




Clinically Validated. Home-Applicable. Parent-Proven.
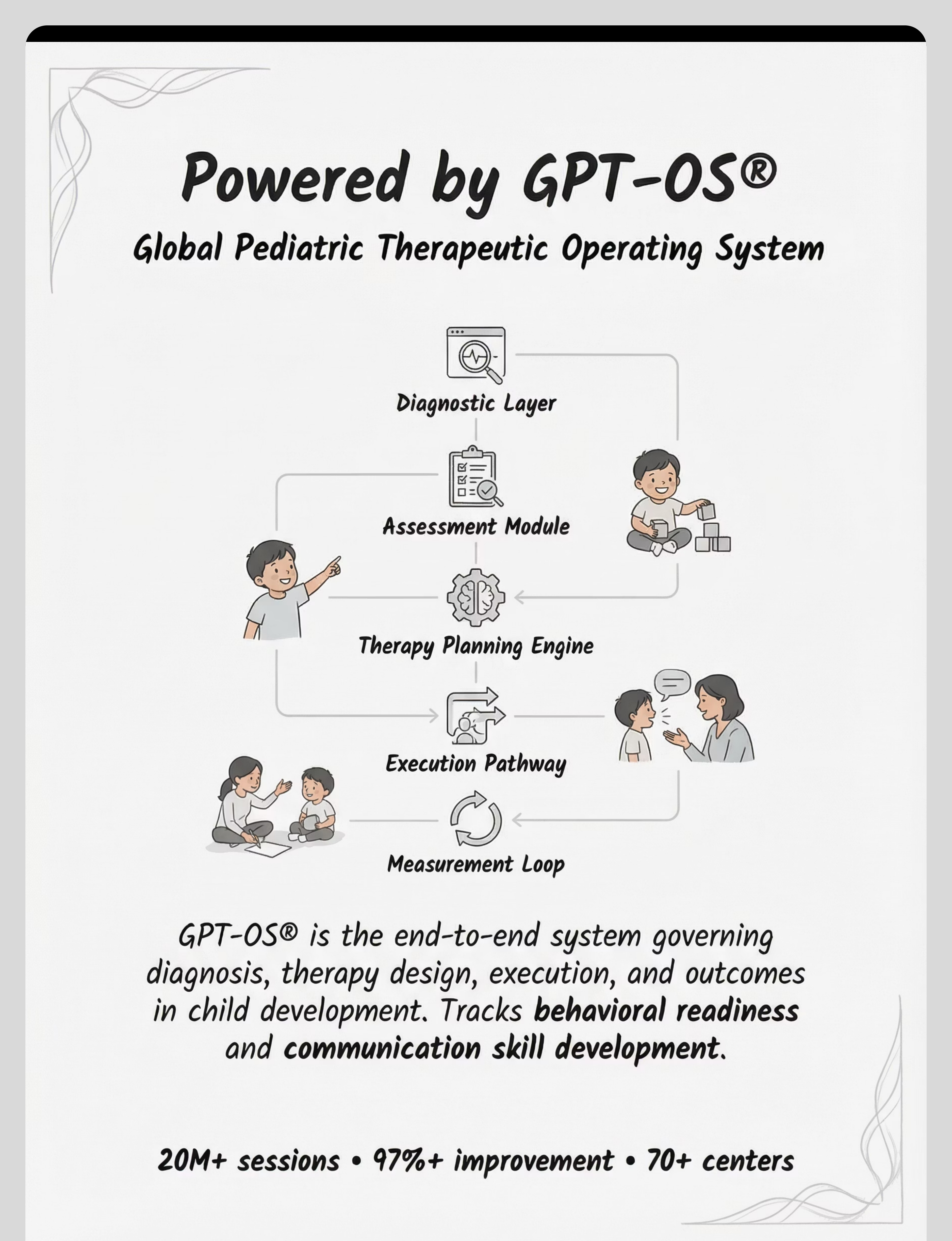
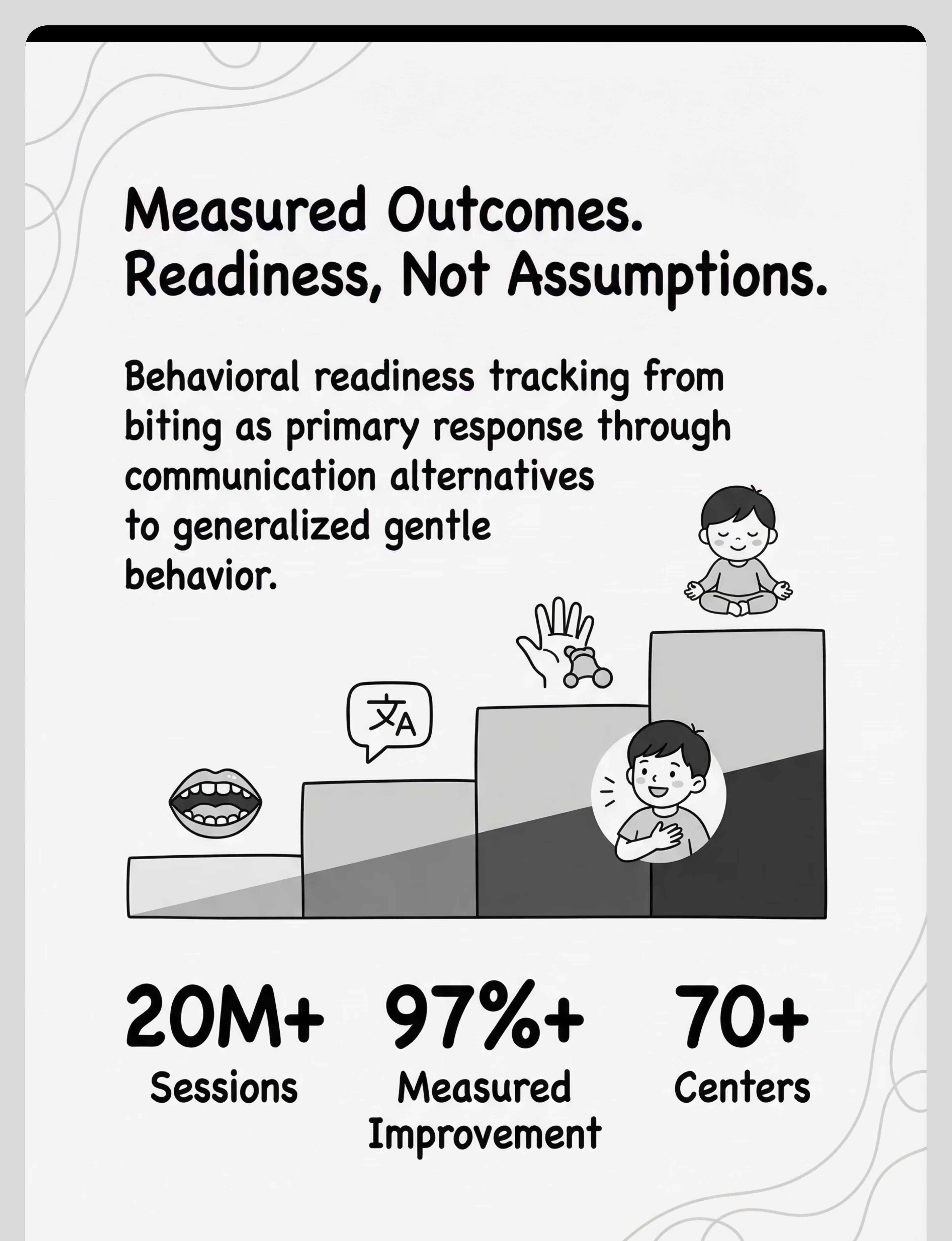
D-382 is not a collection of tips. It is a multi-layered behavioral intervention grounded in the highest levels of clinical evidence. Four landmark bodies of research form its foundation. Functional Communication Training (FCT) — Cochrane-Level Evidence FCT — replacing challenging behavior with a functional communicative equivalent — has the strongest evidence base of any behavior-analytic intervention for biting. Multiple systematic reviews confirm ≥70% reduction in target behaviors when correctly implemented. Source: Behavior Analysis in Practice + BACB literature (2023) Oral Sensory Intervention — Systematic Review (2024) 16 studies (2013–2023) confirm sensory-based oral motor interventions meet criteria as evidence-based practice for children with ASD. Chewy tools and oral motor programs show measurable reduction in oral seeking behaviors. Source: PMC11506176 | Children, 2024 Positive Behavior Support — Meta-Analysis (2024) 24 studies confirm PBS-based approaches (reinforcement systems, visual supports, environmental modification) effectively reduce biting and aggression in early childhood populations. Source: PMC10955541 | World J Clin Cases, 2024 India RCT (Padmanabha, 2019) Home-based structured interventions in Indian pediatric populations demonstrate significant behavioral outcomes when parent-administered protocols are used. Source: DOI: 10.1007/s12098-018-2747-4 | Indian Journal of Pediatrics Therapy Sessions across the Pinnacle Network Measured Improvement in behavioral readiness indexes Centers operating under GPT-OS® clinical standards

Parent-Friendly Alias: "Give the Mouth Somewhere Better to Go"














The complete D-382 intervention can be executed with ₹0 of new purchases. All you need is a frozen washcloth, handmade picture cards, a homemade story, and a paper tally chart. The clinical materials accelerate progress — but the household versions deliver the same therapeutic principle.

• Biting is causing skin-breaking injury — immediate professional consultation required
• Child shows signs of physical illness or extreme distress today
• You or caregivers are feeling overwhelmed or reactive about biting — wait until calm to implement
• Child is in active meltdown — wait for regulation before introducing materials
• Communication cards not used even with prompting after 2 weeks — consult SLP
• Chewy tube is refused consistently — consult OT for oral sensitivity evaluation
• Environment is prepared (see Space Setup card)
• All materials are assembled and accessible
• All caregivers know the plan and will respond consistently
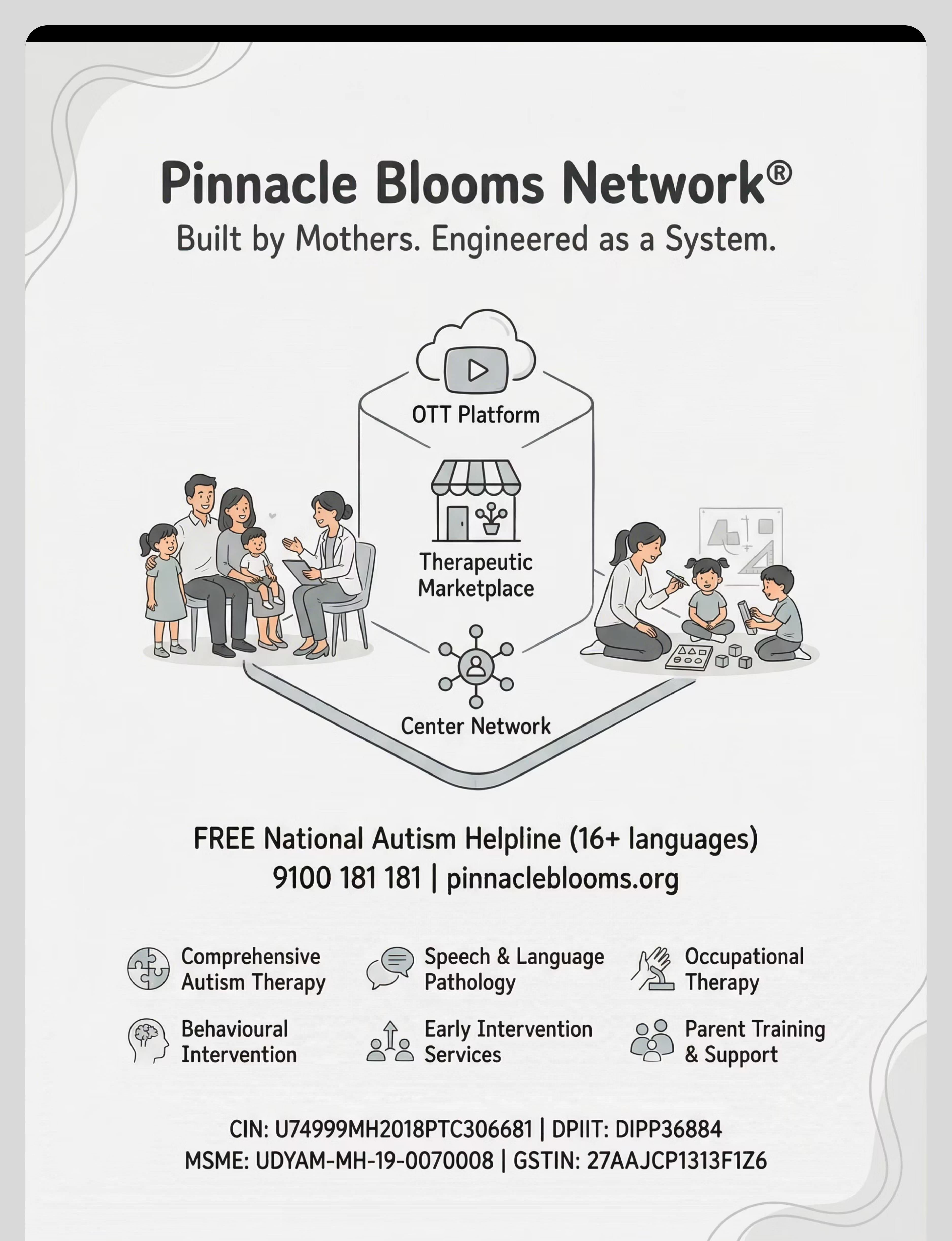
📞Questions about safety or escalation? FREE: 9100 181 181 — Pinnacle National Autism Helpline, 16+ languages, 24x7


✅ Fed | Child has eaten within the past 2 hours. Hunger amplifies frustration and biting risk significantly. | |
✅ Rested | Child is not overtired. Fatigue reduces impulse control to near-zero. | |
✅ Regulated | Child is calm or playfully engaged — not already in an elevated arousal state. | |
✅ No illness | No fever, pain, or physical discomfort today. | |
✅ No recent bite | Child has had at least 30 minutes since last biting event to re-regulate. | |
✅ Materials ready | All 9 materials are in their designated positions. | |
✅ Caregiver calm | You are feeling patient and regulated. Your nervous system is contagious. |

"[Child's name], I have something special for you. Come see."
Hold up the chewy tube or communication card with a warm, neutral expression. Crouch to child's eye level.
- Child moves toward you or the material
- Eye contact or visual attention to the material
- Body language: relaxed, curious, open
- Reaching for the object




3 quality repetitions > 10 forced ones. Therapeutic dosage for behavioral replacement is measured by function, not clock time. A child who uses their communication card 3 times under moderate frustration has received more therapeutic value than a child who sat through 20 minutes of practice at zero arousal.
Material | Daily Repetition Target | When | |
Chewy Tube | Every oral-seeking episode + proactive use before high-risk times | Throughout day | |
Communication Cards | Every natural communication opportunity during peer interaction | All peer play | |
Feelings Book | 1 full reading | Bedtime or quiet morning | |
Social Story | 1 full reading | Consistent daily time | |
Calm-Down Kit | Practice at calm ×1 + real use as needed | Morning + triggered | |
Visual Schedule | Full review ×1 + transition preview ×4–6 | Morning + transitions | |
Reinforcement | Every occurrence of gentle behavior or alternative use | Immediately as it occurs | |
Gentle Touch Practice | Formal session ×1 + natural prompts ×3–5 | Session + throughout day |

Behavior | Script | |
Used chewy instead of biting | "You felt that feeling and you used your chewy! That was AMAZING. One sticker!" | |
Handed communication card | "You showed me MINE/STOP/HELP! You used your words! I heard you!" | |
Practiced gentle touch | "So gentle! That's exactly how we touch. I love your gentle hands." | |
Stayed calm during a transition | "You saw the schedule and you waited so calmly. I'm so proud of you." | |
Named a feeling before escalating | "You told me you were angry — that's so big! Now we can fix it together." |
📞Questions about your reinforcement plan? FREE: 9100 181 181



- Child tolerates chewy tube without rejection — even if not actively using it
- Child looks at or picks up communication card when prompted
- Biting incidents: same or slightly increased (normal — extinction burst phase)
- Parent: familiar with all 9 materials, has implemented 4+ consistently
- All adults in environment know the plan and are implementing consistently
- Spontaneous card use without prompting
- Significant reduction in biting incidents
- Child independently accessing chewy before frustration peak



You started this journey with a child who bit the people around them and a parent who felt helpless, ashamed, and terrified of the next phone call. You are now a parent who understood the function behind the behavior, built an environment that supports alternatives, and stayed consistent through the hardest weeks. That is clinical-grade parenting.





"Biting almost always serves a clear function once we observe carefully. The families who achieve fastest resolution identify the function first, match the replacement to that function, and involve all caregivers in consistent implementation." — Pinnacle Behavior Analysis Team


Need | Specialist | What They'll Do | |
Biting function unknown | BCBA | Functional Behavior Assessment → Behavior Intervention Plan | |
Communication system design | SLP | AAC evaluation, communication card system, FCT training | |
Oral sensory profile | OT | Sensory diet, chewy selection, oral motor program | |
School/daycare coordination | SpEd | School behavior plan, teacher training, consistency across settings | |
Developmental evaluation | NeuroDev Pediatrician | Rule out medical contributors, ASD evaluation if indicated |

🔗BACB.com — FCT Literature Review
🔗PubMed: PMC11506176
🔗PubMed: PMC10955541
🔗DOI: 10.1007/s12098-018-2747-4
🔗nurturing-care.org | PMC9978394


🏷️Title: 9 Materials That Help With Biting Others
📂Series: Behavior Analysis & PBS — Episode 382
⏱️Duration: 75–85 seconds
🎯Domain: D — Behavior Analysis | Sub-domain: BEHAV-BITE
👶Age Range: 1–6 years (peak: 18mo–3yr)
"When children bite, they're telling us something they can't say. Our job is to understand the message AND give them a different way to send it. Here are 9 materials that help." — Pinnacle Blooms Consortium | ABA/BCBA + OT Team
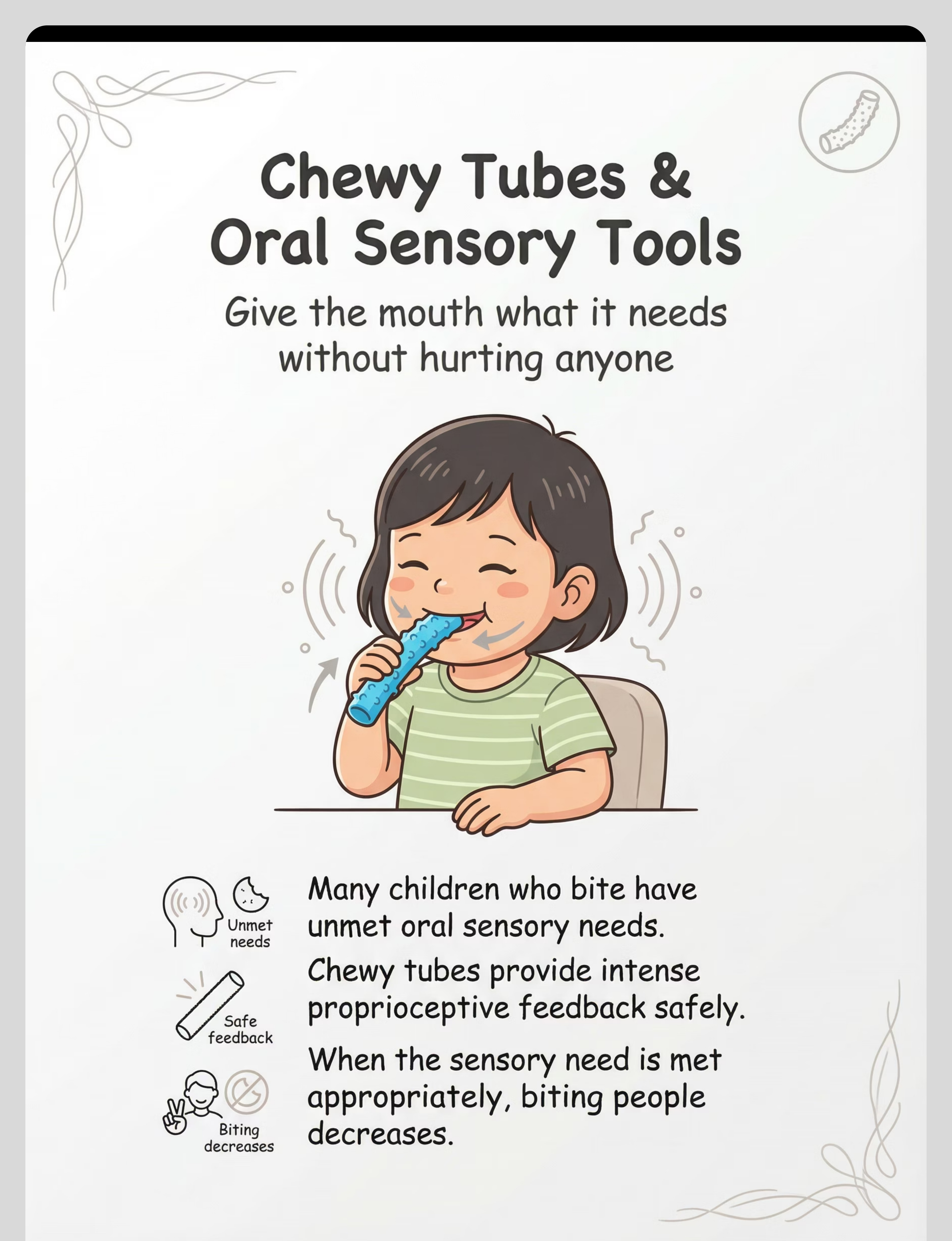
- Chewy Tubes
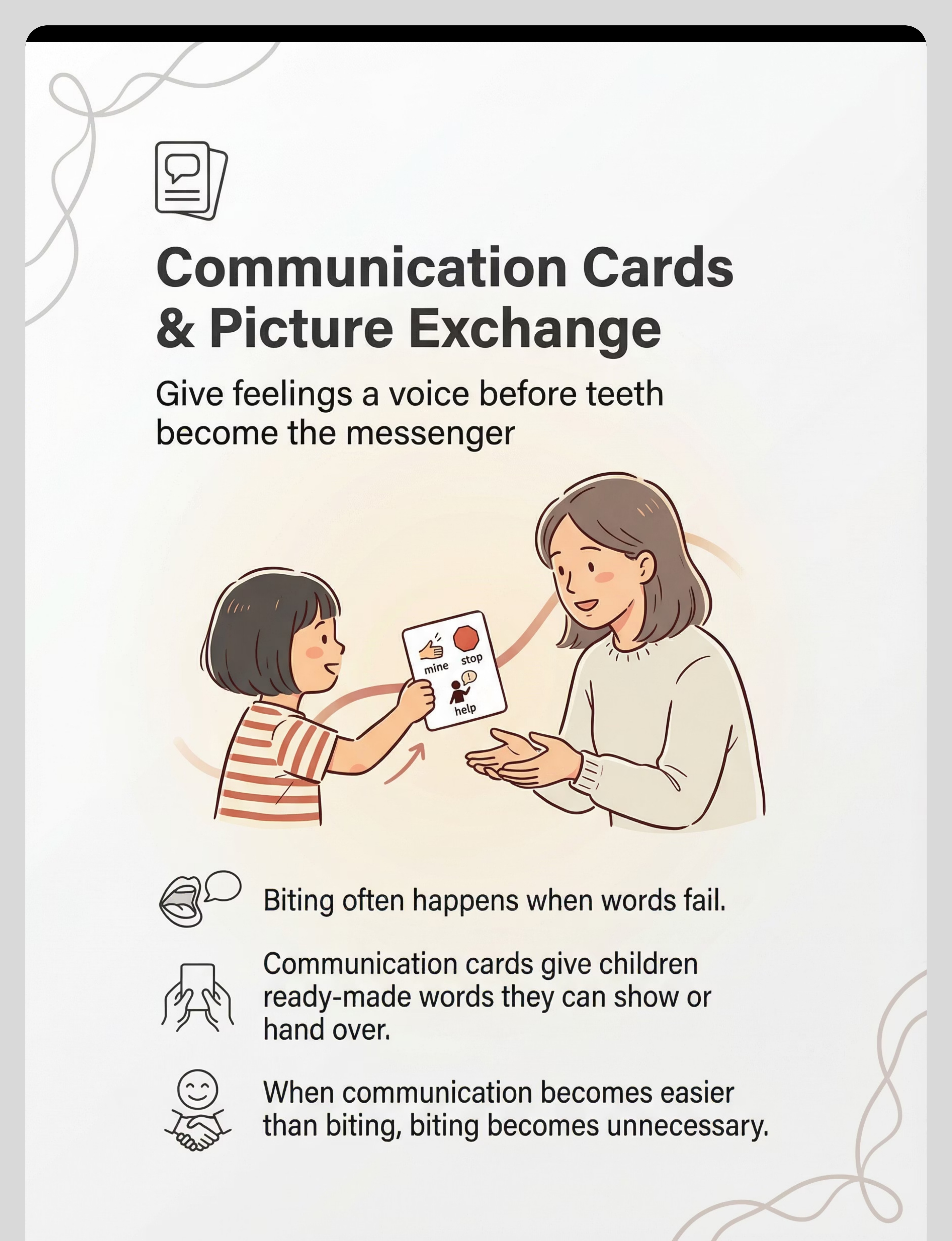
- Communication Cards
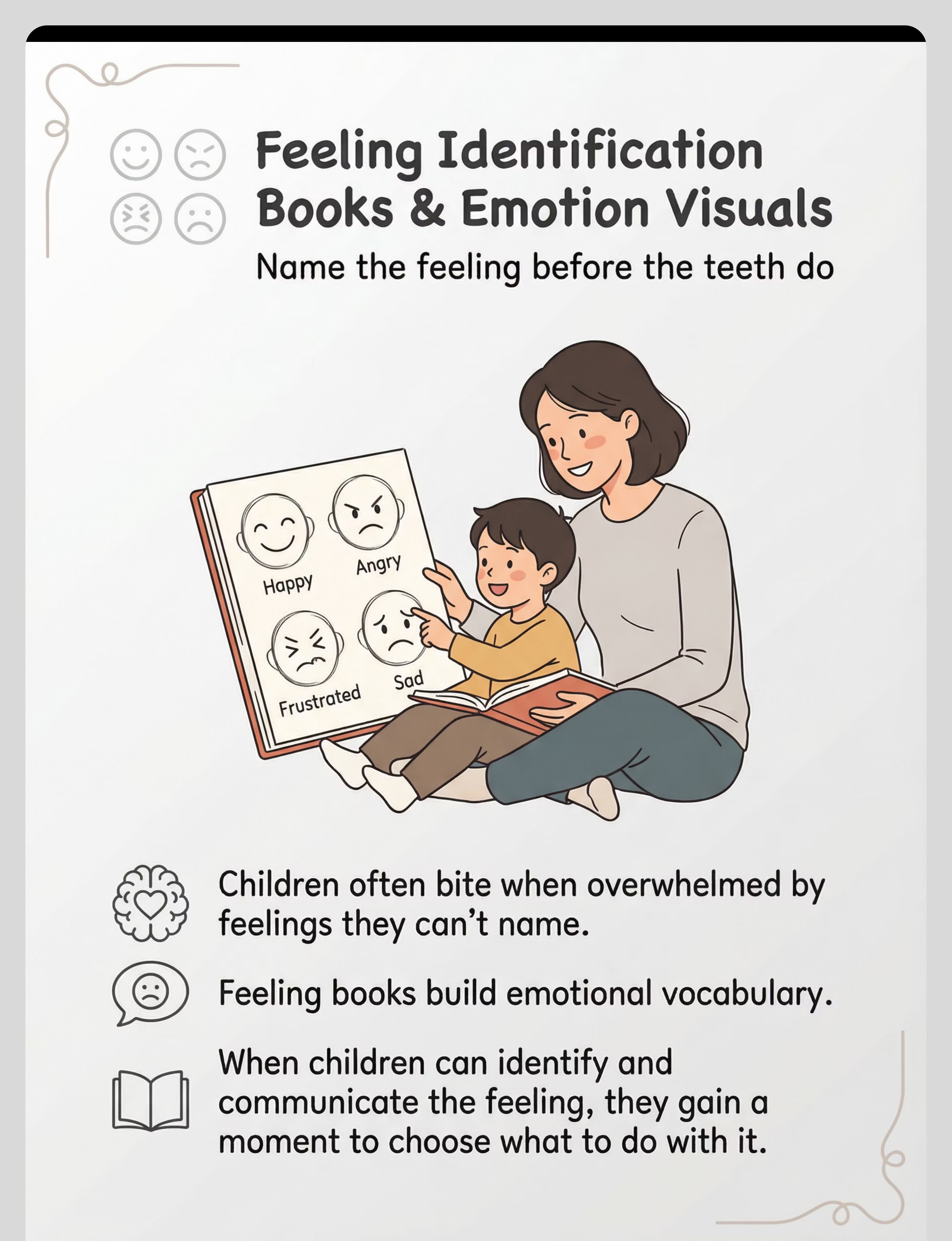
- Feelings Books
- Social Stories
- Calm-Down Kits
- Visual Schedules
- Reinforcement Systems
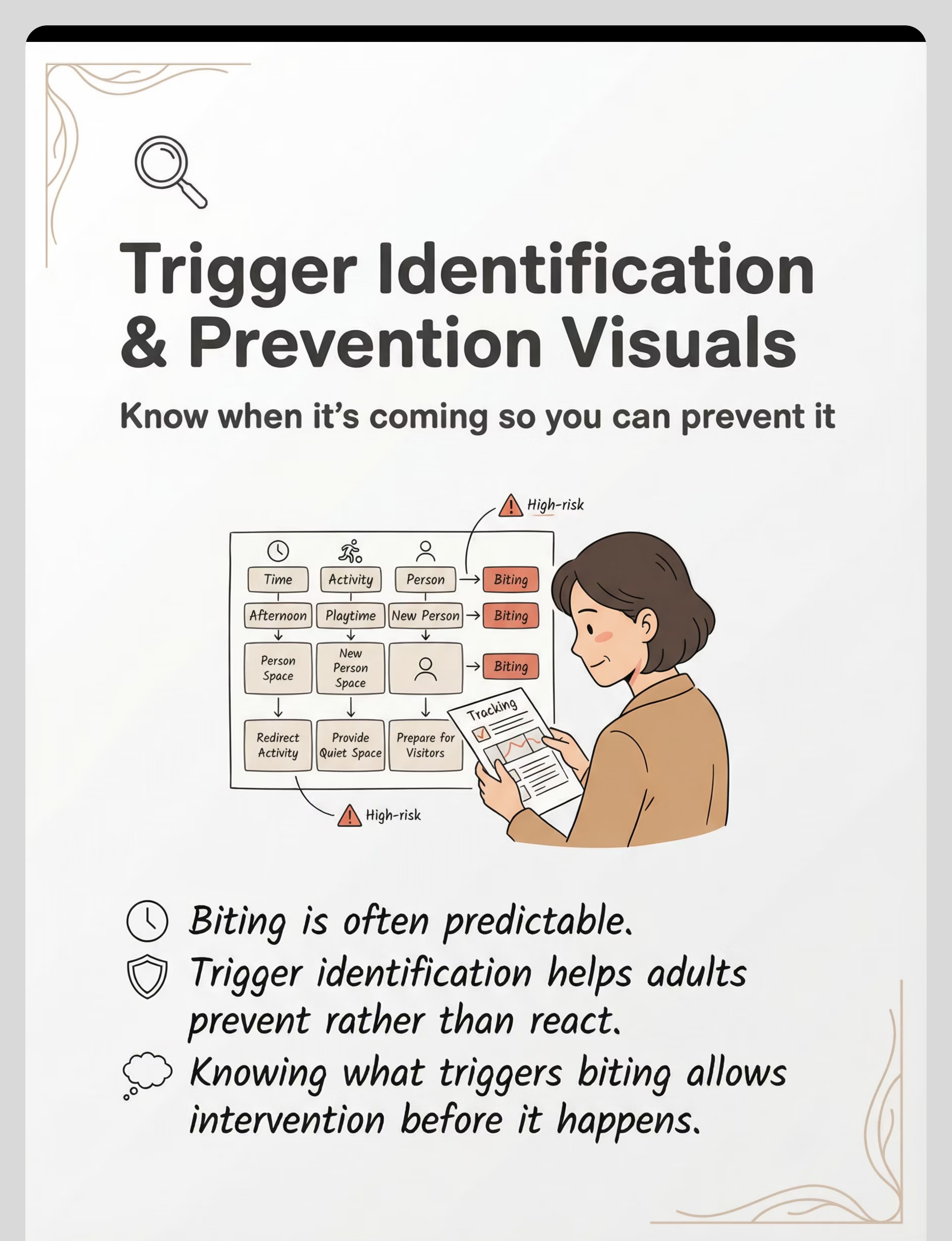
- Trigger Identification
- Gentle Touch Tools



Preview of 9 materials that help with biting others Therapy Material
Below is a visual preview of 9 materials that help with biting others therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.







You arrived at this page with a child who was biting — and a parent who felt helpless, ashamed, and terrified of the next phone call. You now leave with: the neuroscience behind the behavior, 9 evidence-matched materials, a step-by-step protocol, a progress tracking system, a connection to professional support, and the knowledge that your child's mouth was speaking the only language available — and you just gave them 9 better ones.
© 2025–2026 Pinnacle Blooms Network®, unit of Bharath Healthcare Laboratories Pvt. Ltd. All rights reserved. Unauthorized reproduction prohibited.
→ Card 01 of D-383: Hitting & Kicking — the journey continues.