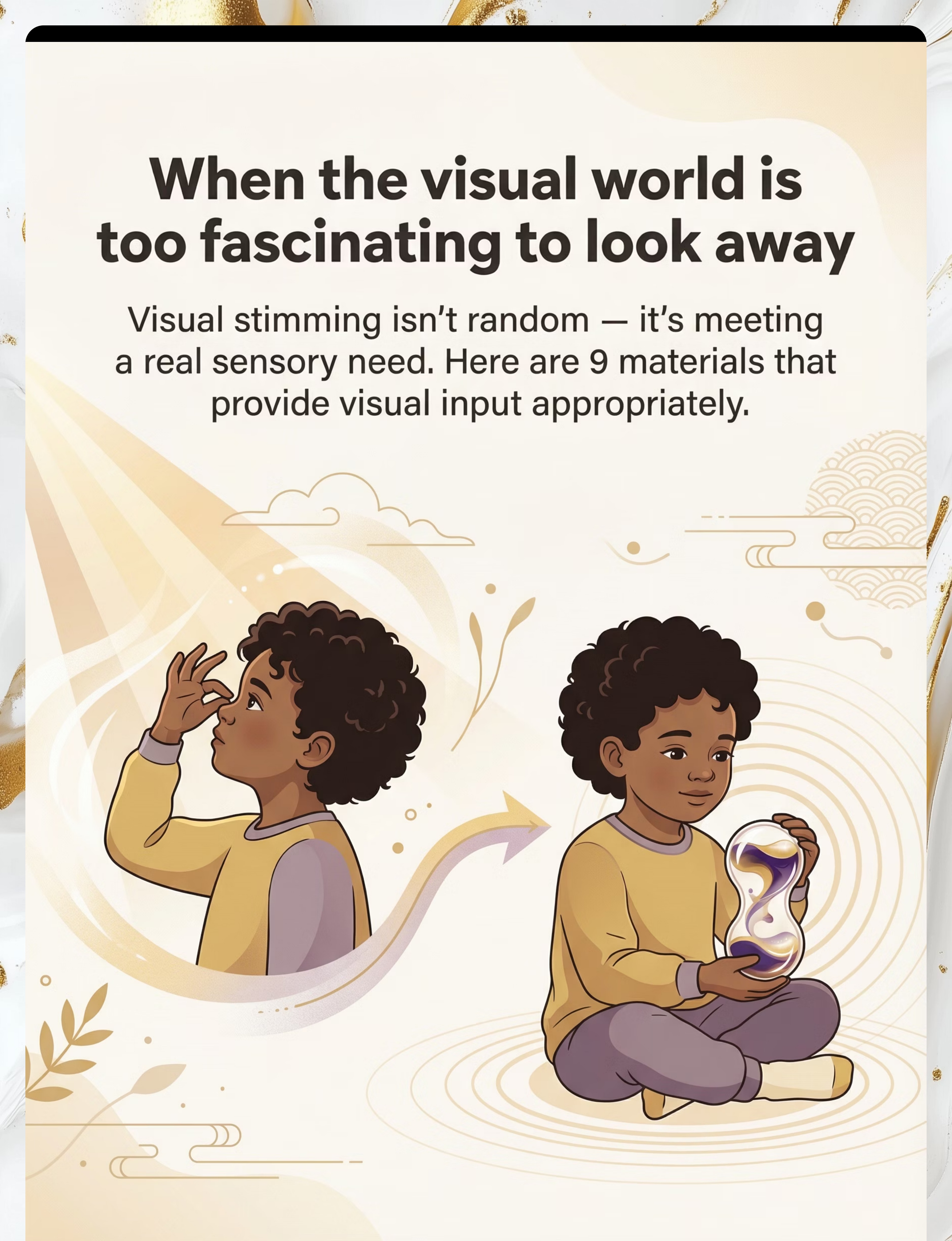
When the visual world is too fascinating to look away
Visual stimming isn't random. It isn't defiance. It isn't a phase. It is your child's nervous system speaking in the only language it knows right now.
"My 4-year-old goes rigid staring at ceiling fans. I have to physically move him away from the window — the light through the blinds catches him for 20 minutes at a stretch. He wiggles his fingers right in front of his eyes, and if I interrupt him, he melts down immediately. Stores with fluorescent lights are impossible. But at home he seeks out every spinning, shimmering, blinking thing he can find." — Parent, Pinnacle Network
9 Materials That Help With Visual Stimming — D-365. You are not failing. Your child's visual system is speaking.
🏥 Pinnacle Blooms Consortium
👁️ Visual Processing
🧠 Sensory Regulation
📍 Series D-365
FREE National Autism Helpline: 9100 181 181 (24x7 · 16+ languages)
Act I: Entry
You are among millions of families navigating this exact challenge.
Visual self-stimulatory behavior is among the most common sensory phenomena in neurodevelopmental conditions — present in autism, ADHD, sensory processing disorder, and developmental delay. It is not rare. It is not unusual. And it is absolutely addressable. When a child stares at lights, spins objects, or moves their hands in front of their eyes — their visual cortex is requesting input it needs to regulate. This is biology, not behavior.
60–70%
Visual Stimming Rate
of autistic children engage in visual stimming behaviors
Lancet Psychiatry, 2023
1/36
India Autism Rate
children in India are diagnosed on the autism spectrum
NIMHANS India Autism Report
21M+
Sessions Delivered
therapy sessions delivered by Pinnacle across sensory domains
Pinnacle GPT-OS® RWE Data
"Sensory processing difficulties affect 80% of children diagnosed with autism." — PRISMA Systematic Review, 2024 (PMC11506176)
This is a wiring difference, not a behavior choice.
Your child's visual brain is not absorbing information the way other children's brains do. Instead of filtering out background visual information — lights, movement, patterns — their visual cortex treats it all as equally compelling. The result: they cannot look away from the fan. They cannot stop watching the wheel spin. Their fingers in front of their eyes create a visual pattern they can actually control — which is deeply satisfying to a nervous system that often feels out of control.
The Visual Stimming Circuit
🔵 Visual Cortex (V1/V2) — Primary visual processing
🔵 Superior Colliculus — Automatic gaze orientation
🟡 Basal Ganglia — Repetitive motor patterning
🟣 Limbic System — Arousal & emotional regulation
⚡ OUTPUT: Repetitive visual-seeking behavior
In visual stimming, this circuit amplifies predictable visual input as a self-regulating feedback loop.
Plain English for Parents
This is called visual self-regulation through stimming. It is not random. It is purposeful. And it responds to intervention.
🧠Ayres Sensory Integration Theory explains that the visual system has direct, powerful connections to the arousal and regulation centres of the brain. Visual stimming is the child's nervous system using the fastest available pathway to achieve regulatory calm.
Reference: Frontiers in Integrative Neuroscience (2020) — DOI: 10.3389/fnint.2020.556660
Your child is here. Here is where we are heading.
Visual stimming typically peaks between ages 3–8, but it is most responsive to structured, material-based intervention during this same window. Understanding where your child sits on the developmental map helps you calibrate expectations and choose the right approach.
1
Zone A (0–18M)
Typical Visual Exploration. All infants gaze at high-contrast patterns. This is normal visual brain wiring — not stimming.
2
Zone B (18M–3Y)
Developmental Visual Seeking. Toddlers briefly explore spinning objects. Becomes clinically significant if it persists and interferes with engagement.
3
Zone C (3–8Y) ★
Peak Visual Stimming Window. This is where D-365 operates. Most intense, most interfering, and most responsive to intervention.
4
Zone D (8Y+)
Integration & Self-Regulation. With support, children learn to self-regulate visual needs and independently select appropriate tools.
Comorbidity Awareness: Visual stimming commonly co-occurs with auditory processing differences, tactile sensitivities, attention dysregulation, sleep difficulties, and anxiety. Assessment across all domains is recommended.

Clinically validated. Home-applicable. Parent-proven.
Every material in this toolkit is evidence-backed. The research base spans systematic reviews, meta-analyses, and India-specific randomized controlled trials — giving you confidence that what you are doing at home is grounded in real science.
📊 Finding 1 — Evidence-Based Practice
Sensory integration intervention meets criteria for evidence-based practice in children with ASD — including material-based visual regulation tools.
PMC11506176 | Children, 2024
📊 Finding 2 — 40–70% Reduction
Providing appropriate sensory alternatives reduces problematic stimming frequency by 40–70% within 8 weeks in structured home programs.
Meta-analysis, World J Clin Cases 2024 | PMC10955541
📊 Finding 3 — Home = Clinic
Home-based sensory interventions administered by trained parents demonstrate significant outcomes equivalent to clinic-based delivery.
Indian J Pediatr, 2019 | DOI: 10.1007/s12098-018-2747-4
✅ Occupational Therapy
✅ Applied Behavior Analysis
✅ NeuroDev Pediatrics
✅ WHO/UNICEF Aligned

The Technique
9 Materials That Help With Visual Stimming
Parent-Friendly Alias: The Visual Regulation Toolkit
Definition: Visual stimming refers to repetitive behaviors that provide visual sensory input — staring at lights, watching spinning objects, finger-flicking near the eyes, seeking reflections or patterns. This technique collection identifies 9 specific materials that provide visual input appropriately — meeting the same sensory need through safer, more functional, socially acceptable objects — without eliminating the regulatory behavior the child depends on.
🏷️ Domain
Sensory Processing / Visual System
🏷️ Age Range
2–12 years
🏷️ Duration
5–20 min per session
🏷️ Frequency
Daily
🏷️ Setting
Home + School + Community
🏷️ Series
Episode D-365

This technique crosses therapy boundaries because the brain doesn't organize by therapy type.
🔴 Occupational Therapy — PRIMARY LEAD
OTs use visual regulation tools as the cornerstone of sensory integration intervention. They conduct the functional assessment, build the sensory diet, and teach proactive visual tool use to regulate arousal states and attention.
🔵 ABA / BCBA
Behavioral therapists use functional behavior assessment to understand the WHY of visual stimming — then implement replacement behavior protocols. Visual tools become the reinforcement-compatible replacement that serves the same function.
🟢 Neurodevelopmental Pediatrics
NeuroDev physicians rule out vision impairment, assess neurological contributors, coordinate medication where indicated, and provide the medical framing that legitimizes sensory-based intervention for the family.
🟡 Special Education
SpEd teachers implement classroom visual regulation strategies — designated sensory corners, quiet visual tools, tinted overlays — that generalize home-learned skills to the educational environment.
"When OT, ABA, and SpEd all use the same visual tool vocabulary, the child's nervous system receives consistent signals across all environments. This convergence — the FusionModule™ principle — is why Pinnacle outcomes exceed single-discipline models." — Pinnacle Clinical Consortium

Visual regulation tools are precision instruments, not generic toys.
Every material in the D-365 toolkit is meticulously mapped to specific neurological targets. By understanding what each therapeutic session is working toward, practitioners and caregivers can move beyond simple observation and begin to track real, incremental progress, even when those developmental shifts appear subtle.
Neurological Targets Mapping

The 9 Materials
9 materials. Every one maps to a specific visual need. Every one available in India today.
Not sure which to start with? Call FREE: 9100 181 181

1. 🌊 Liquid Motion Timer / Bubble Timer
Mesmerizing flow. Safe staring. Built-in stopping point.
The child's visual system gets slow, predictable, beautiful movement — without staring at lights. The natural endpoint teaches that visual breaks can end.
₹300–₹1,000

2. ✨ Fiber Optic Lamp / Light Spray
Safe light-seeking. Touchable. Color-changing.
For children drawn to lights — fiber optics give safe, captivating light input. Touch the fibers (no heat), watch colors shift slowly, satisfy light-seeking without eye damage risk.
₹500–₹2,000

3. 🍾 Sensory Bottle / Glitter Calm-Down Jar
Portable visual stim. Shake-and-watch. Calming arc.
Shake it — glitter swirls. Watch it — glitter settles. The visual chaos slowly resolving to stillness mirrors exactly what the nervous system needs to do. Portable. Unbreakable. Discreet.
₹100–₹800


4. 💡 Light-Up Toys / LED Fidgets / Glow Toys
Controlled light input. Hands-on visual play. Screen-free.
Light control in the child's hands — not passively absorbed from screens. Active light play builds motor skills while meeting visual light-seeking needs.
₹150–₹800

5. 🌀 Spinning Toys / Visual Spinners / Spin Tops
Appropriate rotation to watch. Active control. Visual satisfaction.
Children who watch every wheel spin are seeking rotational visual input. Spinning toys provide this through objects the child controls — building regulation through mastery.
₹100–₹600

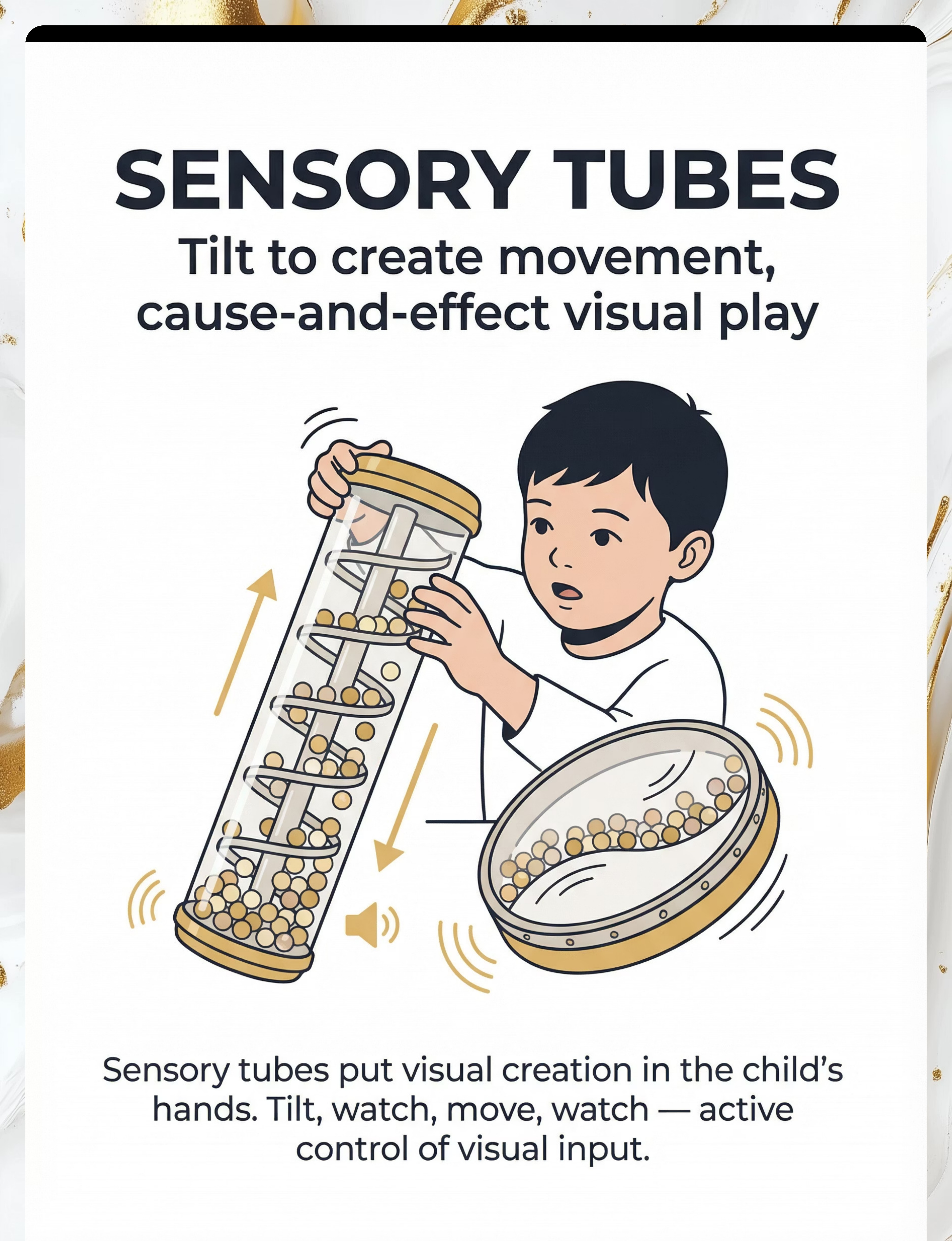
6. 🔴 Visual Sensory Tubes / Rainmaker / Wave Drums
Tilt to create movement. Cause-and-effect visual play.
The child CREATES the visual input by tilting the tube — beads cascade, liquid flows, balls roll. This shifts from passive staring to active creation of visual experience. Regulatory control.
₹300–₹1,200

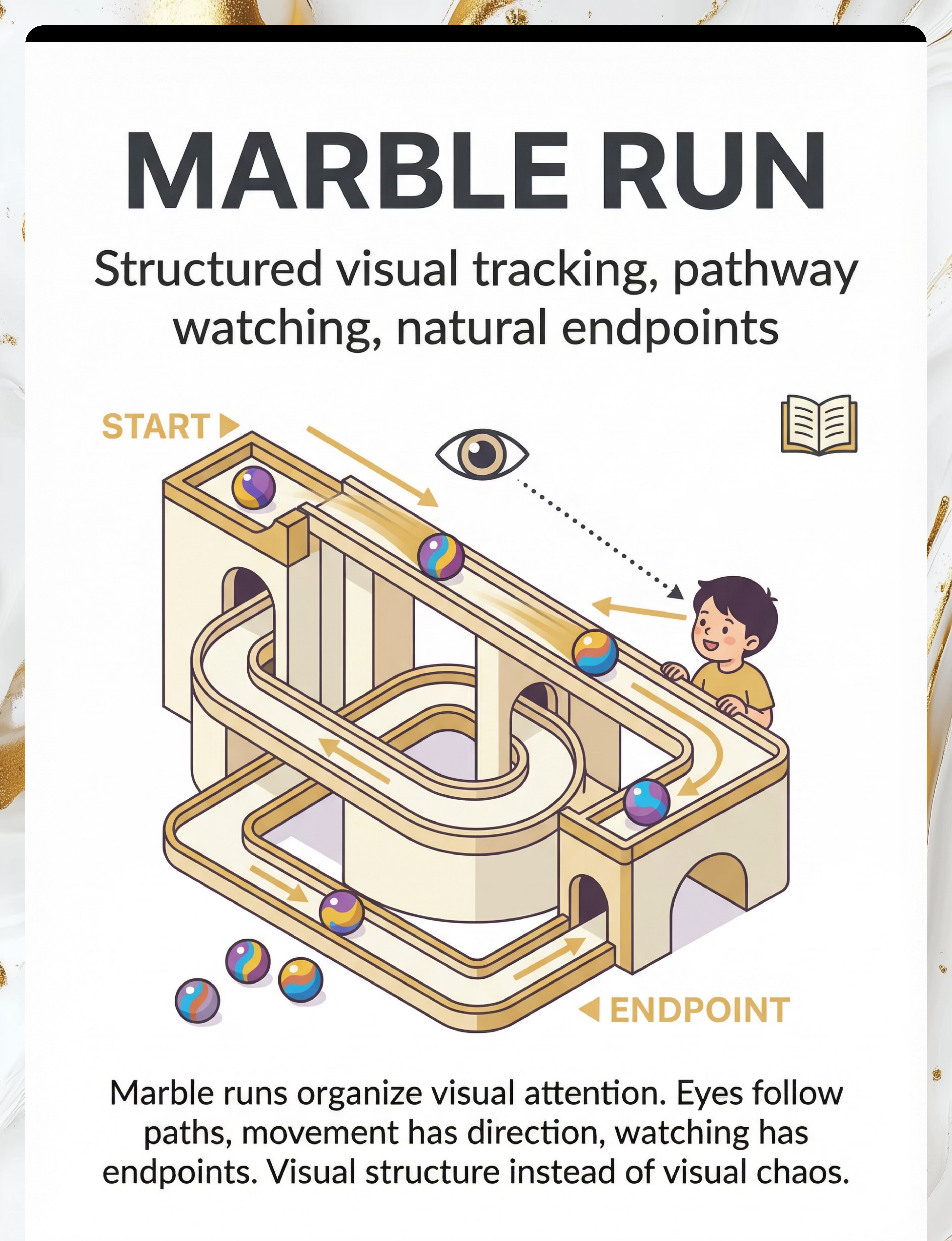
7. 🔮 Marble Run / Visual Tracking Toys / Ball Tracks
Structured visual tracking. Pathway watching. Natural endpoints.
Eyes follow the marble from start to finish — this is organized visual attention, not scattered staring. Marble runs train visual tracking skills that underpin reading readiness.
₹400–₹2,000

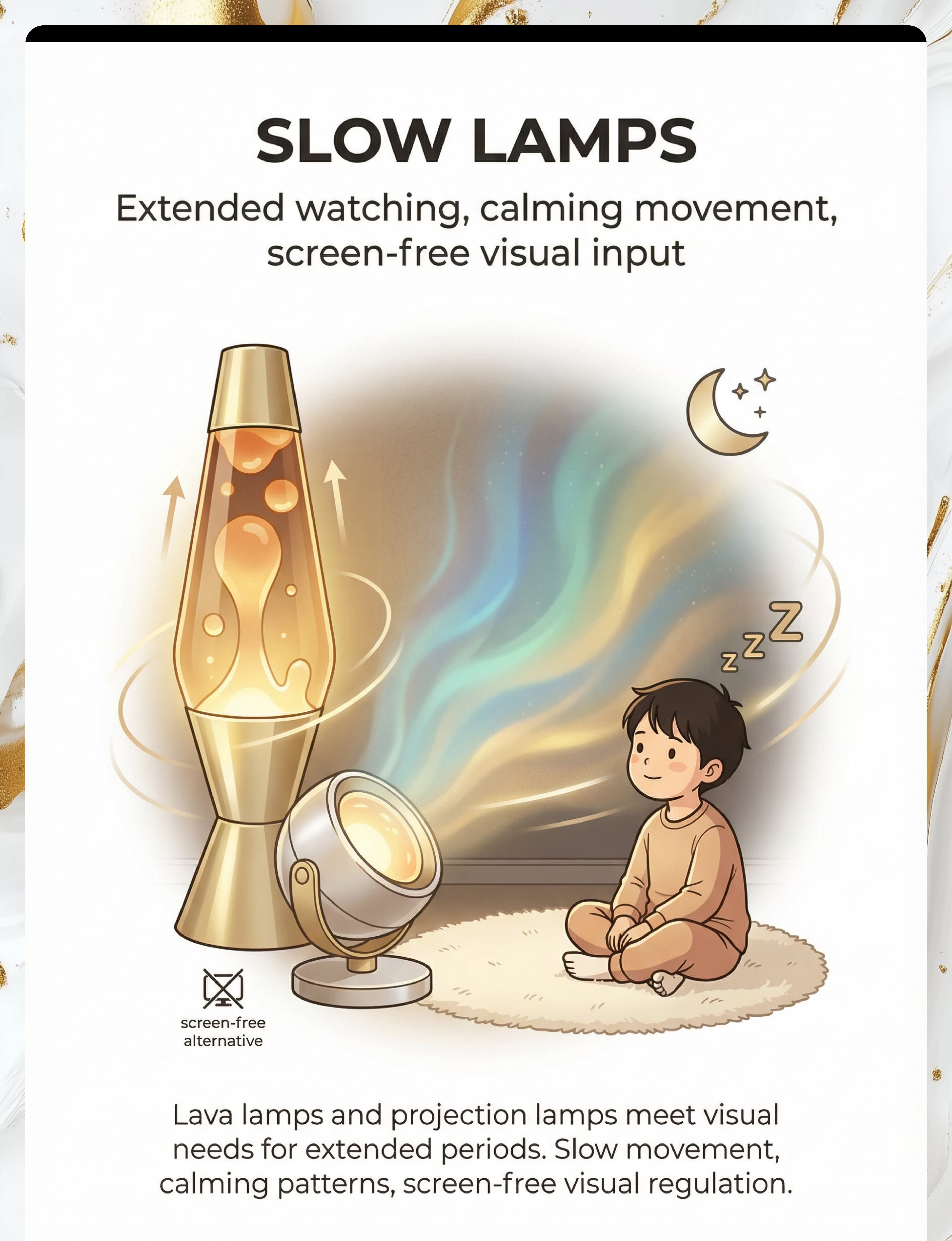
8. 🌋 Lava Lamp / Projection Lamp / Slow-Moving Lamp
Extended watching. Calming movement. Screen-free visual input.
The child needs to watch something moving. Lava lamps and projection lamps answer that need for extended periods — without screens, without blue light, without fast-moving stimulation.
₹600–₹2,500

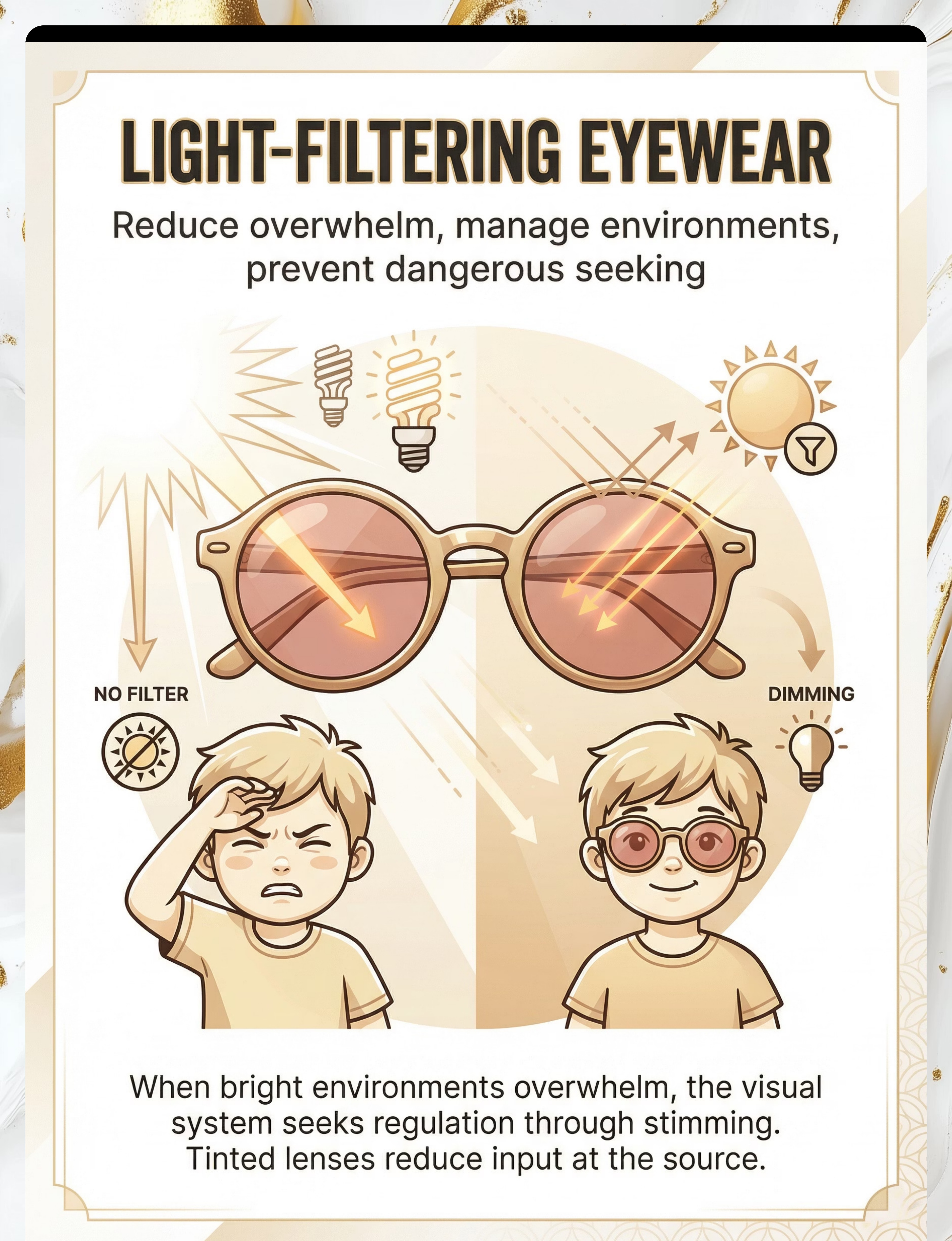
9. 🕶️ Sunglasses / Tinted Lenses / Light-Filtering Eyewear
Reduce overwhelm. Manage environments. Prevent dangerous seeking.
Some visual stimming occurs because the child's visual system is overwhelmed by environmental light. Tinted lenses reduce input at the source — addressing the cause, not just the symptom.
₹200–₹8,000
🏅Pinnacle Recommends: Every material above is clinically mapped by the Pinnacle OT + ABA Consortium. Selection is function-based, not generic.
Every family can start today. Zero budget required.
"Equity-focused interventions must reach every child, regardless of economic status, by leveraging the caregiving environment that already exists within the family." — WHO Nurturing Care Framework
DIY Alternatives for Indian Homes
1-3. Sensory/Touch | DIY sensory bins using pulses (dal), uncooked rice, or sand in old dabbas. | |
4. Light Toys | Use a mobile phone flashlight behind a piece of thin colorful dupatta or cloth. | |
5. Spinners | Cut circles from stiff cardboard, insert a toothpick; paint patterns to watch spin. | |
6. Sensory Tubes | Fill a clean plastic water bottle with water, glitter, and pulses. Seal the cap tightly. | |
7. Marble Run | Use cardboard tubes from kitchen rolls, taped to the wall to create a sloped path. | |
8. Lava Lamp | Slow-moving shadows: shine a torch behind a semi-transparent cloth or curtain. | |
9. Tinted Lenses | Use broad-rimmed hats or caps to shield eyes from harsh overhead lighting. |
Read this before your first session. Safety is non-negotiable.
RED: STOP
Stop immediately if you observe:
- Sun-gazing
- Eye-pressing
- Seizure history or suspected triggers
- Flashing stimuli usage
AMBER: MODIFY
Modify or supervise closely for:
- Fiber optic cord integrity
- Sensory bottle lids (choking risk)
- Small objects like marbles
- Lava lamp heat surfaces
- Battery compartment security
GREEN: PROCEED
Proceed when:
- Child is fed and rested
- Environment is distraction-free
- Dangerous behaviors are ruled out
- You have 10-20 uninterrupted minutes
- All materials are safety-checked
STOP SESSION IMMEDIATELY if the child shows signs of distress, extreme fatigue, or if any component of a DIY material becomes loose or broken.

Spatial precision prevents 80% of session failures. Set the stage before you begin.
A thoughtfully prepared environment is not optional — it is the foundation of a successful visual regulation session. Each element below serves a specific therapeutic purpose.
Material Station
2–3 pre-selected visual tools within child's reach but not all visible at once. Have one primary tool + one backup. Reduce choice paralysis.
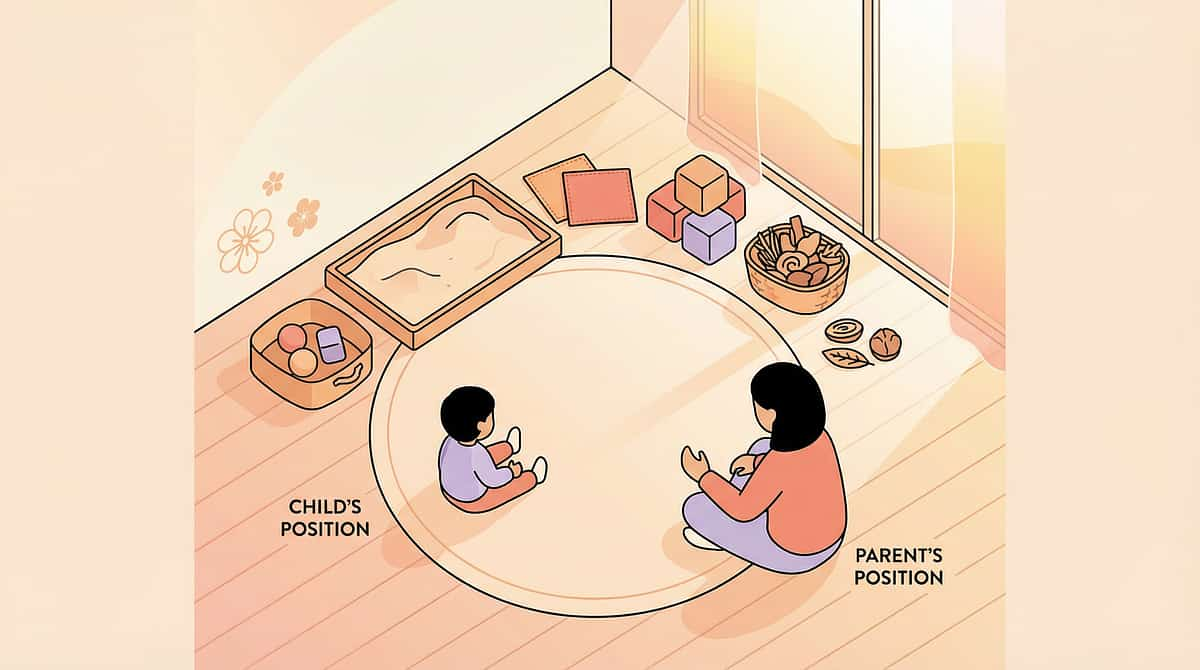
Child Position
Floor mat or low cushion. Seated, comfortable, eye level with materials. Do NOT have child lying down for visual regulation sessions.
Parent Position
Beside or slightly behind the child — not in front of and blocking the visual field. You are a co-regulator, not a barrier.
Lighting
Dim the room slightly. Draw blinds to reduce external visual competition. Fiber optic and lava lamp sessions: dimmer is better.
Sound
Low, consistent background — white noise or gentle instrumental music at low volume. No TV, no other voices competing for attention.
Remove
Other toys, screens, siblings, pets during session. Visual regulation requires focus on the tool, not environmental competition.
Duration Guidance: First sessions: 5–8 minutes. Build to 15–20 minutes over 2–3 weeks. Sessions that end naturally (child disengages) are better than sessions forced to a timer.

The best session is one that starts right.
Before every session, run this quick five-point readiness check. A modified or postponed session is clinical skill — pushing through a wrong-state session teaches the child that regulation tools are associated with distress, the opposite of our goal.
Indicator | ✅ GO | ⚠️ MODIFY | 🛑 POSTPONE | |
Feeding state | Fed within 1–2 hrs | Mildly hungry (offer snack first) | Hasn't eaten | |
Sleep | Rested | Mildly tired | Overtired / post-meltdown | |
Current regulation | Calm or alert | Slightly fussy | Active meltdown | |
Recent events | Normal day | Minor disruption | Major transition / illness | |
Illness | Healthy | Mild cold | Fever, pain, acute illness |
✅ 4–5 Green → START SESSION
Proceed with full protocol. This is optimal.
⚠️ 2–3 Green → MODIFY SESSION
Reduce to 5 minutes. Use child's #1 preferred tool only. No new materials.
🛑 0–1 Green → POSTPONE
Today is data, not failure. Offer calming input freely for 5 minutes with no instruction.

Step 1 of 6
Every session begins with an invitation. Never a command.
Duration: 30–60 seconds
"Hey, I have something cool to show you. Come see."
Hold out the liquid timer or sensory bottle. Don't demand they sit. Let curiosity pull them in.
For non-verbal children: Hold the tool at child's eye level. Wait. Let them approach. If they approach within 30 seconds — that's acceptance. If not — try again tomorrow.
Acceptance Signals — Watch For These
- Child moves physically toward you or the tool
- Child's gaze shifts to the tool, even briefly
- Child's body orientation turns toward session space
- Child reaches out or makes any approach gesture
Parent Body Language Guide
- Relaxed posture. Low energy. Match child's regulation level.
- Tool in YOUR hands first — demonstrate before offering.
- No commands, no eye contact demands in invitation phase.
- Don't prompt multiple times in rapid succession.
Resistance: Place tool in session space and leave it. Natural curiosity often brings them back within 3–5 minutes.

Step 2 of 6
The child is interested. Now you deepen it — gently, slowly, without pressure.
Duration: 1–3 minutes. Place the chosen visual tool within the child's reach. Say nothing for 15–30 seconds. Let the visual material speak first.
Liquid Timer / Sensory Bottle
"Look at that. Watch it go." Say slowly, calmly. Then go quiet.
Fiber Optic Lamp
"It changes colour. See?" Touch one fiber gently. Wait to see if child imitates.
Spinning Top
"Watch this." Spin it yourself. Watch with the child. Don't yet offer control to child.
Marble Run
"Here it goes." Drop marble. Track it with your own eyes dramatically. Child mirrors.
🟢 Engaged
Eye contact with tool, body oriented toward tool, vocalization, reaching for tool
🟡 Tolerating
Nearby but not focused, glances at tool intermittently
🔴 Avoiding
Moving away, escalating distress, covering eyes
When the child looks at or approaches the tool: "Yes! You found it." Simple, immediate, genuine.

Step 3 of 6
This is where the nervous system does its real work.
Duration: 5–10 minutes — the core visual engagement window. Your role is to be present without directing. Let the material lead the regulation.
🌊 Liquid Timer
Child watches liquid flow. After 1–2 minutes say: "It's almost done. Watch till it finishes." This teaches visual engagement has a natural end — a key regulation skill. When complete: "All done. Should we do it again?"
✨ Fiber Optic Lamp
Narrate colour changes gently: "Blue now. Now it's turning purple." This layers language onto visual experience without disrupting regulation. 8–10 minute sustained engagement is optimal.
🍾 Sensory Bottle
Mirror the regulatory arc verbally: "All shaken up... and now it's calming down... settling... settled." This externalizes the regulation process the nervous system is learning.
🔮 Marble Run
Count together: "One... two... three... it made it!" Natural endpoint (marble reaches bottom) is a built-in teaching moment for goal completion.
Step 4 of 6
3 good repetitions are worth more than 10 forced ones.
Duration: 3–5 additional minutes. Aim for 3–5 natural repetitions of the core visual engagement cycle. Choose ONE variation per session to build on what your child has mastered.
Variation A — Speed Change
Slow the spin. Fast the spin. Watch how the child responds to different visual input speeds. This develops visual discrimination.
Variation B — Child Leads
Transfer full control to the child. They decide when to spin, when to shake, when to tilt. Observe what they choose — this is diagnostic information.
Variation C — Second Material
Introduce a second visual tool after 3 repetitions. "Here's another one. Which one do you want to watch?" Building a visual regulation repertoire.
Variation D — Verbal Bridge
Narrate what the child is doing: "You're watching it spin. Your eyes are following it all the way around." This builds body awareness and self-advocacy language.
Satiation Indicators — When to Stop: Child pushes tool away · Child's attention wanders and doesn't return · Child moves toward another activity independently. Do NOT continue past satiation — satiation is success. The visual need was met.

Step 5 of 6
Celebrate the attempt, not just the success. Timing matters more than magnitude.
Deliver reinforcement within 3 seconds of the desired behavior. A 10-second delayed "good job" teaches nothing. An immediate "yes!" teaches everything.
For Verbal Children
"You did it! You used your timer. That's exactly it."
For Social Reward Seekers
High five + smile + brief physical contact if welcomed. Keep it warm and immediate.
For Tangible Reward Seekers
Token on reward chart + specific praise: "One star because you watched the whole way through."
For Low-Key Reinforcement Preferences
Calm nod + quiet: "Good watching." Some children are dysregulated by enthusiastic praise.
Key Insight: For many visual stimmers, the visual tool itself is the most powerful available reinforcer. "First we do [task], then you get your [liquid timer]" harnesses the child's visual seeking in service of therapeutic goals.

Step 6 of 6
No session ends abruptly. The cool-down is part of the therapy.
Duration: 1–2 minutes. Give a transition warning BEFORE ending — not mid-absorption: "Two more looks, then all done."
This four-step sequence ensures the nervous system transitions smoothly from visual regulation mode to next-activity mode — reducing the resistance and meltdowns that often accompany abrupt session endings.
If Child Resists Ending: Set the tool down (don't take it away). Say: "It's resting. It'll be here next time." Walk away calmly. Natural disengagement usually follows within 1–2 minutes when there is no power struggle over the tool.

60 seconds of data now saves hours of guessing later.
Data collection is not a clinical burden — it is a parent superpower. Three data points, captured immediately after each session, reveal the patterns that guide every protocol adjustment.
Session Duration
How many minutes did the child engage with the visual tool? Log the number. Even 2 minutes is a data point worth capturing.
Engagement Quality
🟢 Fully Engaged | 🟡 Partially Engaged | 🔴 Minimal Engagement. Circle one immediately after the session.
Unsafe Stimming Today
Did any unsafe visual stimming occur (sun-gazing, eye-pressing, screen-seeking)? None · Brief · Significant.
Weekly Trend: Track these 3 data points daily for 2 weeks. Look for: ↑ Duration increasing → technique is building engagement. ↑ Quality improving → nervous system is responding. ↓ Unsafe stimming reducing → appropriate alternatives are working.

Session abandonment is not failure. It is data. Here is what to do with it.
Child refused to engage with any visual tool
Why: Wrong timing, wrong material, or child was overstimulated (not under-stimulated). Fix: Wait for a naturally calm moment. Try a material the child has already seen you use.
Child became more agitated with visual tool
Why: Child may be visually hyper-responsive (overwhelmed), not hypo-responsive. Fix: Switch to calming, slow tools (liquid timer, projection lamp). Dim the environment.
Child used the tool but returned immediately to unsafe stimming
Why: The tool worked, but the duration was too short to meet the need. Fix: Extend session by 3–5 minutes. Use the tool BEFORE the child begins seeking inappropriate input.
Child destroyed or broke the tool
Why: Frustration, motor dysregulation, or seeking proprioceptive input alongside visual. Fix: Start with non-destructible options. Consult OT about adding deep pressure activities.
Child fixated and couldn't transition away
Why: Without the cool-down protocol, transitions will be difficult. Fix: Implement the cool-down sequence consistently. Use a visual timer for tool use itself.
Technique works at home but not at school
Why: Environmental generalization requires environmental consistency. Fix: Send a portable visual tool to school with an instruction card for teachers.

No two nervous systems are identical. Here is how to personalize the 9 materials for YOUR child.
🔵 Sensory Seeker (Under-responsive)
Choose: LED fidgets, fast spinners, bright fiber optic lamps. Longer sessions (20–30 min) acceptable. Multiple visual tools available simultaneously. Can add movement while using the tool. Goal: channel intense seeking, don't restrict it.
🔴 Sensory Avoider (Over-responsive)
Choose: Slow lava lamp, dim projection lamp, muted sensory bottle. Shorter sessions (5–8 min), lower visual complexity. Tinted eyewear FIRST before introducing active visual tools. Goal: reduce overwhelm, build tolerance gradually.
🟡 Mixed Profile
Dimly lit calming tools for overwhelming environments. More stimulating tools for low-arousal states. Parent assesses current arousal state before tool selection each day. Goal: dynamic regulation — right tool for right state.
Age | Recommended Approach | |
2–3 years | Passive tools only (lava lamp, liquid timer). Adult controls tool. Short sessions. | |
4–6 years | Introduce active control tools (spinner, marble run). Child chooses from 2 options. | |
7–10 years | Full tool repertoire. Child self-selects. Begins to identify own sensory state. | |
10–12 years | Self-regulation program. Child manages own visual diet. Parent coaches, doesn't lead. |

Weeks 1–2
In weeks 1–2, progress looks like tolerance — not mastery. Know the difference.
Progress So Far
Foundation being laid. Neural pathways forming. Every second with an appropriate visual tool instead of a dangerous one is measurable progress.
✅ What Progress DOES Look Like
- Child accepts the visual tool being present in the room
- Child looks at the tool for 5–10 seconds (up from 0)
- Child tolerates parent demonstrating the tool nearby
- Unsafe stimming episodes are slightly shorter in duration
- Child does not actively avoid the session space
❌ What Progress Does NOT Look Like Yet
- Child does NOT yet independently select the visual tool
- Child does NOT yet interrupt unsafe stimming to use the tool
- Unsafe stimming has NOT disappeared
- Sessions are NOT yet smooth or predictable
Measurement Prompt:"If your child tolerated the liquid timer for 5 seconds more this week than last week — that is real, measurable, neurological progress. Log it."

Weeks 3–4
The nervous system is consolidating. Watch for these signs — most parents miss them.
Consolidation Phase
The nervous system is building new patterns. Anticipation and spontaneous use are the most significant indicators at this stage.
Anticipation
Child shows behavioral signs before the session — moves toward session space, retrieves visual tool independently, hands parent the material.
Preference Emergence
Child begins to show preference for a specific tool. This is the nervous system communicating its optimal input. Follow this signal.
Spontaneous Use
Child picks up a visual tool on their own at a non-session time. This is the first seed of self-regulation — the most significant consolidation sign.
Extended Engagement
Session duration increasing naturally without parent prompting. Reduced intensity of unsafe stimming — episodes shorter and easier to redirect.
"You may notice you're more confident too. You're reading your child's signals with more accuracy. That's real caregiver skill development — and it's just as important as the child's progress."

Weeks 5–8
Mastery: Phase 1 Complete 🏆
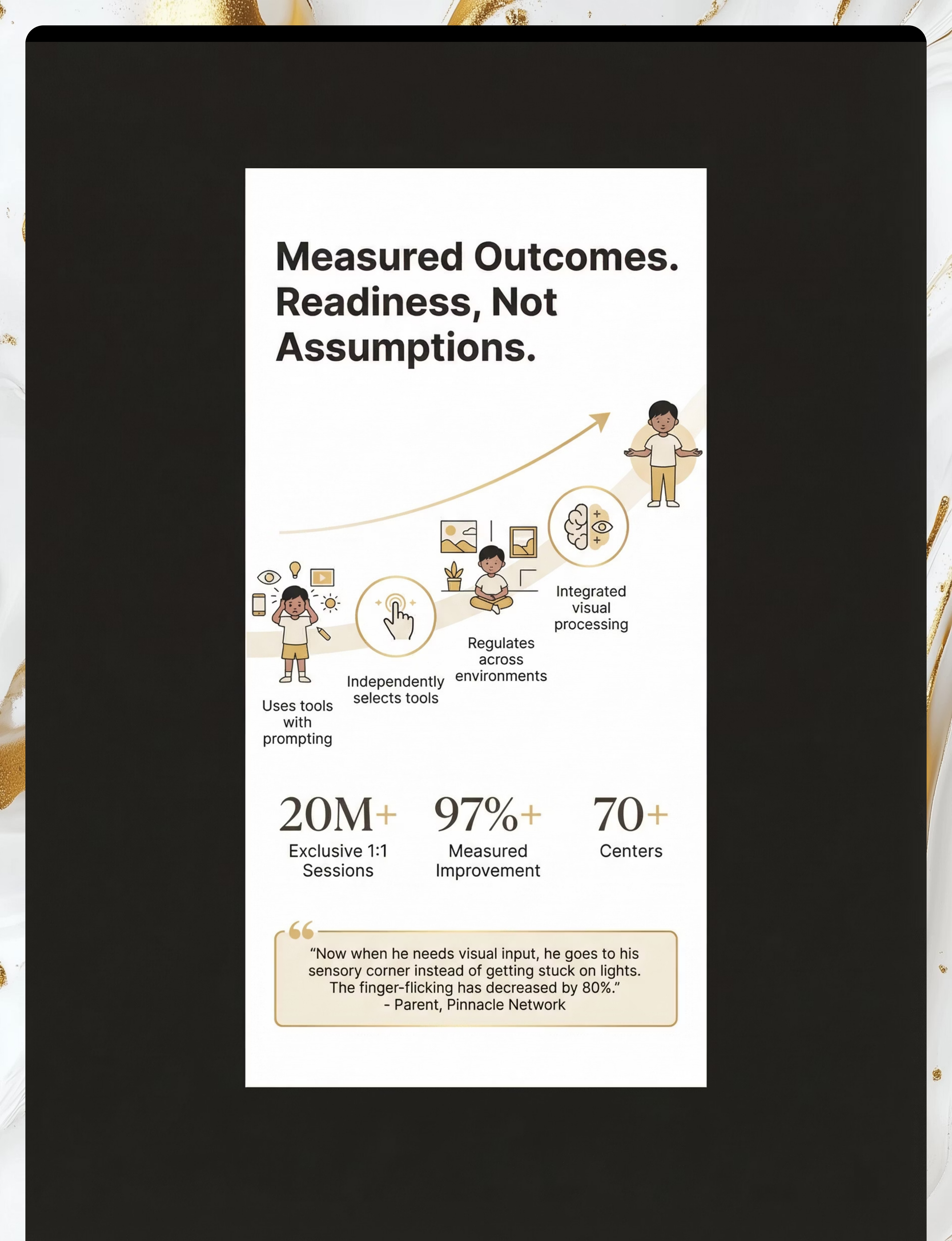
Visual Regulation Readiness
Phase 1 complete. Your child is building genuine self-regulation capacity that will generalize across settings and last a lifetime.
Independence
Child independently selects and uses visual tool when visually dysregulated — without adult prompt — in at least 3 out of 5 opportunities over 1 week.
Generalization
Visual tool use appears in at least 2 different settings (home + school OR home + community).
Maintenance
Unsafe stimming is measurably reduced — ≥40% decrease in frequency or duration from baseline.
Flexibility
Child can use more than one visual tool — not fixated on a single object.
Communication
Child can indicate — verbally or through gesture/PECS/AAC — that they want a visual tool.
When to Progress: 4 of 5 criteria met consistently over 2 consecutive weeks → ready for D-366 Vestibular Stimming integration. When to Strengthen: If criteria met in only 1 setting → focus on generalization before advancing.

You did this. Your child grew because of your commitment.
Five to eight weeks ago, your child stared at ceiling fans until you had to physically move them. They finger-flicked for minutes at a stretch. They missed learning because they were lost in visual absorption. Today, they pick up their sensory bottle. They know where their liquid timer is. They can be redirected. They are learning to regulate their visual world.
This is the beginning of self-regulation. And you built this.
🎉 Create a Visual Regulation Corner
A permanent, dedicated sensory space with their chosen tools. Frame it as their special space — not a therapy station.
📓 Journal Prompt
"Write down what was hardest in week 1 and what you see now. This is evidence. This is your child's story."

Trust your instincts. If something feels wrong, pause and ask.
FREE Helpline: 9100 181 181 (24x7)
🚨 Red Flag 1 — Eye-Pressing Has Begun or Increased
Any behavior involving pressing, rubbing, or poking the eyes requires immediate OT + ophthalmology consultation. This can cause permanent eye damage. Action: Pause visual stimming sessions. Call 9100 181 181 today.
🚨 Red Flag 2 — Sun-Gazing Continues Despite Intervention
If after 4 weeks of consistent visual tool use the child continues to seek the sun or very bright light sources, a specialist assessment is required. Action: Consult Pinnacle OT + optometrist/ophthalmologist.
🚨 Red Flag 3 — Visual Stimming Associated with Seizure-Like Activity
Any visual stimulus triggering stiffening, eye-rolling, or loss of consciousness → photosensitive epilepsy evaluation required immediately. Action: Stop all visual tool use. Neurological consultation urgently.
🚨 Red Flag 4 — Dramatic Sudden Increase in Visual Stimming
Rule out new medication effects, vision deterioration, or medical conditions affecting sensory processing. Action: Medical evaluation before adjusting protocol.
🚨 Red Flag 5 — Complete Inability to Disengage from Visual Tool
If the visual tool becomes an obsessive fixation with 30+ minute absorption and severe distress on removal, reassess tool choice. Action: Teleconsult with Pinnacle OT.
Escalation pathway: Self-resolve → 📞 Helpline 9100 181 181 → Teleconsult → Nearest Pinnacle Center

You are not done. You are at a waypoint on a much larger journey.
D-365 Visual Stimming mastery opens multiple progression pathways depending on your child's remaining needs. Let their profile guide the next step.
Visual regulation stable →
D-366 Vestibular Stimming — add movement-based regulation
Unmet visual needs →
D-368 Advanced Visual Attention — organized visual tracking
Multiple stimming domains →
D-370 Sensory Seeking Overview — comprehensive approach

More visual regulation techniques — using materials you may already own.
D-363: Understanding Stimming
🏷️ Intro | 📚 Foundational Knowledge. Before materials — understand the neuroscience. Start here if you haven't already.
D-364: Auditory Stimming
🏷️ Core | 🎧 Auditory Regulation. If your child also covers ears, hums, or seeks specific sounds — this is D-364's domain.

D-366: Vestibular Stimming
🏷️ Core | 🌀 Movement Regulation. Spinning body, rocking, swinging — the vestibular system often co-activates with visual stimming.

D-367: Tactile Stimming
🏷️ Core | 🤚 Tactile Regulation. Hand-flapping, texture-seeking, rubbing surfaces — frequently co-occurs with visual stimming.

D-368: Visual Attention Training
🏷️ Advanced | 👁️ Visual Tracking. For children who have completed D-365 and are ready to train organized visual attention skills.

K-855: Creating a Sensory Space at Home
🏷️ Parent Guide | 🏠 Home Environment. Build the permanent sensory corner your child needs. Combines visual, tactile, and auditory tools.
This technique is one piece of a much larger plan — your child's complete developmental architecture.
D-365 addresses the Sensory Processing Domain → Visual Sub-domain. This feeds directly into Attention & Regulation, Social-Emotional Development, and Cognitive & Academic readiness. Every visual regulation session you log contributes to your child's personalized developmental trajectory.
View Full AbilityScore® Assessment
Track progress across all 12 domains simultaneously at pinnacleblooms.org/ability-score
Access EverydayTherapyProgramme™
Your personalized daily home protocol at pinnacleblooms.org/programme
From the Pinnacle Center Network — families who started where you are.
Riya, 5 years, Hyderabad
Before (Week 1): Riya would stand at the window for 40 minutes watching car headlights — unreachable, no response to name, no engagement with family dinner. Her mother described it as "watching her disappear into the light."
After (Week 8): Riya has a sensory corner with a fiber optic lamp, two sensory bottles, and a liquid timer. Window episodes have reduced by 70%. She now attends to classroom activities for 15–20 minute blocks and points to her preferred tool — the first intentional communication her family had seen.
"Now when she needs to watch something, she goes to her corner. I used to think the lights were taking her away from me. Now I understand — her brain needed light. We just needed to give her the right lights." — Riya's mother
Arjun, 7 years, Bangalore
Before: Arjun watched the washing machine spin for hours. He could not be engaged in any educational activity if the washing machine was running. Marble runs and spinning tops were added based on OT assessment identifying rotation-seeking as his primary visual need.
After (Week 6): Arjun self-selects his spin top before school preparation, uses it for 8–10 minutes, then transitions to the school routine with markedly less resistance. School reports improved sustained attention.
"The fiber optic lamp replicated the calming function of the ceiling light in a safe, controllable format. The key was proactive access — the corner was available before she became overwhelmed, not after." — Pinnacle OT, FusionModule™ Team
Isolation is the enemy of adherence. You are not navigating this alone.
📱 Visual Stimming Parent WhatsApp Group
Join 2,400+ parents navigating visual stimming. Daily tips, peer support, therapist Q&A every Friday.
💬 Pinnacle Parent Forum
Search the entire D-365 experience thread. Ask questions. Share what worked.
🤝 Peer Mentoring
Matched with a parent who has completed D-365 successfully and is 3–6 months ahead of you.
📍 Local Parent Meetup
In-person parent meetups at Pinnacle centers across 70+ locations. Quarterly sensory sessions for families.

Home + clinic = maximum impact. Your professional team is waiting.
FREE Helpline: 9100 181 181 (24x7 · 16+ languages)
🔴 Occupational Therapist — Primary Lead
Sensory Integration Specialty. Conducts the functional assessment, builds the sensory diet, and guides your entire D-365 journey.
🔵 BCBA / ABA Therapist
Functional Behavior Assessment for stimming. Identifies function, implements replacement behavior protocols, coordinates with OT and school.
🟢 Neurodevelopmental Pediatrician
Medical evaluation if red flags are present. Rules out vision impairment, assesses neurological contributors, provides medical framing for school/insurance.
Teleconsultation Option
30-minute OT teleconsult available within 48 hours. Available in: Hindi · Telugu · Tamil · Kannada · Malayalam · Bengali · Gujarati · Marathi · English + 8 more languages.
Insurance & Funding
Pinnacle works with: CGHS | ESI | Ayushman Bharat (select centers) | Private insurance (case basis)
Deeper reading for the curious parent. Every claim on this page is traceable to peer-reviewed research.
📄 PMC11506176 — Children, 2024
PRISMA systematic review: Sensory integration intervention for ASD — 16 articles, 2013–2023. Conclusion: Meets criteria for evidence-based practice. Visual regulation materials are a core component.
📄 PMC10955541 — World J Clin Cases, 2024
Meta-analysis (24 studies): Sensory integration therapy effectively promotes social skills, adaptive behavior, sensory processing, and motor skills. Effect sizes significant across domains.
📄 DOI: 10.1007/s12098-018-2747-4 — Indian J Pediatr, 2019
Padmanabha et al. — Indian RCT: Home-based sensory interventions administered by parent-trained caregivers demonstrate significant outcomes. India-specific protocol validation.
📄 PMC9978394 — WHO CCD Package, 2023
WHO Care for Child Development implementation across 54 LMICs. Caregiver-administered intervention efficacy at population scale.
📄 NCAEP Evidence-Based Practices Report, 2020
Visual supports, sensory integration therapy, and video modeling all classified as evidence-based practices for autism. National clearinghouse standard.
📄 Frontiers in Integrative Neuroscience, 2020
DOI: 10.3389/fnint.2020.556660 — Neurological basis for sensory-based interventions in ASD. Comprehensive framework analysis.
Your data helps every child like yours. Here is exactly how.
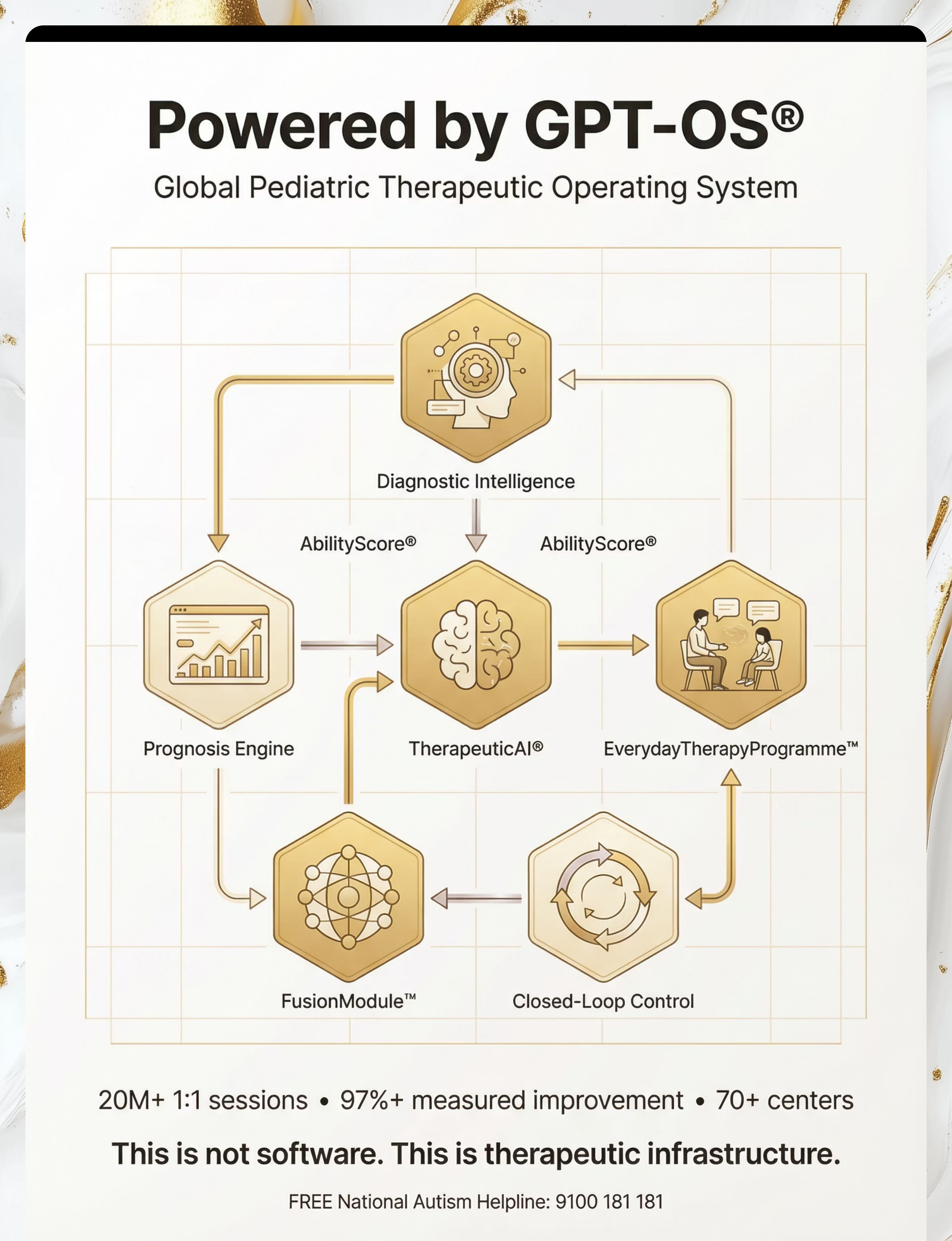
Every session you log on the D-365 tracker enters the GPT-OS® TherapeuticAI® Engine — improving recommendations not just for your child, but for every family in the Pinnacle network.
What GPT-OS® learns from D-365 data: which visual tool produces fastest engagement for a given sensory profile · optimal session duration per age · correlation between visual tool use and next-day social attention · predictors of mastery speed at population level.
🔒Privacy Assurance: All data is: De-identified | DPDP Act compliant | Stored within India | Used only for therapeutic improvement | Deletable on request.
Watch the visual demonstration. See the materials in action.
Reel ID: D-365
9 Materials That Help With Visual Stimming
Series: Sensory Processing in Children — Episode 365
Domain: Visual Stimming / Sensory Seeking / Self-Regulation
Duration: 75–85 seconds
Series: Sensory Processing in Children — Episode 365
Domain: Visual Stimming / Sensory Seeking / Self-Regulation
Duration: 75–85 seconds
"In this reel, our Pinnacle Occupational Therapy team demonstrates all 9 materials — how to introduce each one, what appropriate visual engagement looks like, and what to watch for. Visual learning complements this written protocol for maximum parent skill acquisition." — Pinnacle OT Consortium
Video modeling is classified as an evidence-based practice for autism (NCAEP, 2020). Multi-modal learning (visual + text + demonstration) significantly improves parent skill acquisition and intervention fidelity.
→ D-364
9 Materials That Help With Auditory Stimming
→ D-366
9 Materials That Help With Vestibular Stimming
→ D-363
Understanding Stimming — The Complete Guide

Consistency across caregivers multiplies impact by 3x. Share this now.
Explain to Grandparents — Simplified Version:
"Our child's brain processes visual information differently. When they stare at lights or spin things, they're not misbehaving — their nervous system needs that visual input to feel calm. The doctor and therapist have given us specific tools that give the same input safely. Please use the [liquid timer / sensory bottle] when [child's name] seems to need it. It helps them calm down."
"Our child's brain processes visual information differently. When they stare at lights or spin things, they're not misbehaving — their nervous system needs that visual input to feel calm. The doctor and therapist have given us specific tools that give the same input safely. Please use the [liquid timer / sensory bottle] when [child's name] seems to need it. It helps them calm down."
Teacher/School Communication Template:
"[Child's name] uses visual regulation tools as part of their OT-prescribed sensory diet. These tools have been clinically recommended. Please allow access during transitions and sensory breaks. The IEP/school communication letter from Pinnacle OT is attached."
"[Child's name] uses visual regulation tools as part of their OT-prescribed sensory diet. These tools have been clinically recommended. Please allow access during transitions and sensory breaks. The IEP/school communication letter from Pinnacle OT is attached."

The questions every parent asks — answered by the Pinnacle Consortium.
Q1: Should I try to stop visual stimming completely?
No. Visual stimming serves real regulatory functions. The goal is not elimination — it is channeling. Provide appropriate alternatives (the 9 materials), reduce environmental triggers, and allow regulated visual stimming in safe contexts. Trying to eliminate it entirely creates anxiety and undermines regulation.
Q2: How do I know which of the 9 materials to start with?
Match the material to what your child is currently seeking. If they stare at lights → fiber optic lamp. If they watch things spin → spinning toy. If they like slow, mesmerizing movement → liquid timer. If they need portable options → sensory bottle.
Q3: My child destroys every sensory toy I buy. What do I do?
Destruction is information — it may indicate the need for proprioceptive (heavy, resistive) input alongside visual. Start with indestructible options (sealed sensory bottle, metal spin top). Consult your OT about adding deep pressure activities.
Q4: How long before I see results?
Weeks 1–2: tolerance signs. Weeks 3–4: consolidation. Weeks 5–8: mastery (independent, self-initiated use). Total: 8 weeks for measurable change with daily sessions. Individual variation is significant.
Q5: Is visual stimming dangerous?
Most visual stimming is not dangerous. However: sun-gazing and staring at very bright lights CAN cause retinal damage. Eye-pressing CAN damage the cornea and retina. These specific behaviors are medical urgencies. See the Red Flags card and call 9100 181 181.
Q6: My child has sensory processing disorder, not autism. Do these materials still apply?
Yes. Visual stimming occurs across autism, ADHD, sensory processing disorder, developmental delay, and occasionally in neurotypical children under stress. The materials work by meeting the visual sensory need — they don't require a specific diagnosis.
Q7: Can I use these tools if my child doesn't have a diagnosis?
Yes. The materials are not diagnosis-specific. If your child shows signs of visual sensory seeking that interfere with daily functioning, the materials can help regardless of formal diagnosis. An OT evaluation is recommended for comprehensive understanding.
Q8: My child's teacher says they can't have a sensory bottle at school. What do I do?
Request a written OT recommendation for sensory tools as a school accommodation. This can be added to IEP/504 plan or a simple doctor's letter. Pinnacle OT team can provide school communication letters. Download the template from the Share card.
Preview of 9 materials that help with visual stimming Therapy Material
Below is a visual preview of 9 materials that help with visual stimming therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.







Link copied!

Your child's visual regulation journey starts today. Not tomorrow. Not after the next appointment. Today.
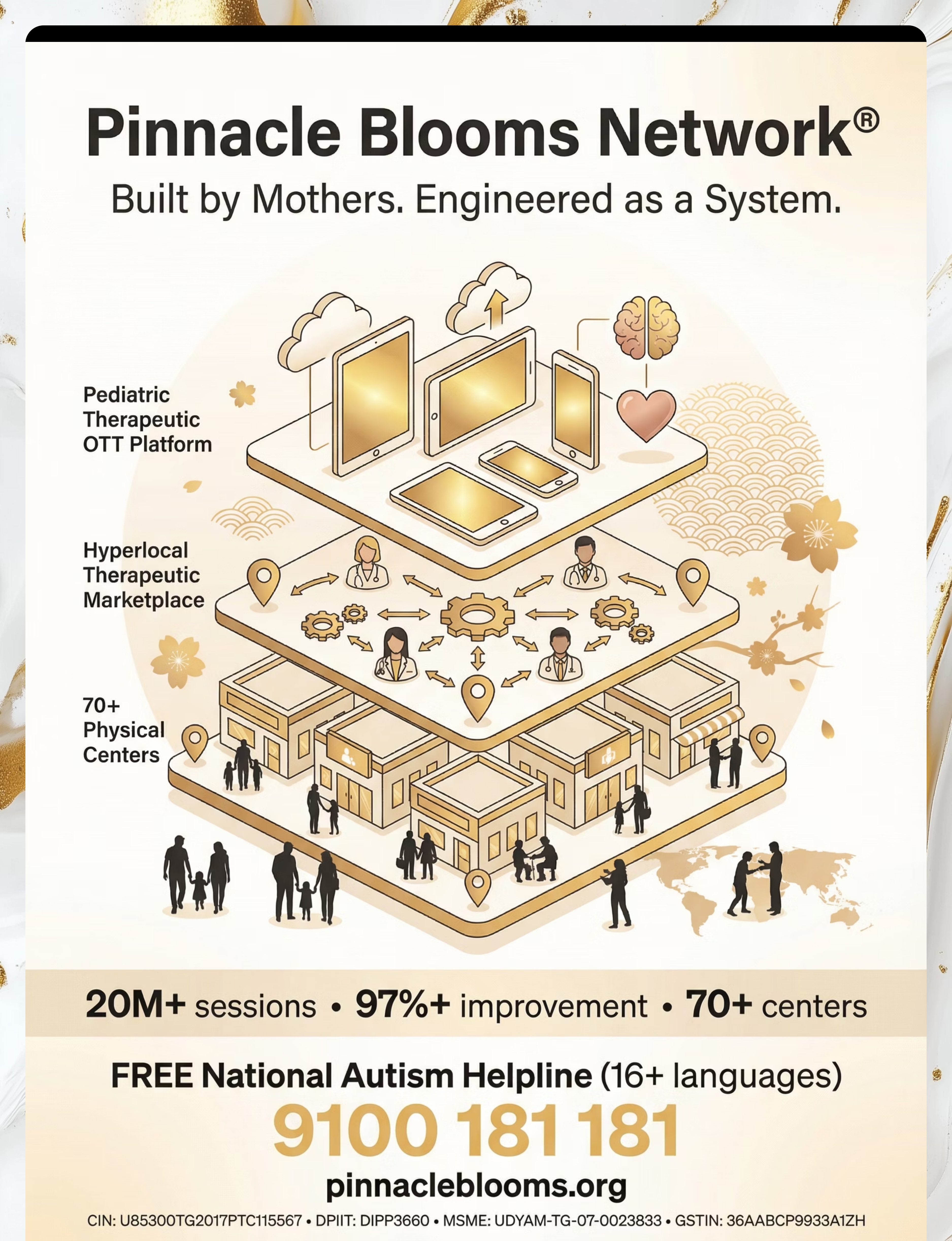
🏛️ Validated by the Pinnacle Blooms Consortium
OT • SLP • ABA/BCBA • SpEd • NeuroDev Pediatrics • CRO | 20M+ sessions | 97%+ measured improvement | 70+ centers
FREE National Autism Helpline: 9100 181 181 · 24x7 · 16+ languages · No appointment needed
🌸 PINNACLE BLOOMS NETWORK® — A unit of Bharath Healthcare Laboratories Pvt. Ltd.
"From fear to mastery. One technique at a time."
D-365 | 9 Materials That Help With Visual Stimming | Part of the techniques.pinnacleblooms.org library — evidence-linked, parent-executable, GPT-OS® governed.
Medical Disclaimer: This content is educational and does not replace individualized assessment and intervention from licensed occupational therapists, behavioral therapists, or medical professionals. Visual stimming may be associated with autism spectrum disorder, sensory processing disorder, vision impairments, or other conditions requiring professional evaluation. Sun-gazing or eye-pressing can cause eye damage — seek immediate medical intervention if these behaviors are present. Always work with qualified professionals to understand the function of stimming behavior before intervention. Individual results may vary. Statistics represent aggregate outcomes across the Pinnacle Blooms Network.
CIN: U74999TG2016PTC113063 | DPIIT Startup India: DIPP8651 | MSME Udyog Aadhaar: TS20F0009606 | GSTIN: 36AAGCB9722P1Z2
© 2025 Pinnacle Blooms Network®, a unit of Bharath Healthcare Laboratories Pvt. Ltd. All rights reserved. GPT-OS®, AbilityScore®, TherapeuticAI®, FusionModule™, EverydayTherapyProgramme™ are proprietary marks of Pinnacle Blooms Network®. Patents filed across 160+ countries.