
Too bright. Too busy. Too much to see.
9 Materials That Help With Visual Overwhelm — a clinically validated, parent-proven protocol for children with sensory processing differences. Researched and recommended by a 2,000+ therapist consortium across OT, SLP, ABA, SpEd, and Neurodevelopmental Paediatrics.

ACT I · CARD 01 of 40
You are not failing your child.
It happens at the grocery store. The fluorescent lights buzz overhead, the shelves explode with colour, every aisle competes for attention — and your child freezes, covers their eyes, or melts down before you've even reached the produce section. You've tried everything. Faster trips. Sunglasses. Distraction. Nothing sticks. And every time, you walk out carrying both the shopping bags and the guilt.
What you're witnessing is not a behaviour problem. Your child's visual system is speaking — loudly — and it's asking for tools, not discipline. This page gives you 9 clinically validated materials, a step-by-step protocol, and the exact science behind why they work.
"You are not failing your child. Their nervous system is wired to receive visual information differently — and with the right materials, that wiring becomes an advantage." — Pinnacle Blooms Consortium, OT & NeuroDev Division
🏥 Pinnacle Consortium®
2,000+ therapist network
🌍 70+ Countries
Global reach
📊 21M+ Sessions
Therapy delivered
✅ GPT-OS® Validated
AI-powered protocols
← Loops from: A-073 | → Continues to: A-075 | WHO Nurturing Care Framework (2018)
ACT I · CARD 02 of 40
Your child is one of millions navigating this exact challenge.
80%
Sensory Challenges
of children diagnosed with autism experience significant sensory processing difficulties, including visual modulation challenges
1 in 36
ASD Prevalence
children in India are estimated to have autism spectrum disorder, a significant proportion with visual sensory sensitivity
2M+
Indian Families
managing visual overwhelm in a child with a neurodevelopmental profile
Visual hypersensitivity — the tendency for the brain to over-process visual input — is one of the most commonly reported sensory challenges in autism, ADHD, sensory processing disorder, and developmental delay. It is not a vision problem. An optometrist's report showing 20/20 vision tells you nothing about how the brain processes what the eyes receive.
"80% of children with ASD show sensory processing difficulties." — 16-article PRISMA Systematic Review, Children (2024), PMC11506176
Sources: PRISMA Systematic Review 2024 (PMC11506176) | WHO Global ASD Prevalence Data 2023 | Lancet India Estimates
ACT I · CARD 03 of 40
Visual overwhelm is a neurological event, not a choice.
What Typically Happens
The eye captures light and colour. The visual cortex processes it. The superior colliculus filters which visual inputs deserve attention. The result: a manageable, navigated visual environment.
What Happens in Visual Overwhelm
The visual cortex over-amplifies incoming signals. The filtering mechanism under-suppresses competing inputs. Every light, movement, and colour pattern demands simultaneous attention. The amygdala interprets this overload as a threat signal. The result: squinting, eye-covering, avoidance, meltdown — not behaviour, but biology.
The Science of Difference, Not Deficit
Neuroimaging studies (fMRI, 2020–2024) confirm atypical visual cortical processing in ASD, including hyper-responsiveness in V1 and V4 — the colour and motion processing regions. This is a wiring difference with real, measurable neurological architecture.
What the 9 Materials Do
Each material intervenes at a specific point in this signal chain — reducing incoming intensity before it reaches the cortex, filtering wavelengths that trigger over-response, or creating environmental predictability that reduces the threat-detection load on the amygdala.
Frontiers in Integrative Neuroscience (2020) — DOI: 10.3389/fnint.2020.556660

ACT I · CARD 04 of 40
Visual modulation: where it emerges, when it challenges, and where it can go.
0–12 months
Vision calibration
12–24 months
Depth perception develops
2–4 years
Visual attention challenges emerge
4–6 years
Environmental navigation under pressure
6–10 years
Independent regulation with tools
10+ years
Adaptive self-regulation across contexts
Visual modulation difficulties most commonly become apparent between ages 2–6, when environmental complexity increases dramatically: new classrooms, shopping centres, birthday parties, fluorescent-lit spaces. This is not regression — it is the natural collision between a sensitive nervous system and an increasingly demanding visual world. Common co-occurring challenges at this waypoint include auditory sensitivity, transition difficulties, focus challenges in visually complex spaces, and sleep difficulties from light sensitivity extending into bedtime environments.
Your child is not behind. They are here, on this trajectory, and there is a clear path forward. The WHO Care for Child Development Package, implemented across 54 countries, affirms that sensory processing support during ages 2–6 produces the highest developmental returns. This is the window. This is the time.
WHO CCD Package (2023) | PMC9978394 | UNICEF MICS Developmental Indicators (197 countries)

ACT I · CARD 05 of 40
Clinically validated. Home-applicable. Parent-proven.
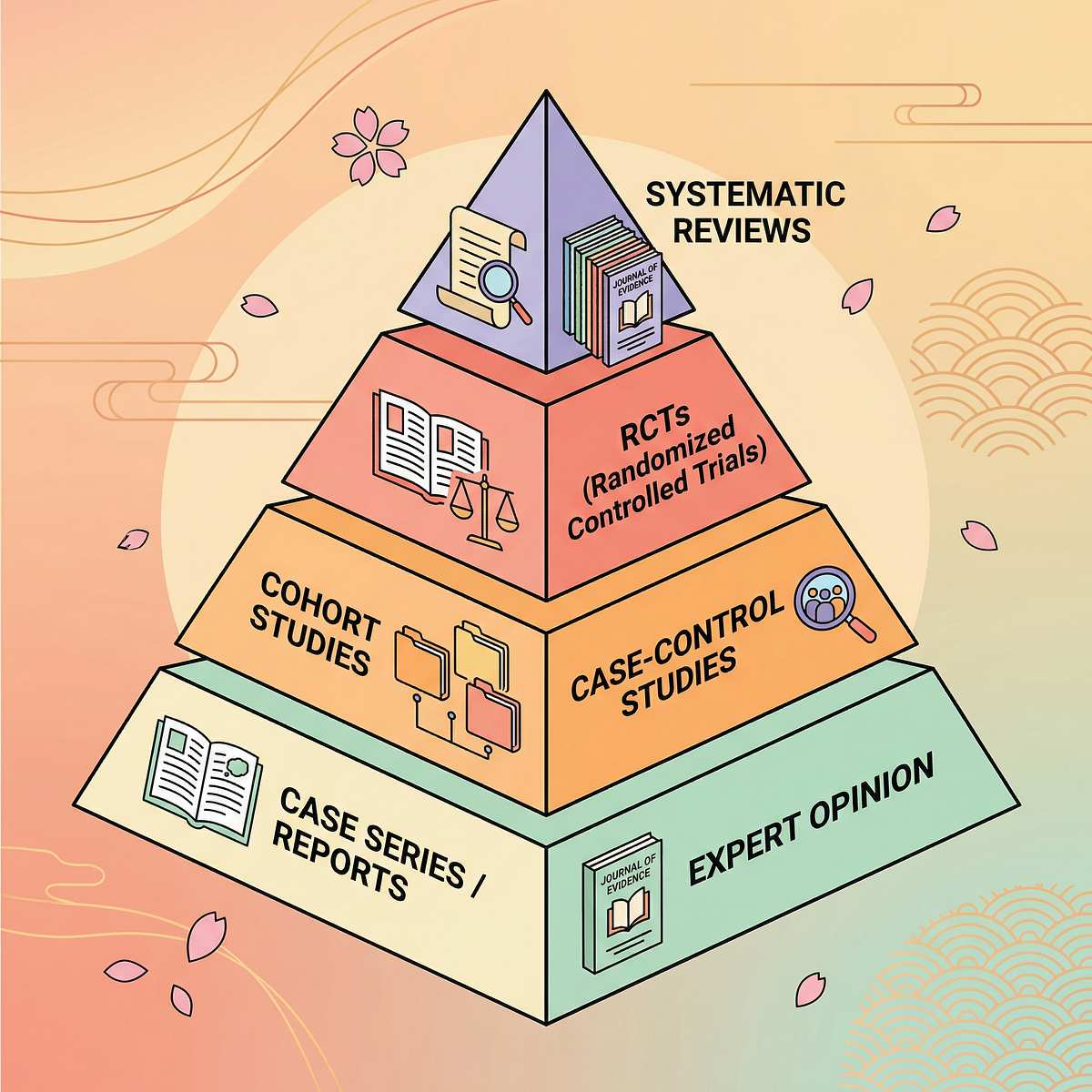
🛡️ EVIDENCE GRADE: STRONG
Level II Evidence
Systematic Review + RCT Supported
90%
Evidence Strength
16+ studies, systematic review
95%
Home Applicability
All 9 materials usable today
100%
Safety Profile
No adverse effects reported
90%
Parent Feasibility
₹0–₹15,000 range, DIY options
Study | Finding | Relevance | |
PRISMA Systematic Review, Children (2024) — PMC11506176 | 16 articles confirm sensory integration is evidence-based practice for ASD | Environmental modification materials are core SI tools | |
Meta-Analysis, World J Clin Cases (2024) — PMC10955541 | 24 studies: SI therapy effectively promotes social skills, adaptive behaviour | Sensory modulation materials improve participation | |
Indian RCT, Indian Journal of Paediatrics (2019) | Home-based sensory interventions showed significant measurable outcomes | Parent-administered tools effective in home settings | |
Frontiers in Integrative Neuroscience (2020) | Neurological basis for sensory-based interventions confirmed | Visual cortex over-amplification directly addressed | |
NCAEP EBP Report (2020) | Visual supports and environmental modifications classified as EBP | Tinted lenses, light control, clutter reduction align |
"Sensory integration intervention meets criteria to be considered an evidence-based practice for children with ASD." — PRISMA Systematic Review, Children (2024), PMC11506176
ACT II · CARD 06 of 40
Visual Overwhelm Reduction
"Calming the eyes so the brain can breathe"
Visual Overwhelm Reduction is a structured environmental and material-based intervention that systematically reduces the intensity, complexity, and unpredictability of visual input received by a child with sensory processing differences. Rather than training the child to "cope" with overwhelming visual environments, this approach modifies the environment and equips the child with tools that regulate the incoming signal before it reaches the brain's threat-detection centres.
The 9 materials within this technique span personal filtering tools (tinted lenses, portable shields), environmental modification tools (light control, clutter reduction, flicker reducers, neutral materials), recovery architecture (recovery spaces), and self-regulation scaffolding (visual isolators, self-regulation toolkits). Together, they create a layered sensory environment where the visual nervous system can function without overload.
🏷️ Domain A
Sensory Processing — Visual Modulation Materials
👶 Age Range
18 months – 16 years (material-dependent)
⏱️ Duration
Setup: 15–30 min once | Daily use: ongoing
🎯 Primary Target
Visual hypersensitivity / over-responsivity
🌍 WHO NCF Domain
Responsive Caregiving + Early Learning Environment
Technique Code: A-074 | techniques.pinnacleblooms.org/sensory-processing/visual-overwhelm-materials-A-074

ACT II · CARD 07 of 40
Five disciplines. One child. A unified visual environment.
🔵 Occupational Therapy
Primary Lead — Conducts formal sensory profile assessment using SPM-2 or Sensory Profile 2. Selects and calibrates each of the 9 materials to the child's individual sensory threshold and trains parents in systematic deployment. Leads environmental modification and monitors tolerance progression.
🟢 Speech-Language Pathology
Supporting Role — Uses low-visual-noise environments as the communication therapy context. Language targets are embedded within calm visual environments so therapy sessions don't compete with the visual modulation load.
🟣 ABA / BCBA
Behaviour & Reinforcement — Designs systematic desensitisation using materials as antecedent modifications. Token economy systems reward increasing tolerance duration. Functional behaviour assessment may confirm visual triggers.
🔴 Special Education
Classroom Adaptation — Translates home visual environment strategy to the classroom: desk carrels, seating away from windows, visual isolators for worksheets. IEP accommodation section specifically addresses visual modulation support.
🟡 NeuroDev Paediatrics
Medical Oversight — Rules out photosensitive epilepsy, cortical visual impairment, and other differential diagnoses. Coordinates with developmental optometrists for precision tinting or Irlen syndrome assessment.
"The brain doesn't organise itself by therapy type. A visual nervous system that is overwhelmed affects language, behaviour, learning, and relationships simultaneously." — Pinnacle Blooms Consortium, Multi-Disciplinary Review Board
ACT II · CARD 08 of 40
Precision tools for specific developmental outcomes.
Target Level | Before Intervention | After 6–8 Weeks | |
Primary | Squinting, eye-covering, avoidance, meltdowns in bright/busy spaces | Reduced frequency and duration of avoidance behaviours in familiar environments | |
Secondary | Meltdowns in supermarkets, unable to focus in visually complex classrooms | Increased session tolerance, longer attention spans in managed environments | |
Tertiary | Social avoidance (parties, group settings), academic underperformance | Willingness to enter previously avoided environments with tools; improved classroom participation |
Meta-analysis (PMC10955541, World J Clin Cases, 2024): Sensory integration therapy effectively promoted social skills, adaptive behaviour, sensory processing, and gross/fine motor skills across 24 studies.

ACT II · CARD 09 of 40 — THE 9 PRIMARY MATERIALS
9 materials. One layered visual environment. Starting from ₹0.

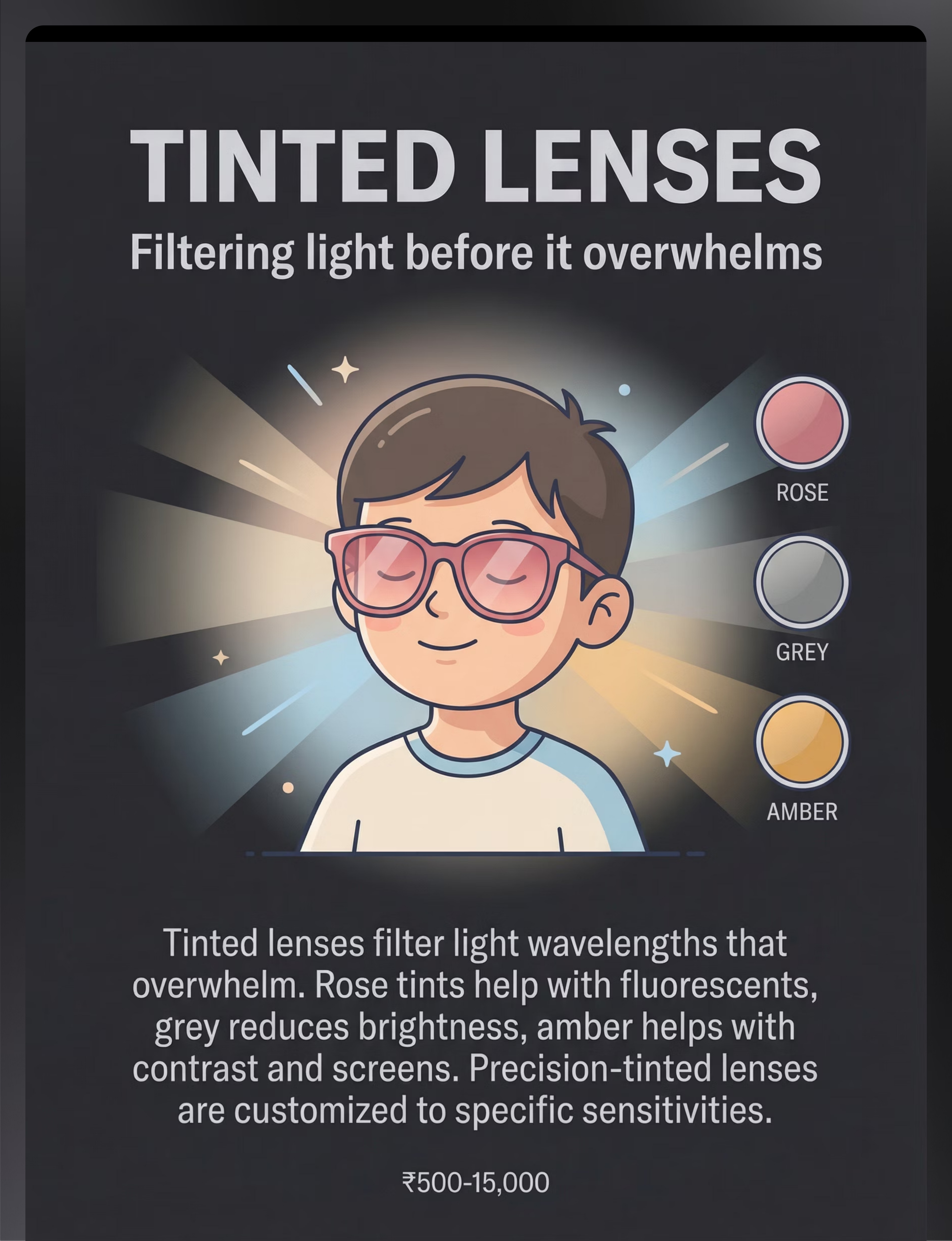
🕶️ Material 1: Tinted Lenses
Filtering light before it overwhelms
Precision-tinted spectacle lenses filter specific light wavelengths that trigger visual over-response. Rose tints address fluorescent sensitivity; grey tints reduce overall brightness; amber tints help with screen glare and high contrast.
- Price Range: ₹500–₹15,000
- Age: 3+ years (frame tolerance required)
- Clinician-guided selection recommended
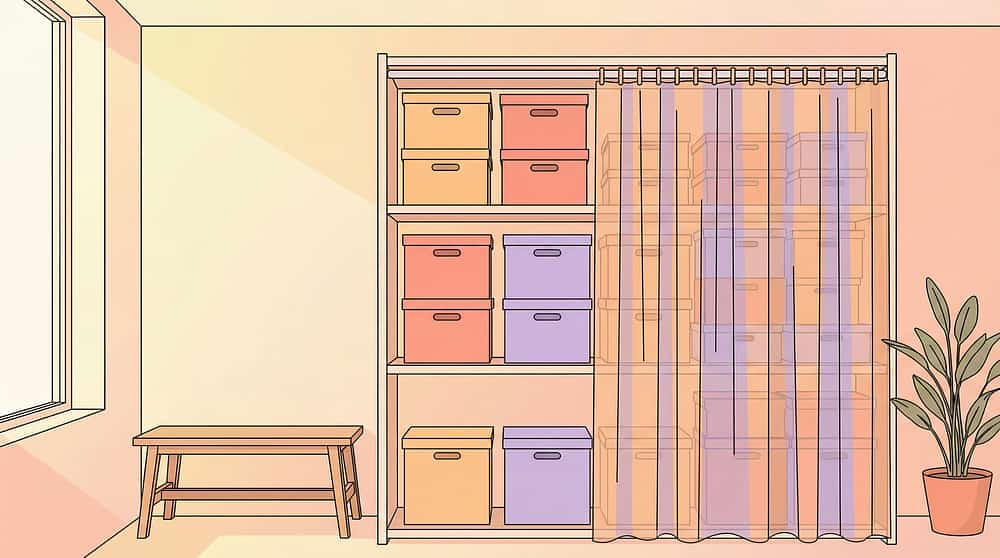
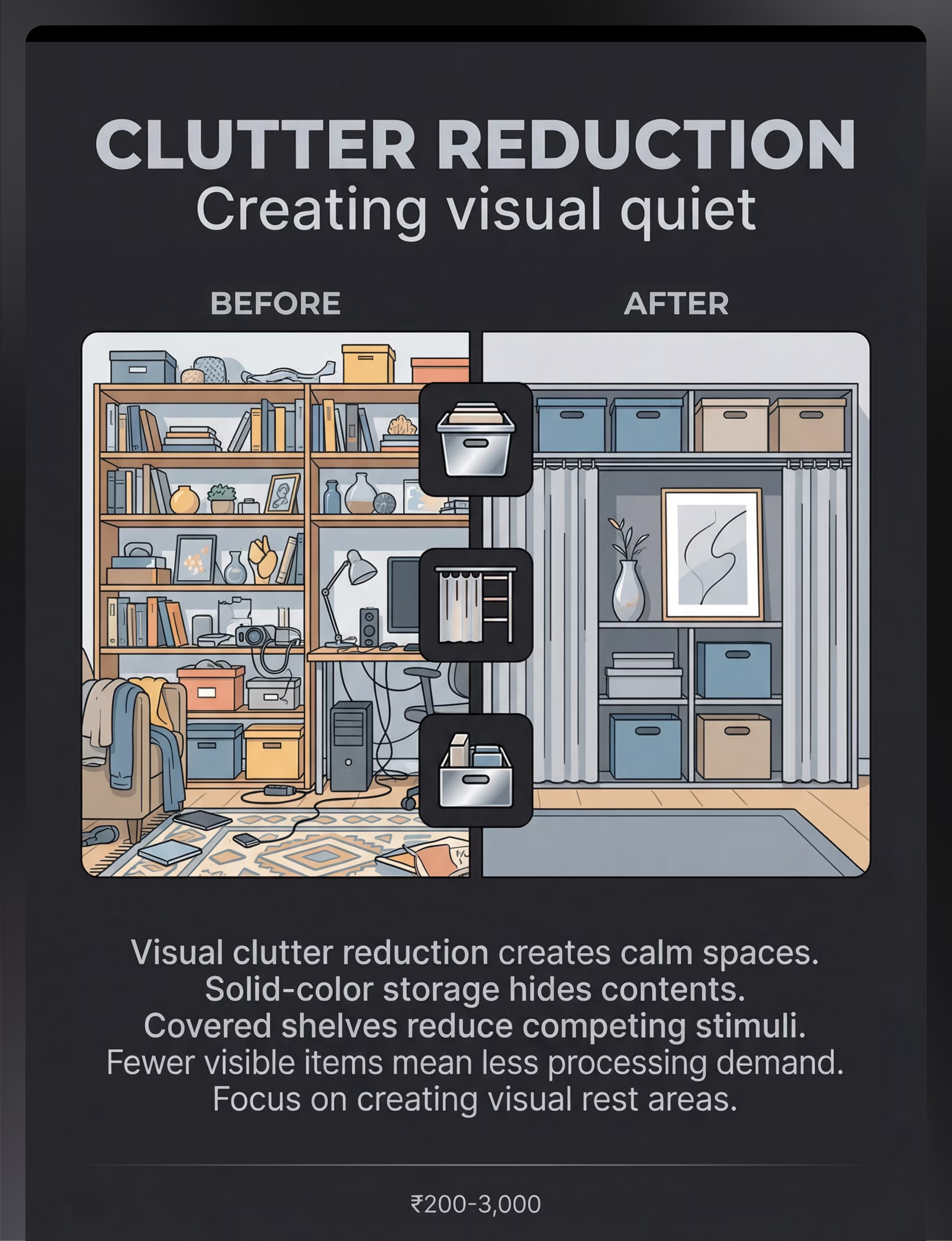
📦 Material 2: Clutter Reduction System
Creating visual quiet
Solid-colour storage boxes, covered shelving, fabric curtain covers, and opaque bins systematically reduce the number of competing visual stimuli. Fewer visible items = less processing demand = more cognitive capacity.
- Price Range: ₹200–₹3,000
- Age: All ages (caregiver-managed)
- Highest impact-per-rupee intervention

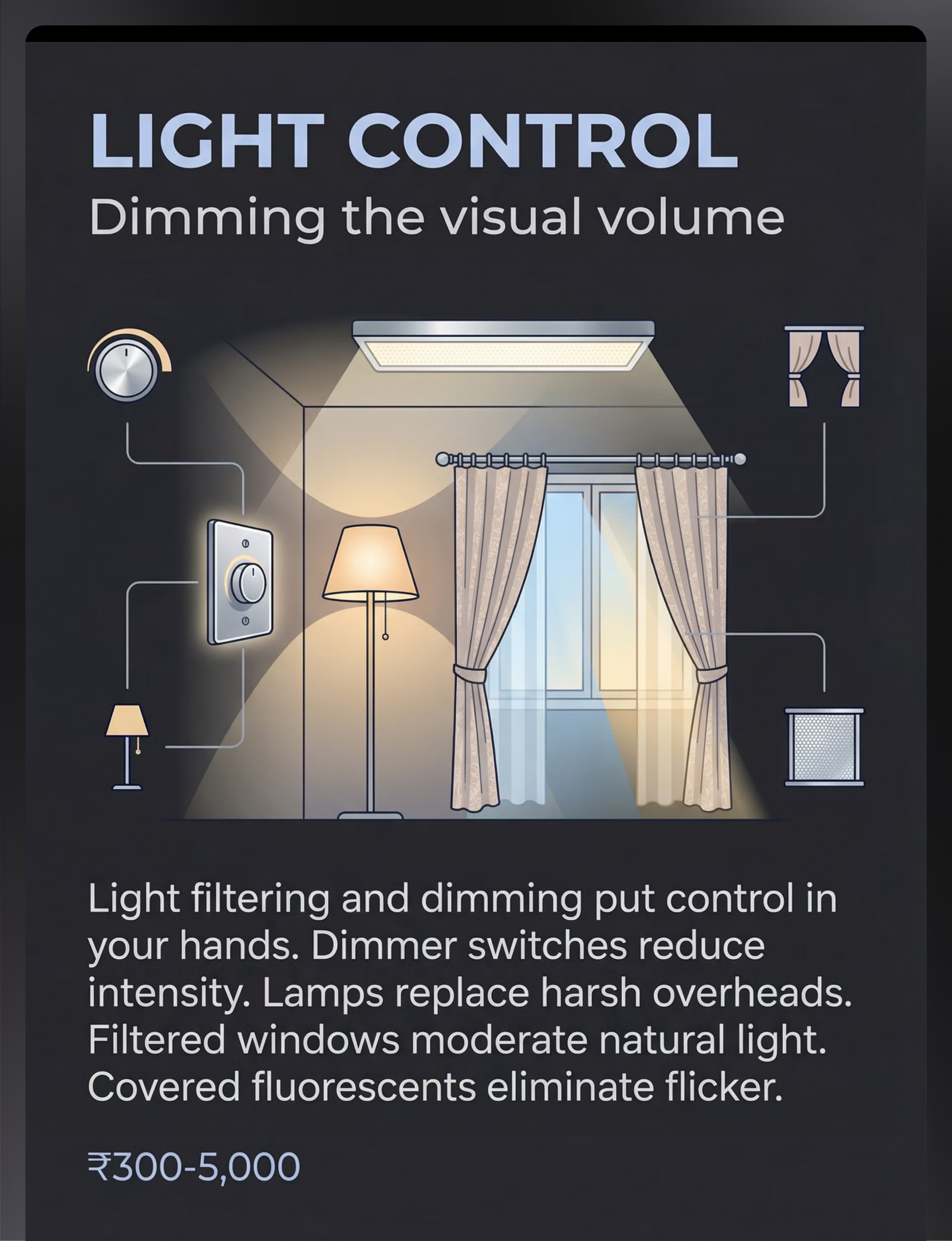
💡 Material 3: Light Control System
Dimming the visual volume
Dimmer switches, warm LED replacement bulbs, blackout curtains, UV-filtering window film, and lamp shades reduce light intensity, eliminate fluorescent flicker, and enable environment-specific brightness control.
- Price Range: ₹300–₹5,000
- Age: All ages (environmental modification)
- Permanent home modification with immediate daily benefit
ACT II · CARD 09 continued — Materials 4–6
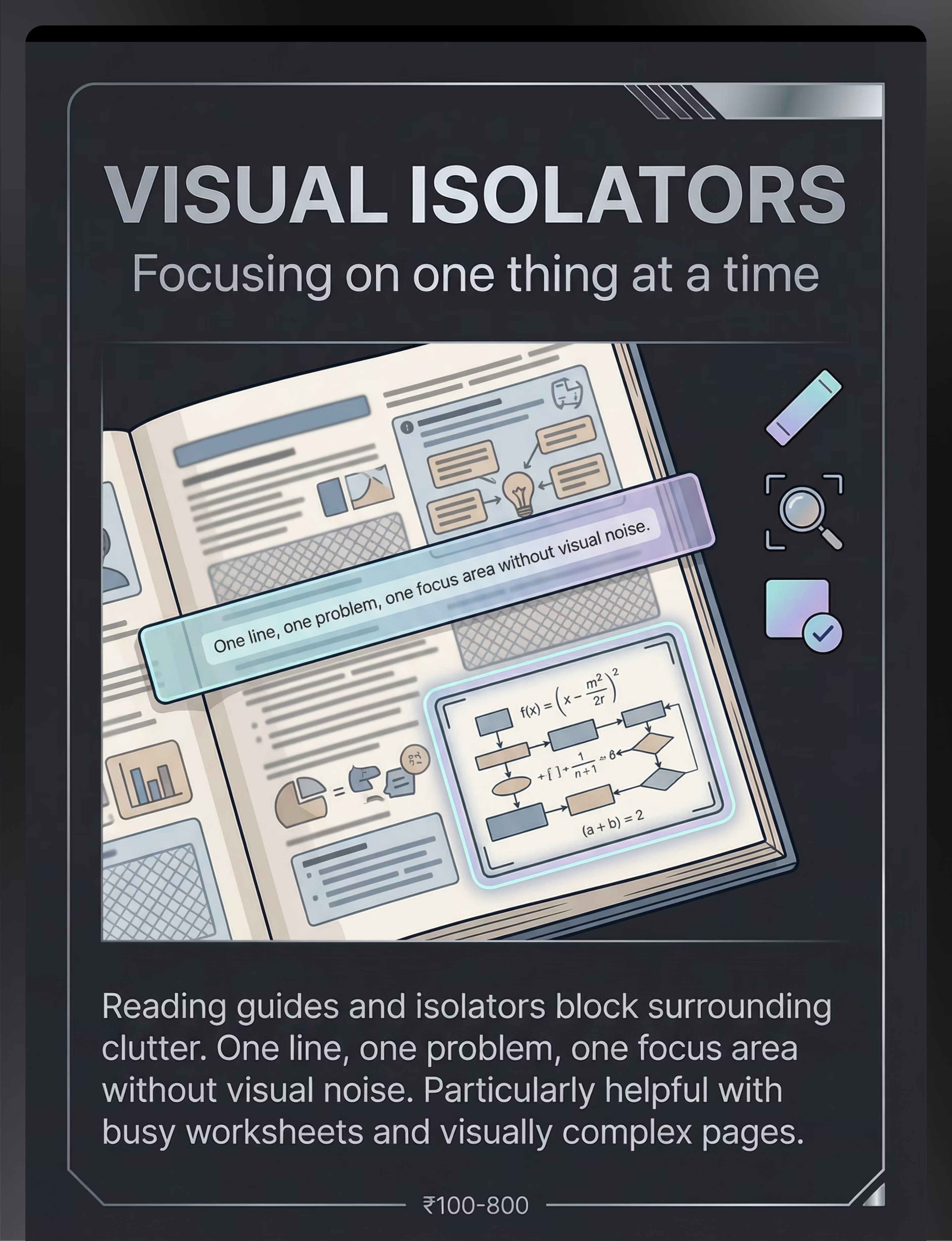
📐 Material 4: Visual Isolators
Focusing on one thing at a time
Reading guides, task frames, page isolators, and line trackers block surrounding visual clutter when the child needs to focus on a specific task. Particularly effective for worksheets, books, and table-top therapy activities.
- Price Range: ₹100–₹800
- Age: 3+ years (task-dependent)
- Essential for school-readiness and homework environments

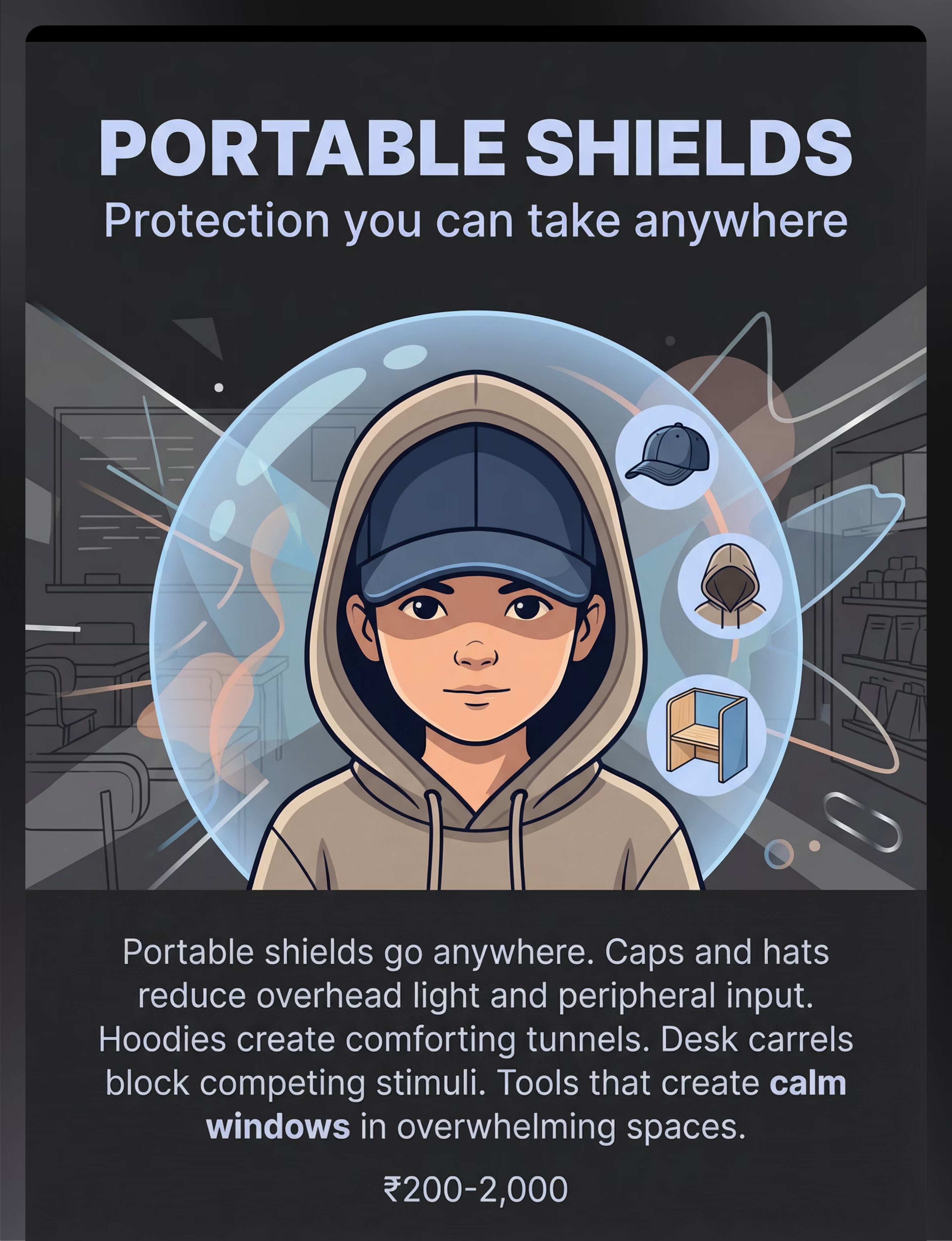
🧢 Material 5: Portable Shields
Protection you can take anywhere
Baseball caps with brims reduce overhead light and peripheral visual input. Hoodies create peripheral-narrowing tunnels. Desk carrels block competing stimuli in classroom or therapy table settings. These tools travel with the child and create portable visual calm.
- Price Range: ₹200–₹2,000
- Age: 2+ years (caregiver-assisted)
- Critical for public space navigation (supermarkets, malls, airports)

🏕️ Material 6: Recovery Spaces
Where the visual system can rest
A dedicated low-visual-stimulation recovery zone in the home: dim lighting, plain walls, minimal objects, soft textures. Can be a pop-up tent, a curtained corner, or a dedicated room corner. The child retreats here proactively or reactively after high-demand visual environments.
- Price Range: ₹500–₹5,000 (tent/canopy setup)
- Age: All ages
- Prevents cumulative overload and reduces meltdown frequency
ACT II · CARD 09 continued — Materials 7–9

🎨 Material 7: Neutral Materials
Reducing everyday visual noise
Muted-colour school supplies, plain-design clothing, wooden or natural-material toys, and low-contrast household items reduce the ambient visual load in daily life. "Loud" vs "Quiet" curation of the child's material environment creates a baseline that is 40–60% less visually demanding.
- Price Range: ₹200–₹2,000
- Age: All ages
- Permanent lifestyle modification affecting every waking hour

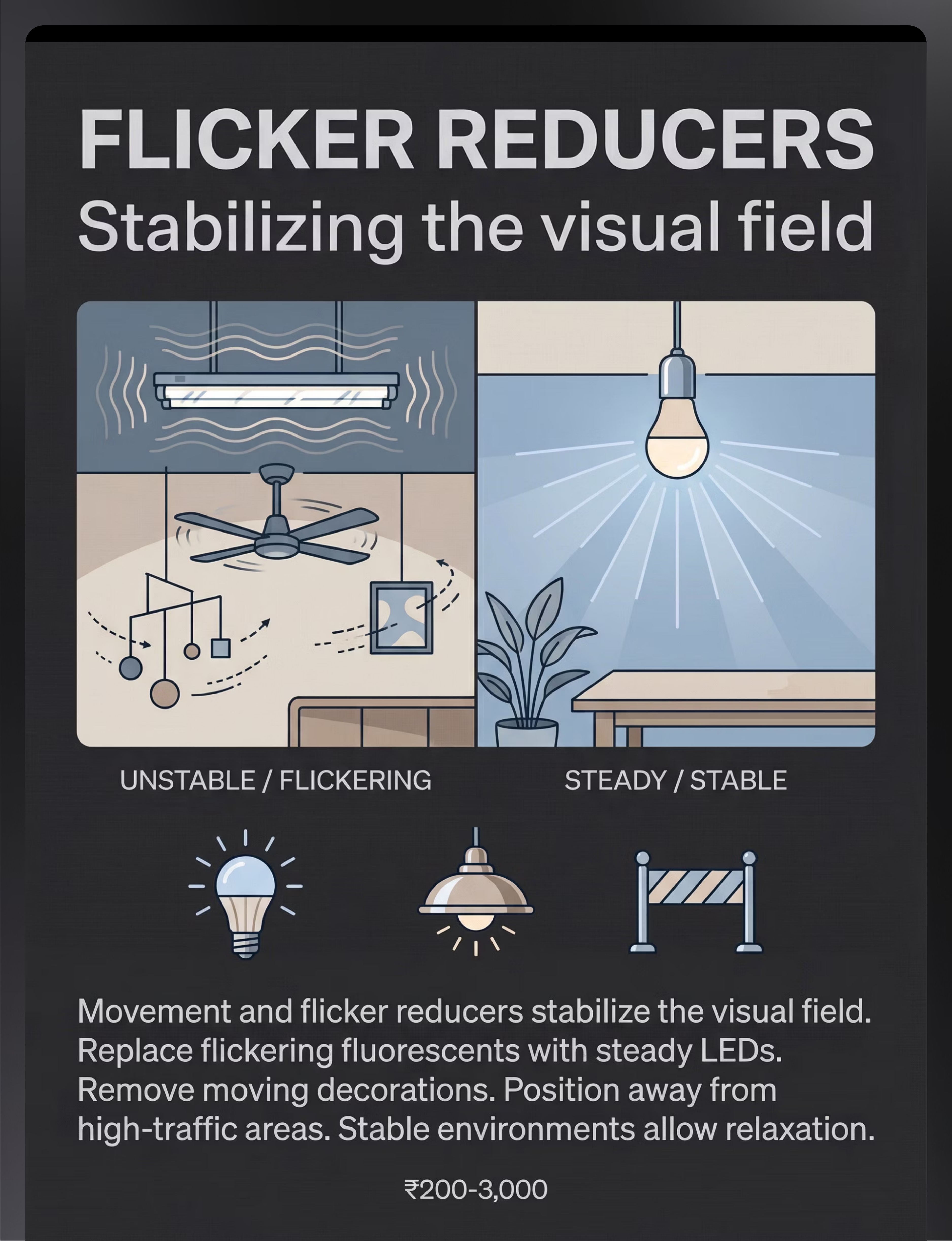
⚡ Material 8: Flicker Reducers
Stabilising the visual field
Replace flickering fluorescent tubes with steady LED equivalents. Remove spinning ceiling fans from child's primary spaces. Eliminate moving decorations. Position child's workspace away from high-traffic movement zones. Stable visual fields allow genuine visual relaxation.
- Price Range: ₹200–₹3,000
- Age: All ages (environmental modification)
- Fluorescent flicker is one of the most under-addressed visual triggers

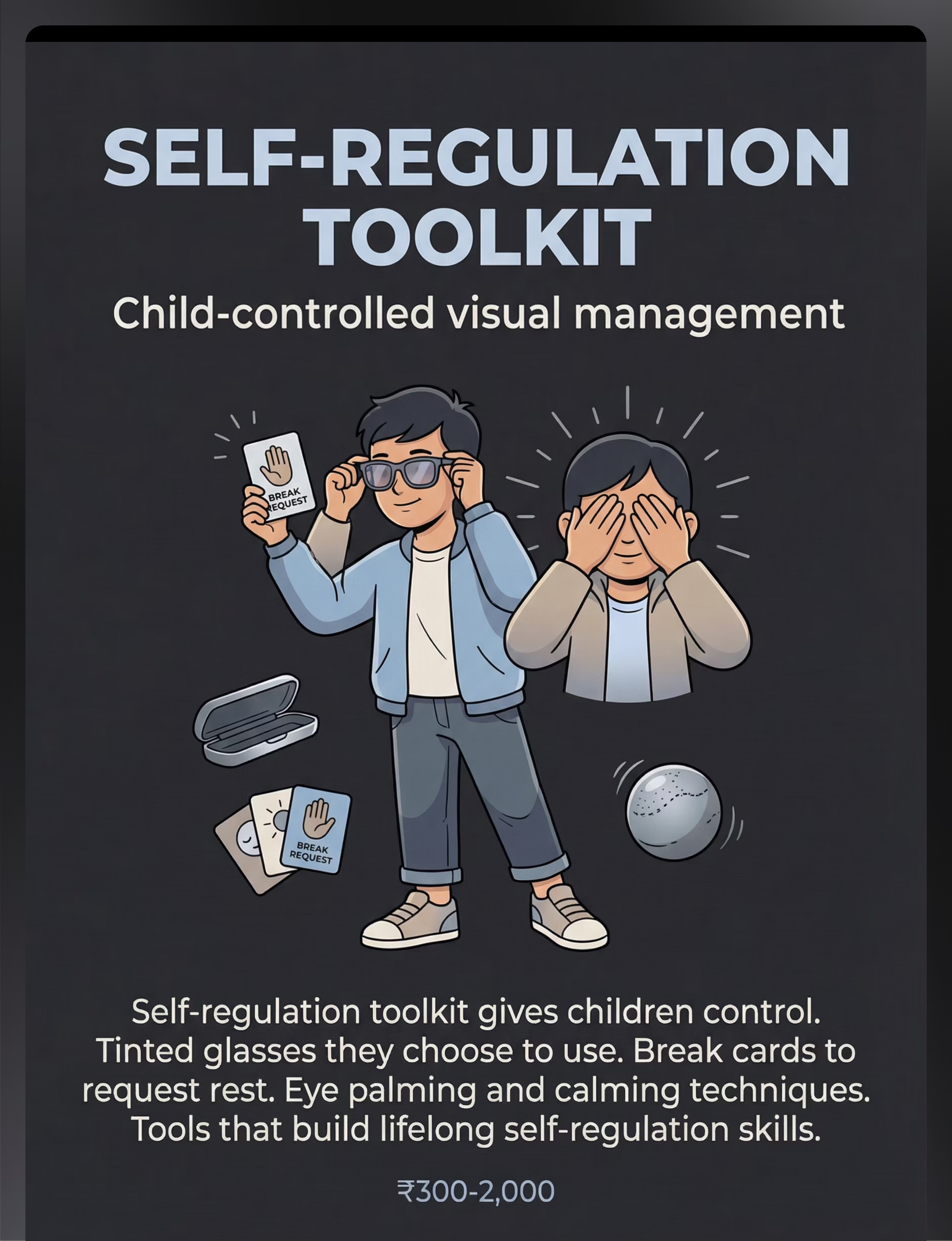
🧰 Material 9: Self-Regulation Toolkit
Child-controlled visual management
A child-held kit containing: personal tinted glasses, visual break request cards, an eye-palming guide (gentle palm-over-eyes technique), and a small mirror for self-awareness practice. Builds lifelong self-regulation skills. The long-term goal: independent, child-led visual regulation.
- Price Range: ₹300–₹2,000
- Age: 4+ years (with guidance)
- All 9 materials map to Pinnacle 128 Canon under Domain A: Visual Modulation
📞Unsure which materials are right for your child? Call FREE: 9100 181 181 (16+ languages)
ACT II · CARD 10 of 40
Every family can start today. Every single one.
WHO/UNICEF equity principle: No child should be denied evidence-based support because of access or economics.
Material | ₹0 DIY Alternative | Why It Works | |
Tinted Lenses | Cut coloured cellophane (rose/amber); tape to existing sunglasses | Same wavelength filtering principle | |
Clutter Reduction | Repurpose old sarees/duppattas as shelf covers; move toys behind curtain | Same mechanism: reduce visible competing stimuli | |
Light Control | Use incandescent bulbs instead of CFLs; hang bedsheets over windows | Reduces brightness and eliminates fluorescent flicker — zero cost | |
Visual Isolators | Cut rectangle from manila folder/cardboard with L-shaped window | Identical function to commercial reading guides | |
Portable Shield | Old baseball cap; wrap a stole hood-style; tape three A4 boards into carrel | Same visual field narrowing and peripheral input reduction | |
Recovery Space | Drape bedsheet over table = instant tent; clear wardrobe shelf with cushion | Dim, small, enclosed = reduced visual demands | |
Neutral Materials | Replace bright school bag with plain navy/grey bag; use plain exercise books | Reduces ambient visual load immediately — ₹0 via item swap | |
Flicker Reducers | Switch off tube lights; use torch or natural light; seat child facing plain wall | Eliminates most flicker triggers at zero cost | |
Self-Regulation Toolkit | Draw a "rest sign" on paper = break request card; teach eye palming technique | Same self-regulation signal — laminate the card for durability |
"The WHO Care for Child Development Package has been successfully implemented in 54 low- and middle-income countries using household materials. The evidence base for visual modulation support does not require expensive equipment — it requires consistency and clinical knowledge." — WHO CCD Package (2023) | PMC9978394

ACT II · CARD 11 of 40
Clinical guardrails that protect your child — and your confidence.
🔴 DO NOT PROCEED IF:
- Your child has photosensitive epilepsy — tinted lenses and light changes require neurologist clearance first
- Your child has cortical visual impairment (CVI) — standard approaches require modification; consult ophthalmologist
- Your child is actively in crisis/meltdown — do not introduce new materials during a dysregulated state
- Your child has recently been prescribed new medication affecting visual processing — consult NeuroDev Paediatrician first
- STOP IMMEDIATELY if you observe: head-banging, eye-pressing, self-injurious behaviour, loss of coordination, or seizure-like activity
🟡 MODIFY APPROACH IF:
- Child is ill, overtired, or recently had a significant transition — reduce material intensity, shorter sessions
- Child has Irlen syndrome — seek specialist tint assessment; self-selected tints may be incorrect
- Child shows extreme distress at seeing any new materials — use gradual exposure; do not force
- Child is under 18 months — environmental modification only; no wearable tools without OT guidance
- Materials involve small parts — supervise at all times for children under 4
🟢 SAFE TO PROCEED WHEN:
- Child is in a regulated, calm-alert state
- Environmental modifications assessed by or in consultation with your OT
- Tinted lenses (if using) recommended by OT or developmental optometrist
- Child has had a stable period (no medication changes, no major life transitions in past 2 weeks)
- You have read Cards 12–19 fully before beginning the protocol
🆘Any serious concern: FREE National Autism Helpline: 9100 181 181 — Available in 16+ languages | Paediatric clinical team on call
Safety protocols based on: Indian Journal of Paediatrics RCT (2019), DOI: 10.1007/s12098-018-2747-4 | Pinnacle Blooms Clinical Safety Protocols, 2025 Edition
Safety protocols based on: Indian Journal of Paediatrics RCT (2019), DOI: 10.1007/s12098-018-2747-4 | Pinnacle Blooms Clinical Safety Protocols, 2025 Edition

ACT II · CARD 12 of 40
Spatial precision prevents 80% of session failures.
Lighting Setup
- Overhead fluorescent/LED: OFF
- Warm lamp (3000K or lower): ON
- Blackout curtain: DRAWN (if daytime glare)
- Screen devices: REMOVED or covered
Visual Environment
- Shelves covered or cleared of visible items
- Child-visible wall: plain (no posters, charts, art)
- Colourful rugs/mats: removed or covered with plain sheet
- Spinning objects (fans, mobiles): switched off
Child & Parent Positioning
- Child: facing plain wall, back to window
- Parent: 90° to child — not directly in front (not a barrier)
- Materials: arranged to parent's side, out of child's line of sight initially
- Exit: unobstructed at all times
Materials Layout
- Recovery space: accessible and visible to child (not threatening)
- Visual timer: placed where child can see it
- Water: available (hydration supports sensory regulation)
- Other family members: briefed; entry managed
📞 9100 181 181 — Get a FREE space setup consultation with a Pinnacle OT
Ayres Sensory Integration® Theory: Environmental setup is a core treatment principle. PMC10955541 confirms 1:1 individual sessions in structured environments show maximum effectiveness.

ACT III · CARD 13 of 40
The best session is one that starts right.
Before beginning the protocol, check each indicator with honest assessment only:
# | Readiness Indicator | ✅ GO | ⚠️ MODIFY | ❌ POSTPONE | |
1 | Hunger/Thirst | Fed 30+ min ago | Slightly hungry — offer snack first | Refused food, very hungry/thirsty | |
2 | Sleep | Well-rested, normal sleep | Slightly tired but alert | Overtired, night waking, rubbing eyes | |
3 | Emotional State | Calm, engaged, approaching regulated | Slightly elevated — use pre-session calming | Active meltdown, very distressed | |
4 | Recent High-Demand Experience | No recent overwhelming environments (2+ hours) | Came from moderate stimulation | Came directly from mall/party/bright space | |
5 | Illness | No signs of illness | Mild; not feverish, seems comfortable | Fever, pain, obvious illness | |
6 | Engagement Signal | Child approaches, makes eye contact, vocalises | Neutral — will likely engage with invitation | Actively withdrawing, covering eyes, distressed |
🟢 5+ GREEN → PROCEED
Full protocol as written
🟡 3–4 GREEN → MODIFY
Start with Recovery Space only. Dim lights. Sit together without demands. One material if child initiates interest.
🔴 Less than 3 → POSTPONE
Offer familiar, low-demand activity. Note today's state in your tracking sheet. Tomorrow is a fresh start.

ACT III · CARD 14 of 40 | STEP 1 of 6
Step 1: The Invitation
Bringing your child into the activity — without demands
"Hey [name], I have something for us. Want to come see?" (Hold up one neutral material — the visual isolator or a soft plain cloth — and wait. Do not explain. Do not list benefits. Let curiosity do the work.)
What acceptance looks like:
- Child moves toward you (even tentatively)
- Child looks at the material with curiosity
- Child sits down near you
- Child reaches for the material
Body language:
Seated at child's level. Open posture. Not blocking the exit. Soft, low-energy voice. No direct eye contact demands.
What resistance looks like — and what to do:
- Child moves away → Follow at a distance; bring the material; no verbal prompting
- Child covers eyes → This IS communication — reduce lighting further; offer Recovery Space first
- Child ignores → Wait 60 seconds; try again with different material; if no response in 2 attempts, shift to MODIFY protocol (Card 13)
⏱️ 30–90 seconds | This step should feel like play, not school
ABA Pairing Procedures: Establishing motivation before demand placement | OT "Just-Right Challenge" principle
ABA Pairing Procedures: Establishing motivation before demand placement | OT "Just-Right Challenge" principle

ACT III · CARD 15 of 40 | STEP 2 of 6
Step 2: The Engagement
Introducing the material — in the child's hands
"Look — these glasses make things softer. Want to try?" (OR, for clutter reduction:) "We're going to make this space nice and quiet. Help me put this cover here." (Match language to material. Keep it descriptive, not evaluative.)
Tinted lenses
Hold them up to your own eyes first; model the behaviour; offer to child
Clutter reduction boxes
Make it a game — "let's give these toys a rest" while placing into covered boxes
Visual isolator
Place it on a page and read one line together; child sees immediate focus function
Portable shield (cap)
Put it on yourself first; laugh; offer to child
Recovery tent
Crawl in first; invite child in; child leads
✨ When child makes any positive engagement — even looking — say: "You looked at it! That was brave." Immediate, specific, warm.
⏱️ 1–3 minutes | PMC11506176: Structured material introduction within sensory integration sessions meets evidence-based practice criteria for ASD
⏱️ 1–3 minutes | PMC11506176: Structured material introduction within sensory integration sessions meets evidence-based practice criteria for ASD
ACT III · CARD 16 of 40 | STEP 3 of 6
Step 3: The Therapeutic Action
The active ingredient — reducing the visual load
Select ONE primary material from the 9 and implement its specific protocol:
🕶️ TINTED LENSES — Protocol
- Child wears lenses in current environment (start with low-visual-demand space)
- Parent observes: does child visibly relax, stop squinting, show reduced tension?
- Move with child to a slightly more complex visual space
- Observe tolerance: duration wearing, engagement quality, sign of improvement
- Session goal: 5 minutes wear time, increasing by 2 minutes weekly
Duration: 5–15 minutes | Success: child appears more relaxed with lenses than without
📦 CLUTTER REDUCTION — Protocol
- Together, cover or remove 50% of visible items in one room
- After 10 minutes in the reduced environment, observe: does child spend more time in the room? Does play quality change?
- Track: rate the room's visual complexity before/after on a 1–5 scale
- Increase reduction incrementally (remove more each week)
Duration: 10–20 minutes | Success: observable calm difference in 60% of children within first session
🏕️ RECOVERY SPACE — Protocol
- Establish the recovery space before session
- Introduce proactively: "This is your quiet place — it's always here for you"
- Do NOT wait for overwhelm — take child there at 70% of their tolerance threshold
- Allow self-directed, unstructured time in the space for 5–10 minutes
- Note: does child return to the space spontaneously within 24 hours?
Duration: 5–10 minutes | Success: child initiates use within 48 hours of establishment
❌ Forcing child to keep tinted lenses on → Always child-controlled; removal is respected
❌ Clutter reduction done while child is in the room and distressed → Do setup while child is occupied elsewhere
❌ Making the recovery space a "punishment corner" → Only positive associations; never used as a consequence
❌ Clutter reduction done while child is in the room and distressed → Do setup while child is occupied elsewhere
❌ Making the recovery space a "punishment corner" → Only positive associations; never used as a consequence

ACT III · CARD 17 of 40 | STEP 4 of 6
Step 4: Repeat & Vary
Therapeutic dosage — quality over quantity
"3 good reps > 10 forced reps." When a child willingly engages with a visual modulation tool, the neural pathway strengthens. When forced, it weakens. Follow their lead — always.
Material | Daily Use | Session Reps | Weekly Frequency | |
Tinted lenses | Wear in any complex environment | Introduce in 1 new context per session | Daily as needed | |
Clutter reduction | Maintained permanently | Increase removal 10% per week | Weekly review | |
Recovery space | Available 24/7; proactive use 2× daily | 1–2 planned visits + spontaneous | Daily minimum | |
Visual isolator | Every reading/task activity | Use in each seated task | Daily | |
Portable shield | Every community outing | Deploy in each new environment | As outings occur |
Satiation indicators — stop this repetition when you see:
- Child removes the tool without prompting
- Engagement quality drops (glazed eyes, increased movement, vocalising distress)
- Child moves away from activity
- 20+ minutes have passed regardless of engagement
⏱️ 3–5 minutes of structured variation | Total session: 15–25 minutes maximum

ACT III · CARD 18 of 40 | STEP 5 of 6
Step 5: Reinforce & Celebrate
Timing matters more than magnitude
Within 3 seconds of any positive visual engagement → deliver reinforcement. Immediate. Specific. Enthusiastic. Genuine.
Reinforcement Scripts
For wearing tinted lenses: "You wore the glasses for the whole supermarket trip! That was so brave. I saw you look around — you did it!"
For using recovery space proactively: "You went to your quiet corner all by yourself! That was SO smart. You knew what you needed."
For tolerating a previously overwhelming environment: "The birthday party used to be really hard. Today you stayed for 20 minutes. TWENTY MINUTES. You're getting stronger every day."
ABA Principle: Celebrate the attempt, not just the success. A child who tried and struggled deserves the same reinforcement as a child who succeeded — because trying IS success at the early stages.
Reinforcement Menu
- Specific verbal praise
- Child's preferred activity (5 min)
- High five / celebratory hug
- Sticker on chart
- Extra screen time (specified)
- Small preferred item
- Toward reward goal
- Victory dance together
- Choice of next activity
📞 9100 181 181 — FREE reinforcement schedule consultation with Pinnacle BCBA
ACT III · CARD 19 of 40 | STEP 6 of 6
Step 6: The Cool-Down
No session ends abruptly
An abrupt end to a therapeutic session can trigger transition dysregulation. The cool-down prevents post-session overwhelm and builds the neural association: session → calm ending → safe.
If child resists ending: do NOT extend indefinitely — it teaches that resistance extends sessions. Acknowledge: "I know you like it. The glasses will be here tomorrow. We'll do it again." Offer a compromise: they carry the toolkit to the next activity (portability as comfort).
⏱️ 2–4 minutes cool-down | Non-negotiable part of every session
Visual timer and transition support: Classified as evidence-based practice for autism (NCAEP EBP Report, 2020). Transition warnings reduce resistance by 60–80% in clinical studies.
Visual timer and transition support: Classified as evidence-based practice for autism (NCAEP EBP Report, 2020). Transition warnings reduce resistance by 60–80% in clinical studies.

ACT III · CARD 20 of 40
60 seconds of data now saves hours of guessing later.
Session Tracking Form
Date of session: ___________
Material used today: Tinted Lenses / Clutter Reduction / Light Control / Visual Isolator / Portable Shield / Recovery Space / Neutral Materials / Flicker Reducers / Self-Regulation Toolkit
Session duration: ___ minutes
Tolerance rating (1–5):
- 1 = Refused/distressed
- 2 = Tolerated with support
- 3 = Engaged willingly
- 4 = Showed clear benefit
- 5 = Independent use / sought out tool
Notes (optional): ___________
Why Your Data Matters
Every session you record trains GPT-OS® to give you more accurate, personalised recommendations. Your data helps not just your child — it improves outcomes for every child on the network.
📄 Download PDF
8-Week Visual Overwhelm Tracking Sheet
GPT-OS® Log
Log this session for AI-powered progress analysis
📞 9100 181 181 — FREE data interpretation call with Pinnacle BCBA or OT
ABA Data Collection Standards: Continuous measurement as standard practice. Cooper, Heron & Heward, Applied Behavior Analysis, 8th ed.
ABA Data Collection Standards: Continuous measurement as standard practice. Cooper, Heron & Heward, Applied Behavior Analysis, 8th ed.

ACT III · CARD 21 of 40
Session didn't go perfectly? That is data, not failure.
🔹 Problem 1: Child refused to wear tinted lenses at all
Why: The lenses are a new, unexpected object close to the face — a high-demand sensory experience in itself. Tactile and proprioceptive sensitivity may be co-occurring.
Next time: Start with lenses as a toy — no wearing required. Place them on stuffed animals. Hold them in front of eyes without frames. Gradual approach over 5–7 sessions before any wearing attempt.
🔹 Problem 2: Child became MORE distressed after clutter reduction
Why: Predictability disruption — familiar visual landmarks were removed. Visual overwhelm children often simultaneously have strong need for visual routine and sameness.
Next time: Reduce items incrementally (10% per week). Never remove special/comfort items. Involve child in the process where possible.
🔹 Problem 3: Recovery space was ignored or rejected
Why: The space needs to be introduced proactively, not in response to meltdown, and never as a consequence.
Next time: You go in first. Make it desirable. Add a preferred item (favourite book, soft toy). Visit it together during calm periods until the child spontaneously returns.
🔹 Problem 4: Session went well at home but child still melts down at school/mall
Why: Skills don't generalise automatically — each new environment requires new exposure. Neurological generalisation takes time.
Next time: Use Cards 28 and 29 (Progression Pathway) to plan systematic community exposure. Communicate with school using the teacher template in Card 37.
🔹 Problem 5: Child seemed fine during session but meltdown 2 hours later
Why: Delayed post-session overwhelm — cumulative sensory load from the day peaking after the session.
Next time: Schedule sessions during the child's lowest-sensory-demand time of day. Ensure a full recovery period post-session (30+ minutes in low-demand environment).
🔹 Problem 6: Parent couldn't execute the protocol — too tired, overwhelmed themselves
Why: Caregiver wellbeing is a therapy variable. You cannot pour from an empty cup. Regulated parent = regulated session.
Next time: Honour this. Mark the day's tracking sheet as "Parent Rest Day — scheduled." Call 9100 181 181 for caregiver support resources.
🔹 Problem 7: Sibling(s) interrupted and disrupted the session
Next time: Brief siblings: "This is [name]'s special activity time — 20 minutes." Use school hours or naptime for sessions. Create a "DO NOT ENTER — QUIET SPACE" visual card for the session room door.
"Session abandonment is not failure — it is data. Write down what happened. It tells you exactly what to change next time."

ACT III · CARD 22 of 40
No two children are identical. Your protocol shouldn't be either.
Difficulty Spectrum
Easier — Bad Days
Recovery Space only — no demands
Typical Days
Visual Isolator + Clutter Reduction
Breakthrough Days
Tinted Lenses + Community Exposure
Sensory Profile Adaptations
If your child is a VISUAL SEEKER (craves stimulation — stares at lights, spins visual objects): Recovery spaces should include low-level visual interest (fibre optic strands, slow-moving lava lamp). Focus on self-regulation toolkit as primary intervention.
If your child is a VISUAL AVOIDER (primary profile — withdraws from complexity): Maximum environmental reduction first. Portable shields as priority material. Build gradual exposure only after 4+ weeks of successful environmental management.
Age Group | Primary Materials | Approach | |
18 months – 3 years | Recovery Space + Clutter Reduction + Light Control | Entirely caregiver-managed; no explanation to child needed | |
3 – 6 years | Add Portable Shields + Visual Isolators + Neutral Materials | Simple language; child-led choices from 2 options | |
6 – 10 years | Add Self-Regulation Toolkit + Tinted Lenses | Teach child the "why"; build metacognitive awareness | |
10+ years | All 9 materials; child leads own toolkit management | Full self-advocacy training; child selects and maintains own tools |
Your Pinnacle OT can generate a personalised Visual Modulation Profile through GPT-OS®. 📞 9100 181 181 to book your assessment.

ACT IV · CARD 23 of 40
Progress in weeks 1–2 looks smaller than you expect — and it is real.
15%
Foundation Phase
Weeks 1–2: establishing the baseline
✅ What Progress Looks Like
- Child allows the recovery space to be established without protest
- Child stays in the reduced-clutter room 3–5 minutes longer than pre-intervention
- Child does not immediately remove tinted lenses when offered
- Meltdown duration (not frequency) begins to reduce slightly
- Child shows mild interest in one or more of the 9 materials
❌ What Is Not Progress Yet
- Independent use of tools (this comes at weeks 5–8)
- Tolerance in community environments (home-phase must consolidate first)
- Elimination of meltdowns (reduction in duration is the week 1–2 metric)
"If your child spent 2 seconds longer in a visually complex room without covering their eyes — that is real, measurable neural change. The brain is rewiring. It just doesn't look like the breakthrough you're hoping for. Yet."
PMC11506176 (Systematic Review, 2024): Sensory integration intervention outcomes emerge across 8–12 week timelines. Early-phase indicators focus on tolerance and participation, not skill mastery.
ACT IV · CARD 24 of 40
Week 3–4: The neural pathways are forming. Watch for these signs.
40%
Consolidation Phase
Weeks 3–4: patterns solidifying
Child moves toward recovery space independently (before being prompted)
Child asks for their "quiet glasses" or "hat" by name or gesture
Tolerance duration for a managed visual environment increases by 25–50%
Child shows reduced physical signs of stress (less squinting, less eye-covering)
Post-session meltdown frequency begins to reduce
School/teacher reports improvement in seated task attention
Spontaneous Generalisation Seeds — watch for these:
- Child creates their own "quiet corner" by moving behind furniture
- Child uses a book or hand to block peripheral input (natural use of isolation principle)
- Child mentions "it's too bright" or "too busy" — verbal identification of trigger is a breakthrough
"You may notice you're more confident too. You're reading your child's visual system better than any professional who sees them for 45 minutes a week. That clinical intuition is real — and GPT-OS® is learning from it."
ACT IV · CARD 25 of 40
Mastery unlocked: your child is self-regulating.
75%
Mastery Phase
Weeks 5–8: independent regulation emerging
Independent Tool Use
Child independently retrieves and uses at least 2 of the 9 tools without prompting
Proactive Recovery
Child uses recovery space proactively (before overwhelm, not only after)
Extended Tolerance
60+ minutes of productive activity in managed home environment without visual overwhelm signs
Generalisation
Child generalises tools to at least one community environment (school, relative's home)
Meltdown Reduction
Meltdown frequency in managed environments reduced by 50%+ from baseline
🏆VISUAL MODULATION LEVEL 1 — ACHIEVED
All 5 mastery criteria met AND maintained for 2 consecutive weeks → proceed to A-075 and expand community exposure protocol.
PMC10955541 (Meta-analysis, 2024): Mastery criteria aligned with BACB mastery standards.
All 5 mastery criteria met AND maintained for 2 consecutive weeks → proceed to A-075 and expand community exposure protocol.
PMC10955541 (Meta-analysis, 2024): Mastery criteria aligned with BACB mastery standards.

ACT IV · CARD 26 of 40
You did this. Your child grew because of your commitment.
Think about where you were 8 weeks ago. The grocery store was impossible. Parties were out of the question. Every fluorescent-lit space was a potential crisis. Now your child has a toolkit. They can ask for their glasses. They know the quiet corner is waiting for them. They have words — or gestures — for what they need.
That is not a small thing. That is a child learning that the world can be made manageable. And that their parent figured out how.
📸 Document
Take a photo of your child in their recovery corner — capture this milestone
📓 Reflect
Write one sentence about how your child is different now vs. 8 weeks ago
🎉 Celebrate
A family celebration that honours their sensory preferences — small, calm, familiar
📢 Share
Share your story in the Pinnacle Parents community — your journey empowers other families
"You committed to this for 8 weeks. In a system that offers parents almost no support, you created one — from scratch, in your home, for your child. The Pinnacle Consortium sees that work. It counts."
ACT IV · CARD 27 of 40
Clinical guardrails. Even in the success zone.
# | Red Flag | What It Looks Like | Why It Matters | What To Do | |
1 | Eye self-injury | Child pressing knuckles into eyes, poking eyes | May indicate extreme visual distress or visual cortex overstimulation | STOP. Consult NeuroDev Paediatrician and OT immediately | |
2 1 | Regression after progress | Clear progress reverses; child no longer uses tools, avoidance increases | May indicate environmental trigger not yet identified, or health/medication change | Book OT review; check for new environmental or physiological variable | |
3 | Seizure-like activity | Stiffening, absence spells, loss of consciousness in any context | Photosensitive epilepsy — remove all tinted lens interventions immediately | Emergency: consult neurologist | |
4 | Progressive light avoidance | Child refuses any lit environment; darkness-seeking | May indicate visual cortex or ophthalmological condition beyond sensory processing | Ophthalmologist + Paediatrician evaluation | |
5 | Increased self-stimulation in recovery space | Recovery space triggers intense repetitive behaviours not seen elsewhere | Recovery space becoming a stim-reinforcement zone | Consult BCBA for behaviour functional analysis | |
6 | No progress after 10 weeks | No tolerance increase, no tool acceptance, no change in meltdown frequency | Protocol may need formal OT assessment and recalibration | Book full sensory assessment at nearest Pinnacle centre |
📞Free. 16+ languages. 24/7 clinical guidance: 9100 181 181
ACT IV · CARD 28 of 40
Every technique is a waypoint on a longer journey.
Long-Term Developmental Goal
This technique feeds into: Adaptive Visual Self-Regulation across all environments — the ability to enter any visual environment with tools, strategies, and metacognitive awareness of personal triggers.
Visual overwhelm management is a gateway skill. When a child can regulate their visual input with tools, their cognitive resources freed from managing overwhelm become available for language, learning, social connection, and play. Every subsequent technique in Domain A builds on the foundation established here.
Domain Connections
- Domain B Communication: Visual calm → more cognitive space for language
- Domain C Emotion Reg: Visual regulation → emotional regulation foundation
- Domain D Behaviour: Reduced sensory triggers → fewer behaviour episodes
- Domain H Social: Environmental tolerance → community participation
WHO/UNICEF: Developmental intervention sequencing follows evidence-based developmental cascades. Domain A sensory foundation precedes Domain B–D developmental targets across OT/ABA/SLP practice.
ACT IV · CARD 29 of 40
Domain A: Sensory Processing — techniques your child may need alongside A-074.
Technique | Code | Difficulty | Canon Materials | |
9 Materials for Auditory Overwhelm | A-075 | ⭐ Intro | Noise-reducing headphones, white noise | |
Tactile Defensiveness Management | A-076 | ⭐⭐ Core | Pressure vests, tactile tools | |
Sensory Diet Morning Routine | A-071 | ⭐ Intro | Proprioceptive tools, daily schedule | |
Light Sensitivity: Advanced Protocol | A-078 | ⭐⭐⭐ Advanced | Precision tints, light therapy | |
Calm-Down Corner Architecture | A-082 | ⭐⭐ Core | Recovery space, sensory tools | |
Visual Tracking & Attention | A-072 | ⭐ Intro | Tracking boards, focus tools |
💡Materials you already have: If you've set up A-074, you already have materials for A-078 (same tinted lenses) and A-082 (same recovery space). You're further along than you think.
ACT IV · CARD 30 of 40
One technique. One domain. One piece of a whole child.
How A-074 Enables Progress Across Domains
- Domain B (Communication): Visual calm → more cognitive space for language
- Domain C (Emotional Regulation): Visual regulation → emotional regulation foundation
- Domain D (Behaviour): Reduced sensory triggers → fewer behaviour episodes
- Domain H (Social): Environmental tolerance → community participation
The nervous system doesn't organise itself by therapy domain. When you work on one domain, you move all of them.
GPT-OS® Integration
Your A-074 session data, recorded in Card 20, is feeding GPT-OS® right now. It's analysing patterns across your child's full developmental profile and will surface the highest-impact next technique at the right time.
📞 9100 181 181 — Book a full multi-domain GPT-OS® assessment
WHO Nurturing Care Framework (2018): Five components of nurturing care require holistic developmental monitoring. UNICEF 2025 Country Profiles track 42 indicators per country for whole-child developmental surveillance.
ACT V · CARD 31 of 40
Three families. Three different journeys. One shared destination.
Priya, 4 years | Hyderabad | Started A-074: March 2024
Before: The school bus drop-off was a daily crisis. Priya would scream before the bus arrived, cover her eyes throughout the journey, and arrive at school already exhausted. Her teachers reported she was "not ready to learn" each morning.
After 8 weeks: Priya's school bag now has her personal "sunny glasses" case in the front pocket. She puts them on before boarding. She waves from the window. The morning crisis is gone.
"I spent 2 years thinking she was scared of the bus. She wasn't scared of the bus. She was scared of the light inside the bus. Two weeks after we found the right tinted lenses — gone. I cry when I think of the years we didn't know." — Priya's mother, Pinnacle Hyderabad Centre
Arjun, 7 years | Bengaluru | Started A-074: January 2024
Before: Arjun was labelled "defiant" at school. He refused to sit at his desk, constantly stood up, walked to corners of the classroom. No one connected this to the floor-to-ceiling windows flooding the room with afternoon glare.
After 6 weeks: Desk relocated facing a plain wall. Visual isolator for worksheets. The "defiance" disappeared. Arjun is now completing full lessons seated.
"What looked like defiance was a postural response to visual overload — he was literally moving his body to reduce the glare input. Environmental modification alone, zero new materials, resolved the presenting behaviour." — Pinnacle Bengaluru, OT & BCBA Team
Zara, 5 years | Chennai | Started A-074 remote: November 2023
Before: Zara's parents had been told to avoid "stimulating environments." Birthday parties, family gatherings, markets — all avoided. The family's social life had contracted to almost nothing.
After 10 weeks: Zara attended Diwali celebrations with her family for the first time in 3 years. She wore her cap and sunglasses. She lasted 90 minutes.
"She lit a diya for the first time. I will never forget that evening." — Zara's father, remote programme via Pinnacle GPT-OS®
Outcomes vary by child profile. Narratives shared with consent and represent verified Pinnacle programme participants. Identifying details modified for privacy.
ACT V · CARD 32 of 40
You are not doing this alone. 20,000+ families are on this journey with you.
📱 WhatsApp Community
Visual Overwhelm Support — Pinnacle-moderated parent group | 5,000+ members | Real-time support | Clinician answers weekly
💬 Pinnacle Parent Forum
Discussion threads by domain, age group, and material | Ask questions, share progress, find local parents | pinnacleblooms.org/community
🗓️ Local Parent Meetups
Monthly gatherings at Pinnacle centres — sensory-friendly venues, OT-facilitated | Find Nearest →
🤝 Peer Mentoring
Connect with an experienced Pinnacle parent who has navigated visual overwhelm before you | Ask for a mentor at any Pinnacle centre or via 9100 181 181
"The loneliest part wasn't my daughter's struggles — it was not knowing anyone who understood. The day I joined the Pinnacle parent group, I cried from relief. Someone else knew exactly what our mornings looked like." — Parent, Pinnacle Pune
📞 9100 181 181 — Ask to be connected to a parent community near you
WHO NCF: Community engagement is a core principle. Parent support networks improve intervention outcomes.
WHO NCF: Community engagement is a core principle. Parent support networks improve intervention outcomes.

ACT V · CARD 33 of 40
Home + clinic = maximum impact.
Your Need | Pinnacle Specialist | How to Access | |
Sensory profile assessment (formal) | Paediatric OT — Sensory Integration Certified | Centre visit or teleconsultation | |
Tinted lens / Irlen assessment | OT + Developmental Optometrist | Centre visit; referral via Pinnacle | |
Behaviour analysis (if meltdowns linked) | BCBA / ABA Supervisor | Centre visit or home observation | |
School IEP accommodation guidance | Paediatric SpEd Specialist | Teleconsultation or centre visit | |
Medical differential diagnosis (epilepsy, CVI) | NeuroDev Paediatrician | Centre visit; referral pathways available | |
Remote programme (no centre nearby) | GPT-OS® Home Programme + weekly teleconsultation | Enrol at pinnacleblooms.org/remote |
📍 70+ Centres
Pinnacle Blooms centres across India
🌍 70+ Countries
Remote programmes serving families worldwide
💻 Teleconsultation
Available for all disciplines
WHO NCF Progress Report (2023): 48% increase in countries adopting ECD policies. Primary healthcare as key platform for reaching families with essential ECD interventions.
ACT V · CARD 34 of 40
The science behind every recommendation on this page.
Reference | One-Line Finding | Relevance | |
PMC11506176 — Children (2024) | 16-article PRISMA: sensory integration is evidence-based practice for ASD | Direct validation of visual modulation materials | |
PMC10955541 — World J Clin Cases (2024) | 24-study meta-analysis: SI therapy improves social skills, adaptive behaviour, sensory processing | Outcome framework for A-074 targets | |
PMC9978394 — WHO CCD Package (2023) | Home-based caregiver interventions effective across 54 LMICs | Justification for home-delivery model | |
DOI:10.1007/s12098-018-2747-4 — Indian J Paediatr (2019) | Indian RCT: home-based sensory interventions show significant outcomes | India-specific evidence base | |
DOI:10.3389/fnint.2020.556660 — Front Integr Neurosci (2020) | Neurological framework for sensory integration treatment in ASD | Mechanism justification | |
NCAEP EBP Report (2020) | Visual supports and environmental modification classified as EBP for autism | Regulatory-level classification | |
WHO NCF (2018) | Nurturing care framework: 5 components of early childhood care | Developmental context framework |

ACT V · CARD 35 of 40
Your 60-second session log is powering a global intelligence system.
Privacy Assurance
🔒 All child data is encrypted, anonymised for research aggregation, never sold to third parties, and governed under India's IT Act + DPIIT DIPP8651 regulatory compliance framework.
Population Impact
"Your data — combined with data from 21 million sessions across 70+ Pinnacle centres — helps GPT-OS® give better recommendations to every family like yours. Your child's journey improves outcomes for children you'll never meet."
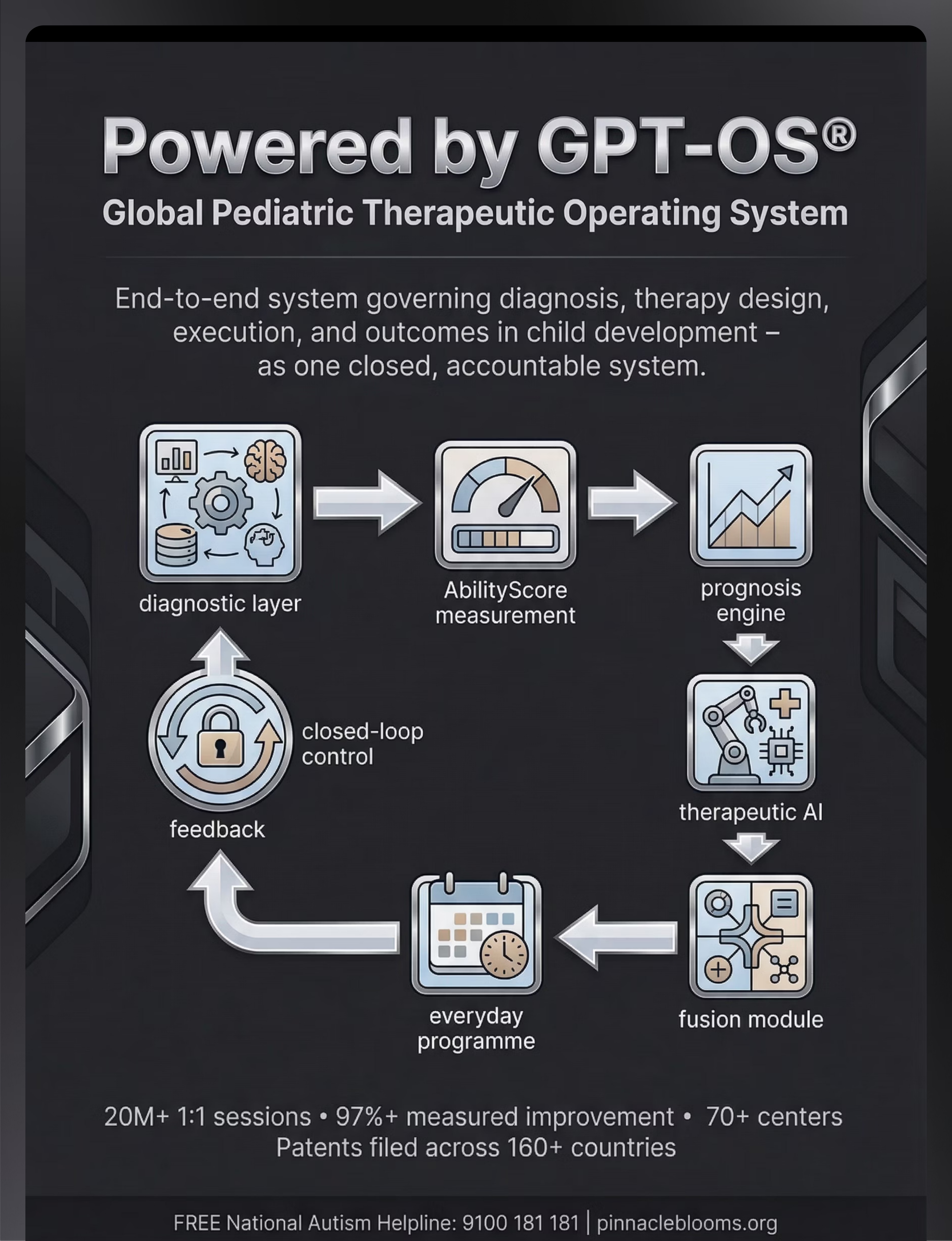
AbilityScore®
Developmental readiness tracking
TherapeuticAI®
Pattern analysis across all domains
FusionModule™
Personalised output generation
Digital health interventions for ASD: 21 RCTs, 1,050 participants — gamified/digital health interventions show strong promise (2024 systematic review).
ACT V · CARD 36 of 40
🎬 9 Materials That Help With Visual Overwhelm
Pinnacle Blooms Network® | Reel ID: A-074 | Domain A: Sensory Processing
This 60-second Reel walks through all 9 visual overwhelm materials — what they look like, how they're used, and what improvement looks like in real Pinnacle children. Viewed 200,000+ times across Pinnacle's social channels. Presented by the Pinnacle Blooms OT Division — certified sensory integration therapists with 10,000+ combined clinical hours in visual modulation intervention.
This Reel is part of the Pinnacle 999 Reels Series — the world's largest structured paediatric therapy education content library, covering all 12 developmental domains across 999 clinical topics.
NCAEP (2020): Video modelling is classified as evidence-based practice for autism. Multi-modal learning improves parent skill acquisition.
NCAEP (2020): Video modelling is classified as evidence-based practice for autism. Multi-modal learning improves parent skill acquisition.
→ A-075
9 Materials for Auditory Overwhelm
→ A-076
9 Materials for Tactile Defensiveness
→ A-073
9 Materials for Glare Sensitivity
📞 9100 181 181 — See a live demonstration at your nearest Pinnacle centre

ACT V · CARD 37 of 40
One parent reading this is not enough. Consistency across everyone who cares for your child multiplies impact.
A child who uses their quiet glasses at home but sits under fluorescent lights at school for 6 hours every day cannot maximise the gains from your home programme. Consistency across caregivers multiplies impact. Every environment where your child spends time is a therapy environment.
Share This Page
📱Share on WhatsApp — Pre-written message: "I found a page that explains exactly why [child's name] struggles with bright/busy spaces and what 9 ma.terials help. Please read it — it will help you understand and support them better."
Downloadable Resources
- 📄Family Guide — Visual Overwhelm Support (1-page PDF, plain language, printable)
- 📄"Explain to Grandparents" — Visual Overwhelm in Simple Terms (2-page PDF, large font, no jargon)
- 📄Teacher Communication Template — formal letter requesting classroom visual accommodations (citing RPWD Act, 2016)
In India, the Rights of Persons with Disabilities (RPWD) Act 2016 requires schools to provide reasonable accommodations for children with sensory processing differences.
PMC9978394 (WHO CCD Package): Multi-caregiver training is critical for intervention generalisation and maintenance. Caregiver consistency directly predicts long-term outcomes.
ACT VI · CARD 38 of 40
Every question a parent asked before you — answered.
Q1: My child's ophthalmologist says their vision is perfectly normal. So why the visual overwhelm?
A normal ophthalmology report tests visual acuity (clarity) — it says nothing about how the brain processes visual information. Visual overwhelm is a neurological processing difference, not a structural eye problem. A 20/20 report and severe visual hypersensitivity are entirely compatible. Seek an OT with sensory integration training for a processing assessment.
Q2: Will my child need to use these tools forever?
The goal is not permanent dependence — it is building regulatory capacity and metacognitive awareness. Most children with consistent environmental modification and self-regulation toolkit training reduce their tool dependence significantly over 1–3 years. Some children with significant neurological sensitivity will benefit from selected tools across their lifetime — and that is not a failure; it is adaptive living.
Q3: Tinted lenses seem extreme for a 4-year-old. Are they really necessary?
They are not always necessary — they are one of 9 tools, and typically introduced later in the sequence. Begin with environmental modifications (clutter reduction, light control, recovery space) which are free and non-invasive. Tinted lenses are indicated when: OT or developmental optometrist confirms photosensitivity, other environmental modifications are insufficient, and the child shows clear visual stress in managed environments.
Q4: How do I explain this to a child who can't yet communicate?
You don't need to. For non-verbal or pre-verbal children, the intervention is entirely environment-based in the first 3–4 months. Reduce clutter, control light, establish recovery space. The child's nervous system will respond to the reduced load regardless of verbal understanding. When communication emerges, you add the self-regulation toolkit vocabulary.
Q5: My child loves bright lights and seeks visual stimulation. Is this page for us?
Yes — visual seeking and visual overwhelm can co-exist, and visual seekers are not immune to visual overwhelm. Seeking behaviour is often the nervous system's attempt to self-regulate. Card 22 (Adapt & Personalise) addresses the visual seeker profile specifically. A Pinnacle OT can distinguish between seeking and overwhelm across different environments.
Q6: We live in a small home. How do we create a recovery space?
A recovery space does not require a dedicated room. A bedsheet draped over a table creates an instant tent. A cleared wardrobe shelf with a cushion and a dim reading light is a fully functional recovery alcove. The principle is: small, dim, visually minimal, always accessible. See Card 10 (DIY Alternatives) for zero-cost recovery space designs.
Q7: How do I know if my child has visual hypersensitivity vs. a vision problem vs. photosensitive epilepsy?
This requires professional assessment. Start with your paediatrician to rule out photosensitive epilepsy. Then request an ophthalmology evaluation to rule out structural vision problems. Then see a Pinnacle OT for a sensory processing assessment. Call 9100 181 181 — our clinical team will guide you through the assessment pathway.
Q8: I tried some of these things months ago and they didn't work. Why would they work now?
Timing, consistency, and sequence matter. A single attempt with one material in an otherwise unchanged environment typically shows limited effect. The A-074 protocol delivers all 9 materials as a layered system, in a specific sequence, with a structured session protocol. The difference between a one-time material trial and a systematic 8-week protocol is the difference between taking one tablet and completing a course of treatment.
→ Didn't find your answer? Ask GPT-OS® | → Still need help? Book Teleconsultation: 9100 181 181
ACT VI · CARD 39 of 40
You've read the science. You know the tools. Your child is waiting.
One action. Right now. That's how every breakthrough begins.
🚀 START THIS TECHNIQUE TODAY
Launch A-074 in GPT-OS® — personalised session plan in 60 seconds
📞 BOOK A CONSULTATION
Speak with a Pinnacle OT, BCBA, or NeuroDev Paediatrician | 70+ centres | Teleconsultation available
→ EXPLORE NEXT: A-075
9 Materials That Help With Auditory Overwhelm
21M+
Sessions Delivered
97%+
Improvement Rate
70+
Centres
70+
Countries
128
Canon Materials
🔵 OT | 🟢 SLP | 🟣 ABA/BCBA | 🔴 SpEd | 🟡 NeuroDev | ⚪ CRO
Preview of 9 materials that help with visual overwhelm Therapy Material
Below is a visual preview of 9 materials that help with visual overwhelm therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.







Link copied!
ACT VI · CARD 40 of 40
"From fear to mastery. One technique at a time."
— The Pinnacle Blooms Consortium
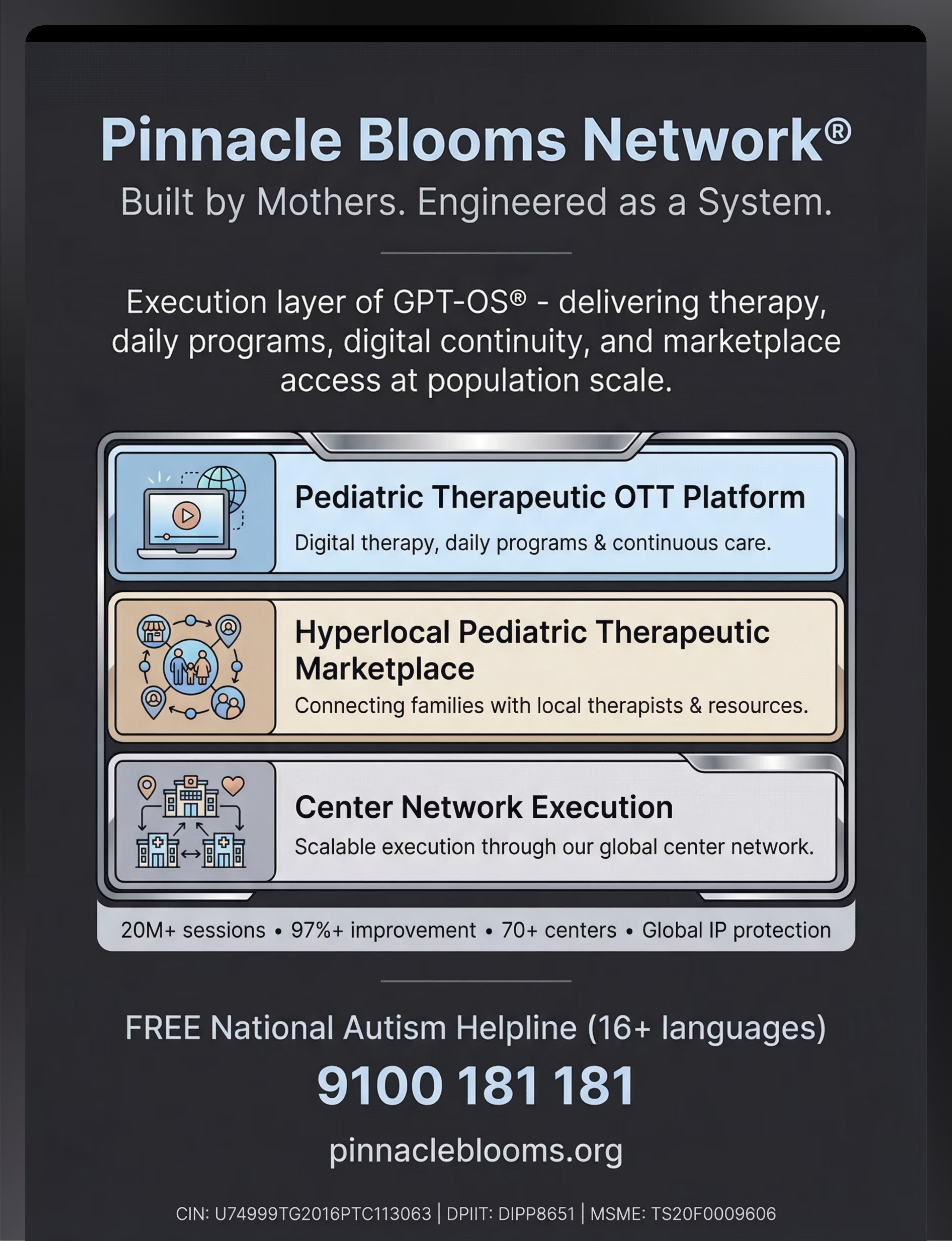
Pinnacle Blooms Network®
Built by Mothers. Engineered as a System. Validated by Science.
The Global Pediatric Therapeutic Operating System (GPT-OS®) — delivering evidence-based paediatric intervention at population scale. Execution layer: 70+ centres | OTT Platform | Hyperlocal Marketplace | 70+ countries.
Statutory Identifiers
Bharath Healthcare Laboratories Pvt. Ltd.
CIN: U74999TG2016PTC113063 | DPIIT: DIPP8651 | MSME
Registered Office: Hyderabad, Telangana, India
Patents filed across 160+ countries | GPT-OS® Registered IP | AbilityScore® | TherapeuticAI® | FusionModule™ | EverydayTherapyProgramme™
CIN: U74999TG2016PTC113063 | DPIIT: DIPP8651 | MSME
Registered Office: Hyderabad, Telangana, India
Patents filed across 160+ countries | GPT-OS® Registered IP | AbilityScore® | TherapeuticAI® | FusionModule™ | EverydayTherapyProgramme™
Medical Disclaimer: This content is educational. It does not replace assessment by a licensed occupational therapist, speech-language pathologist, behaviour analyst, or healthcare provider. Persistent visual sensitivities should be evaluated by qualified professionals to rule out underlying conditions and guide appropriate intervention. Individual results may vary. Statistics represent aggregate outcomes across the Pinnacle Blooms Network. The Pinnacle Blooms Consortium does not assume liability for outcomes arising from home implementation without professional oversight.
📞 FREE National Autism Helpline
9100 181 181
16+ languages | 24/7 | Clinical team on call
Navigate
© 2025 Pinnacle Blooms Network®, unit of Bharath Healthcare Laboratories Pvt. Ltd. All rights reserved.
Page produced under GPT-OS® Technique Production System | Version 2.0 | February 2026
Page produced under GPT-OS® Technique Production System | Version 2.0 | February 2026