
He keeps hitting his head. Over and over. And nothing I do makes it stop.
You've tried holding his hands. Saying "no." Redirecting. Crying in the bathroom when he can't see you. What if the hitting is not a behavior problem — but a message your child's nervous system is sending, and nobody has taught you how to read it yet?
Technique A-108
Sensory Solutions Series • Episode 108
Domain: Proprioceptive Processing
🔵 Validated by the Pinnacle Blooms Consortium: OT • ABA/BCBA • SLP • SpEd • NeuroDev

You Are Not Alone. These Numbers Prove It.
When your child hits themselves for sensory input, they are doing exactly what their nervous system is programmed to do: seek the proprioceptive feedback it cannot register any other way. This is one of the most common — and most misunderstood — behaviors in sensory processing disorder.
80%
Children with ASD
experience significant sensory processing difficulties — making sensory-based interventions among the highest-priority therapeutic targets in pediatric practice.
1 in 36
Children in India
currently identified with autism spectrum disorder, per National Trust India and NIMHANS estimates.
4.7M
Indian Families
estimated to be navigating sensory-seeking self-hitting right now, per GPT-OS® population modeling.
"80% of children with ASD display sensory processing difficulties, making sensory-based interventions among the highest-priority therapeutic targets in pediatric practice." — World Journal of Clinical Cases, Meta-Analysis, 2024 | PMC10955541
You are among millions of families navigating this exact challenge. And there are 9 clinically validated materials that change everything.
Their Brain Is Not Getting the Signal
The Proprioceptive Pathway
In a typical nervous system, sensory receptors in muscles and joints send signals up the spinal cord, through the brainstem, and into the somatosensory cortex — producing a clear sense of body position and force.
In children with sensory processing disorder or autism, this pathway is often hypo-responsive — it fires too weakly. The brain receives a faint whisper when it needs a shout.
So the child provides their own input. Hitting generates the intense proprioceptive signal the nervous system craves. From the inside, it feels like relief — like finally being able to hear.
Plain English: What's Happening
The proprioceptive system lives in your child's muscles, joints, and connective tissue. Its job: tell the brain where the body is in space, how hard something is, and how much force to use.
When this system is under-responsive, the brain's signal bar reads critically low. Your child isn't hitting out of defiance or aggression. They are hitting because it is the most efficient way their nervous system knows how to feel regulated.
"This is a wiring difference, not a behavior choice. The proprioceptive system requires more input than typical to achieve a regulated state." — SPD Foundation
This is not aggression. This is not defiance. This is a nervous system asking for help in the only language it currently knows.
Your Child Is Not Behind. They Are At a Waypoint.
Self-hitting most commonly emerges between ages 2–4, precisely when proprioceptive seeking behaviors peak in development. Understanding where your child sits on the developmental map turns fear into a clear, actionable path forward.
1
Birth–12 Months
Body awareness foundations established through touch, movement, and caregiver interaction.
2
12–24 Months
Proprioceptive exploration begins — rolling, climbing, and rough-and-tumble play provide essential heavy-work input.
3
2–4 Years ⭐ A-108 Zone
Seeking behaviors peak. Most common window for self-hitting to present. Typical motor play channels may be insufficient for sensory-different nervous systems.
4
4–7 Years
Self-regulation strategies emerge with consistent intervention. Child begins initiating safe input alternatives.
5
7–10 Years
Independent regulation becomes possible. Child self-selects materials, requests input verbally, regulates across multiple environments.
What Commonly Co-Occurs
- Teeth grinding (A-107)
- Oral seeking / chewing everything (A-109)
- Tactile defensiveness
- Gravitational insecurity
- Vestibular seeking behaviors
Where You're Heading
"Your child is here. Here is where we're heading — to a child who seeks input safely, spontaneously, through the 9 materials on this page."

Clinically Validated. Home-Applicable. Parent-Proven.
Evidence Confidence
High — based on systematic reviews and RCT support for sensory integration intervention in ASD.
Home Applicability
Very High — all 9 materials can be implemented in a standard home environment without clinical equipment.
Parent Feasibility
Very High — validated by the Pinnacle Blooms Network across 21 million therapy sessions.
Study | Finding | Source | |
PRISMA Systematic Review (2024) | 16 studies confirm proprioceptive-based SI meets evidence-based practice criteria for ASD | PMC11506176 | |
Meta-analysis, 24 studies (2024) | SI therapy effectively promotes adaptive behavior, social skills, sensory processing, gross/fine motor | PMC10955541 | |
Padmanabha et al., Indian RCT (2019) | Home-based sensory interventions demonstrated significant outcomes in Indian pediatric population | DOI: 10.1007/s12098-018-2747-4 | |
NCAEP Evidence Review (2020) | Sensory-based interventions classified as evidence-based practice for autism across multiple domains | NCAEP 2020 Report |
"This technique is backed by international research, Indian RCT data, and 21 million therapy sessions within the Pinnacle Blooms Network®."

What Is Technique A-108?
Proprioceptive Input Substitution Protocol
Parent-Friendly: "Replace Hitting with Healing Input"
Formal Definition
When a child hits themselves for sensory input, their proprioceptive system is under-responsive — it isn't registering body position, force, and movement signals adequately through typical activity.
This intervention provides functionally equivalent proprioceptive alternatives: materials that deliver the same deep-pressure, heavy-work, and impact sensation the child is seeking — through safe, structured, clinician-designed channels.
The goal is not to stop the behavior through punishment or restraint. The goal is to replace it with something that works better.
At a Glance
Domain A
Sensory Processing
Sub-Domain
Proprioceptive & Deep Pressure
Age Range
2–10 years
Session Duration
10–20 minutes
Canon Materials: Weighted Equipment • Resistance Tools • Impact Alternatives • Enclosure Devices
Pinnacle ID: A-108 | Sensory Solutions Series | GPT-OS® Behavioral Self-Regulation Index
Five Disciplines. One Unified Goal. Zero Self-Hitting.
Effective intervention for sensory-seeking self-hitting is never a single-discipline effort. Each professional sees a different facet of the same child — and every facet matters.
Occupational Therapist (OT) — Primary Lead
Conducts Sensory Profile assessment to confirm proprioceptive hypo-responsivity. Designs the sensory diet, selects and sequences the 9 materials, monitors arousal level, and calibrates weight, resistance, and timing throughout intervention.
ABA / BCBA — Behavior Specialist
Conducts Functional Behavior Assessment (FBA) to confirm sensory-seeking function. Designs the replacement behavior protocol, tracks frequency reduction data, and implements the reinforcement schedule for material use.
Speech-Language Pathologist (SLP)
Addresses oral-proprioceptive seeking often co-occurring with self-hitting. Integrates oral motor protocol when needed and provides communication supports so the child can request sensory input verbally.
Special Educator (SpEd)
Integrates sensory breaks into the academic schedule, trains classroom aides on material use, and transfers the home protocol to the school environment to ensure generalization across settings.
NeuroDevelopmental Pediatrician
Rules out medical causes (ear infection, headaches, dental pain) before sensory intervention begins. Monitors injury risk and coordinates with OT and BCBA on combined intervention plan.
"The brain does not organize by therapy type. Every one of these disciplines sees a different facet of the same child. This technique requires all of them — and at Pinnacle, all of them are present." — Pinnacle Blooms Consortium Clinical Philosophy
Precision Targets. Not Random Activity.
Technique A-108 is designed with a clear behavioral hierarchy — a primary target, measurable secondary outcomes, and broad tertiary benefits that ripple across all areas of your child's development.
🎯 Primary Target
Reduction of self-hitting frequency. Observable indicator: fewer self-hit episodes per hour → per session → per day. Measured via frequency count (tally) and GPT-OS® Behavioral Self-Regulation Index.
⭕ Secondary Targets
- Body awareness improvement — child begins to locate body in space without intense input
- Arousal regulation — less dysregulation during transitions and low-stimulation periods
- Self-initiation — child reaches for crash pad or putty instead of hitting
⬜ Tertiary Targets
- Improved attention and learning readiness
- Reduced anxiety and meltdown frequency
- Enhanced parent-child interaction quality
- Foundation for self-regulation skills across all domains
Behavioral Signs It's Working
What to Watch For | |
Child pauses before hitting → looks at crash pad → moves toward it | |
Hitting frequency drops from ~30x/day to ~10x/day in 2–3 weeks | |
Child requests "squeeze" or brings vest to parent independently | |
Less hitting during high-stimulation events (parties, transitions) | |
Sleep quality improves (proprioceptive regulation affects sleep onset and quality) |
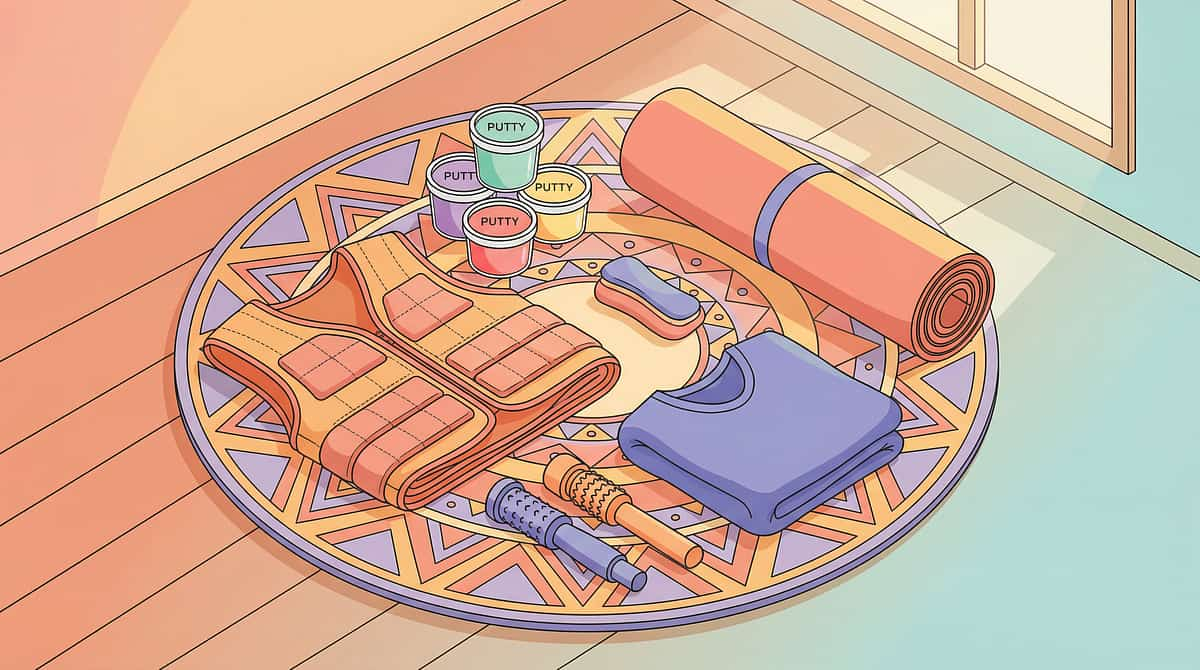
9 Materials That Replace Hitting with Healing
Each of the following materials provides the same proprioceptive signal the child is seeking — safely, scientifically, and within your home. You do not need all 9 to start. Begin with one and build your sensory toolkit over time.
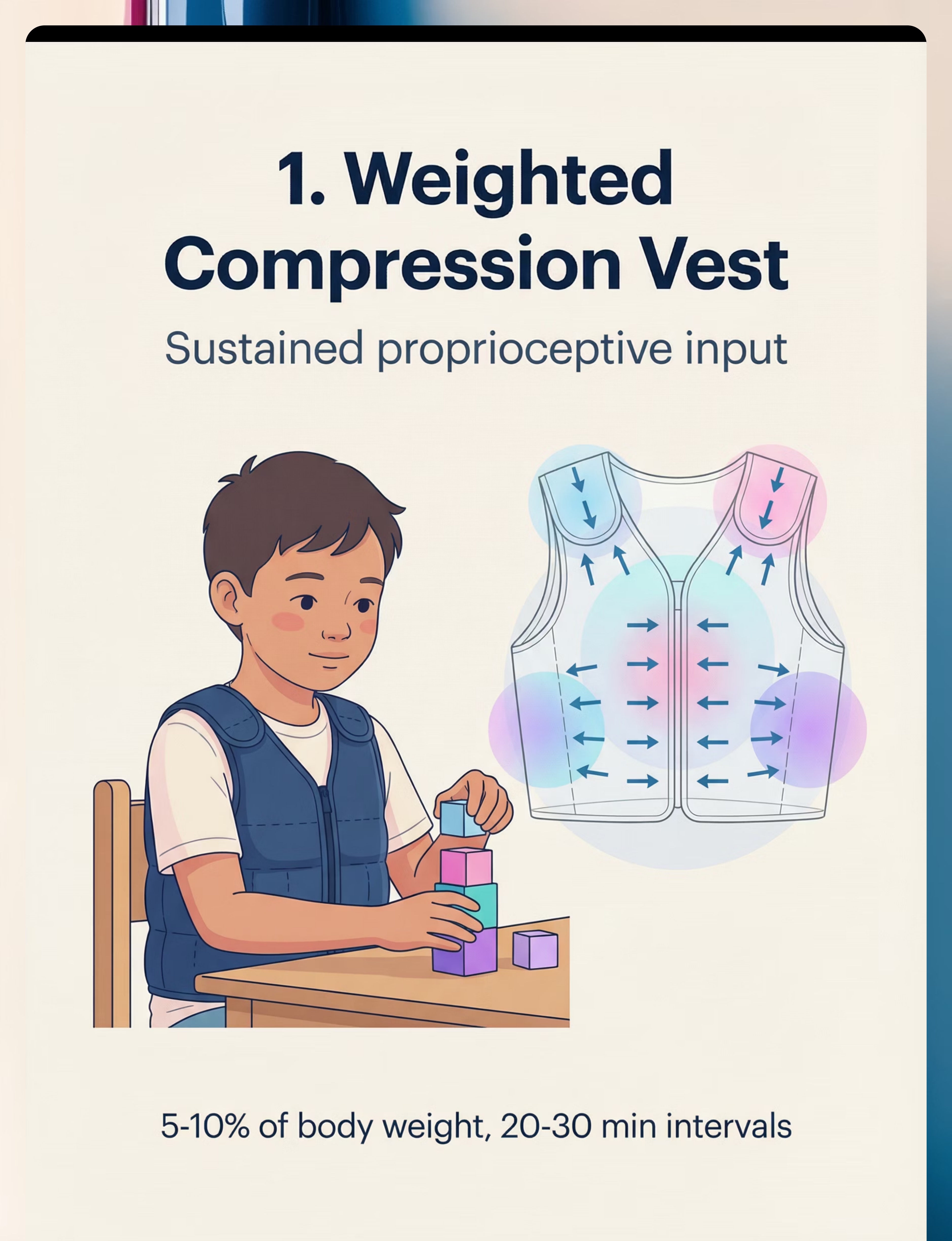
Weighted Compression Vest
🟢Sustained Proprioceptive Input
Body Sock / Lycra Resistance Tunnel
🟢Full-Body Proprioceptive Resistance
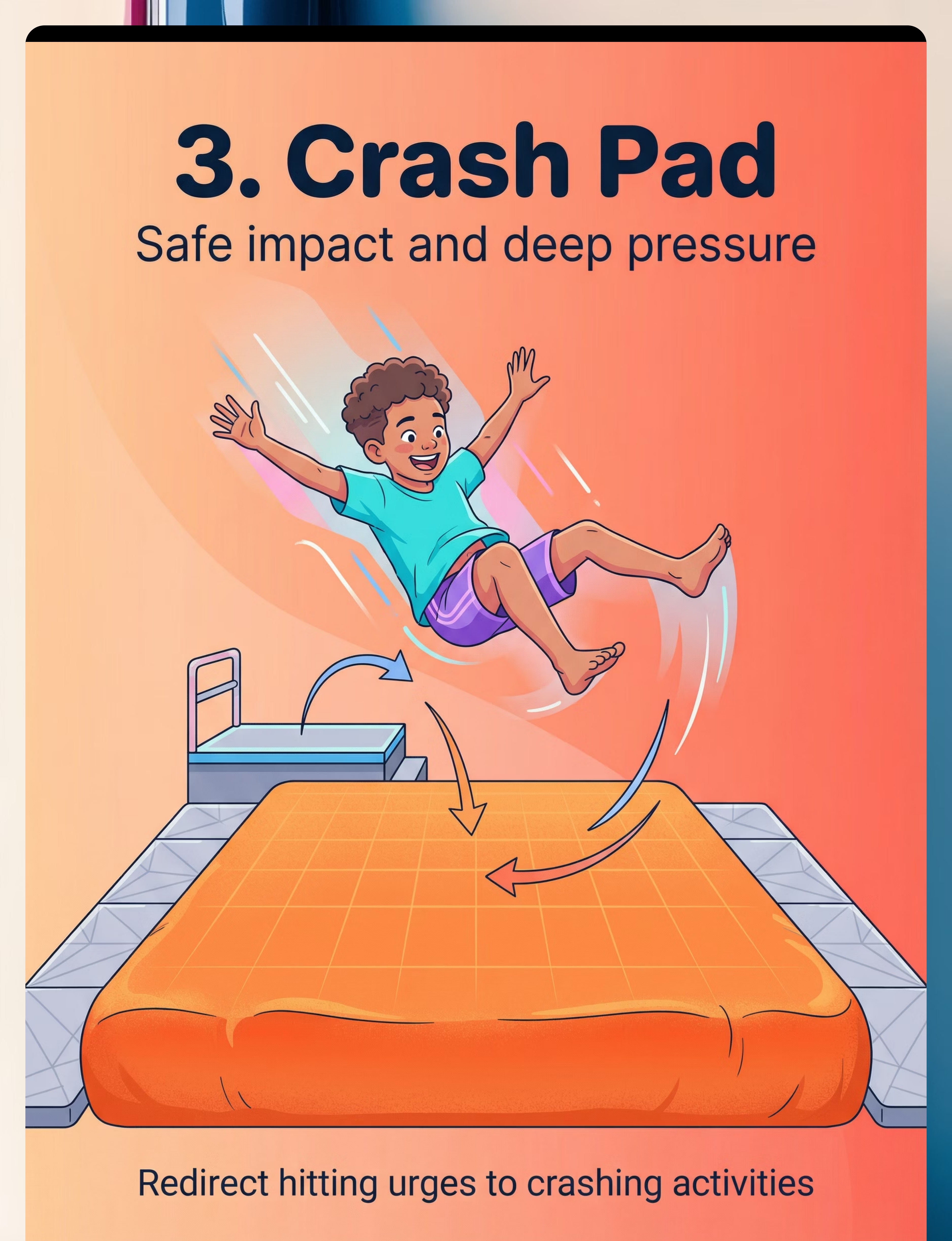
Crash Pad / Crash Mat
🟠Safe Impact and Deep Pressure
Vibrating Massage Tools
🔵High-Intensity Input Without Impact
Therapy Putty / Resistance Dough
🟡Hand-Based Heavy Work Input
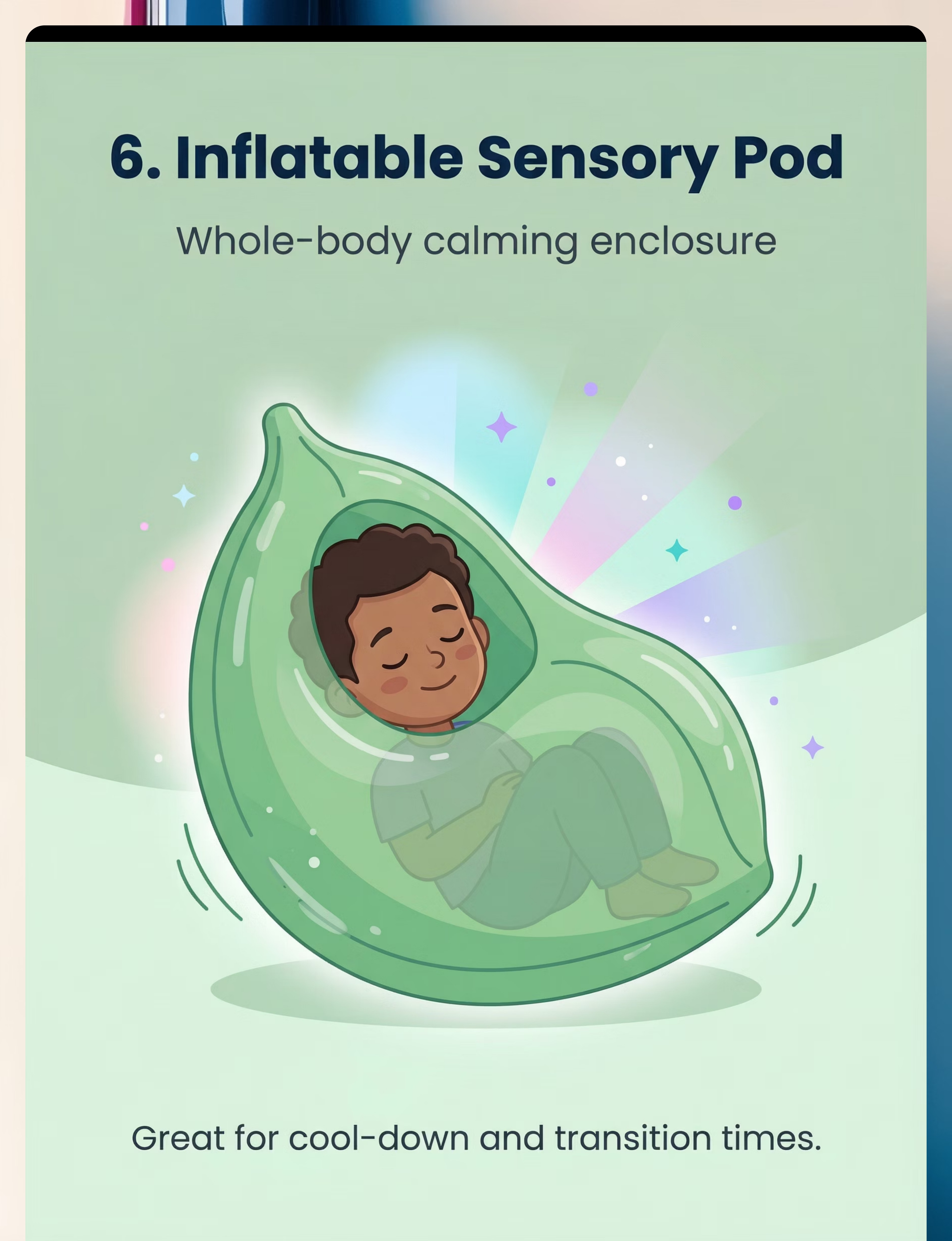
Inflatable Sensory Pod / Peapod
🟢Whole-Body Calming Enclosure
Arm and Leg Weights
🟠Continuous Movement Resistance
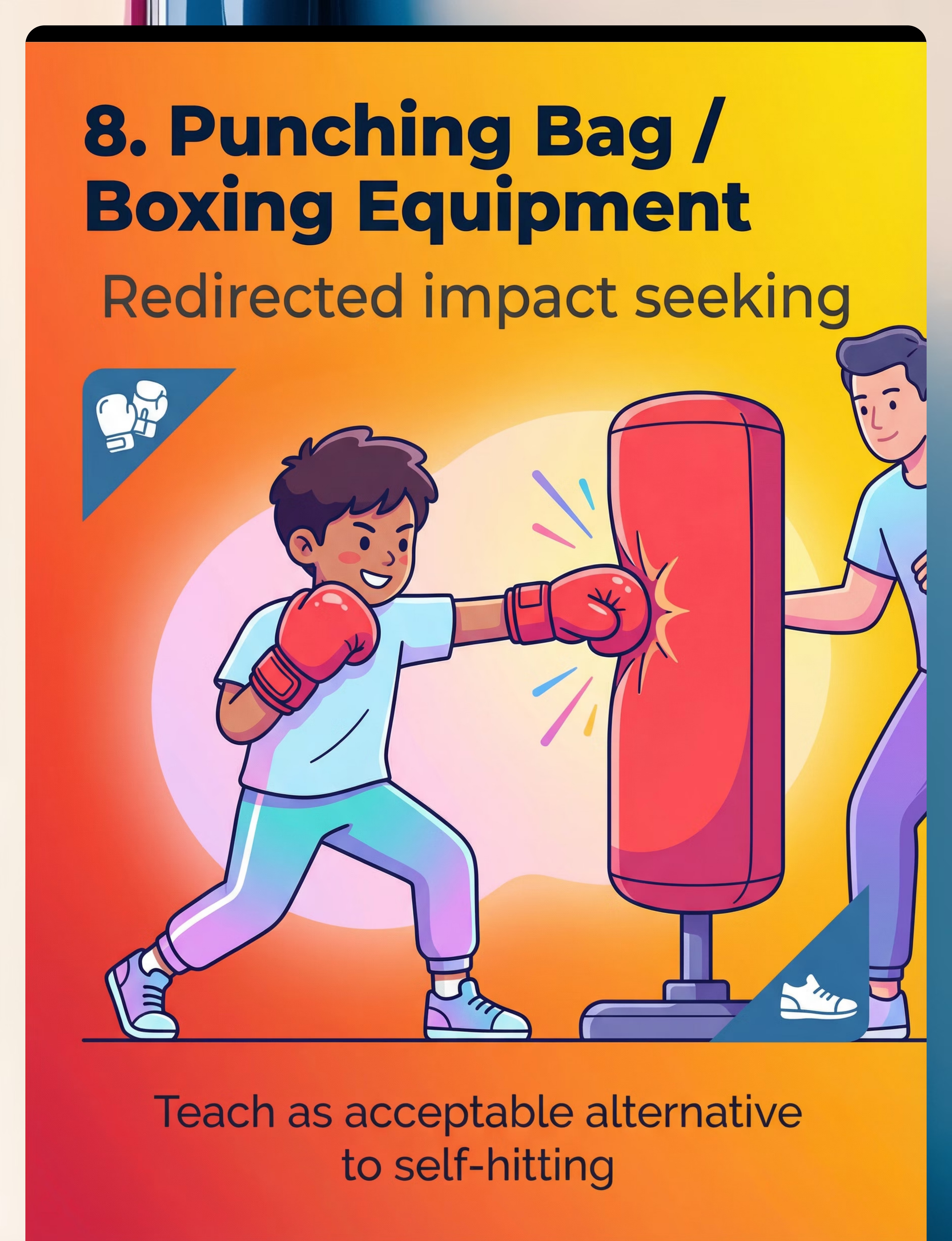
Punching Bag / Boxing Equipment
🔴Redirected Impact Seeking
Theraband Resistance Exercises
🟣Structured Heavy Work Program
Essential Starter Priority Guide
Priority | Material | Hitting Type Addressed | Price Start | |
⭐ Essential | Crash Pad | Full body impact | ₹3,000 | |
⭐ Essential | Therapy Putty | Hand/arm hitting | ₹300 | |
⭐ Essential | Weighted Vest | Constant background seeking | ₹2,500 | |
🔄 Add Week 2–3 | Body Sock | Full body resistance need | ₹1,200 | |
🔄 Add Week 2–3 | Vibrating Tools | High-intensity urgent seeking | ₹500 |

Material 1 — Weighted Compression Vest
🟢 Sustained Proprioceptive Input
OT Lead | Proprioceptive Regulation
Why It Works
Continuous deep pressure across the torso provides the constant proprioceptive feedback the nervous system craves — without any hitting. The vest essentially gives your child's body a sustained, gentle "hug" that signals body position and calms the regulatory system throughout the wear period.
This is the single most effective background-level sensory tool — it works passively throughout the day while your child goes about normal activity.
How to Use
- Duration: 20–30 min intervals with breaks — never all day
- Weight: 5–10% of child's body weight (OT calibrated)
- Best timing: Before known high-demand periods (school, transitions, mealtimes)
Where to Find It
Price range: ₹2,500–5,000
Canon Category: Weighted Equipment / Deep Pressure Tools
Material 2 — Body Sock / Lycra Resistance Tunnel
🟢 Full-Body Proprioceptive Resistance
OT Lead | Proprioceptive + Vestibular
Why It Works
Every movement inside the body sock creates resistance. The child must push, stretch, and work against the lycra fabric with their entire body — flooding the proprioceptive system with input through full-body engagement. Most children find this joyful and seek it out spontaneously after initial introduction.
Unlike the vest, the body sock requires active engagement — making it ideal for children who need movement-based input rather than passive pressure.
How to Use
- Duration: 5–15 min active play
- Supervision: Always supervised — face must remain visible at all times
- Games to try: "Butterfly wings," "cocoon to butterfly," "snake stretching"
- Safety rule: Child must always be able to exit independently
Where to Find It
Price range: ₹1,200–2,500
Canon Category: Resistance Tunnels / Body Socks

Material 3 — Crash Pad / Crash Mat
🟠 Safe Impact and Deep Pressure
OT Lead | Proprioceptive + Vestibular
Why It Works
The crash pad is the most powerful hitting-replacement material available. Jumping, crashing, and falling onto the pad provides the same intense proprioceptive input as self-hitting — distributed safely across the whole body instead of concentrated at a single impact point.
For children whose self-hitting is full-body or involves head-banging, this material provides the closest functional equivalent. Many families report the crash pad as the single most transformative material in the A-108 toolkit.
How to Use
- Duration: 5–10 min active crashing
- Space: Clear 2m radius of all hard furniture before use
- Positioning: Against wall, not in open room center
- Games: "Big crash countdown," "superhero landing," jumping challenges
Where to Find It
Price range: ₹3,000–8,000
Canon Category: Crash Pads / Impact Mats

Material 4 — Vibrating Massage Tools
🔵 High-Intensity Input Without Impact
OT Lead | Tactile + Proprioceptive
Why It Works
Handheld vibration delivers intense sensory input to large muscle groups — arms, legs, back — activating proprioceptors and tactile receptors simultaneously. The nervous system receives a strong, clear signal without any impact or force being applied.
This is particularly effective for children who seek high-intensity input urgently. The vibration tool can be deployed quickly during a seeking episode as an immediate redirect — no setup required.
How to Use
- Duration: 3–5 min per muscle group
- Application: Arms, legs, shoulders — avoid face and head
- Timing: Most effective during or immediately after a seeking episode
- Note: Some children find vibration aversive initially — introduce gradually
Where to Find It
Price range: ₹500–2,000
Canon Category: Vibration Tools / Sensory Massagers

Material 5 — Therapy Putty / Resistance Dough
🟡 Hand-Based Heavy Work Input
OT Lead | Proprioceptive — Hand/Finger
Why It Works
Squeezing, pounding, and pulling therapy putty delivers intense proprioceptive input to the hands and arms. For children whose self-hitting is concentrated in hand and arm areas, this is the most targeted replacement available.
Putty is portable, quiet, and socially unobtrusive — making it the most versatile material in the toolkit. It can be used anywhere: in the car, at a restaurant, at school, in a waiting room. It is the recommended Essential Starter for families just beginning.
How to Use
- Duration: 5–10 min | Any time, any location
- Resistance: Match to child's hand strength — start softer, progress to firmer
- Activities: Squeeze, pound, pull, roll, pinch, make shapes
- Tip: Work putty alongside child — parallel engagement builds acceptance
Where to Find It
Price range: ₹300–800
Canon Category: Putty / Resistive Hand Tools

Material 6 — Inflatable Sensory Pod / Peapod
🟢 Whole-Body Calming Enclosure
OT Lead | Proprioceptive + Vestibular + Tactile
Why It Works
The sensory pod creates a cocoon of gentle, sustained pressure around the entire body — enveloping the child's nervous system in a safe, proprioceptively rich environment. Unlike active tools such as the crash pad, the pod provides calming input without any demands on the child.
It is especially effective for cool-down and transition times — precisely the moments when hitting risk is highest. Many families keep the pod in a quiet corner as a permanent "regulation station."
How to Use
- Best timing: Cool-down periods, transition support, post-meltdown recovery
- Duration: 10–20 min
- Enhancement: Add soft music, dim lighting, or a preferred calm toy inside
- Setup: Designate a permanent corner — reduces transition resistance
Where to Find It
Price range: ₹4,000–10,000
Canon Category: Sensory Pods / Enclosure Devices

Material 7 — Arm and Leg Weights
🟠 Continuous Movement Resistance
OT Lead | Proprioceptive — Full Body
Why It Works
Wearable weights add resistance to every movement throughout the day, providing continuous proprioceptive input with zero additional effort from the parent or child. Every step, reach, and gesture becomes a small proprioceptive dose — creating a passive sensory diet that reduces the overall seeking drive that leads to self-hitting.
This is the most "invisible" material in the toolkit — it works in the background while the child attends school, plays, and goes about daily life normally.
How to Use
- Duration: Waking hours in 30-min blocks — alternate with breaks
- Starting weight: 0.5 lb — increase gradually under OT guidance only
- Placement: Wrists and/or ankles depending on where hitting is concentrated
- Contraindication: Do not use with joint hypermobility without OT clearance
Where to Find It
Price range: ₹600–1,500
Canon Category: Weighted Wearables / Resistance Accessories
Material 8 — Punching Bag / Boxing Equipment
🔴 Redirected Impact Seeking
ABA/BCBA Lead | Behavioral Replacement
Why It Works
The punching bag is the most direct hitting replacement available: the same movement, the same impact sensation, the same proprioceptive payoff — directed at an appropriate target. The nervous system receives exactly what it is seeking, with no injury risk to the child.
This material is BCBA-led because it requires explicit rule-setting and behavioral protocol — the child must learn that the bag is the target, not their own body or others. When implemented correctly, this material can produce the fastest frequency reduction of any tool in the toolkit.
How to Use
- Always use with boxing gloves — never bare hands
- Adult supervision required at all times
- Rules first: Establish clear target rules before first session
- Script: "Hitting goes on the bag. The bag is for hitting."
- BCBA coordination: Pair with replacement behavior protocol
Where to Find It
Price range: ₹1,500–4,000
Canon Category: Impact Redirection Equipment

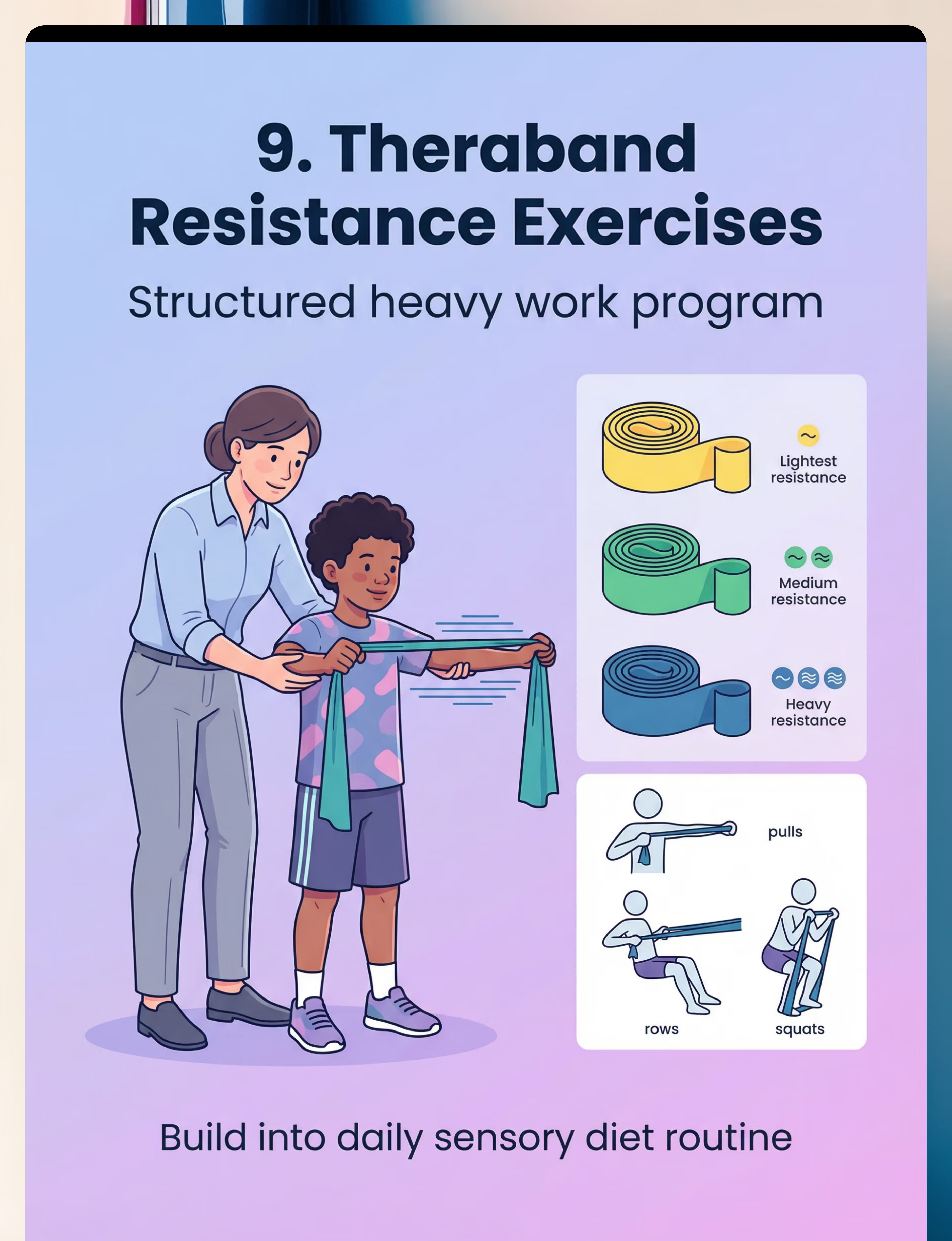
Material 9 — Theraband Resistance Exercises
🟣 Structured Heavy Work Program
OT Lead | Proprioceptive — Muscle/Joint
Why It Works
Pulls, rows, and squats with resistance bands deliver sustained, controlled proprioceptive input to muscles and joints across the entire body. Unlike passive tools, theraband exercises build active body awareness — the child learns where their body is, how much force they can produce, and how to regulate that force.
This material is ideal for older children (5+) who can follow simple exercise instructions and benefits most those whose self-hitting is driven by a need for deep muscle activation.
How to Use
- Frequency: 2–3x daily | 5–10 reps per exercise
- Exercises: Seated row, overhead pull, standing squat, arm curl
- Integration: Build into morning and pre-transition sensory diet
- Resistance: Start lightest band — increase over weeks, not days
Where to Find It
Price range: ₹300–700
Canon Category: Resistance Bands / Heavy Work Equipment

Every Material Has a ₹0 Version. Therapy Should Never Be a Privilege.
WHO/UNICEF Equity Principle: The child in a rural home deserves the same sensory support as the child near a clinic. Every single material in A-108 can be approximated with household items at zero or minimal cost.
🛒 Buy This | 🏠 Make This (₹0–50) | |
Weighted Compression Vest | Snug-fitting old T-shirt + rice bags in pockets (2 bags × 200g each). Pin pockets shut. Total weight ≈ 5–8% body weight. | |
Body Sock | Large pillowcase with a head hole cut in the closed end. Let child push in. Supervise. MUST allow face visibility. | |
Crash Pad | Stuff 3–4 old quilts/mattresses into a large bedsheet. Stitch edges. Minimum 6-inch thickness. Test with your own body first. | |
Vibrating Tools | Electric toothbrush handle (brush head removed) provides gentle vibration to arms/legs. Or: massage cushion from any pharmacy. | |
Therapy Putty | 2 cups flour + 1 cup salt + 2 tbsp cream of tartar + 2 cups boiling water + 2 tbsp oil. Knead until dough forms. Firmer = more flour. | |
Sensory Pod | Line a large laundry basket or cardboard box with cushions on all 4 sides + a blanket at the bottom. Child sits inside cocooned by pillows. | |
Arm/Leg Weights | Fill tube socks with dry rice (200–400g). Knot securely. Wrap around wrists/ankles with velcro strips from old shoes. | |
Punching Bag | Hang a large bed pillow from a door frame hook in an old pillowcase. Reinforce with a second pillowcase. Add kitchen oven mitts. | |
Theraband | Long strips of stretchy fabric cut from old T-shirts (inter-lock ribs stretch best). Tie ends for hand grips. Test snap resistance before use. |
⚠️When clinical-grade is non-negotiable: If your child's self-hitting causes bruising, swelling, or open wounds, DIY materials are insufficient. A clinical-grade weighted vest calibrated by an OT is required. Contact helpline: 9100 181 181

Read This Before You Touch Any Material.
This card is not optional. It takes 2 minutes. It protects your child.
🔴 RED — Absolute Contraindications
Do NOT proceed if ANY apply:
- Child has current injuries, bruises, or open wounds from self-hitting
- Child has been diagnosed with joint hypermobility syndrome without OT clearance
- Self-hitting includes head-banging against hard surfaces that has caused swelling
- Child has respiratory or cardiac conditions (for weighted vest use)
- Child cannot understand basic safety instructions (for punching bag)
- Onset of self-hitting is SUDDEN and NEW (may indicate pain — see a doctor first)
🟠 AMBER — Modify and Monitor
Proceed with caution if any apply:
- History of claustrophobia (avoid body sock and pod without gradual introduction)
- Child is under 2 years old (lightest materials only, very brief sessions)
- History of sensory aversion (test one material at a time)
- Child is ill, overtired, or recently experienced a meltdown
- Child has never used these materials before (see introduction protocol)
🟢 GREEN — Safe to Proceed When:
- Child is calm, fed, rested, and in a regulated state
- Space is clear of hazards (2m radius around crash pad)
- Parent has read all 9 material safety notes
- OT has recommended these materials (or helpline has been contacted)
- You have a cool-down plan ready
🛑Stop immediately if: Child becomes severely distressed | Skin redness or marks from wearable items | Child uses materials to target others | Self-hitting INCREASES after using materials (seek FBA immediately)
Emergency Action: Call 9100 181 181 | Available 24x7 | 16 languages
Emergency Action: Call 9100 181 181 | Available 24x7 | 16 languages

Your Home Is About to Become a Sensory Gym.
Spatial precision prevents 80% of session failures. Set the stage before the session begins — an environment that is safe, calm, and purposefully arranged makes the difference between a successful session and a dysregulated one.
Child's Zone
Clear 2m circle. Non-slip mat on floor. This is where the session centers — unobstructed and safe.
Parent Position
Behind and beside — never blocking the exit. Your child needs to feel free, not cornered.
Crash Pad
Against wall, minimum 2m from any furniture. Test the clearance yourself before the session.
Materials Station
Low table or floor tray. Child must be able to reach independently — this builds self-initiation.
Cool-Down Corner
Sensory pod or cushion nest — semi-enclosed, dimly lit. Permanent setup is ideal.
Remove From Space
- Hard furniture with sharp corners within crash zone
- Screens/devices (distraction that prevents sensory engagement)
- Other children during initial sessions (reduce variables)
- Loud appliances running (washing machine, mixer)
Environment Settings
- 💡Lighting: Dim or natural — avoid harsh fluorescent
- 🔊Sound: Low music or white noise optional | No sudden loud sounds
- 🌡️Temperature: Comfortable — not hot (overheating increases dysregulation)

Is Your Child Ready? — 60-Second Readiness Check
Sixty seconds before every session determines the entire session outcome. This readiness check is not a formality — it is clinical judgment that your occupational therapist would make before every session in a clinic. You are now doing the same.
Check | 🟢 Go | 🟠 Modify | 🔴 Postpone | |
🍽️ Fed in last 2 hours? | Yes | More than 3 hrs ago | Not eaten today | |
😴 Rested? | Yes, slept well | Mild fatigue | Sleep-deprived | |
😐 Regulated state? | Calm/alert | Slightly activated | Dysregulated/distressed | |
🤒 Unwell signs? | None | Mild cold | Fever/ill | |
📅 Recent meltdown? | More than 2 hrs ago | 1–2 hrs ago | Less than 1 hr ago | |
💊 Medications due? | Already given | Not due | Overdue |
🟢 All Green → Full Session
Proceed to the invitation. Begin with the plan. Trust the protocol.
🟠 2+ Ambers → Modified Session
Choose ONE material only (therapy putty recommended). Reduce session to 5 minutes. Drop expectations. Presence is enough.
🔴 Any Red → Postpone
Provide a calming activity: sensory pod, soft music, heavy blanket. No protocol today. Rest is therapeutic.
"The best session is one that starts right. A postponed session is not a failure — it's clinical judgment. Your OT would make the same call."

Step 1 — The Invitation
Step 01
Timing: 30–60 seconds
What to Say
"Hey — want to do something fun with me? I have something super cool to show you."(Hold up the crash pad OR the putty — whichever the child tends to reach for)"Look, it's squishy/bouncy/stretchy! Want to try?"(Let child see and touch before any demand)
Body Language That Works
- Get to the child's physical level — kneel or sit on the floor
- Turn your body at a slight angle — not full-on facing (less confrontational)
- Smile, but don't over-animate if child is sensitive to facial expression
- Hold the material where child can see it, 30–60cm away
Reading the Response
- ✅Acceptance: Looks at material | Reaches toward it | Moves toward space | Positive vocalization
- ⚠️Turns away: Wait 10 seconds, try once more. If still no, postpone.
- ⚠️Runs to material immediately: That's acceptance — follow, don't catch.
- ⚠️Self-hitting at this moment: Calmly offer the material: "You can hit this instead."

Step 2 — The Engagement
Step 02
Timing: 1–3 minutes
Once the child engages with the material, your job is to deepen the interaction without adding demands. Parallel engagement — working the material alongside the child — is far more effective than directive instruction at this stage.
Crash Pad Script
"Can we do a BIG jump? Ready... 3... 2... 1... CRASH!"
Jump yourself first to model. Child joins when ready.
Jump yourself first to model. Child joins when ready.
Therapy Putty Script
"Let's make it into a snake! Squeeze it! Pull it! Make it flat!"
Work putty alongside child — parallel engagement before cooperative.
Work putty alongside child — parallel engagement before cooperative.
Body Sock Script
"You're a butterfly! Can you stretch your wings out wide?"
Keep face visible. Stay beside child throughout.
Keep face visible. Stay beside child throughout.
Weighted Vest Script
"This is your superhero vest! Let's put it on — it helps your body feel strong."
Child participates in putting it on — increases buy-in.
Child participates in putting it on — increases buy-in.
Reinforcement Timing: Praise IMMEDIATELY when child makes contact with material. "Yes! You did it! That's awesome!" — Timing matters more than magnitude. Within 3 seconds. Every time.

Step 3 — The Therapeutic Action
Step 03
Timing: 5–10 minutes
You are not doing therapy TO the child. You are creating the conditions for them to experience the sensation they need — safely.
Level | Material | Input Type | Duration | |
1 (Lowest) | Therapy Putty | Hand proprioception | 5–10 min | |
2 | Weighted Vest | Torso deep pressure | 20–30 min | |
3 | Body Sock | Full-body resistance | 5–15 min | |
4 | Vibration Tools | High-intensity tactile + proprioceptive | 3–5 min | |
5 (Highest) | Crash Pad | Full-body impact | 5–10 min |
Follow the child's lead on intensity — never force deeper input
If the child retreats from a higher-level material, return to a lower level. Comfort precedes intensity.
If child self-hits during material use, redirect calmly
"You can hit the crash pad!" — steady voice, offer the material, no punishment.
Watch for regulation signals
Relaxed jaw, slower breathing, reduced stimming, increased eye contact — these confirm the nervous system is regulating. Do not interrupt.
Do not narrate excessively
Let the sensory input do the work. Silence is therapeutic. Language can be overstimulating during heavy proprioceptive work.

Step 4 — Repeat and Vary
Step 04
Timing: 3–5 additional minutes
Material | Reps / Duration | Satiation Signal | |
Crash Pad | 8–12 jumps/crashes | Child walks away, lies flat, loses interest | |
Therapy Putty | 5–7 min continuous | Hands relax, child sets it down voluntarily | |
Body Sock | 3–5 min active movement | Child stops stretching, becomes still | |
Weighted Vest | 20–30 min wear | N/A — continuous input, not rep-based | |
Vibration Tools | 3–5 min per muscle group | Child pulls away or requests stop |
The 3 > 10 Rule: "3 good, fully-engaged repetitions of therapeutic input are worth more than 10 forced, distress-adjacent repetitions." Quality of neurological response, not quantity of execution.
Variation Strategies to Maintain Engagement
Change Material
Putty → crash pad → body sock — within one session if the child tolerates transitions well.
Change Position
Standing → lying → sitting. Proprioceptive input changes character with body orientation.
Change Social Context
Child alone → parallel with parent → cooperative. Gradual social layering maintains novelty.
Add a Game Layer
Crash pad competition, putty sculptures, body sock animal games. Playfulness sustains engagement better than any other variable.
Step 5 — Reinforce and Celebrate
Step 05
Timing: Throughout session — immediate delivery
The Timing Law: Within 3 seconds of desired behavior. Every time. Without exception. Brain plasticity is time-sensitive. A 4-second delay halves reinforcement effectiveness.
Reinforcement Scripts — Use Varied
"YES! You used the crash pad! I love that!"
"You did it! That was SO strong!"
"Your body asked for input and you gave it the safe way. That's HUGE."
[Non-verbal: thumbs up + eye contact + big smile — for children who prefer less verbalization]
Type | Example | Notes | |
Social | High-five, hug, thumbs up, specific verbal praise | Most sustainable long-term | |
Token | Sticker on chart after each material use | ||
Activity | 5 min preferred activity immediately after | Must be immediate and brief | |
Tangible | Small preferred item from Reward Jar | Use sparingly, phase out over time |
"Celebrate the ATTEMPT, not just the success. If the child reached toward the crash pad instead of hitting themselves — that is a neurological milestone. Treat it like one."

Step 6 — The Cool-Down
Step 06
Timing: 2–3 minutes
Abrupt ending = nervous system dysregulation. The child's arousal is elevated from proprioceptive input. A structured cool-down transitions safely back to baseline and prevents post-session self-hitting spikes. This step is non-negotiable.
2-Minute Warning
"Two more crashes/squeezes/stretches, then we're all done." (Hold up 2 fingers — visual support)
Final Rep
"One more — make it a big one!" Give the final rep extra energy — ending on a high creates positive closure.
Cool-Down Sequence
Choose one: Sensory pod (2–3 min) | Heavy blanket wrap (2 min) | Joint compressions ×10 (OT guidance first) | Preferred calming toy (2–3 min)
Material Put-Away Ritual
"Okay, crash pad is going to sleep now. Let's give it a pat and say goodnight." Child participation in put-away teaches transition routine.

60 Seconds of Data Now Saves Weeks of Guessing Later.
When self-hitting frequency drops from 30 episodes per day to 15, then 10, then 5 — you are watching neuroplasticity happen in real time. The data is not bureaucracy. It is proof that your work is working.
Data Point | What to Count | How to Record | |
Self-hitting episodes | How many times did child hit themselves today (all day)? | Tally (IIII) | |
Material use | Which material(s) did child use today? | Circle: Vest / Sock / Crash / Vibration / Putty / Pod / Weights / Bag / Bands | |
Regulation rating | How regulated was child after session? | Scale: 1 (very dysregulated) → 5 (calm/happy) |
GPT-OS® Integration
If you're using GPT-OS®, record this data in your child's profile under: Behavioral Self-Regulation Index → Sensory Regulation Strategies → A-108 Proprioceptive Substitution.
The system automatically adjusts protocol recommendations, flags regression risk in a 7-day window, and benchmarks your child against similar profiles across the Pinnacle network.
One Consistent Rule
Record data immediately after the session — before you move on to anything else. Memory of frequency counts fades within 20 minutes. Three data points. Sixty seconds. Every day.
No Two Children Are Identical. Here Is How to Make This Technique Yours.
A-108 is a framework, not a script. The child's profile, age, sensory history, and communication level all determine how the protocol is shaped. Use this guide to calibrate the technique to your specific child.
Easier Version
Therapy putty only | Sitting at table | 5 minutes | No demands — just play alongside child with own putty | Reinforcement: smile only
Standard Version
2–3 materials in sequence | Standing/floor | 15–20 minutes | Full protocol: invitation → engagement → action → reinforce → cool-down | Data recording immediately after
Advanced Version
All 9 materials available | Child self-selects | Sessions in different environments | Child puts own materials away and records data symbol
Child Profile | Adaptation | |
Sensory Seeker (Under-responsive) | Higher intensity: crash pad first, longer sessions, resistance exercises | |
Sensory Avoider | Start with least aversive material only. Minimal touch. Follow child's distance. | |
Mixed Profile | Test each material individually. Map child's preference hierarchy before combining. | |
Non-verbal child | Use visual schedule showing material sequence. Picture-based choice board for selection. | |
Verbal child | Teach child to say/sign "I need crash pad" or "squeeze please" as replacement behavior. | |
2–4 years | Shorter sessions (5–8 min), more child-led, simpler materials, constant supervision | |
5–7 years | Introduce choice-making, social story for why materials help, star chart | |
8–10 years | Self-monitoring checklist, child logs own data, builds self-advocacy skills |
Weeks 1–2: The Brain Is Listening. Even If It Doesn't Show Yet.
Progress Bar: 15%
Tolerance Building Phase
✅ Real Progress in Weeks 1–2
- Child tolerates crash pad for 3 seconds more than last week
- Self-hitting frequency drops even slightly (30 → 25/day)
- Child's body appears calmer for 5–10 min post-session
- Child recognizes material when shown
- Parent feels more confident in one material
❌ NOT Progress Yet — and That Is Normal
- Child independently seeks material without prompting
- Self-hitting stops entirely
- Child uses material at school or in public
- Child can explain why they need input
- All 9 materials are accepted
"If your child tolerates the crash pad for 3 seconds longer than last week — you have just witnessed their nervous system beginning to learn a new language. That is extraordinary."
Session Frequency Guidance — Weeks 1–2
Week 1: 1 Session/Day
Any material — introduce and allow exploration. No performance expectations. Just familiarity.
Week 2: 1–2 Sessions/Day
Begin structured protocol (Steps 1–6). Consistency matters more than duration: 10 minutes every day beats 60 minutes once a week.
Weeks 3–4: The Neural Pathway Is Forming. Watch for These Signs.
Progress Bar: 40%
Consolidation Phase
Around weeks 3–4, the investment you've made in daily sessions begins to show up as observable, measurable neurological change. These consolidation indicators are your milestones — each one represents a neural pathway strengthening in real time.
Anticipation
Child moves toward the material when session begins — without prompting. The nervous system is beginning to associate the material with relief.
Preference Emerges
Child has a favorite material they reach for first. This is critical information — it tells you which sensory channel is most efficient for this child.
Hitting Changes Character
Shorter episodes, less intensity, faster recovery. The hitting itself tells you regulation is improving — even if frequency hasn't dropped dramatically yet.
Generalization Seeds
Child squeezes own hands, seeks parent bear hug, presses against wall — approximations of material behavior emerging spontaneously.
"Around week 3–4, most parents notice they're more confident too. They've stopped dreading sessions. They can read their child's signals. That change in you is clinically significant — parental self-efficacy is the strongest predictor of intervention continuation."

Weeks 5–8: Mastery Emerging.
Progress Bar: 75%
🏅 Proprioceptive Self-Regulation — Level 1
The mastery phase is marked by independence. Where the child once needed prompting, guidance, and structure, they now show spontaneous, self-directed use of materials. These are the milestones that confirm the neural pathway is stable.
50% Frequency Reduction
Self-hitting reduced ≥50% from baseline, sustained across 2+ consecutive weeks without protocol changes.
Independent Initiation
Child approaches 1+ material without prompting in at least 3 sessions — the most powerful mastery indicator.
Generalization
Material use observed in a second environment — school, grandparent's home, car. Behavior is no longer context-dependent.
Parent Independence
Parent implements full protocol independently with fewer than 2 issues per week. You have become the expert on your child's sensory system.
Maintenance Check: Remove one material from the rotation for one week. If self-hitting baseline holds → generalization is stable, move to Level 2. If baseline returns → restore full protocol for 2 more weeks before testing again.
🌸 You Did This.
You read the science when you were exhausted. You set up the crash pad when you'd rather have sat down. You tried therapy putty for the 14th time when the first 13 didn't work. You logged the data on the day everything felt impossible.
Your child hit themselves 30 times a day. Now it's fewer. That is a neural pathway you built — session by session, repetition by repetition.
This is not a small thing. This is therapeutic infrastructure, built inside your home, by you.
✅ 9 Materials Introduced
Tested and calibrated to your child's specific sensory profile.
✅ Full Protocol Mastered
All 6 steps — invitation through cool-down — implemented with consistency and confidence.
✅ Sensory Diet Integrated
Sessions are now part of daily rhythm, not an interruption to it.
✅ Self-Hitting Reduced
Frequency documented, trajectory confirmed, and safe alternatives observed in use.
Journal Prompt: "What did I notice about my child this week that I couldn't have noticed 8 weeks ago?"

You Are Not Done. You Are On a Journey. Here Is the Map.
Technique A-108 is not the destination — it is the foundation. Every skill your child builds here unlocks the next level of the sensory regulation journey. Use this progression map to plan what comes next.
Child's Response to A-108 | Recommended Next Step | |
Crash pad is the most preferred material | A-115: Heavy Work Program (advanced crash-pad expansion) | |
Oral seeking also present alongside hitting | A-109: Child Chews Everything (parallel track) | |
Regulation broadly improved but meltdowns persist | A-103: Calming Strategies for Regulation | |
Ready for integrated sensory diet | A-122: Building a Sensory Diet (master technique) |
Long-Term Developmental Goal: The child's journey from being regulated by materials → to using materials when prompted → to self-selecting materials without prompting → to regulating without materials in natural environments.

Real Families. Real Journeys. Real Change.
Hyderabad, 2023 — Arjun, Age 4
Before: Arjun was hitting his head 40–50 times per day. His parents had tried holding his hands, saying "no," timeouts — nothing reduced frequency. At school, aides were calling parents daily. Father was researching helmets.
After (Week 6): The crash pad changed everything. Week 1, Arjun refused it. Week 2, he stood near it during episodes. Week 3, he jumped onto it after a 5-second redirect. By week 6, he was going to the crash pad before hitting in 60% of episodes.
"The crash pad looked absurd in our living room. I didn't care. My son stopped bleeding."
Therapist's Note (OT): Arjun's sensory diet was expanded in Week 7 to include a weighted vest for mornings. Self-hitting dropped to 3–5 episodes per day by Week 10 — a 90% reduction from baseline.
Chennai, 2024 — Priya, Age 6
Before: Priya hit her thighs constantly during school transitions, car rides, and meals. Three months of behavioral intervention without sensory tools had zero impact. BCBA FBA confirmed proprioceptive function.
After: Therapy putty during car rides + body sock sessions 3x daily. Within 4 weeks, thigh-hitting during meals dropped to near zero.
"She was starving for input and we kept trying to stop the behavior instead of feeding the need."
Therapist's Note (BCBA + OT): FBA-confirmed proprioceptive function required OT-lead sensory intervention, not behavioral extinction. The combined BCBA + OT approach via FusionModule™ protocol was decisive.
Vignettes represent composite cases from the Pinnacle Blooms Network. Names changed. Individual results vary. Outcomes dependent on frequency of implementation, child profile, and professional guidance.
Home + Clinic = Maximum Impact
Your home protocol is most powerful when backed by professional guidance. The combination of daily home sessions with regular clinical oversight produces outcomes that neither approach achieves alone.
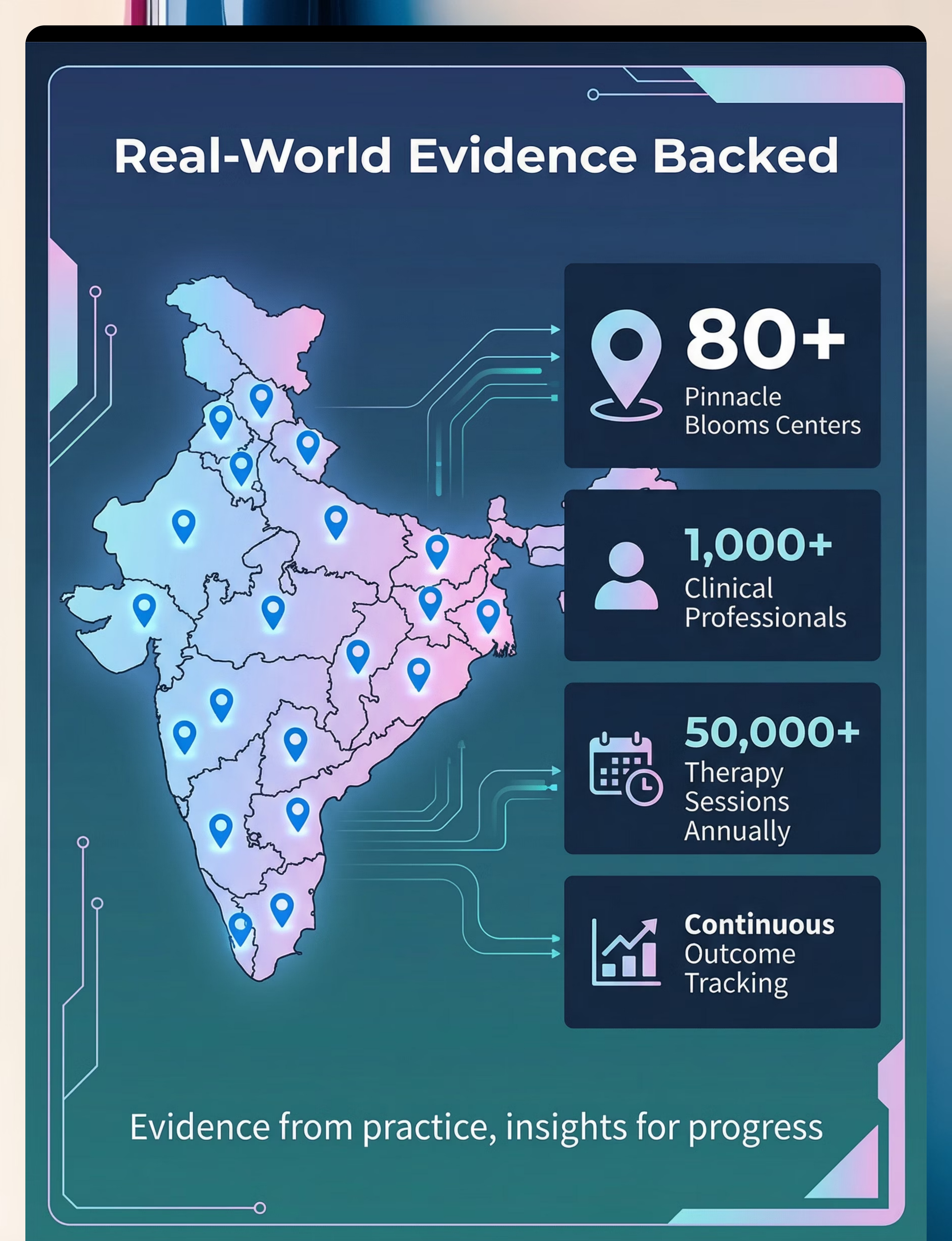
🏥 Nearest Pinnacle Center
70+ centers across India. OT, ABA, SLP, SpEd, NeuroDev under one roof. Services relevant to A-108: Sensory Integration Therapy • Functional Behavior Assessment • AbilityScore® Assessment.
→ Find nearest center
→ Find nearest center
📱 Teleconsultation
30-minute session with a Pinnacle OT or BCBA. Specifically for A-108: session review, sensory diet design, and FBA clarification from the comfort of your home.
→ Book at pinnacleblooms.org/teleconsult
→ Book at pinnacleblooms.org/teleconsult
📞 FREE National Autism Helpline
9100 181 181 | 16 languages | 24x7 | FREE. For first guidance on this technique, urgent red flags, or locating your nearest center — this number is always available.
💡Insurance/Funding: Many private health insurance policies in India now cover OT and behavioral therapy for autism. → Insurance navigation guide at pinnacleblooms.org/insurance
One Parent Learning A-108 Is Good. Five Caregivers Knowing It Is Transformative.
Generalization — the single most important predictor of long-term success — only happens when every adult in your child's life understands why these materials exist and how to use them. Share this page with your family, your child's school, and any caregiver who spends regular time with your child.
"Explain to Grandparents" Script
"Your grandchild's brain needs strong physical input to feel comfortable. They are not being naughty. They are not in pain. These objects — the putty, the crash mat — give their brain what it's asking for. When you see them hitting themselves, please show them one of these objects instead. It works. The doctors recommended it."
Teacher / School Communication Template
"Dear [Teacher's name], [Child] is currently implementing a proprioceptive sensory diet at home under OT guidance for sensory-seeking self-hitting. The materials used are crash pad, therapy putty, and weighted vest. Would it be possible to allow [Child] access to putty during difficult transitions? I can provide the OT's contact if helpful."
Share This Page

You've Read the Science. You've Seen the Materials. You Have Everything You Need to Begin.
Your child's nervous system is ready. Are you?
🚀 Start This Technique Today
Guided session with real-time data capture. Free for registered families. GPT-OS® walks you through every step of the protocol in real time.
📅 Book a Consultation
OT or BCBA. 30 minutes. Technique-specific guidance for your child's specific sensory profile and hitting function.
→ Explore the Next Technique
A-109: Child Chews Everything for Input — the next most common proprioceptive seeking behavior, and the next step in the Sensory Solutions Series.
📞FREE National Autism Helpline: 9100 181 181 — 24x7 | 16 Languages | No appointment needed | Completely free
Preview of 9 materials that help when child hits self for input Therapy Material
Below is a visual preview of 9 materials that help when child hits self for input therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.









Link copied!

The Pinnacle Promise
🌸 Pinnacle Blooms Network®
Global Pediatric Therapeutic Operating System
"From fear to mastery. One technique at a time."
Technique Completion
✅ Technique A-108 | Sensory Solutions Series | Domain A: Proprioceptive
Part of 70,000+ intervention techniques | techniques.pinnacleblooms.org
Part of 70,000+ intervention techniques | techniques.pinnacleblooms.org
Navigate the Series
- ← Previous:A-107: Teeth Grinding Alternatives
- 🏠Domain Home:All Domain A: Sensory Techniques
Contact and Support
- 📞9100 181 181 | Free National Autism Helpline | 24x7 | 16 Languages
Consortium
OT ● SLP ● ABA/BCBA ● SpEd ● NeuroDev Pediatrics ● CRO ● WHO-Aligned ● UNICEF-Aligned
This page is for educational and informational purposes only. It does not constitute medical advice, diagnosis, or treatment. Self-hitting behavior requires professional assessment to determine function and appropriate intervention. Every child's needs are unique — consult qualified healthcare professionals including occupational therapists and behavior analysts before implementing any strategies. Individual results may vary.
CIN: U74999TG2016PTC113063 | DPIIT: DIPP8651 (Govt. of India) | MSME: Udyog Aadhaar TS20F0009606 | GSTIN: 36AAGCB9722P1Z2
© 2025 Pinnacle Blooms Network®, a unit of Bharath Healthcare Laboratories Pvt. Ltd. All rights reserved. GPT-OS®, AbilityScore®, TherapeuticAI®, FusionModule™, EverydayTherapyProgramme™ are proprietary systems of Bharath Healthcare Laboratories Pvt. Ltd. Patents filed across 160+ countries.