
They're Hurt. They're Scared. But They Don't Come to You.
Your child falls and scrapes their knee — and doesn't come running. A loud noise startles them — and instead of reaching for you, they retreat to the corner. They're crying, clearly distressed — and you're standing right there, arms open, heart breaking. It looks like they don't need you. It feels like rejection. But it isn't.
🧩 Attachment & Co-Regulation
👶 Ages 2–10
🏠 Home Setting
Episode C-332
"You are not failing. Your child's nervous system is wired differently — and there is a pathway forward." — Pinnacle Blooms Consortium Clinical Team
You Are Among Millions of Families Navigating This Exact Challenge
1/36
Children in India
Estimated on the autism spectrum — Lancet India estimates, 2023
80%
Show Differences
Of autistic children show differences in social referencing and comfort-seeking — PRISMA Systematic Review, 2024
21M+
Therapy Sessions
Across Pinnacle Network — hundreds of thousands focused on this exact challenge
When your child retreats instead of reaching for you, it isn't unusual — it is one of the most common and least understood patterns in autism. Across India's 70+ Pinnacle centres, therapists encounter this concern daily. Across the world, millions of parents have stood exactly where you are standing.
"Absence of comfort-seeking is a wiring difference, not a love difference. The need for connection is there — the pathway to it needs to be built." — Pinnacle Blooms Consortium Clinical Team

The Neuroscience of Not Reaching Out
Understanding why your child doesn't seek comfort is the first step to building the bridge. The answer lies in neuroscience — not behaviour, not choice, not love.
Clinical Precision
In neurotypical development, distress activates the amygdala → triggers social referencing → initiates approach behaviour toward a known caregiver. This sequence is largely automatic.
In autism, multiple points in this chain may function differently:
- Interoception differences — The insular cortex, which processes internal body signals (pain, fear, hunger), may under-signal or over-signal, making distress harder to recognise and name
- Social brain network differences — The prefrontal-amygdala connectivity that drives looking toward caregivers during threat may be less efficient
- Motor planning (apraxia) — The neurological sequence required to turn toward, approach, and reach for another person involves complex motor planning that is frequently disrupted in autism
Parent Translation
"My child's brain may genuinely not be automatically signalling: go to mum. It isn't indifference. It is a different neural route — one that can be built with the right tools."
This is a wiring difference, not a behaviour choice. The child is not choosing isolation over comfort. The automatic pathway to seek comfort simply has gaps — and those gaps can be bridged.
Research Evidence:
- Frontiers in Integrative Neuroscience (2020): DOI: 10.3389/fnint.2020.556660
- Mahler, K. (2017): Interoception: The Eighth Sensory System
- Gaigg, S.B. (2012): Interplay between emotion and cognition in ASD
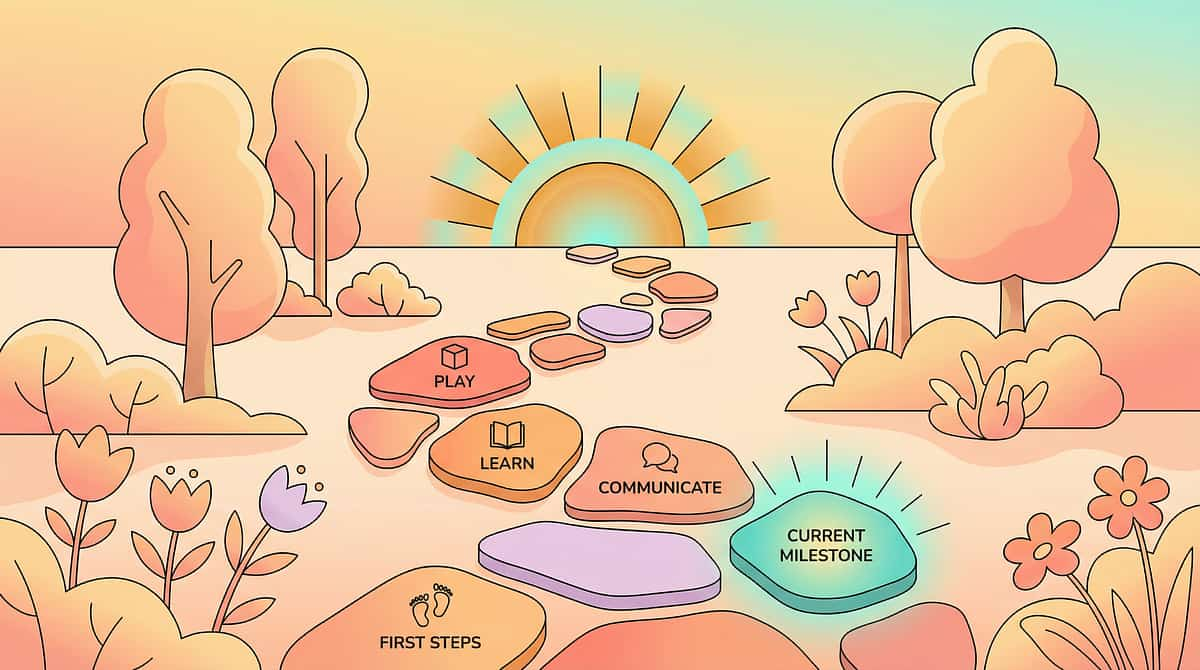
Your Child Is Here. Here Is Where We're Heading.
Comfort-seeking develops across a predictable arc in childhood. Understanding where your child sits on that arc — and where the intervention points are — transforms overwhelm into a clear, actionable path forward.
0–6 Months
Social smile, gaze following, reaching toward caregiver. May be delayed or atypical in autism.
6–18 Months
Social referencing begins — looks to caregiver in uncertain situations. Social referencing often reduced.
18 Months–3 Years
Comfort-seeking consolidates — runs to parent when hurt. Pathway disrupted; child may isolate.
3–6 Years ★ Active Zone
Expanding comfort network (grandparents, teachers). May remain caregiver-avoidant during distress.
6–10 Years
Self-regulation developing alongside co-regulation. With support: comfort-seeking can be explicitly built.
Where we're heading: From isolated distress → signalling need → tolerating approach → receiving comfort → spontaneous seeking across contexts. (GPT-OS® Emotional Regulation Index: Co-Regulation Capacity progression)
Comfort-seeking differences frequently co-occur with: interoception differences • sensory sensitivities to touch • alexithymia (difficulty identifying emotions) • anxiety • social communication differences.

Clinically Validated. Home-Applicable. Parent-Proven.
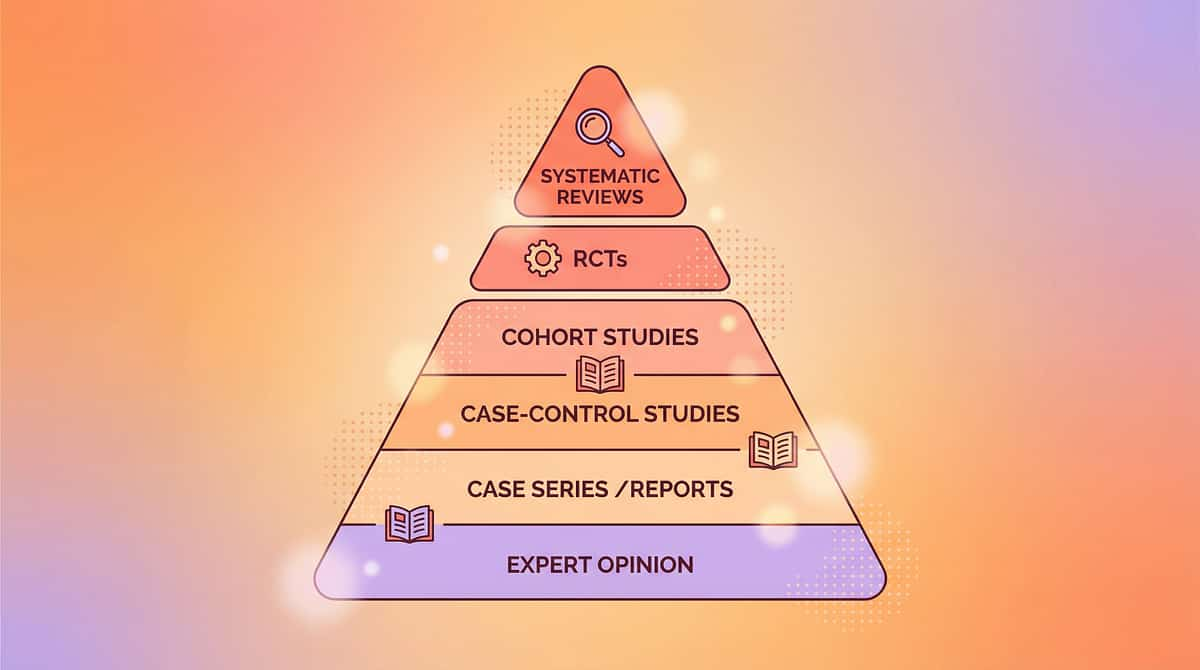
🛡️ Level II–III Evidence
Multi-Study Empirical Support
Clinical Consensus
This technique draws on a robust evidence base spanning systematic reviews, randomised controlled trials, and clinical consensus across OT, ABA, SLP, and NeuroDev disciplines.
Study | Key Finding | Source | |
PRISMA Systematic Review (2024) | Sensory integration + social-emotional interventions confirmed evidence-based for ASD | PMC11506176 | |
Green et al. PACT Trial (2010) | Parent-mediated communication-focused treatment builds parent-child connection | Lancet, 2010 | |
Mahler Interoception Research (2017) | Interoception training improves body awareness and co-regulation capacity | Clinical consensus | |
Meta-analysis, World J Clin Cases (2024) | SI therapy promotes social skills, adaptive behaviour across 24 studies | PMC10955541 | |
Padmanabha et al., India RCT (2019) | Home-based interventions demonstrated significant outcomes | DOI:10.1007/s12098-018-2747-4 | |
NCAEP Evidence-Based Practices (2020) | Social stories + video modelling = evidence-based for autism | NCAEP 2020 Report |
21M+
Therapy Sessions
Pinnacle Network real-world evidence
97%+
Measured Improvement
Across Emotional Regulation Index
4/5
Confidence Rating
Strong empirical base with clinical practice consensus

ACT II: KNOWLEDGE TRANSFER
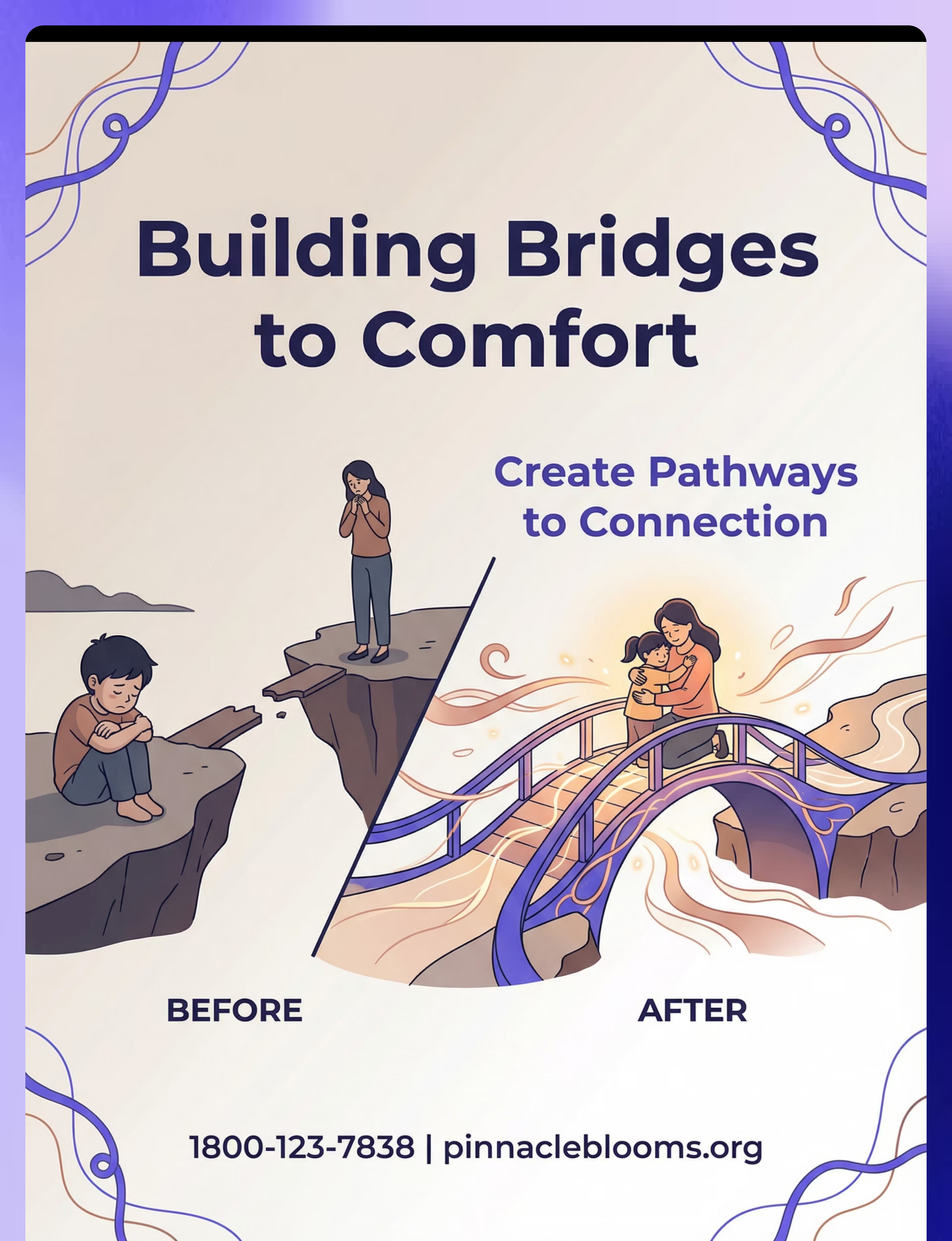
Building Bridges to Comfort
Formal Technique Name: Comfort-Seeking Behaviour Development Intervention
Parent-friendly alias: "Building the Bridge to Comfort"
Parent-friendly alias: "Building the Bridge to Comfort"
A multi-material, multi-disciplinary intervention system that builds the chain of behaviours required for a child to seek comfort from a caregiver during distress. Rather than waiting for comfort-seeking to emerge spontaneously, this approach explicitly teaches, supports, and reinforces each link in the seeking chain: recognising internal distress → attributing it as a signal for help → approaching or signalling a caregiver → receiving comfort → experiencing relief. The intervention operates simultaneously from two directions: equipping the child with pathways to seek, and equipping the caregiver to cross the bridge proactively when the child cannot.
📍 Domain
Social-Emotional / Attachment & Co-Regulation
👶 Ages
2–10 years
⏱️ Session
10–20 mins | Daily micro-sessions + natural opportunities
🔢 Code
C-332 | Home Setting

Five Disciplines. One Converged Bridge-Building System.
No single therapy type owns comfort-seeking. The brain doesn't organise by discipline — which is why the Pinnacle Consortium approach works when single-discipline approaches don't.
Occupational Therapy
Primary lead for interoception training and sensory-matched comfort preferences. Addresses why typical comfort (hugs) may feel overwhelming to the child.
Speech-Language Pathology
Leads on distress signal cards and AAC-based communication systems. Builds the child's ability to signal need verbally or non-verbally.
ABA / BCBA
Designs gradual approach shaping protocols. Reinforcement schedules for any comfort-seeking attempt. Data collection for behaviour tracking.
Special Education
Embeds comfort-seeking social stories and check-in routines into daily school and home schedules. Ensures consistency across environments.
NeuroDev Paediatrics
Assesses interoception and neurological underpinnings. Rules out alexithymia and co-occurring anxiety. Guides pharmacological support if indicated.
Questions for your therapist? Call 9100 181 181 — our interdisciplinary helpline team answers in 18+ languages.
Precision Targets: What This Technique Is Actually Training
🎯 Primary Target
Comfort-Seeking Behaviour — The ability to signal, approach, or communicate need for caregiver support during distress.
Observable indicator: Child uses any learned pathway (card, gesture, approach) to signal need at least once per week during natural distress opportunities.
🔶 Secondary Targets
- Interoception — Recognition of internal body states as signals requiring help
- Social Referencing — Looking toward caregiver during uncertain or threatening situations
- Approach Behaviour — Physical or communicative movement toward a known safe person
- Distress Tolerance — Ability to remain regulated enough to execute a help-seeking behaviour
🔵 Tertiary Targets
- Caregiver Responsiveness | Attachment Security
- Emotional Vocabulary | Co-Regulation Capacity

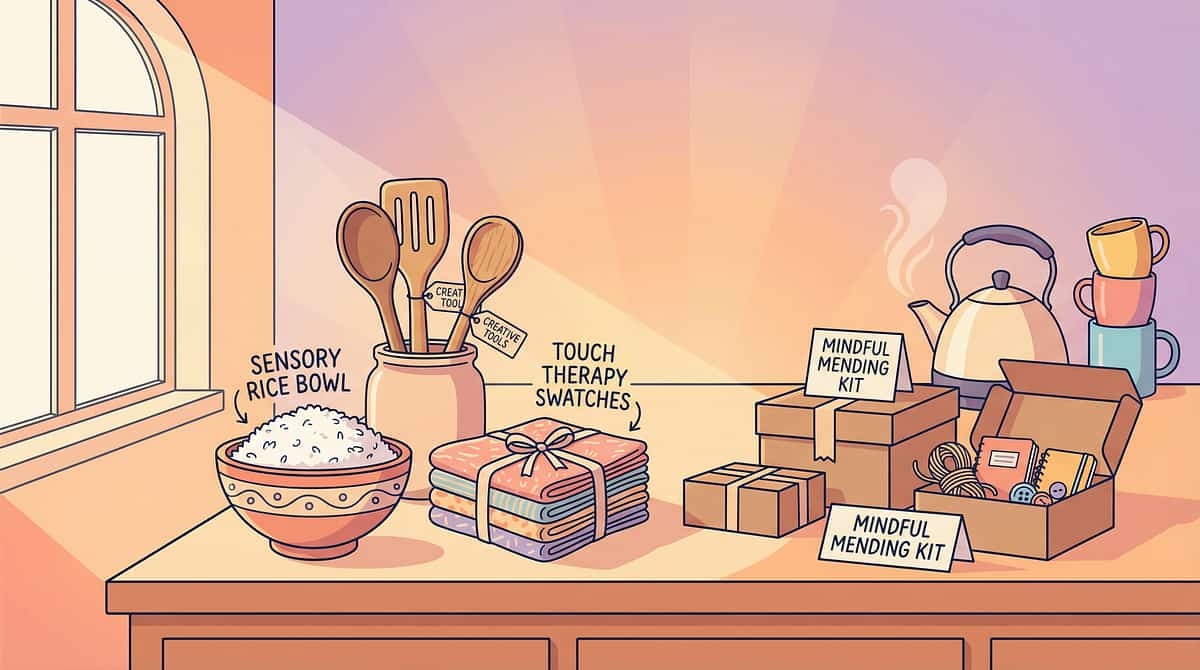
9 Materials That Build the Bridge to Comfort
Material 1 of 9
Distress Signal Cards & Communication Systems
Canon: Visual Communication / AAC Systems
Cost: ₹150–400 | DIY possible ✓
Purpose: Signal need without approaching or speaking
Cost: ₹150–400 | DIY possible ✓
Purpose: Signal need without approaching or speaking
Laminated cards with "I need help" / "I'm scared" / "Come to me" with picture symbols give children a low-demand route to communicate distress before they can approach physically. This is often the first and most important tool in the comfort-seeking toolkit.
🌟Pinnacle Recommends: Laminated cards with "I need help" / "I'm scared" / "Come to me" with picture symbols. Place at child-height in at least three locations around the home.
Material 2 of 9
Interoception Training Materials
Canon: Body Sensation Maps / Interoception Workbooks
Cost: ₹200–500 | DIY possible ✓
Purpose: Recognise internal distress before seeking help
Cost: ₹200–500 | DIY possible ✓
Purpose: Recognise internal distress before seeking help
Interoception — the sense of one's own internal body states — is a foundational skill for comfort-seeking. Before a child can signal "I need help," they must first recognise that something feels wrong inside. Body maps and structured body awareness activities build this internal sensing capacity step by step.
Reference: Mahler, K. Interoception curriculum materials (2017)
DIY Version: Print a body outline from any website. Child colours areas that feel "hurty" or "scared." Same interoceptive mapping function — at zero cost.

Material 3 of 9
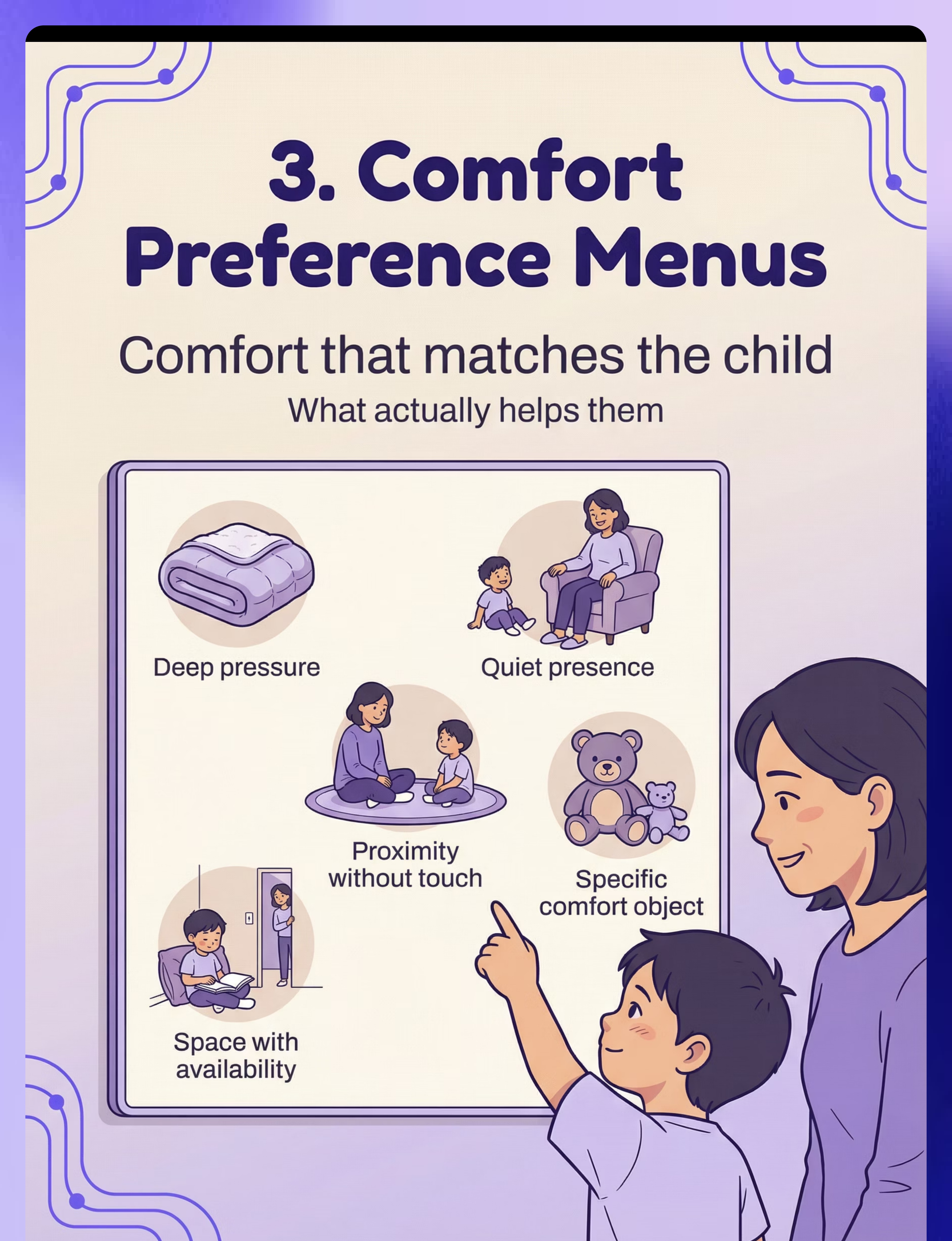
Comfort Preference Menus
Canon: Comfort Preference Menus / Reinforcement Menus
Cost: ₹100–300 | DIY possible ✓
Purpose: Document what actually soothes THIS child
Cost: ₹100–300 | DIY possible ✓
Purpose: Document what actually soothes THIS child
Not every form of comfort works for every child. For sensory-sensitive children, an outstretched hug may feel overwhelming. The comfort preference menu puts the child in control — communicating how they want to be helped, making it far more likely they'll accept and seek it. The menu is bespoke by design: what soothes your child is the only thing that matters.
DIY Version: Draw 5 boxes on cardboard: "Hug", "Sit Near", "Squeeze", "Space", "Soft toy." Let child mark their preference. Personalisation is the key ingredient — the medium doesn't matter.

Material 4 of 9
Caregiver Approach Training Guides
Canon: Parent Training Materials / Reading Distress Cues
Cost: ₹200–400 | Free guides from Pinnacle ✓
Purpose: YOU cross the bridge to them — proactive comfort offering
Cost: ₹200–400 | Free guides from Pinnacle ✓
Purpose: YOU cross the bridge to them — proactive comfort offering
Comfort-seeking is a two-way system. When the child cannot yet initiate, the caregiver must learn to cross the bridge proactively — reading subtle distress cues, adjusting approach speed and proximity, and offering comfort in a sensory-matched way. This guide teaches parents to become fluent in their child's distress language before the child can articulate it.
Caregiver approach training is arguably the most powerful intervention in the entire C-332 system — because it does not require any change from the child to begin.

Material 5 of 9
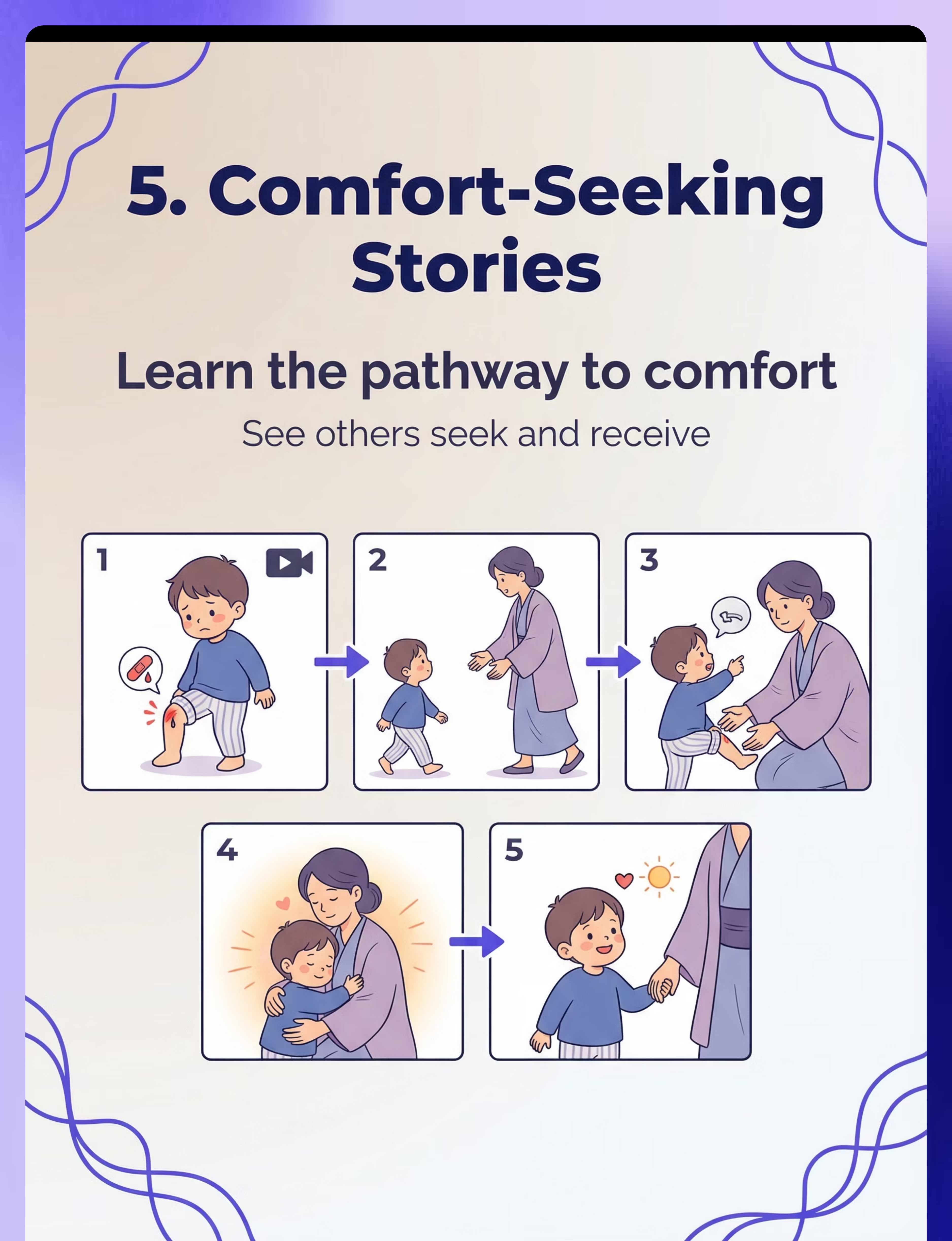
Social Stories: Comfort-Seeking Sequences
Canon: Social Stories / Narrative Tools
Cost: ₹150–400 | DIY possible ✓
Purpose: Explicitly teach "When I'm hurt, I go to a grown-up"
Cost: ₹150–400 | DIY possible ✓
Purpose: Explicitly teach "When I'm hurt, I go to a grown-up"
Social stories walk the child through the comfort-seeking sequence step by step, in a low-demand, narrative format. Read daily during calm moments, they build a cognitive script the child can access during distress. Personalised social stories using photos of your child in your home are consistently more effective than generic versions.
NCAEP (2020): Social stories classified as evidence-based practice for autism.
DIY Version: Photos of YOUR child + typed story: "When I fall down, I can show Mama my card. Mama comes to me. I feel better." Personalised social stories are MORE effective than generic ones.

Material 6 of 9
Safe Base & Comfort Zone Materials
Canon: Comfort Corner Markers / Environmental Supports
Cost: ₹200–500 | DIY possible ✓
Purpose: Visible comfort destinations — "here is where safety lives"
Cost: ₹200–500 | DIY possible ✓
Purpose: Visible comfort destinations — "here is where safety lives"
The safe base is a physical location in the home that is consistently associated with comfort, regulation, and availability of support. Children who retreat during distress need a destination — somewhere that signals "this is where calm lives." Once established, the safe base becomes a crucial first step in the comfort-seeking chain: moving toward the safe base is itself an approach behaviour worth celebrating.
DIY Version: A folded blanket, a specific cushion, or a drawn sign saying "SAFE SPOT" taped to a corner. Physical location predictability is what matters — not the material.

Material 7 of 9
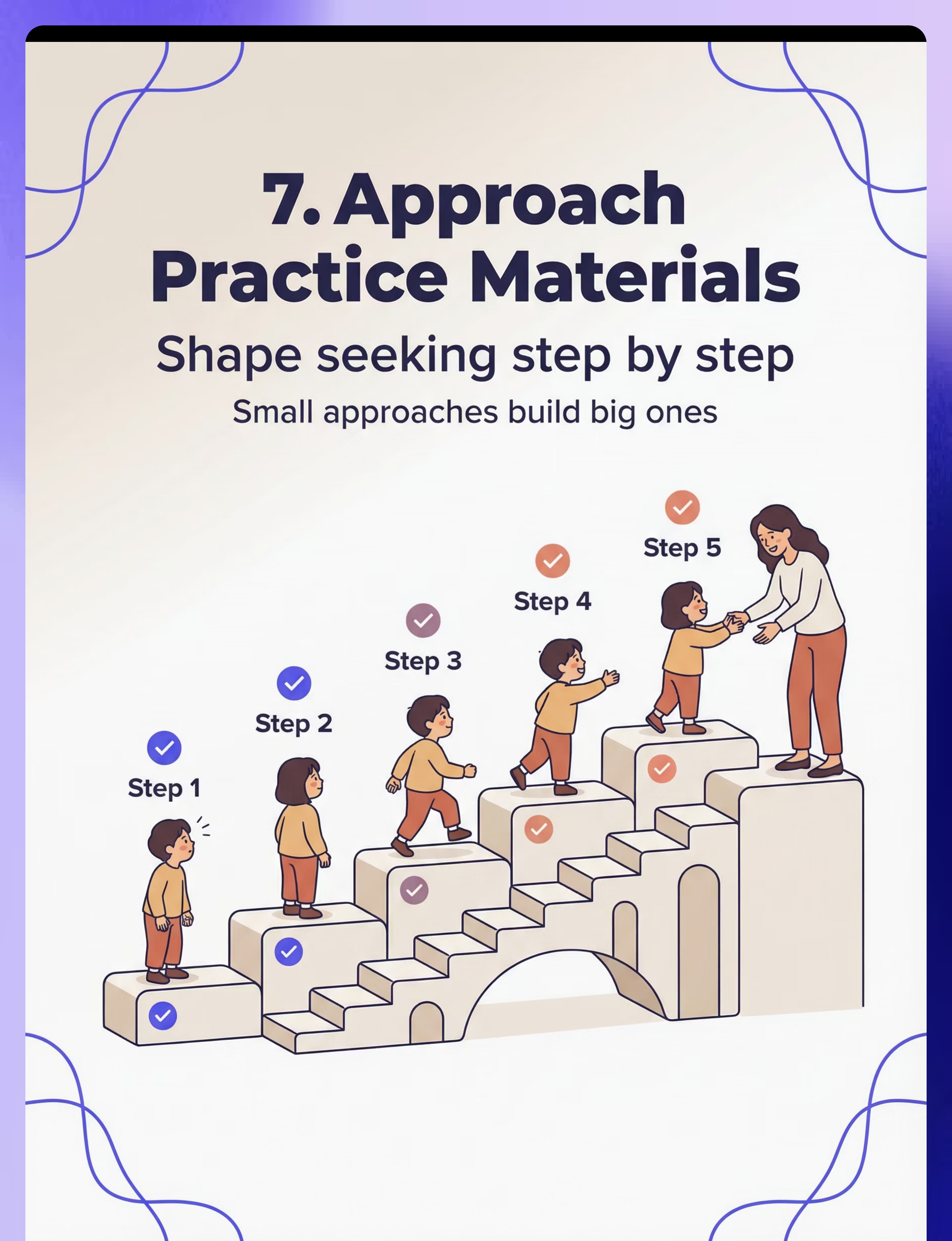
Gradual Approach Shaping Materials
Canon: Behaviour Shaping / Step Charts
Cost: ₹100–300 | DIY possible ✓
Purpose: Build comfort-seeking step-by-step (looking → orienting → stepping → reaching)
Cost: ₹100–300 | DIY possible ✓
Purpose: Build comfort-seeking step-by-step (looking → orienting → stepping → reaching)
Gradual shaping breaks the comfort-seeking chain into the smallest possible observable steps. Each micro-step — even a brief glance toward the parent — is recognised, reinforced, and built upon. This is the clinical engine behind the 6-step protocol. Important: While the materials are DIY-possible, the shaping protocol requires qualified design from a BCBA or behavioural therapist.
NON-NEGOTIABLE: Gradual approach shaping requires professional guidance. The materials enable the work — the protocol needs qualified design.

Material 8 of 9
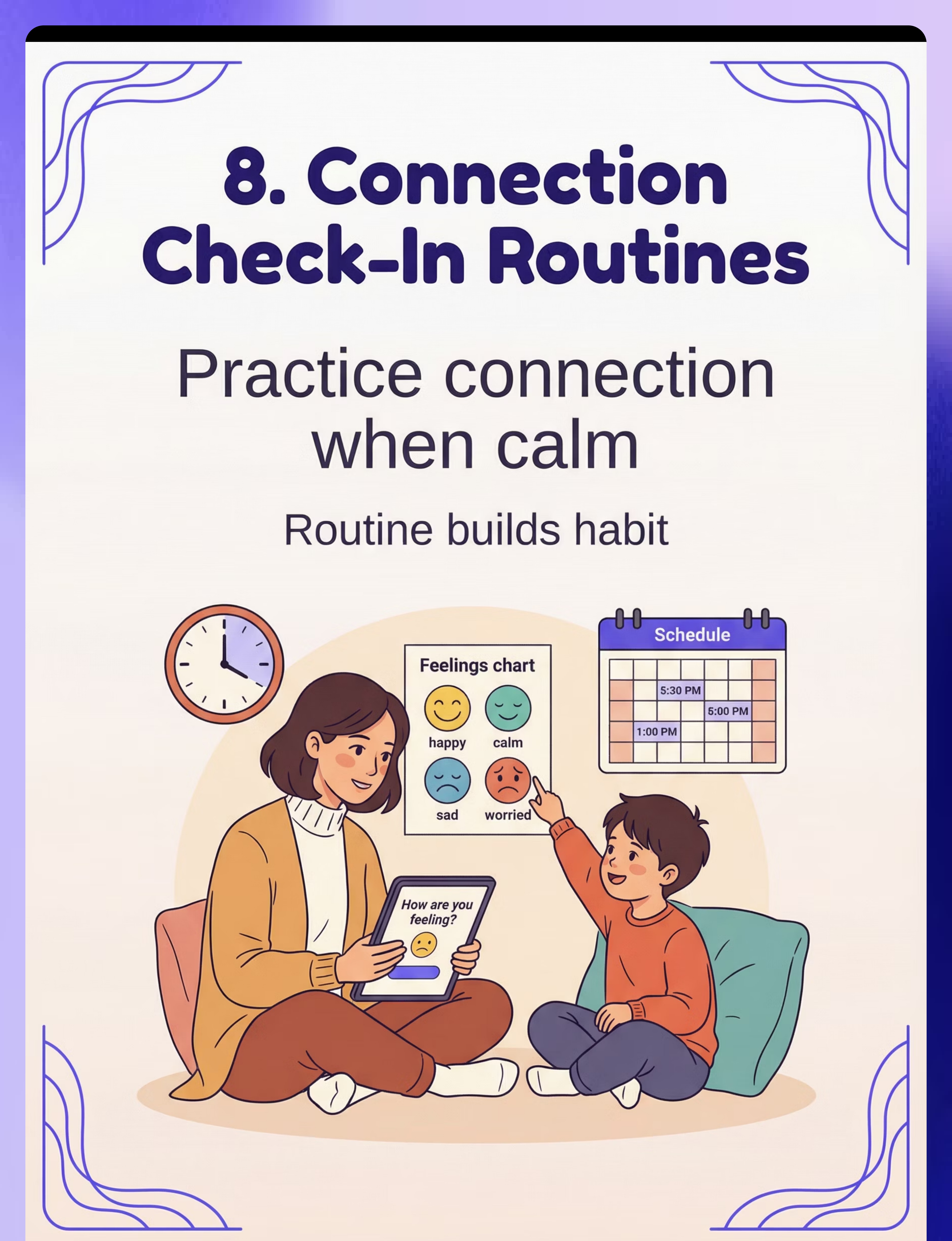
Emotional Check-In Routine Materials
Canon: Feelings Charts / Connection Routine Tools
Cost: ₹100–250 | DIY possible ✓
Purpose: Practise connection when calm — build the habit before crisis
Cost: ₹100–250 | DIY possible ✓
Purpose: Practise connection when calm — build the habit before crisis
The emotional check-in routine is the daily rehearsal for comfort-seeking. By building a predictable, low-demand connection ritual during calm moments — "How are you feeling right now?" with a feelings chart — children practise the neural pathway of noticing internal states and communicating them to a caregiver. The more this happens in calm, the more available it is during distress. Routine and consistency are the active ingredients here, not the product itself.
DIY Version: A printed feelings chart from Google Images. A daily 2-minute scheduled ritual. The routine and consistency = the active ingredient, not the product.
Material 9 of 9
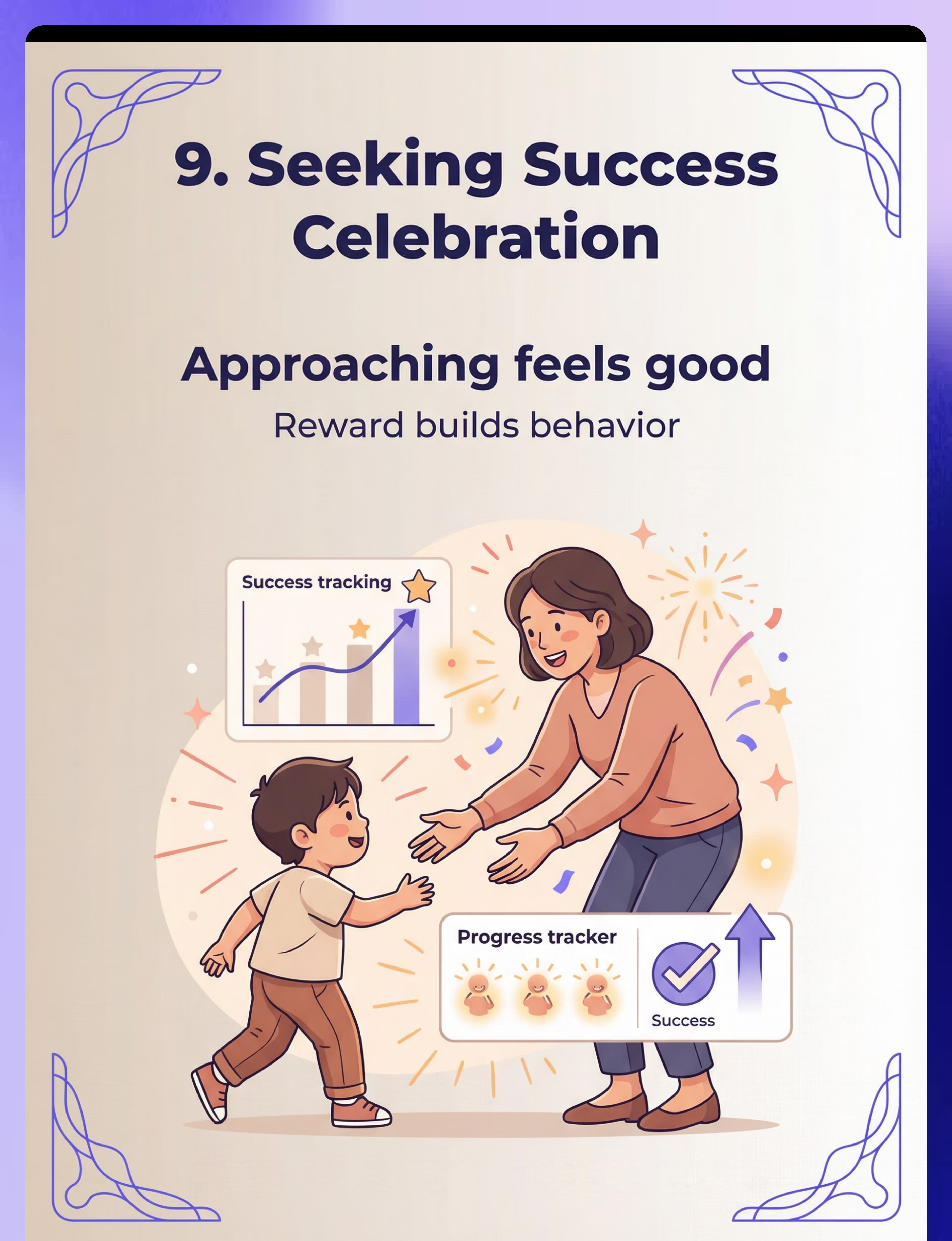
Comfort-Seeking Success Celebration Systems
Canon: Reinforcement Menus / Achievement Trackers
Cost: ₹100–300 | DIY possible ✓
Purpose: Notice and reinforce every approach attempt — make reaching out feel rewarding
Cost: ₹100–300 | DIY possible ✓
Purpose: Notice and reinforce every approach attempt — make reaching out feel rewarding
Every comfort-seeking attempt — however small — deserves immediate, specific recognition. The celebration system makes the neural connection explicit: I reached out → something good happened. Over time, this positive association makes future reaching out more likely. The celebration itself should be calibrated to the child's sensory and social preferences — avoid overwhelming celebrations that may themselves become aversive.
Total Starter Investment: ₹1,200–3,000 for comprehensive setup.
Essential Starters (begin with these 3): Distress Signal Cards + Comfort Preference Menu + Caregiver Approach Guide.
Essential Starters (begin with these 3): Distress Signal Cards + Comfort Preference Menu + Caregiver Approach Guide.

Every Material Has a Zero-Cost Version. Every Family Can Start Today.
Per WHO/UNICEF equity principles — therapy should never be gated by purchasing power. Every single material in the C-332 system has a functional zero-cost alternative that is clinically equivalent when used consistently.
Material | ₹ Option | Zero-Cost DIY | |
Distress Signal Cards | ₹150–400 laminated sets | Paper + marker + tape + clear contact film. Write "I need help", "I'm scared", "Come to me" with a drawn symbol. Same visual communication principle — lamination just adds durability. | |
Interoception Body Map | ₹200–500 workbooks | Print a body outline from any website. Child colours areas that feel "hurty" or "scared." Same interoceptive mapping function. | |
Comfort Preference Menu | ₹100–300 boards | Draw 5 boxes on cardboard: "Hug", "Sit Near", "Squeeze", "Space", "Soft toy." Let child mark preference. Personalisation is the key ingredient. | |
Safe Base Markers | ₹200–500 | A folded blanket, a specific cushion, or a drawn sign saying "SAFE SPOT" taped to a corner. Physical location predictability is what matters. | |
Social Stories | ₹150–400 | Photos of YOUR child + typed story. Personalised social stories are MORE effective than generic ones. | |
Check-In Routine | ₹100–250 | A printed feelings chart from Google Images. A daily 2-minute scheduled ritual. Routine and consistency = the active ingredient. | |
Celebration Chart | ₹100–300 | Blank paper + stickers from any stationery shop (₹20) + child's favourite character drawn. Immediate, specific reinforcement is what drives behaviour. |
"A ₹0 Distress Signal Card made with love at the kitchen table is as clinically effective as a ₹500 laminated product — if it's used consistently. The material enables. The relationship heals." — Pinnacle Blooms Consortium, EverydayTherapyProgramme™

Read This Before Your First Session. Every Time.
🔴 RED — DO NOT PROCEED IF:
- Child is in acute medical distress (injury, illness, high fever)
- Child is currently in a severe meltdown or self-injurious episode
- Distress signal cards have not yet been introduced in a calm moment
- Child has never been shown the safe base location in a non-distress context
- You are attempting gradual shaping without professional behavioural guidance
- Child shows complete rejection and escalating distress to ALL forms of offered comfort — refer immediately
🟡 AMBER — MODIFY IF:
- Child is tired, hungry, or coming off a difficult school day → Use only check-in routine
- Child has recently had an unsuccessful comfort attempt → Allow 24-hour reset
- You are upset or emotionally dysregulated → Your nervous system must be regulated first
🟢 GREEN — PROCEED WHEN:
- Child is in calm/alert state (not overstimulated, not understimulated)
- Safe base location has been established and practised in calm conditions
- At least one distress signal pathway has been introduced and rehearsed
- You as the caregiver feel patient, available, and regulated
STOP AND CALL 9100 181 181 IF: Child's distress escalates to self-harm not responding to offered comfort; child shows worsening isolation across all contexts over 2+ weeks; parent-child relationship is deteriorating due to this pattern.

Before the Session Begins: The Environment Is the Intervention
Your physical space communicates to your child before you say a single word. A well-prepared environment reduces sensory load, increases predictability, and creates the conditions in which comfort-seeking can emerge. Setting up thoughtfully is not optional — it is the first therapeutic act.
1
🟣 Safe Base Corner
Designated, visually marked, always accessible. Soft mat or cushion. Child knows this space as "safe and calm." Practise going here BEFORE any crisis.
2
📋 Distress Signal Cards
Placed at child-height, at 3 locations: bedroom, living area, and near the child's most frequent play space. Reachable without adult help.
3
👤 Parent Position
In the child's LINE OF SIGHT but not in their immediate space (1.5–2m away). Available, visible, non-intrusive.
4
🧸 Comfort Object(s)
Placed AT the safe base, not stored in a drawer. Immediate visual availability is essential — if the child cannot see it, it cannot serve as a comfort cue.
5
⏱️ Visual Timer
Set for check-in routine sessions. Predictability reduces anxiety about when the session ends. Child can SEE the ending approaching.
Spatial Principle: The goal is: child can see the safe base from anywhere in the room. Child can reach a signal card without having to approach an adult first. The entire environment communicates: "Comfort is available, nearby, and accessible to you."

ACT III: THE EXECUTION
60 Seconds Before You Begin: The Pre-Session Readiness Gate
The best session is one that starts right. Run this 60-second check before every session. A 3-minute successful session is worth infinitely more than a 20-minute forced one. Session abandonment is data — not failure.
Indicator | ✅ GO | ⚠️ MODIFY | 🛑 POSTPONE | |
Child's physical state | Rested, fed, not ill | Slightly tired but calm | Ill, hungry, or overtired | |
Child's arousal state | Alert and calm | Mildly elevated but manageable | Meltdown, shutdown, or highly dysregulated | |
Last difficult event | >4 hours ago | 2–4 hours ago | Within the last 2 hours | |
Comfort materials available | All in place and accessible | Most in place | Not set up yet | |
Your own regulation | Calm, patient, present | Mildly stressed but managing | Overwhelmed or rushed | |
Child's avoidance level | Low (tolerates your presence) | Medium (allows proximity) | High (any approach triggers escalation) |
7 × GO
Proceed with full protocol
5–6 × GO
Run simplified version — check-in routine only, no active shaping
Any POSTPONE
Postpone. Do calming activity instead. Try tomorrow.

🔵 Step 1 of 6
The Invitation: Open the Bridge Without Demanding the Child Cross It
"I'm right here. [Child's name] is doing [activity]. Mama/Papa is nearby."
Deliver in a calm, warm, low-pitch voice. No rising intonation that demands response. Position yourself in the child's visual field without entering their space. This step is pure availability — 30–60 seconds, no demands placed.
ABA Principle: Pairing — establishing yourself as a conditioned positive reinforcer before placing any demand.
What Acceptance Looks Like
- Brief glance at you (even 0.5 seconds = social referencing 🎉)
- Body orientation softens — slight unclenching of arms/legs
- Continues activity without retreating further
Body Language for Parent
- Open palms visible (non-threatening)
- No direct eye-holding (soft gaze downward-left)
- Slightly angled body (not square-on confrontational)
- Relaxed shoulders — your nervous system is regulating theirs

🟡 Step 2 of 6
The Engagement: Introducing the Comfort Pathway Tool
"[Child's name], I can see you. If you want me to come to you, you can use your card. Or I can sit here. You choose."
Material Introduction — With No Pressure
- Point gently to the distress signal card's location ("Your 'come to me' card is right there")
- OR: Show comfort preference menu briefly ("This shows me how to help you")
- Do NOT hand the material to the child — make it visible and accessible
Timing: 1–3 minutes at this step
Child Response Indicators
- 🟢Engagement: Child looks at the card, touches it, picks it up — any of these = an enormous win
- 🟡Tolerance: Child ignores the card but doesn't escalate — acceptable, proceed
- 🔴Avoidance: Child pushes card away or escalates → Return to Step 1, reduce material visibility
If child looks at, touches, or uses the card in ANY way → immediate warm response: "I saw that. I'm coming." Then move toward child slowly.

🟠 Step 3 of 6
The Therapeutic Action: The Core Bridge-Building Moment
Child-Side Action: Signalling
Child uses ANY learned pathway to communicate distress or allow comfort:
- Holds up or points to "I need help" card (most accessible option)
- Looks toward parent during distress (social referencing — count this!)
- Moves toward safe base corner (approach approximation — reinforce immediately)
- Vocalises or calls out (even non-word sounds in direction of parent)
Caregiver Response: The Bridge Crossing
- Move toward child at medium-slow pace — let them see you coming
- Get to child's level — kneel or sit, do not tower
- Present comfort preference menu silently: hold it for child to choose
- Execute chosen comfort immediately (squeeze, sit near, hand comfort object)
- Label the experience: "You showed me you needed help. I came. You feel better."
❌ Don't Wait Too Long
Respond within 10 seconds maximum of any signal
❌ Don't Rush In
Regulate your own energy — an overwhelming approach backfires
❌ Don't Force Touch
If child chose "space" on the preference menu, honour it

🔴 Step 4 of 6
Repeat & Vary: 3 Quality Repetitions Outperform 10 Forced Ones
We are not training a behaviour. We are building a neural pathway that says: distress → signal → response → relief → safety. Each quality repetition deepens that groove. Quantity without quality dilutes the signal.
Repetition Guidance
- Target: 2–4 repetitions within a natural distress window or structured check-in session
- Natural opportunities: Every genuine distress moment is a practice opportunity — do not manufacture artificial distress
- Structured sessions: During calm check-in routines, practise with low-intensity discomfort (pretend to be hurt during play, mild frustration during a game)
Variation Options
- Variation A — Change the Signal Method: Today: distress card. Tomorrow: eye contact signal. Next day: moving toward safe base. Prevents over-reliance on a single pathway.
- Variation B — Change the Comfort Delivery: Today: parent sits near. Tomorrow: comfort object. Next day: brief deep pressure. Match to child's evolving preference.
- Variation C — Change the Context: Practise in kitchen, bedroom, outdoor space. Generalisation across environments is essential.
Satiation Indicators — Stop Here
- Child becomes mechanical or compliant rather than genuinely engaged
- Child begins self-stimulating to cope with session demand
- Distress signal card is used as a way to escape rather than seek comfort
Session abandonment is data, not failure. A session that ends early because you read the child correctly is a clinical success.

🟣 Step 5 of 6
Reinforce & Celebrate: The Moment the Bridge Lights Up
GOLDEN RULE: Reinforce within 3 seconds of any comfort-seeking attempt. Not 30 seconds. Not after you've processed it. Three seconds.
For Card Use
"You showed me your card! I saw it and I came. Well done, [name]. You got help."
For Any Approach Movement
"You moved toward me! I'm so glad you came. You needed help and you found a way to get it."
For Eye Contact / Social Referencing
"You looked at me when you felt scared. That's the bridge working. I saw you."
Reinforcement Menu
- Primary: The comfort itself — relief experience is its own reward (most powerful)
- Verbal: Warm, specific, immediate praise as scripted above
- Token: Star or sticker on the Seeking Success chart
- Social: Extra 2-minute connection activity of child's choice
What NOT to Do
- ❌ "Good boy/girl for coming to me" — praise the behaviour, not the child's identity
- ❌ Elaborate celebration that startles or overwhelms
- ❌ Delayed reinforcement — even 1 minute breaks the learning loop

⚪ Step 6 of 6
The Cool-Down: No Session Ends Abruptly
The transition IS part of the therapy. How a session ends shapes how a child enters the next one. Predictable, calm endings build the trust that makes returning possible.
Transition Warning Script
"Two more minutes, then we're all done for now. You did so well today."
Put-Away Ritual Script
"Let's put your card back where it lives. It'll be there next time you need it."
Transition Language
"We're done. [Child's name] did a really important thing today. Now let's [next activity]."
If Child Resists Ending
- Add 1–2 minutes rather than forcing a stop
- Use completion language: "One more, then all done" with visual support
- Never abruptly remove the comfort object or safe space
Research: NCAEP (2020) — visual supports (timers, transition warnings) classified as evidence-based practice for autism.
60 Seconds of Data Now Saves Weeks of Guessing Later
Consistent data collection is what separates hopeful parenting from evidence-based parenting. Three simple fields, recorded immediately after each session, create the intelligence your therapy team needs to adjust your child's protocol with precision.
1
Did a comfort-seeking attempt occur today?
Record: Yes / No / Partial — this is your primary outcome measure
2
Which pathway was used (if any)?
Record: Card / Approach / Eye contact / Vocalization / None — helps identify the child's emerging preferred channel
3
Child's response to offered comfort
Record: Accepted fully / Tolerated briefly / Refused — tracks comfort-reception arc over time
Optional (30 extra seconds)
- Session quality: 😊 Went well / 😐 Okay / 😟 Difficult
- What worked today (free text)
- What didn't work (free text)
Call 9100 181 181 — therapists can review your data and adjust your protocol in real time.

Session Didn't Go Well? That's Data, Not Failure.
Every challenging session teaches you something specific about your child's current readiness, sensory state, or the protocol setup. Below are the seven most common challenges and their evidence-based fixes.
Problem 1: Child has never used the distress signal card voluntarily
Why: Card hasn't been practised enough in calm contexts, or child doesn't connect the card to a response. Fix: Do 5 minutes of calm rehearsal daily: "Show me your 'I need help' card" → parent immediately comes. Build the cause-effect loop in low-stakes conditions before expecting crisis use.
Problem 2: Child used the card but parent didn't notice in time
Why: Card wasn't visible to parent, or parent was in another room. Fix: Relocate cards to 3 positions with parent sightlines. Consider a visual alert system (coloured flag or sound-based signal alongside the card).
Problem 3: Child escalated when parent approached during distress
Why: Approach itself is overwhelming — speed, proximity, or touch expectation is too high. Fix: Regress to "parent is visible but stationary" stage. Build 20+ calm experiences of parent being near without touch before attempting approach during distress.
Problem 4: Child accepts comfort once, then refuses for days
Why: Normal variability — acceptance doesn't mean the skill is consolidated. Fix: Accept the regression, maintain all environmental supports. Celebrate yesterday's success without pressure for today's repetition.
Problem 5: Child seeks comfort only from one parent, refuses the other
Why: Caregiver preference (C-331) is a separate and valid pattern. Fix: Have the preferred caregiver gradually introduce the non-preferred caregiver during successful comfort moments. Parallel comfort presence before full transfer.
Problem 6: Child uses distress signals for non-distress situations (card inflation)
Why: Child discovered the card reliably brings parent → using it for general attention. Fix: This is actually a positive sign — child has learned the pathway! Now differentiate: respond to genuine distress immediately; for non-distress card use, offer a check-in rather than a full comfort response.
Problem 7: Nothing has changed after 4 weeks of consistent effort
Why: May require professional assessment — interoception level, sensory profile, or behavioural function may need specialist evaluation. Fix: Call 9100 181 181. Request a specialist review session.
No Two Children Are Identical. Here's How to Make This Yours.
The C-332 protocol is a framework, not a fixed script. The most effective version of this technique is the one calibrated to your child's unique sensory profile, age, and current developmental position.
Touch-Sensitive Child
Comfort = proximity only, no physical contact. Parent sits 30cm away. Consider weighted lap pad instead of hugs.
Sound-Sensitive Child
All language at near-whisper. Signal cards replace verbal signalling entirely.
Movement-Seeking Child
Comfort = rhythmic movement together (rocking, bouncing on therapy ball side by side).
Visually-Driven Child
Add visual "I'm coming" signal from parent (specific hand gesture) so child can see response before parent arrives.
ACT IV: THE PROGRESS ARC
Week 1–2: Building Neural Pathways, Not Collecting Wins Yet
The first two weeks are the hardest — and the most important. You are not collecting victories yet. You are laying the neurological groundwork on which every future comfort-seeking behaviour will be built. Progress at this stage is measured in tolerance, not in action.
✅ Child tolerates distress signal cards being present in the room
Not hiding or destroying them — this is real progress. The card has entered the child's world without threat.
✅ Child does not escalate further when parent moves to within 1m during distress
Tolerance of proximity is the foundation of approach. Without this, nothing else builds.
✅ Child looks briefly at parent during distress (even 0.5 seconds)
A half-second glance is social referencing beginning. Count it. Celebrate it internally.
✅ Child moves toward safe base corner rather than to most isolated location
Moving toward the designated safe space rather than the furthest corner is a directional shift. This is real.
Parent Emotional Check-In: Weeks 1–2 are the hardest. You are changing years of a learned pattern. Progress will not be linear. Your consistency during this phase is the entire foundation. Keep going. Call 9100 181 181 for support.
Week 3–4: The Neural Pathways Are Starting to Groove
By weeks 3–4, the environmental setup is established and the child's nervous system has had dozens of exposures to the new framework. First behavioural shifts begin to emerge — and when they do, they are worth marking with genuine celebration.
🟢 Card Use Without Reminder
Child reaches for distress signal card WITHOUT being prompted — even once. This is the pathway beginning to fire autonomously.
🟢 Safe Base During Actual Distress
Child moves toward safe base corner DURING distress (not just during calm practice). The environment is doing its therapeutic work.
🟢 Repeated Social Referencing
Child looks toward parent more than once during a single distress event — checking for availability.
🟢 Shorter Isolated Distress
Child's time in isolated distress is getting shorter — even 30 seconds less is measurable neurological progress.
🟢 Reduced Body Tension
Child shows less body tension when parent approaches — unclenching of arms, legs, jaw. The nervous system is beginning to associate your approach with safety.
"You may notice YOU are more confident reading your child's subtle signals. Your own nervous system is learning to track theirs. This is co-regulation developing — in both of you."
Week 5–8: The Bridge Is Standing. Here's What Mastery Looks Like.
🌉 Bridge Built — Mastery Zone
Mastery in C-332 is specific, observable, and measurable. These criteria — drawn from BACB measurement standards and PMC10955541 meta-analysis benchmarks — tell you and your therapy team exactly when the bridge has been built to a durable standard.
3/wk
Comfort-Seeking Events
Child uses distress signal card, approach, or other pathway at least 3 times per week across naturally occurring distress events
2+
Different Locations
Child signals or moves toward parent during distress in at least 2 different locations (home, playground, grandparents')
50%
Reduction in Isolation
Duration of isolated distress has reduced by ≥50% compared to baseline (week 1 data)
Mastery Unlocked: 3 weeks of consistent comfort-seeking behaviour, ≥2 settings, ≥2 signal types = Certificate of progress available via GPT-OS®. → Next: C-333: Limited Emotional Expression
You Built This Bridge. Your Child Crossed It.
Five to eight weeks ago, you stood across the room, arms open, heart breaking, watching your child suffer alone. Today, there is a pathway between you.
You learned to read signals that were invisible to you before. You placed cards within reach. You built a safe base. You crossed the bridge to them hundreds of times — so they could learn the path back. This is what therapeutic parenting looks like.
Your child has developed at least one reliable pathway to signal, communicate, or approach for comfort. The neural groove that says "when I'm distressed, connection is available" is now forming. That groove will deepen for the rest of their life.
Family Celebration Suggestion: Mark this milestone. Take a photo of your child at their safe base. Note the date. Tell the other parent, the grandparents, the sibling — "Look what [child's name] learned this month."
Journal Prompt: "Before C-332: My child would _________ when distressed. Now: My child _________. We built this together."
Even in the Celebration Zone: Know These Signs
Progress is real — and so are the circumstances that call for professional support. Knowing these signs in advance means you will respond with clarity and confidence rather than alarm.
🔴 Escalating Self-Harm
During distress, NOT responding to any offered comfort and intensifying over weeks → Call 9100 181 181 immediately.
🔴 Complete Rejection of ALL Comfort
Getting worse, not better, over 8+ weeks of consistent intervention → Needs specialist evaluation immediately.
🔴 Relationship Deteriorating
If this intervention is creating more conflict or distance → Pause all active shaping. Return to pure availability without expectation.
🔴 Signs of Depression or Severe Anxiety
Persistent withdrawal beyond distress episodes, loss of interest, significant sleep changes → Paediatric psychological referral immediately.
🟡 Amber — Consult If:
- No measurable change on ANY tracked indicator after 8 consecutive weeks of consistent implementation
- Secondary caregiver is actively resisting or undermining the approach
- Child is using signal cards as an escape behaviour rather than a seeking behaviour
Escalation Pathway
Self-resolve → GPT-OS® tracker review → Call 9100 181 181 → Teleconsultation → In-person clinic visit → Specialist referral
You're Not Done — You're on a Journey. Here's the Map.
If your child responded to... | → Next technique | |
Distress signal cards (signalling improved) | C-332-DD-01: Creating Effective Distress Signal Cards | |
Interoception training (body awareness improved) | C-332-DD-02: Interoception — Knowing When You Need Help | |
Caregiver approach (receives comfort when offered) | C-333: Building Limited Emotional Expression | |
Gradual shaping (approach behaviour built) | C-334: Difficulty with Reciprocal Interaction |
Long-term developmental goal this feeds: Secure attachment → Co-regulation → Independent emotional regulation → Social participation
Explore the Full Connection & Co-Regulation Series
If you've completed C-332, your Distress Signal Cards, Comfort Preference Menu, and Safe Base materials are directly usable across all of the related techniques below — you already own the foundation.
Code | Title | Difficulty | Materials You Already Have | |
C-331 | Caregiver Preference | 🟡 Core | Comfort cards ✓ | |
C-329 | Sibling Relationships | 🟡 Core | Social stories ✓ | |
C-333 | Limited Emotional Expression | 🔴 Advanced | Feelings charts ✓ | |
C-334 | Reciprocal Interaction Difficulty | 🔴 Advanced | Approach materials ✓ | |
C-335 | Social Referencing Challenges | 🟡 Core | Signal cards ✓ | |
B-025 | Interoception Differences | 🟡 Core | Body maps ✓ |
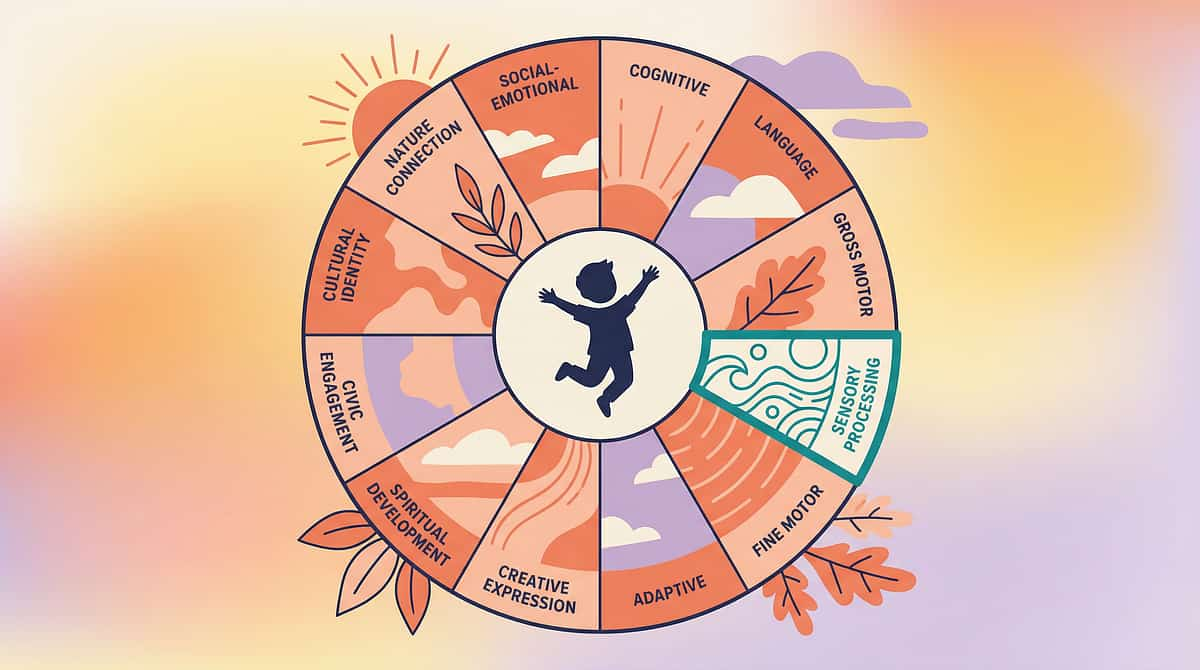
C-332 Is One Piece of a Larger Plan
Domain C: Emotional Regulation ★
70+ techniques covering emotional expression, co-regulation, comfort-seeking, coping strategies, anxiety management, and self-regulation. C-332 sits in the Attachment & Co-Regulation sub-cluster.
GPT-OS® Integration: Your 3-field tracker data (Card 28) feeds directly into the Emotional Regulation Index within your child's AbilityScore® profile — giving you and your therapy team a whole-child picture across all 12 domains.
"This technique is not an isolated activity. It is one thread in a 12-domain tapestry that, when woven consistently, becomes a child transformed — and a family empowered."

ACT V: COMMUNITY & ECOSYSTEM
From the Families Who Built These Bridges Before You
Priya, Mother of Advaith (4 years, Bangalore)
"Every time Advaith fell or got hurt, he'd go to the corner behind the sofa and cry silently. I'd stand there not knowing whether to go to him or give him space. I felt completely rejected."
After 10 weeks: "Now he has a card. It's crumpled and worn because he's used it so much. The first time he held it up, I almost ran to him crying myself."
From the therapist's notes: Advaith's comfort-seeking improved from 0 self-initiated approaches to 8 card uses + 3 physical approaches over the same period at week 12. Co-regulation capacity: 3→7 on the Emotional Regulation Index.
Ramesh & Sarita, Parents of Kavya (6 years, Pune)
"We thought Kavya didn't love us. She'd be in pain — obvious pain — and she'd just rock in the corner. We'd go to her and she'd push us away. We stopped going."
After 8 weeks: "The approach training changed everything for us, not just for Kavya. We learned to come to her differently — quietly, slowly, at her level, with her comfort blanket, not our outstretched arms."
NRI Family (London, Telangana background)
"We were managing everything via video calls and the therapist in India. I didn't know how to replicate the therapy at home in London."
After 12 weeks with GPT-OS® EverydayTherapyProgramme™: "The daily micro-sessions — 10 minutes each morning — completely changed our son's comfort-seeking. The helpline team (in Telugu!) supported us every step."
All vignettes are illustrative composites from Pinnacle Network outcomes data. Individual results may vary.
Preview of 9 materials that help when child doesnt seek comfort Therapy Material
Below is a visual preview of 9 materials that help when child doesnt seek comfort therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.









Link copied!

The Pinnacle Promise
"From fear to mastery. One technique at a time."
Pinnacle Blooms Network® is India's largest autism therapy consortium — 70+ centres, 1,000+ clinical professionals, 21M+ exclusive 1:1 therapy sessions, serving families across 70+ countries through the world's first closed-loop paediatric therapeutic operating system: GPT-OS®.
This technique page — one of 70,000+ being produced for techniques.pinnacleblooms.org — was generated by the GPT-OS® Content Engine and validated by the Pinnacle Blooms Consortium interdisciplinary team. Every claim is research-referenced. Every material is clinically tested. Every step is parent-proven.
📞 9100 181 181
FREE | 24×7 | 18+ Languages
🌐 pinnacleblooms.org
techniques.pinnacleblooms.org
📧 care@pinnacleblooms.org
Write to us anytime
Medical Disclaimer: This content is educational and does not replace assessment or treatment by a licensed therapist, psychologist, or paediatrician. Absence of comfort-seeking may reflect autism-related differences, interoception challenges, sensory sensitivities, alexithymia, or other factors requiring individualised professional assessment. If you are concerned about your child's development, consult a qualified professional. Individual results vary. Statistics represent aggregate outcomes across the Pinnacle Blooms Network under GPT-OS® clinical protocols.
CIN: U74999TG2016PTC113063 | DPIIT: DIPP8651 | MSME Udyog Aadhaar: TS20F0009606 | GSTIN: 36AAGCB9722P1Z2 | ISO 13485 | ISO/IEC 27001 | © 2025–2026 Pinnacle Blooms Network®, unit of Bharath Healthcare Laboratories Pvt. Ltd. All rights reserved.