"You are among millions of families navigating this exact challenge. The difference is that now there is a system designed to help."


"Clinically validated. Home-applicable. Parent-proven."
Graded Exposure Therapy for Height and Climbing Fear
Parent-friendly name: "Building Height Confidence From the Ground Up" Definition: Graded exposure therapy for height fear is a systematic, child-paced approach to building tolerance and competence with elevation, climbing activities, and situations involving vertical challenge. It combines vestibular integration, motor skill development, anxiety management, and carefully sequenced exposure from near-zero height to age-appropriate climbing — using specific therapeutic materials at each stage. Domain Vestibular Processing + Motor Development + Anxiety Ages 2–10 years Session Duration 10–20 minutes Frequency 3–5× per week Setting Home + Playground + Therapy The approach addresses the sensory, motor, and emotional components of height fear simultaneously, ensuring the child develops both the physical skills and the psychological confidence to navigate height safely. Who Uses This Technique Balance & Vestibular Equipment

"This technique crosses therapy boundaries because the brain doesn't organise by therapy type."










Material | Buy This | Make This (Free) | |
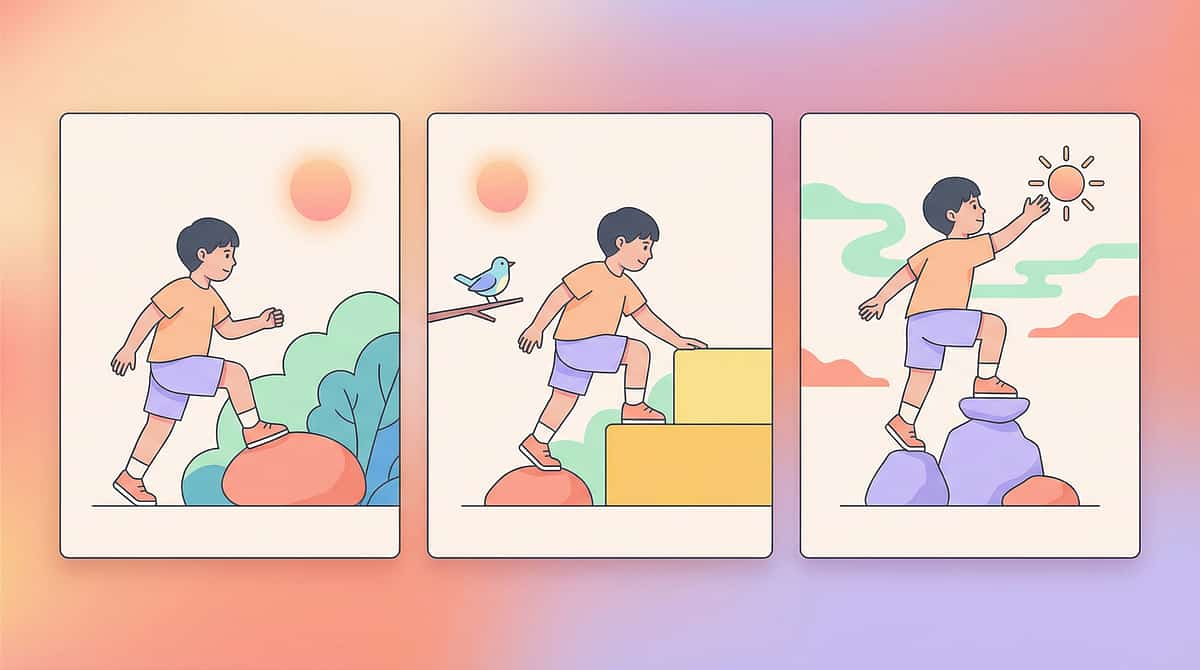
Graded Climbing Surfaces | Commercial step stools and platforms (₹2,000–15,000) | Thick book → yoga block → 1-step stool → 2-step stool → low stairs → playground equipment. Create a household hierarchy from nearly flat to actual climbing. | |
Crash Mats | Foam crash mat (₹1,500–8,000) | Layer mattresses, thick blankets, or couch cushions beneath practice areas. Multiple layers for extra cushioning. Even a pillow at the base helps. | |
Vestibular Equipment | Therapy swing or rocker (₹2,000–12,000) | Rocking chair → rocking on parent's lap → sitting on yoga ball → slow spinning on office chair → playground swing with minimal movement. | |
Climbing Harnesses | Safety climbing harness (₹3,000–10,000) | Hold the child's waist or hand firmly during climbing. Your body as physical spotter. Your arms are the first harness. | |
Visual Anchors | Specialty stickers and markers (₹100–500) | Stickers or colourful tape at eye level on stairs. Favourite toy at the top destination. Your face positioned as the visual anchor. | |
Proprioceptive Prep | Weighted vest, therapy tools (₹0–500) | Wall pushes (10 seconds), carry something heavy, 5 jumping jacks, bear walks, wheelbarrow walking, squeeze a ball. All free. All effective. | |
Height Exposure Games | Structured game kits (₹200–1,500) | Treasure hunt at progressively higher locations. Rescue stuffed animals "stuck" on stairs. Pretend cooking with ingredients on step stools. | |
Balance Builders | Balance boards and wobble discs (₹500–5,000) | Tape lines on floor, step over obstacles, walk on pillows, floor-level 2×4 board, hopping games. | |
Coping Tools | Fidget sets and calm-down kits (₹100–1,000) | Three slow breaths before each step. "Feel your feet" grounding. "I am safe, I can do this." Count slowly while climbing. |
"Every parent, regardless of economic status, can execute this technique TODAY with household items. This is the WHO/UNICEF inclusion principle in action."

"The best session is one that starts right. The worst session is one that damages trust."

- ✅ Clear the area of distractions (turn off TV, remove unrelated toys)
- ✅ Ensure adequate lighting (not too bright, not dim)
- ✅ Remove trip hazards and sharp edges near practice area
- ✅ Temperature comfortable (anxiety already elevates body temperature)
- ✅ Quiet environment preferred (reduce competing sensory input)
- ✅ Shoes with good grip OR barefoot for better proprioceptive feedback
- ✅ Comfortable clothing that doesn't restrict movement
"Spatial precision prevents 80% of session failures."


"Hey [child's name], want to play a game with me? I have something fun set up. Come see what we've got today."
- Get down to child's eye level
- Relaxed posture, gentle voice
- No urgency in your body or words
- Touch the materials yourself first (modelling safety)
- Child approaches the area willingly
- Child touches or explores materials
- Child makes eye contact with you at the practice area
- Child asks questions or shows curiosity
- Child won't approach → Move materials to where the child is comfortable
- Child says no → "That's okay. Want to just feel how soft the mat is?"
- Child seems anxious → Start with proprioceptive prep (wall pushes, heavy carrying) before returning

"Look at this! Feel how soft the mat is underneath — even if you slip, it's like landing on a cloud. And see this [sticker/toy] up here? Let's see if you want to reach it."

- Stay at or just slightly beyond current comfort zone — one step beyond, not ten
- Child sets the pace, not the parent
- Success is measured in seconds of tolerance, not inches of height
- If the child reaches the goal — celebrate. If the child takes one step — celebrate that step.
"3 good reps > 10 forced reps"
"When you see these signs, move to cool-down. Pushing past satiation erases gains."

"You stepped up! You did it! Your feet were on the step and you were so brave!"
- Immediate: Within 3 seconds of the behaviour
- Specific: Name exactly what the child did ("You stepped up" — not just "good job")
- Enthusiastic: Match your energy to the achievement
- Celebrate the attempt, not just success: "You tried! You put your foot on the step even though it was scary. That's courage."
- Verbal praise (always first)
- High-five or physical celebration the child enjoys
- Token/sticker on a chart (building toward a preferred activity)
- Brief access to a preferred activity
- Natural consequence: the toy at the top of the climb

"Two more tries, then we're all done for today."
"All done with climbing practice! You worked so hard. Now let's [preferred next activity]."

"Session abandonment is not failure — it's data."


- Child tolerates the practice area without immediate refusal
- Duration at lowest level increases (2 sec → 5 sec → 10 sec)
- Child begins to engage with crash mats and materials on the ground
- Resistance decreases from session to session
- Proprioceptive and vestibular prep activities becoming familiar
- Child climbing the playground structure (weeks/months away)
- Complete elimination of fear
- Independent stair navigation
- Enjoyment of height (tolerance comes before enjoyment)
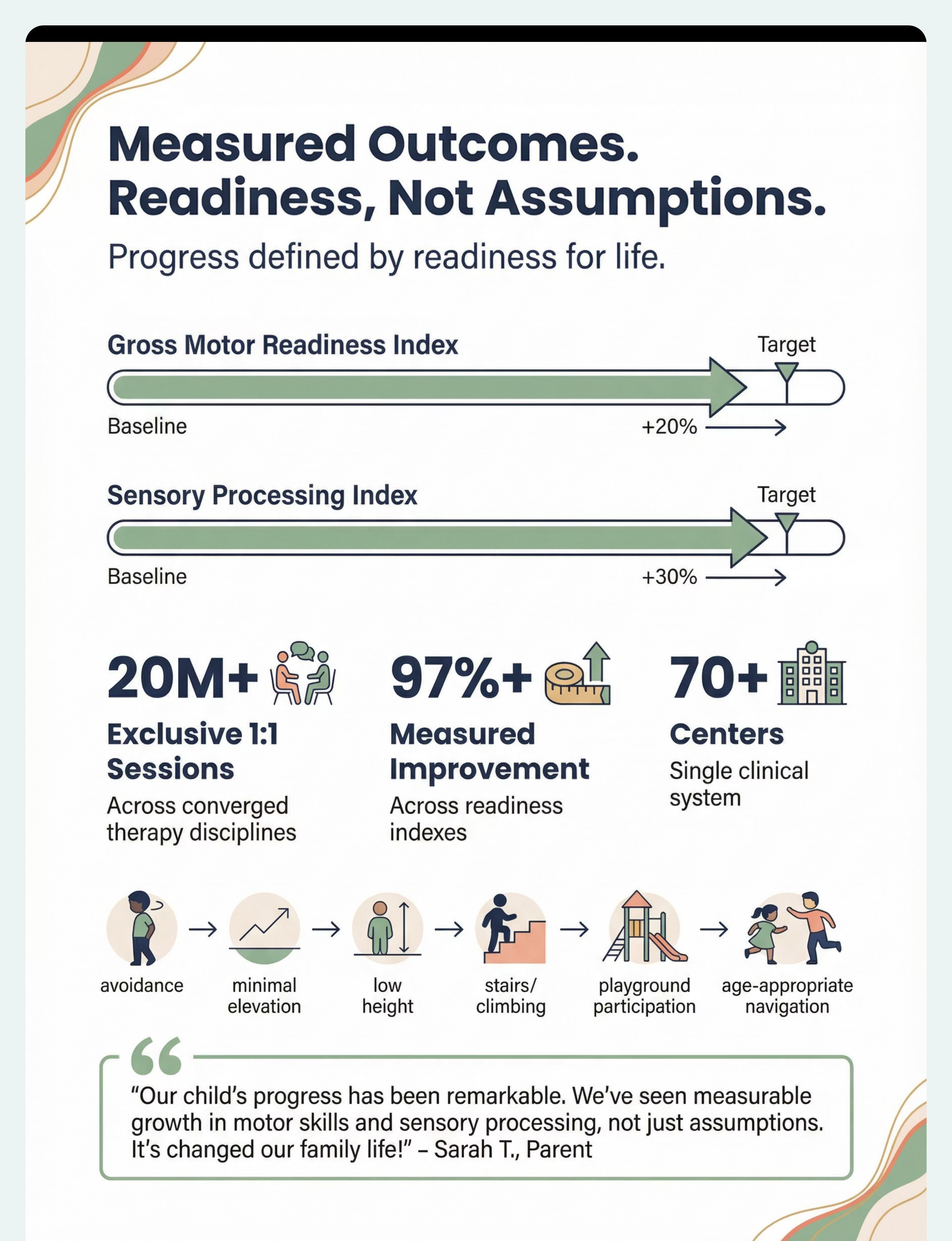
"If your child tolerates the material for 3 seconds longer than last week — that's real progress."
- Child begins to anticipate the practice session — may approach area voluntarily
- Height tolerance increases by one level on the hierarchy
- Coping strategies used more independently ("I'm breathing!")
- Fear response present but shorter — distress resolves faster
- Child may begin spontaneously stepping onto low surfaces outside sessions (generalisation seeds)
- Your own confidence building alongside your child's
- The practice becoming routine rather than dreaded
- Crash mats being used for play between sessions
- Child referencing height activities positively: "I did the step today!"


"From the ground up, one brave step at a time."
📸 Journal Prompt: Write down what your child can do today that they couldn't do 8 weeks ago. Keep this. You'll need it on hard days ahead.

"Trust your instincts — if something feels wrong, pause and ask."
- Foundational vestibular tolerance
- Basic motor coordination at ground level
- Established trust in the therapeutic relationship
- Vestibular primary → A-081: Swing Fear
- Motor primary → A-082: Balance Difficulties
- Anxiety primary → A-084: Playground Exclusion
- Lateral → A-085: Stair Navigation Difficulties
Technique | Level | Materials You Already Own | Primary Focus | |
A-079: Movement Seeking Behaviour | Core | Vestibular equipment, proprioceptive tools | Channelling sensory-seeking safely | |
A-081: Swing Fear | Intro | Vestibular equipment, crash mats | Rotary and pendular motion tolerance | |
A-082: Balance Difficulties | Core | Balance builders, visual anchors | Advanced motor coordination | |
A-083: Movement Avoidance | Core | Vestibular equipment, exposure games | Approach behaviour for movement | |
A-084: Playground Exclusion | Advanced | All 9 materials from this page | Social-motor generalisation | |
A-085: Stair Navigation | Intro | Graded surfaces, visual anchors, coping tools | Functional stair independence |
"You already own materials for all of these techniques."
→ See Your Child's GPT-OS® Profile — pinnacleblooms.org/gpt-os/profile
"This technique is one piece of a larger plan."

"Height fear often masks multiple underlying systems working overtime — vestibular alarm, motor uncertainty, anxiety cascade. When we address all three simultaneously through graded exposure with the right materials, the progression is remarkably consistent. The timeline varies, but the trajectory is reliable." — Pinnacle Therapist Note

"Your experience helps others — consider sharing your journey."

"Home + clinic = maximum impact."

"Deeper reading for the curious parent."
- Your child's rate of height tolerance improvement
- Which materials produce the strongest response
- Whether vestibular, motor, or anxiety components are dominant
- When to recommend professional assessment vs. continued home practice
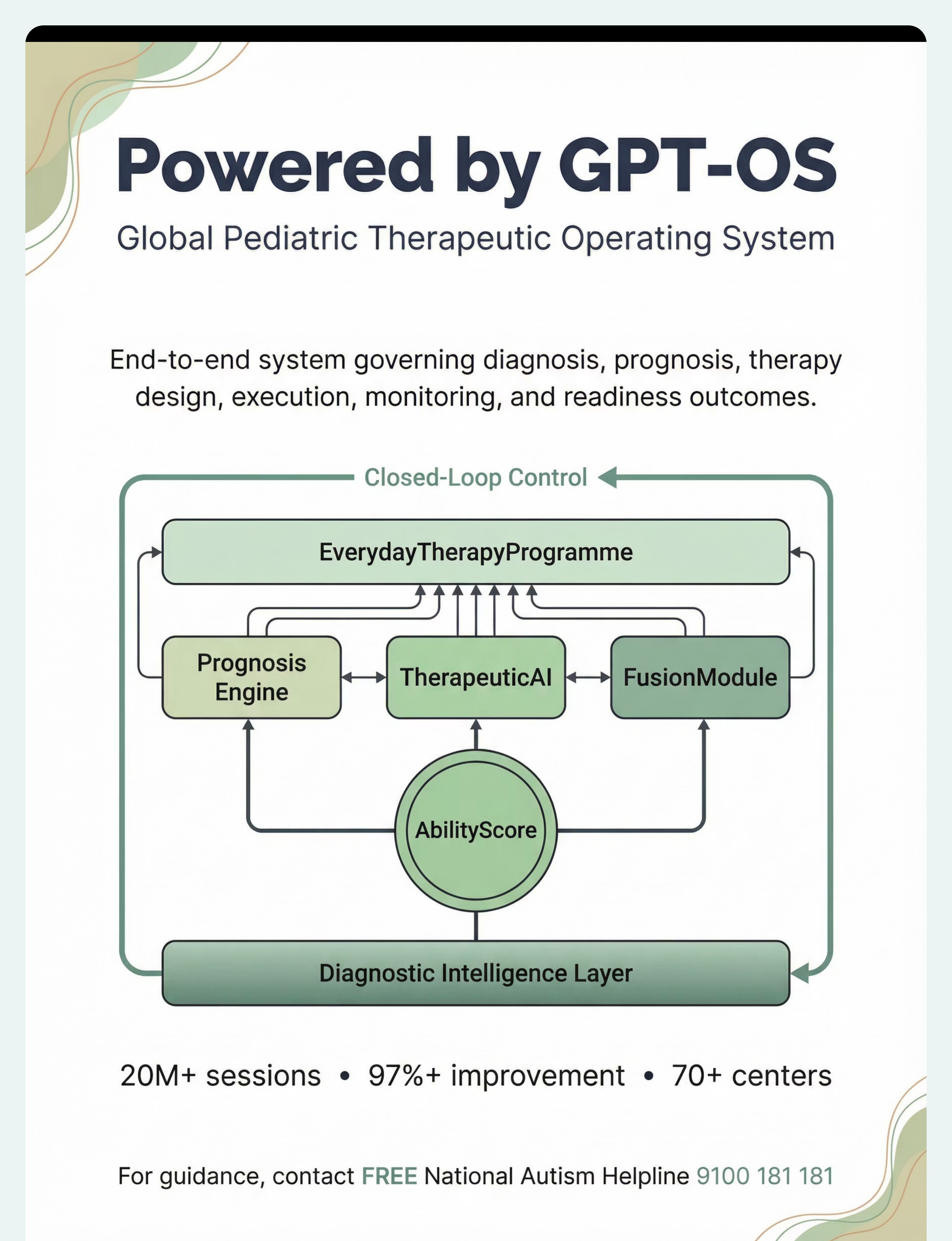
- How your child's trajectory compares to 20M+ therapy sessions
- Protected under ISO/IEC 27001 information security standards
- Data used to improve your child's recommendations and population-level research
- You control your data — view, export, or delete at any time
"Your data helps every child like yours."
60 seconds | Therapist-guided material demonstration
Preview of 9 materials that help with height and climbing fear Therapy Material
Below is a visual preview of 9 materials that help with height and climbing fear therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.