
She Reaches for Her Cup — and Knocks It Off the Table. Again.
He walks into the same doorframe he's passed a hundred times. You've watched them trip, crash, and apologize — and you still don't know why. Poor Body Awareness — your child isn't being careless. Their brain is working without a complete map of where their body is.
A-109: Poor Body Awareness
Sensory Solutions — Episode 109

ACT I: UNDERSTAND
80% of Children With Autism Experience This. Your Child Is Among Millions.
80%
Sensory Processing Difficulties
of children with autism display sensory processing difficulties including proprioception
1 in 36
Worldwide ASD Diagnosis
children worldwide diagnosed with autism spectrum disorder (CDC, 2023)
72M+
Children in India
children in India under age 10 — millions navigating body awareness challenges
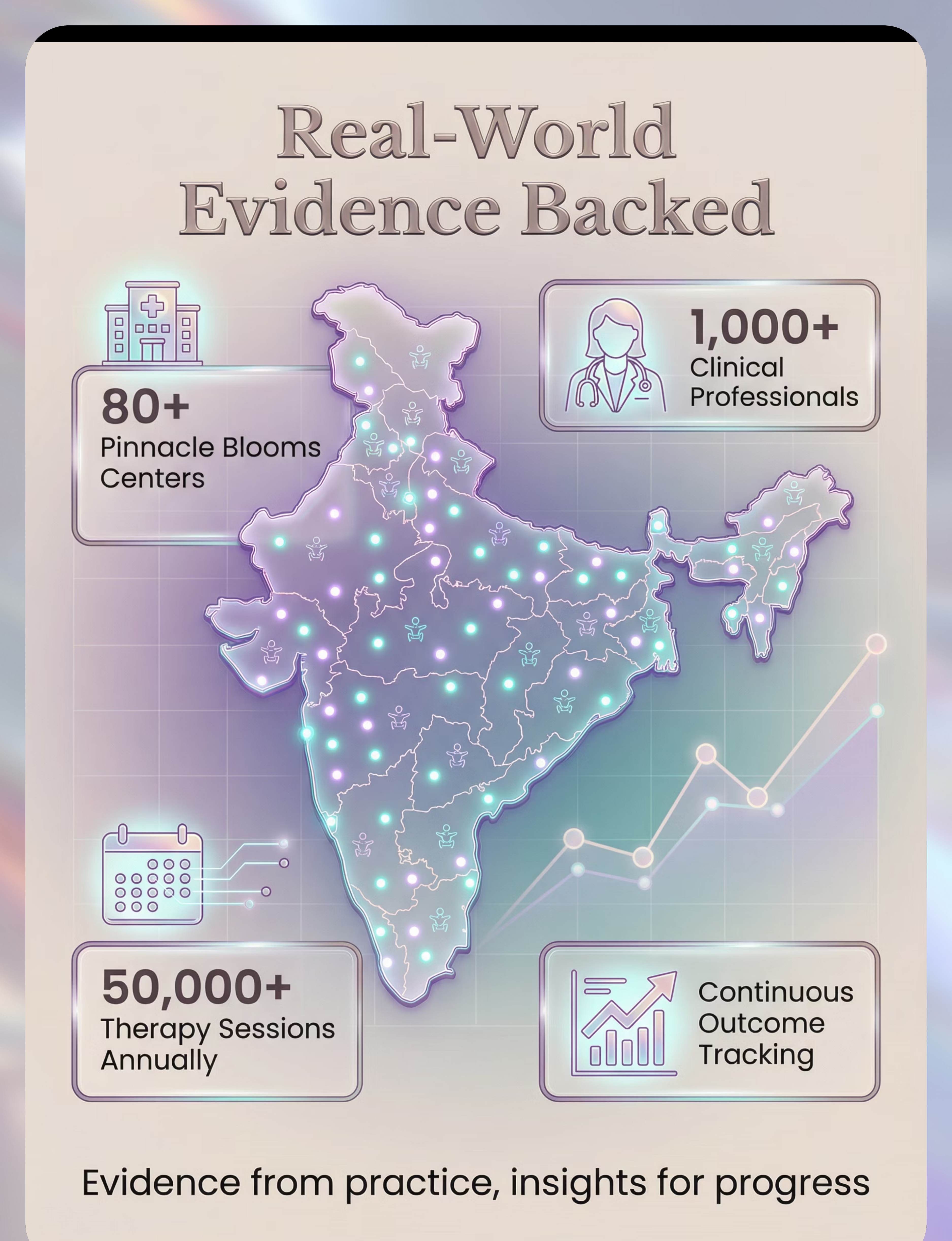
Proprioceptive processing deficit — the clinical name for poor body awareness — is not rare, not mysterious, and not your child's fault. It is the second most common sensory processing challenge in children with autism, behind tactile defensiveness. A 2024 PRISMA systematic review of 16 studies confirmed sensory integration intervention is evidence-based practice for this exact challenge.
"When the therapist told me 80% of kids with autism experience this — I cried. I had thought we were uniquely broken." — Parent, Pinnacle Network, Hyderabad
The Sixth Sense Your Child's Brain Isn't Reading Clearly
What Proprioceptors Do
Inside every muscle, joint, and tendon in your child's body are microscopic sensors called proprioceptors. Their job: constantly report to the brain — where am I? how fast am I moving? how much force am I using?
In children with proprioceptive processing deficit, this reporting system is under-responsive. The signals are sent, but the brain doesn't register them clearly enough to build an accurate internal body map — what scientists call the body schema.
What This Means for Your Child
Without a complete body map, your child literally cannot feel where their arm ends and the wall begins. They cannot gauge how much force to use picking up a glass. They navigate the world like someone trying to walk in a completely dark room.
This is a wiring difference — not a behavior choice. Not defiance. Not clumsiness personality.
🧠The Proprioceptive Pathway: Muscle spindles and GTOs → Dorsal column → Thalamus → Primary somatosensory cortex (S1) → Motor cortex feedback loop. When S1 receives under-amplified proprioceptive signals, the internal body map remains incomplete.
Body Awareness Builds From Birth — But It Can Be Trained At Any Age
The body awareness development zone spans 18 months through 8 years — and targeted intervention shows neural plasticity gains well into adolescence. Your child is not too late, and you are not too early. This is exactly the right time to act.
Commonly Co-Occurs With
Tactile Defensiveness
A-108 — often present alongside proprioceptive deficit
Motor Planning (DCD)
Developmental Coordination Disorder — A-125
Vestibular Differences
Balance and movement processing challenges
Low Muscle Tone
Hypotonia — affects force modulation
Clinically Validated. Home-Applicable. Parent-Proven.
Confidence Rating
Based on 16 systematic review studies and 24 international trials
Effect Size (Max)
Standardized mean difference — clinically significant improvement in motor coordination
Evidence Grade
Level I: Systematic Review + Meta-Analysis evidence across all key studies
Study | Finding | Grade | |
PRISMA Review, Children (2024) — PMC11506176 | SI intervention meets evidence-based practice criteria for ASD, 16 studies 2013–2023 | Level I | |
Meta-analysis, World J Clin Cases (2024) — PMC10955541 | SI therapy promotes gross motor, adaptive behavior, social participation across 24 studies | Level I | |
Indian RCT, Indian J Pediatr (2019) | Home-based sensory interventions demonstrated significant outcomes in Indian pediatric population | Level II RCT | |
WHO/UNICEF CCD Package (2023) — PMC9978394 | Caregiver-delivered sensory-motor stimulation across 54 LMICs with measurable outcomes | Level I |
"16 peer-reviewed studies. 24 international trials. One clear finding: targeted proprioceptive input builds body awareness."

ACT II: LEARN
Poor Body Awareness Intervention — Building the Internal Body Map
Clinical Definition
Poor body awareness — clinically termed Proprioceptive Processing Deficit or Impaired Body Schema — refers to the inability to sense where one's body is in space without looking. The proprioceptive system (muscles, joints, tendons) fails to send clear signals to the brain, leaving the child without a reliable internal map of their own body.
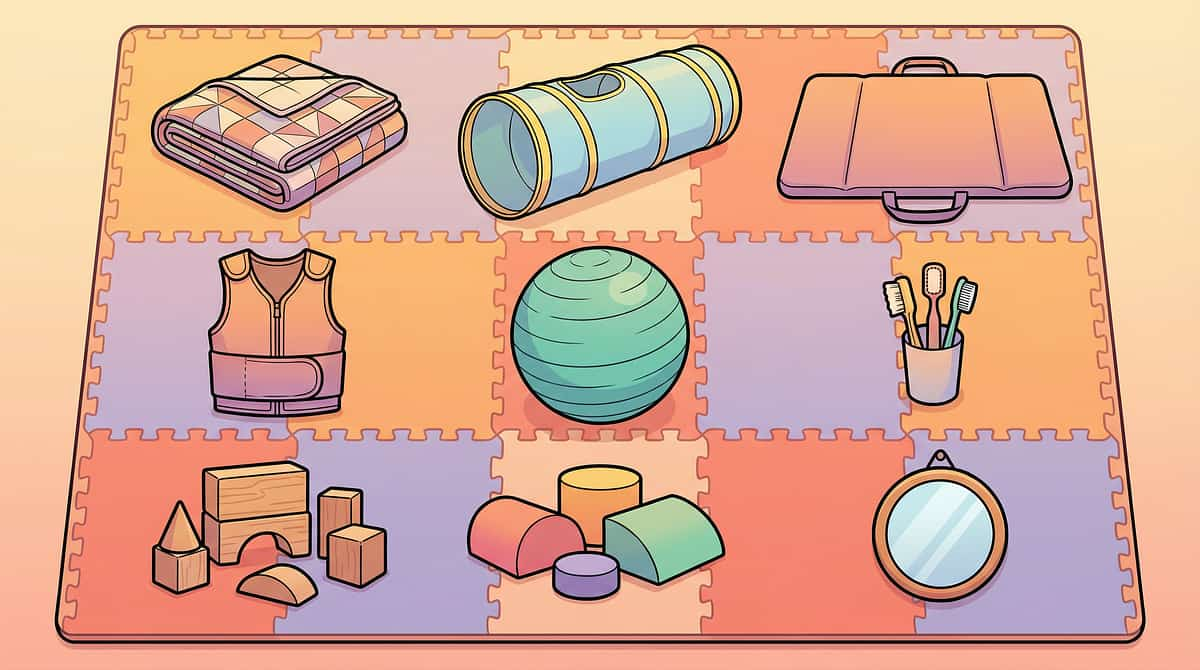
These 9 materials provide targeted proprioceptive input — deep pressure, resistance, compression, heavy work — that trains the nervous system to register and map the body with increasing precision.
Technique Specifications
- 🏥Domain: Sensory — Proprioceptive (SEN-PROP)
- 👶Age Range: 2–10 years
- ⏱️Session Duration: 15–30 minutes
- 📅Frequency: Daily integration recommended
- 🏠Setting: Home and Clinic
- 📋Canon Materials: Deep Pressure Tools | Resistance Equipment | Compression Garments | Heavy Work Equipment | Body Mapping Tools
Reel A-109: Sensory Solutions Series, Episode 109

This Technique Crosses Therapy Boundaries — Because the Brain Doesn't Organize by Therapy Type
Occupational Therapy (Primary Lead)
OTs lead proprioceptive intervention using sensory integration frameworks (Ayres SI). They assess the body schema deficit, prescribe the sensory diet, and train parents in safe material use. Joint compression protocols, heavy work schedules, and weighted equipment selection are OT-driven.
Speech-Language Pathology (Supporting)
Poor body awareness affects oral motor coordination, breath support for speech, and the physical confidence needed for communication. SLPs integrate proprioceptive input before speech sessions to improve oral motor readiness and reduce sensory-seeking behaviors that interrupt communication.
ABA / BCBA (Behavior Layer)
ABA practitioners use proprioceptive activities as antecedent interventions — providing heavy work before demands to reduce sensory-seeking behaviors. Reinforcement schedules are built around successful body awareness activities. Data collection for proprioceptive response tolerance is ABA's contribution.
Special Education (Classroom Integration)
SpEd teachers integrate compression seating, fidget tools, and movement breaks into the classroom using the sensory diet prescribed by OT. Body mapping activities support spatial awareness needed for handwriting, PE, and classroom navigation.
NeuroDevelopmental Pediatrics (Diagnostic Authority)
NeuroDev pediatricians confirm the proprioceptive processing profile, rule out neurological red flags, co-manage hypotonia or DCD if present, and coordinate the multi-disciplinary intervention plan through GPT-OS®.

Not a Random Activity. A Precision Intervention.
🎯 Primary Target: Body Schema Formation
- Child stops bumping into furniture and walls during daily navigation
- Force modulation improves: no longer breaks toys or presses too hard writing
- Child can identify and point to body parts without looking at them
- Personal space awareness emerges in social interactions
🎯 Secondary Target: Motor Planning and Coordination
- New motor skills learned with fewer repetitions (shoe tying, ball skills)
- Balance and postural control improve during seated and standing activities
- Dressing independence increases (buttons, zippers, shoes)
- Gait normalizes — fewer trips and falls
🎯 Tertiary Target: Social, Emotional and Academic Readiness
- Social confidence increases as physical awkwardness reduces
- Reduced frustration meltdowns triggered by physical failures
- Handwriting quality improves as hand pressure regulation develops
- Classroom participation improves (less distraction from proprioceptive seeking)

Material 1 of 9: Weighted Blanket
Weighted Blanket
Canon: Deep Pressure Tools
₹2,500–6,000
Recommended weight: 10% of body weight
Full-body proprioceptive mapping. Provides deep pressure across all body boundaries simultaneously — the most comprehensive single-material body schema input available for home use.
How It Works
The distributed weight activates mechanoreceptors across the entire body surface at once, giving the nervous system a simultaneous whole-body "location report." Over repeated sessions, this builds the foundation of the body schema — the brain's map of where the body begins and ends.
Pinnacle Recommends
- GOTS-certified cotton covers
- Glass bead filling (even weight distribution)
- Removable, washable cover

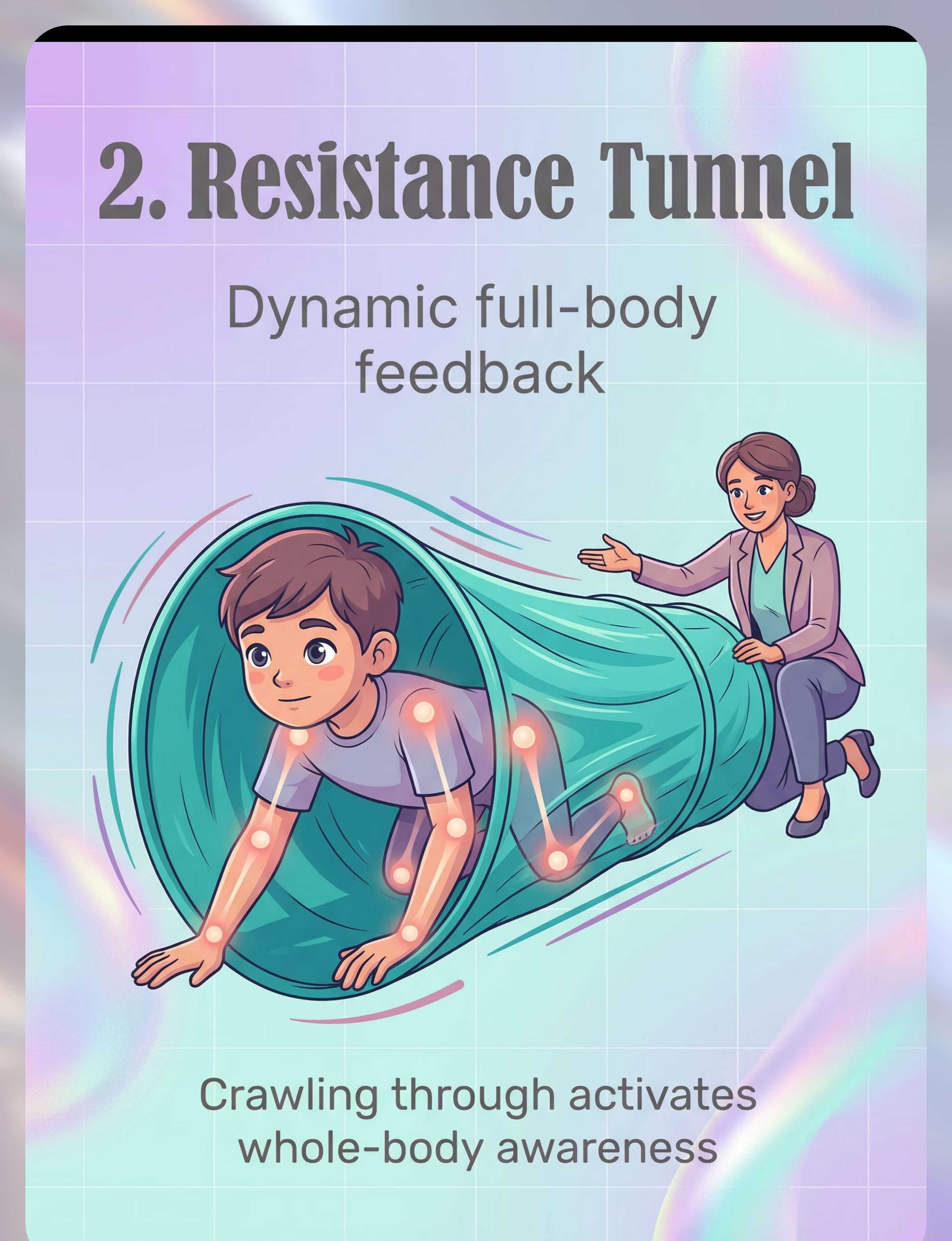
Material 2 of 9: Resistance Tunnel / Lycra Tunnel
Resistance Tunnel / Lycra Tunnel
Canon: Resistance Equipment
₹3,000–7,000
Dynamic full-body feedback. Resistance against all body surfaces during crawling activates whole-body proprioceptive registration — one of the most powerful active input tools available for home use.
How It Works
As the child pushes through the tunnel's stretchy fabric, every surface of their body receives simultaneous resistance feedback. This activates muscle spindles and joint receptors throughout the entire body at once — a full proprioceptive registration event that helps the nervous system map the body in motion.
Session Use
- 3–5 complete traversals per session
- Vary speed: slower builds more registration
- Progress to feet-first for novel proprioceptive challenge

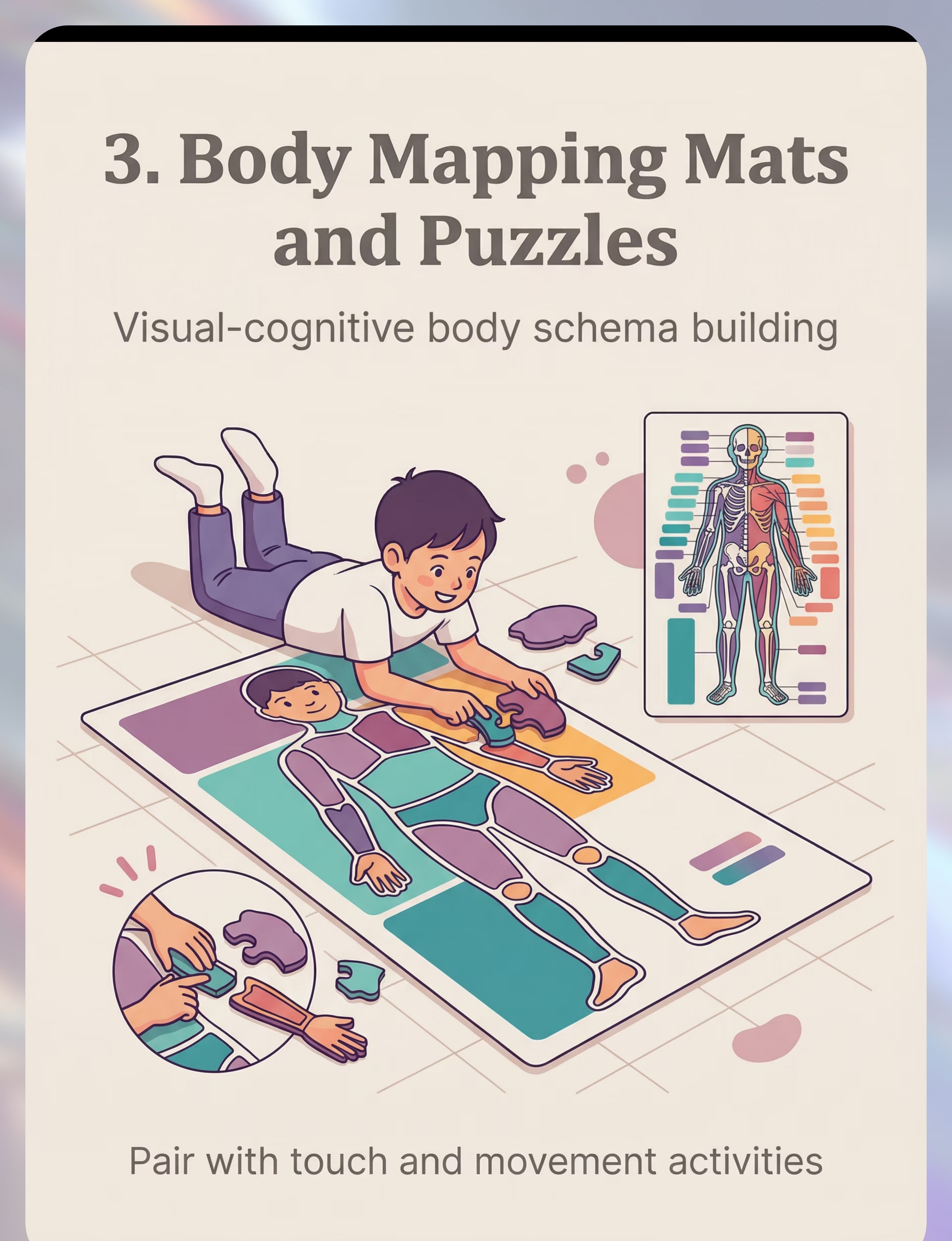
Material 3 of 9: Body Mapping Mat and Puzzle
Body Mapping Mat and Puzzle
Canon: Body Awareness Tools
₹800–2,500
Visual-cognitive body schema building. Matching puzzle parts to body outline builds the mental model that proprioception refines — bridging the gap between felt experience and cognitive understanding of the body.
How It Works
The body mapping mat creates a visual representation of the body schema that the child can interact with directly. As the child matches puzzle pieces to the body outline — while simultaneously touching those body parts — they build the neural bridge between what they see, what they touch, and what they feel internally.
Therapeutic Action
- Parent traces child's body outline with finger while child observes
- Child assembles puzzle pieces while touching each body part named
- 2–3 full body tracing cycles per session, 10–15 minutes

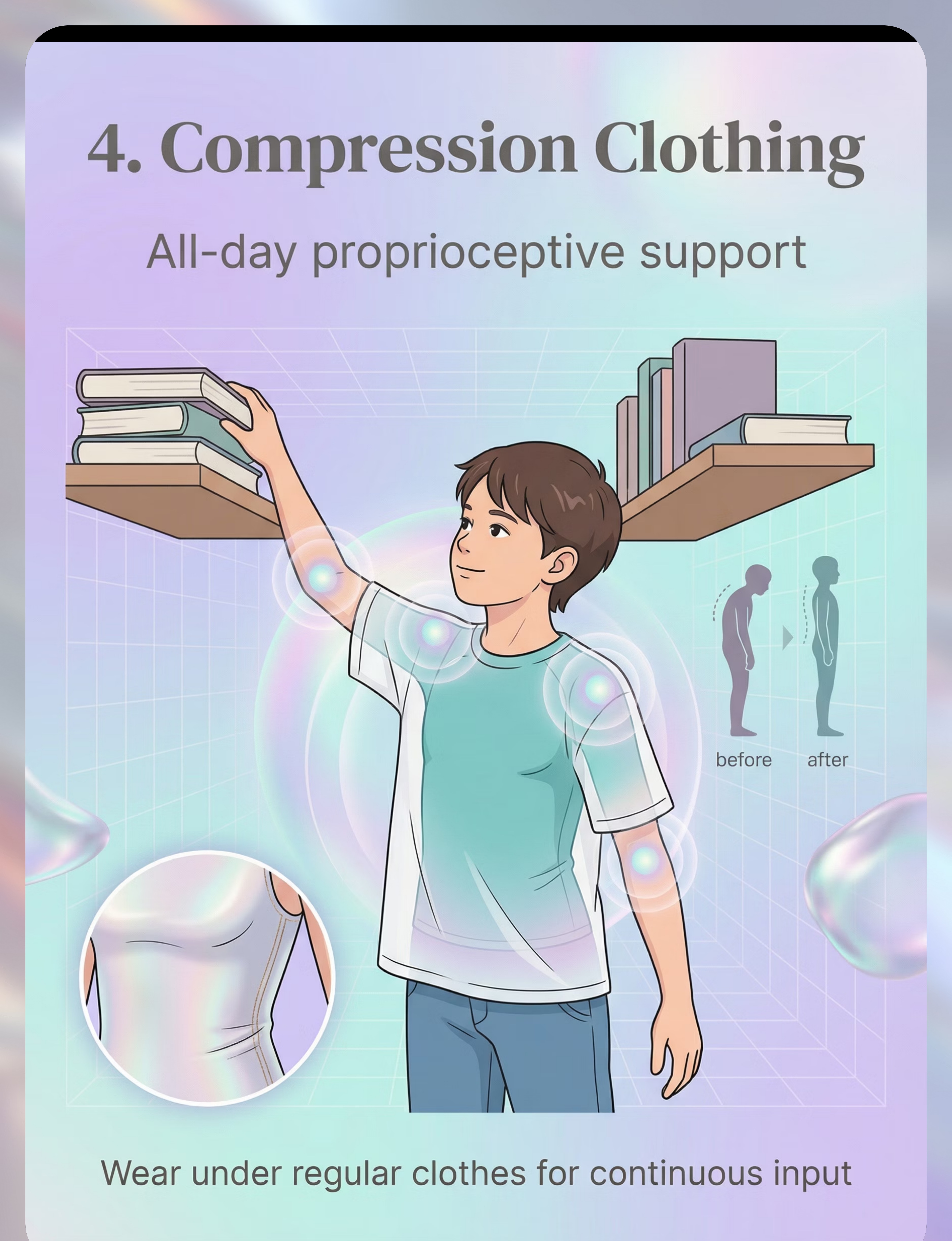
Material 4 of 9: Compression Clothing / Sensory Garment
Compression Clothing / Sensory Garment
Canon: Compression Garments
₹1,500–4,000
All-day proprioceptive support. Continuous gentle pressure maintains body awareness through every activity — turning ordinary daily life into a constant low-level proprioceptive input session.
How It Works
Compression garments apply consistent, gentle pressure to the skin and underlying muscles throughout the day. This continuous sensory feedback keeps the proprioceptive system mildly activated at all times — like a persistent gentle reminder to the nervous system of where the body is. Over time, this continuous input helps consolidate the body schema.
Usage Guidelines
- Worn for 1–2 hours maximum per session
- Monitor for skin irritation or signs of overheating
- All other A-109 activities can occur while wearing
- Check fit: snug but not restrictive

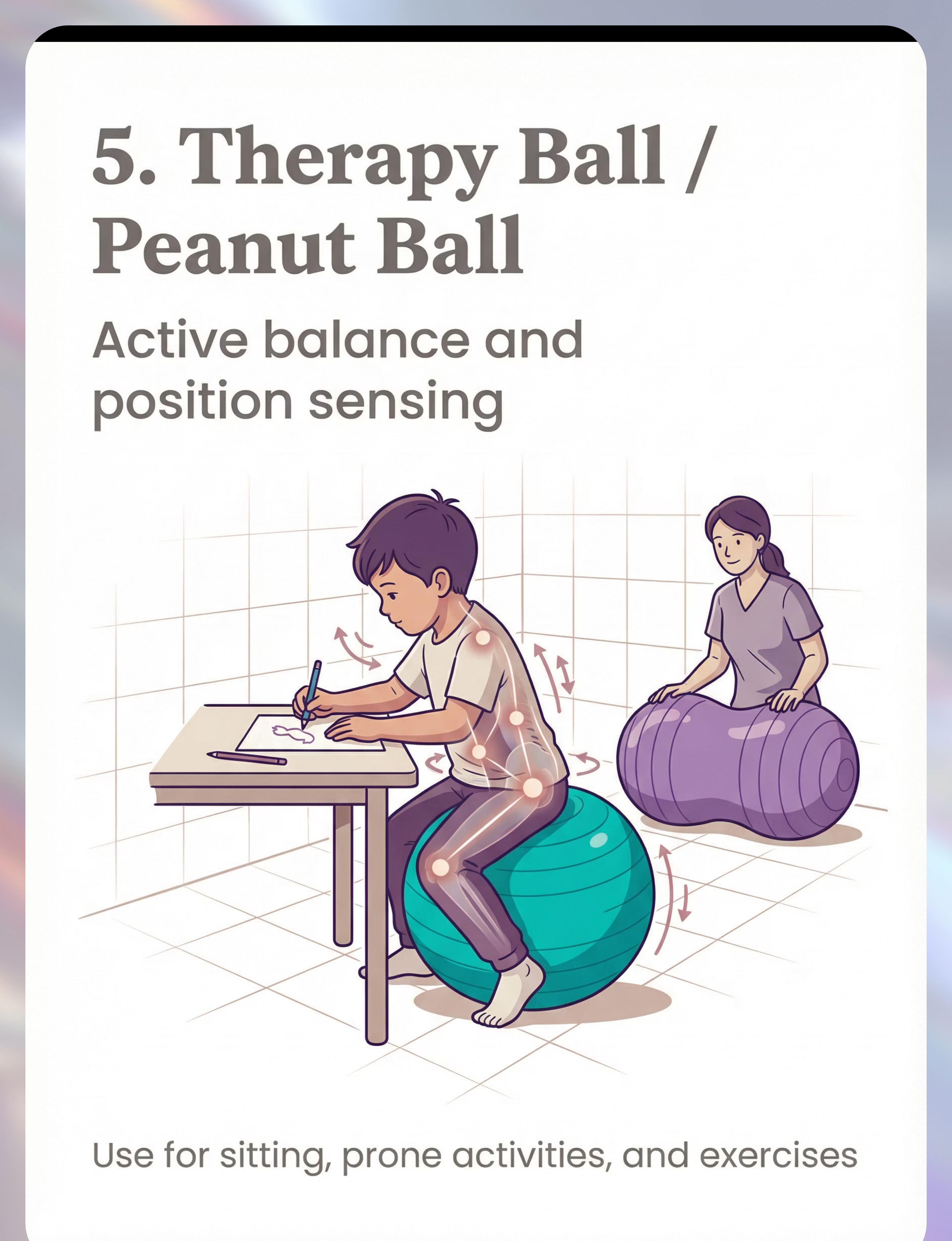
Material 5 of 9: Therapy Ball / Peanut Ball
Therapy Ball / Peanut Ball
Canon: Balance and Vestibular Equipment
₹800–2,000
Active balance and position sensing. The unstable surface demands constant micro-postural adjustments, training real-time proprioceptive response throughout the entire session.
How It Works
The therapy ball's unstable surface means the child's body must continuously self-correct to maintain position. Each micro-adjustment fires proprioceptors throughout the core, hips, legs, and trunk simultaneously — creating a rich, dynamic proprioceptive environment that sharpens the body's real-time positional awareness far more effectively than a stable seated surface.
Therapeutic Progression
- Start with supported sitting, parent stabilizing hips
- Progress to adding reaching tasks while seated
- Advanced: eyes closed, hands in lap, staying balanced
- Hips and knees should be at 90° when seated

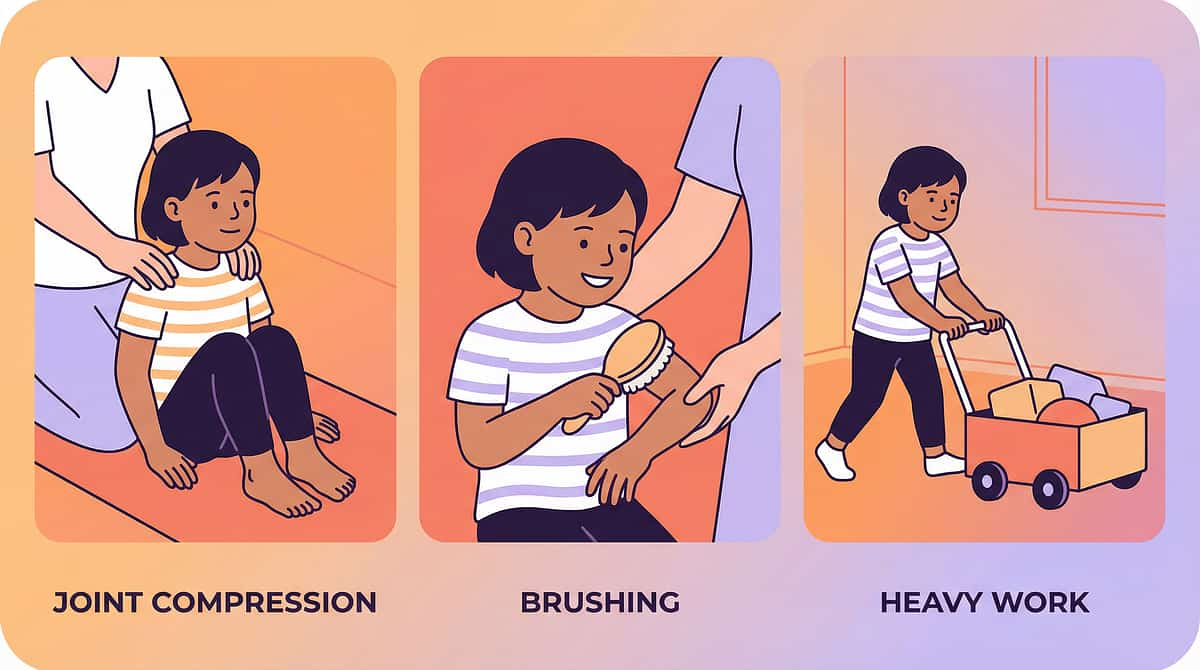
Material 6 of 9: Joint Compression and Therapeutic Brushing Tools
Joint Compression and Therapeutic Brushing Tools
Canon: Deep Pressure Tools
₹300–800 (brush) + OT Training Required
Direct proprioceptive activation. Systematically activates joint receptors and skin mechanoreceptors to recalibrate body awareness at the neurological source.
How It Works
Joint compression applies firm pressure through major joints in sequence — shoulders, elbows, wrists, hips, knees, ankles — activating the Golgi tendon organs and joint mechanoreceptors directly. This is the most targeted proprioceptive input available and produces rapid, measurable changes in body awareness when applied correctly.
⚠️OT Training Required for Wilbarger Brushing Protocol. Parent-applied joint compressions (10 firm presses per joint, 2 sequences per session) can be taught by your OT. Brushing without training can cause adverse effects — do not attempt unsupervised.

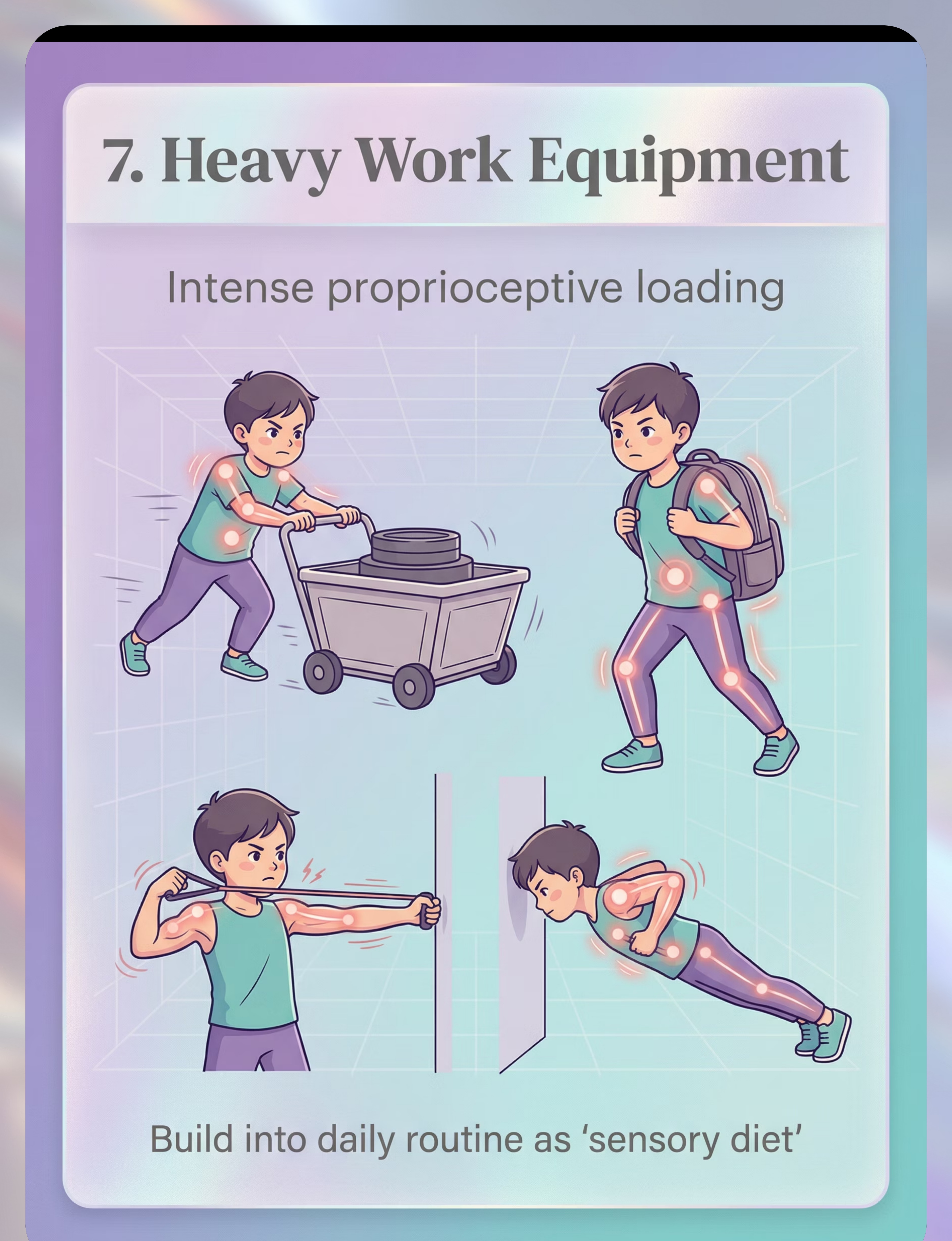
Material 7 of 9: Heavy Work Activity Equipment
Heavy Work Activity Equipment
Canon: Heavy Work Tools
₹500–3,000
Intense proprioceptive loading. Pushing, pulling, lifting, carrying — the most powerful proprioceptive input available. Heavy work activates the full proprioceptive system at maximum intensity.
The Heavy Work Circuit
Heavy work is the backbone of any proprioceptive sensory diet. The resistance created by working against weight or gravity fires muscle spindles and Golgi tendon organs throughout the entire body — producing the strongest and most lasting proprioceptive registration effect of all 9 materials.
- Bear walk → push heavy box → carry weighted backpack 10 steps → wall push-ups ×10 → crab walk
- Each exercise 30–60 seconds | Total circuit: 10–15 minutes
- Build to daily "sensory diet" routine before school or demanding activities

Material 8 of 9: Obstacle Course Components
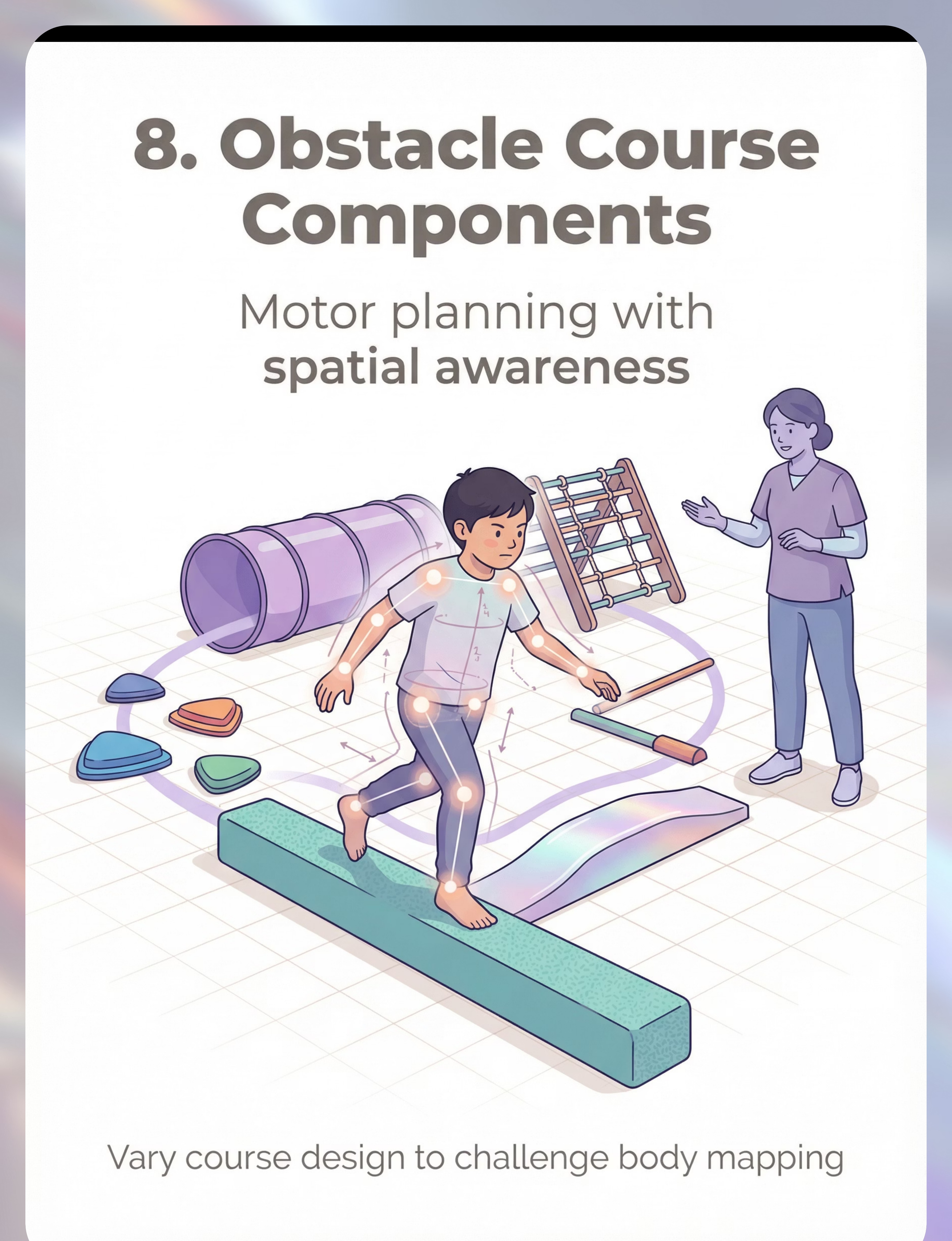
Obstacle Course Components
Canon: Motor Planning Equipment
₹2,000–8,000
Motor planning with spatial awareness. Complex navigation through physical challenges demands integrated proprioceptive, vestibular, and visual processing — the most cognitively advanced of the 9 materials.
How It Works
Obstacle courses are uniquely powerful because they require the child to plan movement through space — step over, crawl under, squeeze through, balance across — demanding constant real-time proprioceptive feedback to navigate successfully. Each challenge builds motor planning on top of body schema, creating the neural integration needed for real-world navigation.
Therapeutic Progression
- 3–5 complete runs per session with verbal body-position cues
- Progress: add elements, reduce verbal cues as awareness improves
- Advanced: novel environments, rearranged obstacles, blindfold element

Material 9 of 9: Mirror and Video Feedback System
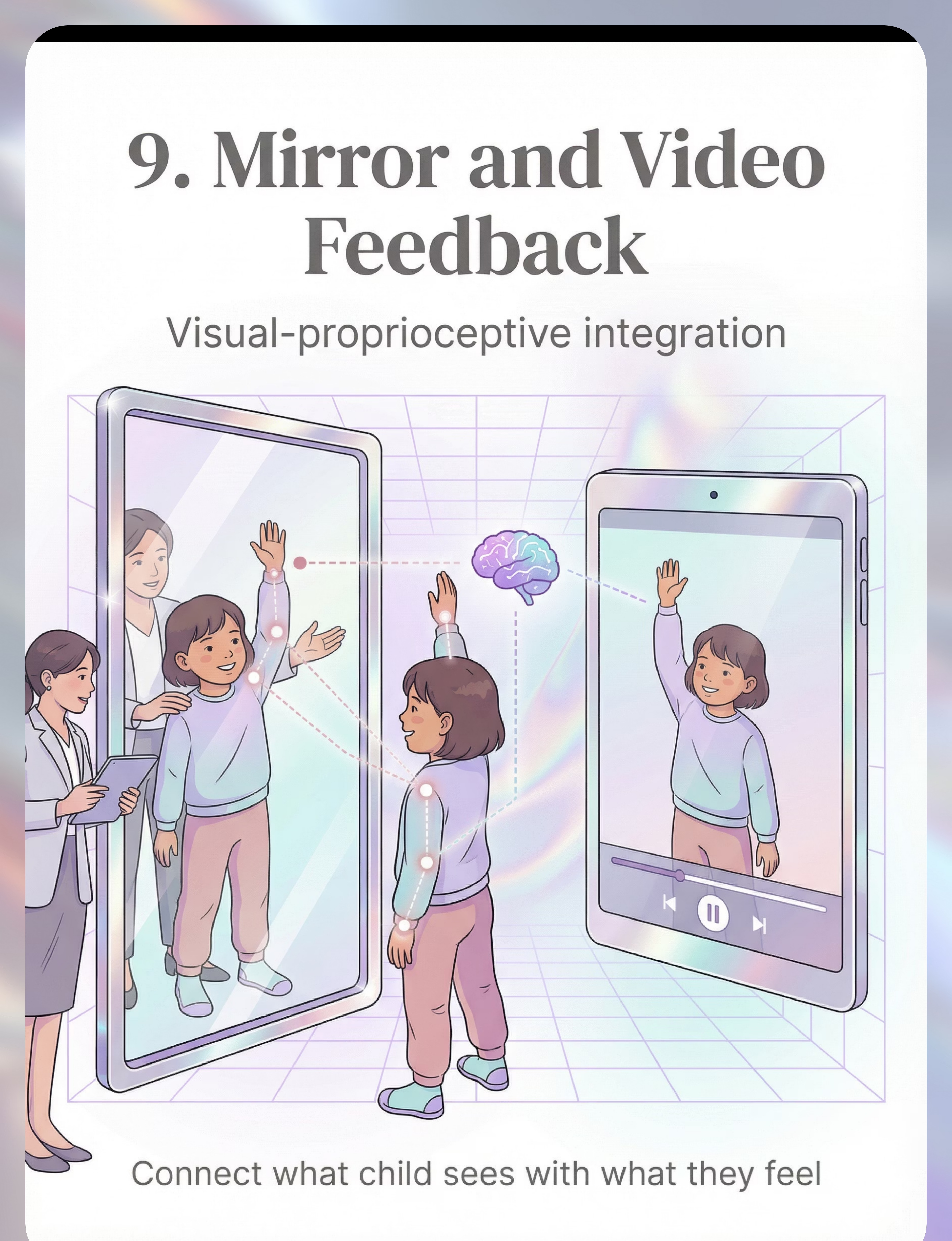
Mirror and Video Feedback System
Canon: Visual Feedback Tools
₹1,500–5,000
Visual-proprioceptive integration. Watching the body move while feeling it move builds the neural bridge between external observation and internal sensing — training the brain to connect visual and proprioceptive body maps.
How It Works
Mirror work targets the neural disconnect at the heart of body awareness deficit. When a child watches themselves move in real time, the visual cortex and somatosensory cortex must reconcile their inputs — strengthening the neural connections between "I see my arm moving" and "I feel my arm moving." Over repeated sessions, the internal body map grows more reliable.
Therapeutic Sequence
- Stand beside child facing mirror | Do slow movements: raise right arm | Child mirrors
- "Look — your arm is up. Can you FEEL your arm up without looking?"
- Child closes eyes, holds position — confirms with eyes open
- 5–10 minutes | 5–8 movement sequences per session
All 9 Materials at a Glance — Your Complete Starter Guide
Material | Canon Category | Price Range (INR) | Primary Action | |
1. Weighted Blanket | Deep Pressure Tools | ₹2,500–6,000 | Full-body proprioceptive mapping | |
2. Resistance Tunnel | Resistance Equipment | ₹3,000–7,000 | Dynamic full-body feedback | |
3. Body Mapping Mat | Body Awareness Tools | ₹800–2,500 | Visual-cognitive schema building | |
4. Compression Clothing | Compression Garments | ₹1,500–4,000 | All-day proprioceptive support | |
5. Therapy Ball | Balance Equipment | ₹800–2,000 | Active position sensing | |
6. Joint Compression Tools | Deep Pressure Tools | ₹300–800 + OT training | Direct proprioceptive activation | |
7. Heavy Work Equipment | Heavy Work Tools | ₹500–3,000 | Intense proprioceptive loading | |
8. Obstacle Course | Motor Planning Equipment | ₹2,000–8,000 | Spatial navigation training | |
9. Mirror / Video System | Visual Feedback Tools | ₹1,500–5,000 | Visual-proprioceptive integration |
Essential Starter Kit
Weighted Blanket + Heavy Work items + Body Mapping Mat
₹4,000–10,000 — everything you need to begin immediately
Comprehensive Setup
All 9 materials for a complete home therapy environment.
₹13,000–38,000 total investment estimate
📞 Not sure which to buy first? Call 9100 181 181 — FREE OT guidance based on your child's specific profile.

Every Family Can Start Today. ₹0 Options Exist for Every Material.
Per WHO/UNICEF equity principles: effective intervention cannot be gated behind product availability.
Material | DIY Version | Why It Works | |
Weighted Blanket | Duvet cover + 1–2 kg rice in sealed cloth pouches, distributed evenly. Total ≈ 10% of body weight | Same deep pressure input via distributed weight across body surface | |
Resistance Tunnel | King-size fitted sheet stretched between two chairs OR old lycra/spandex fabric sewn into a tube | Fabric resistance activates same proprioceptors as commercial tunnel | |
Body Mapping Mat | Trace child's full body on large newspaper sheets, cut into body part shapes, child reassembles | Identical visual-cognitive body schema building at zero cost | |
Compression Clothing | Tight-fitting athletic wear, rash guards, snug undershirts layered | Same continuous pressure input — check that fit is snug but not restrictive | |
Therapy Ball | Any exercise ball (available ₹300–500) | Unstable surface principle identical — hips and knees at 90° when seated | |
Joint Compression | Manual joint compressions: 10 firm presses through shoulders → elbows → wrists → hips → knees → ankles | Direct receptor activation — same pathway, hands-only version | |
Heavy Work | Backpack with books, carry grocery bags, push laundry basket, wall push-ups, bear walks, crab walks | Heavy work principle requires resistance, not equipment | |
Obstacle Course | Sofa cushions, chairs with blankets, tape lines on floor, hula hoops, pillows stacked | Same motor planning + proprioceptive demand | |
Mirror | Smartphone selfie camera (real-time view), any bathroom mirror | Visual-proprioceptive integration works with any reflective surface |
⚠️When clinical-grade materials are non-negotiable: Joint compression brushing (Wilbarger Protocol) requires a Therapressure brush AND trained OT. DIY brushing without training can cause adverse effects. Weighted blankets for children under 2 must be correctly weighted — DIY requires precise calculation (10% body weight maximum).

Every Technique Has a Safety Gate. Read This Before the First Session.
🔴 RED — DO NOT PROCEED if:
- Child is under 2 years for weighted blanket use
- Child has respiratory, cardiac conditions, or diagnosed hypermobility/joint instability
- Child cannot remove weighted blanket independently
- Wilbarger brushing without direct OT training
- Child shows signs of acute illness, fever, or extreme distress
- Joint compressions if child has diagnosed hypermobile Ehlers-Danlos syndrome
🟡 AMBER — MODIFY before proceeding if:
- Child has tactile defensiveness alongside proprioceptive deficit — introduce slowly
- Child has claustrophobia — start with open-ended resistance before tunnel
- Child is post-meltdown or highly dysregulated — use calming input first
- Child is tired or hungry — feed and rest before session
- Session is in an unfamiliar environment — establish the space first
🟢 GREEN — PROCEED when:
- Child is in a calm-alert state (fed, rested, regulated)
- Materials have been checked for weight appropriateness and safety
- You have read the execution cards fully before starting
- An emergency exit strategy is in place (child can always disengage)
- Environment is cleared of sharp corners, excessive noise, and clutter
⚠️STOP SESSION immediately if you observe: Sudden extreme distress or inconsolable crying | Complaints of pain from materials | Sudden change in skin color, breathing, or alertness | Self-injurious behavior escalation | Child becomes completely non-responsive. 📞 Unsure about safety? 9100 181 181 — FREE OT consultation.

Spatial Precision Prevents 80% of Session Failures.
Room Setup Checklist
- Clear a 3m × 3m movement space — remove sharp furniture, loose rugs, cords
- Position materials at child's access height — floor level for most activities
- Parent position: within 1 arm's length for safety, not blocking movement path
- Lighting: natural or warm white — no flickering, no harsh fluorescent
- Sound: background hum acceptable; no TV, no competing screens
- Temperature: comfortable — note compression clothing heat considerations
- Remove: preferred toys not in the session (reduces competing motivation)
- Set up: visual timer (analog sand timer or phone timer visible to child)
- Prepare: data tracking sheet within reach
- Exit route: child always has a clear, unobstructed path to exit the space
Material-Specific Spatial Notes
- Resistance tunnel: 3m clear crawl-out space at both ends
- Therapy ball: Non-slip mat underneath, 1m clearance on all sides
- Obstacle course: Walk the path yourself before the child enters
- Mirror work: Position so full body is visible, child can maintain comfortable distance
Environmental setup is a core principle of Sensory Integration Theory (Ayres). A structured, predictable, safe environment is not optional — it is part of the therapeutic protocol itself.

ACT III: EXECUTION
The Best Session Is One That Starts Right.
60-Second Pre-Session Assessment — Before Every Session
Indicator | ✅ Go | ❌ Postpone | |
Nutrition | Child ate within last 90 minutes | Child is hungry or just finished a large meal | |
Rest | Child is alert but not hyperactive | Child is visibly tired, yawning, rubbing eyes | |
Regulation state | Calm, curious, or slightly active (optimal) | In/just exiting a meltdown, crying, shutdown | |
Illness check | No fever, no complaints of pain | Elevated temperature, runny nose, lethargy | |
Receptivity signal | Responds to name, makes eye contact or shows awareness | Unresponsive, in deep stim, completely avoidant |
🟢 GO
4–5 checkmarks. Proceed to Step 1: The Invitation.
🟡 MODIFY
3 checkmarks. Use simplified version — just one material, 5 minutes, no new challenges.
🔴 POSTPONE
2 or fewer checkmarks. Offer deep pressure hold or weighted blanket passively. No formal session.
"A postponed session is not a failed session. It is a session with perfect timing."

Step 1 of 6: The Invitation
⏱️ 30–60 seconds
"Every Protocol Begins With an Invitation, Not a Command."
What to Say — Exact Scripts
"I found something really interesting. Want to come see?"
"I need your super-strong help with something."
"I have a special [material name] that only big kids use."
Body Language
- Lower yourself to child's eye level
- Hold the material casually — don't present directly yet
- Face slightly away — parallel engagement invites, direct fronting can feel demanding
- Stay relaxed — children read parental anxiety and mirror it
What Acceptance Looks Like
- Physical approach toward you or the material
- Eye glance at the material
- Any vocalization or gesture toward it
- Body orientation turns toward you
What Resistance Looks Like (and What to Do)
- Complete ignoring → wait 30 seconds, try alternate script, or place material visibly nearby
- Walking away → this is data, not failure. Try again in 10 minutes with a different material
- Distress → POSTPONE. Move to readiness check modification protocol

Step 2 of 6: The Engagement
⏱️ 1–3 minutes
"The Material Enters. The Nervous System Begins Its Work."
🏋️ Weighted Blanket
Demonstrate on yourself first: "Look, I'm putting it on my legs. It feels like a big hug." Offer to child's lap first (least threatening — not full body).
🌀 Resistance Tunnel
Crawl through yourself first if space allows. "I'm going through the tunnel! Can you follow me?" Keep tunnel entrance open and inviting.
📐 Body Mapping Mat
Lie down on the mat yourself: "Look — I'm a giant! Now it's your turn — let's see if you fit." Child lies on the outline, matches their body to the shape.
⚽ Therapy Ball
"This ball is bouncy AND it helps your body know where it is. Can you sit like a frog?" Support the child's hips if needed for first 30 seconds.
🧥 Compression Clothing
"This is a body-hug shirt. It reminds your arms and legs where they are all day." Help child put it on like a superhero suit.
Reinforcement starts now: Every approach and acceptance gets immediate specific praise: "You touched the blanket! That was so brave!"
Step 3 of 6: The Therapeutic Action (Materials 1–5)
⏱️ 5–15 minutes — This Is Where the Brain Builds Its Map
1. Weighted Blanket → Stationary Deep Pressure
Drape blanket over child (seated or lying). Apply gentle additional pressure across major body segments (shoulders, thighs) for 5–10 seconds each. Say: "I'm pressing here — can you feel your shoulder? Now here — can you feel your knee?" Build the verbal-proprioceptive connection. ⏱️ 10–20 minutes | Begin at 2 minutes, build to 20 over weeks
2. Resistance Tunnel → Dynamic Body Feedback
Child crawls through tunnel independently. Provide gentle resistance at tunnel opening to slow the movement: "Push through! Feel your whole body working." 3–5 complete traversals per session. ⏱️ 5–10 minutes
3. Body Mapping Mat → Schema Building
Parent traces child's body outline with finger while child observes: "I'm tracing your arm — here — all the way to your hand." Child then assembles puzzle pieces while touching each body part: "Put the arm piece — and touch YOUR arm." ⏱️ 10–15 minutes
4. Therapy Ball → Active Position Sensing
Child seated on ball for table activities (drawing, puzzles, snack). Parent may provide lateral gentle displacement: "Stay sitting! Feel your body balance." Progress to: eyes closed, hands in lap, staying balanced. ⏱️ 10–20 minutes continuous use
5. Heavy Work → Proprioceptive Loading
5-exercise circuit: Bear walk → push heavy box → carry weighted backpack 10 steps → wall push-ups ×10 → crab walk. Each exercise 30–60 seconds. Build to daily sensory diet routine before school or demanding activities. ⏱️ 10–15 minutes
Step 3 Continued: The Therapeutic Action (Materials 6–9)
⏱️ 5–15 minutes — The Active Ingredient Continues
6. Joint Compression (Parent-Applied)
Parent applies 10 firm (not hard) compressions through: shoulders → elbows → wrists → hips → knees → ankles in sequence. Each compression: press firmly, hold 1 second, release. Child seated, relaxed. Entire sequence: 2–3 minutes. Repeat 2× per session.
7. Obstacle Course → Spatial Navigation
Child navigates course with verbal body-position cues: "Step OVER the pillow — where are your feet? Now crawl UNDER the chair — can you feel the chair near your back?" Progress: add elements, reduce verbal cues as awareness improves. ⏱️ 10–15 minutes
8. Mirror Work → Visual-Proprioceptive Bridge
Stand beside child facing mirror. Do slow movements: raise right arm. Child mirrors. Say: "Look — your arm is up. Can you FEEL your arm up without looking?" Child closes eyes, holds position: "Your arm is still there — feel it?" Open eyes to confirm. ⏱️ 5–10 minutes
9. Compression Clothing → Passive Integration
Worn for 1–2 hours maximum per session. All other activities can occur while wearing. Monitor for skin irritation, signs of overheating. ⏱️ 60–120 minutes wear time
✅ Ideal Response
Engaged, seeking, showing reduced compensation strategies, attempting tasks previously avoided
✅ Acceptable Response
Tolerating the input without distress, completing on request
⚠️ Concerning Response
Escalating distress, rigid refusal, pain responses → stop and reassess immediately

Step 4 of 6: Repeat and Vary
⏱️ 3–5 minutes
"3 Good Repetitions Are Worth More Than 10 Forced Ones."
Material | Target Reps | Variation Options | |
Weighted Blanket | 10–20 min continuous | Change body position: seated, prone, side-lying | |
Resistance Tunnel | 3–5 full traversals | Change direction: feet first, faster, slower | |
Body Mapping Mat | 2–3 full body tracing cycles | Add touch while naming, add movement before lying down | |
Therapy Ball | Continuous 10–20 min | Add reaching tasks, add balance challenges | |
Heavy Work Circuit | 2–3 full circuits | Change weight, change animal walk, add climbing | |
Joint Compressions | 2 full body sequences | Add vibration, change pressure depth | |
Obstacle Course | 3–5 complete runs | Rearrange obstacles, add blindfold element | |
Mirror Work | 5–8 movement sequences | Add delayed mirror (video playback), add rhythm |
Satiation indicators — when to stop for the day: Child begins to disengage, wander, or lose interest | Child completes actions without attention or presence | Child escalates rather than calms with continued input | You reach the target repetitions — stop even if child seems ready for more. "End on success — always." The last repetition should be one the child completes well.
Step 5 of 6: Reinforce and Celebrate
Ongoing Throughout Session — Timing Matters More Than Magnitude. Within 3 Seconds. Every Time.
Reinforcement Script Library
🗣️Verbal (always):
"You pushed through the tunnel! Your whole body worked so hard!"
"Look at you balancing! Your body KNOWS where it is!"
"You carried that heavy bag — your muscles are learning!"
"Look at you balancing! Your body KNOWS where it is!"
"You carried that heavy bag — your muscles are learning!"
🤝Social (pair with verbal):
High five, fist bump, celebratory squeeze, thumbs up — keep it brief and joyful
🏆Token Economy (if child uses token system):
1 token per completed repetition. 5 tokens = chosen activity from reinforcement menu.
Reinforcement Menu Options
- ⭐Reward Stickers — 1800+ stickers, ₹364
- 🫙Reward Jar — Rosette Imprint, ₹589
- 30 seconds of preferred activity
- Proprioceptive reward that also serves therapy: bounce on trampoline, swing, jump
- Social praise from another family member
Critical principle: Celebrate the attempt, not just the success. A child who tolerated 3 seconds of weighted blanket contact deserves the same enthusiasm as one who completed 20 minutes. You are reinforcing the direction, not the destination.
Step 6 of 6: The Cool-Down
⏱️ 2–3 minutes — No Session Ends Abruptly. The Nervous System Needs a Landing.
Transition Warning (2 Minutes Before Ending)
"Two more times through the tunnel, then we're all done."
"One more minute of balancing, then we'll put the ball away."
"One more minute of balancing, then we'll put the ball away."
Use a visible sand timer or phone timer: "When the sand runs out, we're done." Visual timer is classified evidence-based practice by NCAEP (2020) for autism.
If Child Resists Ending
Acknowledge: "I know — this is fun. Two more, then we stop." Follow through. Consistent endings build trust and reduce next-session resistance.
Cool-Down Sequence (Pick One)
- Deep pressure hold: 30-second firm full-body hug or blanket wrap — transition from active to calm proprioceptive input
- Slow rocking: 60 seconds rhythmic gentle rocking — activates vestibular calming
- Wall push-ups: 5 slow, controlled — burns remaining activation energy
- "Big squeeze": Child squeezes parent's hands firmly ×5 — controlled proprioceptive discharge
Material Put-Away Ritual
Child participates in putting materials away — "Help me fold the blanket / put the ball back." This provides incidental heavy work AND builds the closure routine that children with proprioceptive deficits rely on.

What Gets Measured Gets Improved. Takes 60 Seconds.
Minimum Viable Data — Track After Every Session
Data Point | How to Record | Example | |
Session date and time | Note day + time | "Tuesday 4:30pm" | |
Materials used | Check ✅ | ✅ Weighted Blanket ✅ Heavy Work | |
Duration tolerated | Minutes | "12 minutes weighted blanket" | |
Tolerance rating | 1–5 scale | 3/5 — tolerated with some resistance | |
Notable response | One phrase | "Stopped bumping into table during snack" |
Tracking Options
- 📱 GPT-OS® In-App Tracker: data feeds directly into AbilityScore® progress monitoring
- 📝 Simple notebook: Date | Material | Duration | Rating (1–5)
Why this matters: 3 data points per session × 5 sessions per week × 8 weeks = 120 data units that allow your OT to see exactly which materials work, which timing is optimal, and when to advance the protocol. This is GPT-OS® data intelligence — proprioceptive response patterns improve recommendations for all children like yours.
Most Sessions Aren't Perfect. The Technique Needs Adjustment — Not You.
"Session abandonment is not failure. It is data."
Child refused to engage with the material at all
Why: Novelty aversion or tactile defensiveness may be present alongside proprioceptive deficit. Solution: Leave material in play space visible but untouched for 3 days. Let curiosity build. Start with the least physically demanding material (heavy work, mirror) before deep pressure items.
Child engaged for 30 seconds then ran away
Why: Short engagement windows are normal at the start. Proprioceptive registration takes time. Solution: 30 seconds IS success. Record it. Celebrate it. Build from there: 30 sec → 1 min → 2 min over weeks.
Child became more hyper and dysregulated during the session
Why: Heavy work can be activating before it becomes organizing in the first 1–2 weeks. Solution: Switch to calming input — slow weighted blanket or deep pressure hold. Reduce session length. If persistent after 2 weeks, consult OT.
Child cried when compression clothing was put on
Why: Tactile defensiveness to tight clothing is separate from proprioceptive needs. Solution: Do not force. Begin with loose compression (rash guard, not tight compression shirt). Build tolerance over days/weeks.

Troubleshooting Continued — Problems 5, 6, and 7
Child showed no visible change after 2 weeks
Why: 2 weeks is early. Most studies show observable changes at 4–6 weeks. Consistency matters — 2 sessions are not the same as 14 sessions. Solution: Check session consistency using your tracking data. Have you been doing 5 sessions/week? If yes and no change at 6 weeks, consult OT for protocol adjustment.
Other family members undermined the technique
Why: Proprioceptive therapy looks like play. Family buy-in requires education. Solution: Share the Family Guide (Card 37) with them. Point to the evidence grade (Card 5). Consider: "This is prescribed by our OT based on 16 clinical studies."
Child became severely distressed mid-session
Why: Sensory overload, unexpected trigger, or the session was pushed past the child's window of tolerance. Solution: Stop immediately. Deep pressure hold if child accepts. Remove materials. After child is regulated, record what happened for your OT. Do not retry the same material the same day.
📞 Experiencing a challenge not listed here? Call 9100 181 181 — FREE OT consultation, available 24×7.

No Two Children Are Identical. This Technique Has a Version for Every Profile.
🔎 Sensory Seeker (always crashing, seeking intense input)
Needs HIGH intensity proprioceptive input to register. Heavy work circuit first, then compression clothing all day. Resistance tunnel, obstacle courses, and body mapping. Begin with intense, reduce over weeks as registration improves.
🙈 Sensory Avoider (resists touch, doesn't like tight things)
Start with PASSIVE input: weighted blanket with child's own hands placing it. Mirror work before body touch. Build input tolerance before resistance or compression. Go slow, respect boundaries consistently.
👶 Younger Child (2–3 years)
Simplify to: heavy work (animal walks, carrying boxes) + mirror play + deep pressure hugs. Formal protocols require child cooperation — at this age, embed everything in play.
🎒 Older Child (7–10 years)
Introduce movement breaks at school (compression shorts, exercise band at desk). Engage child in understanding their own sensory system. Self-advocacy language: "My body needs heavy work before I can focus."

ACT IV: PROGRESS
Weeks 1–2: You're Building the Foundation — Not the House.
Progress at Week 2
Foundation phase — neural pathway is activating, even before visible change appears
🎯 Observable Indicators at Week 1–2
- Child tolerates weighted blanket for at least 3–5 minutes without resistance (versus initial refusal)
- Heavy work circuit completed with prompting (versus refusal at Day 1)
- Body mapping mat engaged with curiosity (touching body parts when named)
- ONE instance of reduced bumping or better force modulation observed in daily life
What Is NOT Progress Yet
- Spontaneous navigation without bumping (takes 4–6+ weeks)
- Requesting proprioceptive materials independently (takes 3–4 weeks)
- Generalization to school or unfamiliar environments (takes 6–8+ weeks)
The brain is receiving the input. The neural pathway is being activated. The body schema is starting to form. None of this is visible yet — but it is happening. Your consistency right now is the most important variable.

Week 5–8: Mastery. The Body Map Is Working.
Progress at Week 8
Mastery phase — observable, measurable improvements across multiple environments
Mastery Indicator | Measurable Form | |
Navigation improvement | Fewer than 3 bumps per day in familiar environments (from baseline 10–15) | |
Force modulation | Handles fragile items without breaking 80%+ of attempts | |
Body part awareness | Identifies all major body parts by touch (eyes closed) on 4/5 trials | |
Motor learning speed | New motor skill learned in 30% fewer repetitions | |
Heavy work requests | Spontaneously seeks 1+ heavy work activity per day | |
Generalization | Shows improved navigation in 2+ unfamiliar environments |
"Mastery Unlocked" criteria: 4 of 6 indicators met consistently for 2 consecutive weeks.
If 5–6 mastery criteria met → advance to A-118 (Heavy Work for Daily Routines) or A-125 (Motor Planning). If 2–3 criteria met → strengthen current protocol for 2 more weeks before advancing.

You Did This. Your Child Grew Because of Your Commitment.
"You showed up when this felt pointless. You pressed shoulders and did animal walks and folded weighted blankets when your child ran away. You tracked data when you were exhausted. And now your child navigates their world with a body map they didn't have before."
Your Specific Achievement — Technique A-109
- You built a child's proprioceptive foundation
- You gave a nervous system the input it was missing
- You translated a clinical deficit into a home-based daily practice
That is not something most parents know how to do. You do now.
Document This Milestone
- 📸 Photo prompt: Child doing their favorite heavy work activity
- 📹 Video prompt: Child navigating a familiar obstacle — compare to Week 1
- 📓 Journal prompt: "The moment I knew it was working was when..."
Family celebration suggestion: Take a video of your child navigating a familiar obstacle or carrying something without bumping or breaking it. Compare it to a video from Week 1. That difference is your evidence.

Home + Clinic = Maximum Impact. Professional Guidance Multiplies Every Home Session.
Full Center-Based OT (Maximum Impact)
In-clinic sensory integration therapy 2–3×/week with trained OT. Home protocol integrated through EverydayTherapyProgramme™. AbilityScore® tracking every 4 weeks. → Find your nearest Pinnacle center
Teleconsultation (Remote Families)
45-minute video consultation with Pinnacle OT. Protocol setup, material selection guidance, troubleshooting support for families anywhere in India and beyond. → pinnacleblooms.org/teleconsult | Call: 9100 181 181
EverydayTherapyProgramme™ (Digital)
AI-guided daily home program generated from your child's AbilityScore®. Sessions arrive on your phone each morning. OT-designed, GPT-OS® personalized. → pinnacleblooms.org/everyday
📞FREE National Autism Helpline: 9100 181 181 | Available 24×7 | 16+ languages | No appointment needed. "Consistency across home and clinic is the multiplier that transforms outcomes."

Consistency Across All Caregivers Multiplies Impact.
"A technique practiced by one parent, undone by one grandparent, is a technique practiced by zero people."
Share This Page
- 📲unknown link
- 🔗 Copy link: techniques.pinnacleblooms.org/sensory/poor-body-awareness-A-109
- 📥unknown link (simplified version for spouses, grandparents, and school teachers)
"Explain to Grandparents" Summary
"The doctor says [child's name] has difficulty feeling where their body is in space. It's not naughtiness. The therapy is to give their body more physical input — heavy lifting, tight clothing, deep pressure. When you see them carrying heavy things or asking for firm hugs, please support it. Don't stop it."
Teacher Communication Template
"Dear [Teacher], [Child's name] is receiving OT for proprioceptive processing. A 2-minute heavy work break (wall push-ups, carrying stack of books) before demanding seat work can significantly improve focus and reduce bumping in the classroom. This is supported by research and prescribed by our OT."

ACT VI: START NOW
The Session That Builds Your Child's Body Map Starts Today.
You now hold 40 cards of scientific guidance drawn from 21 million therapy sessions, 16 systematic reviews, and the combined wisdom of occupational therapists, speech-language pathologists, ABA specialists, special educators, and neurodevelopmental pediatricians. Use it.
📱 Your personalized A-109 session plan — generated from your child's AbilityScore® in 3 minutes
📞FREE National Autism Helpline: 9100 181 181 | 24×7 | 16+ Languages | No appointment needed. ✦ Validated by the Pinnacle Blooms Consortium ✦ OT • SLP • ABA/BCBA • SpEd • NeuroDev Pediatrics • CRO • WHO/UNICEF Aligned
Preview of 9 materials that help with poor body awareness Therapy Material
Below is a visual preview of 9 materials that help with poor body awareness therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.







Link copied!

🌸 Pinnacle Blooms Network® — The Pinnacle Promise
Our Mission
"From fear to mastery. One technique at a time."
We exist to transform every home into a 24×7 personalized, multidisciplinary, evidence-based therapy environment — so no child anywhere in the world loses developmental time to resource barriers.
What you hold in this page: 40 cards. 6 acts. 8 weeks of scientific guidance. Drawn from 21 million therapy sessions, 16 systematic reviews, and the combined wisdom of occupational therapists, speech-language pathologists, ABA specialists, special educators, neurodevelopmental pediatricians, and the mothers who built this system.
You are now a more effective therapeutic partner for your child than you were when you landed on Card 01.
Navigate Forward
- → unknown link
Contact
Medical Disclaimer
This content is educational and for informational purposes only. It does not replace assessment, diagnosis, or treatment by a licensed occupational therapist, developmental pediatrician, or qualified healthcare professional. Body awareness deficits require individualized professional evaluation. Individual outcomes vary based on diagnosis severity, consistency of intervention, and child profile. Always consult your child's healthcare team before implementing new therapeutic strategies.
Statutory Identifiers
CIN: U74999TG2016PTC113063 | DPIIT: DIPP8651 (Govt. of India) | MSME Udyog Aadhaar: TS20F0009606 | GSTIN: 36AAGCB9722P1Z2
© 2025 Pinnacle Blooms Network®, unit of Bharath Healthcare Laboratories Pvt. Ltd. GPT-OS®, AbilityScore®, TherapeuticAI®, FusionModule™, EverydayTherapyProgramme™ are registered/filed trademarks and proprietary systems. All rights reserved. Patents filed across 160+ countries.
techniques.pinnacleblooms.org | A-109 | Version 2.0 | February 2026 | GPT-OS® Content Engine