
9 Materials That Help With Pinching Others
D-386 | Pinnacle Blooms Network® | Behavior Support Series
Science-backed sensory tools, communication supports, and behavior strategies — for every family navigating pinching behavior. Ages 2–12 · ABA + Occupational Therapy · Free Helpline: 📞 9100 181 181
Science-backed sensory tools, communication supports, and behavior strategies — for every family navigating pinching behavior. Ages 2–12 · ABA + Occupational Therapy · Free Helpline: 📞 9100 181 181
It Happened Again.
D-386 · Behavior Support Series
ABA + Occupational Therapy · Ages 2–12
The Moment Every Parent Knows
"It happened again. Your child reached out and pinched — hard. You watched the red mark form on someone's arm, saw their face, felt the shame flood through you before you'd even drawn breath."
You've said "no pinching" a thousand times. You've tried consequences. You've tried charts. People are starting to avoid your family. Birthday invitations have stopped coming.
There is a WHY behind every pinch. And when you meet the WHY — the pinching stops.
You Are Not Failing
Your child's nervous system — or communication system — is speaking the only language it has right now. This page gives it better words.
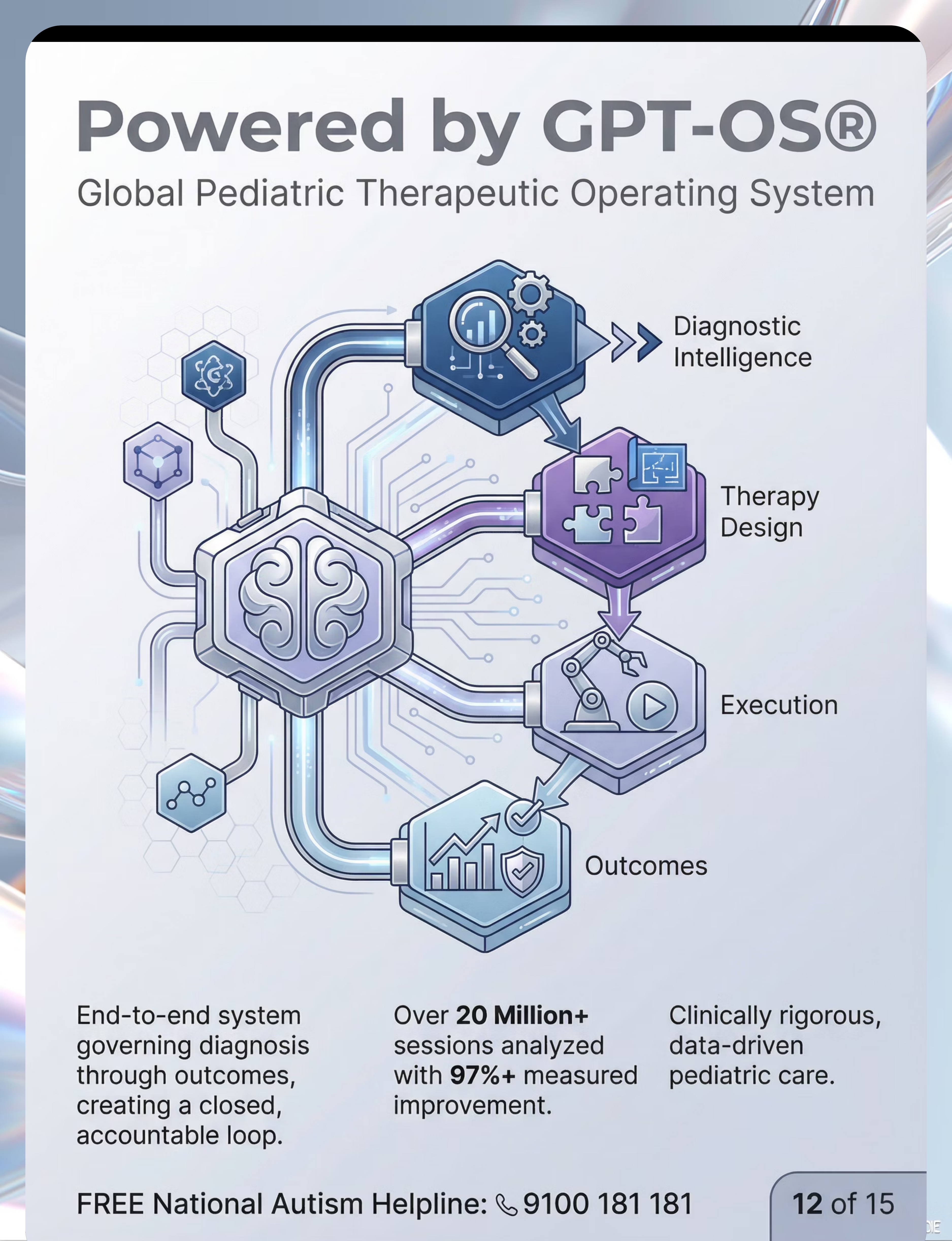
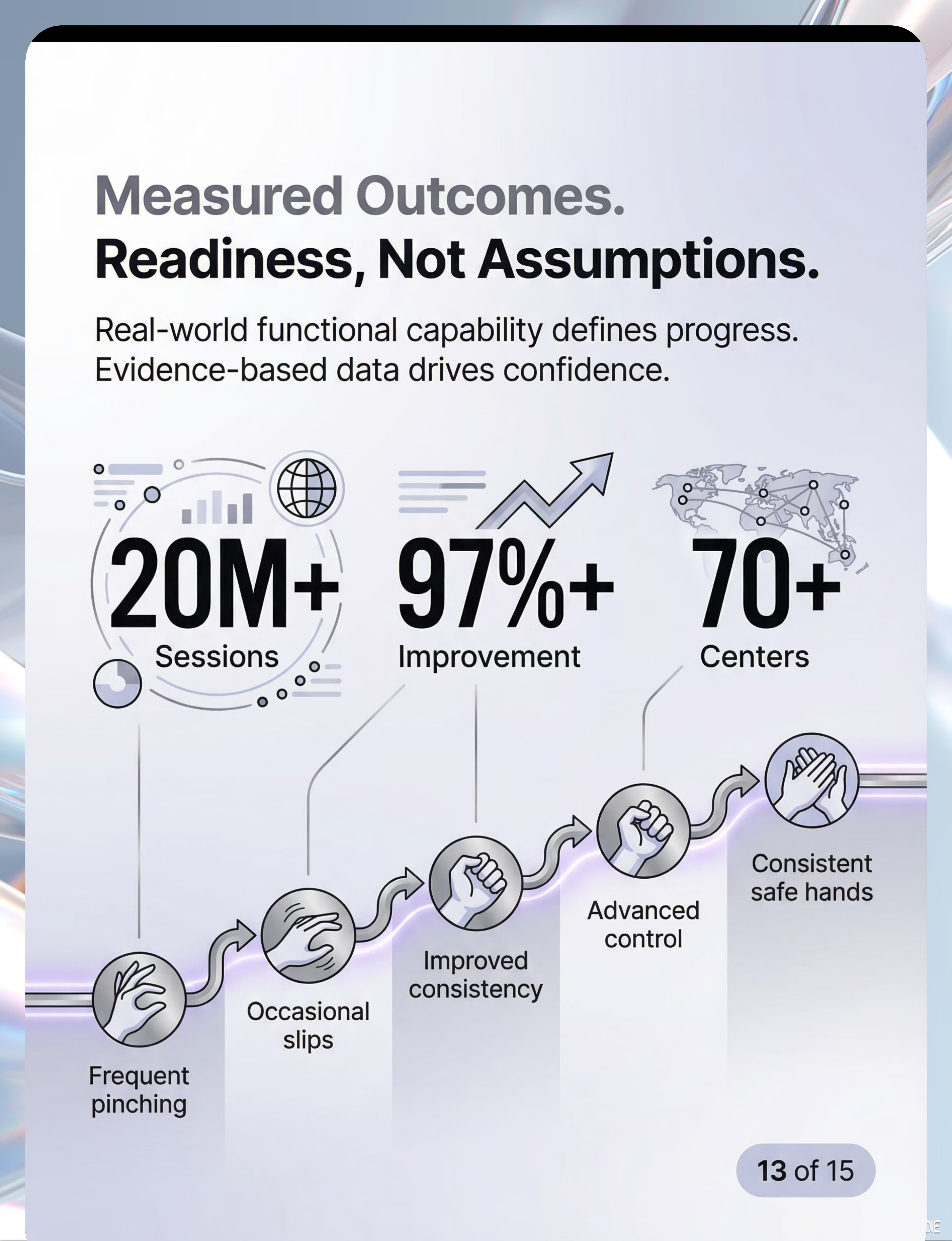
"Clinically validated. Home-applicable. Consortium-proven. Across 20M+ therapy sessions in the Pinnacle GPT-OS® system."
📞FREE National Helpline: 9100 181 181 — 24x7 · 16+ Languages. Call anytime you feel overwhelmed.
You Are Among Millions of Families
Pinching is among the most isolating challenging behaviors families face. It leaves visible marks, happens suddenly, and damages relationships. And it almost never responds to punishment alone — because punishment doesn't address the function that pinching is serving.
1/36
Children with Autism (US)
CDC 2023. In India, estimated 1 in 68 — over 18 million children living with ASD.
80%
Experience Sensory Differences
Of children with ASD, hands among the highest-impacted sensory channels. (PRISMA Systematic Review, 2024 · PMC11506176)
67%
Aggression from Unmet Needs
Of children with ASD who display aggressive behaviors do so because of unmet sensory or communication needs — not defiance. (JABA literature review)
"Across Pinnacle Blooms Network®'s 70+ centers, pinching behavior is one of the most commonly presented concerns — and one of the most successfully addressed when the function is identified."

What's Happening in Your Child's Brain
Mechanism 1 — Proprioceptive Seeking
The somatosensory cortex processes pressure, force, and position. In some children, this system is under-responsive — it needs MORE input to register sensation. Pinching delivers intense proprioceptive feedback to the hands: muscles contract, joints compress, tendons load. For a sensory-seeking nervous system, this feels organizing — almost like a pressure valve releasing.
Mechanism 2 — Communication Pathway
When the prefrontal cortex is under-developed or differently wired, the limbic system bypasses verbal communication entirely. Frustration, overwhelm, desire — these travel the fast path: body action before words. Pinching communicates what language cannot.
Mechanism 3 — Reinforcement Loop
Every time pinching achieves its function — gets attention, ends an unwanted demand, delivers sensory input — the neural pathway strengthens. The brain learns: "pinching works." This is not stubbornness. It is learning.
Key Insight: "This is a wiring difference and a learned pattern. Both can be changed. Neither is the child's fault." — Frontiers in Integrative Neuroscience (2020) DOI: 10.3389/fnint.2020.556660
Where This Sits in Development
Your child is not behind. They are on a different path — with a clear forward direction. WHO/UNICEF developmental guidelines confirm: the most powerful intervention period is NOW — whatever age your child is.
Ages 0–2
Exploratory pinching is developmentally normal — cause-effect discovery phase.
Ages 2–3
Language development typically reduces pinching naturally as words replace actions.
Ages 3–5 ⚠️
Intervention Window — pinching that persists beyond this point signals unmet need requiring targeted support.
Ages 5–8
Critical period for replacement behavior consolidation — neural pathways are highly plastic.
Ages 8–12
Generalization and self-regulation mastery. Intervention window is wider but time-sensitive for children with ASD/SPD.
What commonly co-occurs: Sensory Processing Differences (80% of ASD children), limited expressive language or AAC need, difficulty with emotional regulation, theory of mind differences, and ADHD impulsive motor action.

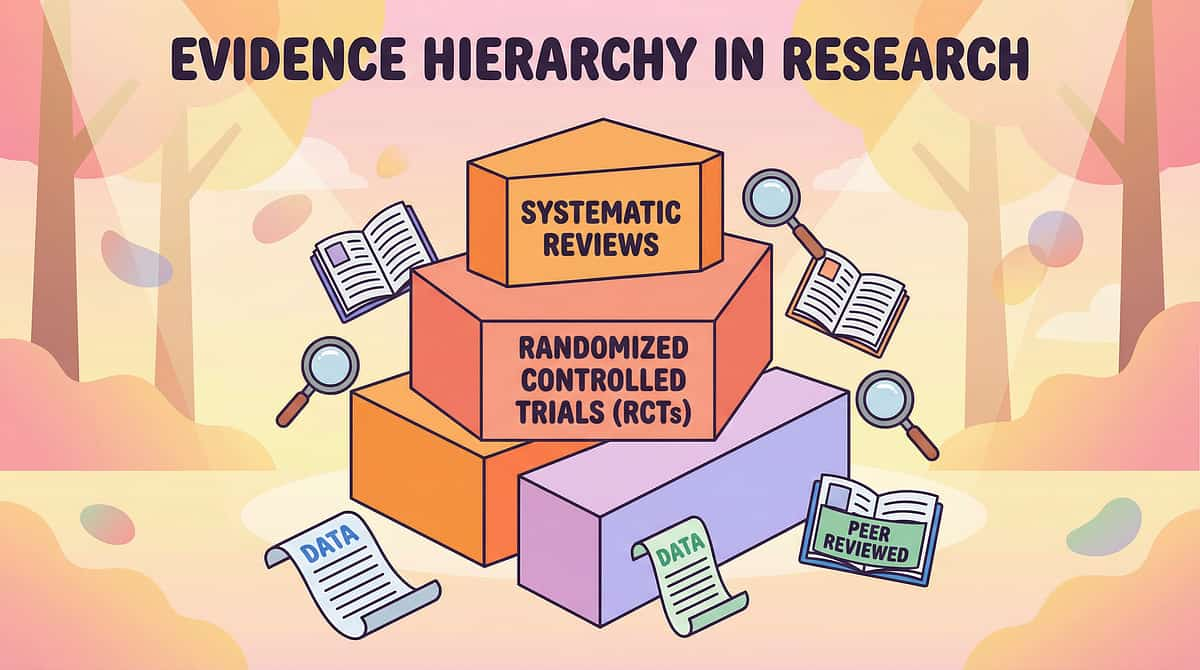
The Evidence Behind This Technique
Level I Evidence
Systematic Review + Meta-Analysis
Study | Finding | Level | |
PRISMA Review 2024 (PMC11506176) | Sensory integration meets evidence-based criteria for ASD — 16 studies | Level I | |
Meta-analysis WJCC 2024 (PMC10955541) | SI therapy: social skills, adaptive behavior, sensory processing all improved | Level I | |
NCAEP Report 2020 | FCT, token economy, visual supports: all EBP for ASD | Level I | |
Indian RCT 2019 (Padmanabha et al.) | Home-based sensory interventions: significant outcomes demonstrated | Level II |
Confidence Rating
Based on 16 systematic review studies + 24 meta-analysis studies — 78% High Confidence
Punishment alone for pinching: low effectiveness
Function-based replacement: high effectiveness
Sensory + Communication + Reinforcement combined: highest effectiveness
Function-based replacement: high effectiveness
Sensory + Communication + Reinforcement combined: highest effectiveness

What Is the "9 Materials" Approach?
Parent Alias: The Safe Hands Toolkit
Pinching Others is a challenging behavior characterized by the child using thumb and forefinger to squeeze another person's skin with force sufficient to cause pain or marks. Like all behavior, pinching serves a function — it communicates something, meets a sensory need, or achieves an outcome the child cannot access another way. The "9 Materials" intervention addresses the ROOT CAUSE by replacing pinching with safer alternatives that meet the same function.
ABA
Applied Behavior Analysis
OT
Pediatric Occupational Therapy
SLP
Speech-Language Pathology
SpEd
Special Education
NeuroDev
Neuro-Developmental Pediatrics
Age: 2–12 years · Session: 5–20 min · Frequency: Daily + As-needed · Domain: D — Behavior & Flexibility

Who Uses This Technique?
This technique crosses therapy boundaries — because pinching doesn't care which discipline is treating it. All five disciplines input simultaneously in the Pinnacle GPT-OS® FusionModule™.
ABA — Behavior Analyst (Primary Lead)
Functional Behavior Assessment to identify WHY the child pinches. Designs replacement behavior programs, token economies, and reinforcement schedules. Measures frequency, intensity, and duration.
Occupational Therapist
Sensory processing profile assessment. Identifies whether pinching is sensory-seeking or sensory-avoiding. Designs sensory diet with putty, fidgets, and deep pressure tools.
Speech-Language Pathologist
Communication function assessment. Designs AAC systems, communication cards, and Functional Communication Training as pinching alternatives.
Special Educator
Classroom implementation of visual behavior supports. Social story design for "gentle hands." Coordination with school for consistent reinforcement across settings.
NeuroDev Pediatrician
Rules out pain-based or medical drivers of pinching. Reviews medication affecting sensory threshold or impulse control. Provides neurodevelopmental context for intervention intensity.
What Does This Technique Target?
Observable Behavior Indicators
- Primary: "No pinching incidents in the last 3 days" → Week 1–2 goal
- Secondary: Child uses squeeze ball or communication card when frustrated
- Tertiary: Child invited to and participates in peer social events
GPT-OS® Readiness Indexes Targeted
- Behavior Safety Readiness Index
- Self-Regulation Readiness Index
- Social Interaction Readiness Index
- Sensory Processing Readiness Index
- Communication Readiness Index

The 9 Materials — What to Get
9 Materials · 5 Functions · One Goal
Give hands somewhere better to go. Starter Kit: ₹2,000–4,000 · Full Comprehensive Kit: ₹4,000–12,000

1. Therapy Putty
Proprioceptive Replacement · ₹300–800
2. Pinch Fidgets
Right Action, Safe Object · ₹150–600 · Portable

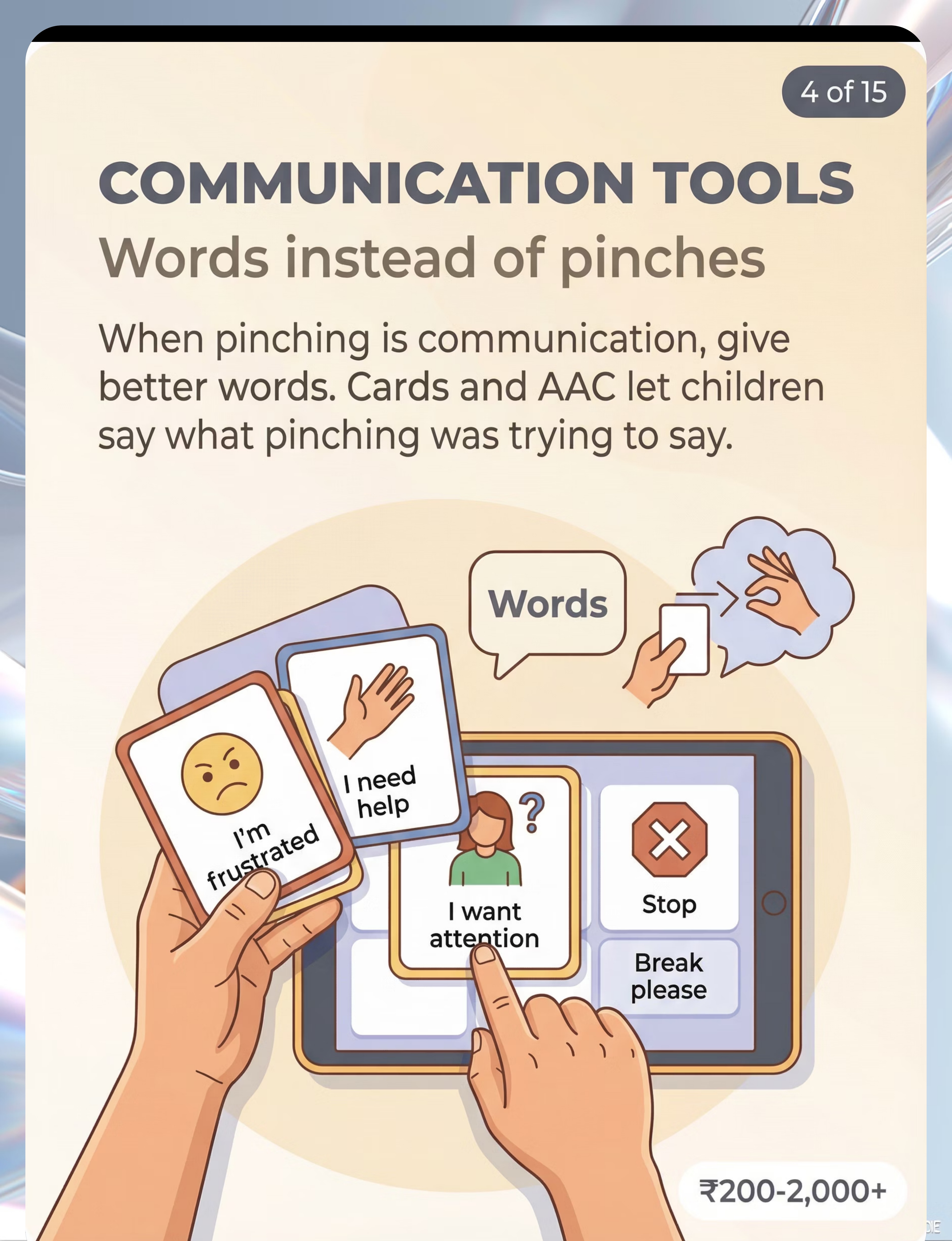
3. Communication Cards / AAC
Replace the Message · ₹200–2,000+ · Essential

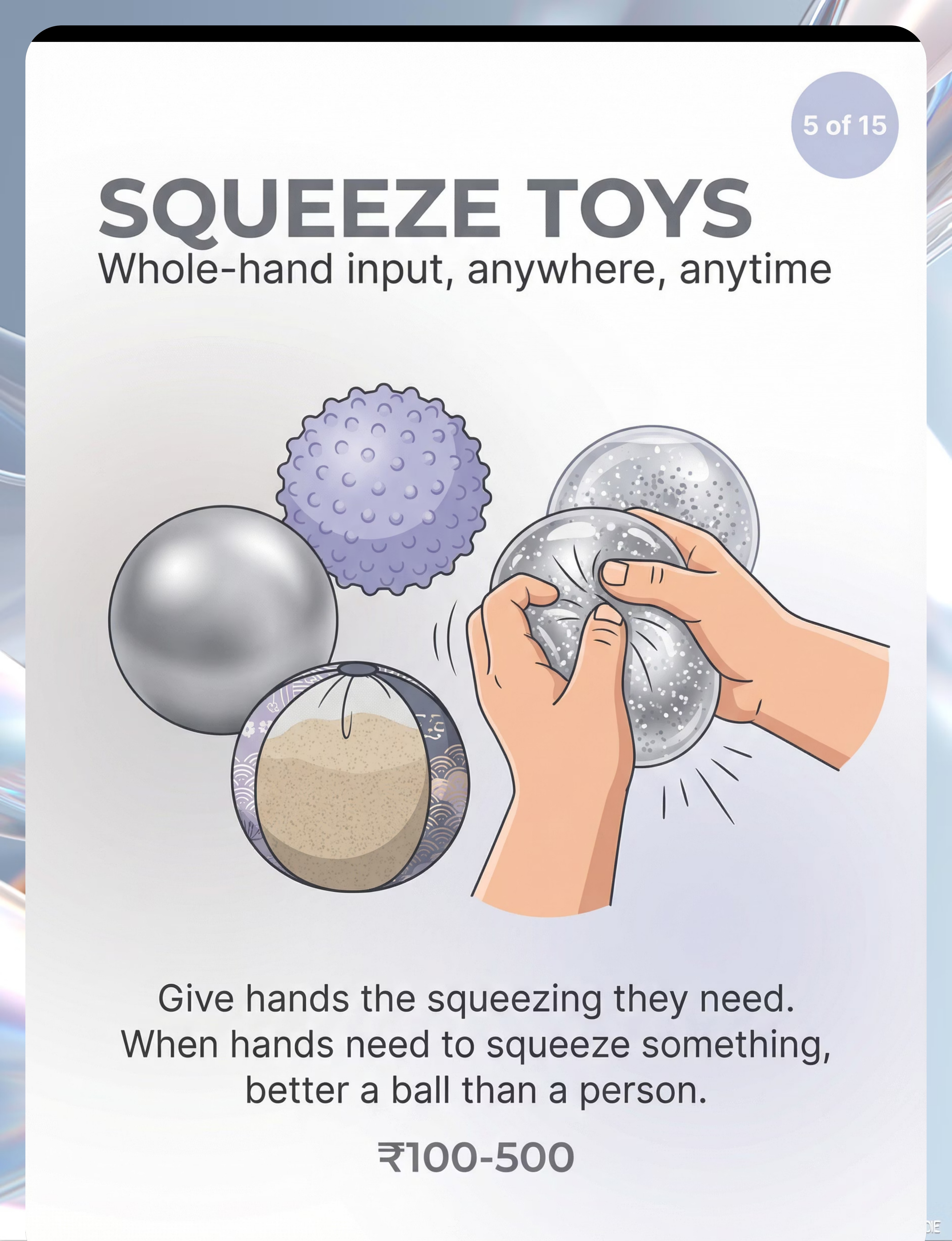
4. Stress Balls / Squeeze Toys
Whole-Hand Input · ₹100–500 · Multi-location

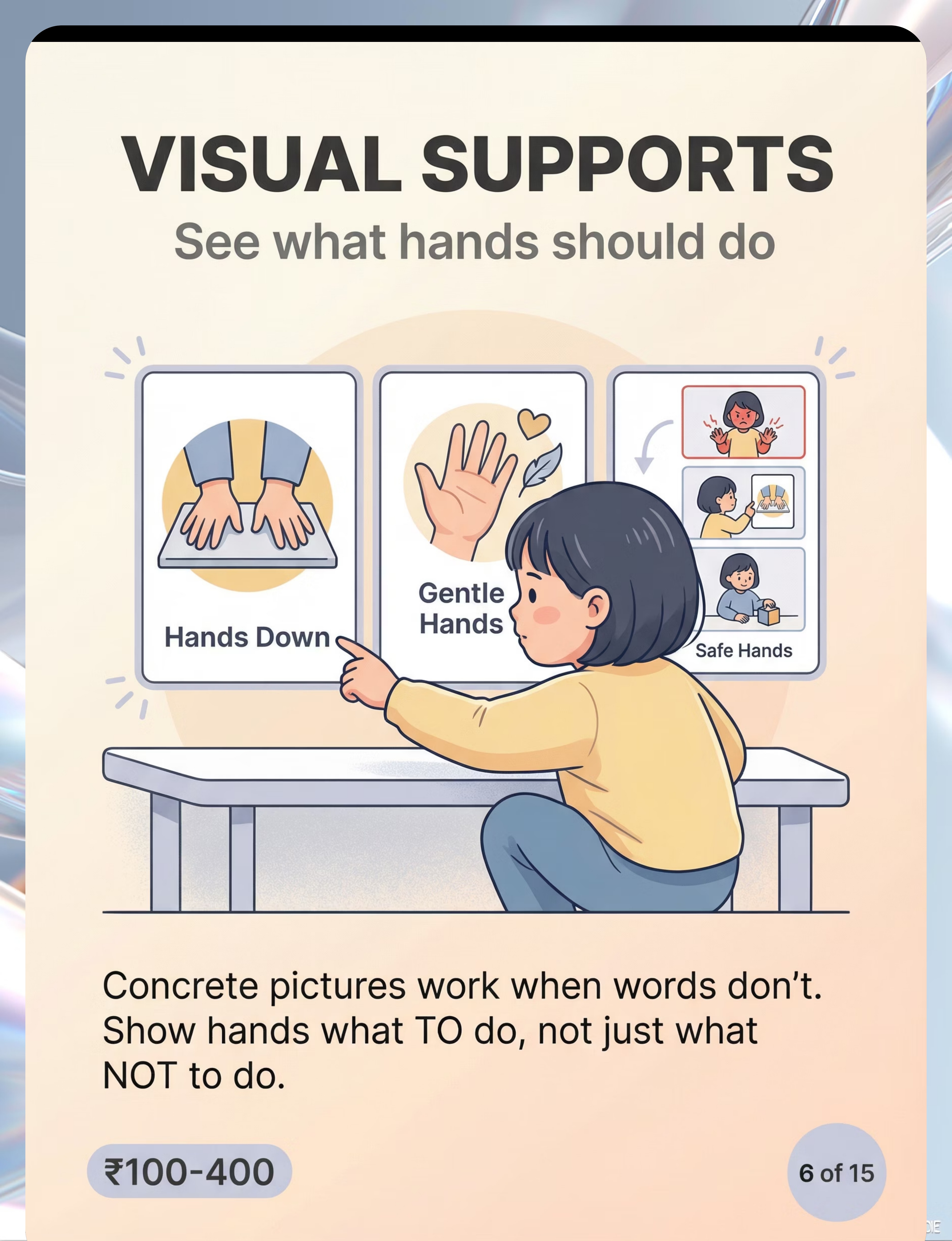
5. Visual Behavior Supports
Show Hands What TO Do · ₹100–400 · DIY possible

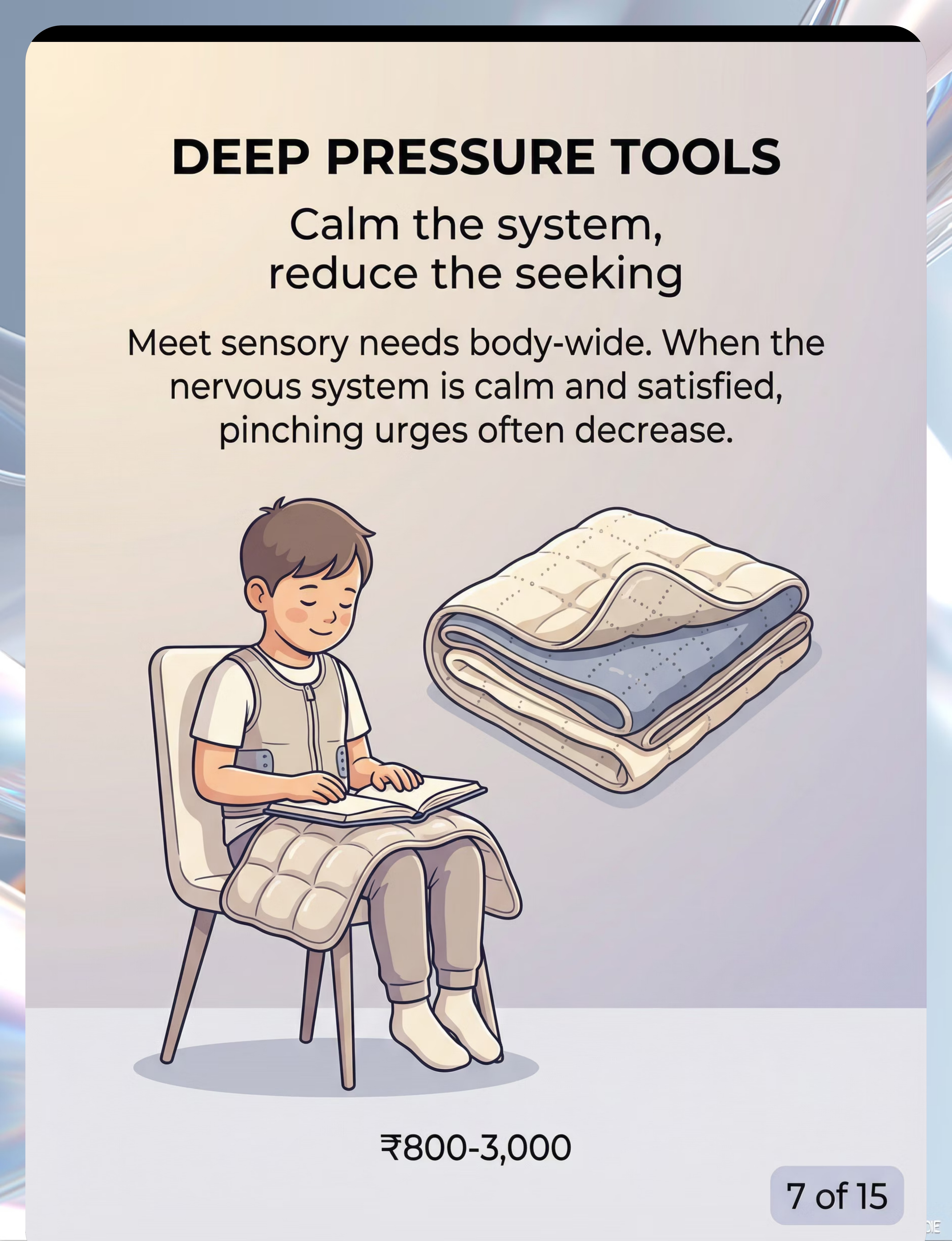
6. Deep Pressure Tools
Calm the System · ₹800–3,000 · OT recommended

7. Social Skill Games
Practice Safe Touch in Play · ₹400–1,500

8. Calm Down Kits
Everything for Regulation · ₹500–2,000

9. Token Boards / Reinforcement Systems
Make Safe Hands Worth Choosing · ₹200–600
⭐Pinnacle Recommends: Token/Reinforcement System ₹589 · Reinforcement Menu Cards ₹364 · Transition Comfort Item ₹425 — all available on Amazon.in
DIY & Substitute Options
Every family can run this intervention — regardless of budget. WHO/UNICEF equity principle: context-specific interventions must be accessible to all.
Clinical-Grade (Buy)
- Therapy Putty — ₹300–800
- Pinch Fidgets — ₹150–600
- Communication Cards / AAC — ₹200–2,000+
- Stress Balls — ₹100–500
- Visual Behavior Supports — ₹100–400
- Weighted Lap Pad — ₹800–3,000
- Social Skill Games — ₹400–1,500
- Calm Down Kit — ₹500–2,000
- Token Board — ₹200–600
Household (Make Today)
- Homemade playdough (flour + salt + water + extra flour for resistance)
- Clothespins padded with rubber band grip; bubble wrap squares
- Free PECS symbols from Boardmaker library; phone photos laminated
- Balloon filled with flour or rice — double-balloon for durability
- Phone photo of child with "gentle hands," laminated; autismspeaks.org
- Sock filled with rice/dried beans (~10% body weight)
- Sock puppets; emotion cards printed and cut; home role play
- Shoebox with: putty, comfort toy, breathing card, small coloring book, timer
- Paper + velcro dots; star stickers; hand-drawn chart — works identically
Zero-Cost Complete Kit Is Possible. When clinical-grade is non-negotiable: formal AAC device evaluation (requires SLP), sensory profile-specific putty resistance (OT), and compression vest fit (OT must fit properly).

Safety First — Before You Begin
Read this before starting. Every time. These protocols are adapted from Padmanabha et al. (Indian J Pediatr, 2019) and BACB ethical guidelines for behavior intervention.
🔴 Do NOT Proceed If
- Child is in active meltdown or crisis state — wait for full regulation
- Pinching has caused open wounds or serious injury — call 9100 181 181 immediately
- Using weighted items — do NOT exceed 10% of child's body weight
- Any material has small parts and child mouth-stuffs unsupervised
- Child shows signs of illness, fever, or significant pain
⚠️ Modify Before Starting If
- Child is hungry, overtired, or recently dysregulated (within 1 hour)
- Unusual schedule change or transition just occurred
- New people present — higher anxiety baseline possible
- Check for latex allergy before putty or squeeze materials
- DIY balloon stress balls — monitor for burst risk; do not share between children
✅ Safe to Proceed When
- Child is calm, regulated, alert — not in fight/flight/freeze
- Materials have been sanitized (putty not shared between children)
- All caregiver adults know the plan and are using the same language
- Space is prepared per the setup guide (Card 12)
- You have 15–20 uninterrupted minutes
📞Emergency Escalation: If pinching is causing significant injury, seek professional support immediately. FREE National Autism Helpline: 9100 181 181 (24x7, 16+ languages)

Set Up Your Space
Spatial precision prevents 80% of session failures. Meta-analysis confirms 1:1 individual treatment in a structured environment is most effective (PMC10955541). Sensory Integration Theory (Ayres) identifies environmental setup as a core principle.
Setup Positions
- Child position: Floor mat / low chair / bean bag — child's preferred regulation surface
- Parent position: 45 degrees to child — not directly in front (less confrontational)
- Materials station: Within child's reach, organized basket/tray — not scattered
- Visual supports: Posted at child's eye level on wall or portable stand
- Token board: Visible to child from sitting position
- Exit clear: Child can leave the space without obstacle — never trapped
What to Place in the Space
- Selected 2–3 materials (don't overwhelm with all 9 at once)
- Token board / reinforcement menu visible
- Visual "gentle hands" support at eye level
- Visual timer (hourglass preferred — 5–10 minute sessions to start)
- One preferred reinforcer (earns at session end)
What to Remove
- Distracting screens (unless screen IS the reinforcer)
- Other children initially — introduce peers gradually
- Items the child may grab and throw if frustrated
- Clutter — clear surfaces reduce overstimulation
- Items that typically trigger demand avoidance
Environment Settings
- Lighting: Natural or warm — fluorescent increases arousal
- Sound: Calm music or white noise at low volume, or silence
- Temperature: Comfortable — heat increases dysregulation
- Time of day: After snack/meal, mid-morning or mid-afternoon
Is Your Child Ready? — Readiness Check
The best session is one that starts right. Run this 60-second checklist before every session.
Child State
- Fed within the last 1–2 hours (not hungry, not overfull)
- Rested — not showing signs of fatigue or sleepiness
- No fever, illness, or visible pain
- Calm or alert state — not in active cry, tantrum, or withdrawal
- Last significant dysregulation: more than 45 minutes ago
Environment + Caregiver State
- Space set up, materials clean and ready, timer visible, token board in position
- No unexpected schedule conflicts in the next 30 minutes
- You are regulated — calm, patient, not rushed
- You know which of the 9 materials you're introducing today
- You have the reinforcer ready
Decision Gate
✅ALL GREEN → Proceed: Begin the Invitation (Step 1)
⚠️SOME AMBER → Modify: Use the "lite" version — 5 minutes, one material, low demand
🔴RED FLAG PRESENT → Postpone: Offer a calming activity. Try again in 30–60 minutes.
Alternative for Postpone Days: Leave putty or fidget accessible and unrestricted. Passive access still builds positive association without session demand.

Step 1 of 6
The Invitation
"Never start with a demand. Start with an offer." The invitation phase sets the entire emotional tone of the session. Body language communicates before words do.
Body Language Guidance
- Get to child's physical level — sit, kneel, or match their position
- Open body posture — no crossed arms, relaxed shoulders
- Soft eye contact — offered, not demanded
- Hold the material loosely in your hand — visible but not pushed forward
Acceptance Cues (What YES Looks Like)
- Reaches toward the material or leans forward
- Eye contact with the item or relaxed posture / smile
- Any vocalization expressing interest
Resistance Cues (What NO Looks Like)
- Turns away or pushes item away → Back off, try in 2 minutes
- Increases arousal or agitation → Not the right moment
- No response after 15 seconds → Try a different material first
The Invitation Script
For Sensory Materials (putty, fidget, squeeze ball):
"Hey, look what I have. [Hold out material.] Want to try it?" [Pause. Wait 5–10 seconds. Let curiosity work.]
For Communication Tools:
"I have a special card I want to show you. This card is magic — it gets you [what they want]."
For Token Board:
"Look at this! Every time your hands are gentle, you get a star. [X stars] = [reward]. Ready to try?"
Timing: 30–60 seconds for the invitation phase. ABA Pairing Procedures — establishing motivating operations before demand.

Step 2 of 6
The Engagement
"Material is in hand. Now let the material teach." (PMC11506176 — structured material introduction in SI intervention)
For Therapy Putty
Present putty in its container. Open it. Show color and texture. "Look — you can squeeze this, pull it, poke it." Model briefly yourself. Place in child's hands if accepted. Observe: squeeze? explore? mouth? (Redirect if mouthing.)
For Pinch Fidgets
Show the specific pinching mechanism. "You can press this — see?" Pop the bubbles, squeeze the pinch point, demonstrate. Hand to child. Most children begin immediately with no prompt needed.
For Communication Cards
Hold up ONE card — the most immediately relevant. "When you feel like this, you show me this card." Practice: "Let's try it — show me the card." Prompt hand over card if needed. Celebrate ANY attempt at card use with enthusiasm.
For Token Board
Place board visibly. "Every 2 minutes of gentle hands = 1 star." Set timer. "Ready — we start now." First interval should be SHORT (60–90 seconds). Success builds motivation for the next interval.
Engagement Indicators
🟢 Full engagement: Using the material independently, exploring it
🟡 Tolerated engagement: Holding material, minimal use — still valid
🔴 Refusal or distress: Back off, offer different material, don't force
🟡 Tolerated engagement: Holding material, minimal use — still valid
🔴 Refusal or distress: Back off, offer different material, don't force
Reinforcement Cue — Begin Here
When child touches, holds, or uses material → IMMEDIATE SPECIFIC PRAISE: "Yes! You squeezed the putty! Great job, safe hands!" Timing: 1–3 minutes total for this phase.
Step 3 of 6
The Therapeutic Action
"This is the active ingredient. Presence and precision here makes the difference." Sessions of 10–20 min with core action occupying 40–60% of session time are most effective (PMC10955541). Functional Communication Training is classified as EBP by NCAEP (2020).
Sensory Pathway (Putty, Fidgets, Squeeze Toys)
Child squeezes, pinches, pulls, or presses the material for 5–15 minutes. Parent narrates: "You're squeezing! That feels good for your hands." Parent does NOT interrupt — let it run. The proprioceptive input is doing the work. Trust the science. Do not over-talk.
Communication Pathway (AAC / Communication Cards)
When a pinching trigger appears: [1] Intercept BEFORE pinch — redirect hands to card. [2] Prompt: "Show me. Use your card." [3] HONOR THE COMMUNICATION IMMEDIATELY. [4] Praise: "You USED your words! Your card worked!" The card must ALWAYS win faster than pinching does.
Visual Support Pathway (Behavior Visual Cards)
Post "gentle hands" visual at eye level. Before a trigger context, point: "Look — gentle hands." During a near-pinch, calmly point only — no lecture. After successful gentle hands, point again: "You did THAT." Simple, consistent, calm.
Token Pathway (Token Board)
When timer sounds: immediately check hands. Safe hands? → Deliver token + praise + physical celebration. Pinching occurred? → Neutral: "Hands try again. Timer reset." Do NOT lecture. Do NOT express disappointment. Stay regulation-neutral throughout.
Common Execution Errors: Over-talking during sensory engagement · Waiting more than 5 seconds to deliver reinforcement · Lecturing after pinching (provides attention = reward for wrong behavior) · Removing communication tools during frustration

Step 4 of 6
Repeat & Vary
"3 good interactions > 10 forced ones. Dosage matters." SI dosage research recommends 2–3 sessions per week, 8–12 weeks typical protocol. When satiation signals appear — stop immediately.
Repetition Guidance
- Sensory materials: Sustained engagement of 5–15 min total — not a fixed rep count. Vary: squeeze, roll, poke, pull.
- Communication cards: Aim for 3–5 successful uses per trigger context daily. Vary the message: frustration, break, attention, stop.
- Token board: Start with 4–6 tokens per session (achievable quickly). Gradually lengthen intervals as success builds.
Satiation Indicators
- Throwing or pushing away the material
- Yawning or consistently looking away
- Motor restlessness increasing (not decreasing)
- Vocalizations of protest
Variation Options to Maintain Engagement
- Change the putty color or resistance level each week
- Introduce small objects to hide/find in putty (hidden coin, bead)
- Change the squeeze toy texture each week
- Let child choose which material from a visual menu
- Add a new communication card as vocabulary expands
- Practice in different rooms and contexts for generalization
- Have another family member prompt card use to build breadth
Timing: 3–5 minutes for repetition/variation phase.

Step 5 of 6
Reinforce & Celebrate
"Timing matters more than magnitude. Immediate. Specific. Enthusiastic." ABA reinforcement principles + token economy evidence from multiple systematic reviews in autism intervention.
The Reinforcement Window
Within 3 seconds of safe hands behavior → deliver reinforcement. After 5 seconds — the signal degrades. The child's brain connects the reward to the most recent behavior, which may no longer be safe hands.
Sensory Alternative Use: "YES! You squeezed the putty! SAFE HANDS! Amazing!"
Communication Card Use: "You USED YOUR CARD! That was so smart! I heard you!" [Then immediately give what the card requested]
Interval Safe Hands (token): [Deliver token immediately] "GENTLE HANDS! You earned a star!" [High five if child likes touch]
Unprompted Safe Hands in Trigger Context: "I SAW THAT. Your hands were gentle. THAT IS HUGE."
Reinforcer Categories — Match to YOUR Child
- Social: Praise, hug, tickle, high five, clapping
- Access: Preferred toy/screen/food for 2 minutes
- Sensory: Preferred sensory input as reward
- Activity: Chosen activity, special privilege
- Token: Earns toward larger backup reinforcer
⭐ Reinforcement Menu Set — ₹364 · Token Economy System — ₹589 (Amazon.in)
"Celebrate the ATTEMPT, not just the success. Reinforcement must be individualized — ask, observe, test."

Step 6 of 6
The Cool-Down
"No session ends abruptly. Transition is a therapy skill." Visual timer and transition supports are classified as evidence-based practice for autism (NCAEP, 2020).
The Transition Script
"2 more squeezes, then we're all done." [2 minutes before ending]
"One more, then putty goes to sleep."
"Timer going off — all done! Amazing work today."
"One more, then putty goes to sleep."
"Timer going off — all done! Amazing work today."
Cool-Down Sequence
- Transition warning (2 min before): "2 more, then done"
- Final reinforcement delivery — celebrate the session
- Material put-away ritual — child participates if able: "Help me put the putty in the jar"
- Transition comfort item bridge — hand child their item (₹425 · Amazon.in)
- Brief debrief if child can engage: "Your hands were SO safe today."
- Clear next activity cue: "Now we're going to [next activity]"
If Child Resists Ending
- "One more, then done" — honor this ONCE only
- Visual timer is the neutral enforcer — not the parent
- Material goes into a designated "sleeping" spot — same place each time
- This builds the expectation: materials are here, materials rest, materials return
Transition Comfort Item: Keep one small, consistent comfort item that appears only at session-end. The child anticipates it. It signals regulation time is transitioning. This is separate from the session reinforcer. Timing: 2–4 minutes total.
Capture the Data — Right Now
60 seconds of data now saves hours of guessing later. BACB ABA data collection standards require continuous measurement of frequency, duration, and latency (Cooper, Heron & Heward, Applied Behavior Analysis).
What to Record After Every Session
Field | What to Track | |
Pinching Incidents | Number during/after session · Was anyone injured? Y/N | |
Replacement Behavior | How many times did child use alternative (putty/card/fidget)? · Prompted or spontaneous? | |
Session Quality | Rate 1–5 · Child's regulation level at end: Dysregulated / Neutral / Regulated | |
What Worked | One thing that worked · One thing to adjust next session |
GPT-OS® Integration
Data from your session tracking feeds directly into your child's Behavior Safety Readiness Index and informs GPT-OS® TherapeuticAI® session recommendations.
"If pinching decreased by even 1 incident this week: that is progress. Celebrate it. Document it. It compounds."

What If It Didn't Go As Planned?
"Session abandonment is not failure — it is data." ABA troubleshooting draws on functional analysis principles and antecedent modification strategies from behavioral literature.
Child Refused All 9 Materials
Why: Over-demand, wrong arousal state, or materials are still novel. Do: Pair materials with preferred activities for 1 week before requesting use. Leave materials in accessible spots with no demand. Novelty → familiarity → acceptance.
Used Material AND Still Pinched
Why: Material is addressing a different function. Putty for sensory, but pinching is communicative. Do: Reassess function. Attention-seeking → communication tools more relevant. Sensory → increase material resistance/intensity.
Token Board Isn't Working
Why: Backup reinforcer is not motivating enough OR intervals are too long. Do: Shorten intervals dramatically (start at 30 seconds). Find what your child IS motivated by — observe what they reach for. The token is only as powerful as what it earns.
Communication Card Use Not Honored Fast Enough
Why: Normal — it takes caregiver practice too. Do: Communication card use MUST be honored immediately and consistently. If the card works slower than pinching, the child will return to pinching. The card must ALWAYS win.
Pinching Escalated to Biting or Hitting
Why: Demand too high, wrong material, wrong timing, or multiple functions in play. Do: Stop session immediately. Ensure safety. Do not punish. Consult BCBA for Functional Behavior Assessment. Call 9100 181 181 for triage guidance.
Pinches at School But Not at Home
Why: Replacement behavior hasn't generalized. Materials not available at school. Different adults, different reinforcement contingencies. Do: Send materials to school with written protocol. Meet with the teacher. Use the teacher communication template.
No Change After 2 Weeks
Why: Function not correctly identified, or intensity insufficient. Do: Formal Functional Behavior Assessment by BCBA recommended. Call 9100 181 181 for professional referral. This is not failure — it is graduating to the appropriate level of support.

Adapt & Personalize
Your child is unique. This toolkit adapts. Individualized intervention principles span OT (sensory profile-based), ABA (function-based), and SLP (communication profile-based).
Easier Modifications
Difficult days, early phase. Softest putty resistance, 3–5 min sessions, ONE material at a time, 30–60 sec token intervals, single communication card, continuous co-regulation, child's most preferred location.
Standard Protocol
Most days, consolidation phase. Medium resistance, 10–15 min sessions, 2–3 materials rotating, 2–5 min token intervals, 3–5 card vocabulary, structured setup space, gradual fading of parent prompts.
Harder Modifications
Mastery phase, generalization. Firmer resistance, 15–20 min sessions, materials in community settings, 10–15 min token intervals, full vocabulary deck, new caregivers and settings, self-monitoring practice begins.
Sensory Seeker vs. Avoider
Seeker (craves input): Focus putty, pinch fidgets, deep pressure tools. Sensory diet throughout entire day, not just sessions.
Avoider (pinches as protest/escape): Focus communication cards, visual supports. Build in more breaks and choices. Token board for tolerance-building in small increments.
Avoider (pinches as protest/escape): Focus communication cards, visual supports. Build in more breaks and choices. Token board for tolerance-building in small increments.
Age-Based Modifications
- Ages 2–4: 3–5 min, highly tangible reinforcers, maximum parent scaffolding
- Ages 5–8: Standard protocol, token system primary, peer practice introduced
- Ages 9–12: Self-monitoring tools, social skill focus, independence in material use

Week 1–2: What to Expect
Early Tolerance Phase · Progress: 15%
Most parents expect dramatic change. In Week 1–2, look for something smaller — and more significant. SI intervention outcomes emerge across 8–12 week timelines; early phase focuses on tolerance and participation (PMC11506176).
✅ Real Progress Signs (Week 1–2)
- Child accepts material being present without refusal (even if not using it yet)
- Child touches/explores material with curiosity for even 30 seconds
- One pinching incident averted because you redirected to material in time
- Child looks at communication card when prompted (even without using it)
- Caregiver (you) feels more confident and less reactive during trigger moments
- At least one session completed without meltdown
Not Progress Yet — And That's Normal
- Spontaneous, independent replacement behavior — too early
- Significant drop in overall pinching frequency — too early
- Generalization to school or grandparents' house — too early
- Child asking for the putty themselves — typically Weeks 3–4+
Patience Metric: "If your child tolerates the material for 3 seconds longer than last week — that is real progress. Synaptic pathways are forming. You just can't see them yet."

Week 3–4: Consolidation Signs
Consolidation Phase · Progress: 40% · Neural Pathways Forming
Something is shifting. Your child's brain is building new architecture.
🟢 Behavioral Signals
- Child begins to anticipate session — shows positive anticipation when materials appear
- Child reaches toward putty/fidget before tension fully escalates
- Communication card use increasing — even one spontaneous, unprompted use is significant
- Pinching incidents reducing in specific, predictable contexts
- Pinching intensity reducing even if frequency is the same
🧠 Neural Pathway Formation
- Shorter time to regulation after a pinching incident (faster bounce-back)
- Child begins associating the material with calming (reaches for putty when stressed, not just when offered)
- Token board needs fewer reminders — pattern is becoming habitual
🌱 Generalization Seeds (Early)
- Child uses putty unprompted in a different room
- Child hands a caregiver the communication card in a new context
- Sibling reports less pinching than previous weeks
"You may notice you're more confident too. You can see the escalation curve coming and you know exactly what to do. This is your skill growing, not just your child's."

Week 5–8: Mastery Indicators
Mastery Phase · Progress: 75%
Mastery criteria from behavioral measurement standards (PMC10955541 · BACB mastery criteria). When all three primary benchmarks are met for two consecutive weeks: mastery confirmed.
Primary Mastery Benchmarks
- Pinching frequency reduced by 70%+ from baseline Week 1 frequency
- Pinching not causing injury in the last 2 weeks
- Child uses at least ONE replacement behavior spontaneously (unprompted) in most trigger contexts
Generalization Indicators
- Safe hands behavior appearing in at least 2 different settings
- Replacement behavior used with at least 2 different caregivers
- Child demonstrates safe hands during at least one previously high-risk context
When to Stay and Strengthen
- Mastery in home but not generalized to school — stay until 2+ settings
- Mastery with parents but not grandparents/teachers — expand caregivers first
- Mastery with one material but not others — expand material repertoire
⭐ Mastery Unlocked
When all 3 primary benchmarks are met for 2 consecutive weeks:
- Reduce session frequency from daily to 3× per week
- Begin introducing materials in new community settings
- Progress to next level: peer interaction with safe hands
GPT-OS® Threshold: When Behavior Safety Readiness Index shows 70%+ for 2 consecutive weeks, TherapeuticAI® marks this domain ready for next-level progression.
Celebrate This Win
This Is What You Did
- You showed up for sessions when you were exhausted
- You held steady during the sessions that went wrong
- You tracked data when it was hard to see progress
- You adapted when the first approach didn't work
- You believed in your child when results weren't yet visible
This Is What Your Child Did
- Learned that there are other ways to meet their needs
- Built new neural pathways — literally rewired their brain
- Chose replacement behavior over and over, slowly and then suddenly
- Found safer ways to communicate what they couldn't say in words
- Became safer to be around — and felt that safety reflected back
"From __ pinching incidents per day to __. In __ weeks." — Fill in your family's specific numbers. Do something TODAY that you couldn't do 8 weeks ago because of pinching. Go to the playground. Visit a family member. Have a friend over. Feel how different it is now.
"Share this moment with other families. Your story is someone else's hope." — Parental self-efficacy research confirms parent confidence is the strongest predictor of continued home-based intervention.

Red Flags — When to Pause
Trust your instincts — if something feels wrong, pause and ask. This is not fear. This is clinical awareness. WHO NCF Progress Report (2023) — referral pathways integrated into service delivery.
🔴 Pinching Intensity Escalating to Serious Injury
Pinches now causing bruising, breaking skin, or injury requiring medical attention. Risk level has crossed into safety territory. PAUSE all protocol. Seek immediate professional behavioral health support. Call 9100 181 181 NOW.
🔴 Behavior Generalizing to Self-Injury
Child begins pinching themselves in addition to others. Self-injurious behavior requires immediate professional functional assessment. Do not address at home alone. Contact BCBA and NeuroDev pediatrician immediately.
🔴 No Response to Consistent Intervention — 3 Weeks
Frequency unchanged despite daily, consistent implementation. Function may not be correctly identified. Formal Functional Behavior Assessment needed. Call 9100 181 181 for referral to a BCBA.
⚠️ Pinching + New Behaviors (Biting, Hitting)
Multiple topographies of aggression emerging simultaneously. Increased complexity requires professional behavior intervention planning. Consult BCBA. Accelerate professional support timeline.
⚠️ Child's Anxiety or Distress Increasing
Child seems more stressed since beginning intervention. Protocol may be too demanding or wrong function is targeted. Reduce demand, reassess. Consider telehealth OT/ABA consultation.
⚠️ Family Safety Cannot Be Maintained
Siblings or other family members regularly injured despite protocol. Family safety is non-negotiable. Temporary physical separation strategies + immediate professional consultation required.
📞Escalation Pathway: Self-resolve → Call 9100 181 181 (triage) → Teleconsult booking → Clinic visit (nearest Pinnacle center). Free · 24x7 · 16+ languages.
The Progression Pathway
D-386 is one waypoint in your child's behavioral safety journey. WHO/UNICEF developmental trajectory framework — intervention sequencing follows evidence-based developmental cascades.
"Safe Hands in All Contexts → Social Inclusion → Peer Relationships → Community Participation → Full developmental trajectory restored."
Related Techniques in Domain D
In Domain D (Behavior & Flexibility), here are the most closely related techniques. If you have the D-386 starter kit — putty + communication cards + token board — you already own materials for four related technique pages.

D-384 · Hitting Others
⬤ Core Difficulty
Materials: Squeeze toys, visual supports, token boards
✅ Your D-386 kit covers this.
Materials: Squeeze toys, visual supports, token boards
✅ Your D-386 kit covers this.

D-385 · Biting Others
⬤ Core Difficulty
Materials: Chewy tools, AAC communication, sensory tools
Focus: Oral motor and communication pathways
Materials: Chewy tools, AAC communication, sensory tools
Focus: Oral motor and communication pathways

D-387 · Hair Pulling
⬤ Core Difficulty
Materials: Tactile replacements, calming tools, social stories
✅ Your D-386 putty and calm down kit covers this.
Materials: Tactile replacements, calming tools, social stories
✅ Your D-386 putty and calm down kit covers this.

D-388 · Scratching Others
⬤ Core Difficulty
Materials: Fidgets, gloves, sensory redirects
✅ Your D-386 fidgets and visual supports cover this.
Materials: Fidgets, gloves, sensory redirects
✅ Your D-386 fidgets and visual supports cover this.

D-390 · Aggression Toolkit
⬤ Advanced
Multi-topography behavior intervention for complex presentations
Multi-topography behavior intervention for complex presentations

C-Series · Emotional Regulation
⬤ Core → Advanced
For when emotion drives behavior — underpins all Domain D techniques
For when emotion drives behavior — underpins all Domain D techniques
Your Child's Full Developmental Map
Pinching is one behavior. Your child's development is a 12-domain landscape. The WHO/UNICEF Nurturing Care Framework's five components of nurturing care require holistic developmental monitoring across all domains.
What Domain D Connects To
- Domain A (Sensory): Many D challenges have sensory roots → assess together
- Domain B (Communication): Many D challenges are communication failures → address together
- Domain C (Emotional): Regulation capacity determines behavior threshold → co-treat
- Domain J (Self-Care): Safe hands is a prerequisite for assisted self-care → sequence after
Your Child's Full Profile
"This technique is one piece of a larger plan. The plan is your child's life."
Or call: 📞9100 181 181

Families Who've Been Here
Pinnacle Blooms Network® · 20M+ Sessions · 97%+ Measured Improvement
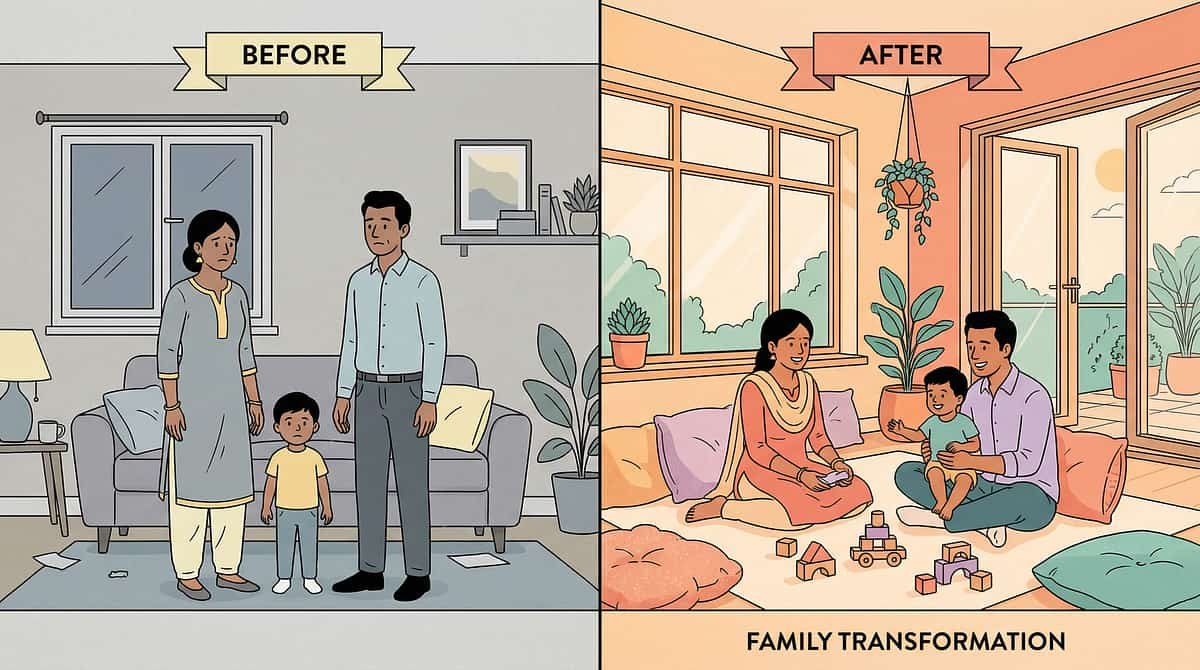
Sensory-Seeking Function — Before & After
"Our son was leaving marks on everyone — his little sister, his classmates. Every day, multiple incidents. The school was talking about removing him from inclusion. We were terrified."
8 weeks with therapy putty + deep pressure routine:
"The BCBA at Pinnacle told us he was seeking proprioceptive input — his hands literally craved that pressure. Within 3 weeks of daily putty and a fidget on his desk, incidents dropped by half. By week 8, he was going days without pinching. He now asks for his 'squeeze toy' when he feels the urge. He's still in inclusion."
Therapist's note: "Sensory-based pinching responds well when the replacement provides equivalent proprioceptive intensity."
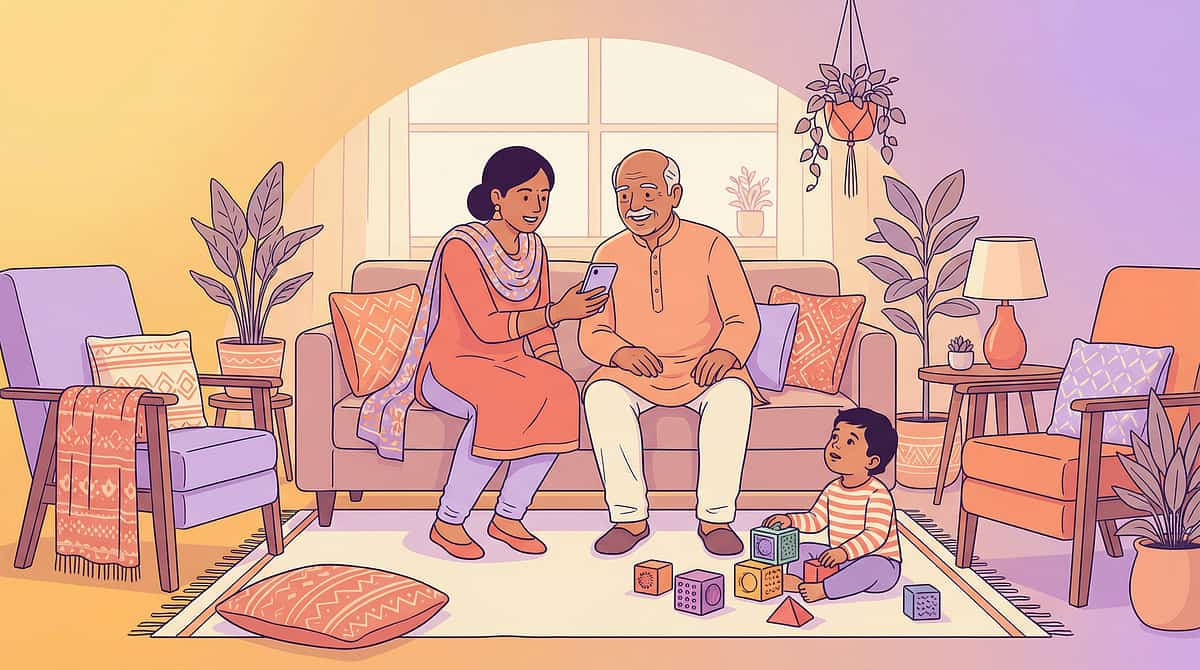
Communication Function — Before & After
"She pinched whenever she was frustrated or wanted our attention. We had no idea it was communication. We thought she was being aggressive. We feel terrible that we punished her for communicating."
6 weeks with communication cards + parent training:
"Her SLP helped us understand that pinching was her loudest word. We made cards for 'I'm mad,' 'I need a break,' and 'Look at me.' Within 2 weeks she started using the 'I'm mad' card. The pinching is almost gone. And we communicate so much better now — all of us."
"Your child isn't pinching because they're bad. They're pinching because it worked. Give them something that works better." — Pinnacle Blooms Consortium Behavior Support Team
Connect With Other Parents
Isolation is the enemy of adherence. You need a community, not just a protocol. Over 1,000 individuals from 111 countries contributed to the WHO Nurturing Care Framework — because raising children who need extra support requires community.
Pinnacle Parent WhatsApp Group
Connect with parents managing pinching, biting, hitting, and other challenging behaviors. Share what's working. Ask what isn't. Join at pinnacleblooms.org/community
Pinnacle Online Forum
Post your questions. Share your wins. Anonymous if preferred. The peer knowledge in this community is extraordinary. Visit pinnacleblooms.org/forum
Local Parent Meetup
70+ centers across India — each running monthly parent meetups. Find your nearest center and connect with families in your city. Real, local, human support.
Peer Mentor Matching
Connect with a family who was exactly where you are 6 months ago — and is now on the other side. The most powerful support comes from someone who actually lived it. Request a match: 9100 181 181
📞FREE National Autism Helpline: 9100 181 181 — 24x7 · 16+ Languages. When you are 6 months ahead of where you are now, consider sharing your journey. The parent who is where you were right now needs to hear from you.
Your Professional Support Team
Home + clinic = maximum impact. The two multiply each other. Every home session is more effective when supervised by a professional. Every clinic session is more effective when supported at home.
Therapist Matching for D-386 Pinching Others
BCBA — Primary Discipline Match
For formal Functional Behavior Assessment + Behavior Intervention Plan. Essential if pinching is causing injury or not responding to home strategies.
Pediatric Occupational Therapist
For sensory processing profile assessment + sensory diet design. Identifies whether sensory input is the driver behind pinching behavior.
Speech-Language Pathologist
If communication is the function — AAC evaluation and Functional Communication Training program design.
Consultation Options
📞Call FREE Helpline: 9100 181 181
24x7 · 16+ languages · Immediate triage guidance
24x7 · 16+ languages · Immediate triage guidance
🏥Book Center Consultation
In-person comprehensive assessment · 70+ locations
pinnacleblooms.org/book
In-person comprehensive assessment · 70+ locations
pinnacleblooms.org/book
💻Teleconsult from Home
For families in remote locations or outside India
pinnacleblooms.org/teleconsult
For families in remote locations or outside India
pinnacleblooms.org/teleconsult
Pinnacle centers work with multiple insurance providers. Government schemes and NHFDC funding may be applicable.

The Research Library
For the parent who wants to go deeper. The evidence is vast. Here is where to start. Confidence rating: 78% High Confidence — based on 16 systematic review studies + 24 meta-analysis studies.
PRISMA Systematic Review (Children, 2024)
16 studies (2013–2023) confirm sensory integration intervention meets evidence-based practice criteria for children with ASD across behavioral outcomes including aggression. Level I Evidence. → PMC11506176
Meta-Analysis (WJCC, 2024)
24 studies: SI therapy effectively promoted social skills, adaptive behavior, sensory processing, and gross/fine motor skills. Level I Evidence. → PMC10955541 · DOI: 10.12998/wjcc.v12.i7.1260
NCAEP Report (2020)
Functional Communication Training, token economies, and visual supports classified as evidence-based practices for autism with highest level evidence. Level I Evidence.
Indian RCT — Padmanabha et al. (2019)
Home-based sensory interventions in Indian pediatric populations: significant outcomes demonstrated. First Indian RCT for home-based ASD intervention. Level II Evidence. → DOI: 10.1007/s12098-018-2747-4
WHO Care for Child Development Package (2023)
Age-specific evidence-based recommendations for caregivers, implemented in 54+ LMICs. Validates family-delivered, home-based intervention as effective. → PMC9978394
Frontiers in Integrative Neuroscience (2020)
Comprehensive neurological framework for sensory processing treatment in ASD — establishes brain-based evidence for sensory-based behavior interventions. → DOI: 10.3389/fnint.2020.556660

How GPT-OS® Uses Your Data
Your session data doesn't disappear. It becomes intelligence — for your child, and for every child like yours. Digital health interventions for ASD: 21 RCTs, 1,050 participants (2024 meta-analysis).
What GPT-OS® Learns from D-386 Data
- Pinching frequency trajectory — is the curve moving correctly?
- Which of the 9 materials shows the strongest replacement behavior rate
- Token interval at which consistency is highest
- Communication card use — which messages are most frequently accessed
- Time-of-day and context patterns for remaining incidents
Privacy & Data Protection
- 🔒 All data encrypted and anonymized for population-level analysis
- 🔒 Individual data accessible only to your authorized care team
- 🔒 No data sold or shared with third parties
- 🔒 DPDP Act (India) compliant · GDPR-aligned
"When 1,000 families track D-386 sessions, GPT-OS® identifies patterns that make the next family's outcomes better. Your data helps every child like yours."
Watch the Reel
"9 Materials That Help With Pinching Others" — Reel D-386 · Domain D: Challenging Behaviors · Episode 386 of 999 · Presented by Pinnacle Blooms Network® Behavior Support Consortium (ABA/BCBA + OT + SLP integrated). Video modeling is classified as an evidence-based practice for autism (NCAEP, 2020).
What You'll See in This Reel
- Therapy putty demonstrating proprioceptive replacement in real time
- Pinch fidgets showing right action, right target
- Communication cards in real use with a child
- Token board for safe hands reinforcement
- All 9 materials in 60 seconds — practical, visual, parent-executable
"Watching this reel is itself a therapeutic learning activity — for you and your child. Video modeling improves parent skill acquisition across multiple modalities."
Share This With Your Family
Consistency across caregivers multiplies impact. If only one caregiver executes this protocol, the child gets partial intervention. If everyone uses the same language, the same materials, the same reinforcement — the results multiply. (WHO CCD Package — multi-caregiver training as critical for generalization)
Share Buttons
Pre-Written WhatsApp Message:
"Hi! I found this page from Pinnacle Blooms Network on helping children who pinch others. It has 9 materials, step-by-step instructions, and the science behind it. Thought it would help: techniques.pinnacleblooms.org/behavior-support/9-materials-pinching-others-D386"
"Hi! I found this page from Pinnacle Blooms Network on helping children who pinch others. It has 9 materials, step-by-step instructions, and the science behind it. Thought it would help: techniques.pinnacleblooms.org/behavior-support/9-materials-pinching-others-D386"
Explain to Grandparents — Simple Version
- Offer the squeeze ball immediately when child looks like they're about to pinch
- Say: "Hands on ball, not on people"
- If they use it: celebrate loudly: "Safe hands! Amazing!"
- If they pinch: say calmly "Ouch. Hands down." Offer ball again.
- No lectures. No long discussions. Keep it simple.
Downloadable Family Guide
"D-386 Family Guide — 1 Page PDF" — A simplified, printable version for:
- Grandparents who prefer paper
- School teachers for classroom implementation
- Babysitters and caregivers new to the approach
Teacher/School Communication Template
"Dear [Teacher's name], our child uses the following behavior support system at home and we would appreciate consistency in school. Here are the 3 things that help most..."

Frequently Asked Questions
Every question you're afraid to ask — answered. If you don't find your answer here, ask GPT-OS® at pinnacleblooms.org/ask or book a teleconsultation via 9100 181 181.
My child's pinching is getting worse since I started. Is that normal?
Sometimes behavior temporarily increases at the start — called an "extinction burst." This happens when pinching briefly stops working and the child escalates trying to get the old response. This is actually a sign the intervention is working. Stay consistent. Typically resolves within 1–2 weeks. If intensity reaches injury level, call 9100 181 181 immediately.
How long before I expect a reduction in pinching?
Most families see initial reduction in 2–4 weeks with consistent implementation. Significant reduction (50%+) typically in 4–8 weeks. Full mastery 8–12 weeks. If no change after 3 weeks of consistent daily implementation, reassess the function — the wrong tool may be addressing the wrong function.
My child only pinches at school, not at home. Why?
Different environments have different triggers and reinforcement contingencies. The function may differ at school (escape from academic demands) vs. home (attention-seeking). The solution must be implemented where the behavior occurs. Use the teacher letter template to implement the protocol at school with the same materials.
Can I use all 9 materials at once?
Start with 1–2 materials that match the most likely function, then expand. Overwhelming with all 9 immediately can feel confusing. Begin with putty (sensory) + one communication card + a simple token board. Add others as these consolidate over 2–3 weeks.
My child doesn't seem to like any of the sensory materials. What then?
This may indicate pinching is primarily communicative or attention-seeking. Shift focus to communication cards and token board. If sensory, consider more intense alternatives — deep pressure vest, body sock, resistance band work — and consult an OT for sensory profile assessment.
My spouse doesn't believe this approach will work. How do I get buy-in?
Track data from Day 1 (session log) and show the trend. Numbers convert skeptics more reliably than explanation. The shareable WhatsApp link and grandparent explanation on the previous card also helps. The Pinnacle helpline (9100 181 181) can also speak directly with family members who have questions.
We've tried this and other approaches and nothing works. Are we doing something wrong?
No. Some children's pinching has multiple functions simultaneously, or the function is complex and requires formal professional Functional Behavior Assessment. If consistent implementation over 4+ weeks shows no improvement, this is the signal for professional FBA. Call 9100 181 181 and ask for BCBA referral. This is not failure — it is graduating to the appropriate level of support.
Preview of 9 materials that help with pinching others Therapy Material
Below is a visual preview of 9 materials that help with pinching others therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.






Link copied!

Your Next Step — Start Now
You have everything you need. The next step is the only one that matters.
70+
Centers Across India
In-person comprehensive assessment and therapy available nationwide
20M+
Therapy Sessions
Pinnacle Blooms Network® clinically validated outcomes data
97%+
Measured Improvement
Across families who implement consistently with professional guidance
"You don't need to be perfect. You need to be consistent. Consistent and imperfect beats perfect and sporadic — every time."
★ Validated by the Pinnacle Blooms Consortium ★
OT · SLP · ABA/BCBA · SpEd · NeuroDev Pediatrics · CRO
📞FREE National Helpline: 9100 181 181
24x7 · 16+ Languages
India's only free national autism helpline
24x7 · 16+ Languages
India's only free national autism helpline
© 2025–2026 Pinnacle Blooms Network® · Unit of Bharath Healthcare Laboratories Pvt. Ltd. · CIN: U74999TG2016PTC113063 · DPIIT: DIPP8651 · MSME: TS20F0009606 · GSTIN: 36AAGCB9722P1Z2
This content is educational and informational only. It does not replace individualized assessment and intervention from licensed professionals. Pinching behavior that causes injury or does not respond to consistent home-based intervention requires immediate professional evaluation. Individual results vary.