
"She holds everything sideways. Tilts her head to look at the world from its corners. Her eyes work perfectly. But she sees differently."
Every morning, you watch her angle herself just so — tilting, positioning, viewing her breakfast from the side of her eye as if direct looking would miss something important. The doctor says her vision is perfect. The ophthalmologist confirmed it twice. And yet, this sideways world is the one she chooses. You are not failing. Your child's visual system is speaking.
🔬 Technique A-073
Visual Processing + Sensory Regulation
Sensory Solutions — Episode 73
Pinnacle Blooms Network® | GPT-OS® Validated | OT + ABA + NeuroDev + SLP + SpEd | WHO Nurturing Care Framework (2018): Early identification and parental awareness during the first years of life directly impacts long-term developmental outcomes.

The numbers say this is seen, studied, and supported.
Side-eye gazing — viewing the world from the periphery despite healthy eyes — is one of the most commonly reported and least understood atypical visual behaviors in children with sensory processing differences. It is not rare. You are among millions of families who have noticed exactly this.
1 in 36
Children with Autism (US)
CDC, 2023. Visual processing differences affect 80%+ of them.
18M+
Children in India
Children with developmental differences requiring support (WHO South-East Asia, 2023).
97%+
Families Improved
Families using structured visual sensory intervention through GPT-OS® reported measurable improvement (20M+ sessions).
"Your child's world is not broken. It is wired differently. And different can be understood, supported, and expanded." — Pinnacle Blooms Consortium, OT + NeuroDev Team
Research: PMC11506176 | PRISMA Systematic Review (2024): 80% of children with ASD display sensory processing difficulties across multiple domains including visual processing. PMC10955541 | World J Clin Cases (2024): Sensory integration therapy effectively promotes adaptive behaviour and social skills.
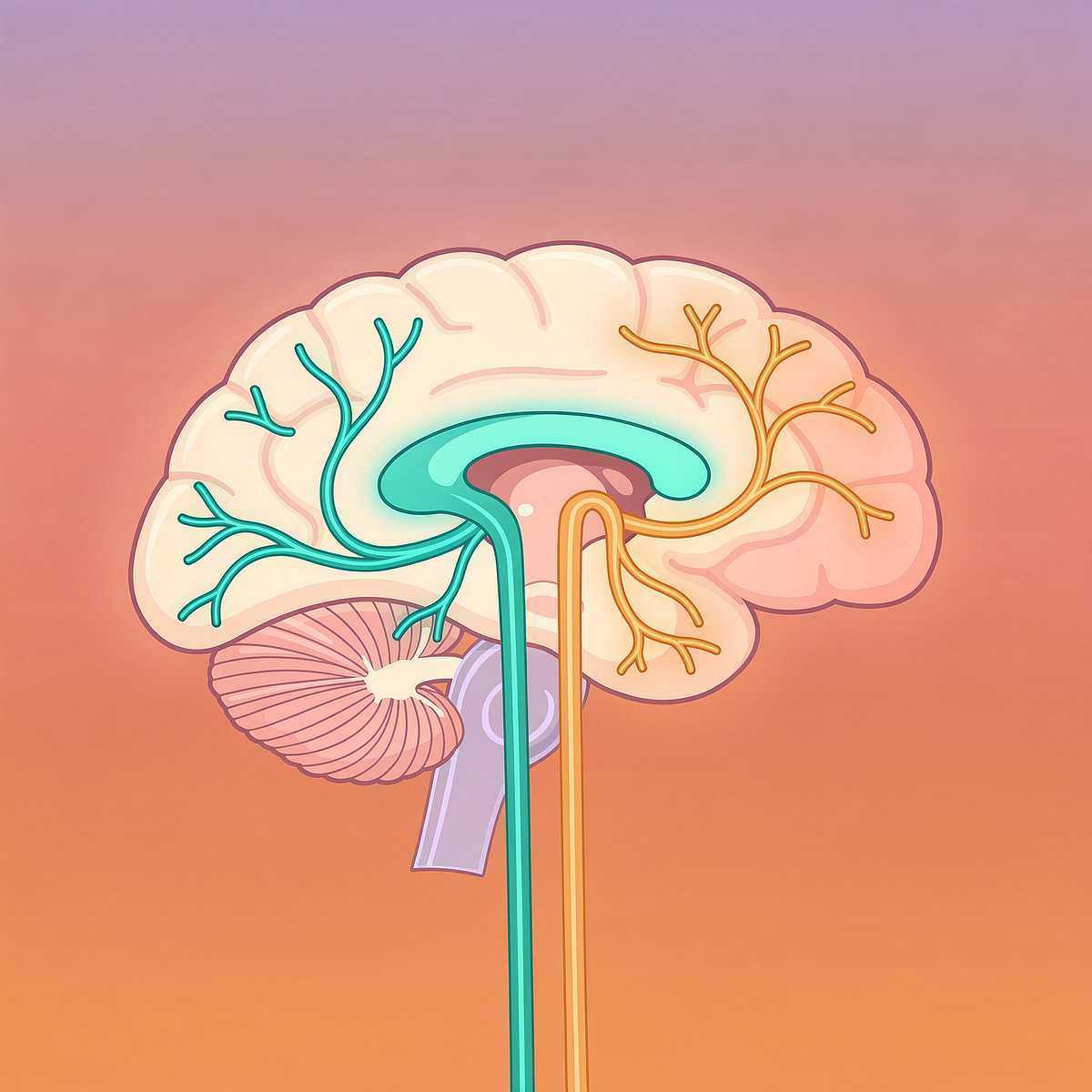
Two visual systems. One brain. Different preferences.
Central (Foveal) Vision
The detail-oriented, high-resolution, colour-sensitive system used to read, recognise faces, and focus directly on objects. For some children, this system is over-amplified — processing every direct visual detail at overwhelming intensity.
Peripheral Vision
Motion-sensitive, spatially aware, lower resolution. In children with sensory processing differences, the peripheral visual system may function more comfortably — providing the same information at a more tolerable intensity level.
What this means for your child
Side-eye gazing is not random. The brain is choosing the processing pathway that feels safer, more comfortable, or more informationally satisfying. This is a wiring difference, not a behaviour choice.
The Peripheral Advantage in Motion Detection: Peripheral vision detects movement 5× faster than central vision — an evolutionary feature. Children who rely on peripheral viewing may be experiencing enhanced motion perception as a genuine sensory benefit. We work with this strength.
Research: Frontiers in Integrative Neuroscience (2020): Established neurological basis for sensory-based interventions, confirming that visual processing differences in ASD relate to differential pathway activation, not structural eye defects. DOI: 10.3389/fnint.2020.556660
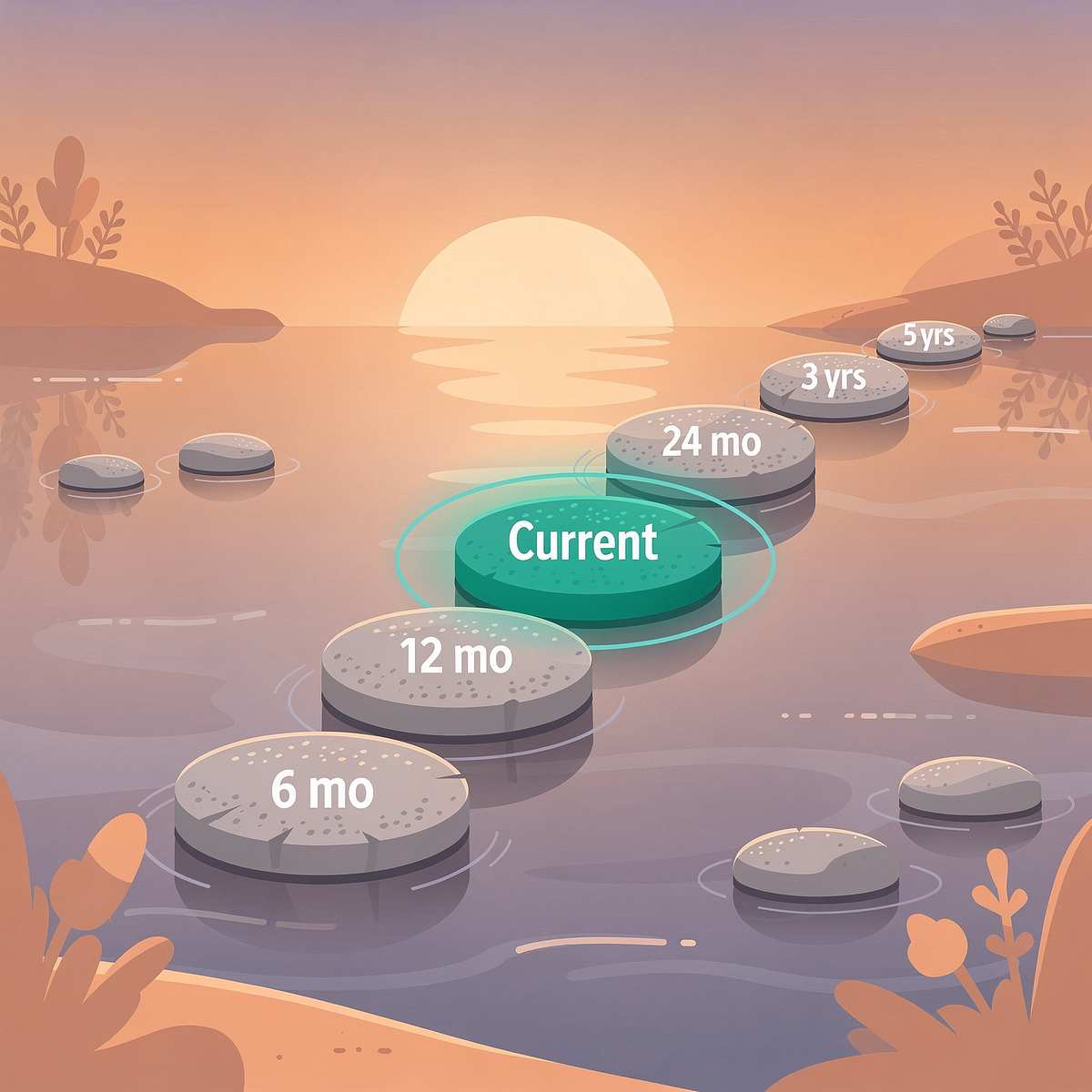
Your child is here. Here is where we're heading.
0–3 months
Prefers high contrast, begins central fixation. Foundation for foveal preference.
4–8 months
Tracks moving objects, social gaze emerges. Tracking + social looking developing.
9–18 months
Points, follows gaze, looks at shared reference. Joint attention requires central gaze.
⚠️ 2–5 years
CHALLENGE ZONE: Peripheral preference may dominate. A-073 intervention window.
5–8 years
Visual learning, reading, social gaze consolidate. Extended intervention benefit window.
8+ years
Flexible visual patterns for learning and social. Mastery + generalisation target.
Co-occurring behaviours to be aware of: Light sensitivity / photophobia | Closing one eye to look (A-072) | Intense fascination with moving objects (A-075) | Avoidance of eye contact (A-080) | Other visual stimming behaviours
The window for the most impactful visual processing intervention is 2–8 years, when neural plasticity is highest. Every structured visual experience in this period shapes how your child's brain integrates visual information for the rest of their life. You found this at the right time.
Research: PMC9978394 | WHO Care for Child Development Package (2023): Age-specific evidence-based recommendations implemented across 54 countries.
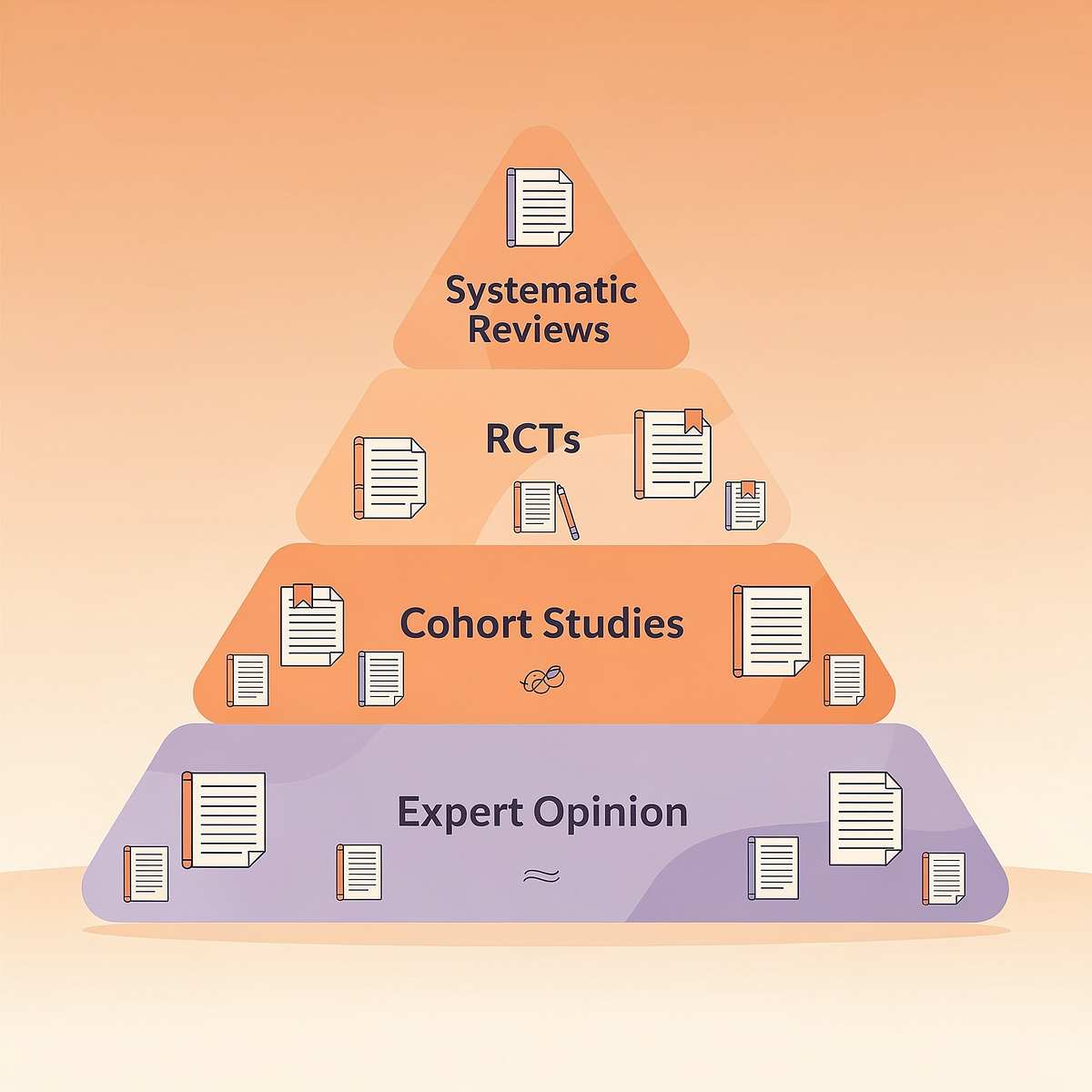
The evidence behind Technique A-073.
🛡️ LEVEL II-B EVIDENCE
Systematic Review + Clinical Consensus + Real-World Evidence
A-073 is grounded in peer-reviewed research, validated across millions of sessions, and clinically confirmed for home delivery. Here is the evidence base that supports every step of this technique.
Study | Finding | Relevance | |
PMC11506176 (Children, 2024) | Sensory integration intervention meets evidence-based practice criteria for ASD across 16 RCTs | Direct: visual-sensory materials validated | |
PMC10955541 (World J Clin Cases, 2024) | Meta-analysis of 24 studies: SI therapy promotes adaptive behaviour, sensory processing | Direct: peripheral-to-central visual expansion | |
DOI:10.1007/s12098-018-2747-4 (Indian J Pediatr, 2019) | Indian RCT: Home-based sensory interventions show significant outcomes in Indian paediatric population | Direct: home applicability confirmed | |
NCAEP (2020) | Visual supports + video modelling classified as evidence-based practice for autism | Supporting: visual material use validated | |
WHO NCF (2018) | Responsive caregiving with structured materials improves development in LMICs | Supporting: equity, home execution validated |
"Clinically validated. Home-applicable. Parent-proven. Across 20 million sessions. In 70+ centers. In 70+ countries."

Visual Peripheral Engagement Shaping
Parent-friendly alias: "Expanding the Visual World" | Technique A-073
What It Is
A structured multi-material approach that works with — not against — a child's preference for peripheral (side) vision to gradually expand visual engagement, build central vision comfort, and develop flexible visual processing patterns across home and therapy settings.
Who It's For
Children aged 2–8 years who consistently prefer viewing objects, people, or visual stimuli from the side (corner of the eye) rather than directly, despite normal ophthalmological findings.
What It Does
Provides 9 specific material categories that honour the child's peripheral preference while creating progressively rewarding conditions for central vision engagement, visual tracking, and social visual interaction — without forcing, demanding, or pathologising the child's current visual pattern.
Session Parameters
⏱️ 10–20 min
Per session
📅 3–5×
Per week
📊 8–12 wks
Protocol
👶 Ages 2–8
Years
🧠 Visual Processing
🎯 Sensory Regulation
👁️ Atypical Visual Behaviours
🤝 Social-Visual Engagement
⚖️ Sensory Integration

The brain doesn't organise by therapy type. This technique crosses every boundary.
🏥 Occupational Therapist (OT) — PRIMARY LEAD
Sensory integration assessment, visual-vestibular protocol design, sensory diet including visual activities. Leads the A-073 clinical plan.
🧬 NeuroDev Pediatrician — Co-Lead
Rules out structural causes, confirms sensory basis, guides clinical severity determination.
📊 ABA/BCBA Therapist — Supporting
Reinforcement scheduling during visual activities, data collection, behaviour shaping for approach behaviours.
🗣️ Speech-Language Pathologist — Supporting
Social visual engagement during communication activities, joint attention building, face-looking during interaction.
📚 Special Educator — Supporting
Classroom accommodations, visual learning modifications, educator training on peripheral viewing.
👨👩👧 Parent/Caregiver — Daily Executor
Home implementation of all 9 material protocols across the EverydayTherapyProgramme™.
FusionModule™ — The Convergence Layer: GPT-OS® coordinates all disciplines into one therapeutic plan. No fragmented care. No conflicting advice. One converged visual processing pathway — executed at home and reinforced across every therapy session.

What Technique A-073 Targets
Three rings of therapeutic impact — from the primary goal at the core to the broader developmental outcomes that flow from flexible visual engagement.
Target | "Before" Behaviour | "After" Behaviour | |
Primary | Consistent head-tilt, side-eye viewing of all objects | Flexible gaze; direct viewing in engaging contexts | |
Tracking | Limited smooth pursuit; loses objects quickly | 3–5 second tracking of moving objects | |
Social | Looks past people during interaction | Brief face-directed gaze during playful exchange | |
Regulation | Peripheral viewing used to avoid central overwhelm | Uses regulated environments without avoidance pattern |
Research: PMC10955541 | Meta-analysis (2024): Sensory integration therapy effectively promoted social skills (primary), adaptive behaviour (secondary), sensory processing, and motor skills (tertiary) across 24 studies.

9 Evidence-Aligned Materials. One for Every Visual Function.
Each of the 9 material categories below targets a specific mechanism of visual processing change — from calming the environment to building social visual engagement. Start with what you have, add as you go.

M1: High-Contrast Visual Materials
Black/white pattern cards, bold geometric panels. ₹200–1,500 | DIY-Friendly. Pulls central vision toward direct looking through rewarding contrast.

M2: Light-Based Visual Toys
Fiber optic sprays, LED panels, colour-changing toys. ₹500–3,000 | Pinnacle Recommends. Meets visual-sensory seeking while enabling both peripheral and central engagement.
M3: Motion-Rich Visual Toys
Spinning tops, marble runs, pinwheels, pendulum toys. ₹300–2,000 | DIY-Friendly. Honours the 5× peripheral motion advantage while building visual tracking.

M4: Visual Tracking Materials
Bubble machines, slow-moving balls on tracks, tracking apps. ₹300–1,500 | DIY: bubbles + flashlight. Builds smooth pursuit eye movement starting in the child's comfort zone.

M5: Peripheral Visual Enrichment
Wide visual panels, side-positioned arrays, wrap-around environments. ₹200–1,500 | DIY-Friendly. Enriches the peripheral field with central elements — expansion, not restriction.

M6: Cause-Effect Visual Toys
Light-up press toys, pop-up reveals, lever-action displays. ₹400–2,500 | Pinnacle Recommends. Child-created visual events drive intrinsic motivation for central looking.

M7: Visual-Vestibular Equipment
Therapy swing + visual target, balance board + visual activity. ₹500–4,000 | OT-Guided. Visual and balance systems co-develop; vestibular regulation helps regulate visual processing.

M8: Regulated Visual Environment
Neutral storage, room dividers, calm-colour materials. ₹200–2,000 | DIY: Declutter = Free. Reducing overwhelm reduces the protective peripheral behaviour.

M9: Social Visual Games
Peek-a-boo props, silly glasses, bubble wands for near-face play. ₹100–500 | DIY: Peek-a-boo = ₹0. Looking at people becomes rewarding through joy, never through demand.

Every family can start today. Zero-cost versions exist for all 9 materials.
WHO Nurturing Care Framework (2018): "Equity-focused interventions must be accessible regardless of economic context." All 9 materials in A-073 have household equivalents.
Material | Commercial Option | Free/DIY Alternative | Why It Works | |
M1 High-Contrast | ₹200 pattern cards | Black marker + white paper | Same contrast principle; foveal reward pathway is material-agnostic | |
M2 Light Toys | ₹500 fiber optic toy | Smartphone flashlight + coloured cellophane | Light intensity = same sensory input | |
M3 Motion Toys | ₹300 marble run | Rolling empty bottle, spinning plate lid | Motion detection principle is object-independent | |
M4 Tracking | ₹300 bubble machine | Blow bubbles with dish soap + straw | Child tracks the bubble = same smooth pursuit training | |
M5 Enrichment | ₹200 visual panels | Rearrange colourful household items at sides | Peripheral field enrichment = environmental | |
M6 Cause-Effect | ₹400 light-up toy | Light switch on wall; pop-up lid box | Child creates event = same intrinsic motivation to look | |
M7 Vestibular | ₹500 therapy swing | Lap swing on doorframe; caregiver lap swing | Vestibular input + visual tracking = combined principle | |
M8 Environment | ₹200 organisation kit | Declutter + cover busy backgrounds with plain cloth | Visual overwhelm reduction = behavioural | |
M9 Social Visual | ₹100 props | Peek-a-boo (hands only) — ₹0 | Playful face engagement = foundational |
The ₹0 Protocol — Start Right Now: 1. Clear one corner of a room. 2. Blow bubbles for your child to track. 3. Play peek-a-boo with a hand towel. 4. Roll a bottle across the floor for motion tracking. 5. Turn a light switch on/off for cause-effect looking. This is A-073. Right now. No purchase required.
Research: PMC9978394 | WHO CCD Package: Household-material-based interventions demonstrated efficacy across 54 low-and-middle-income countries. Access is not a barrier when the therapeutic principle is understood.

Before every session: 90 seconds of awareness.
🔴 RED — DO NOT PROCEED
- Comprehensive vision examination refused or pending — complete ophthalmological assessment first
- Child shows signs of pain, illness, or elevated distress
- Visual-vestibular activity (M7) planned without OT vestibular clearance
- Child has photosensitive epilepsy — avoid all light-based materials (M2) without neurological clearance
🟡 AMBER — MODIFY AND PROCEED
- Child is tired or post-meltdown — reduce session to 5 minutes
- Increased peripheral viewing today — honour it; use enrichment materials only (M5)
- Using cause-effect toys with under-2s — ensure no small parts choking risk
- First-time session with any material — reduce stimulus intensity and duration
🟢 GREEN — PROCEED
- Child is fed, rested, regulated
- Ophthalmological examination completed (normal findings)
- Space is prepared (see Card 12)
- Parent has read all material safety notes
STOP IMMEDIATELY IF: Child covers eyes or shows signs of visual pain | Significant crying/distress specifically in response to visual material | Child loses balance during vestibular + visual activities | Any seizure activity near light-based materials
Research: DOI: 10.1007/s12098-018-2747-4 | Indian J Pediatr (2019): Home-based sensory intervention safety protocols established and validated for parent-administered sessions.

Your home is now a visual therapy space. It takes 3 minutes to prepare.
6 Setup Steps
1
Clear the Space
Remove visually busy backgrounds — curtains, posters, cluttered shelves visible from child's position.
2
Set Centre Materials
Place today's primary material directly in front of child's eye level at 60–90cm distance.
3
Set Peripheral Zone
Place peripheral enrichment material (M5) at 45° side angle, same height as child's eye level.
4
Lighting Check
Natural diffuse light preferred. Avoid glare directly in child's visual field. No strobe/flicker sources.
5
Parent Position
Sit at child's eye level, slightly to one side — not directly blocking the central material.
6
Remove Distractions
TV/tablets off. Minimise competing visual noise from other rooms or windows.
🔆 Lighting
Natural soft light | No harsh fluorescents
🔇 Sound
Calm background | Avoid competing noise
📐 Space
Minimum 2×2 metre clear area
⏱️ Setup Time
3–5 minutes before session

Is Your Child Ready? 60 Seconds. Then You'll Know.
Before every session, run through this readiness checklist. Your child's regulation state is the most important material you work with.
Fed
Child has eaten in the last 90 minutes. Hungry = dysregulated.
Rested
Not immediately post-nap or visibly fatigued.
Regulated
No active meltdown, distress, or elevated anxiety in the last 30 minutes.
Alert
Child is engaged with environment — not zoned out or overstimulated.
Vision Clear
No recent eye rubbing, squinting complaints, or headache indicators.
Safe Space + Materials Ready
Room prepared per Card 12. Today's chosen materials are set up.
Checklist Result | Score | Action | |
All clear | 6/6 | ✅ GO — Proceed to Step 1 (Invitation) | |
Minor items | 4–5/6 | 🟡 MODIFY — Use simpler material, reduce session to 10 min | |
Multiple gaps | 3 or fewer | ❌ POSTPONE — Try a calming activity instead; return tomorrow |
If Postponed: Not today is a valid clinical decision. Session abandonment is data — record what wasn't ready and adjust tomorrow's session.

Step 1: The Invitation
STEP 1
⏱️ 30–60 seconds
The first move belongs to your child.
"Look what I found! Let's see what this does..." — Place material in child's near-peripheral visual field — not directly in front, but at the side where they naturally look.
Guidance
- Body language: Sit at the child's level. Relaxed posture. Open hands. No demand in your face.
- Vocal tone: Curious, not expectant. You're discovering the material together.
- Positioning: Introduce the material at the angle the child naturally looks — peripheral. Start there.
- No demands: Do not say "Look at this" or "Come here." The material speaks first.
✅ Acceptance Cues
- Child orients toward material (even peripherally — this counts!)
- Child leans slightly toward material
- Child reaches for material
- Child's gaze direction shifts at all toward material
- Child does not move away from the space
⚠️ Resistance Cues
- Moves away → Bring material further into peripheral field; reduce distance to 30cm
- Ignores → Make the material active before re-offering
- Shows distress → Pause, calm, re-read Card 13 readiness check

Step 2: The Engagement
STEP 2
⏱️ 1–3 minutes
The child is watching. Now the material works.
M1 — High-Contrast Materials
Hold the pattern card at child's peripheral angle. Slowly rotate it. Wait for gaze to shift. Move the card 5° toward centre. Pause. Wait for the gaze to follow. This is tracking therapy disguised as pattern play.
M2 — Light-Based Toys
Activate the light. Allow the child to observe peripherally. Slowly move the light source through their visual field. Note where direct fixation occurs — that is the target zone for building central engagement.
M3 — Motion-Rich Toys
Spin the top or roll the ball directly in front of the child. Peripheral vision detects it immediately. Watch the child's head angle. Does the motion draw even brief central fixation? That brief moment IS the therapeutic goal at this stage.
Child Response | Clinical Meaning | Parent Action | |
Engages peripherally | ✅ Baseline engagement | Maintain; begin slow movement toward centre | |
Brief central fixation | ✅ Therapeutic moment | Enthusiastic praise within 3 seconds | |
Reaches for material | ✅ Active engagement | Hand it to them; let them control it | |
Avoidance | ⚠️ Reduce intensity | Step back to peripheral distance | |
Distress | ❌ Stop this material | Switch to regulated environment (M8) |
Reinforcement Cue: First moment of central fixation, even 1 second: "YES! Look at that!" — immediate, specific, enthusiastic.

Step 3: The Therapeutic Action
STEP 3
⏱️ 5–10 minutes — core therapeutic window
This is where the brain rewires. Stay with it.
The active ingredient of A-073 is the consistent, gentle, intrinsically-motivated movement of visual engagement from exclusive peripheral preference toward flexible central-peripheral integration. Every material produces this through a different mechanism.
M1: High-Contrast — Central Vision Invitation
Hold pattern card in centre. Tilt it 45° toward the child's peripheral preference. Maintain 10 seconds. Slowly bring to 20° from centre. Wait 10 seconds. Move to centre. The child's fovea will chase the detail if the contrast is compelling enough. 3 repetitions.
M2: Light Toys — Peripheral-to-Central Arc
Activate light in peripheral field (60°). Hold 5 seconds. Slowly arc to 30°. Hold 5 seconds. Arc to centre (0°). Hold 3 seconds. Return to periphery. The child's eyes will often follow without any demand. 5 repetitions.
M3: Motion Tracking — Smooth Pursuit Building
Roll a ball slowly from left to right across the child's field of vision at eye level. The goal is for the visual system to track it through centre. 3 passes. Increase speed by 20% when 3-second central tracking is achieved.
M6: Cause-Effect — Agency-Driven Looking
Let the child press the button. The result appears in their centre visual field. The intrinsic motivation to see what they caused will often drive direct looking. Record each moment of looking directly at the effect. 5 activations.
M9: Social Visual — Peek-a-Boo Protocol
Cover your face. Slowly separate hands 1cm. Maintain anticipation silence for 3 seconds. Open fully: "PEEK-A-BOO!" The joy-driven face reveal triggers central visual attention toward a face — never through demand. 3–5 repetitions. Let the child lead pacing.
Research: PMC10955541 | Meta-analysis (2024): Home-based sessions of 10–20 minutes with core therapeutic action occupying 40–60% of session time showed optimal outcomes.
Step 4: Repeat and Vary
STEP 4
⏱️ 3–5 minutes
3 good repetitions outperform 10 forced ones. Always.
Week | Target Reps | Rest Between | Material Variety | Session Length | |
Week 1–2 | 3 reps/material | 30 seconds | 1 material | 10 min | |
Week 3–4 | 5 reps/material | 20 seconds | 2 materials | 15 min | |
Week 5–8 | 7–10 reps | 15 seconds | 3 materials | 20 min |
Variation Options
Visual arc exercises:
- Horizontal arc (left → centre → right)
- Vertical arc (below → centre → above)
- Diagonal arc (lower-left peripheral → centre)
Motion tracking:
- Rolling ball (horizontal)
- Dangling toy (vertical bounce)
- Bubbles (unpredictable path — most advanced)
Satiation Indicators — When to Stop This Material
- Child stops tracking after starting (satiation, not avoidance)
- Child begins stimming with the material rather than engaging visually
- Child starts looking away from the activity zone entirely
- 10+ minute mark reached on a single material
The Rule: 3 good reps with engagement > 10 forced reps with avoidance.

Step 5: Reinforce and Celebrate
STEP 5
⏱️ Immediate — within 3 seconds
The moment they look directly — that 1 second is worth celebrating like a milestone.
Central Visual Fixation (even 1 second)
"YES! You looked RIGHT at it! Amazing eyes!"
Visual Tracking
"Your eyes followed it all the way! Wow!"
Social Visual — Peek-a-Boo
"YOU SAW ME! That's my favourite! Do it again!"
Child Profile | Best Reinforcer | |
Social motivator | Exuberant verbal praise + clapping + "high five" | |
Object motivator | Brief access to a preferred item (15 seconds) | |
Activity motivator | 30-second access to a preferred activity | |
Token economy | Sticker on chart → build to larger reward |
Core Principle: Celebrate the attempt, not just the success. Every peripheral-to-central movement, however brief, is the brain rewiring. You are witnessing neuroplasticity in real time.

Step 6: The Cool-Down
STEP 6
⏱️ 2–3 minutes
No session ends without a landing.
"Two more times, then all done." [2 final repetitions] "All done with [material name]! Let's put it away together." [Child helps return material] "Beautiful. Now let's do something calm."
Any visible countdown — sand timer, phone countdown, hand signals — is classified as an evidence-based practice for autism (National Clearinghouse on Autism Evidence and Practice, 2020). Visual timers build predictability and reduce resistance to endings.
If Child Resists Ending: Do not abruptly remove the material. Extend by 1 repetition only. Then use the material put-away as a natural activity: "Can you put the spinner in the box? Thank you."

Capture the Data: Right Now
60 seconds of data now saves hours of guessing later.
The 3 Data Points to Record
1
Duration
How many minutes did the session last? Even 5 minutes counts and is valuable data.
2
Central Fixation Count
How many times did the child look directly at the material? Use a simple tally mark for each moment.
3
Child State (1–5)
Rate their regulation on arrival: 1 = dysregulated → 5 = well-regulated.
Track Online
Access the GPT-OS® A-073 Session Tracker at pinnacleblooms.org/tracker/A-073
Or download the printable tracking sheet PDF at pinnacleblooms.org/track/A-073
Data Insight
When central fixation count increases week over week — even from 2 to 3 — that is measurable neural progress. You are tracking brain change.
Date | Material Used | Duration (min) | # Central Fixations | Child State (1–5) + Notes | |

What If It Didn't Go As Planned?
Most sessions don't go perfectly. Perfect sessions are the rare exception. Useful sessions are the goal.
Problem 1: Child refused all materials entirely
What happened: Child was likely not in the optimal regulatory state, or materials were too novel.
Next time: Start with M8 (regulated visual environment) only — no material demands. Just calm the visual space. That IS intervention.
Next time: Start with M8 (regulated visual environment) only — no material demands. Just calm the visual space. That IS intervention.
Problem 2: Child used the material incorrectly
What happened: Child explored with their preferred sensory system, not the targeted visual system. Developmentally expected.
Next time: Pre-teach material use in a brief non-therapy context. Demonstrate purpose first.
Next time: Pre-teach material use in a brief non-therapy context. Demonstrate purpose first.
Problem 3: Side-eye gazing INCREASED during session
What happened: Visual stimuli may have been too intense, triggering the protective peripheral response.
Next time: Reduce stimulus intensity. Lower contrast, dimmer lights, slower motion. Start smaller.
Next time: Reduce stimulus intensity. Lower contrast, dimmer lights, slower motion. Start smaller.
Problem 4: Child showed no central fixation at all
What happened: Material may not be at the right intensity or type for this child's profile.
Next time: Try a different material type. If light-based didn't work, try motion-rich. If motion didn't work, try cause-effect.
Next time: Try a different material type. If light-based didn't work, try motion-rich. If motion didn't work, try cause-effect.
Problem 5: Session ended in distress or meltdown
What happened: Session exceeded the child's current capacity — duration or intensity.
Next time: Reduce session length to 5 minutes. Do 2 repetitions only. Finish before saturation.
Next time: Reduce session length to 5 minutes. Do 2 repetitions only. Finish before saturation.
Problem 6: Parent felt frustrated or inadequate
What happened: Parent expectations exceeded what Week 1–2 looks like clinically. Neural change is invisible and gradual.
Next time: Re-read Card 23 (Week 1–2 expectations). Log the session. You did enough.
Next time: Re-read Card 23 (Week 1–2 expectations). Log the session. You did enough.
Session Abandonment Is Data: If you stopped early — record why. That data is diagnostic information for your GPT-OS® clinical team.
Adapt and Personalise: No Protocol Fits Every Child from Day One.
Adaptation is clinical intelligence, not failure. Use this guide to calibrate every session to exactly where your child is today.
EASIER
Bad days / early weeks: M5 (peripheral enrichment) + M8 (regulated environment) only. 5-minute sessions. No central demands. Accept peripheral engagement as success.
STANDARD
Weeks 2–4: 2–3 materials per session. 10–15 minutes. Begin gentle central visual arcs. Track and reinforce any central fixation.
HARDER
Mastery emerging: Add tracking across midline. Combine vestibular + visual (swing + track). Introduce face-level bubble play. Increase motion speed of tracking materials.
Child Profile | Best Starting Materials | Caution | |
Visual-sensory seeker | M2 (light toys), M3 (motion), M6 (cause-effect) | Risk of pure stimming — structure the engagement | |
Visual-sensory avoider | M8 (regulated environment), M5 (peripheral enrichment) | Do NOT push central demands early | |
Social visual avoider | M9 (social games) at very low intensity | Never demand eye contact | |
Mixed profile | M4 (tracking) + M1 (contrast) as bridge materials | Read response moment-to-moment |
Ages 2–3
5–8 min sessions. Adult-initiated. Simpler materials.
Ages 4–6
10–15 min. Child can begin choosing between 2 materials.
Ages 7–8
15–20 min. Child understands purpose. Self-monitoring emerging.
Week 1–2: What to Expect
📊 15% Progress
FOUNDATIONS PHASE
This week, you're not building new skills. You're building the conditions for new skills.
✅ Signs of Progress (Specific, Observable)
- Child tolerates the material in their visual field for 3+ seconds (versus immediate turning away)
- Child shows curiosity behaviour (leaning, reaching) even while maintaining peripheral viewing
- Sessions end without distress — child is comfortable with the activity
- Parent completes session with confidence → begins data logging
❌ What Is NOT Expected Yet
- Central fixation (direct looking) — not the goal at week 1–2
- Visual tracking across midline — too early
- Reduced peripheral viewing in daily life — neuroplasticity takes 6–8 weeks minimum
- Social visual improvement — this comes much later
"If your child tolerates the material for 3 more seconds than they did on Day 1 — that is real, measurable, neurological progress. Write it down. Celebrate it."
Week 1–2 Focus Materials: M5 (peripheral enrichment) + M8 (regulated environment) + M9 (social visual games, very low intensity)
Research: PMC11506176 | Children (2024): Sensory integration intervention outcomes emerge across 8–12 week timelines. Early-phase indicators focus on tolerance and participation rather than skill mastery.

Week 3–4: Something Is Shifting. Here's What It Looks Like.
📊 40% Progress
CONSOLIDATION PHASE
Neural Pathway Forming
Child begins to anticipate the session — moves toward the material area before it's set up. Reaches for materials proactively.
Central Fixation Emerging
Head tilt angle beginning to reduce. Brief (1–2 second) central fixation occurring spontaneously with preferred materials.
First Tracking Moments
Eyes follow motion objects for 2–3 seconds. First moments of visual tracking emerging naturally.
Spontaneous Generalisation Seeds
Child begins noticing lights or motion in other settings. Looking at faces during play slightly more frequent. Less resistance to forward-facing positioning in daily activities.
When to Increase: If child achieves 5+ central fixation moments per session in Week 4 → introduce a new material type and extend session by 5 minutes.
"You may notice that you are more confident in the session now too. You are reading your child's visual responses. That is clinical skill. You earned it."

Week 5–8: Mastery Indicators
📊 75% Progress
🏆 MASTERY EMERGING
Visual Engagement Flexibility — Level 1
Skill | Mastery Threshold | How to Measure | |
Central fixation | 10+ moments/session, 3+ seconds each | Session tally | |
Visual tracking | Tracks moving object across full visual field (periphery → centre → periphery) | Observe + record | |
Environmental tolerance | Comfortably engaged in visually richer environments | Parent observation | |
Social visual | 2–3 seconds of face-directed gaze during peek-a-boo or play | Session record | |
Head tilt reduction | Head tilt angle reduced in engaged contexts | Video comparison Week 1 vs Week 8 |
Generalisation
Skill appears in non-therapy contexts — playtime, mealtimes, school settings without prompting.
Independence
Central viewing maintained without material scaffolding. Flexible use of both peripheral and central vision.
Maintenance Check
Pause structured sessions for 1 week. If behaviour retreats significantly → return to maintenance sessions 2×/week.
When to Progress: When mastery criteria are met → move to A-074 (Stares at Lights) or A-075 (Spinning Objects) depending on child profile.

You did this. Your child grew because of your consistency.
🏆 Week 8 Milestone
Over 5–8 weeks, you set up a therapeutic space in your home 3–5 times per week, learned to read your child's visual response patterns, delivered structured visual engagement without forcing or demanding, captured data that is now part of the world's largest paediatric therapy outcome database, and created conditions where your child's visual world expanded from its corners toward its centre.
🎂 Share the Data
Share the Week 8 chart as a family achievement milestone
📸 Looking Forward Photo
Document the visual engagement you're now seeing
📓 Family Journal
Write one paragraph: "What changed in 8 weeks"
💬 Share Your Story
Share anonymously with the Pinnacle parent community
"The sideways world didn't close. It opened up to include the centre too. That happened because of you."

Red Flags: When to Pause
Trust your instincts. If something feels wrong, pause and ask.
🚩 All Visual Engagement Avoided
Child begins avoiding ALL visual engagement — even materials they previously enjoyed. May indicate: sensory overload; over-intensified protocol; emerging sensory sensitivity.
🚩 Side-Eye Gazing Increases Outside Sessions
Significant increase in peripheral gazing outside of sessions. May indicate: generalised visual overwhelm; environmental triggers requiring assessment.
🚩 Eye Pain / Headaches / Eye Rubbing
Any new complaints of eye pain, headaches, or eye rubbing. May indicate: ophthalmological change requiring immediate eye examination.
🚩 New Light Sensitivity
Child shows increased light sensitivity (new or worsening). May indicate: neurological assessment warranted; pause all light-based materials (M2).
🚩 Regression in Other Domains
Regression in other developmental areas coinciding with visual intervention. May indicate: overall dysregulation; FusionModule™ review of full therapeutic plan needed.
🚩 Seizure Activity Near Light Materials
Any seizure activity especially near light-based materials. STOP all light materials immediately; neurological consultation urgent.
Situation | Action | |
Mild concern | Self-monitor 48 hours; reduce intensity; call 9100 181 181 | |
Moderate concern | Pause sessions; teleconsultation with GPT-OS® team | |
Eye/neurological concern | Same-day ophthalmological or neurological assessment | |
Acute safety concern | Emergency medical care immediately |

The Progression Pathway: You Are Here. Here Is Where You're Going.
Your response to each material category guides your next technique. If your child responded best to light materials (M2) → A-074 builds on this. If motion materials (M3, M4) were the strongest → A-075 extends this. If social visual (M9) was the greatest gain → A-080 is the natural next step.
Long-Term Developmental Goal: Flexible visual engagement → Joint attention → Visual learning readiness → Literacy and social cognition development (Ages 5–8 target)

The Visual Sensory Domain: Every Technique Your Child Might Need.
A-071 | Child Stares at Fingers/Hands
Difficulty: Intro | Overlapping materials: Visual, motion. Entry point to the visual sensory domain.
A-072 | Child Closes One Eye to Look
Difficulty: Intro | ✅ You have these materials. Immediate predecessor to A-073.
A-073 | Child Side-Eye Gazes ★ CURRENT
Difficulty: Core | All 9 materials. You are here.
A-074 | Child Stares at Lights
Difficulty: Core | ✅ M2 (light toys) you already have. Natural progression from A-073.
A-075 | Child Watches Spinning Objects
Difficulty: Core | ✅ M3 (motion toys) you already have. Motion-visual stimming pathway.
A-080 | Child Avoids Eye Contact
Difficulty: Advanced | ✅ M9 (social visual games) you already have. Social visual development next step.
Materials You Already Own: You've purchased materials for A-073. The same materials cover A-072, A-074, and A-080. Your therapy kit investment spans 4+ techniques.
A-073 Is One Piece. Here Is the Whole Child.
Your Current Domain
Domain A — Visual Sensory Processing
Techniques in domain: 80+ | Series A-071 through A-080+
Techniques in domain: 80+ | Series A-071 through A-080+
GPT-OS® Full Profile
Your child's AbilityScore® maps progress across all 12 domains simultaneously. A-073 progress feeds the Visual Processing Index — one of six readiness indexes tracked in real time.
GPT-OS® Integration
- AbilityScore® (0–1000) updates with each session
- Visual Processing Index: tracks A-073 specific progression
- FusionModule™: coordinates all discipline inputs into one plan
- EverydayTherapyProgramme™: tells you which technique is next, every day
From the corners of the world. To its centre.
Family Story 1 — Hyderabad
Before: "My son, age 4, would only look at anything from the far left corner of his eye. He'd contort his body into these positions — completely sideways — to watch his tablet, his food, his toys. His vision was tested four times. Perfect each time. The ophthalmologist had no answers. His teachers thought he was 'not paying attention' in class. We felt completely alone in this."
After (Week 10): "He still uses his peripheral vision more than typical kids do — probably always will. But now he also looks directly at things. He looked right at me during peek-a-boo in Week 3 and I started crying. He tracks his ball across the room. His teacher says he 'seems more present' in circle time. The sideways world opened up."
📍 Pinnacle Blooms Centre, Hyderabad | A-073 | Visual OT + GPT-OS®
Family Story 2 — Parent-Executed
Before: "My daughter, 3 years old. She'd hold everything — food, toys, phones — up to the absolute side of her face. Her head was permanently tilted. Strangers would stop and ask if something was wrong with her neck. Nothing was wrong with her neck. Nothing was wrong with her eyes. But something was different about how she saw the world."
After (Week 8): "The regulated visual environment card changed everything for us. We didn't know how overwhelming our home was visually. We decluttered one room, used calm colours, reduced the clutter. Within 2 weeks, her peripheral viewing in that room decreased noticeably. Eight weeks later, she reads picture books with direct looking."
📍 Parent-executed A-073 | EverydayTherapyProgramme™ | GPT-OS® guided
"Side-eye gazing is not random. Every child I've worked with using this pattern had a functional reason for it — overwhelm protection, motion seeking, or processing efficiency. When we understand the function, the intervention practically designs itself. We don't remove the coping strategy; we expand the visual world so the strategy is no longer needed as heavily." — OT Specialist, Pinnacle Blooms Network
Individual results vary. These are illustrative narratives. Statistics represent aggregate outcomes across 20M+ sessions.

You are not the only parent watching their child see the world from its edges.
A-073 Visual Sensory Parent Group
WhatsApp community for families navigating peripheral visual preference together. Join via calling 9100 181 181.
Pinnacle Blooms Parent Community
Online forum for sharing progress, questions, and encouragement. Visit pinnacleblooms.org/community
Local Parent Meetup
In-person connections at 70+ centres across India. Find your nearest: pinnacleblooms.org/centers
Peer Mentoring
1:1 match with an experienced parent who has completed A-073. Every mentor has minimum 8 weeks of A-073 experience. Request via helpline.
Isolation is the #1 predictor of home intervention dropout. Families who share the journey maintain sessions 3× longer than families working alone. Connect today.

Home + Clinic = Maximum Impact. Here's Your Professional Support Network.
Find your nearest Pinnacle centre with Visual OT specialists. 70+ centres across India. pinnacleblooms.org/centers
Specialist Type | For A-073 Need | Availability | |
Paediatric OT (Visual-Sensory) | Primary: sensory integration assessment + protocol design | In-clinic + telehealth | |
NeuroDev Paediatrician | Differential: rule out structural causes | In-clinic | |
ABA/BCBA Therapist | Reinforcement design + session structure | In-clinic + home | |
Parent Training OT | Home execution support | Telehealth + home visits |
"Our 70+ centre therapists have executed this protocol over 20 million times. When you come to Pinnacle, you're not getting a session — you're getting a system."
The Science Behind What You've Been Doing.
Deeper reading for the curious parent — and for clinicians who want the full evidence base.
Study | Type | Key Finding | Link | |
PMC11506176 | Systematic Review (2024) | SI intervention meets evidence-based practice criteria for ASD across 16 studies | ||
PMC10955541 | Meta-Analysis (2024) | SI therapy effectively promotes social skills, adaptive behaviour, sensory processing across 24 studies | ||
PMC9978394 | WHO CCD Implementation | Home-based caregiver interventions across 54 LMICs — equity evidence base | ||
DOI:10.1007/s12098-018-2747-4 | Indian RCT (2019) | Home-based sensory interventions: significant outcomes in Indian paediatric population | ||
NCAEP 2020 | Evidence Classification | Visual supports + video modelling = evidence-based practice for autism | ||
WHO NCF (2018) | Policy Framework | Responsive caregiving improves outcomes in 197 countries | Responsive caregiving improves outcomes in 197 countries |
Full evidence base with DOI links available at: pinnacleblooms.org/research/A-073

How GPT-OS® Uses Your Data: Every Session Makes the System Smarter.
What GPT-OS® Learns from A-073 Data
- Which materials drive the fastest peripheral-to-central visual shift for each child profile
- Optimal session duration and frequency for age band and severity level
- Environmental modification factors that correlate with intervention success
- Readiness indicators that predict successful session starts
🔒 Privacy Assurance
Your child's data is anonymised and encrypted. Pinnacle adheres to India's PDPB framework and international healthcare data standards.
Your Data Helps
20 million sessions across India and 70+ countries makes GPT-OS® the world's most data-rich paediatric therapy intelligence system. Your sessions today improve outcomes for children diagnosed tomorrow.

See a Therapist Demonstrate These 9 Materials.
60 seconds that clarifies hours of reading.
What the Reel Shows
- The characteristic side-eye gazing behaviour — compassionate, non-pathologising depiction
- Each of the 9 materials in real use with a child
- The peripheral-to-central visual arc technique in action
- Reinforcement delivery timing
Reel Series Navigation
Research: NCAEP 2020: Video modelling is classified as an evidence-based practice for autism. Multi-modal learning (visual + text + demonstration) improves parent skill acquisition.

Consistency Across All Caregivers Multiplies Impact. Share This Today.
Share Buttons
For Grandparents and Extended Family
Our child looks at things from the side of their eye — this is called peripheral visual preference. Their eyes are perfectly healthy. Their brain just finds sideways looking more comfortable right now.
What helps: Play with them using lights, bubbles, and motion toys. Play peek-a-boo. Keep their play space calm and uncluttered.
Please do NOT ask them to "look here" or force direct eye contact. Let them look however feels comfortable while they build trust with visual engagement.
This is being treated by therapists. Your consistent approach at home doubles the therapy's effectiveness.
Research: PMC9978394 | WHO CCD Package: Multi-caregiver training is critical for intervention generalisation and maintenance across all caregiving contexts.
Every Question Parents Ask. Answered by the Consortium.
Q1: My child's vision is perfect. Why does side-eye gazing happen if the eyes are fine?
Perfect ophthalmological findings are actually expected with side-eye gazing as a sensory behaviour. The eyes are structurally healthy — but the visual brain's processing preferences differ. Central vision processes detailed information at high intensity; for some children this intensity is overwhelming. The behaviour is a neural preference, not an eye defect. This is why vision therapy doesn't resolve it — and sensory integration therapy does.
Q2: Should I stop my child from looking sideways? Force them to look forward?
Never force direct looking or demand eye contact. Forcing direct gaze increases avoidance, damages the trust needed for therapeutic engagement, and often intensifies the behaviour. The goal is creating conditions where direct looking becomes naturally rewarding — not compelling it.
Q3: How do I know if this is autism or just a visual habit?
Side-eye gazing as an isolated behaviour requires comprehensive evaluation rather than assumption. It is associated with sensory processing differences that occur across several developmental profiles. A comprehensive developmental assessment with AbilityScore® will map your child's full profile. Call 9100 181 181 to begin.
Q4: Which of the 9 materials should I start with?
For most children, begin with Material 8 (Regulated Visual Environment) — declutter one room. This is free and takes 20 minutes. Then add Material 9 (Social Visual Games — peek-a-boo). These two require no purchase and address both the environmental modulation function AND the social visual development function.
Q5: How long before I see results?
The first measurable change most parents notice is increased tolerance — the child doesn't immediately move away from the material anymore. This typically occurs within 2–3 weeks of consistent practice. Central fixation usually emerges by week 3–5. Flexible visual patterns across contexts emerge at week 6–10. Full mastery is typically 8–12 weeks.
Q6: Can I really do this at home, or is an OT required?
You can do this at home, and home practice is essential — 1 therapy session per week without home practice is approximately 3% of waking hours. With the EverydayTherapyProgramme™, home sessions provide the remaining 97%. OT clinic sessions provide assessment, protocol design, and progress monitoring. Both are necessary for maximum impact.
Q7: My child is 7 years old — have I missed the window?
No. The optimal window is 2–5 years (highest neuroplasticity), but meaningful intervention outcomes occur across the 2–8 year range and beyond. Neural plasticity never entirely closes — it diminishes with age but remains present. Start today. Every week matters.
Q8: Can I use these materials in school too?
Yes. Download the Teacher Communication Template (Card 37). School accommodations: position the child near the centre of the visual field, use high-contrast materials for instruction, reduce visual clutter in the learning space, do not measure attention by eye contact, and allow varied physical positioning when it supports visual engagement.

You came here for your child. Leave with a plan.
🚀 Start Technique A-073 Today
Launch your first session with the GPT-OS® Session Launcher. Everything you need is ready.
📱 Book a Consultation
Pinnacle Centre or Telehealth. Monday–Saturday | 9 AM–8 PM IST | Video + Voice available.
→ Explore Next Technique
A-074: Child Stares at Lights — your natural next step after completing A-073 mastery.
"Every child who gained visual flexibility started exactly where you are now — reading this page, wondering if they should try."
20M+
Sessions
97%+
Measured Improvement
70+
Centres
DPIIT
Recognised
Preview of 9 materials that help when child side eye gazes Therapy Material
Below is a visual preview of 9 materials that help when child side eye gazes therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.




















Link copied!

The Pinnacle Promise
"From fear to mastery. One technique at a time. For every child. In every home. In every language." — Pinnacle Blooms Network®
OT
Occupational Therapy
SLP
Speech-Language Pathology
ABA
Applied Behaviour Analysis
SpEd
Special Education
NeuroDev
Neuro-Developmental
This content is educational and does not replace assessment by a licensed developmental specialist, occupational therapist, vision specialist, or healthcare provider. Persistent atypical visual behaviours should be evaluated within a comprehensive developmental and vision assessment. Individual results vary. Statistics represent aggregate outcomes across the Pinnacle Blooms Network.
© 2025–2026 Pinnacle Blooms Network®, unit of Bharath Healthcare Laboratories Pvt. Ltd. | CIN: U74999TG2016PTC113063 | DPIIT: DIPP8651 (Govt. of India) | MSME: TS20F0009606 | GSTIN: 36AAGCB9722P1Z2 | All rights reserved. Content licensed under GPT-OS® Content System. Reproduction prohibited without written consent. | techniques.pinnacleblooms.org | pinnacleblooms.org | care@pinnacleblooms.org