
Every Car Ride Is a Battle Your Child Doesn't Choose to Fight
The pale face before you've even left the driveway. The white-knuckled grip on the seat. The plastic bags always within arm's reach. The family vacation that ended before it began — seven stops, five episodes, one ruined trip. Your child isn't being difficult. Their vestibular system is sending distress signals that other children's brains simply don't generate. This is Motion Sickness — and it is physiological, not behavioral.
Vestibular-Aligned Motion Sickness Intervention Protocol: 9 Materials That Help
"You are not failing. Your child's nervous system is processing movement differently. And there is a combination of tools — not one magic fix, but a system — that can make travel possible again."
Sensory Processing
Vestibular Function
Travel Tolerance
Ages 2–12
Series Episode 78
🏛️Pinnacle Blooms Consortium: CRO · Pediatric OT · SLP · ABA · Special Education · NeuroDevelopmental Pediatrics

You Are Among Millions of Families Navigating This Exact Challenge
25–60%
Children Affected
Of all children experience motion sickness to some degree — one of the most common travel-related health issues in paediatric populations worldwide.
2–12
Peak Age Window
The vestibular system is still maturing during these years. Susceptibility peaks in this window and typically decreases as sensory integration pathways develop.
155M+
Indian Children Affected
Estimated 65–155 million Indian children experience some degree of motion sensitivity — significant given India's reliance on winding roads and long-distance road travel.
Motion sickness is not rare. It is not unusual. It is not a sign of weakness, anxiety, or behavioural manipulation. The American Academy of Paediatrics recognises kinetosis as a genuine physiological condition involving the vestibular, visual, and autonomic nervous systems. An estimated 150–360 million children worldwide experience it. Your family is not navigating this alone. Slightly higher prevalence occurs in girls than boys, with strong hereditary components — if you experienced motion sickness as a child, your child is significantly more likely to as well.
📖Research Citation: PRISMA Systematic Review (2024): 80% of children diagnosed with ASD display sensory processing difficulties, with vestibular processing being a primary affected domain. Meta-analysis across 24 studies confirms sensory integration therapy effectively addresses vestibular processing challenges. References: PMC11506176 | PMC10955541 | DOI: 10.12998/wjcc.v12.i7.1260
The Sensory Conflict Your Child Cannot Control
The Neurological Pathway
The vestibular apparatus in each inner ear contains three semicircular canals detecting rotational movement, and two otolith organs detecting linear acceleration and gravity. During vehicle travel, these structures correctly detect acceleration, deceleration, turns, and bumps.
Simultaneously, the visual system — focused on the stationary car interior — reports no movement. This visual-vestibular mismatch reaches the vestibular nuclei in the brainstem, which interprets the conflict as potentially toxic exposure — an evolutionary protective mechanism. The brainstem activates the vagus nerve, triggering the autonomic nausea response: pallor, cold sweats, salivation, and eventually vomiting.
In Plain Language
Their inner ear tells their brain: "We are moving forward at 40 km/h, turning left, going over bumps."
Their eyes, looking at the seat in front of them, tell their brain: "Nothing is moving. We are still."
The brain receives both messages and panics. In evolutionary terms, the only time your senses disagree this dramatically is when you've ingested something toxic. So the brain's protective response kicks in: "Get rid of whatever is in the stomach. Now."
This is a wiring difference, not a behaviour choice. Your child's brain is doing exactly what it's designed to do — protect them from perceived danger. The problem is that the danger isn't real, but the response absolutely is.
📖Research Citation: Frontiers in Integrative Neuroscience (2020): Comprehensive neurological framework establishing sensory conflict as the primary mechanism of motion sickness, with vestibular-visual integration deficits identified as the core pathway. DOI: 10.3389/fnint.2020.556660

Your Child Is Here. Here Is Where We're Heading.
The vestibular system continues maturing throughout childhood and into early adolescence. Understanding where your child sits on this developmental arc helps set realistic expectations — and reveals why targeted intervention during this window matters so much.
1
Birth–1 Year
Vestibular system developing. Basic head control emerges.
2
2–4 Years
⚠️ ONSET ZONE. Motion sickness symptoms begin. Mature walking established.
3
4–8 Years
🔴 PEAK SEVERITY WINDOW. School bus issues, car sickness most frequent. Current challenge zone.
4
8–10 Years
Natural improvement begins. Interventions accelerate resolution.
5
10–12 Years
Significant improvement for most. Self-management skills building.
6
Adolescence
Resolution for most children. Some individuals remain susceptible.
Motion sickness rarely travels alone. Children with severe kinetosis often also experience other vestibular processing differences (balance challenges, movement avoidance or seeking), anxiety about travel and novel situations, and sensory processing sensitivities in other domains. For some children, it's an early indicator of broader sensory integration differences. The interventions in this technique accelerate natural resolution and make the waiting years livable — not just survivable.
📖Research Citation: WHO Care for Child Development (CCD) Package: Age-specific evidence-based caregiver recommendations implemented across 54 low- and middle-income countries. References: PMC9978394 | WHO/UNICEF CCD Package (2023)

Clinically Validated. Home-Applicable. Parent-Proven.
🛡️ Evidence Level II-B
Moderate Evidence, Multiple Modalities
Acupressure Effectiveness
Multiple RCTs demonstrate P6 acupressure reduces nausea severity and vomiting frequency in motion sickness, with paediatric studies showing 60–70% of children reporting symptom improvement.
Ginger Supplementation
A systematic review of 12 controlled trials confirms ginger reduces nausea scores in motion provocation studies. Bioactive gingerols and shogaols demonstrate anti-emetic activity through 5-HT3 receptor antagonism.
Visual-Vestibular Alignment
Consistent evidence shows visual horizon fixation reduces sensory conflict duration and nausea severity by up to 50% compared to fixed-interior visual conditions.
Multi-Modal Superiority
Clinical consensus confirms combined interventions (3–4 simultaneous strategies) outperform single-modality approaches. Children receiving structured vestibular interventions at Pinnacle demonstrate 97%+ measurable improvement across readiness indexes.
📖Research Citations: PRISMA Systematic Review (Children, 2024): PMC11506176 | Indian RCT (Padmanabha et al., 2019): DOI: 10.1007/s12098-018-2747-4

Vestibular-Aligned Motion Sickness Intervention Protocol
Parent-Friendly Name: "The Travel Toolkit — 9 Materials That Make Car Rides Possible"
This is a multi-modal intervention protocol combining 9 categories of materials and strategies that work together to reduce motion sickness (kinetosis) in children aged 2–12 years. Rather than relying on a single remedy, this protocol addresses motion sickness from three directions simultaneously:
1
Reduce Sensory Conflict
Materials 2, 4, 7 — reducing the conflict between what the eyes see and what the inner ear feels.
2
Physiological Relief
Materials 1, 3, 5, 6 — providing direct nausea relief through acupressure, ginger, aromatherapy, and cooling.
3
Reduce Anticipatory Anxiety
Materials 8, 9 — reducing anxiety and anticipation that amplify symptoms before and during travel.
🧠 Domain
Sensory Processing · Vestibular Function
👶 Age Range
2–12 years
⏱️ Duration
15–60 min pre-travel + during travel
🔄 Frequency
Every travel event + daily vestibular activities

This Technique Crosses Therapy Boundaries — Because the Brain Doesn't Organise by Therapy Type
Occupational Therapist (Primary Lead)
The OT is the vestibular expert. They assess your child's sensory processing profile, determine whether motion sickness is part of a broader vestibular processing pattern, design desensitisation protocols, and select the specific combination of materials optimised for your child. The OT understands that motion sickness is a window into how your child's entire sensory system processes movement information.
NeuroDevelopmental Paediatrician
Evaluates whether motion sickness exists as an isolated vestibular sensitivity or as part of a broader neurodevelopmental profile. Rules out medical conditions mimicking motion sickness. Prescribes medication for severe cases unresponsive to non-pharmaceutical intervention.
Board Certified Behaviour Analyst (BCBA)
Addresses the anxiety-nausea cycle using antecedent-based interventions. Develops desensitisation protocols through graduated exposure. Creates reinforcement schedules for successful travel experiences. Manages avoidance behaviours that develop around travel.
Special Educator
Ensures school-based travel accommodations for field trips and bus transport. Creates visual supports for travel preparation. Communicates with school staff about positioning and material needs during school-related travel.
📖Research Citation: Adapted UNICEF/WHO Nurturing Care Framework for SLPs (2022): Multiple disciplines contributing to responsive caregiving components across developmental domains. DOI: 10.1080/17549507.2022.2141327

This Isn't a Random Activity. It's a Precision Tool.
Observable behaviour indicators tell you whether this protocol is working: your child completes a car ride without vomiting; face colour stays normal during the trip; your child asks to go somewhere that requires driving; your family completes a trip without emergency stops. These functional milestones — not clinical abstractions — are what success looks like on the ground.
📖Research Citation: Meta-analysis (World J Clin Cases, 2024): Sensory integration therapy effectively promoted social skills, adaptive behaviour, sensory processing, and motor skills across 24 studies. PMC10955541
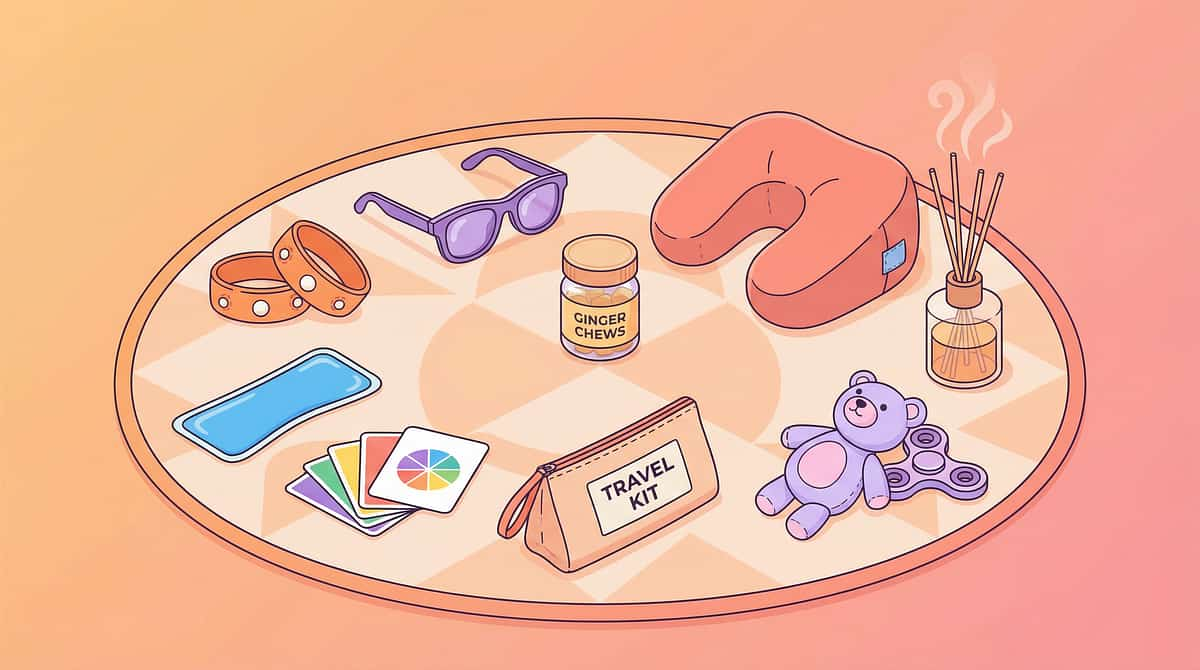
Your Motion Sickness Toolkit — 9 Materials, One System
These 9 material categories work together as a system. The starter set (Materials 1, 3, 8) can begin this week for under ₹2,600. The full toolkit, at ₹1,800–₹14,900, delivers the complete multi-modal protocol. 🏷️ Pinnacle Recommends materials 1, 3, 4, 5 as clinically validated first-line interventions.
# | Material | What It Does | Price (INR) | Buy | |
1 🏷️ | Acupressure Wristbands (Sea-Band or equivalent, child-size) | Stimulates P6 point to reduce nausea via pressure therapy | ₹200–600 | ||
2 | Motion Sickness Glasses (liquid-horizon technology) | Aligns visual and vestibular input to resolve sensory conflict | ₹1,500–4,000 | ||
3 🏷️ | Ginger Products (real ginger candies, chews, biscuits) | Natural anti-emetic via 5-HT3 receptor antagonism | ₹100–500 | ||
4 🏷️ | Positioning Supports (booster seat, neck pillow, head stabiliser) | Stabilises head and improves forward visual orientation | ₹500–3,000 | ||
5 🏷️ | Aromatherapy Materials (peppermint inhaler, lavender roll-on, citrus diffuser) | Grounding olfactory input; may directly reduce nausea | ₹200–1,000 | ||
6 | Cooling Aids (portable fan, cooling towel, misting fan) | Reduces autonomic overactivation; fresh air reduces nausea | ₹200–1,500 | ||
7 | Visual Focus Materials (window games, car bingo, audio entertainment) | Redirects gaze outward; audio eliminates screen-based conflict | ₹100–800 | ||
8 | Pre-Travel Preparation Kit (organised bag with all supplies) | Reduces anticipatory anxiety; ensures materials are accessible | ₹300–1,500 | ||
9 | Distraction & Calming Materials (headphones, audiobooks, tactile fidgets) | Reduces anxiety overlay and keeps nervous system regulated | ₹200–2,000 |
Total Investment Range: ₹1,800–₹14,900 (full toolkit) | Essential Starter Set (Materials 1, 3, 8): ₹600–₹2,600

Material 1: Acupressure Wristbands
How It Works
Commercial acupressure bands (such as Sea-Band in child size) contain a small plastic button that applies firm, continuous pressure to the P6 (Nei-Kuan) acupoint, located on the inner wrist. This acupoint has been used for centuries in traditional medicine and is now supported by multiple randomised controlled trials demonstrating 60–70% of children report symptom improvement when it is properly stimulated.
The proposed mechanism involves the stimulation of nerve pathways that modulate the brainstem's nausea response — essentially interrupting the signal chain between the vestibular conflict and the vomiting centre.
How to Use It
Finding P6: Place three of your child's own finger-widths from the wrist crease, between the two central tendons on the inner forearm. The P6 point is precisely there.
Application timing: Apply bands 15–30 minutes before departure for best effect. Both wrists.
DIY alternative: Locate P6 and apply firm, steady pressure manually. Or wrap a firm button against the point with a hair tie or elastic band — free and often surprisingly effective.
Safety note: Bands must be snug, NOT tight enough to restrict circulation. Check fingers for colour changes during the trip.

Material 2: Motion Sickness Glasses
How They Work
Motion sickness glasses use liquid-horizon technology — coloured liquid in transparent frames creates an artificial horizon line that the wearer's visual system can track. By providing the eyes with a moving reference that matches what the vestibular system is sensing, these glasses resolve the core visual-vestibular mismatch that causes nausea.
Put them on at departure. Most children can remove them after 10–15 minutes once their vestibular system stabilises, having used the glasses to "bridge" the highest-conflict first phase of the journey.
Price: ₹1,500–₹4,000 | Available on Amazon.in
If You Can't Buy Them
No effective DIY alternative exists for the liquid-horizon technology itself. However, the same principle can be approximated: direct your child's gaze to the road ahead or distant passing scenery. Seeing real movement outside achieves visual-vestibular alignment without the technology.
Position matters: If your child can see the horizon or the road ahead, they are achieving the same basic alignment principle these glasses were engineered to deliver.
Best used for: Severely affected children on longer journeys; the first 10 minutes of any trip.

Material 3: Ginger Products
The Science Behind Ginger
Ginger (Zingiber officinale) is one of the most well-studied natural anti-emetics in paediatric medicine. A systematic review of 12 controlled trials confirms its effectiveness in reducing nausea scores in motion provocation studies. The bioactive compounds — gingerols and shogaols — exert anti-emetic activity through 5-HT3 receptor antagonism and gastrointestinal motility modulation. In plain terms: ginger interferes with the signal pathways that cause vomiting.
How to Use It
Timing: Give ginger 30–60 minutes before departure. The anti-emetic effect takes time to establish.
Forms (choose what your child tolerates):
- Ginger candies or hard sweets (widely available)
- Ginger chews (moderate flavour, easy to carry)
- Ginger biscuits (mildest flavour — good starting point)
- Ginger ale made with real ginger (not artificial flavouring)
DIY: Grate fresh ginger into hot water, cool, sweeten with honey (children over 1 year only). Fresh ginger chewed directly also works — taste is strong but effective. Home-baked ginger biscuits are an excellent budget option.
Safety: Safe in food amounts. Not recommended for children under 2 without medical guidance. Start with small amounts to assess tolerance.

Material 4: Positioning Supports
Why Position Matters
Head stability is underestimated as a motion sickness intervention. When a child's head is unsupported and moves independently with every bump and turn, the vestibular system receives a cascade of conflicting micro-signals. Stabilising the head in a forward-facing, upright position dramatically reduces this noise.
Elevating the child so they can see out of windows is equally critical — it enables the visual horizon fixation that counteracts sensory conflict. A child slumped below window level, staring at the seat back, is in the worst possible visual condition for a motion-sensitive nervous system.
Optimal Positioning
Best seat position: Middle back seat (best forward view) OR front passenger seat if age-appropriate and legal in your jurisdiction.
What to use: Age-appropriate booster seat, travel neck pillow, head stabiliser, or firm cushions to elevate and support.
DIY: Rolled towels or blankets to stabilise head position. Stack firm cushions to elevate so child can see out of windows. Position child in the middle back seat for the best unobstructed forward view.
Price: ₹500–₹3,000
⚠️Safety First: ALL positioning must comply with car seat safety laws for your child's age, weight, and height. NEVER compromise safety for comfort.

Material 5: Aromatherapy Materials
How Aromatherapy Helps
Scent provides immediate, powerful grounding input to the nervous system via the olfactory nerve — one of the most direct sensory pathways to the brain. Peppermint in particular has a sharp, cooling quality that many children find nausea-interrupting. Lavender provides calming input that counters the anxiety component of motion sickness. Citrus scents offer bright, alerting input.
While robust RCT evidence specifically for paediatric travel aromatherapy is limited, clinical use across vestibular therapy settings and caregiver-reported outcomes consistently support it as a useful adjunct — particularly in the moment-of-need intervention sequence.
How to Use It
Timing: Offer aromatherapy inhaler within 60 seconds of any early symptom signs.
Options:
- Peppermint inhaler stick (₹200–500) — most portable
- Lavender roll-on (pre-diluted for children) — apply to wrist
- Citrus diffuser pendant worn around the neck
DIY: Drops of peppermint or lavender oil on a cotton ball stored in a small sealed container. Fresh mint leaves in a cloth bag. Lemon peel in a zip bag. Child sniffs when needed.
Safety: ALWAYS diluted for children. Never apply undiluted oil to skin. Keep away from eyes. Test for sensitivity first (small amount on forearm, wait 24 hours).

Material 6: Cooling Aids
Why Cooling Works
Heat intensifies motion sickness significantly. The autonomic nervous system, already dysregulated by the vestibular-visual conflict, is further overloaded by thermal stress. Keeping a motion-sensitive child cool activates the parasympathetic nervous system — the body's "rest and digest" counterpart to the nausea-triggering "fight or flight" response.
Fresh air — even a crack in the window — is one of the most consistently reported helpful interventions by parents worldwide. It provides cooling, increased oxygen flow, and a mild proprioceptive grounding effect.
Your Cooling Arsenal
- Portable battery fan (₹200–800): Direct airflow to face. Charge before every trip.
- Cooling towel (₹200–400): Pre-activate with water. Apply to forehead or back of neck.
- Misting fan (₹500–1,500): Combined cooling and moisture.
DIY (₹0): Open windows (even a crack helps enormously). Frozen water bottles wrapped in cloth as cooling packs. Direct car AC vents toward the child. Wet cloth for forehead and neck.
Safety note: Portable fans must have appropriate child-safe guards. Ensure secure positioning so the fan cannot fall or be grabbed by small hands.
Material 7: Visual Focus Materials
The Visual Principle
The fundamental rule: eyes forward and outside, not on interior fixed objects. Any activity that keeps a child's gaze directed out of the window — at the horizon, the moving landscape, the passing road — actively reduces the visual-vestibular mismatch that causes nausea.
Conversely, looking at books, tablets, or any fixed item inside the vehicle while the vehicle moves is one of the single most powerful triggers for motion sickness. The transition away from in-vehicle screens is often the most impactful single change a family can make.
What to Use
Window games (best option):
- "I Spy" focused entirely on things outside
- Counting specific objects: blue cars, motorcycles, trees, cows
- Verbal storytelling set in the landscape they're passing through
- Car bingo with outdoor objects
Audio entertainment (critical replacement for screens):
- Downloaded audiobooks (age-appropriate)
- Children's podcasts or radio
- Music and singing together
The key principle: audio only — not visual screens. This is the most important behavioural change in the entire protocol. It will require transition support, but it is clinically critical.
Material 8: Pre-Travel Preparation Kit
Why a Kit Changes Everything
The preparation kit serves dual purposes: it ensures all materials are accessible in the moment they're needed, and it dramatically reduces anticipatory anxiety — for both child and parent. When your child sees the familiar bag being assembled, it signals safety and control. When you know everything is ready, you travel with calm instead of dread.
A chaotic scramble for supplies when a child is already symptomatic is the worst possible scenario. The kit eliminates that scramble by making preparation automatic.
Rule: Keep it permanently in the car. Refresh after each use. It should live in the vehicle, not in the house.
Kit Contents Checklist
- Plastic/sick bags (minimum 5) — accessible on the seat, NOT inside the bag
- Change of clothes (full set)
- Small towels (2–3)
- Wet wipes (large pack)
- Water bottle
- Ginger products (candies, biscuits)
- Aromatherapy inhaler or cotton ball container
- Spare acupressure bands
- Cooling towel
- Child's preferred fidget or comfort item
Price: ₹300–₹1,500 depending on bag choice and materials included.
DIY: Any dedicated bag works. The organisation and consistency matter more than the bag itself.

Material 9: Distraction & Calming Materials
The Anxiety-Nausea Cycle
Motion sickness and anxiety form a self-reinforcing cycle. Anticipatory anxiety activates the autonomic nervous system before the vehicle even moves, lowering the child's nausea threshold from the start. The memory of past sickness generates fear. The fear generates physiological arousal. The arousal amplifies motion sensitivity. Each bad trip makes the next one more likely to be bad.
Breaking this cycle requires addressing the anxiety component directly — not just the physical sensation. Calming materials work at the nervous system level to reduce baseline arousal before and during travel.
What to Use
- Over-ear headphones: Provide auditory immersion and gentle proprioceptive input to the head. Combine with audiobooks or music.
- Audiobooks and podcasts: Keep cognitive engagement high without requiring any visual effort.
- Tactile fidgets: Stress balls, textured rings, koosh balls — provide regulated sensory input that calms the nervous system.
- Comfort item: Familiar stuffed animal or blanket — olfactory and tactile familiarity grounds an anxious child.
DIY (₹0): Conversation. Singing together. Verbal storytelling. 20 Questions. Downloaded audio on the parent's phone. The key is audio-only — no screens.
Price: ₹200–₹2,000

DIY & Substitute Options — Every Parent Can Start Today
The WHO/UNICEF equity principle in action: every family, regardless of economic status, can execute this technique with household items.
Material | Buy This | Make This (₹0 Cost) | |
Acupressure Bands | Sea-Band child-size (₹200–600) | Locate P6 point: 3 finger-widths from wrist crease between two tendons. Apply firm pressure manually, or wrap a firm button against the point with a hair tie. | |
Motion Glasses | Liquid-horizon glasses (₹1,500–4,000) | No effective DIY exists. Instead: have child look out the window at distant passing scenery. Same visual-vestibular alignment principle. | |
Ginger Products | Ginger candies/chews (₹100–500) | Grate fresh ginger into hot water, cool, sweeten with honey. Home-baked ginger biscuits. Even chewing a small piece of fresh ginger works. | |
Positioning | Booster seat/neck pillow (₹500–3,000) | Rolled towels and blankets to stabilise head. Stack firm cushions to elevate. Middle back seat for best forward view. Safety first: all positioning must comply with car seat laws. | |
Aromatherapy | Essential oil inhaler (₹200–1,000) | Drops of peppermint or lavender on a cotton ball in a small sealed container. Fresh mint leaves in a cloth bag. Lemon peel in a zip bag. | |
Cooling | Portable fan (₹200–1,500) | Open windows. Wet cloth for forehead and neck. Frozen water bottles wrapped in cloth. Direct AC vents toward child. | |
Visual Focus | Window games (₹100–800) | "I Spy" outside. Counting specific objects (blue cars, trees). Verbal storytelling. Singing together. Free and often the most effective strategy. | |
Preparation Kit | Organised travel bag (₹300–1,500) | Any bag: plastic bags (5+), change of clothes, towels, wet wipes, water bottle, ginger, and materials. Keep permanently in the car. | |
Distraction | Headphones/audiobooks (₹200–2,000) | Conversation. Singing. 20 Questions. Downloaded audio on parent's phone. Audio only — not visual screens. |
✅Zero-Cost Version Possible: Positioning optimisation, fresh air, visual focus, ginger (if available at home), and verbal distraction are all completely free.

Safety Gate — Read This Before Your Next Trip
🔴 Do NOT Proceed If:
- Child has dizziness or nausea WITHOUT any motion — may indicate inner ear disorder
- Child has recently had a head injury or concussion
- Child has ear infection, ear pain, or hearing changes
- Symptoms include severe headache, vision changes, or loss of consciousness
- Child is under 2 years showing unusual distress during travel — investigate other causes
🟡 Modify and Monitor If:
- Child is currently ill (fever, stomach virus) — interventions won't help illness-induced nausea
- Child is extremely anxious about the trip — address anxiety first
- Child has recently eaten a heavy or greasy meal — wait 1–2 hours if possible
- Weather is extremely hot — increase cooling measures and reduce trip duration
🟢 Proceed If:
- Child is in their usual state of health
- Travel is planned (not emergency)
- Materials are prepared and accessible
- Parent is calm and prepared — your anxiety transfers to your child
Material-Specific Safety Reminders: Acupressure bands must be snug, not tight — check fingers for colour changes. Ginger: not for children under 2 without medical guidance. Essential oils: always diluted, never near eyes, test for sensitivity first. Positioning: ALL positioning must comply with car seat safety laws. Portable fans: child-safe guards only. Plastic bags: on the seat within arm's reach, NOT in the boot.
Your Vehicle Is Now a Therapy Environment. Set It Up Right.
The ★ optimal child position is the middle back seat (best forward view) OR front passenger seat if age-appropriate and legal in your jurisdiction.
Temperature
Cool the vehicle before child enters. Set AC to cool, not cold. Crack a window slightly for fresh air flow.
Position Child
Elevate with appropriate booster or cushions so they can see out of windows. Head supported and stable.
Apply Acupressure Bands
On both wrists, button pressing the P6 point. 15–30 minutes before departure is ideal.
Give Ginger
Ginger candy or chew 30–60 minutes before departure.
Prep Remaining Materials
Aromatherapy ready and accessible. Cooling fan charged. Plastic bags on the seat. Audio entertainment loaded and tested. Preparation kit within arm's reach.
Remove Visual Temptations
No books, no tablets, no visual games visible. Audio only. Parent check: you are calm, you have a plan, you are prepared for anything.
The 60-Second Pre-Travel Assessment
Before every trip, run through this quick readiness check.
1
Fed Appropriately?
Light meal 1–2 hours before travel. Not empty stomach, not full stomach. Avoid greasy, heavy, or strong-smelling foods.
2
Rested?
A tired child is a more motion-sensitive child. Avoid travel during overtired periods where possible.
3
Regulated?
Child is in a calm, baseline state. Not post-meltdown, not highly excited, not crying.
4
Healthy?
No current illness, no fever, no recent vomiting from other causes.
5
Hydrated?
Small amount of water available — dehydration worsens nausea.
6
Materials Ready?
All 9 categories checked and accessible per the vehicle setup guide.
✅ GO (5–6 checks)
Proceed with full protocol.
⚠️ MODIFY (3–4 checks)
Shorter route, extra breaks planned, simplified protocol (bands + ginger + positioning only).
🛑 POSTPONE (0–2 checks)
If discretionary, reschedule. If necessary, use minimal protocol with maximum compassion.

Step 1 — Inviting Your Child Into the Travel Experience
Step 1 of 6
2–5 minutes before entering vehicle
Calm, positive, matter-of-fact
"We're going to [destination] today. I've got your travel toolkit all ready. Your wristbands are here — want to put them on? And here's your ginger candy for the road. Your fan is charged, your window will be open, and I downloaded two new audio stories for the drive. We're prepared for a great trip."
Body Language Guidance
- Calm, unhurried energy — don't rush the preparation
- Let the child participate: putting on their own bands, choosing their ginger product
- Do NOT ask "Are you going to be sick?" or "Do you feel okay?" — this primes anxiety
- Be matter-of-fact: this is routine preparation, not crisis management
When Your Child Resists
Verbal refusal: Don't force. Offer choice within the protocol: "Do you want the ginger candy or the ginger biscuit?" — choice within the system, not opt-out of it.
Physical resistance (crying, clinging): Acknowledge fear. "I know car rides have been really hard. We have new tools today. Let's try them together."
Extreme distress: Assess whether trip can be shortened or postponed. Proceed only if necessary and with maximum compassion and support.

Step 2 — The Critical First 10 Minutes
Step 2 of 6
0–10 minutes after departure
Active monitoring + prevention
The first 10 minutes are when most motion sickness develops. If you can get through this window without symptoms, the trip has a strong chance of success.
1
Minutes 0–3
Start audio entertainment immediately. Begin conversation or singing. Point to things outside: "Look at that big truck!" Keep eyes oriented outward from the very start.
2
Minutes 3–5
Check acupressure band position — haven't shifted? Offer aromatherapy inhaler: "Want a sniff of your peppermint?" Ensure cool air is flowing toward the child.
3
Minutes 5–10
If motion glasses are being used, they're most valuable now. Watch for early pallor signals. Child can often remove glasses by minute 10–15 once their system stabilises.
😊 Engaged
Talking, looking outside, participating in audio/games. EXCELLENT — continue current approach.
😐 Tolerating
Quiet but not distressed, slightly still. ACCEPTABLE — increase distraction gently.
😰 Avoiding
Closing eyes, very still, swallowing frequently, face colour changing. CONCERNING — escalate to Step 3 immediately.

Step 3 — Active Symptom Management: When You See the Signs
Step 3 of 6
Execute within 60 seconds of early symptoms
When your child shows ANY early symptoms — pallor, quietness, frequent swallowing, yawning, loss of interest in conversation — execute these steps IN ORDER within 60 seconds.
Action 1 — AIR (Immediate)
Open the window nearest the child. If weather allows, fully open. Turn AC vent directly toward child's face. Activate portable fan and direct at their face.
Action 2 — LOOK (Immediate)
"Look out the window at that [distant object]." Point to something on the horizon. If the child has motion glasses, ensure they're on. Direct gaze to the road ahead or distant scenery.
Action 3 — BREATHE (Within 30 seconds)
"Take a slow, deep breath through your nose." Model it with them. Slow breathing activates the parasympathetic nervous system, counteracting the nausea response.
Action 4 — SCENT (Within 60 seconds)
Offer the aromatherapy inhaler or scented cotton ball. "Take a sniff of your peppermint." The sharp, cooling scent provides grounding input and may directly reduce nausea.
Action 5 — ASSESS (Within 2 minutes)
Has colour improved? Is the child responsive? If symptoms are stabilising, continue with all support measures active. If escalating despite intervention — STOP the vehicle safely.
📖Research Citation: Meta-analysis (World J Clin Cases, 2024): Structured therapeutic sessions with clear action sequences demonstrate maximum effectiveness. PMC10955541

Step 4 — For Longer Trips: Rhythm, Breaks, and Re-Application
Step 4 of 6
For trips over 30 minutes
The 20-Minute Check Cycle
Every 20 minutes on a longer trip, run through a mini-check:
- Is air still flowing toward the child?
- Is the child looking outside or has gaze drifted inward?
- Would another ginger candy help? (Offer, don't push)
- Is the acupressure band still positioned correctly?
- Are they engaged in audio entertainment or has it ended?
Planned Break Protocol
- Severely affected: Stop every 20–30 minutes initially
- Moderately affected: Stop every 45–60 minutes
- Mildly affected: Standard rest stops every 1.5–2 hours
A good break: Pull over safely. Child exits vehicle. Fresh air, standing, walking for 3–5 minutes minimum. Small sip of water if tolerated. Re-apply ginger if longer than 30 minutes since last one. Check band position. Child re-enters when ready — not rushed.
Maintain engagement: Change audio content. Switch from music to audiobook or vice versa. Change which window the child looks out of. Variety prevents habituation.

Step 5 — Every Successful Kilometre Is a Victory Worth Naming
Step 5 of 6
Reinforce during AND after the trip
"You've been riding for twenty minutes and you're doing amazing." | "Look at you — we're almost there and you look great!" | "That was a long drive and you handled it like a champion."
Reinforcement Rules
- Immediate. Specifically. Enthusiastically.
- Name the specific achievement: "You rode for 30 minutes without feeling sick!"
- Never compare to failures: NEVER "See? You can do it if you try."
- Celebrate the process, not just the outcome: "You used your peppermint inhaler all by yourself — that was so smart."
Post-Trip Reinforcement
- Favourite activity at the destination
- Verbal celebration: "We just drove to [place] together and made it!"
- Log it: mark successful trips on a family calendar (visual progress tracking)
- Let the child share: "Tell Daddy how our drive went today"
Travel Champion Chart: Each successful trip (defined by achievable criteria — NOT "no vomiting" but "used your tools") earns a sticker toward a chosen reward.
"Celebrate the attempt, not just the success."

Step 6 — When It Happens Despite Everything: The Calm Response
Step 6 of 6
The 5-Minute Emergency Reset
1
Minute 1 — STOP SAFELY
Pull over when safe. Don't panic. Don't express frustration. Your child is already feeling terrible — your calm is their anchor.
2
Minute 2 — AIR + EXIT
If safe, have the child exit the vehicle. Fresh air. Feet on solid ground. This immediately begins resolving the sensory conflict — stationary visual + stationary vestibular = agreement.
3
Minute 3 — CLEAN + CHANGE
Wipes for face and hands first (comfort before cleanliness). Change clothes if needed. Clean the vehicle area matter-of-factly — no drama, no sighing, no "again?"
4
Minute 4 — RECOVER
Small sips of water when ready. Fresh air continues. Aromatherapy inhaler if tolerated. Gentle conversation or silence — follow the child's lead.
5
Minute 5 — ASSESS + DECIDE
How far to destination? If symptoms have fully resolved and destination is close, re-enter with all measures active. If destination is far and child is significantly distressed — consider whether this trip is essential.
⛔What NEVER to Do: Never shame ("You ruined the trip"). Never minimise ("It's not that bad"). Never force continuation if the child is severely distressed. Never blame — this is physiological. Your child has no more control over this than over a sneeze.

60 Seconds of Data Now Saves Hours of Guessing Later
Record these three data points within 5 minutes of arriving at your destination after every trip.
1
Trip Duration Tolerated
How many minutes did the child travel before symptoms appeared? If no symptoms: record total trip duration. Example: "22 minutes symptom-free | 22 total trip minutes."
2
Symptom Severity
🟢 None | 🟡 Mild discomfort, no vomiting | 🟠 Nausea, stopped trip briefly | 🔴 Vomiting occurred. One mark, one minute — this is all you need.
3
Interventions Used
Note which of the 9 materials were deployed. Add a one-sentence note on what seemed to help most — this becomes your personalisation guide over time.
Where to Record
- 📱 GPT-OS® In-App Tracker
- 📄 Downloadable PDF Tracking Sheet
- 📓 Paper notebook kept in the preparation kit
Why It Matters
Progress in motion sickness intervention is often gradual — invisible to feeling but visible to data. Tracking trip-duration-to-symptoms over 10 trips reveals an improvement trend your memory cannot reliably hold. "Track to learn. Learn to adapt. Adapt to improve."

Session Abandonment Is Not Failure — It's Data
Troubleshooting the most common challenges
"Nothing worked. My child vomited within 5 minutes."
This may be a severe presentation requiring pharmaceutical support alongside these materials. Consult your paediatrician. Meanwhile, shorten all trips to under the vomiting threshold — even if that's 3 minutes — and build from there. The combination approach works for most children, but severity varies.
"My child refused to wear the acupressure bands."
Don't force. Try making them a "superhero bracelet" or let the child choose the colour. Some children prefer applying manual pressure themselves. The bands are one of 9 tools — skip temporarily and focus on the others.
"The ginger made my child gag."
Try ginger biscuits (milder taste), ginger ale with real ginger, or crystallised ginger coated in sugar. If all ginger is rejected, this tool can be skipped — the others compensate.
"My child won't look out the window — they insist on the tablet."
This is the single most important behavioural change to make. Screens in moving vehicles dramatically worsen motion sickness. Replace with audio entertainment. Start with audiobooks more engaging than the video content they're replacing. It will be a difficult transition but it is clinically critical.
"My child seems WORSE since we started trying these tools."
Possible causes: increased anticipatory anxiety (child is now hyperaware), too many new things introduced at once (overwhelming), or coincidental illness. Scale back to 2–3 tools only (positioning + air + ginger). Add one new tool per trip.
"My child is now afraid of ALL travel because of past experiences."
This is an anxiety overlay on the physiological condition. Start with extremely short, successful trips (5 minutes, destination has a reward) to rebuild positive associations. A BCBA can design a formal desensitisation protocol if avoidance is severe.
No Two Children Are Identical. Customise This Protocol.
1
Mild Motion Sickness
Occasional discomfort, rare vomiting. Essentials only: positioning + fresh air + ginger before long trips. Audio entertainment instead of screens. Apply for trips over 20 minutes.
2
Moderate Motion Sickness
Frequent nausea, occasional vomiting. Full protocol: all 9 materials deployed. Preparation kit always in car. Regular break schedule. Consider adding motion glasses. Apply for ALL trips.
3
Severe Motion Sickness
Vomiting on most trips, even short ones. Full protocol PLUS pharmaceutical support (consult paediatrician). Extremely gradual trip duration extension (add 2 minutes per week). Possible formal vestibular desensitisation programme with OT. Apply to every single trip, no exceptions.
Ages 2–3
Parent-managed entirely. Ginger only if age-appropriate. Focus on positioning and air. Simplified toolkit.
Ages 4–6
Child begins participating — choosing ginger product, using inhaler. Introduction of window games.
Ages 7–9
Child manages own bands, inhaler, fan. Can track symptoms verbally. Begins self-advocacy.
Ages 10–12
Self-management of most tools. Learning to predict and prevent. Building lifetime travel skills.

Weeks 1–2: Building the Baseline
Progress Stage 1
~15% of the journey
Progress in the first two weeks is real, even when it doesn't feel dramatic. You are establishing the system, building familiarity, and identifying which of the 9 tools your specific child responds to best.
✅ What IS Progress
- Child tolerates having materials present (bands on wrists, ginger accepted, fan available)
- Symptom onset may be delayed by even a few minutes compared to previous baseline
- Parent has a routine — preparation is faster and less stressful
- You're identifying which tools your child responds to most
⏳ What Is NOT Progress Yet
- Complete elimination of symptoms — too early
- Child requesting travel — unlikely yet
- Consistent results — you will have good trips and bad trips
Metric to track: Average minutes of symptom-free travel across your first 5–6 trips. If your baseline was "symptoms within 5 minutes" and you're now averaging 8–10 minutes, that is a 60–100% improvement in tolerance. Real progress, even if it doesn't feel dramatic.
"If your child tolerates the travel 3 minutes longer than last week — that's real progress."

Weeks 3–4: The Protocol Is Becoming Routine
Progress Stage 2
~40% of the journey
Child Consolidation Signs
- "Where's my ginger candy?" — the child is integrating tools into their own routine
- Child begins to anticipate and participate in pre-travel preparation
- Symptom-free travel duration is consistently longer than baseline
- Successful completion of previously impossible trips (e.g. a 20-minute drive completed without symptoms)
- Reduced anticipatory anxiety — child doesn't protest when told about upcoming travel
Neural Pathway Formation
The vestibular system is adapting. Repeated exposure to motion WITH successful symptom management teaches the brain that the sensory conflict is not dangerous. Each successful trip is a data point that retrains the nausea threshold. This is vestibular desensitisation happening in real life.
Parent Milestone
You may notice that preparation feels automatic now. You're less anxious before trips. Your toolkit is organised without thinking about it. That's YOUR progress — and your calm directly benefits your child. Two systems are growing simultaneously.
Weeks 5–8: Travel Is Becoming Possible
Progress Stage 3
~75% of the journey
Child completes previously impossible trips without vomiting on 3+ consecutive occasions
Anticipatory anxiety is minimal — child may still be cautious but is not distressed about upcoming travel
Child uses 2–3 tools independently — self-applies ginger, requests window down, uses inhaler
Family has completed a previously avoided activity — long drive, bus ride, family trip
Generalisation indicators: Child applies strategies in non-car settings (bus, taxi, train). Child communicates needs to other adults: "I need to sit where I can see out." Child has a preference profile: "Ginger works for me, but I don't need the glasses anymore."
What "Mastery" means here: Mastery does NOT mean motion sickness is cured. It means your family has a reliable system that makes travel possible and manageable. The goal is functional participation in life — not perfection.
🏆MASTERY UNLOCKED: When your family can plan a trip and your primary emotion is anticipation, not dread.
More Sensory Processing Techniques — Including Ones That Use Materials You Already Own
🔗 A-076: Materials for Movement Avoidance
Difficulty: Intro | Materials Overlap:✅ Positioning, Calming Materials

🔗 A-079: Materials for Noise Sensitivity
Difficulty: Intro | Materials Overlap:✅ Headphones, Calming Materials

🔗 A-080: Materials for Light Sensitivity
Difficulty: Intro | Materials: Sunglasses, Environmental Modifications

🔗 A-082: Materials for Activity Anxiety
Difficulty: Core | Materials Overlap:✅ Preparation Kits, Calming Materials
✅ = You already own materials for these techniques from your motion sickness toolkit. 🔗Browse All Sensory Processing Techniques

From Dread to Destination: Real Families, Real Progress
Family Vignette 1 — 6 Weeks
"Every car ride was a battle. He'd be green before we left the driveway, vomiting by the first traffic light. Then we got organised: the right seat position so he could see out, acupressure bands on before we started, a ginger chew, his special fan ready, window cracked, and audio stories instead of videos. It wasn't one thing — it was the combination. Now we can drive an hour with no incidents most of the time."
— Parent, Pinnacle Network (Illustrative; outcomes vary by child profile)
Family Vignette 2 — 8 Weeks
"School bus was impossible. I was driving her every single day. She missed three field trips last year. We worked with her OT on a bus-specific protocol — front seat, window, bands, peppermint inhaler, and absolutely no reading. Her teacher knows the routine now. She rode the bus to the science museum last month. First field trip in two years."
— Parent, Pinnacle Network (Illustrative; outcomes vary by child profile)
"Motion sickness responds remarkably well to systematic multi-modal intervention. The children who improve most are those whose families commit to the combination approach consistently — not looking for a single magic solution, but building a reliable system." — Occupational Therapist, Pinnacle Blooms Network
You're Not Navigating This Alone Anymore
Motion Sickness & Vestibular Support — WhatsApp Group
Connect with families managing the same challenge. Share tips, celebrate wins, ask questions. Join Group
Pinnacle Parent Forum — Sensory Processing Thread
Longer-form discussions, resource sharing, and therapist Q&A sessions. Visit Forum
Peer Mentoring
Connect with an experienced parent who's been through this journey. Your most valuable guide may be someone who was exactly where you are now. Request Peer Mentor
Local Pinnacle Parent Meetups
In-person connections at your nearest Pinnacle centre. Find Local Group
"Your experience helps others — consider sharing your journey."
Powered by GPT-OS® — Global Paediatric Therapeutic Operating System
What GPT-OS® Does With Your Data
Every trip you track feeds into the Diagnostic Intelligence Layer, which compares your child's pattern against population-level data from 21 million+ therapy sessions. This produces personalised recommendations that improve with each data point you contribute.
🔒 Privacy Assurance
Your child's data is protected under Indian Data Protection standards and ISO/IEC 27001 information security protocols. Data used for population-level analysis is de-identified and aggregated.
"Your data helps every child like yours."

From Reading to Doing. Your Child's Next Trip Can Be Different.
🟢 Start This Technique Today
GPT-OS® will walk you through your first trip preparation step-by-step, personalised to your child's age and severity level.
📞 Book a Consultation
Connect with a paediatric occupational therapist who specialises in vestibular processing.
Pinnacle Centre Booking | Call 9100 181 181
🔗 Explore Next Technique
Continue your sensory processing journey with the next technique in the series.
🏛️Validated by the Pinnacle Blooms Consortium — 🧩 OT · 🗣️ SLP · 🧠 ABA · 📚 SpEd · 🩺 NeuroDev
Preview of 9 materials that help with motion sickness Therapy Material
Below is a visual preview of 9 materials that help with motion sickness therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.




















Link copied!