
When Tiny Fingers Refuse to Cooperate
Your child reaches for the small piece of banana. Their whole hand swipes at it — and it rolls away. They try again. The palm closes around air. The banana is gone. Their face crumples. This moment is not clumsiness. This moment is a developmental signal — and it has a name.
F-592 · Pincer Grasp Development
9 Materials That Help Tiny Fingers Learn Precision

"You are not failing your child. Their cortical motor circuits are still forming the precise thumb-index opposition that makes human dexterity possible. You have just found the technique that accelerates that formation."
🏛️ Pinnacle Blooms Consortium
Multi-disciplinary pediatric therapy leadership — OT, SLP, ABA, SpEd, NeuroDev united.
🔬 OT-Led Protocol
Designed by Pediatric Occupational Therapists and validated across 20M+ sessions.
📅 Ages 8 months – 6 years
From emerging raking grasp to refined pre-writing precision.
⏱ 10–15 min/session
Short, focused, parent-delivered sessions. 3–5 times per week.
WHO Nurturing Care Framework 2018 | nurturing-care.org/ncf-for-ecd/

You Are Among Millions of Families Navigating This
Pincer grasp — the precise opposition of thumb and index fingertip — typically emerges between 9 and 12 months. For children with neurodevelopmental differences, sensory processing variations, or hypotonia, it may be absent, delayed, or inconsistently present well into the toddler and preschool years. When it is delayed, the downstream effects cascade: self-feeding, button fastening, pencil grip, scissor use, and academic writing all depend on this one foundational pattern. You are not overreacting by prioritizing it now.
1 in 36
Children with ASD Globally
CDC ADDM Network 2023 — fine motor delays affect 87% of this population.
~4M
Children in India
With developmental delays affecting hand function. ICMR National Burden of Disease Report.
80%
Children with ASD
Show measurable fine motor deficits including pincer grasp delay. PRISMA Systematic Review, PMC11506176 (2024).
"You are among millions of families around the world working on this exact skill. The techniques work. The materials help. The data is on your side."
Sources: PMC11506176 | PMC10955541 | DOI:10.12998/wjcc.v12.i7.1260
The Neuroscience of Pincer Grasp — In Plain English
Key Brain Regions Involved
🧠 Primary Motor Cortex (M1)
Commands finger movement — the brain's instruction center for hand precision.
🤚 Somatosensory Cortex (S1)
Receives fingertip feedback — tells the brain "I've gripped it."
🎯 Cerebellum
Coordinates precision and timing — the fine-tuning engine.
🔗 Corticospinal Tract
The motor highway — still myelinating between 18 months and 3 years.
What This Means for Your Child
Pincer grasp requires simultaneous activation of the primary motor cortex (M1), somatosensory cortex (S1), and the cerebellum's coordination circuits. In the developing child, the corticospinal tract — the neural highway from brain to hand — completes myelination between 18 months and 3 years.
In children with neurodevelopmental differences, this myelination may be slower, sensory feedback from fingertips may be muted or amplified, and the proprioceptive signals that tell the brain "I've gripped it" may not register at the right threshold.
Every time your child practices pincer grasp with the right materials, they are literally building new neural connections. The brain is not fixed — it is plastic. This is called neuroplasticity, and it is your most powerful therapeutic tool.
"Your child is not being stubborn or lazy. Their nervous system is requesting a different kind of input to build the precision map it needs."
Source: Frontiers in Integrative Neuroscience, 2020 | DOI:10.3389/fnint.2020.556660
The Pincer Grasp Developmental Map — Where Is Your Child?
Understanding where your child sits on the developmental timeline is the essential first step to choosing the right materials and setting realistic expectations for progress.
6–7 Months
Raking grasp — all fingers sweeping. Hand-to-mouth, whole-hand reach.
8–9 Months
Inferior pincer — thumb + side of index. Picks up small objects with side of finger.
9–10 Months
Emerging pincer — thumb + pad of index. Begins using fingertip, imprecise.
10–12 Months ⭐
True pincer grasp — thumb tip + index fingertip. This is the target.
12–18 Months
Refined pincer — controlled release. Places objects precisely, picks up tiny crumbs.
2–5 Years
Tool use + pre-writing — crayon hold, fork feeding, tripod pencil grip, scissor coordination.
Commonly Co-Occurring Conditions
Pincer grasp delay commonly co-occurs with: hypotonia, sensory processing differences, autism spectrum conditions, developmental coordination disorder (DCD), and prematurity-related fine motor delays.
WHO/UNICEF Alignment
This technique aligns with the WHO Care for Child Development (CCD) Package milestones — implemented across 54 low- and middle-income countries as the international gold standard for early developmental support.
Source: PMC9978394 | WHO/UNICEF CCD Package 2023

Pincer Grasp Development via Material Progression
The Tiny Fingers Protocol
F-592
Domain F: Fine Motor
Pincer grasp development through material progression is a structured fine motor intervention where specific tactile and resistive materials are presented sequentially to train the precise opposition of the thumb tip and index fingertip. Each material is selected for its unique sensory feedback, resistance profile, and intrinsic motivation properties — enabling the child to naturally practice the thumb-index pinch pattern hundreds of times across play sessions without perceiving it as work.
Corticospinal Pattern
Builds the neural motor pattern for precise digit opposition — thumb tip to index fingertip.
Intrinsic Muscle Strength
Targets the first dorsal interosseous and flexor pollicis longus — the small muscles within the hand itself.
Tactile Discrimination
Develops the fingertip's ability to "feel" a successful grasp — without visual confirmation.
Tool Use Foundation
Prepares the foundation for pencil, scissors, buttons, and cutlery — every future precision task.
🏷️ Age
8 months – 6 years
⏱ Duration
10–15 minutes per session
📅 Frequency
3–5 sessions per week
🔬 Reel
F-592 (Fine Motor Series)

This Technique Crosses Every Therapy Boundary
Pincer grasp is simultaneously a motor, sensory, behavioral, communicative, and educational target. The Pinnacle Blooms consortium approach integrates five disciplines around this single developmental goal.

🤲 Pediatric Occupational Therapist (Primary Lead)
The OT is the architect of pincer grasp progression. They assess grip patterns using standardized tools (PDMS-2), select the correct material resistance level, and design the 8-week progression protocol.

🗣️ Pediatric Speech-Language Pathologist
Uses pincer grasp materials to develop oral motor precision. The same thumb-index motor control that picks up a peg also controls the precision movements of the articulators — water droppers and tweezers train identical graded force control.
🎯 ABA/BCBA Behavior Analyst
Designs the reinforcement architecture around pincer practice. Establishes the shaping program, calibrates reinforcement schedules, and uses Discrete Trial Training (DTT) for targeted finger discrimination work.

📚 Special Educator
Integrates pincer practice into pre-writing curriculum. Ensures classroom accommodations align with the OT's precision targets — coloring, cutting, and early writing all build on pincer grasp.

🧠 NeuroDevelopmental Pediatrician
Monitors neurodevelopmental trajectory, rules out tone disorders requiring medical management, and coordinates the therapy team's progression targets with the child's overall neurodevelopmental profile.
20M+
Sessions Delivered
97%+
Measured Improvement
70+
Centers Across India
70+
Countries Served

What Exactly Are We Building? The 9 Functional Targets
Every session with these materials trains one or more of these precise neuromotor and functional capacities. Mastery of all 9 targets translates directly to self-feeding, dressing independence, pre-writing readiness, scissor use, and full classroom participation.
1
Digit Opposition
The ability to bring the tip of the thumb precisely to the tip of the index finger, creating the "O" shape of a perfect pincer grasp.
2
Intrinsic Muscle Strength
Strength of the small muscles within the hand: first dorsal interosseous, palmar interossei, flexor pollicis longus. These cannot be strengthened by gross grip exercises.
3
Force Grading
The ability to modulate grip pressure — enough to hold without dropping, not so much as to crush. Critical for handling delicate objects.
4
Tactile Discrimination
The fingertips' ability to recognize a successful grasp — without visual confirmation. The child eventually doesn't need to watch their hand.
5
Release Control
The ability to place an object precisely where intended and release at the correct moment. Equally important as the grasp itself.
6
Bilateral Hand Coordination
One hand holds/stabilizes while the other performs the pincer action. Pre-requisite for scissors, buttons, and all tool-based tasks.
7
Sustained Attention
The ability to remain engaged with a small-scale manual task for 3–10 minutes. Attention and motor skill develop together.
8
Motor Planning (Praxis)
The ability to plan the sequence: reach → orient fingers → grasp → lift → transport → place → release. Each step must be automatized.
9
Hand Dominance Emergence
Consistent preference for one hand in precision tasks. Emerges through repeated practice and is fully established by ages 3–4.
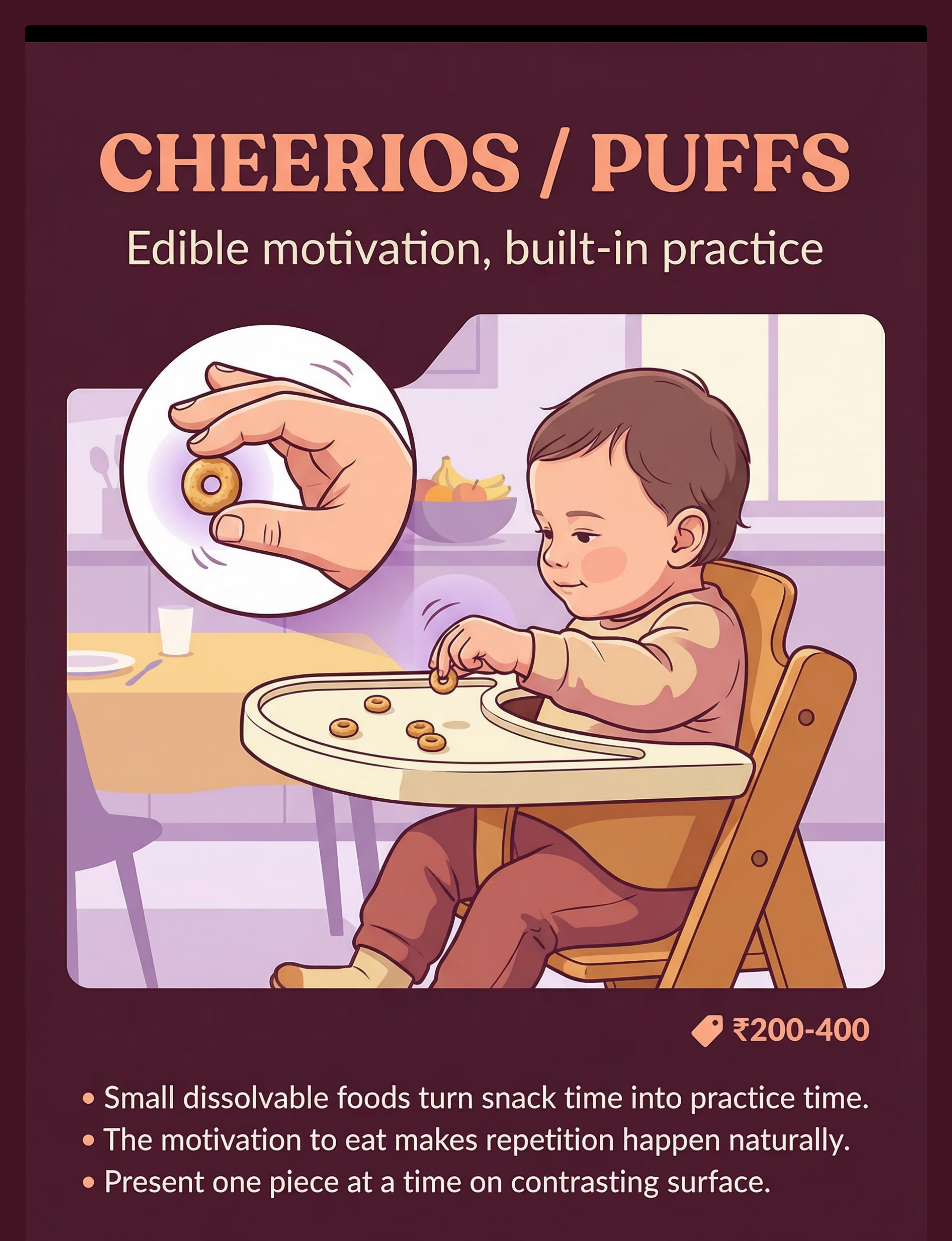
🥣 Material 1 — Cheerios / Puffs
Easiest · Start Here
Pinnacle Recommends
Edible Motivation, Built-In Practice
Small dissolvable cereals or baby puffs turn snack time into therapy time. The motivation to eat drives natural repetition without any therapeutic framing. The child attempts the pincer grasp hundreds of times per day across meals.
Why It Works
- Size forces true fingertip opposition — the piece is too small for a palm grasp
- Dissolvable texture eliminates choking risk
- Intrinsic motivation (hunger + taste preference) provides continuous reinforcement
How to Use
Present 3–5 pieces at a time on a contrasting flat surface — a white plate or dark tray. Offer one piece at a time. Resist helping. Let the child figure it out.
Progression Tips
- Start with puffs (slightly larger, easier to grasp)
- Progress to Cheerios (smaller circumference)
- Progress to any similar-sized preferred food
Cost & Accessibility
₹200–400 for commercial puffs/Cheerios · DIY: Any small, safe, dissolvable food your child enjoys — raisins, small idli pieces, cereal pieces
This is the single most important material for children 8–14 months. Food motivation is the most powerful, lowest-barrier entry point into pincer practice.

⭐ Material 3 — Sticker Sheets
Pinnacle Recommends
Built-In Reinforcer
Peel, Stick, Repeat — Forever
Peeling stickers from backing paper requires precise fingertip opposition and controlled pull. A child will practice this for 45 minutes without noticing it is therapy. The reward is placing the sticker — a built-in reinforcer that requires no external management.
Why It Works
- Peeling action demands finger opposition + controlled traction force
- Placing action trains precise release at exactly the right moment
- Intrinsic motivation (beautiful stickers + creative placement) sustains repetition
- Zero safety concerns — completely safe for all ages above 12 months
How to Use
Present the sticker sheet on a flat surface. Let the child choose which sticker. A reward chart backing doubles as the placement target — giving the release action a clear purpose.
Progression Tips
- Start with large stickers (easier peel edge)
- Progress to smaller dot stickers
- Add a precise placement target (small boxes on paper) for older children
Cost & Accessibility
₹50–300 · Canon product link: amazon.in (₹364) · DIY: Any adhesive labels, folded tape pieces on paper backing
🦾 Material 4 — Tweezers & Tongs
Canon: Tweezers / Tongs / Transfer Activities
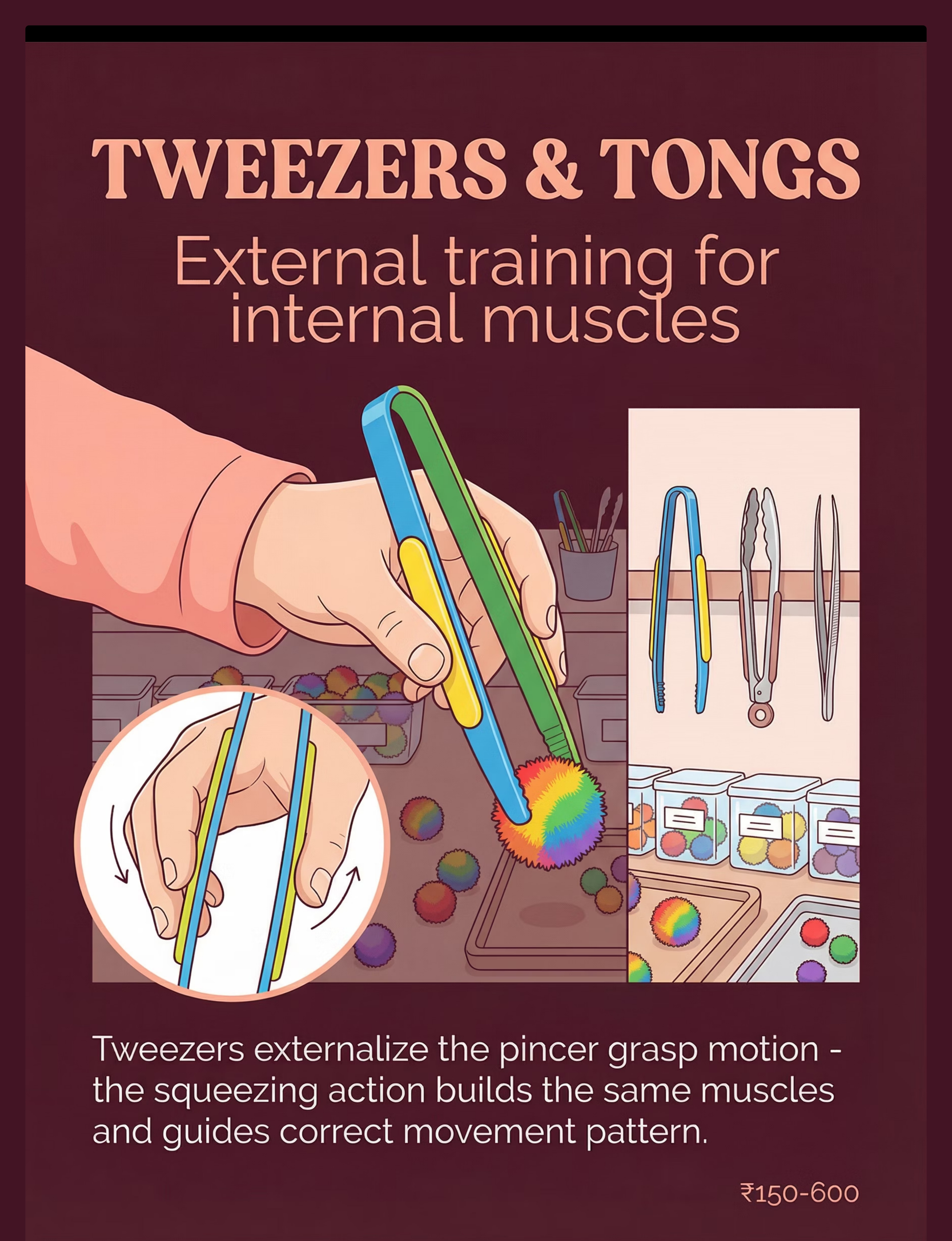
External Training for Internal Muscles
Tweezers externalize the pincer grasp motion — the squeezing action builds the same intrinsic muscles and guides the correct movement pattern. The tool amplifies the motor learning signal, making the invisible motion visible and accessible. The larger leverage handle makes the motion accessible for children who lack fingertip strength.
Why It Works
- Resistance of spring-loaded tweezers strengthens finger opposition muscles directly
- Progressive tool sizes allow systematic grading of difficulty
- The tool guides the correct finger position even before the child can execute it independently
How to Use
Transfer pom poms from one container to another. Begin with large silicone tongs → progress to craft tweezers → progress to fine-point tweezers. 5 transfers = 1 set. Count aloud with the child.
Progression
- Large silicone tongs (most accessible)
- Standard craft tweezers
- Fine-point tweezers (most demanding)
Cost & Accessibility
₹150–600 · Amazon.in: "therapy tweezers children fine motor" · DIY: Chopsticks rubber-banded at the top, or binder clips with rubber padding — same squeeze-opposition pattern

🎉 Material 5 — Pom Poms (Graded Sizes)
Canon: Tactile Sensory Kit
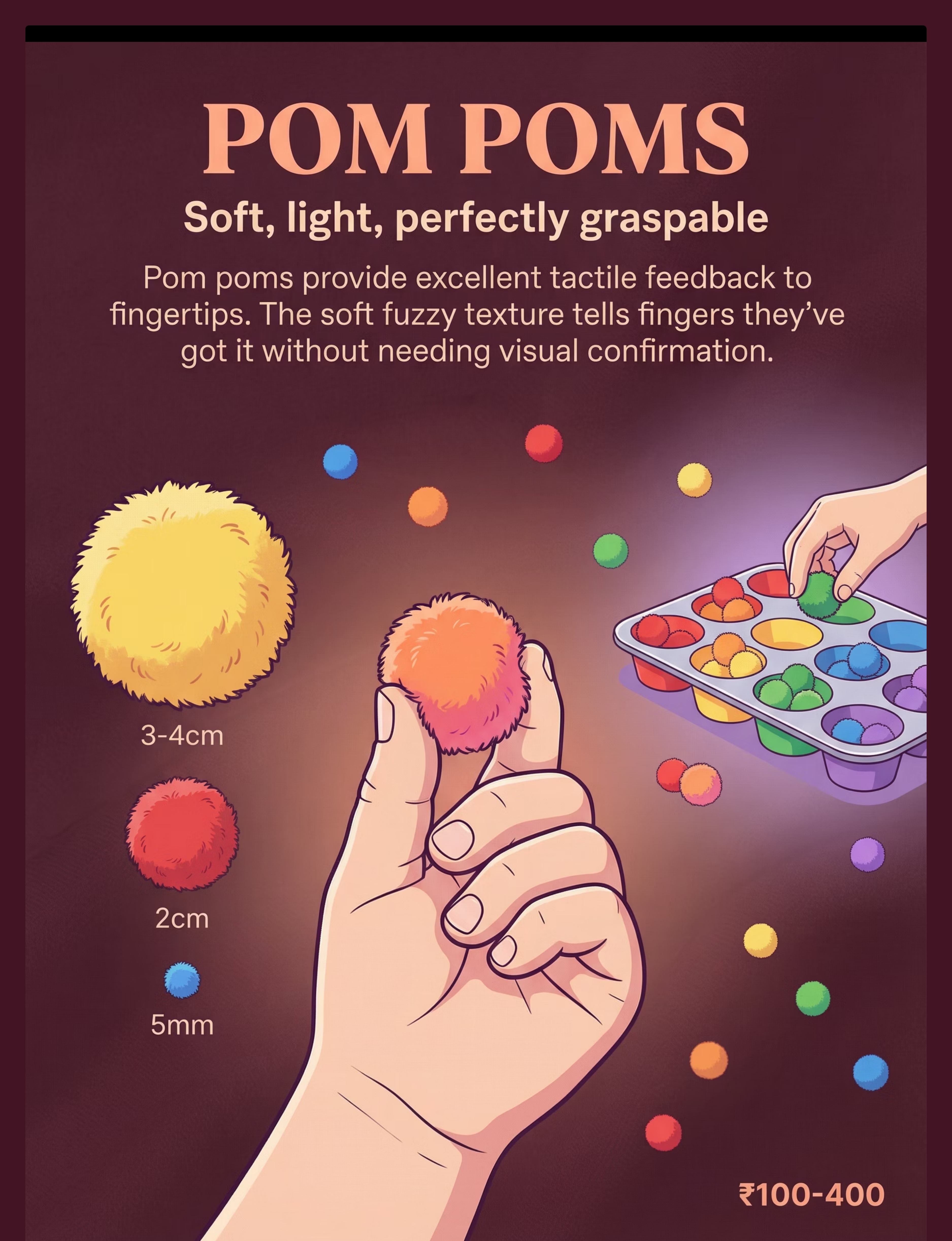
Soft, Light, Perfectly Graspable
Pom poms provide excellent tactile feedback to the fingertips. The soft fuzzy texture tells the fingers they have grasped it — without needing visual confirmation. This tactile signal is the training ground for independent grasp awareness.
Why It Works
- Tactile feedback from textured surface trains fingertip discrimination
- Graded sizes enforce pincer progression — force the hand to adapt
- Light weight eliminates grip-strength barrier, isolating precision as the only variable
Size Progression
- 3–4 cm — Beginner (wide margin for error)
- 2 cm — Intermediate (demands real fingertip use)
- 5 mm — Advanced (true pincer required)
How to Use
Color-sort pom poms into a muffin tray using fingers only. Progress the grasp pattern: palm → 3 fingers → 2 fingers → pincer. Count successes, not failures.
Engagement Ideas
- Sort by color into a muffin tin
- Transfer from bowl to bowl using only two fingers
- Build a "pom pom tower" (place on top of each other)
- Count pom poms into small cups
Cost & Accessibility
₹100–400 for craft pom pom sets · DIY: Tightly rolled cotton balls or torn tissue balls provide the same tactile feedback principle at zero cost

📿 Material 6 — Beads & Lacing
Canon: Lacing / Beading / Threading Activities
Advanced
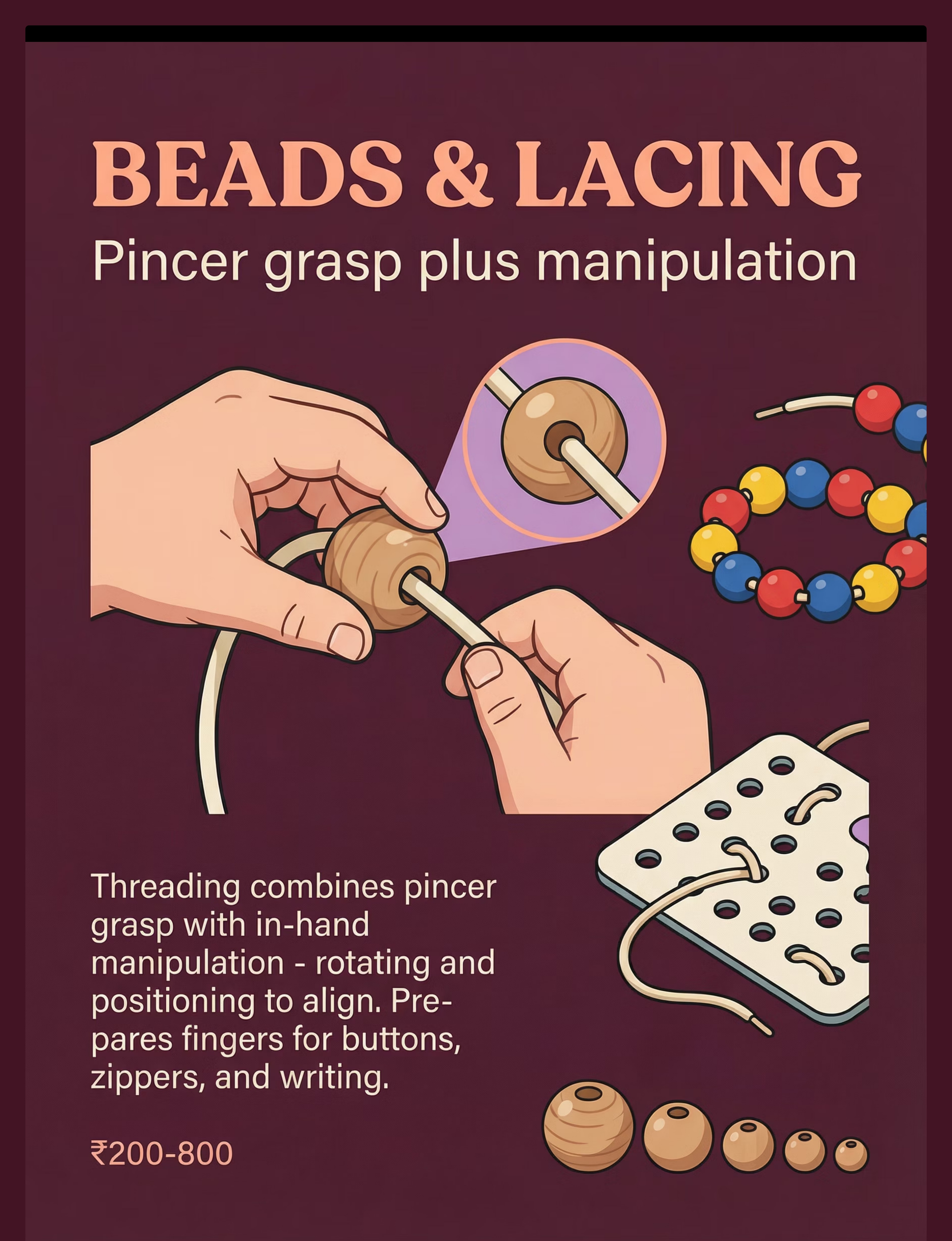
Pincer Grasp Plus Manipulation
Threading beads onto a lace combines pincer grasp with in-hand manipulation — rotating and positioning to align the hole. This is the advanced pincer training that prepares fingers for buttons, zippers, and writing. It is the closest analog to pencil holding of any material in this protocol.
Why It Works
- Threading requires sustained pincer hold + bilateral coordination + hole alignment precision
- The sequence demands motor planning at every single step
- Completing a "necklace" provides a natural, visual reward for sustained effort
How to Use
Start with large-hole wooden beads + thick shoelace. Model threading slowly and with exaggerated finger positioning. Progress systematically:
- Large-hole wooden beads + shoelace
- Smaller beads + thinner cord
- Needle + large-hole card (pre-sewing activity)
Cost & Accessibility
₹200–800 · Amazon.in: "wooden lacing beads toddler montessori" · DIY: Pasta tubes (rigatoni, penne) on a shoelace — same threading + manipulation demand at near-zero cost
Threading is slow — prioritize quality over speed. 3 excellent threads are worth more than 10 rushed attempts.
🪵 Material 7 — Clothespins
Canon: Therapy Putty / Resistive Hand Tools
Canon: Therapy Putty / Resistive Hand Tools
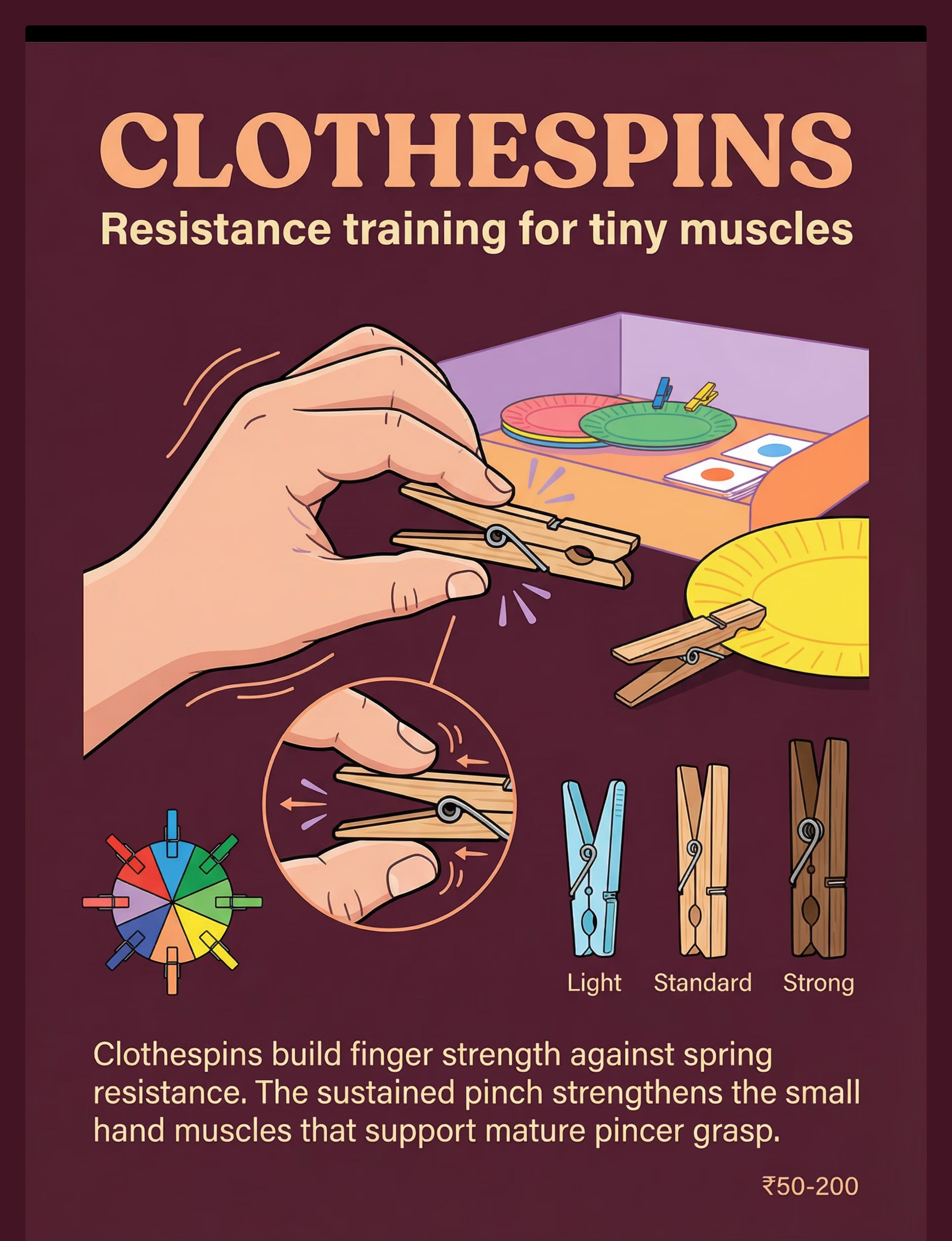
Resistance Training for Tiny Muscles
Clothespins build finger strength against spring resistance. The sustained pinch directly strengthens the small hand muscles that support mature pincer grasp. Available in light (child-accessible), standard, and strong resistance grades — making them one of the most systematically adjustable materials in the protocol.
Why It Works
- Spring resistance provides graded, calibrated strengthening
- Open-close action directly targets pincer opposition muscles
- The clip-onto-rim activity combines grasp, force grading, and precise placement in one motion
Resistance Progression
- Soft plastic clothespins (most accessible)
- Standard wooden clothespins
- Strong wooden clothespins (most demanding)
How to Use
Clip clothespins around the rim of a plastic bowl or plate. Color-match to a color wheel or color chart to add cognitive engagement. One full circle around the bowl rim = one set.
Engagement Ideas
- Match colored clothespins to colored dots on bowl rim
- Clip onto a cardboard "hedgehog" — spines made of clothespins
- Use to hang "artwork" on a mini clothesline
- Clip and unclip onto the edge of a thick board book
Cost & Accessibility
₹50–200 for standard clothespins · DIY: Any spring-loaded clip with rubber padding applied to the grip area — same spring resistance mechanism

🌈 Material 8 — Therapy Putty With Treasures
Canon: Playdough / Therapy Putty / Modeling Clay
Dig, Find, Extract, Repeat
Hiding small objects (beads, coins, mini toys) in resistive putty combines strengthening with precision. Every extraction is a perfect pincer grasp disguised as treasure hunting. The intrinsic motivation of discovery drives repetition that no amount of external prompting could match.
Why It Works
- Resistive putty requires sustained pincer force to extract objects
- The intrinsic motivation of treasure hunting drives high-frequency repetition
- Resistance grade is clinically adjustable — soft, medium, and firm grades available
- Resistive proprioceptive input is calming for sensory-seeking children
How to Use
Hide 5–8 small objects in putty. Child excavates with thumb + index finger only (no full fist). Count treasures found. Celebrate each extraction as a major event.
Resistance Progression
- Soft putty / homemade dough (most accessible)
- Medium resistance commercial putty
- Firm resistance putty (most demanding)
Cost & Accessibility
₹200–600 for commercial therapy putty · DIY: Homemade dough — 1 cup flour + ½ cup salt + ½ cup water + 1 tbsp oil. Knead firm. Add hidden objects. Same resistive property at ₹0 material cost.

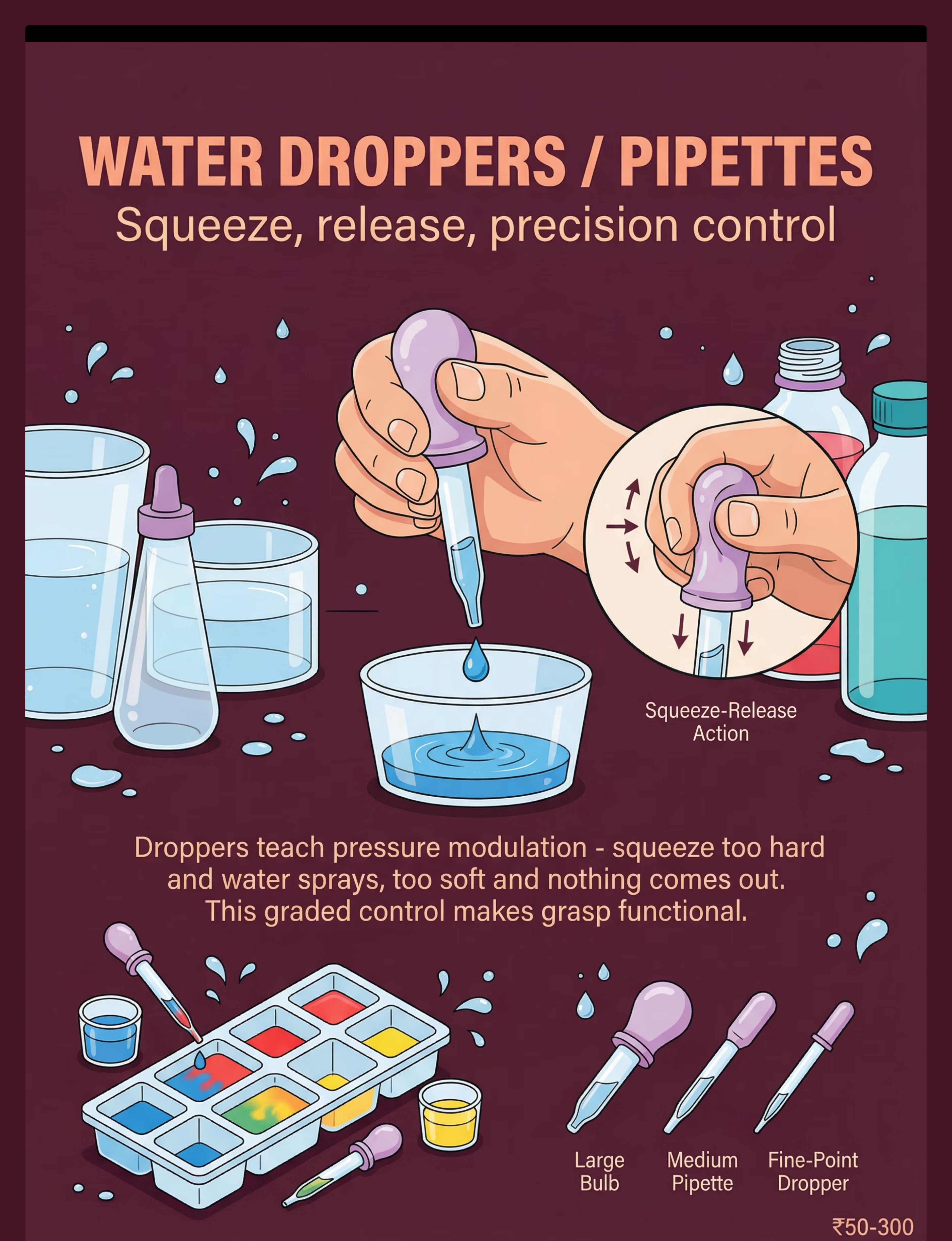
💧 Material 9 — Water Droppers / Pipettes
Canon: Tweezers / Tongs / Transfer Activities
Advanced
Squeeze, Release, Precision Control
Droppers teach pressure modulation — the same graded force control that makes a precise pincer grasp functional. Squeeze too hard and water sprays; too soft and nothing comes out. This graded biofeedback makes grasp not just present, but functional.
Why It Works
- Squeeze-release action mirrors pincer force grading precisely
- The visual feedback of water drop size teaches calibration in real time
- Color mixing play sustains motivation across many squeeze cycles
- Targets Force Grading (Target 3) and Release Control (Target 5) simultaneously
How to Use
Transfer colored water into ice cube trays. Mix colors in the tray as a reinforcement activity. The child watches results of their own precision — an immediate, visual, motivating consequence.
Tool Progression
- Large bulb dropper (most accessible)
- Medium pipette
- Fine-point dropper (most demanding)
Cost & Accessibility
₹50–300 for pharmacy bulb syringes or pipette sets · DIY: Clean empty ketchup bottle, small squeeze bottle, or any bulb syringe — same graded force feedback at minimal cost
Color mixing play is one of the highest-engagement activities for children ages 2–5. Leverage this natural motivation fully.

Every Family Can Start Today — With ₹0 or ₹100
WHO Equity Principle
Evidence-based intervention must be accessible to every family, regardless of economic status. Every material in this protocol has a household substitute that delivers the same therapeutic mechanism. A complete 15-minute pincer grasp session can be run today using small food pieces on a plate, a homemade dough ball with hidden coins, and a clean squeeze bottle with colored water. Total material cost: ₹0.
Material | Clinical Option | DIY / Household Substitute | |
Cheerios/Puffs | Any baby puff cereal | Small, soft, safe food (raisin, small idli piece) | |
Pom Poms | Craft pom poms 3–4cm | Tightly rolled cotton balls, tissue balls | |
Stickers | Sticker sheets | Any adhesive label, folded tape pieces | |
Tweezers | Spring tweezers or craft tongs | Chopsticks rubber-banded at top, binder clips | |
Therapy Putty | Commercial putty (soft/medium/firm) | 1 cup flour + ½ cup salt + ½ cup water + 1 tbsp oil | |
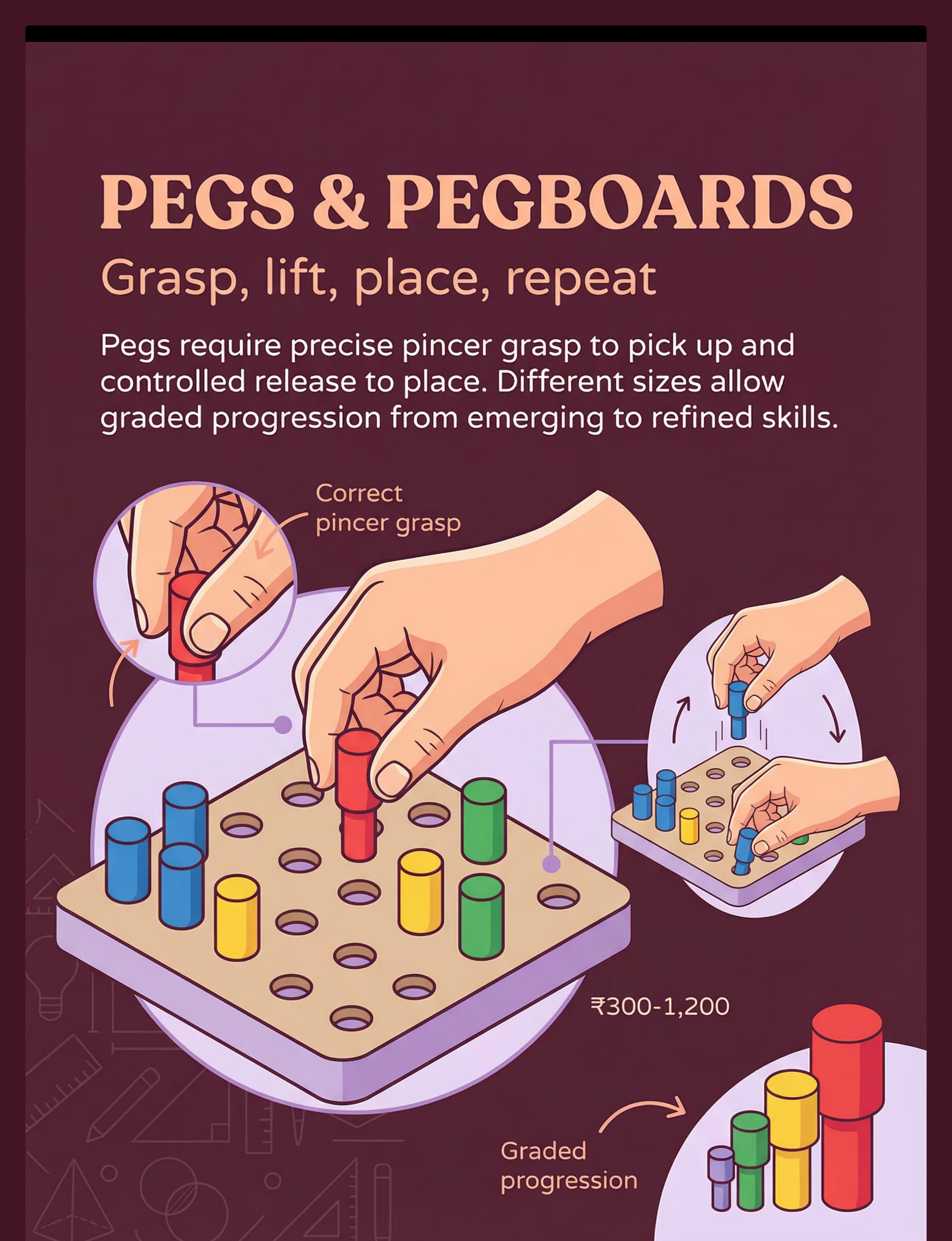
Pegs/Pegboard | Commercial wooden pegboard | Golf tees inserted into foam / Styrofoam block | |
Beads + Lace | Wooden beads + lace | Pasta tubes + shoelace; uncooked rigatoni on cord | |
Clothespins | Standard clothespins | Binder clips with rubber padding | |
Droppers | Pharmacy bulb syringe | Clean ketchup bottle / small squeeze bottle |
Important Caveat: When the child's challenge includes significant hypotonia or sensory defensiveness, clinical-grade materials with calibrated resistance are preferred. Consult your OT for personalized material selection guidance. Source: WHO NCF 2018 | PMC9978394

⚠️ Read This Before Every Session — Safety First
Every session begins with this safety assessment. It takes 60 seconds and protects both your child and the therapeutic relationship you are building.
🔴 RED — Do NOT Proceed if:
- Child is showing signs of illness, fever, or significant fatigue
- Child has had a meltdown or significant dysregulation in the past 2 hours
- Child has open wounds, abrasions, or skin sensitivity on hands or fingers
- Child has a known latex allergy (check commercial putty packaging)
- Session involves food materials and child has known food allergies
🟡 AMBER — Modify if:
- Child is mildly dysregulated (simplify to easiest material: puffs only)
- Child has tactile defensiveness (begin with clothespins or pegs before putty)
- Child is 8–12 months: use only food materials with full adult supervision
- Child is showing avoidance: reduce demand to observation/imitation only
🟢 GREEN — Proceed when:
- Child is rested, fed (but not immediately post-meal), and in a calm-alert state
- Environment is prepared per the Space Setup card
- You have 15 uninterrupted minutes
- All materials have been inspected for integrity
Choking Safety (Critical): All small materials require constant adult supervision. Children 8–24 months: food materials ONLY unless the child has demonstrated safe object handling. Never leave a child unattended with small materials. The finger rule: if it fits through a toilet paper roll, it is a choking hazard for under-3s. If a child shows strong aversion to a material (palm withdrawal, distress vocalization), do NOT force. Respect the nervous system's signals.
📞Pinnacle Helpline: 9100 181 181 — free clinical guidance in 16 languages. Source: DOI:10.1007/s12098-018-2747-4 — Padmanabha et al., Indian J Pediatr 2019

Stage the Therapy Space in 3 Minutes
Studies confirm that 80% of session failures occur before the technique begins — in the environment setup phase. Get this right and you have already won half the session.
1
Seat the Child Correctly
Chair height so feet are flat (use a step stool if needed). Hips at 90°. Table height at elbow level. Good posture = better motor control.
2
Clear the Work Surface
No toys, screens, or distractions on or near the therapy tray. One material visible at a time. Simplicity is therapeutic.
3
Prepare Materials in Order
Lay out today's planned materials on the side table in sequence. Keep them out of the child's view until needed. Novelty sustains attention.
4
Create Contrasting Surface
Use a dark tray for light-colored materials (pom poms, puffs) and a light surface for dark materials. Visual contrast is essential for accurate reaching and grasp precision.
5
Position Yourself Correctly
Sit beside the child (not across). This enables side-by-side modeling and prevents face-to-face confrontation dynamics that increase demand perception.
6
Remove All Distractions
Turn off TV. Move other toys out of sight. One child, one parent, one material at a time.
7
Add a Visual Timer
A sand hourglass or digital visual timer shows session length — reduces the child's anxiety about "when will this end?" and dramatically improves session completion rates.
Source: PMC10955541 | Sensory Integration Theory (A.J. Ayres)

The 60-Second Pre-Flight Check
Read Before EVERY Session
The best session is one that starts right. Run this check before every single session — including when you're feeling rushed. Two minutes of assessment prevents 15 minutes of frustration.
✅ Awake for at least 30 minutes
Not drowsy — a sleepy child cannot build motor pathways effectively.
✅ Light meal or snack within 1–2 hours
Not hungry, not overfull — both states reduce fine motor engagement quality.
✅ No significant meltdown in past 2 hours
Cortisol levels need time to return to baseline before precision motor work.
✅ Hands clean and dry
Wet or dirty hands alter tactile feedback and may increase material aversion.
✅ Child is alert and orienting to environment
Eye contact or environmental awareness — the calm-alert state is the optimal learning state.
✅ You have 15 uninterrupted minutes
Your calm, patient presence is as important as any material.
🟢 GO (6–7 ticks)
Proceed to Step 1 — begin the session with full protocol.
🟡 MODIFY (4–5 ticks)
Use simplest version — one food-based material only, 5 minutes maximum, no performance expectations.
🔴 POSTPONE (3 or fewer)
Today is not the day. Offer a preferred sensory activity instead. Document and try again tomorrow.
"A modified session that ends positively is worth more than a perfect session that ends in distress. Positive endings build motivation for tomorrow."

Step 1 — The Invitation
30–60 Seconds
ABA Pairing + OT Just-Right Challenge
Every pincer grasp session begins with an invitation, not a demand. The child is offered a choice, not given an instruction. This is where ABA's pairing principle meets OT's "just-right challenge" — and where the session's emotional tone is set for everything that follows.
Your Script by Language Level
For Verbal Children
"Look what I have! Want to play the picking-up game?"
For Pre-Verbal Children
Place one puff on tray. Look at child. Wait 5 seconds. Point to material. Smile. No words required.
For Reluctant Children
Demonstrate picking up the material yourself with exaggerated pincer grasp. Narrate: "Ooh, I picked one up! So tiny! So tricky!"
Body Language Guide
- Lean slightly toward child — engagement signal
- Open palm toward material — inviting gesture
- Eyebrows slightly raised — curious, not demanding
- No physical prompting yet — observe natural response first
Acceptance Cues → Proceed to Step 2
- Child reaches toward material
- Child looks from material to caregiver
- Child picks up material in any grasp pattern
- Child smiles or vocalizes in response
Resistance Cues → Modify
- Child turns away or pushes tray
- Child shows distress → Remove tray, offer preferred sensory activity, try again in 10 minutes

Step 2 — The Engagement
1–3 Minutes
Step 2 of 6
The child is now interacting with the material. This step deepens engagement by presenting the material correctly and beginning reinforcement. Do not correct grasp pattern yet — only observe and reinforce the attempt.
Material Presentation
- Present ONE piece at a time on the contrasting surface
- Place it in the child's midline, reachable distance (20–30cm from body)
- Height: flat on surface — elevated objects invite palmar grasp
- Distance encourages full reach, not a lazy grab
Begin Reinforcement Immediately
The moment the child touches the material: "You reached! Great reaching!"
When they pick it up — regardless of grasp quality: "You got it! Excellent!"
Observe the Grasp Pattern — Don't Correct Yet
What You See | What It Means | |
Full palm/raking | 6–8 month level — use easiest materials | |
Inferior pincer (side of index) | 8–9 month level — you're in the right zone | |
Pad-to-pad opposition | 9–10 month level — close to target | |
Tip-to-tip pincer | Target achieved — use harder materials |
Engagement Indicators — Green Lights
- Child looking at material and at their own hands
- Child attempting repeatedly after drops
- Child vocalizing or showing excitement
Source: PMC11506176 | Reinforcement scheduling, ABA literature

Step 3 — The Therapeutic Action
3–8 Minutes
The Active Ingredient
This is where the neurological work happens. For each material, follow this precise execution sequence every single time — consistency of presentation is itself a therapeutic input.
1
Place
Set one item on the contrasting surface in the child's midline.
2
Wait
Give 5 seconds for spontaneous attempt before any prompt. Spontaneous attempts are worth 3x prompted attempts.
3
Model
If needed: demonstrate with your own hand using an exaggerated, slow pincer grasp. No verbal instruction needed.
4
Observe
Record the grasp pattern used — mentally or on the session data sheet.
5
Allow
Let the child complete the action: place in container, eat the food, clip the peg.
6
Reinforce
Immediate reinforcement — within 3 seconds of success (see Step 5).
7
Reset
Replace the item and repeat. Each trial is a new neural practice opportunity.
❌ Child uses raking/palmar grasp consistently
✅ Switch to an even smaller or rounder material. Reduce surface area so palm cannot gain purchase. Try 5mm pom pom instead of 3cm.
❌ Child refuses to touch the material
✅ Desensitize — put material in parent's hand first, then on surface near child. Never force contact.
❌ Child picks up but drops immediately
✅ Provide a clear target container (muffin tin, small cup) — gives the release action a purpose.
❌ Child uses the same hand only
✅ Under age 2, do NOT force hand switching. Above 2, gently place next piece on the other side of midline.

Step 4 — Repeat & Vary
3–5 Minutes
Therapeutic Dosage
3 excellent, self-motivated pincer attempts are worth more than 15 prompted, forced repetitions. Watch for the satiation point — and use variation to push it further out.
Material | Target Reps | Notes | |
Puffs / Cheerios | 20–50 naturally | Let hunger drive repetition during snack time | |
Pom Poms | 10–15 transfers | Color sorting adds motivation without adding demand | |
Stickers | 8–12 peel-and-place | One sticker book page per session is a natural boundary | |
Tweezers/Tongs | 10–15 transfers | Count aloud with the child — adds language enrichment | |
Putty + Treasures | 5–8 extractions | Stop when putty loses novelty — re-hide for next session | |
Pegs | 8–12 insert-remove | One row of pegboard = one set — clear visual completion | |
Beads | 3–6 threads | Threading is slow — quality over speed always | |
Clothespins | 8–10 clip-unclip | Around bowl rim — one full circle = one complete set | |
Droppers | 6–10 squeeze cycles | Color-mixing sustains interest beyond the motor task |
🔄 Material Switch
If engagement drops, switch to a different material mid-session — novelty restores motivation instantly.
🎯 Target Change
Switch the container — muffin tin → small cup → tiny bottle. Same material, new challenge.
🏆 Challenge Up
Reduce material size when child consistently succeeds. Always follow the child's mastery signal.
⬇️ Challenge Down
Return to an easier material immediately if frustration appears. There is no shame in regression — only data.
"End every session on a success. Set up one very easy final trial and make it a big celebration. The last impression drives motivation for the next session."

Step 5 — Reinforce & Celebrate
Within 3 Seconds of Success
ABA Reinforcement Principles
Timing matters more than magnitude. Immediate, specific, enthusiastic reinforcement delivered within 3 seconds of the desired behavior is 400% more effective than delayed, generic praise. The brain needs the connection between action and consequence to be near-simultaneous.
1
For the reach attempt:
"You reached! I saw those fingers working!"
2
For a successful pick-up (any grasp):
"You got it! Excellent picking up!"
3
For a true pincer grasp attempt:
"PINCER! Look at those fingers — thumb AND pointer! YES!"
4
For controlled release into target:
"You placed it! Perfect! Right in the cup!"
🌟 Social Reinforcement
High-five, fist bump, specific verbal praise, happy dance, thumbs up, excited face. Most generalizable — works everywhere, always.
🏅 Token Economy
Sticker on chart for each 5 successful pincer attempts → earns a preferred activity. Builds delayed gratification alongside motor skill.
🎯 Natural Consequence
The food gets eaten. The sticker goes on the chart. The treasure is found. The colors mix. Zero setup required.
🎮 Activity Reinforcement
3 minutes of preferred screen or toy after achieving session target — for highly motivated, goal-oriented children.
"Celebrate the attempt, not just the success. A child who tries and fails a pincer grasp deserves the same enthusiastic response as one who succeeds perfectly — you are reinforcing the effort, the courage to try."
The Rosette Imprint Reward Jar (₹589) — a physical, tangible reward jar system providing visual and tactile reinforcement for session completion. 🔗amazon.in/d/02C5R9Jn

Step 6 — The Cool-Down
1–2 Minutes
Nervous System Transition
No session ends abruptly. The child's nervous system needs a transition signal. Abrupt endings are the primary cause of post-session dysregulation — the tantrum after therapy. A consistent, predictable ending ritual prevents this entirely.
1
60-Second Warning
"Two more. Then all done!" Hold up two fingers. This transition warning gives the brain time to prepare for the shift.
2
Final 2 Trials
Make them the easiest possible. Set the child up to succeed. Big celebration on the very last one.
3
"All Done" Ritual
"All done with finger practice! Let's put everything away." Child participates in cleanup — this naturally extends fine motor practice.
4
Transition to Next Activity
"Finger practice is finished. Now it's [preferred activity] time." A visual schedule card showing the next activity helps enormously.
If Child Resists Ending
- Give one more trial ("One bonus round!")
- Let them put the last piece away themselves ("You finish it!")
- Redirect attention to the next activity before materials are removed
Calming Sensory Input (if needed)
- Hand washing in warm water — gentle proprioceptive + thermal input
- Gentle hand massage provided by parent
- "Hand hug" — child squeezes parent's hand firmly 3 times
Source: NCAEP 2020 — Visual supports as evidence-based practice | Pinnacle OT transition protocols

Track Progress in 60 Seconds — Right After the Session
Data Collection
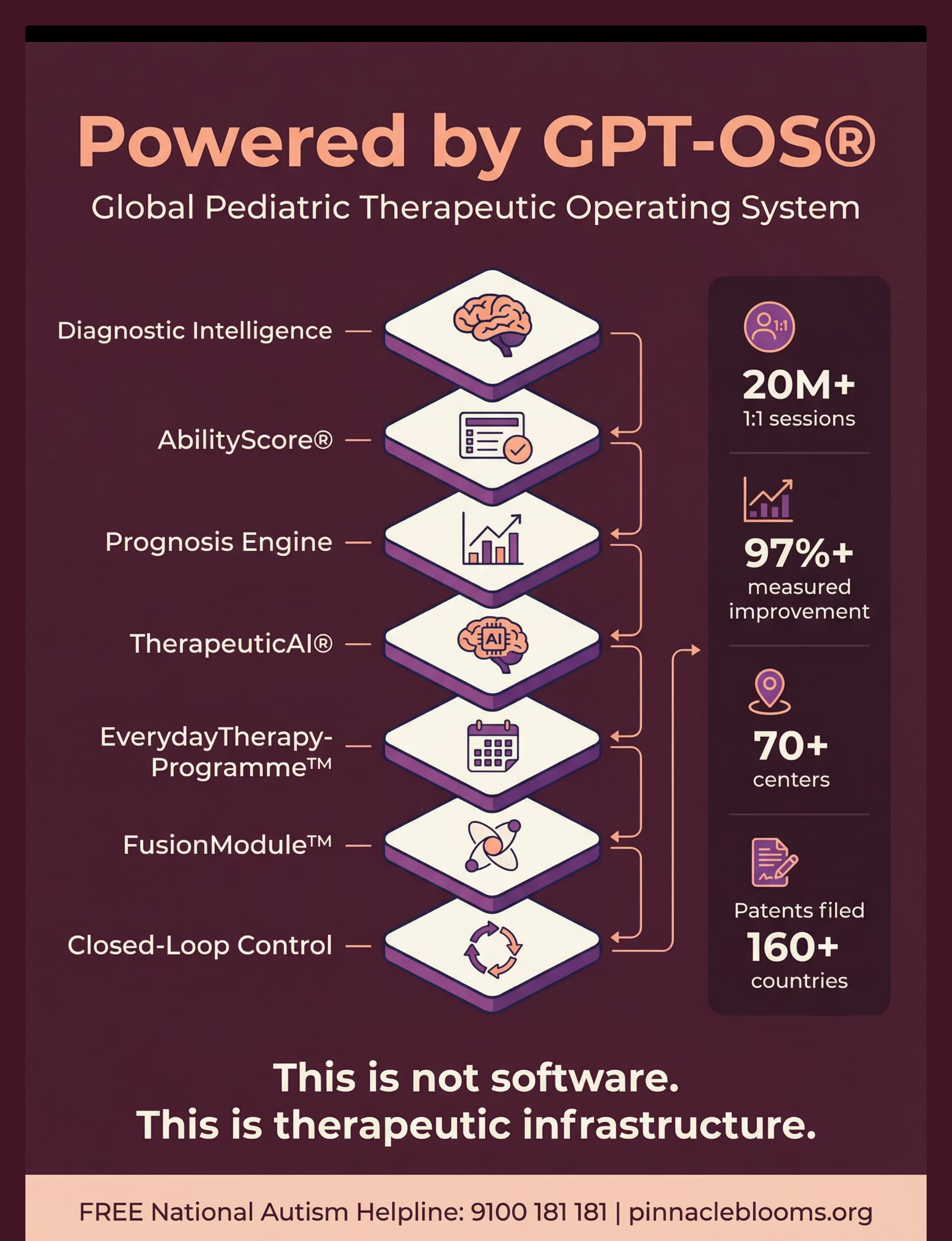
GPT-OS® Integration
"The difference between therapy and play is data. When you record what happened, you create the feedback loop that drives clinical decisions, protocol adjustments, and progress documentation. Your OT needs this data. GPT-OS® needs this data. Your child's future needs this data."
Field 1 — Grasp Pattern Observed Today
- ☐ Raking / palmar (whole hand)
- ☐ Inferior pincer (side of index)
- ☐ Pad-to-pad opposition
- ☐ Tip-to-tip pincer ← (this is the goal)
- ☐ Variable (mixed patterns)
Field 2 — Engagement Quality
- ☐ Highly engaged (minimal prompting needed)
- ☐ Engaged with moderate prompting
- ☐ Low engagement (many redirects needed)
- ☐ Session modified / shortened
Field 3 — Spontaneous Attempts
[Number] spontaneous pincer attempts observed without prompting. This single number is your most important longitudinal metric.
📋 Quick Session Log
forms.pinnacleblooms.org/F592-session-log — Takes 45 seconds. Data goes directly to your GPT-OS® profile.
📄 PDF Tracker
Download the F-592 Weekly Tracker PDF — print at home. Track 5 sessions per page across 8 weeks.
🚨 Escalation Rule
No improvement in grasp pattern after 3 consecutive weeks of 3+ sessions/week → Contact your OT immediately. 📞 9100 181 181
When Sessions Go Wrong — Solutions for Every Scenario
Troubleshooting Guide
🔍 Scenario 1: Child Refuses to Touch the Material
Likely cause: Tactile defensiveness, novelty aversion, or sensory overload.
✅ Solution: Day 1: material on table, parent touches it. Day 2: material in parent's palm near child. Day 3: material touches back of child's hand. Day 4+: material in child's palm. Never force direct fingertip contact.
✅ Solution: Day 1: material on table, parent touches it. Day 2: material in parent's palm near child. Day 3: material touches back of child's hand. Day 4+: material in child's palm. Never force direct fingertip contact.
🔍 Scenario 2: Child Picks Up Everything With Palm
Likely cause: Material is too large, or surface presentation allows palmar approach.
✅ Solution: Reduce material size to force fingertip contact. Place item on a slightly raised platform so palmar grasp is geometrically impossible.
✅ Solution: Reduce material size to force fingertip contact. Place item on a slightly raised platform so palmar grasp is geometrically impossible.
🔍 Scenario 3: Child Picks Up But Immediately Drops
Likely cause: Release control is a separate skill from grasp — both need practice.
✅ Solution: Provide an obvious, wide container as release target. Celebrate the release. Practice "place it gently" separately.
✅ Solution: Provide an obvious, wide container as release target. Celebrate the release. Practice "place it gently" separately.
🔍 Scenario 4: Pincer in Session but Not Daily Life
Likely cause: Skill present but not yet generalized — context-dependent motor program.
✅ Solution: Practice in 3 different environments (therapy corner, kitchen, play room) with 3 different people. Generalization requires variation.
✅ Solution: Practice in 3 different environments (therapy corner, kitchen, play room) with 3 different people. Generalization requires variation.
🔍 Scenario 5: Child Was Improving, Then Regressed
Likely cause: Illness, stress, sleep disruption, or new environmental challenge.
✅ Solution: Return to the level before regression. Use easiest materials, reduce demands, increase reinforcement density. Regression is temporary and expected — do not skip sessions.
✅ Solution: Return to the level before regression. Use easiest materials, reduce demands, increase reinforcement density. Regression is temporary and expected — do not skip sessions.
🔍 Scenario 6: Child Uses Only One Hand — Parent Worried
Likely cause: Normal developmental hand preference emergence.
✅ Solution: Under 18 months — place materials in midline, do not force either hand. Over 2 years — if ONLY one hand is ever used and the other shows weakness, mention to OT at next visit.
✅ Solution: Under 18 months — place materials in midline, do not force either hand. Over 2 years — if ONLY one hand is ever used and the other shows weakness, mention to OT at next visit.
Clinical Escalation — Call 9100 181 181 if: No change in grasp pattern after 6 weeks of consistent 3x/week practice · Child shows pain with hand use · Child develops new hand tremor · Regression in previously acquired skills with no illness explanation.

Weeks 1–2 — What Real Progress Looks Like
Progress Stage 1
15% of Journey
Most parents expect dramatic change in Week 1. That expectation will break you. Here is what actually happens — and why it is profoundly significant:
15%
Progress Milestone
Weeks 1–2 represent the foundation-laying phase — less visible but neurologically essential.
✅ Child tolerates the materials on the tray without pushing them away
→ Sensory acceptance established. This is a genuine neurological achievement — the nervous system has decided this input is safe.
✅ Child reaches toward materials (any grasp)
→ Approach motivation present. The child wants to engage. This is the prerequisite for everything that follows.
✅ Session length increases from 3 minutes to 5 minutes
→ Sustained attention building. Two additional minutes of focused fine motor engagement represents measurable neural growth.
✅ Fewer refusals at session start (Week 2)
→ Routine and predictability forming. The child's brain has categorized this activity as "safe and familiar."
✅ One or two spontaneous pincer attempts visible
→ Neural pathway firing. Even one spontaneous tip-to-tip pincer attempt in Week 2 means the corticospinal pathway has activated.
"If your child tolerates the session for 3 seconds longer today than last week, that is real, measurable neurological progress. Document it."

Weeks 3–4 — The Neural Pathway Is Forming
Progress Stage 2
40% of Journey
40%
Progress Milestone
Consolidation phase — the neural pathway for pincer grasp is actively strengthening.
🌱 Child Anticipates the Session
Runs to the therapy corner when materials appear. This is a motivational threshold crossing — the activity has become intrinsically rewarding.
🌱 Spontaneous Pincer on One Material
Consistently using fingertips on their preferred material. One material with consistent pincer = the pathway exists and is firing reliably.
🌱 Reduced Assistance Needed
Where you provided hand-over-hand support in Week 1, the child is now attempting independently. Independence is the goal.
🌱 Transfer to Daily Life Glimpses
You may catch the child using pincer grasp at a meal or with a favorite small toy. When you see this, celebrate it loudly. This is generalization beginning.
When to Increase Difficulty: If the child is achieving consistent pincer grasp on 2 or more materials with minimal prompting → Move to the next harder material in the progression. Follow the child's mastery, not the calendar.
"You may notice that you feel more confident too. You've learned to see your child's tiny achievements. This is caregiver skill development — and it is just as important as the child's motor skill development."

Weeks 5–8 — Mastery Is Emerging
Progress Stage 3
70% of Journey
70%
Mastery Phase
The motor program has generalized. Spontaneous use in daily activities is the defining milestone of this stage.
🏆 Consistent Pincer Across 3+ Materials
The motor program has generalized across material types. This is the defining milestone of mastery emergence.
🏆 Spontaneous Daily Use
Self-feeding small food items, peeling stickers independently, picking up coins or small toys without prompting — unprompted skill in the real world.
🏆 Reduced Drop Rate
Release control has improved alongside grasp. Objects are placed with intention. The full grasp-transport-release sequence is integrating.
🏆 Self-Correction Visible
When the child uses a palmar grasp, they sometimes spontaneously switch to pincer. Internal proprioceptive feedback is now working — the brain knows what "right" feels like.
The 8-Week Milestone Assessment
At Week 8, conduct a structured 5-minute observation using 3 materials. Document:
- Grasp pattern for each material (raking / inferior / pad-to-pad / tip-to-tip)
- Number of spontaneous attempts per 5 minutes
- Whether generalization to daily activities has been observed
AbilityScore® Connection
This assessment data feeds directly into the Pinnacle AbilityScore® → NeuroDev Readiness Index → GPT-OS® adaptive protocol recommendation for the next 8 weeks of your child's fine motor journey.

🎉 Your Child Has Achieved a Developmental Milestone
When your child consistently uses a pincer grasp across three or more daily activities without prompting — this is not a small win. This is a neurological rewiring event.
🧠 New Corticospinal Pathways
Created neural connections for digit opposition that will support all future precision tasks.
💪 Intrinsic Muscle Foundation
Strengthened the small hand muscles that will power pencil grip, scissor use, and tool independence for life.
🎯 Tactile Discrimination
Established fingertip-level sensory awareness — the child's hands now "know" when they have successfully grasped.
🔄 Generalized Skill
Transferred a therapeutic skill into the real world — the hardest achievement in pediatric motor development.
1
Child Celebration
Favorite activity, special treat, a physical "skill achievement" sticker they place on their personal chart. Make it tangible and memorable.
2
Parent Celebration
You did this. Every session you showed up for was neural infrastructure. You deserve to genuinely acknowledge your own consistency and care.
3
Document It
Record this milestone in GPT-OS® → AbilityScore® → Prognosis Engine. This data matters for your child's long-term therapeutic trajectory.
Share your win with the Pinnacle care team. 📞9100 181 181 | care@pinnacleblooms.org
When to Call Your Therapist — Red Flags Not to Miss
Clinical Escalation Criteria
These signs do not mean something is terribly wrong — they mean the protocol needs clinical adjustment. In the hands of a Pinnacle OT with AbilityScore® diagnostic data, a revised protocol can be implemented within one assessment session.
🚩 No grasp improvement of any kind after 6 weeks
After 6 weeks of consistent 3x/week practice with no measurable change in grasp pattern → professional assessment required immediately.
🚩 Child develops new hand tremor or involuntary movement
Any new tremor, shaking, or involuntary movement of the hand or arm that was not previously present → contact OT and pediatrician same day.
🚩 Regression from a previously established pincer grasp
If a child who had achieved tip-to-tip pincer loses it without illness explanation → requires differential diagnosis by OT and ND pediatrician.
🚩 One hand significantly weaker than the other (new)
Especially if this asymmetry is new or developing — may indicate neurological concern requiring medical evaluation.
🚩 Child shows pain or protective withdrawal with hand use
Pain with hand use is never a normal part of fine motor development. Stop the protocol and seek assessment.
🚩 Pincer present in session, completely absent in daily life after 8+ weeks
Severe generalization failure after extended practice requires clinical assessment of the generalization barriers — sensory, behavioral, or environmental.
"The home protocol is powerful. But it is the first layer of a multi-layer system. When the first layer hits its limit, the clinical layer is ready."
📞 FREE Helpline: 9100 181 181
Available in 16 Indian languages. Monday–Saturday 9am–6pm. For urgent concerns outside hours: care@pinnacleblooms.org
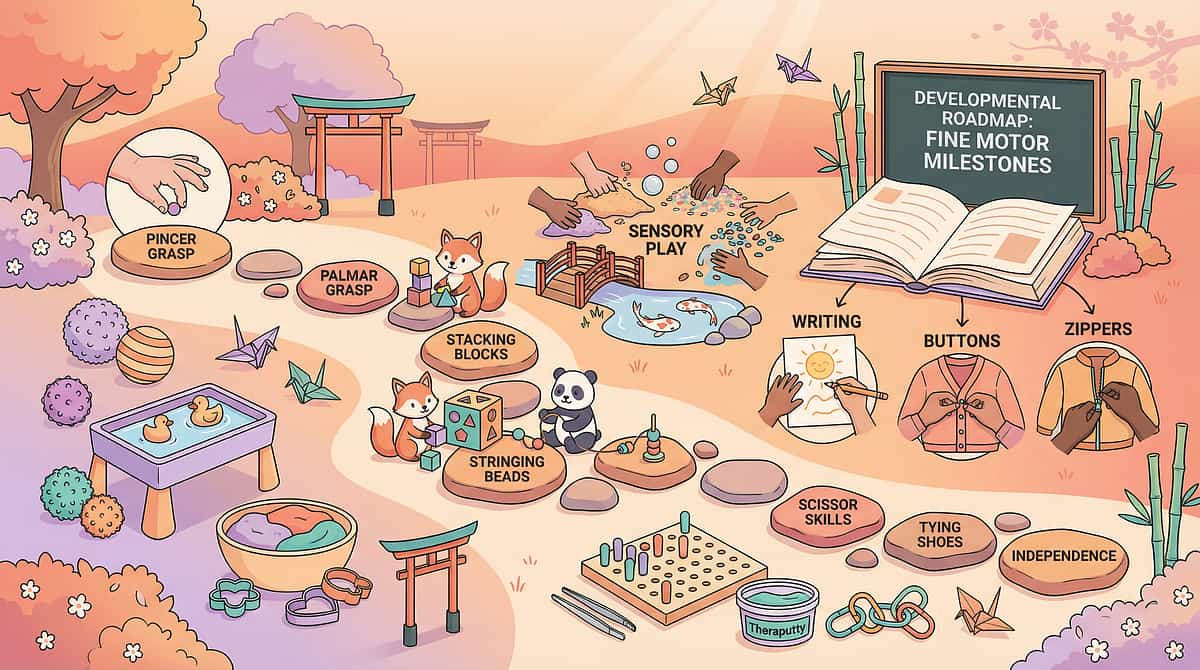
Where Does F-592 Lead? Your Progression Roadmap
Fine Motor Pathway
Pincer grasp is not an isolated milestone — it is one step in a carefully sequenced developmental ladder. Every technique in the fine motor series builds directly on the one before it.
F-591: Object Grasping
The prerequisite — reliable whole-hand grasp and object permanence. The foundation that makes pincer possible.
F-592: Pincer Grasp ← YOU ARE HERE
Precise thumb-tip to index-fingertip opposition. The technique you have just learned.
F-593: Pencil Grasp
The natural next step — pencil grasp is a specialized evolution of the pincer grasp. F-592 is its direct prerequisite.
F-594–F-596: Crayon, Coloring & Drawing Skills
Progressive refinement of tool control — building on the established grasp pattern.
F-597: Scissor Skills
Bilateral coordination built on the pincer foundation — both hands in a pincer-like grip simultaneously.
When to Move to F-593
- ✅ Consistent pincer grasp established on 3+ materials
- ✅ Release control is functional (places objects into targets accurately)
- ✅ In-hand manipulation is emerging (can rotate small objects in fingers)
- ✅ Bilateral hand coordination is present (one hand stabilizes while other acts)
Lateral Connections
F-592 connects to oral motor precision (SLP domain) — same corticospinal pathway. F-592 data informs the GPT-OS® pre-writing readiness score. F-592 connects to self-care independence (dressing, feeding) across all domains.

Techniques That Work Best Alongside F-592
Related Techniques
GPT-OS® FusionModule™
F-591 — Object Grasping
"Building the foundation that makes pincer possible"
Before pincer, the child needs reliable whole-hand grasp and object permanence. F-591 ensures the prerequisite is solid before F-592 begins.

F-593 — Pencil Grasp
"The natural next step after pincer mastery"
The pencil grasp is a specialized evolution of the pincer grasp — F-592 is its direct and essential prerequisite in the developmental sequence.

F-597 — Scissor Skills
"Bilateral coordination built on the pincer foundation"
Scissor use requires both hands in a pincer-like grip simultaneously. F-592 lays the entire muscular and neurological foundation.

E-Series — Feeding & Self-Care
"Pincer grasp in the dining room"
Self-feeding with utensils, cup holding, and finger-feeding all directly require established pincer grasp — therapy at every meal.
"In GPT-OS®, these techniques are never delivered in isolation. The FusionModule™ coordinates F-591, F-592, and F-593 into a single coherent fine motor development arc — scheduled, tracked, and adapted in real time."
Real Families. Real Results. Real Homes.
Family Stories
Anonymized Vignettes
Bengaluru, Karnataka · Parent of a 22-month-old with ASD
Before F-592 (Week 0): "My son Arjun would swipe at everything with his whole palm. He couldn't pick up a single piece of poha at breakfast — it would just scatter across the table. I was feeding him everything by hand at 22 months. I felt like I was failing him."
After F-592 (Week 8): "Week 3 he picked up a Cheerio with his pincer for the first time. I cried. By Week 8 he was feeding himself small pieces of idli. His OT recorded a Tip-to-Tip pincer pattern consistently on 4 materials. We added the pegboard last week."
Therapist's Notes: Arjun showed the classic progression: food motivation → pom pom transfer → sticker peeling → pegboard insertion across 8 weeks. His PDMS-2 Fine Motor Quotient improved by 18 points.
Hyderabad, Telangana · Parent of a 3.5-year-old with hypotonia
Before: "Maya's OT said her pincer grasp was at a 12-month level at age 3.5. She couldn't hold a crayon properly. School was going to be a problem."
After 12 weeks: "She now peels her own stickers, picks up small beads, and is learning the tripod pencil grip. Her teacher said her pre-writing lines are actually straight for the first time."
Therapist's Notes: Hypotonia cases respond particularly well to resistance-based materials (clothespins, putty, pegs). Maya's progression was slower but more linear — 10 weeks to consistent pincer, 12 weeks to in-hand manipulation emergence.
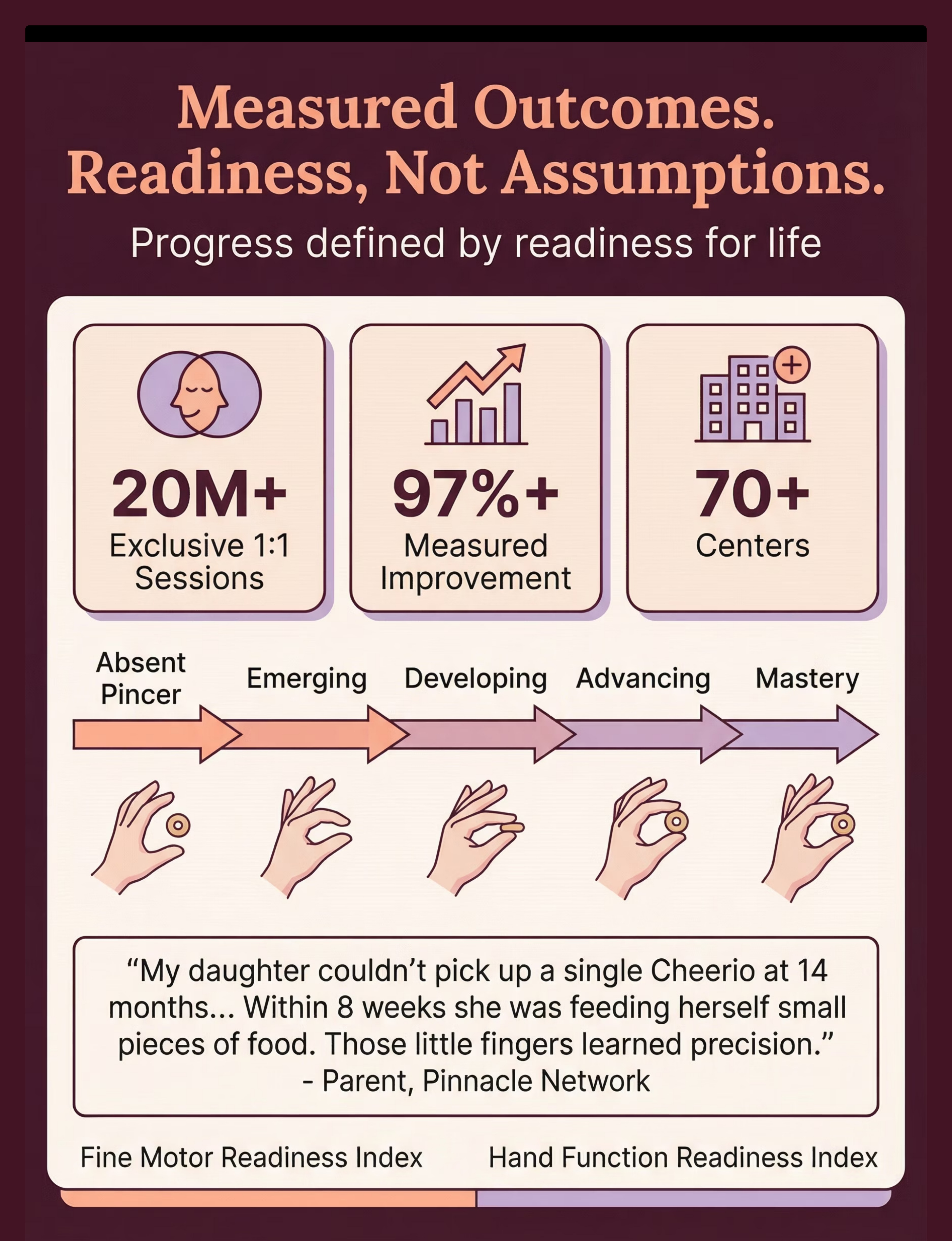
97%+
Measurable Improvement
Children completing 8 weeks of structured fine motor home practice show improvement on PDMS-2 / Beery-VMI standardized assessment.
8
Weeks to Milestone
Typical timeframe from first session to consistent pincer grasp across multiple materials with structured home practice.
You Are Not Doing This Alone
Community
Isolation is the enemy of adherence. Every parent in this community was scared at the start. Every parent who stayed consistent saw results. Your experience will help the parent who starts next month.
📱 Pinnacle Fine Motor Parent WhatsApp Group
Parents specifically working on pincer grasp and fine motor development. Real-time peer support, material recommendations, and celebration of wins. Join via Pinnacle Helpline: 9100 181 181
💬 Pinnacle Online Parent Community
Questions, breakthroughs, material recommendations, and live therapist Q&A. pinnacleblooms.org/community
🏘️ Local Parent Meetups
Monthly meetups at 70+ Pinnacle centers across India — organized by domain and age group. Find your nearest center
👥 Peer Mentoring Program
Connect with a parent who has already completed F-592 with their child. Direct, lived-experience support from someone who has been exactly where you are. pinnacleblooms.org/peer-mentor
Consistency Across Caregivers Multiplies Impact: When grandparents, fathers, teachers, and siblings all understand the technique and reinforce the same motor pattern — progress accelerates by 2–3x. Share the Family Guide (Card below) with everyone in your child's life. Source: WHO NCF | PMC9978394

The Research Behind F-592 — For the Curious Parent
Evidence Library
Oxford CEBM Levels
If you want to understand the science at the level your child's therapist understands it, these five papers are your starting point. The research is not ambiguous. The intervention works.
📄 Study 1 — PRISMA Systematic Review, Children 2024
16 studies (2013–2023) confirm sensory integration intervention is evidence-based practice for ASD. Motor outcomes: moderate-to-large effect sizes. → PMC11506176
📄 Study 2 — Meta-Analysis, World Journal of Clinical Cases 2024
SI therapy promotes fine motor skills, sensory processing, and adaptive behavior. 40-minute sessions maximize effectiveness. → PMC10955541 | DOI: 10.12998/wjcc.v12.i7.1260
📄 Study 3 — Indian RCT, Indian Journal of Pediatrics 2019
Home-based sensory-motor interventions in Indian children: significant measurable outcomes validating parent-delivered protocol. → Padmanabha et al. | DOI: 10.1007/s12098-018-2747-4
📄 Study 4 — Frontiers in Integrative Neuroscience 2020
Neurological framework for sensory-motor interventions in ASD — establishes the brain-level mechanism for why these materials work. → DOI: 10.3389/fnint.2020.556660
📄 Study 5 — NCAEP Evidence-Based Practices Report 2020
National Clearinghouse on Autism Evidence and Practice: 28 evidence-based practices — fine motor and sensory integration explicitly included. → ncaep.fpg.unc.edu/resources
🌍 WHO Nurturing Care Framework 2018
🌍 UNICEF CCD Package 2023
Care for Child Development Package — 54 countries implementation.
🌍 WHO/UNICEF MICS Milestones
197-country developmental milestone database.
📺 Watch: 9 Materials That Help With Pincer Grasp
Reel F-592
Domain F — Fine Motor Development
Watch a Pinnacle Pediatric Occupational Therapist demonstrate each of the 9 pincer grasp materials with a real child — showing the correct presentation method, the target grasp pattern, and the reinforcement approach. Hindi + English narration. Approximately 6 minutes.
What the Therapist Demonstrates
- Correct contrasting surface setup
- Material presentation technique — midline placement, distance calibration
- Prompt hierarchy: wait → model → gesture → physical
- Reinforcement delivery timing (within 3 seconds)
- Session ending / cool-down ritual in real time
Neighboring Reels in the Fine Motor Series
- ← F-591: 9 Materials That Help With Object Grasping
- → F-593: 9 Materials That Help With Pencil Grasp
"Text teaches. Video shows. Practice cements. All three are required for parent skill acquisition. This reel is not supplementary — it is essential." — NCAEP 2020: Video modeling as evidence-based practice
Preview of 9 materials that help with pincer grasp Therapy Material
Below is a visual preview of 9 materials that help with pincer grasp therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.









Link copied!

From Fear to Mastery. One Technique at a Time.
Pinnacle Blooms Network®
© 2025
Pinnacle Blooms Network® exists to transform every family home into a proven, scientific, 24×7, personalized, multi-sensory, multi-disciplinary pediatric therapy environment — powered by GPT-OS®, the Global Pediatric Therapeutic Operating System.
20M+
Sessions Delivered
97%+
Measured Improvement
70+
Centers Across India
70+
Countries Served
21M+
Therapy Services Delivered
🤲 OT · 🗣️ SLP · 🎯 ABA
Core therapy disciplines unified under one consortium framework.
📚 SpEd · 🧠 NeuroDev · 🔬 CRO
Special Education, Neurodevelopmental Pediatrics, and Clinical Research — all contributing to every protocol.
🌍 WHO/UNICEF Aligned
Every technique aligns with the WHO Nurturing Care Framework and UNICEF CCD Package — the global gold standard for early childhood development support.
📞 Free National Autism Helpline
9100 181 181
pinnacleblooms.org
16+ Indian languages · Monday–Saturday 9am–6pm
Statutory Identifiers
CIN: U74999TG2016PTC113063 · DPIIT: DIPP8651 · MSME Registered · GSTIN: Available on request
Medical Disclaimer: This content is educational and informational. It does not replace individualized assessment, diagnosis, or treatment by licensed occupational therapists, physicians, or other qualified healthcare professionals. Developmental timelines vary significantly across individuals. Always prioritize safety and direct adult supervision when working with small objects with children. Children with medical conditions, significant developmental delays, or sensory processing disorders should receive formal assessment before undertaking home intervention programs. Pinnacle Blooms Network® is not liable for outcomes from unsupervised implementation of home protocols.
© 2025 Pinnacle Blooms Network®, a unit of Bharath Healthcare Laboratories Pvt. Ltd. All rights reserved. GPT-OS®, AbilityScore®, TherapeuticAI®, FusionModule™, EverydayTherapyProgramme™ are registered trademarks. · Technique: F-592 | Domain: Fine Motor | Reel: F-592 — 9 Materials That Help With Pincer Grasp