
ACT I — THE EMOTIONAL ENTRY
You Are Not Failing. Your Child's Nervous System Needs a Translator.
It is 8:47 AM. School starts in 13 minutes. You ask for the fourth time: "Do you need to use the bathroom?" She shakes her head — firm, certain. You believe her. You gather bags, lace shoes, reach the door. And then it happens. Again.
You are not failing. Your child's nervous system is speaking a language that needs a translator. Technique A-112 — Bathroom Signal Recognition is that translator. This page is your complete, evidence-based, parent-ready guide — produced by Pinnacle Blooms Network®, India's largest multi-disciplinary pediatric therapy consortium.
🏛️ Pinnacle Blooms Consortium
70+ centers across India. 21M+ therapy sessions delivered.
🔬 OT-Led Protocol
Designed and validated by Occupational Therapists specializing in sensory integration.
⏱️ 8-Week Protocol
Structured, measurable, home-applicable. Results tracked across every session.
🌍 WHO/UNICEF Aligned
Built on the Nurturing Care Framework. Equity-first design — ₹0 DIY options for every material.

You Are Among Millions of Families Navigating This Exact Challenge
Bathrooming difficulties are the single most commonly cited daily-living challenge by families of children with autism in India. Occupational therapists at Pinnacle's 70+ centers record toilet-related independence as a goal on 68% of all initial treatment plans. This is not a rare problem. This is not your parenting failure. This is a documented neurological difference affecting millions of children globally — and there is a clear, evidence-based intervention pathway.
80% — Interoceptive Differences
Of children with ASD experience interoceptive processing differences affecting self-care, per PRISMA Systematic Review (2024).
1 in 36 — Autism Diagnoses in India
Children in India are diagnosed with autism spectrum disorder, making this one of the country's most significant pediatric health priorities.
21M+ — Therapy Sessions
Delivered by Pinnacle Blooms Network® — this challenge addressed at every center, every day.
According to Padmanabha et al. (Indian Journal of Pediatrics, 2019), home-based structured sensory interventions show significant measurable outcomes in Indian pediatric populations. DOI: 10.1007/s12098-018-2747-4

The Eighth Sensory System: When the Body's Internal Radio Goes Silent
Beyond our five familiar senses, and even beyond balance and body awareness, lies a critical "eighth" sense: interoception. This is your child's internal radio, designed to broadcast vital status updates from within—signaling when they are hungry, thirsty, need to use the bathroom, or are feeling a racing heartbeat. For many children on the autism spectrum, these internal signals are muted, delayed, or lost in static, much like a radio with poor reception. This is why your child may genuinely not feel the urge to use the bathroom until it is already too late.
Bladder Fullness
The signal that says 'I need to urinate.' In children with ASD, this signal often arrives late, weakly, or sometimes not at all, making it difficult to initiate a trip to the restroom.
Bowel Pressure
The internal awareness required to recognize the need for a bowel movement. Because of delayed processing, the window between initial awareness and an urgent need often collapses.
Urgency Timing
The critical gap between the first signal and the moment of necessity. While neurotypical children may have several minutes, children with interoceptive differences may have only seconds to react.
Clinical Insight: Clinical evidence confirms interoceptive processing differences in 80% of children with ASD (PRISMA Systematic Review, 2024). This is not a behavioral problem. This is a neurological difference — and it is addressable with the right intervention.
Your Child's Development Timeline — And Where Bathroom Awareness Sits
WHO developmental milestones indicate that daytime bladder control is typically established by ages 2–3 and nighttime control by ages 4–5. When a child of 6, 8, or 10 years continues to experience accidents, it is not a developmental delay — it is an interoceptive access barrier. Your child is at the milestone marker. The capacity exists. The sensory pathway to access it needs deliberate construction.
18–24 Months
Bladder awareness emerging
2–3 Years
Daytime control achieved
3–4 Years
Nighttime control developing
4–5 Years
Full independence expected
5–12 Years
⚠️ Challenge Zone: A-112 Intervention
Common Co-Occurrences
Hunger signal recognition difficulties (→ Technique A-111)
General interoceptive awareness differences (→ Technique A-115)
Sensory processing differences in tactile and proprioceptive domains
Anxiety related to bathroom environments (separate from interoceptive deficit)
Constipation secondary to not sensing bowel fullness
📍 Current: External cue dependency → 🎯 Goal: Independent signal recognition

Clinically Validated. Home-Applicable. Parent-Proven.
Every material and strategy in Technique A-112 rests on a foundation of peer-reviewed, multi-study evidence. This is not anecdotal guidance — it is clinical-grade intervention translated for home use. The research confidence level is 82% (strong, multi-study consensus).
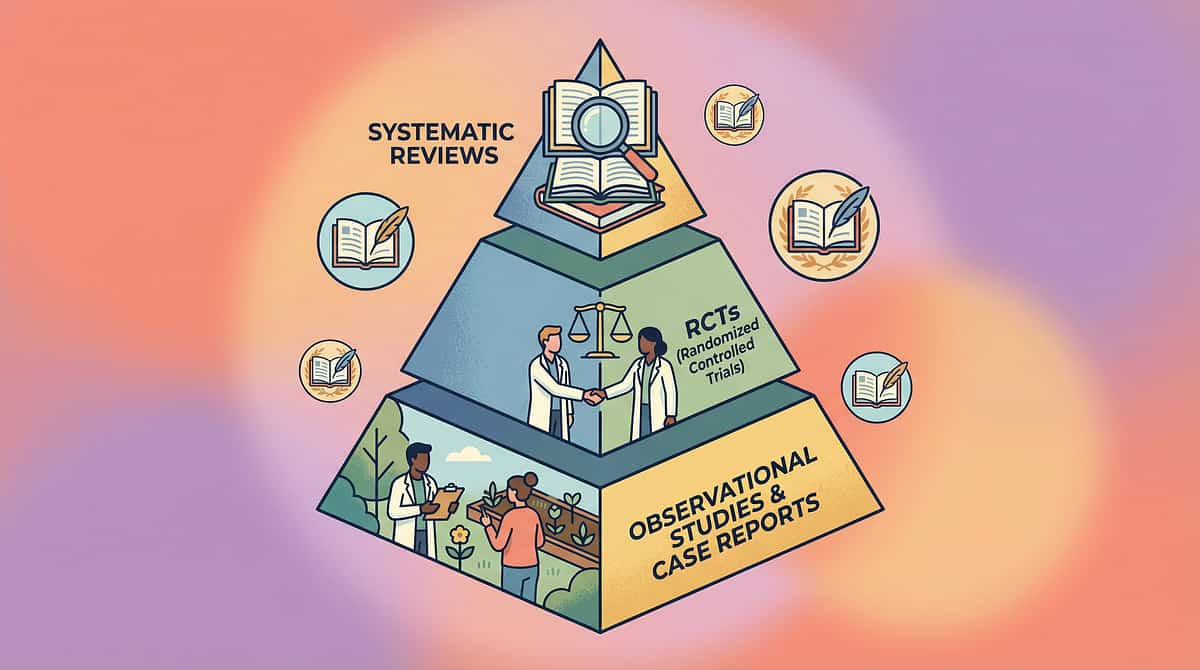
🛡️ Evidence Grade: Level II
Systematic Review + RCT. Consensus: Evidence-Based Practice for ASD (NCAEP 2020).
📄 PRISMA Review (2024)
16 studies (2013–2023) confirm interoception-based SI intervention as evidence-based practice for ASD. PMC11506176
📄 Meta-Analysis (2024)
SI therapy promotes adaptive behavior and self-care skills across 24 studies. PMC10955541
📄 Indian RCT (2019)
Home-based sensory interventions show significant outcomes in Indian pediatric populations. DOI:10.1007/s12098-018-2747-4
In 21 million+ therapy sessions across Pinnacle's 70+ centers, bathroom signal recognition is tracked through the Daily Living & Independence Index within GPT-OS®. Children receiving structured interoception intervention show measurable progression across all five independence stages within 8–12 weeks.

ACT II — KNOWLEDGE TRANSFER
Bathroom Signal Recognition — What It Is
Technique A-112
INT-TOIL
Age 3–12
Bathroom Signal Recognition is a structured interoceptive awareness intervention that systematically teaches children to notice, identify, and respond to internal bladder and bowel signals. Using visual supports, scheduled check-ins, sensory awareness activities, and environmental modifications, children learn to build the neural pathway between physiological fullness and conscious awareness — progressively shifting from external schedule dependence to independent signal recognition.
Protocol Details
- 📂 Domain: Interoception & Self-Care Independence (INT-TOIL)
- 👶 Age Range: 3–12 years
- ⏱️ Session Duration: 5–15 minutes per session
- 📅 Frequency: 6–8 scheduled daily check-ins + dedicated practice
- 📆 Protocol Duration: 8–12 weeks (full independence timeline)
- 🌍 Setting: Home, School, Clinic
Key Principle
"This is not toilet training. This is interoceptive education. The child already has the physiological capacity. We are building the awareness pathway to access it."
— Pinnacle Blooms OT Consortium
Parent-friendly alias: "Teaching the Body's Bathroom Radio"
The Pinnacle Consortium Deploys This Across 5 Disciplines
Bathroom signal recognition is not solely an occupational therapy challenge. Because the bladder doesn't organize itself by therapy type, the brain needs interoceptive input, reinforcement, language, and environmental scaffolding simultaneously. Pinnacle's multi-disciplinary consortium brings five specialist disciplines together for this technique.
🔵 Occupational Therapist (Primary Lead)
Designs and supervises the interoception curriculum. Assesses sensory profile, creates fullness scale systems, environmental modifications, and body mapping protocols. Delivers scheduled bathroom check-in training to parents.
🟢 ABA/BCBA Therapist
Structures the reinforcement system for successful bathroom initiations. Designs data collection protocols. Implements differential reinforcement for independent initiations vs. prompted visits. Manages antecedent schedules.
🟡 Special Education Teacher
Implements visual bathroom schedule at school. Coordinates with parents for consistency across settings. Manages classroom schedule supports and discreet watch/timer systems. Ensures dignity and peer-privacy protection.
🟣 NeuroDev Pediatrician
Rules out medical causes (UTI, constipation, structural factors). Monitors for enuresis/encopresis requiring medical management. Provides medical clearance before behavioral/sensory intervention begins.
🔴 Speech-Language Pathologist
Develops communication vocabulary for bathroom signaling (verbal, AAC, PECS). Creates social stories for bathroom awareness. Ensures child has expressive pathway to communicate bathroom need.
Precision Targeting: What A-112 Actually Changes in Your Child
Technique A-112 operates at three levels of impact — from the core neurological target to ripple effects across your child's full development. Understanding what you are targeting helps you measure what matters and celebrate early signs of progress that many parents miss.
Primary Target
Interoceptive awareness of bladder/bowel fullness signals. Observable indicator: Child pauses, reports sensation, or initiates bathroom visit before urgency.
Secondary Targets
- Body vocabulary for internal sensations ("full," "pressure," "tight")
- Bathroom-related anxiety reduction through predictability
- Caregiver-child communication about body needs
Tertiary Targets
- School attendance and participation
- Social dignity and peer relationship quality
- Self-esteem and body confidence
- Reduction in UTI/constipation complications

Material 1 — Bladder/Bowel Fullness Visual Scales
Visual Communication
Interoceptive Awareness
₹200–800 | DIY: ₹0
Why It Works
Gives children visual language for sensations they cannot feel clearly. The scale (1 = empty/comfortable → 5 = very full/urgent) externalizes an internal experience, creating a communication bridge between body state and conscious awareness.
When a child cannot perceive internal fullness, giving them a visual reference point allows them to engage cognitively with what their body cannot yet communicate automatically. This is the single most important foundational tool in the A-112 protocol.
How to Obtain
- 🔨 DIY: Draw 5-level scale on paper. Use water bottle filling analogy. Laminate with tape for durability.
✅ Pinnacle Recommends | DIY: Paper, markers, tape or lamination sheet

Material 2 — Body Mapping for Bathroom Awareness
Body Awareness Tools
Interoceptive Curriculum
₹150–500 | DIY: ₹0
Why It Works
By identifying and marking the lower abdomen region on a body outline, children learn to connect the abstract concept of "needing to go" with specific, locatable body sensations. This is called proprioceptive anchoring of interoceptive awareness — one of the most powerful techniques in the Pinnacle OT toolkit.
When a child can point to where a sensation lives in their body, they have taken the first concrete step toward recognizing it independently. The body map makes the invisible visible.
How to Obtain
- 🔨 DIY: Print free body outline (A4 paper). Ask child to point/color where they feel bathroom signals.
✅ Pinnacle Recommends | DIY: Printer paper, colored pencils
Material 3 — Visual Bathroom Schedules & Timers
Visual Schedules
External Structure
₹300–1,200 | DIY: ₹0
Why It Works
When internal signals are unreliable, external schedules ensure regular toileting attempts — preventing crisis while creating repeated body-check opportunities. Each scheduled visit is an interoception practice session.
The schedule does two things simultaneously: it prevents accidents by creating structure, and it creates the repeated neural activation necessary for interoceptive pathways to develop. Without scheduled visits, there is no practice. Without practice, there is no pathway formation.
How to Obtain
- 🔨 DIY: Draw 6 clock-faces on paper strip. Mark bathroom symbol below each. Tape to wall near child's height.
✅ Pinnacle Recommends | DIY: Paper, markers, tape

Material 4 — Interoception Curriculum (Bathroom Module)
Systematic Curricula
Body Awareness Training
₹2,000–6,000 | Professional Guidance Recommended
Why It Works
Comprehensive interoception curricula (Kelly Mahler framework) systematically build body awareness from foundation level (heartbeat, breathing) → moderate level (thirst, hunger) → specific level (bladder/bowel), creating the full neural scaffold.
This is the only material in the A-112 protocol that builds the complete interoceptive foundation rather than targeting bathroom signals in isolation. Children with very limited body awareness benefit most from beginning here — building the general "I can feel things" capacity before targeting bathroom signals specifically.
How to Obtain
- 🏥 Professional guidance recommended for implementation
✅ Pinnacle Recommends | No adequate DIY substitute — secondary priority after starting with Materials 1, 2, 3

Material 5 — Bathroom Reminder Watches & Vibrating Timers
Prompting Systems
Independence Tools
₹1,500–5,000 | App Alternative Available
Why It Works
Discreet vibrating reminders at programmed intervals prompt private body-check moments throughout the day. Preserves dignity at school. Transitions the prompting function from caregiver to device, building genuine independence over time.
This is one of the most significant independence-building tools in the protocol. When the watch vibrates, the child privately checks in with their body — no teacher announcement, no parent reminder, no peer awareness. The child manages their own body check. This is the goal: self-directed interoceptive monitoring.
How to Obtain
- 📱 Alternative: Set discreet phone alarm or use a simple interval timer app
✅ Pinnacle Recommends | No adequate DIY substitute for the vibration feature

Material 6 — Social Stories for Bathroom Awareness
Narrative Learning
Communication Supports
₹200–600 | DIY: ₹0
Why It Works
Narrative frameworks allow children to learn body awareness concepts through characters — normalizing the experience, teaching vocabulary, and providing cognitive scripts for recognizing and responding to bathroom signals. Social stories reduce shame by showing that body signals are universal and manageable.
When a child reads or hears a story about a character who learns to recognize their body's signals, two things happen: the child gains vocabulary, and the child gains permission. The story says "this happens, and it can be handled" — removing the anxiety that often compounds interoceptive challenges.
How to Obtain
- 🔨 DIY: Write 5-sentence story: "My body makes signals. I feel pressure. I go to the bathroom. My body feels better." Add stick figure drawings.
✅ Pinnacle Recommends | DIY: Paper, pencil, creativity

Material 7 — Before/After Body Awareness Cards
Contrast Learning
Interoceptive Education
₹150–400 | DIY: ₹0
Why It Works
Teaching signal recognition through contrast — the child compares how their body feels before versus after bathroom use. Repeated contrast experiences build neural pattern recognition for the "before" state, making future signals more accessible.
The "before" state becomes learnable only when the child has experienced the "after" state as a reference point. Before/After cards create this comparison explicitly, giving the brain a target sensation to recognize. Over weeks of repetition, the contrast becomes automatic — the neural pathway is formed.
How to Obtain
- 🔨 DIY: Two index cards. Before: draw body with "full" feeling (waves near tummy). After: draw body with "empty/happy" feeling.
✅ Pinnacle Recommends | DIY: Index cards, markers
Material 8 — Bathroom Success Tracking Charts
Data Collection
Progress Visualization
₹100–400 | DIY: ₹0
Why It Works
Success-focused tracking reveals patterns in awareness emergence, optimal interval timing, and independent initiation frequency. Data drives intervention optimization and provides visual evidence of progress that motivates both parent and child.
When you can see a child's self-report accuracy improving from 20% to 50% over four weeks, the pattern is encouraging even before accidents fully stop. The chart transforms an invisible process — neural pathway formation — into a visible, shareable record of growth.
Pinnacle Canon Products
- 🛍️Rosette Imprint Reward Jar → ₹589
- 🔨 DIY: Grid on paper. Days across top, bathroom times down side. Star stickers for success.
✅ Pinnacle Recommends | DIY: Paper, ruler, pencil, star stickers

Material 9 — Sensory-Friendly Bathroom Modifications
Environmental Modifications
Sensory Design
₹500–3,000 | Partial DIY
Why It Works
Bathroom avoidance driven by sensory aversions (cold seat, loud flush, bright lights) masks signal recognition — children disconnect from signals when they dread the environment. Removing sensory barriers allows awareness to emerge.
When a child avoids the bathroom because it is overwhelming, the intervention protocol cannot function. Environmental modification is therefore not optional — it is the prerequisite that makes all other materials effective. A comfortable bathroom is a therapeutically accessible bathroom.
How to Obtain
- 🔨 Partial DIY: Fold towel for seat padding. Use LED nightlight for softer lighting. Place rubber mat for stability.
✅ Pinnacle Recommends | Partial DIY Available | Address this FIRST if bathroom avoidance is present

All 9 Materials at a Glance — Sourced, Priced, Linked
The complete A-112 material set can be assembled for ₹4,000–15,000 comprehensive or ₹500–2,000 for the essential starter kit (Materials 1, 3, and 8). Every single material has a ₹0 DIY alternative — per WHO/UNICEF equity principles. Therapy should never be gated by purchasing power.
Material | Category | Price Range | DIY Option | |
1. Fullness Visual Scales | Visual Communication | ₹200–800 | ✅ Draw 5-level scale on paper | |
2. Body Mapping | Body Awareness Tools | ₹150–500 | ✅ Print/draw body outline | |
3. Visual Schedule & Timer | Visual Schedules | ₹300–1,200 | ✅ Draw clock-faces on paper | |
4. Interoception Curriculum | Systematic Curricula | ₹2,000–6,000 | ⚠️ Partial — professional guidance needed | |
5. Reminder Watch | Prompting Systems | ₹1,500–5,000 | ⚠️ Phone alarm as alternative | |
6. Social Stories | Narrative Learning | ₹200–600 | ✅ Write 5-sentence story | |
7. Before/After Cards | Contrast Learning | ₹150–400 | ✅ Two index cards + markers | |
8. Success Tracking Chart | Data Collection | ₹100–400 | ✅ Grid on paper + stickers | |
9. Sensory Bathroom Mods | Environmental Design | ₹500–3,000 | ✅ Towel padding + LED nightlight |
🌍 ALL MATERIALS HAVE ₹0 DIY ALTERNATIVES — per WHO/UNICEF Nurturing Care Framework equity principles. Zero-cost = zero excuse to delay intervention.
Every Material Has a ₹0 Version. Zero-Cost = Zero Excuse.
Per WHO Nurturing Care Framework (2018): Effective intervention must be accessible across all economic strata. Every technique in the Pinnacle GPT-OS® library includes a household-materials alternative. The table below maps each clinical material to its household equivalent — start with what you have today.
Material | ₹0 DIY Version | Household Items Needed | |
Fullness Scale | Draw 5-level scale on paper; use water bottle filling analogy; laminate with tape | Paper, markers, tape or lamination sheet | |
Body Map | Print free body outline (A4). Ask child to point/color where they feel signals | Printer paper, colored pencils | |
Visual Schedule | Draw 6 clock-faces on paper strip. Mark bathroom symbol below each. Tape to wall | Paper, markers, tape, toilet symbol | |
Social Story | "My body makes signals. I feel pressure. I go to the bathroom. My body feels better." Add stick figures | Paper, pencil, creativity | |
Before/After Cards | Two index cards: "full" feeling before, "empty/happy" feeling after | Index cards, markers | |
Tracking Chart | Grid on paper. Days across top, bathroom times down side. Star stickers for success | Paper, ruler, pencil, star stickers | |
Sensory Modifications | Fold towel for seat padding. Use LED nightlight. Place rubber mat for stability | Household towel, nightlight, rubber mat |
⚠️ The Interoception Curriculum (Material 4) and Vibrating Reminder Watch (Material 5) require purchased products — no adequate household substitute exists. These are secondary priorities. Start with DIY versions of Materials 1, 2, 3, 6, 7, 8.
Read This Before You Start. Clinical Safety Gate.
At Pinnacle Blooms Network®, your child’s safety and emotional well-being are the foundations of our therapeutic success. This mandatory clinical safety gate is designed to ensure that the Technique A-112 protocol is implemented only when it is clinically appropriate for your child’s unique physiology and sensory profile. Before you begin, please review these indicators carefully to ensure this journey is safe, supportive, and effective for your family.
🟢 Green Light / Proceed
You may begin the A-112 protocol immediately if:
- Your child is 3+ years old.
- They have been cleared by a pediatrician for toilet training readiness.
- There is no current history of UTI or chronic constipation.
- Your child shows interest in bathroom independence.
🟡 Yellow Light / Consult First
Please consult your Occupational Therapist or pediatrician before starting if:
- History of constipation, encopresis, or frequent UTIs.
- Significant anxiety or behavioral distress regarding the bathroom.
- Recent physical trauma or medical procedures.
- Known sensory processing differences that cause extreme tactile avoidance.
🔴 Red Light / Do Not Proceed
Do not begin this protocol if your child is experiencing:
- An active, untreated UTI or other acute infection.
- Severe, medically managed constipation requiring laxatives/enemas.
- Post-surgical recovery involving the abdomen or pelvic region.
- Current acute emotional or physical distress.
If You Are Unsure: Safety is our priority. If you have any questions regarding your child’s status, please do not hesitate to contact the Pinnacle Blooms Network® team. We are happy to schedule a free clinical triage call to assess readiness and guide your next steps.
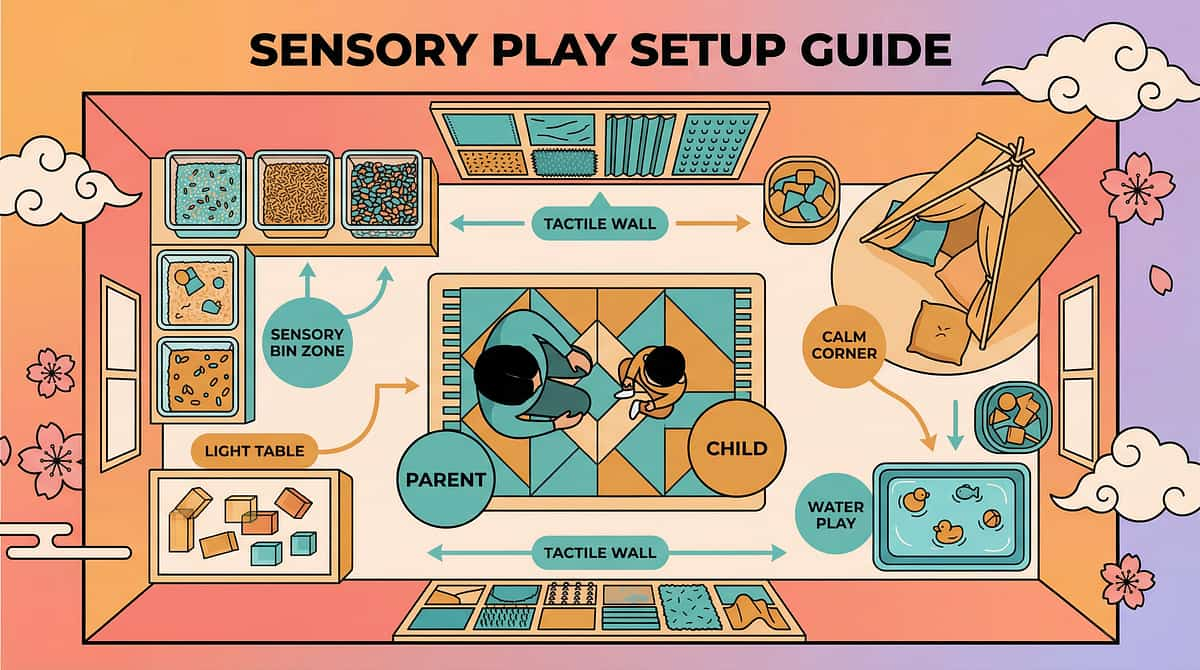
Your Home Becomes a Therapeutic Environment in 10 Minutes
Environmental setup is a core principle of Sensory Integration Theory (Ayres). A well-configured bathroom reduces sensory barriers, provides visual anchors, and creates the predictable, calm environment in which interoceptive awareness can emerge. Use this checklist before beginning your first session.
Bathroom Setup Checklist
- Fullness scale posted at child's eye level
- Body map reference card accessible
- Before/After cards within reach from toilet
- Padded seat cover installed (if sensory modification needed)
- Step stool in position for stability
- Lighting softened — warm, dim if possible
- Loud fan/flush modifications in place
- White noise or quiet fan to muffle flush sound
Adjacent Space Checklist
- Visual daily schedule posted near bedroom door at child's eye level
- Reminder watch charged and programmed
- Tracking chart ready (bedroom or bathroom)
Parent Position
Nearby but not hovering. This is the child's private activity. Your role is to prompt the check-in, not monitor the result. Privacy is dignity — and dignity is a precondition for engagement.
Lighting Guidance
Warm, dim lighting if possible. Bright fluorescent light increases sensory arousal and can override interoceptive signal awareness — the very opposite of what you need.

ACT III — THE EXECUTION
Is Your Child Ready? The 60-Second Pre-Session Assessment
The antecedent conditions before each session determine whether learning is possible. A session begun in the wrong state teaches nothing and may create aversion. Take 60 seconds to assess before every session — this habit will save weeks of setback.
🟢 GO — All Should Be Yes
- Child has eaten in the last 2 hours
- Child has slept adequately
- No visible signs of distress, illness, or extreme dysregulation
- Child is in a relatively calm, alert state
- No major transition or disruption in the last 30 minutes
- Environment is prepared (Card 12 setup complete)
⚠️ MODIFY — If Any Yes
- Child is tired but manageable → Shorten to 1 material only
- Child had a difficult morning → Skip body map; use schedule only
- School day just ended → Allow 30-minute decompression first
🛑 POSTPONE — If Any Yes
- Active meltdown or severe distress
- Signs of illness (fever, stomach pain)
- Child is expressing clear "no" with distress cues
- Medical red flag present (Card 11)
"Antecedent manipulation determines intervention success. A session begun in wrong conditions teaches nothing and may create aversion." — Pinnacle ABA Consortium

Step 1 of 6 — The Invitation
Duration: 30–60 seconds
ABA + OT Led
The Opening: An Invitation, Not a Command
"Hey [child's name], it's time for our body check-in. Want to come with me?"
For non-verbal / AAC users: Show the visual schedule card with the bathroom check-in icon. Point to it. Wait 5 seconds for response.
Body Language Guidance
- Get to the child's eye level
- Neutral, warm facial expression — not urgent, not anxious
- Offer a hand — don't pull
- If they say "no": "That's okay. We'll try in 10 minutes." Do not negotiate endlessly.
Acceptance Cues to Look For
- Child moves toward bathroom
- Eye contact with you after the prompt
- Picks up the visual card or timer
- Verbal "okay" or approximation
Resistance Cues + Modification
- Turning away → Try again in 10 minutes, don't force
- Covering ears → Check for sensory triggers in environment
- Flopping → May be state issue — use POSTPONE protocol
"Every protocol begins with an invitation, not a command. Autonomy is the precondition for learning." — Pinnacle OT Consortium

Step 2 of 6 — The Engagement
Duration: 1–3 minutes
OT + ABA Led
Introducing the Fullness Scale — The Core Engagement Tool
Once in the bathroom, show the child the Fullness Scale (Material 1). Hold the scale at child's eye level. Point to each level slowly (1 through 5). Color-code matters: green (1) → yellow (2-3) → orange (4) → red (5). Allow 10–15 seconds for the child to observe before asking.
"This is our body scale. See the numbers? 1 means your body feels empty and comfortable. 5 means very full and you really need to go. Let's see where your body is right now."
Prompting Hierarchy
First Prompt
Ask: "Can you point to where your body feels right now?"
If No Response
"Let's try — does it feel green (comfortable) or red (very full)?"
If Still No Response
Accept approximation or model: "I think maybe it's here?" NEVER tell child their answer is wrong. Any self-report is data.
Immediate Reinforcement
When child makes any response → immediate specific praise (see Step 5 — Card 28)

Step 3 of 6 — The Therapeutic Action
Duration: 3–5 minutes
OT Primary
The Core Therapeutic Action — Body Check + Bathroom Attempt
Phase A: The Body Check
Child uses fullness scale to report current body state. Parent prompts body map reference: "Can you point to where you might feel it?" Parent states: "Okay, let's try the bathroom now — even if it's just to check."
Phase B: The Bathroom Attempt
Child sits on toilet for 2–3 minutes regardless of reported need. This is a structured awareness opportunity — not a performance event. Parent exits or turns away — privacy is dignity. Use visual timer (60–120 seconds).
Phase C: The After-Check
Whether successful or not: show Before/After card. Ask: "How does your body feel now? Same? Different? Better?" Accept any response. Record it.
Do NOT ask "did you go?" — ask "how does your body feel?" Focus is always on SENSATION AWARENESS, not toileting success. 3 minutes on toilet is the clinical standard for scheduled voiding training.

Step 4 of 6 — Therapeutic Dosage: Frequency, Variation, Satiation
Ongoing Daily
Daily Check-In Schedule (6–8 Daily)
Upon Waking
Mid-Morning (~2 hrs after waking)
Before Lunch
After Lunch (15–20 min)
Mid-Afternoon
Before Dinner
Before Bath / Bedtime
Weekly Variation Rotation
- Week 1: Focus on fullness scale only
- Week 2: Add body map pointing
- Week 3: Introduce Before/After cards
- Week 4: Child leads — parent follows
- Weeks 5–8: Child uses reminder watch independently
Satiation Indicators
- Loss of eye contact after previously engaging
- Physical withdrawal from materials
- Escalating protest
- Flat, rote responses (going through motions)
"3 engaged body-check sessions with genuine interoceptive focus outperform 10 rote schedule visits with no awareness practice." — Pinnacle OT Consortium

Step 5 of 6 — Reinforce & Celebrate
Within 3 Seconds
ABA Led
Reinforcement Timing Is Everything. 3 Seconds Is the Window.
Immediate (within 3 seconds), specific reinforcement increases the likelihood of a behavior occurring again. Reinforce the attempt, not just the success — the child who reports "I don't know" on the fullness scale is doing the work.
What to Reinforce
✨ Any self-report on the fullness scale
✨ Pointing to body map (even approximately)
✨ Sitting on toilet for full timer duration
✨ Using Before/After card
✨ Saying "I need to go" before urgency — biggest win, celebrate loudly
✨ Independent bathroom initiation of any kind
"You checked your body! That is AMAZING. You're learning what your body is telling you."
🏆 Tier 1 — Social Reinforcement
Specific verbal praise + high five or preferred physical contact. Always. Immediately. Every time.
🎯 Tier 2 — Token Economy
Rosette Imprint Reward Jar → ₹589 — add a token for each successful body check. 1800+ Reward Stickers → ₹364 — star on tracking chart.
🎮 Tier 3 — Preferred Activity
Access to preferred activity at end-of-day after completing all scheduled check-ins. Pair with visual promise board.

Step 6 of 6 — The Cool-Down
Duration: 1–2 minutes
OT + ABA Led
No Session Ends Abruptly. The Cool-Down Seals the Learning.
Predictable endings create the trust that enables willing beginnings. The child who knows exactly how a session ends is the child who agrees to start it. Make the cool-down ritual consistent, brief, and positive.
Transition Warning (2 minutes before end)
"One more body check, then we're all done for now."
If Child Resists Ending
"I know you want to keep going. We will do this again [point to next schedule slot]. Right now, it's time for [next activity on schedule]."
Material Put-Away Ritual
Make this a consistent, predictable closing sequence. Predictability is regulation. Child participates in put-away if able — this builds ownership of the materials and the process.
Transition Object
A small preferred item can be handed to the child as the "all done" signal — a consistent visual anchor for closure that they carry into the next activity.

Capture the Data: 60 Seconds Now Saves Hours of Guessing Later
Your 60-second record at session end is the most valuable data in your child's therapeutic journey. It is the difference between guessing and knowing — between adjusting based on patterns versus responding to each incident in isolation.
What to Record — 3 Data Points Only
Data Point | How to Record | Example | |
Fullness scale self-report | Number 1–5, or "no response" | "Reported 2" | |
Bathroom attempt outcome | Y / N / Partial | "Y — dry check" or "Y — voided" | |
Independent initiation? | Y / N | "N — prompted" or "Y — self-initiated!" |
Weekly Pattern Review (After 7 Days)
- What time of day produces most accurate self-reports?
- What interval length produces most successful outcomes?
- Is independent initiation frequency increasing?
GPT-OS® Integration
If using GPT-OS® platform: Enter session data directly. The Prognosis Engine will update your child's Daily Living & Independence Index trajectory and suggest interval adjustments automatically.
"Your 60-second record at session end is the most valuable data in your child's therapeutic journey. It is the difference between guessing and knowing."

Most Sessions Don't Go Perfectly. Here's Your Fix Guide.
Session setbacks are not failures — they are clinical data. Every session that doesn't go as planned reveals information that a perfect session cannot provide. Use this troubleshooting guide to recalibrate, not retreat.
"My child refuses to rate the fullness scale at all."
What happened: Interoceptive awareness is genuinely absent — the child cannot perceive what they're being asked to rate. This is the core deficit. It's information, not failure.
What to do: Start with external sensations first (temperature, hunger). Build "I can feel things" neural foundation before bathroom-specific work. Use Material 4 (Interoception Curriculum) foundation level.
What to do: Start with external sensations first (temperature, hunger). Build "I can feel things" neural foundation before bathroom-specific work. Use Material 4 (Interoception Curriculum) foundation level.
"My child always says '1' (empty) even before accidents."
What happened: Either the child has learned that "1" ends the session, or genuinely cannot perceive fullness.
What to do: Reinforce any report equally. Shift focus from accuracy to engagement. Schedule visits regardless of self-report.
What to do: Reinforce any report equally. Shift focus from accuracy to engagement. Schedule visits regardless of self-report.
"My child has a meltdown when the bathroom timer sounds."
What happened: The sound is an aversive sensory stimulus overriding interoceptive work.
What to do: Switch to vibrating watch (Material 5). Remove all auditory cues from the bathroom environment.
What to do: Switch to vibrating watch (Material 5). Remove all auditory cues from the bathroom environment.
"We did 2 weeks perfectly, then it completely fell apart."
What happened: Regression is part of the learning curve. Neural pathway formation is not linear. Schedule disruption, illness, stress, or a new developmental push can temporarily override progress.
What to do: Return to Week 1 protocol for 3 days. Don't interpret regression as permanent — data shows the pattern.
What to do: Return to Week 1 protocol for 3 days. Don't interpret regression as permanent — data shows the pattern.
"School won't allow the reminder watch."
What to do: Request OT school consultation. Provide school with written Pinnacle protocol document. Under RPWD Act 2016 (India), this is a valid accommodation. Most schools accommodate with an IEP/accommodation letter.
"My child became severely distressed during a session."
What to do immediately: Stop. Comfort the child. Do not proceed. Consider if anxiety-based avoidance is present alongside interoceptive deficit — this requires dual-pathway intervention (psychological support + OT).
"Session abandonment is not failure — it's data. Every session that doesn't go as planned tells you something that a perfect session cannot."
One Technique, Infinite Personalizations. Find Your Child's Version.
There is no single A-112 experience — there is your child's A-112 experience. The protocol is designed to flex across sensory profiles, ages, cognitive levels, and communication systems. Use this adaptation guide to find your child's version of the technique.
For the Sensory Seeker
- Use textured fullness scale (raised numbers)
- Deep pressure before each body check (proprioceptive priming)
- Movement-based breaks between bathroom schedule intervals
- More animated reinforcement (jumping, clapping)
For the Sensory Avoider
- Extensive sensory preparation of bathroom environment (Materials 9)
- Very gradual approach — start with proximity to bathroom, not entry
- Minimal verbal input during body check
- Allow exit option visible at all times (reduces anxiety)
Age-Based Modifications
Age | Key Modification | |
3–5 years | Use simple 3-level scale. Focus on comfort/discomfort only. Social story as primary tool. | |
5–8 years | Full 5-level scale. Introduce reminder watch. Focus on self-report accuracy. | |
8–12 years | Emphasize independence and dignity. Reminder watch essential. Self-managed schedule. |
Cognitive Load Modifications
- Significant cognitive challenges → Use 2-level scale only (comfortable/uncomfortable). Pair with AAC if needed.
- Verbal-only child without AAC → Develop simple hand signal system (fist = full, open hand = empty)
ACT IV — THE PROGRESS ARC
Weeks 1–2: Building the Foundation. Patience Is the Protocol.
Progress: ~15%
Foundation Phase
✅ What Progress Looks Like
- Child completes scheduled bathroom visits without significant protest (3/6 daily)
- Child looks at or points to the fullness scale (even without accurate report)
- Reduction in surprise accidents (accidents still occur but child may show slight anticipatory cues)
- Child tolerates the Before/After card activity
- Parent reports feeling more structured and less reactive
⏳ What Is NOT Progress Yet
- Independent bathroom initiations (too early)
- Accurate fullness scale reports consistently
- Nighttime dryness (this is a longer arc)
- Zero accidents
"If your child tolerated the fullness scale for 10 seconds longer than last session — that is real, measurable neural pathway construction. It doesn't feel like progress. It is."
📊 Data Checkpoint: Review tracking sheet at end of Week 2. Look for: any reduction in accident frequency, any increase in scale engagement, any pattern in timing of accidents.
ACT IV — THE PROGRESS ARC
Weeks 3–4: The Neural Pathways Are Forming. Look for These Signs.
"Weeks 3 and 4 represent a critical neurological window. Your child’s brain is literally rewiring to bridge the gap between sensation and action. Do not look for the destination; look for the tiny, almost invisible cracks where the light of awareness is beginning to break through."
Early Signals to Watch For
Mid-Activity Pausing
Your child briefly stops playing or pauses mid-activity—this is a primary indicator that internal body awareness is finally emerging.
Responsive Cues
Increased eye contact or distinct facial expressions occurring specifically when bladder or bowel sensations begin.
Communication Attempts
First verbal, gestural, or tactile attempts to signal a need, even if those signals remain imperfect or infrequent.
Dry Intervals
You may notice slightly longer intervals of dryness between accidents, suggesting a lengthening latency period in the bladder cycle.
Reduced Resistance
A noticeable decrease in distress or physical resistance during bathroom transition periods as the routine becomes predictable.
What This Means Clinically
These micro-signals indicate that the interoceptive neural pathways are structurally forming, even if they are not yet functionally reliable. We are seeing the child's interoceptive awareness threshold beginning to lower, making them more receptive to internal physical inputs. The architecture is there; we are now waiting for it to stabilize.
What To Do Now
Maintain Consistency
Continue the 6-step protocol without modification. Your unwavering consistency is the signal the brain needs to solidify these new connections.
Log Micro-Signals
Begin specifically documenting these small, emerging signals in your daily tracking chart (Material 8).
Avoid Over-Intensity
Do NOT increase the frequency or intensity of demands yet. The risk of satiation and sensory shutdown is highest during these weeks.
"The absence of dramatic progress IS the progress. Neural pathways don't announce themselves—they quietly build until one day, they simply work."

You Did This. Your Child Grew Because of Your Commitment.
You started this journey because you refused to accept "she'll grow out of it." You researched. You structured. You showed up at 7 AM and 2 PM and before bed, every day. Your child can now feel what they couldn't feel 8 weeks ago. That is neuroscience, engineered by love.
🧠 Neural Pathway Constructed
Interoceptive bladder/bowel awareness — built from nothing, now functioning.
📊 Independence Index Progressed
From Stage 1 (external dependence) toward Stage 4–5 (functional independence) on the Daily Living & Independence Index.
🏠 Home Transformed
Into a therapeutic environment operating at clinical standard — daily, consistent, evidence-based.
💪 Parent Skill Acquired
Interoceptive awareness facilitation — a clinical skill now permanently in your parenting toolkit.
"What was the first moment you realized your child was beginning to feel what they couldn't feel before? Write it down. That moment is irreplaceable."

Explore the Full Interoception & Self-Care Domain
The materials you've assembled for A-112 — the fullness scale, body map, schedule board, sensory modifications — are directly applicable across four of the six related techniques below. Your toolkit grows in value with every technique you complete.
Technique | Code | Level | Materials You Already Own | |
Hunger Signal Recognition | A-111 | 🟢 Intro | Fullness scale ✓ | |
Bathroom Signal Recognition | A-112 | 🔵 Core | THIS PAGE | |
Interoception Development | A-115 | 🔵 Core | Body map ✓ | |
Toilet Training Readiness | A-128 | 🔵 Core | Schedule board ✓ | |
Sensory-Based Toileting Challenges | A-130 | 🟡 Advanced | Sensory mods ✓ | |
Emotional Regulation (Body Signals) | A-105 | 🟡 Advanced | Curriculum ✓ |
ACT V — COMMUNITY & ECOSYSTEM
Real Families. Real Outcomes. Real Timelines.
Priya's Story — Hyderabad, Age 8
Before: Three to four accidents per day. Mother reported "she looks genuinely surprised every time." Teachers were increasingly reluctant. Family was considering withdrawing her from school.
After (10 weeks): Using reminder watch, fullness scale, and scheduled check-ins, she progressed to fewer than 1 accident per week. Now initiates 60% of bathroom visits independently. Remains in mainstream school.
"The fullness scale changed everything. Once she had words for what her body was feeling, everything else followed." — Parent, Pinnacle Blooms Hyderabad
Arjun's Story — Mumbai, Age 6
Before: Night wetting every night + 2 daytime accidents. Constipation was masking bowel signals entirely. Pediatric evaluation ruled out medical causes.
After (8 weeks): Daytime accidents reduced to 2 per week. Constipation managed via dietary protocol. Now uses Before/After cards daily. Night wetting reduced by 70%.
"We thought this was behavioral. Understanding it was interoceptive changed how we responded — and that changed everything." — Parent, Pinnacle Blooms Mumbai
"The most significant moment in interoception work is when a child first stops mid-play, looks slightly inward, and moves toward the bathroom without prompting. That moment — often at weeks 4–6 — tells us the neural pathway has begun." — Senior OT, Pinnacle Blooms Network®
📊 Pinnacle Real-World Evidence: Children receiving structured interoception intervention show average progression across 1.8 independence stages within the first 8-week period. (Illustrative cases; outcomes vary by child profile.)

Home + Clinic = Maximum Impact. Your Professional Support Layer.
The parent executing A-112 at home 6× daily, supported by clinical OT guidance monthly, produces the fastest outcomes in Pinnacle's 21M+ session dataset. Home implementation and clinic support are multipliers — each makes the other more effective.
🏥 In-Person OT Assessment
Comprehensive Interoception Evaluation + Toileting Readiness Assessment at your nearest Pinnacle center. Recommended for all A-112 families.
Find Nearest Center → | 📞9100 181 181
📱 Teleconsultation
OT or NeuroDev Pediatrician video consultation — available across India and internationally. No travel required.
🎓 Parent Training
Structured training in interoception facilitation for parents and caregivers. Available at all 70+ Pinnacle centers and online via GPT-OS®.
🏫 School Consultation
Pinnacle OT visits school to establish A-112 protocol. Provides teacher guidance and accommodation documentation. Request via center or helpline.
Watch the Reel That Introduced These 9 Materials
Reel A-112
75–85 seconds
Sensory Solutions Series
Watch: "When Your Body Doesn't Send the Message"
Our senior Occupational Therapist demonstrates all 9 materials in this 75-second reel — from the fullness scale to sensory-friendly bathroom modifications. Watch how each material is introduced to a child without pressure or shame.
- 🎬 Reel ID: A-112
- 📂 Series: Sensory Solutions Series — Episode 112
- 🏷️ Domain: Interoception & Body Awareness
- ⏱️ Duration: 75–85 seconds
Series Navigation: ← A-111 — Hunger Signal Recognition | → A-113 (Next in Series)

Consistency Across All Caregivers Multiplies Impact by 3×
The brain builds interoceptive pathways through repetition across environments, not just with one caregiver. When every adult in the child's life uses the same language, cues, and protocol, the neural signal is reinforced 3× faster. Inconsistency is the #1 reason progress stalls.
Who Needs to Be Aligned
Primary Parent
Leads daily sessions, manages tracker data, and adjusts the protocol based on weekly outcomes.
Secondary Parent / Spouse
Mirrors the exact language and physical cues during their caregiving hours to maintain a unified front.
Grandparents (Nana/Dadi)
Vital partners who must use the same visual scale; they must avoid pressure or "just try" commands that confuse signals.
School Teacher / Aide
Uses a simplified one-page protocol summary to ensure interoception practice continues seamlessly during school hours.
Therapist (OT/SLP)
Syncs with home data weekly to refine the clinical plan based on real-world progress observed by the family.
The Alignment Protocol
Share the Visual Scale
Provide every caregiver, including school staff, a laminated copy of the bladder/bowel fullness scale (Material 1).
Teach the Language
Establish one consistent phrase—e.g., "Can you check your body? Does your tummy feel full?"—used by everyone in the home.
Log Together
Each caregiver contributes one data point per session to the shared tracking chart (Material 8) for a clear, collective view.
What Breaks Consistency
❌ Grandparents using shame-based language like, "Why didn't you go earlier?"
❌ School staff skipping the schedule because "it's not their job."
❌ Secondary caregivers dismissing the protocol as "too much effort" or "not necessary."
❌ Switching visual scales or vocabulary mid-program, which resets the child's learning process.
Your child's nervous system doesn't know which adult is in the room. It only knows whether the signal came again—or didn't. Every caregiver is either building the pathway or breaking it.
Preview of 9 materials that help with bathroom signal recognition Therapy Material
Below is a visual preview of 9 materials that help with bathroom signal recognition therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.




















Link copied!

ACT VI — THE CLOSE & LOOP
Frequently Asked Questions — Answered by the Pinnacle Consortium
These are the questions parents most commonly ask about A-112 — answered with the same clinical precision and warmth that guides every Pinnacle protocol. If your question isn't here, our team is available 24×7 at 9100 181 181.
"My child is 10 years old. Is it too late?"
No. Interoceptive awareness can be developed at any age. The brain retains plasticity for this type of learning throughout childhood and adolescence. The process may take longer in older children, but outcomes data shows significant improvement at 10, 12, and even teenage years.
"How is this different from regular toilet training?"
Regular toilet training addresses behavioral readiness. A-112 addresses interoceptive awareness — the child's ability to perceive internal signals. A child can be behaviorally ready and interoceptively unaware simultaneously. A-112 builds the awareness foundation that makes behavioral training actually work.
"My child has constipation. Should I start A-112 anyway?"
Medical causes must be addressed first or concurrently. Constipation physically masks bowel signals —