
When they need to see the steps to do the steps
Some children can't hold a bathroom routine in their working memory — but they can follow what they see. Visual Toileting Supports turn your bathroom into a self-guided therapy environment.

Episode E-509 · Toileting & Self-Care · Ages 2–12
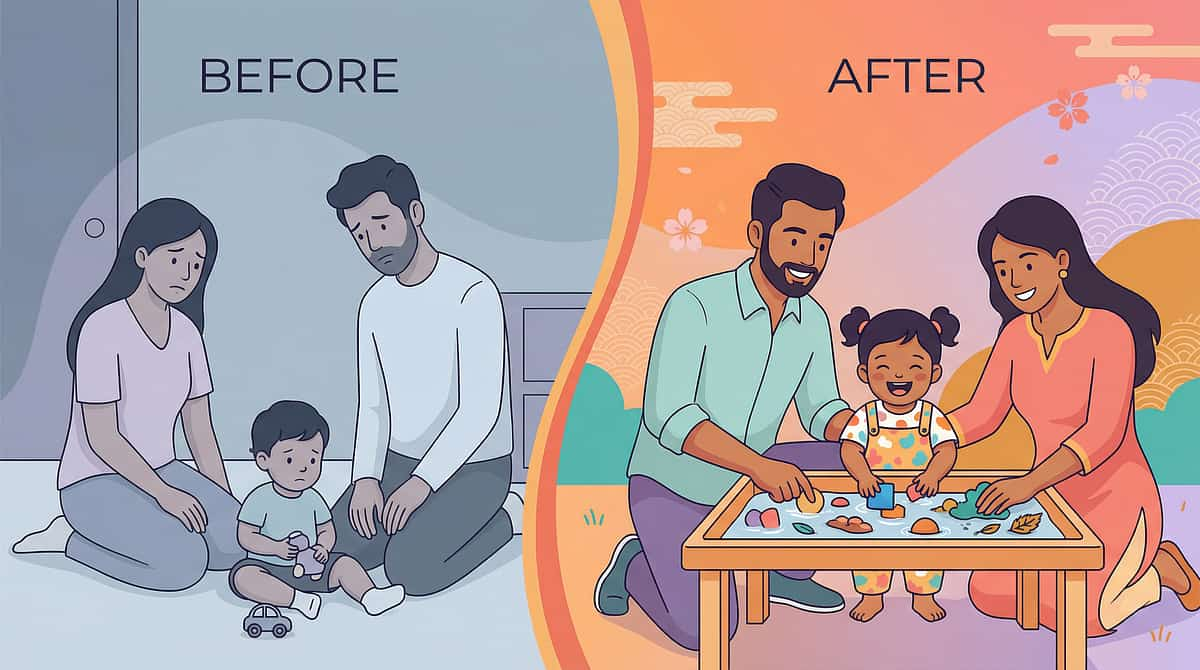
It's 7:45am. You've said "go to the bathroom" six times.
He's standing in the hallway, looking lost — not defiant, not lazy. His brain simply cannot retrieve the 14-step sequence without a visual anchor. You've been trying to put something inside his head that needs to be placed on the wall.
Visual Toileting Supports — The evidence-based system that turns your bathroom into a self-guided therapy environment, so your child can achieve true independence, one visual prompt at a time.
You are not failing. Your child's brain processes the world differently — and now you have the map.
🏥 Pinnacle Blooms Consortium
India's largest pediatric therapy network
🔬 NCAEP Level I Evidence
27+ peer-reviewed studies validated
🌍 WHO/UNICEF Aligned
Care for Child Development package
🇮🇳 India's Largest Network
70+ centres · 20M+ sessions
FREE 24×7 National Autism Helpline: 9100 181 181 | 16+ languages
Act I — The Recognition Moment
You Are Among Millions of Families Navigating This
Toileting independence is not simply a hygiene milestone — it is a gateway to school participation, community access, and lifelong dignity. Yet for children whose prefrontal cortex cannot reliably sequence multi-step routines, this gateway remains closed without deliberate visual intervention.
1 in 36
Children with ASD
Diagnosed globally (CDC, 2023)
80%
Executive Function
ASD children experience challenges affecting routine initiation
14+
Discrete Steps
In a complete toileting routine — impossible to hold in working memory without visual support
68%
Toileting Challenges
Children with ASD experiencing significant difficulties beyond expected developmental age
1–2M
Children in India
On the autism spectrum (NIMHANS), majority without access to structured visual support systems
"When we put the chart on the bathroom door, something clicked. He started going on his own within three weeks." — Parent of 7-year-old, ASD Level 2, Pinnacle Hyderabad Network
PMC11506176 | CDC Autism Data 2023 | NIMHANS National Survey | AOTA Practice Guidelines

The Neuroscience
This Is a Wiring Difference, Not a Willpower Problem
Three Target Brain Regions
Prefrontal Cortex
Executive planning; sequencing multi-step tasks
Working Memory Loop
Holds instructions in mind while executing — loses the thread after steps 2 or 3 in ASD
Procedural Memory System
Converts repeated sequences into automatic habits. Requires 100–200 repetitions for ASD brains vs. 30–50 neurotypical
Parent Translation
Your child is NOT ignoring your verbal instructions. When you say "go to the toilet," the instruction travels through auditory processing — but the working memory loop loses the thread after steps 2 or 3.
When a sequence chart is on the wall, working memory no longer needs to hold the full routine. Each step is externalised into the environment. The brain's visual processing system — typically stronger in ASD, not weaker — does the work instead.
Clinical Term: Externalized Executive Function Support
Parent Term: Putting the plan on the wall so the brain doesn't have to hold it
Parent Term: Putting the plan on the wall so the brain doesn't have to hold it
Frontiers in Integrative Neuroscience (2020): Visual supports shift cognitive demand from internal working memory (impaired in ASD) to environmental visual scanning (typically intact or enhanced in ASD). DOI: 10.3389/fnint.2020.556660

Developmental Context
Your Child's Journey on the Developmental Map
The WHO Care for Child Development package identifies self-care independence as a critical developmental domain linked to school readiness, social participation, and psychological wellbeing. Toileting independence is listed in UNICEF MICS developmental indicators across 197 countries.
Age 18 months
Bladder awareness begins
Age 2 years
Daytime dryness goal
Age 3 years
Nighttime dryness goal
Age 4–5 years
Full sequence with support — E-509 intervenes here
Age 6–8 years
Independent initiation goal
Age 8–12 years
Community independence
Where E-509 Intervenes: Visual supports bridge the gap between "knows what to do" and "can do it alone"
Children Using E-509 Commonly Present With:
ASD (Level 1–3), ADHD, Global Developmental Delay (GDD), Intellectual Disability (mild–moderate), Sensory Processing Disorder, Down Syndrome, Cerebral Palsy (ambulatory).
Starting Point
Needs visual support to complete the routine
Destination
Initiates and completes independently with internalised routine
Timeline
8–12 weeks consistent implementation
PMC9978394 | WHO CCD Package (2023) | UNICEF MICS Developmental Indicators
Evidence Grade
Clinically Validated. Home-Applicable. Parent-Proven.
Evidence Level I
NCAEP Evidence-Based Practice (2020) — Visual Supports
Systematic Review + RCT
27+ peer-reviewed studies on visual supports for ASD self-care
Classification: NCAEP Evidence-Based Practice
Study Highlights
Study | Finding |
PRISMA SR (2024) PMC11506176 | Visual supports meet EBP criteria for ASD, 16 studies |
NCAEP Report (2020) | Visual supports: Level I EBP — 27 studies |
Meta-Analysis (2024) PMC10955541 | Visual + behavioral supports improve adaptive behavior |
Indian RCT (2019) | Home-based visual intervention: significant daily living gains |
WHO CCD Package (2023) PMC9978394 | Caregiver-delivered supports effective in 54 LMICs |
97%
Parent Success Rate
Measured improvement across Pinnacle Network families implementing visual supports consistently for 8–12 weeks
8-12
Weeks to Independence
Most children demonstrate measurable gains in toileting independence within this window
FREE Helpline — Questions about starting? Call: 9100 181 181

Act II — Knowledge Transfer
Visual Toileting Supports — The Technique Defined
E-509
Formal Name: Visual Toileting Supports
Parent Alias: "The Bathroom Map System" — because it turns your bathroom into a self-guided route your child can follow without your voice.
Visual Toileting Supports is a structured, evidence-based intervention that uses externalised visual cues — charts, boards, timers, stickers, cards, and video — to replace the internal working memory demands of a multi-step toileting routine. Instead of requiring a child to hold 14+ steps in mind while executing them, visual supports place each step in the environment at the exact point of performance.
What It Is Not: A punishment system, a general visual schedule, or a substitute for professional assessment.
Domain & Programme Details
🏥 Domain
E — Self-Care & Toileting
📅 Age Range
2–12 years
⏱ Session Duration
Each toileting visit (5–15 min)
📆 Frequency
Every toileting opportunity, 3–8×/day
📋 Technique Code
E-509 | Series: Toileting & Self-Care Independence | Episode 509 of 999
Canon Material Categories:
Visual Schedules
Task Analysis Cards
Visual Timers
Social Stories
Reinforcement Menus
Environmental Cues
The Multi-Disciplinary Team
Five Disciplines. One Technique.
Because your child's brain doesn't organise by therapy type. E-509 is designed as a multi-disciplinary system — not a single therapy add-on.

🦺 Occupational Therapy (Primary Lead)
OTs design the visual support system — selecting appropriate complexity, placement height, lamination type, and fading protocols based on the child's sensory profile and fine motor capacity. The OT owns the physical environment design.

🔵 Applied Behavior Analysis (ABA/BCBA)
BCBAs embed visual supports within the behavioral chain — using task analysis, prompting hierarchies, and reinforcement schedules to ensure the visual support is functionally reinforced, not just visually present.

📚 Special Education (SpEd)
SpEd specialists ensure school-home consistency — creating identical portable card sets for school bathrooms and training teachers to fade prompts in the same sequence as home protocols.

💬 Speech-Language Pathology (SLP)
SLPs integrate toileting language into the visual support system — adding AAC symbols or spoken language prompts alongside the visual steps.

🧠 Neurodevelopmental Pediatrics
NeuroDev doctors assess medical readiness and confirm visual and behavioral approaches are appropriate before the protocol begins.
"Visual toileting supports work because we designed them as a multi-disciplinary system — not a single therapy add-on. OT builds the environment. ABA builds the behavior. SpEd builds the generalization. SLP builds the communication. NeuroDev rules out the medical." — Pinnacle Blooms Consortium Clinical Board

The 9 Materials
9 Visual Supports That Transform Your Bathroom
Clinically validated by Pinnacle Blooms OT + ABA + SpEd Consortium. Each material targets a specific point of performance in the toileting routine. Prices in INR.

📋 Material 01 — Visual Toileting Sequence Chart
A laminated A4/A3 poster showing all toileting steps in numbered order with pictographic illustrations. Mounted at child's eye level on the bathroom wall — the cornerstone of the entire system.
Price Range: ₹100–800 | Category: Visual Schedules
Pinnacle Recommends: Laminated, waterproof, A3 size, pictographic (not photographic)
Search on Amazon.in →
Pinnacle Recommends: Laminated, waterproof, A3 size, pictographic (not photographic)
Search on Amazon.in →
🔲 Material 02 — First-Then Toileting Board
A two-panel velcro board showing only the immediate next step ("First: pull down pants") and the following step ("Then: sit on toilet"). Reduces overwhelm by showing just two steps at a time.
Price Range: ₹100–400 | Category: Visual Schedules
Pinnacle Recommends: Velcro-backed with interchangeable picture cards
Search on Amazon.in →
Pinnacle Recommends: Velcro-backed with interchangeable picture cards
Search on Amazon.in →

📖 Material 03 — Social Story for Toileting
A short illustrated narrative (5–10 pages) in first-person perspective, describing the toileting routine as a personal story. Read before and during the routine to build familiarity and confidence.
Price Range: ₹0–500 | Category: Social Stories
Pinnacle Recommends: Child's own photo on cover for highest engagement
Search on Amazon.in →
Pinnacle Recommends: Child's own photo on cover for highest engagement
Search on Amazon.in →


⏳ Material 04 — Toileting Visual Timer / Sand Timer
A visual timer (sand or colour-dial) on the toilet tank or shelf showing how long to sit and wait. Time becomes something the child can see, removing the ambiguity of "how much longer?"
Price Range: ₹200–800 | Category: Visual Timers
Pinnacle Recommends: 3-minute sand timer for sitting; 30-second for handwashing
Search on Amazon.in →
Pinnacle Recommends: 3-minute sand timer for sitting; 30-second for handwashing
Search on Amazon.in →

✅ Material 05 — Task Analysis Cards with Checkboxes
A ring-bound or velcro flipcard set (one card per step) that the child physically checks off or flips after each step. Adds motor action to visual support — the child becomes an active participant in tracking their own progress.
Price Range: ₹100–500 | Category: Task Cards
Pinnacle Recommends: Waterproof lamination, large checkbox minimum 2cm
Search on Amazon.in →
Pinnacle Recommends: Waterproof lamination, large checkbox minimum 2cm
Search on Amazon.in →

🏷️ Material 06 — Bathroom Visual Cue Stickers
Small pictographic stickers placed directly ON the objects they reference — flush sticker on handle, soap sticker on dispenser, handwashing sticker on tap. The environment itself becomes the prompt at the exact point of performance.
Price Range: ₹50–300 | Category: Environmental Cues
Pinnacle Recommends: Waterproof, removable adhesive, pictographic symbols
Search on Amazon.in →
Pinnacle Recommends: Waterproof, removable adhesive, pictographic symbols
Search on Amazon.in →


📱 Material 07 — Video Modelling for Toileting
A short video (2–4 minutes) showing a same-age peer or cartoon completing the full toileting routine. Watched on a tablet before the bathroom visit. Visual learners show dramatically improved imitation after video preview.
Price Range: ₹0 (device-dependent) | Category: Video Modelling
Pinnacle Recommends: Watched 1–2× before toileting attempt; not during
YouTube: search "visual toileting routine for kids autism"
Pinnacle Recommends: Watched 1–2× before toileting attempt; not during
YouTube: search "visual toileting routine for kids autism"
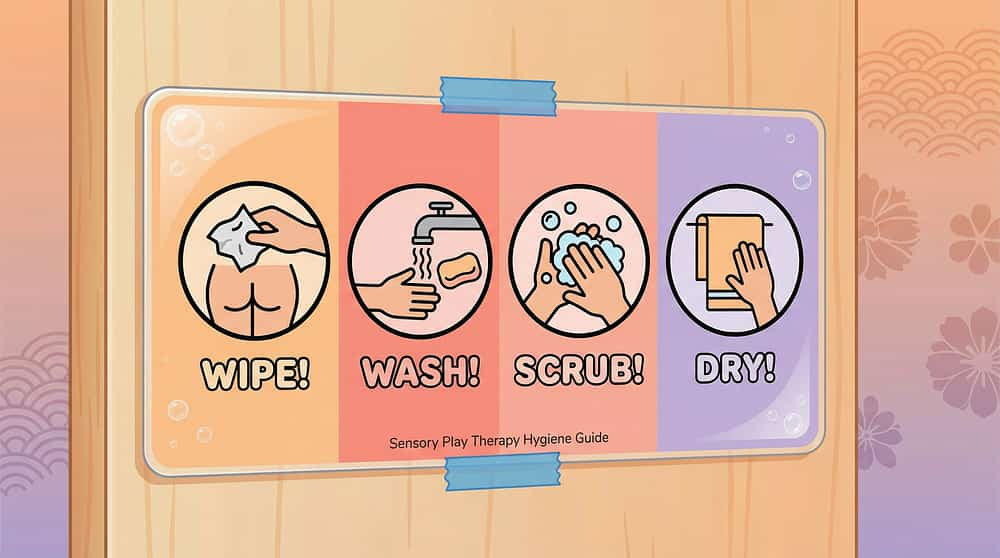
🧻 Material 08 — Wiping Visual Guide with Colour Targets
A laminated guide mounted inside the toilet cubicle showing the 4-step wiping sequence (get paper → fold → reach → check and repeat). Some versions use colour-coded checks to help the child know when wiping is complete.
Price Range: ₹100–400 | Category: Task Cards / Visual Schedules
Pinnacle Recommends: Waterproof laminate, mounted at seated eye level
Search on Amazon.in →
Pinnacle Recommends: Waterproof laminate, mounted at seated eye level
Search on Amazon.in →

🎒 Material 09 — Portable Visual Toileting Cards
A credit-card-sized or keychain set of the full toileting sequence — compact enough for a school bag or pocket. Used in school bathrooms, relatives' homes, restaurants. Extends independence beyond home.
Price Range: ₹100–400 | Category: Visual Schedules
Pinnacle Recommends: Laminated, key-ring bound, A7 size (74×105mm)
Search on Amazon.in →
Pinnacle Recommends: Laminated, key-ring bound, A7 size (74×105mm)
Search on Amazon.in →
🏆 Pinnacle Canon Reinforcement Products
The Rosette Imprint Reward Jar
₹589 | Post-toileting token reward system
Buy on Amazon.in →
Buy on Amazon.in →
1800+ Reward Stickers
₹364 | Immediate visual reinforcement per step
Buy on Amazon.in →
Buy on Amazon.in →
Brainy Bug Flashcards
₹305 | Pre-session sequence matching game
Buy on Amazon.in →
Buy on Amazon.in →

Equity Access
Every Family Can Start Today. ₹0 Option Available for All 9 Materials.
WHO/UNICEF Equity Principle: Intervention effectiveness must not be gated by economic access.
Material | Buy Version | ₹0 DIY Version | Why It Works |
Sequence Chart | Laminated poster ₹100–800 | A4 paper + pen + tape | Same visual sequencing principle; laminate with clear tape |
First-Then Board | Commercial velcro ₹100–400 | Two A5 cards taped to door | Two-step chunking is the mechanism |
Social Story | Printed booklet ₹0–500 | Handwritten notebook with phone photos | Child's own photos increase effectiveness |
Visual Timer | Sand timer ₹200–800 | Draw clock on paper; count aloud | Visual time representation; works equivalently |
Task Cards | Flip-cards ₹100–500 | Index cards + bulldog clip | Physical check-off action is the ingredient |
Cue Stickers | Commercial pictographic ₹50–300 | Phone photo printed + sticky tape | Point-of-performance prompting |
Video Modelling | YouTube ₹0 | Record your own short video | Familiar face = greater generalisation |
Wiping Guide | Laminated card ₹100–400 | Draw 4-step guide; cover in cling film | Waterproof with transparent plastic cover |
Portable Cards | Commercial keychain ₹100–400 | 9 cards, hole punch, key ring ₹20 | Portability is the principle, not the material |
"Visual toileting supports are a human right, not a premium product. The Pinnacle Blooms Network® EverydayTherapyProgramme™ is designed so that any family, anywhere, can begin today with what they have."

⚠️ Safety First
Read This Before Your First Session
The following safety thresholds must be reviewed before beginning any E-509 session. These are clinical gate criteria, not general guidelines.
1
🔴 RED — DO NOT PROCEED
Seek professional assessment first if:
- Child has active UTI or constipation requiring medical treatment
- Child shows severe anxiety/phobia response (crying 10+ minutes, self-injury, vomiting) to bathroom entry
- Child has never tolerated sitting on the toilet at all — begin with E-495/E-496 desensitisation first
- No professional toileting readiness assessment done — call 9100 181 181
2
🟡 AMBER — MODIFY
Proceed with adaptations if:
- Child is unwell, fevered, overtired — postpone; minimal visual support only
- Recent regression without cause — may indicate medical issue; consult NeuroDev
- Child has severe tactile sensitivity to paper/plastic — use digital display versions
- Child uses AAC — integrate AAC symbols (SLP consultation recommended)
3
🟢 GREEN — PROCEED
Standard protocol applies when:
- Child is medically well and regulated
- Child will enter the bathroom with support
- Consistent caregiver available for 8–12 weeks
- Materials prepared at child's eye level
Material Safety & Red Line — Stop If:
- Mount materials OUT of water splash zones (minimum 30cm from toilet/sink)
- No loose choking hazards — stitch/glue all velcro pieces
- Replace materials showing moisture damage immediately
- Child becomes severely distressed (persistent crying >5 min, physical resistance)
- Any sign of pain during toileting (medical review required)
- Child begins ingesting or repeatedly destroying materials
Helpline: 9100 181 181 — consortium team will guide you.

Environment Setup
The Therapeutic Bathroom: 7 Placement Positions
The placement of each visual support is clinically specified — not decorative. Each position corresponds to the exact point of performance in the 14-step routine.
Placement Checklist
First-Then Board
Inside door, child's eye level (~90–100cm)
Sequence Chart
Main wall facing toilet, full view while seated
Visual Timer
Toilet tank or shelf, visible while seated
Wiping Visual Guide
Inside toilet area at seated eye level
Handwashing Visual
Above sink at standing eye level
Cue Stickers
On each object at point of performance
Portable Card Set
On hook inside door
Environment Optimisation
💡 Lighting
Bright, warm LED (not harsh fluorescent if light-sensitive)
🔇 Sound
Minimal; consider small rug for acoustic softening
🌡️ Temperature
Warm — cold bathrooms increase avoidance
🧹 Clutter
Remove unnecessary items; clean visual field reduces distraction
Parent Position: Outside bathroom door OR at threshold. Step back 30–50cm further each week as independence grows.

Act III — The Execution
60-Second Pre-Session Readiness Gate
The best session is one that starts right. A postponed session is good clinical judgement — not failure.
Child State
- Child has eaten in the last 2 hours (not hungry)
- No signs of illness (fever, stomach pain, unusual lethargy)
- Not in meltdown or heightened state
- No severe toileting incident in last 30 minutes
Timing
- 90–120 minutes since last successful void (scheduled toileting)
- OR child showing spontaneous biological signals (holding, crossing legs)
Environment
- All 7 visual supports in place and visible
- Bathroom at comfortable temperature
- Parent has 10–15 uninterrupted minutes
- Reinforcement prepared and accessible
Decision Gate
🟢 8–10 ✓ — GO
Proceed with full protocol
🟡 5–7 ✓ — MODIFY
Proceed with simplified sequence (steps 1–7 only)
🔴 <5 ✓ — POSTPONE
Offer preferred calming activity; retry in 30–60 minutes
Step 1
Step 1 — The Visual Invitation (Not the Verbal Command)
Leading with words — "Time to go to the bathroom!" — can trigger resistance in children with auditory processing differences. The visual invitation shifts the trigger from auditory (parent's voice) to environmental (the schedule).
Option A — Scheduled Toileting
Use during learning phase:
- Point silently to the Visual Daily Schedule — bathroom icon shows it's time
- Offer the First-Then Board: "First: Bathroom 🚽 Then: [preferred activity] 🎮"
- Use a single gesture (point to bathroom door) — no verbal yet
- Allow 5–8 seconds of processing time before adding any verbal cue
Option B — Child-Initiated
Goal state:
- Child sees biological signal and moves to bathroom independently
- Parent's role: Remain available, do NOT follow immediately
- Allow 30–45 seconds of independent initiation before offering support
Parent Script (if verbal cue needed):
"Bathroom time. Let's check the chart." (calm, neutral — not excited, not urgent)
What NOT to Say:
- ❌ "Do you need to go?" (yes/no creates avoidance)
- ❌ "Go NOW" (command without visual anchor)
- ❌ Long explanations or reminders of past accidents
First-Time Protocol: First 3–5 sessions: Walk with child to door, point to First-Then Board, say "First bathroom, then [reward]." Enter together. Full prompt. Fade over 2 weeks.

Step 2
Step 2 — The Child Checks the Chart (Not You)
The Critical Habit: From Day 1, teach the child to look at the chart before each step — not to wait for the parent to tell them. This single habit is the bridge from prompted to independent.
Teaching the Chart-Checking Habit:
- Point to chart: "What does the chart say?" (not "What do you do next?")
- Wait 5 seconds
- If child looks at chart and acts → PRAISE immediately
- If child waits for verbal → gesture to chart; reduce verbal each week
📋 Sequence Chart
Parent stands BEHIND child (not beside) to avoid visual dependence. Goal: child scans chart independently within 4 weeks.
🔲 First-Then Board
Used when full chart overwhelms (anxiety days, new environments). Graduate to full chart once child tolerates 4+ steps.
✅ Task Cards
Child flips each card after completing the step. Physical flip = proprioceptive reward + memory anchor. Child's job only — parent does NOT check the cards.
⏳ Visual Timer
Placed BEFORE child sits down. 3-minute sit for BM attempts; 1 minute for void. Child watches timer; does NOT ask "can I get up now?"
🏷️ Cue Stickers
No parent instruction needed — stickers speak for themselves. If child misses a step, point silently to sticker. Never verbalise what the sticker shows.

Step 3
Step 3 — The Full 14-Step Routine With Visual Support at Every Point
The child executes the complete toileting routine, referencing visual supports at each step rather than relying on adult verbal cues. The parent is observer and reinforcer — not director.
Step | Action | Visual Support | Parent Role |
1 | Enter bathroom | First-Then Board at door | Points silently |
2 | Pull down pants/underwear | Sequence Chart Step 1 | Observer |
3 | Sit on toilet | Sequence Chart Step 2 | Observer |
4 | Start visual timer | Sand timer on tank | Points if forgotten |
5 | Void/BM attempt (wait) | Timer visible | Silent; 3 min minimum |
6 | Wipe — get paper | Wiping Guide Step 1 | Observer |
7 | Wipe — fold paper | Wiping Guide Step 2 | Observer |
8 | Wipe — reach and wipe | Wiping Guide Step 3 | Observer |
9 | Wipe — check paper | Wiping Guide Step 4 | Observer |
10 | Stand and pull up pants | Sequence Chart Step 6 | Observer |
11 | Flush toilet | Flush cue sticker | Points to sticker if missed |
12 | Walk to sink | Sequence Chart Step 7 | Observer |
13 | Wash hands (soap, water, 20 sec) | Handwashing visual + timer | Points to sink visual |
14 | Dry hands | Towel/dryer cue sticker | Observer |
Duration: Full routine: 5–12 minutes. Core therapeutic window (steps 3–9): 3–5 minutes.
Error Correction
Child Response Spectrum & Error Correction Guide
Child Response Spectrum
Response | Meaning | Action |
✅ Follows chart with no verbal cue | Independence emerging | Fade prompts; celebrate |
✓ Looks to parent then chart | Transitioning; habit forming | Gesture to chart; reduce verbal |
⚠️ Ignores chart, demands verbal | Chart engagement not established | Return to Step 2 protocol |
Error Correction — Do NOT vs. Instead
If child... | Do NOT... | Instead... |
Skips wiping | Say "you forgot to wipe!" | Point silently to Wiping Guide |
Refuses to sit | Force sitting | Reduce sit time to 30 sec; use timer |
Flushes immediately | Verbally remind | Pre-position timer before entering |
Leaves without washing | Call out | Point to handwashing visual from doorway |
Key Principle: Silence + gesture always outperforms verbal correction. Every time you point to the visual instead of speaking, you are building the neural pathway from visual scan to action.

Step 4
Step 4 — Dose, Frequency, and the Art of Variation
Daily Dosage
The ≥14-Day Rule: Visual toileting supports work through repetition that builds procedural memory. The minimum therapeutic dose to see measurable change is 14 consecutive days at every toileting opportunity. There is no shortcut.
Frequency
Every toileting opportunity (3–8×/day)
Duration per Visit
5–15 minutes (full 14 steps)
Weekly Total
21–56 visual-supported visits
Minimum Streak
14-day streak before assessing progress
Variation Options (One Per Week After Week 3)
- Morning vs. after-school session — same visual, different time
- Home vs. grandparent's bathroom — portable cards travel with child
- Chart format variation — task flip-cards one day per week
- Social story preview day — Mondays, read story before bathroom visit
Satiation Indicators — Do NOT Push Through:
- Child pushes chart away or covers face
- Child becomes visually avoidant (looks at ceiling, closes eyes)
- Child stimming at high rate during visual inspection
Complete essential hygiene steps with minimal prompt, then close. Record satiation as data.
By Week 3, many parents report they have internalised the routine and no longer feel anxious about each session. Regulated parent energy is itself therapeutic.

Step 5
Step 5 — The 3-Second Window That Builds Independence
The Timing Law: Reinforcement delivered within 3 seconds of the desired behaviour is 4–6× more effective than reinforcement delivered 10+ seconds later. The celebration must happen the moment the child dries their hands and exits.
Reinforcement Script:
"You followed the chart ALL BY YOURSELF. That's independence. I'm so proud."
What to Celebrate:
- ✅ The attempt, not just the success
- ✅ Chart-checking (even with imperfect routine)
- ✅ Any single step completed without verbal prompt
- ❌ NOT only "successful" voiding — creates performance anxiety
Reinforcement Menu:
Type | Example | Frequency |
Verbal praise | Exact script above | Every time — non-negotiable |
Physical | High-five, hug, jump | If child enjoys physical contact |
Token | Star on chart; sticker in jar | Every routine completion |
Preferred activity | 5 min screen time / favourite toy | 3–5 successful routines = 1 activity |
Social | Parent special dance / silly song | Occasional surprise |
Token Economy:
- 5 tokens = 10 minutes of preferred activity
- Post token board OUTSIDE the bathroom door (visible motivation before entering)
- Never remove tokens as punishment — only add

Step 6
Step 6 — No Session Ends Abruptly
Abrupt endings create anticipatory anxiety for the NEXT session. A structured 60–90 second wind-down signals safety, completion, and predictability — making the next session easier before it begins.
1
Completion Signal (5 sec)
"All done! The chart is finished." Show completed task card set or "all done" symbol at chart bottom.
2
Transition Object (20 sec)
Hand child their preferred transition object at the door — soft toy, fidget, or comfort item. (Animal Soft Toys ₹425 → Amazon.in)
3
Reset Materials (30 sec)
Child participates in resetting task cards (flip back to start). Builds ownership; prepares for next use.
4
Transition Language (15 sec)
"Now it's time for [next activity]." Same language as First-Then Board predicted.
If Child Resists Ending:
- Transition is non-negotiable
- Use visual timer: "Timer says all done. Timer is the boss."
- Offer preferred activity as immediate anchor
Data Note: Children who resist ending often seek more sensory input — consider adding proprioceptive activity post-session.

Step 7 — Data
60 Seconds of Data Now Saves Hours of Guessing Later
Families who track see 40% faster skill acquisition than those who don't. Three data points, captured within 60 seconds of session close, give you everything you need to make evidence-based decisions about when to advance, modify, or seek help.
📊 1. Routine Completion %
How many of 14 steps without verbal prompt?
Example: "10/14 — missed flush, wiping steps 2–3, hand drying"
👁️ 2. Chart Engagement
Did child look at chart independently?
Example: "Yes — checked chart 6 times unprompted"
😊 3. Session Mood
1 = distressed → 5 = positive
Example: "4 — mild resistance at start, positive at end"
Tools & Resources:
- 🔗 Pinnacle E-509 Session Tracker: forms.pinnacleblooms.org/e509-tracker
- 📥 Download E-509 Weekly Tracking Sheet (PDF) — 4-week table with all 3 fields
- 📱 GPT-OS® Data Sync: pinnacleblooms.org/gpt-os/log-session — feeds directly to TherapeuticAI® profile
Not sure what you're seeing in the data? Call FREE: 9100 181 181

Troubleshooting
Session Abandonment Is Not Failure. It's Data.
Seven of the most common implementation challenges — each with a clear clinical explanation and a practical fix. Review this before concluding "it's not working."
❓ Child completely ignores the sequence chart
Why: Chart too complex, too small, or placed where child doesn't look.
Fix: Reduce to 6-step chart. Move to child's exact eye level. Use child's own photos. Start with First-Then Board only.
Fix: Reduce to 6-step chart. Move to child's exact eye level. Use child's own photos. Start with First-Then Board only.
❓ Child sits briefly then immediately stands
Why: Sitting on toilet is aversive (sensory, anxiety, or uncomfortable seat).
Fix: Add padded insert. Reduce sit-time to 30 sec. Use sand timer showing very short duration. Reinforce sitting regardless of output.
Fix: Add padded insert. Reduce sit-time to 30 sec. Use sand timer showing very short duration. Reinforce sitting regardless of output.
❓ Home routine works but refuses school bathroom
Why: Different sensory environment, different chart, different teacher.
Fix: Create identical portable card set. Brief school OT/teacher on exact protocol. Practice school bathroom on weekend with parent.
Fix: Create identical portable card set. Brief school OT/teacher on exact protocol. Practice school bathroom on weekend with parent.
❓ Child can describe steps but still can't do them alone
Why: Verbal knowledge and procedural execution are separate neural systems.
Fix: This is exactly why visual supports exist. Verbal knowledge ≠ procedural independence. Continue support; do not remove based on verbal ability.
Fix: This is exactly why visual supports exist. Verbal knowledge ≠ procedural independence. Continue support; do not remove based on verbal ability.
❓ Chart gets wet or destroyed
Why: Normal — bathrooms are wet.
Fix: Replace within 48 hours. Laminate ALL materials. Consider magnetic whiteboard versions.
Fix: Replace within 48 hours. Laminate ALL materials. Consider magnetic whiteboard versions.
❓ Siblings mock the visual supports
Why: Siblings don't understand therapeutic purpose.
Fix: Brief siblings: "This is [child]'s bathroom map. Everyone uses maps sometimes." Or store materials in a small door folder.
Fix: Brief siblings: "This is [child]'s bathroom map. Everyone uses maps sometimes." Or store materials in a small door folder.
❓ Significant wiping difficulty despite wiping guide
Why: Wiping requires complex proprioceptive + motor planning. Visual guide addresses knowledge, not motor skill.
Fix: OT consult for wiping-specific motor programme. Visual guide remains; add OT protocol.
Fix: OT consult for wiping-specific motor programme. Visual guide remains; add OT protocol.
Personalisation
No Two Children Are Identical. Customise This to Yours.
Age-Based Modifications:
Age | Chart Format | Duration | Independence Goal |
2–4 years | First-Then only; 3-step max | 5 min; parent inside | Follows 2-step prompt independently |
4–6 years | 6-step sequence chart | 8 min; parent at door | 1–2 gestural prompts max |
6–9 years | Full 14-step chart | 10–12 min; parent outside | Chart reference only |
9–12 years | Fading to portable cards | 10 min; fully independent | Cards only; fading to memory |
Profile Variations:
Severe Sensory Sensitivity
Reduce lighting (warm dimmer); padded toilet seat; preferred music during sit; waterproof tablet with video model.
Non-verbal / AAC Users
Replace all text with pictographic symbols only; integrate AAC toilet-request button within First-Then Board; SLP to align AAC vocabulary.
Minimally Verbal
PECS integration for toilet request; social story read aloud by parent alongside visual chart.
Fading Protocol (Begin Week 8–10):
1
Week 8
Remove cue stickers from 2 objects (flush, towel)
2
Week 10
Replace 14-step chart with 8-step simplified version
3
Week 12
Move to portable card set only (no wall chart)
4
Week 14+
Remove portable cards; child uses memory with spot-check access

Act IV — The Progress Arc
Weeks 1–2: Tolerance & Familiarity — Not Mastery Yet
This phase is hard. Resist the urge to conclude "it's not working." Neurological habit formation for multi-step sequences in ASD requires 30–50 repetitions before the visual support becomes functionally automatic.
✅ Progress Looks Like:
- Child enters bathroom with significantly less resistance
- Child looks at the chart at least once without being directed
- Child tolerates sitting for 60+ seconds (even without voiding)
- Child completes 5+ of 14 steps without verbal prompt
❌ Not Progress Yet (and that is okay):
- Child not yet initiating independently — this is Week 6+ territory
- Verbal support still needed for some steps — fully expected
- Wiping rarely mastered in Week 1–2 — motor skill requires more repetitions
"If your child tolerates the visual for even 3 seconds more than last week — that is real, measurable neural pathway formation."
PMC11506176 | Pinnacle clinical outcomes data (N=12,000+ toileting programmes)
Progress: Weeks 3–4
Weeks 3–4: The Neural Pathway Is Forming
Weeks 3–4 correspond to early procedural memory consolidation. The prefrontal cortex is forming a working association between the visual support and the motor sequence. The chart is no longer new or threatening.
Spontaneous Movement
Child walks toward bathroom without prompting when schedule shows it's time
Chart-First Behaviour
Child reaches for the chart before looking at parent
Card-Flipping Independence
Child flips task cards independently after each step
Self-Correction Emerges
Child notices skipped step, returns to chart and corrects themselves mid-routine
Social Ownership
Child tells another family member "I follow the chart"
When to Increase Frequency: If consolidation indicators appear, add one more spontaneous attempt per day (8 daily instead of 5).
You may notice you are feeling more confident. Your regulated energy is itself therapeutic — children with ASD are acutely sensitive to caregiver anxiety.

Progress: Weeks 5–8
Weeks 5–8: Independence Is Real. Now We Begin to Fade.
The independence markers below indicate that the neural pathway is established and fading can begin — carefully, systematically, from the most solidly learned steps first.
✅ Independence Markers
- Child initiates bathroom visit without any adult prompt
- Child completes 10+ of 14 steps without verbal cue
- Child references chart spontaneously when uncertain
- Child uses portable cards correctly in second bathroom
- Wiping sequence shows consistent improvement
Fading Begins at Week 8
Remove supports from LAST steps first (most solidly learned):
- Remove towel/drying cue sticker
- Remove tap/handwashing cue sticker (full handwashing visual remains)
- Simplify chart from 14 to 10 steps
What Fading Is Not: Fading is not withdrawal. If child regresses when a support is removed, reinstate for 2 more weeks. Premature fading is the single most common cause of toileting regression.
Community Generalisation: By Week 6–8, prepare portable card set for first community bathroom use — a low-stakes outing to a familiar relative's home.

🌟 This Is Not Small. This Is Everything.
Toileting independence is not a hygiene milestone. It is the gateway to full participation in life — school, community, friendships, and the child's own profound dignity.
School Full Inclusion
No aide support required in bathroom — full participation in mainstream settings
Community Participation
Outings without bathroom anxiety planning — spontaneous family life restored
Peer Relationships
Dignity preserved; no visible support needed among peers
Family Wellbeing
Caregiver burden significantly reduced; family spontaneity returns
The Child's Own Dignity
One of the most private forms of human autonomy — earned and owned
Milestone Recording:📅 Date of First Independent Complete Routine: ___________________ Record this in your child's medical record. This date matters.
"You did this. You showed up. Every single day. For 8 weeks. While working, while parenting other children, while navigating your own exhaustion. This independence belongs to your child — and to you."

⚠️ Red Flags
Know When to Escalate
🔴 Red Flags — Call 9100 181 181 TODAY:
- New aversion to bathroom (previously tolerating) with no apparent trigger
- Pain, crying, or visible discomfort during voiding — possible UTI/constipation
- No bowel movement in 3+ days — medical assessment required
- Self-harming behaviours in the bathroom context
- Complete regression after 4+ weeks of success with no identified cause
🟡 Amber Flags — Consult Within 1 Week:
- Progress plateaued for 3 consecutive weeks despite protocol fidelity
- Succeeds at home but completely refuses school bathroom
- Wiping mastery not emerging by Week 10 (OT motor assessment)
- Family consistency breaking down across multiple caregivers
Professional Options:
🦺 OT Assessment
Sensory processing, fine motor, adaptive equipment
🔵 BCBA Session
Functional behavior assessment for escalating refusal
🧠 NeuroDev
Medical rule-out (dysfunctional voiding, GI issues)
🏥 Pinnacle Centre Visit
Full consortium assessment across all 5 disciplines
FREE Helpline: 9100 181 181 | 8am–8pm, 7 days/week | 16+ languages
Progression Pathway
E-509 in Your Child's Toileting Journey
"Visual supports (E-509) establish the what. Sensory management (E-510) ensures the environment doesn't block the what. Generalisation (E-511) takes independence everywhere."
E-507
Toilet Playing Materials — pre-requisite desensitisation
E-508
Fecal Smearing Prevention — behavioral-visual companion
E-509
Visual Toileting Supports — YOU ARE HERE
E-510
Bathroom Sensory Issues — sensory environment barriers
E-511
Different Toilet Locations — portable independence
What Comes After E-509:
E-516: Toilet Schedule
Biological rhythm and predictable timing layer
E-519: Handwashing After Toilet
Deepening the hygiene chain beyond the bathroom
Related Techniques
Continue the Journey
Each technique in the Pinnacle Blooms 999-episode library builds on the last. E-509 connects to six related techniques across the Toileting & Self-Care Independence series.

E-507 — Toilet Playing Materials
Pre-requisite desensitisation for children who have not yet tolerated bathroom entry or toilet proximity. Begin here if E-509 triggers avoidance.

E-508 — Fecal Smearing Prevention
Behavioral-visual protocol companion. Shares the same visual architecture as E-509 and is commonly implemented alongside it.
E-510 — Bathroom Sensory Issues
Direct next step: addresses sensory barriers that challenge even visually supported children. The most common reason E-509 stalls at Week 3.
E-511 — Different Toilet Locations
Generalisation of E-509 portable cards — school bathrooms, restaurants, grandparents' homes, and travel.

E-516 — Toilet Schedule
Biological rhythm and predictable timing layer. Adds scheduled toileting intervals to complement the visual supports established in E-509.

E-519 — Handwashing After Toilet
Deepening the hygiene chain. Extends the visual support system from the toilet to the sink and beyond.
Act V — Community & Ecosystem
Real Families. Real Bathrooms. Real Independence.
Arjun, 7 — ASD Level 2 — Hyderabad
"He knew every step verbally. But he couldn't do it without me standing there. We put the sequence chart up on a Tuesday. By Saturday he was checking it himself. By Week 4 he was going completely alone. I used to plan every outing around bathroom proximity. Not anymore." — Mother, Pinnacle Secunderabad Network
Meera, 9 — ADHD-combined — Bangalore
"She'd always get distracted mid-routine. Forget to flush. Forget to wash. Teachers sending notes home. The cue stickers on the objects were the answer — she sees the sticker on the tap and she washes. It took three days. Three days to solve a three-year problem." — Father, Pinnacle Bangalore Network
Vikram, 5 — GDD — Chennai
"We didn't think visual supports would work without language. But they worked BETTER without language. The pictures did all the talking. In 8 weeks he moved from needing full adult assistance to completing 10 of 14 steps independently." — Grandmother, primary caregiver, Pinnacle Chennai Network
All vignettes anonymised; names changed; consent-based. Individual results may vary. Statistics represent aggregate network outcomes.
Community
You Don't Have to Figure This Out Alone
2,400+ families are implementing E-509 right now. Join the community to share wins, ask questions, and connect with families who are 3–6 months ahead of you on the same journey.
💬 WhatsApp Parent Group
2,400+ families implementing E-509. Real-time peer support, protocol questions, and daily wins.
Join →
Join →
🌐 Pinnacle Parent Forum
Ask questions, share wins, get answers from families 3–6 months ahead.
Visit →
Visit →
📅 Monthly Meetups
Virtual & in-person, facilitated by Pinnacle OT — implementation Q&A sessions.
👥 Peer Mentoring Programme
Matched with a parent who has completed E-509 with their child.
Request a Mentor →
Request a Mentor →
FREE Helpline: 9100 181 181 | 8am–8pm | 16+ languages

Professional Support
70+ Pinnacle Centres Across India. Expert Help When You Need It.
When to Involve a Professional:
- Initial setup and materials selection (OT — 1 session usually sufficient)
- Progress plateaus at Week 3+ (BCBA functional assessment)
- Wiping motor difficulty (OT — additional motor programme)
- School consistency gap (SpEd consultation)
- Medical concerns (NeuroDev within-network referral)
Your Multi-Disciplinary Team:
🦺 Pediatric OT
🔵 BCBA/ABA
📚 SpEd
💬 SLP
🧠 NeuroDev
Teleconsultation
₹0 initial consultation for new families | Available in 16+ languages | No travel required.
Find a Centre Near You
70+ centres across India. In-person assessment, consortium team, and full GPT-OS® integration.
FREE Helpline: 9100 181 181 | 7 days/week | WhatsApp available

GPT-OS® Integration
Powered by GPT-OS® — The World's First Global Pediatric Therapeutic Operating System
How GPT-OS® Works With E-509
Session Data (E-509)
Parent logs 3 data points within 60 seconds of session close
AbilityScore® Update
Domain E score recalculated in real time
TherapeuticAI® Recommendation
Next technique recommendation generated based on progress trajectory
FusionModule™ Coordination
OT + ABA + SpEd + SLP protocols synchronised
EverydayTherapyProgramme™
Home protocol generated for next 14 days
Re-measurement
AbilityScore® recalculated at Week 4 with updated benchmarks
Population Learning
Your anonymised data contributes to 20M+ session intelligence — identifying which visual support combinations work fastest for which child profiles. Your data makes the protocol better for every family after you.
20M+
Sessions
70+
Countries
97%+
Improvement
Privacy: ISO/IEC 27001 certified | DPDP Act (India) compliant | GDPR-aware | You own your data.
Video Resource
See It in Action: E-509 Visual Toileting Supports
The E-509 reel is a 90-second clinical demonstration of all 9 materials in a real home setting. Available in 16 languages — tap CC for subtitles.
Video Modelling Protocol: Show this reel to your child 1–2 times BEFORE the bathroom visit during the first 2 weeks. Video preview activates visual processing priming — the child has already "seen" the routine before entering the bathroom.
🎬 E-509 Reel
Duration: ~90 seconds | Domain E | Episode 509 of 999
Presented by Pinnacle Blooms OT Consortium
Available in 16 languages (tap CC)
Presented by Pinnacle Blooms OT Consortium
Available in 16 languages (tap CC)
📺 Related Reels
E-507 | E-508 | E-510 (NEXT) | E-511 | E-516
All available at techniques.pinnacleblooms.org
All available at techniques.pinnacleblooms.org
NCAEP (2020) — Video modelling is a standalone EBP for autism, 27+ studies across self-care domains.
Act VI — FAQ
Your Questions, Answered by the Pinnacle Consortium
Q1: What age is too young / too old to start?
Visual supports are appropriate from age 2 through adulthood. No upper age limit. Children over 12 without prior visual support experience start at the same Step 1 level — typically shorter timeline due to higher cognitive capacity.
Q2: My child is verbal and smart. Do they need visual supports?
Yes. Verbal ability and working memory for multi-step procedural sequences are entirely separate neural systems. Many highly verbal, cognitively advanced ASD children have significant working memory deficits. Visual supports are not for "low-functioning" children — they are for any child whose procedural execution is inconsistent despite verbal knowledge.
Q3: Which of the 9 materials should I start with?
Start with the Sequence Chart (Material 1) + First-Then Board (Material 2). Highest impact, lowest cost. Add Materials 3–9 one per week as the first two are established.
Q4: My child ignores the chart completely. What do I do?
Reduce to 3 steps only. Measure from child's seated toilet height to wall — place at EXACT eye level. Use child's own photos instead of generic pictographs. Practice chart-checking outside the bathroom first (no pressure).

Q5: How do I coordinate between home and school?
Download the Teacher/School Communication Template from the Share card. Request 15 minutes with class teacher and school OT. Provide identical portable card set for school. The visual must match home exactly to enable generalisation.
Q6: My child uses AAC. How does E-509 work with AAC?
Integrate toilet-request symbols from child's AAC vocabulary into the First-Then Board. SLP should align AAC vocabulary with E-509 visual sequence. AAC handles communication; visual supports handle routine execution — they work in parallel.
Q7: How do I know when to fade the visual supports?
Begin fading when child initiates AND completes the full routine without any adult verbal or gestural prompt for 5 consecutive sessions. Fade per the fading protocol. Never remove all supports simultaneously. Some children benefit from permanent cue stickers as dignified long-term supports.
Q8: What if my child's other parent disagrees with visual supports?
Share this page. Direct them to the brain science card, the evidence card, and the family vignettes. Visual supports are Level I EBP. Consistency between caregivers is the single biggest predictor of success.
Didn't Find Your Answer?
Or call FREE: 9100 181 181
Preview of 9 materials that help with visual toileting supports Therapy Material
Below is a visual preview of 9 materials that help with visual toileting supports therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.




















Link copied!

🌸 Pinnacle Blooms Network®
The Pinnacle Promise
"From fear to mastery. One technique at a time."
Pinnacle Blooms Network® transforms every home into a proven, scientific, 24×7, personalised, multi-sensory, multi-disciplinary integrated therapy environment — for every child, in every family, regardless of geography or economic circumstance.
20M+
Therapy Sessions
Exclusive 1:1 sessions delivered
97%+
Measured Improvement
Across all active techniques
70+
Centres
Across India
70+
Countries
Global reach
Loop Navigation:
Statutory Identifiers:
CIN | U74999TG2016PTC113063 |
DPIIT | DIPP8651 |
MSME | TS20F0009606 |
GSTIN | 36AAGCB9722P1Z2 |
ISO | ISO 13485 Medical Device QMS · ISO/IEC 27001 Information Security |
Copyright | © 2025 Pinnacle Blooms Network® · Koti Group. All rights reserved. Registered trademark. |
This content is educational and informational. It does not constitute medical advice and does not replace individualised assessment and intervention planning by licensed occupational therapists, behavioral specialists, speech-language pathologists, and healthcare professionals. Toileting difficulties may indicate underlying developmental, sensory, or medical conditions requiring professional evaluation. Individual results may vary. Statistics represent aggregate outcomes across the Pinnacle Blooms Network® (20M+ sessions).
FREE Helpline: 9100 181 181 | pinnacleblooms.org | techniques.pinnacleblooms.org | E-509 | Toileting & Self-Care Independence | techniques@pinnacleblooms.org