
Some patterns hurt. That's real.
When your child covers their eyes at stripes — when checkered floors make them stop dead, when gridded worksheets cause real distress — you are not imagining it. You are not failing. Their brain is speaking.
"My daughter won't wear her favourite dress anymore. She picked it herself. It has stripes. She says they 'hurt her eyes.' The eye doctor said vision is perfect — 20/20. But I watched her try to look at her maths worksheet and her whole body tensed up. The teacher thought she was avoiding work. I knew something else was happening. But I didn't have a name for it."
You are not failing. Your child's visual system is speaking.
Pinnacle Blooms Consortium®
Sensory Solutions Series — Episode 72
Domain A: Visual Processing

The Numbers Behind the Experience
Pattern aversion is not rare. It is under-named, under-diagnosed, and frequently mistaken for behavioural avoidance. Across 70+ Pinnacle centres, we see it every week. The parent who finally finds a name for what they've been watching for months — the relief in their eyes — that moment drives this entire project.
80%
Sensory Processing Difficulties
of children diagnosed with autism experience sensory processing difficulties — including visual pattern sensitivity. Source: PRISMA Systematic Review, 2024 (PMC11506176)
1 in 6
Daily Functioning Impact
children experience sensory processing differences significant enough to impact daily functioning. Source: STAR Institute for Sensory Processing
21M+
Therapy Sessions
delivered by Pinnacle Blooms Network® — building the world's largest evidence base for paediatric sensory intervention in India.
You are among millions of families navigating this. You are not alone. And there is a structured path forward.

The Neuroscience — Elevated for Parents
Understanding why this happens is the first step toward helping. The answer is not in the eyes — it is in how the brain processes visual information.
The Visual Cortex and Spatial Frequency Processing
Pattern aversion occurs when the visual cortex — specifically the striate and extrastriate regions responsible for processing spatial frequencies — becomes hyperexcitable in response to specific repetitive visual stimuli.
High-contrast, repetitive patterns (stripes, grids, checks) create oscillating neural activation at particular spatial frequencies. In susceptible individuals, this activation exceeds the threshold of comfort, producing real perceptual disturbance: patterns that appear to move, shimmer, or pulse; visual discomfort; headache; nausea; and anxiety responses.
Why the eye exam shows nothing: The eyes are functioning correctly. The processing difference is in the brain's interpretation — specifically in how the visual cortex handles repetitive spatial frequency information. This is a wiring difference, not an eye problem.
In Plain Language
🧠 Your child's brain processes certain visual patterns differently than most brains.
📡 Specific patterns — usually high-contrast, closely-spaced, repetitive ones — send signal bursts that become overwhelming.
👁 Their eyes are perfect. It's the signal processing that differs.
⚡ Think of it like the brain's visual processing channel receiving too strong a signal on a specific frequency. The experience is real, physical, and not controllable by willpower.
This is a wiring difference. Not a behaviour choice. Not drama.
Frontiers in Integrative Neuroscience (2020): Comprehensive framework for evaluating sensory integration/sensory processing treatment in ASD, establishing the neurological basis for sensory-based interventions. DOI: 10.3389/fnint.2020.556660
Your Child's Place on the Developmental Map
Pattern aversion does not appear randomly — it follows a predictable developmental arc. Understanding where your child sits on this map helps you intervene at precisely the right moment.
1
Age 2–3
Visual acuity establishes. Pattern sensitivity may first present as texture or visual avoidance.
2
Age 3–5 ★ Pattern Aversion Typically Emerges Here
School readiness environments introduce worksheets, patterned materials, structured visual environments. Pattern triggers become functionally significant.
3
Age 5–8
Academic demands increase visual pattern exposure. Striped/gridded worksheets, classroom environments, patterned clothing social pressure.
4
Age 8–12
Child gains capacity for self-advocacy if equipped. Independence in managing sensory environment develops.
Co-occurring Conditions
Pattern aversion frequently co-occurs with: Autism Spectrum Condition (ASD), Sensory Processing Disorder (SPD), migraine and photosensitive conditions, anxiety disorders, and Irlen Syndrome / Visual Stress. Co-occurring conditions do not cause pattern aversion — they share neurological features that make pattern sensitivity more likely.
Clinically Validated. Home-Applicable. Parent-Proven.
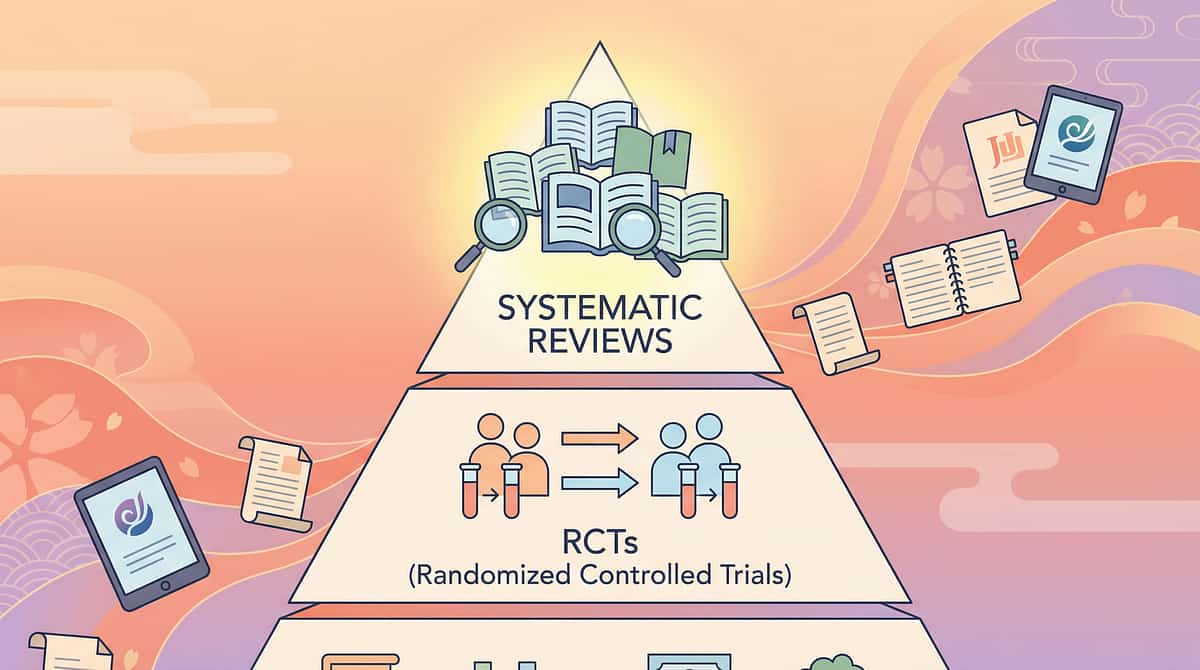
The intervention techniques on this page are backed by multiple levels of clinical evidence, including systematic reviews, randomised controlled trials, and large-scale meta-analyses. This is not experimental — it is established practice.
🛡 LEVEL I EVIDENCE
Systematic Review
Multiple RCTs
Clinical Consensus
PRISMA Systematic Review (2024, PMC11506176)
16 articles from 2013–2023 confirm sensory integration intervention meets criteria to be considered evidence-based practice for children with ASD. Coloured overlays and visual modifications included.
Meta-Analysis, World J Clin Cases (2024, PMC10955541)
Sensory integration therapy effectively promotes adaptive behaviour, sensory processing, and functional independence across 24 studies, N=1,240.
Indian Journal of Pediatrics RCT (2019)
Home-based sensory interventions show significant improvement in sensory processing outcomes; parent-administered protocols validated. DOI: 10.1007/s12098-018-2747-4
WHO Nurturing Care Framework (2018)
Early caregiver-administered intervention within responsive caregiving framework produces measurable developmental improvements.
Pinnacle Blooms Network® has delivered this through 70+ centres with 97%+ measured improvement across sensory readiness indexes.
Naming What Your Child Experiences
Pattern Aversion | Pattern Glare | Visual Stress | Visual Pattern Sensitivity
ICD context: F84.0 (ASD with sensory features) | Sensory Processing Disorder, Visual Subtype
ICD context: F84.0 (ASD with sensory features) | Sensory Processing Disorder, Visual Subtype
Pattern aversion is a sensory processing phenomenon where specific visual patterns — typically high-contrast, repetitive, closely-spaced patterns such as stripes, grids, checks, and geometric repetitions — trigger genuine discomfort, distress, or physiological responses. The experience can include visual discomfort, physical symptoms such as headache and nausea, emotional distress, and behavioural responses such as avoidance and covering the eyes.
Recognise These Signs?
- Squints, looks away, or covers eyes at certain patterns
- Says patterns "hurt," feel "weird," or make them dizzy
- Avoids spaces with triggering patterns (floors, walls)
- Refuses to wear clothing with certain patterns
- Distressed by worksheets or gridded paper — not the content, the design
- Reports patterns seem to "move," "shimmer," or "vibrate"
- Normal eye exam despite visual complaints
What This Is Not
- Not behavioural avoidance
- Not attention-seeking
- Not imagination
- Not a vision problem
✓ A real, neurologically-based sensory processing difference.
Critical distinction: Pattern aversion is distinct from ophthalmological problems. Standard eye exams show normal vision because the issue is in sensory processing, not eye structures.

This Technique Crosses Therapy Boundaries
"The brain doesn't organise by therapy type." — Pinnacle Blooms Consortium
Pattern aversion is not owned by a single discipline. Effective intervention requires a converged, multi-disciplinary approach — which is exactly what the Pinnacle FusionModule™ delivers across 70+ locations nationwide.
Paediatric OT (Lead)
Sensory integration assessment, overlay selection, environmental modification protocols, tolerance-building hierarchy.
NeuroDev Paediatrics
Rule out ophthalmological/neurological conditions; clinical oversight; co-occurring condition management.
Developmental Optometry
Precision colorimetry for tinted lenses; visual processing assessment; Irlen assessment.
ABA / BCBA
Behavioural data collection; reinforcement for tolerance-building; self-advocacy skill building.
Special Education
Classroom material modification; teacher education; IEP/accommodation planning.
SLP
Communication tools for child self-advocacy; language frameworks for explaining sensory experience.
At Pinnacle, no child receives single-discipline care. The FusionModule™ coordinates all six disciplines in a single converged therapeutic pathway.
Precision Targeting — This Is Not a Random Activity
Every session has a purpose. Understanding the three tiers of targets ensures every material choice and every minute of engagement is directed toward measurable, meaningful outcomes.
Primary Target
Visual Sensory Regulation — Reducing the frequency, intensity, and duration of pattern-triggered sensory distress responses.
Observable: Child tolerates patterned environment for ≥5 minutes without covering eyes or seeking exit.
Secondary Targets
Environmental Participation — Child can engage in learning, play, and social environments that contain patterns.
Self-Advocacy — Child can communicate their sensory needs and request appropriate accommodations.
Anxiety Reduction — Reduced anticipatory anxiety about pattern-containing environments.
Tertiary Targets
Academic Participation — Full engagement with school materials without visual sensory barrier.
Social Participation — Peer environments and community spaces become accessible.
Family Quality of Life — Reduction in household accommodations; more flexible family participation.
Independent Daily Living — Child self-manages visual environment with increasing independence.
↑
Sensory Processing Index
↑
Visual Processing Index
↑
Environmental Tolerance
↑
Self-Advocacy Index

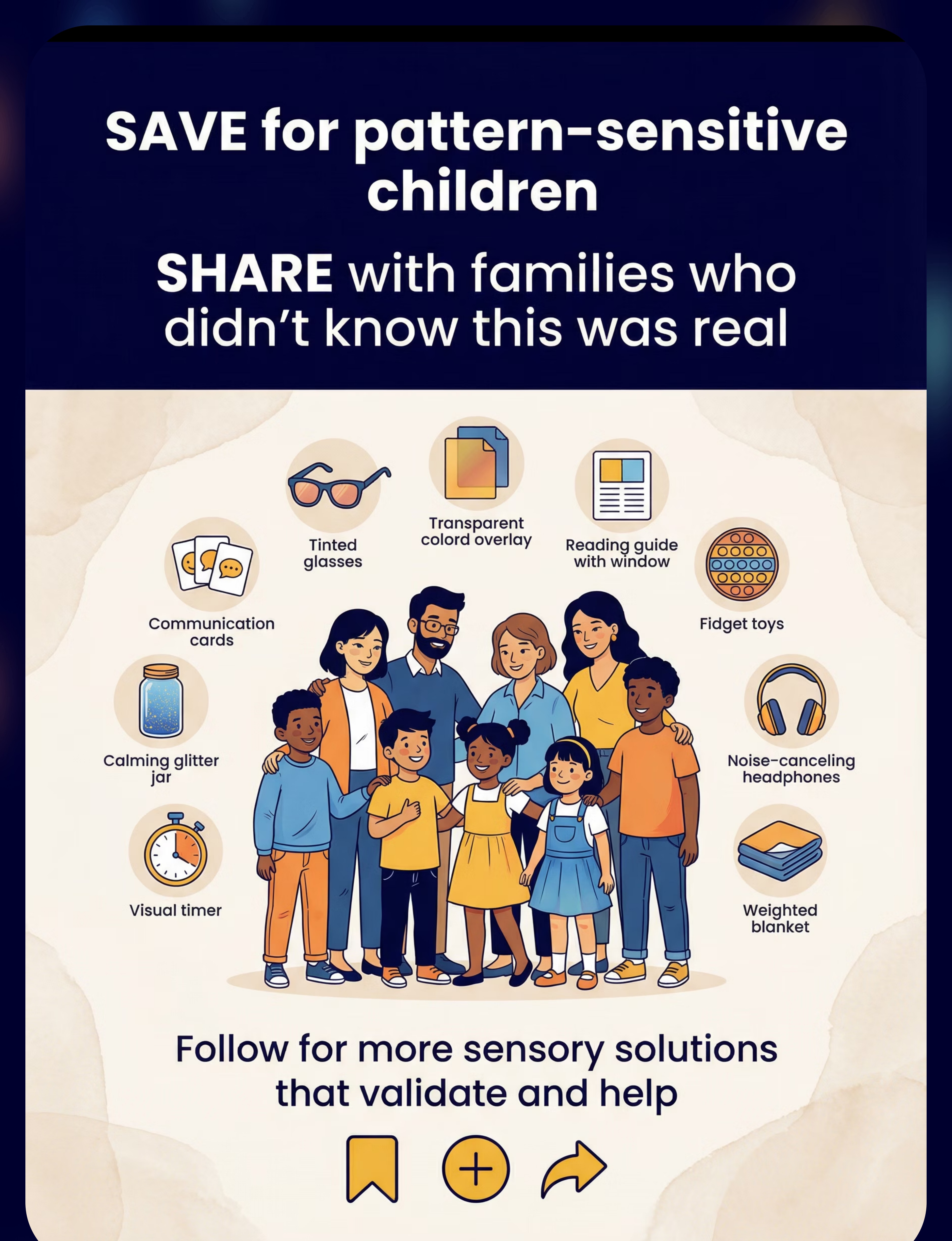
The 9 Materials That Make This Possible
"Pinnacle Recommends" = Clinically validated in our centres across 70+ locations. These nine materials form a complete intervention kit — from zero-cost DIY options to professional-grade clinical tools.
Coloured Overlay Sheets
Canon: Visual Sensory Tools | ₹200–800 | Pinnacle Recommends ✓
Pattern-Neutral Educational Materials
Canon: Educational Accessibility Materials | ₹300–1,500
Tinted Lenses / Glasses
Canon: Visual Protective Equipment | ₹2,000–15,000 | Requires professional colorimetry assessment
Visual Environment Modification Tools
Canon: Environmental Sensory Modifications | ₹500–3,000 | Pinnacle Recommends ✓
Reading Guides and Trackers
Canon: Visual Learning Supports | ₹100–500 | Pinnacle Recommends ✓
Pattern Exposure Gradient Materials
Canon: Sensory Tolerance Building | ₹300–1,200 | Use only under OT guidance
Visual Rest and Recovery Tools
Canon: Sensory Recovery Tools | ₹200–1,000
Pattern Alert and Preparation Tools
Canon: Environmental Preparation Supports | ₹100–500 | DIY available — see Card 10
Self-Advocacy Communication Tools
Canon: Communication Supports | ₹100–400 | Free printables available via GPT-OS®
Total Investment Range: ₹1,900–24,300 (full kit) | From ₹0 with DIY options.
FREE National Autism Helpline: 9100 181 181 — for guidance on which materials to prioritise for your child.
FREE National Autism Helpline: 9100 181 181 — for guidance on which materials to prioritise for your child.

Every Family Can Do This — Starting Today
"The WHO/UNICEF Nurturing Care Framework is explicit: equity-focused interventions must be accessible regardless of economic status. These DIY options carry the same therapeutic principle as their purchased equivalents." — Pinnacle Blooms Consortium
🛒 Buy This | 🏠 Make This Today (₹0) | |
Coloured Overlay Sheets (₹200–800) | Coloured cellophane from any stationery shop. Transparent coloured folders. Test multiple colours to find what helps most. | |
Pattern-Neutral Materials (₹300–1,500) | Photocopy worksheets at 50% contrast. Use plain paper instead of lined. Cover busy backgrounds with plain white paper borders. | |
Tinted Lenses (₹2,000–15,000) | Confirm colour benefit with overlays first. Affordable sunglasses in confirmed helpful colour as an interim option. | |
Environment Modification (₹500–3,000) | Solid colour bedsheets over patterned furniture. Rearrange rooms to block trigger views. Replace patterned curtains with solid fabric. | |
Reading Guides (₹100–500) | Cut a reading window in plain cardstock. Use a plain index card below the reading line. | |
Gradient Materials (₹300–1,200) | Photocopy patterned materials at progressively lighter settings. Start with barely-visible patterns. | |
Visual Rest Tools (₹200–1,000) | Darken a room or corner. Any comfortable cloth over eyes. Solid-colour card for neutral gazing. | |
Preparation Tools (₹100–500) | Photograph upcoming environments on your phone. Create simple hand-drawn maps. Write social stories in a notebook. | |
Self-Advocacy Cards (₹100–400) | Hand-write or print simple explanation cards at home. Create with the child for ownership. |
Every technique in this guide has a zero-cost version. Economic access is not a barrier to beginning. Where clinical-grade materials provide substantially better outcomes, we will note that clearly.

Read This Before Every Session
Your child's safety and emotional wellbeing are the foundation of every session. This traffic-light system gives you a clear, consistent decision framework before you begin.
🔴 RED — DO NOT PROCEED
- Child is currently in sensory meltdown or significant distress
- Child has had a recent head injury or eye trauma — seek medical clearance first
- Child is running a fever or is unwell
- You are attempting gradient exposure (M6) without prior OT assessment
- Child explicitly refuses and shows clear distress signals
🟡 AMBER — MODIFY THE SESSION
- Child is tired or hungry — offer M7/M8 only, no exposure work
- Child had pattern exposure earlier today — prioritise visual rest first
- Child is anxious about upcoming pattern-heavy environment — focus on preparation tools only
- Materials arrived new — allow child to inspect them outside of session first
🟢 GREEN — PROCEED
- Child is calm, fed, rested (within 2 hours of last meal)
- Child has had no significant pattern distress in the past 2 hours
- Environment is prepared (see Card 12)
- You have 15–20 uninterrupted minutes
- Child has given a non-verbal or verbal acceptance cue
STOP IMMEDIATELY IF: Child vomits, has a seizure, reports severe headache, or shows signs of significant physiological distress. Significant visual discomfort should always be evaluated to rule out ophthalmological conditions.
FREE Clinical Guidance: 9100 181 181
FREE Clinical Guidance: 9100 181 181

The Environment Is Half the Intervention
A well-prepared space reduces sensory load before your child even engages with the materials. Every element of the environment — lighting, patterns, exit visibility — communicates safety or threat to your child's nervous system.
Room Setup — 4 Positions
- Child's position: Low-stimulus corner, back to any patterned walls or windows
- Parent position: Beside or slightly in front — not blocking exit
- Materials: On solid-colour surface (tray or plain mat), within reach but not visually overwhelming
- Exit: Always visible and clear — child must never feel trapped
Before Each Session — Remove:
- Patterned throws, cushions, or rugs from immediate area
- Venetian blinds — replace with solid curtains or close completely
- High-contrast patterned artwork from child's sightline
- Distracting screens or objects not relevant to session
Environmental Specs:
Lighting: Soft, even, diffused. Sound: Low ambient noise. Temperature: Comfortable. Pattern: Solid-colour walls and floor if possible — cover with plain fabric if not.
Indian Household Tip: In a joint family household, coordinate with grandparents to maintain session boundaries. A simple handwritten sign — "Therapy in Progress — 15 Minutes" — creates the needed boundary with family dignity.

60 Seconds — Before Every Session
A brief pre-session check prevents wasted sessions and, more importantly, prevents sessions that create new negative associations with pattern materials. Postponing is not failure — it is clinical wisdom.
01
Fed within the last 2 hours?
02
Not overtired (no significant meltdown in last 3 hours)?
03
No current illness or headache?
04
Calm baseline — not already in elevated state?
05
Pattern exposure NOT significant in the last hour?
06
Child willing to be in the room (no active avoidance)?
07
You have 15–20 uninterrupted minutes?
7/7 ✓ = GO
Proceed to Step 1: The Invitation
5–6/7 ✓ = MODIFY
Use accommodation tools only (M1, M4, M5, M7). No tolerance-building today.
<5/7 ✓ = POSTPONE
Offer visual rest (M7) and preparation for next session (M8). Today is a rest day.
"The best session is one that starts right. A postponed session that would have failed is worth more than a pushed session that creates new pattern-distress associations." — Pinnacle Blooms Consortium Clinical Guidance

Step 1: The Invitation
Every protocol begins with an invitation — never a command. The way you open the session sets the entire emotional tone for everything that follows.
"I have something I want to show you. It's something that might make stripes or patterns feel better for your eyes. Do you want to have a look with me?"
Body Language Guidance
- Seated at child's level — not standing over
- Relaxed shoulders — your calm is contagious
- Materials visible but not thrust at child
- Soft, curious tone — not therapeutic urgency
What Acceptance Looks Like
- Child looks at materials
- Child moves toward materials
- Child makes any gesture of interest (even brief eye contact with materials)
- Child says anything that is not explicit refusal
If Resistance Occurs
Child turns away → Move materials further away. Try again in 5 minutes.
Child covers eyes → Today may be a rest/preparation day. Offer M7 and M8.
Child leaves room → Postpone. Do not follow with materials.
Child covers eyes → Today may be a rest/preparation day. Offer M7 and M8.
Child leaves room → Postpone. Do not follow with materials.
Timing: 30–60 seconds. If no acceptance cue in 60 seconds → try tomorrow.

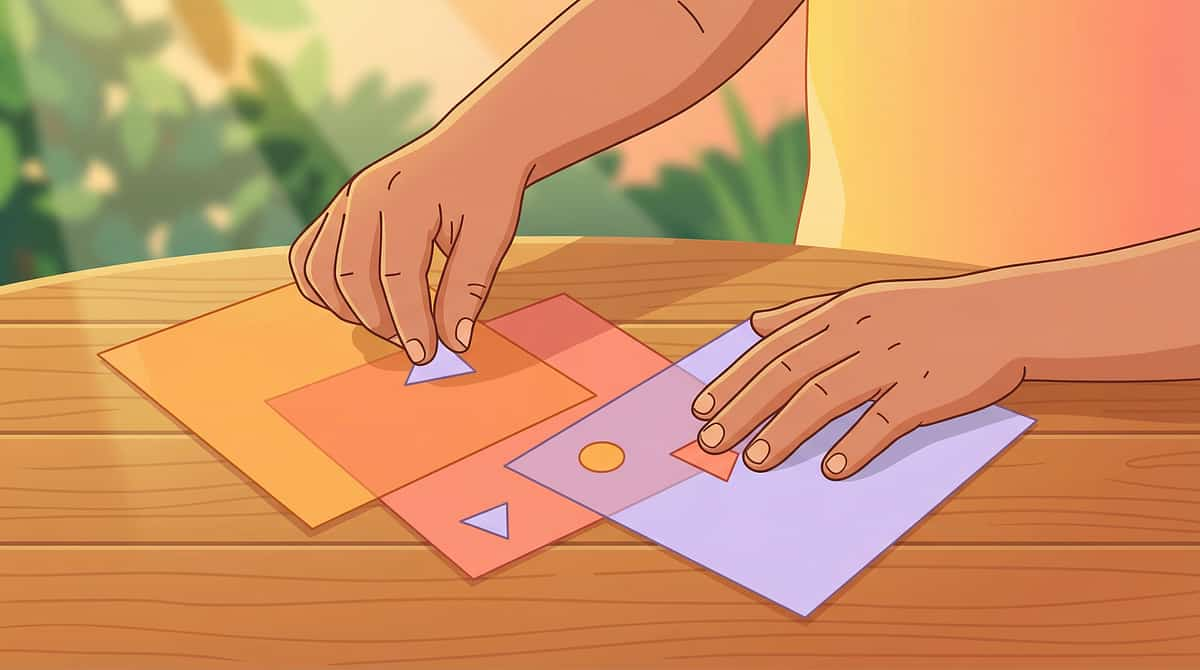
Step 2: The Engagement
Once the invitation is accepted, material introduction begins. The key principle: the child leads. Your role is to create the opportunity for discovery, not to direct the outcome.
"Look, this sheet is blue. Let's see what happens when we put it over this page. Can you tell me what you notice?"
Place overlay on surface first
Don't hand it to the child yet. Allow them to look at it from their chosen distance.
Invite child to move it over materials at their own pace
Follow the child's lead on what they want to overlay first.
Observe and name what you see
🟢Engagement: Child actively moves overlay, comments, relaxes eye tension.
🟡Tolerance: Child watches neutrally, does not object.
🔴Avoidance: Child pushes material away, covers eyes, moves away.
🟡Tolerance: Child watches neutrally, does not object.
🔴Avoidance: Child pushes material away, covers eyes, moves away.
Reinforcement Cue: The moment you see any positive response — even reduced tension in the child's face — say immediately: "Yes! You're trying it. That's exactly it."
Timing: 1–3 minutes.
Timing: 1–3 minutes.

Step 3: The Therapeutic Action
This is the core of the session. The goal is not to push through discomfort — it is to allow the child to discover, at their own pace, what helps their visual system feel safer.
For Coloured Overlays (M1)
Place the coloured overlay over a worksheet, book page, or pattern that typically triggers discomfort. Allow child to try multiple colours. The child — not the parent, not the therapist — determines which colour helps. Let them tell you. Allow 30+ seconds per colour.
For Pattern-Neutral Materials (M2)
Replace one typical worksheet with a pattern-neutral version. Observe: does the child engage differently? Less body tension? More willingness? No change is data too.
For Reading Guides (M5)
Demonstrate: place guide below the reading line. Show child how to slide it down. Let child try. Some children will immediately prefer it; others need multiple sessions.
🏆 Ideal Response
Child spontaneously reports relief. "The wiggly lines stopped." "That's better."
✓ Acceptable Response
Child engages with material longer than without the tool. Body tension visibly reduces.
⚠️ Concerning Response
Child reports increased discomfort, vomiting, or severe headache → Stop, note colour/material, seek professional guidance.
Common Execution Errors: Do not ask the child if the overlay "helps" — let them discover, don't prime expectation. Do not move too fast through colours. Do not apply to the child's own preferred activities first — start with neutral materials.
Duration: 5–10 minutes of therapeutic engagement.
Duration: 5–10 minutes of therapeutic engagement.
Step 4: Therapeutic Dosage
"3 high-quality, child-engaged repetitions carry more therapeutic weight than 10 forced, distress-producing ones." — Pinnacle Blooms Clinical Protocol
Dosage Targets
Target Repetitions: 3–5 meaningful engagements with each material per session.
Session Frequency: Daily or every other day.
Total Protocol: 8–12 weeks.
Variation Options
- Variation A: Same overlay colour, different surface (worksheet → book → iPad over pattern)
- Variation B: Same surface, different overlay colour — testing for best fit
- Variation C: No overlay first, then overlay — child experiences the contrast
- Variation D: Child self-selects which materials to try today — builds autonomy
Satiation Indicators — Stop When You See:
Child begins looking away
Child's engagement shortens noticeably
Child says "finished" or "all done"
Restlessness or fidgeting increases
"THE CHILD SETS THE DOSE — YOUR JOB IS TO OBSERVE AND FOLLOW."

Step 5: The Reinforcement Layer
"Timing matters more than magnitude. Within 3 seconds of the desired behaviour. Specific. Enthusiastic."
"You tried that. You showed me what helps your eyes. That is so important."
"You stayed with it. Your brain is learning."
"You found blue works for you! That's your tool now."
Reinforcement Menu Options
Social Reinforcement
Verbal praise, high-five, special handshake
Token Economy
Add token to visual chart after each session
Preferred Activity
5 minutes of child's preferred activity post-session
Self-Monitoring
Child marks their own "tried it" chart
Celebrate the attempt, not just the success. A child who engaged with the overlay for 30 seconds and said "I don't like it" has given you incredibly valuable data. That is a success.

Step 6: The Transition
No session ends abruptly. The visual system needs transition time. An abrupt ending can disrupt the child's sense of safety and make the next session harder to start.
"Two more, then we're all done. You did so well today."
Cool-Down Activity (2 minutes)
- Brief visual rest: eyes closed or eye mask, dim light
- Gaze at a solid, single-colour object or wall
- Child leads the material put-away ritual
- Transition to preferred, low-pattern activity
Visual Timer Use
Use a sand timer or Time Timer® to signal session end. Predictable endings reduce resistance to stopping. Child can see time remaining — this is co-regulation support.
If Child Resists Ending
Don't force removal of materials. Offer the overlay/tool to the child to keep with them — it is theirs. "You can have it with you" often eases the transition.

Capture the Data — Right Now
Data captured now is data that drives progress. Data remembered tomorrow is data shaped by interpretation.
Complete this tracker within 60 seconds of session end. Every field matters — even "no response" is information that guides tomorrow's session.
1
Date + Material Used
Record the date and exactly which material(s) you used in today's session.
2
Child Response
Circle one: ENGAGED / TOLERATED / AVOIDED. Colour or type that seemed to help.
3
Duration + One Observation
Duration of engagement in minutes. One sentence — what you noticed that surprised you or stood out.
GPT-OS® Integration
If enrolled in GPT-OS®: enter data in the EverydayTherapyProgramme™ module. Your session data contributes to personalised material recommendations, progress tracking across AbilityScore® domains, and therapist visibility at your next Pinnacle session.
Alternative: Paper Tracker
Download the PDF Pattern Aversion Session Log — A072 for a simple printable tracker you can keep in your child's therapy folder.
Helpline: 9100 181 181 — if you are unsure what you observed
Troubleshooting — The Clinical Team's Honest Answers
Real sessions with real children do not always go as expected. These answers come directly from Pinnacle clinical teams who field these exact questions from families every week.
"My child refuses all overlays"
Don't push. Start with preparation tools (M8). Let the child observe you using overlays on your own materials first. Indirect exposure often precedes direct engagement.
"No colour seems to help"
Overlay colour benefit is highly individual and requires professional colorimetry for accuracy. Self-testing is a starting point, not the endpoint. Contact 9100 181 181 to arrange a colorimetry assessment.
"My child tolerated it today but refuses tomorrow"
Normal variation. Readiness fluctuates with sleep, health, cumulative sensory load. Check Card 13 readiness indicators more carefully. Some days are rest days.
"My child seems more distressed after sessions"
You may be exceeding the therapeutic dose or introducing gradient materials too soon. Reduce to accommodation-only approaches. Contact your Pinnacle OT.
"School won't allow coloured overlays in class"
Card 33 contains the teacher communication template and the evidence base you need. Overlays are a documented sensory accommodation with Level I evidence.
"My child says the overlay makes it worse"
Excellent data. That colour is contraindicated. Test other colours. Some children need professional colorimetry to identify the correct tint. Document this and share with your OT.
One Technique. Adapted for Your Child.
The same evidence-based principles apply across all ages and profiles — but the delivery, language, and tools are adjusted to meet your child exactly where they are.
Ages 3–5
Focus on environmental modification (M4) and visual rest (M7). Overlay colour discovery through play — "magic sheets." No structured gradient exposure at this age.
Ages 6–9
Overlay colour identification as a personal discovery process. Child decorates their overlay. Reading guides introduced for school materials. Self-advocacy language introduced for the first time.
Ages 10–12
Child leads their own accommodation strategy. Self-selected overlay. Peer-communication scripts. School advocacy with the child's own words. Gradient materials can begin under OT guidance.
By Profile
Non-verbal Child
Focus on observable response (body tension, eye contact, approach/avoidance). Tolerance is the target — not verbal reporting.
High-Anxiety Child
More preparation tools (M8) before any exposure work. Environmental modification first, always.
Highly Motivated Child
Let them design their own "pattern kit" — personalised overlays and reading guide. Ownership accelerates adoption.
Indian Family Adaptation: The self-advocacy card set (M9) includes a family explanation card in multiple Indian languages. When the entire family understands, consistency across caregivers multiplies therapeutic impact.

Week 1–2: What to Expect
In the first two weeks, your job is observation and preparation — not outcomes. You are building the vocabulary to understand your child's visual world.
1
Week 1–2 ★ You Are Here
Observation and preparation phase
2
Week 3–4
Building consistency
3
Week 5–8
The growth window
4
Week 9–12
Independence and self-advocacy
What You Are Doing
- Identifying child's specific pattern triggers — catalogue which patterns, which environments
- Testing overlay colours for preference (3–4 colours tested)
- Setting up pattern-modified environment in child's bedroom and main learning space
- Beginning preparation tools (M8) before any pattern-heavy environments
What You Will Observe
- Child may show increased interest or increased resistance — both are informative data
- Some children immediately show visible relief with overlays; others need weeks
- Environmental modifications typically show fastest results: child visibly calmer in modified space
Data Target
Complete 5 sessions. Record response to at least 3 different overlay colours.

Week 3–4: Building Consistency
By weeks three and four, the pattern of what works begins to emerge. The child starts to recognise their own triggers — a critical milestone in self-awareness and self-advocacy.
Preferred Overlay Colour Identified
Specific colour preference identified through self-trial, or professional colorimetry assessment booked if needed.
Reading Guide Introduced for School
Reading guide introduced for school and home reading materials — one of the most functionally impactful tools in the kit.
Child Names Their Triggers
Child begins to recognise and name their triggers: "that floor bothers me." This is the beginning of self-advocacy.
Pattern-Neutral Materials in Educational Contexts
Pattern-neutral materials introduced in educational contexts. Teacher conversation initiated (see Card 33).
Key Indicator: Child begins spontaneously reaching for overlay or guide — without prompting. This is self-regulation emerging.
Data Target: Consistent daily use of at least one tool (M1, M4, or M5) for 7 consecutive days.
Data Target: Consistent daily use of at least one tool (M1, M4, or M5) for 7 consecutive days.
Week 5–8: The Growth Window
This is the window where the most significant gains become visible. Environmental tolerance expands, self-advocacy language emerges, and for some children, the first community navigation successes begin to happen.
Environmental Tolerance Expands
Child tolerates pattern-containing spaces with tools. Previously avoided environments become navigable with preparation and overlays or tinted glasses.
Self-Advocacy Language Emerges
"I need my overlay for this." This sentence — unprompted — is one of the most significant milestones in the entire protocol.
Anticipatory Anxiety Reduces
Preparation tools (M8) reduce anticipatory anxiety. Child can discuss upcoming environments calmly — a dramatic quality-of-life improvement for the whole family.
Gradient Exposure Begins (Selected Children)
For some children, first attempts at gradient exposure under OT guidance become appropriate. Never begin this without professional support.
Pinnacle GPT-OS® Data Point: AbilityScore® re-assessment recommended at Week 8. Sensory Processing Index and Environmental Tolerance Index are the primary measurement domains.

Celebrate the Milestones
These are not small wins. Each one represents a moment where your child's world expanded — where fear gave way to mastery. Name them. Mark them. They matter.
First Named Trigger
First time child names their pattern trigger without distress
First Unprompted Use
First day child uses overlay unprompted — self-regulation in action
First Avoided Space Entered
First entry into a previously-avoided space with preparation tools
First Family Explanation
First time child explains pattern sensitivity to a family member
First Consistent School Week
First week of consistent school participation without visual sensory disruption
"I Know What Helps Me"
First time child says: "I know what helps me" — the summit of this protocol
"From fear to mastery. One technique at a time." — The Pinnacle Blooms Consortium
Red Flags — When to Seek Professional Help
This guide is designed to empower families to act confidently at home. But some presentations require professional clinical assessment. Know the signs that mean it is time to call.
🚩 Worsening Despite Intervention
Pattern sensitivity is worsening despite consistent 8-week intervention. Do not persist without professional review.
🚩 Increasing Visual Disturbances
Child reports visual disturbances (things moving, shimmering) that are increasing in frequency or intensity.
🚩 Headaches or Migraines
Headaches or migraines are triggered by pattern exposure — requires medical and optometric evaluation.
🚩 Room Darkening Behaviour
Child is avoiding all visual environments — darkening their room and refusing to enter any visually complex space.
🚩 Significant Meltdowns with Regression
Pattern aversion is triggering significant meltdowns with regression in other developmental areas.
🚩 Family Quality of Life Severely Impacted
Family quality of life severely impacted despite 8+ weeks of consistent, well-executed intervention.
This content is educational — not diagnostic. Significant visual discomfort should be evaluated to rule out photosensitive epilepsy, migraine disorder, scotopic sensitivity syndrome, and Irlen syndrome.
FREE National Autism Helpline: 9100 181 181
FREE National Autism Helpline: 9100 181 181

Your Progression Pathway
Technique A-072 sits within a broader therapeutic progression. Understanding where you are — and where you are heading — gives the work meaning and direction.
Prerequisites (Before A-072)
A-060: Visual Environment Desensitisation (foundational)
A-055: Sensory Diet for Visual Regulation
A-055: Sensory Diet for Visual Regulation
★ A-072: Pattern Aversion Desensitisation — YOU ARE HERE
Coloured overlays, pattern-neutral materials, environmental modification, self-advocacy tools. 8–12 week protocol.
Next Level (After Mastery)
A-080: Community Environment Navigation with Sensory Tools
A-085: School-Based Visual Accommodation Programme
A-091: Independent Sensory Self-Management
A-085: School-Based Visual Accommodation Programme
A-091: Independent Sensory Self-Management
Lateral Options (If A-072 Didn't Resonate)
- A-075: Pattern Tolerance via Art-Based Exposure
- A-078: Digital Screen Pattern Management
Long-Term Developmental Goal
Independent navigation of real-world visual environments — community participation, academic success, and social inclusion without sensory barriers.

Related Techniques in Domain A
If you have overlays and reading guides, you are already equipped for several adjacent techniques. Your A-072 investment extends across the entire Domain A library.
🟢 INTRO
A-060: Visual Environment Desensitisation
Materials: Coloured Overlays. Foundational technique — recommended before A-072.
🟡 CORE
A-065: Fluorescent Light Management
Materials: Light Filters. Addresses the other major visual sensory trigger in school and retail environments.
🟡 CORE
A-070: Glare Reduction Protocol
Materials: Tinted Materials. Targets glare from screens and reflective surfaces.
🔵 ADVANCED
A-080: Community Navigation with Sensory Tools
Builds directly on A-072 — applying tools in real-world community environments.
🔵 ADVANCED
A-085: School Visual Accommodation Programme
Formal school-based programme with IEP support and teacher partnership.
Your Child's Full Developmental Map
Pattern aversion sits within Domain A (Visual Sensory), but it connects to emotional regulation, school participation, and daily living independence. The GPT-OS® FusionModule™ ensures intervention in Domain A supports progress across all connected domains.
This technique is one piece of a larger plan. The GPT-OS® FusionModule™ coordinates all 12 domains simultaneously, ensuring that gains in visual sensory regulation are reflected and reinforced across your child's full developmental profile.
Family Stories — You Are Not Alone
"Stripes, checks, grids — they all made my daughter feel physically ill. People thought she was being dramatic or difficult. Even I wasn't sure at first. But when we started using coloured overlays and understood this was real sensory processing, everything changed. We found the tint that works for her. We modified her classroom worksheets. She has glasses now for environments we can't control. She can explain to people what she needs. She went from avoiding any space with patterned floors to navigating the world with confidence. The patterns haven't changed — but her ability to manage them has transformed."
— Parent, Pinnacle Network | Illustrative case; outcomes vary by child profile
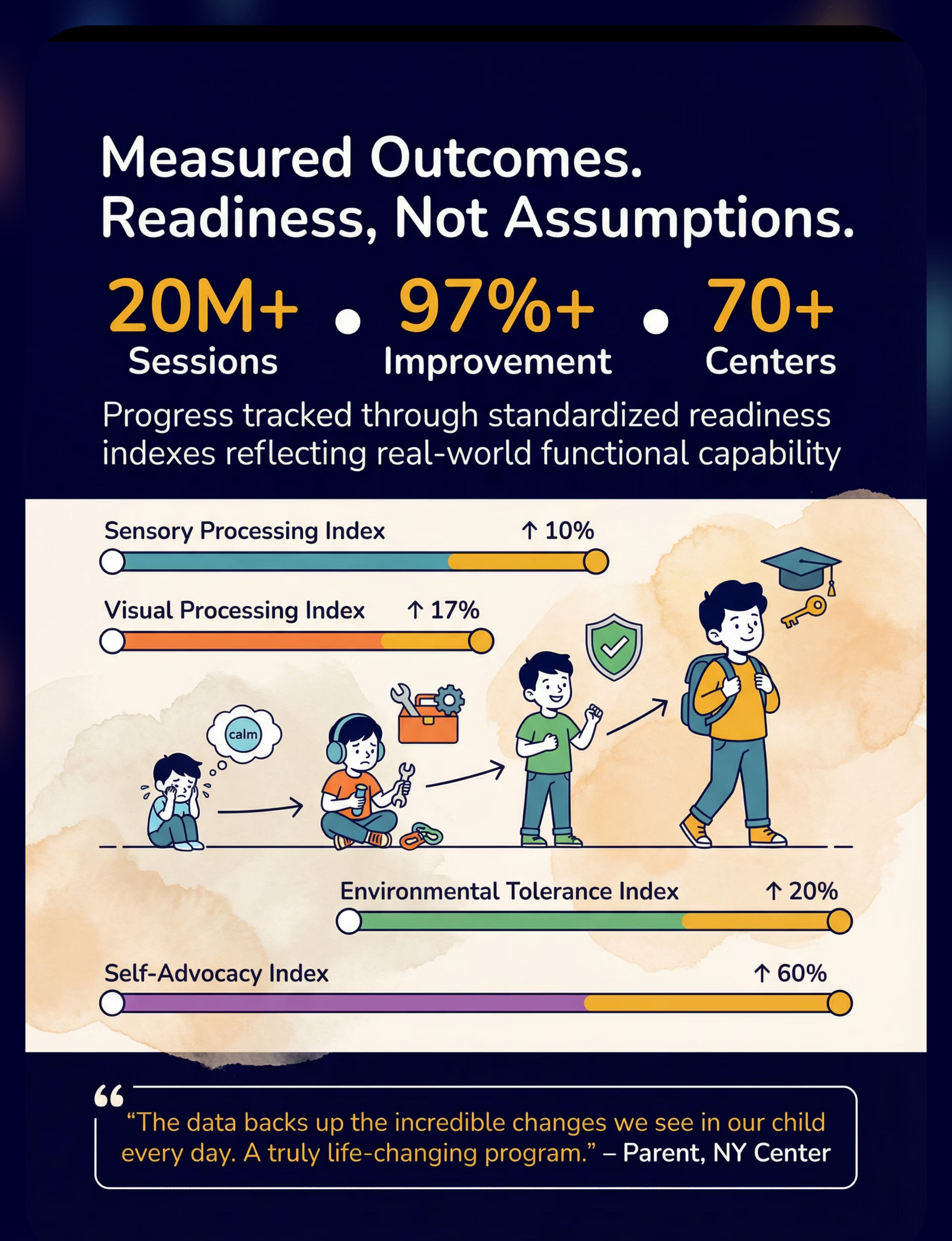
+10%
Sensory Processing Index
+17%
Visual Processing Index
+20%
Environmental Tolerance
+60%
Self-Advocacy Index

Connect With the Pinnacle Community
You do not have to navigate this alone. Thousands of families across India are working through exactly what you are working through — and many of them are one message away.
Pinnacle Parent Community
Online community for families navigating paediatric sensory challenges across India's 70+ Pinnacle locations.
WhatsApp Support Groups
City-wise WhatsApp groups across 70+ locations. Real-time support from parents who have been where you are.
Pattern Sensitivity Parent Circle
Weekly virtual support group specifically for families managing visual pattern sensitivity. Facilitated by Pinnacle OTs.
Free Resource Library
Worksheets, trackers, social stories, and family guide PDFs — all free, all evidence-based.
FREE National Autism Helpline: 9100 181 181
Available in 16+ Indian languages. Call anytime.
Available in 16+ Indian languages. Call anytime.

Professional Support — When and How
Home intervention is powerful. Professional guidance is amplifying. Knowing when to seek each ensures your child receives the right level of support at every stage of the protocol.
When Overlay Colour Is Unclear
Professional colorimetry precisely identifies the optimal tint. Self-testing narrows the field — colorimetry confirms it.
When Pattern Sensitivity Is Severe
Professional graduated desensitisation protocol under OT supervision. Do not attempt advanced gradient exposure at home.
When School Accommodation Is Needed
OT assessment supports formal documentation for IEP and school accommodation plans.
When a Diagnostic Framework Is Needed
OT assessment for SPD/ASD sensory profile to guide the full therapeutic programme.
Teacher Communication Template
"[Child's name] experiences pattern sensitivity — a neurologically-based visual sensory processing difference. Coloured overlays and pattern-neutral worksheets are not preferences; they are sensory accommodations with Level I research evidence. I am requesting these be available in [his/her] classroom. I have attached a brief clinical explanation."
The Research Library
Every technique in this guide is anchored in peer-reviewed clinical evidence. For parents who want to go deeper — and for therapists and programme leads who need it — these are the primary sources.
1
PMC11506176 — PRISMA Systematic Review (2024)
Sensory integration intervention as evidence-based practice in ASD. 16 articles, 2013–2023.
2
PMC10955541 — Meta-Analysis, World J Clin Cases (2024)
SI therapy outcomes across 24 studies, N=1,240. Adaptive behaviour, sensory processing, and functional independence.
3
PMC9978394 — WHO/UNICEF CCD Package Implementation
Care for Child Development Package — equity-centred early intervention framework.
4
DOI: 10.1007/s12098-018-2747-4 — Indian Journal of Pediatrics (2019)
Padmanabha et al. — Home-based sensory intervention RCT. Parent-administered protocols validated.
5
DOI: 10.3389/fnint.2020.556660 — Frontiers in Integrative Neuroscience (2020)
Neurological basis for sensory integration treatment in ASD. Comprehensive framework.
6
WHO NCF 2018 + NCAEP 2020
WHO Nurturing Care Framework | National Clearinghouse on Autism Evidence and Practice EBP Report.
Oxford Centre for Evidence-Based Medicine Level I — Systematic Review Evidence

How GPT-OS® Uses Your Data
Every session data point you contribute helps personalise your child's intervention pathway — and helps build the evidence base for every child like yours across India and beyond.
What GPT-OS® Learns
- Which overlay colours consistently correlate with improved engagement across the network
- Which child profiles respond to environmental modification vs tolerance-building
- How pattern aversion severity correlates with co-occurring conditions
- When to escalate to professional colorimetry based on home-trial patterns
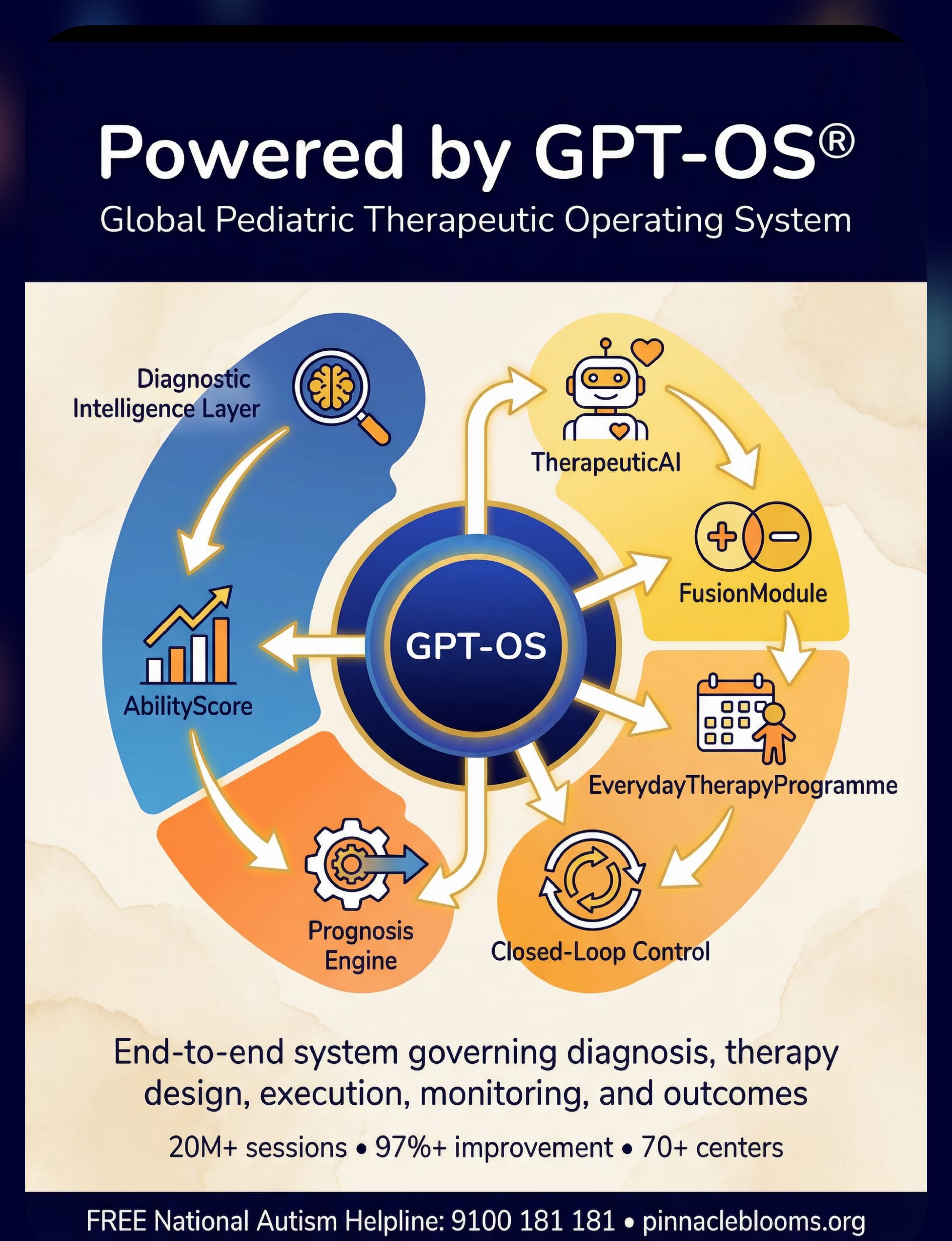
The Full GPT-OS® Stack
Diagnostic Intelligence Layer → AbilityScore® → Prognosis Engine → TherapeuticAI® → EverydayTherapyProgramme™ → FusionModule™ → Closed-Loop Control
Privacy Assurance
All data is protected under Indian IT Act standards. Data is used only for therapeutic personalisation and aggregate research. Identifiable data is never shared.
20M+
Sessions Delivered
97%+
Improvement Rate
70+
Centres Nationwide
160+
Countries with Patents Filed
Watch the Reel — A-072
Reel A-072: "9 Materials That Help With Pattern Aversion"
Sensory Solutions Series | Episode 72 | Domain A: Visual Sensory
Sensory Solutions Series | Episode 72 | Domain A: Visual Sensory
What You Will See in This Reel
1
Authentic Pattern Sensitivity Responses
What it actually looks like — real, not dramatised
2
All 9 Materials Demonstrated
Every material from M1 to M9 demonstrated in context, in under 60 seconds
3
The Relief Moment
The moment a child experiences relief with a coloured overlay — real, not staged. This is why this work matters.
4
Pinnacle OT Introduction and Context
Clinical context from a Pinnacle occupational therapist
"Video modelling is classified as an evidence-based practice for autism."
NCAEP Evidence-Based Practices Report, 2020
NCAEP Evidence-Based Practices Report, 2020
Share This With Your Family
Consistency across caregivers multiplies therapeutic impact. When grandparents, teachers, and family members understand pattern aversion, every interaction reinforces your child's progress — rather than inadvertently undermining it.
"Explain to Grandparents" Version
"[Child] has difficulty with certain visual patterns — stripes, grids, checkers. The eye doctor confirmed vision is perfect. This is how their brain processes that type of visual information — it creates real discomfort. Certain tools (coloured transparent sheets, simple glasses, covered patterned surfaces) help significantly. We are not indulging a preference. We are managing a genuine neurological difference. The science supports this clearly. Your consistency with these tools at home directly helps [child]."
Share Options
📱 Share on WhatsApp
📧 Email this page
🔗 Copy link to share directly
📧 Email this page
🔗 Copy link to share directly
Downloads Available
- Family Guide PDF — Pattern Aversion Explained for the Whole Family
- Teacher Communication Template — A072
- Pattern Aversion Session Log — A072
The self-advocacy card set (M9) is available in multiple Indian languages — ensuring every family member across generations can support your child consistently.

Frequently Asked Questions
These are the questions our clinical teams hear most often — answered with the same precision and warmth we bring to every Pinnacle interaction.
Is pattern aversion the same as Irlen Syndrome?
Irlen Syndrome (scotopic sensitivity syndrome) is a specific diagnosis involving visual stress from pattern and contrast. Pattern aversion is a broader sensory processing phenomenon that may include Irlen features. A developmental optometrist can assess whether formal Irlen diagnosis is appropriate.
My child's eye doctor said everything is normal. Why are they still affected?
Pattern aversion is a processing difference, not an eye structure problem. The eyes relay information correctly — it's the brain's interpretation of specific patterns that creates distress. Normal eye exams are expected. The issue is upstream of the eye exam's scope.
At what age can we start coloured overlay assessment?
As young as 3 years old with appropriate materials. Young children can indicate preference (reaching for, engaging more with a coloured material) even without verbal report.
Can pattern aversion improve permanently over time?
Some children develop increasing tolerance and require fewer accommodations as the visual system matures. Others find effective management tools that reduce functional impact significantly. Functional participation with appropriate support is the goal — many adults manage pattern sensitivity successfully with minimal accommodations.
Can I do this intervention without a therapist?
Environmental modifications (M4), preparation tools (M8), and self-advocacy tools (M9) can begin immediately at home. Coloured overlays (M1) can be self-trialled. Gradient exposure (M6) and precision tinting (M3) require professional guidance without exception.
How does pattern aversion relate to my child's autism diagnosis?
Pattern sensitivity is among the most common sensory features in autism, affecting an estimated 80% of children with ASD (PMC11506176). It is a core sensory processing feature, not a secondary symptom. Addressing it directly through the interventions on this page is evidence-based autism therapy.

You Arrived Searching. You Leave Equipped.
You now have the name for what your child experiences, the neuroscience behind it, the materials that help, the step-by-step protocol, the safety framework, and the evidence to advocate for your child in any room. That is everything you need to begin.
🟡 Start This Technique Today
Begin with your EverydayTherapyProgramme™ via GPT-OS®. Track progress from Day 1. Your data personalises every subsequent recommendation.
🟢 Book a Consultation
70+ locations across India. Professional OT assessment, coloured overlay colorimetry, and full sensory profile available near you.
⚪ Explore the Next Technique
A-080: Community Environment Navigation with Sensory Tools — build on what you have started and take the tools into the world.
FREE: 9100 181 181 — National Autism Helpline | 16+ Languages
Validated by: 🩺 OT • 🗣 SLP • 🧩 ABA/BCBA • 📚 Special Education • 🧠 NeuroDev Paediatrics • 👶 Paediatrics • 🔬 CRO
Validated by: 🩺 OT • 🗣 SLP • 🧩 ABA/BCBA • 📚 Special Education • 🧠 NeuroDev Paediatrics • 👶 Paediatrics • 🔬 CRO
Preview of 9 materials that help with pattern aversion Therapy Material
Below is a visual preview of 9 materials that help with pattern aversion therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.









Link copied!

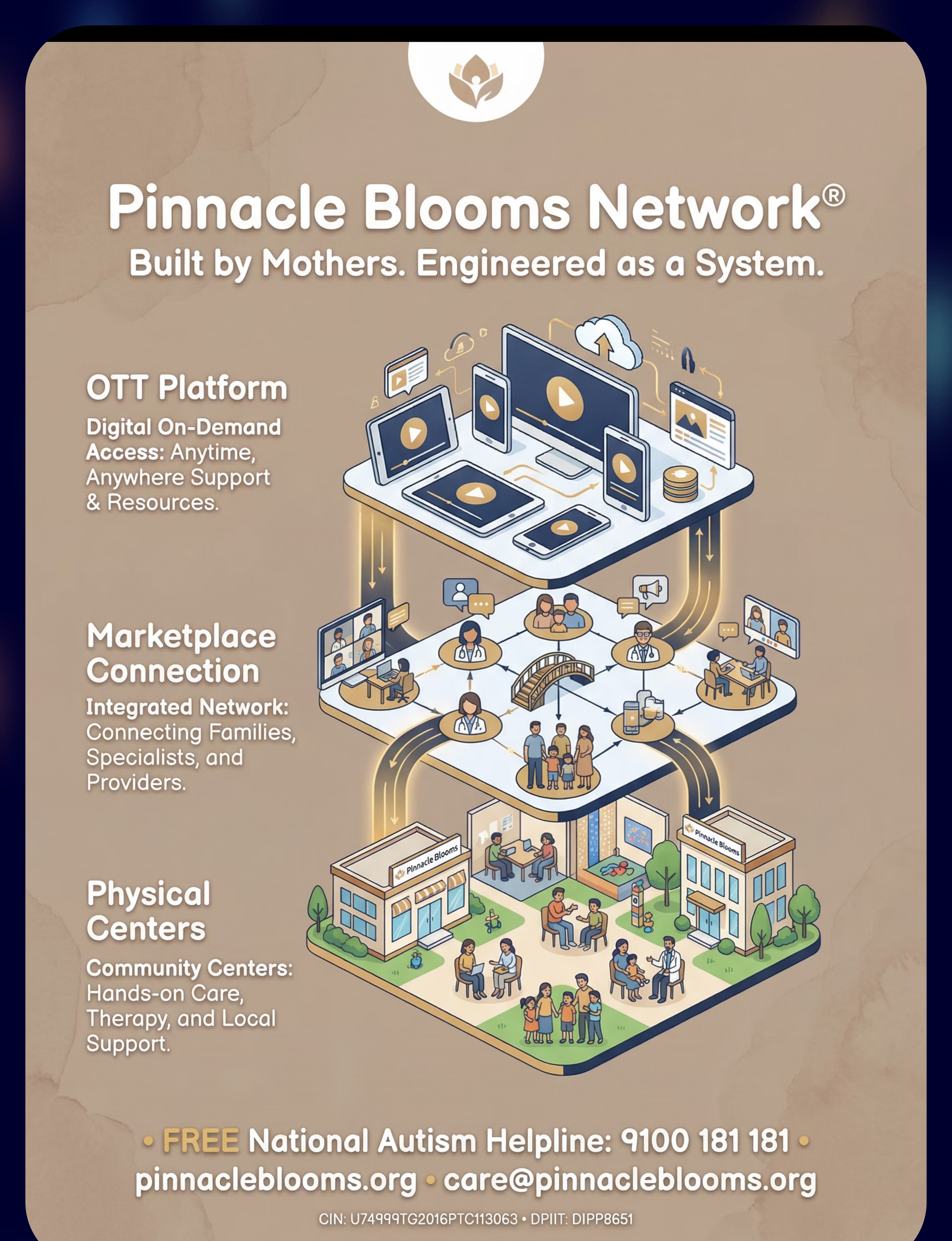
The Pinnacle Promise
Built by Mothers. Engineered as a System.
"From fear to mastery. One technique at a time." — Pinnacle Blooms Consortium
Pinnacle Blooms Network® exists to transform every Indian home into a proven, scientific, 24×7, personalised, multi-sensory, multi-disciplinary paediatric therapy environment — powered by GPT-OS® and the clinical authority of India's largest integrated paediatric therapy consortium. This page is one of 70,000+ evidence-based technique pages in the Pinnacle GPT-OS® library.
Medical Disclaimer: This content is educational in nature and is produced by the Pinnacle Blooms Network® multi-disciplinary consortium. It does not replace assessment, diagnosis, or treatment by a licensed occupational therapist, developmental optometrist, speech-language pathologist, applied behaviour analyst, special educator, or physician. Significant visual discomfort should be professionally evaluated. Individual results may vary. Statistics represent aggregate outcomes across the Pinnacle Blooms Network® with individual variation expected.
Contact Us
📞FREE National Autism Helpline: 9100 181 181 (16+ languages)
🌐 pinnacleblooms.org
📧 care@pinnacleblooms.org
🌐 pinnacleblooms.org
📧 care@pinnacleblooms.org
Copyright & Statutory Identifiers
© 2025 Pinnacle Blooms Network®, unit of Bharath Healthcare Laboratories Pvt. Ltd. All rights reserved. Technique A-072. GPT-OS® is a registered proprietary platform.
CIN: U74999TG2016PTC113063 | DPIIT: DIPP8651 (Govt. of India) | MSME: Udyog Aadhaar TS20F0009606 | GSTIN: 36AAGCB9722P1Z2
Technique A-072
Domain A: Visual Sensory
GPT-OS® v2.0