
"Talking TO them. Not WITH them."
Every conversation is a monologue. She's eager to connect — but doesn't yet understand that connection requires curiosity about others. This is a skill gap — and it can be built.

ACT I — Recognition
You Are Not Alone: The Numbers
When a child's conversations are consistently one-sided — when they talk at people rather than with them — peers disengage, friendships fail to form, and the child is left confused about why. This isn't rare. And it isn't permanent.
80%
Social Communication Differences
of children with autism experience reduced conversational reciprocity
1in36
Children in the US
are diagnosed with ASD — social reciprocity challenges affect families worldwide
20M+
Therapy Sessions
across Pinnacle's network have addressed social communication and pragmatic language challenges
Sources: PMC11506176 (PRISMA Systematic Review, 2024) | PMC10955541 (Meta-analysis, World J Clin Cases, 2024) | WHO Nurturing Care Framework 2018 | 📞 FREE Helpline: 9100 181 181

ACT I — Recognition
The Recognition Moment
"My daughter can talk for twenty minutes straight about her favourite video game — every character, every level, every detail — without once pausing to check if the other person is interested, or asking them a single question. At school, her teacher says she dominates group conversations. Kids don't want to sit with her at lunch because they know they won't get a word in. She genuinely wants friends. She just doesn't understand that connection requires curiosity about others — not just sharing about yourself."
You are not failing. Your child is not selfish. This is a skill gap — and it can be built.
📞 FREE National Autism Helpline: 9100 181 181 | Available 24×7 in 16+ languages
ACT I — Recognition
What's Happening in Your Child's Brain
This is a perspective-taking difference — not a character flaw.
What's Actually Happening
The child's brain doesn't spontaneously generate the question: "What does the other person want to talk about?" Their own interests feel so salient that others' minds become less visible. This isn't selfishness in any moral sense — it's a pattern in how social attention is directed.
The prefrontal cortex's Theory of Mind network — the social cognition pathway — shows a pattern where the salience of one's own interests eclipses awareness of others' inner worlds.
What This Means for Intervention
Conversational reciprocity — the back-and-forth of true dialogue — isn't automatic for this child. It needs to be made explicit, visual, and practiced deliberately.
The neural pathways can be strengthened through structured intervention. This is not a permanent wiring — it is a trainable skill.
"This is a wiring pattern — not a choice." — Frontiers Integrative Neuroscience 2020 | DOI: 10.3389/fnint.2020.556660

ACT I — Recognition
Where This Sits in Development
Your child is here. Here is where we're heading. Understanding the developmental timeline helps parents know that intervention now is both timely and effective.
1
Ages 2–3
Parallel play; simple turn-taking emerges in basic exchange
2
Ages 3–5
One-sided conversation is typical; reciprocity actively developing
3
Ages 5–7
Expected shift: child asks questions, sustains partner's topics
4
Ages 7–10 ← B-216
Reciprocal exchange expected; persistent one-sidedness now signals a gap. Optimal intervention window.
5
Ages 10–14
Friendship-sustaining conversation; mutual interest; social reciprocity consolidated
📍 Often co-occurs with: Perspective-taking differences (B-215) | Difficulty reading listener cues (B-214) | Interrupting (B-210) | Pragmatic language challenges | WHO Care for Child Development Package | PMC9978394

ACT I — Evidence
The Evidence Behind This Technique
⭐ LEVEL I EVIDENCE — Systematic Review + Multiple RCTs. Every material in this protocol is grounded in peer-reviewed science and validated clinical practice guidelines.
Source | Finding | |
PRISMA Systematic Review (Children, 2024) — PMC11506176 | Social communication interventions meet evidence-based practice criteria for ASD across 16 studies (2013–2023) | |
Meta-analysis, 24 studies (World J Clin Cases, 2024) — PMC10955541 | Social skills, conversational reciprocity, and adaptive behaviour improved through structured intervention | |
NCAEP Evidence-Based Practices (2020) | Social Stories™, Video Modeling, and Visual Supports classified as evidence-based for autism | |
ASHA Clinical Guidelines | Pragmatic language intervention including reciprocity training is established SLP practice | |
Padmanabha et al., Indian J Pediatr (2019) | Home-based parent-administered intervention shows significant outcomes. DOI: 10.1007/s12098-018-2747-4 |
"Clinically validated. Home-applicable. Parent-proven."
📞 FREE Helpline: 9100 181 181 | PubMed: PMC11506176 | PMC10955541 | PMC9978394 | NCAEP 2020 | WHO NCF 2018
ACT II — Knowledge Transfer
The Technique: What It Is
Technique Identity
Formal Name: Conversational Reciprocity Intervention — Material-Supported Protocol
Parent-Friendly Alias: "Building Two-Way Conversations"
Reel ID: B-216 | Social Communication & Pragmatic Language Series — Episode 216
Definition
Conversational Reciprocity Intervention uses structured materials — visual trackers, question prompts, reciprocity games, social narratives, and cue systems — to build the back-and-forth exchange that characterises genuine dialogue.
One-sided conversation patterns reflect challenges in perspective-taking, social curiosity, and pragmatic language learning. This protocol makes the invisible rules of conversation explicit, provides tools for generating questions, and creates structured practice for mutual exchange. Delivered at home, in therapy, and at school.
🧠 Domain
Social Communication & Pragmatic Language
👶 Ages
5–14 years
⏱️ Duration
10–15 min/session | 3–5×/week
📅 Programme
8–12 weeks for consolidation
🏥 Setting
Home + Therapy + School

ACT II — Knowledge Transfer
Who Uses This Technique
"This technique crosses therapy boundaries — because the brain doesn't organise by therapy type."
🗣️ SLP — Lead Discipline
Pragmatic language assessment, reciprocity intervention, Social Stories™, question generation training, conversational analysis
🖐️ OT
Supports self-monitoring, attention regulation during conversation, visual supports implementation
🎯 BCBA / ABA
Reinforcement of question-asking behaviour, data collection on reciprocal exchanges, token economy for asking
📚 SpEd
Explicit instruction in conversational rules, peer interaction support, classroom accommodation
"A child's difficulty with conversational reciprocity is simultaneously a language challenge, a social cognition challenge, a self-monitoring challenge, and a learning challenge. Effective intervention addresses all layers." | Source: UNICEF/WHO Nurturing Care Framework for SLPs (2022)

ACT II — Knowledge Transfer
What This Technique Targets
Precision targets. Not random activities. Every material and every session step is mapped to a specific developmental outcome.
Observable behaviour indicators confirm progress: child asks at least one question per conversation ✅ | child responds to partner's topic before redirecting ✅ | child notices listener disengagement ✅ | child retains information others share across sessions

ACT II — The 9 Materials
What You Need: The 9 Canon Materials
Nine materials. One goal: from monologue to dialogue. Each material addresses a different layer of conversational reciprocity. You don't need all nine — start with what resonates.
🌟Pinnacle Recommends: Start with Materials 1 + 2 + 5. These three alone create the foundation for change.
1
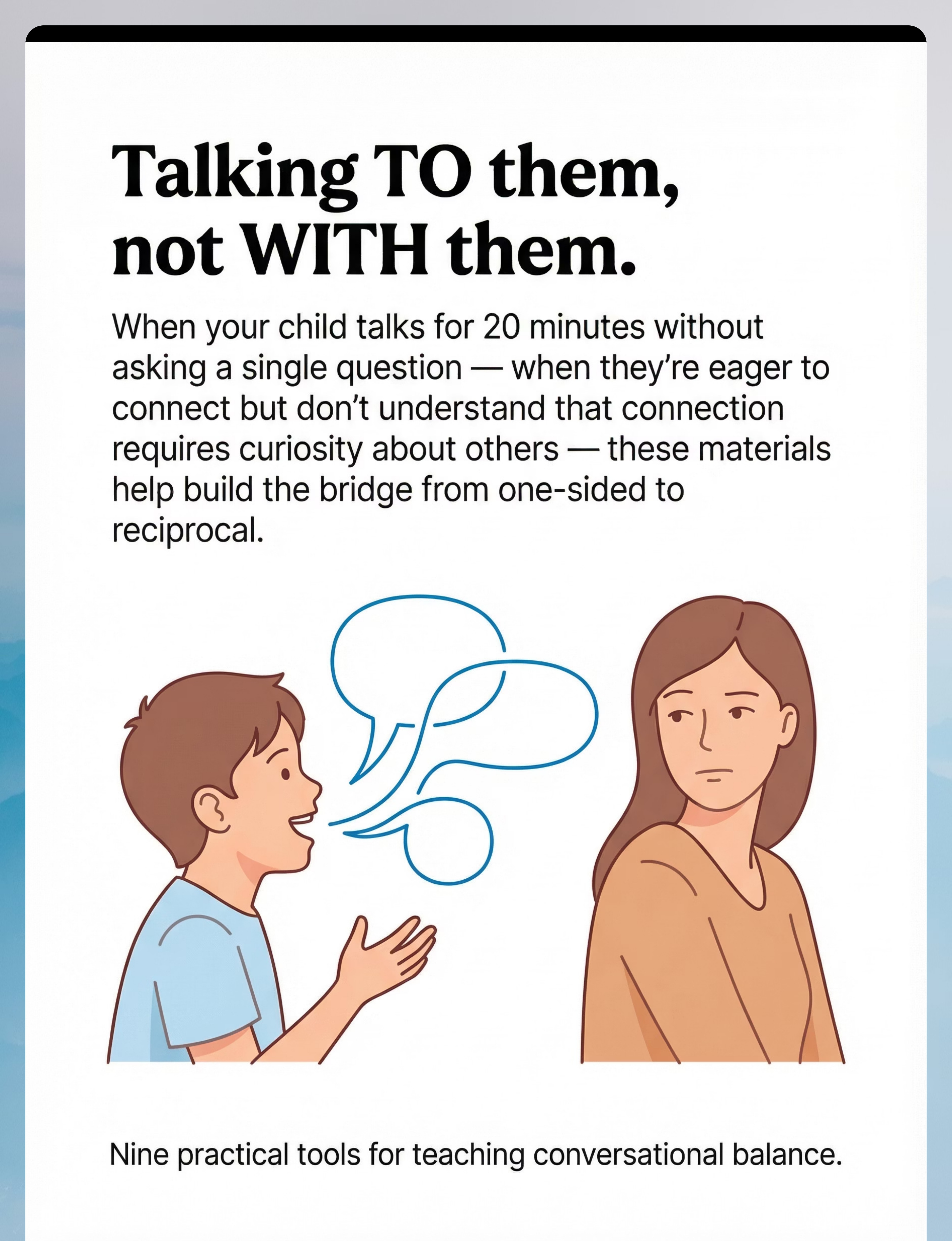
🔰 Conversation Balance Scales & Visual Trackers
Makes reciprocity visible — shows imbalance literally | ₹0–1,000
2
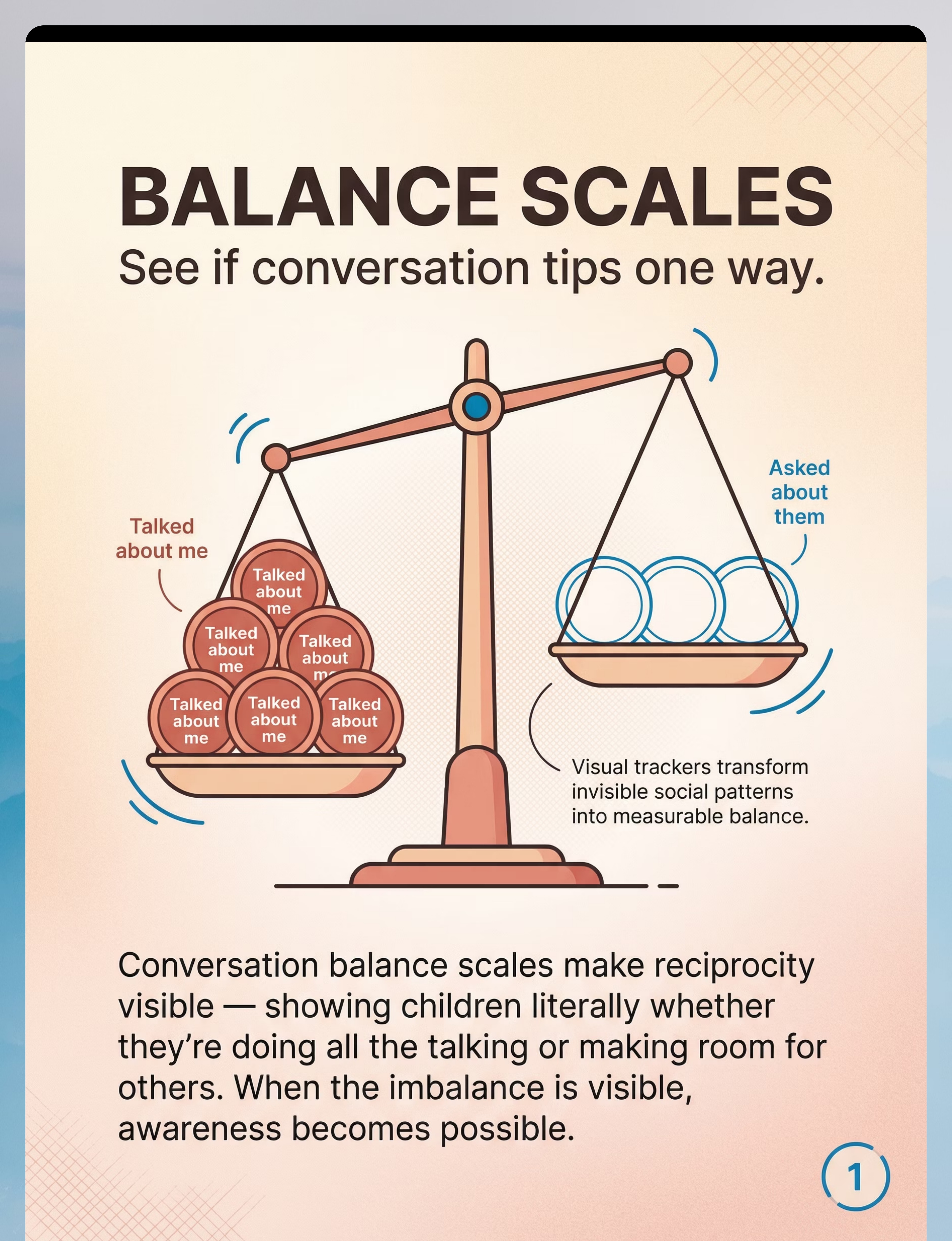
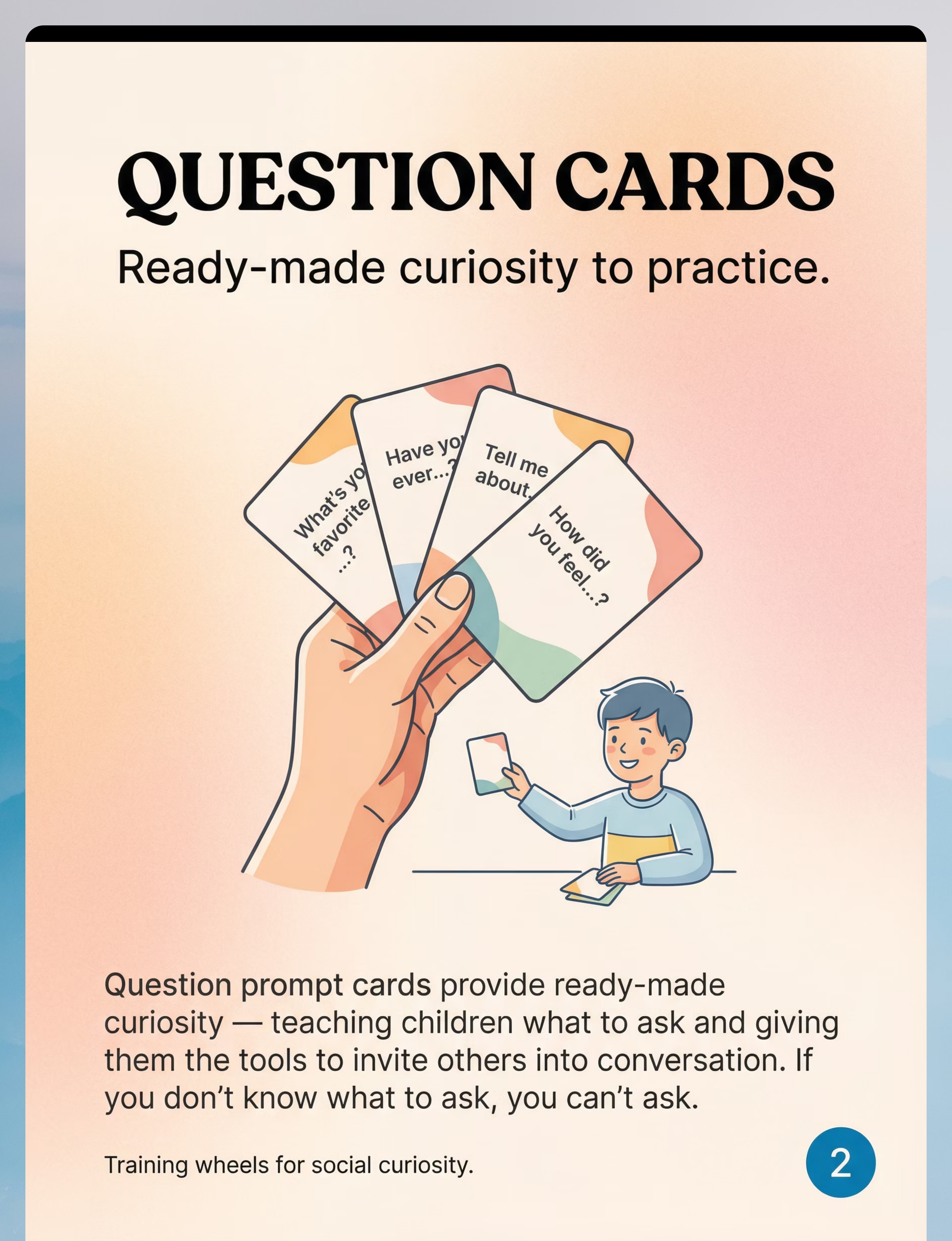
📋 Question Prompt Cards & Starters
Provides ready-made questions — removes the "I don't know what to ask" barrier | ₹100–600
3
🎮 Conversation Reciprocity Games
Builds back-and-forth as a game rule — practice without feeling corrected | ₹300–1,500
4
🗂️ Interest Inventory Cards
Turns learning about others into a mission — builds social curiosity | ₹100–500
5
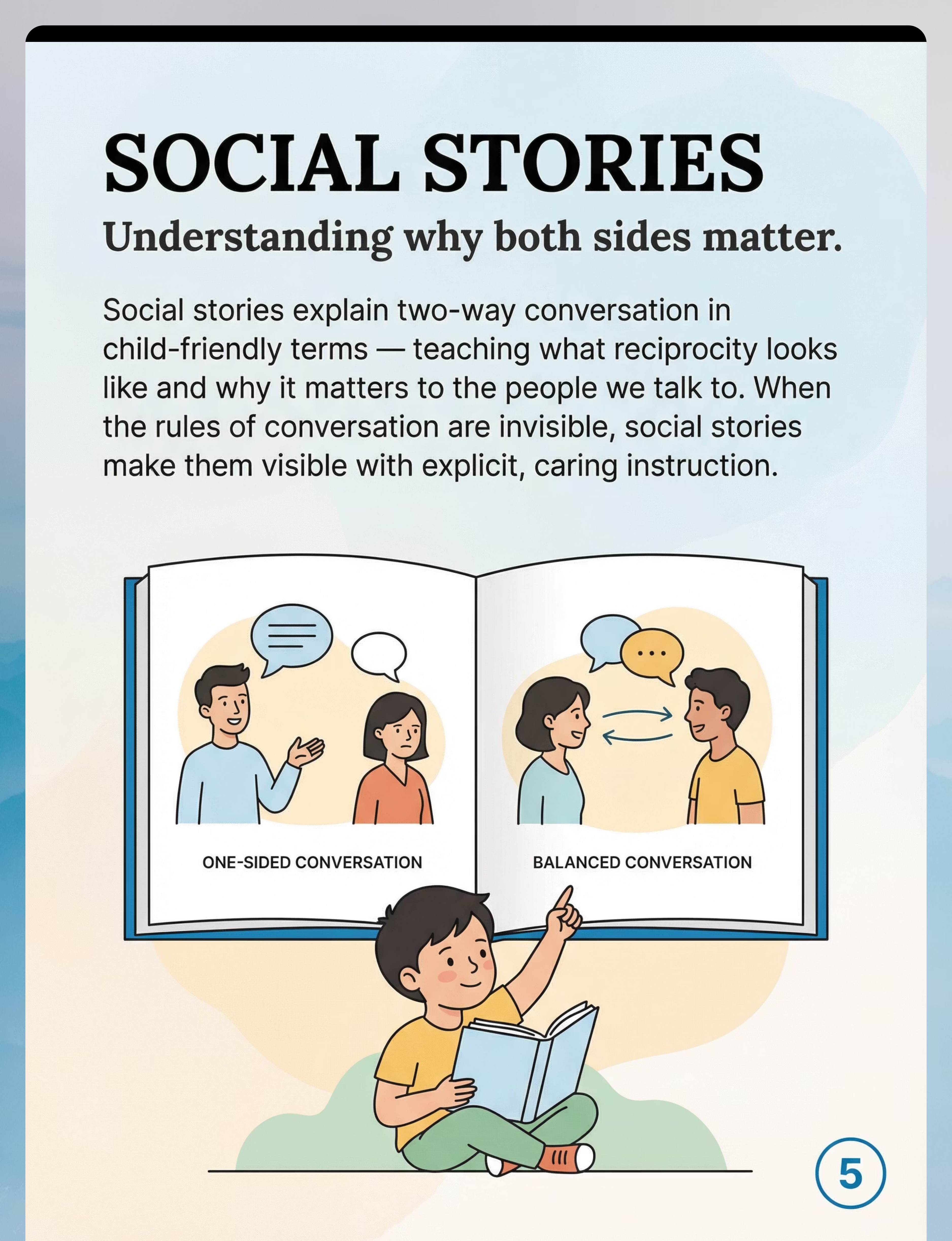
📖 Social Stories™ About Two-Way Conversations
Explains WHY reciprocity matters in child-friendly narrative | ₹200–1,000
6
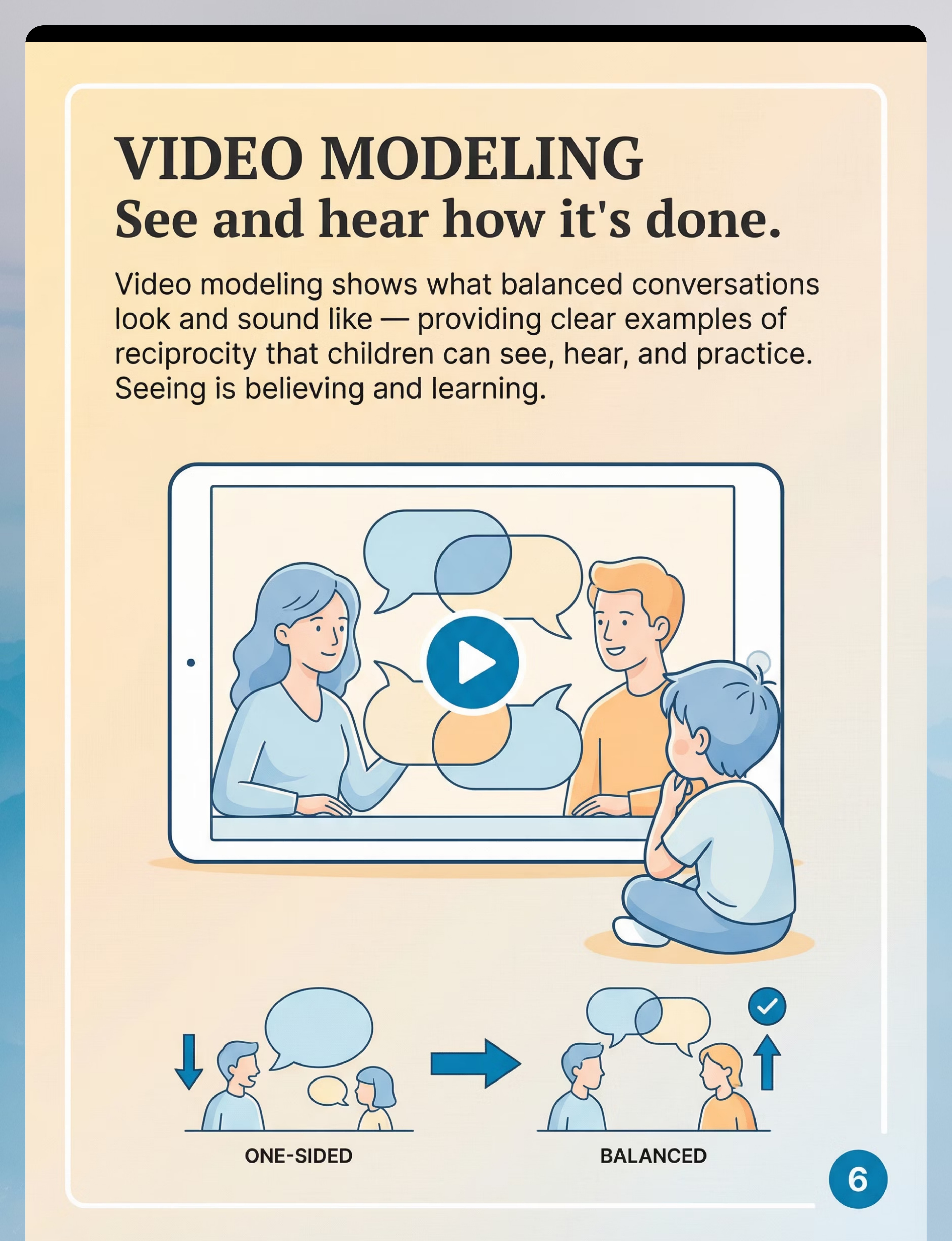
📹 Video Modeling of Balanced Conversations
Shows AND sounds like — a visual template for reciprocity | ₹0–1,000
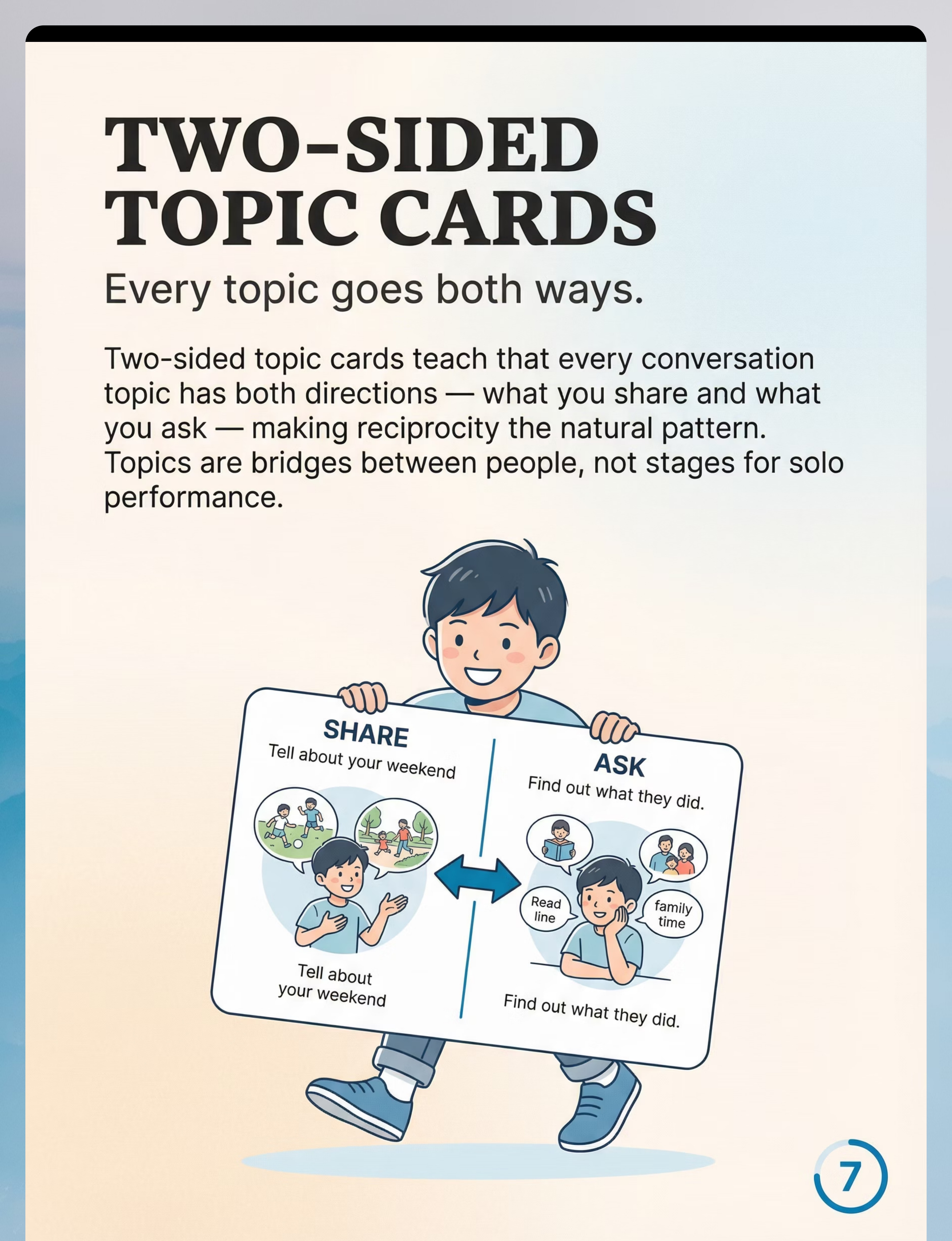
7
🃏 Two-Sided Topic Cards
Every topic has a SHARE side AND an ASK side — reciprocity built in | ₹100–500
8
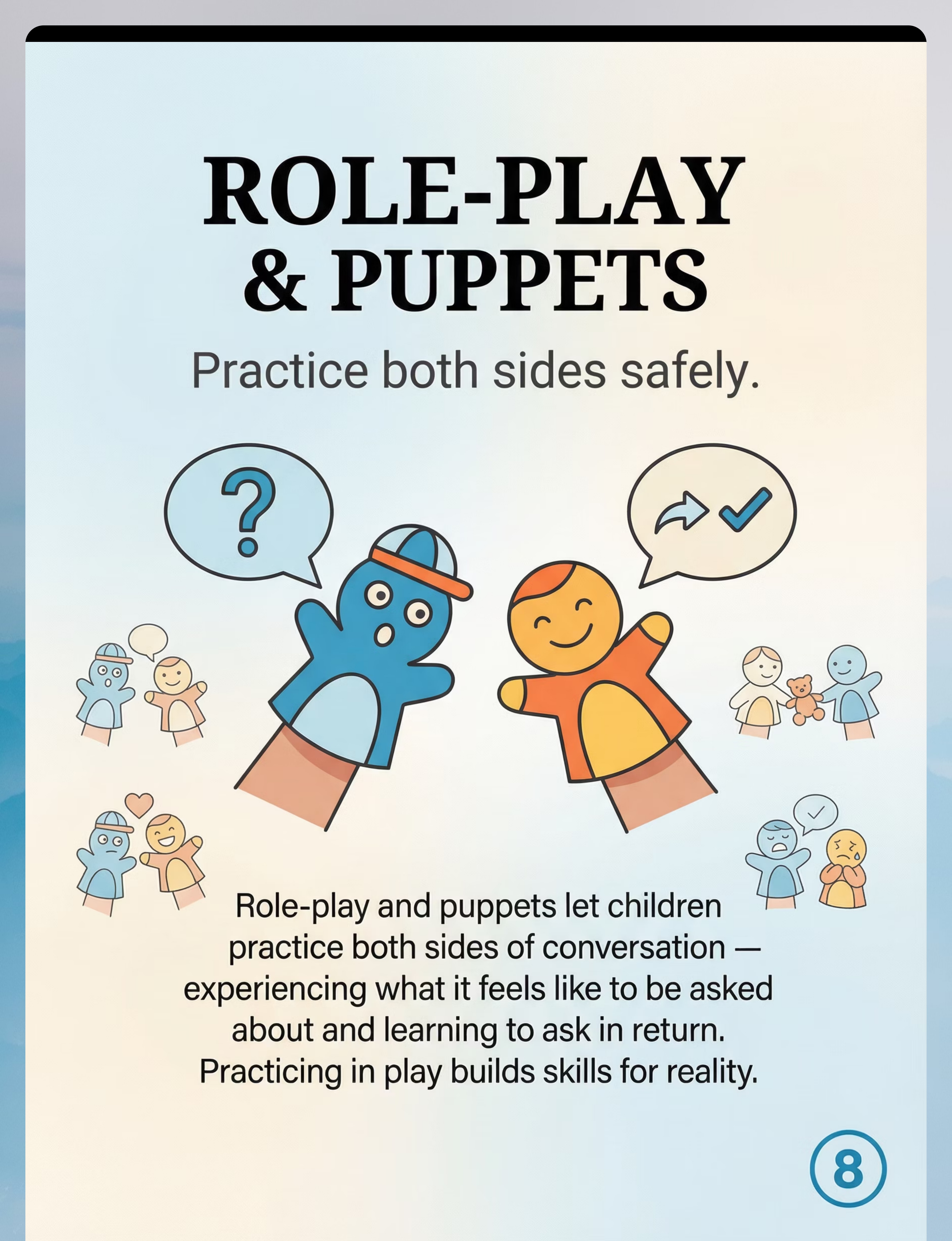
🤹 Role-Play Scenarios & Puppets
Safe practice for both sides of conversation | ₹300–1,500
9
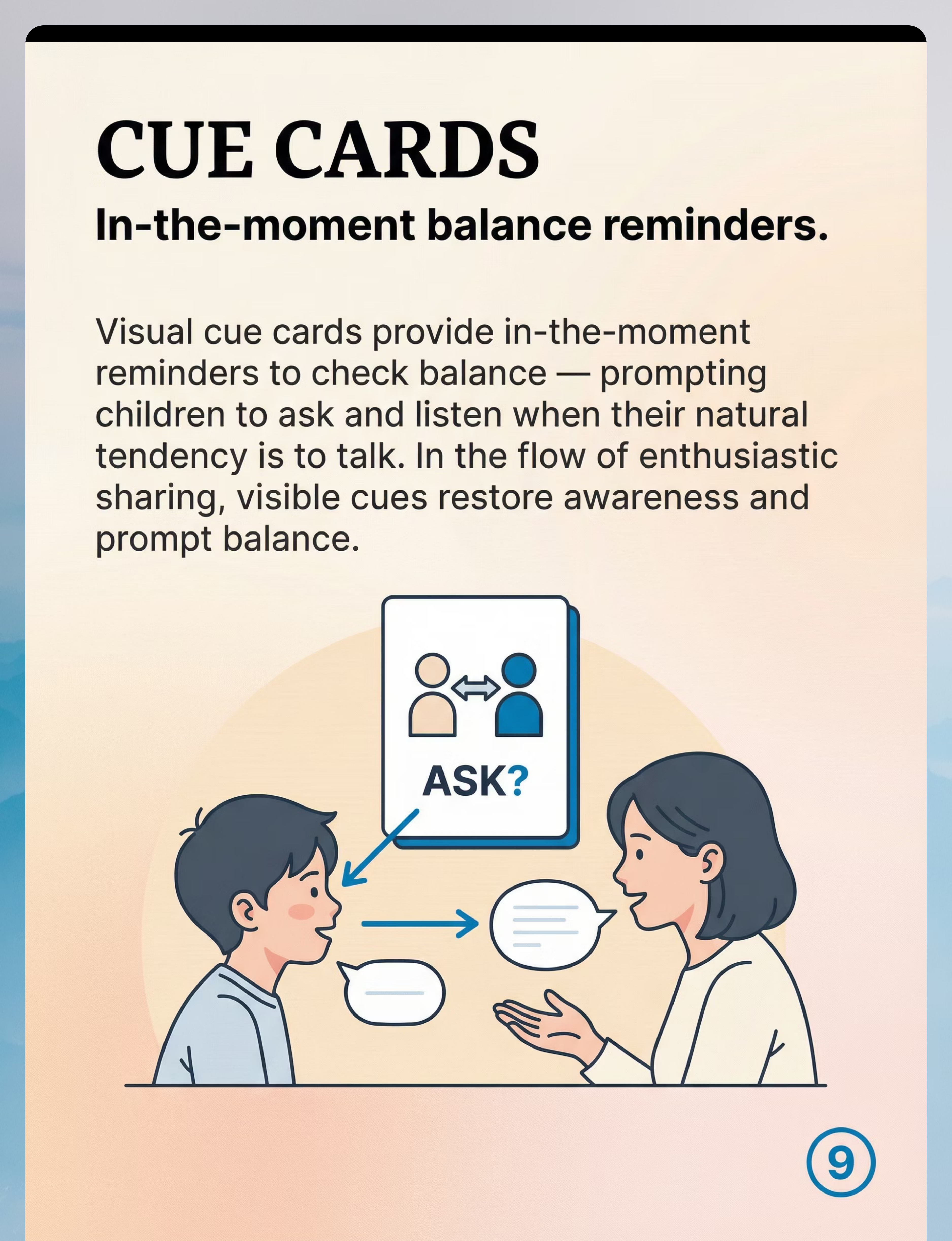
👁️ Visual Cue Cards for Conversation Monitoring
In-the-moment reminder to check balance | ₹50–300

ACT II — Knowledge Transfer
DIY & Substitute Options
Every material has a zero-cost version. Start today. Effective therapy cannot be gated by purchasing power — WHO Nurturing Care Framework, Equity Principle.
Commercial Version | Zero-Cost DIY Alternative | |
Physical balance scale + tokens (₹500–1,000) | Paper T-chart: "Me" vs "Them" columns with tally marks or a two-colour visual thermometer | |
Question prompt card deck (₹300–600) | Index cards with starters: "What's your favourite...?", "Have you ever...?", "Tell me about..." Ring-bind 20 cards. ₹50 total. | |
Conversation reciprocity board game (₹800–1,500) | Modify any existing game: "Before your turn, ask a question." The rule is the material. | |
Interest inventory workbook (₹300–500) | "All About [Name]" sheet: Favourite food, what makes them happy, something they're good at. Repeat for 5 people in their life. | |
Published Social Story book (₹400–800) | Write a personalised social story using Carol Gray's framework (free online). 4–6 pages with photos. | |
Video modeling library (₹0–1,000 for app) | Record a 3-minute home video — one-sided conversation, then a balanced one. Watch together. Free. | |
Two-sided topic cards (₹200–400) | Index cards, each with "Tell about your ___" and "Ask about their ___" on the same card. | |
Puppet set (₹400–800) | Any stuffed animals, dolls, or action figures. The character holds the practice, not the specific toy. | |
Visual cue card set (₹150–300) | One laminated card: a question mark + two arrows going both ways. Stick to conversation areas. |
Source: PMC9978394 | WHO/UNICEF CCD Package — household-material intervention evidence

ACT II — Safety
Safety First: Before You Begin
Read before starting. Clinical safety, in plain language. The traffic-light system below helps you decide when and how to proceed at every session.
🟢 GREEN — Proceed
Child is calm, regulated, and not hungry or overtired | No recent significant social distress in last 2 hours | Parent has read this full protocol | Space is set up per setup card
🟡 AMBER — Modify First
Child mildly dysregulated → use abbreviated 5-minute version | Difficult social day → use puppets only | Child shows resistance → games only, no balance scale today
🔴 RED — Do Not Proceed Today
Child in active emotional distress or meltdown recovery | Child just experienced peer rejection and is emotionally raw | Any illness, high fever, or significant sleep deprivation
⚠️Critical framing rule: NEVER frame the balance scale as evidence of failure. Always: "Let's see what our conversation looks like." Never: "Look how you dominated." | STOP IMMEDIATELY if you observe shame response, shutdown, or escalating distress. | SLP Note: Evaluation by a licensed speech-language pathologist is recommended if patterns are persistent. | 📞 FREE 24×7: 9100 181 181
ACT II — Setup
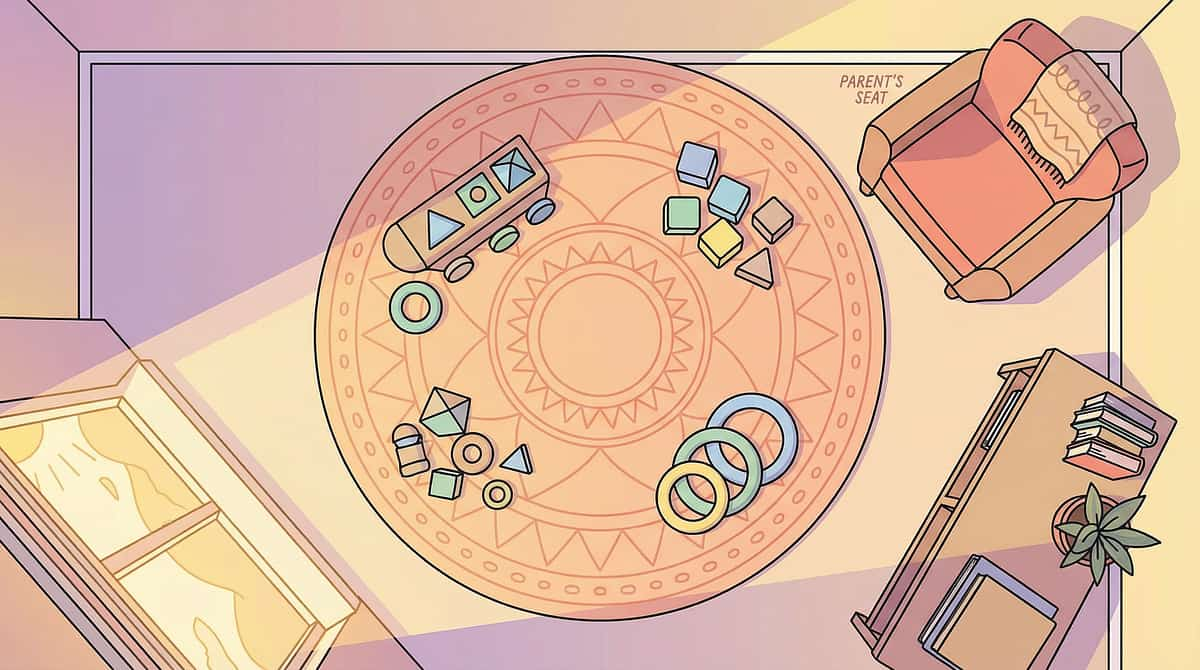
Set Up Your Space
"Spatial precision prevents 80% of session failures." Set up your space before the child enters — delays in setup signal that "a lesson is coming" and prime resistance.
Room Layout
📋 Materials tray — left of child | 👁️ Cue card — at child's eye level | 👶 Child and 👨 Parent — seated face-to-face, 1 metre apart, same eye level | 🔰 Balance scale visible to both | 📖 Social story nearby | Timer visible to both
Remove: Screens, loud toys, pets. No sibling intrusions during session.
Full Setup Checklist
- Quiet, distraction-minimal space
- Materials set out BEFORE child enters
- Seating: face-to-face, same eye level
- Balance scale (or T-chart) visible to both
- Visual cue card at child's eye level
- Question cards accessible to child
- Timer visible (10–15 min)
- Your tone: warm, curious, playful — not instructional
- Natural light preferred; background noise minimal
Source: PMC10955541 | SI Theory (Ayres) Environmental Setup Principles

ACT III — Execution
Is Your Child Ready? Readiness Check
"The best session is one that starts right." Run this checklist every time — conditions change daily, and a child's readiness state determines session quality more than any other factor.
Fed and hydrated within last 2 hours?
Not visibly tired or ill?
No active emotional distress?
Not fixated on a strong interest?
If yes → use THAT interest as the session material today
Makes brief eye contact or social orienting?
Willing to come to the space without forced redirection?
Last conversation attempt not ended in distress within last hour?
✅ 6–7 Checks
GO — Begin full protocol
✅ 4–5 Checks
MODIFY — Shorten to 8 min, puppets or games only
✅ 0–3 Checks
POSTPONE — Offer low-demand connecting activity. Try again later.
Source: ABA Antecedent Manipulation Principles | BACB Clinical Guidelines | PMC11506176

ACT III — Step 1
Step 1: The Invitation
"How you open the session shapes everything that follows." The invitation must feel like play, not instruction. Choose the script that feels most natural for your child today.
Option A — Interest-Hook Opening
"Hey, I want to play a conversation game with you. I'm going to try to find out things about YOU — and I bet you can find out things about me too. Want to try?"
Option B — Balance-Scale Hook
"I have this cool scale. I want to see what our conversation looks like on it — who talks more, who asks more. Let's find out together."
Option C — Direct (Older Children)
"Can we practice something together? It's about conversations — how they go both ways. We'll use some tools to help. 10 minutes."
If the child declines: Don't push. Say: "No problem. Let me know if you change your mind." Try again tomorrow. Forced sessions undo progress. | Source: ABA Motivating Operations Principles | PMC11506176

ACT III — Step 2
Step 2: Establish the Anchor Concept
"Before the tools — plant one concept." Deliver the anchor concept in 60 seconds. Keep it concrete, visual, and joyful — not instructional.
"Conversations are like a ball game. I throw the ball — that's sharing something. You catch it and throw it back — that's asking about me or sharing something back. When one person keeps the ball the whole time, nobody has fun. Today we're going to practice throwing the ball both ways."
Visual support: Draw two stick figures with a ball arc between them. Label: "SHARE ↔ ASK"
For Younger Children (Ages 5–8)
Use the balance scale now. Place one token on the "me" side: "I just shared something." Ask: "What do you do now?" Guide: "Add a token to 'them' by asking me something." Make it concrete before abstract.
For Older Children (Ages 9–14)
"You've probably had conversations where you leave feeling like the other person never asked about you once. How did that feel? That's what we're going to help you avoid doing to others — not because you're being unkind, but because you haven't had the tools."
Source: Social cognition intervention principles | Theory of Mind developmental research

ACT III — Step 3
Step 3: The Therapeutic Action — Core Protocol
The 6-step protocol. Run this every session. ⏱️ Total session: 10–15 minutes. Three genuine reciprocal exchanges are worth more than 30 forced ones.
01
3A — Deploy Balance Scale / Tracker
Set out the balance scale or T-chart. Every share → token on child's side. Every question asked → token on parent's side. Start a natural conversation on any topic.
02
3B — Run a Timed Conversation (3–5 min)
Talk naturally. Let the child lead their usual topic. Place tokens in real time. Do NOT correct during — observe. After: "Look at our scale. What do you notice?"
03
3C — Introduce Question Cards
Child picks a card from the Question Prompt set, asks the question. Parent answers fully. Parent asks child the same question back. Two-way exchange on one topic.
04
3D — Two-Sided Topic Card Exchange
Pull one Two-Sided Topic Card. Child reads SHARE side → shares. Then reads ASK side → asks. Parent responds. Repeat with 2–3 cards.
05
3E — Reciprocity Game (5 minutes)
Play one round of a reciprocity-structured game. Reciprocity is enforced by game mechanics — not parental correction.
06
3F — Role-Play Scenario (optional)
Puppet/role-play brief: "2-minute conversation where we both ask at least one question." Child plays both roles if possible — the talker AND the listener who isn't asked.
Source: PMC10955541 (session structure efficacy) | ABA session principles | NCAEP 2020
ACT III — Step 4
Step 4: Repeat & Vary
"Therapeutic dosage: how many reps, when to vary." The pattern must be practiced in variation to generalise. Same material, same context, same partner every time → skills stay in the practice box.
Week 1–2
2–3 question exchanges per session. Prioritise Material 1 (balance scale) + Material 2 (question cards) only.
Week 3–4
Introduce Material 7 (two-sided topic cards) and Material 3 (games). 4–5 reciprocal exchanges per session.
Week 5–8
All 9 materials in rotation. 6–8 reciprocal exchanges. Begin fading visual balance tracker.
Variation menu (keep fresh across sessions):
- Rotate question card topics: interest, experience, opinion, feeling
- Change the game format each week
- Vary who starts: parent leads first vs. child leads first
- Bring in a sibling or grandparent for a tri-person session (Week 5+)
- Take the skill out: practice at dinner, at a playground
Satiation signal: Child becomes irritable or asks "are we done?" → close the session. | Source: SI therapy dosage research | ABA generalisation protocols

ACT III — Step 5
Step 5: Reinforce & Celebrate
"Timing beats magnitude. Immediate, specific, enthusiastic." Reinforce within 3 seconds of the desired behaviour. Verbal praise is the minimum — layer with tokens, stickers, or natural rewards.
"You just asked me a question — I loved that."
"You actually listened to my answer before going back to your topic — that's huge."
"You noticed I stopped responding — and you asked if I was interested. That is a real skill."
"The balance scale is more even today than last week."
Reinforcement menu: Sticker/token (younger children) | Mark progress on "Reciprocity Tracker" chart | Let them choose next game or topic | For teens: genuine curiosity shown back ("I'm going to look that up!") | 🏆 Rosette Imprint Reward Jar (₹589) | 🌟 1800+ Reward Stickers (₹364) | DIY free "Conversation Champion" chart
"Celebrate the attempt, not just the success. A question asked awkwardly is worth 100 sessions of theory." | Source: ABA Reinforcement Principles | BACB ethical guidelines | 📞9100 181 181

ACT III — Step 6
Step 6: The Cool-Down
"No session ends abruptly. The cool-down prevents post-session dysregulation." A predictable, warm closing sequence helps the child transition and preserves the positive association with practice.
1
Warning (2 min before end)
"Two more questions, then we're all done."
2
Closing Exchange
"What was one thing you found out about me today? What was one thing you shared?" — brief bilateral review.
3
Material Put-Away Ritual
Child helps pack materials — closing the session physically signals the end.
4
Transition Out
"Now you choose what we do next." — restores child autonomy.
5
Positive Closing Statement
"You practiced something really important today. I'm proud of you."
If child resists ending: "Let's do one more question each, and then we stop. That's the deal." | If child seems distressed by balance scale result: "That's information, not a grade. Every session, the scale gets more even." | Source: NCAEP 2020 | Visual timer and transition support evidence

ACT III — Data
Capture the Data — Right Now
"60 seconds of data now saves hours of guessing later." Record immediately after each session while memory is fresh. This data feeds the GPT-OS® Conversational Reciprocity Index.
Data Point | How to Record | Why It Matters | |
Questions child asked | Tally: ___ / session | Primary progress marker | |
Responded to partner's topic before redirecting? | Y / N / Partial | Listener monitoring indicator | |
Balance scale result | Child heavy / Balanced / Partner heavy | Visual reciprocity measure | |
Materials used today | Circle: 1 / 2 / 3 / 4 / 5 / 6 / 7 / 8 / 9 | Tracks protocol fidelity | |
Child engagement quality | 1 (resistant) – 5 (enthusiastic) | Readiness trend indicator | |
Standout moment | Free text | Qualitative clinical insight |
📄 Download Pinnacle B-216 Session Tracker PDF (printable, A5) | GPT-OS® integration: data feeds into Conversational Reciprocity Index + Pragmatic Language Function Index automatically. | Source: ABA Data Collection Standards | BACB Guidelines | Cooper, Heron & Heward (ABA, 8th ed.)

ACT III — Troubleshooting
What If It Didn't Go As Planned?
"Session abandonment is not failure — it's data." Every difficult session contains clinical information. Here are the seven most common challenges and exactly what to do next.
Child refused to participate
Why: Felt pressured or sensed a lesson coming. Solution: Next session, start with the game only — no scale, no cards. Let them win. Then introduce one card casually.
Child shut down at the balance scale
Why: Shame response — the tool surfaced what they already feel about themselves. Solution: Put scale away. Pivot to natural conversation. Reintroduce after 2+ sessions when trust is rebuilt.
Questions felt scripted / robotic
Why: They're learning. Scripted questions ARE progress. Don't correct the quality — celebrate the attempt. Naturalness comes with practice.
Child answered then immediately redirected to their topic
Why: Habit is strong. Gently use visual cue card (Material 9): "Check the balance?" One gentle prompt, not repeated correction.
Session devolved into their favourite topic lecture
Why: That's the pattern you're treating. Redirect: "I love hearing about this AND let's put one token on your side. Now what can you find out about me in the same amount of time?"
No change after 3 weeks
Why: Multiple possible factors. Action: Review session data. Are sessions happening 3×/week? Contact FREE Helpline 9100 181 181 for clinical support.
ACT III — Personalise
Adapt & Personalise
"No two children are identical. Here's how to adjust." The protocol has a standard form — but clinical excellence means knowing when and how to flex it for the individual child in front of you.
🎯 The Intense-Interest Child
Use THEIR topic as the practice material. "Tell me about Minecraft — but after each thing you tell me, I'll ask you something, and then you ask me something." Their passion is the fuel; reciprocity is the frame.
😟 The Anxious Child
Skip the balance scale in early weeks — it can feel like surveillance. Start with question cards and games only. Introduce scale at Week 4 when safety is established.
👶 Younger Children (Ages 5–8)
Concrete, game-based only. No meta-discussion about reciprocity. Balance scale with physical tokens. Puppets. Award a sticker for every question asked.
🧑 Older Children / Adolescents (Ages 11–14)
Frame as social intelligence, not a deficit. "Understanding that others have inner worlds as interesting as yours is a superpower." Less scale, more reflection. Fade visual supports earlier.
Source: OT/ABA/SLP individualised planning principles | Sensory profile-based practice

ACT IV — Progress Arc
Week 1–2: What to Expect
"If your child tolerates the scale without shutting down — that's real progress."
✅ What IS Expected (Week 1–2)
- Child engages with materials without significant resistance
- Child produces 1–2 prompted questions per session (with cards)
- Child can identify the imbalance on the balance scale (even if can't change it yet)
- Parent feels more confident running the protocol
❌ What Is NOT Expected Yet
- Spontaneous question-asking in natural conversations
- Reduced one-sidedness outside sessions
- Genuine visible curiosity about others
"You are planting roots right now. Nothing visible happens above ground for the first two weeks. That doesn't mean nothing is happening." Week 1–2 is often the hardest for parents — this is normal.
Progress: ~15% of the 8-week arc. Consistency now pays off in Week 4–6. | Source: PMC11506176 | General intervention timeline literature
ACT IV — Progress Arc
Week 3–4: Consolidation Signs
"Watch for the neural pathway forming. These are the signs." Week 3–4 is when the explicit teaching begins converting into emerging habit — the first signs that the brain is integrating the new pattern.
Child picks up question cards with less prompting
Child begins to notice balance scale without being directed to look
Child asks 1–2 questions per session WITHOUT cards on 1–2 occasions
Child sometimes sustains a topic the parent introduced (even briefly)
Parent notices child remembering something they told them in a previous session
Behavioural signals of neural pattern formation: Child anticipates the session and comes willingly | Child makes a spontaneous comment about someone else's life outside sessions | Child applies a question card phrasing in a natural conversation (even clumsily)
When to increase frequency: If Week 3–4 shows consistent 3+ indicators → increase to 4–5 sessions/week and introduce Material 7 (two-sided topic cards) in natural dinner conversation. | Progress: ~40% of 8-week arc. | Source: Neuroplasticity evidence — synaptic strengthening through repeated structured input
ACT IV — Progress Arc
Week 5–8: Mastery in Formation
"The skills are beginning to live in the child — not just in the materials." This is the phase where structured practice begins transforming into genuine, internalised social skill.
✅ Mastery Indicators (Week 5–8)
Child generates questions without card prompts in some situations | Balance scale shows measurably more balanced conversations | Child reports or parent observes a genuine moment of curiosity | Peer response beginning to shift: classmate stays in conversation longer | Child self-corrects: "Oh wait — what do YOU think?"
🔄 Generalisation Check (Critical)
Does the skill appear at home with parents? (Week 4+) | With familiar siblings? (Week 5+) | In one-on-one peer context with a known friend? (Week 6+) | With adults outside the home? (Week 7+)
📉 Visual Supports Fade Protocol
Begin fading balance scale by Week 6 — move from physical scale to internal counting: "I've shared 3 times. Have I asked anything?"
Progress: ~65% of 8-week arc. | Source: PMC11506176 | Generalisation literature | Neuroplasticity evidence

ACT IV — Milestones
Celebrate the Milestones
"Every question asked is a friendship that could happen. Mark these moments."
1
🥉 Bronze — First Unprompted Question
Your child asked someone a question — without a card, without a reminder. Write the date. Frame it. This is the day the skill became real.
2
🥈 Silver — First Genuine Curiosity Moment
Your child remembered something someone told them and asked a follow-up. "How did your sister's recital go?" They retained it. They cared.
3
🥇 Gold — Reciprocal Conversation (Both Sides)
A conversation that felt — to the other person — genuinely mutual. They didn't end it to escape. They left wanting to talk to your child again.
4
💎 Diamond — Chosen Connection
A peer chose to sit with your child at lunch. A classmate sought them out. A relative left saying "I love talking with them."
"From fear to mastery. One question at a time." — Pinnacle Blooms Consortium® | 📞9100 181 181

ACT IV — Safety
Red Flags: When to Seek Professional Help
"This page is educational. These signs mean: please call a professional." Home intervention is powerful — and knowing when to escalate is a sign of clinical wisdom, not failure.
🚨 Seek SLP Evaluation If:
One-sided patterns persist beyond 3 months of consistent home intervention with no measurable change | Child becomes significantly distressed by the concept of asking questions | Child has never asked a question in any context — even about their own needs | One-sidedness is part of a pattern: also struggles with eye contact, understanding jokes, reading facial expressions
🚨 Seek Psychological / Developmental Evaluation If:
Pattern accompanied by rigid thinking, intense restricted interests, or sensory differences | Child has experienced significant peer rejection or bullying related to conversation patterns | Child reports feeling "broken" or "weird" about social interactions | Parent suspects autism, ADHD, or social communication disorder as underlying profile
01
FREE: Call Pinnacle Helpline 9100 181 181 (24×7, 16+ languages) for initial guidance
02
Request AbilityScore® Assessment — comprehensive developmental evaluation
03
SLP + Psychologist coordinated evaluation
04
GPT-OS® Diagnostic Intelligence Layer generates personalised intervention plan
Source: ASHA Clinical Guidelines | Autism diagnostic criteria (DSM-5) | 📞9100 181 181

ACT IV — Pathway
Your Progression Pathway
"You're not done — you're on a journey." B-216 sits within a carefully sequenced cluster of social communication techniques. Where you've come from — and where you're headed — matters for treatment planning.
1
B-214
Reading Listener Cues — prerequisite awareness
2
B-215
Perspective-Taking — seeing others' minds
3
B-216 ← YOU ARE HERE
One-Sided Conversations — building reciprocal exchange
4
B-217
Maintaining Friendships — the next frontier
5
B-218
Social Problem-Solving — advanced social navigation
Prerequisite check: Before B-216 consolidates fully, ensure child has basic awareness of listener cues (B-214) and emerging perspective-taking (B-215). If absent, address in parallel. | Lateral connection: If B-216 isn't working → explore B-210 (Interrupting). | Source: WHO/UNICEF Developmental Milestones Framework | GPT-OS® 12-Domain architecture
ACT IV — Domain Map
Related Techniques in This Domain
"More techniques in the Social Communication Domain." If you've implemented B-216, you already own the materials needed for several related techniques — no additional purchases required.
Technique | Focus | Level | Materials You Already Own | |
B-214 | Reading Listener Cues | 🟢 Intro | Visual supports | |
B-215 | Perspective-Taking & Theory of Mind | 🟡 Core | Social stories, question cards | |
B-210 | Interrupting — When They Can't Wait | 🟢 Intro | Visual cue cards | |
B-206 | Conversation Turn-Taking | 🟢 Intro | Balance scale, game | |
B-217 | Maintaining Friendships | 🔴 Advanced | All 9 materials from B-216 | |
B-218 | Social Problem-Solving | 🔴 Advanced | Social stories, role-play |
Browse full domain → techniques.pinnacleblooms.org/domain/social-communication | "You already own materials for B-214, B-215, and B-217 if you've implemented B-216."
ACT IV — Full Picture
Your Child's Full Developmental Map
"B-216 is one piece of a larger plan. See the full picture." This technique addresses Domain B (Social Communication). Across the 12 Domains, your child has active intervention areas mapped by their AbilityScore® profile. Each domain is a river — B-216 is one tributary.
GPT-OS® maps your child's developmental profile across all 12 domains simultaneously, ensuring that B-216 work is coordinated with every other active intervention area — not siloed.
Source: WHO/UNICEF Nurturing Care Framework | GPT-OS® 12-Domain architecture
ACT V — Community
A Family's Story
"My son could talk for an hour about Minecraft without ever asking what the other person liked. His grandmother would nod politely while he lectured. His classmates would find excuses to leave. We started with conversation balance — literally a scale with tokens. Something clicked around month three. He started asking his grandmother questions about her garden — something he'd never cared about before. 'Tell me about your tomatoes, Grandma.' She almost cried. He still loves Minecraft — still wants to share about it — but he knows to check in now. 'What are you into these days?' he asks. And then he actually listens. He has friends now who choose to sit with him."
— Parent, Pinnacle Network(Illustrative case; outcomes vary by child profile)
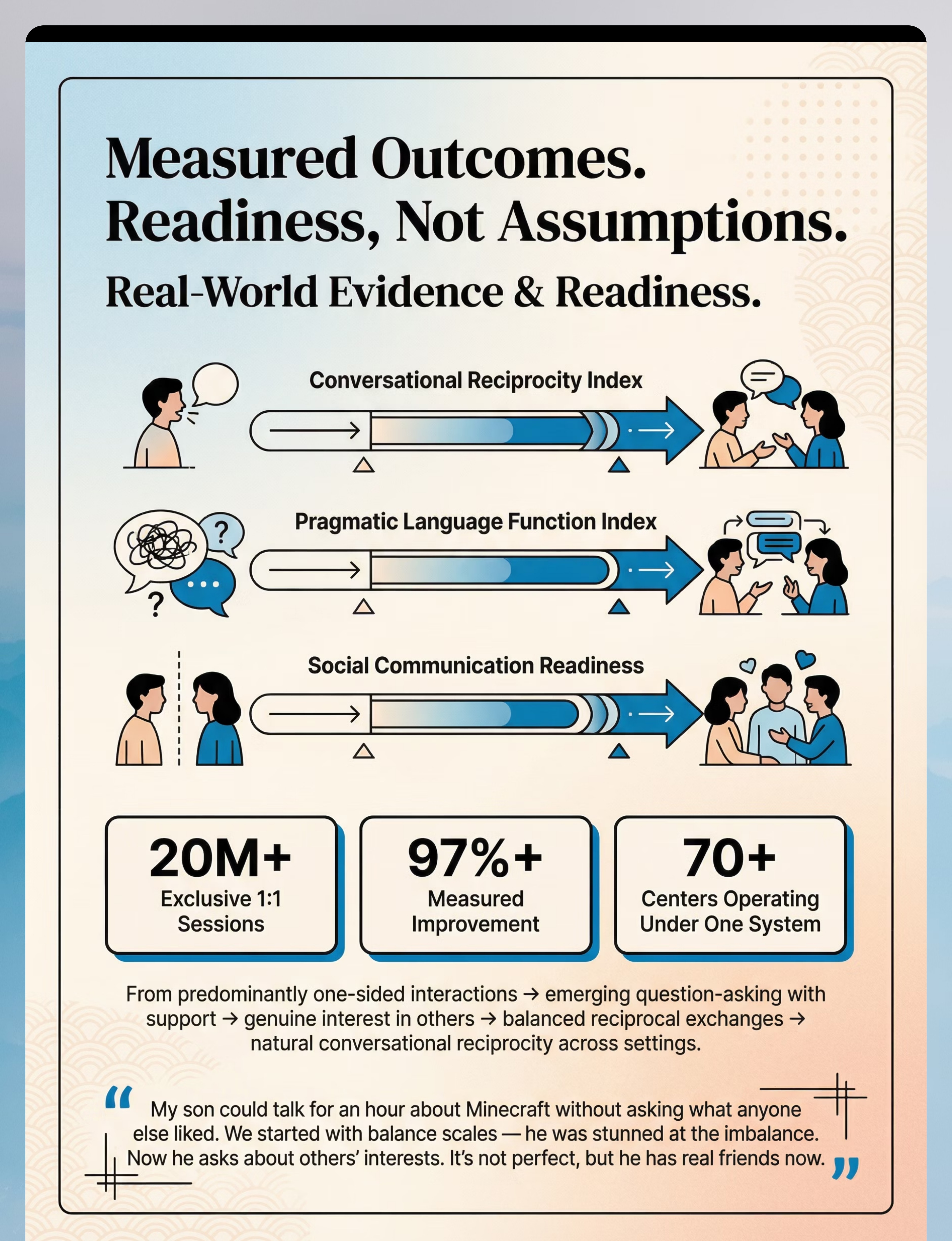
Conversational Reciprocity Index progression: Predominantly one-sided → Emerging reciprocity with supports → Balanced exchanges in familiar contexts
📞 FREE Helpline: 9100 181 181 | Available 24×7 in 16+ languages
ACT V — Community & Ecosystem
Connect With the Community
"You are not solving this alone. Join the global community." Every family navigating this shares your hope and your exhaustion. The community exists because no parent should figure this out alone.
🌍 Pinnacle Parent Community
pinnacleblooms.org/community — global parent network sharing strategies, wins, and support
💬 WhatsApp Support Groups
Ping 9100 181 181 to join your city's group — local caregivers, real conversations
📱 Instagram Community
@pinnacleblooms — daily tips, parent stories, and therapist insights
🎥 YouTube Library
999 Reels Library including B-216 video content and full technique walkthroughs
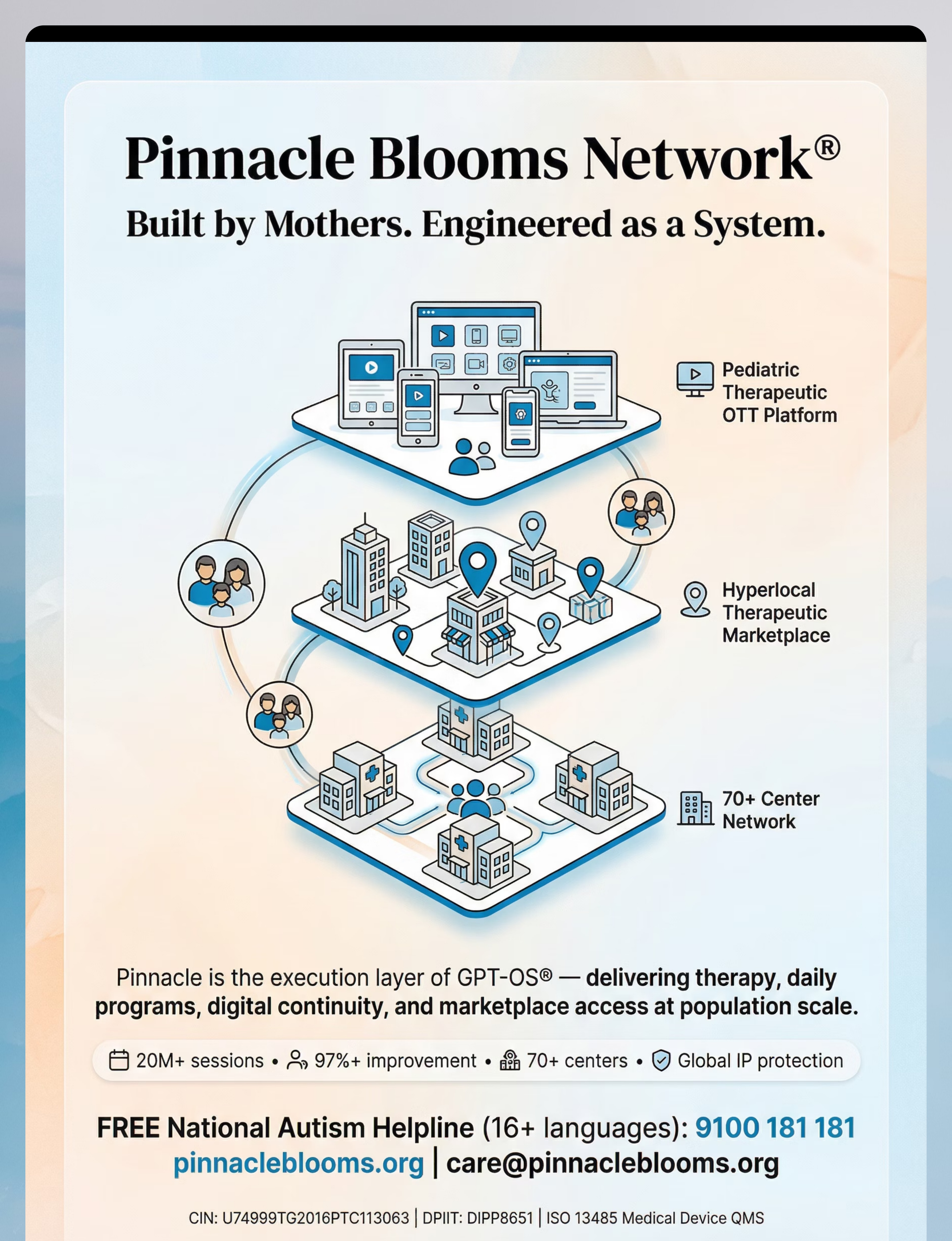
Global reach: 70+ countries | 16+ languages | 21 million therapy services | 70+ centers
📧 care@pinnacleblooms.org — write to our clinical team | 📞 FREE 24×7: 9100 181 181 in 16+ languages

ACT V — Ecosystem
Find a Professional Near You
"70+ centers. One system. Your city." No center nearby? Full assessment and therapy planning is available via video consultation — access is never a barrier.
What You Get at a Pinnacle Center
- AbilityScore® Assessment (comprehensive developmental profile)
- GPT-OS®-governed therapy plan across all active domains
- SLP + OT + BCBA/ABA + SpEd convergent team
- EverydayTherapyProgramme™ — your home protocol, clinically designed
- Social Skills Group (peer practice for B-216 goals)
- Progress tracking via Conversational Reciprocity Index
How to Get Started
📞 Call 9100 181 181 (FREE) → tell us your city → nearest center or teleconsult scheduled within 48 hours.
Teleconsultation available: Full assessment and therapy planning via video consultation if no center is nearby.
Professional referral note: Referring clinician? Request assessment pathway at care@pinnacleblooms.org
CIN: U74999TG2016PTC113063 | DPIIT: DIPP8651 | ISO 13485 Medical Device QMS
ACT V — Research Library
Research Library
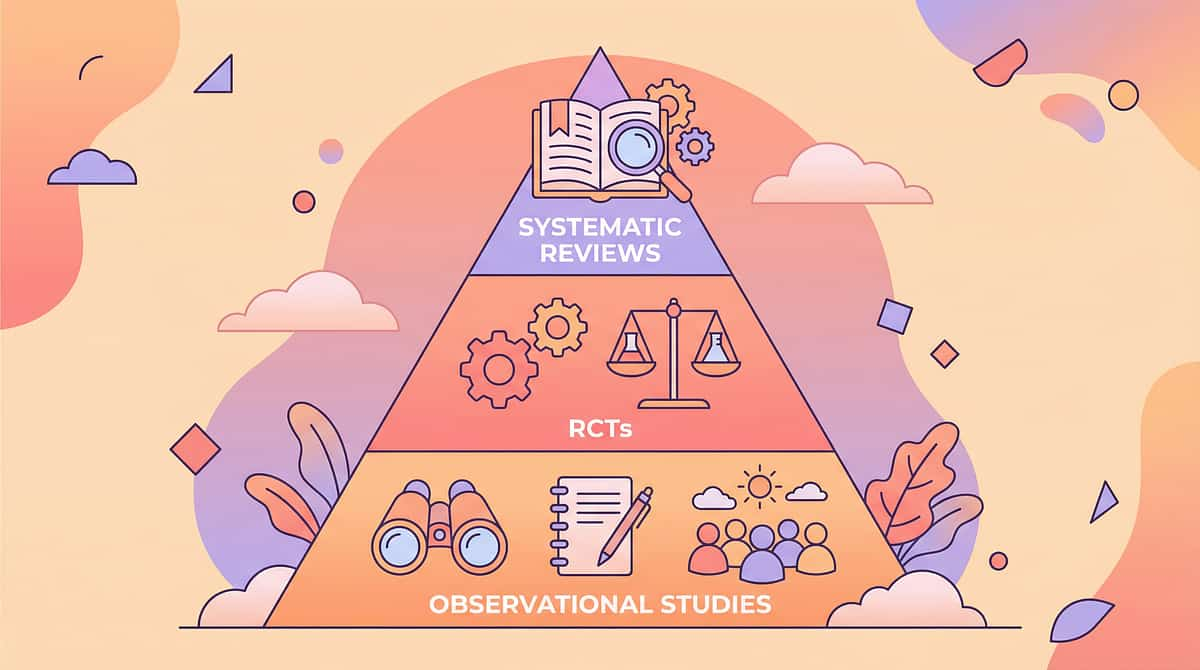
"Deeper reading for the curious parent." Every claim in this protocol traces to peer-reviewed evidence. Here is the full evidence hierarchy supporting B-216.
1
Level I — Systematic Reviews & Meta-analyses
PMC11506176 — PRISMA (2024): Social communication interventions evidence-based for ASD | PMC10955541 — Meta-analysis (2024): Social skills + pragmatic language outcomes, 24 studies
2
Level II — RCTs
Padmanabha et al., Indian J Pediatr (2019): Home-based parent-administered intervention | PMC9978394 — CCD Package outcomes across 54 LMICs
3
Level III — Clinical Practice Guidelines
NCAEP 2020: Social Stories™, Video Modeling, Visual Supports — evidence-based | ASHA Clinical Guidelines: Pragmatic language intervention | WHO NCF 2018
4
International Standards
WHO/UNICEF CCD Package (2023) | DOI: 10.1080/17549507.2022.2141327 | Frontiers Integrative Neuroscience 2020

ACT V — Technology
How GPT-OS® Uses Your Data
"Transparency: how your session data becomes your child's personalised plan." Data privacy is protected under ISO/IEC 27001 Information Security standards. Individual data is never shared or sold.
B-216 Session Data Feeds:
- Conversational Reciprocity Index (primary)
- Pragmatic Language Function Index (secondary)
- Question-Asking Function sub-index
- Social Curiosity Function sub-index
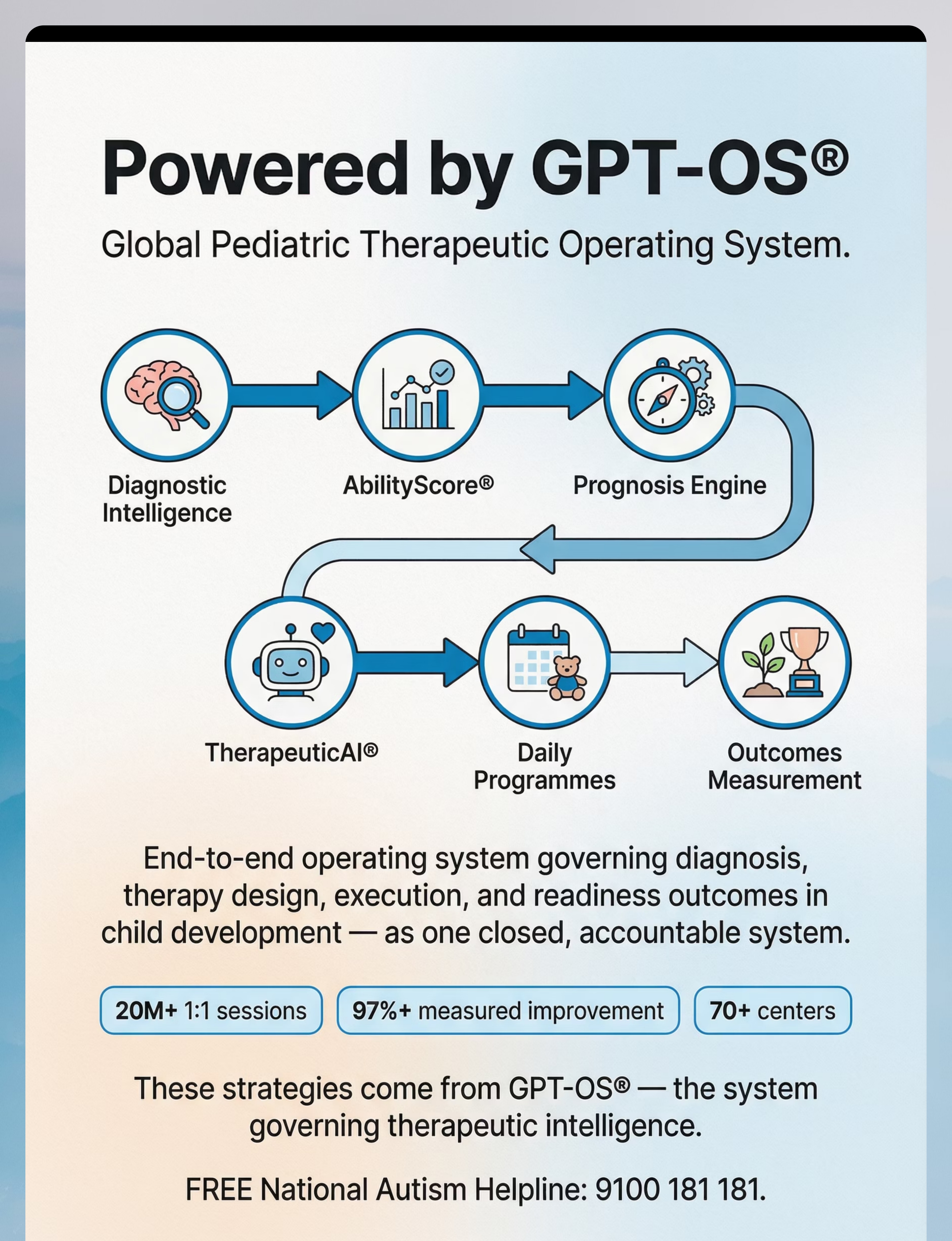
GPT-OS® Technology Stack
Diagnostic Intelligence → AbilityScore® → Prognosis Engine → TherapeuticAI® → FusionModule™ → EverydayTherapyProgramme™ → Re-measurement
"Your data helps every child like yours."
Source: Digital health ASD intervention evidence (21 RCTs, 1,050 participants, 2024 meta-analysis)

ACT V — Watch & Learn
Watch the Reel
"See it. Then do it." Multi-modal learning — video + text + demonstration — is proven to improve parent skill acquisition. NCAEP (2020): Video modeling is an evidence-based practice for autism.
🎬 Reel B-216 Details
Title: 9 Materials That Help With One-Sided Conversations
Series: Social Communication & Pragmatic Language Solutions
Reel ID: B-216 | Episode 216 of 999
Duration: ~75–85 seconds
Presenter: Pinnacle SLP Consortium Therapist
What This Reel Shows
- The recognition moment: child talking while listener disengages
- Each of the 9 materials in 4–5 second demonstrations
- The transformation: child asking a genuine question, both people engaged
- The GPT-OS® system that powers the protocol
Watch on: @pinnacleblooms (Instagram) | Pinnacle YouTube Channel | pinnacleblooms.org/reels

ACT V — Share
Share This With Your Family
"Consistency across caregivers multiplies impact." When grandparents, teachers, and siblings all understand the protocol — the child gets reinforcement across every environment, not just therapy sessions.
📄 Family Guide PDF
1-page summary of the B-216 protocol for grandparents, teachers, and caregivers. Download and share before the next family gathering.
💬 "Explain to Grandparents" Version
"When [child's name] talks for a long time without asking about you, please don't feel offended. They're learning. The best thing you can do: wait for a pause and ask 'Can I tell you something?' When they look surprised, that's progress — it means they noticed."
📚 Teacher / School Communication Template
"Dear [Teacher], we are working on conversational reciprocity at home. [Child] may benefit from: structured turn-taking prompts in group work, a visual cue card at their desk, and positive reinforcement when they ask a question. Happy to share the home protocol."
WHO CCD Package: Multi-caregiver training is critical for intervention generalisation. PMC9978394
ACT VI — The Close
Frequently Asked Questions
"Your questions. Answered by the Consortium."
My child asks questions but they feel robotic and forced. Is that progress?
Yes. Scripted questions ARE progress. Naturalness comes with practice — 100 clumsy questions before one fluent one. Celebrate every attempt.
My child understands reciprocity but still doesn't DO it. Why?
Knowing ≠ doing. The skill must be practiced until it becomes automatic. Understanding alone doesn't build the neural pathway — structured practice 3–5×/week does.
At what age should I be concerned about one-sided conversations?
Persistent significant one-sidedness beyond age 7 that is affecting peer relationships warrants evaluation. Mild one-sidedness in a 5–6-year-old is within normal developmental range.
Could this be autism?
Reduced conversational reciprocity is a core feature of autism. If your child also shows difficulty with eye contact, restricted interests, or sensory differences, a comprehensive evaluation is recommended. Call 9100 181 181.
Can I use these materials with multiple children?
Absolutely. Conversational reciprocity is a skill all children benefit from strengthening. Run the protocol as a family game — no "patient" label required.
When does a child "complete" this intervention?
When your child spontaneously asks questions, listens to answers, and maintains mutual exchange with familiar people — the skills are consolidated. Maintenance continues informally.
Didn't find your answer? → Ask GPT-OS® at pinnacleblooms.org | Call 📞9100 181 181
Preview of 9 materials that help with one sided conversations Therapy Material
Below is a visual preview of 9 materials that help with one sided conversations therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.





Link copied!

ACT VI — Start Now
Your Child Wants to Connect. The Tools Are Right Here.
From fear to mastery. One technique at a time. B-216 is validated by a consortium of speech-language pathologists, occupational therapists, behaviour analysts, special educators, and neurodevelopmental pediatricians — all united behind one goal: helping your child build the connections they deserve.
20M+
1:1 Sessions Delivered
97%+
Measured Improvement
70+
Centers Worldwide
70+
Countries Reached
🌸 Validated by the Pinnacle Blooms Consortium® | 🗣️ Speech-Language Pathology | 🖐️ Occupational Therapy | 🎯 Applied Behaviour Analysis | 📚 Special Education | 🧠 NeuroDevelopmental Pediatrics
This content is educational and does not replace assessment by a licensed speech-language pathologist, psychologist, or healthcare provider. Individual results may vary. Statistics represent aggregate outcomes across the Pinnacle Blooms Network. © 2025 Pinnacle Blooms Network®, unit of Bharath Healthcare Laboratories Pvt. Ltd. CIN: U74999TG2016PTC113063 | DPIIT: DIPP8651 | ISO 13485 | ISO/IEC 27001 | 📞 9100 181 181 | pinnacleblooms.org | care@pinnacleblooms.org