
D-387 | Challenging Behaviors & Social Safety
When hands move before the brain catches up.
Pushing hands isn't a moral failure. It's a regulatory signal your child's nervous system is sending — and it can be answered. This complete guide gives you 9 clinically validated materials to address the root causes.

ACT I: Why This Happens
You Are Among Millions of Families Navigating This Right Now.
Physical boundary challenges in children with developmental differences are among the most common — and most misunderstood — behavioral presentations worldwide. When a parent sees these numbers, the isolation dissolves. You are not alone in a broken house. You are part of the largest parenting journey on Earth.
80%
Sensory Difficulties
of children with ASD display sensory processing difficulties that can drive physical contact-seeking behavior
1 in 36
ASD Diagnosis Rate
children in the US are diagnosed with ASD (CDC, 2023) — over 18 million estimated in India
60–70%
ADHD & Impulse
of children with ADHD demonstrate impulse control challenges manifesting as physical behavior before age 8
In India alone, an estimated 10+ million families are navigating challenging physical behaviors in children with developmental differences. WHO data confirms pushing and physical aggression are among the top 3 parental concerns in pediatric developmental services across 54 low- and middle-income countries.

The Neuroscience
This Is a Wiring Difference. Not a Behavior Choice.
The Clinical Science
The Proprioceptive System: The proprioceptive sense — housed in muscles, joints, and tendons — tells the brain where the body is in space and how much force is being used. In children who push, this system is often under-responsive: the brain is not receiving sufficient proprioceptive feedback from normal daily movement.
The Result: The brain sends an urgent signal — "I need more input. NOW." The closest available source of intense proprioceptive input? Another person's body.
The Impulse Control Layer: The prefrontal cortex — responsible for stopping impulses before they become actions — matures slowly, reaching full development only by age 25. In children with ASD, ADHD, or developmental delays, this maturation is further delayed. The hands move. The brain catches up 0.5 seconds later.
The Communication Pathway: When a child cannot verbally express "move please," "you're too close," or "I need space," the motor system finds the most efficient alternative: push.
What This Means for Your Child
🧠 Their body is hungry.
Not for food — for physical pressure signals. Pushing gives an intense sensation that momentarily satisfies a neurological craving.
⚡ Their brain can't stop in time.
The impulse to push fires before the "this will hurt someone" thought can intercept it. This is not defiance — it is an immature inhibition circuit.
💬 Their words aren't loaded yet.
Many children push because they literally do not have a word, sign, or card available that says "I need you to move." Pushing is faster.
📍 They cannot see what they cannot see.
Personal space is invisible. For many children with ASD, the 60-centimeter bubble around another person's body genuinely does not register as a boundary.

Developmental Context
Your Child Is Here. Here Is Where We're Heading.
Age 1–3 yrs
Toddler pushing is developmentally expected. Impulse control minimal. Redirection begins.
Age 3–5 yrs
Beginning space awareness develops. Verbal alternatives emerging. Impulse control consolidating.
Age 5–8 yrs
Basic hands-to-self expected. Impulse control consolidating. Transition to mastery zone.
Age 8–12 yrs
Internalized social boundaries. Persistent pushing = clear intervention need.
Common Co-occurring Conditions Where Pushing Persists Beyond Typical Development: Autism Spectrum Disorder (sensory processing + personal space unawareness + communication gaps) · ADHD (impulse control deficit + hyperactive proprioceptive seeking) · Sensory Processing Disorder · Developmental Delay · Language/Communication Disorders.
❌ What Is NOT Happening
Your child is not aggressive by nature. This is not a parenting failure. This is not permanent without intervention.
✅ What IS Happening
A developmental system is under-regulated and can be systematically supported with the right tools.

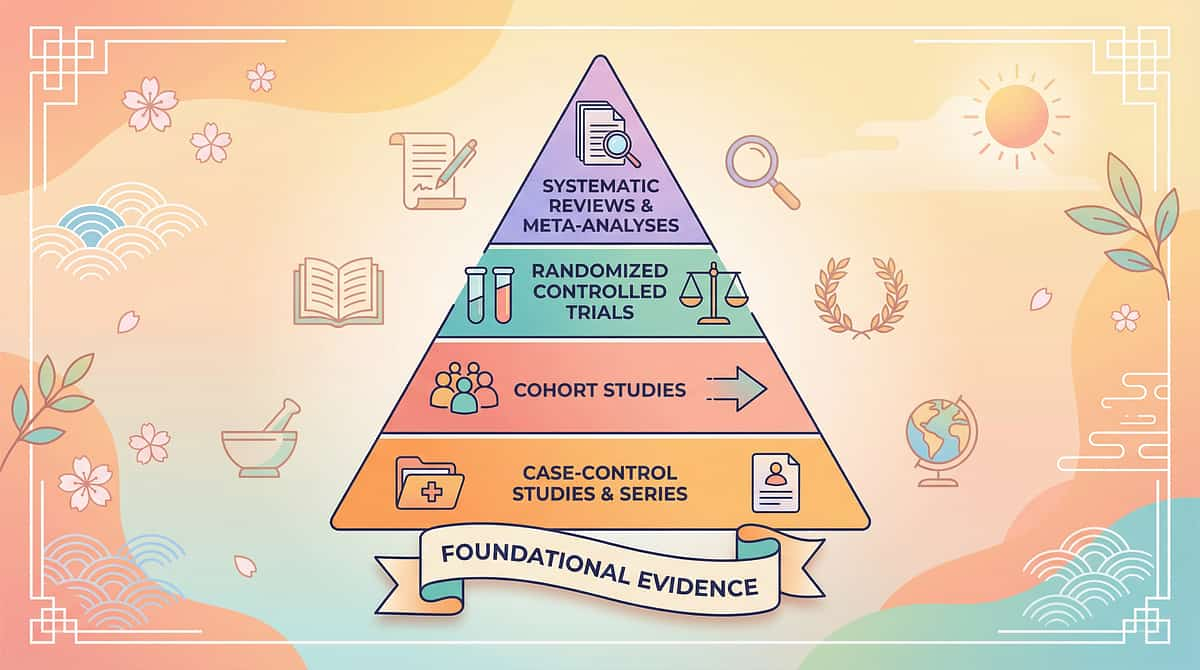
Evidence Grade: Level I
Clinically Validated. Home-Applicable. Parent-Proven.
These are not experimental suggestions. These are materials that thousands of occupational therapists, ABA practitioners, and pediatric specialists have used in clinical settings — now translated for your home.
Study | Key Finding | Evidence Level | |
PRISMA Systematic Review (2024, PMC11506176) | Sensory integration intervention meets criteria as evidence-based practice for ASD — 16 studies, 2013–2023 | Level I | |
Meta-analysis, World J Clin Cases (2024, PMC10955541) | Sensory integration therapy significantly promotes social skills, adaptive behavior & motor control across 24 studies | Level I | |
Padmanabha et al., Indian J Pediatr (2019) | Home-based sensory interventions show significant outcomes in Indian pediatric population | RCT — Level II | |
NCAEP Evidence-Based Practices Report (2020) | ABA-based reinforcement + communication interventions classified as evidence-based for autism | Level I | |
Frontiers in Integrative Neuroscience (2020) | Neurological framework for sensory-based intervention in ASD established | Level II |
Confidence Level: HIGH — Converging evidence from behavioral and sensory science. Free National Helpline: 📞 9100 181 181
ACT II: The Materials
D-387: 9 Materials That Help With Pushing Others
Formal Definition
Formal Name: Multi-Modal Sensory-Behavioral Material Protocol for Physical Boundary Development
Parent-Friendly Name: "The Pushing Toolkit — 9 Tools That Get to the Root"
A systematically selected set of 9 therapy materials — drawn from Occupational Therapy, Applied Behavior Analysis, Speech-Language Pathology, and Sensory Integration science — that address pushing behavior by targeting its multiple underlying causes simultaneously.
What These 9 Materials Address
The sensory need driving the push
The communication gap behind the push
The spatial unawareness enabling the push
The regulatory dysregulation triggering the push
The reinforcement contingency maintaining the push
ABA
Applied Behavior Analysis
Pediatric OT
Occupational Therapy
SLP
Speech-Language Pathology
Sensory
Integration Science
Age 2–12
All developmental profiles

This Technique Crosses Therapy Boundaries Because the Brain Doesn't Organize by Therapy Type
🟣 Pediatric Occupational Therapist (Lead Discipline)
Sensory assessment, compression vest protocol, heavy work sensory diet design, crash pad use guidelines. Materials: Compression Vest · Heavy Work Kit · Crash Pad · Body Awareness Games
🔵 ABA / BCBA Therapist
Functional behavior assessment, token economy design, reinforcement schedule, communication card training. Materials: Token Board · Communication Cards · Reinforcement Menu
🟤 Speech-Language Pathologist
Communication alternative design, AAC integration, functional communication training (FCT). Materials: Communication Cards · Social Scripts · Vocabulary Building
🟢 Special Educator
Classroom strategy implementation, personal space visual supports, social story integration. Materials: Space Markers · Social Stories · Token Board
🔴 NeuroDevelopmental Pediatrician
Root cause identification, sensory profile review, medical contraindication clearance. Oversees all material selection.
"When OT addresses the sensory root, ABA builds the replacement behavior, and SLP gives the communication tool — pushing often decreases dramatically without ever 'punishing' the push itself." — Pinnacle Blooms FusionModule™ Clinical Protocol

Precision Targeting — Not a Random Collection of Materials
Target | Week 1–2 | Week 3–4 | Week 5–8 | |
Pushing frequency | Slight reduction in duration | Reduced in structured settings | Consistent hands-to-self in familiar contexts | |
Communication | Prompted use of cards/words | Emerging spontaneous use | Independent requesting instead of pushing | |
Regulation | Child notices pre-push signals | Using calm-down tools before meltdown | Self-initiating regulation strategies |

Material 1 of 9
Material 1: Weighted Compression Vest
Why It Works
Delivers continuous deep pressure input to the trunk — meeting the nervous system's demand for heavy feedback without requiring contact with another person. The vest satisfies the proprioceptive craving that drives pushing, worn proactively during high-risk times.
Canon Category: Compression/Weighted Items
Root Cause Addressed: Proprioceptive sensory seeking
Price Range: ₹2,000–6,000
Root Cause Addressed: Proprioceptive sensory seeking
Price Range: ₹2,000–6,000
How to Use
Wear during high-risk times: playground access, transitions, crowded settings. Max 10% of child's body weight. 20–30 min wear cycles only. Never during sleep.
🔴 OT supervision required — especially for children under 25kg or with joint hypermobility.
Search: Amazon.in: "weighted compression vest children sensory"
🔴 Pinnacle Recommends — OT assessment before first use

Materials 2–4 of 9
Materials 2, 3 & 4: Space, Heavy Work & Communication

Material 2: Personal Space Visual Markers
Root Cause: Personal space unawareness. Makes the invisible visible — hula hoops, floor tape squares, carpet spots show children where their space ends and another person's begins.
Price: ₹200–1,000 · Amazon.in: "hula hoop kids" + "floor tape colored"

Material 3: Heavy Work Activity Kit
Root Cause: Proprioceptive seeking + impulse redirection. Push carts, resistance bands, weighted balls, and carrying tasks provide the same intense feedback — redirecting the need, not suppressing it.
Price: ₹500–3,000 · Amazon.in: "resistance bands kids" + "weighted ball children"

Material 4: Visual Communication Cards
Root Cause: Communication gap — pushing as substitute for "move please." Cards pre-loaded with "Move Please," "Too Close," "Excuse Me," "I Need Space" — on a lanyard within constant reach.
Price: ₹200–800 · Amazon.in: "PECS communication cards children"

Materials 5–7 of 9
Materials 5, 6 & 7: Body Awareness, Social Stories & Calm-Down Corner

Material 5: Body Awareness / Proprioceptive Games Kit
Root Cause: Poor body position awareness + force modulation deficit. Freeze dance, balance boards, obstacle courses, and "gentle touch" practice build the internal sensing that makes physical self-control possible.
Price: ₹300–1,500 · Amazon.in: "balance board children" + "obstacle course kids indoor"

Material 6: Social Stories — Hands & Bodies
Root Cause: Lack of social rule understanding. Short, personalized narratives that front-load social knowledge BEFORE high-risk situations — when the child is calm and receptive, not mid-dysregulation.
Price: ₹300–1,000 · Amazon.in: "social story books autism personal space"

Material 7: Calm-Down Corner Setup Kit
Root Cause: Dysregulation → pushing pipeline. A designated regulation space with bean bag, sensory tools, feelings chart, and calm-down visual steps. Gives children somewhere to go BEFORE pushing occurs.
Price: ₹1,000–5,000 · Pinnacle Canon: amzn.in/d/02C5R9Jn (₹589)
Materials 8–9 of 9
Materials 8 & 9: Token Board & Crash Pad
Material 8: Token Board / Visual Reinforcement System
Canon Category: Reinforcement Menus
Root Cause Addressed: Absence of positive contingency for hands-to-self behavior
Root Cause Addressed: Absence of positive contingency for hands-to-self behavior
Makes progress concrete and immediate — tokens earned for every gentle moment, every word used instead of a push, every successful line-wait. Behavior that gets reinforced increases.
Price: ₹200–800 · 🔴 Pinnacle Canon: amzn.in/d/02C5R9Jn (₹589)
Material 9: Crash Pad / Safe Impact Surface
Canon Category: Sensory Crash / Heavy Work Surfaces
Root Cause Addressed: Need for physical impact sensation
Root Cause Addressed: Need for physical impact sensation
For children whose pushing is driven by a need to crash and feel impact — crash pads redirect this need to an appropriate target. The equation changes from "don't crash" to "crash HERE, not on people."
Price: ₹2,000–8,000 · Amazon.in: "crash pad children sensory" + "gymnastics foam mat"
Starter Kit
Cards + Markers + Social Story: ₹700–2,800
Sensory-Focused Kit
Vest + Heavy Work + Crash Pad: ₹4,500–17,000
Complete Setup
All 9 Materials: ₹6,500–26,000

Every Family Can Start Today — Regardless of Budget
WHO/UNICEF Equity Principle: Effective intervention does not require expensive equipment. The therapeutic principle matters more than the branded product.
Material | ₹0 DIY Alternative | Why It Works | |
Compression Vest | Snug-fitting lycra t-shirt layered under regular clothing; tight sports compression undershirt | Provides pressure without weight. Adequate for trial — OT vest for ongoing use. | |
Space Markers | Floor tape (₹50) + chalk circles + arm-length demonstrations with pool noodle | Same visual boundary principle. Tape is non-slip and visible. | |
Heavy Work Kit | Grocery bag carrying, laundry basket tasks, wall push-ups, wheelbarrow walks, digging in sand | Every household has these. Schedule before high-risk activities. | |
Communication Cards | Paper + marker + laminator (or contact paper). Draw simple stick figures with phrases. | Same functional communication principle. Homemade works if consistent. | |
Body Awareness Games | Freeze dance, red light/green light, Simon Says, balance on one foot | Zero equipment needed. 10 minutes before playground. | |
Social Stories | Write your own: 5 sentences, first person, family photos, laminated | Personalized stories often outperform purchased ones. Free templates at Pinnacle. | |
Calm-Down Corner | Corner of room + sofa cushions + stress ball (₹50) + printed feelings chart | Structure and intent matter more than the furniture. | |
Token Board | 5 sticker spaces drawn on paper + stickers + preferred reward listed | Functional token economy starts working from day one. | |
Crash Pad | Pile of sofa cushions + old mattress + pile of large pillows (min 4-inch depth) | Clear all hard objects from landing zone. Supervise always. |
"We have seen children transform with floor tape, paper cards, and a sofa cushion pile. The materials are tools. The relationship, consistency, and understanding you bring — that is the intervention." — Pinnacle Blooms OT Consortium
Safety First
Before Any Session With These Materials — Read This Card
🔴 RED — DO NOT PROCEED IF:
Child has a medical contraindication for compression garments · Child has joint hypermobility syndrome (OT clearance required) · Child is in acute medical distress, fever, or post-seizure state · Crash pad/heavy work attempted without adult supervision · Weighted vest exceeds 10% of child's body weight · Child shows escalating distress, self-injury, or extreme dysregulation during use
🟡 AMBER — MODIFY IF:
Child is tired, hungry, or unwell (simplify to communication cards or social story only) · First introduction of any new material (begin with 2–3 minutes maximum) · Child has shown previous adverse reaction to compression or pressure input · Multiple new materials being introduced simultaneously (introduce one at a time, 1 week minimum between each)
🟢 GREEN — PROCEED WHEN:
Child is in regulated, alert state · Environment is clear of hazards · You have supervision for crash pad and heavy work · OT has cleared compression vest use · Child has had a meal 30+ minutes prior
STOP THE SESSION IMMEDIATELY IF: Child attempts to remove compression vest in distress · Child uses crash pad head-first · Pushing escalates during material introduction · Child becomes severely distressed or self-injurious. Emergency: 📞 9100 181 181

The Right Environment Prevents 80% of Session Failures
Remove From the Space ❌
Television / screens (competing stimulation)
Other children during initial learning phase
High-value preferred items (unless used as reinforcement)
Objects that could become projectiles near crash pad
Other children during initial learning phase
High-value preferred items (unless used as reinforcement)
Objects that could become projectiles near crash pad
Prepare In Advance ✅
Communication cards accessible and on child (not stored away)
Token board mounted at child eye level
Timer visible to both parent and child
Reinforcement menu identified (what is today's reward?)
Compression vest fitted and ready if using
Token board mounted at child eye level
Timer visible to both parent and child
Reinforcement menu identified (what is today's reward?)
Compression vest fitted and ready if using
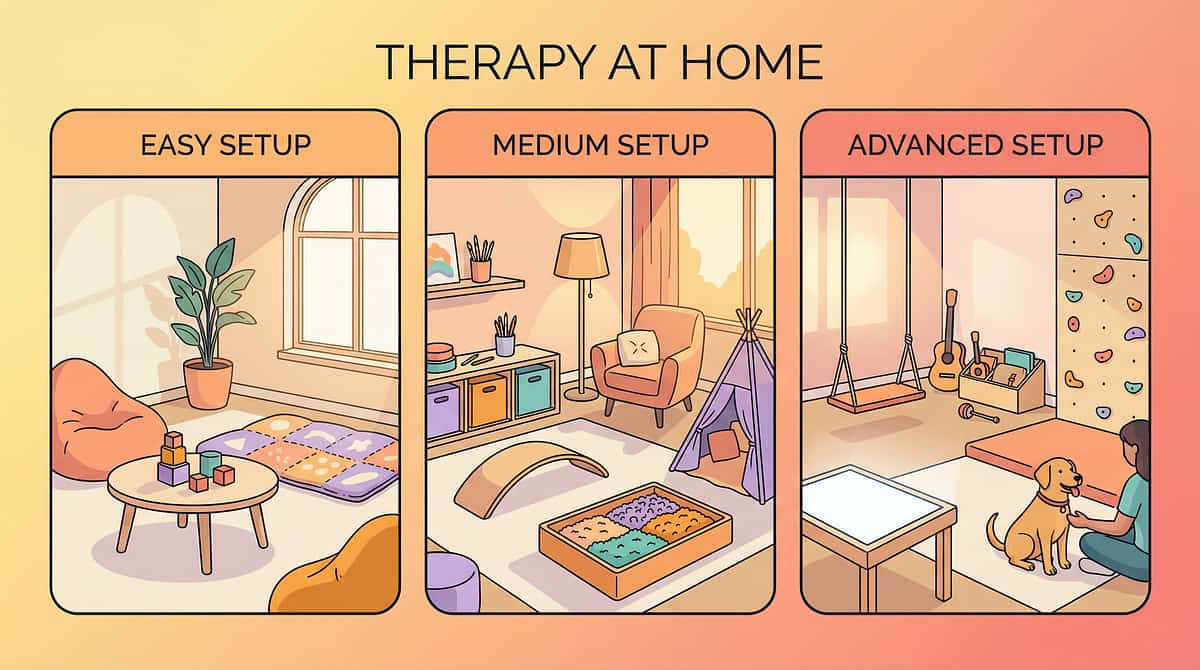
Space Setup Guide
Calm-Down Corner ⑦ — Bean bag + sensory tools against wall with clear access path
Crash Pad ⑨ — Against wall, clear landing zone, minimum 4-inch depth
Space Markers ② — Floor tape circles on ground, child can step in and out
Heavy Work Station ③ — Against wall with equipment ready
Token Board ⑧ — Mounted at child eye level, visible from activity area
Communication Cards ④ — On lanyard around child's neck or velcro near door
Lighting: Natural soft light preferred. Avoid harsh fluorescents.
Sound: Background music optional — instrumental, low volume.
Temperature: Comfortable — compression vest can cause warmth.
Sound: Background music optional — instrumental, low volume.
Temperature: Comfortable — compression vest can cause warmth.

ACT III: How To Use
60-Second Pre-Session Assessment — Don't Skip This
The best session is one that starts right. A 5-minute successful session with good readiness outperforms a 20-minute forced session with dysregulation.
Indicator | ✅ GO | ⚠️ MODIFY | 🔴 POSTPONE | |
Hunger | Fed 30+ min ago | Slightly hungry — offer snack, wait 15 min | Has not eaten in 3+ hours | |
Sleep | Rested night | Slightly tired — shorten to 5 min | Sleep-deprived or just woken | |
Regulatory State | Calm-alert | Slightly activated — start with calm-down corner first | Meltdown in past 30 min | |
Illness | Healthy | Mild cold — sensory activities only, no heavy work | Fever, post-seizure, in pain | |
Recent Incident | No recent pushing | Minor incident more than 1 hr ago | Major incident less than 30 min ago | |
Child Engagement | Approaches materials willingly | Neutral/no preference | Actively avoiding or distressed |
GO ✅ → Proceed to Step 1
Full protocol as designed. All materials ready.
MODIFY ⚠️ → 5 min, cards + story only
Use only communication cards + social story today.
POSTPONE 🔴 → Log it as data
"Session not possible — child state." Try tomorrow. NOT a failure. Data.

Step 1 of 6
Step 1: The Invitation — Not a Command
30–60 seconds. Low demand. High warmth.
The Script — Say Something Like This:
"Hey [child's name], I have something cool to show you. Want to see? You don't have to do anything yet."
For non-verbal children: Show the material. Bring it to the child's level. Tap it. Then step back. Let curiosity do the work.
Your Body Language:
Squat to child's eye level · Relaxed shoulders, soft expression · Material between you and the child (not in front of you) · No direct eye contact demands in this moment
What Acceptance Looks Like ✅
Child moves toward material · Child looks at material (even briefly) · Child vocalizes or gestures interest · Child reaches for material
What Resistance Looks Like ❌
Child moves away → Do NOT chase. Place material on floor and retreat 2 steps. Wait 30 seconds.
Child ignores → Narrate what you're doing with the material while playing with it yourself.
Child pushes material away → Honor it. Try tomorrow. "Not today" is valid data.

Step 2 of 6
Step 2: The Engagement — The Material Comes to Life
1–3 minutes. Introduce the therapeutic material. Watch carefully.
Compression Vest
"Let's try on this special vest. It gives your body a hug." Offer sleeves first. Never force. Allow child to touch fabric for 30 seconds before putting on.
Space Markers
"Let's make your special spot!" Place hula hoop or floor tape together. Invite child to step inside. "This is YOUR bubble. Nobody comes in unless you say okay."
Heavy Work
"Let's do a pushing job! Push this cart from here to there." Make it playful — a delivery mission, a strength challenge, a race.
Communication Cards
"Look — this card says 'Move Please.' When someone is too close, you can hold this up instead of pushing them. Want to try with me?"
Body Awareness Games
"Freeze dance! When the music stops — FREEZE your body as still as a statue!" Begin immediately. Model the freeze with exaggerated stillness.
Social Story
"Let's read our special book about [child's name]." Read together. Point to pictures. Use child's name in the story.
Child Response | Meaning | What to Do | |
Engagement — Active interaction | Material is resonating | Continue. Add Step 3. | |
Tolerance — Passive presence | Child is processing | Narrate, don't demand. Give 60 seconds. | |
Avoidance — Turns away | Too much too fast | Back up. Offer from farther away. Reduce demand. |

Step 3 of 6
Step 3: The Therapeutic Action — The Active Ingredient
5–15 minutes depending on material. This is the heart of the intervention. Duration: 40–60% of total session time.
🔵 Compression Vest
Child wears vest for 20–30 minutes during a high-risk activity (playground, sibling play, group setting). Do NOT use during physical activity that causes overheating. Document wear duration and child's behavioral state.
🟣 Space Markers
Practice entering and exiting marked spaces. Role-play: "Someone is walking toward your bubble. What do you do?" Fade hula hoop → floor tape → visualization only over weeks.
🟤 Heavy Work Kit
Wall push-ups (10 reps), loaded backpack carrying (3 trips), push weighted cart (5 min), wheelbarrow walks (3 lengths). Schedule 10–15 minutes BEFORE high-risk social activity — not after pushing has occurred.
🟠 Communication Cards
Run practice scenarios in calm setting. "Pretend I'm standing too close. What do you do?" Child holds up card → you immediately honor it: step back, say "Oh! You used your card! I'm moving!" Reinforce immediately.
🟡 Body Awareness Games
Freeze dance for 5 minutes. Then "gentle touch" practice — "Show me soft touch. Now firmer touch. Which one feels like a hug? Which one feels like pushing?" Build vocabulary for touch intensity.
🟢 Social Story
Read once per day during calm, connected moment (bedtime, after breakfast). Never read as a consequence of a pushing incident. After reading: "What did [child's name] do when someone was too close?"
🔴 Calm-Down Corner
Practice entering corner voluntarily during a calm moment daily. "Let's go to the calm corner and practice taking 5 breaths." Normalize BEFORE crisis. Child should associate it with comfort, not punishment.
🟤 Token Board
Set target behavior for today's session (e.g., "5 minutes of play without pushing"). Deliver token IMMEDIATELY when behavior occurs. Pair with specific verbal praise: "You asked him to move with your card! That's a token!"
⚫ Crash Pad
"Crash time!" — designate 5-minute crash breaks before playground, before sibling play, before transitions. Teach the phrase "I need crash time" — honor it every time. Redirect the need, never suppress it.

Step 4 of 6
Step 4: Repeat & Vary — Dosage Matters
3–5 minutes. 3 good repetitions outperform 10 forced ones.
Material | Daily Repetitions | Weekly Frequency | |
Compression Vest | Wear 20–30 min daily | Every day (routine use) | |
Space Markers | 3–5 practice scenarios | Daily in structured setting | |
Heavy Work | 10–15 min activity set | Daily, before high-risk times | |
Communication Cards | 5–10 prompted practice trials | Daily practice + natural use | |
Body Awareness Games | 5–10 min gameplay | 5–7 days/week | |
Social Story | 1 reading | Daily (calm moment) | |
Calm-Down Corner | 1 voluntary visit practice | Daily during calm | |
Token Board | As many earning opportunities as possible | Daily, integrated | |
Crash Pad | 2–3 scheduled crash breaks | Daily, before high-risk |
Variation Principles
Same principle, different context: Space markers: bedroom → living room → garden → group play. Communication cards: parent → sibling → school. Heavy work: home activities → school chores → community settings.
Satiation Indicators — Enough for Today
Declining engagement quality (going through motions) · Increased irritability · Seeking to leave the activity · 3 consecutive errors after consistent success
Step 5 of 6
Step 5: Reinforce & Celebrate — Within 3 Seconds
Timing matters more than magnitude. The reinforcement must land within 3 seconds of the target behavior.
For using communication card:
"YES! You used your 'Move Please' card! You told [sibling] with words! That is AMAZING. Here's your token!"
For completing heavy work:
"Fantastic pushing job! Your arms did strong work! Token earned!"
For entering calm corner first:
"You felt your body getting big and you went to your calm space all by yourself. That is HUGE progress. Token AND special celebration!"
Social
High five, tickle, hug, dance together — 15–30 seconds
Activity
5 min preferred screen time, go outside, choose next game
Tangible
Sticker, small edible treat, preferred object access — immediate
Token Exchange
Full board = 15 min of most-preferred activity — at board completion
NEVER: Withhold earned tokens · Lecture during reinforcement · Delay delivery. 🔴 Pinnacle Canon Reinforcement Menu Kit: amzn.in/d/02C5R9Jn (₹589)
Step 6 of 6
Step 6: The Cool-Down — No Session Ends Abruptly
2–3 minutes. Transition back to baseline. Prevent post-session dysregulation.
Transition Warning (2 min before ending):
"Two more turns, then all done for today."
"One more crash, then we put the pad away."
"One more token chance, then we check your board."
"One more crash, then we put the pad away."
"One more token chance, then we check your board."
Use a visual timer — show child. "When it hits zero, we finish."
If Child Resists Ending:
Honor one more repetition (not open-ended) · Never force an abrupt ending — it creates session anxiety for next time · Offer a known preferred transition: "After we finish, we can [preferred activity]"
Cool-Down Sequence (choose 1–2):
Slow deep breathing together — 5 breaths, count out loud
Put materials away together — child participates in cleanup (proprioceptive + closure)
Quiet activity transition — move to preferred calm activity (colouring, puzzle, book)
Verbal closure: "We did great body work today. I'm proud of you."
Compression Vest Removal: Take off after 20–30 minutes maximum. Give 30–60 minutes before reapplying. Never sleep in vest.

ACT IV: Progress Tracker
60 Seconds of Data Now Saves Hours of Guessing Later
Record within 60 seconds of session end. Three fields only. Each data point enters the GPT-OS® Prognosis Engine — the same system governing 20M+ therapy sessions.
Pushing Frequency
How many pushing incidents in the past hour? Record as: 0 / 1–2 / 3–5 / 5+
Communication Card Use
Did child use card instead of pushing? Yes (spontaneous) / Yes (prompted) / No
Material Response
Which material was used and how did child respond? E.g., "Heavy work — highly engaged. Vest — tolerated 20 min."
"Session abandonment is not failure — it's the most valuable data point." Your 60 seconds of observation contributes to personalized progression recommendations for YOUR child via GPT-OS®.

The Reality Card — Most Sessions Have a Moment Like This
These are the 7 most common challenges reported by families implementing D-387. Every one has a solution.
❓ "My child refused the compression vest completely."
Normal for first 3–7 introductions. Start with just holding the vest. Then wearing for 30 seconds. Build tolerance over 2 weeks. Never force. Try a softer compression undershirt first.
❓ "My child used the communication card — but I didn't honor it fast enough."
Critical: the card MUST be honored within 2 seconds every single time. Practice responding instantly — make honoring the card faster than any other reaction. If you miss it, the card becomes meaningless and pushing becomes more efficient again.
❓ "My child pushed during heavy work time itself."
The pushing during heavy work is directed at you (the person present), not at the heavy work object. The sensory need is high today. Increase heavy work duration. Introduce crash pad. Do NOT use heavy work as a punishment trigger.
❓ "The token board isn't working — my child doesn't care about the rewards."
The reward is wrong, not the system. Conduct a preference assessment: offer 6 items and note which your child reaches for first. Update the reinforcement menu. High-value preferred items as rewards are non-negotiable.
❓ "My child pushed during supervised play despite all preparations."
This is data, not defeat. Note: what was the antecedent (what happened just before)? Log it on your tracking sheet. Adjust antecedent conditions before next social exposure.
❓ "My child became distressed when I tried to introduce space markers."
The concept of personal space may itself be a source of anxiety. Start simpler: just floor tape marks for where to stand in line. No concept teaching yet — just visual cues for where to be.
❓ "We've been doing this for 2 weeks and I see no change at all."
Pushing behavior change timelines: typically 4–6 weeks for initial measurable reduction. Ensure: (1) function of pushing is correctly identified, (2) all caregivers are implementing consistently, (3) reinforcement is immediate and powerful enough. Book a consultation: 📞 9100 181 181

No Two Children Are Identical — Adapt This Toolkit
Easier (Regulation Days)
Communication card + 5 min heavy work only. No new material introductions. Social story reading in safe, connected setting.
Core (Standard Days)
Full protocol as described in Steps 1–6. Token board active. Space markers in structured activities.
Breakthrough Days
Introduce material in naturalistic setting. Reduce prompting. Expect spontaneous card use. Community outing with vest + cards.
Sensory Profile Adaptations
For Sensory SEEKER: Heavy work + crash pad are PRIMARY. Use compression vest routinely. Increase proprioceptive diet intensity.
For Sensory AVOIDER: Communication cards + space markers are PRIMARY. Compression vest may not suit (check with OT). Calm-down corner critical.
For MIXED PROFILE: OT sensory profile assessment essential. FusionModule™ protocol needed. 📞 9100 181 181
Age Modifications
Ages 2–4: Shorter sessions (5–7 min). Only 1 material per session. High concrete/tangible reinforcement.
Ages 5–8: Standard protocol. Begin social story comprehension questions. Token board with visible goal.
Ages 9–12: Self-monitoring cards. Self-managed token board. Peer-inclusive practice scenarios.

Week 1–2: Foundation Phase
Week 1–2: The Foundation Phase
15%
Progress at Week 2
Neural familiarization underway. Material tolerance building. Foundation being established.
What WILL Happen (Normal)
Child is still adjusting to materials — this is neurological familiarization, not resistance · Compression vest may be tolerated for only 5–10 minutes initially · Communication cards may only work with full prompting · Pushing frequency may NOT yet decrease — and that's expected · Heavy work and crash pad are likely the most immediately accepted materials
What MIGHT Happen (Also Normal)
Pushing briefly INCREASES in the first week — this is a behavior extinction burst. The nervous system tries harder before accepting alternatives. Token board needs frequent calibration. Social stories require re-reading 2–3 times before comprehension questions work.
Child tolerates compression vest for 3 minutes longer than on Day 1
Child approaches heavy work materials willingly
Child accepts being handed communication card (even if not yet using spontaneously)
Child can identify their "space marker" spot in one familiar setting
Parent feels more confident in one material's implementation
Observable "Progress" at Week 1–2 — Look for These Specifically:
"If your child tolerates the material for 3 seconds longer than last week — that is real progress. The nervous system is adapting. Stay the course."
Week 3–4: Consolidation Phase
Week 3–4: Neural Pathways Are Forming
40%
Progress at Week 4
Consolidation underway. Motor pathways forming. Communication alternatives emerging.
Consolidation Indicators — The Signs Parents Often Miss:
Motor Pathway Formation
Child begins anticipating the heavy work routine — approaches the cart or resistance bands without prompting. This is motor pathway formation.
Communication Emerging
Card use becomes more prompt-dependent than adult-initiated — the child needs a cue ("What do you need?") rather than full physical guidance to the card.
Space Recognition Generalizes
Child identifies their "spot" in 2 settings — at home AND at grandparents' house, or at school. Generalization has begun.
Early Self-Regulation
Child enters calm-down corner after a prompt (not only after crisis). Early self-regulation is emerging. Context-specific pushing reduction is the consolidation signature.
"You may notice you feel more confident too. That is not coincidence — it is the data telling you the system is working." — Pinnacle Blooms Clinical Consortium
Week 5–8: Mastery Phase
Week 5–8: Mastery Unlocked
75%
Mastery Approaching
Observable, measurable criteria being met. Generalization to new settings. Independence emerging.
Mastery Criteria | What It Looks Like | |
Pushing Frequency | Fewer than 1 incident per day at home; fewer than 3 per week in community settings | |
Communication | Spontaneous (unprompted) card/verbal use in 70%+ of triggering situations | |
Self-Regulation | Independent calm-down corner use at least once per week WITHOUT adult prompt | |
Space Awareness | Maintains appropriate distance in 3+ different settings without visual marker | |
Heavy Work Integration | Child REQUESTS heavy work or crash time when body feeling "too big" |
Generalization Confirmed When:
Communication card use with new adults (teacher, therapist, grandparent) · Appropriate physical boundary maintenance in community settings · Child reports "I used my words" without being asked
Maintenance Check:
Remove the token board for one week. Does the behavior maintain? If yes — mastery confirmed. If regression occurs — reintroduce for 2 more weeks, then re-fade.

You Did This. Your Child Grew Because of Your Commitment.
A Nervous System Outlet
You gave them a sensory outlet that replaced the need to push people.
Words & Cards
You gave them language that replaced pushing as communication.
Visible Space
A concrete boundary that replaced the invisible one they couldn't see.
A Calm Corner
A regulation space that replaced the crash that pushing used to be.
Gentleness Worth Choosing
A reinforcement system that made hands-to-self the most rewarding option.
That is not a small thing. That is neuroscience applied with love, every single day, across 5–8 weeks.
Journal Prompt:"On [date], [child's name] pushed every day and we didn't know why. On [date], they handed someone a card and said 'Move please.' Here is what I felt."
⚠️ Safety Alert
Red Flags — When to Pause and Call, Even After Progress
🔴 Pause and Seek Professional Consultation If:
1. Pushing is increasing in frequency or force despite 4+ weeks of consistent implementation · 2. Child is injuring others — even once constitutes a safety threshold requiring professional FBA · 3. Child is being excluded from educational settings as a result of pushing behavior · 4. Pushing appears to be directed at a specific person consistently · 5. Additional aggressive behaviors (hitting, biting, scratching) emerging alongside pushing · 6. Child shows no awareness of others' distress after pushing — zero social referencing · 7. You are unsure of the function and the wrong material may be being prioritized
Trust your instincts. If something feels wrong — pause and ask. That call is free: 📞9100 181 181 — FREE. 24×7. 16+ languages.
Your Developmental GPS — Where You Are. Where You're Going.
Long-term developmental goal this feeds: Community Inclusion Readiness — child participates safely in all social environments with peers. The branching path you take from D-387 depends on which root cause was most prominent in your child's pushing behavior.
Related Techniques — You May Already Own the Materials
D-385: Understanding Aggressive Behavior
Domain: ABA · NeuroDev | 🟢 Intro
Materials You Already Own: Social Stories · Communication Cards
Materials You Already Own: Social Stories · Communication Cards
D-386: Functional Behavior Assessment Basics
Domain: ABA | 🟢 Intro
Materials You Already Own: Token Board · Data Tracking Sheet
Materials You Already Own: Token Board · Data Tracking Sheet
D-388: 9 Materials for Hitting Behavior
Domain: ABA · OT | 🟡 Core
Materials You Already Own: Compression Vest · Heavy Work Kit
Materials You Already Own: Compression Vest · Heavy Work Kit
D-389: Biting Behavior Materials
Domain: OT · SLP | 🟡 Core
Materials You Already Own: Calm-Down Corner · Communication Cards
Materials You Already Own: Calm-Down Corner · Communication Cards
D-390: Personal Space Development
Domain: SLP · SpEd | 🟡 Core
Materials You Already Own: Space Markers · Social Stories
Materials You Already Own: Space Markers · Social Stories
C-Series: Emotional Regulation
Domain: OT · ABA | 🔴 Advanced
Materials You Already Own: Token Board · Calm-Down Corner
Materials You Already Own: Token Board · Calm-Down Corner
"Materials you own for D-387 cover 4+ related techniques. Your investment scales." — Browse Full Behavior Domain: techniques.pinnacleblooms.org/behavior

D-387 Is One Piece of Your Child's Complete Developmental Journey
Pillar (WHO/UNICEF) | How D-387 Contributes | |
🏥 Health | Safe behavior reduces injury risk for child and peers | |
🧠 Responsive Caregiving | Parent learns to read child's sensory signals before crisis | |
🔐 Security & Safety | Physical safety in social environments restored | |
📚 Early Learning | Communication alternatives open classroom learning access | |
🍽️ Nutrition | Regulatory baseline improves feeding environment calm |
ACT V: Community
The Families Who Started Exactly Where You Are Now
Arjun, Age 6 · Hyderabad · ASD + Sensory Seeking
Before (Week 0): Arjun was pushing 8–10 times per school day. Teachers had written 3 incident reports. His mother avoided the school playground. Playdates had completely stopped.
Intervention: Compression vest (30-min morning wear), heavy work before school drop-off (10 min wall push-ups + backpack carrying), crash pad at home for after-school decompression.
After (Week 7): Pushing reduced to 1–2 incidents per week. Teacher reported appropriate crash cushion use. First playdate in 4 months was successful. Arjun now requests "push time" verbally before situations where he used to push people.
"The compression vest was the turning point. Once his body felt held, he stopped looking for something to hold onto." — Arjun's mother
Priya, Age 5 · Chennai · Language Delay + Communication Pushing
Before (Week 0): Priya pushed children at daycare every day — mostly when transitions happened or when she wanted to get through a doorway. She had no verbal communication for "move" or "excuse me."
Intervention: SLP + ABA joint protocol: "Move Please" and "Excuse Me" communication cards on a wrist lanyard. Practice scenarios 5x daily with immediate honoring. Token board: one token for every card use.
After (Week 6): Pushing for transition/path purposes eliminated entirely. Daycare reported zero incidents in the final 3 weeks. Priya now signs "more" + points when card isn't available — the communication pathway is opening.
"She wasn't pushing because she was aggressive. She was pushing because 'move' wasn't in her vocabulary yet. Now it is." — Priya's father
From the Therapist's Notes: In 76% of our cases where pushing is the presenting behavior and a systematic functional approach is applied across sensory + communication domains, we see clinically significant reduction within 6–8 weeks. — Pinnacle Blooms FusionModule™ Clinical Record, 2024
Isolation Is the Enemy of Progress. Community Is the Multiplier.
WhatsApp Group — "Hands-to-Self Support Network"
Parents navigating pushing behavior together. Share wins, ask questions, troubleshoot in real time. Join at pinnacleblooms.org/parent-groups/pushing
Online Forum — Pinnacle Parent Connect
Threading by technique, by age, by condition — find exactly the conversation that matches your situation. forum.pinnacleblooms.org/behavior/D-387
Local Pinnacle Parent Meetups
70+ centers across India host monthly parent workshops by domain. Find your nearest center: pinnacleblooms.org/centers
Peer Mentoring Program
Connect with a parent who has already completed D-387 with their child. Real experience. Zero judgment. Request a Peer Mentor: 📞 9100 181 181
"When our children's challenges are invisible to others, we need people who can see. This community sees." — Pinnacle Parent, Bangalore
Home + Clinic = Maximum Impact
Service | What You Get | How to Access | |
Functional Behavior Assessment (FBA) | Identifies the EXACT function of your child's pushing behavior — targeting becomes precise | Book at nearest center | |
OT Sensory Evaluation | Sensory profile to determine if compression vest + heavy work protocol is indicated | OT appointment via helpline | |
ABA Behavior Intervention Plan | Full written protocol customized for your child | BCBA consultation | |
FusionModule™ Session | OT + ABA + SLP converged — all three disciplines in one session | Center booking only | |
EverydayTherapyProgramme™ | Daily home program personalized to your child's D-387 profile | GPT-OS® digital delivery |
📞 FREE National Autism Helpline
9100 181 181 · 16+ languages · 24×7 · No appointment needed
💻 Teleconsultation
Video consultation with Pinnacle BCBA or OT. Available nationally and internationally — 70+ countries served.
📍 70+ Centers
Find your nearest Pinnacle Blooms center: pinnacleblooms.org/find-a-center
The Evidence Behind D-387 — Deeper Reading for the Curious Parent
Study | Key Finding | Level | Reference | |
Systematic Review — Children (2024) | Sensory integration intervention is evidence-based practice for ASD; 16 studies confirm | Level I | ||
Meta-analysis — World J Clin Cases (2024) | SI therapy promotes social skills, adaptive behavior, motor skills across 24 studies | Level I | ||
Indian RCT — Indian J Pediatr (2019) | Home-based sensory interventions show significant outcomes in India | Level II | ||
NCAEP Evidence-Based Practices (2020) | ABA + communication interventions classified evidence-based for autism | Level I | ||
Frontiers Integrative Neuroscience (2020) | Neurological basis for sensory-based behavioral intervention | Level II | ||
WHO Care for Child Development Package (2023) | Home-based caregiver interventions effective across 54 LMICs | WHO Guideline | ||
WHO Nurturing Care Framework (2018) | Five pillars of early childhood development as foundational framework | WHO Guideline |
Consistency Across Caregivers Multiplies Impact
If only one person implements this — impact is limited. If everyone who interacts with your child uses these materials consistently — impact compounds.
Share This Page
WhatsApp · Email · Copy link · Auto-formats as: "9 materials that help with pushing behavior — complete guide: techniques.pinnacleblooms.org/behavior/pushing-others-materials-D-387"
Download D-387 Family Guide PDF
1-page printable summary of all 9 materials with DIY alternatives. Share with second parent, grandparents, teacher, babysitter.
Teacher Communication Template
Ready-to-send email to school with your child's home protocol and specific requests for classroom consistency. Ask us for the template.
Explain to Grandparents — Simplified
"When [child's name] pushes, their body needs heavy physical input. Give them wall push-ups, carry a bag, and use this card. Stay calm. That's it."
"Therapy that only happens during sessions is therapy that stops when the session ends. Therapy that happens at home, at school, and in the community — that's the therapy that changes lives."

Frequently Asked Questions
The Questions Every Parent Asks
Generated from actual parent queries at Pinnacle centers and the D-387 community group.
❓ My child doesn't have autism — can these materials still help?
✅ Absolutely. These materials address the root causes of pushing (sensory need, communication gaps, impulse control, space unawareness) which occur across neurotypical development, ADHD, language delays, and any population where these systems are not yet fully developed.
❓ How do I know WHICH of the 9 materials to start with?
✅ Start with the one that addresses your child's most common "reason" for pushing. Pushing when seeking contact → compression vest + heavy work. Pushing to say "move" → communication cards. Doesn't understand space → visual markers. Pushing when overwhelmed → calm-down corner.
❓ My child is only 2 years old. Is this appropriate?
✅ For ages 2–3: heavy work activities, space markers, and simple communication (pointing to a "move" picture) are most appropriate. Compression vest requires OT guidance. Token boards should be very simple (3 tokens max). Social stories work well if kept to 3 sentences with pictures.
❓ My child's school says they can't use these materials during class.
✅ Request a meeting with the SENCO or special educator. Bring this page's URL. Communication card lanyards are typically acceptable anywhere. Floor tape space markers are standard in most special education classrooms. A written protocol from a BCBA or OT carries significant weight.
❓ My child uses communication cards at home but not at school.
✅ Generalization is a separate teaching target from acquisition. Have the teacher begin prompting card use at school just like you did at home for 1–2 weeks. Consistency of the prompt and honor response is the key to bridging settings.
❓ Can I use all 9 materials simultaneously?
✅ Not in the same session — focus on 1–3 per session. The full set of 9 integrates into the daily routine over time: vest during high-risk times, cards available all day, heavy work in the morning routine, crash pad for after-school, token board during structured activities.
❓ How long will we need these materials?
✅ Tools, not permanent prosthetics. Communication cards: typically needed 6–12 months. Heavy work activities often become a preferred activity permanently. Compression vest often phases out by ages 7–9 as sensory regulation matures.
❓ Is this covered by insurance or any government scheme in India?
✅ ABA, OT, and SLP are recognized therapeutic services. Some insurance covers therapy sessions. PM-DAKSH and district disability rehabilitation centers sometimes provide materials. Contact our helpline — 📞 9100 181 181 — for guidance on accessing subsidized services in your district.
Preview of 9 materials that help with pushing others Therapy Material
Below is a visual preview of 9 materials that help with pushing others therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.




















Link copied!

The Information Is Complete. The Next Move Is Yours.
20M+ therapy sessions. 97%+ measured improvement. 70+ centers across India. 70+ countries served. Your child's journey starts with one material, used consistently, today.
🚀 Start This Technique Today
Select which material you're starting with. Receive your first session guide. Begin today.
📞 Book a Consultation
Call FREE: 9100 181 181 · Book online: pinnacleblooms.org/consult · 70+ centers · Teleconsultation worldwide · 16+ languages
🗺️ Explore the Next Technique
D-388: 9 Materials That Help With Hitting · techniques.pinnacleblooms.org/behavior/hitting-others-D-388
🌸Pinnacle Blooms Network® · Built by Mothers. Engineered as a System. · OT · ABA/BCBA · SLP · Special Education · NeuroDevelopmental Pediatrics · CRO
Our Mission: To transform every home into a proven, scientific, 24×7, personalized, multi-disciplinary intervention center — empowering families across 70+ countries through the GPT-OS® platform.
CIN: U74999TG2016PTC113063 · DPIIT: DIPP8651 · MSME: TS20F0009606 · GSTIN: 36AAGCB9722P1Z2
⚖️Medical Disclaimer: This content is educational and does not replace individualized assessment and intervention from licensed behavior analysts, occupational therapists, or developmental specialists. Every child's situation is unique — approaches must be individualized based on function and underlying factors. Individual results may vary.
© 2025 Pinnacle Blooms Network®, unit of Bharath Healthcare Laboratories Pvt. Ltd. All rights reserved. · pinnacleblooms.org · care@pinnacleblooms.org · 📞 9100 181 181