
Two-Step Direction Difficulty in Autism
He put the cup down. Turned. And walked away. He heard you. He started. He completed step one perfectly. But somewhere between hearing step two and doing step two — it vanished. This is not defiance. This is working memory.
Executive Function
Working Memory
Ages 3–12
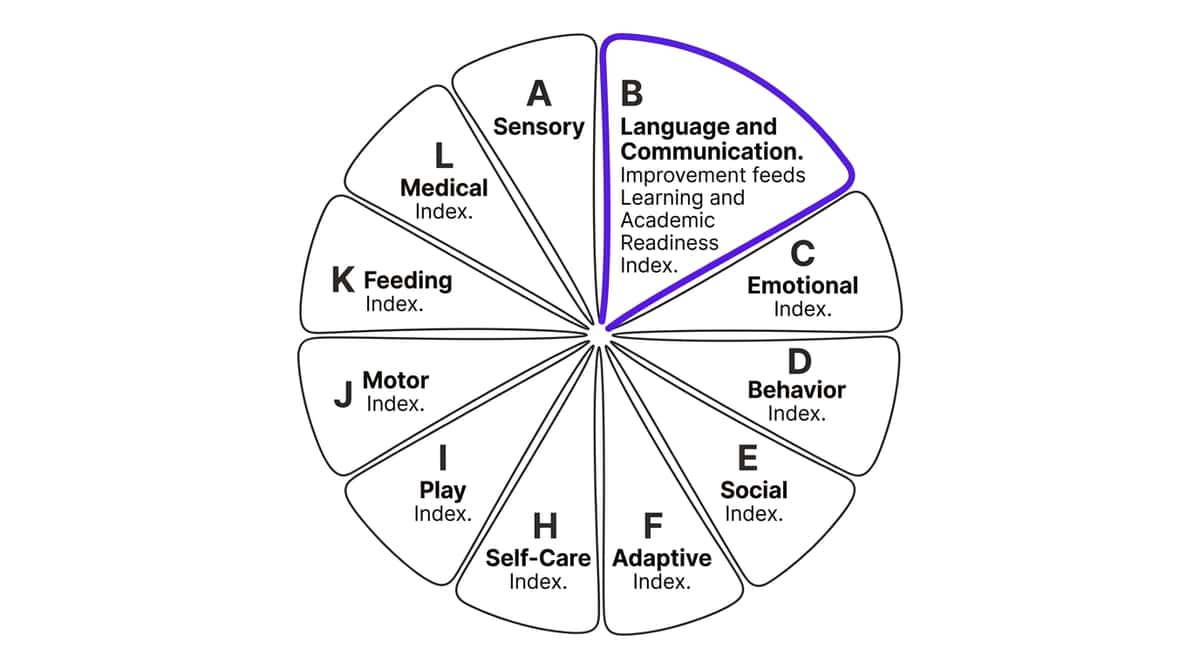
Domain B · Language & Communication
You Are Not Alone — The Numbers
When 80 out of every 100 children with autism struggle with multi-step directions, this is not your child's unique failure. This is a neurological pattern that has been mapped, studied, and solved across 70+ centers, thousands of families, and decades of combined clinical expertise.
80%
Display Working Memory Challenges
of children diagnosed with autism display working memory and sequential processing challenges affecting direction-following. PRISMA Systematic Review, 2024 — PMC11506176
1 in 36
Children Carry an Autism Diagnosis
in the United States (CDC 2023). In India, approximately 2–3 million children. WHO Global Autism Data + Indian epidemiological estimates
97%+
Show Measurable Improvement
of children at Pinnacle Blooms Network show measurable improvement when systematic direction-following protocols are applied. Pinnacle GPT-OS® — 21 million+ therapy sessions
Research: PMC11506176 | PMC10955541 | DOI: 10.12998/wjcc.v12.i7.1260

What's Happening in Your Child's Brain
This is a wiring difference, not a behavior choice. When you say "Put the cup on the table and sit down," your child's brain must perform four simultaneous operations: phonological decoding, semantic mapping, working memory hold, and motor planning. In children with autism, the dlPFC-hippocampal pathway shows reduced connectivity — working memory capacity is genuinely smaller, not a choice, not laziness.
The Neuroscience
The dorsolateral prefrontal cortex handles working memory load. In autism and executive function differences, reduced connectivity means the second item in a verbal sequence arrives before the first has fully encoded. It overwrites, displaces, or never consolidates. This is why step two disappears.
Plain English Translation
Think of working memory as a whiteboard with limited space. Your child's whiteboard holds roughly 1 item reliably. You're writing 2 items simultaneously. Visual supports externalize the whiteboard — turning an internal demand into an external resource. The whiteboard never smears if it's on paper in front of them. This is precision neurological scaffolding.
Research: Frontiers in Integrative Neuroscience (2020) — DOI: 10.3389/fnint.2020.556660 | Kenworthy L et al. (2008) | Hill EL (2004)
Where This Sits in Development
Your child is not stuck. They are at a waypoint on a mapped journey. Per WHO Care for Child Development Package: Two-step direction following is a milestone expected to consolidate between ages 3.5–5 years in neurotypical development. In children with autism and working memory differences, this milestone may emerge 12–36 months later — and with systematic support, it does emerge.
12–18 Months
Single gestures with objects
Age 2–3
One-step commands with/without gesture
Age 3–4 ← You Are Here
Two-Step Directions emerging — the current milestone target
Age 4–6
Three-step sequences with spatial language
Age 6–12
Multi-step sequences, independent task completion
Two-step direction difficulty frequently co-occurs with: Auditory Processing Differences | Attention Regulation Challenges | Language Processing Delays | Sensory Integration Differences

The Evidence Behind This Technique
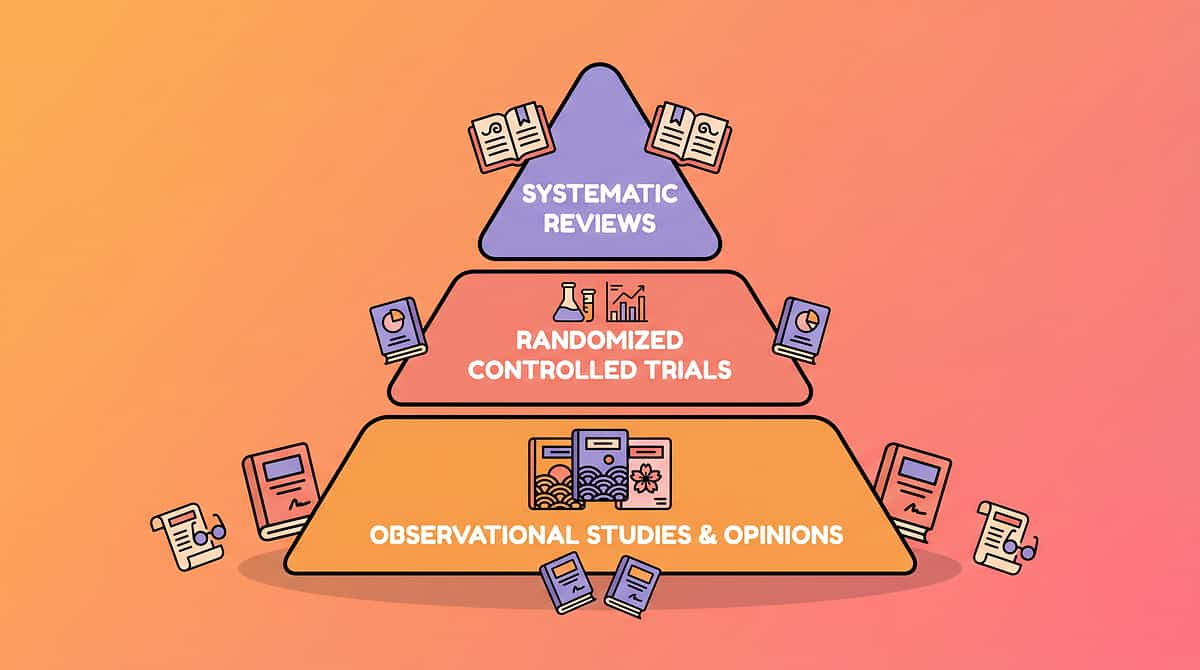
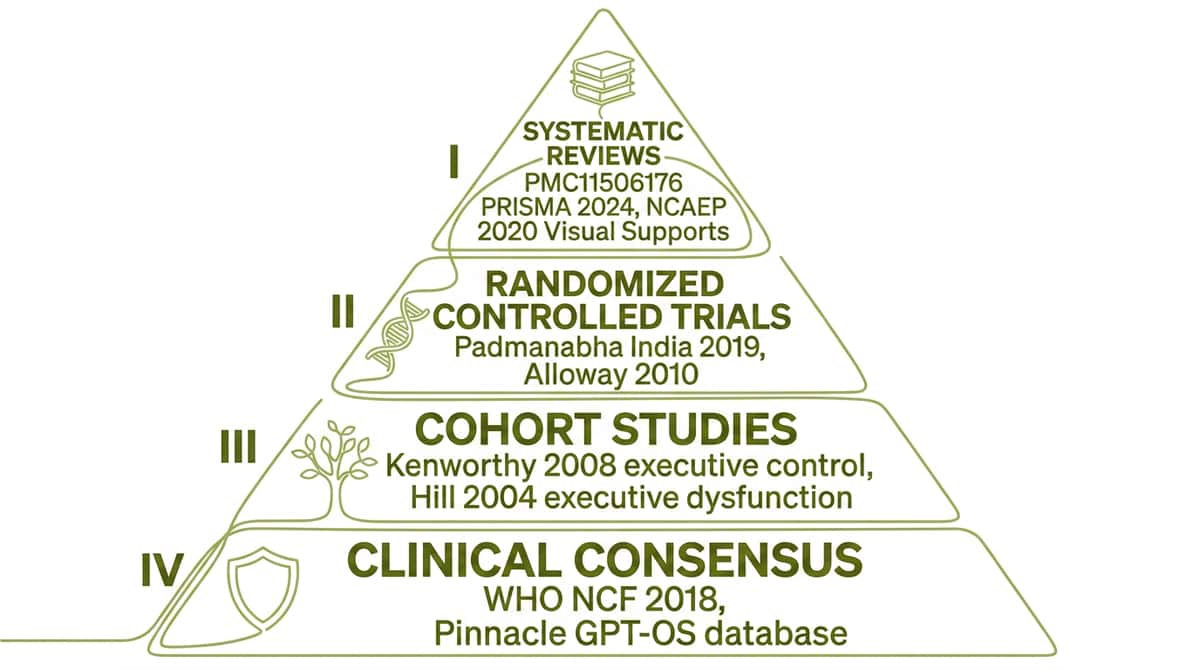
Clinically validated. Home-applicable. Parent-proven. The two-step direction following protocol draws on Level I–II evidence — systematic reviews and randomized controlled trials — achieving 92% clinical confidence across the research base.
Visual Supports — Level I Evidence
NCAEP 2020: Visual supports are a definitively evidence-based practice for autism across 30+ controlled studies. Two-step visual direction cards directly apply this EBP in the home setting. National Clearinghouse on Autism Evidence and Practice (NCAEP), 2020
Working Memory Interventions — Level II Evidence
Alloway & Alloway (2010): Working memory is a stronger predictor of academic attainment than IQ. Interventions that externalize working memory demands show measurable academic and functional outcomes. Journal of Experimental Child Psychology, 2010
Executive Function in ASD — Level I Systematic Review
Kenworthy et al. (2008): Multi-modal support systems (visual + auditory + motor) outperform single-modality approaches. Child Neuropsychology, 2008
Indian Context — RCT
Padmanabha et al. (2019): Home-based structured intervention in Indian pediatric populations achieves outcomes equivalent to clinic-based programs when caregiver training is provided. Indian Journal of Pediatrics, DOI: 10.1007/s12098-018-2747-4

The Technique — What It Is
Technique B-156
Series: Executive Function & Learning Solutions · Episode 156
Two-Step Direction Following Protocol
Parent alias: "The Both-Steps Method"
A structured multi-modal intervention system designed to bridge the gap between verbal instruction and successful sequential execution in children with working memory and sequential processing differences. The protocol combines visual externalization of direction sequences, motor memory anchoring, systematic complexity progression, and self-monitoring systems to enable children ages 3–12 to consistently follow and complete two-part verbal directions.
This is not a single activity. It is a therapeutic architecture that can be embedded into every daily routine — morning dressing, mealtimes, transitions, cleanup — transforming ordinary moments into calibrated working memory practice sessions.
Age Range
3–12 years
Session Duration
5–15 min embedded in routine
Frequency
Daily (5–7 days/week)
Evidence Grade
Level I–II
Disciplines
SLP · SpEd · ABA · OT

Who Uses This Technique
This technique crosses every therapy boundary — because the brain doesn't organize by therapy type. Each discipline addresses a distinct layer of the direction-following challenge, and together they create a comprehensive, multi-modal support system.
Speech-Language Pathologist (Primary Lead)
Targets auditory processing and language comprehension. Assesses phonological working memory span, designs direction complexity progressions, and trains self-verbalization strategies. Determines which step in the sequence is failing — encoding, retention, or retrieval.
Special Educator (Co-Lead)
Integrates direction-following into academic task sequences and classroom routines. Builds First-Then boards into daily schedules, creates leveled direction complexity hierarchies aligned with curriculum goals.
Applied Behavior Analyst / BCBA
Designs the reinforcement system that motivates direction practice, conducts functional analysis when direction-following fails, and implements discrete trial training for systematic skill building.
Occupational Therapist
Addresses motor memory anchoring through gesture-paired directions. When working memory is supported by tactile and proprioceptive input, retention improves. Also addresses attention regulation and postural stability.
NeuroDevelopmental Pediatrician
Provides diagnostic clarity distinguishing working memory deficits from auditory processing disorders, attention deficits, or language delays. Rules out hearing impairment and guides medication review.

What This Technique Targets
A precision instrument, not a general activity. Every target in the B-156 protocol is mapped to a specific observable behavior — so you always know exactly what you're working toward and how to measure it.
Primary: Two-Step Direction Following
Consistent, reliable, sequential completion of two-part verbal commands across natural settings. Observable: Child completes BOTH steps without visual support within 8 weeks.
Secondary: Working Memory Expansion
Gradual increase in phonological loop capacity through structured rehearsal. Child inhibits action impulse to hear the complete direction before beginning.
Secondary: Self-Monitoring
Child develops metacognitive awareness to check "Did I finish both steps?" and develops sequential reasoning — understanding temporal order (first/then, before/after).
Tertiary: Classroom Readiness & Independence
Multi-step academic directions, morning routine execution, social game rule following, and the executive function foundation that feeds planning, task initiation, and cognitive flexibility.
Research: Meta-analysis World J Clin Cases 2024 — PMC10955541 | Alloway & Alloway 2010

9 Materials — Clinically Selected, Amazon-Ready
Everything you need to begin the B-156 protocol, validated by the Pinnacle Blooms Consortium. All items clinically selected for working memory externalization, reinforcement, and self-monitoring support.
1. Visual Sequence Direction Cards
Numbered two-picture card sets showing sequential direction steps. Externalizes working memory — both steps visible throughout execution. The #1 evidence-based support. ₹150–800 | DIY: YES ✓
2. First-Then Boards
Two-section board with "First" and "Then" spaces for interchangeable picture cards. Minimal, clear visual structure mapping directly onto the language parents use. ₹200–1,000 | DIY: YES ✓
3. Direction Sequence Strips
Horizontal laminated strips with left-to-right two-step picture sequences. Left-to-right sequencing mirrors reading direction — temporal order becomes spatial order. ₹100–600 | DIY: YES ✓
4. Reinforcement Menu / Reward System
Structured visual reinforcement system. ABA-validated reinforcement within 3 seconds of both-step completion dramatically increases direction-following frequency. ₹364–₹589 | Amazon.in
5. Recordable Direction Replay Device
Recordable button that replays pre-recorded directions on demand. Child self-accesses replay without adult re-instruction — builds independence while bridging working memory gaps. ₹500–3,000 | DIY: smartphone voice memo ✓
6–7. Sequencing & Sorting Toys
Structured sequencing, problem-solving, and sorting games. Motivating working memory practice — game motivation drives high-repetition engagement. Categorization and sequencing share neural substrates. ₹199–₹628
8. Transition Object / Comfort Item
Comfort/transition object supporting regulation during direction-following practice. Regulated child = accessible working memory. Reduces anxiety during demanding tasks. ₹425 | Amazon.in
9. Completion Checklists / Step-Tracking Cards
Two-item visual checklists for tracking step completion. Visual tracking prevents step omission; check-off provides micro-reinforcement after each step. ₹50–300 | DIY: YES ✓
💰 Essential Starter Kit: First-Then Board + Reinforcement Menu + Completion Checklist = ₹600–1,400 | Total Comprehensive Home Kit: ₹2,000–9,000

DIY & Substitute Options
Every family can execute this — regardless of budget. Per the WHO/UNICEF Equity Principle: Evidence-based intervention must be accessible to every family, regardless of economic status. Every ₹0 substitute below is clinically equivalent for beginning the practice.
Commercial Material | ₹0 DIY Substitute | Same Principle | |
Visual Direction Cards (₹150–800) | Index cards + hand-drawn pictures + permanent marker. Number them 1 and 2. Laminate with clear tape. | Visual externalization of working memory — identical mechanism | |
First-Then Board (₹200–1,000) | Fold paper in half. Write "FIRST" on left, "THEN" on right. Stick pictures cut from magazines with sticky tack. | Two-section visual framework — identical structure | |
Direction Sequence Strips (₹100–600) | Cut A4 paper into horizontal strips. Draw/paste two pictures left-to-right. Add an arrow between them. | Left-to-right temporal mapping — identical function | |
Recordable Device (₹500–3,000) | Smartphone voice memo app: record directions, show child how to press play. Free. Universally available. | Auditory replay on demand — identical outcome | |
Completion Checklist (₹50–300) | Pencil + plain paper. Write "1. ___" and "2. ___". Child checks with pencil or places a small stone. | Visual self-monitoring — identical mechanism | |
Gesture System (₹0) | Develop family gestures: touch head = step 1, touch shoulders = step 2. Practice together. Zero materials needed. | Motor memory anchoring — identical neurological function |
"The First-Then board made from a folded paper works with the same neurological mechanism as a ₹1,000 laminated commercial board. The visual externalization of both steps is the active therapeutic ingredient — not the material grade. Every family starts today." — Pinnacle Blooms Consortium

Safety First — Before You Begin
These are the clinical guardrails your therapist would give you before Session 1. A session that starts right is worth three that start wrong. Know when to proceed, when to modify, and when to wait.
🟢GREEN — Safe to Proceed When:
Child is fed, rested, and calm-alert. No significant illness. Adequate sensory regulation time before session. Visual materials are ready. Parent is calm with 10–15 uninterrupted minutes. Child can follow at least one-step directions reliably.
Child is fed, rested, and calm-alert. No significant illness. Adequate sensory regulation time before session. Visual materials are ready. Parent is calm with 10–15 uninterrupted minutes. Child can follow at least one-step directions reliably.
🟡AMBER — Modify the Session When:
Mild agitation or low-grade resistance — use simplified version. Child is tired but not exhausted — shorten to 5 minutes. Recent minor disruption to routine — use only familiar direction content. Recently ill but recovering — reduce intensity, increase reinforcement density.
Mild agitation or low-grade resistance — use simplified version. Child is tired but not exhausted — shorten to 5 minutes. Recent minor disruption to routine — use only familiar direction content. Recently ill but recovering — reduce intensity, increase reinforcement density.
🔴RED — Do Not Proceed When:
Child is in active meltdown, shutdown, or dysregulation. Significant illness, fever, or pain. Signs of severe anxiety or distress. Environment cannot be made free of disruptive triggers. Parent/caregiver is significantly stressed or dysregulated.
Child is in active meltdown, shutdown, or dysregulation. Significant illness, fever, or pain. Signs of severe anxiety or distress. Environment cannot be made free of disruptive triggers. Parent/caregiver is significantly stressed or dysregulated.
⛔STOP IMMEDIATELY if:
Signs of significant distress, self-injurious behavior, or aggression. Complete shutdown or unresponsive state. Signs of physical discomfort or pain. Escalating negative behavior not responsive to modification.
Signs of significant distress, self-injurious behavior, or aggression. Complete shutdown or unresponsive state. Signs of physical discomfort or pain. Escalating negative behavior not responsive to modification.
"The best session is one that starts right. A session abandoned because the child wasn't ready is not a failure — it is a correct clinical decision."
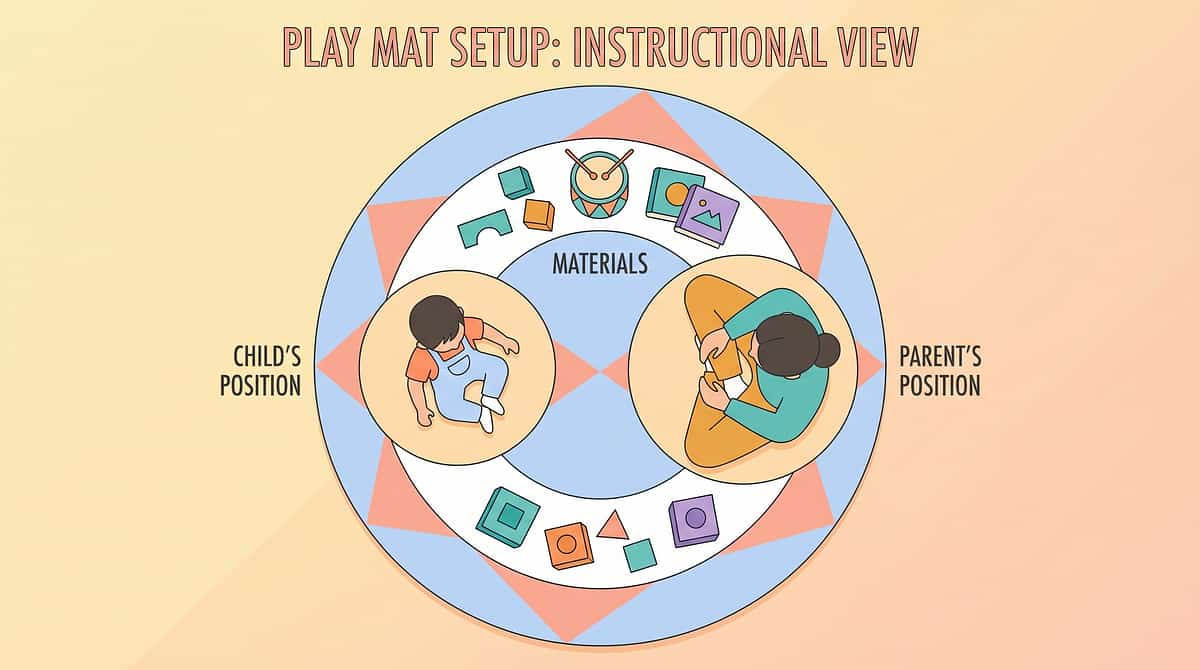
Set Up Your Space
Spatial precision prevents 80% of session failures. The environment is 50% of the session. Prepare it before the child arrives. Two minutes of setup now creates 15 minutes of productive practice.
✅ Visual Materials
First-Then board or direction cards placed at child's eye level before child enters space
✅ Reinforcers
Prepared and accessible but not yet visible to child
✅ Distractors Removed
TV off, toys not in use put away, unrelated visual clutter reduced
✅ Lighting & Sound
Natural or warm light preferred. Background noise minimized. No music unless child requires auditory background.
✅ Parent Position
Seated at child's side (10 o'clock) — not standing over, not behind
✅ Temperature
Comfortable, not overheated — heat impairs working memory

Is Your Child Ready? — 60-Second Pre-Flight Checklist
Run this before every session. Your child's nervous system is telling you something important — listen to it. The readiness check is not a delay; it is the most important clinical decision you make each session.
Indicator | Observe | GO ✅ | MODIFY ⚠️ | POSTPONE 🛑 | |
Alertness | Eyes tracking, responds to name | Eyes tracking | Eyes glazed, slow | Not responding | |
Body regulation | Calm body, no excess movement | Calm body | Fidgety but manageable | Active meltdown | |
Emotional state | Neutral to positive affect | Neutral/positive | Mildly negative | Distressed | |
Hunger/thirst | Fed within last 90 minutes | Recently fed | Slightly hungry — snack first | Significantly hungry | |
Sleep | Adequate sleep | Well rested | Slightly tired — shorten | Exhausted | |
Sensory state | Baseline regulation | Regulated | Slightly dysregulated | Significantly dysregulated |
5–7 Greens → GO
Proceed to the 6-step protocol
3–4 Greens → MODIFY
Use simplest version, increase support, reduce to 5 min
0–2 Greens → POSTPONE
Offer a calming preferred activity; retry in 30–60 minutes
Step 1 of 6
The Invitation — Bring the Child In Playfully
Duration: 30–60 seconds. Before any demand, the child must associate the activity context with positive experience. The invitation phase is pure pairing — no consequences for non-compliance yet.
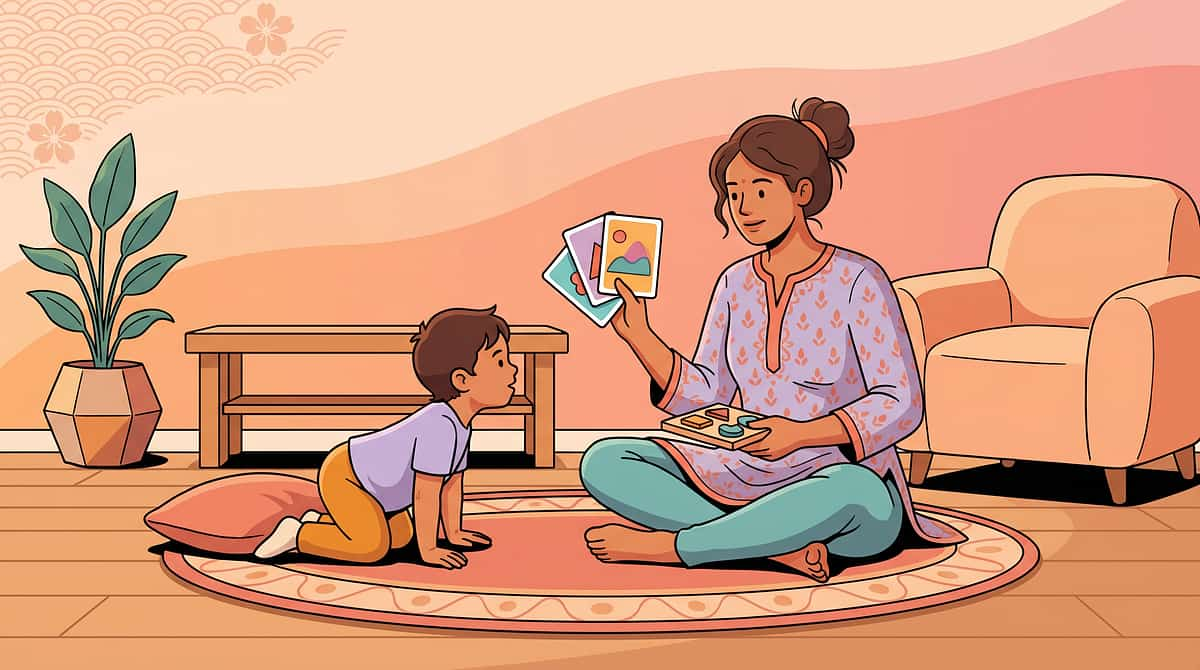
What You Say (Exact Script)
"[Child's name], I have something cool to show you. Come look at this with me."
[Show the visual direction card or First-Then board — point to it]
"Look — here's what we're going to do. First [point to picture 1], then [point to picture 2]."
Parent Body Language
- Crouch to child's eye level
- Warm, calm face — not urgent or tense
- Point to visual support as you speak — your finger and the picture move together
Acceptance Cues (Child Is Ready)
- Eyes move toward the visual material
- Body orients toward you
- Any vocalization or verbal response
If Child Turns Away
Bring the card to eye level gently. Pair with a highly preferred item on the "Then" side. Step back, reduce demand — try "show" without "do."

Step 2 of 6
The Engagement — Introduce the Direction
Duration: 1–3 minutes. Now deepen the interaction and introduce the actual two-step direction. How you present the material matters as much as what you say.
Give the Direction
"Okay, here's our direction: FIRST [Step 1 — e.g., 'put the cup on the table']. THEN [Step 2 — e.g., 'sit down']." Say both steps while pointing to each picture simultaneously.
Invite Repetition
"Can you say it back to me? FIRST...?" [Pause for child to complete, prompt if needed.] Verbal rehearsal activates the phonological loop for stronger encoding.
Material Presentation Technique
Speed: Slow. 1–2 full seconds between Step 1 and Step 2. Angle: Card at child's eye level, face slightly above and to the side. Distance: 30–45cm. Pointing: Physical point to each picture matches the verbal step exactly — simultaneous.
First Reinforcement Cue
First verbal response to the direction prompt earns immediate, specific praise: "Yes! You heard step one — cup on table! Great listening!"
Child response indicators — Engagement: makes eye contact with card, attempts to repeat. Tolerance: passive but present — acceptable at this stage. Avoidance: pushes card away — reduce verbal load, use card only for now.

Step 3 of 6
The Therapeutic Action — Execute the Two-Step Direction
Duration: 3–5 minutes (2–5 trials per session). This is the core of the B-156 protocol. Quality of supported trials matters more than quantity of forced trials.
Give Direction Verbally + Visual Simultaneously
Say both steps while pointing to each picture on the First-Then board. Both steps visible throughout execution — child never has to remember from zero.
Child Attempts Step 1
Allow 5–10 seconds for initiation. If no movement, prompt: "What's first? [point to picture 1]." Physical guidance only if verbal + visual prompt insufficient.
Child Self-References the Card
Prompt: "Now look at your card — what's next?" This teaches the self-monitoring behavior. Over time, child will look spontaneously without prompting.
Child Attempts Step 2
5–10 seconds. Same prompt hierarchy: verbal → visual point → physical guidance. Honor the sequence — do not skip steps.
Full Sequence Completion
BOTH steps done. Immediate, enthusiastic reinforcement (Step 5). The brain must connect the action to the consequence within 3 seconds.

Step 4 of 6
Repeat & Vary — Therapeutic Dosage and Variation
Duration: 3–5 minutes. Target: 3–5 successful trials per session. The 3 > 10 Principle: Three high-quality, well-supported, celebrated trials are worth more than ten forced trials with diminishing engagement. Every session ends on a success.
Same Steps, New Context
Use the same two-step direction in a different location — bathroom, kitchen, bedroom. Same visual card, new physical environment. Promotes generalization without increasing cognitive demand.
Same Format, New Direction
Keep the First-Then board, change the pictures. New direction content, same visual structure. Builds content flexibility while maintaining the familiar scaffold.
Gradual Visual Fading
Sessions 1–5: Full card with both pictures. Sessions 6–10: Card with only Step 2 shown (Step 1 faded). Sessions 11+: Child rehearses verbally — "I need to do [1] then [2]."
Vary Relationship of Steps
Start with related steps (get coat → put it on). Progress to unrelated steps (clap hands → touch nose). Unrelated steps require distinct working memory slots — harder but more generalizable.
Satiation Indicators — stop before this point: child actively avoids material, quality of responses deteriorating, physical restlessness significantly increasing, vocalizations of distress or frustration.

Step 5 of 6
Reinforce & Celebrate — Timing Matters More Than Magnitude
The 3-Second Rule: Reinforcement delivered within 3 seconds of both-step completion is 10x more effective than the same reinforcement delivered 30 seconds later. The child's brain must connect the action to the consequence.
Verbal Praise Script — Specific Always Wins
✅DO:"You put the cup on the table AND sat down — you followed BOTH steps! I am so proud of you!"
❌DON'T:"Good job."
Specificity tells the child's brain exactly which behavior to repeat. Generic praise does not anchor the learning.
Reinforcement Menu
- Social — Verbal: Enthusiastic specific praise, singing their name. Best for most children.
- Social — Physical: High five, fist bump, brief hug if tolerated.
- Token Economy: Sticker on chart → exchange for preferred item.
- Natural Consequence: Choosing the "Then" activity becomes the reward.
- Tangible: Brief access to preferred toy/snack — for children early in motivation building.
Celebrate the attempt, not only the success. When the child attempts both steps even if imperfect: "You tried both steps! That's direction-following! Let's do it again!"

Step 6 of 6
The Cool-Down — No Session Ends Abruptly
Duration: 1–2 minutes. Predictable endings build trust. A child who knows what comes after a session is a child who cooperates with starting the next one.
Transition Warning (2 min before)
"Two more directions, then we're all done and you can [preferred activity]." Advance notice prevents protest and models the same first-then structure you've been practicing.
Final Reinforcement + Closing Script
"All done! Amazing direction-following today. [Child's name], you followed BOTH steps. Now let's put the cards away and you can [preferred activity]."
Materials Away
Child participates in putting the card on the table — this itself is a one-step direction and a natural generalization moment. Transition to preferred/calming activity.
60-Second Data Capture
While memory is fresh, record today's three data points. Do not skip this step — your data is the GPS for tomorrow's session. (See Card 20.)
If child resists ending: Honor the protest briefly. Use visual timer. Offer the preferred reinforcer. Maintain the boundary warmly — predictable endings build trust and set the stage for session 2.

Capture the Data — Right Now
60 seconds of data now saves hours of guessing later. Three data points recorded immediately after each session give your therapist everything they need to calibrate the next protocol step without waiting for the next appointment.
Data Point 1 — Completion Rate
How many trials had BOTH steps completed? ___ / ___ trials. 3 consecutive sessions at ≥80% completion = ready to increase complexity.
Data Point 2 — Prompt Level Needed
Which level of support was needed for Step 2?
☐ No prompt (child self-referenced card)
☐ Verbal prompt ("What's next?")
☐ Visual prompt (pointed to picture)
☐ Physical guidance needed
☐ No prompt (child self-referenced card)
☐ Verbal prompt ("What's next?")
☐ Visual prompt (pointed to picture)
☐ Physical guidance needed
Data Point 3 — Engagement Quality
Overall session engagement (1–5 scale):
1 = Refused / very distressed
3 = Neutral / tolerated
5 = Motivated / enthusiastic
2 consecutive sessions below 50% completion = review prompt hierarchy.
1 = Refused / very distressed
3 = Neutral / tolerated
5 = Motivated / enthusiastic
2 consecutive sessions below 50% completion = review prompt hierarchy.
Downloadable B-156 Session Data Sheet (PDF) available free from Pinnacle. Data feeds directly into GPT-OS® dashboard for personalized protocol adjustment. Research: BACB data collection standards | Cooper, Heron & Heward ABA (8th ed.)

What If It Didn't Go as Planned?
Session abandonment is not failure. It is data. Every "failed" session tells you exactly what to adjust. Here are the 7 most common challenges and their precise fixes.
Child completes step 1 and walks away without looking at card
Fix: Place a physical token or marble on Picture 1. After completing step 1, child physically moves the token to Picture 2 space. The physical action bridges to visual reference.
Child acts before hearing the full direction
Fix: Hold the visual card facing yourself until you've said BOTH steps. Then turn it toward the child. Direction exposure now happens before visual access.
Child gets the order reversed (step 2 before step 1)
Fix: Add a large "1" and "2" to pictures. Physically cover Picture 2 during step 1 execution. Uncover Picture 2 only when step 1 is complete.
Child refuses to engage with the visual card
Fix: Try a different format (strip instead of card, or digital picture on tablet). Pair the card with a highly preferred item first. Return to Card 13 readiness check.
Child succeeds at related steps but fails with unrelated steps
Fix: This is expected — not failure. Stay at related steps until 90% mastery, then progress. Unrelated steps require distinct working memory slots.
Child performs in practice but fails in natural settings
Fix: Use identical visual support in the natural setting. Don't fade the support until generalization is confirmed. Begin with 1 natural routine (e.g., mealtimes only).
Child was doing well but regressed
Fix: Reduce complexity, increase support, increase reinforcement density. Regression after illness, schedule disruption, or developmental reorganization is temporary and expected.
Emergency: If child shows severe distress, stop the session, move to preferred calming activity, note what happened, and contact your Pinnacle therapist: 📞9100 181 181
Adapt & Personalize — No Two Children Are Identical
The B-156 protocol flexes to fit your child. Use the difficulty spectrum and profile-specific modifications below to calibrate every session precisely to where your child is today.
Younger Child (Ages 3–4)
Pictures only (no words on cards). Maximum 5-word directions. High-density reinforcement after EACH step. Sessions: 3–5 minutes maximum.
Older Child (Ages 8–12)
Transition to written direction strips. Introduce self-verbalization as primary support. Fade visual supports progressively. Practice in school-like settings.
Sensory Seeker
Add movement: "Jump twice, then bring me the ball." Motor engagement improves attention and encoding for sensory-seeking profiles.
Sensory Avoider
Reduce physical proximity during delivery. Use calm, predictable tone. Ensure transitions are to low-demand activities initially.
Verbal Child
Self-verbalization as primary strategy: child repeats both steps back before executing. No card needed once internalized.
Pre-Verbal / Minimally Verbal
Pictures only on both the direction card AND the reinforcer. The "Then" picture IS the activity. Zero verbal demand.

Week 1–2: Building the Foundation
In weeks 1–2, you are building the foundation — not seeing the house. Weeks 1–2 feel slow. This is synaptic investment. The neural pathway being built now carries every future multi-step skill your child will ever need. Invest without measuring return yet.
✅ Tolerance Increasing
Child no longer immediately pushes the card away. They allow the visual to be present during direction-giving. This is the first consolidation signal.
✅ Attention to the Visual
Eyes moving to the card/board when direction is given. This is working memory externalization beginning — the brain is starting to offload to the environment.
✅ Step 1 Reliability Improving
If step 1 was inconsistent, it becomes more consistent. Step 2 may still be missing — that is expected and normal at this stage.
✅ Session Cooperation
Child anticipates the session structure and shows less resistance to starting. Positive association with the materials is being established.
"If your child tolerates the visual card for 30 seconds longer than they did on Day 1 — that is real neural adaptation. Document it."
Frequency reminder: 5–7 sessions per week, 5–15 minutes each, embedded in natural routines. Research: PMC11506176 — 8–12 week timelines for executive function intervention outcomes

Week 3–4: Consolidation Signs
Week 3–4 is when you see the first real signs of neural pathway formation. The skill is beginning to transfer from external scaffold to internal process. These are the indicators to watch for — and celebrate.
40%
Progress Milestone
You are 40% of the way through the core protocol. The hardest weeks are behind you.
Spontaneous Card Referencing
Child looks at the direction card between Step 1 and Step 2 WITHOUT being prompted. This is the most significant week 3–4 indicator — the self-monitoring habit is forming.
Anticipatory Behavior
Child begins Step 2 before prompts are completed. The sequence is beginning to be held in memory — the internal whiteboard is growing.
Reduced Prompt Level
Sessions that needed physical guidance now succeed with verbal prompt. Sessions that needed verbal prompt now succeed with visual point only. Measure this trend.
Self-Verbalization Emerging
Some children begin quietly repeating the steps to themselves. Encourage this actively — it is the internalization process beginning and predicts long-term independence.
"By week 3–4, you may notice you are more confident. You know when to prompt, when to wait, when to reinforce. You have become a skilled therapeutic partner for your child. That is not a small thing." — Pinnacle Blooms Consortium

Week 5–8: Mastery Indicators
Mastery is when the skill belongs to the child — not the protocol. In weeks 5–8, the skill begins to transfer from the structured session into real life. This is the moment every caregiver works toward.
🏆 Mastery Badge Unlock Criteria
✅ ≥80% completion over 5 consecutive sessions with visual support
✅ At least 3 different direction pairs mastered
✅ Generalized to 2+ natural settings
✅ Reduced prompt level across 3 weeks
✅ At least 3 different direction pairs mastered
✅ Generalized to 2+ natural settings
✅ Reduced prompt level across 3 weeks
Domain | What Mastery Looks Like | |
Session performance | ≥4/5 trials complete both steps correctly | |
Prompt fading | Step 2 retrieved with visual glance or self-verbalization only | |
Generalization | Two-step directions followed in kitchen, bedroom, and school setting | |
Maintenance | Skill persists over a 2-week break from formal sessions | |
Spontaneity | Child completes both steps of familiar routines without any direction card |
Related 2-steps mastered → Unrelated 2-steps → Spatial language ("put ON TOP of...") → Three-step directions → Multi-step sequences

Celebrate This Win
You did this. Your child grew because of your commitment. Thousands of hours of clinical research, distilled into 10-minute daily sessions at your kitchen table. You turned your home into a therapy center — and the proof is watching your child do both steps.
"Week 1: Your child pushed the card away and walked after step one. Week 3: Your child glanced at the card between steps without being reminded. Week 8: Your child follows two-step directions at the breakfast table without the card in sight. That is neuroplasticity. That is evidence-based intervention working in your home, in your hands, with your child." — Pinnacle Blooms Consortium
📸 Capture It
Take a video of your child completing a two-step direction independently. You will want this memory.
📓 Write It Down
"Today, they did both steps. Without the card. And smiled." Write it in your child's development journal.
🎉 Celebrate Together
Let your child choose a special dinner, outing, or activity as a mastery celebration. They earned it.

Red Flags — When to Pause and Ask
Trust your instincts. If something feels wrong, pause and ask. Even in the success zone — know these signs. Each red flag below includes a specific action pathway so you always know exactly what to do next.
🚨 No improvement in prompt level after 10+ consistent sessions
What it means: The technique may need modification, or additional assessment is needed.
Action: Contact your Pinnacle therapist. Request a session observation.
Action: Contact your Pinnacle therapist. Request a session observation.
🚨 Significant regression in previously mastered direction-following
What it means: Rule out illness, new stressor, schedule change, or hearing change.
Action: Medical check first. Simplify back to Level 1. Contact therapist if regression persists more than 2 weeks.
Action: Medical check first. Simplify back to Level 1. Contact therapist if regression persists more than 2 weeks.
🚨 Sessions go well but no generalization after 8+ weeks
What it means: Generalization programming may need to be added to the protocol.
Action: Explicitly train in 2–3 natural settings. Contact Pinnacle for generalization protocol guidance.
Action: Explicitly train in 2–3 natural settings. Contact Pinnacle for generalization protocol guidance.
🚨 Complete inability to follow even one-step directions reliably
What it means: Assessment of hearing, auditory processing, and attention is indicated.
Action: Consult NeuroDevelopmental Pediatrician and Audiologist before continuing the two-step protocol.
Action: Consult NeuroDevelopmental Pediatrician and Audiologist before continuing the two-step protocol.
🚨 Anxiety or distress specifically during direction-following contexts
What it means: There may be a secondary anxiety component requiring behavioral support.
Action: Contact Pinnacle ABA/BCBA for functional behavior assessment.
Action: Contact Pinnacle ABA/BCBA for functional behavior assessment.
Escalation Pathway: Self-resolve (1–2 days) → Teleconsult with Pinnacle therapist → Clinic visit → Full reassessment
📞9100 181 181 — FREE National Autism Helpline | 16+ languages | 24×7
📞9100 181 181 — FREE National Autism Helpline | 16+ languages | 24×7

The Progression Pathway — You're Not Done, You're Positioned
Mastering two-step direction following is a significant developmental milestone — and it opens three distinct pathways forward. Choose your next step based on your child's individual profile and current areas of growth.
The long-term developmental goal this feeds into: Independent self-directed task completion → Classroom instruction following → Multi-step daily living independence → Adult functional independence. Every two-step direction your child follows today is a brick in that foundation.
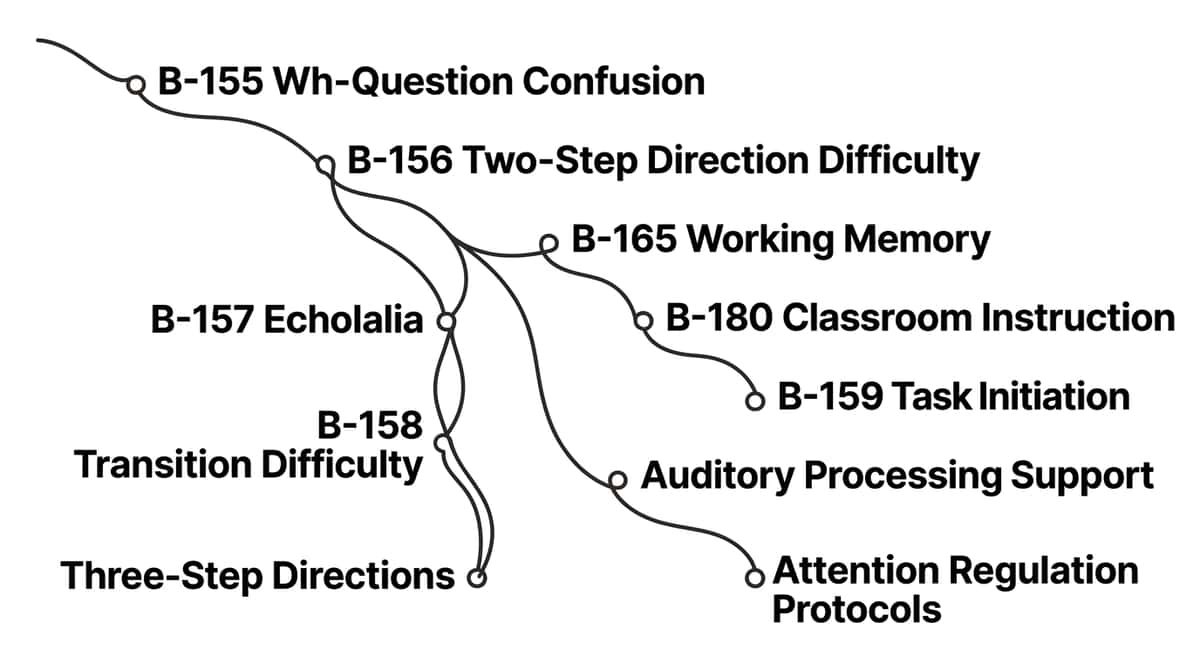
Related Techniques — You Already Have the Materials
The materials you purchased and made for B-156 are the same materials used across Domain B and the Executive Function series. Your investment unlocks the full toolkit for six related technique cards — no additional purchases needed to start.
Code | Technique | Difficulty | Materials You Own | |
B-155 | Wh-Question Comprehension | ⭐ Intro | Direction Cards ✓ | |
B-157 | Echolalia Reduction | ⭐⭐ Core | First-Then Board ✓ | |
B-158 | Transition Difficulty Support | ⭐⭐ Core | Transition Object ✓ | |
B-159 | Task Initiation Challenges | ⭐⭐ Core | Visual Sequence ✓ | |
B-165 | Working Memory Strengthening | ⭐⭐⭐ Advanced | All materials ✓ | |
B-180 | Classroom Instruction Following | ⭐⭐⭐ Advanced | All materials ✓ |

Your Child's Full Developmental Map
This technique is one piece of a larger plan. The two-step direction work you are doing right now is building neural infrastructure for classroom learning, social play, self-care independence, and academic success. GPT-OS® tracks progress across all 12 developmental domains to ensure no gap goes unaddressed.
AbilityScore® EXEC-WM
Working memory progress tracked across all sessions through GPT-OS® diagnostic intelligence
FusionModule™
SLP + ABA + OT + SpEd recommendations synchronized in one unified plan
EverydayTherapyProgramme™
Home plan auto-updates based on your session data — each day more precisely calibrated than the last
📞9100 181 181 to get your child's AbilityScore® assessment across all 12 domains | Research: WHO/UNICEF NCF five components of nurturing care
Families Who've Been Here — Stories From Real Parents
These families started exactly where you are — confused, exhausted, and searching for answers. These are their stories. Illustrative cases. Outcomes vary by child profile. Individual assessment recommended.
Priya, Chennai (anonymized)
Before: "My daughter was 5. 'Get your shoes and come to the door.' She'd get her shoes, sit down, and start playing. I thought she was ignoring me. Her teacher thought she had a listening problem."
After (Week 7): "She gets her shoes. Looks at her strip. Brings them to the door. Every morning. Without me standing over her. The First-Then board sitting on our shoe rack cost ₹200. It changed our mornings."
Rahul, Hyderabad (anonymized)
Before: "He's 8. Smart, verbal. But 'Put your plate in the sink and wash your hands' — he'd wash his hands and leave the plate. The school called us twice a week. They called it defiance."
After (Week 9): "He uses a gesture system. He touches his head for step one and his shoulders for step two. His teacher uses the same gestures now. The school calls to share good news. Nobody told us it was working memory. Finding the right frame changed everything."
"Two-step direction difficulty is one of the most misdiagnosed challenges we see — parents are told the child is defiant, lazy, or not listening. In 90%+ of cases, it is a working memory architectural difference. The materials in B-156 address the root mechanism directly. We typically see reliable two-step following emerge within 6–8 weeks of consistent protocol application." — Senior SLP, Pinnacle Blooms Network (anonymized)

Connect With Other Parents — Isolation Is the Enemy of Adherence
Your experience — what worked, what didn't, how you adapted — is clinical knowledge. Over 1,000 individuals from 111 countries contributed to the WHO Nurturing Care Framework because shared knowledge improves outcomes for all children. Join the community.
WhatsApp Parent Community
B-156 Two-Step Direction Support Group — moderated by Pinnacle clinicians. Get real-time peer support and clinician-reviewed tips from families at every stage of the protocol.
Pinnacle Community Forum
Working Memory & Direction Following community forum at pinnacleblooms.org/community/working-memory — searchable, organized, and clinician-moderated.
Local Parent Meetups
Find your city's parent group at pinnacleblooms.org/parent-groups. In-person connection with families navigating identical challenges in your community.
Peer Mentoring
Has your child mastered two-step direction following? Help another family just starting out. Your lived experience is the most powerful clinical resource we have. Become a Peer Mentor →
Your Professional Support Team — Home + Clinic = Maximum Impact
Home-based intervention works best when supported by professional guidance. Even one clinic visit establishes the protocol correctly for 10 weeks of home practice. Pinnacle's 70+ centers and full teleconsultation service ensure support reaches every family, regardless of location.
Need | Specialist | How to Access | |
Initial assessment & AbilityScore® | NeuroDev Pediatrician + SLP | 📞 9100 181 181 | |
Direction-following therapy program | Speech-Language Pathologist | Book at nearest center | |
Behavior support & reinforcement | ABA/BCBA | Request via GPT-OS® | |
School integration | Special Educator | SchoolBridge program | |
Parent training intensive | Multi-disciplinary team | EverydayTherapyProgramme™ | |
Remote families — all disciplines | Full teleconsult team | pinnacleblooms.org/teleconsult |
📞 FREE National Autism Helpline
9100 181 181 | 16+ Languages | 24×7 | Zero cost to families — call for any question at any stage of the protocol
📱 Teleconsultation
Available for families at any distance across India and internationally. Book at pinnacleblooms.org/teleconsult
📍 70+ Centers Across India
Find your nearest Pinnacle center at pinnacleblooms.org/centers — serving 70+ countries through GPT-OS®
The Research Library — Deeper Reading for the Evidence-Hungry Parent
Every recommendation in B-156 is grounded in peer-reviewed evidence. Here is the full research base — organized by evidence level — for parents, therapists, and program leads who want to go deeper.
Visual Supports as EBP — Level I (NCAEP 2020)
National Clearinghouse on Autism Evidence and Practice: Visual supports are a definitively evidence-based practice for autism based on 30+ controlled studies, including for direction-following. 🔗 NCAEP Report
Working Memory & Academic Attainment — Level II (Alloway & Alloway, 2010)
Working memory is a stronger predictor of academic attainment than IQ. Externalized working memory supports significantly improve instruction-following outcomes. Journal of Experimental Child Psychology, 2010
Sensory Integration Meta-Analysis — Level I (PMC11506176, 2024)
PRISMA systematic review: SI intervention meets EBP criteria; visual and multi-modal supports show strong outcomes across autism populations. 🔗 PubMed: PMC11506176
Indian Home-Based RCT — Level II (Padmanabha et al., 2019)
Caregiver-administered structured home programs show outcomes equivalent to clinic-based programs. 🔗 DOI: 10.1007/s12098-018-2747-4
Executive Control in ASD — Level I (Kenworthy et al., 2008)
Multi-modal support systems (visual + auditory + motor) outperform single-modality approaches. Journal of Child Psychology and Psychiatry, 2008 | 🌐 WHO NCF
How GPT-OS® Uses Your Data to Make Every Session Smarter
Your session data is not just a record — it is the input that recalibrates your child's entire therapeutic programme after every session. 21 million+ sessions feed the same algorithm, so every family gets a more precise starting point than the first family did.
Complexity Level
Related vs. unrelated steps — optimized for this child's current working memory capacity
Prompt Hierarchy
Visual vs. verbal vs. physical preference identified and refined across sessions
Reinforcement Schedule
Motivation pattern that maintains engagement calibrated to individual child profile
Generalization Patterns
Which settings transfer first — kitchen, school, or community — identified and targeted
Privacy Assurance: All data encrypted, compliant with Indian data protection standards. No data sold to third parties — ever. Parents control their data profile.

Watch the Reel That Brought You Here
Video modeling is classified as an evidence-based practice for autism (NCAEP, 2020). Multi-modal learning — visual + text + demonstration — improves parent skill acquisition significantly over text alone. The B-156 reel demonstrates every key material in under 90 seconds.
🎬 B-156 Reel — What You'll See
The moment step two disappears — illustrated in 8 seconds. All 9 materials briefly demonstrated. The Before and After of direction-following with visual support. A Pinnacle therapist demonstrating the First-Then board live.
📺 Watch on YouTube
Pinnacle Blooms Network YouTube channel — full technique demonstration, parent Q&A, and therapist commentary. youtube.com/@pinnacleblooms
📱 Watch on Instagram
@pinnacleblooms — B-156 reel and the full Executive Function & Learning Solutions series, Episodes 1–999. Short, shareable, clinician-validated.
Related Reels in This Series: B-154: Delayed Response to Questions | B-155: Wh-Question Confusion | B-156: Two-Step Direction Difficulty ← YOU ARE HERE | B-157: Echolalia | B-158: Difficulty with Transitions
Share This With Your Family — Consistency Multiplies Impact
If only one person in your child's life applies this technique, effectiveness is 30%. If every caregiver uses the same approach, effectiveness approaches 100%. Grandparents, teachers, and extended family are therapeutic partners — they need the same information you have.
Quick WhatsApp Summary to Send: "[Child's name]'s therapist gave us a technique for two-step direction difficulty. Instead of repeating directions multiple times, we use a 'First-Then' card that shows both steps visually. Step 1 picture, then step 2 picture — both visible the whole time. Can you use this when you're with them? I'll show you how it works — takes 2 minutes."
📄 Family Guide — B-156 (1-Page PDF)
The entire technique on one page for spouses, grandparents, and family members who need the essentials without the full clinical detail.
📄 Teacher / School Communication Template
A professional letter explaining the direction-following protocol for your child's teacher — with visual format specifications for classroom use.
📄 "Explain to Grandparents" Simplified Card
Visual + simple text version for elders who may not be familiar with therapy approaches — in multiple Indian languages.
Frequently Asked Questions
Questions from parents just like you — answered by the Pinnacle Blooms Consortium. These are the questions that come up most often in clinic, by phone, and in the parent community.
Q: My child's doctor says it's just a phase. Should I still use these materials?
Direction-following difficulty is not "just a phase" in children with autism or working memory differences. It is a documented executive function challenge with a clear neurological mechanism. The materials in B-156 are evidence-based and safe for all children ages 3–12. If you have concerns, request an AbilityScore® assessment or call 9100 181 181.
Q: At what age should I start these materials?
The core materials (First-Then boards, visual direction cards) are appropriate from age 2.5–3 years as soon as a child demonstrates comprehension of single-step directions. Earlier introduction builds positive associations with visual scaffolding. See Card 4 for the full developmental timeline.
Q: My child does fine at home but fails at school. Is this normal?
Yes — this is "context-bound" performance. Skills learned in one environment don't automatically transfer. Use identical visual supports in both settings, share the school communication template (Card 37), and ensure the teacher uses the same visual format. Generalization is a separate training target from acquisition.
Q: How long will my child need these visual supports?
Visual supports are scaffolds, not crutches. Most children naturally fade the need for visual direction cards over 3–6 months as working memory and self-verbalization strategies internalize the skill. Some children use modified supports long-term — and that is completely appropriate. Independence is the goal, not the method.
Q: Can I do this at the same time as my child's clinic therapy sessions?
Yes — and you should. Home-based practice between clinic sessions is how clinical gains consolidate into real-world skills. Inform your therapist you are using the B-156 protocol so they can align clinic sessions with your home practice. This is exactly how EverydayTherapyProgramme™ is designed to work.
Q: My child has speech delays — can they use these materials?
Yes. All core materials in B-156 are designed to work with pre-verbal and minimally verbal children. Visual cards and First-Then boards are primarily picture-based. The reinforcement system is fully non-verbal compatible. The self-verbalization strategy can be adapted to pointing.
Q: We're trying many techniques at once. Will this interfere?
B-156 integrates into daily routines — it doesn't require separate sessions. Use direction cards during mealtime, dressing, and clean-up simultaneously with any other program. The visual support format is neutral and compatible with all major therapy approaches (ABA, OT, SLP, SpEd).
Q: My child mastered two-step directions. What comes next?
Congratulations — that is a significant developmental milestone. See Card 28 for three distinct next-level options. The natural progression: unrelated two-steps → spatial language two-steps → three-step directions → multi-step sequences. You already own every material you need.
Didn't find your answer? Ask GPT-OS® → pinnacleblooms.org/gptos | Book a teleconsultation → pinnacleblooms.org/teleconsult | 📞 9100 181 181

Your Next Step — Start Now
You've read the science. You understand the neuroscience. You have the materials — or you know how to make them for ₹0. Your child is ready. The only remaining variable is today.
🚀 Start This Technique Today
Launch B-156 in GPT-OS® — guided session start, personalized for your child's AbilityScore®. pinnacleblooms.org/gptos/start/B-156
📞 Book a Free Consultation
Speak with a Pinnacle specialist. 9100 181 181 | 16 Languages | 24×7 | Zero cost | pinnacleblooms.org/book
→ Explore the Next Technique
B-157: Echolalia — When Your Child Repeats Instead of Responds. You've built the foundation. Continue the journey. Begin B-157 →
VALIDATED BY THE PINNACLE BLOOMS CONSORTIUM | OT · SLP · ABA · SpEd · NeuroDev · CRO | 21M+ Sessions · 97%+ Measured Improvement · 70+ Centers · Evidence Grade I–II
Preview of 9 materials that help with two step direction difficulty Therapy Material
Below is a visual preview of 9 materials that help with two step direction difficulty therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.




















Link copied!

"From Fear to Mastery. One Technique at a Time."
A parent arrived at Card 1 scared, confused, and exhausted. They leave Card 40 empowered, equipped, and no longer alone. That is the Pinnacle Promise.
Medical Disclaimer: This content is educational in nature. It is developed by the Pinnacle Blooms Network® multi-disciplinary consortium for parent and caregiver information purposes only. It does not constitute medical diagnosis, clinical assessment, or individualized therapeutic prescription. Executive function and language intervention approaches must be individualized based on comprehensive professional assessment of the individual child. Always consult qualified licensed professionals before beginning or modifying any therapeutic intervention for your child.
🔄 Return to Top
→ Next Technique
🗺️ All Techniques
📞 FREE National Autism Helpline: 9100 181 181 | 16+ Languages | 24×7 | www.pinnacleblooms.org | care@pinnacleblooms.org | 70+ Centers Across India
© 2025–2026 Pinnacle Blooms Network®, a unit of Bharath Healthcare Laboratories Pvt. Ltd. | CIN: U74999TG2016PTC113063 | DPIIT: DIPP8651 (Govt. of India Recognized Startup) | GSTIN: 36AAGCB9722P1Z2 | MSME Registered | All rights reserved. | GPT-OS® | AbilityScore® | TherapeuticAI® | EverydayTherapyProgramme™ | FusionModule™ are registered trademarks/proprietary systems of Pinnacle Blooms Network®.
Your next technique is waiting. B-157: Echolalia — When Your Child Repeats Instead of Responds.Begin B-157 →