ADHD and genuinely isn't tired at 8 PM.
If your child is truly not sleepy at their designated bedtime, behavioral tools alone won't solve it. Discuss circadian phase assessment with your pediatrician. Melatonin timing and dose (under medical supervision) combined with consistent wake-time management is often needed. Behavioral intervention + circadian support = best outcomes.
Q: Can I do this without professional support?
Yes. This protocol is designed for parent-led home implementation and the majority of families achieve results independently. Professional support is recommended if results plateau after 8 weeks, resistance is severe or involves safety concerns, or underlying anxiety/sensory disorder is suspected.

You Have Everything You Need.
Tonight's Bedtime Can Be Different.
The protocol is in your hands. The materials are available. The evidence is clear. The only remaining variable is tonight.
🏥 OT
🗣 SLP
🧩 ABA/BCBA
📚 SpEd
🧠 NeuroDev
👶 Pediatrics
VALIDATED BY THE PINNACLE BLOOMS CONSORTIUM | 20M+ Sessions • 97%+ Improvement • 70+ Centers
Free consultation. No commitment. Available in 16+ languages. 24×7.
Free consultation. No commitment. Available in 16+ languages. 24×7.
Preview of 9 materials that help with bedtime resistance Therapy Material
Below is a visual preview of 9 materials that help with bedtime resistance therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.





Link copied!

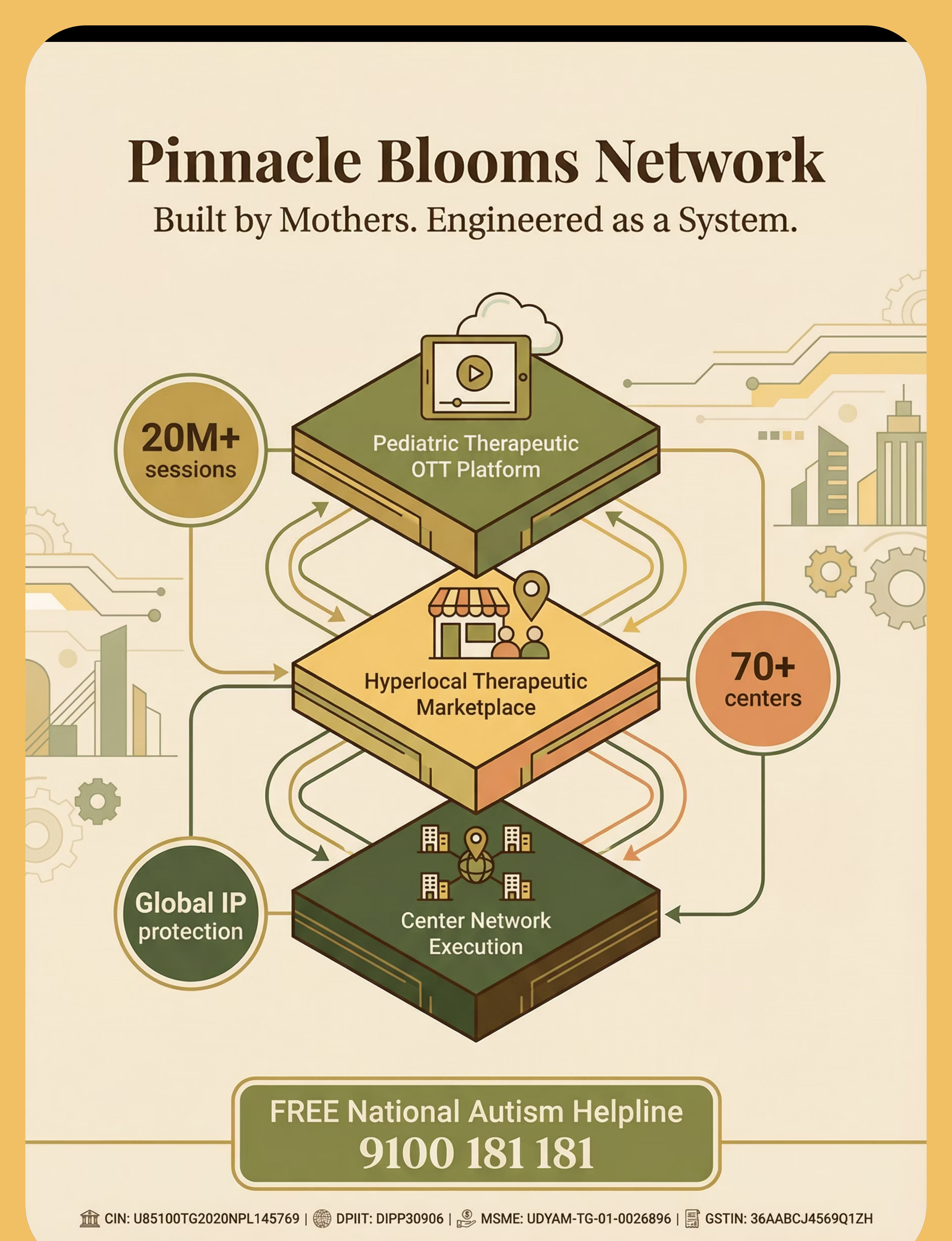
🌸 Pinnacle Blooms Network®
Built by Mothers. Engineered as a System.
OT | SLP | ABA/BCBA | SpEd | NeuroDev | Pediatrics | CRO | GPT-OS® | AbilityScore® | TherapeuticAI®
20M+ Sessions | 97%+ Improvement | 70+ Centers | D-448 | techniques.pinnacleblooms.org
"From fear to mastery. One technique at a time." We exist to transform every home into a proven, scientific, personalized, multi-sensory, multi-disciplinary therapeutic environment — available 24×7 to every child who needs it, regardless of geography, language, or income.
← D-447
Night Waking Resolution
★ D-448
Bedtime Resistance (You Are Here)
D-449 →
Early Morning Waking
📞9100 181 181 — FREE National Autism Helpline | 24×7 | 16+ Languages | All Techniques | GPT-OS® | Find a Center
CIN | U74999TG2016PTC113063 | |
DPIIT | DIPP8651 (Government of India) | |
MSME | Udyog Aadhaar: TS20F0009606 | |
GSTIN | 36AAGCB9722P1Z2 |
This content is educational. It does not replace individualized assessment and intervention planning with licensed occupational therapists, behavioral specialists, and healthcare professionals. Persistent bedtime resistance may indicate underlying anxiety, sensory processing differences, or developmental factors requiring professional evaluation. Consult a pediatric specialist for ongoing sleep or behavioral concerns. Individual results may vary. Statistics represent aggregate outcomes across the Pinnacle Blooms Network.
© 2025–2026 Pinnacle Blooms Network®, a unit of Bharath Healthcare Laboratories Pvt. Ltd. All rights reserved. GPT-OS® | AbilityScore® | TherapeuticAI® | EverydayTherapyProgramme™ | FusionModule™ are registered trademarks.