
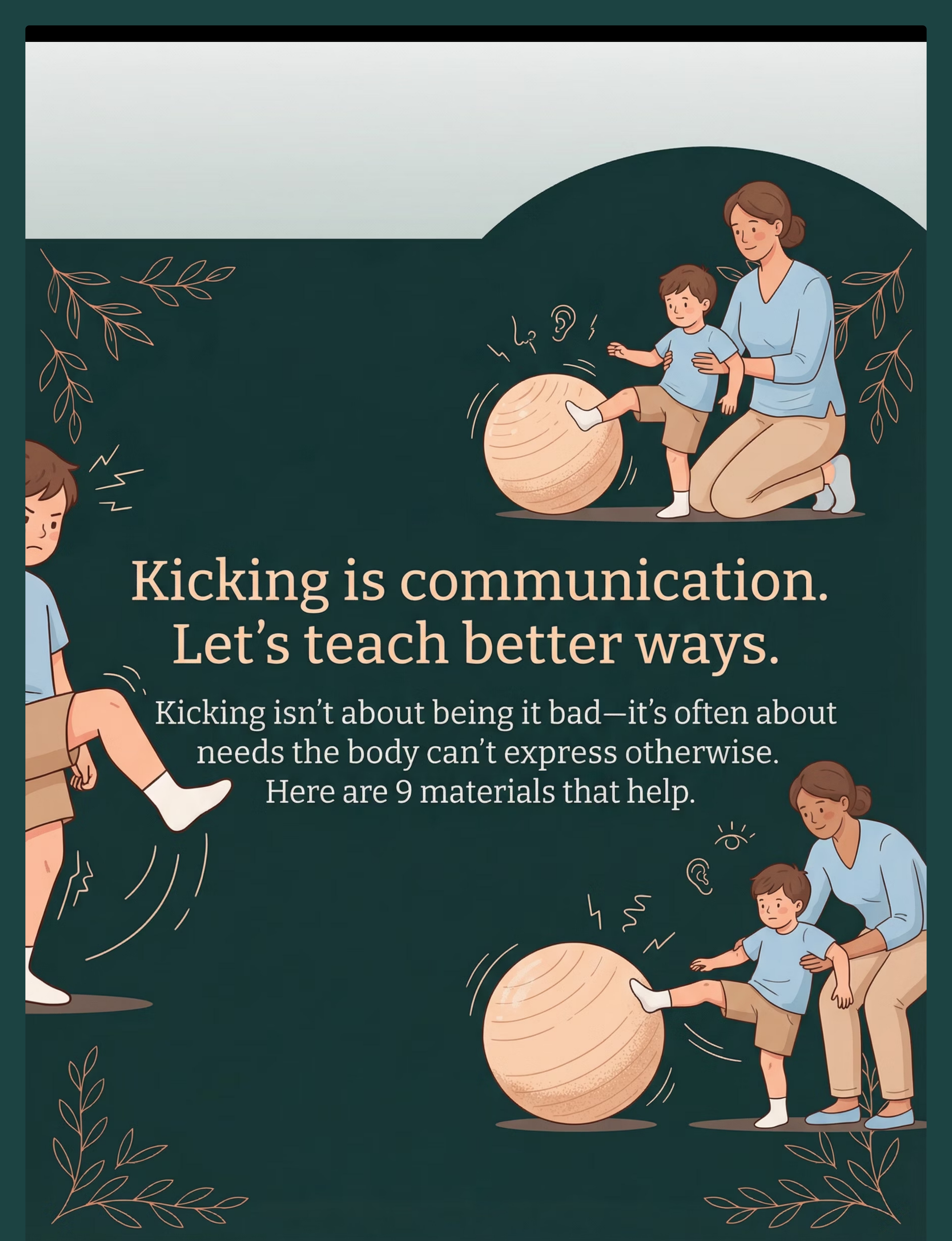
"Kicking is communication. Let's learn the language."
The call came during lunch. Again. "Your son kicked a classmate during circle time." You go through the motions — apologies, pickup, the drive home in silence. He looks out the window, face blank. You don't think he's bad. You know he's not bad. But you're running out of explanations to give other parents. You're running out of space between his needs and the world's expectations.
You are not failing. Your child's nervous system is speaking in the only language it currently has.
Technique D-383
9 Materials That Help With Kicking Others
Domain: Behavior & Flexibility | Sub-Domain: Physical Aggression / Kicking
Age Band: 2–10 years | Setting: Home, School, Community
Consortium Lead: ABA (BCBA) + Occupational Therapy
Age Band: 2–10 years | Setting: Home, School, Community
Consortium Lead: ABA (BCBA) + Occupational Therapy
This technique collection addresses kicking through 9 precisely selected materials that target the behavior's root functions, teach safer replacements, and provide the nervous system with the input it seeks through appropriate channels. We are not suppressing kicking — we are building the skills that make kicking unnecessary.
- Reinforcement Menus & Token Boards
- Sensory-Motor Tools & Proprioceptive Input
- Communication Cards & Visual Supports
- Social Stories & Transition Objects
Pinnacle Blooms Network®
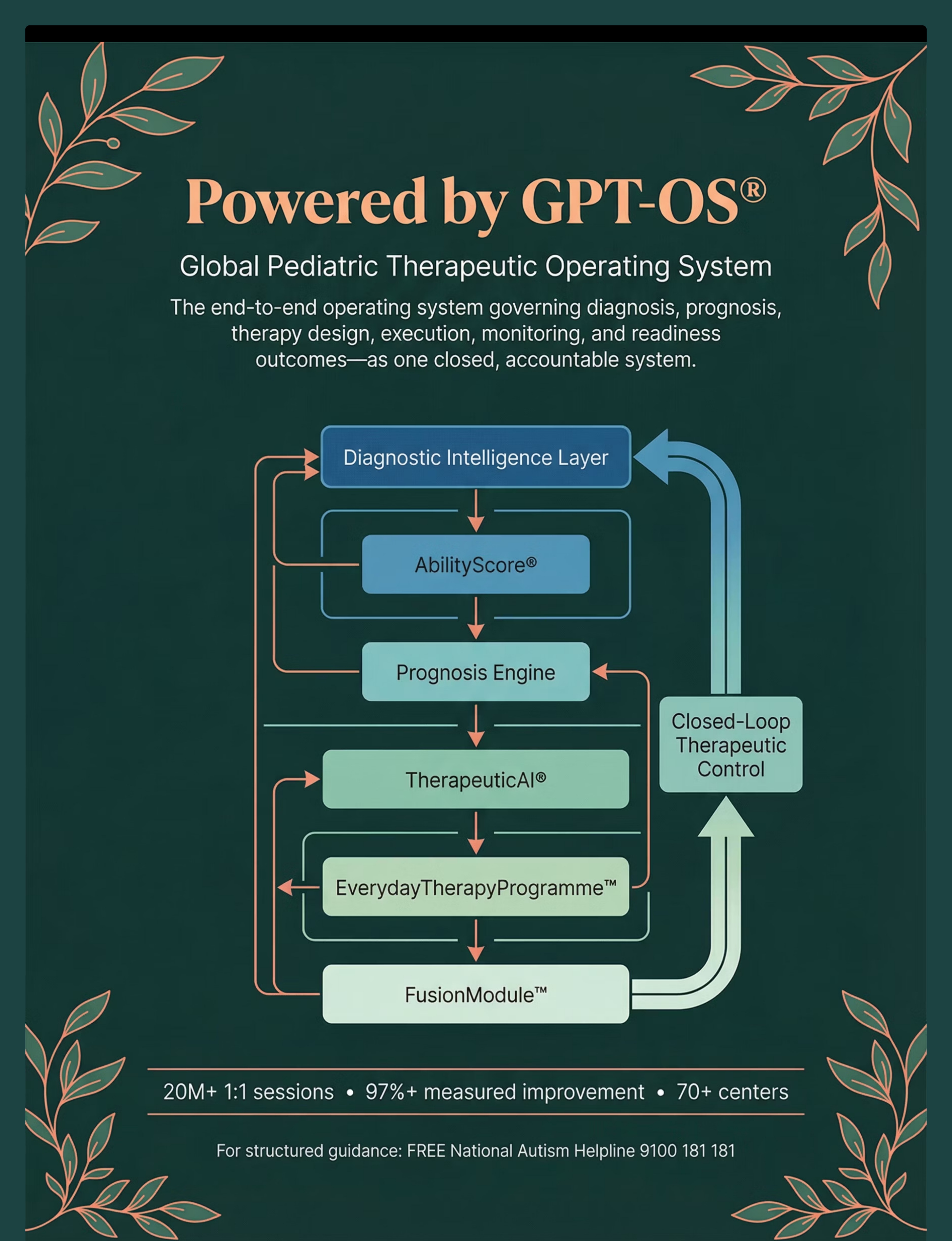
GPT-OS® Verified | WHO-Aligned
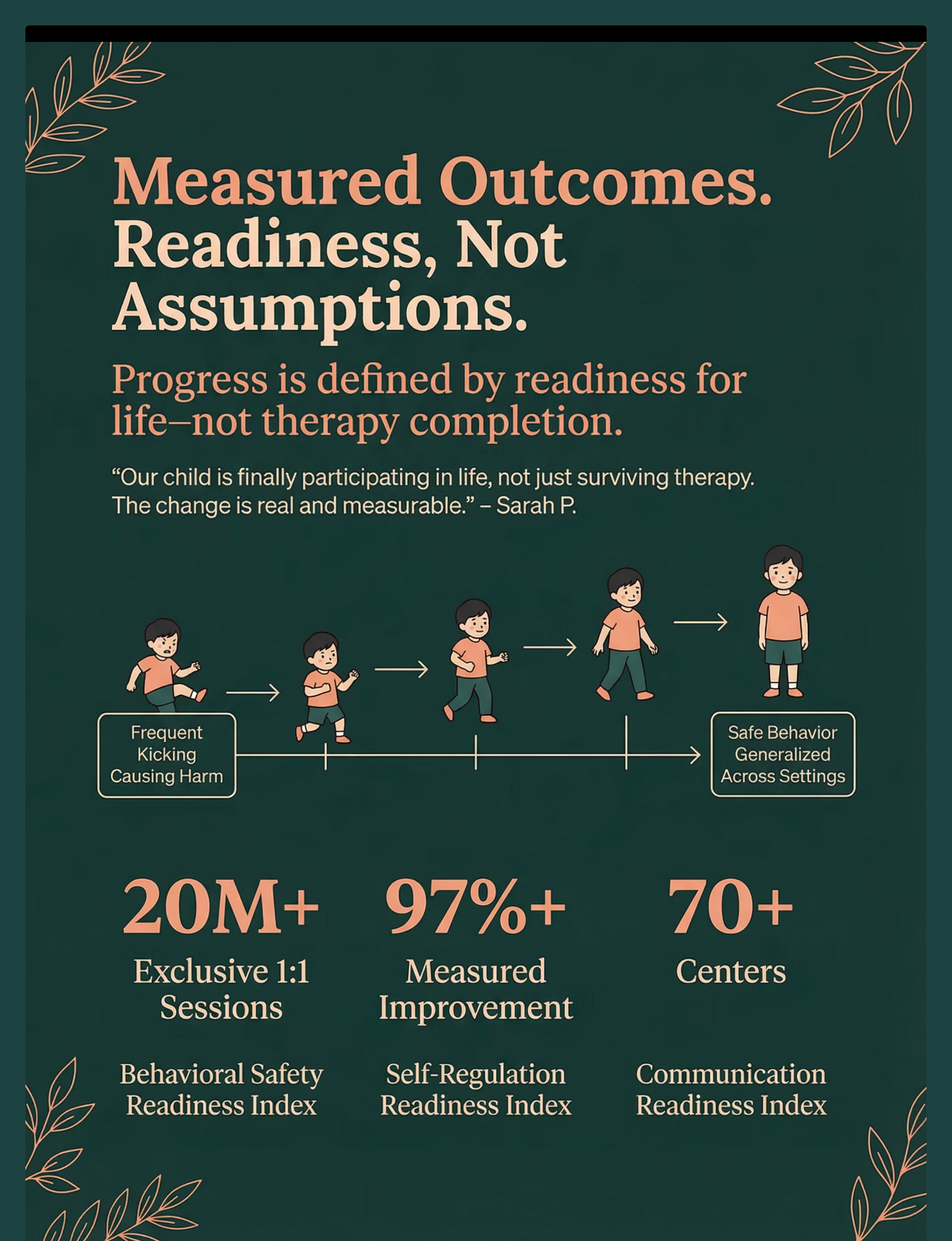
20M+ exclusive 1:1 therapy sessions
97%+ measured improvement
70+ centers across India
97%+ measured improvement
70+ centers across India
📞 FREE Helpline
9100 181 181
16+ Languages | 24×7
9100 181 181
16+ Languages | 24×7

ACT I: Understand
Your Family Is Among Millions Navigating This Exact Challenge
1 in 36
Children with Autism
Children in India diagnosed with autism spectrum conditions — a documented, researched, addressable population.
80%
Sensory Difficulties
Children with ASD experience sensory processing difficulties that can manifest as physical behaviors including kicking.
60–70%
Lower-Extremity Aggression
Kicking is reported as the most common lower-extremity aggression in children aged 2–8 years.
Across Pinnacle's 70+ centers and 21 million therapy sessions, kicking is among the top 5 behaviors families seek help for. In India's pediatric therapy landscape, physical aggression — including kicking — is identified as a primary barrier to school inclusion for an estimated 2.3 million children with developmental needs (NIMH India, 2023). You are not alone in this room.
"You are among millions of families. And millions of families have found a path forward."

The Kick Isn't the Problem. It's the Signal.
What's Happening in the Brain
When your child's nervous system perceives threat, invasion of space, overwhelming sensory input, or unmet motor need — the amygdala (the brain's alarm system) fires. In a developing brain, especially one wired differently, the signal goes straight to the legs — a powerful motor response — before the prefrontal cortex (the "thinking, braking" part) can intervene.
The Proprioceptive Dimension
Many children who kick are not seeking to harm. They are seeking proprioceptive input — deep pressure feedback from muscles and joints that helps regulate the nervous system. The kick feels satisfying, regulating. This is neurology, not defiance.
The Wiring Difference
"This is a wiring difference, not a behavior choice. The brain your child has is doing exactly what it was built to do — it just needs better tools."
The Pattern
Threat/Overwhelm → Amygdala Fires → Motor Pathway Engages → Kick Happens → Consequence Arrives → Need Remains Unmet → Next Trigger → Same Pattern Repeats
The Intervention: Address the need BEFORE the pattern fires.

Developmental Context
Your Child Is Here. Here Is Where We're Heading.
Kicking that persists beyond age 4–5, or that increases in frequency or intensity, signals that the child's developing brain needs additional scaffolding. This is not failure — it is an intervention window. The WHO/UNICEF Care for Child Development Package, implemented in 54 countries, provides age-specific guidance for caregivers. This technique aligns with those behavioral scaffolding principles.
Co-Occurring Factors
- Sensory processing differences (80% of ASD children)
- Limited functional communication
- Difficulty with transitions
- Impulse control developmental lag
The Forward Path
- Weeks 1–4: Kicking with reduced intensity
- Weeks 5–8: Kicking becomes rare, replaced by alternatives
- Beyond: Safe behavior generalized across settings

Evidence Grade
Clinically Validated. Home-Applicable. Parent-Proven.
Evidence Grade: Level I
Systematic Review + Multiple RCTs
"Kicking decreases when the underlying function is identified and addressed — not when it is suppressed through punishment alone." — Synthesis of function-based intervention literature, JABA
Pinnacle Real-World Evidence
20M+ exclusive 1:1 therapy sessions | 97%+ measured improvement | Physical aggression reduction is among the most consistently demonstrated outcomes
Key Studies
PRISMA Systematic Review (2024) — PMC11506176
16 studies confirm sensory integration intervention meets evidence-based practice criteria for ASD. Confidence: HIGH ⬛⬛⬛⬛⬛
16 studies confirm sensory integration intervention meets evidence-based practice criteria for ASD. Confidence: HIGH ⬛⬛⬛⬛⬛
Meta-Analysis World J Clin Cases (2024) — PMC10955541
SI therapy promotes adaptive behavior and motor skills across 24 studies. Confidence: HIGH ⬛⬛⬛⬛⬛
SI therapy promotes adaptive behavior and motor skills across 24 studies. Confidence: HIGH ⬛⬛⬛⬛⬛
Indian RCT, Indian J Pediatr (2019)
Home-based sensory interventions showed significant outcomes in Indian pediatric population. Confidence: HIGH ⬛⬛⬛⬛◻
Home-based sensory interventions showed significant outcomes in Indian pediatric population. Confidence: HIGH ⬛⬛⬛⬛◻
NCAEP Evidence-Based Practice Report (2020)
Function-based intervention + visual supports = evidence-based for autism. Confidence: HIGH ⬛⬛⬛⬛⬛
Function-based intervention + visual supports = evidence-based for autism. Confidence: HIGH ⬛⬛⬛⬛⬛

ACT II: Learn
D-383: The Technique — What It Is
Parent-Friendly Alias: "Safe Feet Strategy Kit" | Series: Challenging Behaviors & Safety — Episode 383
Kicking others is a form of physical aggression involving forceful lower-extremity movement directed at people. Like all behavior, it serves a function — it is never random, even when it appears impulsive. Common functions include escape (kicking to leave overwhelming situations), access (kicking to obtain desired items), attention (kicking to generate adult response), and sensory/automatic (kicking because the proprioceptive sensation itself is regulating).
Domain D
Behavior & Flexibility
ABA/BCBA
Primary Lead
OT
Secondary Lead
Age 2–10
Home + School
Daily
10–20 min sessions
"We are not suppressing kicking. We are building the skills that make kicking unnecessary." — Pinnacle Blooms BCBA Consortium
Who Uses This Technique
This technique crosses therapy boundaries — because the brain doesn't organize by therapy type. All disciplines contribute their assessment simultaneously in Pinnacle's FusionModule™.
BCBA / ABA — Primary Lead
Functional Behavior Assessment, replacement behavior training, reinforcement system design, and data collection protocols. The behavioral foundation of the entire intervention.
Occupational Therapy — Co-Lead
Sensory processing evaluation, proprioceptive diet, heavy work programming, calm-down kit design, and environmental setup. Addresses the sensory root of kicking.
Speech-Language — Communication Layer
Functional Communication Training — teaching the child to use words or communication cards instead of kicks. Builds the alternative voice.
Special Education — Generalization Layer
Social stories creation, classroom boundary systems, transition support, and school-home consistency to ensure skills transfer across environments.
What This Targets: A Precision Tool
Observable Indicators by Tier
Primary (Weeks 1–4): Kicking incidents decrease by 50%+ from baseline
Secondary (Weeks 2–6): Child uses communication card or verbal request ≥1x/day
Secondary (Weeks 3–8): Child accesses calm-down kit before escalation
Tertiary (Weeks 6–12): No kicking incidents reported at school for 2 consecutive weeks
GPT-OS® Readiness Indexes
Behavioral Safety Readiness Index
Self-Regulation Readiness Index
Communication Readiness Index
All three indexes are tracked automatically when you log sessions on GPT-OS®.

Materials 1–3
What You Need: Primary Materials (1–3)

Material 1 — Kick-Appropriate Target
Large Exercise/Therapy Ball — 65cm
Canon Category: Sensory-Motor Tools
Price Range: ₹800–2,500
Canon Category: Sensory-Motor Tools
Price Range: ₹800–2,500
The cornerstone of the entire protocol. Provides safe, appropriate proprioceptive outlet for kicking urge.

Material 2 — Reinforcement System
Rosette Imprint Reward Jar — ₹589
1800+ Reward Stickers — ₹364
Canon Category: Reinforcement Menus ✓ ACTIVE IN CANON
1800+ Reward Stickers — ₹364
Canon Category: Reinforcement Menus ✓ ACTIVE IN CANON
Token economy and sticker reward system for reinforcing safe feet behavior within 3 seconds of occurrence.

Material 3 — Transition Object
Animal Soft Toy — ₹425
Canon Category: Transition Objects / Comfort Items ✓ ACTIVE IN CANON
Canon Category: Transition Objects / Comfort Items ✓ ACTIVE IN CANON
Familiarity is the therapeutic ingredient. Used during cool-down and transitions to support self-regulation.
Materials 4–6
Primary Materials (4–6)
Material 4 — Visual Timer
Visual Countdown Timer
Canon Category: Visual Support Materials
Price Range: ₹400–900
Canon Category: Visual Support Materials
Price Range: ₹400–900
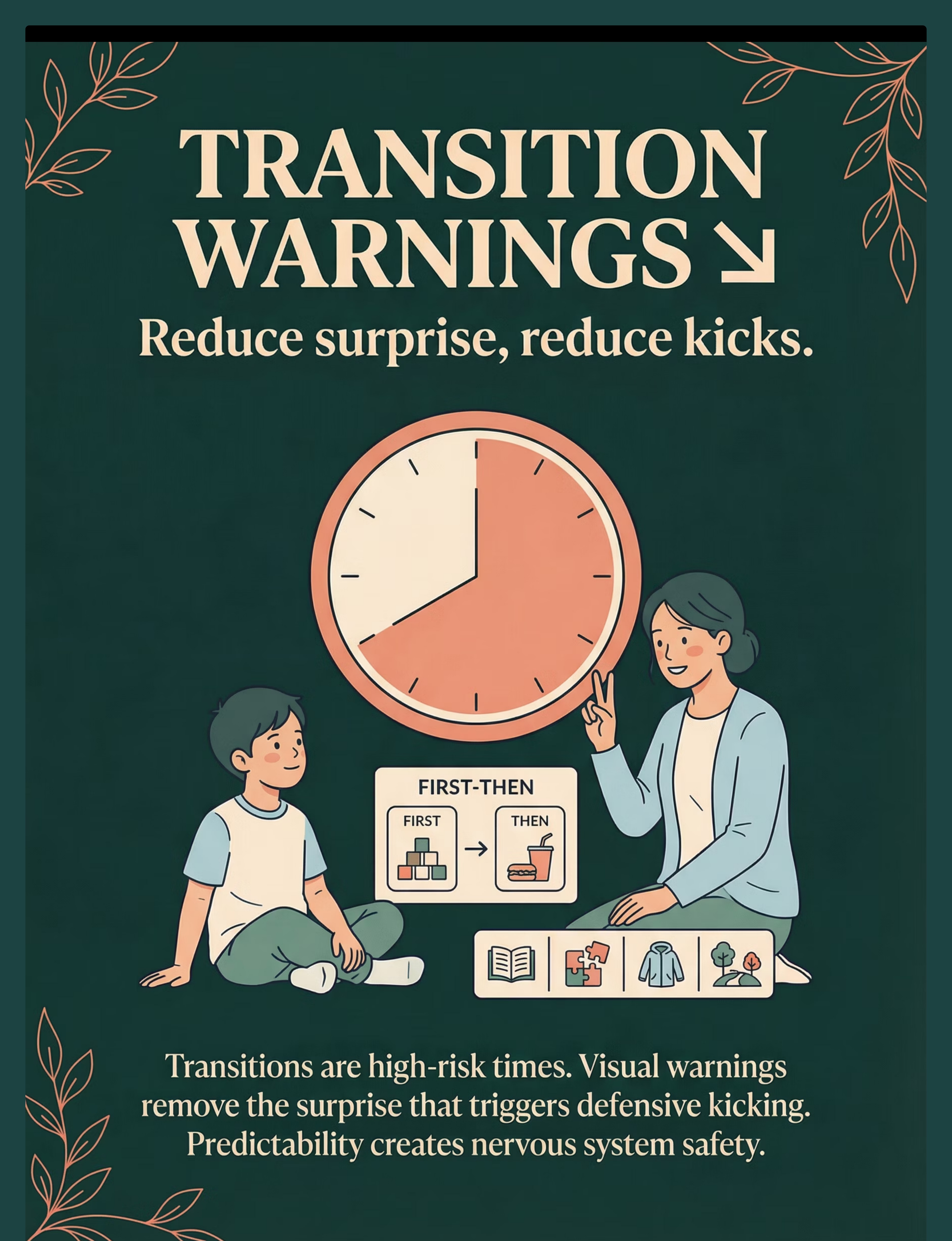
Creates visible predictability for transitions. The child sees time ending — it is never a surprise. Critical for transition-triggered kicking.

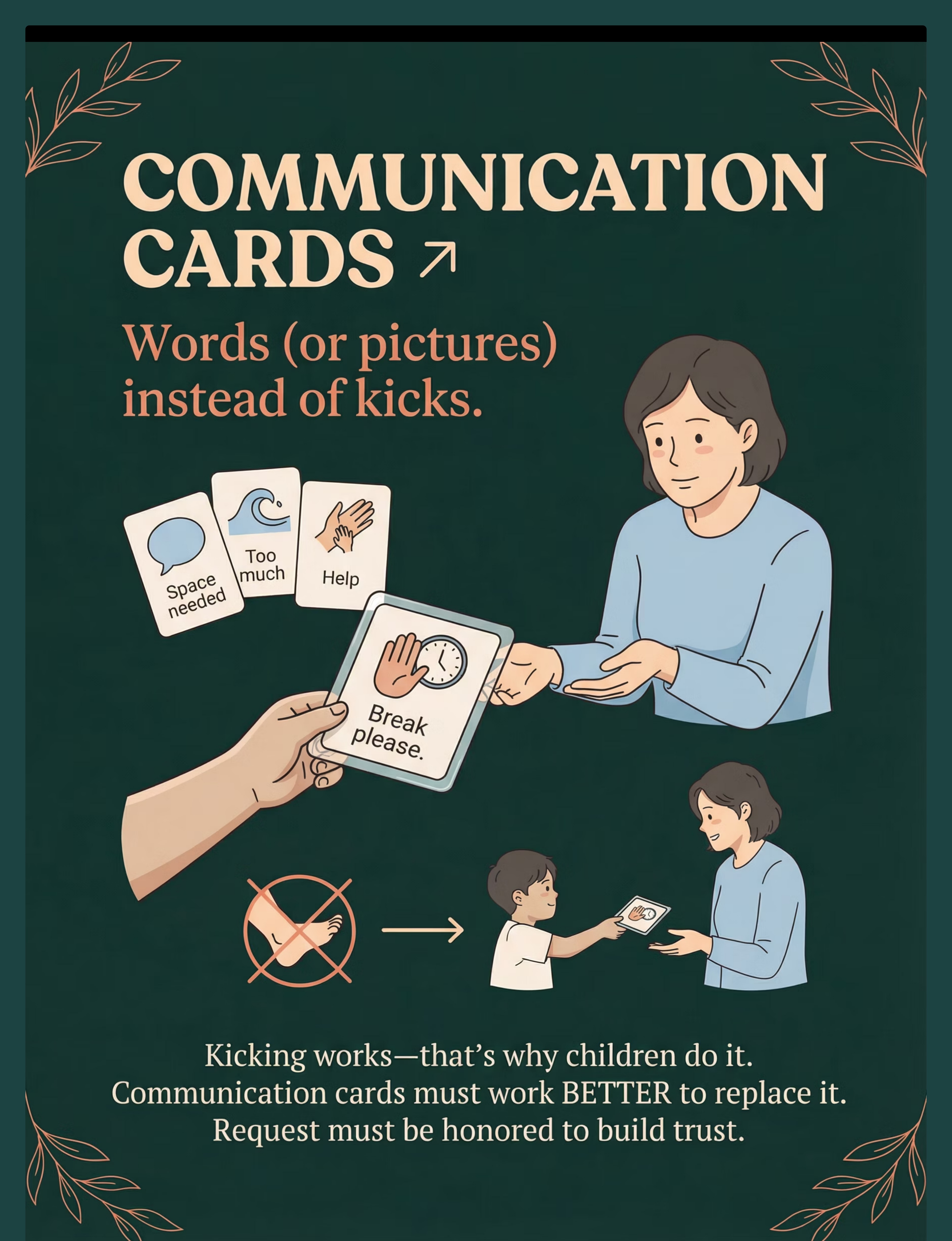
Material 5 — Communication Cards
Laminated AAC Communication Cards Set
Canon Category: Communication Cards
Price Range: ₹150–500
Canon Category: Communication Cards
Price Range: ₹150–500
The child's voice when words aren't available. The break card — when honored reliably — replaces kicking as a communication strategy.
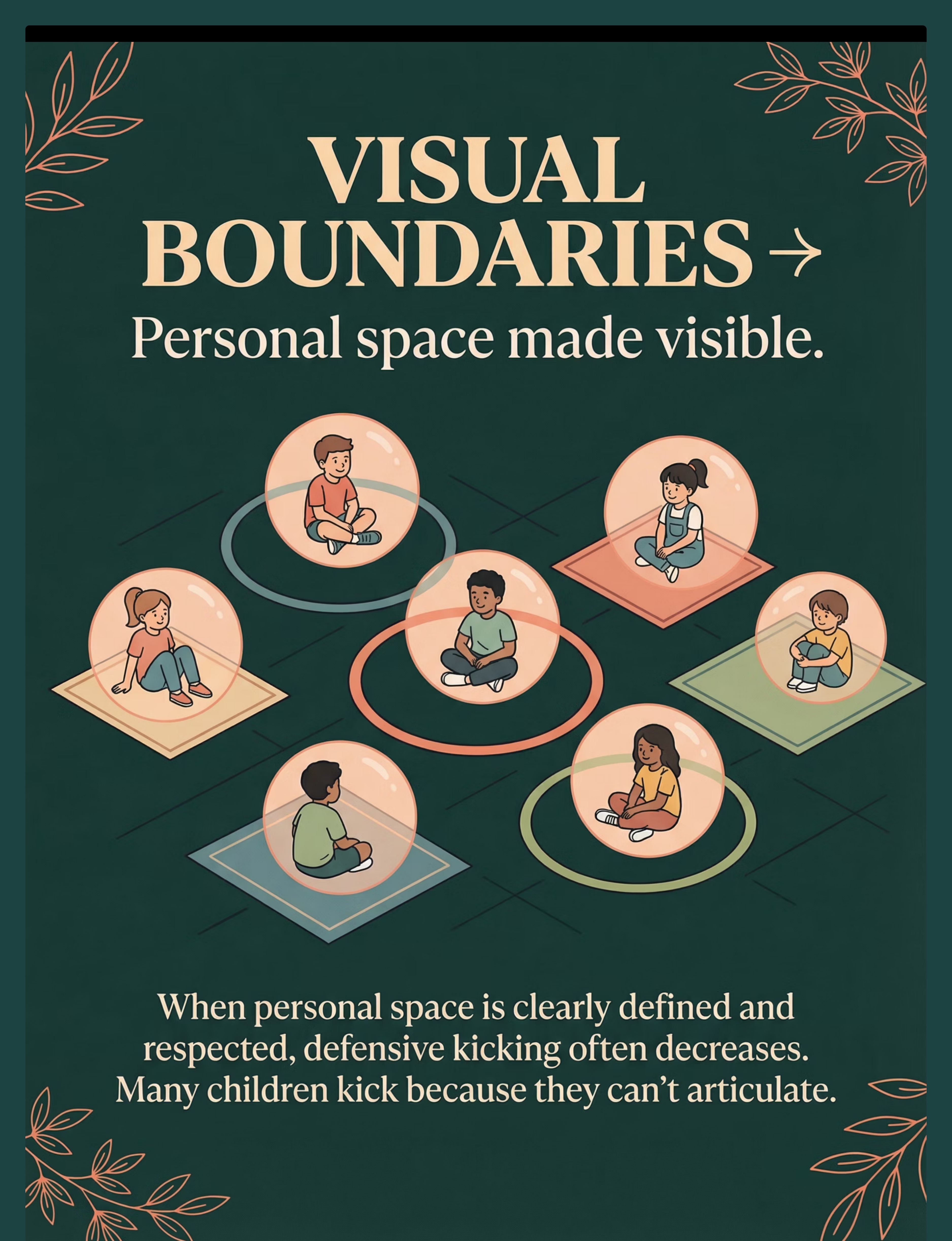
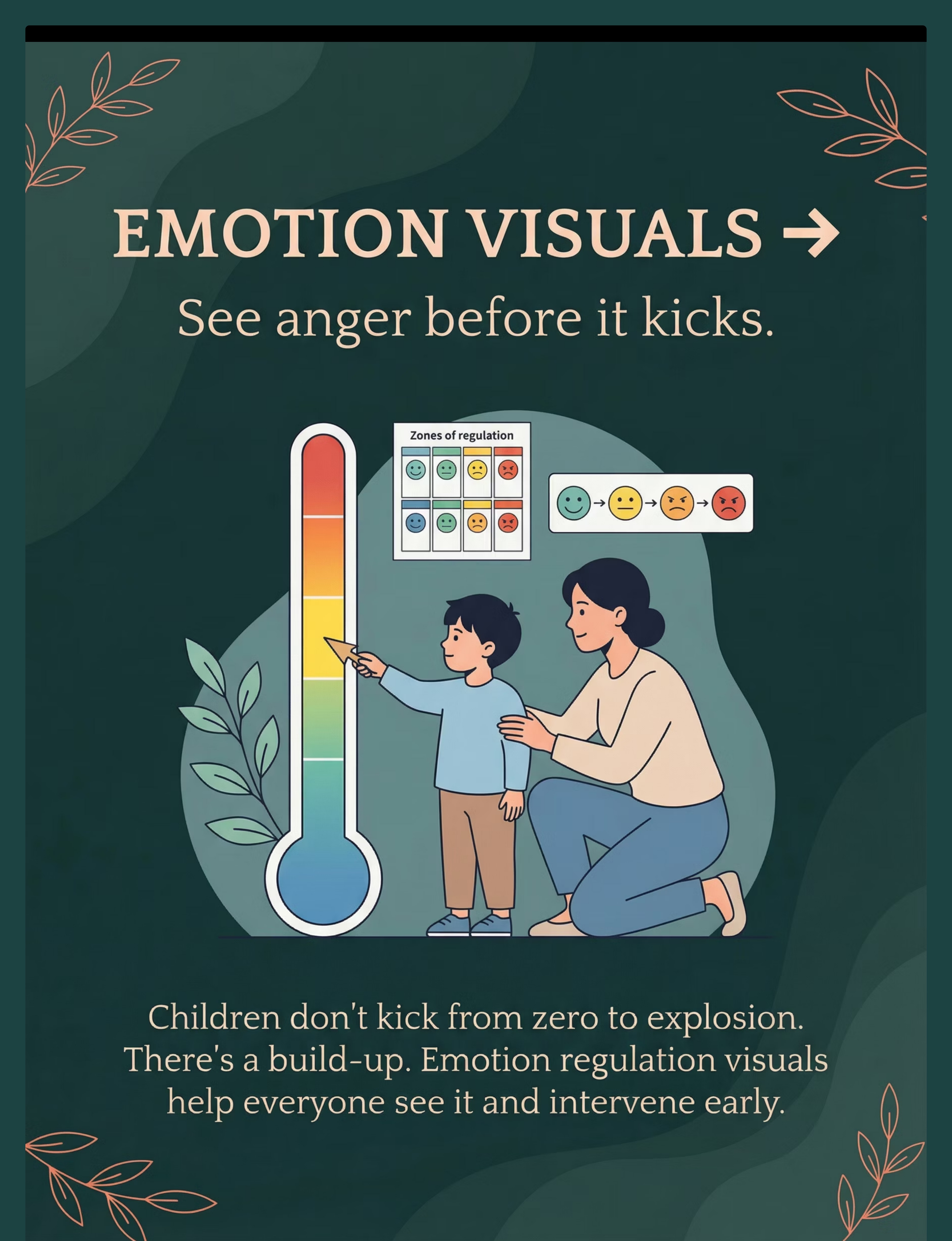
Material 6 — Emotion Regulation Visual
Zones of Regulation / Anger Thermometer Chart
Canon Category: Visual Support Materials
Price Range: ₹100–400
Canon Category: Visual Support Materials
Price Range: ₹100–400
Builds interoceptive awareness. Children who can name their emotional state are more likely to use tools before escalating.

Materials 7–9
Primary Materials (7–9)

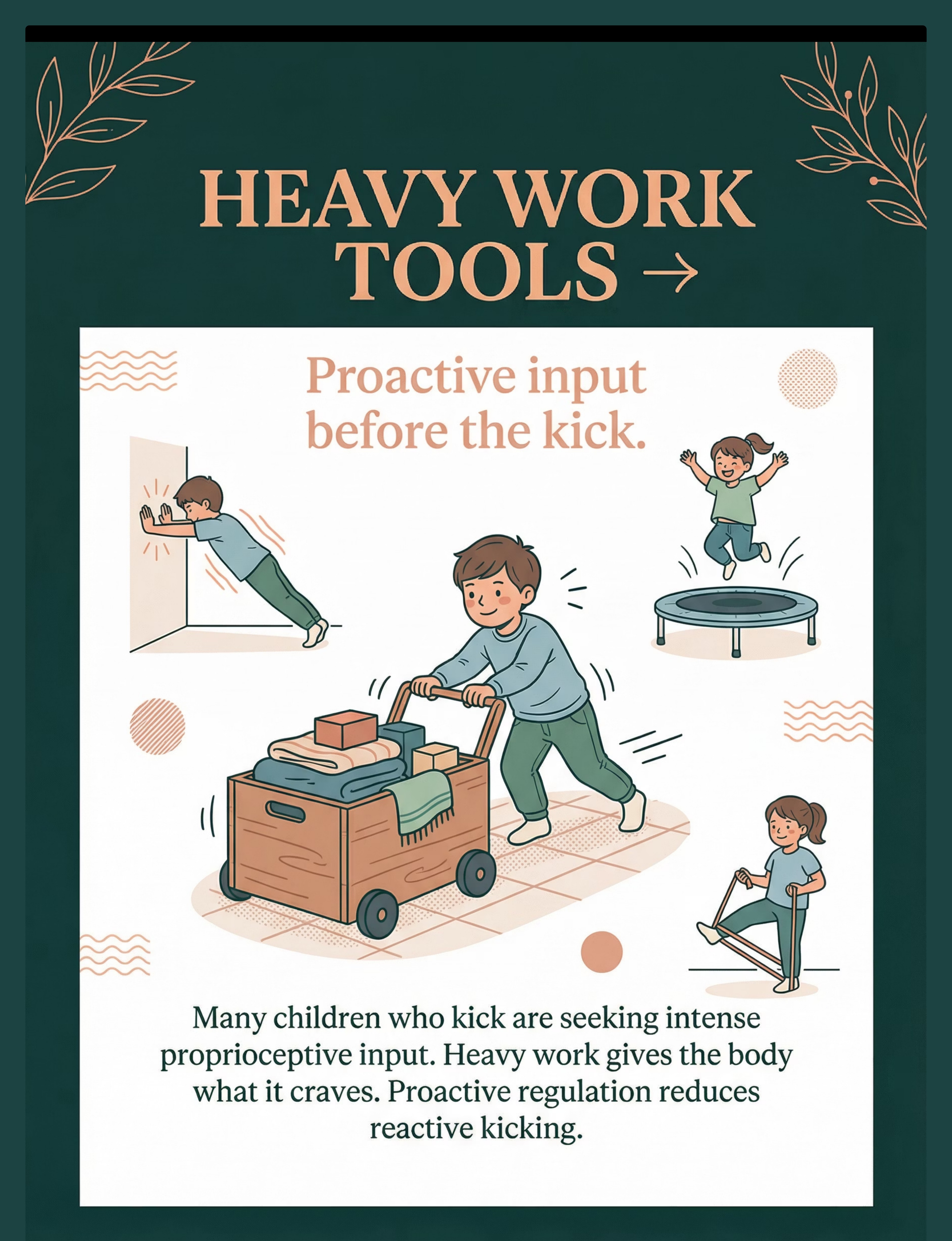
Material 7 — Heavy Work Tools
Resistance Bands (Light/Medium) + Mini Trampoline
Canon Category: Sensory-Motor Tools
Price Range: ₹500–2,500
Canon Category: Sensory-Motor Tools
Price Range: ₹500–2,500
Provides pre-loading proprioceptive input that reduces baseline arousal before it reaches the kicking threshold.

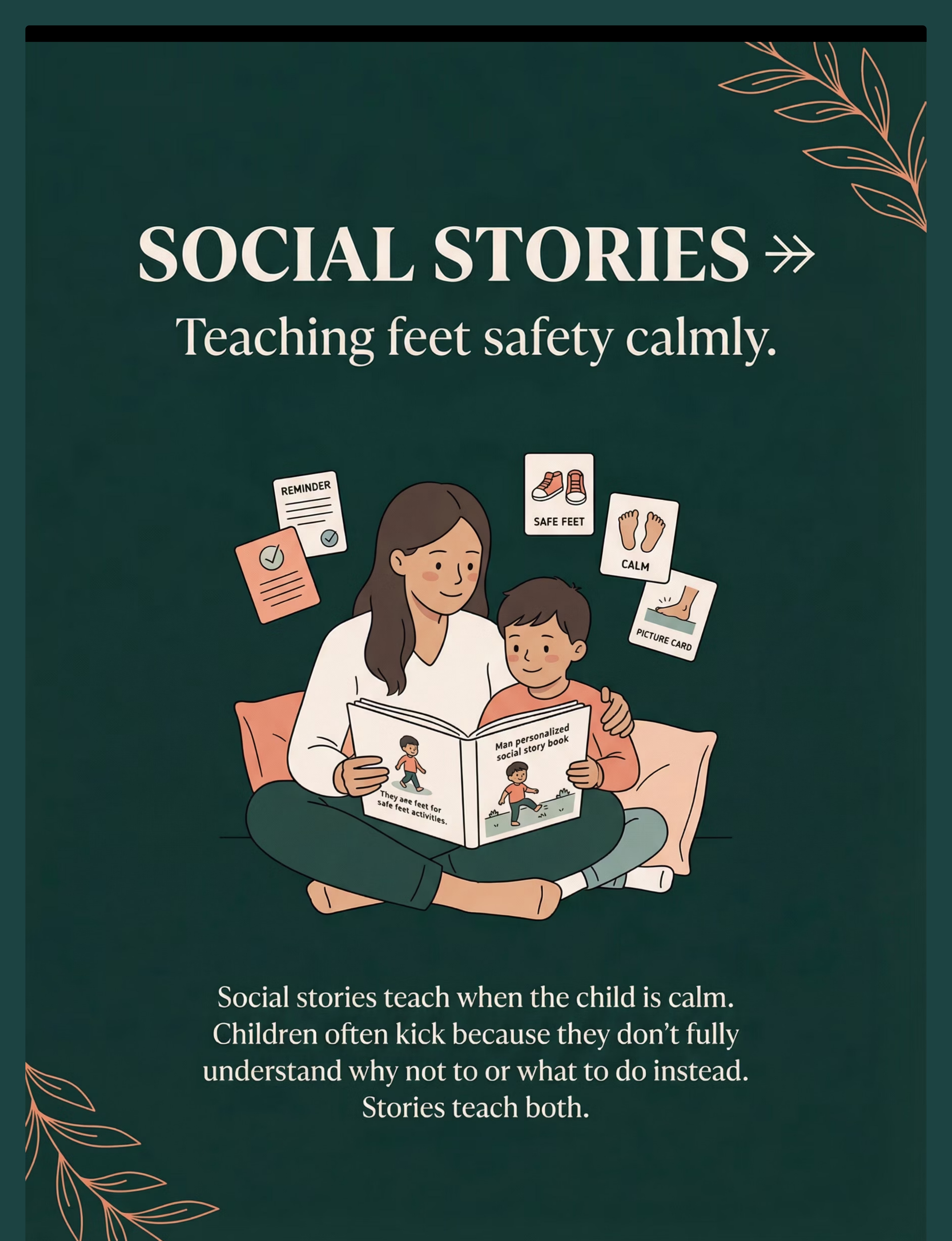
Material 8 — Social Story Book
Personalized Social Story: "My Safe Feet"
Canon Category: Social Stories / Narrative Tools
Price Range: ₹0 (printable DIY) – ₹400
Canon Category: Social Stories / Narrative Tools
Price Range: ₹0 (printable DIY) – ₹400
Personalized stories featuring your child's own photos are more effective than commercial versions. This is one place where homemade wins.

Material 9 — Weighted Lap Pad
Weighted Lap Pad (1–2 kg)
Canon Category: Sensory-Motor Tools
Price Range: ₹600–1,800
Canon Category: Sensory-Motor Tools
Price Range: ₹600–1,800
Deep pressure stimulation that calms the nervous system. Use during cool-down or proactively in high-trigger environments. Max 10% of child's body weight.
Total Starter Kit Cost: ₹953 (Canon-stocked items only) | Full kit with all 9 materials: ₹2,800–8,000

Every Parent, Regardless of Budget, Can Execute This Technique Today
WHO/UNICEF mandate: Interventions must be available to all families. Every material in this technique has a ₹0 equivalent. Here is what you can make right now, with what you already have at home.
Material | Commercial | DIY Equivalent & Why It Works | |
Therapy Ball | ₹800–2,500 | Large inflated balloon or heavy pillow — same proprioceptive impact when kicked firmly | |
Visual Timer | ₹400–900 | Kitchen timer turned face-out or hourglass — visible countdown creates predictability | |
Communication Cards | ₹150–500 | Index cards with hand-drawn pictures or phone photos — image + function = identical effectiveness | |
Emotion Thermometer | ₹100–400 | A4 paper with hand-drawn temperature levels colored with crayons — self-made versions have higher child ownership | |
Weighted Lap Pad | ₹600–1,800 | 1kg bag of rice in a pillowcase or folded heavy blanket — deep pressure = same regulatory effect | |
Social Story | ₹0–400 | Photos of YOUR child + handwritten text in a stapled booklet — personalized stories are MORE effective | |
Token Board | ₹100–300 | A4 paper grid + sticker stars — function identical; child may prefer homemade | |
Transition Object | ₹425 | Any small preferred object the child already owns — familiarity is the therapeutic ingredient |
Zero-Cost Complete Kit Total: ₹0. A large pillow, kitchen timer, index card with "BREAK," hand-drawn thermometer, rice bag in pillowcase, shoebox with regulation items, photo booklet, star chart on fridge, and the child's existing comfort toy.

Safety First: Before You Begin
Safety is the first intervention. Use this traffic-light system before every session. Your regulation transfers directly to your child — if you are dysregulated, postpone.
🟢 Green Light — Proceed
- Child is fed, rested, and baseline regulated
- No recent meltdown within 2 hours
- You have 20 uninterrupted minutes
- Materials are prepped and accessible
- You are in a calm emotional state yourself
🟡 Amber — Modify
- Child slightly elevated but not in crisis → Use simplified 5-minute version only
- Child had a difficult morning → Reduce materials, increase support
- You are stressed → Reschedule; your regulation transfers to the child
🔴 Red Line — Do Not Proceed
- Child is in active meltdown or post-ictal state
- Child shows signs of illness, pain, or fatigue
- Kicking caused injury within the last 30 minutes
- You feel unsafe
Material Safety Checklist
- Therapy ball/kick target is stable; will not tip
- Resistance bands are not worn or likely to snap
- Weighted lap pad max 10% of child's body weight
- No small parts in calm-down kit for under-3s
- Visual timer screen is not cracked or sharp
Emergency Path
Remove yourself and others from kick range → De-escalate with minimal language, maximum space → If injury occurs: contact medical support
📞 Pinnacle Helpline: 9100 181 181
FREE | 24×7 | 16+ Languages
FREE | 24×7 | 16+ Languages

Set Up Your Space: The Right Environment Prevents 80% of Session Failures
Space Layout Principles
Kick Target: Large therapy ball or pillow zone — 1.5m from walls, in the child's clear line of sight. The child must be able to reach it in 3 steps or fewer.
Child Position: Floor mat or carpet square, facing the kick target. Comfortable, grounded, clear.
Visual Timer: In child's eyeline — never hidden or behind them.
Communication Cards: On a lanyard the adult wears or mounted at child's eye level.
Emotion Chart: On the wall at child's eye height, not above their eyeline.
Parent Position: Beside the child, slightly behind, non-threatening posture, open palms visible.
What to Remove
- Electronic screens (attention fragmentation)
- Loose objects that could become projectiles
- Other children's belongings (territorial triggers)
- Your phone — your attention is the therapeutic ingredient
Sensory Environment Settings
Lighting: Natural or warm LED — no harsh fluorescent
Sound: Quiet or soft white noise — no TV/music during session
Temperature: Comfortable — dysregulation increases in heat
Clutter: Minimal — visual overwhelm increases arousal
The Space Rule
"This space is safe. Kicking the ball here is allowed. Kicking people here is not."
Establish this rule verbally AND visually BEFORE the first session. Post it on the wall if needed.

ACT III: Execute
Is Your Child Ready? Pre-Flight Check
The best session is one that starts right. Run this check before every session. It takes 60 seconds and prevents 80% of session failures.
Indicator | ✅ Go | ⚠️ Modify | ❌ Postpone | |
Fed within last 2 hours? | Yes | Snacked | No — feed first | |
Slept adequately last night? | Yes | Partial | No — reduce intensity | |
Current emotional state? | Calm/Alert | Slightly elevated | Distressed/Escalated | |
Last kicking incident? | >2 hours ago | 1–2 hours ago | <1 hour ago | |
Signs of illness/pain? | None | Mild | Yes — postpone | |
Child's engagement level? | High | Neutral | Actively resistant |
ALL GREEN → Full Protocol
Proceed with full 6-step protocol (Steps 1–6).
MIXED → Simplified Version
Proceed with 5-minute simplified version only.
ANY RED → Postpone Today
Offer a movement break or sensory calming input. Document why session was postponed — this data is valuable.

Step 1 of 6 | 30–60 seconds
Step 1: The Invitation
Every protocol begins with an invitation, not a command. This is the ABA principle of pairing — establishing materials and space as associated with good things before introducing any demand.
The Script — Say This Exactly
"Hey [child's name], I've got something really cool here. Wanna see?"
[Gesture toward kick-appropriate target without touching it]
"This is our kicking ball. Only for kicking. Want to try?"
Body Language
Crouch to eye level | Open palms visible | Relaxed facial expression | Give 10–15 seconds to process before expecting response
Acceptance Cues (What YES Looks Like)
- Moving toward the material
- Eye gaze toward the target
- Body orientation shifts toward the space
- Verbal "yeah" or approximation
If Child Resists
Moves away: "That's okay, we can just look at it for now." Reduce demand.
Ignores: Wait 30 seconds, re-present with preferred item nearby.
Tries to kick you: Calmly step back: "The ball is for kicking, not me." No emotional reaction.
Step 2 of 6 | 1–3 minutes
Step 2: The Engagement
The child is in. Now deepen the interaction. Introduce each material with a clear, simple script. The goal is familiarity and positive association before any demand is placed.
Introduce Kick-Appropriate Target
"See this ball? This is our safe kicking ball. Watch this." [Adult gently kicks ball — model the action] "Now you try. Give it a good kick!" Provide gestural or light physical guidance if needed.
Introduce Communication Card
"And look — this is your BREAK card. When you want a break, you hand me this. And I'll always say yes." Practice once in low-stakes context immediately.
Show Emotion Chart
"This is our feelings chart. This is calm. This is frustrated. This is REALLY frustrated. Let's practice pointing." Keep tone light, curious, exploratory.
Reinforcement Cue: First successful kick of appropriate target = immediate specific praise: "You kicked the ball! Safe feet!" This is the moment the new neural pathway begins to form.

Step 3 of 6 | 5–12 minutes
Step 3: The Therapeutic Action
This is where change is built. Repetition is the medicine. The core session has four components executed in sequence. Spend 40–60% of your total session time here.
A. Appropriate Outlet Training
Present kick urge trigger (verbally or naturally occurring). Immediately prompt: "Feet need to kick? Kick the ball!" Guide child to target. Allow full-force kick. Narrate: "Kick the BALL. Safe feet. Good kick."
B. Communication Replacement Drill
Practice break card exchange in 3 graduated scenarios: low demand → medium demand → approaching frustration. At each level: child hands card → parent immediately says "Okay, break!" (2-min break honored every time.)
C. Heavy Work Proprioceptive Input
3–4 minutes of structured heavy work: wall push-ups ×10, resistance band leg press ×8, jumping on spot ×20. Script: "Let's give your body the heavy work it's asking for."
D. Emotion Check-In
Point to emotion chart: "Where are you right now?" Validate whatever level is named. If elevated: implement calming strategy BEFORE level reaches red. Do not wait for escalation.
Critical Error to Avoid: Never provide the kick target AFTER a child kicks a person — this accidentally reinforces aggression. Provide the target PROACTIVELY, before the kick occurs.

Step 4 of 6 | 3–5 minutes
Step 4: Repeat & Vary
3 good repetitions are worth more than 10 forced ones. Watch for satiation signs — when the child disengages or looks away, end the cycle. Do not force repetition past natural satiation.
Material | Target Reps | Satiation Signs | |
Kick-appropriate target | 5–8 quality kicks | Child stops seeking target spontaneously | |
Communication card use | 2–3 successful exchanges | Child hands card without prompting | |
Heavy work sequence | 1 full round (10-8-20) | Visible arousal reduction; body softens | |
Emotion chart check-in | 2–3 check-ins | Child anticipates and initiates check-in |
Variation Options to Prevent Saturation
Change the Target: Swap therapy ball for floor kick target. Same proprioceptive principle, new stimulus.
Increase the Distance: Move kick target 1m further. Motor challenge increases with same outlet.
Add Language: "What are you going to kick?" → child responds "BALL" before kicking. Communication + action together.
Child Leads: "You be the teacher today. You tell me the rules." Metacognitive step for older children.
Simulated Trigger: With older children, roleplay a frustrating scenario (someone takes toy). Practice card + redirection before a real event.

Step 5 of 6 | 1–2 minutes
Step 5: Reinforce & Celebrate
What gets celebrated, gets repeated. Reinforcement delivered within 3 seconds of the desired behavior is 4× more effective than delayed praise. Timing matters more than magnitude.
Behavior | Exact Script | Delivery | |
Kicks target instead of person | "You kicked the BALL! Safe feet! That was PERFECT!" | Immediate, enthusiastic, with token if using board | |
Uses break card | "You used your words! Amazing! Break — 2 minutes, starting now." | Honor break FIRST, praise second | |
Names emotion on chart | "You told me you're frustrated. That's so smart. Let's handle it together." | Warm, validating tone | |
Completes heavy work | "Look at those strong legs! All that energy — in the right place!" | High-five or fist bump if tolerated | |
Full session with safe feet | "Safe feet all session! You EARNED it!" | Preferred reward from menu |
Celebrate the Attempt Too
"You tried to use the card. That was a brave try. Next time you'll be faster."
Effort-based reinforcement builds resilience and encourages continued attempts even when the skill is not yet fluent.
Step 6 of 6 | 2–3 minutes
Step 6: The Cool-Down
No session ends abruptly. The cool-down is the last therapeutic act. Abrupt endings are a major trigger for transition-related kicking — the very behavior you are treating.
Transition Warning Script
"Two more kicks on the ball, then we're all done for today."
[After 2nd kick]: "One more. Last one."
[After final]: "All done! Great work today. Let's put the ball away together."
Use the Visual Timer
Show the timer counting DOWN during cool-down. The child sees time ending — it is never a surprise.
Cool-Down Sequence
- Material put-away ritual — child participates
- 2 minutes of quiet sensory activity (weighted lap pad, slow rocking)
- Transition object placement — give child the soft comfort toy
- Transition to next activity with First-Then board
- Final affirmation: "I'm proud of you today."
If Child Resists Ending
"No, more!" (regulated): Honor 2 more kicks, then firm: "All done now."
Meltdown at session end: Session was too long — note for adaptation and shorten next time by 20%.

ACT III: Data
Capture the Data: 60 Seconds of Data Now Saves Hours of Guessing Later
What to Record (2–3 Data Points Only)
1. Kicking Incidents Today: [ ] 0 [ ] 1 [ ] 2 [ ] 3+
Target kicked instead of person? [ ] YES [ ] NO
Target kicked instead of person? [ ] YES [ ] NO
2. Communication Card Used: [ ] Independently [ ] With prompt [ ] Not used
3. Overall Regulation (1–5):
1 = Fully calm | 5 = Crisis
1 = Fully calm | 5 = Crisis
Notes: Any patterns, triggers, surprises, or wins worth recording for your therapist.
Download Tracking Sheet
GPT-OS® Integration
Data entered feeds into your child's Behavioral Safety Readiness Index on GPT-OS®. Each data point is one step toward a more personalized intervention plan.
GPT-OS® learns which of the 9 materials produces the fastest behavioral reduction for your specific child profile — and updates your plan automatically.

What If It Didn't Go As Planned?
Session abandonment is not failure. It's data. Every difficult session tells you something precise about your child's nervous system. Here are the 6 most common challenges and exactly what to do.
"Child refused to engage with kick target at all"
Why: Unfamiliarity, target too stiff/soft, or high baseline arousal. Fix: Remove demand. Introduce target passively — put it in the space without requiring use. Let child encounter it at own pace over 3 days before requesting its use.
"Child kept trying to kick me instead of the target"
Why: Target not close enough; function may be attention-seeking. Fix: Place target between you and child. Say once: "Ball, not me." Step back (remove attention). When child kicks ball: REWARD massively.
"Child used break card, I honored it, then kicked immediately after"
Why: Card use is in early stages — still being tested for reliability. Fix: This is PROGRESS. Lengthen break slightly. Stay consistent — consistency beats perfection every time.
"Child got more escalated during heavy work"
Why: Some children are aroused UP by heavy work before regulating. Fix: Move heavy work to 30 min BEFORE session as pre-loading, not during. Or switch to calming proprioceptive input (weighted lap pad, bear hugs).
"Child kicked sibling during session"
Why: Sibling = proximity trigger. Session was not in protected space. Fix: Enforce one-person rule for sessions. Use visual "therapy in progress" indicator on door.
"Nothing went right and I ended up in tears"
Why: This is a hard road. You are human. Fix: Rest. The session failing is information, not verdict. 📞 Call: 9100 181 181 — our team is there for you.
Adapt & Personalize: No Two Children Are Identical
This technique bends to fit your child. Use the profile guides below to modify the protocol based on your child's sensory style, communication level, age, and setting.
Sensory Seeker
Loves intense input → Increase kick target firmness | Add heavier resistance bands | Increase heavy work duration | May need more reps before satiation
Sensory Avoider
Sensitive to input → Softer kick target | Start with hand pressing instead of full kicking | Lighter weighted lap pad | Shorter sessions, more cool-down time
Limited Communication
Pre-verbal → Picture exchange for break card | Single symbol board | Heavy reliance on visual boundary markers | Prioritize heavy work over language-based steps
Older Child (7–10)
Involve child in designing token board | Introduce self-monitoring checklist | Practice explaining needs to teacher | Social story becomes collaborative writing
Age | Focus | Duration | Setting | |
2–3 years | Kick target + heavy work only | 5–8 min | Home only | |
4–5 years | Full kit; introduce communication card | 10–15 min | Home + school with support | |
6–10 years | Full protocol + self-monitoring | 15–20 min | Home + school + community |
ACT IV: Progress
Week 1–2: Don't Look for Mastery. Look for Tolerance.
15%
Progress Arc
Week 1–2 position on the full intervention arc. Foundation is being laid. Neural pathways are forming their first impressions.
What You Might See | What It Means | |
Child kicks target 2–3 times then tries to kick you again | Normal. Target is new. Function hasn't transferred yet. | |
Child holds break card, doesn't use it yet | Awareness is emerging. This is a win. | |
Heavy work provides brief calm then child escalates again | Short regulatory window is expected. It will extend. | |
Kicking frequency may temporarily INCREASE | Extinction burst — the old behavior is being challenged. NORMAL and TEMPORARY. | |
Child seems more interested in kick target than in session | Perfect. This means the target is reinforcing. |
Parent Emotional Preparation: Weeks 1–2 are the hardest. You will doubt. Track the data (Card 20). The data will tell you what your emotions can't see yet. "If your child tolerates the kick target for 3 seconds longer than last week — that is real neurological progress."
Week 3–4: Neural Pathways Are Forming. Watch for These Signs.
40%
Progress Arc
Week 3–4 consolidation phase. The new pattern is beginning to compete with the old one — and starting to win.
Behavioral Signal | What's Happening Neurologically | |
Child moves toward kick target before kicking occurs | Anticipatory planning — prefrontal engagement increasing | |
Break card used 1–2x without prompting | Functional communication replacing motor behavior | |
Emotion chart pointed to without adult initiation | Interoceptive awareness developing | |
Kicking at persons is less impulsive — there's a pause | Inhibitory control emerging | |
Child names the kick target ("my ball") | Ownership = sustained engagement |
Week 5–8: Mastery Indicators
Mastery is not perfection. It's independence. The goal is a child who accesses their tools without being prompted — across settings, across caregivers, across days.
75%
Progress Arc
Week 5–8 mastery zone. Skills are generalizing. Independence is emerging. The intervention is working.
Mastery Criteria — Specific, Observable, Measurable
Child accesses kick target independently when frustrated (without adult prompt) — 4 out of 5 opportunities
Child uses break card or verbal equivalent independently — 3 out of 5 opportunities
Kicking of persons reduced ≥70% from baseline across 2 consecutive weeks
Behavior maintained across 2+ settings (home + school OR home + community)
Parent reports confidence managing behavior without crisis feeling
Maintenance Check (Week 8): Remove kick target for 3 days. Does kicking behavior remain reduced? Does child seek alternative regulation? YES to both = true skill acquisition. NO = more practice needed; return to protocol.

Celebrate This Win
"You showed up, session after session, even on the days you doubted everything. You gave your child a safer body, a more connected nervous system, and a voice that doesn't need to kick to be heard."
Appropriate Outlet ✅
Your child now has at least one appropriate outlet for motor need.
Communication Tool ✅
Your child has a communication tool that adults honor — and that works.
Nervous System ✅
Your child's nervous system has been given the input it was seeking — appropriately.
School Access ✅
Your child's school access and inclusion are protected.
Journal Prompt: "Write 3 sentences about the day you first saw your child reach for the ball instead of kicking you. Keep that page forever."
Red Flags: When to Pause and Seek Help
Trust your instincts. If something feels wrong, pause and ask. This protocol is designed for mild-to-moderate kicking that responds to antecedent management. Some situations require professional escalation immediately.
What It Looks Like | What to Do | Level | ||
🔴 | Kicks becoming harder or more targeted even after 4+ weeks | Stop protocol; seek BCBA functional re-assessment | Level 2–3 | |
🔴 | Child causes injury to self or others | Medical assessment first; crisis protocol | Level 3–4 | |
🔴 | Biting, hitting, throwing begin alongside kicking | Expanded behavioral assessment needed | Level 3 | |
🔴 | Sudden return to baseline or worse after apparent progress | Check for medical trigger (pain, illness, sleep disruption) | Level 2 | |
🔴 | Parent or sibling at genuine risk | Immediate professional consultation | Level 4 | |
🔴 | Child cannot participate in school due to kicking | Requires FBA + BIP through BCBA immediately | Level 3 |
📞 FREE National Autism Helpline: 9100 181 181 | Available in 16+ languages | 24×7
"Call before the next incident. Not after."
"Call before the next incident. Not after."
Domain Navigation
Related Techniques: You Already Have the Materials
The 9 materials in your D-383 kit overlap significantly with adjacent techniques in Domain D. You are already resourced to begin several of these without additional investment.
D-381: Hitting Others
🟡 Core | Primary Material: Communication Cards — which you already have from D-383
D-382: Pushing and Shoving
🟡 Core | Primary Material: Visual Boundaries — your emotion chart and floor markers serve this purpose
D-385: Throwing Objects
🟡 Core | Primary Material: Kick Target (same ball serves as throw target with modification)
D-390: Aggression During Transitions
🟡 Core | Primary Material: Visual Timer (same) — you are already equipped
C-254: Emotion Regulation Body Strategies
🟢 Intro | Primary Material: Emotion Chart — already in your kit
D-384: Biting Others
🔴 Advanced | Primary Material: Oral-Motor Tools + Communication Cards — partial kit overlap
Your Child's Full Developmental Map
This technique is one piece of a larger plan. Your child's journey is not defined by one behavior. It is mapped across all 12 domains, personalized, and progressing.
Current Position: Domain D
D-383 addresses behavioral safety — one of 5 readiness pillars tracked by GPT-OS®. You are building the foundation that makes all other domains accessible.
Common Co-Active Domains
Domain A: Sensory Processing — often the root driver of kicking
Domain C: Emotional Regulation — supports the self-management layer
Domain B: Social Communication — provides the alternative voice

ACT V: Community
Families Who've Been Here: From the Same Fear to a Different Life
Before — Then After (8 Weeks)
Before: "He was about to be expelled from preschool at age 4. Three kicking incidents in one week. I had a meeting with the principal and I cried the whole way home."
After: "He's in a regular classroom. Last month his teacher said he had his first week with zero incidents. I kept that message." — Parent, Pinnacle Hyderabad Network (anonymized)
Before — Then After (6 Weeks)
Before: "My daughter would kick during every transition. School pickup, bath time, dinner. It felt like we were tiptoeing through our own house."
After: "We set up a visual timer for every transition. She watches it. The kicking at transitions almost completely stopped. It was so simple. I can't believe we didn't have this years ago." — Parent, Pinnacle Bengaluru Network (anonymized)
"In our clinical experience across 70+ centers, the most common turning point is when parents begin to see the behavior as communication. Once that reframe happens, the intervention follows naturally. The materials just give that reframe a structure." — BCBA Senior Supervisor, Pinnacle Blooms Network
Individual results may vary. Vignettes are composite and anonymized. Statistics represent aggregate outcomes across the Pinnacle Blooms Network.

Connect With Other Parents: You Are Not a Solo Operator
WhatsApp Parent Group
Pinnacle Parent WhatsApp Group — Behavior Support: 400+ families navigating the same challenges, moderated by a Pinnacle BCBA. Join to share wins, ask questions, and find solidarity.
Online Community Forum
Pinnacle Parent Community Forum with discussion threads specific to Domain D challenges. Find parents at exactly the same stage you are — Week 1, Week 3, post-mastery.
Peer Mentoring
Connect with a parent who has completed D-383 successfully and can offer lived-experience guidance. Their story is your roadmap. Their confidence is your permission slip.
Local Parent Meetups
Monthly parent support groups at all 70+ Pinnacle centers. In-person connection with families on the same journey — in your city, in your language.

Your Professional Support Team: Home + Clinic = Maximum Impact
Your Need | Specialist | How They Help | |
Behavior assessment + BIP | BCBA | Functional Behavior Assessment, replacement behavior design, data-driven intervention planning | |
Sensory processing evaluation | Pediatric OT (SI Certified) | Proprioceptive diet, sensory profile, heavy work programme design | |
Communication alternatives | Pediatric SLP (AAC Specialist) | Communication card design, PECS, alternative communication systems | |
School-based support | Special Educator | Teacher training, classroom BIP, academic inclusion planning | |
Medical evaluation | NeuroDev Pediatrician | Rule out pain, medical drivers, medication review when relevant |
Teleconsultation Available
Can't visit a center? Our teletherapy service brings Pinnacle's consortium expertise to your screen — wherever you are in India.
70+ Centers Across India
Hyderabad, Bengaluru, Chennai, Mumbai, Delhi, and 65+ more cities. One center. Every discipline. One converged plan.
📞 9100 181 181 | FREE | 16+ Languages | 24×7

How GPT-OS® Uses Your Data: Your Data Helps Every Child Like Yours
What GPT-OS® Learns From Your Data
- Which of the 9 materials produces fastest behavioral reduction for your child's profile
- Whether your child's function is primarily sensory, escape, or communication
- How your week-by-week trajectory compares to similar child profiles
- When to recommend escalating to clinical support vs. continuing home protocol
Privacy Assurance
All data is processed under Indian IT Act (2000) and GDPR-aligned standards. Data is anonymized at population level. Your child's identity is never shared.
Your data makes everyone's child better — contributing to a continuously improving population-level therapeutic intelligence system.

Frequently Asked Questions
Real questions from real families, answered by Pinnacle's BCBA Consortium. Didn't find yours? Call 9100 181 181 or book a teleconsultation.
"Isn't providing a kick target just rewarding the kicking behavior?"
No. Providing an appropriate outlet addresses the sensory-motor need driving the behavior. You are redirecting the impulse to an appropriate target while teaching discrimination (safe targets vs. people). This is a core function-based intervention principle. Withholding all kicking opportunities often escalates behavior.
"My child uses the break card to avoid everything. When do I honor it?"
In weeks 1–4: ALWAYS honor it, every time, with no delay. The break card must be more effective than kicking for the replacement to work. After reliable card use (weeks 5–8), you can introduce a "just 1 more minute" delay protocol. The foundation must be unconditional trust first.
"How long will this take to see real results?"
Based on 20M+ sessions: most families see measurable reduction within 3–4 weeks of consistent daily execution. Full behavioral mastery (generalized to school and community) typically requires 6–12 weeks. Consistency is the single strongest predictor of success.
"What if kicking happens at school and I can't control the environment?"
This is why the teacher communication template (Card above) is critical. A portable school kit — communication card, mini visual timer, transition warnings — can be implemented by the teacher with minimal training. Contact Pinnacle for school support programs.
"My child kicks when I try to implement the protocol. Is it counterproductive?"
This is common in weeks 1–2 (extinction burst). Behavior temporarily increases when an old reinforcer is removed. It is not a sign the protocol is failing — it is a sign the old pattern is being challenged. The burst typically peaks in days 3–7 and then begins to reduce.
"Do we need a BCBA or can we do this at home?"
For mild-moderate kicking that responds to antecedent management: home implementation as described is appropriate. For kicking that causes injury, results in school exclusion, or includes multiple aggressive topographies: a BCBA functional behavior assessment is strongly recommended before proceeding.

The Pinnacle Promise
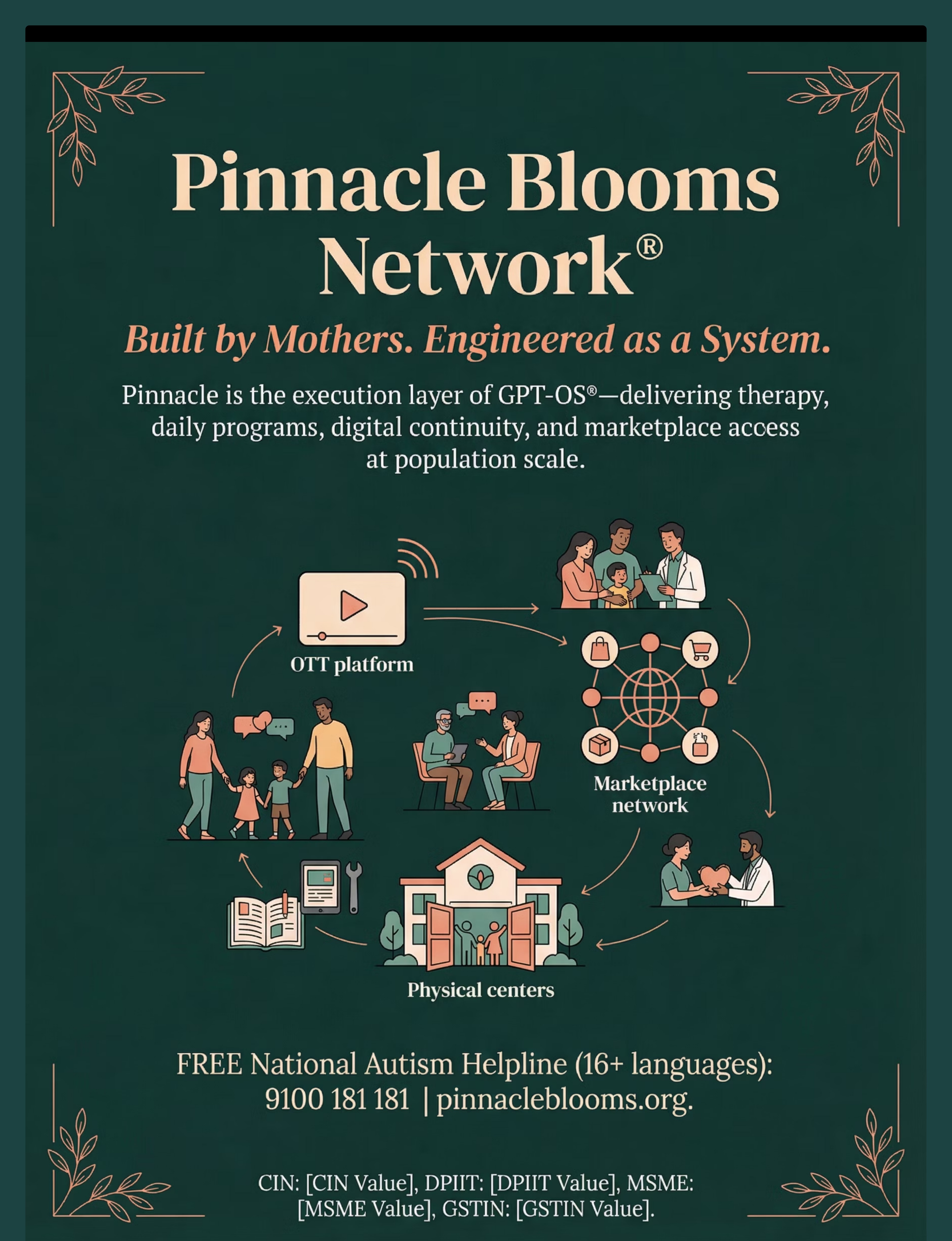
🌿 Pinnacle Blooms Network®
Built by Mothers. Engineered as a System.
OT │ SLP │ ABA/BCBA │ SpEd │ NeuroDev │ CRO
WHO/UNICEF-Aligned │ DPIIT Recognised │ MSME
WHO/UNICEF-Aligned │ DPIIT Recognised │ MSME
"From fear to mastery. One technique at a time."
You arrived on this page scared and exhausted. You leave with 9 materials, a 6-step protocol, a progress arc, a community, a research foundation, and a team. That is what GPT-OS® was built to give every family on Earth.
Navigate This Resource
Medical Disclaimer
This content is educational. It does not replace individualized assessment by licensed behavior analysts, occupational therapists, or developmental specialists. Physical aggression that causes harm, prevents participation, or is resistant to basic strategies should be addressed by qualified professionals. Individual results may vary.
Statutory Identifiers
© 2025 Pinnacle Blooms Network®, unit of Bharath Healthcare Laboratories Pvt. Ltd. | CIN: U74999TG2016PTC113063 | DPIIT Recognition: DIPP8651 | GSTIN: 36AAGCB9722P1Z2

More Frequently Asked Questions
"Is kicking a sign of autism?"
Kicking behavior is not diagnostic of autism — it appears across neurotypical children and those with various developmental profiles. It is more common and more persistent in children with sensory processing differences, communication deficits, and impulse control challenges — which are more prevalent in autism. Kicking behavior alone is not a diagnostic indicator.
"My child is 8 and still kicks. Is it too late?"
No. Function-based intervention works across the age range. Older children may require longer skill-building timelines and explicit metacognitive strategies (self-monitoring, social reasoning), but the core approach remains valid. Pinnacle has successfully supported children through adolescence with persistent aggression challenges.
Didn't find your answer? Call 📞9100 181 181 (FREE, 16+ languages, 24×7) | Ask GPT-OS® → | Book Teleconsultation with BCBA →
Preview of 9 materials that help with kicking others Therapy Material
Below is a visual preview of 9 materials that help with kicking others therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.








Link copied!
Your Next Step: Start Now
The best time to start was at the first kick. The second best time is right now.
20M+
Therapy Sessions
Exclusive 1:1 sessions delivered across the Pinnacle Blooms Network
97%+
Measured Improvement
Across readiness indexes in children who complete the full protocol
70+
Centers in India
Across Hyderabad, Bengaluru, Chennai, Mumbai, Delhi, and 65+ more cities
📞FREE National Autism Helpline: 9100 181 181 | 16+ Languages | 24×7 | Pinnacle Blooms Consortium Validated: OT • SLP • ABA/BCBA • SpEd • NeuroDev • CRO • WHO/UNICEF-Aligned • DPIIT Recognised