9 Materials That Help With No Babbling
Your baby is too quiet — no bababa, no mamama. Discover 9 evidence-based materials to stimulate babbling and unlock your child's voice. Consortium-validated by Speech-Language Pathologists, Occupational Therapists, and NeuroDevelopmental Pediatricians.

ACT I — THE EMOTIONAL ENTRY
"My Baby Is So Quiet."
You listen. You wait. You lean in close. Nothing. No "bababa." No "mamama." No little sounds drifting from the crib during morning playtime. Just silence — or the occasional vowel: "aaah," "eeee" — soft and shapeless, without the consonants that other babies seem to make effortlessly.
You watch videos of your friend's baby at the same age — babbling away, strings of sounds tumbling out like practice conversations. And your baby just watches. Listens. Stays quiet. You've started Googling. You've started counting months. You've started wondering if something is wrong.
You are not imagining this. And you are not alone.
"My baby is 9 months old and has never said bababa or mamama. She just makes soft vowel sounds. I talk to her all day but she never talks back — not even baby sounds." — Parent, Pinnacle Blooms Network Community
Millions of Parents Share This Exact Worry
Absent or delayed babbling is one of the most common early concerns parents bring to developmental pediatricians. Here's what the research shows — and why your concern is clinically valid, not overreaction.
7–10 Months
Canonical babbling — repeated consonant-vowel syllables like "bababa" and "mamama" — typically emerges during this window.
5–8% of Infants
Show delayed onset of canonical babbling beyond 10 months. You are far from alone. (Oller et al., 1999)
6 Months
Reduced vocalization frequency identified as early as 6 months in infants later diagnosed with autism. (Paul et al., 2011)
All Cultures
Delayed babbling occurs across all cultures, languages, and socioeconomic levels. This is a neurodevelopmental pattern — not a parenting failure.
The American Speech-Language-Hearing Association (ASHA) identifies absence of canonical babbling by 10 months as a significant communication red flag warranting evaluation. A delay is a signal — not a diagnosis. And signals can be responded to.

The Babbling Timeline: Where Your Baby Is — And Where They're Going
Understanding typical vocal development helps you see exactly where your child stands and what comes next. The window for maximum impact is the first 18 months — when neural circuits for speech motor planning are at peak plasticity.
0–2 Months: Reflexive Sounds
Crying, vegetative sounds. Communication through needs.
2–4 Months: Cooing
"Aaah," "oooh," "eeee" — soft vowel sounds, social smiling emerges.
4–6 Months: Vocal Play
Squeals, growls, raspberries, pitch variation. Baby experimenting with voice.
6–7 Months: Marginal Babbling
Consonant-like sounds emerging, not yet rhythmic or repetitive.
⭐ 7–10 Months: Canonical Babbling
"Bababa," "mamama," "dadada" — THE milestone. Absence by 10 months = significant red flag.
12–18 Months: First Words
Babbling patterns become recognizable words. Jargon with sentence-like intonation.
Per WHO and ASHA clinical standards: By 6 months, baby should make vocal sounds beyond crying. By 10 months, canonical babbling should be present. By 12 months, variegated babbling with multiple CV combinations. Stimulation during the first 18 months has dramatically higher efficacy than intervention starting after 24 months.

ACT II — THE KNOWLEDGE TRANSFER
Vocal Stimulation Through Multi-Modal Environmental Enrichment
Parent-Friendly Name: "Unlocking Baby's Voice." A systematic approach to stimulating babbling by optimizing three conditions simultaneously: positioning the baby for maximum face-to-face vocal input, activating the oral muscles that produce consonant-vowel combinations, and creating immediate rewarding consequences every time the baby vocalizes — teaching their brain that using their voice makes wonderful things happen.
Domain
Speech & Language Development — Prelinguistic Vocalizations (SPL-PRELING-VOC)
Age Range
4 months – 18 months
Session Duration
5–15 minutes, 3–5 times daily integrated into natural routines
Materials Required
9 materials total. 5 of 9 have zero-cost household alternatives.
Total Investment
₹2,700–10,500 comprehensive setup | ₹400–1,500 essential starters
Evidence Level
Level I–II — Systematic Reviews + Controlled Studies

Four Disciplines. One Voice.
This technique crosses therapy boundaries because the brain doesn't organize development by therapy type. Four specialist disciplines each contribute a critical piece of the puzzle.

🗣 Speech-Language Pathologist — PRIMARY LEAD
Designs the vocal stimulation protocol. Assesses oral-motor readiness. Sequences targets from vowel sounds → canonical babbling → variegated babbling. Monitors phonological inventory. The SLP determines WHICH sounds to target and in WHAT order.
🤲 Occupational Therapist — CO-LEAD: ORAL-MOTOR
Addresses the sensory-motor foundation for speech. Oral defensiveness assessment. Oral-motor desensitization protocols. Positioning for optimal vocal production. The OT ensures the MOUTH IS READY to produce the sounds.

🧩 Board Certified Behavior Analyst — REINFORCEMENT
Designs reinforcement contingencies that make vocalization rewarding. Establishes cause-and-effect between voice use and positive outcomes. Preference assessments. The BCBA ensures the baby WANTS to use their voice.

👨⚕️ NeuroDevelopmental Pediatrician — DIFFERENTIAL DIAGNOSIS
Rules out hearing impairment, oral-motor structural differences, childhood apraxia, and global developmental delay. Monitors for autism indicators. Orders audiological evaluation. The pediatrician ensures no MEDICAL BARRIER to babbling.

Precision Targets: What Changes When Babbling Activates
Every technique has a primary goal, secondary skills it builds, and long-term developmental gains it unlocks. Here is exactly what this protocol is designed to change — from the first session through mastery.
PRIMARY: Canonical Babbling Production
Production of consonant-vowel (CV) combinations: "ba," "ma," "da." Repetitive syllable strings: "bababa," "mamama." Observable: 2+ different CV combinations in a 10-minute observation period. Measured by vocalization frequency count per session.
SECONDARY: Vocal Foundation Skills
Increased vocalization frequency overall. Vocal turn-taking with caregiver. Oral-motor activation (lip closure, tongue elevation, jaw grading). Auditory self-monitoring. Sound imitation attempts.
TERTIARY: Long-Term Developmental Gains
Foundation for first words. Oral-motor strength for feeding progression. Social communication intent. Receptive language development. Feeds into Domain D (Receptive Language), Domain K (Play & Social Interaction), and Domain E (Expressive Language).
THE 9 MATERIALS
Your 9-Material Babbling Stimulation Kit
These nine carefully selected material categories work together to activate the three conditions for babbling: optimal positioning, oral-motor activation, and rewarding reinforcement. Each plays a unique role in the stimulation protocol.

Material 1: Face-to-Face Positioning Supports
What It Is
Boppy pillows, floor seats, positioning wedges, and nursing pillows that support baby in an upright or semi-reclined position — making their face accessible, their mouth visible, and their body stable for vocal effort.
Why It Matters
Optimal positioning is the foundation of everything. A baby who is slumped, strained, or uncomfortable cannot produce voluntary vocalizations efficiently. Supported posture frees the diaphragm and oral structures for speech motor activity.
How to Use
Position baby so their face is at your eye level, 12–18 inches away — the optimal distance for infant face perception. Ensure head is midline and supported. Body should be symmetrical.
Price Range
₹500–₹2,500
Category
Positioning & Seating
DIY Option
Rolled towels or firm household pillows. Get within 12–18 inches during floor time.
Material 2: Oral-Motor Stimulation Tools
What It Is
ARK Z-Vibe, vibrating teethers, textured Chewy Tubes, and NUK massage brushes. These tools directly activate the lips, tongue, cheeks, and jaw — the very muscles that must coordinate to produce consonant-vowel babbling.
Why It Matters
In some children, the oral muscles are literally "asleep" to the task of speech — they have insufficient proprioceptive awareness of what their mouths are doing. Vibration and tactile input wake up these receptors, increasing oral awareness and readiness for intentional movement.
How to Use
Begin with external stimulation — gently stroke lips and cheeks before introducing vibration. Offer vibrating teether near lips first, then allow oral exploration. Always watch for tolerance; oral defensiveness requires OT evaluation.
Price Range
₹300–₹1,500
Category
Oral-Motor Tools
DIY Option
Clean textured washcloths for gentle oral massage. Cold refrigerated damp cloths as teethers.

Material 3: Sound-Activated Toys
What It Is
Voice-activated light-up balls, echo microphones, and sound-responsive animals that react immediately to any sound baby produces — creating a direct cause-and-effect relationship between vocalization and an exciting response.
Why It Matters
Infants learn through contingency: "When I do X, Y happens." Sound-activated toys teach the most critical early lesson — my voice has power. This rewires the brain's reinforcement circuitry to associate vocal output with positive consequences, dramatically increasing the frequency of vocalizations.
How to Use
Introduce after the oral-motor warm-up. Hold toy at baby's eye level. Model a sound near it. When it activates, show dramatic delight. Then wait. Any baby vocalization that activates it = immediate celebration.
Price Range
₹400–₹1,200
Category
Cause & Effect Toys
DIY Option
YOU become the "reward" — respond immediately and dramatically to ANY sound baby makes with wide smile, clapping, and delight.

Material 4: Mirror Play Materials
What It Is
Baby-safe floor mirrors, tummy time mirrors, and handheld safety mirrors — shatter-resistant, acrylic-based materials specifically designed for infant use.
Why It Matters
Mirrors provide real-time visual feedback of mouth movement. When babies see their own lips press together for "b" or "m," they receive a visual confirmation loop that strengthens the motor-visual connection. Watching your mouth in the mirror simultaneously is even more powerful — baby sees both the model and their own attempt side by side.
How to Use
Position the mirror so baby can see their own face during vocalizations. Sit beside baby and model sounds while both of you face the mirror. Point to your mouth: "Watch!" Then point to baby's mouth: "Your turn!" Use exaggerated, slow lip movements.
Price Range
₹300–₹1,000
Category
Visual Feedback Tools
DIY Option
Polished steel plate (thali) as mirror. Smartphone front camera works beautifully — free.

Material 5: Musical & Rhythmic Instruments
What It Is
Baby-safe shakers, drums, tambourines, bells, and egg shakers. Musical instruments that introduce rhythm, timing, and the joyful connection between movement and sound production.
Why It Matters
Rhythm is the scaffolding of speech. The temporal patterning of babbling — "ba-ba-BA, ma-ma-MA" — requires the same rhythmic motor coordination as musical play. Instruments make sessions irresistible, naturally integrate vocal play into joyful movement, and provide a multi-sensory experience that reinforces the oral-motor loop.
How to Use
Shake maraca and sing "Ba-ba-ba!" in rhythm. Pause. Offer the instrument. Any sound baby makes while holding it = celebration. Drum on baby's tummy while saying "Da-da-da." Let musical play be spontaneous and joyful.
Price Range
₹200–₹800
Category
Musical Instruments
DIY Option
Sealed containers with rice or dal. Steel tumbler + spoon as drum. Bangles as bells. All free.
Material 6: Puppets & Animated Toys
What It Is
Mouth puppets with visible lips, singing puppets, and animated talking toys. Any toy whose "mouth" can be exaggerated to demonstrate lip closure, opening, and consonant-vowel movements in an engaging, social way.
Why It Matters
Puppets introduce a third social partner into the interaction — one that's fascinating, non-threatening, and totally focused on mouth movement. They reduce performance pressure (the puppet asks, not the parent), use the mirror neuron system through third-party imitation modeling, and create turn-taking opportunities that feel like play rather than therapy.
How to Use
Have puppet approach baby: "I'm going to say ba-ba-ba!" with exaggerated lip movement. Puppet then looks at baby expectantly. After any baby sound, puppet celebrates dramatically. Puppet can also "fail" at sounds and need baby to show it how.
Price Range
₹200–₹600
Category
Social Play Materials
DIY Option
Sock puppet with marker face. Any stuffed animal — make it "talk" with exaggerated visible mouth movements.

Material 7: Bubbles & Blow Toys
What It Is
Bubble wands, pinwheels, party blowers, and child-safe whistles. Tools that require or demonstrate controlled breath and lip movement — the same physiology required for bilabial consonants like "b," "p," and "m."
Why It Matters
Blowing is one of the most direct bridges between breathing and speech production. The lip rounding and breath control required for bubbles mirrors the oral-motor preparation for bilabial sounds. Bubbles are also visually captivating — they float at baby's eye level, encouraging visual tracking and anticipatory excitement that naturally triggers vocalization attempts.
How to Use
Blow bubbles at eye level. Before each blow, pause and say "Buh-bles!" emphasizing the "B" with a visible lip press. For 8+ months: hold pinwheel near baby's mouth for any breath output. Any breath toward the pinwheel or any "b" attempt = major celebration.
Price Range
₹100–₹500
Category
Oral-Motor Tools
DIY Option
Dish soap + water + straw for bubbles. Paper pinwheel made from scrap paper. Free.
Material 8: Vocal Play Books & Visual Supports
What It Is
Board books with mouth photos and articulation images, books featuring faces with exaggerated expressions, speech sound articulation books, and evidence-based speech stimulation apps designed for prelinguistic development.
Why It Matters
Visual representations of mouth positions provide a stable, repeatable model that doesn't disappear when the parent finishes speaking. Books create a ritual ("book time = sound practice") that babies come to anticipate with positive affect. Large, clear photos of mouths in different positions are powerful tools for babies whose visual processing is stronger than auditory.
How to Use
Open to a page with a big mouth photo. Point: "Look at that mouth! Aaaaah!" Make the same face. Point to baby's mouth. Pause and wait. Use books as a closing ritual after vocal play — a calming, beautiful ending to each session.
Price Range
₹300–₹1,000
Category
Books & Visual Supports
DIY Option
Photo book of family members making sounds with exaggerated mouths. Print and laminate. Free to create.
Material 9: Recording & Playback Toys
What It Is
Talk-back plush toys, dedicated voice recorders, and echo microphones that record and immediately replay sounds. When baby vocalizes into a recording toy and hears their own voice played back, something remarkable happens in the auditory feedback loop.
Why It Matters
Hearing your own voice is one of the most powerful natural reinforcers for continued vocalization. Recording toys close the auditory feedback loop instantly — "That sound came from ME!" This self-recognition triggers fascination and the desire to do it again. For babies who haven't yet discovered the pleasure of their own voice, playback can be the spark that lights the babbling fire.
How to Use
Record yourself saying "da-da-da." Play back. Then say it live. Then record baby's sounds — even a cough or grunt — and play back immediately. Watch their face. The moment of recognition is magic. Use phone voice recorder app as a free alternative.
Price Range
₹400–₹1,500
Category
Technology-Assisted Tools
DIY Option
Phone voice recorder app — record baby's sounds and play back immediately. Completely free.

Complete Kit Overview & Pricing
All 9 materials at a glance — with pricing tiers to fit every budget. Remember: 5 of 9 materials have zero-cost household alternatives. The technique matters more than the tools.
# | Material | Price Range | Category | DIY? | |
1 | Face-to-Face Positioning Supports | ₹500–₹2,500 | Positioning & Seating | ✅ Yes | |
2 | Oral-Motor Stimulation Tools | ₹300–₹1,500 | Oral-Motor Tools | ✅ Yes | |
3 | Sound-Activated Toys | ₹400–₹1,200 | Cause & Effect | ✅ Yes | |
4 | Mirror Play Materials | ₹300–₹1,000 | Visual Feedback | ✅ Yes | |
5 | Musical & Rhythmic Instruments | ₹200–₹800 | Musical | ✅ Yes | |
6 | Puppets & Animated Toys | ₹200–₹600 | Social Play | ✅ Yes | |
7 | Bubbles & Blow Toys | ₹100–₹500 | Oral-Motor Tools | ✅ Yes | |
8 | Vocal Play Books & Videos | ₹300–₹1,000 | Books & Visual | ✅ Yes | |
9 | Recording & Playback Toys | ₹400–₹1,500 | Tech-Assisted | ✅ Yes |
💰 Budget Start
Materials 4, 5, 7 — all DIY-friendly
₹300–₹1,000
₹300–₹1,000
⭐ Essential Starters
Materials 1, 3, 4
₹1,200–₹4,700
₹1,200–₹4,700
🏆 Comprehensive Setup
All 9 materials
₹2,700–₹10,500
₹2,700–₹10,500
✨ Zero-Cost Version
Rolled towel + phone mirror + rice shaker + sock puppet + dish soap + phone recorder = ₹0
WHO Nurturing Care Framework (2022): Context-specific, equity-focused interventions using locally available materials demonstrate equivalent efficacy when responsive interaction principles are maintained.

Set Up Your Babbling Practice Space
The environment you create is as important as the materials you use. Competing stimulation — TV, background noise, siblings, bright overhead lights — significantly reduces the efficacy of vocal stimulation sessions. Here is exactly how to set up your space.
Position Baby (Position 1)
Supported on soft mat — floor seat, tummy time with wedge, or reclined on nursing pillow. Face fully accessible. Head midline. Body symmetrical and relaxed.
Position Yourself (Position 2)
On the floor at baby's eye level. 12–18 inches away — the optimal distance for infant face perception. Your face is the most important material in the room.
Arrange Materials (Position 3)
Within your reach but hidden from baby's view. Each material introduction is a surprise — novelty increases engagement and vocal response rates.
Place Mirror (Position 4)
Baby-safe mirror at baby's eye level. Baby should be able to see their own face and mouth while vocalizing. This visual feedback loop is powerful.
TV Off
No competing audio stimulation
Phone Silent
You need full presence
Door Closed
Siblings out of the room
Soft Lighting
Warm temperature — comfortable for both of you

Step 1: The Invitation — "Hello, Sweet Voice."
The First 2 Minutes. Do NOT start by trying to make baby vocalize. Start by connecting. The goal of Step 1 is to establish safety: session time = positive, your face = interesting, your mouth = fascinating. Only then will baby experiment with their own voice.
Position at Eye Level
12–18 inches away. Make eye contact and smile warmly. Wait 10 seconds. Just be present.
Exaggerated Facial Expressions
Open mouth wide. Stick out tongue. Puff cheeks. Big, slow, visible mouth movements — WITHOUT sound first. Let baby study your mouth.
Add Sound Slowly
Prolonged vowel: "Aaaaaah." Hold 3 seconds. Watch baby's face. Then pause and WAIT 5–10 seconds of silence. The pause creates space for baby to attempt sound.
Celebrate ANY Response
If baby makes any sound — coo, grunt, squeal, vowel — respond with IMMEDIATE delight: "Oh! You said something! What a beautiful sound!"
Parent Script: "Hi [baby's name]! Look at my mouth! Aaaaaah. [pause 5 sec] Aaaaaah. [pause] Ooooooh! [pause] Your turn! [wait 10 seconds in silence]"

Step 2: Engagement — Wake Up the Mouth
Minutes 2–5. Oral-motor activation prepares the lips, tongue, cheeks, and jaw for intentional speech movement. Think of this phase as warming up an athlete's muscles before competition. Three phases, each 1 minute.
Phase A: External Stimulation
Gently stroke baby's lips with clean finger or NUK brush — upper, lower, corners. Gently tap cheeks alternating left-right. Watch for enjoyment (smiling, opening mouth) or distress (turning away → STOP).
Phase B: Vibration Input
Offer vibrating teether near lips — not inside mouth initially. Let baby feel vibration on cheeks, chin, lips. Vibration activates proprioceptive receptors, increasing oral awareness and readiness.
Phase C: Blowing + Breath
Blow bubbles at eye level. "Buh-bles!" emphasizing the "B." Pinwheel blowing. For 8+ months: hold pinwheel near baby's mouth for any breath output. Model "Bbbbb" with lips together, then release "ba!"
⚠️ STOP SIGNAL: If baby shows any oral distress — gagging, turning head consistently, crying — STOP. Return to Step 1 face-to-face. Oral defensiveness requires professional OT desensitization before this phase continues.
Step 3: The Babbling Activation Protocol
Minutes 5–12. The core vocal stimulation. Use the Sound Ladder — always starting at the rung that matches your baby's current level. Never skip rungs. Celebrate every attempt on every rung.
Rung 1: Vowel Sounds (Start Here)
Face baby. "Aaaaaah" with big mouth. Pause 5 sec. "Ooooooh" with rounded lips. "Eeeeeee" with spread lips. Accept ANY vocal response — grunt, squeal, cough-turned-sound all count. Immediately deliver reward after ANY sound.
Rung 2: Consonant-Vowel Combinations
At mirror: "Ba...ba...ba" with slow, exaggerated lip closure. "Ma...ma...ma" with visible lip press. "Da...da...da" with tongue touching palate. Pause 5–10 sec between each model. Wait for any attempt. Puppet models alongside you.
Rung 3: Varied Combinations
Mix: "bada," "maba," "dama." Deliver in different ways: singing, whispering, excited voice. Multiple family members modeling (generalization). This rung is only when canonical babbling has emerged.
Rule 1
ONE attempt at a time. Say sound ONCE. Wait.
Rule 2
CELEBRATE EVERYTHING. Any vocalization is victory.
Rule 3
5–8 sound models per session with pauses between each.
Rule 4
STOP before baby is tired. 7 engaged minutes beats 15 forced minutes.

Step 4: Repeat & Vary — 5 Rotation Strategies
Variety prevents habituation — baby's brain responds to novelty with increased attention and vocalization. Rotate through 2–3 of these strategies each session. Pick 5–8 models per rotation. Total session: 5–12 minutes.
Musical Babbling
Shake maraca + sing "Ba-ba-ba!" Pause. Offer maraca. Any sound while holding it = major celebration with dancing and delight.
Mirror Babbling
Both face mirror. Point to your mouth: "Watch! Ma-ma-ma!" Point to baby's mouth. Wait. Both of you watching both mouths creates a powerful feedback loop.
Puppet Babbling
Puppet approaches: "I'm going to say ba-ba-ba!" Exaggerated mouth movements. Puppet celebrates any baby sound and looks at baby expectantly before each model.
Recording Babbling
Record yourself saying "da-da-da." Play back. Then say it live. Record baby's sounds and replay immediately. Instant fascination and self-recognition.
Peek-a-Boo Babbling
Hide behind cloth. Pop out: "[Name]! Ba!" Hide. Pop out: "Ma!" Anticipation + surprise reliably triggers vocalization attempts in most babies.
Satiation signal (stop when): Baby turns away, fusses, eyes glaze, or 12+ minutes have elapsed. Ending on a positive moment makes the next session easier to start.

Step 5: Reinforce & Celebrate — Every Sound Is a Victory
Timing is everything. Reinforcement must arrive within 1–3 seconds of any vocalization. Delayed reinforcement does not work with infants — the connection between the behavior and the reward must be immediate for the brain to link them.
Social Reinforcement (Always Free)
Wide smile + eye contact + "Oh! You made a sound!" Gentle clapping. Imitation: baby says "aah," you say "aah" back with delight. Social reinforcement is the most powerful and generalizes everywhere.
Activity Reinforcement
Blow bubbles immediately. Spin pinwheel. Shake maraca together. Peek-a-boo round. Activity reinforcers are highly motivating and maintain engagement across the session.
Tangible Reinforcement
Show sparkly toy for 5 seconds. Offer vibrating teether. Activate sound-responsive toy. Use tangibles early in training; fade as social reinforcement takes over.
"OH! Did you hear that? You said 'aaah!' AMAZING!"
"[Name] is using their voice! More bubbles for that beautiful sound!"
"You went 'mmmm!' Your mouth is learning!"
Fading Plan: Reinforce EVERY sound first. After 2–3 weeks → every 2nd–3rd sound → primarily social reinforcement. Goal: babbling becomes self-reinforcing through auditory feedback. You are teaching baby that their voice is wonderful — then that lesson runs on its own.

Step 6: Cool-Down & Transition — Ending Right
How you end a session determines how eagerly baby accepts the next one. A gentle, predictable closing ritual signals: this experience is safe, complete, and wonderful. It will happen again.
Signal Ending (30 seconds before)
"Two more sounds, then all done!" Predictability reduces resistance and gives baby closure without surprise.
Final Model
One slow, gentle "Aaaaaah" together. No pressure. No expectation. Just shared sound.
Calming Activity
Gentle rocking, soft humming, quiet holding. Let the nervous system settle from the stimulation of the session.
Put-Away Ritual
"Bubbles going night-night. Mirror going night-night." Naming what's being put away builds routine and language exposure.
Final Celebration
"You used your voice today. So proud of you, [name]." Close with warmth and specificity — not generic praise, but honoring the exact thing that happened.
Post-Session Practice: Continue responding to ANY vocalization all day long. Structured sessions prime the pump — but real learning happens during spontaneous babbling in the bath, during diaper changes, during play. Every moment is a therapy moment.
Track Progress: What Gets Measured Gets Improved
Consistent data collection is what separates guessing from knowing. These simple tracking fields take less than 2 minutes per session and give you — and any professional you consult — a clear picture of your baby's trajectory over time.
Field | Record | |
Date & Time | ___/___ /___ at ___:___ | |
Session Duration | ___ minutes | |
Rotations Used | Musical / Mirror / Puppet / Recording / Peek-a-boo | |
Sound Models Given | ___ (target: 5–8 per rotation) | |
Baby's Vocalizations | Vowels: ___ / CV attempts: ___ / Canonical: ___ | |
New Sounds | ___ | |
Baby's Engagement | High / Medium / Low / Refused | |
Session Quality | Great / Good / Modified / Postponed |
Weekly Summary: Total vocalizations ___ | % sessions with CV attempts ___% | New sounds this week ___ | Trend: Improving / Stable / Declining
GPT-OS® tracks the full progression arc: Pre-vocal → Cooing → Early Babbling → Canonical Babbling → Variegated Babbling → Jargon. Each stage is mapped against 21M+ session patterns to generate personalized recommendations.

Troubleshooting: When It's Not Working
Every baby will present unique challenges. These 7 solutions address the most common obstacles parents encounter in the first 8 weeks. If your concern isn't listed here, call 9100 181 181 for free teleconsultation.
Problem 1: Baby doesn't attend to face or sounds
Fix: Approach from the side. Use a sparkly toy near your face as a lure. If consistent avoidance of face-to-face interaction persists — note for professional evaluation. This pattern warrants a developmental screen.
Problem 2: Baby cries during oral-motor stimulation
Fix: Oral defensiveness. STOP all oral-motor work immediately. Focus ONLY on positioning + mirror + music for 2 weeks. Seek OT evaluation. Do not push through distress.
Problem 3: Baby makes sounds alone but not during sessions
Fix: Performance anxiety or overstimulation. Reduce structure dramatically. Respond to incidental vocalizations during independent play. Solo babbling = the motor system works. Build from there.
Problem 4: Only vowels after 4 weeks — no consonants
Fix: Progress! Increase oral-motor warm-up duration. Focus first on bilabial consonants ("ba," "ma") — baby can SEE your lip movement. Tongue sounds come later. Vowels mean the vocal motor system is activating.
Problem 5: Family members don't follow protocol
Fix: Share the simplified Family Guide. Core message: "When baby makes a sound — get excited and smile. That's it." Consistency across caregivers dramatically improves generalization.
Problem 6: Babbles for one person only
Fix: Context-specific learning — normal early stage. Have the primary person present during sessions with the new caregiver, then gradually fade out. Transfer takes 1–2 weeks.
Problem 7: No improvement after 6+ weeks
Fix: Professional evaluation trigger. Call 9100 181 181 for free teleconsultation. Do NOT wait more than 8 weeks without professional input. Early escalation is always better than prolonged waiting.
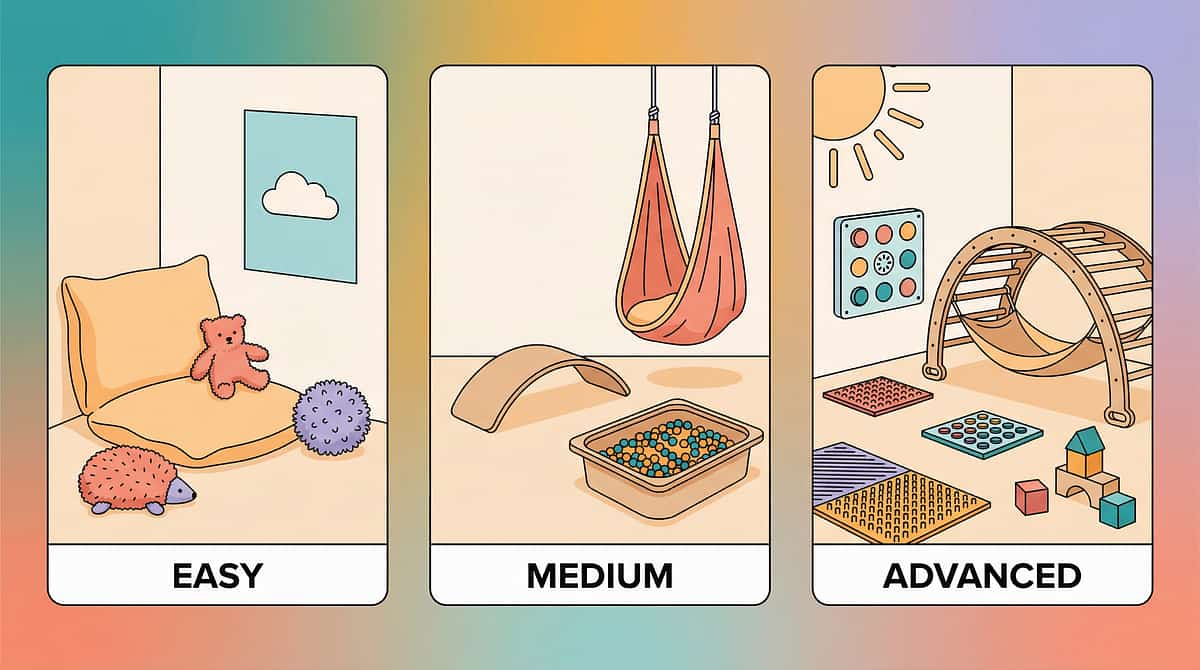
Adapt to Your Child: The Difficulty Slider
One protocol does not fit all babies. Use these three tiers — plus profile modifications — to ensure your sessions are appropriately calibrated for your child's exact developmental level, sensory profile, and physical presentation.
⬇️ EASIER (4–6 months or just starting)
Face-to-face positioning ONLY. Vowels only — no consonant targets yet. 3–5 sound models per session. 3-minute sessions maximum. Social reinforcement only — no tangibles needed.
⬜ STANDARD (7–12 months)
Full protocol: positioning + oral-motor + vocal stimulation. CV models at mirror. 5–8 models × 2–3 rotations. 5–12 minute sessions. Multi-type reinforcement as needed.
⬆️ ADVANCED (12–18 months or already babbling)
Variegated babbling focus. Turn-taking sequences. Word approximations targeted. Multiple settings and callers for generalization. 10–15 minute sessions. Primarily social reinforcement.
🌟 Sensory Seeker
MORE vibration, louder instruments, bigger reactions, simultaneous multi-sensory input. These babies thrive on intensity.
🌊 Sensory Avoider
Whispered models, soft instruments, dim lighting, increased distance (2 ft). Let baby approach YOU. Reduce all intensity.
👂 Hearing Aids / Cochlear Implants
Ensure devices are ON. Position on better-hearing side. Exaggerate visual mouth cues. Work with audiologist on protocol timing.
💪 Down Syndrome / Low Tone
Extended oral-motor warm-up. Lip closure + jaw stability focus. Extra positioning support. Allow more time between models.

ACT IV — THE PROGRESS ARC
Week 1–2: The Foundation Phase — What to Expect
The first two weeks are an investment phase, not a results phase. You are building the neural and emotional foundation that makes everything else possible. Manage your expectations with clinical precision: these are normal benchmarks for weeks 1–2.
✅ WILL LIKELY SEE
• Baby tolerating sessions without fuss
• Increased visual attention to your mouth
• Some overall vocalization increase
• Brief vocal turn-taking moments
• Positive affect during sessions — smiling, engagement
• Increased visual attention to your mouth
• Some overall vocalization increase
• Brief vocal turn-taking moments
• Positive affect during sessions — smiling, engagement
❌ PROBABLY NOT YET
• Consistent CV babbling
• Immediate imitation
• Babbling on demand
• Socially-directed vocalizations
• Dramatic changes in vocal frequency
• Immediate imitation
• Babbling on demand
• Socially-directed vocalizations
• Dramatic changes in vocal frequency
Data Benchmark: 0–15% of sound models resulting in any vocal response is completely normal for weeks 1–2. These weeks are about building the association: session time = positive, face = interesting, mouth = fascinating. You are investing, not failing.
