When the School Cafeteria Becomes Impossible
"He stops at the cafeteria door every single day. While other children rush in for lunch, my son stands there — hand over his nose, eyes watering, already gagging before he's taken a single step inside. The teachers think he's being dramatic. He's not. He genuinely cannot walk into that room without feeling sick."
9 Materials That Help When Your Child Gags at Smells — protection strategies, environmental modifications, and nervous system support that can give your child back the spaces they've lost.
"You are not failing. Your child's nervous system is speaking. The gagging is real — it is involuntary, physiological, and neurological. Not a behavior. Not drama. Not manipulation. Your child deserves to breathe without fear, and that starts here."
🏛️ Pinnacle Blooms Network® Consortium
Validated by OT • SLP • ABA • SpEd • NeuroDev Pediatrics
Research Evidence: WHO Nurturing Care Framework (2018) — Early identification and parental awareness directly impacts developmental outcomes. The period from pregnancy to age 3 is key for development, and sensory processing challenges identified early respond best to structured intervention. 📎 Reference: nurturing-care.org/ncf-for-ecd

You Are Not Alone — The Numbers
Olfactory hypersensitivity with gagging is among the most functionally impairing sensory sensitivities — because smells are everywhere, and the gagging response is involuntary. This is not rare. This is not unusual. And it is not untreatable.
80%
Sensory Difficulties in ASD
Children diagnosed with autism display sensory processing difficulties (PRISMA Systematic Review, 2024)
40-70%
Olfactory Over-Responsivity
Autistic children show olfactory over-responsivity — severe presentations with gagging affect a significant subset
1 in 36
ASD Diagnosis Rate
Children in the U.S. diagnosed with ASD (CDC, 2023) — India's estimates place 2–3 million children on the spectrum
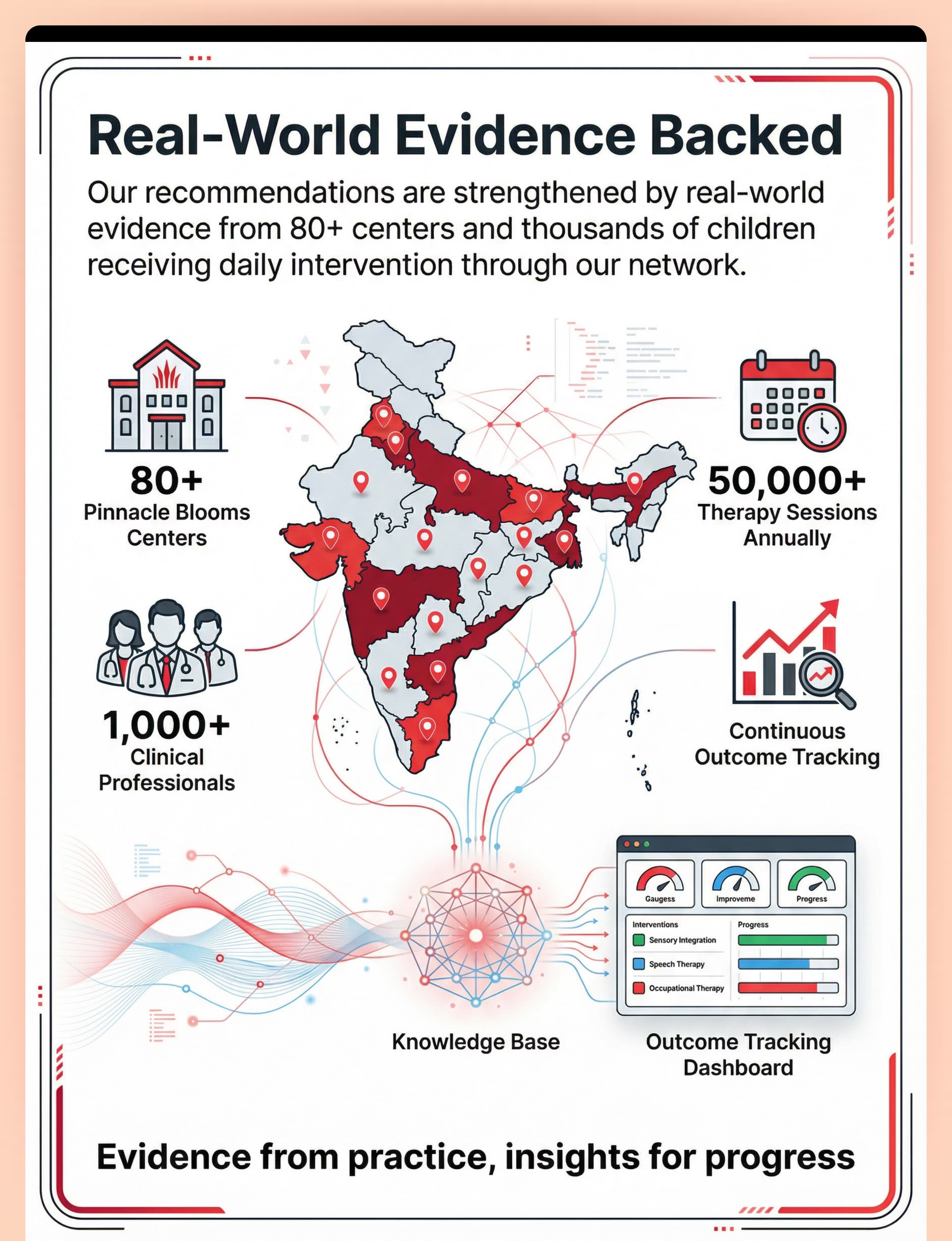
India-Specific Context: Across Pinnacle Blooms Network's 70+ centers, olfactory sensitivity is among the top 10 presenting concerns at initial sensory assessment. Families from Tier-1, Tier-2, and Tier-3 cities across India report the same core challenge: a child who cannot participate in daily life because ordinary smells trigger distress.
Research Evidence: PRISMA Systematic Review (2024): 16 articles from 2013–2023 confirm 80% sensory processing difficulty prevalence in ASD. Meta-analysis (World J Clin Cases, 2024): Sensory integration therapy effectively promotes social skills, adaptive behavior, sensory processing, and motor skills across 24 studies. 📎 References: PMC11506176 | PMC10955541 | DOI: 10.12998/wjcc.v12.i7.1260

What's Happening in Your Child's Brain
The Neuroscience, Translated
When your child smells something — cooking food, a cleaning product, someone's perfume — here's what happens differently in their nervous system:
Olfactory Receptors Fire
Scent molecules enter the nose and activate receptors. In your child, these receptors are more sensitive, firing at lower thresholds.
Signal Amplification
The olfactory bulb transmits signals to the brain. In olfactory hypersensitivity, this signal is amplified — what registers as "food cooking" in a typical brain registers as "toxic chemical" in your child's brain.
Amygdala Activation
The brain's threat center activates. This is not a choice — it is an automatic danger response. The brain genuinely believes the smell is harmful.
Vagus Nerve Activation
The body's protective reflex system engages. The vagus nerve triggers the gagging reflex — a physiological attempt to protect the body from what the brain perceives as a noxious substance.
"This is a wiring difference, not a behavior choice. Your child's brain is doing exactly what it's supposed to do when it detects danger — the difference is that the danger threshold is set far too low. Ordinary smells are being flagged as threats."
Research Evidence: Frontiers in Integrative Neuroscience (2020): Comprehensive framework establishing the neurological basis for sensory-based interventions in ASD. 📎 Reference: DOI: 10.3389/fnint.2020.556660
Where This Sits in Development
1
0–3 Months
Newborn scent recognition — baby distinguishes mother's scent within hours of birth
2
6–12 Months
Smell preference development — infant begins showing scent likes and dislikes
3
1–3 Years
Olfactory discrimination — child develops mature smell identification abilities
4
3–6 Years
Social smell awareness — navigating environments with strong smells. Challenge zone begins here.
5
6–14 Years
Smell-environment navigation → Independent sensory management. Current intervention window.
Olfactory processing develops early — newborns can distinguish their mother's scent within hours of birth. By age 3, children typically have mature olfactory discrimination. When olfactory hypersensitivity with gagging persists or emerges in the 3–14 age band, it indicates persistent sensory processing differences that benefit from structured intervention.
Comorbidity Awareness
Olfactory hypersensitivity frequently co-occurs with:
- Gustatory (taste) sensitivity — affecting food acceptance and nutrition
- Tactile over-responsivity — particularly around the face and mouth
- Anxiety — anticipatory anxiety about potential smell exposures
- Food refusal — smell-based rejection before any tasting occurs
- Social avoidance — withdrawing from environments where smells are present
"From severe aversion → to managed sensitivity → to functional tolerance. This is a journey, not a single event. And your child's nervous system has the capacity to adapt when supported correctly."
Research Evidence: WHO Care for Child Development (CCD) Package: Age-specific evidence-based recommendations for caregivers. Implemented in 54 low- and middle-income countries. 📎 References: PMC9978394 | WHO/UNICEF CCD Package (2023)

The Evidence Behind These Strategies
Evidence Grade: Level II — Strong
Based on systematic reviews, meta-analyses, and randomized controlled trials supporting sensory integration interventions and environmental modification strategies for olfactory over-responsivity.
1
PRISMA Systematic Review (2024)
16 articles from 2013–2023 confirm that sensory integration intervention meets criteria to be considered evidence-based practice for children with ASD. Olfactory desensitization and environmental modification are components of comprehensive sensory programs. 📎 PMC11506176
2
Meta-Analysis (World J Clin Cases, 2024)
Sensory integration therapy across 24 studies demonstrated effective promotion of social skills, adaptive behavior, and sensory processing. Effect sizes were significant for sensory regulation outcomes. 📎 PMC10955541
3
Indian RCT (Padmanabha et al., 2019)
Home-based sensory interventions demonstrated significant outcomes for Indian families, validating parent-administered protocols across diverse socioeconomic contexts. 📎 DOI: 10.1007/s12098-018-2747-4
4
NCAEP Evidence Report (2020)
Sensory integration is classified as evidence-based practice. Visual supports, environmental modification, and self-management strategies are all classified as evidence-based. 📎 NCAEP Report (2020)
"Clinically validated. Home-applicable. Parent-proven. These are not experimental approaches — they are evidence-based strategies deployed across 70+ Pinnacle centers and refined through 20 million+ therapy sessions."

ACT II: THE KNOWLEDGE TRANSFER
Olfactory Protection & Desensitization Protocol
Parent-Friendly Name: "The Smell Shield Strategy"
A multi-layered intervention approach that combines environmental modification, personal protection tools, preferred scent strategies, nervous system regulation, and gradual desensitization to enable children with severe olfactory hypersensitivity to participate in daily environments that were previously inaccessible due to gagging responses. The protocol works on three levels simultaneously: blocking overwhelming smells (protection), building tolerance (desensitization), and supporting the nervous system (regulation).
Domain
Sensory Processing (Domain A) — Olfactory Over-Responsivity with Gagging — SPD-OLF-OR
Age Range
3–14 years
Session Duration
10–20 min home protocol
Frequency
Daily environmental mods + 2–3 structured sessions/week
Canon Material Badges
Aromatherapy/Scent Kit
Sensory Tent/Calm Space
Breathing/Relaxation Tools
Visual Schedules
Communication Cards
Weighted/Deep Pressure Tools
📎 128 Canon Materials: Explore at materials.pinnacleblooms.org

Who Uses This Technique — Your Multidisciplinary Team

🩺 Occupational Therapist (Primary Lead)
Designs the sensory protocol. Conducts the olfactory sensitivity assessment using standardized sensory processing profiles. Determines which materials match the child's specific triggers. Guides the desensitization hierarchy and monitors nervous system responses. Trains parents on environmental modification.

🗣️ Speech-Language Pathologist
Addresses the intersection of olfactory sensitivity with feeding and nutrition. When gagging at food smells prevents eating, SLPs work on expanding food acceptance through smell-based feeding therapy. Coordinates oral-motor strategies that reduce the gagging reflex.

📊 Board Certified Behavior Analyst
Develops the behavioral framework: reinforcement schedules for approaching challenging environments, data collection systems for tracking gagging frequency and tolerance duration, and functional analysis of avoidance patterns. Designs the antecedent management strategy.

👨⚕️ NeuroDevelopmental Pediatrician
Rules out medical causes of gagging (GERD, cyclical vomiting syndrome, GI conditions). Monitors for red flags requiring medical intervention. Provides the diagnostic context within which sensory interventions operate.
"This technique crosses therapy boundaries because the brain doesn't organize by therapy type. Your child's olfactory sensitivity affects feeding (SLP), daily participation (OT), behavioral patterns (ABA), and medical wellbeing (Pediatric). That's why Pinnacle's FusionModule™ coordinates all four disciplines into a single intervention pathway."
Research Evidence: Adapted UNICEF/WHO Nurturing Care Framework for SLPs (2022). 📎 Reference: DOI: 10.1080/17549507.2022.2141327

What You Need — Primary Materials
Everything on this card can be sourced within India. Prices in INR. Direct purchase links included.
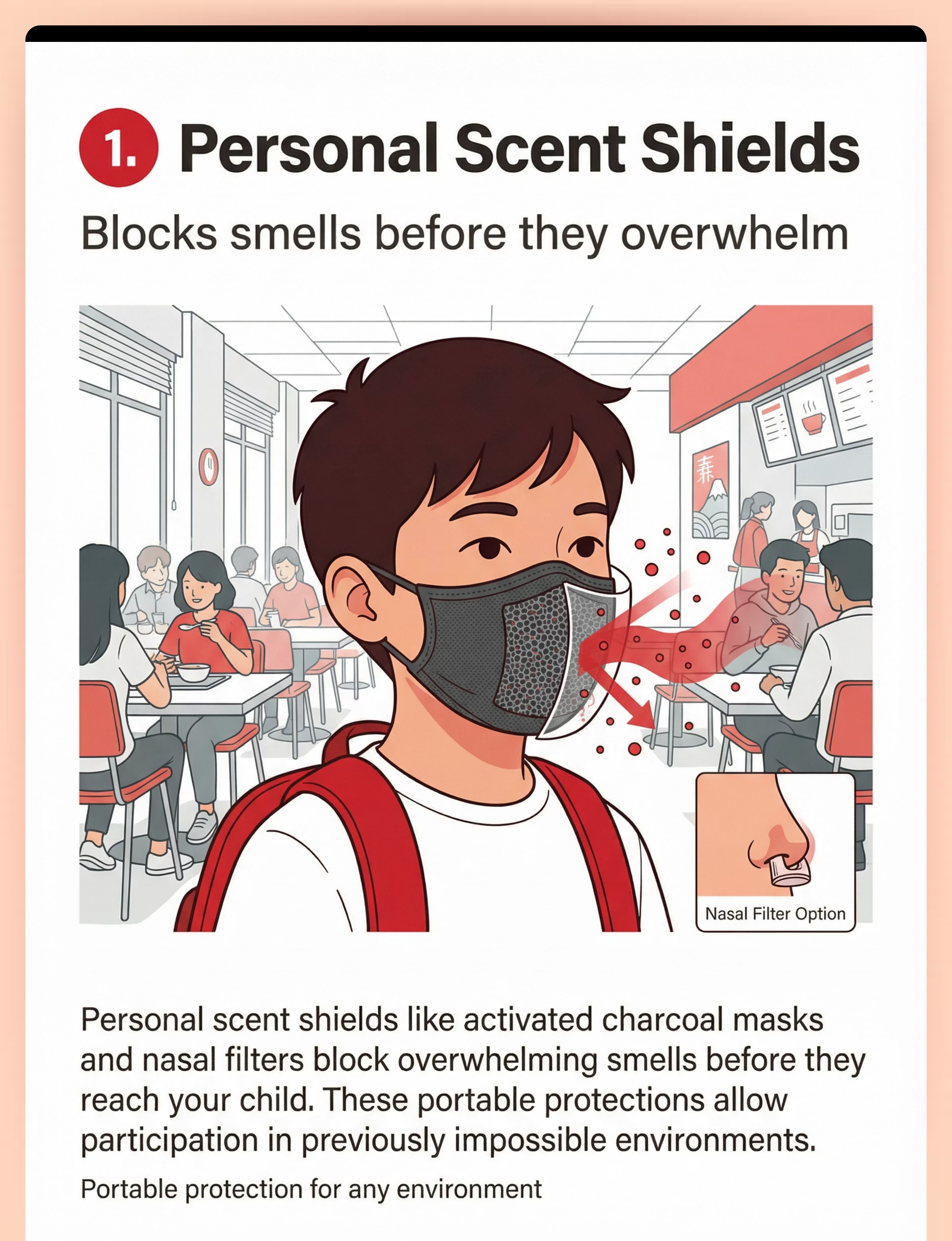
Personal Scent Shields
Activated charcoal masks and nasal filters
🏷️ Canon: Sensory Regulation Tools
💰 ₹300–1,500
🏷️ Canon: Sensory Regulation Tools
💰 ₹300–1,500
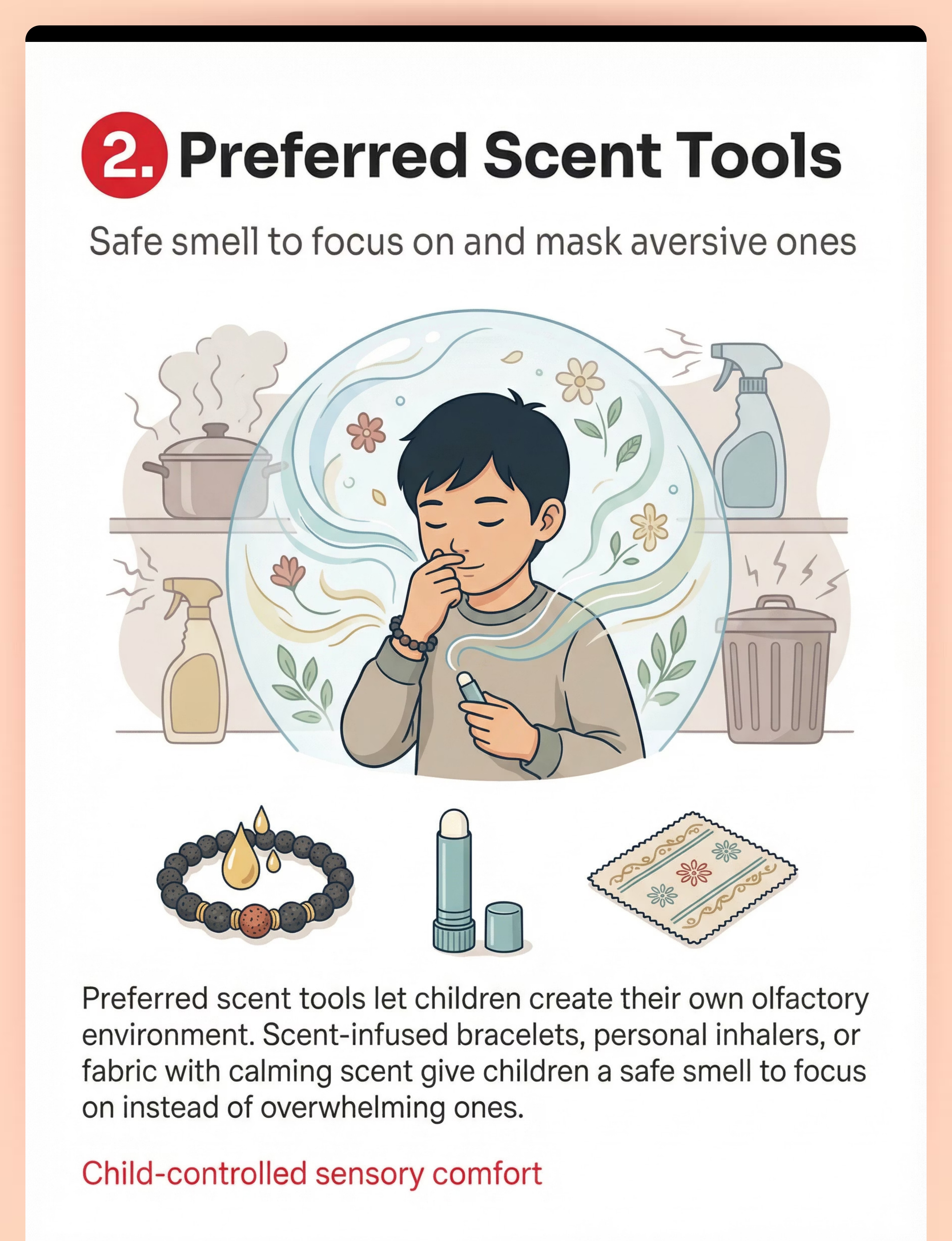
Preferred Scent Tools
Aromatherapy bracelets, personal inhalers, scented fabric
🏷️ Canon: Aromatherapy/Scent Kit
💰 ₹200–800
🏷️ Canon: Aromatherapy/Scent Kit
💰 ₹200–800
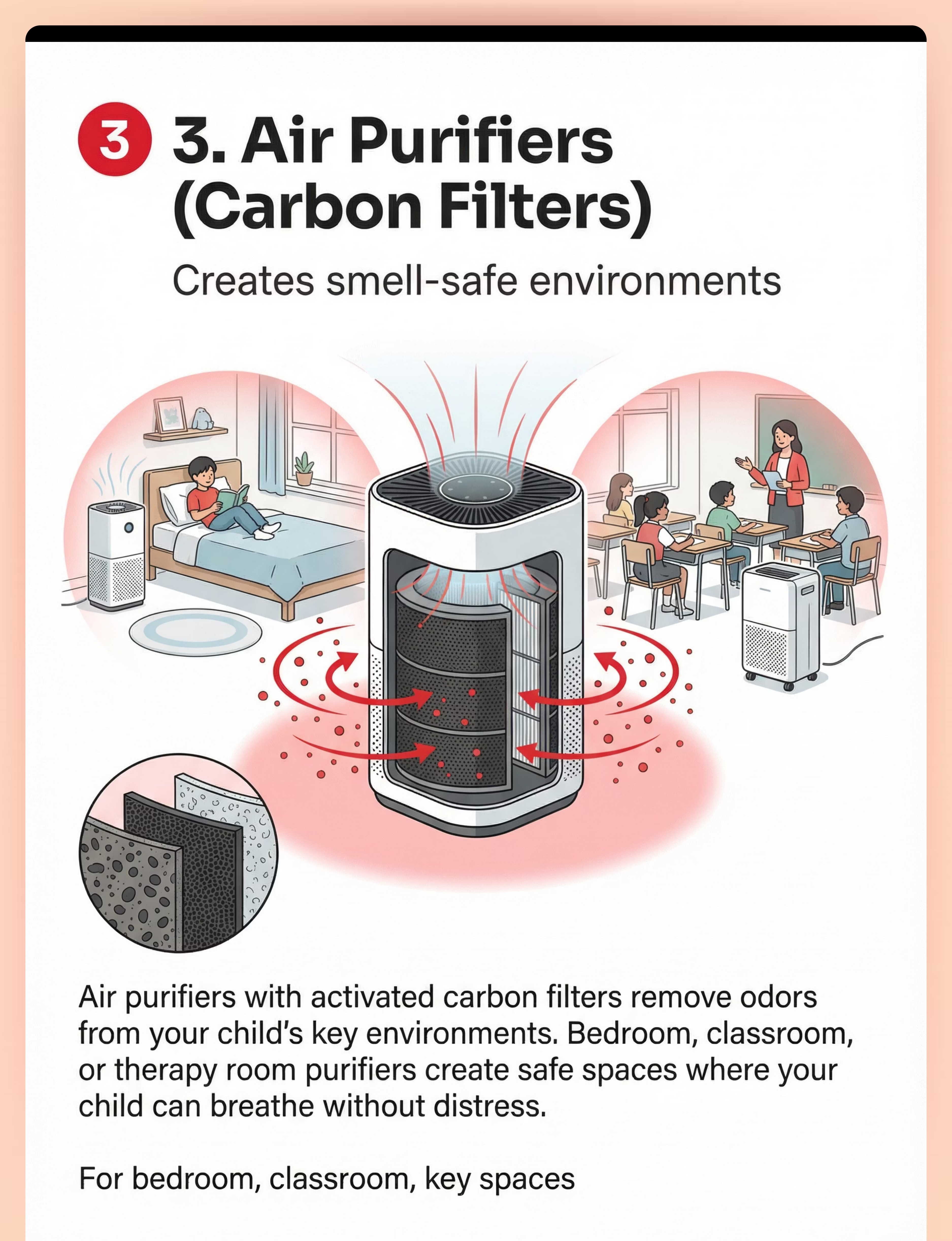
Air Purifiers
HEPA + activated carbon filters
🏷️ Canon: Environmental Modification
💰 ₹3,000–15,000
🏷️ Canon: Environmental Modification
💰 ₹3,000–15,000
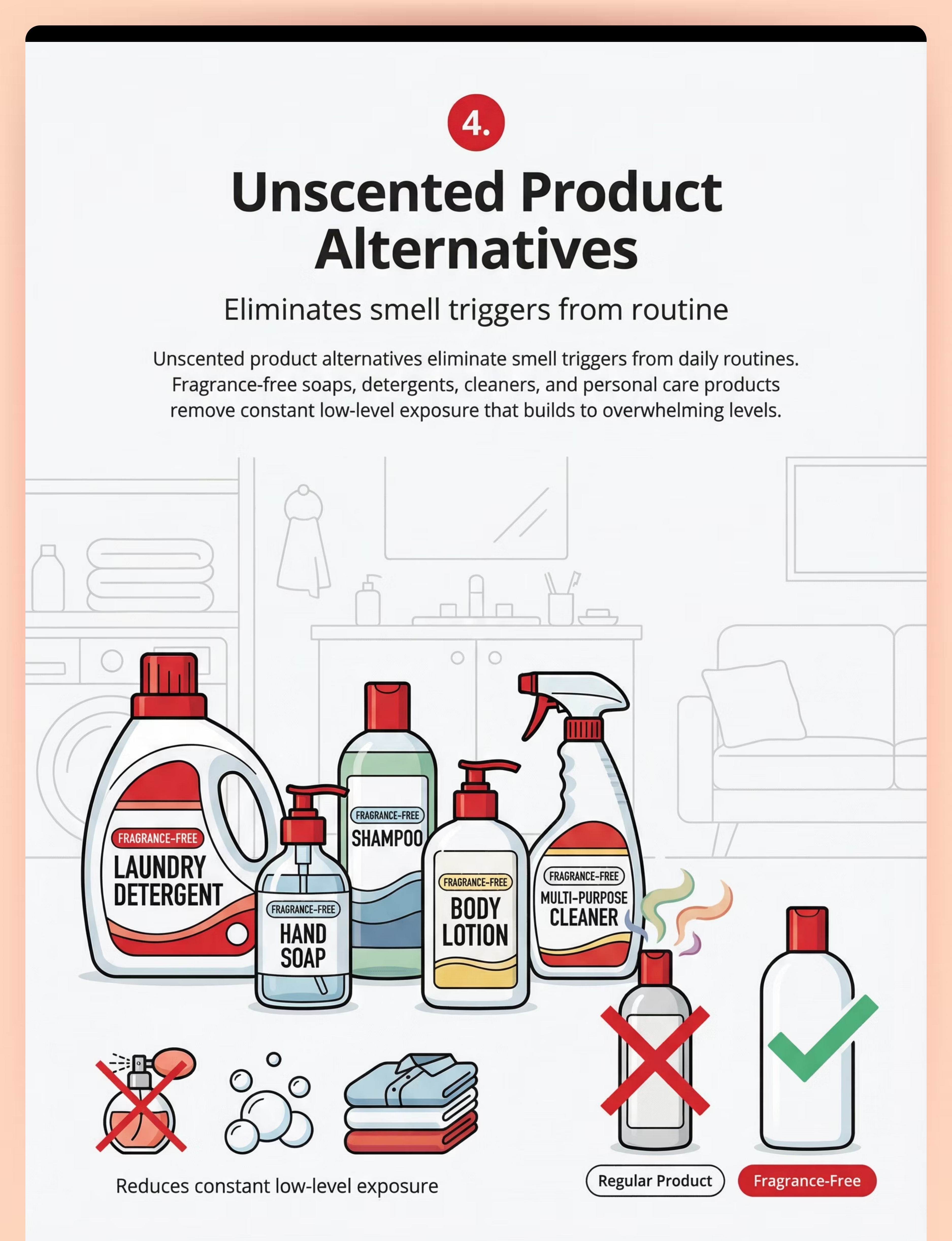
Fragrance-Free Products
Unscented soap, detergent, shampoo, cleaner
🏷️ Canon: Environmental Modification
💰 ₹200–800
🏷️ Canon: Environmental Modification
💰 ₹200–800
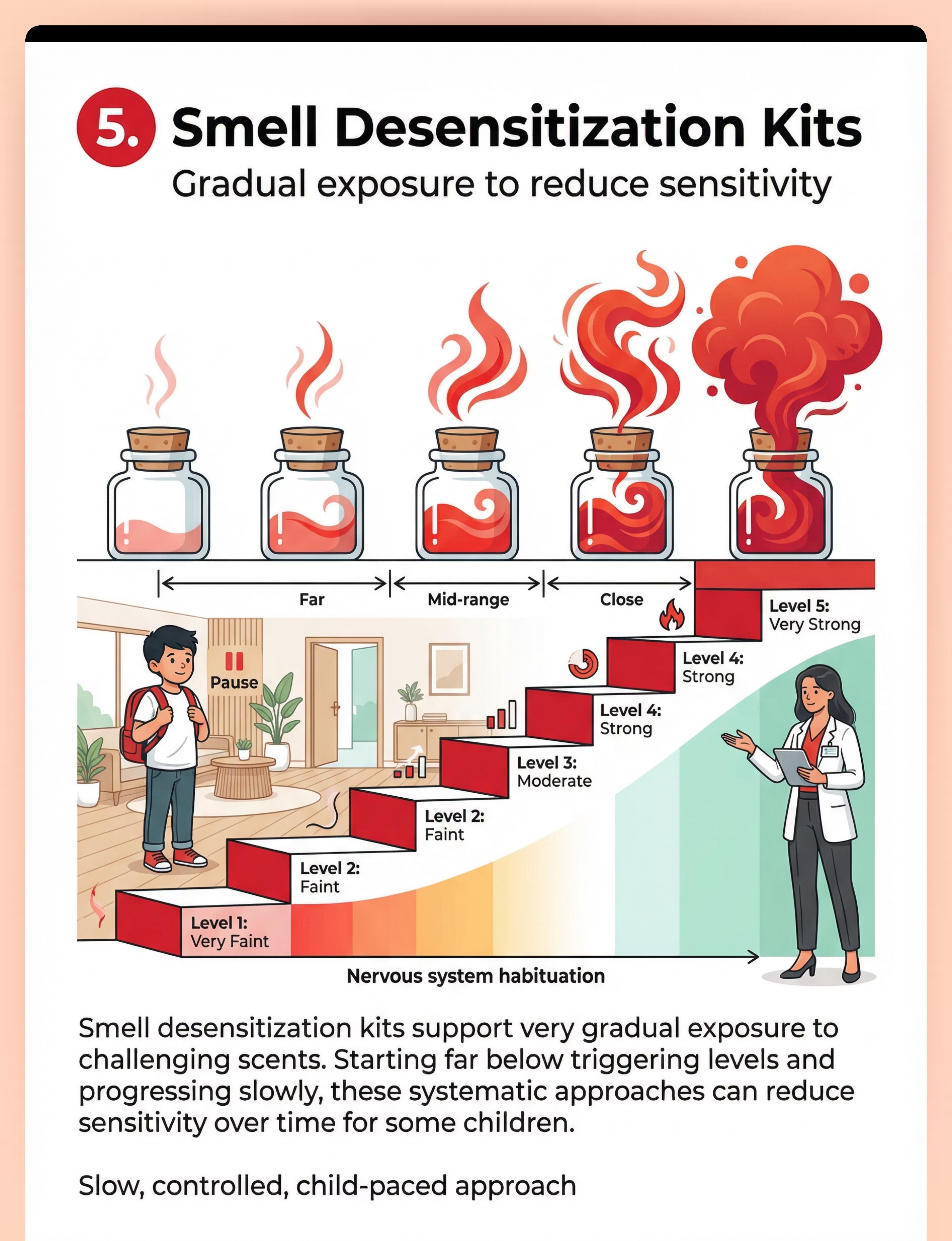
Desensitization Kit
Graded scent jars, distance markers, progress chart
🏷️ Canon: Aromatherapy/Scent Kit
💰 ₹500–2,000
🏷️ Canon: Aromatherapy/Scent Kit
💰 ₹500–2,000
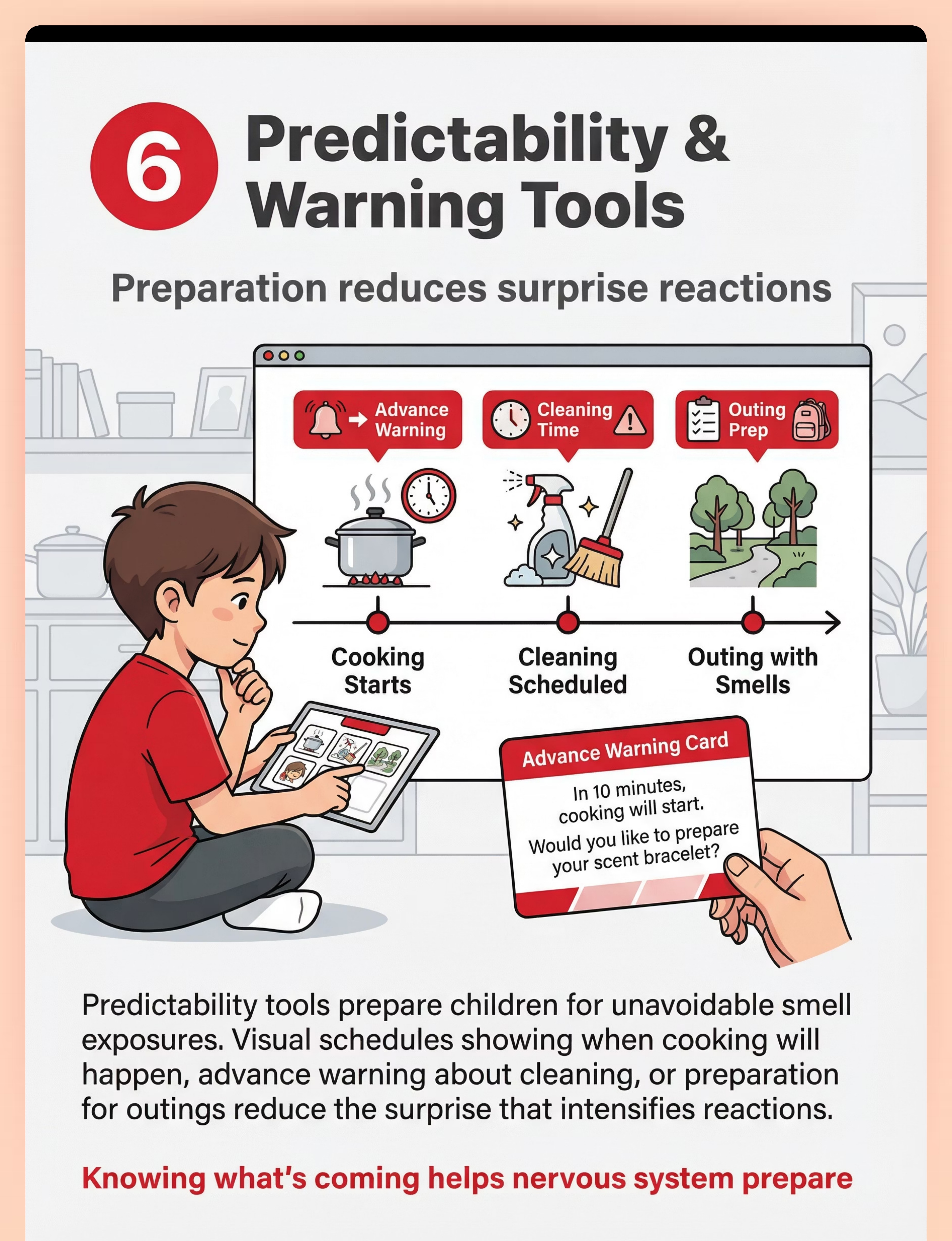
Predictability Tools
Visual schedules, smell warning cards, timers
🏷️ Canon: Visual Schedules
💰 ₹100–400
🏷️ Canon: Visual Schedules
💰 ₹100–400
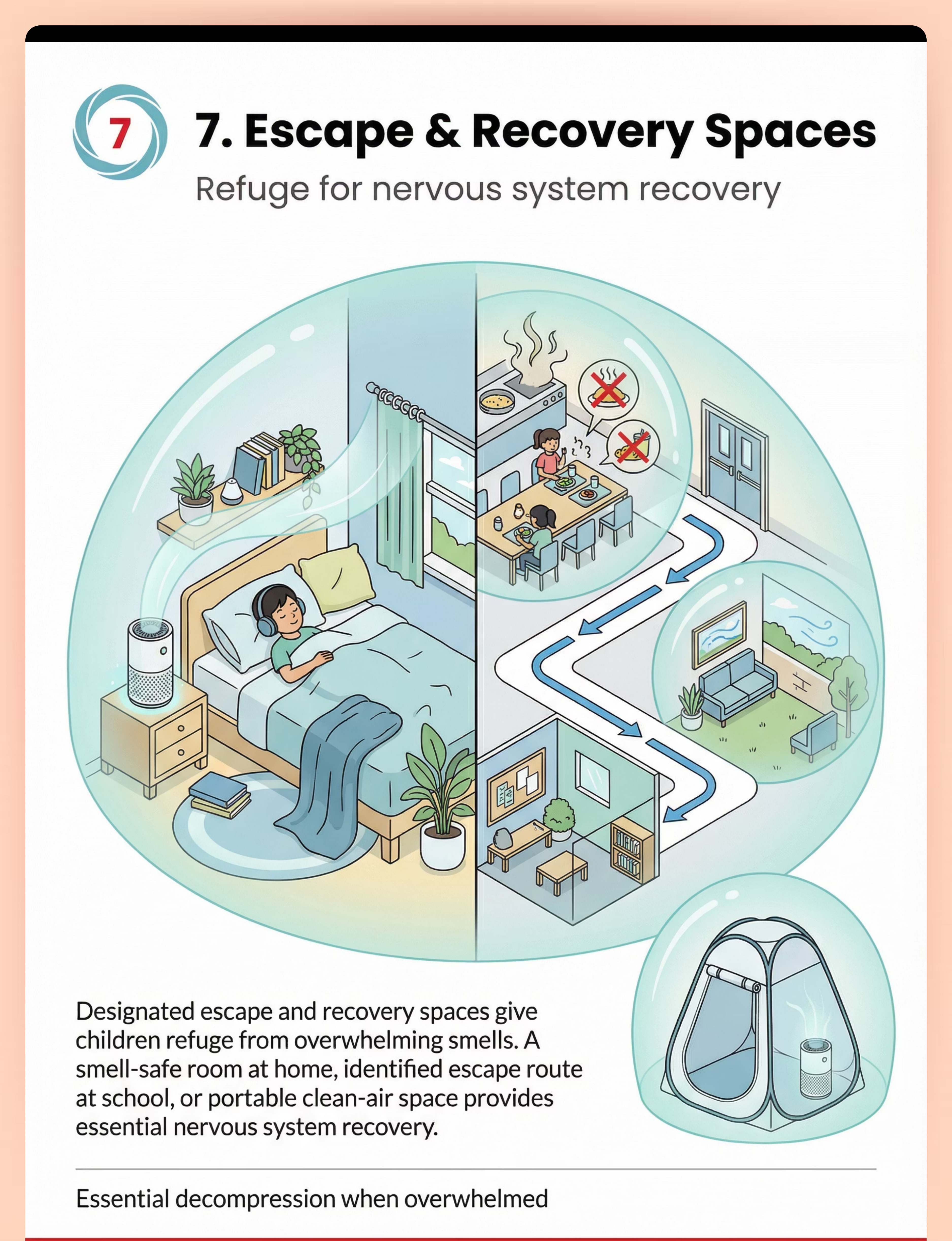
Escape & Recovery Kit
Portable clean-air space, air purifier, calming items
🏷️ Canon: Sensory Tent/Calm Space
💰 ₹500–3,000
🏷️ Canon: Sensory Tent/Calm Space
💰 ₹500–3,000
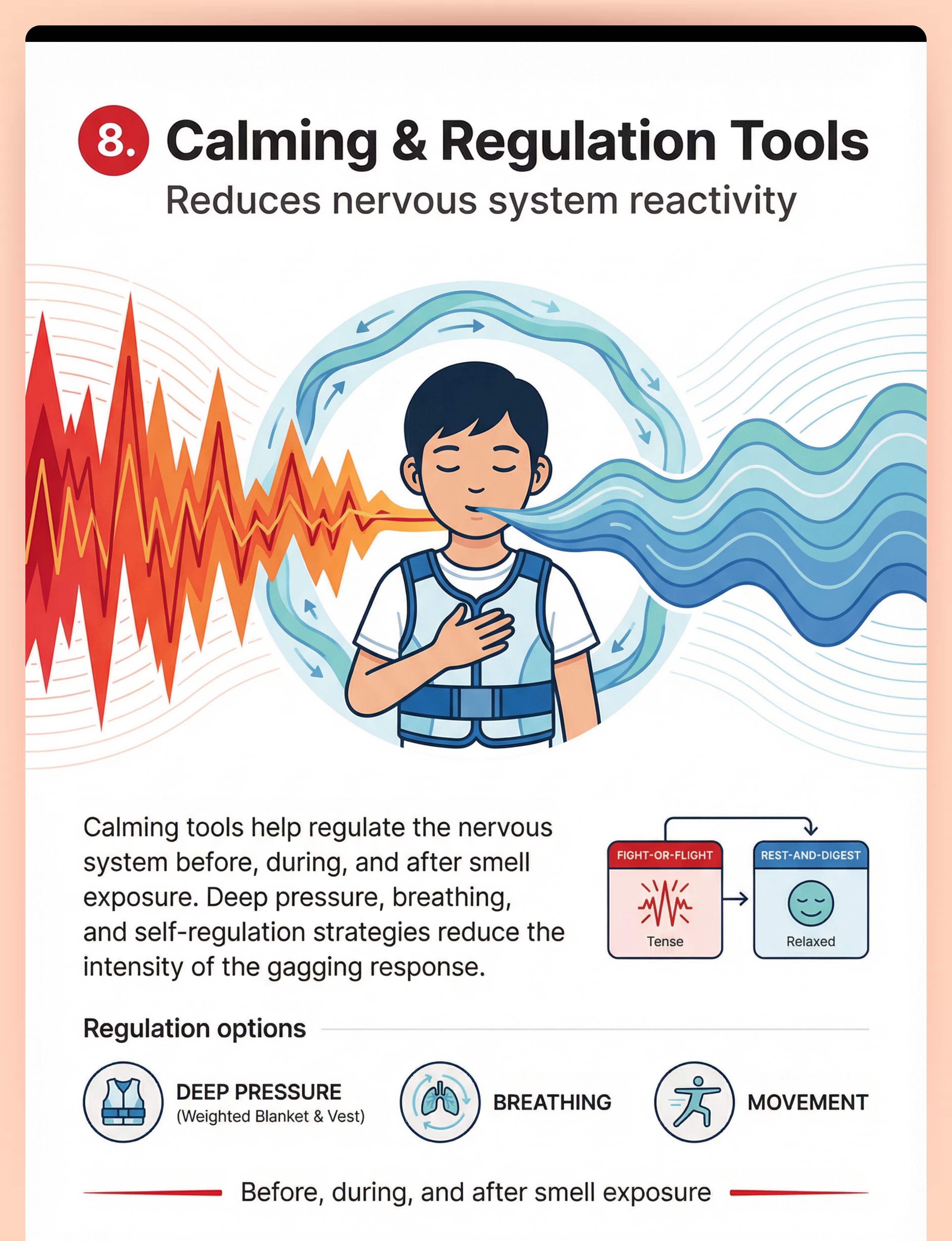
Calming & Regulation Tools
Weighted blanket/vest, breathing tools
🏷️ Canon: Deep Pressure + Breathing Tools
💰 ₹500–3,000
🏷️ Canon: Deep Pressure + Breathing Tools
💰 ₹500–3,000
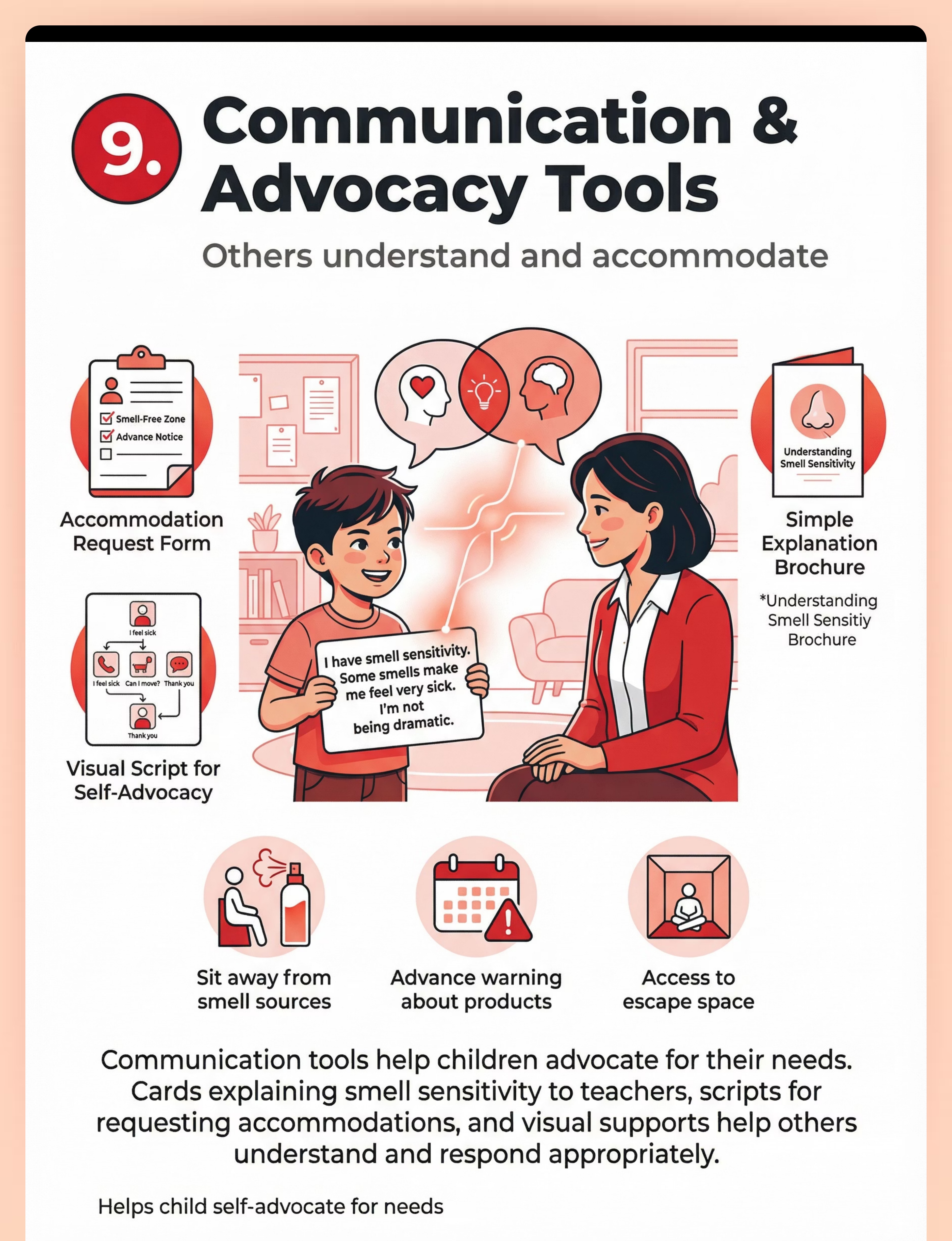
Communication & Advocacy Tools
Explanation cards, accommodation templates, self-advocacy scripts
🏷️ Canon: Communication Cards
💰 ₹100–300
🏷️ Canon: Communication Cards
💰 ₹100–300
💰 Total Investment Range
₹5,400–27,000 for comprehensive setup
💡 Essential Starters (Budget)
Personal Scent Shields + Air Purifier + Preferred Scent Tool + Escape Space = ₹4,000–20,000
DIY & Substitute Options — Start Today with What You Have
Not every family can order from Amazon. Not every town has same-day delivery. Every parent, regardless of economic status, can execute this technique TODAY with household items. This is equity in action.
Material | Buy This | Make This (₹0 Cost) | |
Scent Shield | Activated Charcoal Mask (₹300–1,500) | Layer a regular cloth mask with a charcoal insert from aquarium supplies. Dab child-approved essential oil on mask exterior. | |
Aromatherapy Bracelet | Lava Bead Bracelet (₹200–800) | One drop of preferred essential oil on a cotton ball in a small container, or corner of a handkerchief. Refresh daily. | |
Air Purifier | HEPA+Carbon Purifier (₹3,000–15,000) | Open windows for cross-ventilation. Use baking soda bowls in key rooms. Cook with exhaust fan on and kitchen door closed. | |
Fragrance-Free Products | Full product swap (₹200–800) | Audit products for fragrances. Start with items touching child's skin: unscented soap, rinse clothes twice, avoid fabric softener. | |
Desensitization Kit | Graded Scent Jars (₹500–2,000) | Work with OT. Create scent hierarchy: sealed container at distance → very diluted scent → gradual approach. Child controls pace. | |
Visual Schedule | Printed Schedule Cards (₹100–400) | Hand-draw a daily smell schedule on paper. Use clock symbols for cooking, cleaning, outings. Give 10-minute advance warning. | |
Escape Space | Pop-Up Tent Kit (₹500–3,000) | Designate child's bedroom as smell-safe sanctuary. Remove all scented products. Keep window crackable. Add calming items. | |
Calming Tools | Weighted Blanket (₹500–3,000) | Deep pressure: tight hugs, heavy blanket from home. Breathing: bubble breaths, counted exhales. Heavy work: wall pushes. | |
Communication Cards | Printed Card Set (₹100–300) | Write on an index card: "I have smell sensitivity. Some smells make me feel very sick. I may need to step away." |
Zero-Cost Protocol: A parent can begin today with: 1) A cotton ball with a preferred scent in a small container, 2) Advance verbal warnings before cooking/cleaning, 3) A designated escape room, 4) Deep breathing practice, 5) A handwritten explanation card. Cost: ₹0.
Research Evidence: WHO NCF (2018): Context-specific, equity-focused interventions. CCD Package implemented across 54 LMICs. 📎 References: PMC9978394 | WHO NCF Handbook (2022)

⚠️ Safety First — Before You Begin
🔴 RED — DO NOT PROCEED IF
- Child is experiencing active vomiting (not gagging) — seek medical evaluation
- Child has unexplained weight loss or failure to thrive
- Signs of dehydration from frequent vomiting episodes
- Smell sensitivity is of sudden new onset (may indicate neurological issue)
- Known GERD, cyclical vomiting, or GI condition not medically managed
- Child shows other new neurological symptoms alongside smell sensitivity
🟡 AMBER — PROCEED WITH MODIFICATION
- Significant anxiety component — pair with anxiety management first
- Tactile sensitivity to masks — trial mask wear during calm times first
- Child in a heightened anxiety state — use protection-only, no desensitization
- Some "unscented" products still have chemical smells — trial individually
- New materials may have their own smell — air out 24+ hours before use
🟢 GREEN — PROCEED WHEN
- Medical causes ruled out or being managed
- Child is in a regulated emotional state
- Parent has identified specific smell triggers and can describe intensity
- Materials pre-tested for child acceptability
- Escape route identified and accessible
- Child is not hungry, tired, or recently stressed
Material Safety Checklist
- Essential oils: Never apply undiluted to skin. Keep away from eyes. Some oils not safe for children under 6 — verify with pediatrician.
- Charcoal masks: Ensure proper fit and breathing space. Child should never feel restricted.
- Air purifiers: Choose ozone-free models. Some units produce motor sounds — consider auditory sensitivity.
- Desensitization: NEVER force exposure. Professional guidance essential. Some children sensitize (worsen) rather than desensitize — monitor carefully.
RED LINE: "Stop immediately if: gagging intensifies to repeated vomiting, child becomes severely distressed and cannot be calmed, child develops new physical symptoms, or child's food intake drops significantly. Trust your instincts — if something feels wrong, pause and ask."
Research Evidence: Indian Journal of Pediatrics RCT (2019). 📎 Reference: DOI: 10.1007/s12098-018-2747-4
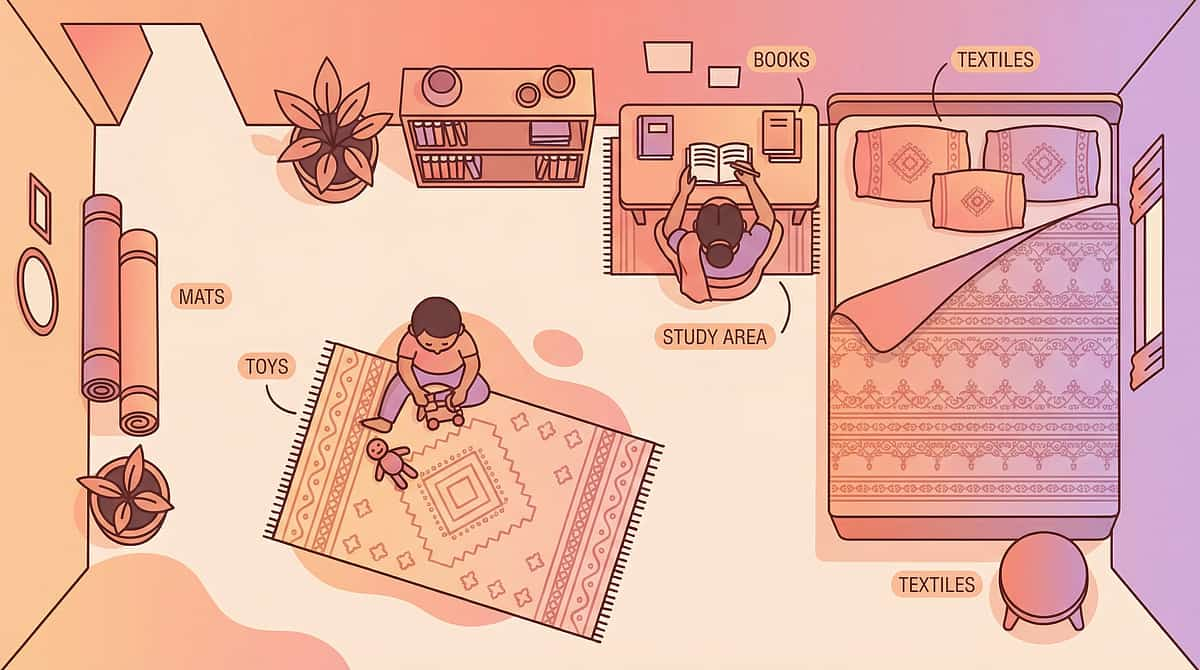
Set Up Your Space — The Smell-Safe Environment
The Smell-Safe Sanctuary (Bedroom)
Air Purifier
Position beside bed, running continuously. Choose HEPA + activated carbon model.
Remove All Scented Items
Check for: plug-in fresheners, scented candles, fragranced lotions, scented drawer liners, scented laundry detergent residue on bedding.
Preferred Scent Station
Small container with child's preferred scent tool, accessible by the child independently.
Calming Corner
Weighted blanket, deep pressure tools, breathing visuals within arm's reach.
Door Sign
"Smell-Safe Zone" — signals to all family members to not bring scented items in.
The Escape Route (Home-Wide)
Post a simple visual showing: "Kitchen is cooking → Go to bedroom" / "Cleaning happening → Go to bedroom" / "Feeling overwhelmed → Go to bedroom." Ensure the route is always clear — no obstacles between the child and the sanctuary.
The School Setup
- Provide a letter to the teacher explaining olfactory sensitivity
- Request seating away from cafeteria doors, cleaning supply storage, and bathrooms
- Establish standing permission to leave to a pre-identified clean-air space
- Provide the child's portable protection kit (mask, scent tool, communication card)
What to Remove from the Space
❌ Scented candles, plug-in fresheners, potpourri ❌ Fragranced cleaning products ❌ Strong personal care products ❌ New furniture/materials with off-gassing (air out before bringing into child's space)
Research Evidence: Sensory Integration Theory (Ayres): Environmental setup is a core principle. 📎 Reference: PMC10955541

ACT III: THE EXECUTION
Is Your Child Ready? — Pre-Session Checklist
✅ Child has eaten within the last 2 hours (empty stomach increases gagging sensitivity)
✅ Child has slept adequately (fatigue amplifies sensory reactivity)
✅ Child is in a calm/regulated state (not post-meltdown, not anxious)
✅ No recent distressing smell exposure (wait minimum 30 minutes after an episode)
✅ Child's preferred scent tool is ready and has been refreshed
✅ Escape route is clear and child knows how to access it
✅ Materials are prepared and within reach (not requiring parent to leave)
Decision Gate
1
ALL ✅ → GO
Begin the protocol
2
1–2 ❌ → MODIFY
Simplified, lower-demand version focusing on protection strategies only
3
3+ ❌ → POSTPONE
Do a calming activity instead. Try again when conditions improve.
If MODIFY: Focus only on protection (scent bracelet, mask availability) and escape readiness. Skip desensitization. Goal: maintain positive association with the tools.
If POSTPONE: Deep breathing together, preferred activity, time in smell-safe sanctuary. "The best session is one that starts right."
If POSTPONE: Deep breathing together, preferred activity, time in smell-safe sanctuary. "The best session is one that starts right."

Step 1 — The Invitation (30–60 seconds)

Parent Script (Say Exactly This)
"Hey [child's name], I have something cool. Remember your special smell bracelet? Would you like to wear it today? We can put your favorite smell on it."
Body Language Guidance
- Sit at child's level or slightly below
- Present the material casually — NOT as a "therapy tool"
- Use warm, playful tone — not clinical
- Hold the scent tool near you first, not thrusting it toward the child
- Smile. Relax your own body language.
What Acceptance vs. Resistance Looks Like
✅ Acceptance
- Child looks at the tool with interest
- Child reaches for or accepts the tool
- Child allows the scent to be applied
- Child puts on the bracelet or holds the scent tool
⚠️ Resistance — How to Modify
- Child turns away → Place tool nearby. "It's here whenever you want it."
- Child says no → "That's okay. It's yours whenever you're ready."
- Child shows distress → Abort this session. Move to calming strategy.
Timing: 30–60 seconds. If not accepted within 60 seconds, don't push. Place the tool within reach and move on.

Step 2 — The Engagement (1–3 minutes)
Parent Script
"Let's put one tiny drop of your favorite smell on the bracelet. You tell me if it's too much or just right."
How to Present the Material
- Add one drop of preferred essential oil to lava bead or fabric
- Hold it at arm's length first — let the child control the approach distance
- Wait for the child to lean in or bring it closer — never move the scent toward the child's face
- If the child sniffs and smiles: "You found your safe smell!"
Child Response Indicators
Engagement
Child sniffs, smiles, wants more, puts bracelet on → Continue
Tolerance
Child sniffs, neutral response, doesn't reject → Continue gently
Avoidance
Child pulls away, covers nose, shows discomfort → Pause, reduce intensity, offer choice to stop
Reinforcement Cue:"You found a smell you like! That's YOUR smell. You can use it anytime things feel too strong."
Research Evidence: Systematic review (Children, 2024): Sensory integration intervention with structured material introduction meets evidence-based practice criteria. 📎 Reference: PMC11506176
Step 3 — The Therapeutic Action (3–5 minutes)
This step practices the child's complete protection sequence in a controlled environment before they need it in the real world.
Parent Script for Each Step
Detect
"I'm going to open this container from far away. It has a very mild smell. You tell me when you can first notice it."
Decide
"On your smell scale — is this a 1 (barely notice), a 2 (notice but okay), or a 3 (too much)?"
Deploy
"What would you like to do? Use your bracelet? Put on your mask? Go to your room?"
Debrief
"You noticed the smell, you used your bracelet, and you stayed comfortable. That's exactly the plan."
Common Execution Errors
- ❌ Using the child's actual trigger smells — too early. Use neutral, mild scents first.
- ❌ Moving the scent closer without the child's permission
- ❌ Skipping the child's self-rating — the child must maintain control
- ❌ Extending the session past the child's tolerance window
Response Spectrum:Ideal: Child rates, chooses strategy, uses it successfully, reports feeling in control. Acceptable: Child participates but needs parent guidance at each step. Concerning: Child gags, becomes distressed, or refuses → Stop immediately. This is data, not failure.
Research Evidence: Meta-analysis (World J Clin Cases, 2024): 40-minute therapy sessions showed maximum effectiveness. Home sessions 10–20 min; core action occupies 40–60% of session time. 📎 Reference: PMC10955541
Step 4 — Repeat & Vary (3–5 minutes)
Target Repetitions: 2–4 cycles of the Detect → Decide → Deploy → Debrief sequence per session. 3 good repetitions > 10 forced ones.
Variation Options to Maintain Engagement
Change the Scent
Different neutral scent for each cycle
Change the Distance
Start farther, then slightly closer if child is comfortable
Change the Strategy
Cycle 1 uses bracelet, Cycle 2 tries mask, Cycle 3 uses breathing
Change the Setting
Move from bedroom to hallway to kitchen (no cooking happening)
Add Play
"Let's pretend you're a detective and your nose is your superpower!"
Satiation Indicators (When to Stop)
- Child says "I'm done" or equivalent
- Child's engagement drops noticeably
- Child starts to show signs of stress not present earlier
- Child has completed 3+ successful cycles — celebrate and end on success
The Golden Rule: "3 good reps > 10 forced reps." End when the child is successful, not when they're exhausted.

Step 5 — Reinforce & Celebrate (1–2 minutes)
Reinforcement Script (Within 3 Seconds of Completion)
"You are so brave! You detected the smell, you used your bracelet, and you stayed comfortable the whole time. That is exactly what a smell-shield champion does!"
Reinforcement Timing: Within 3 seconds of the desired behavior. Immediate, specific, enthusiastic.
Reinforcement Menu
🗣️ Verbal
Specific praise describing exactly what the child did well
⭐ Token
Add a star to the "Smell Shield" chart
🎮 Activity
5 minutes of preferred activity immediately after session
🤗 Physical
High-five, fist bump, or hug (if child-initiated)
Key Principle: "Celebrate the attempt, not just the success." If the child tried to use their strategy but still gagged — that attempt is still reinforced. The effort to engage with the protocol IS progress.
Research Evidence: ABA Reinforcement Principles: Immediate, specific reinforcement increases behavior occurrence. Token economy systems show strong evidence in autism intervention.

Step 6 — The Cool-Down (1–2 minutes)
Transition Warning Script
"One more practice, and then we're all done for today. You can choose what we do after."
Cool-Down Activity Options

🫧 Bubble Breathing
Slow, deep breaths visualized as blowing bubbles — 5 breaths

🧸 Preferred Scent Comfort
30 seconds with their preferred scent tool — "breathe in your good smell"
🏠 Sanctuary Time
2 minutes in the smell-safe space with preferred calming items

🤲 Deep Pressure
30-second bear hug, weighted blanket wrap, or compression
Material Put-Away Ritual
"Let's put your smell shield tools back in their special place so they're ready for next time." — Child participates in putting away materials if able.
Transition to Next Activity:"You're done! You practiced your smell shield today. What would you like to do now?"
If Child Resists Ending: The child wants to continue — this is a GOOD sign. "You love practicing! We can do more tomorrow. Right now your nose needs a rest."
Research Evidence: Visual timer and transition support: Visual supports classified as evidence-based practice for autism (NCAEP, 2020).

📊 Capture the Data — Right Now (60 Seconds)
Within 60 seconds of session end, record these 3 data points. This is not research — it is your child's progress story.
Data Point | How to Record | Example | |
Gagging Episodes Today | Tally count: How many gagging episodes during the practice session? | III (3 episodes) | |
Tolerance Duration | Time: How long did the child engage before showing stress? | 4 minutes 30 seconds | |
Strategy Used | Circle: Which strategy did the child prefer today? | Bracelet ✓ |
Optional Bonus Data
- Child's self-reported smell scale rating (1-3)
- New environments successfully entered today
- Notes: anything unusual or breakthrough moments
Tracking Options
📋 Printable PDF
Download printable PDF tracking sheet — A4, one page per week
📱 GPT-OS® In-App Tracker
Auto-graphs progress over time. Launch GPT-OS® Tracker →
📓 Notebook
Simple tally marks in a notebook work perfectly
"60 seconds of data now saves hours of guessing later. Your observations are the raw material from which progress becomes visible."
Research Evidence: ABA Data Collection Standards: Continuous measurement (frequency, duration, latency) as standard practice. 📎 Reference: Cooper, Heron & Heward (Applied Behavior Analysis)

What If It Didn't Go as Planned?
Most sessions don't go perfectly. That's not failure — that's data.
❓ "My child refused to try the scent tool at all"
Not uncommon in the first 1–3 sessions. Place the tool near them during a preferred activity. Let familiarity build. Try again in 24 hours. Don't discuss it as "therapy" — just leave it available.
❓ "The preferred scent made my child gag too"
The scent may be too strong. Dilute significantly. Or the scent wasn't genuinely preferred — trial different options during calm moments. Some children are too sensitive for ANY added scent — use mask-only strategy.
❓ "My child panicked when I introduced the practice smell"
The practice smell was too strong or too close. Next session: start with just a picture of the smell source (visual only, no actual smell). Build from there. This is not a setback — your child's nervous system is telling you the starting point.
❓ "My child used the strategy but still gagged"
The strategy reduced the response even if it didn't eliminate it. Was the gagging less intense? Shorter? That IS progress. Continue with the same level — don't increase difficulty yet.
❓ "We couldn't find a scent my child tolerates"
Focus on blocking strategies (charcoal mask, nasal filters) and environmental modification (air purifier, unscented products) rather than scent-based approaches. Not every child benefits from preferred scent tools.
❓ "My child had a meltdown after the session"
The session was too long, too intense, or started when the child wasn't ready. Next session: shorter, lower demand, preceded by a regulation activity. If meltdowns continue after 3 modified attempts, consult your OT.
❓ "Other family members won't cooperate"
Start with the child's immediate environment only (their bedroom, their clothes, their soap). Provide the "Understanding Smell Sensitivity" card to family members. Progress to household-wide changes gradually.
"Session abandonment is not failure — it's data. Your child just told you exactly where their threshold is. That information is valuable."

Adapt & Personalize — No Two Children Are Identical
EASIER Version (High-Sensitivity Days)
Protection only — no desensitization. Child wears preferred scent tool passively during preferred activities. No new environments. Focus on comfort and safety. Session: 2–3 minutes.
STANDARD Version (Regulated Days)
Full Detect → Decide → Deploy → Debrief cycle. 2–4 repetitions with mild neutral scents. Practice in familiar environment. Session: 10–15 minutes.
HARDER Version (Breakthrough Days)
Slightly stronger scent or closer distance. Mildly challenging environment. Add generalization in a non-home setting. Session: 15–20 minutes.
Age-Based Modifications
Aspect | Ages 3–5 | Ages 6–9 | Ages 10–14 | |
Approach | Playful, game-based | Story-based, detective theme | Self-management, independence | |
Tool Access | Parent controls all tools | Child begins to self-select | Child manages own protection kit | |
Session Length | 2–3 minutes | 5–10 minutes | 10–20 minutes | |
Tracking | Visual cue cards | Written self-rating scales | Digital self-monitoring |
Sensory Profile Variations
Sensory Avoider (Most Common)
Go slower, prioritize protection and escape over desensitization. May never fully desensitize — management is a valid goal.
Mixed Profile (Seeking + Avoiding)
Child may seek some smells while gagging at others. Map specific trigger smells vs. safe smells to build an accurate sensory diet.

ACT IV: THE PROGRESS ARC
Week 1–2: What to Expect
15%
Progress Bar
Early-stage — building foundations
Observable Indicators
- Child tolerates the preferred scent tool being present (not necessarily using it)
- Child begins to accept wearing or holding the scent bracelet during calm moments
- Environmental modifications show impact: child appears calmer in purified bedroom
- Gagging episodes may not decrease yet — this is normal at this stage
- Child may show curiosity about the protection tools
What Progress Looks Like
"If your child allows the aromatherapy bracelet to be placed on the table near them without removing it — that is real progress. If your child sniffs the preferred scent once without pulling away — that is real progress."
What Is NOT Progress Yet (Managing Expectations)
- Gagging elimination — far too early
- Entering the cafeteria comfortably — not yet
- Independent strategy use — still learning
Parent Emotional Preparation: This stage feels like nothing is happening. It is. Neural pathways are forming beneath visible behavior. Your consistency IS the intervention.
Research Evidence: Systematic review (Children, 2024): Early-phase indicators focus on tolerance and participation rather than skill mastery. 📎 Reference: PMC11506176

Week 3–4: Consolidation Signs
40%
Progress Bar
Building momentum — consolidation phase
Consolidation Indicators
Self-Initiation
Child reaches for the scent tool before entering challenging environments
Self-Rating
Child reports smell intensity using the rating scale without prompting
Measurable Decrease
Gagging episodes show measurable decrease in frequency or intensity
Effective Escape
Child uses escape protocol — goes to sanctuary, recovers, and returns
Communication
Child may spontaneously communicate about smells ("that smells strong to me")
Behavioral Changes Signaling Neural Pathway Formation
- Anticipatory behavior: child prepares before entering challenging spaces
- Self-regulation attempt: child takes deep breaths when smelling something strong
- Spontaneous generalization: child uses the strategy in settings where it wasn't specifically practiced
When to Increase: If the child consistently uses protection strategies successfully for 5+ consecutive sessions → consider introducing mildly challenging environments with full protection toolkit available.
"You may notice you're more confident too. You've gone from 'I don't know what to do' to 'I have a plan.' That confidence is contagious — your child feels it."
Week 5–8: Mastery Indicators
75%
Progress Bar
Approaching mastery — skills consolidating
🏅 Mastery Badge: Smell Shield Champion
Mastery Criteria (Specific, Observable, Measurable)
- Child independently selects and uses preferred protection strategy before entering challenging environments
- Gagging episodes reduced by 50%+ from baseline in at least 2 settings
- Child can remain in previously avoided environments for functional durations (complete a meal, attend a class period, participate in a family outing)
- Child can communicate their needs to unfamiliar adults using their advocacy tools
- Child demonstrates recovery — when overwhelmed, uses escape → regulation → return sequence
Generalization Indicators
- Strategy use appearing in settings where it was NOT specifically practiced (friend's house, restaurant, car)
- Child adapts the strategy independently (chooses mask for strong smells, bracelet for mild smells)
- Child begins to distinguish between "uncomfortable but manageable" and "I need to leave" — nuanced self-awareness
Maintenance Check
- Reduce structured practice sessions to 1x per week
- Monitor: do strategies persist without the structured protocol? If yes → maintenance achieved
- If strategies fade without practice → return to 2–3x per week and reassess
Research Evidence: Meta-analysis (2024): Sensory integration therapy across 24 studies showed effective promotion of skills. 📎 References: PMC10955541 | BACB mastery criteria standards
🎉 Celebrate This Win
"5–8 weeks ago, your child could not walk into the school cafeteria. Today, they carry their smell shield kit, know how to use it, and participate in spaces that were previously impossible. You made that happen."
Parent Affirmation
"You did this. Your child grew because of your commitment. Every time you refreshed that bracelet scent, every time you gave the 10-minute advance warning, every time you drove to the store for fragrance-free products — that was therapy. That was love in action."
Family Celebration Suggestion
Choose a new environment to visit together — with the full protection toolkit. A restaurant the family hasn't been to. A park with food vendors. A relative's house during cooking time. Celebrate by USING the skills in real life.
📸 Photo/Journal Prompt: Document this milestone. Take a photo of your child in a space they couldn't enter 8 weeks ago. Write the date. This is evidence of what's possible.
Research Evidence: Parental self-efficacy research: Parent confidence is the strongest predictor of continued home-based intervention implementation.
🚨 Red Flags — When to Pause
🔴 STOP — Seek Medical Evaluation
- Weight loss or failure to thrive from food avoidance
- Dehydration from frequent vomiting episodes
- New onset of smell sensitivity not present before
- Smell sensitivity combined with new neurological symptoms (headaches, vision changes, balance issues)
🔴 STOP — Consult Your OT/BCBA
- Complete school avoidance developing or worsening
- Severe social isolation — child withdrawing from all social contact
- Desensitization making things worse — gagging increasing
- Anxiety escalating — new fears or avoidance beyond smell
- Overall functioning declining despite intervention
🟡 PAUSE — Reassess
- No measurable progress after 4 weeks of consistent implementation
- Child becoming resistant to the protocol or materials
- Family stress increasing rather than decreasing
- Other sensory challenges emerging or worsening
Escalation Pathway
1
Self-Resolve
2
Teleconsultation
FREE: 9100 181 181
3
Clinic Visit
4
Specialist Referral
"Trust your instincts — if something feels wrong, pause and ask. You know your child better than any protocol does."

The Progression Pathway — Your Developmental GPS
Related Techniques in the Journey
A-6: Oral Sensory Seeking
A-20: Smell Sensory Seeking
A-47: Gagging Around Food Textures
A-84: Food Texture Acceptance
A-115: Emotion Body Awareness

Related Techniques in Sensory Processing
Technique | Difficulty | Materials Overlap | Key Focus | |
A-6: Oral Sensory Seeking | Core | Aromatherapy Kit, Oral Motor Tools | Oral sensory input needs | |
A-20: Smell Sensory Seeking | Intro | Aromatherapy Kit, Scent Jars | Smell-seeking behaviors | |
A-47: Gagging/Vomiting Around Food Textures | Advanced | Feeding Tools, Desensitization Kit | Texture-based gagging | |
A-84: Food Texture Acceptance Materials | Core | Feeding Tools, Visual Supports | Expanding food repertoire | |
A-115: Emotion Body Awareness | Core | Emotion Cards, Body Maps | Interoceptive awareness | |
A-117: Next Sensory Topic | Core | Coming Soon | Upcoming technique |
"You Already Own Materials for These": If you have the aromatherapy kit, preferred scent tools, visual schedules, and communication cards from this technique — you already have core materials for A-6, A-20, and A-84. Your investment extends across multiple interventions.

Your Child's Full Developmental Map
The 12 Developmental Domains
A. Sensory Processing ★
CURRENT
B. Motor
C. Communication
D. Social Skills
E. Behavioral Regulation
F. Cognitive
G. Adaptive Living
H. Academic Readiness
I. Emotional Regulation
J. Play & Leisure
K. Family & Community
L. Transition Planning
This Technique's Position:"You are working in Domain A: Sensory Processing, specifically addressing Olfactory Over-Responsivity. This feeds directly into Domain G (Adaptive Living), Domain D (Social Skills — participation in social environments), and Domain K (Family & Community — family outings and activities)."
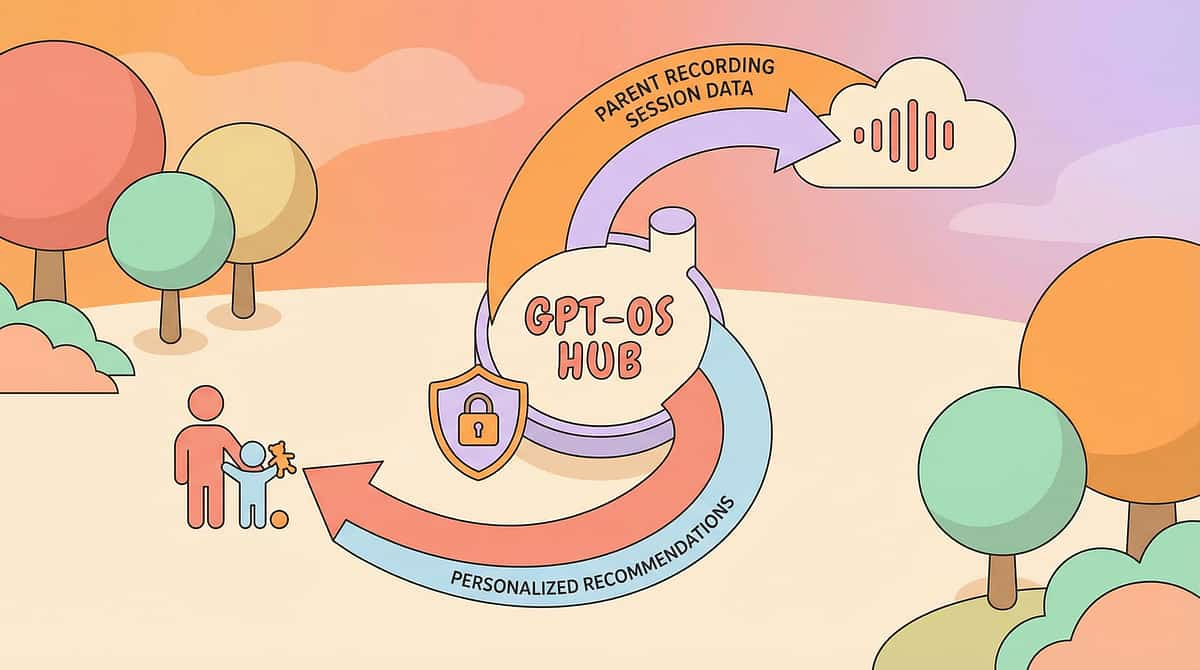
GPT-OS® Integration:"Your data from this technique feeds into GPT-OS® to personalize recommendations across all 12 domains. The more you practice and track, the more precise your child's developmental pathway becomes."
Research Evidence: WHO/UNICEF Nurturing Care Framework: Five components of nurturing care require holistic developmental monitoring. 📎 References: WHO NCF (2018) | UNICEF 2025 Country Profiles

ACT V: THE COMMUNITY & ECOSYSTEM
Families Who've Been Here
Rohan's Story — Age 7
Before: Gagged every time the family cooked dinner. Ate all meals alone in his room. School cafeteria completely avoided — he ate a packed lunch in the hallway.
After (12 weeks): Now wears his charcoal mask in the cafeteria and eats with two friends. At home, uses his scent bracelet during cooking and sits at the dinner table for 15 minutes. Last week, the family went to a restaurant for the first time in two years.
"He used to gag the moment we entered any restaurant. Now with his mask and breathing routine, we can actually eat out as a family again." — Parent, Pinnacle Network
Aisha's Story — Age 5
Before: Would vomit from the smell of cleaning products. Mother couldn't clean the house during waking hours. The bathroom was a daily battle.
After (8 weeks): Complete fragrance-free product transition at home. Gagging reduced by 70%. She now uses her "breathe bear" when she encounters strong smells outside. She told her teacher, "Smells make me sick. Can I sit by the window?"
Note: Illustrative cases; outcomes vary by child profile.
From the Therapist's Notes: "Olfactory hypersensitivity with gagging is among the most impactful but also among the most responsive sensory challenges when families commit to environmental modification. The protection-first approach — making the world safe for the child rather than demanding the child tolerate an unsafe world — is the breakthrough most families need."

Connect with Other Parents
You Are Not a Solo Operator.
🟢 Sensory Processing Parent WhatsApp Group
Connect with parents navigating the same olfactory sensitivity challenges. Share tips, ask questions, celebrate wins. Join Sensory Processing Parent Group →
🟢 Pinnacle Parent Community Forum
Online discussions, resource sharing, and peer support across all 12 developmental domains. Visit Community Forum →
🟢 Local Pinnacle Parent Meetups
Monthly gatherings at your nearest Pinnacle center. Connect face-to-face with families who understand. Find Local Meetups →

🟢 Peer Mentoring
Connect with a parent who's been through this journey and is now supporting others. Request a Peer Mentor →
"Your experience helps others — consider sharing your journey."
Your Professional Support Team
Find Your Nearest Center
70+ centers across India. Center Locator →
Therapist Matching
OT with Sensory Processing specialization matched to your child's profile. Match Me →
Teleconsultation
Video consultation with sensory specialist. 16+ languages. Book Now →
FREE Helpline
📞9100 181 181 — 24/7, 16+ languages. Ask any developmental question.
"Home + clinic = maximum impact. Professional guidance accelerates what families build at home."
Research Evidence: WHO NCF Progress Report (2023): Primary health care identified as key platform for reaching all families with essential ECD interventions.

The Research Library — For the Curious Parent
📄 PRISMA Systematic Review (2024)
"16 articles from 2013–2023 confirm sensory integration intervention meets criteria for evidence-based practice in ASD." Read on PubMed: PMC11506176
📄 Meta-Analysis — SI Therapy (2024)
"Across 24 studies, sensory integration therapy effectively promoted social skills, adaptive behavior, sensory processing, and motor skills." Read on PubMed: PMC10955541
📄 WHO CCD Package (2023)
"Home-based, caregiver-administered interventions demonstrated efficacy across 54 low- and middle-income countries." Read on PubMed: PMC9978394
📄 Indian RCT — Padmanabha et al. (2019)
"Parent-administered sensory protocols showed significant outcomes in Indian pediatric populations." Read: DOI 10.1007/s12098-018-2747-4
📄 NCAEP Evidence Report (2020)
"Sensory integration, visual supports, self-management, and environmental modification classified as evidence-based practices for autism." Read NCAEP Report
Additional Sources
- WHO Nurturing Care Framework (2018): nurturing-care.org/ncf-for-ecd
- SPD Foundation & STAR Institute Research: spdstar.org
- Ben-Sasson A, et al. (2009): Meta-analysis of sensory modulation symptoms in ASD
- Miller LJ, et al. (2007): Concept evolution in sensory integration — proposed nosology
- Tavassoli T, et al. (2014): Sensory over-responsivity in adults with ASD

How GPT-OS® Uses Your Data
What GPT-OS® Learns from THIS Technique's Data
- Which protection strategies work best for YOUR child's specific trigger profile
- Optimal session timing and duration based on your child's response patterns
- When to progress, when to maintain, and when to modify
- Cross-domain insights: how olfactory tolerance improvement affects feeding, social participation, and school attendance
🔒 Privacy & Data Protection: Your child's data is encrypted, anonymized for research purposes, and never shared with third parties without consent. Pinnacle adheres to Indian data protection laws and international best practices.
"Your data helps every child like yours. When 70+ centers and thousands of families contribute session data, GPT-OS® improves recommendations for all families navigating olfactory sensitivity."
Research Evidence: Digital health interventions for ASD: 21 RCTs with 1,050 participants demonstrate promise for gamified digital health interventions.

🎬 Watch the Reel — A-116
Reel Title
9 Materials That Help When Child Gags at Smells
Series
Sensory Solutions Series — Episode 116
Domain
Sensory Processing | Olfactory Over-Responsivity
Duration
75 seconds
What You'll See: A Pinnacle therapist walks you through all 9 materials in 75 seconds — showing each material being used by a child in a real-world setting. Visual demonstration reinforces everything you've read on this page.
Multi-Modal Learning:"You've read it. Now watch it. Video modeling is classified as an evidence-based practice for autism (NCAEP, 2020). Seeing a therapist demonstrate these materials increases your confidence in executing them at home."

Share This With Your Family
If only one parent knows this technique, it's limited. Consistency across caregivers multiplies impact.
"Explain to Grandparents" — Simplified Version
"[Child's name] has a condition called olfactory hypersensitivity. Their brain processes smells much more intensely than ours. When they gag, it's not drama — it's their nervous system reacting to what it perceives as a dangerous smell. Here's how you can help: 1) Use unscented products around them, 2) Give them advance warning before strong smells, 3) Let them use their 'smell shield' tools, 4) Let them leave a room if they need to — no questions asked."
Teacher/School Communication Template
📄 Download School Accommodation Letter (PDF) — Contains: explanation of olfactory sensitivity, specific accommodations requested, emergency protocol, and Pinnacle clinical contact for teacher questions.
Research Evidence: WHO CCD Package: Multi-caregiver training critical for intervention generalization and maintenance. 📎 Reference: PMC9978394

ACT VI: THE CLOSE & LOOP
Frequently Asked Questions
Q1: Is my child's gagging at smells related to autism?
Olfactory hypersensitivity occurs in 40–70% of autistic children, but it can also occur in children without autism who have sensory processing differences. A comprehensive sensory processing evaluation by an OT can determine the underlying pattern. Either way, these protection strategies are effective.
Q2: Will my child ever "grow out of" smell sensitivity?
Some children's olfactory sensitivity decreases naturally with neural maturation. Others maintain sensitivity but develop effective management strategies. The goal is functional tolerance — the ability to participate in daily life — not necessarily elimination of sensitivity.
Q3: Should I avoid all smells to protect my child?
Total avoidance is neither possible nor therapeutic. The strategy is layered: 1) Eliminate unnecessary triggers (fragrance-free products), 2) Protect against unavoidable triggers (masks, preferred scents), 3) Prepare for expected exposures (predictability tools), 4) Support gradual tolerance building when appropriate.
Q4: Is smell desensitization safe to do at home?
Basic protection strategies (masks, preferred scents, environmental modification) are safe for home implementation. Formal desensitization — systematic, graded exposure — should be guided by a qualified OT. Some children sensitize (worsen) rather than desensitize, and professional monitoring prevents this.
Q5: My child's school says he's "being dramatic." How do I advocate?
Use the School Accommodation Letter template. Request a meeting with the school SENCO or counselor. Provide clinical documentation. Key message: "This is a neurological difference documented by licensed professionals, not a behavioral choice."
Q6: How much does the full setup cost?
Comprehensive: ₹5,400–27,000. Essential starters: ₹4,000–20,000. Zero-cost start (DIY): ₹0. Every budget level has a pathway. See Card 10 for DIY substitutes.
Q7: Can these strategies work for adults?
Yes. Protection and environmental modification strategies are age-agnostic. Adults benefit from charcoal masks, preferred scent tools, fragrance-free environments, and self-advocacy. Desensitization protocols may differ.
Q8: How is this different from clinic sessions?
Clinic sessions focus on controlled therapeutic exposure and skill-building. Home implementation focuses on daily protection, environmental modification, and generalization. They are complementary — the EverydayTherapyProgramme™ bridges clinic to home.
Didn't Find Your Answer?

Your Next Step — Start Now
🟢 START THIS TECHNIQUE TODAY
Launch a GPT-OS® guided session. Follow the protocol step by step with real-time guidance and automatic data tracking.
🔵 BOOK A SENSORY OT ASSESSMENT
Get your child's complete sensory processing profile assessed by a licensed OT. Available at 70+ centers or via teleconsultation.
📞FREE Helpline: 9100 181 181 (24/7, 16+ languages)
⚪ EXPLORE NEXT TECHNIQUE → A-117
Continue your child's sensory processing journey with the next recommended technique based on the progression pathway.
🏛️ Validated by the Pinnacle Blooms Consortium
OT • SLP • ABA • SpEd • NeuroDev Pediatrics
Evidence-Based
WHO/UNICEF-Aligned
Preview of 9 materials that help when child gags at smells Therapy Material
Below is a visual preview of 9 materials that help when child gags at smells therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.





Link copied!

The Pinnacle Promise
"From fear to mastery. One technique at a time."
Medical Disclaimer: This content is educational and does not replace assessment by a licensed occupational therapist, pediatrician, or sensory specialist. Individual results may vary. Statistics represent aggregate outcomes across the Pinnacle Blooms Network. Olfactory sensitivity with gagging may have multiple causes including sensory processing differences, anxiety, GI conditions, and other medical factors. Severe gagging with vomiting, weight loss, or dehydration requires immediate medical evaluation. Desensitization approaches require professional guidance. Please consult with qualified healthcare professionals before implementing any strategies.
Copyright & Attribution: © 2025 Pinnacle Blooms Network®, a unit of Bharath Healthcare Laboratories Pvt. Ltd. All rights reserved. CIN: U74999TG2016PTC113063 | DPIIT: DIPP8651 (Govt. of India) | MSME: TS20F0009606 | GSTIN: 36AAGCB9722P1Z2
Powered by GPT-OS® — Global Pediatric Therapeutic Operating System
Patent-protected across 160+ countries | 20M+ exclusive 1:1 therapy sessions | 97%+ measured improvement
Patent-protected across 160+ countries | 20M+ exclusive 1:1 therapy sessions | 97%+ measured improvement
Site: techniques.pinnacleblooms.org | pinnacleblooms.org | 📞 9100 181 181