
"He crashes into everything. But he won't let me touch him."
Morning. Seven-year-old Arjun explodes out of bed, charges down the corridor, slams into the sofa. You reach to straighten his shirt — he flinches like you've burned him. At breakfast, he refuses every food that isn't beige. The school bag goes on for the fifth time because the straps feel "wrong." By 8 AM, you're both exhausted and the day hasn't started.
This isn't defiance. This isn't a parenting failure. This is a nervous system asking — loudly — for the right kind of input.
🏥 Pediatric Occupational Therapy
🧠 Sensory Processing
👶 Age 2–12
🏠 Home-Executable
"You are not failing. Your child's nervous system is speaking. And today, you learn its language." — Pinnacle Blooms Consortium®

ACT I — Recognition
The Numbers That End Your Isolation
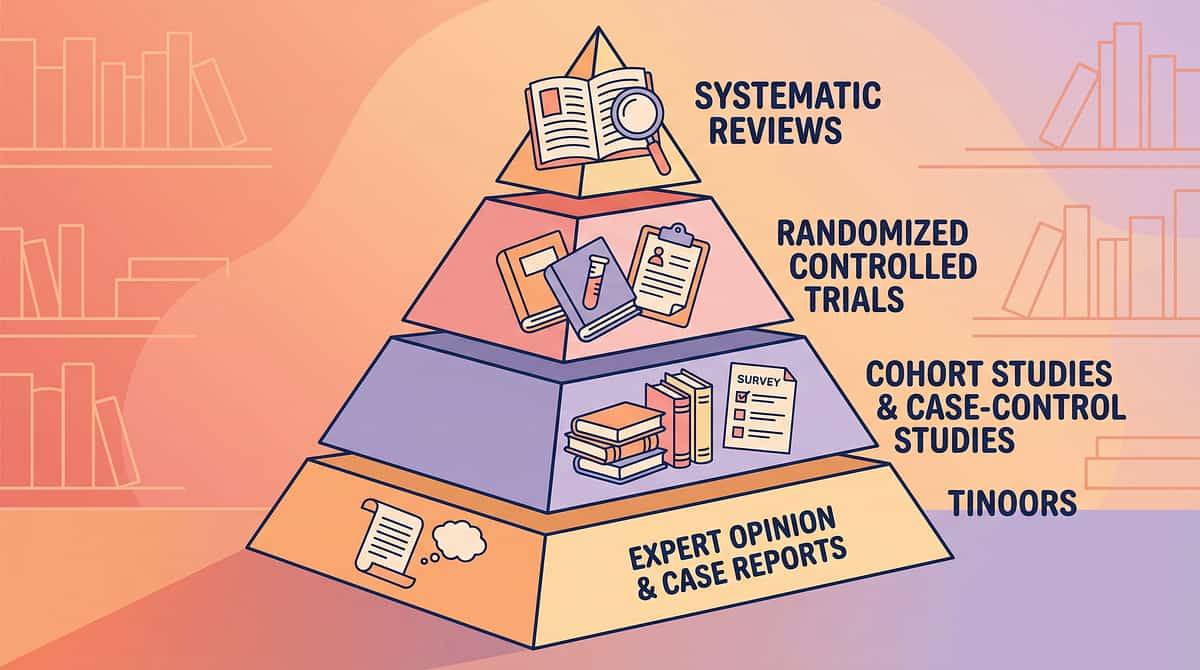
You are among millions of families navigating this exact challenge. A 2024 PRISMA systematic review of 16 studies confirmed that sensory integration challenges are not rare, not isolated, and not the parent's creation. They are among the most universal neurological features of autism spectrum conditions — documented consistently across 70+ countries.
1
Experience Sensory Challenges
of children with ASD experience significant sensory processing difficulties
2
Children in India
diagnosed with autism — sensory integration challenges affect the majority
3
Therapy Sessions
delivered by Pinnacle's GPT-OS® tracking sensory outcomes
In India alone, the Padmanabha et al. (2019) RCT in the Indian Journal of Pediatrics demonstrated that home-based sensory interventions produce significant, measurable outcomes when implemented with the right materials and guidance.
"You are among millions of families navigating this exact challenge. The difference between struggle and mastery is often just the right information — delivered in time." — Pinnacle Blooms Consortium®
📞National Autism Helpline: 9100 181 181 — Free · 16 languages · 24x7
PRISMA Systematic Review (2024) · PMC11506176 | Meta-analysis World J Clin Cases 2024 · PMC10955541 | Padmanabha et al., Indian J Pediatr 2019 · DOI:10.1007/s12098-018-2747-4
PRISMA Systematic Review (2024) · PMC11506176 | Meta-analysis World J Clin Cases 2024 · PMC10955541 | Padmanabha et al., Indian J Pediatr 2019 · DOI:10.1007/s12098-018-2747-4

The Neuroscience in Plain English
Understanding what's happening in your child's brain transforms frustration into compassion — and confusion into action.
🧠 The Nervous System Hierarchy
The vestibular system (inner ear) sits at the base of the brain's sensory hierarchy. It governs movement, balance, and postural control — and modulates every other sense.
The proprioceptive system (muscles, joints, tendons) tells the brain WHERE the body is in space and HOW MUCH force to use. It's the body's GPS.
The tactile system (skin) processes touch, pressure, temperature, texture.
When these three systems don't communicate efficiently, the result is sensory integration dysfunction. The somatosensory cortex over-amplifies ordinary light touch. The vestibular nucleus under-responds to movement. The proprioceptive system miscalibrates force.
What Does This Mean for Your Child?
When Arjun crashes into the sofa, he's not being destructive. His vestibular system is starved for input — so he seeks it with full-body impact. When he flinches from your touch, his tactile system is sending CODE RED signals for input that most people experience as neutral.
This is a wiring difference. Not a character defect.
The extraordinary news is that the brain is neuroplastic. Controlled, patterned sensory input — delivered consistently through the right materials — builds new neural pathways. The vestibular, proprioceptive, and tactile systems become better at talking to each other.
A. Jean Ayres, PhD called this Sensory Integration Therapy — and the 2024 systematic review across 16 studies confirms it meets the gold standard of evidence-based practice for children with ASD.
Frontiers in Integrative Neuroscience (2020) · DOI:10.3389/fnint.2020.556660 | PMC11506176
Developmental Context
Your Child's Place on the Developmental Map
Sensory integration develops most rapidly in the first 7 years of life — the window during which the brain builds the neural highways that allow multiple sensory streams to be processed simultaneously.
For children with autism, ADHD, prematurity, or developmental differences, this integration develops atypically — not incorrectly, but differently. And with the right input, the brain continues to adapt throughout childhood. What commonly co-occurs with sensory integration challenges: attention and focus difficulties, emotional regulation challenges, motor planning difficulties (Dyspraxia), language processing differences, and sleep difficulties.
The WHO/UNICEF Care for Child Development (CCD) Package, implemented across 54 low- and middle-income countries including India, identifies the 0–8 year window as the period of maximum neurological leverage for intervention. WHO Care for Child Development Package (2023) | PMC9978394
⚜ Level I Evidence
This Isn't Alternative Therapy. This Is Science.
📄 2024 PRISMA Systematic Review
16 studies (2013–2023) | Journal: Children | PMC11506176
"Sensory integration intervention meets criteria to be considered evidence-based practice for children with ASD."
Improved: social skills, adaptive behavior, sensory processing, gross/fine motor
📄 2024 Meta-Analysis
24 studies | World J Clin Cases | PMC10955541
"Sensory integration therapy effectively promoted social skills, adaptive behavior, sensory processing, and motor skills."
Effect sizes significant across multiple domains
📄 India-Specific RCT (2019)
Padmanabha et al. | Indian Journal of Pediatrics | DOI:10.1007/s12098-018-2747-4
"Home-based sensory interventions demonstrated significant outcomes when parent-implemented with structured guidance."
Validated for Indian context, home setting, parent delivery
"Clinically validated. Home-applicable. Parent-proven."
NCAEP Evidence-Based Practices Report (2020) | Ayres SI Theory | WHO NCF 2018

ACT II — Knowledge Transfer
The Technique: What It Is
🧩 Formal Definition
Formal: Sensory Integration Therapy — Multi-Material Home Sensory Diet Protocol
Parent-Friendly Alias:"The Sensory Toolbox"
Sensory Integration (SI) therapy is a neuroscience-grounded intervention that uses controlled, purposeful sensory experiences — particularly vestibular (movement/balance), proprioceptive (body position/pressure), and tactile (touch/texture) input — to help the brain develop more efficient pathways for processing and organizing sensory information.
A home sensory diet is the structured, scheduled use of specific sensory materials throughout the day to maintain optimal nervous system regulation. Think of it as nutrition — not for the body, but for the sensory system. Without the right input, the nervous system either starves (seeking) or chokes (avoiding). With the right materials, delivered proactively, the nervous system finds its "just right" zone.
Specs & Domains
👶Age: 2–12 years
⏱Duration: 10–20 min/session
📅Frequency: 3–5x daily (sensory diet integration)
🏠Setting: Home + School + Community
Domain Badges:
🟣 Sensory Processing | 🔵 Pediatric OT | 🟢 Vestibular-Proprioceptive | 🟡 Tactile Discrimination | 🟤 Sensory Modulation
🟣 Sensory Processing | 🔵 Pediatric OT | 🟢 Vestibular-Proprioceptive | 🟡 Tactile Discrimination | 🟤 Sensory Modulation
The goal is not to eliminate your child's sensory differences. The goal is to give their nervous system the input it needs to function optimally — and to teach them, over time, to recognize and meet their own sensory needs.

The Consortium Behind Every Sensory Protocol
Sensory integration therapy crosses therapy boundaries because the brain doesn't organize by therapy type. Sensation, behavior, communication, and learning are one system — and they require one coordinated team.
🔵 Occupational Therapist — PRIMARY LEAD
Designs the sensory diet, selects materials, calibrates intensity, monitors arousal levels. SI assessment and certification guides the full protocol.
🟣 Speech-Language Pathologist — ORAL SENSORY + FEEDING
Addresses oral motor seeking (chewing, mouthing), feeding texture sensitivities, and the impact of auditory processing on communication.
🟢 ABA/BCBA — BEHAVIORAL REGULATION
Structures reinforcement schedules during sensory activities, uses data to track tolerance and approach behavior, manages avoidance.
🟡 Special Educator — CLASSROOM TRANSLATION
Integrates sensory accommodations into learning environments — wobble cushions, fidget tools, noise-reducing headphones, sensory breaks.
🔴 Neurodevelopmental Paediatrician — MEDICAL OVERSIGHT
Rules out underlying medical causes, coordinates sensory processing evaluation, integrates sensory findings with overall developmental profile and medications.
Precision Targets. Not a Random Activity.
Sensory integration therapy targets specific neurological outcomes — organized from innermost (primary) to broader functional gains. Every material, every session, every repetition serves one or more of these targets.
Meta-analysis (PMC10955541): Sensory integration therapy promoted social skills (primary), adaptive behavior (secondary), sensory processing and motor skills (tertiary) across 24 studies · 2024

Your Sensory Toolbox
9 Clinically-Validated Sensory Integration Materials
Every material below is mapped to the Pinnacle 128 Canon Materials System. Each has a DIY alternative (Card 10). These tools work because they provide targeted input to the vestibular, proprioceptive, and tactile systems — the three foundational pillars of sensory integration.
📦Essential Home Sensory Kit (Budget Start): ₹3,400–5,800
Weighted lap pad + Resistance bands + Chew necklace + Sensory bin + Ear defenders + Balance cushion
Begin here. Add swing and crash pad when budget allows.
Weighted lap pad + Resistance bands + Chew necklace + Sensory bin + Ear defenders + Balance cushion
Begin here. Add swing and crash pad when budget allows.

Material 1 of 9
Vestibular Equipment
Therapy Swing
Why It Works
Vestibular input from swinging is the most powerful organizer of the entire nervous system — affecting arousal, attention, postural control, and emotional regulation. Linear swinging (back-forth) is calming and organizing; rotary movement (spinning) is intensely alerting.
Types
- Platform swing (prone, core engagement)
- Bolster swing (bilateral coordination)
- Cocoon/Pod swing (calming, enclosed)
Getting Started
Price range: ₹2,000–15,000
⭐Pinnacle Recommends: Ceiling-mount platform swing with safety mat
Ceiling mount must be professionally installed. Limit spinning. Watch for pallor/nausea — stop immediately.
Material 2 of 9
Proprioceptive Tools / Deep Pressure
Weighted Blanket / Lap Pad
Why It Works
Deep pressure activates the parasympathetic nervous system, reducing fight-or-flight and promoting calm alertness. The weight should be approximately 10% of body weight + 1 lb — this is the clinically established therapeutic dose.
Types
- Weighted blanket (sleep + calm)
- Weighted lap pad (seated attention, school-portable)
Getting Started
Price range: ₹1,500–6,000
⭐Pinnacle Recommends: Washable cover, breathable fabric for Indian climate
Never use weight greater than 10% body weight + 1–2 lbs. Never used on infants or children who cannot self-remove.
Material 3 of 9
Proprioceptive Tools / Body Awareness
Body Sock / Compression Clothing
Why It Works
Continuous proprioceptive input across the whole body. Stretchy resistance increases body-in-space awareness while delivering calming compression. For seekers: constant input. For avoiders: sense of containment and safety.
Types
- Body sock (therapeutic play)
- Compression shirt/shorts (daily wear, discreet)
Getting Started
Price range: ₹800–4,000
Child must be able to exit independently. Ensure adequate ventilation during use.
Material 4 of 9
Tactile Materials
Tactile Exploration Materials
Why It Works
Graded tactile exposure — from preferred to challenging textures — reduces defensiveness and builds discrimination over time. The brain learns: touch is safe. Each session expands the window of tolerance incrementally.
Types
- Sensory bin + fillers
- Textured balls
- Therapy putty
- Kinetic sand
- Fabric swatches
Getting Started
Price range: ₹500–2,500
Graded progression: dry rice → kinetic sand → putty → wet textures. Advance over weeks, not one session.

Material 5 of 9
Vestibular + Proprioceptive Equipment
Crash Pad / Foam Mat
Why It Works
Provides a safe outlet for the intense proprioceptive and vestibular input sensory-seeking children crave. Jumping, crashing, and landing delivers deep pressure through joints plus vestibular activation simultaneously. Proactive crash time prevents unsafe seeking behaviors on furniture.
Getting Started
Price range: ₹3,000–12,000
Minimum 6 inches foam depth. Clear surrounding area before use. Establish rules before every session: feet first, no headfirst diving.

Material 6 of 9
Proprioceptive Tools / Heavy Work
Resistance Bands + Heavy Work Equipment
Why It Works
Proprioceptive "heavy work" — pushing, pulling, lifting against resistance — activates proprioceptors in muscles and joints. This is the most universally regulating sensory input. Calms the hyper, alerts the sluggish. It's the great nervous system equalizer.
Types
- Resistance bands
- Medicine ball
- Weighted cart
- Therapy tunnel
Getting Started
Price range: ₹500–4,000
This is the most portable, life-integrated form of proprioceptive input — usable anywhere, anytime.
Material 7 of 9
Oral Motor Tools
Oral Motor / Chewing Tools
Why It Works
The mouth has the highest proprioceptive nerve density in the body — making chewing one of the most efficient regulatory inputs available. Chewing is self-regulation, not misbehavior. Understanding this reframes everything.
Types
- Chew necklace/bracelet (various resistances)
- Pencil topper
- Varied texture tools
Getting Started
Price range: ₹300–1,500
Food-grade materials only. Inspect before each use — discard immediately if compromised. No improvised substitutes for chewing tools.

Material 8 of 9
Vestibular Equipment / Balance Training
Balance Equipment
Why It Works
Balance activities require real-time integration of vestibular + proprioceptive information — building the exact neural connections sensory integration therapy targets. Wobble cushions on chairs significantly improve seated attention in school and home settings.
Types
- Balance board
- Wobble cushion (chair-based)
- Balance beam
- Stepping stones
Getting Started
Price range: ₹800–4,000
A wobble cushion on a school chair provides continuous low-level vestibular-proprioceptive input throughout the entire school day.

Material 9 of 9
Auditory Protection / Sensory Accommodation
Noise-Reducing Headphones
Why It Works
For auditory-hypersensitive children, ordinary environments are physiologically painful. Headphones turn overwhelming into tolerable — enabling participation in environments that would otherwise trigger meltdowns. Availability alone (knowing they're accessible) reduces anticipatory anxiety.
Types
- Passive ear defenders
- Child-sized noise-canceling
- Earplugs (older children)
Getting Started
Price range: ₹500–3,000
The sense of control — letting the child choose when to put them on — is itself regulatory. Never force. Always offer.
Every Family Can Start Today
WHO/UNICEF Equity Principle: Household-material efficacy is validated across 54 low-and-middle-income countries. The therapeutic principle is the same whether materials cost ₹8,000 or ₹0. The brain doesn't know. It responds to the input.
Clinical Material | DIY / Household Substitute | Why It Works | |
Therapy Swing | Blanket swing (two adults swing child in bedsheet). Playground swing. Hammock hung low. | Same vestibular input — linear swinging activates the same neural pathways | |
Weighted Blanket | Pillowcase filled with dried rice/lentils. Stack 3 regular blankets. "Burrito wrap" in firm blanket. | Deep pressure proprioceptive activation — weight and distribution are what matter | |
Body Sock | Tight-fitting clothing (one size smaller). Sleeping bag. Lycra tunnel stitched from stretchy fabric. | Continuous compression effect — fabric tension does the proprioceptive work | |
Tactile Materials | Sponges, dry rice bin, sand tray, fabric swatches, playdough (flour+salt+water). Nature textures. | Graded tactile exposure works equally well with natural and household materials | |
Crash Pad | Pile of sofa cushions. Old mattress on floor. Large beanbag. Foam blocks from craft store. | Impact absorption + proprioceptive deep pressure — the landing is the therapy | |
Resistance Equipment | Filled backpack. Laundry basket to push. Grocery bags. Wheelbarrow walks. Wall push-ups. | Heavy work activates proprioceptors identically whether tool costs ₹2,000 or ₹0 | |
Chewing Tools | Carrots, celery, dried fruit leather, beef jerky. Silicone straw to chew. | Proprioceptive density in the jaw responds to resistance — food works | |
Balance Equipment | Pillow on floor to stand on. Couch cushion challenge. Curb walking (supervised). Partially deflated ball to sit on. | Proprioceptive + vestibular integration challenge is identical to clinical equipment | |
Noise-Reducing Headphones | Child-safe earplugs. Over-ear music headphones (passive reduction). Quiet retreat corner. | Input reduction is the goal — even partial reduction is therapeutic |
⚠When clinical-grade material is essential: Therapy swings require professionally installed ceiling mounts. DIY weight for blankets must be accurately calculated (10% body weight + 1 lb, maximum). Chewing tools must be food-grade only — no improvised substitutes for chewing.

Safety First
🛑 Read Before Every Session
🔴 STOP — Absolute Contraindications
- Child has had a seizure within the last 24 hours
- Child shows signs of illness, ear infection, or fever
- Recent injury to spine, joints, or head
- Child is severely dysregulated (active meltdown, self-injury)
- Undiagnosed vestibular or balance disorder — consult doctor before swing use
🟡 MODIFY — Proceed with Caution
- Child is overtired or has had fewer than 6 hours of sleep
- Signs of early dysregulation (rocking, increased stimming)
- First session with rotary movement — start with linear only
- Tactile hypersensitivity — begin with deep pressure only
- Child wearing tight or uncomfortable clothing — address this first
🟢 PROCEED — Ideal Session Conditions
- Child is fed, hydrated, and has had a brief rest
- Space is clear, lighting is dim/warm, background noise minimized
- Materials are at room temperature (cold textures startle)
- Preferred calming activity ready for cool-down
- Parent is calm — regulated adult = regulated child
Your Home Sensory Space: 4-Zone Setup
Environmental setup is a core principle of Ayres Sensory Integration Theory. A well-designed space reduces setup time, signals to the child that sensory input is available, and creates the calm conditions under which regulation is most achievable.
✅ Remove from Space
- Background TV/radio
- Cluttered surfaces
- Loose small objects
- Bright overhead lighting
✅ Add to Space
- Warm lamp lighting (2700K)
- White noise machine or nature sounds (optional)
- Visual timer visible to child
- Child's preferred calming object nearby
- Temperature: 22–26°C optimal
Set out all materials before bringing child into the space — no rustling or preparation noise during the session. Your nervous system co-regulates your child's: arrive calm.
ACT III — Execution
The 60-Second Pre-Flight Check
Before every session, run this quick readiness check. The best session is one that starts right — and a session that doesn't start is not failure, it's data.
Indicator | 🟢 Green — Proceed | 🟡 Amber — Modify | 🔴 Red — Postpone | |
Hunger/Hydration | Fed within last 2 hours | Mildly hungry — offer snack first | Hungry or thirsty — feed first | |
Sleep State | Rested, some energy | Slightly tired — shorten session | Overtired — postpone | |
Arousal Level | Calm-alert or slightly dysregulated | Moderately activated | Severe dysregulation / meltdown | |
Physical State | Well, no illness signs | Minor fatigue | Fever, ear pain, any illness | |
Recent Events | Neutral morning/afternoon | Mildly challenging day | Major meltdown within 2 hours | |
Child Signal | Approaches materials with interest | Neutral/passive | Active avoidance / distress | |
Parent State | Calm, present, unhurried | Slightly stressed — take 3 breaths | Highly stressed — reschedule |
Step 1
The Invitation
⏱30–60 seconds | 🎯Goal: Child voluntarily approaches
💬 Say This
"Hey [name]... want to see what's in our sensory corner today?"
Low, calm tone. No urgency. Offer, don't instruct.
Parent Body Language
- Be at child's eye level or below — never looming
- Relaxed shoulders, open palms (not reaching)
- Slow movements — no sudden gestures
- Allow 10–15 seconds of silence after the offer
✅ What Acceptance Looks Like
- Child moves toward the space
- Child makes eye contact with materials
- Child touches an item
- Child vocalizes interest
❌ What Resistance Looks Like — and What to Do
Child ignores → Wait 30 seconds, try once more, offer a favourite object near the sensory area.
Child retreats → Don't pursue. Say: "That's okay. The swing will be here when you're ready."
Child protests → Honour it. Reschedule with the modify protocol.

Step 2
The Engagement
⏱1–3 minutes | 🎯Goal: Active sensory contact established
💬 "This is the [swing/blanket/sensory bin]. Watch — I'll try it first."
Model before asking. Always. Especially for tactile-defensive children.
1
For Vestibular (Swing, Balance Board)
Begin with the child sitting passively in the swing — no movement yet. Let them feel the position. Then introduce the SMALLEST amount of linear movement. Wait for acceptance before increasing amplitude.
2
For Proprioceptive (Weighted Blanket, Body Sock, Heavy Work)
Place the material near the child first. Let them approach it. For weighted blanket — place on knees first, then lap, then full body when tolerated. Never force contact.
3
For Tactile (Sensory Bin, Tactile Materials)
Start with the child watching your hands in the material. Offer the material — don't guide their hands into it. Let them touch on their terms, at their pace.

Step 3
The Therapeutic Action
⏱5–15 minutes | 🎯Goal: Sustained, purposeful sensory input — the active ingredient
Therapy Swing
Rhythmic linear swinging (back-forth) for 5–10 minutes. Watch for eyes softening, body relaxing, reduced stimming — signals the nervous system is organizing. For prone (belly-down) on platform: activates core, neck extensors, and vestibular simultaneously. ⚠ Rotary spinning: maximum 10 rotations, then linear to neutralize.
Weighted Blanket
Once placed, allow 10–20 minutes uninterrupted. Do not talk excessively — the weight is doing the work. Pair with a calm activity. Parasympathetic activation takes 8–12 minutes to fully engage.
Body Sock
Once inside, encourage active movement against the resistance — push the walls, stretch, walk. The resistance creates the proprioceptive input. 5–10 minutes of active play = significant regulatory input.
Tactile Materials
Offer the bin and model play. Bury objects for child to find. Provide no pressure — let the child's hands guide depth of contact. Graded: dry rice → kinetic sand → putty → wet textures (over weeks, not one session).
Crash Pad
Establish rules before: "We jump and land — feet first." Allow the child to jump repeatedly. Landing = deep pressure through every joint. 10–15 jumps is often sufficient for significant regulation. Watch for: decreased seeking behavior, calmer affect.
Resistance Equipment
5–10 minutes of sustained heavy work: pulling resistance band, pushing weighted cart, carrying heavy backpack, wheelbarrow walks. Most portable, life-integrated form of proprioceptive input available.
Chewing Tools
Offer during a cognitively demanding activity (homework, listening). Oral proprioceptive input frees cognitive resources for the task. No need to prompt or direct — let them chew as needed.
Balance Equipment
Stand on wobble board for 3–5 minutes of active balance challenges. Transition to wobble cushion on chair for seated tasks — continuous low-level vestibular-proprioceptive input throughout the session.
Noise-Reducing Headphones
Place in child's hands — let them choose when to put on. Never force. In overwhelming environments, proactively offer. The sense of control is itself regulatory. Allow use for as long as needed.
Concerning response — STOP: Increasing dysregulation, pallor, nausea, self-injury. | PMC10955541: Core therapeutic action = 40–60% of session time.
Step 4
Repeat & Vary
⏱3–5 minutes | 🎯Goal: Dosage without satiation
3 quality repetitions > 10 forced repetitions
Repetition Guidance by Material
- Swing: 5–10 minutes continuous OR 3 bouts of 2–3 minutes with brief pauses
- Crash Pad: 10–15 landings, then pause
- Resistance: 3–5 sets of 1–2 minutes heavy work
- Tactile bin: 5–10 minutes exploration; end when engagement drops
- Weighted blanket: Continuous 15–20 minutes (one session)
Variation Options — Keep the Brain Adapting
- Swing: change angle (front-back → diagonal → side-to-side)
- Tactile: change bin filler (rice → beans → sand → water beads over days/weeks)
- Resistance: change direction, add carrying, try pulling vs. pushing
- Balance: add visual tracking task (catch bean bag while balancing)
Step 5
Reinforce & Celebrate
⏱30 seconds | 🎯Goal: Reinforce engagement — not performance
"Celebrate the ATTEMPT — not just the success."
💬 "You tried that! I'm so proud of you for exploring."
💬 "Look at you on that swing! You're brave."
💬 "You stayed for three whole jumps. That's real work."
Timing is critical: Reinforce within 3 seconds of the desired behavior. Delayed reinforcement loses its signal value.
Type | Example | Best For | |
Verbal Praise | "Brilliant! Look at what you did!" | All children, all the time | |
Social | High five, clap, thumbs up | Children with social motivation | |
Token/Star | Star on chart, sticker in book | Children responding to visual systems | |
Natural Consequence | "Now you're calm and ready for your show" | Older children, intrinsic motivation building |

Step 6
The Cool-Down
⏱2–3 minutes | 🎯Goal: Regulated transition — no abrupt endings
Every session ends with a cool-down. Abrupt endings cause post-session dysregulation — the child's nervous system spikes because the organizing input stopped without warning.
1
Verbal Warning
💬 "Two more swings, then we're all done." — child sees and hears the end coming with a visual timer.
2
Reduce Intensity
Slow the swing, decrease movement amplitude, lower resistance. Gradual deceleration, not a stop.
3
Transition to Calming Input
Deep pressure hug or squeeze, weighted blanket, calm sitting. Let the nervous system land gently.
4
Material Put-Away Ritual
Child participates in putting materials away — this itself is proprioceptive heavy work and a natural closing ritual.
5
Bridge to Next Activity
💬 "Now we're going to have [preferred activity]." Predictable endings = less resistance over time.
NCAEP (2020): Visual supports (timers, schedules) are evidence-based practice for autism.
Capture the Data: Right Now
60 seconds of data now saves hours of guessing later. Your child's response IS the prescription. Consistent tracking across weeks reveals patterns no single session can show — which materials work best, what time of day produces peak regulation, and how the nervous system is adapting.
Quick Session Log — L-984 Sensory Integration
📅 Date: ___________
🕐 Session Time: ___________
🎯 Material Used Today:
[ ] Swing [ ] Weighted [ ] Body Sock [ ] Tactile
[ ] Crash Pad [ ] Resistance [ ] Chewing [ ] Balance [ ] Headphones
[ ] Swing [ ] Weighted [ ] Body Sock [ ] Tactile
[ ] Crash Pad [ ] Resistance [ ] Chewing [ ] Balance [ ] Headphones
⏱ Total Time (minutes): _______
📊 Child Engagement Rating (circle): 1 — 2 — 3 — 4 — 5
🧠 Arousal Level BEFORE: Dysregulated / Activated / Calm-Alert / Low
🧠 Arousal Level AFTER: Dysregulated / Activated / Calm-Alert / Low
📝 One observation: _______________________
What These Numbers Mean
Metric | What It Captures | |
Engagement Rating | 1 = refused/distressed → 5 = fully engaged, sought more | |
Arousal Shift | Did the session regulate UP (from low) or DOWN (from high)? | |
One Observation | Any new behavior, tolerance gain, or challenge |

Troubleshooting
Reality Check: Most Sessions Don't Go Perfectly
"Session abandonment is not failure — it's data. The technique needs adjustment, not the parent."
Child refused to enter the sensory space
Why: Sensory avoidance is a protective response. The nervous system said "not safe yet."
Fix: Reduce to zero-demand. Bring ONE material into their current space. Let them watch you use it. Try again in 24 hours with that single material.
Child became MORE dysregulated during swing
Why: Rotary or irregular movement overshoots the system — especially for vestibular-sensitive children.
Fix: Switch to ONLY linear movement (straight back-forth). Reduce amplitude. If still dysregulating, stop swing — switch to deep pressure (weighted blanket) to organize.
Child screamed when blanket was placed
Why: Tactile defensiveness — the weight felt threatening before the calming effect could register.
Fix: Start with the blanket next to them (not on). Progress to on knees → lap → full body over DAYS, not minutes.
Child bit/damaged the chew tool immediately
Why: Oral seeking was at high intensity — the tool wasn't resistant enough.
Fix: Move to higher-resistance chew tool. Offer crunchy food before tool (pre-loading proprioceptive input).
Child tolerated the material for 10 seconds then fled
Why: Normal early-phase response. The nervous system is testing safety.
Fix: 10 seconds IS progress if it was 0 seconds yesterday. Log it. Celebrate it. Repeat.
Child became aggressive during crash pad session
Why: Intensity of seeking escalated — the pad became a stimulus for unsafe behavior.
Fix: Establish clear rules before EVERY session (feet-first landing, one jumper at a time). Use a visual rule card. If it continues, move crash pad work to clinic.
Nothing seems to be working after 3 weeks
Why: Wrong material match, wrong dosage, wrong timing — OR the child's sensory profile needs professional re-assessment.
Fix: Book a sensory integration assessment with a certified OT. 📞9100 181 181
No Two Children Are the Same. Your Version of This Protocol Is Unique.
Every child's sensory profile is distinct. Use these modifications as a guide — your child's responses are your real-time feedback. Adjust based on what you observe, session by session.
Dimension | Easier Version | Standard | Harder / Advanced | |
Swing movement | Stationary position in swing | Gentle linear, 5 min | Linear + varied angles + prone, 10–15 min | |
Weight (blanket) | Blanket beside the child | Lap pad only | Full weighted blanket, 20 min | |
Tactile exposure | Watching hands in bin | Fingertips touching surface | Full hand buried, novel textures | |
Crash pad | Step down from low height | Jump from floor | Jump from small step, add landing targets | |
Heavy work | Empty backpack carry | Half-filled backpack | Full backpack + grocery bag carry | |
Session duration | 5 minutes | 10–15 minutes | 20 minutes |
ACT IV — The Progress Arc
Week 1–2: What Real Progress Actually Looks Like
Week 1–2 is the hardest week. The child's nervous system is adjusting. There may be an initial increase in seeking behavior as the system becomes aware of what it needs. This is normal. Stay consistent.
❌ What Progress Is NOT in Week 1–2
- Child no longer sensory-seeking
- Meltdowns eliminated
- Child "loves" all materials
- Tolerance across multiple environments
✅ What Progress IS in Week 1–2
- Child tolerates weighted blanket for 3 more seconds than Day 1
- Child approaches sensory bin without being asked (even briefly)
- Crash pad sessions have reduced dangerous furniture-jumping
- Child shows less resistance to putting on headphones when offered
- Parent feels more confident about what the child needs
1
Reduced physical agitation 10–15 minutes post-session
2
Any decrease in clothing/texture meltdown frequency
3
Child begins to seek a specific material spontaneously
4
Sleep onset slightly easier on days sensory diet is implemented
PMC11506176: SI intervention outcomes emerge across 8–12 week timelines. Early-phase: tolerance and participation, not mastery.
Week 3–4: The Nervous System Is Beginning to Trust
The child anticipates the sensory routine — begins moving toward the sensory corner without being invited. This is the first sign of neural pathway formation: the brain is seeking what it has learned is regulatory.
1
Anticipatory Approach
Child heads toward swing/crash pad/weighted blanket spontaneously before the session starts.
2
Extended Tolerance
Sessions that started at 2 minutes now sustain for 8–10 minutes without resistance.
3
Reduced Transition Resistance
Getting dressed, entering loud environments, or touching previously aversive textures shows measurable decrease in resistance.
4
Emerging Self-Advocacy
"I need my headphones" or "I want to jump" — the child beginning to identify and communicate their own sensory needs.
5
Sleep Improvement
For children using weighted blankets nightly, sleep onset time often decreases by Week 3–4.
6
Parent Confidence
You read your child's sensory state more accurately. You know what they need before they escalate.
⭐ Sensory Integration Milestone
Week 5–8: Mastery Indicators
Your child has reached the Week 5–8 mastery zone when you observe 3 or more of the following. These are observable, measurable markers — not impressions, but evidence.
✅ Generalization
Sensory regulation strategies appearing in untrained environments (school, restaurants, public spaces)
✅ Self-Initiation
Child independently accesses sensory materials when dysregulated — without parent prompt
✅ Reduced Frequency
Sensory-triggered meltdowns measurably less frequent than Week 1 baseline
✅ Tolerance Expansion
Previously avoided textures, sounds, and movements now tolerated for longer periods
✅ Communication
Child uses words or signals to indicate sensory state ("too loud," "I need to jump")
✅ Participation
Engaging in environments that were previously inaccessible (school cafeteria, family gatherings)
Next Step: Move to L-985: Body Awareness and Motor Planning (next technique in sequence), or deepen current techniques by increasing complexity and adding new sensory systems. PMC10955541: SI therapy across 24 studies showed measurable skill promotion.
You Did This.
Five to eight weeks ago, you were reading Card 01. Your child's nervous system was overwhelming both of you — too loud, too scratchy, not enough, too much.
You learned the science. You built the space. You showed up — session after session — on the days it worked and the days it didn't. You adapted. You tracked. You celebrated the 3-second tolerance gains that no one else could see.
And something changed.
Not overnight. Not dramatically at first. But steadily, session by session, your child's nervous system built new pathways. The brain that was overwhelmed or underserved began to find its just-right zone.
"You are not your child's problem. You are your child's solution." — Pinnacle Blooms Consortium®
Your Developmental GPS: Where You Are. Where You're Going.
Sensory integration therapy doesn't exist in isolation — it's one piece of a connected developmental architecture. Understanding where L-984 fits helps you plan what comes next.
If Your Child Responded to Proprioceptive Tools
Heavy work, crash pad, weighted blanket → L-985 Body Awareness is the natural next step. The proprioceptive system is organized — now build the praxis (motor planning) layer.
If One System Remained Dominant
Targeted deeper work: L-980 (Sensory Seeking) or L-981 (Sensory Avoiding) for that specific system. L-982 (Tactile) and L-983 (Auditory) remain relevant parallel tracks.
Sensory Processing Domain
More Tools in the Sensory Processing Domain
The materials you've assembled for L-984 give you immediate entry into these adjacent techniques. You already own many of the materials — the expertise is what deepens.
1
L-980 — Sensory Seeking Behaviors
Crash Pad + Swing | Intro → Core
✅ You own materials for this
✅ You own materials for this
2
L-981 — Sensory Avoiding Patterns
Weighted + Compression | Intro → Core
✅ You own materials for this
✅ You own materials for this
L-982 — Tactile Processing
Tactile Materials | Core
✅ You own materials for this
✅ You own materials for this
L-983 — Auditory Processing
Noise-Reducing Headphones | Core
✅ You own materials for this
✅ You own materials for this
L-985 — Body Awareness + Motor Planning
Balance + Resistance | Advanced
✅ You own materials for this
✅ You own materials for this
L-920 — Emotional Regulation
Multiple materials | Core
↗ Some materials shared
↗ Some materials shared
→ Browse all Sensory Processing techniques at techniques.pinnacleblooms.org/sensory-processing | Domain L: Sensory Processing | 20 Categories framework | 128 Canon Materials
ACT V — Community & Ecosystem
From the Families of the Pinnacle Network
"Our son was jumping off every piece of furniture in the house — the sofa, the beds, the dining table. He bit his shirt constantly. The noise at school made him cover his ears and cry. Getting dressed took 45 minutes every morning because every texture was wrong. We were exhausted. He was overwhelmed."
— Family 1 | Hyderabad | Child: 5 years, ASD + Sensory Seeking
After (Week 10): "We built a sensory corner. Swing from the ceiling. Crash pad in the corner. Weighted blanket at bedtime. Chew necklace for school. He knows what he needs now. The furniture-jumping has almost stopped because the crash pad gives him what he was looking for. Sleep — oh, the sleep. The weighted blanket changed everything."
"His OT said: 'He hasn't changed. He's just learned to meet his own needs.' That sentence undid three years of guilt."
"Lunch at school was impossible. The cafeteria noise caused meltdowns. Tags in clothing caused meltdowns. Sand at the beach — forget it. She refused every art activity. Every birthday party was a sensory disaster."
— Family 2 | Mumbai | Child: 7 years, Tactile Defensiveness + Sound Sensitivity
After (Week 8): "Noise-reducing headphones changed school immediately. She goes into the cafeteria now — with headphones when she needs them, without when she doesn't. The tactile bin at home has taken 8 weeks, but she now voluntarily puts her hands in kinetic sand. That was unthinkable in September."
Isolation Is the Enemy of Adherence
Every parent implementing a sensory diet at home eventually hits the same moment: "Am I doing this right? Is anyone else going through this?"
You are not alone. There are thousands of families in the Pinnacle network navigating sensory integration challenges right now — families who understand the 45-minute sock negotiation, who have built crash pads in their living rooms, who have cried over a weighted blanket that finally worked.
📱 Sensory Processing Parent WhatsApp Group
Families implementing L-984 + sensory diet protocols. Share wins, troubleshoot challenges. Live support from parents who've been exactly where you are.
💻 Online Community
pinnacleblooms.org/community — Forums moderated by Pinnacle therapists. Searchable archive of parent questions and therapist answers.
🤝 Peer Mentoring
Connect with an experienced parent who has completed the sensory integration protocol. Book through any Pinnacle center.
📍 Local Pinnacle Parent Meetups
Monthly in-person sessions at Pinnacle centers across India. Real faces, real stories, real support.
"Your child's sensory journey helps every family who comes after you. Consider sharing your story — anonymously — with the Pinnacle community."
Preview of 9 materials that help with sensory integration Therapy Material
Below is a visual preview of 9 materials that help with sensory integration therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.





Link copied!
Pinnacle Blooms Network®
"From fear to mastery. One technique at a time."
India's largest multi-disciplinary pediatric therapy consortium:
Occupational Therapists • Speech-Language Pathologists • ABA/BCBA Behaviour Analysts • Special Educators • Neurodevelopmental Paediatricians • Clinical Research Organisation • WHO/UNICEF-Aligned ECD Specialists • Parent Champions • 70+ Center Network Across India
Occupational Therapists • Speech-Language Pathologists • ABA/BCBA Behaviour Analysts • Special Educators • Neurodevelopmental Paediatricians • Clinical Research Organisation • WHO/UNICEF-Aligned ECD Specialists • Parent Champions • 70+ Center Network Across India
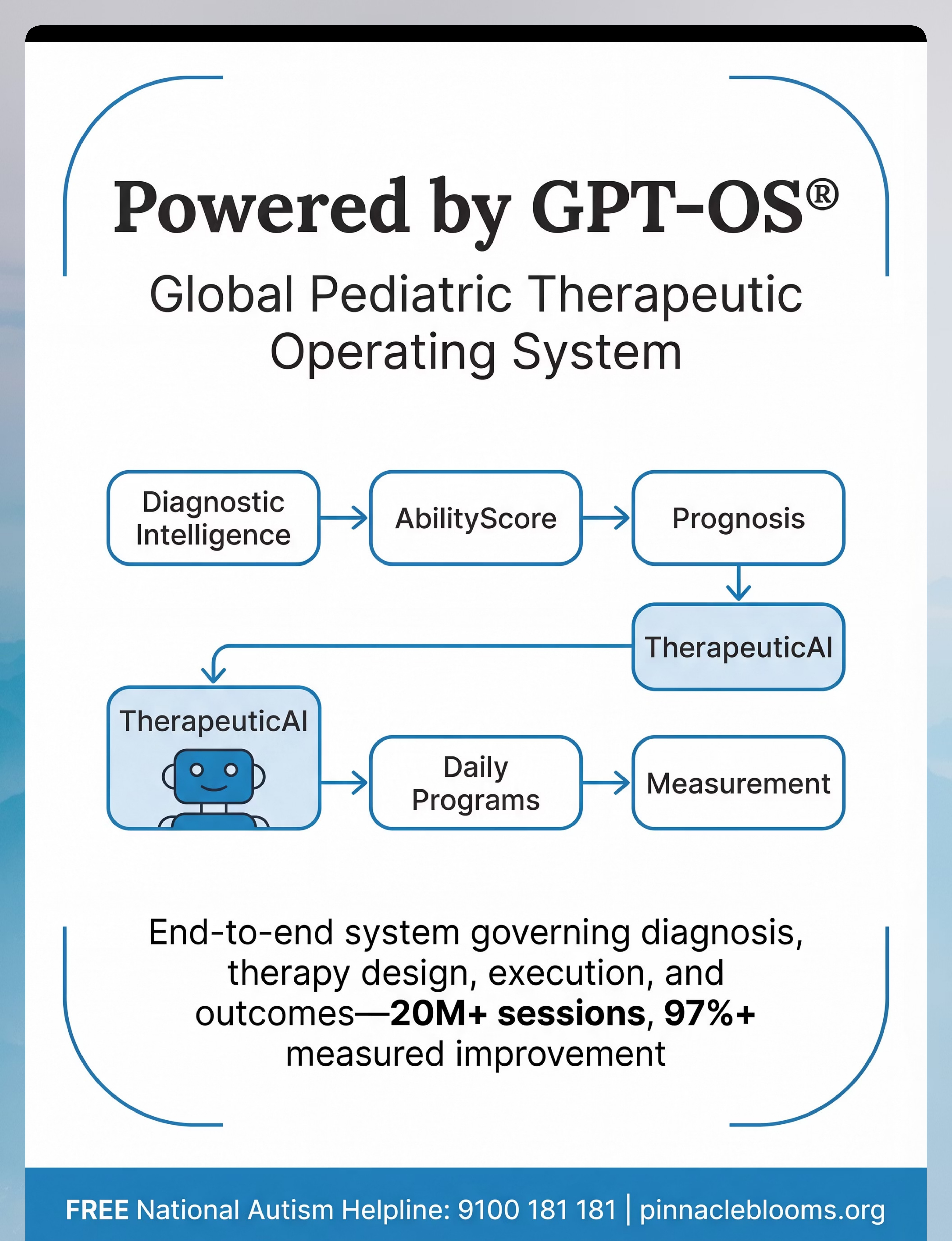
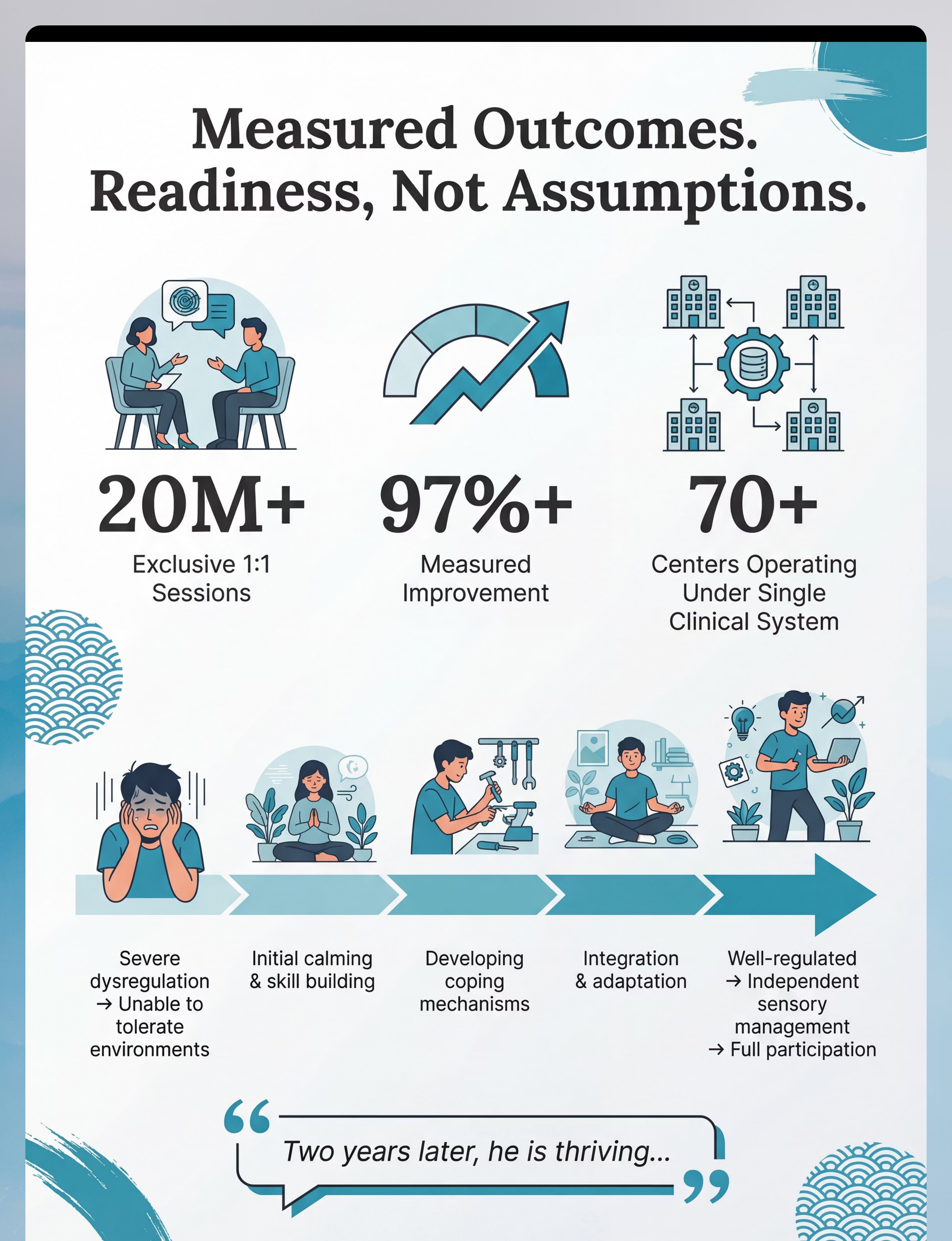
1
Therapy Sessions
Exclusive 1:1 sessions delivered under GPT-OS®
2
Measured Improvement
Across readiness indexes under GPT-OS® governance
3
Centers
Operating under one unified clinical system across India
4
Countries
Where Pinnacle IP is filed and protected
This is not a service. This is therapeutic infrastructure.
This content is educational. It does not replace individualized assessment and intervention from qualified occupational therapists and sensory integration specialists. Sensory needs vary significantly based on individual profile. Consult your child's occupational therapist before implementing a sensory program. Individual results may vary. Statistics represent aggregate outcomes across the Pinnacle Blooms Network® under GPT-OS® governance.
© 2025-2026 Pinnacle Blooms Network® | Unit of Bharath Healthcare Laboratories Pvt. Ltd.
CIN: U74999TG2016PTC113063 | DPIIT Recognition: DIPP8651 | MSME Udyog Aadhaar: TS20F0009606 | GSTIN: 36AAGCB9722P1Z2
All Rights Reserved | Patents Filed Across 160+ Countries
techniques.pinnacleblooms.org/sensory-processing/sensory-integration-materials-L-984
CIN: U74999TG2016PTC113063 | DPIIT Recognition: DIPP8651 | MSME Udyog Aadhaar: TS20F0009606 | GSTIN: 36AAGCB9722P1Z2
All Rights Reserved | Patents Filed Across 160+ Countries
techniques.pinnacleblooms.org/sensory-processing/sensory-integration-materials-L-984