
9 Materials That Help With Vacuum Cleaner Distress
You are not failing. Your child's nervous system is speaking.
Pinnacle Blooms Consortium®
Built by Mothers. Engineered as a System.

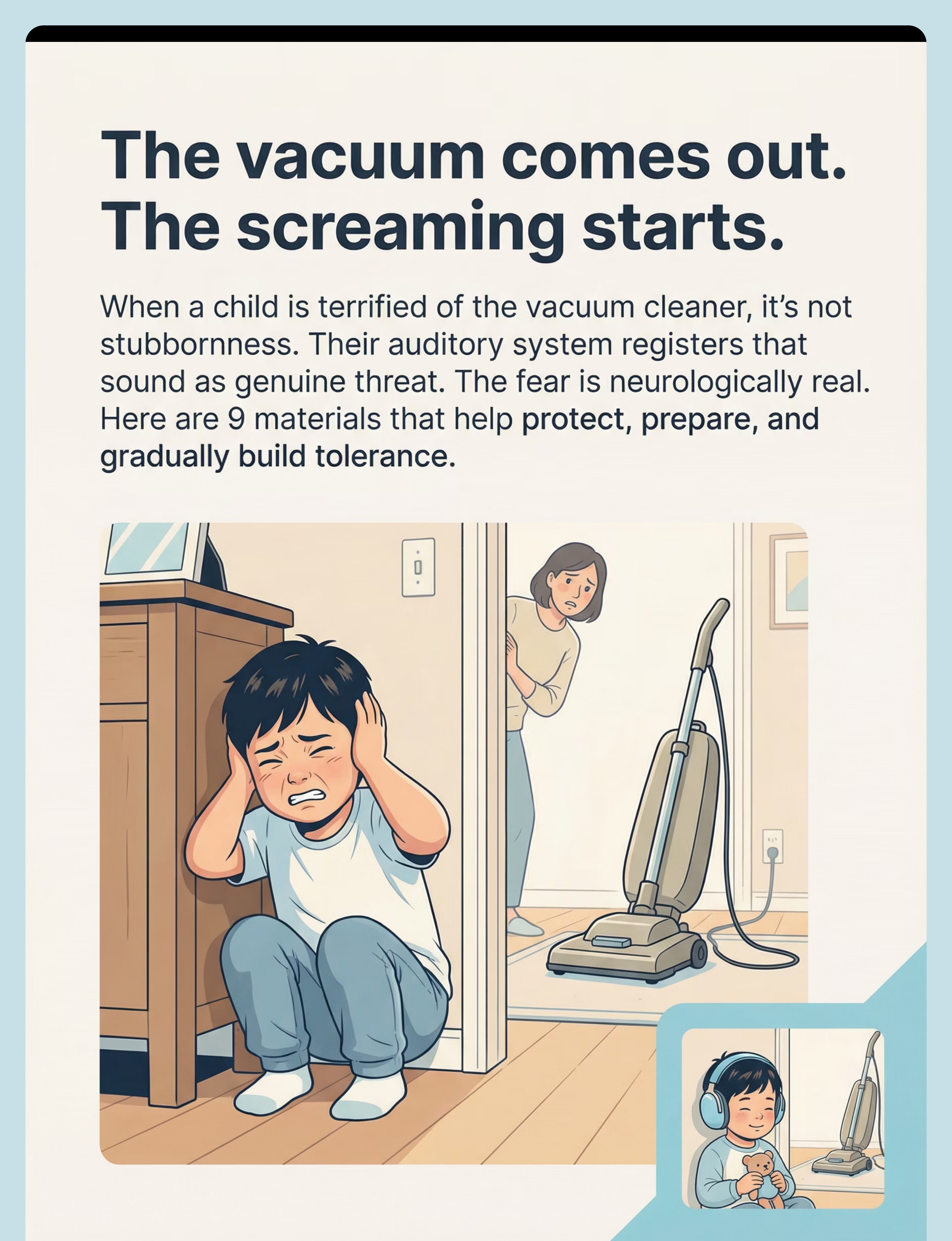
The Vacuum Comes Out. The Screaming Starts.
It's 4 PM. You need to vacuum before guests arrive. The moment your child sees the vacuum emerge from the closet — not even turned on yet — the screaming begins. Not crying. Screaming. Pure terror. He runs to the farthest room, covers his ears, and sobs until his whole body shakes. You haven't even plugged it in.
So you don't vacuum when he's home. You vacuum at midnight. You vacuum when he's at school. Your house is never clean enough because you're working around a fear that nobody seems to understand.
This is not stubbornness. This is not drama. Your child's auditory system is registering that sound as genuine danger. The fear is neurologically real.

You Are Not Alone: The Numbers
You are among millions. Across India and 70+ countries where Pinnacle serves families, vacuum cleaner distress is one of the most commonly reported challenges in pediatric auditory sensitivity. This is not rare. This is not your parenting. This is neurology.
80%
Sensory Processing Difficulties
Of children diagnosed with autism display sensory processing difficulties, with auditory over-responsivity among the most functionally disruptive (PRISMA Systematic Review, 2024 | PMC11506176)
1 in 6
Children Worldwide
Experience some form of sensory processing difficulty that impacts daily functioning (SPD Foundation, 2024)
#1
Household Trigger
Vacuum cleaners consistently rank as the most commonly reported household sound trigger in pediatric auditory sensitivity studies
References: PMC11506176 | PMC10955541 | SPD Foundation: spdfoundation.net
What's Happening in Your Child's Brain
The Auditory Alarm System — Wired Differently
Your child's brain processes sound through the same pathways as every other child. But at a critical junction — where the brain decides "is this sound safe or dangerous?" — the system over-fires.
Typical Processing
Sound enters ear → Brain filters and categorizes → "Vacuum = loud but safe" → No alarm → Child continues playing
Auditory Over-Responsivity
Sound enters ear → Brain's filtering fails to dampen → Limbic system (threat center) activates → "VACUUM = DANGER" → Fight-or-flight fires → Child screams, runs, covers ears, panics
Why Vacuums Specifically?
Vacuum cleaners produce a uniquely triggering combination:
- Low-frequency drone — felt in the body
- High-frequency whine — piercing to sensitive ears
- Unpredictable variations — perceived as threatening
- Loud sustained duration — overwhelming
- Proximal sound source — no escape
This is a wiring difference, not a behavior choice. The child cannot consciously control this response any more than you can control your blink reflex.
References: Frontiers in Integrative Neuroscience (2020) | DOI: 10.3389/fnint.2020.556660 | Porges Polyvagal Theory
Where This Sits in Development
Developmental Context
Understanding when sound sensitivity emerges — and when intervention matters most — helps you act at the right time. The critical window for auditory desensitization aligns with peak neuroplasticity.
Ages 0–2
Startle responses are normal. Auditory system still maturing. Some infants show early signs — excessive crying during loud sounds, difficulty settling in noisy environments.
Ages 2–5 — Critical Window
Auditory over-responsivity becomes clearly identifiable. Children develop anticipatory anxiety. Avoidance patterns solidify. Maximum neuroplasticity advantage for intervention.
Ages 5–8
Without intervention, avoidance patterns expand. The child's world shrinks — they avoid restaurants, birthday parties, school assemblies, public restrooms.
Ages 8–12
Established patterns are harder (not impossible) to change. Child may develop compensatory strategies but also anxiety disorders and social withdrawal.
Common co-occurrences: Tactile sensitivity (doesn't like certain textures), visual sensitivity (light bothers them), vestibular sensitivity (motion sickness, fear of swings), generalized anxiety.
References: WHO Care for Child Development (CCD) Package 2023 | PMC9978394 | UNICEF MICS developmental indicators

The Evidence Behind This Technique
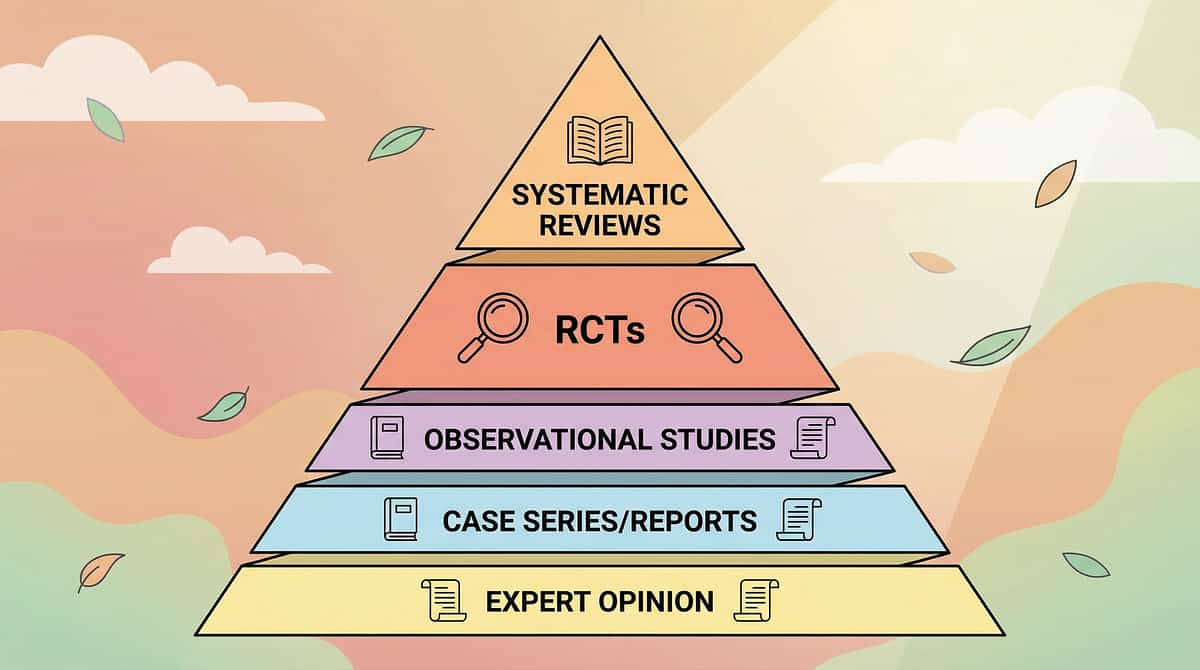
Evidence Grade: Level II
Supported by Systematic Reviews and RCTs
PRISMA Systematic Review (2024)
16 articles from 2013–2023 confirm sensory integration intervention meets criteria for evidence-based practice in children with ASD. Auditory processing interventions specifically included. | PMC11506176
Meta-Analysis (2024)
Across 24 studies, sensory integration therapy effectively promoted social skills, adaptive behavior, sensory processing, and motor skills. Environmental adaptability improved significantly. | PMC10955541
Indian RCT (2019)
Home-based sensory interventions demonstrated significant outcomes when administered by trained parents. Safety and efficacy established for the Indian demographic and home context. | Padmanabha et al., Indian J Pediatr
SPD Foundation Consensus
Auditory over-responsivity intervention combining protection, graduated exposure, and environmental modification is established clinical practice across occupational therapy protocols worldwide.
Clinically validated. Home-applicable. Parent-proven.

The Technique: What It Is
SEN-AUD-DEF
Sensory Processing — Auditory
Auditory Desensitization Protocol for Household Sound Tolerance
Parent-Friendly Name: "Vacuum Bravery Building"
A structured, multi-material approach that combines auditory protection, environmental predictability, graduated sound exposure, nervous system regulation tools, and child-led mastery experiences to systematically reduce fear and build functional tolerance to vacuum cleaner sounds and related household appliance sounds.
This is not one technique — it is a coordinated protocol using 9 evidence-backed materials that work together across the dimensions of PROTECT → PREDICT → EXPOSE → REGULATE → CONTROL.
Age Range
2–12 years
Setting
Home + Therapy + School + Community
Duration
Ongoing (weeks to months)
Frequency
Daily + weekly structured exposure
Who Uses This Technique
This technique crosses therapy boundaries because the brain doesn't organize by therapy type. A coordinated team ensures every dimension of auditory sensitivity is addressed.
Primary: Occupational Therapist (OT)
Designs the sensory diet, selects appropriate auditory protection levels, implements therapeutic listening programs, guides graduated desensitization protocol, and monitors auditory processing improvement through standardized assessment.
Secondary: Board Certified Behavior Analyst (BCBA)
Designs reinforcement schedules for tolerance building, implements systematic desensitization using ABA principles, creates behavior support plans for sound-related distress, and tracks data on tolerance progression.
Contributing: Speech-Language Pathologist (SLP)
Addresses auditory processing components that overlap with receptive language processing. Supports social story development and communication strategies during sound distress.
Contributing: NeuroDevelopmental Pediatrician
Differential diagnosis between auditory over-responsivity, hyperacusis, anxiety disorder, and trauma response. Medical evaluation for underlying auditory system differences. Coordination with audiology if structural concerns exist.
References: Adapted UNICEF/WHO Nurturing Care Framework for SLPs (2022) | DOI: 10.1080/17549507.2022.2141327

What This Targets
Therapeutic Target Map
Primary Target
Auditory Tolerance & Sound Processing Regulation. Child remains in environment during vacuum use. Fear response duration decreases. Anticipatory anxiety reduces. Recovery time after exposure shortens.
Long-Term Gains
Environmental adaptability — child functions in sound-rich environments. Community participation — birthday parties, restaurants, school events. Independence in daily living. Foundational self-regulation transfers to other challenges.
References: PMC10955541 | Meta-analysis on sensory integration therapy targets

What You Need: 9 Primary Materials
Clinically Selected, Home-Ready
# | Material | Canon Category | Price Range (INR) | Priority | |
1 | Noise-Canceling Headphones / Ear Defenders | Sensory Regulation Tools | ₹1,500–8,000 | ESSENTIAL | |
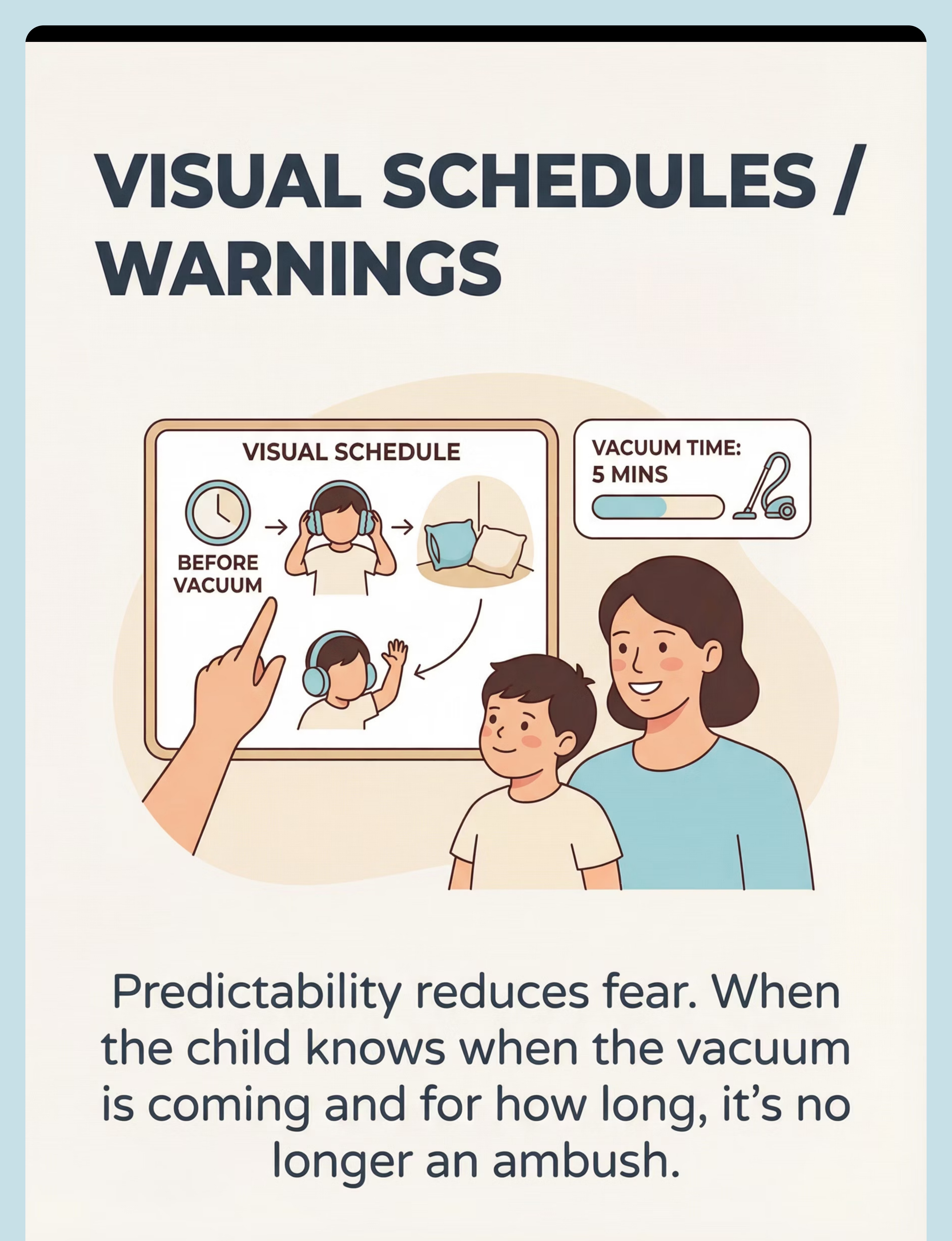
2 | Visual Schedules / Sound Warnings | Visual Supports | ₹100–500 | ESSENTIAL | |
3 | Graduated Sound Exposure Recordings | Auditory Processing Materials | ₹0–500 | ESSENTIAL | |
4 | Safe Space / Retreat Zone Setup | Environmental Modification | ₹500–3,000 | HIGH | |
5 | Social Stories / Therapeutic Narratives | Cognitive-Behavioral Tools | ₹0–500 | HIGH | |
6 | Calming Sensory Tools (weighted, tactile, proprioceptive) | Sensory Regulation Tools | ₹300–2,000 | HIGH | |
7 | Child-Controlled Vacuum Experience | Exposure Therapy Tools | ₹0 | MODERATE | |
8 | Therapeutic Listening Programs | Professional Auditory Tools | ₹5,000–25,000 | PROFESSIONAL | |
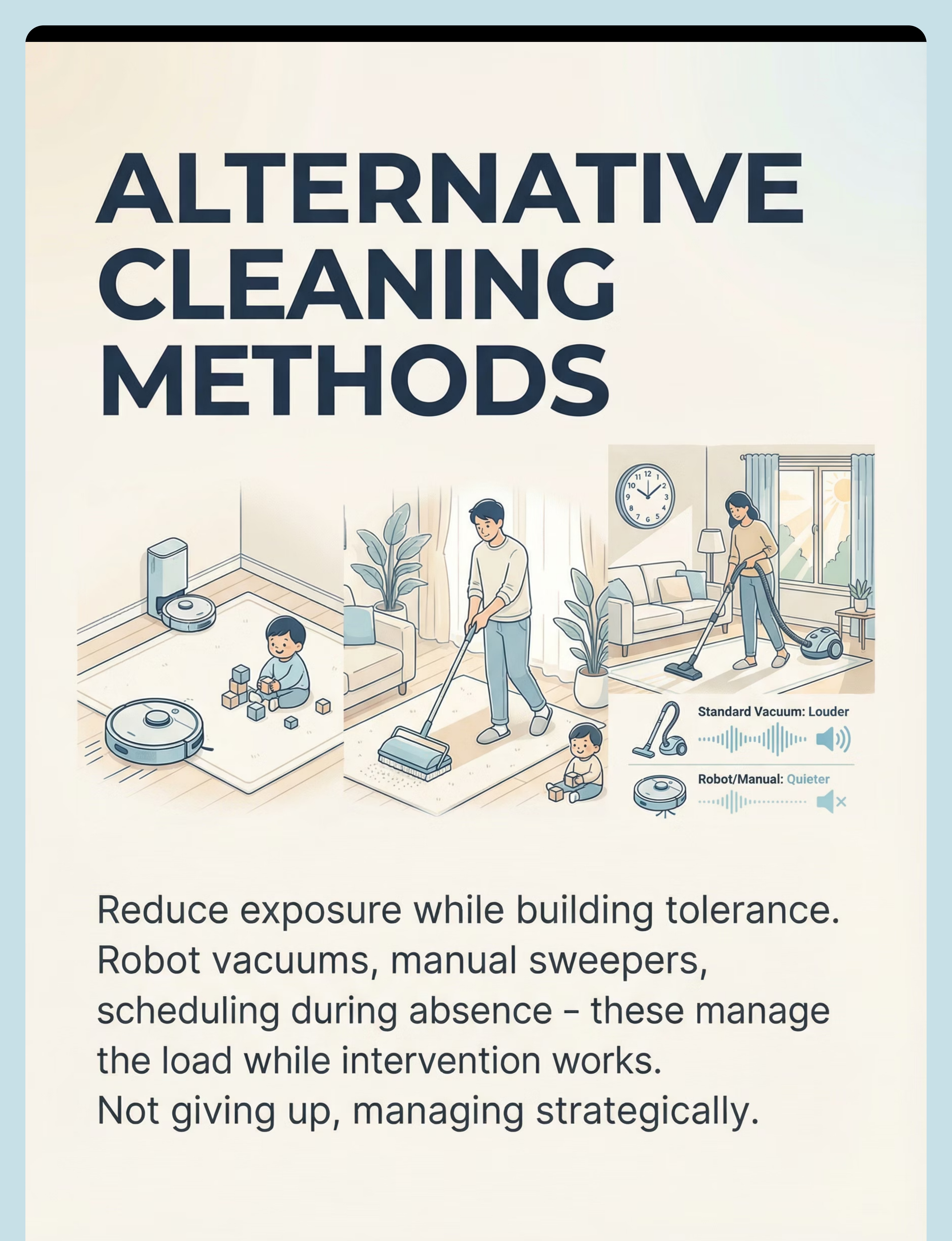
9 | Alternative Cleaning Methods | Environmental Modification | ₹2,000–30,000 | SUPPORTIVE |
Total Investment Range: ₹0–30,000 (essential starter kit: ₹1,600–8,500)
DIY & Zero-Cost Alternatives
Every parent can start TODAY — regardless of budget.
Headphones → Hardware Store Earmuffs
Industrial hearing protection earmuffs from any hardware store (₹300–500) provide excellent passive noise reduction. Over-ear construction headphones work surprisingly well.
Visual Schedule → Hand-Drawn Cards
Hand-drawn picture cards on paper, laminated with clear tape. Use phone photos of your vacuum + clock + headphones to create a custom schedule. Free.
Sound Recordings → Your Phone
Record your own vacuum on your phone. Play from YouTube "vacuum sounds" at the lowest setting. Use your phone speaker at minimum volume. Completely free.
Safe Space → Blanket Fort
Blanket fort with cushions in the farthest room. A large cardboard box with blankets inside works beautifully. Children often prefer their own creations.
Social Stories → Homemade Photo Book
Photograph your child, your vacuum, their headphones, their safe space. Narrate: "The vacuum helps clean. It makes loud noise. The noise won't hurt me. I can wear my headphones. I am brave."
Weighted Animal → Rice-Filled Sock
Fill a sock with rice or lentils, tie closed. Place inside a stuffed animal cover. Instant weighted comfort tool for pennies.
Note: Therapeutic Listening Programs (Material 8) have no DIY substitute — they require trained professional guidance. Contact Pinnacle for assessment.
"The WHO Nurturing Care Framework emphasizes context-specific, equity-focused interventions. These household alternatives honor that principle." | PMC9978394

Safety First: Before You Begin
Critical Safety Check
🔴 DO NOT PROCEED IF
- Child has a history of seizures triggered by sound
- Child has an active ear infection, ear tubes, or recent ear surgery
- Child is currently in severe distress or dysregulated state
- Child has expressed fear of being forced to listen (indicates prior traumatic exposure)
- You are feeling frustrated or impatient — your emotional state transfers to the child
🟡 PROCEED WITH MODIFICATION IF
- Child is tired, hungry, or had a difficult day → shorten session, increase protection
- Child has a cold or congestion → auditory processing may be temporarily altered
- New or unfamiliar environment → baseline anxiety already elevated
- Multiple caregivers present → designate one lead; consistency is critical
🟢 OPTIMAL CONDITIONS
- Child is fed, rested, and in a calm-alert state
- You have at least 20 uninterrupted minutes
- Headphones are fitted and tested; safe space is prepared
- Visual schedule warning has been given
- You feel calm and patient
CRITICAL: Never force exposure. If you see panic, STOP. Retreat to safety. Try again another day. Forced exposure creates trauma, not tolerance.

Set Up Your Space
Room Configuration
Before your first session, set up your home environment for success. Thoughtful positioning creates the physical architecture of safety your child's nervous system needs.
Safe Space (Farthest Room)
Pop-up tent or blanket fort with beanbag or cushions inside. Headphones stored here. Preferred comfort items (stuffed animals, blankets). White noise machine optional. Visual "safe space in use" indicator on door.
Visual Schedule Station (Common Area)
Weekly vacuum schedule posted at child's eye level. Today's vacuum time highlighted. Timer visible. Sequence cards: Warning → Headphones → Safe Space → Vacuum On → Vacuum Off → All Done.
Headphone Station (Child-Accessible)
Headphones hanging on child-accessible hook. Backup earplugs available. Child can self-serve at any time — this is about their control.
Vacuuming Area (Maximum Distance)
As far from safe space as possible in initial phases. Close doors between areas. Use rugs to dampen sound transmission. Consider hallway as sound buffer zone.
Temperature tip: Headphones can make ears warm — ensure the room isn't overheated, especially in Indian summers.
Is Your Child Ready? Readiness Check
60-Second Pre-Session Assessment
Child is fed
Last meal within 2 hours
Child is rested
Adequate sleep last night
No recent stressor
No meltdown or significant stressor in the past hour
Ear health is normal
No infection, no complaints of ear pain
Headphones are ready
Charged, tested, and child is comfortable wearing them
Space is prepared
Safe space accessible, visual schedule warning given
Parent is calm
You are patient and emotionally available
All Checked → GO
Proceed to Step 1
1-2 Unchecked → MODIFY
Shortened protocol only
3+ Unchecked → POSTPONE
Offer calming activity instead
"The best session is one that starts right."

Step 1: The Invitation
The Warning & Preparation
5–10 minutes before vacuum time
"[Child's name], vacuum time is coming in 5 minutes. Let's look at our schedule. See? First we get our headphones. Then we can go to our cozy space. The vacuum will be on for [specific time]. Then it will be ALL DONE. You're safe. Let's get ready together."
Body Language
Calm, unhurried. Get down to child's eye level. Point to each step on the visual schedule. Let the child process each step before moving to the next.
Acceptance Looks Like
- Child reaches for headphones
- Child moves toward safe space
- Child nods or indicates understanding
- Even passive compliance is acceptance at early stages
Resistance Looks Like
- Child begins crying at the warning
- Child freezes or runs away
Response: Do NOT chase or force. Say: "I see you're not ready. That's okay. We'll try again later." Return to preferred activity.
Timing: 5–10 minutes. Do not rush this step. The warning IS the intervention at early stages.

Step 2: The Engagement
Protection & Positioning
2–5 minutes
"Great job getting ready! Let's put on your headphones. How do they feel? Comfortable? Now let's go to our cozy space. Bring [comfort object]. The vacuum will start soon, and you're going to be safe the whole time."
Fit Headphones
Help child put on noise-canceling headphones — check fit, ensure comfort, verify sound reduction
Provide Sensory Tool
Hand child their preferred calming sensory tool — weighted stuffed animal, stress ball, or chewy tube
Enter Safe Space
Guide child to safe space — let them arrange it how they want. Their control matters.
Set Visual Timer
Place timer where child can see it: "The vacuum will be on for [3/5/10] minutes"
Engaged
Actively preparing, seems empowered → proceed normally
Tolerating
Compliant but tense → proceed with extra verbal reassurance
Avoidant
Resists headphones or safe space → offer choice, never force

Step 3: The Therapeutic Action
Vacuum Exposure with Full Protection
3–15 minutes
This is the core therapeutic event. Parent begins vacuuming in the designated area while child is in safe space with full protection — headphones, comfort items, distance, and timer.
Announce
"Starting the vacuum now!" (even if child has headphones — consistency matters)
Vacuum for Exact Time
Vacuum for the EXACT time shown on the timer. Not longer. Consistency builds trust.
Announce Completion
"ALL DONE! Vacuum is off!" — clear, celebratory tone
Duration Guidelines
1
Weeks 1–2
2–3 minutes maximum
2
Weeks 3–4
5 minutes
3
Weeks 5–8
10–15 minutes (normal vacuum duration)
Common Execution Error: Vacuuming longer than the timer shows. This destroys the predictability framework. If the timer says 5 minutes, stop at 5 minutes — even if the floor isn't done.
Monitor from the safe space doorway during vacuuming. Ideal: child is calm, engaged with activity. Acceptable: child is tense but staying. Concerning: child is crying or panicking — STOP vacuuming immediately.

Step 4: Repeat & Vary
Building the Pattern
Ongoing — daily or every-other-day
Repetition Schedule
- Optimal: 5–7 sessions per week at consistent time
- Minimum: 3 sessions per week for progress
- Daily vacuum exposure (even brief) builds tolerance faster than weekly
Satiation Indicators
- Child asks to stop → honor immediately
- Child shows increasing distress despite protection → stop
- Child has been calm for full timer duration → session complete, celebrate!
Variation Options (introduce after 2 weeks of stable tolerance)
Distance
Gradually move safe space closer: farthest room → adjacent room → hallway → same room (opposite end) → same room (closer)
Protection
Reduce layers: headphones + safe space → headphones only → earplugs → no protection with distance → no protection same room
Duration
Gradually increase vacuum time as tolerance permits
Vacuum Type
Different vacuum = different sound profile. Once tolerance builds for one, test with a different type.
"3 good sessions > 10 forced ones. Quality over quantity."
Step 5: Reinforce & Celebrate
Immediate Reinforcement
Within 30 seconds of vacuum off
"You did it! The vacuum was on for [time] minutes and you stayed so brave! I am SO proud of you. [High five / hug]. You earned your [reward]!"
Reinforcement Timing: Within 3 seconds of session completion. Delayed reinforcement loses effectiveness.
Verbal Praise (Specific)
"You stayed in your cozy space for the WHOLE time!" NOT just "Good job." Specific praise reinforces the exact behavior you want repeated.
Physical
High five, hug, thumbs up — follow your child's preference for physical connection
Token
Sticker on chart. After 5–10 stickers → preferred activity or small reward. Visual progress your child can see.
Activity
5 minutes of preferred activity immediately after session. Natural: "Now the floor is clean and we can play on it!"
Pro Tip: Celebrate the attempt, not just the success. If the child tried but needed to stop early — that attempt gets celebrated too.

Step 6: The Cool-Down
Transition Back to Baseline
3–5 minutes
"Vacuum time is all done. You were so brave. Let's take off your headphones when you're ready. No rush. [Pause]. Would you like to [preferred activity] now?"
Announce & Show
Announce vacuum is off and stored away. Some children need to see the vacuum put away to feel safe.
Child-Led Removal
Let child remove headphones at their own pace — do not rush removal. If child wants to keep them on, that's okay.
Offer Calming Input
Deep pressure hug, weighted blanket moment, preferred fidget — whatever grounds your child.
Transition to Preferred Activity
Within 5 minutes. Do NOT discuss the session extensively right after — let the child move on.
If Child Was Distressed: If the session was cut short, do NOT lecture or process. Simply say: "It's all done. You're safe. We'll try again another day." Offer comfort. The child's nervous system needs recovery, not analysis.
References: NCAEP Evidence-Based Practices Report (2020) — Visual supports for transitions

Capture the Data: Right Now
60-Second Post-Session Data Capture
Record these 3 data points within 60 seconds of session end. Fresh data is accurate data — and accuracy drives your child's progress.
1. Duration Tolerated
How many minutes was the vacuum on before child needed it to stop (or timer ran out)? _____ minutes
2. Protection Level Used
Full (headphones + safe space + distance) | Moderate (headphones + same room) | Minimal (earplugs or no protection) | None
3. Distress Level (1-5)
1 = Calm throughout | 2 = Mild tension | 3 = Visible distress but stayed | 4 = Needed to stop early | 5 = Full panic/meltdown
Optional: Notes — anything different today? New behavior? Unexpected reaction?
"60 seconds of data now saves hours of guessing later."

What If It Didn't Go as Planned?
Common Problems & Immediate Fixes
Child panicked even with headphones and safe space
Why: Sound is still too intense, or anticipatory anxiety is overwhelming. Fix: Increase distance. Try double protection (earplugs under headphones). Reduce vacuum to 30 seconds. Consider postponing today.
Child refused to put on headphones
Why: Headphones may cause sensory discomfort (pressure, warmth). Fix: Practice wearing during calm times with preferred music. Try different style (over-ear vs. headband vs. earplugs). Let child choose.
Seemed fine during vacuum, melted down 20 min later
Why: Delayed stress response — nervous system held it together then needed to discharge. Fix: This is actually progress! Add extended cool-down time. Offer more sensory regulation input after.
Okay at home but panics at other vacuums
Why: Generalization hasn't occurred. Different vacuum = different sound = new threat. Fix: Practice with recordings of different types. Bring portable headphones everywhere.
Progress stalled after 3 weeks
Why: May need professional assessment. Fix: Book OT evaluation through Pinnacle. Ensure consistency — inconsistency is the #1 progress killer.
Other family members don't follow the protocol
Why: Grandparents/helpers may vacuum without warning. Fix: Share the Family Guide. Post visual schedule prominently. Explain: "Vacuuming without warning undoes weeks of work."
"Session abandonment is not failure — it's data."
Adapt & Personalize
Personalization Matrix
1
← Easier Version
Vacuum sound recording at lowest volume on phone (not actual vacuum). Farthest room, double protection, 30 seconds, all comfort items, parent nearby for co-regulation.
2
Standard Version
Actual vacuum in designated area. Child in safe space with headphones and comfort items. Timed exposure. Post-session data capture.
3
Harder Version →
Child in same room (with headphones). Child controls on/off switch. Extended duration. Reduced protection. Different vacuums and locations.
Age-Based Modifications
Ages 2–4
Shorter sessions (2–3 min max). Simple visual schedule (2–3 steps). Parent-led entirely. Safe space = parent's lap with headphones.
Ages 5–8
Standard protocol. Child participates in schedule management. Can earn tokens. Social story integration effective.
Ages 9–12
Child-led protocol. Child sets their own goals. Discussion-based (cognitive) alongside sensory approach. Privacy around fear is important — don't embarrass.

Weeks 1–2: What to Expect
Building the Foundation
15%
Progress Bar
Foundation-building phase
What progress looks like at this stage
- Child tolerates putting on headphones (even briefly)
- Child will go to safe space when warned (even reluctantly)
- Fear response is still present BUT recovery time is slightly shorter
- Anticipatory anxiety when seeing schedule — this is PROGRESS (they're reading the schedule, meaning predictability is working)
- Duration tolerated: 1–3 minutes with full protection
What is NOT progress yet (and that's okay)
- Child is not calm during vacuuming — they're tolerating, not enjoying
- Child still doesn't want headphones removed
- Distress is present — but SHORTER and RECOVERABLE
"If your child tolerated the vacuum for 30 seconds longer than last week — that's 30 seconds of new neural pathway. That's real progress."
Parent emotional preparation: You may feel like nothing is working. You are laying invisible groundwork. Neuroplasticity doesn't announce itself.

Weeks 3–4: Consolidation Signs
The Neural Pathways Are Forming
40%
Progress Bar
Consolidation phase
Consolidation indicators
Self-Initiation
Child begins reaching for headphones THEMSELVES when vacuum time is announced — the first sign of self-advocacy emerging.
Reduced Intensity
Reduced crying/screaming — may still look tense but no longer panicking. Startle response to vacuum turning on is less intense.
Curiosity Emerging
Child may peek out of safe space during vacuuming. Some children begin asking "how long?" — this is cognitive engagement with the protocol.
Faster Recovery
Recovery time after session drops from 30+ minutes to under 10 minutes. Tolerance may generalize to vacuum sounds on TV.
When to increase challenge: If child has shown stable tolerance (distress level 1–2) for 5 consecutive sessions → reduce one protection layer OR increase duration by 2 minutes.
"You may notice you're more confident too. Parental self-efficacy is a real metric — and yours is rising."

Weeks 5–8: From Tolerance to Mastery
Mastery Indicators
75%
Progress Bar
Mastery phase
Mastery Criteria
- Child remains in same room as running vacuum with only headphones
- Distress level consistently 1–2 during sessions
- Child can be warned 5 minutes before vacuum (vs. 30 initially) without escalating
- Child voluntarily approaches vacuum (off) — touches it, pushes it
- Some children: child presses the ON button themselves (with headphones)
Generalization Indicators
- Tolerance of blender or mixer grinder improves WITHOUT specific intervention
- Child enters public restrooms with hand dryers (with headphones)
- Reduced startle response to unexpected sounds
- Willingness to attend birthday parties, school assemblies
🏆MASTERY UNLOCKED when child tolerates parent vacuuming in adjacent room without ear protection for 5+ minutes, on 3 separate occasions, without significant distress.
References: PMC10955541 | BACB mastery criteria standards

Celebrate This Win
Remember Card 1? The child who screamed at the sight of the vacuum. The parent who vacuumed at midnight. The house that was never clean enough.
Look where you are now.
Your child has a toolkit. Headphones they reach for themselves. A safe space they chose. A schedule they understand. A vacuum they no longer fear — or at least, a vacuum they can tolerate. And that tolerance? It's spreading to blenders, hair dryers, and school assemblies.
You didn't just build vacuum tolerance. You rebuilt your child's relationship with sound.
Your child grew because of YOUR commitment. Every consistent session. Every patient warning. Every time you stopped the vacuum when the timer said stop — even though the floor wasn't done. Every time you celebrated 30 seconds of bravery like it was a gold medal.
Family celebration suggestion: Let your child vacuum one room (with headphones if needed). Take a photo. Frame it. This is a milestone.
"From fear to mastery. One technique at a time."
Red Flags: When to Pause
Seek Professional Consultation If:
🔴 Sound sensitivity is WORSENING after 4+ weeks
Fear spreading to new sounds. Tolerance decreasing. Avoidance expanding. Action: Book OT sensory processing evaluation → Call Pinnacle Helpline 9100 181 181
🔴 Anticipatory anxiety spreading beyond vacuum
Child anxious in any environment where loud sounds might occur. Refuses kitchens, bathrooms, stores. Action: Developmental pediatrician + OT evaluation
🔴 Signs of trauma response
Nightmares about sounds. Regression in toileting, eating, sleep. Flashback-like responses. Action: Pause all exposure. Seek psychology/counseling. Resume only with professional guidance.
🔴 Physical symptoms during exposure
Nausea, vomiting, headaches, dizziness, or ear pain during/after. May indicate hyperacusis with medical correlate. Action: ENT evaluation + audiology assessment.
🔴 Protocol causing family stress or conflict
Parents arguing about approach. Child's fear becoming the family's central focus. Siblings resentful. Action: Family counseling. Pinnacle parent support group.
"Trust your instincts — if something feels wrong, pause and ask."
The Progression Pathway
Your Developmental GPS
Your path forward depends on your child's unique response. If vacuum tolerance is achieved, you can generalize to other sounds (Path A), pursue deeper auditory processing work with a professional (Path B), or address other sensory areas that need attention (Path C).
Long-term goal: Environmental Adaptability Index improvement → Child functions in sound-rich environments with independence and minimal accommodation.
Related Techniques in This Domain
Domain A: Sensory Processing — Auditory
Technique | Difficulty | Materials You Already Own | |
A-034: Fire Alarm Anxiety | Core | Headphones ✓, Visual Schedules ✓, Social Stories ✓ | |
A-035: Hand Dryer Fear (Public Restrooms) | Core | Headphones ✓, Social Stories ✓, Sensory Tools ✓ | |
A-036: Birthday Party Sound Overwhelm | Core | Headphones ✓, Safe Space concepts ✓, Visual Schedules ✓ | |
A-037: Sensitivity to Sudden Sounds | Advanced | Headphones ✓, Sound Recordings ✓ | |
A-031: Body Awareness Difficulties | Intro | Sensory Tools (partial overlap) | |
A-032: Mouthing Objects Beyond Age | Intro | Chewy tubes from sensory tools ✓ |
"You already own materials for 5 of these 6 techniques." Your investment in noise-canceling headphones, visual schedules, and calming sensory tools transfers directly.
Your Child's Full Developmental Map
The Big Picture
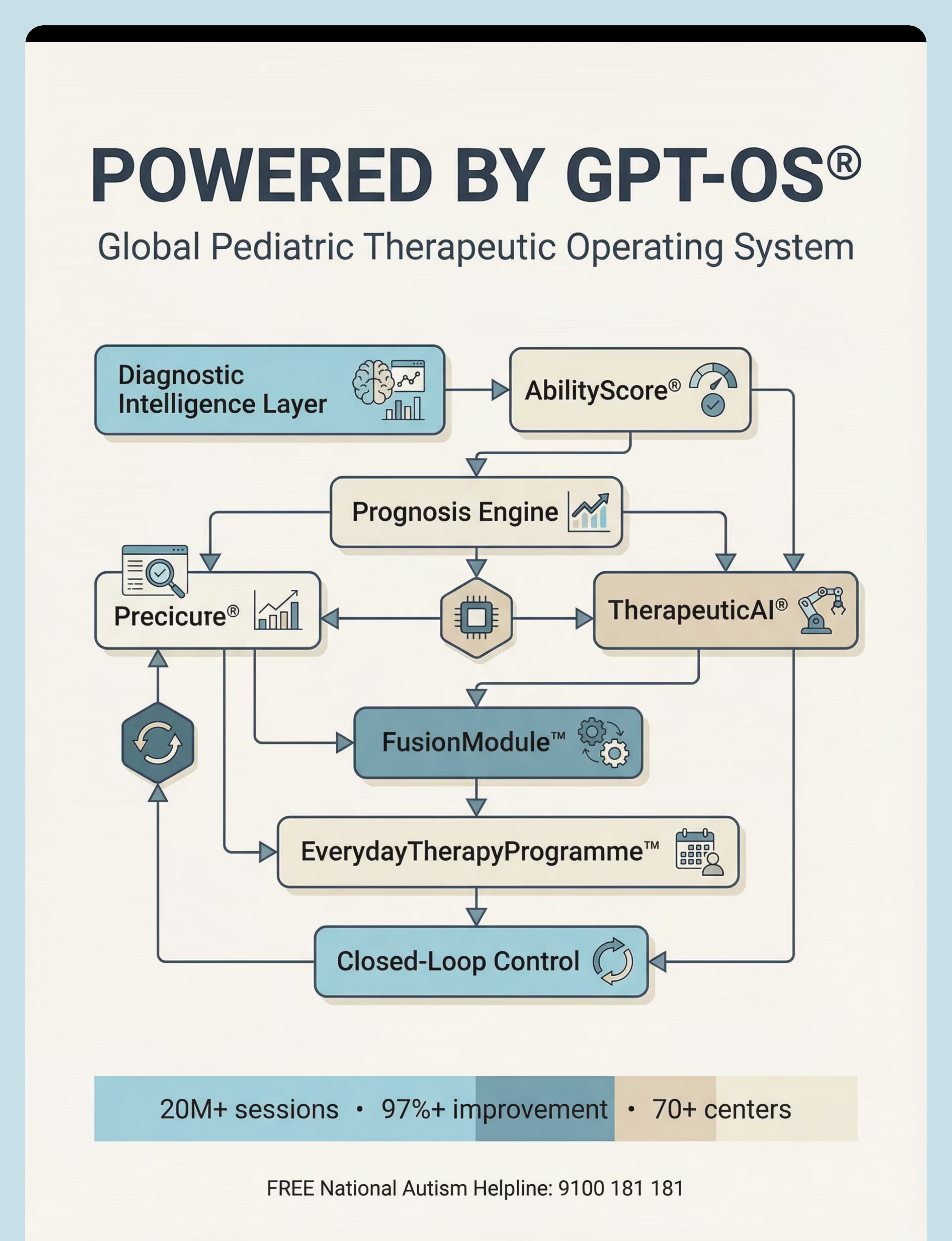
Auditory tolerance is one vital piece of a much larger developmental journey. The Pinnacle GPT-OS® framework encompasses 12 interconnected developmental domains — and this technique feeds into four of them.
A — Sensory Processing
← CURRENT (Auditory sub-domain)
1
B — Communication
Language & interaction
2
C — Social Skills
Interaction & engagement
3
D — Motor Skills
Gross & fine motor
4
E — Adaptive Behavior
Environmental adaptability ↑
5
G — Emotional Regulation
Anxiety reduction ↑
6
This technique (A-033) feeds into: Domain A (primary: Auditory Processing ↑), Domain E (secondary: Environmental Adaptability ↑), Domain G (tertiary: Anxiety Reduction ↑), Domain L (tertiary: Community Participation ↑).

Your Child's Full Developmental Map
The Big Picture
Auditory tolerance is one vital piece of a much larger developmental journey. The Pinnacle GPT-OS® framework encompasses 12 interconnected developmental domains — and this technique feeds into four of them.
A — Sensory Processing
← CURRENT (Auditory sub-domain)
B — Communication
Language & interaction
C — Social Skills
Interaction & engagement
D — Motor Skills
Gross & fine motor
E — Adaptive Behavior
Environmental adaptability ↑
G — Emotional Regulation
Anxiety reduction ↑
This technique (A-033) feeds into: Domain A (primary: Auditory Processing ↑), Domain E (secondary: Environmental Adaptability ↑), Domain G (tertiary: Anxiety Reduction ↑), Domain L (tertiary: Community Participation ↑).
Families Who've Been Here
From the Living Rooms of Real Families
Arun, Age 4 — Hyderabad
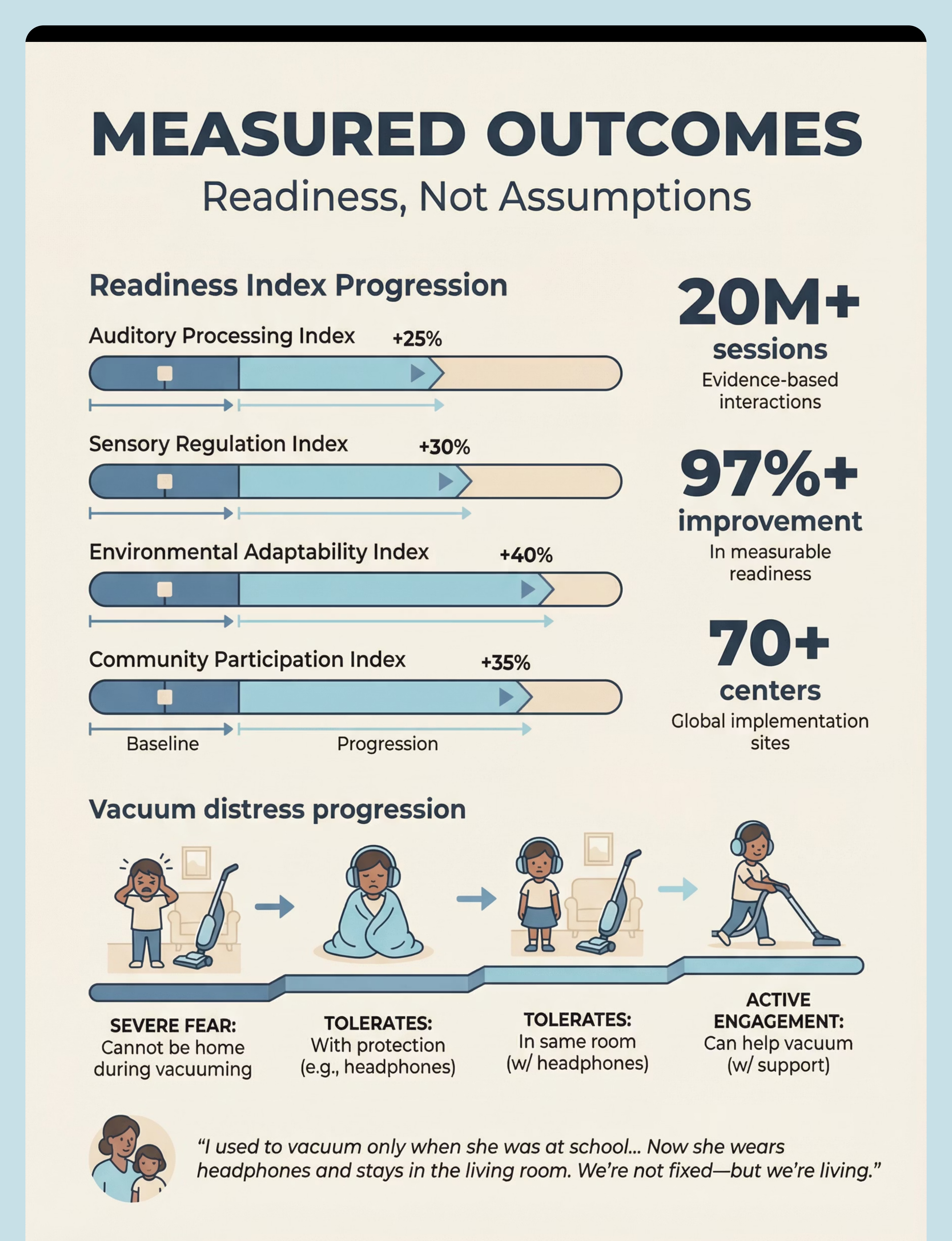
Before: Could not be in the house during vacuuming. Mother vacuumed only during school hours. Neighbors' vacuum triggered meltdowns through walls.
After (12 weeks): Tolerates vacuum with headphones in adjacent room. Stays in living room during blender use. Attended cousin's birthday party with headphones and pre-briefing.
"We're not fixed — but we're living." — Mother
Priya, Age 7 — Bengaluru
Before: Full panic attacks when vacuum turned on — screaming, running, hitting to escape. Mother hadn't vacuumed in months.
After (8 weeks): Watches vacuum from doorway with headphones. Last week, pressed the ON button for 2 seconds.
"The look on her face — she was scared but she was proud. Both at the same time." — Father
Illustrative cases; individual outcomes vary by child profile and protocol adherence.

Connect With Other Parents
You're Not Doing This Alone
The journey through auditory sensitivity is easier when you're walking it with others who understand. Every family in these communities has been exactly where you are — some are just a few weeks ahead.
WhatsApp Group
Sound Sensitivity Parent Group — moderated by Pinnacle OT team. Real-time support from parents who get it.
Community Forum
Share progress, ask questions, and celebrate wins with families across India and globally.
Peer Mentoring
Connect with a parent who has already navigated this challenge. Your future self is someone else's mentor.
"The parent who vacuumed at midnight last year may be the parent who gives YOU hope this year."
Your Professional Support Team
Home + Clinic = Maximum Impact
Therapist Matching
Primary: Occupational Therapist — Sensory Integration Specialist
Supporting: BCBA for behavior support plan | SLP if language processing co-occurs | NeuroDev Pediatrician for differential diagnosis
What to Request
- Comprehensive Sensory Processing Evaluation
- Auditory Processing Profile Assessment
- Therapeutic Listening Program Candidacy
- EverydayTherapyProgramme™ Personalization
Access Points
70+ centers across all states. Teleconsultation available for families without center access — video consultation with Pinnacle OT team.
FREE National Autism Helpline
📞9100 181 181
Available 24x7 | 16+ languages
Available 24x7 | 16+ languages
You're Not Doing This Alone
The journey through auditory sensitivity is easier when you're walking it with others who understand. Every family in these communities has been exactly where you are — some are just a few weeks ahead.
WhatsApp Group
Sound Sensitivity Parent Group — moderated by Pinnacle OT team. Real-time support from parents who get it.
Community Forum
Share progress, ask questions, and celebrate wins with families across India and globally.
Peer Mentoring
Connect with a parent who has already navigated this challenge. Your future self is someone else's mentor.
"The parent who vacuumed at midnight last year may be the parent who gives YOU hope this year."
The Research Library
The Science Behind This Technique
For the curious parent, the committed therapist, or the program lead who needs evidence before scaling — here is the research foundation underpinning every recommendation on this page.
Systematic Review (Level I)
"Sensory Integration for Children with ASD" — PRISMA review of 16 articles (2013–2023). Confirms evidence-based practice status. PMC11506176
Meta-Analysis (Level I)
"Effect of Sensory Integration Therapy on Autism" — 24 studies. Significant improvements in sensory processing, social skills, adaptive behavior. PMC10955541
Indian RCT (Level II)
Padmanabha et al. — Home-based sensory interventions, Indian home context. Parent-administered protocols effective. DOI: 10.1007/s12098-018-2747-4
WHO Framework (Level IV)
Nurturing Care Framework (2018) — Global ECD framework including sensory processing. nurturing-care.org | PMC9978394
Clinical Consensus
SPD Foundation auditory guidelines | AOTA sensory processing practice guidelines | Porges Safe and Sound Protocol® research on auditory processing and nervous system regulation
How GPT-OS® Uses Your Data
Smart Therapy, Protected Privacy
Your session data powers smarter therapy — personalized for your child and contributing to better outcomes for every child navigating auditory sensitivity worldwide.
What GPT-OS® Learns From Your Data
- Your child's unique auditory tolerance curve
- Which protection combinations work best
- Optimal session timing and duration
- When to advance and when to hold steady
Privacy & Security
- ISO/IEC 27001 certified
- GDPR/DPDPA compliant
- Data never sold or shared with third parties
- Request data deletion at any time
"Your anonymized data joins 20M+ session records to improve recommendations for all families."

Watch the Reel
Reel A-033
Sensory Solutions Series — Episode 33
📹 Watch: 9 Materials That Help With Vacuum Cleaner Distress
Watch a Pinnacle therapist demonstrate each of the 9 materials in action — from headphone fitting to graduated exposure technique to the child-controlled vacuum experience. Video reinforces everything you've read on this page.
Domain
Sensory Processing — Auditory
Duration
75–85 seconds
Presented By
Pinnacle Blooms OT Team

Share This With Your Family
Consistency Across Caregivers Multiplies Impact
When every caregiver follows the same protocol, your child gets a consistent message: "You are safe. We are prepared. You can do this." Inconsistent implementation is the number one barrier to progress — sharing this resource is as important as following it yourself.
Family Guide (1-Page PDF)
A simplified version of this entire protocol on one printable page. Put it on the fridge.
"Explain to Grandparents" Guide
Culturally sensitive, simplified explanation for extended family. Addresses common misconceptions: "It's not stubbornness. Here's what to do and what NOT to do."
Teacher Communication Template
Letter template for school: explains auditory sensitivity, headphone accommodation, fire drill preparation, and assembly support.

Frequently Asked Questions
How long does it take for vacuum tolerance to develop?
Most families see initial improvements within 2–4 weeks of consistent daily protocol. Functional tolerance (same-room with headphones) typically emerges at weeks 5–8. Full tolerance without protection may take 3–6 months. Every child's timeline is different — progress is measured in your child's increments.
My child is terrified of the blender and hair dryer too — do I need separate protocols?
Not necessarily. These sounds share similar acoustic profiles. As vacuum tolerance builds, many families report that tolerance generalizes to blenders, hair dryers, and mixer grinders without specific intervention. If it doesn't generalize, the same protocol structure adapts to any household sound trigger.
Is it okay to use headphones all the time? Won't my child become dependent?
Headphones are a bridge tool, not a permanent solution. In early phases, use them freely — they enable tolerance building. The protocol systematically reduces protection over time. Think of headphones like training wheels: necessary at first, gradually removed as skills develop.
My family says I'm "spoiling" the child by accommodating the fear. What do I say?
Share the neuroscience (Card 4) with them. The child's auditory system is registering genuine danger — this isn't manipulation. Accommodating a neurological difference while building tolerance is evidence-based parenting. Share the Family Guide (Card 38).
Should I try therapeutic listening programs on my own?
No. Programs like Therapeutic Listening® and Safe and Sound Protocol® require trained professional guidance. Incorrectly implemented programs can worsen auditory sensitivity. Contact Pinnacle for an OT evaluation.
When should I see a professional instead of doing this at home?
Seek professional evaluation if: no improvement after 4 weeks, sensitivity worsening, multiple sensory domains affected, signs of anxiety disorder beyond sound, or uncertainty about the diagnosis (auditory over-responsivity vs. hyperacusis vs. specific phobia).
Preview of 9 materials that help with vacuum cleaner distress Therapy Material
Below is a visual preview of 9 materials that help with vacuum cleaner distress therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.








Link copied!

From Fear to Mastery
Your Next Step: Start Now
You've read. You understand. Now act. Get your headphones. Set up the safe space. Post the visual schedule. Begin tonight.
PINNACLE BLOOMS NETWORK®
Built by Mothers. Engineered as a System.
Built by Mothers. Engineered as a System.
This page is one of 70,000+ evidence-based intervention techniques in the Pinnacle GPT-OS® knowledge base — the largest structured pediatric intervention knowledge system on Earth.
20M+ exclusive 1:1 therapy sessions • 97%+ measured improvement • 70+ centers • Patents filed across 160+ countries
Medical Disclaimer: This content is educational. It does not replace assessment by a licensed occupational therapist, audiologist, or healthcare provider. Significant auditory sensitivity may require comprehensive sensory processing evaluation and professional-guided intervention. Therapeutic listening programs require trained provider supervision. Individual results may vary.
CIN: U74999TG2016PTC113063 | DPIIT: DIPP8651 | MSME: TS20F0009606 | GSTIN: 36AAGCB9722P1Z2
© 2025 Pinnacle Blooms Network®, unit of Bharath Healthcare Laboratories Pvt. Ltd. All rights reserved.
© 2025 Pinnacle Blooms Network®, unit of Bharath Healthcare Laboratories Pvt. Ltd. All rights reserved.