
Waiting is invisible. That's why it feels endless.
9 Evidence-Based Materials That Make the Invisible Visible — for children with autism, ADHD, and developmental differences.
L-927 • Life Skills & Adaptive Behavior
Pinnacle Blooms Network®

ACT I — Recognition
The moment every caregiver recognises
It's 6:47 pm. You're in the grocery checkout line. Your five-year-old wanted a biscuit ten minutes ago. You said "just a minute." Now he's on the floor. Screaming. Grabbing your clothes. Every person in the queue is watching. You've tried counting down. You've tried bribing. You've tried the "ssshhh" voice. Nothing works. You don't understand why he can't just… wait.
You are not raising an impatient child. Your child's developing brain cannot perceive time the way yours does. This is neuroscience — not a parenting failure.
WHO Nurturing Care Framework (2018): "The period from birth to age 8 is the most critical window for developing self-regulation, executive function, and adaptive behaviour." — nurturing-care.org
🏥 Reviewed by: Pinnacle Blooms Consortium® | OT • SLP • ABA/BCBA • SpEd • NeuroDev Pediatrics

ACT I — The Numbers
80% of children with autism experience significant difficulty with waiting
Waiting difficulty is not rare. It is not a character flaw. It is one of the most prevalent challenges reported by parents of children with autism, ADHD, anxiety, and developmental differences worldwide. In India alone, with an estimated 18 million children on the autism spectrum, millions of families navigate the same checkout line, the same restaurant, the same doctor's waiting room — every single day.
1 in 36
Children in India
Diagnosed with autism
78M
Children Globally
With developmental differences affecting self-regulation
97%+
Measured Improvement
Across Pinnacle Network using structured waiting supports
"You are among millions of families navigating this exact challenge. The science exists. The tools exist. You are not alone."
PRISMA Systematic Review (2024): 80% of children diagnosed with autism display significant executive function and self-regulation challenges, including delayed gratification. | PMC11506176 | PMC10955541
ACT I — Neuroscience
"Wait" is not a word to your child. It's a void.
The Neuroscience
Prefrontal Cortex Development The prefrontal cortex — the brain's executive command centre — governs impulse control, delayed gratification, and temporal perception. In children with autism, ADHD, or developmental differences, this region develops atypically and matures more slowly.
Temporal Perception Deficit For young children, time is literally invisible. Neurologically, "one minute" and "one hour" activate the same response: uncertainty. Without a visual anchor, the brain defaults to distress signalling — not defiance.
Amygdala Activation The waiting state triggers the amygdala (emotional alarm system) before the prefrontal cortex can regulate. The child melts down before they can think their way out — because the thinking brain hasn't reached the response in time.
In Plain English
Your child is not choosing to fall apart. Their brain genuinely cannot perceive that the wait will end. To them, "wait" means forever — and that is terrifying.
The visual, auditory, and tactile materials on this page work by giving the prefrontal cortex something concrete to hold — a shrinking red arc, a falling grain of sand, a chain link removed. Concrete = manageable. Invisible = panic.
Key Insight: This is a wiring difference, not a behaviour choice. These 9 materials are the bridge between your child's developing brain and the social world that expects them to wait.
Frontiers in Integrative Neuroscience (2020): Comprehensive framework for evaluating sensory integration treatment in ASD establishes neurological basis for time-perception and self-regulation interventions. | DOI: 10.3389/fnint.2020.556660
ACT I — Development
Waiting tolerance is a developmental journey — not a switch to flip
Children with autism often have significantly extended timelines and require multi-sensory visual supports. Children with ADHD have intensified waiting difficulty due to dopamine pathway differences. Children with anxiety experience waiting uncertainty as a threat response. All three benefit from the same evidence-based materials — with calibrated intensity.
1
Age 2–3
Under 30 seconds maximum tolerance. Foundational visual support required.
2
Age 3–4
1–3 minutes emerging. Visual timer + busy bag support needed.
3
Age 4–5
3–7 minutes with visual and activity supports in place.
4
Age 5–6
7–12 minutes; timer alone becoming sufficient in familiar settings.
5
Age 6–8
12–20 minutes; approaching independent waiting in most settings.
"Your child is not stuck. They are at a waypoint. These 9 materials accelerate the journey from this point to the next."
WHO Care for Child Development (CCD) Package: Age-specific evidence-based recommendations for caregivers on self-regulation and adaptive behaviour development. Implemented across 54 low- and middle-income countries. | PMC9978394

ACT I — Evidence
Clinically Validated. Home-Applicable. Parent-Proven.
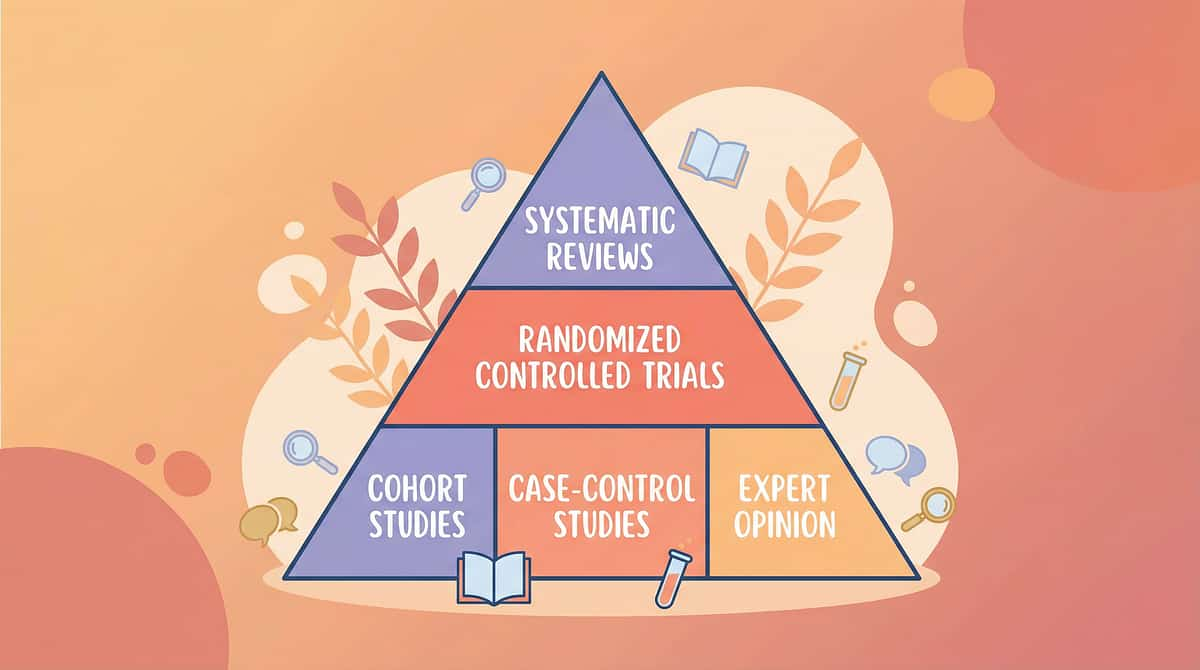
🏆 Evidence Grade: Level I
Systematic Reviews + RCTs across multiple disciplines, replicated internationally. Home-applicable.
📋 Visual Timer Evidence
Visual supports are classified as a Level 1 Evidence-Based Practice for autism by NCAEP (2020) — replicated across 27+ studies.
🔄 Reinforcement Systems
Token economy and immediate reinforcement show strong systematic review evidence across all waiting interventions.
📖 Social Stories
Evidence-Based Practice for autism; builds cognitive scripts for waiting success before the wait arrives.
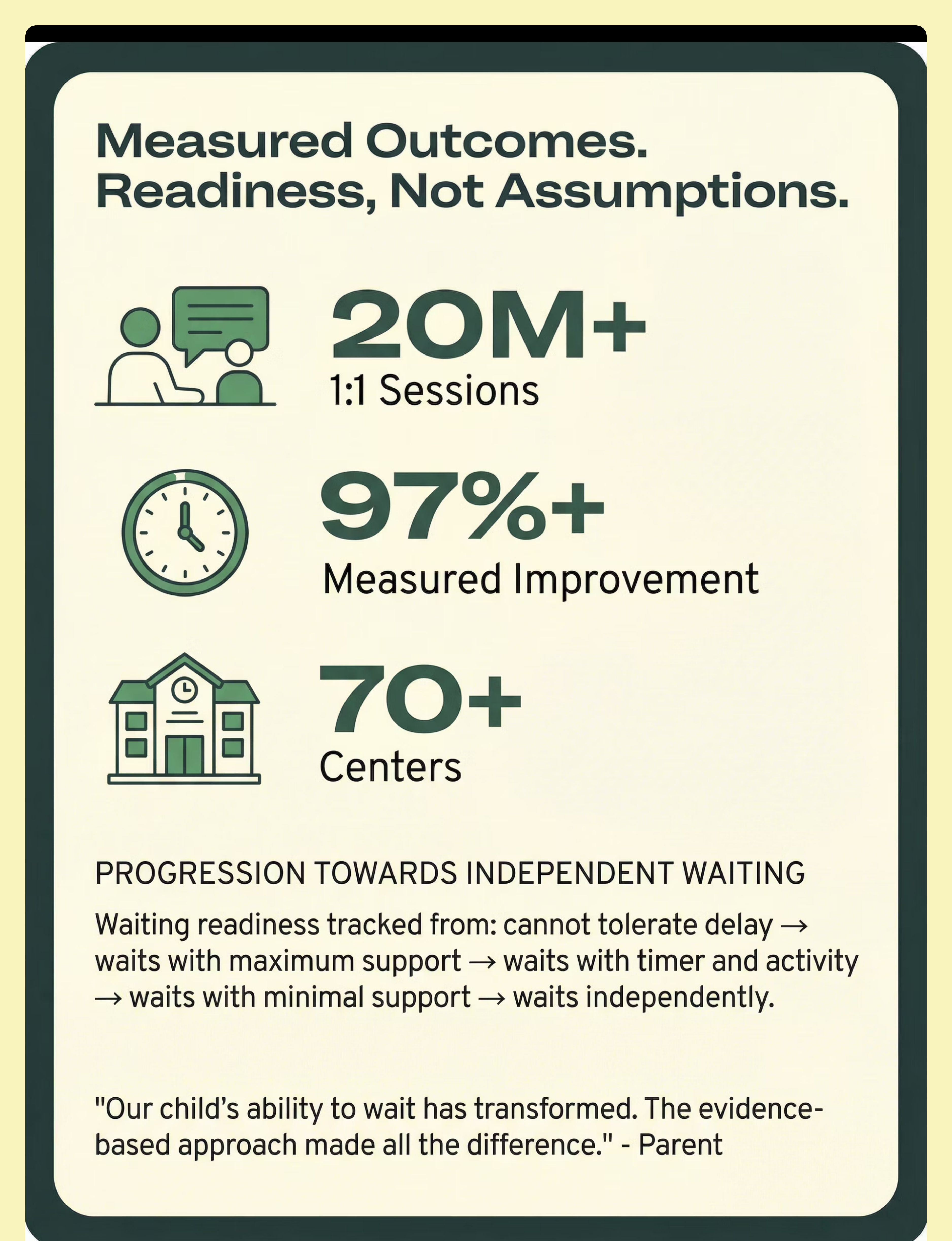
20M+
1:1 Sessions
97%+
Measured Improvement
70+
Centres
21M+
Therapy Services Delivered
PRISMA Systematic Review (2024): 16 articles confirm visual support interventions meet evidence-based practice criteria. | PMC11506176 | NCAEP Evidence-Based Practices Report (2020) | DOI: 10.1007/s12098-018-2747-4

ACT II — The Technique
⏱️ Wait Time Scaffolding
Parent-friendly alias: "Making the Wait Visible"
Definition: Wait Time Scaffolding is the structured use of visual, auditory, tactile, and behavioural materials to make the experience of waiting concrete, bounded, and survivable for children who cannot yet perceive time abstractly.
Waiting requires five simultaneous developmental capacities: (1) understanding that time passes, (2) trusting that the wait will end, (3) tolerating the discomfort of delay, (4) inhibiting the impulse to act immediately, and (5) self-regulating during the gap between wanting and getting. These 9 materials each address one or more of these five capacities. Together, they constitute a complete waiting support toolkit.
Life Skills & Adaptive Behaviour
Self-Regulation
Executive Function
Temporal Understanding
Delayed Gratification
Social Readiness
Age Range: 2–8 years (peak difficulty: 2–5 years) | Frequency: Daily practice across all waiting contexts | Setting: Home + School + Community + Doctor's Office + Restaurants

ACT II — Disciplines
These materials cross every therapy boundary — because the brain doesn't organise by therapy type
🟦 Occupational Therapist
Uses visual timers, calming tools, and sensory fidgets to address self-regulation and sensory processing during delay.
🟩 ABA / BCBA Specialist
Uses reinforcement systems, First-Then boards, and token economies to build waiting behaviour through behavioural shaping.
🟨 Speech-Language Pathologist
Uses social stories and wait cards to build language comprehension of time concepts — "wait," "soon," "my turn."
🟧 Special Education Teacher
Uses turn-taking games and visual schedules to build life skills readiness and classroom waiting tolerance.
🟥 NeuroDev Paediatrician
Guides dosage, progression timeline, and medication interactions with waiting behaviour across all material categories.
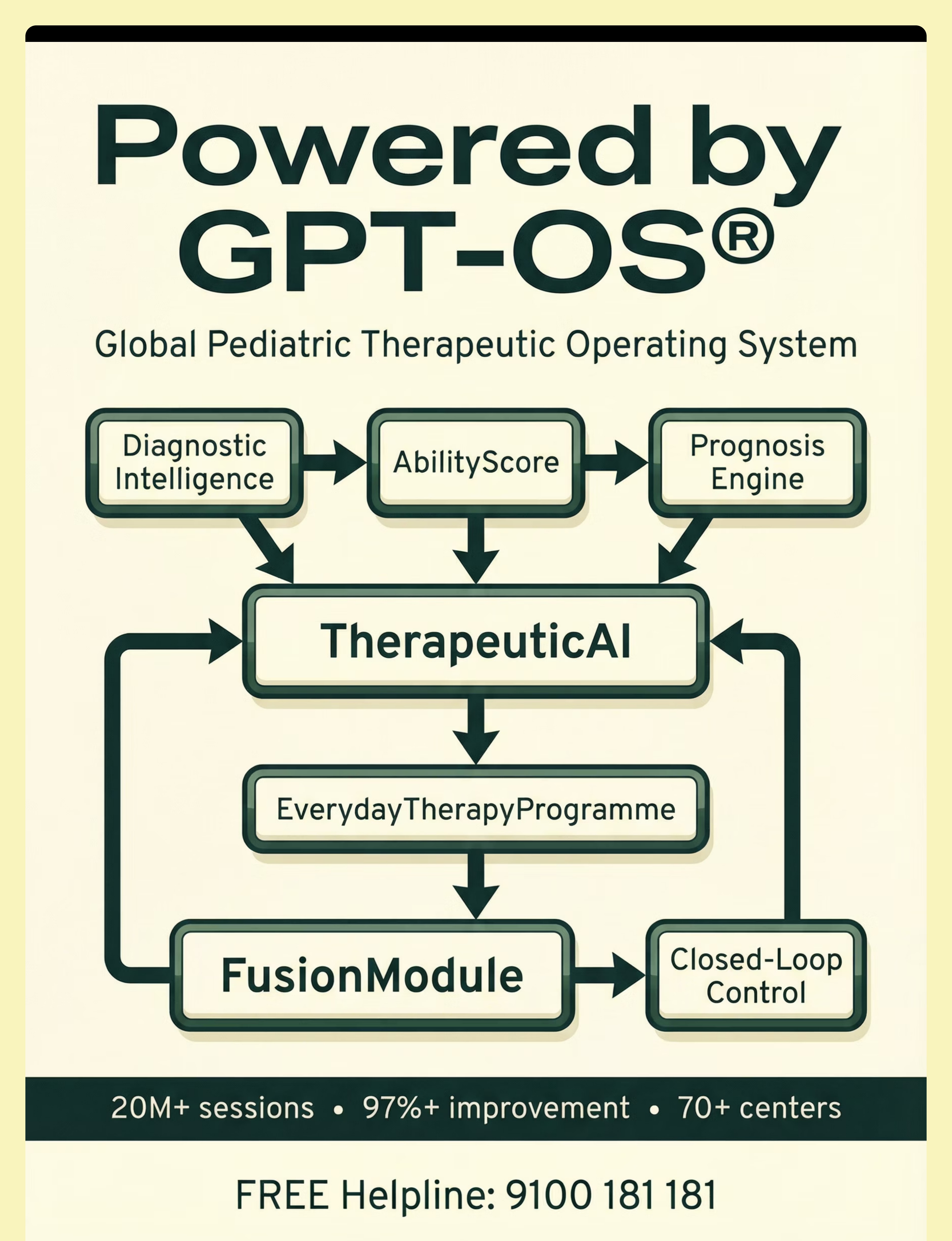
Pinnacle FusionModule™: All five disciplines contribute simultaneously to a child's waiting tolerance — not sequentially. This is why multi-disciplinary support accelerates outcomes beyond single-discipline approaches.
Adapted UNICEF/WHO Nurturing Care Framework for SLPs (2022): Multi-disciplinary convergence in responsive caregiving and executive function development. | DOI: 10.1080/17549507.2022.2141327

ACT II — Material 1 of 9
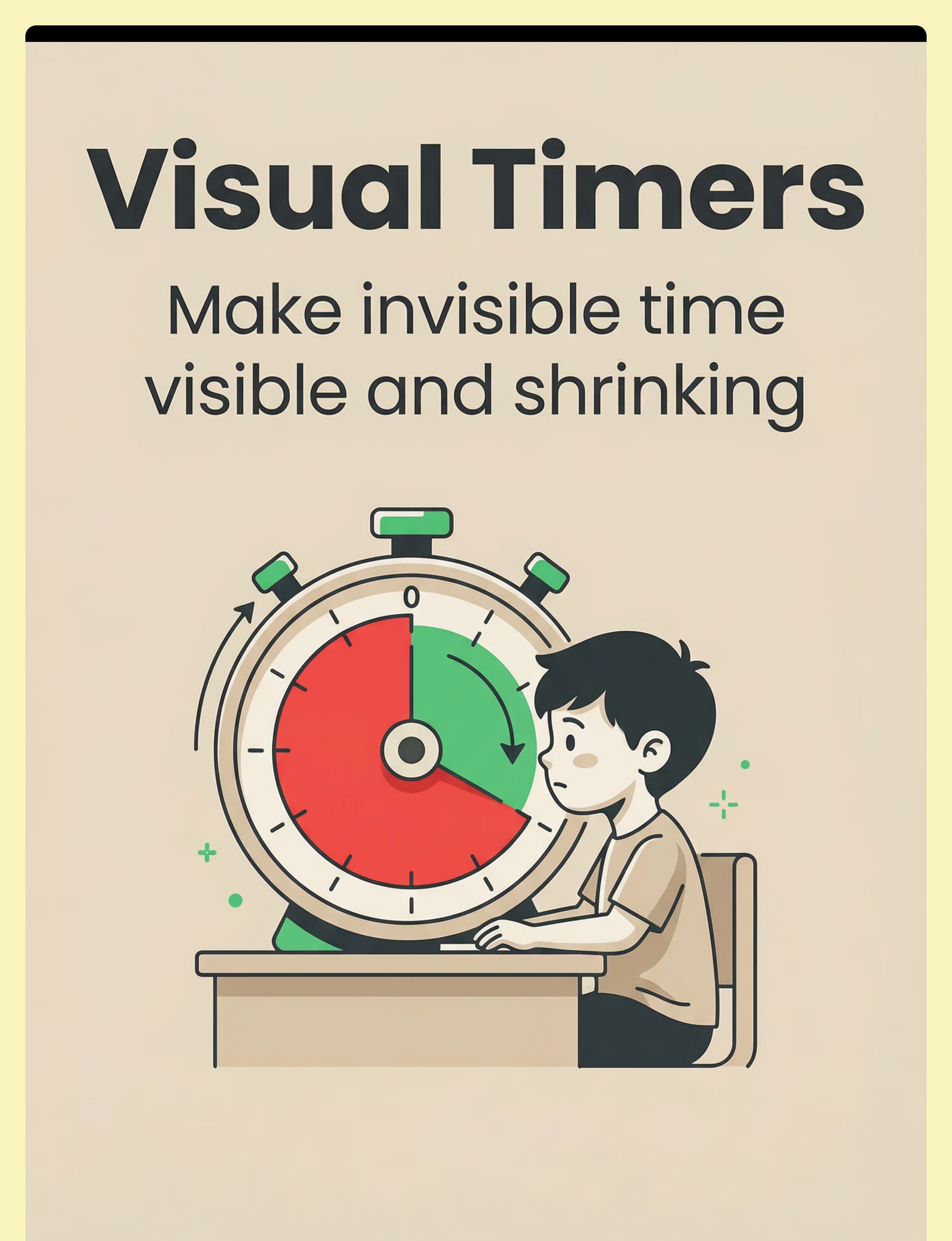
🔴 Material 1: Visual Timers
Clinical Function
Makes invisible time visible and shrinking. The child sees the red arc disappear, sand fall, or dial shrink — transforming an endless void into a concrete, measurable endpoint.
Why It Works
Temporal concretisation — converts abstract time into a visual stimulus that engages the prefrontal cortex rather than triggering amygdala alarm.
Recommended Products
🛒Smartivity DIY Interactive Clockamazon.in/d/0aY06Vfl | ₹673
Canon Category: Cognitive & Learning Price Range: ₹300–1,500
✅ Pinnacle Recommends
📋 NCAEP Level 1 Evidence
ACT II — Material 2 of 9
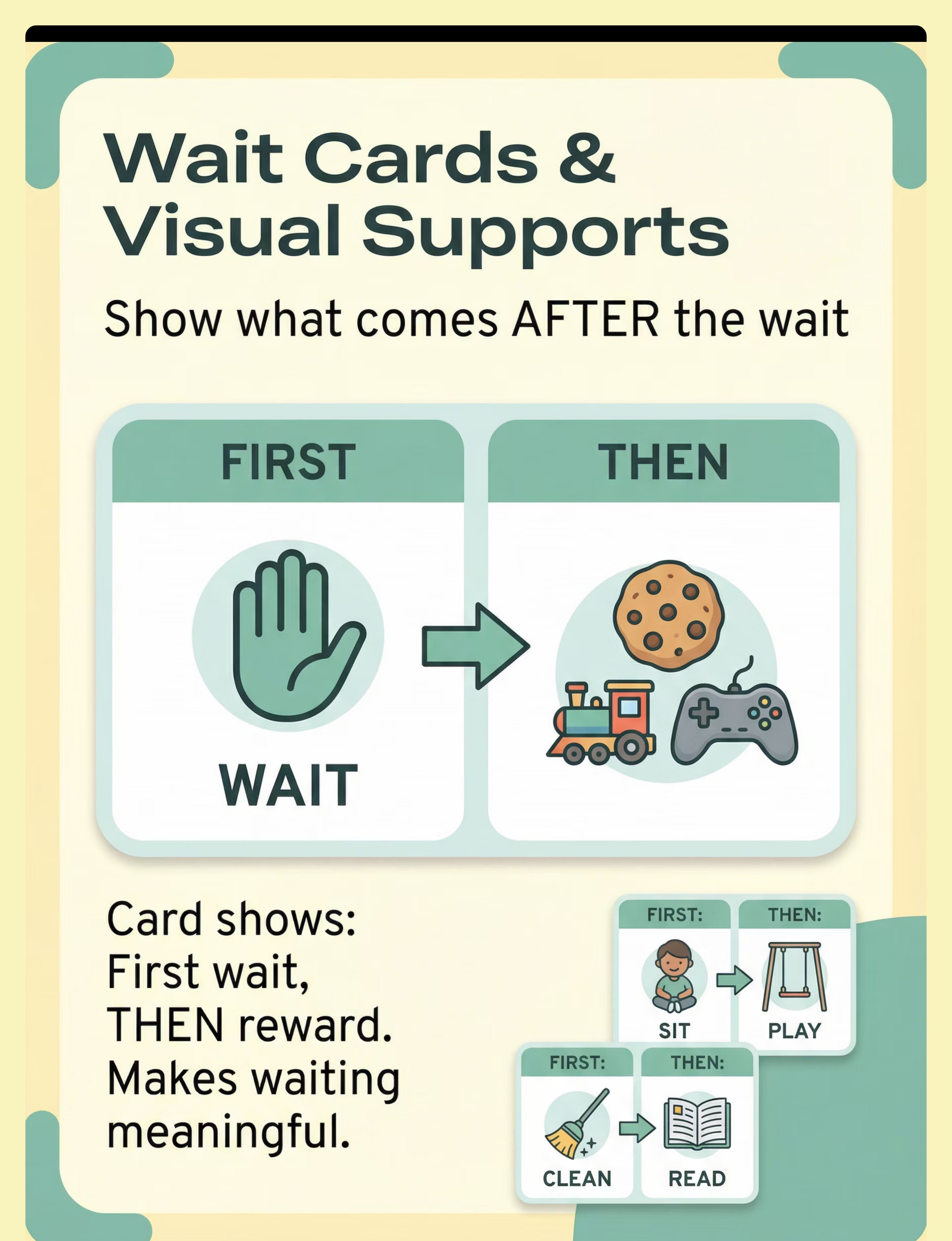
🟡 Material 2: Wait Cards & Visual Wait Supports
Clinical Function
First-Then boards and Wait Cards make the word "wait" concrete — showing WHAT comes AFTER the wait. Transforms an "endless void" into a "meaningful sequence with a visible reward."
Why It Works
ABA contingency clarity — the child can see the reinforcer waiting for them, reducing the aversive quality of the delay. The brain stops sounding the alarm when it can see the endpoint.
Recommended Products
🛒Brainy Bug Resources Flashcardsamazon.in/d/07zQavEk | ₹305
Canon Category: Cognitive & Learning Price Range: ₹100–400
✅ Pinnacle Recommends
📋 ABA + Visual Supports EBP

ACT II — Material 3 of 9
🟢 Material 3: Waiting Busy Bags & Activity Kits
Clinical Function
Fills the wait with purposeful activity. Hands busy, mind occupied, distress dissolved. "Empty waiting is torture. Filled waiting is just playing until your turn comes."
Why It Works
Competing stimulus — occupies sensory and cognitive channels during delay, reducing the aversive waiting signal and giving the nervous system a positive anchor.
Recommended Products
🛒Lattooland Rainbow Sorting Activity Setamazon.in/d/05LnLJZl | ₹628
Canon Category: Cognitive & Learning Price Range: ₹200–800
✅ Pinnacle Recommends
📋 OT Competing Stimulus

ACT II — Material 4 of 9
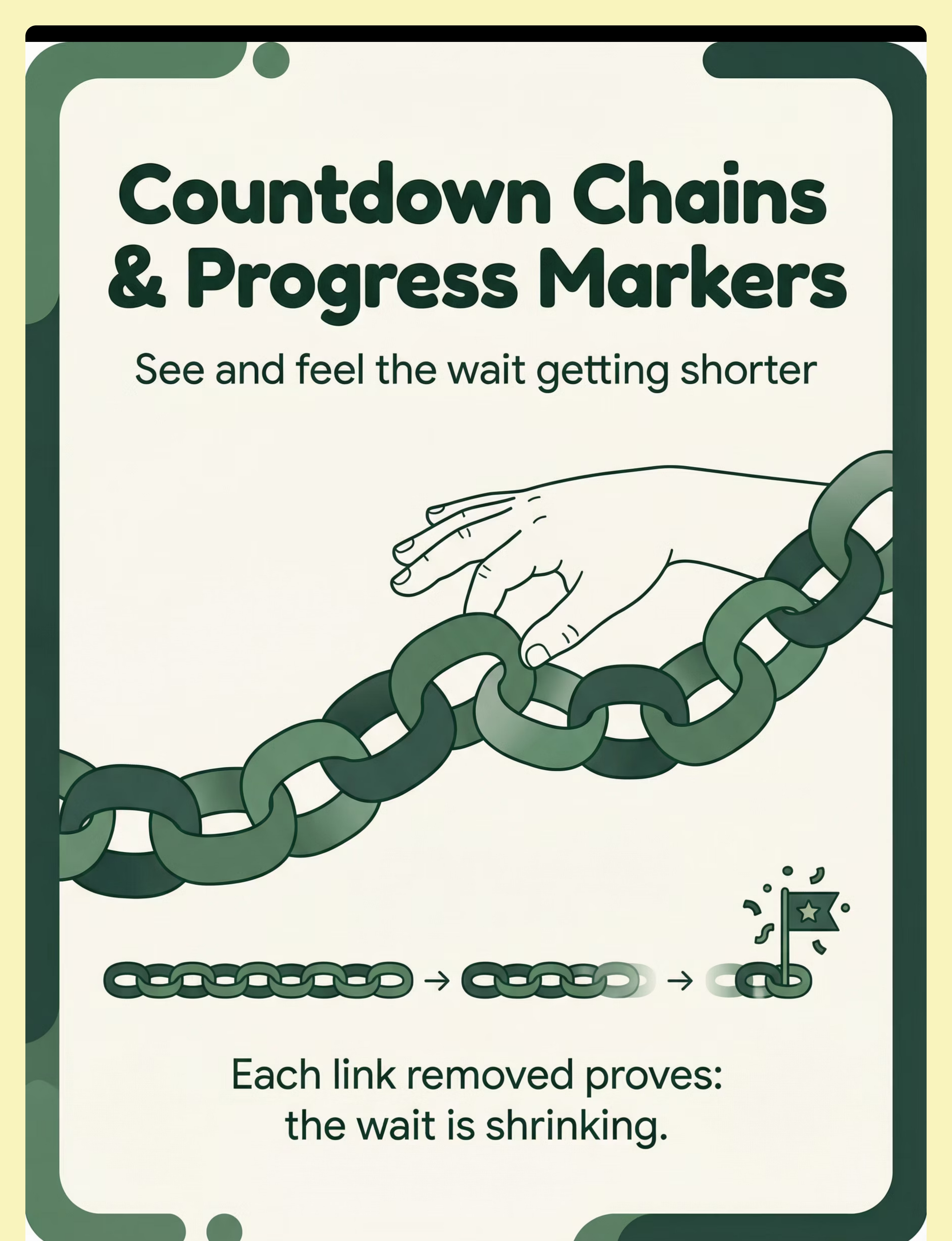
🔵 Material 4: Countdown Chains & Progress Markers
Clinical Function
Physical countdown — each link removed, each step crossed, each token moved shows CONCRETE PROGRESS. The child participates in shrinking the wait. Agency transforms waiting from something that happens to them into something they actively manage.
Why It Works
Participatory temporal concretisation — child agency in marking progress reduces helplessness and increases regulatory control. Removing a chain link is neurologically satisfying.
Recommended Products
🛒Dyomnizy Educational Memory Game (token use)amazon.in/d/0iwJwOiH | ₹519
Canon Category: Cognitive & Learning Price Range: ₹100–400
✅ Pinnacle Recommends
📋 OT + ABA Token Systems

ACT II — Material 5 of 9
🟤 Material 5: Social Stories About Waiting
Clinical Function
Builds a cognitive script for waiting BEFORE the wait arrives. Read when calm, the story creates a roadmap: "I can wait. Waiting ends. I can use my timer." Pre-loading the scenario removes the element of surprise that triggers escalation.
Why It Works
Cognitive scaffolding — pre-loading the prefrontal cortex with a behavioural script reduces amygdala hijack probability during actual waiting moments. The brain already has a plan.
Recommended Products
🛒A Visit to the Hospital Activity & Sticker Bookamazon.in/d/01KczBmp | ₹199
Canon Category: Cognitive & Learning Price Range: ₹150–500
✅ Pinnacle Recommends
📋 NCAEP Level 1

ACT II — Material 7 of 9
🟣 Material 7: Waiting Songs & Auditory Cues
Clinical Function
Songs mark time auditorily. Song begins = wait begins. Song ends = wait ends. Predictable, pleasant, child-known endpoint. Rhythm regulates the nervous system during the wait, providing a comforting temporal container.
Why It Works
Auditory temporal anchoring — rhythm provides co-regulation and a sensory-based endpoint signal that bypasses verbal time comprehension entirely. The nervous system responds to rhythm before language.
How to Use
🛒DIY (₹0) — Choose a familiar 60–90 second song. Consistency builds the association: this song = waiting time. Use the same song every time until the skill is established.
Canon Category: Behaviour Support Price Range: ₹0–200
✅ Pinnacle Recommends
📋 Music Therapy + ABA Cuing

ACT II — Material 8 of 9
⭐ Material 8: Wait-Then Reinforcement Systems
Clinical Function
Makes waiting PAY OFF. Token boards, sticker charts, reward jars — every successful wait earns something meaningful. Waiting ceases to be punishment and becomes investment. The child learns that delay has value.
Why It Works
Operant conditioning — positive reinforcement of delayed gratification builds tolerance incrementally and creates intrinsic motivation. The wait becomes associated with reward, not dread.
Recommended Products
🛒The Rosette Imprint Reward Jaramazon.in/d/02C5R9Jn | ₹589
🛒1800+ Reward Stickers Bookamazon.in/d/01wrHJWX | ₹364
Canon Category: Behaviour Support / Reinforcement Menus Price Range: ₹100–589
✅ Pinnacle Recommends
📋 ABA Reinforcement EBP Level 1
ACT II — Material 9 of 9
💚 Material 9: Calming & Self-Regulation Tools
Clinical Function
Keeps the nervous system regulated DURING the wait. Fidgets, squeeze toys, breathing tools, weighted items — a calm body can wait longer than a dysregulated one. These tools work on the body so the mind can tolerate delay.
Why It Works
Sensory regulation during delay — provides proprioceptive and tactile input that activates the parasympathetic nervous system, reducing cortisol and extending wait tolerance measurably.
Recommended Products
🛒Kidology Pull Out Spike Toy (tactile fidget)amazon.in/d/01aefj5R | ₹380
Canon Category: Behaviour Support Price Range: ₹200–600
✅ Pinnacle Recommends
📋 OT Sensory Regulation EBP
Aggregate Canon: NCAEP (2020) Evidence-Based Practice classifications | PMC11506176 | PMC10955541 | BACB Reinforcement Guidelines

ACT II — DIY Options
Every child deserves these tools — regardless of postcode or budget
These materials work because of their neurological principles — not their price tags. A paper chain is as scientifically sound as a ₹500 token board. A singing parent is as therapeutic as a ₹1,500 visual timer.
Material | ₹0 Household Version | Why It Works Equally | |
Visual Timer | Draw a circle on paper; shade completed portion as time passes | Visual shrinking = same temporal concretisation | |
Wait Card | Paper folded: write "WAIT" on front, draw reward on back | Same contingency clarity, same ABA principle | |
Busy Bag | Old cloth bag + 5 household objects (spoon, small toy, rubber band, sticker, folded paper) | Competing stimulus works with any engaging object | |
Countdown Chain | Torn newspaper strips looped and stapled (remove one per minute) | Physical progress marking = identical neurological effect | |
Social Story | 5 drawn stick figures on paper: child waiting → timer → reward → smile | Cognitive script requires words + picture, not print quality | |
Turn-Taking Game | Ball rolled back and forth = 1 turn each | Simplest turn-taking with 0 cost; maximum efficacy | |
Waiting Song | Any familiar 60-second song; hum it | Auditory temporal anchor requires no equipment | |
Reinforcement | Hand-drawn star on paper with "You waited!" written by parent | Praise + symbolic token = behaviourally equivalent | |
Calming Tool | Smooth stone to hold; rolled sock for squeezing; slow deep breath | Proprioceptive input principle requires no manufactured product |
The Pinnacle Consortium builds every technique to a ₹0 floor — honouring the WHO/UNICEF equity mandate across 70+ countries. ☎️ 9100 181 181
WHO Nurturing Care Framework (2018): Context-specific, equity-focused interventions; household-material-based intervention efficacy across 54 LMICs. | PMC9978394

ACT II — Safety First
Read this before you begin. Your child's safety is the first intervention.
🔴 STOP — Do Not Proceed If:
- Child is in active meltdown or severely dysregulated state
- Child has recently experienced trauma or signs of medical illness
- Material contains small pieces and child mouths objects (choking hazard)
- Child shows signs of sensory overload combined with self-injury
🟡 MODIFY If:
- Child is tired, hungry, or overstimulated (start with 30 seconds maximum)
- Child has had a difficult day (use only high-preference materials)
- First attempt at a new material (introduce during play, not a real wait)
- Public environment (ensure portable kit is discreet and quiet)
🟢 PROCEED When:
- Child is fed, rested, and in baseline-regulated state
- Materials are age-appropriate and choking-safe for this child
- Environment has been prepared (see setup card)
- Parent is regulated — dysregulated parent + dysregulated child = double escalation
Absolute Red Line: Stop immediately and provide comfort if the child becomes inconsolably distressed, shows self-injurious behaviour, or cannot co-regulate with your support within 2 minutes. Session abandonment is not failure — it is appropriate clinical decision-making.
Always honour timer endpoints. If the timer says "done," the wait is done. Broken promises destroy tool trust permanently. ☎️9100 181 181 (safety concerns)
Indian Journal of Pediatrics RCT (2019): Home-based intervention safety protocols for parent-administered sessions. | DOI: 10.1007/s12098-018-2747-4
ACT II — Setup
The environment is the first material. Prepare it.
Before any session begins, your environment needs to be configured deliberately. A poorly set-up space undermines even the best materials. Here is your pre-session environment checklist:
1
Visual Timer
Positioned where child can see it without turning their head. This is non-negotiable.
2
Waiting Bag or Activity
Ready and accessible — not sealed or locked. Child should be able to reach it immediately.
3
First-Then Board
At child's eye level, "Then" item already pictured before the wait begins.
4
Reinforcement Prepared
Token board ready, stickers out — before the wait starts, not during it.
5
Distractions Removed
No competing preferred items visible. TV off. Background audio reduced.
6
Parent's Body
Calm, nearby, not hovering. Child is not cornered — they have physical space.
Environmental calibration: Neutral lighting (not harsh fluorescent). Comfortable temperature — thermal discomfort shortens waiting tolerance. Always practice at home in a familiar environment before generalising to public settings.
Sensory Integration Theory (Ayres) + Meta-analysis: 1:1 structured environment treatment was most effective. Environmental setup is a core OT clinical principle. | PMC10955541

ACT III — Readiness
60 seconds before you start: run the readiness check
Readiness determines outcome more than technique quality. A five-minute session that succeeds is worth ten times more than a twenty-minute session that ends in meltdown. Run this check before every session.
Indicator | ✅ GO | 🟡 MODIFY | 🔴 POSTPONE | |
Regulation state | Calm, engaged baseline | Mildly irritable | Active distress | |
Hunger/thirst | Fed within 2 hours | Slightly hungry | Hungry/thirsty | |
Energy level | Alert, not fatigued | Slightly tired | Drowsy or hyperactive | |
Recent events | Neutral day | Minor difficulty | Major upset/illness | |
Sensory state | Baseline | Mildly overloaded | Severely overloaded | |
Your state | Regulated, patient | Mildly stressed | Overwhelmed |
If MODIFY:
Start with 30-second wait maximum. Use only ONE material (visual timer only). Praise survival, not success.
If POSTPONE:
Replace with a calming co-regulation activity. No judgment. The best session is one that starts right — not one that starts now.
ABA Setting Events and Antecedent Manipulation: Session-level readiness assessment is core to applied behaviour analysis protocol design. | General ABA + Pinnacle Clinical Protocols
ACT III — Step 1 of 6
Step 1: The Invitation
⏱️ Timing: 30–60 Seconds
Every wait begins with an invitation — not a command
"Hey [name], I have a really fun surprise for you in just a little bit! First, let's set this cool timer together…"
For younger children:"Look at this! The red is going to disappear! Let's watch it together…"
Body Language Guidance
- Get to child's eye level (kneel or sit)
- Voice is warm, unhurried, curious — not tense or pre-apologetic
- Present the visual timer as an interesting object, not a command tool
- Smile is genuine; you are genuinely curious with them
Acceptance Cues
- Glances at timer, reaches for it
- Body orients toward you or the material
- Eye contact or body language shift toward engagement
If Child Resists
Say "Okay, we'll look at it later" and wait 2 minutes before trying again. This is the ABA pairing protocol working correctly — not failure.
ABA Pairing Procedures: Establishing motivating operations before demand placement is foundational to behaviour-analytic session structure. | OT "Just-Right Challenge" principle
ACT III — Step 2 of 6
Step 2: The Engagement
⏱️ Timing: 1–3 Minutes
The child is in. Now anchor the wait.
01
Set the Timer Together
Let the child push the button or turn the dial if possible. Shared ownership builds investment.
02
Show the First-Then Board
"See? First we wait [point to wait side]. Then [point to reward picture]." Make the endpoint visible.
03
Open the Waiting Bag
"While we wait, you can play with this." Offer the activity — don't make it conditional.
04
Name What You're Waiting For
"We're waiting for [food / your turn / Mama's phone call] to finish." Specificity reduces uncertainty.
05
Stay Nearby
Available without narrating every second. Be a calm presence, not a commentary track.
Material Introduction Sequence: Timer first → Wait card second → Busy activity third. Each builds on the previous. First instance of child checking timer voluntarily → immediate specific praise: "You're checking the timer! That's exactly right!"
Systematic review (Children, 2024): Structured material introduction with reinforcement scheduling meets evidence-based practice criteria. | PMC11506176

ACT III — Step 3 of 6
Step 3: The Therapeutic Action
⏱️ Target Wait Duration
The wait is happening. Here is what you do during it.
Be a Calm Anchor
Your regulation co-regulates your child's nervous system. Your calm is the most powerful tool in this step.
Check In Intermittently
Every 30–60 seconds for short waits. Narrate the timer for very young children: "Look — the red is getting smaller. We're getting closer!"
Respond to Distress — Not Capitulate
"I hear you. It's hard to wait. The timer is almost done." Empathy without ending the wait early.
Do NOT Extend the Wait
Once set — honour the endpoint absolutely. If wait runs long, end it and address the cause separately.
Week 1–2
30 sec–1 min. Build trust in the system.
Week 3–4
1–3 min. Consolidation phase.
Week 5–8
3–7 min. Extending tolerance.
Month 3+
7–15 min. Approaching functional independence.
"Your job during the wait is not to make it enjoyable. Your job is to make it survivable. The timer, the bag, and your calm presence are doing the work."
Meta-analysis (World J Clin Cases, 2024): Parental co-regulation is a key mediating variable. | PMC10955541
ACT III — Step 4 of 6
Step 4: Repeat and Vary
⏱️ 3–5 Minutes Total Practice Across Day
3 successful waits per day > 1 heroic 20-minute wait
Waiting practice is not a formal "session" — it is embedded in real life (snack time, bath transition, playground turn). Variation maintains engagement: rotate materials between contexts; same principle, different tools.
Context | Primary Material | Timing | |
Snack preparation | Visual timer + waiting song | 2–3 min | |
Sibling's turn with toy | Wait card + fidget | 1–2 min | |
Doctor's waiting room | Busy bag + countdown chain | 5–10 min | |
Grocery checkout | Countdown chain ("3 people ahead") | 3–5 min | |
Waiting for phone call | Social story + reinforcement | 2–4 min |
Dosage: Daily target is 3–5 waiting opportunities of appropriate length. Watch for satiation signals — if child shows fatigue or increased resistance, end the current wait and resume later.
"3 good repetitions are worth more than 10 forced ones. The goal is confident success, not endurance performance."
SI Therapy dosage research: 3 sessions/week across 8–12 weeks; session-level repetition guidance from clinical consensus. | General SI + ABA literature

ACT III — Step 5 of 6
Step 5: Reinforce and Celebrate
⏱️ Within 3 Seconds of Wait Completion
The wait ended. This moment is the most important 3 seconds in the protocol.
"You waited! [Child's name], you WAITED! The timer went off and you stayed calm. That was SO HARD and you did it. [Deliver what was promised immediately]."
Verbal Praise
"You waited so patiently! I'm so proud of you!" — Always, with every successful wait.
Token / Sticker
Sticker on chart; stamp on hand. Use in first 4–6 weeks while skill is building.
Natural Reinforcer
The food, the turn, the activity — what they waited FOR. Always the most powerful reinforcer.
Tangible Bonus
Small special item for milestone waits (first 5-minute wait, etc.).
Timing is everything: Reinforcement within 3 seconds has 10× the effect of reinforcement at 10 seconds. Celebrate the attempt, not just the success — if child waited 1 minute before escalating, that 1 minute gets praised before the meltdown gets addressed.
ABA Reinforcement Principles: Immediate, specific reinforcement is the single most evidenced behaviour-change strategy across all autism intervention research. | BACB Ethical Guidelines
ACT III — Step 6 of 6
Step 6: The Cool-Down
⏱️ 1–2 Minutes
No session ends abruptly. The cool-down is part of the therapy.
Verbal Warning
"One more minute on the timer, then we're all done for now." (30–60 sec before end)
Completion Celebration
"All done! Great job waiting today." Specific, warm, genuine praise.
Material Put-Away Ritual
Child participates in packing the waiting bag — normalises it as a tool, not a toy.
Transition Object
Offer a comfort item or transition to a preferred activity.
If child resists ending (they're enjoying the waiting bag): This is a success indicator. Say: "You can use that again next time we have waiting practice. It lives in your special bag." Do not allow the waiting bag to become a general toy — preserve its specialist function.
Visual timer and transition support: Visual supports classified as EBP for autism (NCAEP, 2020). Transition protocols reduce post-session dysregulation. | NCAEP Evidence-Based Practices Report (2020)
ACT III — Data
60 seconds of data now saves hours of guessing later
What to Track — 3 Data Points Only
Wait Duration Achieved
Circle: <30 sec | 30 sec | 1 min | 2 min | 3 min | 5 min | 7 min | 10+ min
Distress Level
Circle: 0 – No distress | 1 – Mild | 2 – Moderate | 3 – High | 4 – Meltdown
Material Used
Circle: Timer | Wait Card | Busy Bag | Chain | Story | Game | Song | Reinforcement | Calming
Data Insight: Track for 7 days. If distress level is consistently 3–4 with your current wait duration target — the target is too long. Reduce by 50% and rebuild from success. Data reveals the calibration error; guessing does not.
ABA Data Collection Standards: Continuous measurement (frequency, duration, distress rating) and discontinuous measurement are standard for behaviour-analytic intervention. | BACB Guidelines + Cooper, Heron & Heward (ABA, 8th ed.)
ACT III — Troubleshooting
The session didn't go as planned. Here's why — and what to do next time.
❓ Child refused the visual timer
Why: New object + new demand introduced simultaneously. Too much novelty. Fix: Introduce timer during play — no waiting attached. Let child explore it freely for 3–5 days before using therapeutically.
❓ Child kept asking "is it done yet?" every 5 seconds
Why: Timer duration was too long for current skill level; child doesn't trust timer endpoint yet. Fix: Halve the wait duration. Remind gently: "The timer will tell you when it's done — it's your helper." Let the timer answer, not you.
❓ Meltdown before timer finished
Why: Wait duration exceeded current tolerance; or child arrived dysregulated. Fix: This is data. Reduce target to 50% of the duration where meltdown occurred. Rebuild from successful shorter waits.
❓ The materials stopped working after a week
Why: Novelty extinction — materials become familiar and lose interest-generating power. Fix: Rotate busy bag contents every 2–3 days. Introduce one new calming tool. Novelty maintains engagement; plan for regular rotation.
❓ Works at home but not in public
Why: Generalisation hasn't been built yet. New setting = new demand. Fix: Practice in progressively public settings: home → familiar family home → quiet shop → busier environments. Master each before advancing.
❓ Child using waiting tools as play items generally
Why: Materials have lost their specialist function through overexposure. Fix: Materials are ONLY available during designated waiting practice. Put them away between practices. Scarcity preserves therapeutic power.
"Session abandonment is not failure — it is data. Every incomplete session tells you exactly where to recalibrate."

ACT III — Personalise
No two children wait the same way. Here is your personalisation map.
🔍 Sensory Seeker
Child needs high sensory input during waits.
- Weighted lap pad during waits
- Vibrating fidget or textured squeeze toy
- Active waiting activities (stretchy bands, kinetic sand)
- Movement-based waiting songs
🔕 Sensory Avoider
Child is overwhelmed by sensation.
- Smooth, quiet fidgets (stone, fabric)
- Dimmer environments during practice
- Shorter, quieter timers (visual-only end; no alarm)
- Books or puzzles rather than sensory toys
⚡ ADHD Profile
Higher engagement + movement needed.
- Higher-engagement busy bag contents (Lego, pop-it, intricate puzzle)
- Movement breaks structured into wait (3 jumping jacks at halfway)
- Countdown chains with physical participation
- Shorter intervals, more frequent reinforcement
🌀 Autism Profile
Predictability and extended timeline required.
- Same timer, same spot, same sequence every time
- Pre-warn about the wait 5 minutes before it starts
- Visual schedule showing the wait as part of a larger sequence
- Longer timeline for tool fading — don't rush independence
Age 2–3
Sand timer only + one preferred object + maximum parent proximity.
Age 4–5
Visual timer + First-Then + busy bag + verbal countdown.
Age 6–8
Timer alone + self-selected busy activity + data tracking chart involvement.

ACT IV — Progress
Weeks 1–2: You are building trust in the tools — not teaching waiting yet
✅ What IS Progress in Week 1–2
- Child tolerates the visual timer being present without meltdown
- Child glances at or references timer during wait (even once = progress)
- Parent executes all 6 steps consistently (the real Week 1–2 goal)
- Meltdowns slightly shorter or less intense when tools are used
- Child accepts the busy bag at least 50% of attempts
❌ What Is NOT Progress Yet
- Child independently waiting without distress
- Waiting duration significantly extended
- Generalisation to public settings
- Child asking for the timer themselves
"If your child tolerates the visual timer for 30 seconds longer than last week before escalating — that is real, measurable, clinically significant progress. Celebrate the increments."
Systematic review (Children, 2024): Intervention outcomes emerge across 8–12 week timelines. Early-phase indicators focus on tool acceptance and participation, not skill mastery. | PMC11506176
ACT IV — Progress
Weeks 3–4: The brain is forming new pathways. Here's how to see them.
Consolidation Indicators — What to Look For
🧠 Anticipates the Routine
Child reaches for timer, points at busy bag before you prompt them.
🧠 Self-References the Wait
Child begins to say "Timer says wait" or similar self-instruction.
🧠 Duration Extending
30 seconds → 90 seconds → 3 minutes without escalation.
🧠 Faster Recovery
Child recovers faster after a wait-related frustration event.
🧠 Requests Waiting Tools
Child beginning to ask for their waiting bag — "Want my bag."
"By week 4, many parents notice they feel less dread before situations that require waiting. Your confidence is also consolidating — and your child can feel it."

ACT IV — Progress
Weeks 5–8: Mastery Approaching
75%
Phase: Mastery Approaching
Week 5–8 Progress Benchmark
Waits 5+ Minutes
With visual timer, without significant escalation.
Self-Initiates Busy Bag
Reaches for bag independently during wait.
Two+ Different Settings
Skills appearing beyond the home environment.
No Escalation
Maintains behaviour calmly throughout the wait.
Calm Transitions
Moves from wait to reward without behavioural rupture.
Maintenance Check: Skills maintained for 2+ consecutive weeks without regression = ready to progress. If skills regress after illness or travel — resume from Week 3–4 level, not Week 1. Skills consolidate faster on second pass.
Meta-analysis (2024): Sensory integration therapy across 24 studies showed measurable mastery outcomes. | PMC10955541 | BACB Mastery Criteria Standards

ACT IV — Celebrate
You did this. Your child grew because of your commitment.
You spent 5–8 weeks transforming waiting from your child's biggest trigger into a managed, tool-supported skill. You learnt six protocol steps. You calibrated, adapted, and persisted through the sessions that didn't go as planned.
Your child can now:
- Use a visual timer as a temporal anchor
- Access a waiting activity without being prompted
- Wait for periods that once seemed impossible
- Trust that waits end
Family Celebration Ideas
- Print an "I Can Wait!" certificate
- Let the child stick a gold star on the wall
- Mark the date in a family journal
- Take a photo of them using their waiting bag
"The moment I knew the tools were working was _______________. Before this, we couldn't _______________. Now we can _______________."
Your journey helps other families. Consider sharing your experience at pinnacleblooms.org/community

ACT IV — Red Flags
Trust your instincts. These signs mean: pause and seek professional input.
Sign | What It Looks Like | Why It Matters | What To Do | |
No improvement after 8 weeks | Wait tolerance not extending despite consistent protocol | May indicate underlying profile needing clinical assessment | Contact Pinnacle helpline | |
Self-injury during waits | Head banging, biting, scratching | Safety priority; may indicate sensory overwhelm | Immediate professional consultation | |
Escalating aggression | Hitting, throwing, destroying materials | Tools insufficient for current dysregulation level | ABA/BCBA assessment needed | |
Complete regression | Sudden return to baseline after weeks of progress | May signal medical or environmental change | Developmental paediatrician consultation | |
Anxiety generalisation | Child preemptively anxious before any wait | May indicate anxiety disorder requiring separate intervention | Psychological evaluation | |
Avoidance of all waiting contexts | Family withdrawing from all public settings | Quality of life impact requiring professional support | OT + family support |
Self-Monitor at Home
Teleconsultation
In-Person Assessment
Multi-Disciplinary Evaluation
📞FREE HELPLINE: 9100 181 181 | 16+ Languages | 24x7

ACT IV — Pathway
You are not done. You are at a waypoint. Here is the journey ahead.
Wait Time Scaffolding feeds into: classroom readiness, peer play participation, medical compliance, community integration, and ultimately — independent adult life skills. This is not a small skill.
L-925
Following Routines — Prerequisite
L-926
Time Awareness — Foundation
L-927
Wait Time Scaffolding — YOU ARE HERE
L-928
Transition Tolerance — Next Level
L-929
Flexibility With Changes — Advanced
Home Waiting Mastered
→ Advance to L-928: Transition Tolerance (moving between activities smoothly)
Public Waiting Still Challenging
→ Build with community-based practice protocols (see Adapt card)
Turn-Taking Specifically Difficult
→ Explore C-253: Waiting Difficulty (social context focus)
Waiting + Feeding Challenges
→ Explore E-552: Stop and Wait
ACT IV — Related Techniques
Explore the full Life Skills & Adaptive Behaviour series
Technique | Domain | Difficulty | Materials You Already Own | |
L-925: Following Routines | Life Skills | 🟢 Intro | Visual timer ✓ | |
L-926: Time Awareness | Life Skills | 🟡 Core | Same materials ✓ | |
L-927: Wait Time (YOU ARE HERE) | Life Skills | 🟡 Core | — | |
L-928: Transition Tolerance | Life Skills | 🟡 Core | Busy bag ✓ | |
L-929: Flexibility With Changes | Life Skills | 🔴 Advanced | Social stories ✓ | |
C-280: Impulse Control | Emotional Regulation | 🟡 Core | Reinforcement ✓ |
ACT V — Community
From "Wait is a dirty word" to "The timer told me so"
"The day he pointed at the timer and said 'almost done' to me — instead of screaming — I cried in the restaurant bathroom. That's when I knew something had permanently changed."
— Parent of Aryan, age 4
"The countdown chain was the breakthrough. She could SEE the queue shrinking. She wasn't just waiting — she was tracking progress."
— Parent of Meera, age 6 (ADHD)
"What parents consistently report is that the tools don't just help the child — they regulate the parent. Holding a timer gives the parent permission to stop narrating the wait and trust the tool. That parental calm is itself therapeutic." — Senior OT, Pinnacle Blooms Network
Aryan waited less than 45 seconds before full meltdown. By week 8, using a visual timer, First-Then board, and waiting bag, he extended wait tolerance to 7 minutes at a restaurant. Meera's doctor's office tolerance extended from under 2 minutes to 12 minutes with a rotating doctor's waiting bag and countdown chain. Individual outcomes vary.
ACT V — Connect
Isolation is the enemy of consistency. Join the community.
🟢 Pinnacle Parent WhatsApp Community
Join thousands of parents working on waiting skills, transitions, and adaptive behaviour across India and 70+ countries.
🔵 Online Parent Forum
Share wins, ask questions, get peer support from families who are exactly where you are.
🟡 Local Parent Meetup
70+ centres across India host monthly parent support sessions. Find your nearest centre.
🟠 Peer Mentoring Programme
Connect with an experienced parent who has navigated this exact challenge and successfully built their child's waiting skills.
"Your experience — the hard sessions, the breakthroughs, the restaurant triumph — helps the next family that arrives scared. Consider sharing your journey."
WHO NCF: Community engagement is a core principle. Over 1,000 individuals from 111 countries contributed to the NCF framework. Parent support networks improve intervention outcomes.
ACT V — Share
Consistency across all caregivers multiplies impact exponentially
The more consistently all adults in your child's life use these tools, the faster the skill builds and generalises. Share this with everyone who cares for your child.
For Your Spouse / Partner
"Our child is using a visual timer, a First-Then board, and a waiting bag to build waiting skills. When [name] has to wait, set the timer for [X minutes], give them their waiting bag, and remind them what comes after the wait. When the timer ends — the wait ends. No extensions."
For Grandparents
"[Child's name] is learning to wait using special tools. The red timer shows how long to wait. The small bag has things to do while waiting. When the red disappears — waiting is done. If they get upset, say: 'Look at the timer — it's getting smaller!' Don't end the wait early."
For Their Teacher
"We are implementing Wait Time Scaffolding at home (Pinnacle L-927). [Child's name] uses a visual timer and waiting activity. If you have access to a visual timer in class, consistent use would accelerate skill generalisation. Our OT can share our specific protocol."
WHO CCD Package: Multi-caregiver training is critical for intervention generalisation and maintenance. Consistency across settings multiplies outcomes. | PMC9978394
Preview of 9 materials that help with wait time Therapy Material
Below is a visual preview of 9 materials that help with wait time therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.







Link copied!
The Pinnacle Promise
Pinnacle Blooms Network®
A Consortium of Paediatric Experts
Occupational Therapy
Speech-Language Pathology
ABA / BCBA
Special Education
NeuroDev Paediatrics
WHO/UNICEF Aligned
"From fear to mastery. One technique at a time."
Pinnacle Blooms Network® exists to transform every home into a proven, scientific, 24x7 personalised multi-disciplinary paediatric therapy environment — powered by GPT-OS® and the world's largest structured intervention knowledge base.
This content is educational. It does not replace professional evaluation or therapy by qualified professionals. Significant difficulty with waiting may indicate developmental differences that benefit from comprehensive assessment. Intervention should be individualised based on developmental profile. Individual results may vary. Statistics represent aggregate outcomes across the Pinnacle Blooms Network.
CIN: U74999TG2016PTC113063 | DPIIT: DIPP8651 | MSME: TS20F0009606 | GSTIN: 36AAGCB9722P1Z2
© 2025 Pinnacle Blooms Network®, unit of Bharath Healthcare Laboratories Pvt. Ltd. All rights reserved. | techniques.pinnacleblooms.org | GPT-OS® | AbilityScore® | TherapeuticAI® | FusionModule™ | EverydayTherapyProgramme™
📞9100 181 181 | FREE National Autism Helpline | 16+ Languages | 24x7 | care@pinnacleblooms.org