
"My child is 5 years old and still in diapers. We've tried everything."
If that sentence is your Tuesday morning, you are in the right place.
🚽9 Materials That Help With Autism Toilet TrainingSeries: Adaptive Daily Living Skills in Autism — Episode E-492 | Pinnacle Blooms Network® "You are not failing. Your child's nervous system is speaking — and these 9 materials are designed to listen."
OT
SLP
ABA
SpEd
NeuroDev
Pediatrics
WHO Nurturing Care Framework (2018): Early identification and parental awareness directly shapes developmental outcomes. nurturing-care.org/ncf-for-ecd/

You Are Among Millions of Families Navigating This Exact Challenge
1 in 36
Children with Autism
CDC 2023 — approximately 2.8 million new diagnoses annually worldwide
80%
Interoceptive Differences
Of autistic children experience interoceptive processing differences that directly affect toilet training readiness (PMC11506176)
68 mo
Average Age of Completion
In autism vs. 36 months in typical development — the gap is real, and bridgeable with the right approach
"You are not behind. You are not failing. You are navigating something genuinely harder — and science explains exactly why." — Pinnacle Blooms Consortium, 20M+ therapy sessions
🇮🇳India: 1 in 100 children identified with ASD. Toilet training delay is among the top 5 caregiver distress factors reported across Pinnacle's 70+ centers.
Research: PMC11506176 — PRISMA systematic review (2024) | PMC10955541 — Meta-analysis, World J Clin Cases (2024) | DOI: 10.12998/wjcc.v12.i7.1260

Why Toilet Training Is Neurologically Different in Autism
The Brain Regions Involved
- Insula Cortex → Interoceptive signal processing
- Somatosensory Cortex → Body signal interpretation
- Prefrontal Cortex → Sequencing & planning
- Amygdala → Threat detection (bathroom fear)
- Basal Ganglia → Routine formation
↳ Interoception Signal Disruption is the root of toileting difficulty in autism.
🧠 Interoception Differences
The brain's "internal GPS" for body sensations (bladder fullness, bowel pressure) is processed differently. Many autistic children genuinely cannot feel the need to go. This is not defiance. This is neurology.
👂 Sensory Overload in the Bathroom
Echoey acoustics, cold surfaces, unpredictable flush sounds, fluorescent buzz. For a sensory-sensitive nervous system, the bathroom triggers fight-or-flight. A nervous system in threat mode cannot relax enough for elimination.
🗣️ Communication Processing Gaps
Recognizing a body sensation, labeling it, and acting in time requires a multi-step neurological chain. In autism, any link in that chain may process differently.
🔄 Routine Rigidity
Diapers become deeply encoded as "the only safe way." Changing this is not a behavioral decision — it is a neurological retraining task.
📋 Executive Function Sequencing
Toileting involves 8–12 sequential steps the prefrontal cortex must orchestrate. Working memory and sequencing differences make this intrinsically harder.
"This is a wiring difference, not a behavior choice. These 9 materials address the neurological roots, not the surface behavior."
Sources: Frontiers in Integrative Neuroscience (2020): DOI: 10.3389/fnint.2020.556660 | Garfinkel et al. (2016); Price & Hooven (2018)
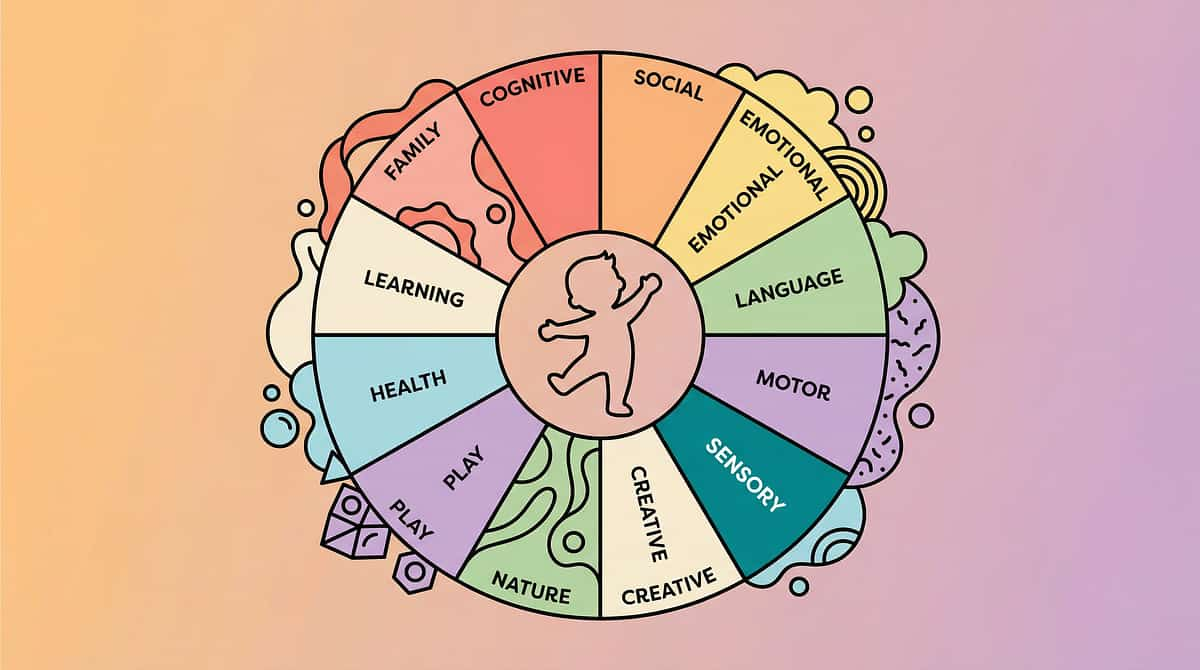
Your Child's Developmental Trajectory — And Where This Fits
Understanding where your child sits on the developmental timeline is the first step toward meeting them exactly where they are — without judgment, without rush.
Age Zone | Typical Milestone | In Autism | |
18–24 months | Bladder/bowel awareness emerging | Often absent or significantly delayed | |
2–3 years | Daytime dryness | Average age 5–6 years in ASD | |
3–4 years | Independent toileting | Often 6–8+ years with ASD | |
5–7 years | Nighttime dryness | May extend to adolescence | |
8+ years | Full independence | Achievable with right supports |
"Your child is here. The trajectory is forward. These 9 materials accelerate the journey."
What Commonly Co-occurs With Toileting Challenges in Autism
GI Differences
Constipation occurs in 46–85% of autistic children
Anxiety
Bathroom becomes a feared stimulus requiring gradual desensitization
Sensory Processing
Tactile, proprioceptive & interoceptive differences affect all phases
ADHD
Impulse control & attention affect training readiness
Sleep Differences
Affect regulation and daytime capacity for learning new routines
Research: PMC9978394 — WHO/UNICEF CCD Package (2023) | who.int

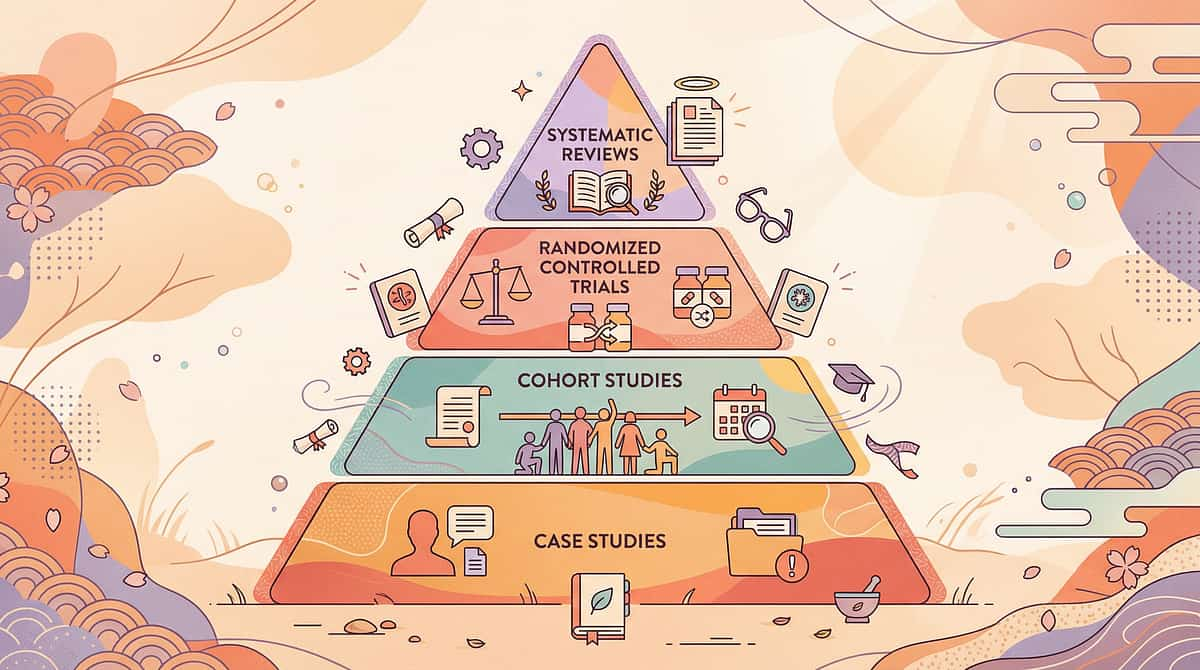
The Evidence Behind This Approach
Evidence Grade: Level I–II
Systematic Reviews + RCTs + Multi-Site Clinical Protocols
🔬 PRISMA Systematic Review (Children, 2024)
16 articles confirm behavioral + sensory interventions meet evidence-based practice criteria for autism self-care skill acquisition. PMC11506176
📊 Meta-Analysis — World J Clin Cases (2024)
24 studies: Sensory integration + behavioral interventions effectively promote adaptive behavior, self-care, and sensory processing in ASD. PMC10955541 | DOI: 10.12998/wjcc.v12.i7.1260
🇮🇳 Indian RCT — Indian Journal of Pediatrics (2019)
Home-based sensory and behavioral interventions demonstrated significant measurable outcomes in Indian pediatric ASD populations. DOI: 10.1007/s12098-018-2747-4 — Padmanabha et al.
🌍 WHO Nurturing Care Framework (2018)
Establishes equity-focused, context-specific home interventions as essential pediatric care infrastructure. nurturing-care.org
✅ NCAEP Evidence-Based Practices Report (2020)
Visual supports, video modeling, and reinforcement systems are classified as EBPs for autism across adaptive skills domains. autismpdc.fpg.unc.edu
"Clinically validated. Home-applicable. Parent-proven. Across 20 million therapy sessions."
Technique E-492
Adaptive Daily Living Skills
🚽 9 Materials That Help With Autism Toilet Training
Formal Name: Autism-Specific Adaptive Toileting Intervention Protocol Parent-Friendly Alias:"The 9-Tool Toilet Training Toolkit"
Autism toilet training is not a parenting approach — it is a clinical intervention requiring autism-specific materials and methods that address the neurological roots of delayed toileting. This protocol identifies and deploys 9 evidence-based material categories — from visual sequencing supports to interoception training tools to sensory environment modifications — that collectively address every barrier unique to autistic neurology: interoceptive differences, sensory sensitivity, communication challenges, routine rigidity, and motivation differences. Unlike neurotypical toilet training methods, this approach never assumes the child "already knows" what their body is telling them. It builds that knowledge from the ground up.
🏥Domain | Adaptive Daily Living Skills / Self-Care | |
📂Canon | Visual Schedules · Reinforcement Menus · Sensory Tools · Body Awareness | |
👶Age Range | 2.5 – 12 years (and beyond) | |
⏱️Session Duration | 15–30 minutes per toilet sit | |
📅Frequency | Every 30–90 minutes during waking hours | |
📈GPT-OS® Index | Toileting Readiness Index + Interoceptive Awareness Index | |
🌐Series | Adaptive Daily Living Skills — Episode 492 of 999 |

This Technique Belongs to No Single Profession — Because Autism Doesn't
Effective autism toilet training is inherently cross-disciplinary. Each professional brings a distinct lens — and your child needs all of them working in concert.
Occupational Therapist (Primary Lead)
Leads sensory environment modification, stability supports, interoception training, and motor sequencing of toileting steps. pinnacleblooms.org/occupational-therapy
BCBA / ABA Therapist (Co-Lead)
Designs reinforcement system, data collection protocol, timed toileting schedule, and behavioral troubleshooting. pinnacleblooms.org/aba-therapy
Speech-Language Pathologist
Develops AAC, PECS, verbal scripts for signaling bathroom needs; creates social stories. pinnacleblooms.org/speech-therapy
Special Educator
Designs visual schedules, school-home coordination, IEP accommodation documentation, and generalization strategies. pinnacleblooms.org/special-education
Developmental Pediatrician / NeuroDev
Rules out medical causes (constipation, UTI, anatomical factors), prescribes stool softeners when needed, monitors neurological factors. pinnacleblooms.org/developmental-pediatrics
Parent / Caregiver (Essential Partner)
The 24×7 implementation engine. The clinic sets the protocol; the home runs it. Parent is not a recipient of therapy — they ARE the therapy delivery system.
"The brain doesn't organize by therapy type. These 9 materials are designed to be used by the whole family — with the whole child — across every setting."
Precision Targeting — What These 9 Materials Are Actually Treating
Target | "Not Yet" Looks Like | "Progress" Looks Like | "Mastery" Looks Like | |
Interoception | Unaware of wetness for 60+ min | Notices wetness within 5 min | Signals need BEFORE accident | |
Sensory | Refuses to enter bathroom | Tolerates bathroom with mods | Enters bathroom independently | |
Sequencing | Can't complete any step independently | Completes 3–4 steps with prompts | Completes full sequence independently |
Research: PMC10955541 — Meta-analysis: adaptive behavior, sensory processing, motor skills as measurable targets | NCAEP 2020
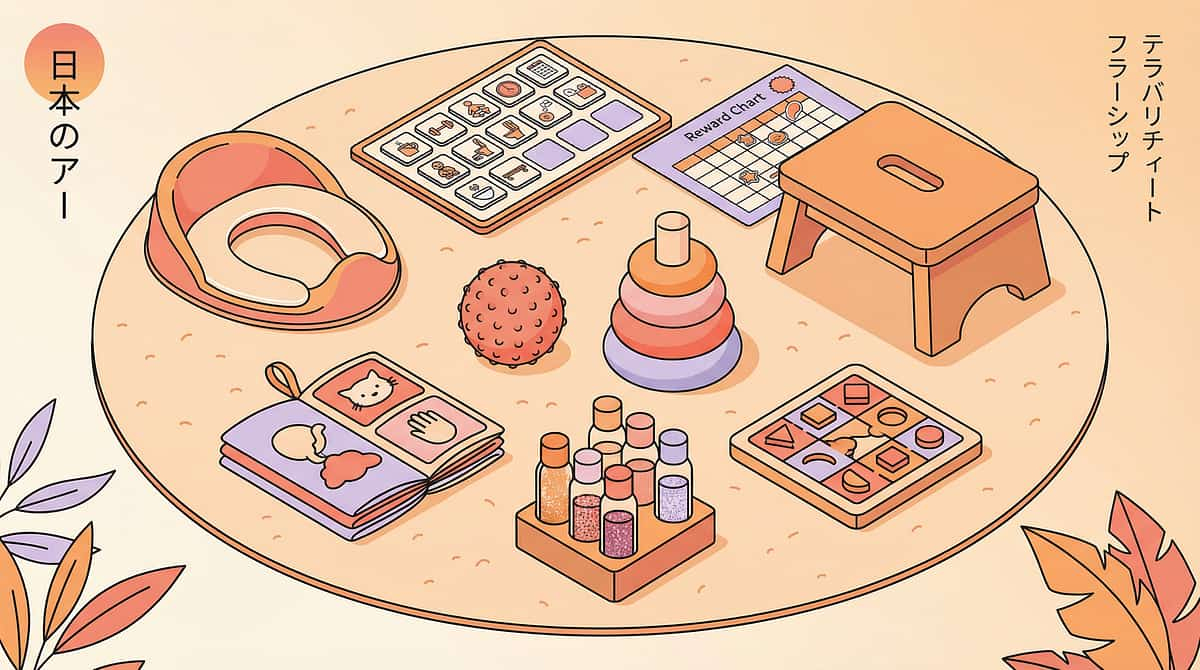
🛒 The 9 Materials
Clinically Mapped from Pinnacle 128 Canon
9 Materials That Address the 9 Real Barriers — Clinically Mapped
From the Pinnacle 128 Canon Materials system — every material exists because a neurological barrier demands it.
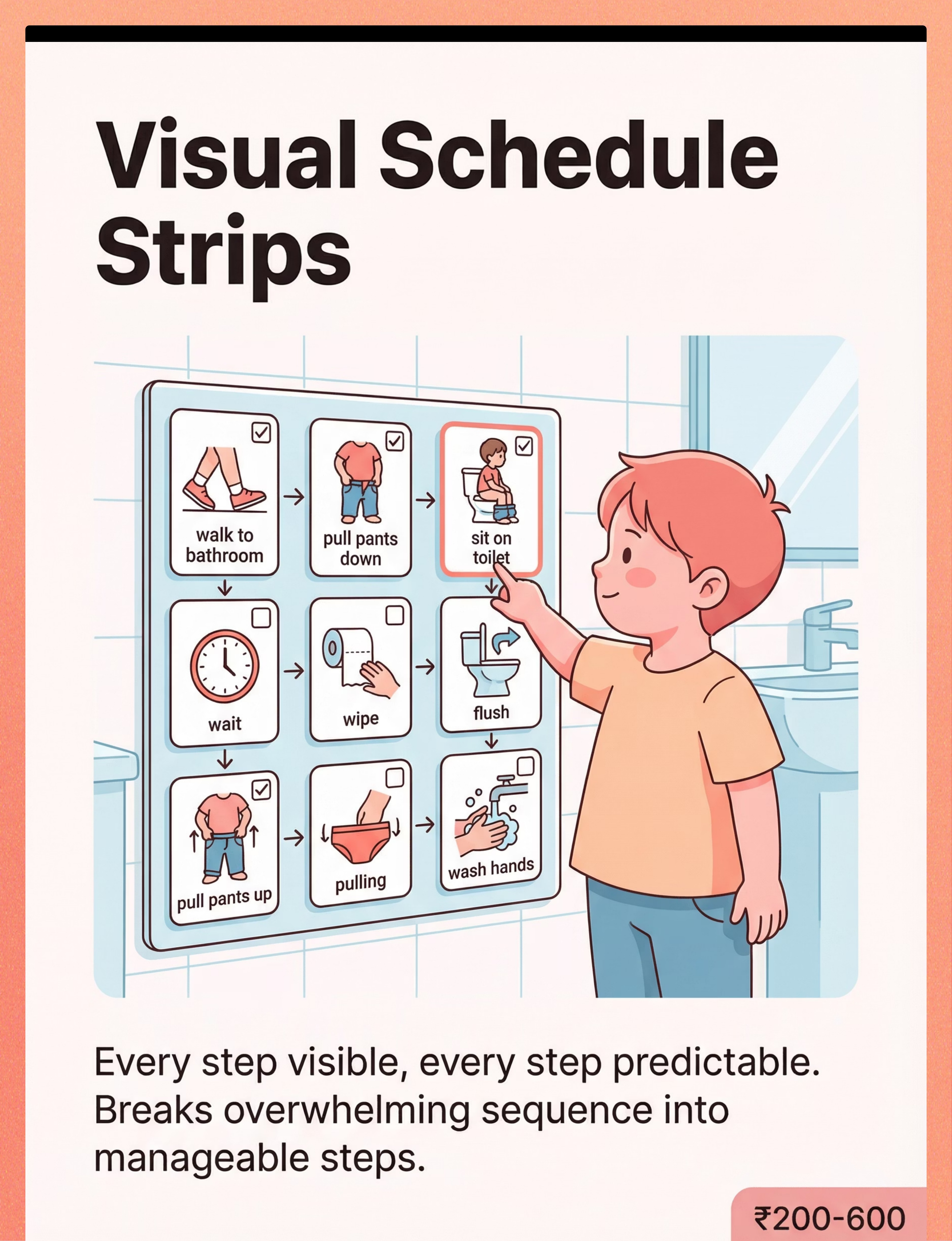
1. Visual Schedule Strips for Toileting Sequence
🏷️ Visual Schedules / PECS Systems Breaks 8-step toileting sequence into visible, predictable picture cards. Leverages visual processing strengths. Removes executive function demand from sequencing. 💰 ₹200–600 | Search Amazon.in
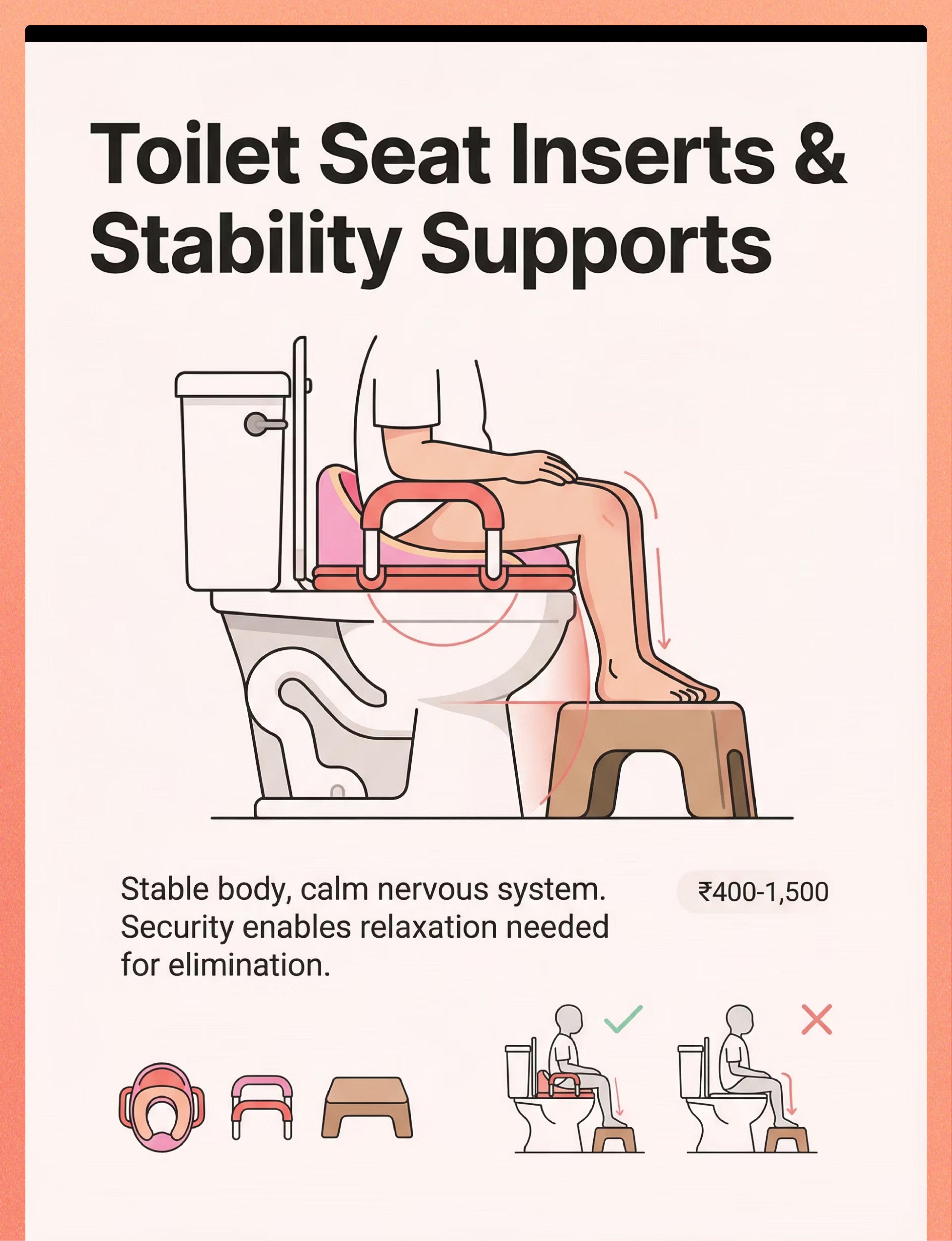
2. Toilet Seat Insert with Handles & Footstool
🏷️ Adaptive Equipment / Physical Support Eliminates falling-in fear. Handles provide proprioceptive security. Feet planted = nervous system grounded. Stability enables physiological relaxation for elimination. 💰 ₹400–1,500 | Search Amazon.in
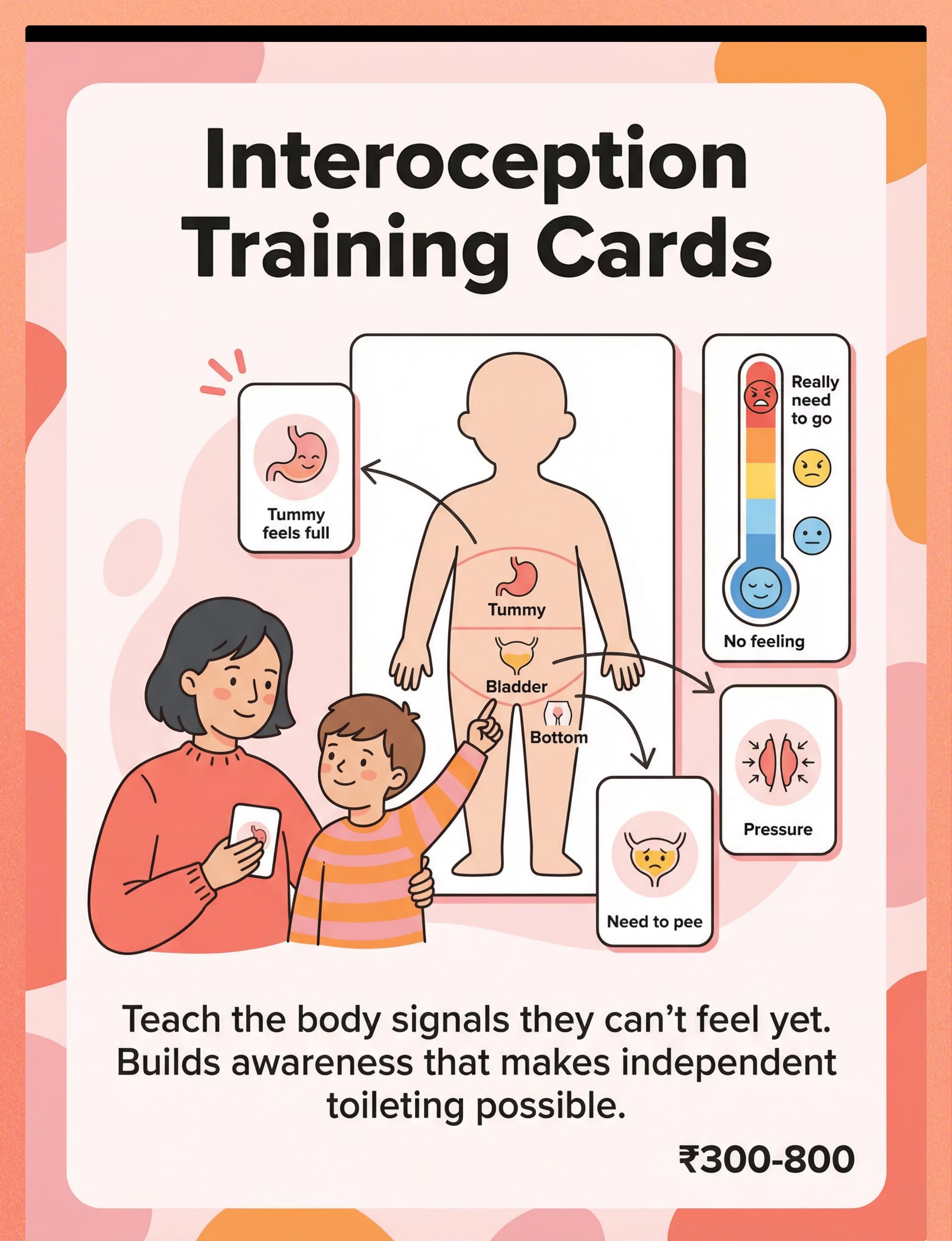
3. Interoception Training Cards & Body Maps
🏷️ Body Awareness / Interoception Tools Teaches children to recognize internal body signals they may not perceive. Body maps + sensation cards + regular check-ins build the awareness that makes independent toileting neurologically possible. 💰 ₹300–800 | Search Amazon.in
4. Sensory Modification Kit for Bathroom
🏷️ Sensory Regulation Tools / Environmental Modification Neutralizes the 5-sense sensory threat of the bathroom. Flush dampener, warm lighting, soft rug, padded seat, noise-reducing headphones — transforms threat into tolerance. Sensory safety is prerequisite to skill learning. 💰 ₹500–2,000 | Search Amazon.in
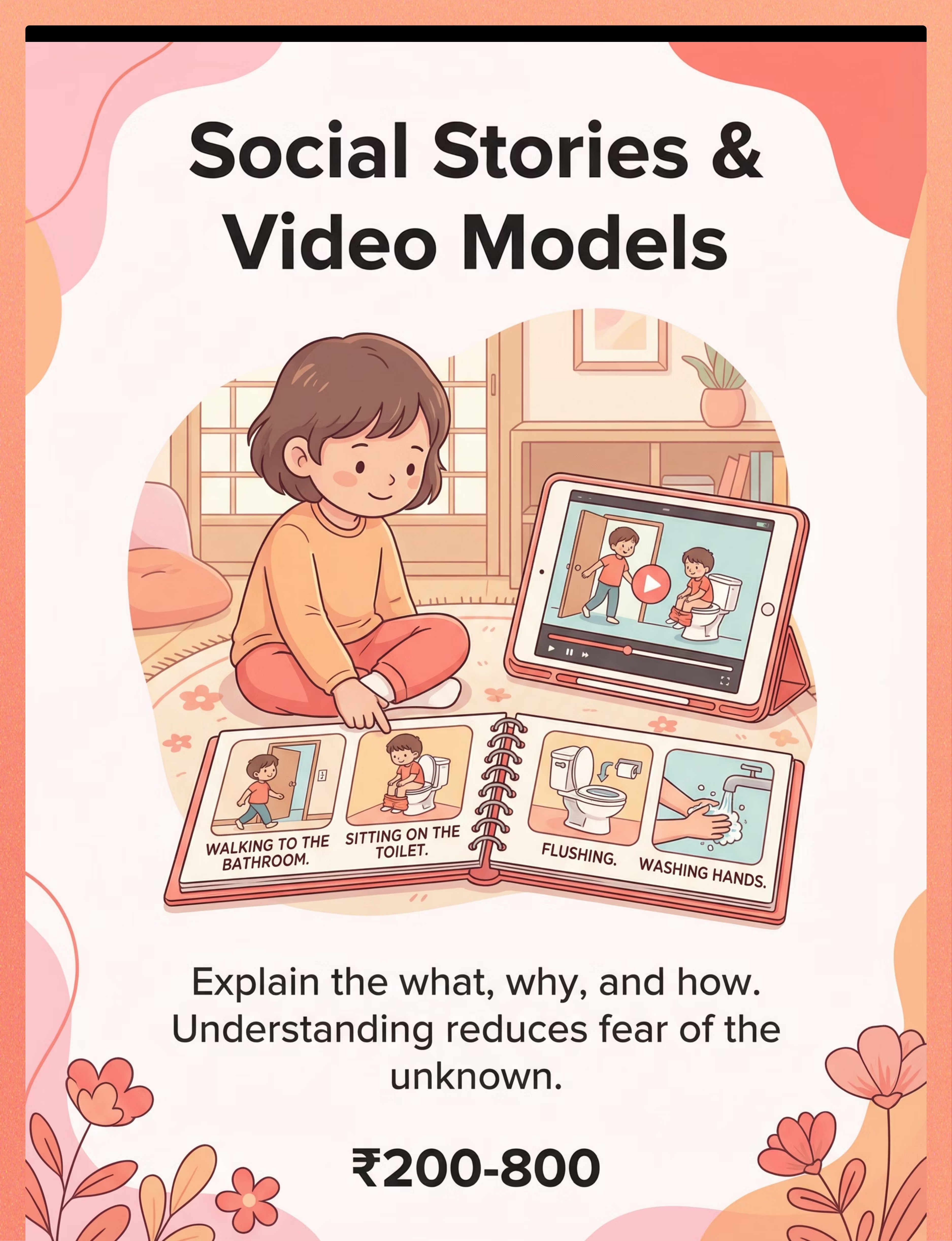
5. Social Stories & Video Models for Toileting
🏷️ Social Stories / Narrative-Based Learning NCAEP evidence-based practice. Social stories explain what will happen and why, reducing fear of the unknown. Video models provide visual template for imitation. Both leverage autism's visual and systematic learning profile. 💰 ₹200–800 | Search Amazon.in
6. High-Interest Reinforcement System
🏷️ Reinforcement Menus / Token Economy Social praise doesn't motivate most autistic children. Individualized high-value reinforcement is the ABA engine that makes toilet learning worth the neurological effort. 💰 ₹100–500 | Token Board ₹589 | Sticker Set ₹364
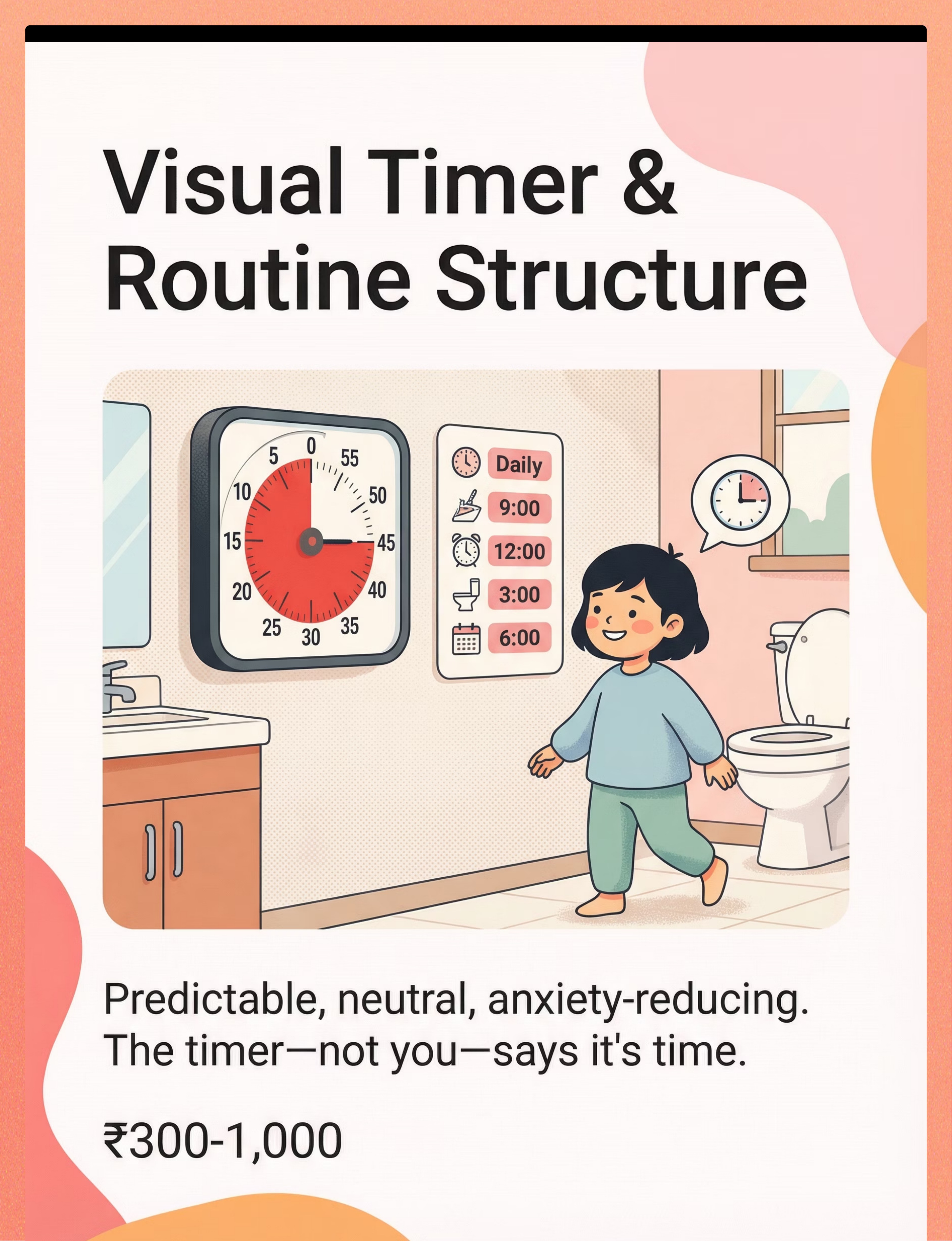
7. Visual Timer & Routine Structure Visuals
🏷️ Visual Timers / Schedule Tools The timer — not the parent — signals toilet time. Removes power struggle. Shows concrete passing of time. Predictability reduces resistance by eliminating surprise. 💰 ₹300–1,000 | Search Amazon.in | Transition Support ₹425
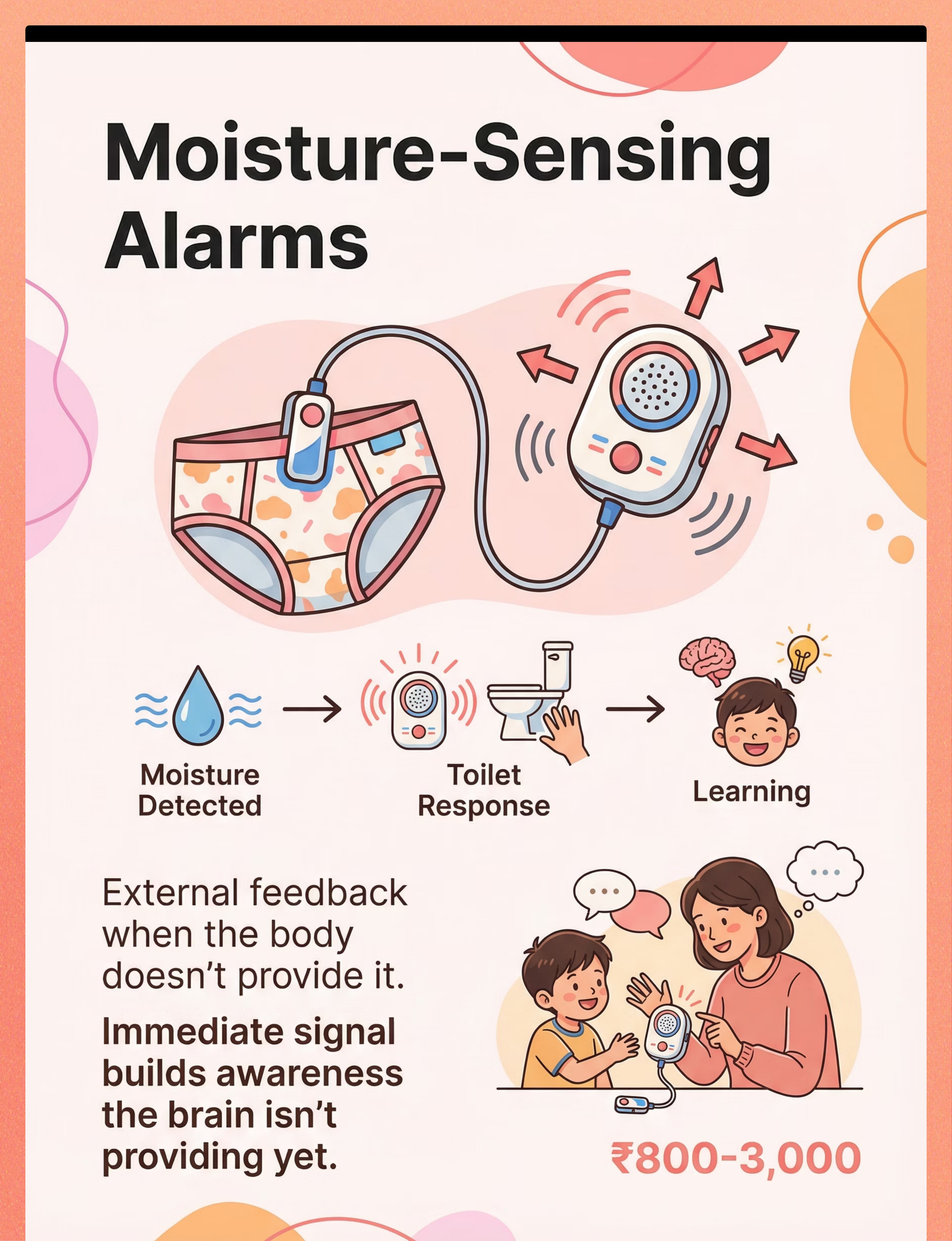
8. Moisture-Sensing Alarms
🏷️ Sensory Feedback Devices / Adaptive Technology For children who do not feel wet after accidents, moisture-sensing technology provides the immediate external feedback the brain isn't generating. Immediate signal builds the neural association the brain is not yet producing independently. 💰 ₹800–3,000 | Search Amazon.in
9. Bowel Movement Support Kit (Positioning + Fiber + Relaxation)
🏷️ Adaptive Positioning / Regulation Support Bowel training requires correct physiology: feet on stool (knees above hips = squatting posture = pelvic floor relaxation), blowing toys activate correct muscle groups, post-meal timing uses gastrocolic reflex. Biology + behavior, together. 💰 ₹200–800 | Search Amazon.in
💰Total Comprehensive Kit: ₹2,800–10,500 | Essential Starter Kit (Budget): Visual Schedule + Seat Insert + Timer + Reinforcer = ₹1,000–2,100

₹0 Version Exists for Every Material. No Family Left Behind.
WHO/UNICEF Equity Principle: Every child deserves access regardless of economic context. Here is how.
Material | Commercial (Buy) | DIY Substitute (Make Today) | |
Visual Schedule | Printed/laminated cards ₹200–600 | Photograph your own bathroom steps on any smartphone. Print at stationery shop. Cut, laminate with packing tape. | |
Seat Insert + Footstool | Commercial insert ₹400–1,500 | Any sturdy plastic stool as footrest. Fold a towel for padded seat. Rolled blanket for side support. | |
Interoception Cards | Printed card sets ₹300–800 | Draw body outline on paper. Label 3 zones: tummy, bladder, bottom. Use emoji faces for sensation levels. | |
Sensory Bathroom Kit | Commercial kit ₹500–2,000 | Warm bulb from hardware store (₹50). Bath mat from home store (₹150). Verbal countdown before flush (₹0). | |
Social Story | Purchased book ₹200–800 | Write 8 sentences: "I walk to the bathroom. I pull down my pants…" Use your own photos. Laminate. | |
Reinforcement System | Token board + items ₹100–500 | Stickers from any stationery store. Child's favorite video (already owned). Chart drawn on paper. | |
Visual Timer | Time Timer ₹300–1,000 | Phone timer with large display. Sand timer from toy shop (₹50–150). Physical countdown "5-4-3-2-1." | |
Moisture Alarm | Commercial alarm ₹800–3,000 | Thin cotton underwear without diaper = faster adult detection. Parent check every 20 minutes. | |
Bowel Support Kit | Footstool + pinwheel ₹200–800 | Any low stool that raises feet. Blow bubbles through a straw while seated. High-fiber foods already in home. |
"The principle matters more than the product. A photographed schedule works just as well as a printed one. The ₹0 version often works first because it's personalized to YOUR bathroom."
⚠️When clinical-grade material is non-negotiable: Moisture-sensing alarms for children who show zero accident awareness after 4+ weeks of timed toileting. Consult OT before substituting for interoception training.

Safety Gate — Read Before Executing Any Protocol
🔴 RED — Do Not Proceed
• Child has unmanaged constipation — medical clearance first. Forced toileting with constipation causes pain and worsening withholding. • Child has active UTI symptoms — medical evaluation first. • Child is in acute distress, illness, or post-meltdown within 30 minutes — reschedule session. • Medical/anatomical cause of toileting difficulty NOT yet ruled out. • Child shows trauma response to bathroom (severe panic, self-injury, inconsolable crying 10+ min) — clinical OT assessment before home protocol.
🟡 AMBER — Proceed with Modifications
• Child is mildly dysregulated — use simplified 2-step version only; skip timed sitting; focus only on bathroom approach. • Child recently regressed after illness — restart from earlier phase with no pressure; regression is expected and temporary. • Child has just had a large sensory event — wait 20 minutes, then offer bathroom in low-demand way. • Moisture alarm causes distress beyond 3 sessions — discontinue and substitute timed toileting.
🟢 GREEN — Proceed
• Child is rested, fed, and in regulated state. • Medical causes have been ruled out. • Bathroom sensory modifications are in place. • At least one high-value reinforcer is identified and ready. • Visual schedule is posted at child's eye level. • All materials are ready before session begins.
🛑STOP if you see these signs during any toilet session: Severe distress beyond 3 consecutive sessions that does not reduce · Self-injurious behavior related to toileting · Blood in stool or urine · Complete refusal across all settings for 2+ weeks despite modifications · Sudden regression with pain, behavioral changes, or medical symptoms
📞FREE Helpline: 9100 181 181 · 24×7 · 16+ Languages · Speak to a clinical team member about any concern

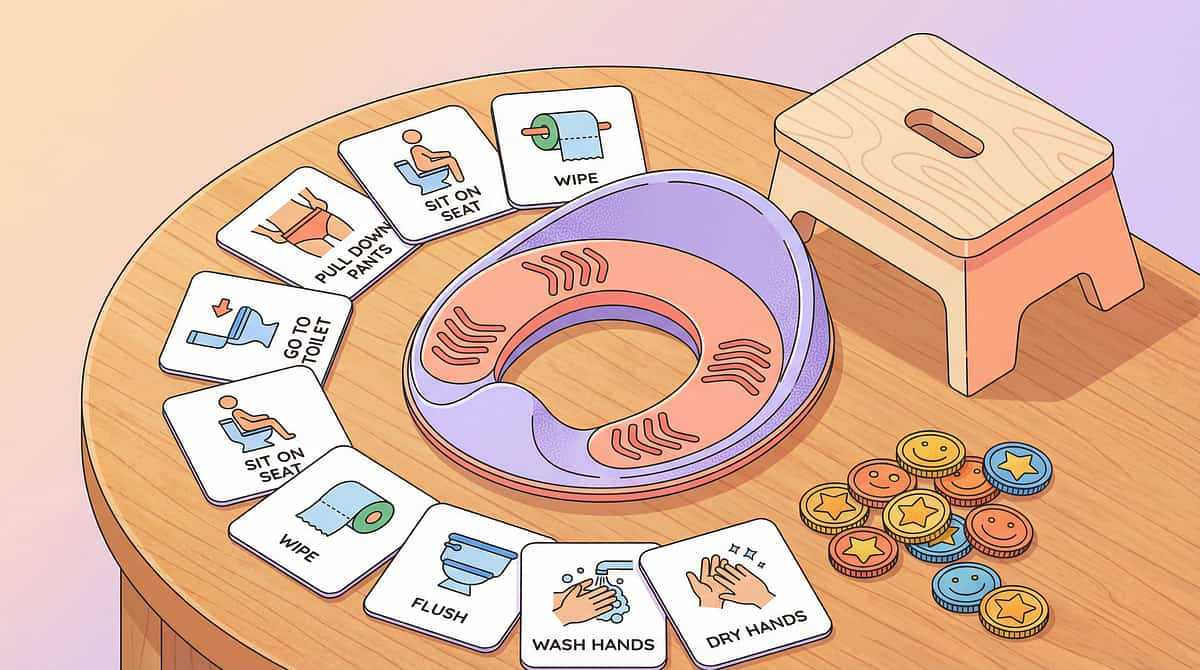
Before You Begin: The Autism-Ready Bathroom Setup
Spatial precision prevents 80% of session failures. Set this up once — keep it consistent.
# | Position | Setup Instruction | |
1 | Toilet | Seat insert with handles installed. Footstool positioned under feet. | |
2 | Eye-Level Wall | Visual schedule strip posted at child's eye level (typically 80–100cm from floor). | |
3 | Timer Position | Visual timer placed where child can see it while seated on toilet. | |
4 | Lighting | Soft warm bulb ON. Overhead fluorescent OFF if possible. Nightlight acceptable. | |
5 | Floor | Non-slip bath mat. Warm rug if child has temperature sensitivity. | |
6 | Sound | Phone or small speaker ready with child's preferred calm music OR silence. | |
7 | Reinforcer | High-value reinforcer READY but not visible — deliver immediately after target behavior. | |
8 | Parent Position | Stand/sit at child's side or slightly behind. NOT between child and exit. Never blocking. | |
9 | Remove | Remove all non-essential items that could become distractions or stimulation. |
Setup Checklist — Complete Before Every Session
- Seat insert + footstool installed and stable
- Visual schedule posted at child eye level
- Timer ready and positioned
- Sensory modifications in place (lighting, sound, temperature)
- High-value reinforcer prepared and ready
- Parent phone/distractions away
- 15–20 minute window of uninterrupted time available
- Bathroom door can be partially open to reduce echo
"Consistency is the protocol. The same bathroom, the same setup, the same sequence, every time — until it becomes the child's internalized routine."

▶️ Execute
Pre-Session Gate
The Pre-Session Check — 60 Seconds Before Every Toilet Sit
The best session is one that starts right. This 60-second check determines whether to proceed, modify, or postpone.
# | Check | ✅ Proceed | ⚠️ Modify | ❌ Postpone | |
1 | Last meal: Child ate 20–45 min ago? | Yes | >90 min ago | <15 min ago | |
2 | Regulation state: Child is calm or playful? | Calm/alert | Mildly distracted | Distressed/mid-meltdown | |
3 | Last sleep: Not awake more than 4 hours? | Yes | 4–5 hours | Severely overtired | |
4 | Bathroom: Setup complete (Card 12)? | All 9 items | 6–8 items | <6 items | |
5 | Reinforcer: High-value reinforcer ready? | Yes | Partial | Not prepared | |
6 | Time: 15+ minutes available? | Yes | 10–15 min | <10 min | |
7 | Last session: No severe distress in 24 hours? | Yes | Mild difficulty | Severe distress |
🔴 3+ POSTPONE
Do not proceed. Offer preferred calm activity instead. No mention of toilet.
🟡 2–3 MODIFY
Proceed with simplified version: bathroom approach only, 2-minute sit max, minimal demand.
🟢 ALL GO
Proceed with full protocol (Steps 1–6).
"The child who is forced through a session they weren't ready for will be harder to engage tomorrow. The child who is respected today will trust the routine tomorrow."

Step 1 of 6
⏱️ 30–60 seconds
The Invitation
Core Principle: Begin with an invitation, never a command. The child's nervous system must associate the bathroom with safety and positive expectation — not authority and compliance.
Parent Script — For Speaking Children
💬 "Hey [name], it's timer time! Want to come with me to the bathroom? Your [favorite character] schedule is waiting for you!"
For Non-Speaking Children
💬 [Show first-then board: toilet icon → child's favorite reinforcer icon]. Point to toilet icon. Wait 3 seconds. Gesture toward bathroom.
Body Language Guidance
- Crouch to child's eye level
- Warm, neutral expression — not anxious, not urgent
- Hold child's visual schedule card as an invitation prop
- Begin walking toward bathroom — child often follows without command
If Child Resists — What To Do
- Runs away or stiffens → Do NOT chase or force. Note "postpone" in data. Try again in 20 minutes.
- Ignores → Add preferred item: "Your [reinforcer] is waiting in the bathroom"
- Protests verbally → Validate: "I hear you. Just 2 minutes on the toilet, then [reinforcer]"

Step 2 of 6
⏱️ 1–3 minutes
The Engagement
Once child is in bathroom or approaching toilet, introduce materials in a warm, structured sequence that makes cooperation feel natural and rewarding from the very first moment.
Point to First Step of Visual Schedule Together
Say: "Step 1 — let's do it together." This externalizes the sequence away from the parent's verbal authority.
Hand-Over-Hand Guidance as Needed
Use least-to-most prompting. Child participates in pulling pants down with graduated physical guidance.
Reinforcement Begins HERE — Not at the End
Token/sticker delivered for: entering bathroom, approaching toilet, touching toilet seat (even if not sitting yet). Reinforce from the FIRST cooperative step.
Child Response | Parent Action | |
Engaged, following schedule | Continue to Step 3. Maintain warm praise. | |
Tolerating but not engaged | Continue — tolerance IS progress at this stage. | |
Slightly avoidant | Slow down. Stay at current step. Increase reinforcer preview. | |
Refusing to participate | Acknowledge feeling. Offer gentle exit with dignity. Note in data. |
Research: PMC11506176 — Structured material introduction in sensory integration protocol | ABA Prompting Hierarchy: System of least prompts for adaptive skill teaching

Step 3 of 6
⏱️ 3–10 minutes
The Therapeutic Action — The Core Event
The Core Therapeutic Event: Child is seated on toilet with seat insert. Feet on footstool. Visual schedule open. Timer running. This is where neurological learning happens.
Feet Positioned
Both feet flat on footstool. Knees at or above hip level. "Feet on the stool" becomes part of the verbal routine.
Sensory Comfort Confirmed
No apparent distress from bathroom environment. If child covers ears or flinches, apply modification (music on, close lid before flush).
Timer Visible
Child can see how much time remains. "We sit until the timer stops." This is the neutral authority — not the parent.
Relaxation Support Offered
For bowel sits: offer pinwheel, bubble tube, or straw to blow. Blowing activates diaphragm + relaxes pelvic floor. This is therapeutic positioning, not entertainment.
Silent Expectancy Maintained
During the sit, minimal verbal demands. Soft background music acceptable. Parent nearby but not hovering. No repeated "are you done?" questions — the timer holds the time.
🟢 Ideal
Child sits calmly, eliminates, completes sequence
🟡 Acceptable
Child sits for full duration without eliminating — still reinforce sitting
🔴 Concerning
Screaming, self-injury, vomiting from distress — exit calmly, note data, consult clinical team

Step 4 of 6
Repeat & Vary — The Timed Toileting Schedule (The Dosage)
Phase | Interval | Rationale | |
Week 1–2 | Every 30–45 minutes waking hours | Catch natural elimination cycle; build success | |
Week 3–4 | Every 45–60 minutes | Consolidate; begin tracking dry/wet patterns | |
Week 5–8 | Every 60–90 minutes | Extend as success rate rises | |
Week 9+ | 90–120 minutes + child-initiated | Transitioning toward self-initiation |
Always Include These Sits Regardless of Schedule
- Immediately upon waking
- 20–30 minutes after every meal (gastrocolic reflex timing)
- Before leaving home
- Before sleep
Variation Options — Keep Engagement Across Days
Seat Variety
Same materials, different seat covers — variety within routine
Music Rotation
Introduce child's preferred music for different days of the week
Reinforcer Choice
Let child select reinforcer from a visual menu — choice-making within structure
Blowing Toy Rotation
Pinwheel → bubbles → party blower across different days for bowel training
"3 calm sits are worth more than 10 forced sits. Always." When a child begins scripting, stimming intensely, or fixating on an unrelated object — this is a satiation signal. Honor it. End the sit. Reinforce what was accomplished.
Step 5 of 6
Reinforce & Celebrate — The ABA Engine That Makes It Work
Behavior that is reinforced increases. The reinforcement must be: IMMEDIATE (within 3 seconds), SPECIFIC (name what they did), and HIGH-VALUE (matched to THIS child's actual interests — not generic praise).
Behavior | Reinforce With | |
Entering bathroom | Warm verbal praise: "You walked to the bathroom! Amazing!" | |
Approaching toilet | "You're doing it!" + token placed on board | |
Sitting on toilet (even briefly) | Verbal praise + token (this is BIG) | |
Sitting for full timer duration | Token + preview of reinforcer | |
Eliminating on toilet | Full high-value reinforcer delivery + enthusiastic praise | |
Completing full sequence | Maximum reinforcer + family celebration |
Reinforcement Menu Template — Customize for Each Child
📱 Preferred Video Clip
2 minutes of their favorite content — delivered immediately and specifically
🧸 Favourite Toy Access
5 minutes with a preferred toy earned through a complete sit
🎵 Favourite Song
Their one specific song played once — powerful and precise
⭐ Stars on Chart
Visual, concrete progress toward a larger earned reward
"Celebrate the attempt. Always. Celebrate the success. Enthusiastically. Celebrate the sitting. Even when nothing happened — sitting was a WIN."

Step 6 of 6
⏱️ 1–2 minutes
The Cool-Down — Neurological Closure
Why cool-down is non-negotiable: Abruptly ending a toilet session and returning to a busy environment can cause post-session dysregulation. The cool-down signals neurological closure: this event is complete, the next event is beginning.
Parent Script for Ending the Sit
💬 "Two more seconds... one more second... ALL DONE! Great job! [Deliver reinforcer]. Now let's flush together, wash our hands, and go play."
A smooth exit sequence reinforces the child's sense of completion and safety. Over time, this cool-down becomes its own predictable routine — one that actually makes the next bathroom visit easier to initiate.
If Child Resists Ending — Wants to Stay or Play in Bathroom
- Use transition visual: first-then board (first bathroom done, then preferred activity)
- Offer bathroom-associated preferred item to carry out (their visual schedule card, a toy they brought in)
- Count down from 5 with visual: "5 more seconds…"
- Never force physical removal — negotiate and exit with dignity

Capture the Data — Right Now
"60 Seconds of Data Now Saves Hours of Guessing Later"
Data collection is not a clinical burden — it is the navigation system that tells you what to do next. Without it, every difficult week looks identical. With it, you can see exactly when to adjust the schedule, when to change the reinforcer, and when to celebrate.
Field | What to Record | Why | |
🕐Time of sit | Time, duration (e.g., 9:15am, 3 min) | Identifies natural elimination pattern | |
💧Outcome | Urinated ✅ / Bowel movement ✅ / Dry (nothing) / Wet before sit / Accident after | Drives schedule optimization | |
😊Behavior score | 1 (distressed) / 2 (tolerating) / 3 (calm) / 4 (engaged) / 5 (initiated) | Tracks comfort trajectory |
Optional Notes Field — Record After Each Session
- Any resistance at which step?
- Which reinforcer was used? Did it work?
- Any unusual factors today?
📥 Download Data Sheet
📊 GPT-OS® Integration
7 days of data = AI-powered insight. Connect to GPT-OS® → pinnacleblooms.org/gpt-os

Real Sessions Aren't Perfect. Here's Your Fix for Every Common Problem.
Session abandonment is not failure — it is data. Every difficult session tells you something precise and actionable about your child's neurological state.
Problem 1: Child Sits But Holds Everything In, Then Has Accident Immediately After Leaving
Why: Anxiety prevents pelvic floor relaxation while on toilet. Child eliminates when the anxiety trigger is removed. Fix: Extend post-toilet time in bathroom (pants up, but stay). Relaxation blowing during sit. Check positioning — feet on stool? OT consult for pelvic floor relaxation techniques.
Problem 2: Child Refuses to Enter the Bathroom at All
Why: Bathroom has been paired with negative experiences. Sensory environment is overwhelming. Fight-or-flight before the door. Fix: Start from 5 meters away. Reinforce any closer approach. Bring preferred activity INTO bathroom (don't link to toilet yet). Sensory kit FIRST — make bathroom feel safe before starting toilet work.
Problem 3: Child Screams When Placed on Toilet Seat
Why: Falling-in sensation, cold surface, instability, or prior forced placement. Fix: Seat insert with handles immediately. Footstool. Padded seat. Try potty chair on floor first. Never place on toilet against their will — only invite. Gradual desensitization: sit on toilet clothed first.
Problem 4: Child Sits Happily But Never Eliminates on Toilet
Why: Schedule doesn't match elimination pattern. Interoception too low to feel urgency. Fix: Review data — when ARE accidents happening? Adjust schedule to be 15 min BEFORE typical accident time. Increase fluid intake for more practice opportunities. Interoception training to build signal awareness.
Problem 5: Child Is Terrified of the Flush Sound
Why: Sensory hypersensitivity to sudden loud sounds. Flush = unpredictable auditory assault. Fix: Child leaves bathroom BEFORE flush. Lid down before flushing muffles sound. Verbal countdown: "Flush in 3-2-1." Noise-canceling headphones during flush. Let child control flush button when ready — agency reduces fear.
Problem 6: Bowel Withholding / Will Only Defecate in Diaper
Why: Diaper is the learned elimination trigger. Toilet = wrong sensory context for bowel release. May have constipation history. Fix: Medical clearance first. Gradual shaping: defecate in diaper → in bathroom → standing → on toilet with open diaper → with cut diaper → on toilet. Maintain preferred position initially.
Problem 7: Good Progress Then Sudden Regression
Why: Illness, life change, new sibling, school transition, anxiety spike, or inconsistency in caregiver approach. Fix: Identify trigger. Return to earlier phase temporarily. No pressure. Maintain routine. "Regression is the nervous system asking for more support — not less." Consult helpline: 9100 181 181
One Technique. Infinite Personalizations.
Your child is not a protocol. The protocol adapts to your child. Use the difficulty levels and sensory profile adaptations below to calibrate every session to your child's exact starting point.
Difficulty Slider: Start Where Your Child Is — Not Where You Think They Should Be
Level | Adaptation | |
Level 1 — Easiest | Bathroom approach only. No toilet contact required. Just enter, look, leave. Reinforce. | |
Level 2 | Touch toilet seat clothed. No sitting required. Reinforce touch. | |
Level 3 | Sit clothed on toilet seat. Timer 1 minute. Reinforce sitting. | |
Level 4 | Sit unclothed. Timer 3–5 minutes. Reinforce duration. | |
Level 5 — Standard | Full protocol: sit, timer, eliminate (if pattern hits), reinforce outcome. |
Sensory Profile Adaptations
Profile | Adjustment | |
🔊 Sound-sensitive | Ear protection during flush. Music during sit. Verbal warnings for all sounds. | |
🌡️ Touch-sensitive | Maximum padding on seat. Warm everything. Minimize novel textures. | |
💡 Light-sensitive | Nightlight only. No overhead fluorescent. | |
🤸 Sensory seeker | Weighted lap pad during sit. Vibrating cushion. Resistive activities before sits. | |
🗣️ Non-speaking | AAC/PECS for "toilet" request. Visual schedule only. No verbal demands. | |
👶 Very young (2.5–4) | Potty chair on floor. Parent sits on floor with child. Maximum playfulness. | |
👦 Older child (8+) | Privacy and dignity paramount. Peer-appropriate social story. No infantilizing language. |
Age-based modifications in brief: Under 3: potty chair, 2-min sits, high-frequency reinforcement · Ages 3–6: standard protocol, visual schedule + timer central · Ages 7–12: privacy, dignity, child chooses reinforcer · Ages 12+: adolescent protocol, specialist BCBA consult

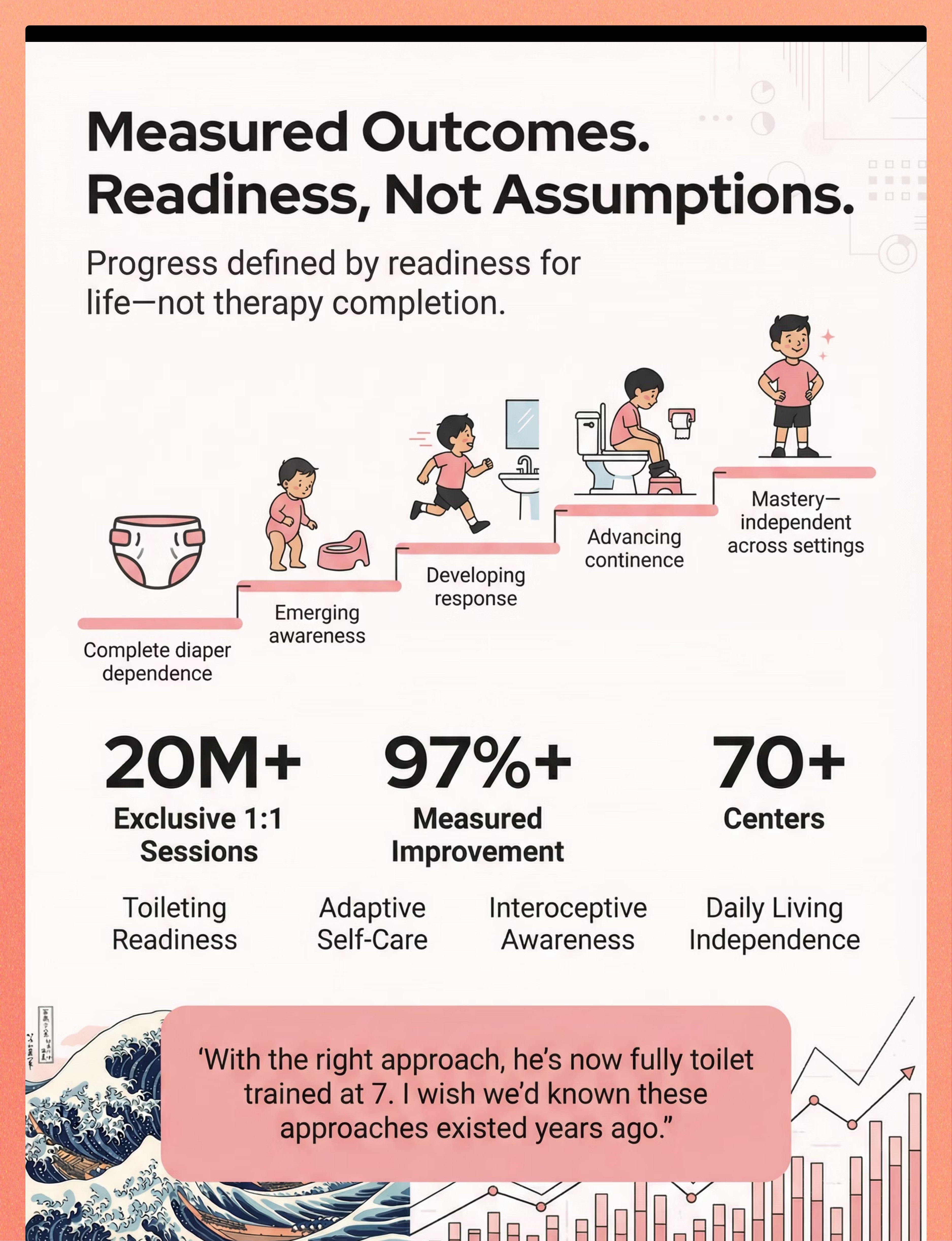
📈 Progress
Weeks 1–2: The Tolerance Phase
Weeks 1–2: The Tolerance Phase
Progress bar: ▓░░░░░░░░░ 15% — You have started. That is everything.
What "Progress" Looks Like Right Now
- Child enters bathroom without immediate meltdown (even with reluctance)
- Child tolerates sitting on toilet for 30+ seconds (even if upset)
- Any elimination on toilet — even once, even accidentally
- Parent completes every scheduled sit for 7 days straight (consistency = progress)
- Data tracking is happening
What Is NOT Progress Yet — Manage Expectations
- Self-initiating toilet trips (this is weeks away)
- Consistent dry periods between sits (pattern emerging, not established)
- Child "understanding" the connection (this builds over weeks, not days)
- Night dryness (this is physiological — months to years, a separate goal)
"In weeks 1–2, you may feel like nothing is working. This is normal. Neural pathways are forming beneath the surface. A child who sits for 30 seconds today and screamed for 30 minutes two weeks ago? That is measurable, meaningful progress."
"If your child tolerates the bathroom for 60 seconds longer than they did last week — that is real progress. Document it. Celebrate it. Build on it."
Research: PMC11506176 — Early-phase outcomes focus on tolerance and participation, not mastery

📈 Progress
Weeks 3–4: Consolidation Phase
Weeks 3–4: Neural Pathways Are Forming — Watch for These Signals
Progress bar: ▓▓▓▓░░░░░░ 40% — Neural pathways are forming. Watch for these signals.
🔵 Reduced Resistance to Bathroom Routine
Less active protest; more passive acceptance; occasionally cooperative — this is measurable movement.
🔵 Anticipation Behavior
Child moves toward bathroom when timer sounds without full prompting — the hippocampus is encoding the new routine.
🔵 Increased Tolerance Duration
Sits for 3–5 minutes without active distress. Duration is the neurological indicator of safety.
🔵 First Spontaneous Signals
Child may gesture toward bathroom, bring visual card, or vocalize in proximity to bathroom — celebrate every one of these moments.
🔵 Post-Accident Awareness Increasing
Child appears to notice wet/dirty sooner than in week 1. Interoception is waking up.
"You may notice you are more confident. The routine feels less like a battle and more like a rhythm. That shift in YOUR nervous system is also real progress — and it feeds back into your child's regulation."
When to increase intensity: If dry periods between sits are extending → increase sit interval by 15 minutes · If child is initiating occasionally → increase reinforcement for ANY initiation · If bowel training hasn't begun → introduce bowel-specific kit now (Card 9, Material 9)
📈 Progress
Weeks 5–8: Mastery Phase
Weeks 5–8: Mastery Phase — When You Know It's Working
Progress bar: ▓▓▓▓▓▓▓▓░░ 75% — Mastery approaching. Check these criteria.
Criterion | Not Yet | Approaching | Mastery | |
Dry periods | <30 min | 60–90 min | 90+ min consistently | |
Self-initiation | 0 times/week | 1–3 times/week | Daily or near-daily | |
Full sequence | Needs full prompting | 3–5 steps independent | Full sequence independent | |
Elimination on toilet | Rare or accidental | 3+ times/day | Consistent across all sits | |
Resistance | High most sits | Low most sits | Minimal or absent | |
Generalization | Home only | Home + 1 other setting | Multiple settings |
🏅Toileting Mastery Badge earned when: 7 consecutive days of 80%+ dry, self-initiated or minimally prompted toilet use, across at least 2 settings.
When to Move to Next Level
- Daytime mastery achieved → Begin nighttime training (separate, physiological, slower)
- Home mastery → Generalize to school / community settings
- Urine mastery → Intensify bowel training protocol if still incomplete
Research: PMC10955541 — Mastery criteria from behavioral measurement standards | BACB mastery criteria: 80%+ correct responding across 3+ sessions

You Did This.
Your child grew because you showed up — every scheduled sit, every difficult session, every time you reinforced the attempt not just the outcome. That is what changed everything.
✅ You transformed a bathroom from a sensory threat to a safe routine
✅ You built interoceptive awareness in a nervous system that didn't have it
✅ You created a reinforcement system that made this worth doing
✅ You maintained consistency when results weren't visible yet
"Your child is progressing toward toilet independence — because of what you did."
📝Write down:"What did my child do today that they couldn't do 8 weeks ago? That gap — that is the measurement of your impact."
🎉Did your child reach a toilet training milestone? Share your story in the Pinnacle Family Community — your journey helps other families believe it's possible. Join Community → pinnacleblooms.org/community

Trust Your Instincts — If Something Feels Wrong, Pause and Ask
These are the specific clinical thresholds that require professional consultation. When in doubt, call first and continue later.
🚩 Red Flag | What It Looks Like | What To Do | |
Severe distress persisting | Every session ends in 10+ minutes of inconsolable distress after 4+ weeks | Stop current protocol. Seek OT / BCBA re-assessment. Sensory or trauma evaluation needed. | |
Self-injury related to toileting | Child hits, bites, or bangs head in relation to bathroom routine | Immediate clinical consultation. This exceeds home protocol scope. | |
Bowel withholding → constipation | No bowel movement for 3+ days, hard stools, abdominal discomfort | Pediatrician immediately. No behavioral intervention before medical management. | |
Blood in stool or urine | Any time | Emergency medical evaluation. Stop all intervention. | |
Sudden total regression + behavioral change | Previously trained, now complete refusal + personality changes | Rule out medical cause (UTI, GI condition), trauma exposure, or environmental stressor. Clinical consult. | |
No progress in 8+ weeks of consistent protocol | All 9 materials, consistent daily implementation, zero measurable progress | Intensive toilet training assessment by experienced OT + BCBA team. Pinnacle specialist referral. |
📞FREE 24×7 Helpline: 9100 181 181 · 16+ languages Speak directly to a Pinnacle clinical team member — no appointment needed.
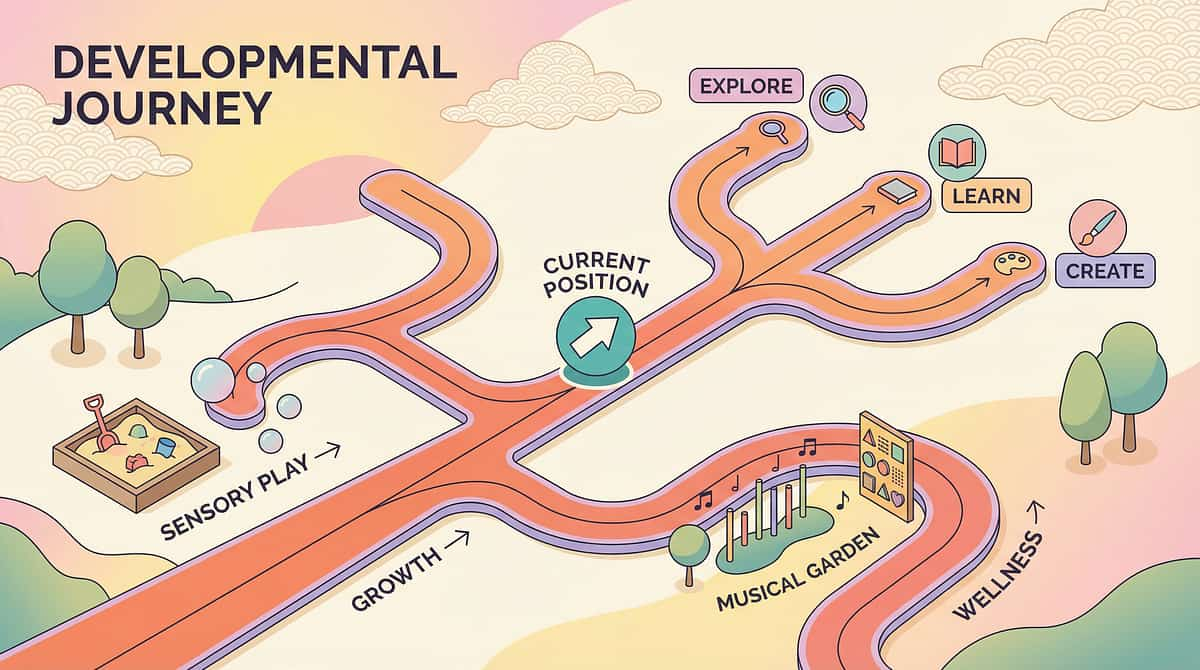
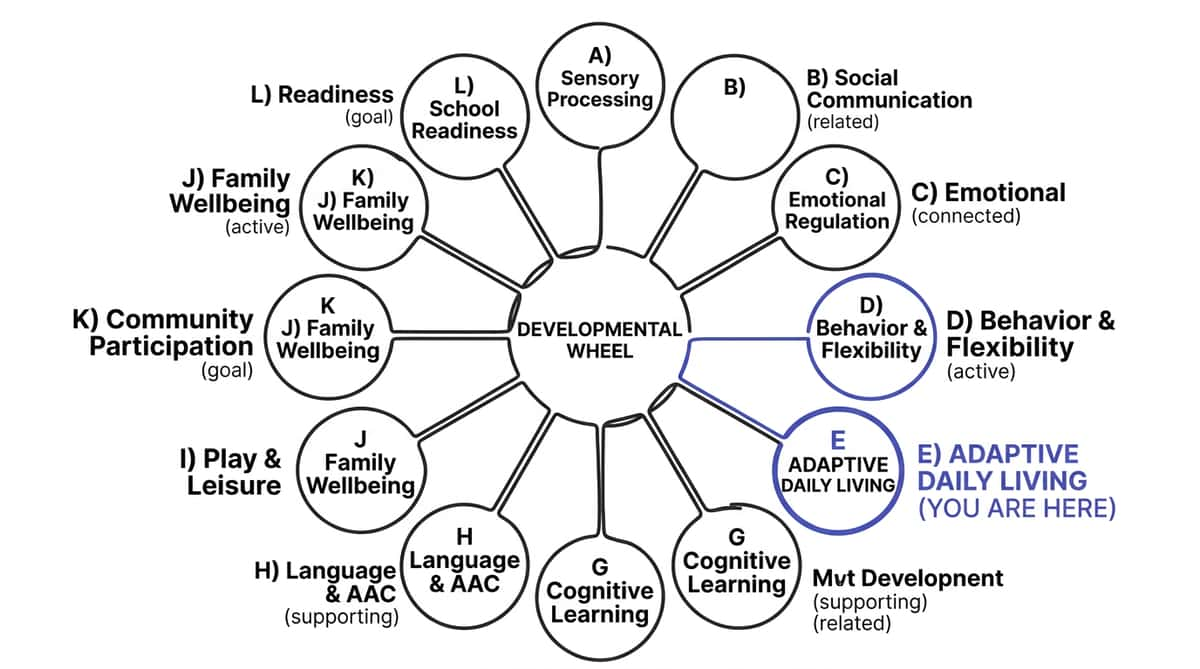
You Are Here. Here Is Where This Leads.
Toilet training is not a single technique — it is a progression through a cluster of interconnected skills. This map shows you exactly where E-492 sits and where to go next based on your child's response profile.
Prerequisites (Before E-492)
📍 YOU ARE HERE — E-492: 9 Materials That Help With Autism Toilet Training

Also in the Toileting Cluster — Techniques You May Need
Domain E: Adaptive Daily Living Skills | Sub-cluster: Toileting (E-491 to E-520). Select the technique that matches your child's current primary challenge.
9 Materials That Help With Toilet Training Readiness
E-491 | 🟢 Intro Level → View E-491
9 Materials That Help With Nonverbal Toilet Training
E-493 | 🟡 Core Level → View E-493
9 Materials That Help With Interoception for Toileting
E-494 | 🟡 Core Level → View E-494
9 Materials That Help When Child Refuses Toilet Sitting
E-495 | 🔴 Advanced Level → View E-495
9 Materials That Help With Toilet Fear
E-496 | 🟡 Core Level → View E-496
9 Materials That Help After Toilet Regression
E-512 | 🟡 Core Level → View E-512
🔗Related in Sensory Domain:A-037: 9 Materials That Help When Child Fears Toilet Flush🔗Related in Emotional Regulation:C-289: 9 Materials That Help With Toilet Fears
One Technique. Twelve Domains. One Child. One Integrated Plan.
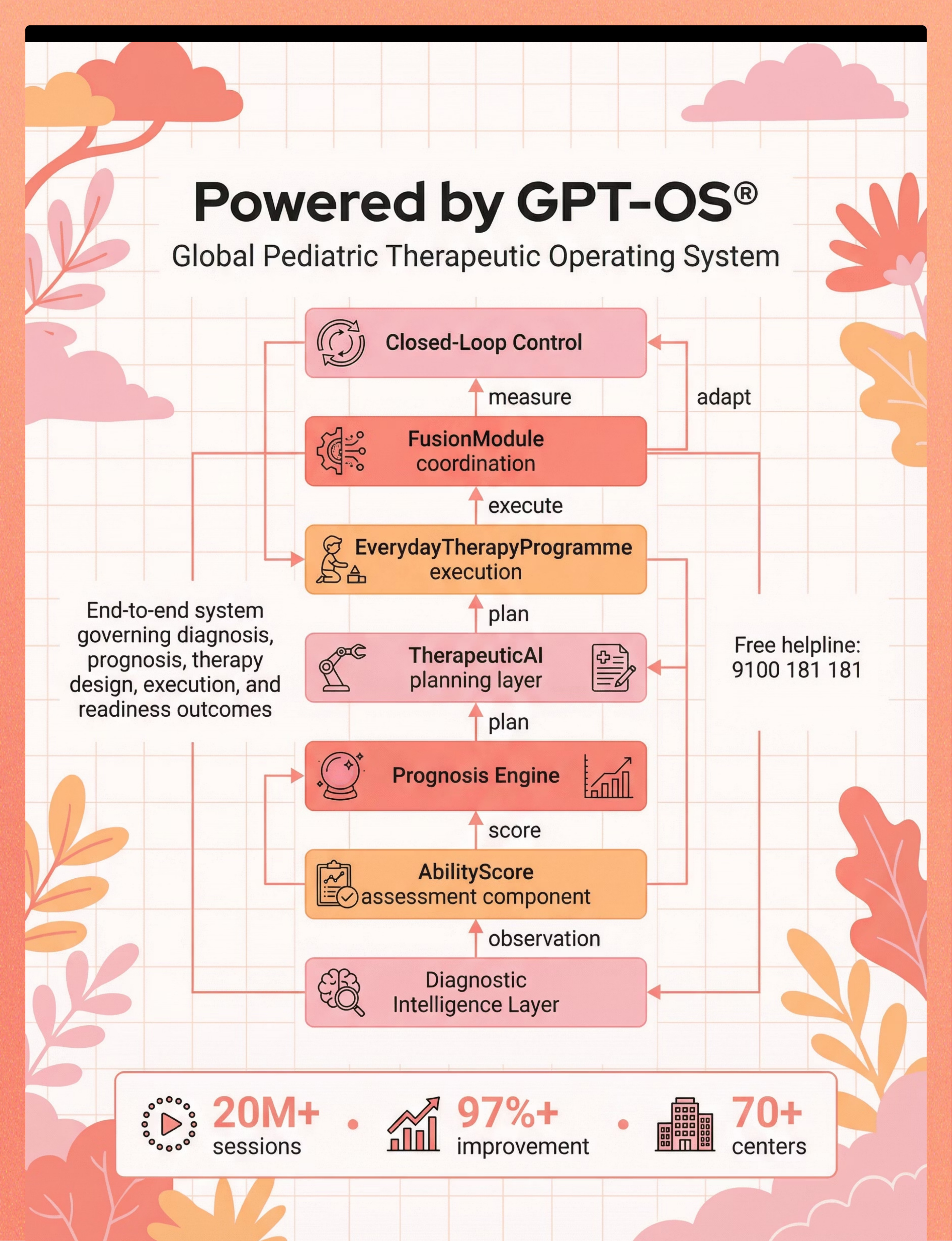
GPT-OS® Integration
"This technique is one piece of a larger plan. GPT-OS® coordinates all 12 domains into a single personalized developmental pathway for your child."
AbilityScore® Assessment
Has your child had an AbilityScore® assessment? It maps developmental status across 349 skills and 79 abilities — establishing the exact starting point for every intervention.
Real Journeys. Real Timelines. Real Outcomes.
Anonymized clinical narratives from the Pinnacle network. Behavioral specificity, not marketing. Individual results vary.
Aryan, 6 years — Hyderabad
Before: Aryan had never sat on the toilet without screaming. Still fully diaper-dependent at 6. The flush sound caused 20-minute meltdowns. His parents had stopped attempting toilet training after 18 months of failed tries. The school was threatening to move him to a special class due to toileting needs.
Intervention: OT-led sensory bathroom modification first (6 weeks). Then visual schedule introduction. Reinforcement system using Aryan's special interest in trains.
After (10 months): Aryan is fully daytime toilet independent. He carries his train token board to the bathroom himself. The flush still requires a warning countdown, but there are no meltdowns. He maintained his school placement.
"I used to dread every diaper change. Now he walks to the bathroom by himself and comes out showing me his token board. I still can't believe it." — Aryan's mother
Therapist's Note: "The critical unlock for Aryan was the sensory kit first — before any behavioral protocol. His nervous system couldn't process the toilet attempt through the bathroom's threat level. Once we modified the sensory environment, the behavioral pieces fell into place within weeks." — Pinnacle OT Specialist
Kavya, 7 years — Bengaluru
Before: Kavya would only have bowel movements in her pull-up, standing behind the sofa. She showed no awareness of wetness for hours. The family had tried 5 different approaches over 3 years.
Intervention: Interoception training 8 weeks before introducing toilet. Moisture-sensing alarm. Timed schedule matching her identified post-meal pattern. High-value reinforcer: specific 3-minute video clip.
After (8 months): Kavya is urinating on toilet independently. Bowel training is at 70% — she signals need approximately half the time. The moisture alarm created the connection her interoception couldn't.
"When the clinical team explained interoception, everything made sense for the first time. She literally couldn't feel it. That wasn't her fault. That changed how we approached everything." — Kavya's father
Individual results vary. Outcomes drawn from aggregate Pinnacle network data. 20M+ therapy sessions · 97%+ measured improvement rate.

Isolation Is the Enemy of Progress. You Don't Have to Do This Alone.
🟢 WhatsApp Groups
Join: Autism Toilet Training India Parent Group — Moderated by Pinnacle clinical team. Real parents, real strategies, real time.
💬 Online Forum
Pinnacle Parent Community Forum: Adaptive Daily Living — Post questions, get responses from experienced parents and clinicians.
📍 Local Parent Meetups
Pinnacle centers in 70+ locations host monthly parent support groups. → Center Locator · pinnacleblooms.org/centers
🤝 Peer Mentoring
Connect with a parent who has been through autism toilet training and is 12+ months out the other side. → Request a Peer Mentor · pinnacleblooms.org/peer-mentoring
"Your experience — the strategies that worked, the ones that didn't, the 3am panic messages — that experience is medicine for another family just starting this journey. Consider sharing it."
📞FREE Helpline: 9100 181 181 · 24×7 · 16+ Languages
📞 Get Help
Home + Clinic = Maximum Impact
These 9 materials work. They work even better when supported by a professional who knows your child. Three pathways — choose the one that fits your family right now.
🏥 In-Person Assessment
AbilityScore® + Toileting Readiness Assessment + Sensory Processing Evaluation. 70+ centers across India. → Book Assessment
💻 Teleconsultation
For families outside major cities or who prefer remote support. 30-minute video consultation with a specialist matched to your child's profile. → Book Teleconsultation
🏠 EverydayTherapyProgramme™
Home-based structured daily program generated by GPT-OS® and monitored by your assigned therapist team. Toilet training module included. → Start EverydayTherapyProgramme™
Discipline Matching for E-492
Challenge | Who to See | |
Sensory bathroom resistance | Occupational Therapist | |
Behavioral protocol design | BCBA / ABA Therapist | |
Communication for toileting | Speech-Language Pathologist | |
Medical co-factors | Developmental Pediatrician | |
Comprehensive integrated plan | GPT-OS® FusionModule™ team |
📞FREE Helpline: 9100 181 181 · 24×7 · 16+ Languages · pinnacleblooms.org/centers
For the Parent Who Wants the Full Science
Deeper reading. Every claim on this page is sourced. Here is where to go. All studies peer-reviewed and accessible via PubMed and WHO repositories.
🔬 Systematic Review (2024) — Level I
PRISMA methodology: 16 studies (2013–2023) confirm behavioral + sensory interventions for autism adaptive skill acquisition meet evidence-based practice criteria. → PMC11506176
📊 Meta-Analysis (2024) — Level I
24 RCTs analyzed: sensory integration + behavioral interventions promote social skills, adaptive behavior, sensory processing, and motor skills in ASD. → PMC10955541 | DOI: 10.12998/wjcc.v12.i7.1260
🇮🇳 Indian RCT (2019) — Level II
Home-based sensory and behavioral interventions: statistically significant outcomes in Indian ASD pediatric population. Padmanabha et al., Indian Journal of Pediatrics. → DOI: 10.1007/s12098-018-2747-4
🌍 WHO Nurturing Care Framework (2018) — Level I Policy
Equity-focused, context-specific home interventions as essential pediatric health infrastructure. → WHO NCF
✅ NCAEP Evidence-Based Practices Report (2020) — Level I
Visual supports, video modeling, token economies, and behavioral intervention classified as EBPs for autism across adaptive skills domains. → NCAEP 2020 Report

Your Data. Your Child's Algorithm. Every Family's Future.
What GPT-OS® Learns from E-492 Data Specifically
Material Effectiveness Ranking
Which of the 9 materials produced the fastest tolerance increase for this child's specific sensory profile
Reinforcer-Outcome Correlation
Which reinforcement type showed highest elimination rate correlation — driving menu optimization
Optimal Sit Interval
This child's personal elimination pattern mapped from 7+ days of data to optimize scheduling
Predicted Independence Timeline
Given current trajectory, when daytime independence is statistically likely — with confidence intervals
🔒 All session data is encrypted, anonymized for population-level analysis, and never shared with third parties. DPDP Act 2023 compliant. Privacy Policy → pinnacleblooms.org/privacy20M+ sessions · 97%+ improvement · 591+ observations · 349 skills · 79 developmental abilities — all converging on one child's personalized plan.
The Reel That Brought You Here
🎬 Reel ID: E-492
9 Materials That Help With Autism Toilet Training
📂 Series
Adaptive Daily Living Skills in Autism — Episode 492 of 999
🎯 Domain
Domain E — Adaptive Daily Living Skills
📹Watch E-492 Reel:Watch on Pinnacle YouTube Channel → youtube.com/pinnacleblooms💬 "In this reel, our consortium OT and BCBA specialists walk you through each of the 9 materials — showing exactly what they look like in a real home bathroom, how to introduce each one, and what a successful session looks like. Watch before your first implementation session."
Related Reels in This Cluster
Reel ID | Title | |
E-491 | 9 Materials That Help With Toilet Training Readiness | |
E-493 | 9 Materials That Help With Nonverbal Toilet Training | |
E-494 | 9 Materials That Help With Interoception for Toileting | |
A-037 | 9 Materials That Help When Child Fears Toilet Flush | |
C-289 | 9 Materials That Help With Toilet Fears |
Research: NCAEP 2020 — Video modeling classified as evidence-based practice for autism | Multi-modal learning (visual + text + demonstration) improves parent skill acquisition

Consistency Across All Caregivers Multiplies Impact 3×
If only one parent knows the protocol, it works for 8 hours a day. If everyone does — it works 24×7. Share this page with every adult who cares for your child.
Downloadable Resources
📥 Family Guide — 1-Page PDF
Simplified version for sharing with grandparents, school staff, and extended family caregivers. Download Family Guide PDF
📥 Daily Data Tracking Sheet
The same 3-field tracker from Card 20, printable for home use. Download Tracker PDF
📥 Visual Schedule Template
Printable toileting visual schedule — photograph your bathroom, cut, laminate. Download Visual Schedule PDF
📥 School Communication Template
For toilet training accommodation requests to teachers and administrators. Download School Template PDF
💬"Explain to Grandparents":"[Child's name] is learning to use the toilet in a way that works for how their brain processes things. They need: the picture schedule on the wall, the special seat, the timer, and [their reinforcer]. Please use these same tools every time — consistency is the therapy."
Questions Every Parent Asks — Answered by the Pinnacle Consortium
Q: My child is 8 years old and still in diapers. Is it too late?
It is never too late. Toilet training in autism does not have a cutoff age. Research documents successful toilet training in adolescents and adults with appropriate intervention. The timeline in autism is different, not limited. Call 9100 181 181 for an age-appropriate protocol consultation.
Q: How long will toilet training take with these 9 materials?
There is no universal timeline. For children with moderate interoceptive differences and sensory sensitivity: 3–6 months of consistent implementation is typical for daytime training. Some children achieve independence in 8–12 weeks; some need 12–18 months. Nighttime training is a separate, longer process. What matters is consistent daily implementation, not speed.
Q: My child's school wants them toilet trained. What do I tell them?
Download the School Communication Template from Card 37. Toilet training for autistic children is an active medical-educational intervention — not a parenting preference. An IEP/504 accommodation for scheduled bathroom breaks and sensory supports is both appropriate and legally supportable. Pinnacle can provide documentation. Call 9100 181 181.
Q: Should I use pull-ups or underwear during training?
Research supports transitioning to thin cotton underwear during waking training hours because the more immediate sensation of wetness provides more feedback. Maintain pull-ups or diapers for sleep until daytime mastery is solid. Discuss this with your OT/BCBA — individual factors matter.
Q: My child was doing well, then completely regressed. Why?
Regression is part of the autism toilet training journey. Common triggers: illness, life changes (new sibling, school transition, move), anxiety spike, inconsistency in protocol across caregivers. Return to an earlier protocol phase without pressure. Rule out medical causes (UTI, constipation). Regression is temporary when protocol resumes consistently.
Q: Can I use these materials for a non-speaking child?
Yes. The materials are specifically designed to work without verbal communication. Visual schedules work for non-speaking children. The first-then board replaces verbal instruction. The reinforcement system uses preferred items, not verbal praise. For AAC-using children, a "toilet" symbol can be added to their communication system. See
Q: My child is afraid of the flush. How do I handle it?
(1) Child leaves bathroom before flush always. (2) Close lid before flushing to muffle sound. (3) Verbal countdown: "Flush in 3-2-1." (4) Noise-canceling headphones for flush phase. (5) Let child push the flush button when ready — agency reduces fear. (6) Gradual desensitization program with OT. See: A-037: 9 Materials That Help When Child Fears Toilet Flush
Q: I've tried everything. Nothing works. What now?
If you have implemented all 9 materials consistently for 8+ weeks and seen no progress, this indicates a need for intensive professional assessment. Factors to rule out: undiagnosed constipation, UTI, anatomical factors, trauma response, motor planning challenges. An intensive toilet training program delivered by an OT+BCBA team can achieve what home implementation cannot. Call 9100 181 181 — this is exactly what the helpline exists for.
💬"Didn't find your answer? Ask GPT-OS® at pinnacleblooms.org/ask"📞"Still need help? Book a teleconsultation — pinnacleblooms.org/teleconsult"

"You Know What Your Child Needs." "Now Give It to Them."
You have the science. You have the materials. You have the protocol. The only thing left is to start.
✦ VALIDATED BY THE PINNACLE BLOOMS CONSORTIUM ✦ 🖐️ OT · 💬 SLP · 📊 ABA · 📚 SpEd · 🧠 NeuroDev · 🩺 Pediatrics
20M+
Therapy Sessions
97%+
Improvement Rate
70+
Centers & Countries
Preview of 9 materials that help with autism toilet training Therapy Material
Below is a visual preview of 9 materials that help with autism toilet training therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.










Link copied!

⬡ Pinnacle Blooms Network®
Multi-Disciplinary Pediatric Therapy Consortium OT · SLP · ABA/BCBA · SpEd · NeuroDev Pediatrics · CRO
"From fear to mastery. One technique at a time."
This page is part of the Pinnacle GPT-OS® Technique Library — 70,000+ evidence-linked, parent-empowering intervention technique pages hosted at techniques.pinnacleblooms.org. Each page is developed by the Pinnacle Blooms Consortium and reviewed against current PubMed literature, WHO/UNICEF frameworks, and Pinnacle's 20M+ session clinical data.
Navigate This Page
📞FREE National Autism Helpline · 9100 181 181 · 24×7 · 16+ Languages🌐pinnacleblooms.org · ✉️care@pinnacleblooms.org
⚠️This content is educational. It does not replace individualized assessment and intervention from licensed occupational therapists, BCBAs, developmental pediatricians, or related specialists. Delayed toilet training may indicate underlying medical conditions requiring evaluation. Always consult your child's healthcare team before making significant changes to toileting approaches. Medical causes of toileting difficulties should be ruled out first. Individual results may vary. Statistics represent aggregate outcomes across the Pinnacle Blooms Network.
© 2025–2026 Pinnacle Blooms Network®, unit of Bharath Healthcare Laboratories Pvt. Ltd. All rights reserved. GPT-OS®, TherapeuticAI®, AbilityScore®, EverydayTherapyProgramme™, FusionModule™ are proprietary trademarks of Pinnacle Blooms Network®. Global IP protection filed.
CIN | U74999TG2016PTC113063 | |
DPIIT | DIPP8651 (Govt. of India Startup India) | |
MSME | Udyog Aadhaar: TS20F0009606 | |
GSTIN | 36AAGCB9722P1Z2 |
🔄This page ends. The next technique begins.→ E-493: 9 Materials That Help With Nonverbal Toilet Training