
She Doesn't Avoid Loud Sounds. She Chases Them.
It's 7:15 AM. Your daughter is already banging a wooden spoon on every pot she can reach. The TV is at maximum volume — again. She stands pressed against the washing machine during the spin cycle, eyes closed, smiling. At her cousin's birthday, while every other child covered their ears during the balloon popping, she was the one doing the popping — right next to her own ear.
You've tried "inside voice." You've tried consequences. You've tried whispering to model quiet behavior. Nothing works for more than thirty seconds before she finds another way to create noise. This is not defiance. This is not a discipline failure. Your child's auditory system is speaking — and it is saying: "I need more."
You are not failing. Your child's nervous system is hungry for sound. And there is a precise, evidence-based way to feed it.
Pinnacle Blooms Consortium
OT • SLP • ABA • SpEd • NeuroDev
Built by Mothers. Engineered as a System.

You Are Among Millions. This Is More Common Than You Think.
Sound-seeking behavior is one of the most disruptive — and most misunderstood — presentations families encounter. You are far from alone. The research is clear, the numbers are staggering, and the solutions are real.
80%
Children with ASD
of children diagnosed with autism spectrum disorder exhibit sensory processing differences — and auditory seeking is among the most disruptive presentations families report.
Source: PRISMA Systematic Review, Children, 2024 | PMC11506176
1 in 6
All Children
children demonstrate sensory processing difficulties significant enough to affect daily functioning — including sound-seeking behaviors that impact family life, school participation, and social relationships.
Source: Ahn et al., American Journal of Occupational Therapy
21M+
Therapy Sessions
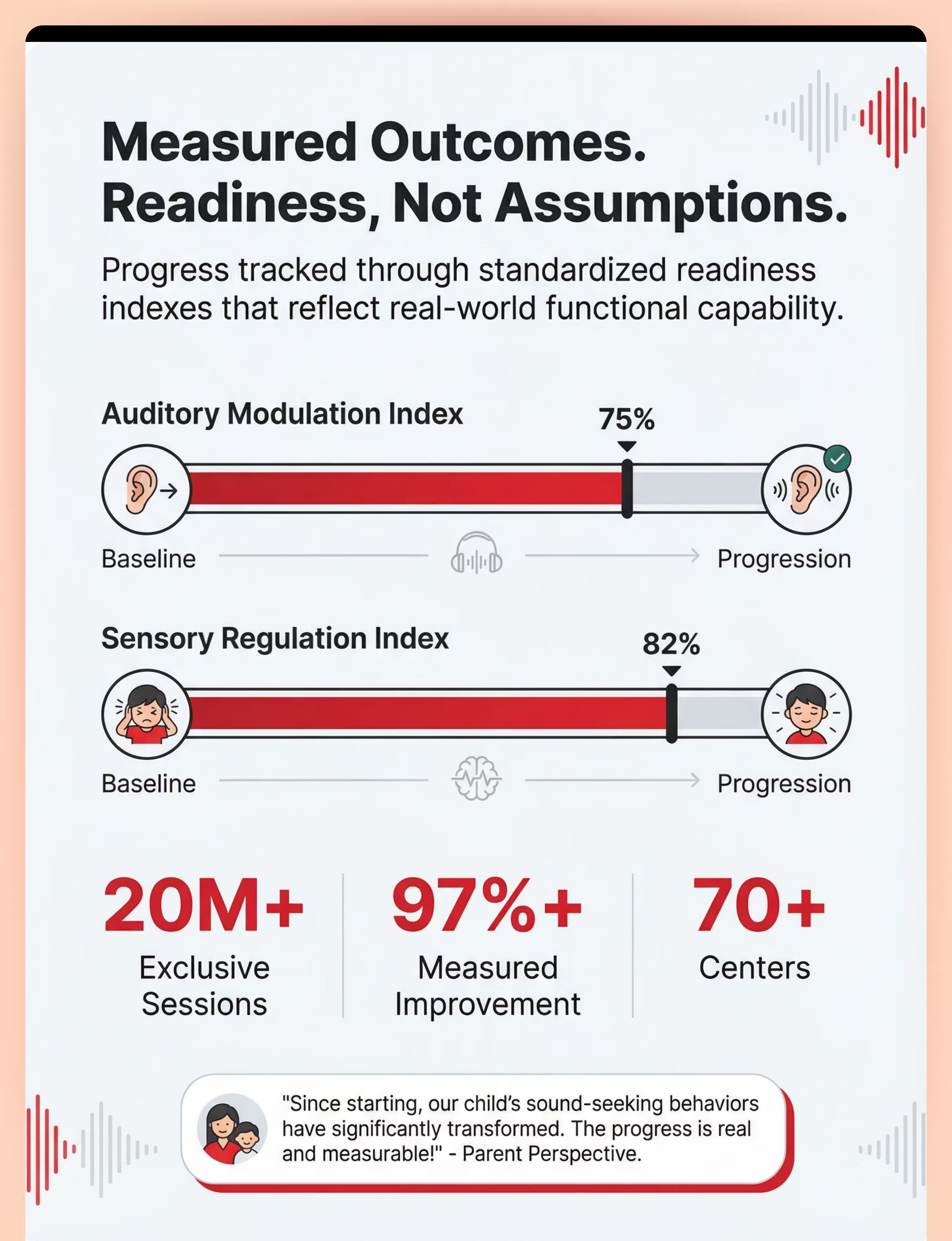
therapy sessions delivered by Pinnacle Blooms Network® across 70+ centers — with 97%+ measured improvement across sensory processing readiness indexes. This is not theory. This is measured, replicated, population-scale evidence.
"You are among millions of families navigating this exact challenge. The sound-seeking is real. The exhaustion is real. And the solution is real." — Pinnacle Blooms Consortium
Why Your Child's Ears Are "Hungry" for Sound
The Neuroscience
Your child's auditory system has a higher neurological threshold for sound input. Where a typical child's auditory cortex registers and processes sound at normal environmental volumes, your child's system requires significantly more intensity to achieve the same registration.
This is called auditory hypo-responsivity — and it's as real and measurable as needing glasses for vision.
In Your Words
Think of it like a fuel gauge. Most children's auditory systems fill up at "normal volume." Your child's gauge sits lower. Normal conversation, typical TV volume, everyday environmental sounds — they don't register enough to satisfy the nervous system's need for auditory input.
So your child seeks louder. Bangs harder. Screams more. Turns the volume higher. Not because they want to annoy you — but because their nervous system is genuinely trying to fill a tank that empties faster and requires more.
This is a wiring difference, not a behavior choice.
Dunn's Model of Sensory Processing | Frontiers in Integrative Neuroscience, 2020 | DOI: 10.3389/fnint.2020.556660

Your Child's Sound-Seeking on the Developmental Map
Sound-seeking behaviors appear at different intensities across childhood. Understanding where your child sits on the developmental timeline helps set realistic expectations and guides intervention timing.
0–12 Months
Emerging auditory awareness. Infants turn toward sounds. Early signs of preference for louder stimuli may appear.
1–3 Years
Auditory processing pathways actively developing. Sound-seeking becomes noticeable — banging objects, seeking appliances, loud vocalizations. Parents often say "my child is just loud."
3–6 Years ◄ Typical Window
Sound-seeking becomes functionally disruptive. The child actively pursues intense auditory input across all environments. This is when most families seek assessment.
6–12 Years
Without intervention, patterns become entrenched. With channeling, children develop self-regulation strategies. The threshold difference persists — the child learns to manage it, not outgrow it.
What Commonly Co-Occurs: Proprioceptive seeking (craving heavy impact, crashing), vestibular seeking (spinning, swinging), tactile seeking (touching everything), attention difficulties, and auditory processing challenges affecting language comprehension in noisy environments.
WHO Care for Child Development Package | UNICEF MICS Indicators | PMC9978394
WHO Care for Child Development Package | UNICEF MICS Indicators | PMC9978394

Clinically Validated. Home-Applicable. Parent-Proven.
Evidence Grade: Level I–II (Strong)
Sensory integration intervention, including structured auditory input channeling, meets criteria for evidence-based practice based on multiple systematic reviews and meta-analyses. This is not experimental territory — it is one of the most thoroughly studied intervention domains in pediatric therapy.
PRISMA Systematic Review (2024)
16 studies (2013–2023) confirm sensory integration intervention as evidence-based practice for children with autism and sensory processing differences. PMC11506176 | Children, 2024
Meta-Analysis — 24 Studies (2024)
Demonstrates sensory integration therapy effectively promotes social skills, adaptive behavior, sensory processing capacity, and gross/fine motor skills. World Journal of Clinical Cases | PMC10955541
Indian RCT — Padmanabha et al. (2019)
Home-based sensory interventions delivered by trained parents demonstrated significant positive outcomes in an Indian pediatric population — validating the home-executable model Pinnacle Blooms deploys. Indian Journal of Pediatrics | DOI: 10.1007/s12098-018-2747-4
Pinnacle Blooms Real-World Evidence
21 million+ exclusive therapy sessions with 97%+ measured improvement across sensory processing readiness indexes. Population-scale validation across 70+ centers.

Auditory Sensory Input Channeling Protocol
Parent-Friendly Name: "Sound Diet — Feeding the Hungry Ears"
A structured sensory intervention protocol that provides children with auditory hypo-responsivity safe, appropriate, and satisfying channels for intense auditory input. Rather than suppressing the seeking behavior — which doesn't work because the underlying neurological need persists — this protocol gives the child what they need through controlled materials, scheduled access, and multi-sensory integration.
The intervention channels chaotic, disruptive sound-seeking into structured, skill-building, family-compatible activities that satisfy the same auditory craving.
Domain
Sensory Processing — Auditory Modulation
Code: SEN-AUD-SEEK
Code: SEN-AUD-SEEK
Age Range
3–12 years
Adaptable for younger children with modifications
Adaptable for younger children with modifications
Duration
15–30 min per structured session + integrated throughout daily routine
Frequency
Daily — multiple short sessions plus sensory diet integration
Setting
Home + School + Community
Flexible, environment-adaptive
Flexible, environment-adaptive
Pinnacle 128 Canon Materials System | 20 Category Classification | Domain A: Sensory Processing

The Consortium Behind This Protocol
This protocol crosses therapy boundaries because the brain doesn't organize by therapy type. Four disciplines collaborate to address every dimension of auditory seeking — from neurological threshold to behavioral function to language development.
Occupational Therapist (OT) — Primary Lead
Designs the sensory diet. Evaluates auditory processing thresholds using standardized assessment. Determines appropriate intensity levels, selects materials, creates the structured auditory input schedule, and monitors for hearing safety.
BCBA / ABA Therapist
Analyzes the function of sound-seeking through functional behavior assessment. Develops reinforcement schedules for appropriate sound use. Creates antecedent strategies that reduce motivation for chaotic seeking. Trains parents in behavioral data collection.
Speech-Language Pathologist (SLP)
Evaluates whether auditory seeking co-occurs with auditory processing disorder or language comprehension challenges. Musical and vocal activities (karaoke, singing) serve dual sensory and speech goals.
NeuroDevelopmental Pediatrician
Rules out medical causes: hearing loss, auditory neuropathy, or otological conditions. Orders audiological evaluation when indicated. Coordinates across therapy disciplines through GPT-OS® integrated care pathway.
Adapted UNICEF/WHO Nurturing Care Framework for SLPs (2022) | DOI: 10.1080/17549507.2022.2141327

Precision Targets: What This Intervention Addresses
This protocol operates on three concentric levels — from the immediate auditory regulation challenge to long-term developmental gains that ripple across every domain of your child's life.
Tertiary Targets — Long-Term Developmental Gains
Skill development through musical instrument learning. Improved social participation. Enhanced auditory processing through structured exposure. Proprioceptive regulation. Self-advocacy skills for sensory needs.
Secondary Targets — Self-Regulation & Daily Functioning
Reduced disruptive noise-making in home and school environments. Increased participation in quiet activities. Improved family functioning. Emerging self-monitoring: child begins to recognize and communicate their auditory needs verbally.
Primary Target — Auditory Modulation
The child develops the ability to regulate auditory input seeking through appropriate channels. Observable: uses headphones instead of maximum TV volume, requests "loud time" instead of random banging, tolerates quiet activities for age-appropriate durations.
Observable Behavior Indicators: ✓ Spontaneously reaches for headphones ✓ Checks visual schedule for "loud time" without prompting ✓ Participates in 10+ minutes of quiet activity after sessions ✓ Reduces random noise-making by 50%+ within 4–6 weeks ✓ Verbalizes "I need my drums" or equivalent request
Meta-analysis: World Journal of Clinical Cases, 2024 | PMC10955541
Meta-analysis: World Journal of Clinical Cases, 2024 | PMC10955541

The 9 Materials That Satisfy Sound-Seeking
Each material below targets the same neurological need — intense auditory input — through a different channel. Use one or combine several, depending on your child's preferences and your family's setup.
Headphones with High-Quality Audio
Category: Sensory Regulation Tools
Price: ₹1,000–10,000 | Over-ear, bass-response, volume-limiting
Why it works: Delivers intense, controlled auditory input directly to the ear canal — satisfying the seeking behavior without environmental disruption.
Price: ₹1,000–10,000 | Over-ear, bass-response, volume-limiting
Why it works: Delivers intense, controlled auditory input directly to the ear canal — satisfying the seeking behavior without environmental disruption.
Drums & Percussion Instruments
Category: Musical & Sound Materials
Price: ₹500–15,000 | Hand drums, djembe, bongos, electronic drum kit
Why it works: Combines loud auditory feedback with proprioceptive impact — doubly satisfying for most sound-seekers.
Price: ₹500–15,000 | Hand drums, djembe, bongos, electronic drum kit
Why it works: Combines loud auditory feedback with proprioceptive impact — doubly satisfying for most sound-seekers.
Musical Instruments (Keyboard, Guitar, Xylophone)
Category: Musical & Sound Materials
Price: ₹1,000–50,000+ | Instruments with loud, immediate feedback
Why it works: Channels seeking into skill-building while providing immediate, intense auditory reward.
Price: ₹1,000–50,000+ | Instruments with loud, immediate feedback
Why it works: Channels seeking into skill-building while providing immediate, intense auditory reward.
Sound-Making Toys & Noise Makers
Category: Cause-Effect & Sensory Toys
Price: ₹200–3,000 | Sound boards, whistles, rattles, musical buttons
Why it works: Accessible, portable outlets that the child can control independently.
Price: ₹200–3,000 | Sound boards, whistles, rattles, musical buttons
Why it works: Accessible, portable outlets that the child can control independently.
Vibration Speakers / Bass-Heavy Devices
Category: Sensory Regulation Tools
Price: ₹1,500–8,000 | Bass speakers, vibration cushions, bone conduction
Why it works: Adds tactile vibration to auditory input — a multi-sensory combination that can rapidly satisfy high-threshold seekers.
Price: ₹1,500–8,000 | Bass speakers, vibration cushions, bone conduction
Why it works: Adds tactile vibration to auditory input — a multi-sensory combination that can rapidly satisfy high-threshold seekers.
Loud Environment Outings (Structured)
Category: Environmental & Activity-Based
Price: ₹0–5,000+ | Arcades, concerts, airports, sports events
Why it works: Provides immersive, community-normalized auditory input that also builds social participation.
Price: ₹0–5,000+ | Arcades, concerts, airports, sports events
Why it works: Provides immersive, community-normalized auditory input that also builds social participation.
Karaoke Machine / Microphone System
Category: Musical & Sound Materials
Price: ₹1,000–10,000 | Karaoke machine, Bluetooth mic, echo mic
Why it works: Vocal sound-seekers get immediate amplified auditory feedback from their own voice — deeply satisfying and skill-building.
Price: ₹1,000–10,000 | Karaoke machine, Bluetooth mic, echo mic
Why it works: Vocal sound-seekers get immediate amplified auditory feedback from their own voice — deeply satisfying and skill-building.
Heavy Work + Sound Activities
Category: Proprioceptive & Multi-Sensory
Price: ₹0–2,000 | Hammer & nails, mortar & pestle, stomping activities
Why it works: The combination of proprioceptive effort and auditory feedback is maximally satisfying — hits two sensory systems at once.
Price: ₹0–2,000 | Hammer & nails, mortar & pestle, stomping activities
Why it works: The combination of proprioceptive effort and auditory feedback is maximally satisfying — hits two sensory systems at once.
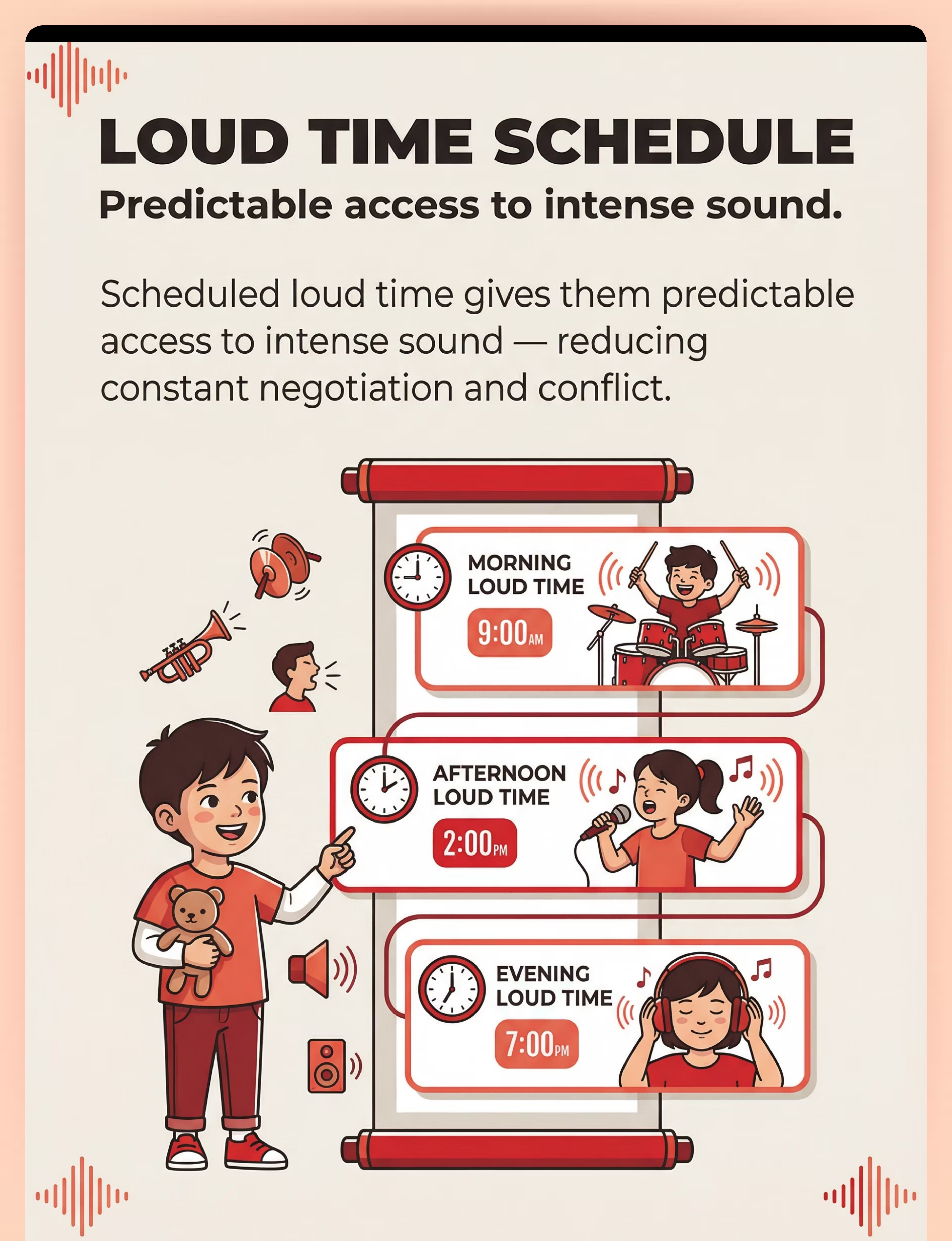
Sound Schedule & Designated "Loud Time"
Category: Visual Supports & Scheduling
Price: ₹0 | Visual schedule, timer, designated space — completely free
Why it works: Gives the child predictability and reduces anxiety about when loud input will be available — reducing random seeking between sessions.
Price: ₹0 | Visual schedule, timer, designated space — completely free
Why it works: Gives the child predictability and reduces anxiety about when loud input will be available — reducing random seeking between sessions.
Total Investment Range: ₹0 (all-DIY) to ₹50,000+ (full professional setup) | Essential Starter Kit: Quality headphones + basic drums = ₹1,500–25,000

Every Family Can Start Today — Regardless of Budget
The neurological principle behind every material is identical — intense auditory input through safe, channeled activities. Whether the drum costs ₹15,000 or is an upturned bucket, the proprioceptive impact and auditory feedback satisfy the same neural pathway.
Buy This
- Quality headphones (₹1,000+)
- Drum kit (₹500+)
- Musical instrument (₹1,000+)
- Sound-making toys (₹200+)
- Vibration speaker (₹1,500+)
- Karaoke machine (₹1,000+)
- Heavy work tools (₹0+)
- Sound schedule card set (₹100+)
Make This (₹0)
- Any available headphones + free music apps (YouTube Kids, Spotify Free)
- Upturned steel buckets + wooden spoons = instant drums
- Pots, pans, lids as cymbals; plastic bottles with rice as shakers
- Homemade rattles (dried beans in sealed container); bells tied to string
- Place child's hands on any speaker during music; phone on vibrate mode
- Sing loudly together; use a paper towel roll as "microphone"
- Stomping on bubble wrap; clapping games; pounding dough
- Draw times on paper when "loud play" is allowed; use a kitchen timer
When Clinical-Grade Materials Are Non-Negotiable: Volume-limiting headphones for sustained use require engineered limits, not guesswork. If your child uses headphones for more than 30 minutes daily, invest in volume-limiting hardware — this is a hearing-safety non-negotiable.
WHO Nurturing Care Framework (2018): Equity-focused, context-specific interventions | PMC9978394
WHO Nurturing Care Framework (2018): Equity-focused, context-specific interventions | PMC9978394

Safety Gate: Read This Before You Start
Safety awareness prevents harm and protects the therapeutic relationship. Review all three levels before your first session and revisit whenever you introduce new materials.
🔴 RED — Do NOT Proceed If:
- Child has a diagnosed hearing impairment not recently evaluated by an audiologist in relation to their sound-seeking
- Child shows signs of ear pain, ear infection, or discharge — seek medical attention first
- Child has a seizure disorder triggered by specific sound frequencies — consult neurologist before introducing new auditory stimuli
- Any question about hearing ability exists and audiologist has not been consulted
🟡 AMBER — Modify and Proceed With Caution:
- Use volume-limiting headphones — even sound-seekers can damage hearing with sustained maximum volume
- Monitor decibel levels: brief loud sounds (drum hits) are less damaging than sustained loud exposure
- Supervise all tool-based activities (hammering, heavy work) — safety goggles and adult presence required
- Assess choking hazards in sound-making toys for children under 4
- If child becomes severely distressed during structured loud time, stop immediately
🟢 GREEN — Proceed When:
- Child is fed, rested, and in a generally regulated state
- Environment is safe — nothing breakable within reach
- Volume-limiting measures are in place
- Adult supervision is present for active materials
- Other family members are prepared or child is using headphones
🔴 ABSOLUTE RED LINE — STOP IMMEDIATELY IF YOU SEE: Child holding ears in pain (physical discomfort, different from overstimulation) | Sudden loss of responsiveness to sound at any volume | Child becoming aggressive toward others or self during sound activities | Any signs the activity has shifted from regulating to dysregulating.
Home-based sensory intervention safety protocols: Padmanabha et al., Indian J Pediatr, 2019 | DOI: 10.1007/s12098-018-2747-4
Home-based sensory intervention safety protocols: Padmanabha et al., Indian J Pediatr, 2019 | DOI: 10.1007/s12098-018-2747-4
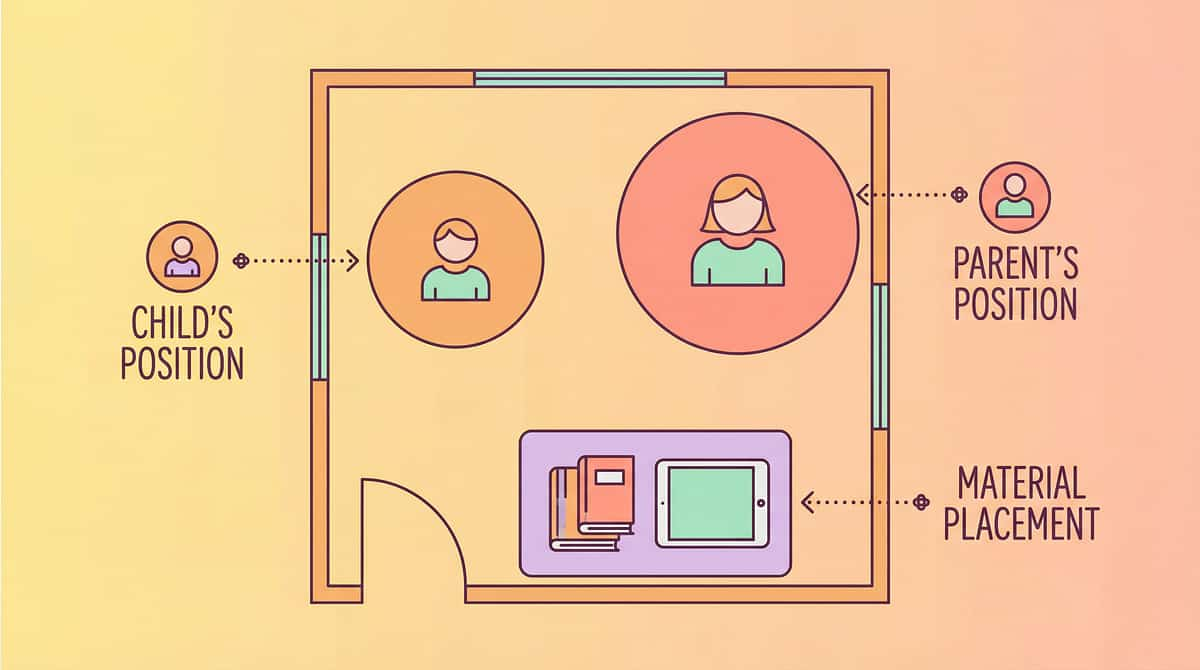
Prepare the Sound Station
Environmental setup prevents the majority of session failures. Dedicate 10 minutes before your first session to prepare the space — it changes everything about how the protocol lands.
Build the Space
- Sound Station: Drums/instruments/sound toys within child's reach. Floor mat underneath for comfort and vibration absorption. Visual schedule on wall showing "loud time" blocks.
- Parent Station: Within arm's reach of child, facing them (not behind). Timer visible to both. Reinforcement items ready.
- Headphone Zone: Bean bag or floor cushion. Device with pre-loaded audio. Volume limiter set and verified before session begins.
Clear the Space
- ✗ Fragile/breakable items within reach
- ✗ Hard objects the child might grab to bang instead of designated materials
- ✗ Younger siblings who might be startled or hurt
- ✗ Pets sensitive to loud sounds
Environmental Settings
- 💡 Natural or warm lighting — not fluorescent
- 🌡️ Comfortable temperature — active sound-making generates body heat
- 🔊 Minimize competing background sounds
- 📱 Screens off (unless providing headphone audio)
Sensory Integration Theory (Ayres): Environmental setup prevents 80% of session failures | PMC10955541
60-Second Pre-Session Check
The best session is one that starts right. This 60-second check prevents 90% of session failures before they happen. Run through it every time — it takes less than a minute and saves the whole session.
Fed?
Child has eaten within the last 2 hours. Hunger increases dysregulation and reduces the child's capacity to benefit from sensory input.
Rested?
Child is not overtired or just waking from sleep. A fatigued nervous system cannot regulate during sensory input — it escalates instead.
Regulated Baseline?
No active meltdown or crying episode in the last 15 minutes. The session builds on a stable foundation — it doesn't rescue from crisis.
No Illness Signs?
No ear pain, fever, or signs of infection. Physical discomfort makes all sensory input unpredictable.
Materials Ready?
Sound station set up, headphones charged, instruments in place, timer set and visible to both parent and child.
Family Prepared?
Other household members know loud time is starting. No surprises — for anyone.
✅ All Green → GO
Begin the protocol. Proceed to Step 1: The Invitation.
🟡 Some Amber → Modify
Use headphone-only session. Shortened 5-minute version. Skip drums and active instruments.
🔴 Any Red → Postpone
Offer calming alternative. Try again in 1–2 hours. Postponement is not failure — it's precision.

Step 1 — Invite, Don't Command
⏱️ 30–60 seconds
Protocol Step 1 of 6
"It's LOUD TIME! Do you want to play your drums first, or do you want headphones with your music?"
Body Language That Works
- Energetic voice — match the child's intensity level, not a library voice
- Point to the visual schedule showing "loud time"
- Hold up 2–3 material options — let the child choose
- Smile — this is supposed to be enjoyable for both of you
What Acceptance Looks Like
- Child approaches materials with excitement
- Child points to or grabs preferred item
- Child vocalizes excitement (loud vocalization is expected and acceptable)
- Child leads you to the sound station
If There's Resistance
- Child ignores invitation: Place the most preferred material within reach and start playing it yourself — auditory seekers are drawn to the sound
- Child is mid-meltdown: Postpone — not the right moment
- Child wants a different sound activity: Allow it if safe — the goal is channeled sound, not rigid compliance

Step 2 — Introduce the Material
⏱️ 1–3 minutes
Protocol Step 2 of 6
Present the chosen material with energy. For instruments, demonstrate one loud hit or strum so the child hears the full potential. For headphones, start at moderate volume and let the child adjust within the volume-limited range. The goal is to activate the child's curiosity and desire to engage.
Headphones Introduction
Place on ears gently. Start audio. Watch the child's face — you'll see the moment the sound registers as satisfying. Ask "More?" or "Louder?" with thumbs up to give the child control.
Drum Introduction
Strike the drum once — hard. Hand the sticks to the child. If they strike softly, model a harder hit. The point is intensity. Don't correct grip or technique.
Karaoke Introduction
Sing one note into the mic loudly. Hand it to the child. Their eyes will light up. The amplified feedback from their own voice is one of the most immediately satisfying sounds for vocal seekers.
Sound Toys Introduction
Press a few buttons to demonstrate the sounds available. Then hand it over entirely — let the child discover and control what they want to hear.
Child Response Indicators:Engaged ✓ — Actively using material, appears focused and satisfied, body organizing (less fidgety, more purposeful). Tolerating ~ — Using the material but underwhelmed. Try a louder option. Avoiding ✗ — Pushes material away. Offer alternative.
Reinforcement Cue: When the child makes their first purposeful sound, immediate verbal reinforcement: "YES! That's YOUR drum! Play it as loud as you want!"
Reinforcement Cue: When the child makes their first purposeful sound, immediate verbal reinforcement: "YES! That's YOUR drum! Play it as loud as you want!"

Step 3 — Let the Sound Flow
⏱️ 5–15 minutes — follow the child's lead
Protocol Step 3 of 6
Allow the child to engage with the auditory material at the intensity they seek. This is the active ingredient. The child is controlling the sound — its volume, rhythm, and duration. Your role is to facilitate, not direct. If they want to bang the drum as hard as possible, that is the intervention working.
Your Role During This Step
- Headphone sessions: Let the child listen at their preferred volume (within limiter range) for the full duration. Watch for relaxed body, closed eyes, slight swaying — these are signs the auditory tank is filling.
- Active sound-making: Join if invited. Mirror the child's intensity. Don't correct rhythm or musicality. This is not a music lesson — it's sensory feeding.
- Heavy work + sound: Hammer alongside them. Stomp together. The combination of proprioceptive effort and auditory feedback is maximally satisfying.
Common Execution Errors to Avoid
- ✗ Asking the child to "play more quietly" — this defeats the purpose
- ✗ Correcting how they hold the sticks — this is not a performance
- ✗ Setting too-short timers that interrupt before satiation
- ✗ Trying to make it "educational" — it's therapeutic first
If Escalation Occurs
Child escalating into self-harmful behavior (hitting own head, biting) — transition to cool-down immediately. This signals the current state was too dysregulated for active sound-making.
Meta-analysis: 40-min sessions showed maximum effectiveness; home sessions of 10–20 min with core action occupying 40–60% of time | PMC10955541

Step 4 — Ride the Wave, Then Vary
⏱️ 3–5 minutes
Protocol Step 4 of 6
Most children cycle through 3–5 "bursts" of intense sound-making with brief pauses. Each burst is a therapeutic repetition. Follow the child's natural rhythm — don't impose an external structure on their internal processing cycle.
🥁 Switch Materials
"You've been drumming — want to try the mic?" Variety maintains engagement and allows you to discover which materials produce deepest satisfaction.
🎧 Switch Audio
"Let's try this song — it has more bass!" For headphone sessions, cycling through different genres and energy levels helps identify optimal auditory profiles.
🔨 Switch Modality
"Let's stomp on the bubble wrap now!" Moving between sound types keeps the session fresh and provides data on which inputs register most satisfyingly.
📣 Add Social
"Let's make noise TOGETHER — on three!" For children ready for social engagement, shared sound-making is a powerful next-level activity.
Satiation Indicators — When the Child Has Had Enough
- Speed and intensity of sound-making naturally decreases
- Child sets down instrument without being asked
- Child begins to explore other (non-sound) items in the room
- Body posture shifts from energized to calm
- Child transitions attention — looks at you, looks around the room
"3 good bursts of satisfying sound > 10 forced minutes of structured play." If the child is satiated at 7 minutes, end. The child's nervous system is the timekeeper, not the clock.

Step 5 — Name What Just Happened
⏱️ Within 3 seconds of desired behavior
Protocol Step 5 of 6
Reinforcement is the bridge between what the child just did and what they'll do again tomorrow. Immediate, specific, enthusiastic — those are the three requirements. Delayed praise loses the neural connection.
"You used your DRUMS when you needed loud! That's exactly right!"
"You put on your headphones all by yourself when you wanted music!"
"You waited for loud time — and now you got it! Great job asking!"
What to Reinforce
- Choosing an appropriate sound-making material instead of random banging
- Using headphones instead of turning TV to maximum
- Requesting "loud time" verbally or with gestures
- Transitioning to quiet after loud time without major resistance
- Any attempt to self-regulate auditory needs through the provided tools
"Celebrate the attempt, not just the success." If the child reaches for the headphones but then drops them and screams instead — reinforce the reach, not the scream. Every approximation toward appropriate behavior is worth naming.
Reinforcement Menu: Verbal praise (always available) → High-five or physical celebration → Extended loud time (1 extra minute as reward) → Token toward a larger reward (sticker chart)
ABA Reinforcement Principles: Immediate, specific reinforcement increases behavior occurrence | BACB Guidelines
Reinforcement Menu: Verbal praise (always available) → High-five or physical celebration → Extended loud time (1 extra minute as reward) → Token toward a larger reward (sticker chart)
ABA Reinforcement Principles: Immediate, specific reinforcement increases behavior occurrence | BACB Guidelines
Step 6 — From Loud to Landing
⏱️ 2–3 minutes
Protocol Step 6 of 6
The cool-down is not an afterthought — it's the neurological bridge from intense auditory activation back to baseline regulation. How you end the session determines how the next 30–60 minutes will go.
The Cool-Down by Material Type
Headphone sessions: Gradually decrease volume over the last minute. Transition to calming audio (nature sounds, soft instrumental) before removing. Don't remove headphones abruptly.
Active sound-making: One final "big hit" or "loud song," then guide the child in putting materials away as a predictable ritual. Hand them a calming item: weighted lap pad, squeeze ball, or quiet sensory toy.
If the Child Resists Ending
- Offer a smaller, portable sound item (headphones with soft music, a quiet fidget)
- Show the visual schedule — point to the NEXT loud time: "Look — you have loud time again at [time]"
- If meltdown: allow 2 extra minutes and reattempt transition
- Tomorrow, add 5 minutes to the scheduled loud time — today's data tells you the session was too short
Transition Script:"Loud time is all done. Your ears got what they needed. Now it's [next activity] time."
Visual supports: NCAEP Evidence-Based Practices, 2020
60 Seconds of Data. Right Now.
The difference between a good protocol and a great one is data. Three fields, 60 seconds, right after the session ends while the information is fresh. This data will guide every adjustment you make over the next 8 weeks.
1
Duration
How many minutes did the child engage in structured sound activity? Record the actual time — not what you planned, but what happened. This is your baseline data point.
2
Intensity Satisfaction (1–5)
Did the child appear satisfied after the session?
1 = Still intensely seeking | 2 = Somewhat seeking | 3 = Neutral | 4 = Mostly satisfied | 5 = Clearly regulated and calm
1 = Still intensely seeking | 2 = Somewhat seeking | 3 = Neutral | 4 = Mostly satisfied | 5 = Clearly regulated and calm
3
Random Noise After Session
How long before the child began random noise-making again?
□ Less than 15 min | □ 15–30 min | □ 30–60 min | □ 1+ hour | □ None until next session
□ Less than 15 min | □ 15–30 min | □ 30–60 min | □ 1+ hour | □ None until next session
What the Data Tells You: If satisfaction is 4–5 and random noise stays low for 1+ hours, the sensory diet is working. If satisfaction is 1–2 and noise returns within minutes, the child needs more duration, more intensity, or different materials.
📥 PDF Tracking Sheet:techniques.pinnacleblooms.org/trackers/A046-auditory-seeking
ABA Data Collection Standards: Cooper, Heron & Heward, Applied Behavior Analysis
📥 PDF Tracking Sheet:techniques.pinnacleblooms.org/trackers/A046-auditory-seeking
ABA Data Collection Standards: Cooper, Heron & Heward, Applied Behavior Analysis

The Reality Card: When Sessions Don't Go Perfectly
Every family hits friction. These are the five most common obstacles — and the precise adjustments that resolve them. Session abandonment is not failure — it's data that tells you what to change.
Child Refuses All Materials, Continues Random Banging
Why: The offered materials may not match their specific auditory preference. Some children prefer percussive impact; others prefer sustained tone; others prefer vocal amplification.
Fix: Observe what they're banging. If it's pots (metallic, sustained ring), try cymbals or xylophone. If it's stomping (impact-based), try drum pedal. Match the material to their natural preference, not the other way around.
Fix: Observe what they're banging. If it's pots (metallic, sustained ring), try cymbals or xylophone. If it's stomping (impact-based), try drum pedal. Match the material to their natural preference, not the other way around.
Child Becomes MORE Dysregulated During Loud Time
Why: Possible sensory overload if combined with other stressors, or the activity is too stimulating for current state.
Fix: Switch to headphone-only session (contained, controlled). Reduce to single material. Check: is the child tired, hungry, or already dysregulated before starting?
Fix: Switch to headphone-only session (contained, controlled). Reduce to single material. Check: is the child tired, hungry, or already dysregulated before starting?
Siblings/Family Members Can't Toleratethe Noise
Why: Other family members have normal or higher auditory sensitivity.
Fix: Prioritize headphone activities. Schedule loud time when sensitive family members can leave the room. Designate specific "loud zones" with door closed.
Fix: Prioritize headphone activities. Schedule loud time when sensitive family members can leave the room. Designate specific "loud zones" with door closed.
Child Won't Transition Out of Loud Time
Why: The auditory tank isn't full yet, or transition warning was insufficient.
Fix: Extend by 5 minutes and reassess. Tomorrow, schedule longer loud time from the start. Always give 2-minute and 30-second warnings.
Fix: Extend by 5 minutes and reassess. Tomorrow, schedule longer loud time from the start. Always give 2-minute and 30-second warnings.
Child Seems to Need MORE Volume Than Is Safe
Why: Very high auditory threshold — standard intensity doesn't register.
Fix: Add vibration speaker to combine modalities. Use bone conduction headphones. Add proprioceptive input (heavy work) simultaneously. Consult audiologist for safe volume parameters specific to this child.
Fix: Add vibration speaker to combine modalities. Use bone conduction headphones. Add proprioceptive input (heavy work) simultaneously. Consult audiologist for safe volume parameters specific to this child.
No Two Sound-Seekers Are Identical
The protocol adapts to the child — not the other way around. Use this framework to calibrate the intervention to your child's current state, developmental stage, and sensory profile.
Easier Version
Bad days / Younger children / Just starting
- Headphones only — single material, no transitions, no demands
- 5 minutes, child controls everything
- No "put away" ritual — parent handles cleanup silently
- Used when: child is sick, tired, post-meltdown, or new to the protocol
Standard Version
Most days / Building routine
- 2–3 material options, child chooses
- 15-minute sessions with 2-minute warning transitions
- Include put-away ritual as part of the sequence
- Data capture after session
Advanced Version
Good days / Older children / Established routine
- Full material rotation with child planning their own loud time
- Introduce musical skill-building (simple rhythms, learning songs)
- Child manages visual schedule independently
- Add social component: play with sibling, join a music class
Sensory Profile Variations
Sound-Seeker + Movement-Seeker
Add bouncing on trampoline while wearing headphones. Dancing to loud music. March-and-drum simultaneously. Two sensory systems satisfied at once.
Sound-Seeker + Tactile-Defensive
Use headphones instead of instruments requiring grip. Karaoke mic with soft grip cover. Avoid instruments causing unexpected vibration through hands.
Sound-Seeker + Language Delay
Use karaoke to encourage vocalization. Name sounds during activities: "BOOM! CRASH! TAP!" Incorporate sound-based communication targets.
Individualized intervention planning: Core principle across OT, ABA, SLP clinical practice

Week 1–2: Building the Foundation
Progress Arc
Week 1–2 of 8
Progress in the first two weeks is subtle but real. The nervous system is learning a new association: "loud time" means something specific is coming. Consistency matters more than perfection right now — every session plants a neural seed, even the messy ones.
✅ What Progress Looks Like
- Child begins to associate loud time with specific materials (reaches for drums when told "loud time")
- SOME random banging may decrease — but don't expect dramatic change yet
- Child may show preference for one material over others — this is valuable diagnostic data
- Family is establishing the schedule — routine is the therapy at this stage
⚠️ What Is NOT Progress Yet
- Child is not yet self-managing auditory needs — that comes later
- Random noise-making may not decrease noticeably this week
- Transition out of loud time is still difficult — completely normal
- Don't expect quiet compliance between sessions yet
"If your child reaches for the headphones instead of screaming once this week — that's real progress."
Sensory integration outcomes emerge across 8–12 week timelines | PMC11506176

Week 3–4: The Neural Pathways Are Forming
Progress Arc
Week 3–4 of 8
Something is changing. You may feel it before you can measure it — the household is quieter in between sessions, or your child says something that surprises you. These are the early signs of neural pathway consolidation. The protocol is working.
Anticipation Emerges
Child anticipates loud time — may go to the sound station unprompted. This is the single strongest indicator that the neural association has formed.
Random Noise Measurably Decreases
Check your data! Compare this week's "time before random noise returns" to Week 1. Most families see a meaningful shift in this field by Week 3.
Transitions Become Easier
Child begins to accept transitions out of loud time with less resistance. The visual schedule showing the NEXT loud time is doing its job — anticipation replaces desperation.
Spontaneous Requests Appear
Child may request a specific material: "I want my drums." This is a language-behavior milestone — the child is self-advocating for their sensory need through words.
Parent Milestone: You may notice you're more confident too. The dread of noise is shifting to appreciation of channeled energy. That's your data telling you: this is working.
Behavioral Signs of Neural Formation: Child CHOOSES appropriate outlets without being directed → Checks visual schedule for next loud time → Volume of environmental noise (TV, random banging) decreases → Other family members comment on the improvement
Behavioral Signs of Neural Formation: Child CHOOSES appropriate outlets without being directed → Checks visual schedule for next loud time → Volume of environmental noise (TV, random banging) decreases → Other family members comment on the improvement
Week 5–8: The Transformation
Progress Arc
Week 5–8 of 8
This is the consolidation phase. The behaviors you've been building are becoming habits — for your child, and for your family. The protocol is no longer something you do to the day; it's part of how the day works.
Independent Tool Use
Child independently manages auditory needs using provided tools 80%+ of the time — the mastery threshold.
Noise Reduction
Random, disruptive noise-making reduced by 50%+ from baseline — measurable on your tracking sheet.
Protocol Complete
Most families reach this stage with consistent daily practice. The foundation for lifelong auditory self-regulation is now in place.
Mastery Criteria (Observable, Measurable)
- Can participate in quiet activities for age-appropriate durations (15+ min for ages 3–6; 30+ min for ages 7–12)
- Spontaneously requests "loud time" or appropriate tools instead of creating chaos
- Transitions in and out of loud time with minimal support
- Skill appears in other settings: school, grandparents' house, car
- All mastery criteria consistent for 2+ consecutive weeks = functional auditory self-regulation achieved
Mastery criteria: BACB standards for behavioral measurement | PMC10955541

You Did This. Your Child Grew Because of Your Commitment.
Remember Card 01? The 7:15 AM pot-banging. The TV at maximum. The exhaustion. The guilt about "why can't I make my child quiet?"
Look at where you are now. Your child isn't "quieted." They're regulated. They have tools. They have a schedule. They have materials that feed the need their nervous system was screaming about. The noise isn't gone — it's channeled. Purposeful. Skill-building.
You didn't fail. You learned. You adapted. You gave your child what they needed in ways that work for the whole family.
Document This Milestone
Take a photo of your child using their tools. This image — your child choosing headphones, reaching for their drums — is the evidence of everything you built together.
Write One Sentence
Write one sentence about how your home sounds different now. This is your story. It belongs to you, and it matters deeply.
Tell Another Parent
Share what you learned with one other family navigating this challenge. Your story could be their turning point — the moment they stop feeling alone.
Parental self-efficacy: Strongest predictor of continued home-based intervention implementation
When to Pause and Seek Professional Guidance
The protocol works for most children with consistent implementation. But some presentations require professional eyes and clinical recalibration. Trust your instincts — if something feels wrong, pause and ask. These flags are worth taking seriously.
🔴 Red Flag 1: Increasing Volume Needs Despite Consistent Sensory Diet
What it looks like: After 6+ weeks of structured loud time, the child needs louder and louder sounds to achieve satisfaction.
Why it matters: Could indicate progressive hearing loss, auditory processing changes, or need for audiological re-evaluation.
Action: Schedule audiological assessment.
Why it matters: Could indicate progressive hearing loss, auditory processing changes, or need for audiological re-evaluation.
Action: Schedule audiological assessment.
🔴 Red Flag 2: Sound-Seeking Behaviors Are Intensifying, Not Stabilizing
What it looks like: Random noise-making increases instead of decreasing. Child becomes aggressive when sound access is delayed.
Action: Consult OT for sensory processing re-evaluation. Current sensory diet may need recalibration.
Action: Consult OT for sensory processing re-evaluation. Current sensory diet may need recalibration.
🔴 Red Flag 3: Signs of Actual Hearing Difficulty
What it looks like: Not responding to name at any volume. Difficulty understanding speech. Complaints of ear ringing.
Action: Urgent audiological evaluation. Rule out noise-induced hearing damage.
Action: Urgent audiological evaluation. Rule out noise-induced hearing damage.
🔴 Red Flag 4: Sound-Seeking Interfering with ALL Daily Functioning
What it looks like: Cannot participate in any activity without concurrent loud noise. Sleep disruption. Complete inability to tolerate necessary quiet environments.
Action: Comprehensive multidisciplinary evaluation at Pinnacle center.
Action: Comprehensive multidisciplinary evaluation at Pinnacle center.
Escalation Pathway: Self-resolve (adjust sensory diet at home) → Teleconsult with Pinnacle therapist → In-person assessment at nearest Pinnacle center
📞 FREE National Autism Helpline: 9100 181 181 | 16+ languages | 24×7
pinnacleblooms.org
📞 FREE National Autism Helpline: 9100 181 181 | 16+ languages | 24×7
pinnacleblooms.org
Where You've Been. Where You're Going.
A-046 is one technique within a larger interconnected system of auditory and sensory processing interventions. Understanding your child's pathway forward — and backward — helps you make informed decisions about what to explore next.
◄ Prerequisite — Where You Were
Basic sensory awareness and understanding of seeking vs. avoiding behavior. Related: A-045 Classroom Auditory Processing
● You Are Here — A-046
Auditory Sensory Input Channeling: 9 Materials for Sound-Seeking
The core intervention for auditory hypo-responsivity. This is your current foundation.
The core intervention for auditory hypo-responsivity. This is your current foundation.
► Path A — Musical Instrument Response
Structured music therapy integration → Formal instrument lessons adapted for sensory needs → Group music activities for social + sensory goals
► Path B — Headphone/Contained Input Response
Auditory processing development activities → Therapeutic listening programs → Graduated tolerance for environmental sounds
► Path C — Proprioceptive Seeking Co-Occurrence
A-055: Seeks Intense Sensory Input — Combined auditory + proprioceptive sensory diet → Heavy work protocol integration
↔ Lateral Alternatives (if this approach didn't resonate):
A-043: Hums to Block Sound — explore if child shows mixed seeking/avoiding behavior
A-047: Doesn't Respond to Name — if non-response to speech at normal volumes is the primary concern
A-043: Hums to Block Sound — explore if child shows mixed seeking/avoiding behavior
A-047: Doesn't Respond to Name — if non-response to speech at normal volumes is the primary concern

More in the Auditory Sensory Processing Domain
Auditory seeking rarely travels alone. These related techniques address the adjacent presentations that frequently co-occur with or follow from A-046 — and you may already own materials that cross multiple protocols.

A-043: 9 Materials for Humming to Block Sound
Domain: Auditory Over-Responsivity | Difficulty: Core
The opposite pattern — when the child uses self-generated sound to block environmental noise. Understanding both directions of the auditory threshold spectrum creates a complete picture.
techniques.pinnacleblooms.org → A-043
The opposite pattern — when the child uses self-generated sound to block environmental noise. Understanding both directions of the auditory threshold spectrum creates a complete picture.
techniques.pinnacleblooms.org → A-043

A-044: 9 Materials for Sensitivity to Specific Sounds
Domain: Auditory Over-Responsivity | Difficulty: Core
When specific frequencies or sound types cause distress. Many families find their child is simultaneously a seeker for some sounds and avoidant of others.
techniques.pinnacleblooms.org → A-044
When specific frequencies or sound types cause distress. Many families find their child is simultaneously a seeker for some sounds and avoidant of others.
techniques.pinnacleblooms.org → A-044

A-045: 9 Materials for Classroom Auditory Processing
Domain: Auditory Processing | Difficulty: Core
When the child can't filter important sounds in noisy environments. The school extension of the home protocol — essential for academic participation.
techniques.pinnacleblooms.org → A-045
When the child can't filter important sounds in noisy environments. The school extension of the home protocol — essential for academic participation.
techniques.pinnacleblooms.org → A-045

A-047: 9 Materials When Child Doesn't Respond to Name
Domain: Auditory Responsiveness | Difficulty: Intro
May co-occur with sound-seeking — the child doesn't respond to speech at normal volumes. Evaluating this alongside A-046 creates a complete auditory profile.
techniques.pinnacleblooms.org → A-047
May co-occur with sound-seeking — the child doesn't respond to speech at normal volumes. Evaluating this alongside A-046 creates a complete auditory profile.
techniques.pinnacleblooms.org → A-047
"You already own materials for A-043, A-044, and A-047" — headphones, sound-making toys, and visual schedules cross multiple auditory techniques. The materials system is designed for overlap and efficiency.
A-050: 9 Materials for Intense Sensory Input Seeking — Broader seeking pattern across auditory, proprioceptive, and vestibular domains. The natural next step when multiple sensory systems are seeking simultaneously.
A-050: 9 Materials for Intense Sensory Input Seeking — Broader seeking pattern across auditory, proprioceptive, and vestibular domains. The natural next step when multiple sensory systems are seeking simultaneously.
This Technique Is One Piece of a Larger Plan
Auditory regulation is Domain A in a 12-domain developmental system. When the auditory system is fed and regulated, attention improves, social participation opens up, and learning becomes possible. Every domain benefits when the sensory foundation is stable.
How A-046 Connects to Every Domain
Auditory regulation (Domain A) directly impacts attention for learning (Domains F + J), social participation (Domain C), classroom performance (Domain J), and behavioral regulation (Domain K). When the auditory system is fed, every other domain benefits — the ripple effect is real and measurable.
GPT-OS® Full Profile
See your child's complete developmental map, personalized recommendations across all 12 domains, and progress tracking across every technique.
Your A-046 data feeds directly into the Auditory Modulation Index and Sensory Regulation Index — contributing to a whole-child developmental picture that guides every next recommendation.
From Chaos to Channeled: Real Family Journeys
These are real families, real households, real noise levels — and real change. The journeys below represent the kinds of transformations Pinnacle Blooms families experience when consistent protocol meets patient implementation.
Family Journey 1 — "The Neighbors Think We Moved"
Before: "Our house sounded like a construction site 16 hours a day. Our son banged everything — pots, doors, his own head against the wall when we took the pots away. We were getting noise complaints from neighbors. We felt like failures."
After (8 weeks): "He still loves noise — that hasn't changed, and it shouldn't. But now he has his drum kit and scheduled loud times three times a day. The random banging dropped by about 80%. He actually sits through dinner without drumming on the table because he knows 7 PM loud time is coming."
Timeline: 8 weeks with consistent daily protocol.
Family Journey 2 — "Karaoke Changed Everything"
Before: "She'd scream at maximum volume — not in anger, just to hear herself. She stood next to the blender, the vacuum, the washing machine. We were terrified about her hearing."
After (6 weeks): "Karaoke machine changed everything. She sings into the mic for 20 minutes, gets the vocal-auditory feedback she was screaming for, and then plays quietly for over an hour. We got an electronic drum kit with headphones — she drums silently from our perspective while hearing it loud. Our audiologist confirmed no hearing damage."
Timeline: 6 weeks, karaoke + electronic drums with headphones.
"Sound-seekers are some of the most satisfying children to work with because the intervention is intuitive: give them what they need, channel it appropriately, and the behavioral change is rapid and dramatic. The key insight families need is that suppression doesn't work — channeling does." — Senior Occupational Therapist, Pinnacle Blooms Network
Outcomes vary by child profile. Statistics represent aggregate Pinnacle Blooms Network data.
You Are Not Alone in This
The most powerful supplement to any protocol is community — parents who understand 7:15 AM pot-banging because they've lived it, families who know exactly what "my child turned the TV to maximum again" feels like. Connect with them.
📱 WhatsApp: "Sound-Seeking Parents"
Challenge-specific parent group for families navigating the exact auditory seeking challenges described in this protocol. Tips, material reviews, commiseration, and celebration — from parents who've been where you are.
🌐 Pinnacle Parent Community
Online forum for parents across all sensory processing challenges. Local Pinnacle parent meetups organized by center. 70+ locations across India — there is likely a community near you.
🤝 Peer Mentoring
Connect with an experienced parent who has been through the auditory seeking journey and can share what worked, what didn't, and what they wish they'd known in Week 1.
"Your experience helps others — consider sharing your journey. One parent's story is another family's turning point."
WHO Nurturing Care Framework: Community engagement is a core principle of effective early childhood intervention
Home + Clinic = Maximum Impact
Home implementation is powerful. Clinical support multiplies that power. The combination of consistent daily home practice and expert clinical guidance produces outcomes that neither achieves alone.
AbilityScore® Assessment
Comprehensive baseline evaluation that establishes your child's starting point across all developmental domains and identifies priority intervention areas.
Sensory Processing Evaluation
Conducted within the Diagnostic Intelligence Layer. Standardized assessment of auditory thresholds, sensory-seeking profile, and co-occurring sensory patterns.
Audiological Assessment
Rule out hearing loss and establish safe volume parameters specific to your child. Essential before sustained headphone use and high-volume instrument activities.
Auditory Modulation Index via GPT-OS®
Ongoing progress tracking that connects your home session data to clinician-level analytics. Real-time visibility into your child's regulatory development.
Find Your Support Team
Primary: Occupational Therapist (sensory integration specialized)
Supporting: Audiologist for hearing assessment
Supporting: BCBA for behavioral strategies
Supporting: Audiologist for hearing assessment
Supporting: BCBA for behavioral strategies
FREE National Autism Helpline
📞9100 181 181
16+ languages • 24×7 availability • No cost to families • Immediate connection to trained specialists who understand sensory seeking behavior
The Evidence: For Parents Who Want to Go Deeper
This protocol is built on a foundation of peer-reviewed research spanning systematic reviews, meta-analyses, randomized controlled trials, and population-scale real-world data. Here is the evidence base that informs every technique card in this series.
Study 1 — PRISMA Systematic Review (2024)
"Sensory Integration Interventions for Children with ASD: A PRISMA Model Systematic Review" — 16 articles confirming sensory integration as evidence-based practice.
🔗 PubMed: PMC11506176
🔗 PubMed: PMC11506176
Study 2 — Meta-Analysis (2024)
"Sensory Integration Therapy for Autism: Meta-Analysis of 24 Studies" — Effective promotion of social skills, adaptive behavior, and sensory processing.
🔗 PMC10955541 | DOI: 10.12998/wjcc.v12.i7.1260
🔗 PMC10955541 | DOI: 10.12998/wjcc.v12.i7.1260
Study 3 — Indian Home-Based RCT (2019)
Padmanabha et al. — Validated parent-administered sensory interventions with significant outcomes in Indian pediatric population.
🔗 DOI: 10.1007/s12098-018-2747-4
🔗 DOI: 10.1007/s12098-018-2747-4
Study 4 — WHO CCD Implementation (2023)
"Care for Child Development Package" — Implemented in 54 low- and middle-income countries. Global validation of home-based caregiver-delivered interventions.
🔗 PMC9978394
🔗 PMC9978394
Additional Frameworks: WHO Nurturing Care Framework (2018) | AOTA Sensory Processing Guidelines | NCAEP Evidence-Based Practices Report (2020) | UNICEF MICS Developmental Indicators (197 countries) | Oxford Centre for Evidence-Based Medicine (OCEBM) Levels of Evidence | Dunn's Model of Sensory Processing (spdfoundation.net)
The Intelligence Layer Behind This Technique
Every session you run, every data point you record, feeds an evidence-based intelligence system that continuously personalizes your child's intervention path. This is what separates a static protocol from a living, adaptive therapeutic system.
How GPT-OS® Works with Your A-046 Data
Input: Duration of sessions, satisfaction ratings, random-noise frequency after sessions — the data from Card 20.
Processing: Auditory Modulation Index tracks your child's progression from "constant, uncontrolled seeking" through "independently manages auditory needs." Cross-references with 21 million+ session data points to predict developmental trajectory.
What You Get Back
- Personalized material recommendations: "Based on your child's response pattern, add vibration speaker on Thursday"
- Schedule optimization: "Morning + evening sessions show best regulation outcomes for your child"
- Progression alerts: "Your child is ready for advanced musical skill-building"
- Related technique recommendations based on full developmental profile
🔒Privacy: All data is encrypted, anonymized for population analysis, and never shared with third parties. You own your data.
Digital health interventions for ASD: 21 RCTs, 1,050 participants per 2024 meta-analysis

See This Technique in Action
Reel A-046
Sensory Solutions — Episode 46
Auditory Hypo-Responsivity
Watch a Pinnacle Blooms therapist demonstrate each of the 9 materials with a child who actively seeks loud sounds. See the transformation from chaotic sound-seeking to channeled, purposeful auditory input — in real time, with real children.
Headphones delivering immersive sound
Watch the child's body language transform the moment intense audio registers through volume-limited over-ear headphones.
Drums providing controlled impact + auditory feedback
The combination of proprioceptive strike and auditory reward — demonstrated at the right intensity level for therapeutic effect.
Karaoke for vocal sound-seekers
A child who screamed to hear herself now sings into a mic — same neurological need, radically more appropriate and skill-building outlet.
Visual loud time schedule in action
See how a simple visual schedule reduces seeking between sessions — the child can see the next loud time is coming, and waits.
Video modeling: Evidence-based practice for autism (NCAEP, 2020)
Consistency Across Caregivers Multiplies Impact
Children don't regulate in one setting and seek in another — the nervous system is portable. When every caregiver in your child's life uses the same framework, the protocol's impact multiplies across every environment your child inhabits.
📱 Share via WhatsApp
One-tap share with formatted summary — the right format for grandparents, aunts, uncles, and anyone involved in daily care.
📥 Download: Family Guide (1-Page PDF)
Everything in one printable page: the 9 materials, the schedule template, the safety rules, and the key message: "This is a sensory need, not misbehavior."
📋 "Explain to Grandparents" Version
"Your grandchild seeks loud sounds because their brain needs more auditory input than typical children. This isn't a behavior problem — it's a neurological difference. Here's how we help: we give them appropriate ways to get loud sound (drums, headphones, karaoke) at scheduled times. Between those times, they're calmer because the need is being met. Please don't tell them to 'be quiet' — instead, offer them their headphones or drums."
📝 Teacher/School Communication Template
"[Child's name] has auditory hypo-responsivity, meaning their nervous system requires more auditory input to register and regulate. They are not being deliberately noisy. Recommended classroom accommodations include headphone breaks with preferred audio, music class participation as regulatory support, and outdoor breaks for vocal release. Formal accommodation documentation available from Pinnacle Blooms."
WHO CCD: Multi-caregiver training is critical for intervention generalization | PMC9978394
Your Questions, Answered
Eight questions that come up again and again — from families just starting out, from grandparents who aren't sure, and from parents who have been at it for weeks and hit a stumbling block. The answers are clinical, but the language is yours.
Q1: Is my child's hearing being damaged by all this noise-seeking?
A: Possibly — which is why audiological evaluation is essential. However, channeling the seeking into volume-limited headphones and monitored drumming is dramatically safer than uncontrolled noise-seeking. An audiologist can establish safe volume parameters specific to your child.
Q2: Will my child outgrow this?
A: The neurological threshold difference typically persists, but the child's ability to self-regulate and use appropriate outlets improves dramatically with intervention. They learn to manage their auditory needs — they don't outgrow them. And that's enough.
Q3: How is this different from my child just being "a loud kid"?
A: All children are noisy. Sensory seeking is persistent, intense, regulatory in function, and continues regardless of consequences or environment. If your child seeks loud sound even when alone, it's likely sensory rather than attention-based.
Q4: My child's teacher says they can't be this loud in class. What do I do?
A: Use the teacher communication template from Card 37. Formal accommodations include headphone breaks, music class participation, and outdoor vocal release. Pinnacle centers provide school consultation documentation.
Q5: Can I do too much loud time?
A: Yes — hearing damage is real. Monitor decibel levels, use volume-limiting headphones, and ensure loud time is intense but not sustained at damaging levels. Brief impacts (drum hits) are safer than sustained high volume (hours of maximum headphones).
Q6: What if we live in an apartment and can't be loud?
A: Prioritize headphones (contained sound). Electronic drum kit with headphone output. Karaoke app with headphones. Schedule outdoor loud time at parks. Even in apartments, the child can have intense personal auditory input without environmental noise.
Q7: Should I get a hearing test?
A: Yes. Always. Rule out hearing loss as a factor. Hearing loss and sensory seeking can coexist or be confused with each other. An audiological evaluation is a prerequisite for safe, sustained intervention.
Q8: How quickly will I see results?
A: Most families report noticeable reduction in random noise-making within 2–3 weeks of consistent daily protocol. Full behavioral consolidation typically occurs at 6–8 weeks. Your data tracker (Card 20) will show you the progression in real time.
Didn't find your answer? Ask GPT-OS® → pinnacleblooms.org/gptos-ask | Still need help? Book a teleconsultation → pinnacleblooms.org/teleconsult

Your Child's Auditory System Has Been Waiting. Start Today.
You have the knowledge. You have the materials — or know how to make them. You have the protocol, the safety guidelines, the data tracker, and the community. There is nothing left to wait for. The nervous system that's been seeking, banging, and screaming for more sound is ready to be met with exactly what it needs.
▶ START THIS TECHNIQUE TODAY
Launch the GPT-OS® guided session for Auditory Sensory Input Channeling. Your personalized protocol begins now.
📞 BOOK A CONSULTATION
Connect with a Pinnacle Blooms OT or audiologist for personalized guidance on implementing this protocol for your specific child.
📞FREE National Autism Helpline: 9100 181 181
🔄 EXPLORE NEXT TECHNIQUE
Ready to keep building? Explore adjacent interventions in the auditory sensory processing domain.
Validated by the Pinnacle Blooms Consortium
OT • SLP • ABA • SpEd • NeuroDev
21M+ Sessions | 97%+ Improvement | 70+ Centers
Preview of 9 materials that help when child seeks loud noises Therapy Material
Below is a visual preview of 9 materials that help when child seeks loud noises therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.









Link copied!

From Fear to Mastery. One Technique at a Time.
You arrived on this page hearing pot-banging, screaming, and the TV at maximum volume. You leave with 9 materials, a daily protocol, a progress tracker, and a community of families who understand.
Your child isn't "too loud." Your child's nervous system is communicating a need. And now you know how to answer it.
Built by Mothers. Engineered as a System. Powered by GPT-OS® — Global Pediatric Therapeutic Operating System.
🌐 Explore More Techniques
techniques.pinnacleblooms.org
The largest structured pediatric intervention knowledge base on Earth.
The largest structured pediatric intervention knowledge base on Earth.
📞 FREE National Helpline
9100 181 181
16+ languages | 24×7
No cost to families
16+ languages | 24×7
No cost to families
🔗 Pinnacle Blooms Network®
Medical Disclaimer: This content is educational. It does not replace assessment by a licensed occupational therapist, audiologist, or healthcare provider. Persistent sound-seeking, hearing concerns, or significant sensory processing differences may require comprehensive evaluation and professional-guided intervention. Individual results may vary. Statistics represent aggregate outcomes across the Pinnacle Blooms Network.
© 2026 Pinnacle Blooms Network®, unit of Bharath Healthcare Laboratories Pvt. Ltd. All rights reserved. CIN: U85100TG2016PTC108492 | DPIIT: 0100089253 | MSME: 0824560731 | GSTIN: 01012235788
techniques.pinnacleblooms.org — The largest structured pediatric intervention knowledge base on Earth.