
"He spins until he falls over. Gets up. Spins again."
It's 7:30 AM and your son is already spinning in the kitchen. Arms out, eyes half-closed, round and round on the tile floor while his breakfast gets cold. You've asked him to stop six times. He can't. His body won't let him. At preschool yesterday, the teacher said he spun through circle time, spun through free play, spun while the other children stared. You don't know if this is a phase, a quirk, or something his nervous system is trying to tell you.
Vestibular Regulation Through Controlled Rotational Input — a clinically validated, multi-material intervention protocol that works WITH your child's spinning need, not against it.
You are not failing. Your child's vestibular system is speaking. And we are going to teach you its language.
Pinnacle Blooms Consortium®
OT • SLP • ABA • SpEd • NeuroDev • CRO

You Are Not Alone — The Numbers
You are among millions of families worldwide navigating this exact challenge. Excessive spinning is one of the most commonly reported vestibular seeking behaviours in paediatric sensory processing profiles. This is not rare. This is not your fault. And there is a clear, evidence-based path forward.
80%
Display Sensory Difficulties
of children diagnosed with autism display sensory processing difficulties, including vestibular seeking patterns like excessive spinning. Source: PRISMA Systematic Review, 2024 (PMC11506176)
1 in 36
Children in the USA
children in the United States is diagnosed with autism spectrum condition. In India, prevalence estimates range from 1 in 68 to 1 in 100 across recent epidemiological surveys. Source: CDC MMWR, 2023 | INCLEN Trust, India
16
Studies Confirm Evidence
Studies from 2013–2023 confirm sensory integration intervention meets evidence-based practice criteria for children with ASD in a PRISMA-model systematic review. Source: Children, 2024 (PMC11506176)

What's Happening in Your Child's Brain
The Vestibular System: Your Child's Internal Gyroscope
Deep inside your child's inner ear sit three tiny, fluid-filled loops called the semicircular canals. These canals detect every movement of the head — rotation, tilting, acceleration. They are the body's internal gyroscope, constantly sending signals to the brain about where the body is in space.
Why Your Child Doesn't Get Dizzy
In most children, a few spins send strong signals that quickly register as "enough." But in children with vestibular under-responsivity, the threshold is set higher. What a typical child feels after 3 spins, your child may need 30 spins to feel. Their vestibular "cup" needs more to fill.
This Is Wiring, Not Willpower
Your child isn't choosing to spin any more than they're choosing their eye colour. The vestibular system's sensitivity threshold is neurologically determined. The spinning is their nervous system's attempt to get the input it needs to feel organised, regulated, and grounded. This is a wiring difference, not a behaviour problem.
Where This Sits in Development
Understanding where excessive spinning falls on the developmental timeline helps parents distinguish typical behaviour from a pattern that needs support.
1
0–12 Months
Vestibular system begins processing. Babies seek gentle rocking. Head control develops. Crawling and pulling to stand engage vestibular-proprioceptive integration. Spinning objects may fascinate.
2
12–24 Months
Walking, climbing, spinning in play are TYPICAL. Brief spinning episodes are developmentally normal and expected as children explore their bodies in space.
3
2–4 Years ⮕ Watch Zone
Excessive, driven, prolonged spinning that interferes with participation emerges as a distinct pattern. Typical spinning decreases; vestibular seeking spinning persists or intensifies. This is when most parents first notice the behaviour has shifted from playful to compulsive.
4
4–7 Years ⮕ Intervention Zone
Social visibility increases. Classroom participation is affected. Peers notice. Without intervention, spinning may become the child's primary regulatory strategy, limiting access to learning and play.
5
7–10 Years ⮕ Outcome Zone
With intervention: a flexible movement repertoire develops and participation flourishes. Without intervention: patterns may consolidate and social isolation may increase over time.
Comorbidity Awareness: Excessive spinning commonly co-occurs with other vestibular seeking behaviours (swinging, running, jumping), proprioceptive seeking (crashing, pushing), difficulty with transitions, attention regulation challenges, and in some children, anxiety-driven movement patterns.
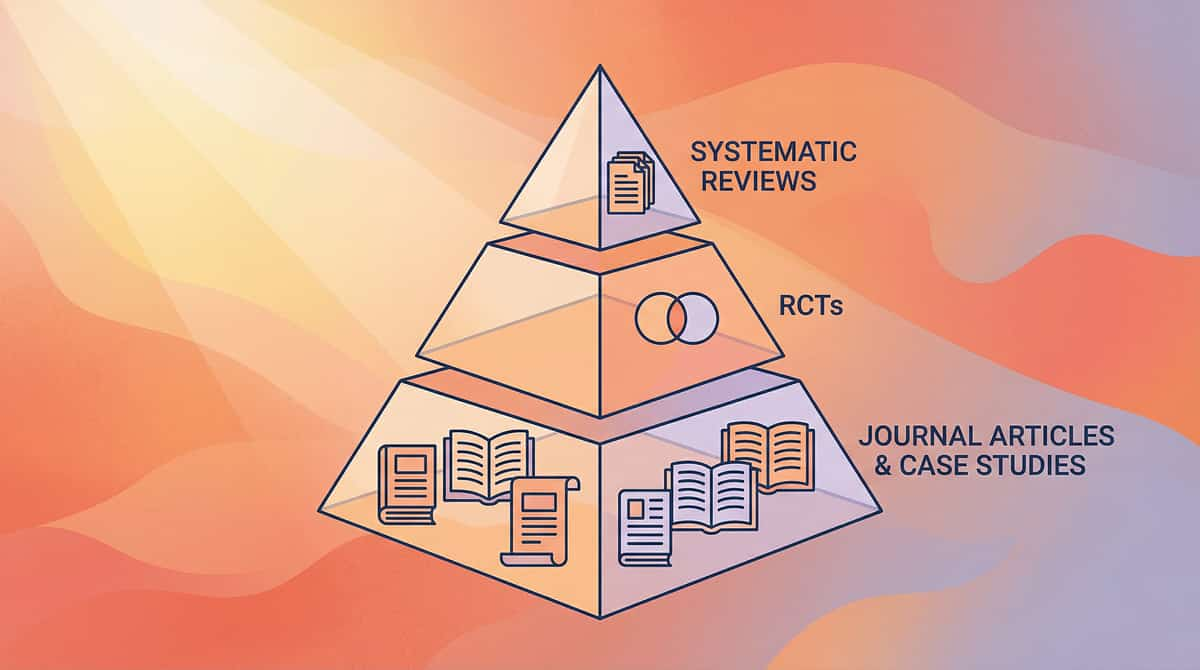
The Evidence Behind This Technique
This technique is not built on intuition. It is built on a growing, robust body of peer-reviewed clinical science — systematic reviews, randomised controlled trials, and global implementation data.
EVIDENCE GRADE: LEVEL I–II
Systematic Reviews + Randomised Controlled Trials
4/5
Strong Evidence Base
Key Supporting Studies
- PRISMA Systematic Review (2024): 16 articles from 2013–2023 confirm sensory integration meets evidence-based practice criteria for ASD. PMC11506176
- Meta-Analysis (2024): 24 studies. Sensory integration therapy effectively promoted social skills, adaptive behaviour, sensory processing, and motor skills. PMC10955541
- Indian RCT (2019): Home-based sensory interventions administered by trained parents showed significant outcomes. DOI: 10.1007/s12098-018-2747-4
- NCAEP Evidence-Based Practices Report (2020): Sensory integration classified as an evidence-based practice. Visual supports and video modelling independently classified as evidence-based.
Clinically validated. Home-applicable. Parent-proven.

The Technique: What It Is
Domain: Sensory Processing / Vestibular System
Ages 2–10
10–20 min/session
Vestibular Regulation Through Controlled Rotational Input"Feeding the Spin: Meeting Your Child's Vestibular Needs Safely"
A multi-material sensory integration protocol that addresses excessive spinning by providing controlled, safe vestibular input through rotation equipment, proprioceptive loading, balance challenges, calming vestibular alternatives, and proactive sensory scheduling. Rather than stopping the spinning (which removes the child's regulatory strategy without replacement), this technique meets the vestibular need through graduated, clinically guided pathways that build processing capacity, expand the child's regulatory repertoire, and reduce the driven, compulsive quality of uncontrolled spinning over time.
Frequency
Daily, with scheduled movement breaks every 30–45 min
Duration
10–20 minutes per session
Materials
Sit-and-Spin, Therapy Swings, Balance Boards, Weighted Vests, Sensory Schedules

Who Uses This Technique
This technique crosses therapy boundaries because the brain doesn't organise by therapy type. Four specialist disciplines collaborate to deliver the most effective outcome for your child.
Occupational Therapist (OT) — Primary Lead
The OT is the primary architect of vestibular regulation protocols. They assess the child's sensory processing profile, design the individualised sensory diet, select appropriate equipment intensity, and train parents on safe execution. The OT determines the balance between rotational input, proprioceptive grounding, and calming vestibular alternatives.
Board Certified Behaviour Analyst (BCBA/ABA)
The BCBA addresses the behavioural function of spinning — whether it serves sensory, emotional, escape, or attention functions. They design the replacement behaviour protocol, create transition supports, establish reinforcement schedules, and ensure data collection systems track both frequency of spinning and use of alternatives.
Speech-Language Pathologist (SLP)
The SLP addresses communication barriers created by excessive spinning. They also work on body awareness vocabulary ("my body needs to move"), interoception language, and self-advocacy scripts that help the child communicate vestibular needs verbally rather than behaviourally.
Special Educator (SpEd)
The SpEd adapts classroom environments for vestibular seekers — movement-permitting seating, scheduled movement breaks integrated into academic routines, sensory corners with rotation equipment, and peer education about movement differences.
What This Technique Targets
The intervention is structured across three concentric rings of outcome — from the core vestibular need outward to whole-child participation.
Meta-analysis (World J Clin Cases, 2024) confirms that sensory integration therapy effectively promoted social skills (primary), adaptive behaviour (secondary), sensory processing, and motor skills (tertiary) across 24 studies. Reference: PMC10955541

What You Need — Primary Materials Overview
This protocol uses 9 clinically selected materials, each targeting a specific aspect of vestibular regulation. Every item has a DIY alternative so that every family can begin today. Total investment ranges from ₹200 (essential starters) to ₹15,000 (full protocol kit under ₹10,000).
1. Sit-and-Spin / Rotation Toys
₹800–3,000 | Vestibular Input Equipment
2. Swings with Rotational Capacity
₹2,000–15,000 | Therapy Swings & Suspension
3. Proprioceptive Loading Materials
₹500–4,000 | Weighted & Compression Tools
4. Balance Equipment
₹500–3,500 | Balance & Vestibular Training
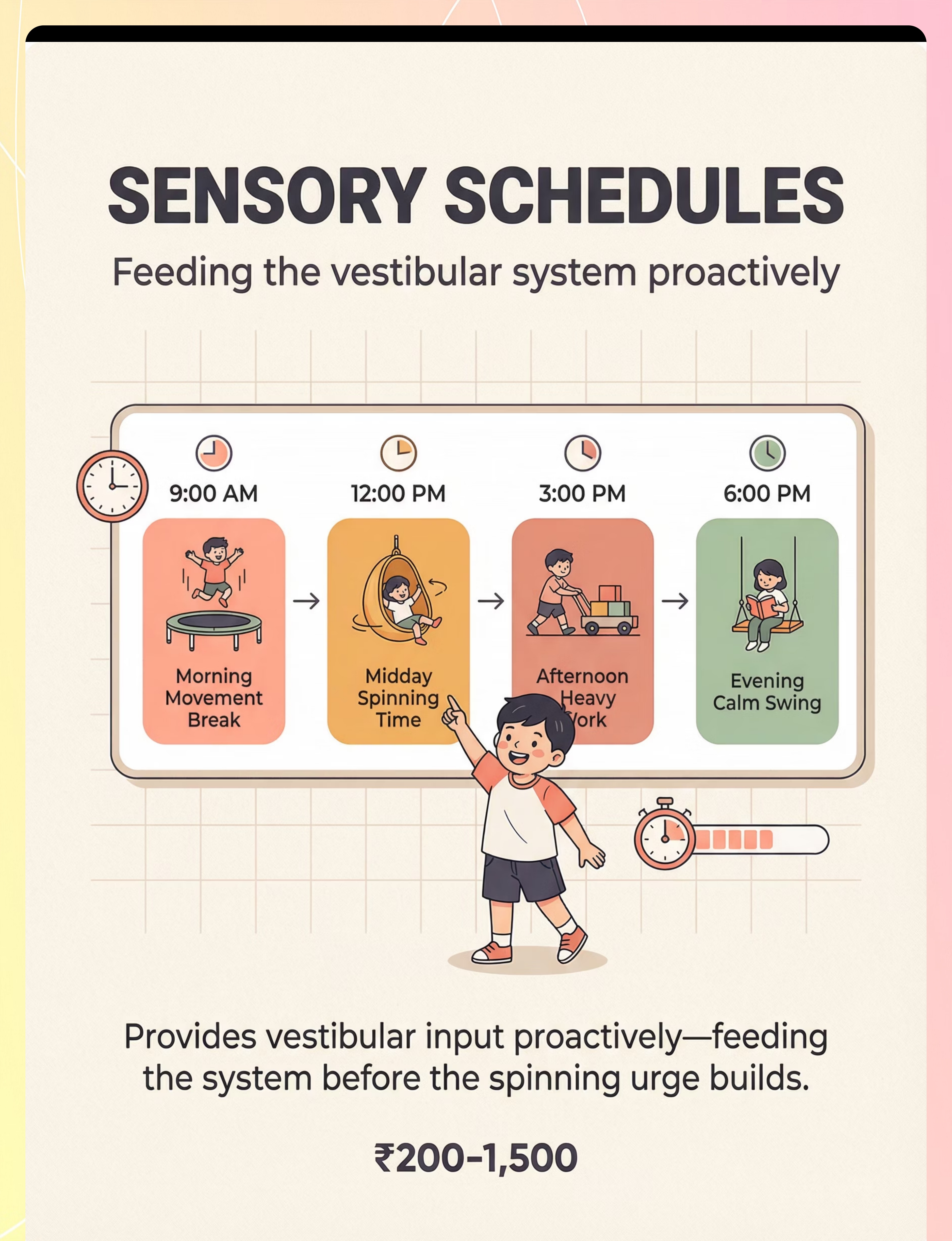
5. Sensory Regulation Schedule Tools
₹200–1,500 | Visual Supports & Schedules
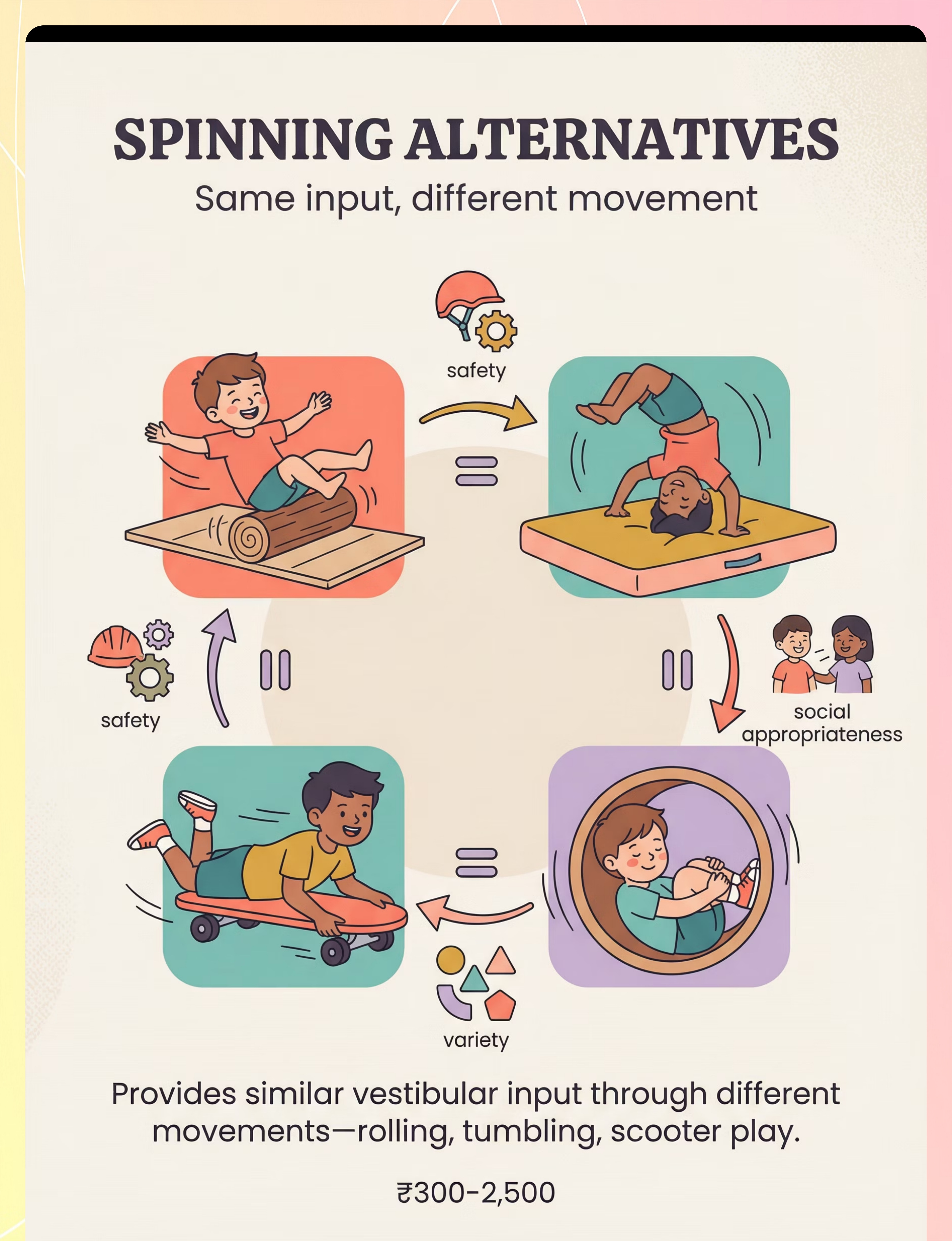
6. Spinning Alternatives / Substitution Materials
₹300–2,500 | Gross Motor & Movement Equipment
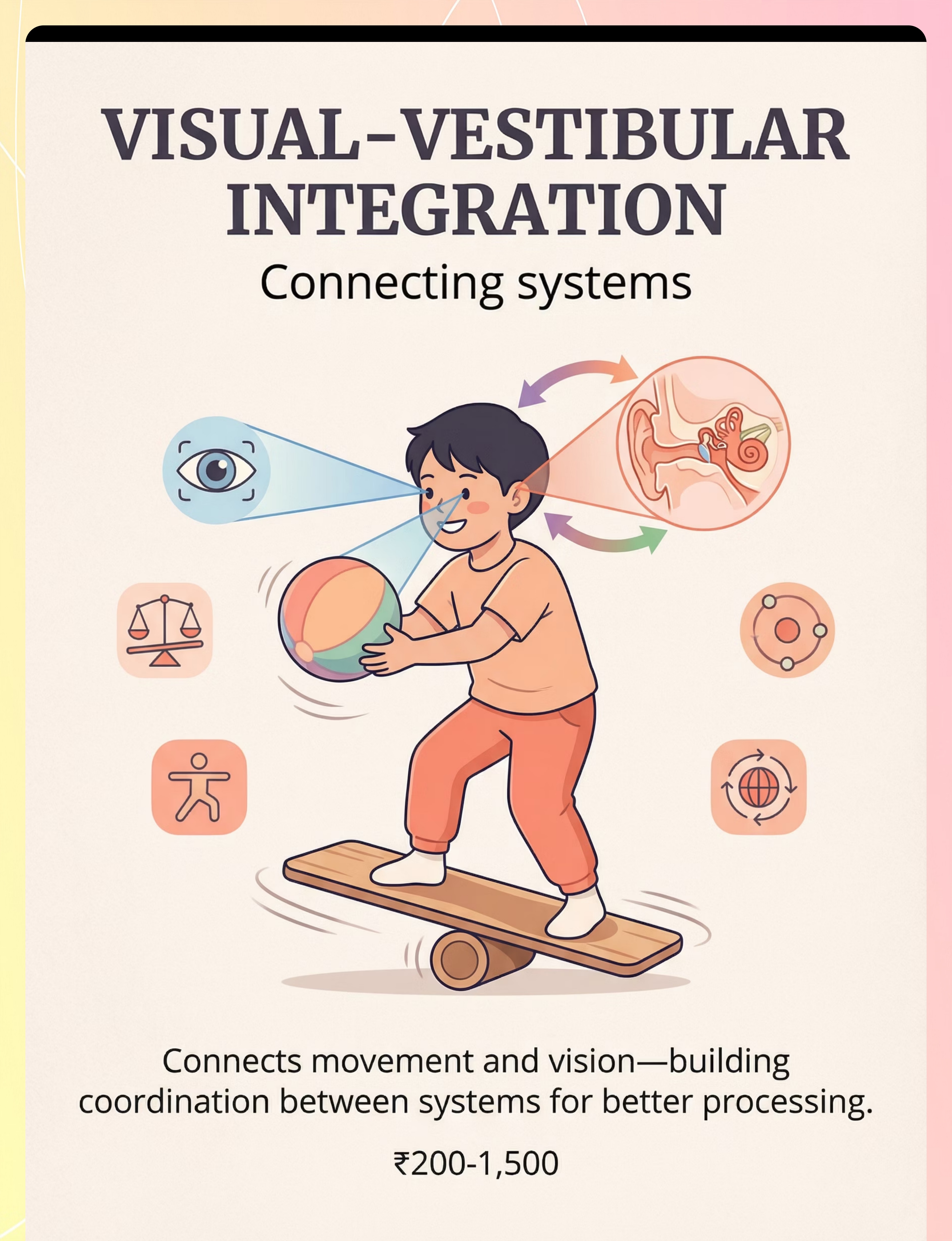
7. Visual-Vestibular Integration Materials
₹200–1,500 | Sensory Integration Tools
8. Calming Vestibular Input Materials
₹1,500–8,000 | Calming & Regulation Equipment
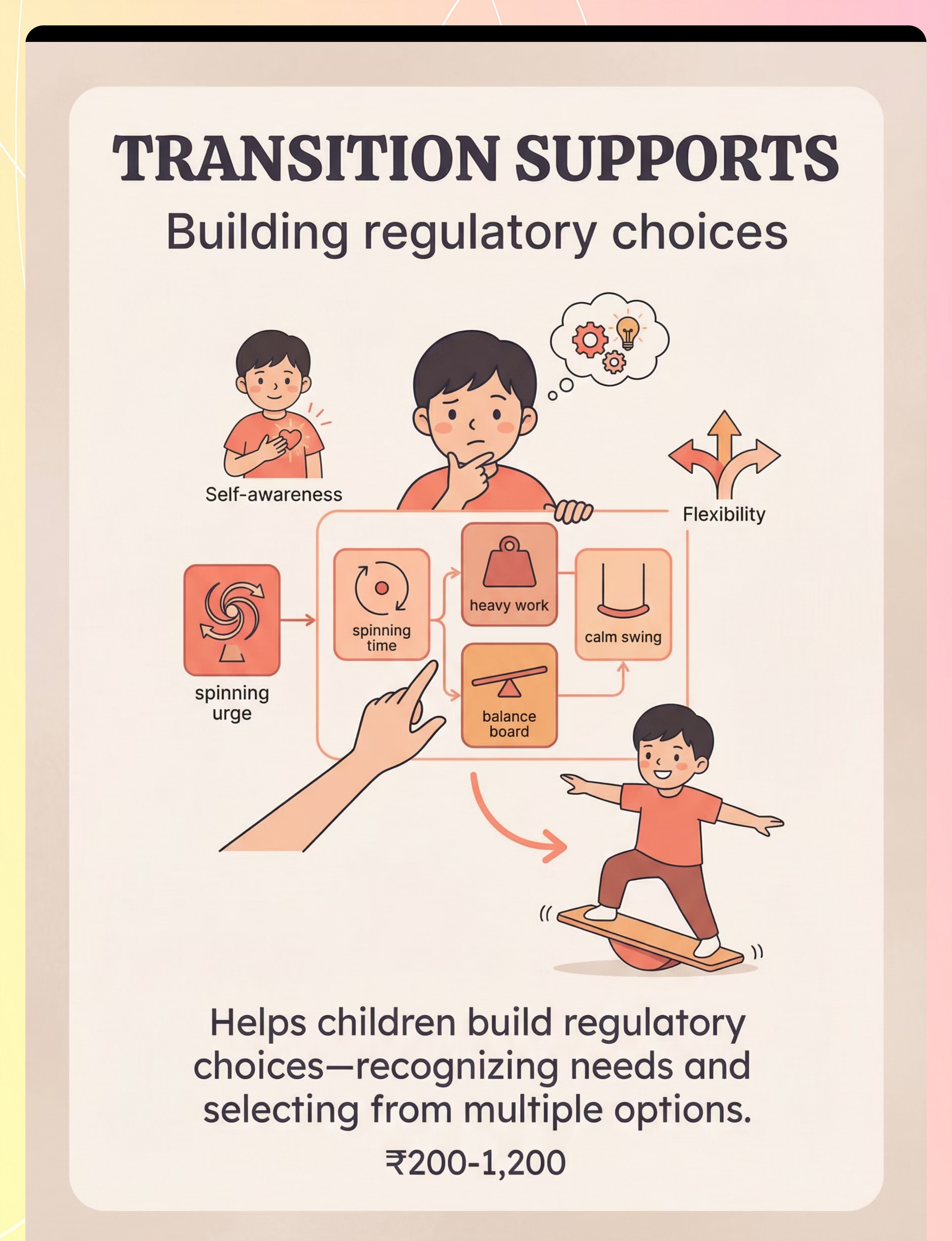
9. Transition and Replacement Supports
₹200–1,200 | Behaviour Support Tools

Material 1 — Sit-and-Spin / Rotation Toys
Vestibular Input Equipment
₹800–3,000
What's included: Sit-and-spin toys, Dizzy Disc Jr., spinning seats, swivel cushions, rotation platforms. These are the frontline tools for providing controlled rotational input in a safe, child-directed format. The child sits securely on the toy and controls both direction and speed, giving the vestibular system exactly the input it is seeking — within boundaries you set.
Why it works: By giving the spinning behaviour a defined "home," you shift it from compulsive floor-spinning to a scheduled, bounded activity. The equipment itself becomes a regulatory anchor — a safe place to spin that the child's nervous system learns to trust.

Material 2 — Swings with Rotational Capacity
Therapy Swings & Suspension
₹2,000–15,000
What's included: Platform swings, disc swings, cocoon swings with rotation, tire swings, therapy bolster swings. Swings that allow rotation provide a broader vestibular experience than floor-based spinning — the child's entire body moves through space, engaging the semicircular canals from multiple angles simultaneously.
Why it works: Suspension swings engage both the linear and rotational vestibular systems. The child can control the degree of spin by twisting the chains and releasing, learning to self-regulate the input. This is a significant step toward self-monitoring vestibular needs.

Material 3 — Proprioceptive Loading Materials
Weighted & Compression Tools
₹500–4,000
What's included: Weighted vests (5–10% of body weight), weighted lap pads, resistance bands, body socks and compression garments. Proprioceptive input — pressure and resistance through the joints and muscles — is the essential counterpart to rotational vestibular input. After spinning, the nervous system needs grounding.
Why it works: Proprioceptive input is inherently organising and calming. It "grounds" the vestibular system after rotation, reducing the alerting effect of spinning and helping the child transition back to a regulated baseline. Without proprioceptive grounding, rotation alone may leave the system more activated, not less.
Safety: Weighted vests should be 5–10% of the child's body weight. Never use during sleep. Consult an OT for individualised weighting recommendations.
Material 4 — Balance Equipment
Balance & Vestibular Training
₹500–3,500
What's included: Balance boards (rocker, wobble), wobble cushions, balance beams, stepping stones, balance pods. Balance equipment challenges the vestibular system in a different direction than rotation — it requires the brain to make rapid micro-adjustments to maintain upright posture, building the precision processing capacity that excessive spinning alone does not develop.
Why it works: Balance activities integrate visual, vestibular, and proprioceptive systems simultaneously. As the child becomes better at balance challenges, the vestibular system becomes more efficient at processing all types of input — including rotation. You are, in effect, expanding the system's capacity from the inside out.

Material 5 — Sensory Regulation Schedule Tools
Visual Supports & Schedules
₹200–1,500
What's included: Visual sensory schedules, sensory diet activity cards, movement break timers, regulation routine charts, activity choice boards. The schedule is the invisible infrastructure of this entire protocol. Without predictable, structured access to vestibular input, the child's nervous system remains in a constant state of seeking — compulsive, unscheduled, and uncontrolled.
Why it works: When a child knows that spinning time is coming — at 9 AM, at 12 PM, and at 3 PM — the desperation driving the uncontrolled spinning diminishes. The schedule teaches the nervous system that the need will be met, reducing the urgency. Visual schedules are classified as an evidence-based practice for autism (NCAEP, 2020).

Material 6 — Spinning Alternatives / Substitution Materials
Gross Motor & Movement Equipment
₹300–2,500
What's included: Scooter boards, tumbling mats, barrel rolls, therapy balls, tunnels. Spinning alternatives are the substitution repertoire — the growing menu of movement activities that meet vestibular needs through different pathways. The goal is not to eliminate spinning, but to expand the child's regulatory toolkit so that spinning becomes one option among many, rather than the only strategy available.
Why it works: Each alternative provides a different flavour of vestibular input. Log rolling on a mat provides linear movement. Somersaults combine rotation with proprioceptive input. Tunnels engage the whole body in a contained, calming movement. Together, these build the movement vocabulary that replaces the single-note strategy of compulsive floor-spinning.

Material 7 — Visual-Vestibular Integration Materials
Sensory Integration Tools
₹200–1,500
What's included: Balls for catching during movement, tracking games, bubble play during vestibular activities, target games. Visual-vestibular integration materials add a second processing demand to movement activities, forcing the brain to coordinate what the eyes see with what the vestibular system feels. This is a higher-order skill that typically emerges once basic vestibular regulation is established.
Why it works: The vestibulo-ocular reflex (VOR) is the neurological bridge between the inner ear and the eyes. When a child catches a ball while swinging, they are simultaneously training the VOR, building visual tracking, and providing vestibular input. This multisensory integration is the hallmark of advanced vestibular processing development and a key goal of weeks 5–8 of the protocol.

Material 8 — Calming Vestibular Input Materials
Calming & Regulation Equipment
₹1,500–8,000
What's included: Rocking chairs, glider rockers, hammocks, therapy swings (used slowly), porch swings. Not all vestibular input is alerting. Linear, rhythmic, slow vestibular input — rocking, gentle swinging, hammocking — is inherently calming to the nervous system. These materials serve a critical function in the cool-down phase of every session and as a first-line response to dysregulation.
Why it works: Slow, rhythmic linear movement activates the parasympathetic nervous system, reducing arousal and promoting regulation. When a child who has been spinning compulsively is transitioned to gentle rocking, the nervous system shifts from "seeking" mode to "satisfied" mode. Calming vestibular input is the landing pad after the rotational input has been delivered.

Material 9 — Transition and Replacement Supports
Behaviour Support Tools
₹200–1,200
What's included: Movement choice boards, regulation check-in cards, body signals charts, alternative activity cards, self-regulation visual supports. These are the communication and self-management tools that bridge the gap between "I need to spin NOW" and "I know what my body needs and I can choose how to meet that need." They are the language of the protocol — the external scaffolding that eventually becomes internal self-awareness.
Why it works: Choice boards give the child agency within a structured set of appropriate options. Regulation check-in cards build interoceptive awareness — the ability to notice and name internal states. Together, these tools move the child from reactive behaviour (compulsive spinning) toward proactive self-regulation ("my body needs to move; I'll use the spin chair").

DIY & Substitute Options
Because every family can start this technique today — regardless of budget. The WHO/UNICEF Nurturing Care Framework emphasises context-specific, equity-focused interventions. Heavy work activities require no equipment. Rolling on the floor is free. Every family can begin this protocol TODAY with household items.
Buy This | Make This (Zero-Cost / Low-Cost) | |
Sit-and-Spin Toy (₹800–3,000) | Stable swivel chair or office chair with adult supervision. Child sits, parent controls rotation speed. | |
Rotational Swing (₹2,000–15,000) | Playground swings — teach child to twist chains and release for controlled spinning. Blanket swing between two adults. | |
Weighted Vest (₹500–4,000) | Heavy backpack with books. Rice-filled fabric pouch as lap pad. Carrying groceries, pushing laundry baskets, wheelbarrow walking, bear walks, crab walks. | |
Balance Board (₹500–3,500) | Sturdy plank over a small ball or foam roller. Pillow walking. Tape lines on floor for balance beam pathways. | |
Sensory Schedule (₹200–1,500) | Hand-drawn picture schedule on chart paper. Phone timer for movement breaks every 30–45 minutes. Index cards with movement activity drawings. | |
Scooter Board (₹300–2,500) | Rolling on the floor — log rolling, somersaults (supervised, soft surface). Wheelbarrow walking. | |
Tracking Games (₹200–1,500) | Catching/throwing a ball while on a swing. Blowing and popping bubbles while on movement equipment. | |
Rocking Chair (₹1,500–8,000) | Rocking in parent's lap. Gentle swinging on playground swing (slow, rhythmic). Hammock made from a bedsheet. | |
Choice Board (₹200–1,200) | Paper with pictures of 4 movement options. "When I want to spin, I can also..." card with hand-drawn alternatives. |
⚠️ Safety First — Before You Begin
🔴 DO NOT PROCEED IF:
- Child has a diagnosed inner ear condition, vertigo, or balance disorder without medical clearance
- Child has a seizure disorder that may be triggered by vestibular input (consult neurologist first)
- Child shows signs of illness: fever, ear infection, vomiting, or recent head injury
- Child is in acute distress, meltdown, or severe dysregulation
- Equipment is unstable, damaged, or exceeds weight limits
🟡 MODIFY IF:
- Child is tired, hungry, or mildly dysregulated (use shorter, calmer version)
- Child has recently eaten a large meal (wait 30 minutes before rotational activities)
- Environment is crowded or has hard surfaces near spinning zones
- Child is on medication that may affect vestibular processing
🟢 SAFE TO PROCEED WHEN:
- Child is fed, rested, and in a regulated baseline state
- Environment cleared of obstacles within 2 metres of activity zone
- Appropriate safety surfacing (mat, carpet, grass) under all equipment
- Adult supervisor is present and undistracted throughout
- Equipment checked for stability and weight capacity
🛑 STOP IMMEDIATELY IF: Paleness, sweating, or skin colour change (vestibular overload) · Nausea or vomiting · Sudden stillness or "glazed" expression · Crying, distress, or fear · Uncontrolled falling with inability to recover balance. Weighted Items: 5–10% of child's body weight maximum. Do NOT use during sleep. Consult an OT for individualised recommendations.

Set Up Your Space
A prepared environment is not optional — it is a clinical prerequisite. Sensory Integration Theory (Ayres) establishes environmental setup as a core principle. The space you create is the first therapeutic intervention.
Lighting
Natural or soft. No flickering fluorescents.
Sound
Quiet. Turn off TV, reduce background noise.
Temperature
Comfortable. Child should not be overheated.
Remove
Breakable objects, sharp edges, distracting toys.
Have Ready
Water bottle, preferred calming object, visual timer.
Is Your Child Ready? — Readiness Check
The best session is one that starts right. Before every session, run this pre-flight checklist. Two minutes of assessment now prevents thirty minutes of dysregulation later.
1
Fed
Child has eaten within the last 2 hours (not immediately before)
2
Rested
Child has had adequate sleep and is not overtired
3
Regulated
Child is at baseline — not in active meltdown, not post-meltdown, not escalating
4
Healthy
No fever, ear pain, nausea, or recent head injury
5
Time
You have at least 20 uninterrupted minutes (10 min activity + 5 min cool-down + 5 min buffer)
6
Adult Focus
You can give full, undivided attention (phone away, other children supervised)
🟢ALL GREEN → PROCEED to Step 1 | 🟡1–2 AMBER → MODIFY: Use a shortened, gentler version. Focus on calming vestibular and proprioceptive input only. | 🔴ANY RED → POSTPONE: Offer a calming activity. Try again later. Postponing is not failure — it's data.
Step 1 — The Invitation
Step 1
🕐 1–2 minutes
Every session begins with an invitation, not a command. You are bringing your child into the activity through playful, low-demand engagement. Pair yourself with fun. The equipment should predict good things.
Approach your child at their level. Have the sit-and-spin or balance board visible but not pushed at them. Say in a warm, excited tone:"Look what we have today! This is your special spinning chair. Do you want to try sitting on it?"If the child is already spinning: "I can see your body wants to spin! I have something really cool that lets you spin EVEN BETTER. Want to see?"
Acceptance Looks Like
- Child approaches the equipment with curiosity
- Child looks at you and the equipment
- Child touches or sits on the equipment
- Child vocalises interest or leads you toward the equipment
Resistance: How to Modify
- Child ignores: Place the equipment where they're spinning. Don't force. Wait.
- Child moves away: Leave the equipment available. Try again in 10 minutes.
- Child becomes upset: Abandon the introduction. Offer a preferred activity. Try a different material tomorrow.

Step 2 — The Engagement
Step 2
🕐 2–3 minutes
The child is showing interest. Now deepen the interaction by introducing the therapeutic material actively. Match your energy to the child's — keep the tone playful, warm, and encouraging throughout.
For Sit-and-Spin / Rotation Equipment
Help the child sit comfortably. Show them how to hold on. Begin with a SLOW spin — 2–3 rotations. Pause. Watch the child's face. Smiling? Reaching for more? Calm? That's engagement. "You're spinning! Your body likes this, doesn't it? Let's try a few more."
For Balance Equipment
Guide the child onto the balance board. Hold their hands. Let them feel the wobble. Rock gently side to side. Count together: "One... two... three!" Make it a game, not a task.
For Proprioceptive Loading
Offer the weighted vest. "This is your strong vest! It helps your body feel grounded." Help them put it on. Begin a heavy work activity — carrying a basket of laundry, pushing a box, bear crawls across the room.
✅Engagement: Smiling, reaching, requesting more, calm body | ⚠️Tolerance: Neutral face, staying with the activity — continue gently | 🛑Avoidance: Turning away, rigidity, crying — stop and offer a preferred activity. The moment you see engagement, praise immediately.

Step 3 — The Therapeutic Action
Step 3
🕐 5–8 minutes — Core Therapeutic Event
This is the structured vestibular input session. You are providing controlled rotational and movement input that satisfies your child's vestibular system through safe, appropriate channels.
1
Phase A: Controlled Rotation (3–5 min)
Let the child spin at THEIR pace on the sit-and-spin or rotation equipment. Count rotations. After every 10 rotations, pause for 15 seconds. Observe post-rotary nystagmus (tiny eye movements after stopping) — a neurological sign the system is processing input.
2
Phase B: Proprioceptive Grounding (1–2 min)
Immediately after rotation: heavy work. Have the child carry a weighted object, do 5 bear crawls, or receive firm deep pressure squeezes to joints (shoulders, hips, knees). This grounds the system after rotational input. Do NOT skip this phase.
3
Phase C: Balance Challenge (1–2 min)
Stand on the balance board for 30 seconds. Arms out. Catch a softly tossed ball while balancing. This integrates visual-vestibular systems and builds multi-sensory processing capacity.
❌Common Errors: Allowing unlimited spinning without breaks → vestibular overload | Skipping proprioceptive grounding → leaves system unorganised | Forcing child on equipment when distressed → breaks trust | Doing this immediately after meals → nausea risk

Step 4 — Repeat & Vary
Step 4
🕐 3–5 minutes
Complete the A→B→C sequence (Rotation → Grounding → Balance) 2–3 times per session. Vary the specific activity within each phase across days to build a broad vestibular repertoire and prevent habituation. Three good repetitions are worth more than ten forced ones.
Rotation Variations
- Day 1: Sit-and-spin
- Day 2: Twisted swing release
- Day 3: Office chair spins (supervised)
- Day 4: Rolling on the floor (log rolls)
- Day 5: Somersaults on a mat (supervised)
Grounding Variations
- Bear crawls, crab walks, wheelbarrow walking
- Carrying heavy books across the room
- Wall push-ups (10 repetitions)
- Resistance band pulls
- Deep pressure hugs (firm, sustained)
Balance Variations
- Wobble cushion standing
- Walking along a tape line on the floor
- Standing on one foot while catching a ball
- Stepping stones across the room
Satiation Indicators — Stop when: Child spontaneously moves to a different activity (vestibular "cup" is full) · Child becomes drowsy or calm (system is organised) · Child refuses the next repetition without distress · Any amber/red safety signs appear.

Step 5 — Reinforce & Celebrate
Step 5
🕐 Within 3 seconds of desired behaviour
Reinforcement is the fuel that drives repetition. The more rewarding the experience of using the equipment, the more the child's nervous system will seek it out as a preferred regulatory strategy — over time, replacing the compulsive floor-spinning with intentional, bounded equipment use.
"You're spinning on your special chair! Your body is getting exactly what it needs!"
"Look at those strong bear crawls! You're grounding your body like a champion!"
"You're balancing AND catching! Two things at once — your brain is working so hard!"
"You chose the spin chair instead! That's such a smart choice for your body. I'm so proud of you."
Reinforcement Menu: Natural reinforcers — vestibular input itself IS reinforcing for these children. Social reinforcers — high-fives, specific praise, enthusiastic narration. Token options — "Earn 3 stars for using your spin equipment → choose tomorrow's first movement activity." Celebrate the attempt, not just the success. A child who sits on the balance board for 5 seconds has done something brave.
Step 6 — The Cool-Down
Step 6
🕐 3–5 minutes
No session ends abruptly. The cool-down transitions your child from therapeutic engagement back to baseline. Use a visual timer. Make the ending predictable and kind.
"Two more spins, then all done with spinning time."(Show the time remaining on a visual timer.)"One more spin... and... all done! Great job. Now let's help your body feel calm."
Slow Rocking
In your arms or in a rocking chair (1–2 minutes). Rhythmic, predictable, calming.
Gentle Swing
At a SLOW pace. Linear movement only — no rotation during cool-down.
Deep Pressure
Firm hugs, weighted blanket, or "burrito roll" in a blanket.
Quiet Sensory Activity
Play dough, water play, or sand play to transition back to tabletop regulation.
Material Put-Away Ritual: Have the child help put materials away if able. This provides additional proprioceptive input and creates a clear "session end" signal. If child resists ending: offer a "one more" compromise once, then use the visual timer.
Step 7 — Capture the Data: Right Now
Step 7
🕐 60 seconds
60 seconds of data now saves hours of guessing later. Within 60 seconds of session end, record these 3 data points. This data feeds your understanding of your child's trajectory and — if you use GPT-OS® — drives personalised protocol adjustments.
1
Spinning Frequency Today
How many times did your child spin uncontrollably (NOT on equipment) today?
☐ 0–2 times | ☐ 3–5 times | ☐ 6–10 times | ☐ 10+ times
2
Equipment Engagement Duration
How long did your child engage with the rotation/balance equipment during the session?
☐ Under 1 minute | ☐ 1–3 minutes | ☐ 3–5 minutes | ☐ 5+ minutes
3
Regulation Quality After Session
After the session, was your child:
☐ Calm and organised | ☐ Slightly keyed up but functional | ☐ Overstimulated/dysregulated | ☐ No change from before session
What If It Didn't Go as Planned?
Session abandonment is not failure — it's data. Every challenge reveals something about your child's current vestibular processing capacity and points you toward the next adjustment. Here are the seven most common problems and their solutions.
Child refused equipment and kept spinning on the floor
Why: The equipment is new. New alternatives need time. What to do: Place the sit-and-spin where the child typically spins. Don't force. Pair it with something the child loves (snack, music). Try for 3 days — most children explore it by day 2–3.
Child became nauseous or pale during rotation
Why: You may have exceeded the vestibular system's current capacity. Even seekers can overload. What to do: Stop all rotation immediately. Offer firm deep pressure. Next session, reduce rotation by 50% and build up gradually.
Child got MORE hyper after the session, not calmer
Why: Rotation is ALERTING vestibular input. Without adequate proprioceptive grounding, the system stays activated. What to do: Increase the proprioceptive grounding phase. Double the heavy work time. Add 5 minutes of slow rocking or deep pressure at the end.
Child tantrums when session ends
Why: The equipment IS meeting their need — a good sign! They haven't yet learned the session has boundaries. What to do: Use a visual timer from Day 1. Offer a schedule: "Spinning time at 9 AM and 3 PM." Knowing it will come back reduces the desperation.
Child can't or won't do the balance activities
Why: Balance demands are too high. The just-right challenge hasn't been found yet. What to do: Reduce the challenge. Start with standing on a wobble cushion while holding your hands. 10 seconds is a win. Build from there.
Child spins at school and protocol can't be done there
Why: School requires adapted strategies. What to do: Share the safety guidelines and sensory schedule with the teacher. Request movement breaks every 30 minutes. Ask about a wobble cushion for the child's chair.
Nothing changed after a week
Why: Neurological change takes time. 1 week is barely the introduction phase. What to do: Continue for 4 weeks minimum. Look for MICRO-changes: 1 fewer spinning episode per day, 5 seconds longer on equipment, slightly calmer after sessions. These are real progress.

Adapt & Personalise
No two children's vestibular systems are identical. Use this guide to calibrate the protocol to your child's current state, age, and profile. Adjust week by week as you observe their responses.
1
Easier Version (Bad days, early weeks, ages 2–3)
Skip rotation equipment. Focus only on proprioceptive loading (heavy work) and calming vestibular (gentle rocking). Session: 5–7 minutes. 1 repetition only. Parent provides all physical support.
2
Standard Version (Regulated days, weeks 2–4, ages 3–7)
Full A→B→C protocol: Controlled Rotation → Proprioceptive Grounding → Balance Challenge. Session: 10–15 minutes. 2–3 repetitions. Child has increasing independence on equipment.
3
Advanced Version (Breakthroughs, weeks 5+, ages 5–10)
Add visual-vestibular integration: catching balls while on balance board, tracking targets while on swing. Child selects from choice board independently. Session: 15–20 minutes. Child self-monitors body needs.
For the HIGH SEEKER (15+ spins/day)
Increase rotation equipment access. Allow longer spinning times on equipment. Focus heavily on proprioceptive grounding AFTER rotation. These children need MORE input, not less.
For the ANXIOUS SPINNER
Focus on CALMING vestibular options (rocking, slow swing) and transition supports (choice boards, regulation check-ins). The spinning may be anxiety-driven, not purely vestibular seeking.
For the YOUNG CHILD (2–3 years)
Parent-assisted throughout. Shorter sessions. More play-based. Lap rocking, gentle swinging, and heavy work through play rather than formal equipment use.
Week 1–2: What to Expect
Act IV: Progress Arc
Weeks 1–2
15%
Progress at Week 2
Early phase — tolerance and exploration
✅ Observable Indicators
- Child explores the rotation equipment (even briefly — 30 seconds is progress)
- Child tolerates the equipment being present in their space
- Proprioceptive loading activities are accepted (heavy work, deep pressure)
- You notice 1–2 fewer uncontrolled spinning episodes per day
- Child may begin to approach the equipment independently
❌ Not Expected Yet
- The child using the equipment instead of spinning every time
- Complete cessation of uncontrolled spinning
- The child asking for the equipment verbally
- Other people noticing a behavioural difference
If your child sits on the sit-and-spin for 30 seconds longer this week than last week — that is real, measurable, neurologically significant progress. Progress in weeks 1–2 is measured in tolerance, not mastery.

Week 3–4: Consolidation Signs
Act IV: Progress Arc
Weeks 3–4
40%
Progress at Week 4
Consolidation — neural pathways forming
The neural pathways are beginning to form. The child's nervous system is starting to recognise the equipment as a reliable source of vestibular input. Look for these consolidation signs — they are the hallmarks of real neurological change.
Anticipatory Behaviour
Child anticipates the session — may go to the equipment area spontaneously before you suggest it. This is self-initiation: the highest early-phase indicator.
Duration Increase
Equipment engagement duration increases from 1 minute to 3–5 minutes. The vestibular "cup" is taking longer to fill, but the child is seeking to fill it through the equipment.
Spinning Episodes Decreasing
Uncontrolled spinning episodes decrease by 30–50% from baseline. Track this using your data sheet (Step 7).
Post-Session Regulation
Child is calmer for longer after sessions. The proprioceptive grounding is working. The system is learning to organise itself after controlled input.
If the child consistently engages for 5+ minutes and shows clear regulation improvement post-session, increase to 2 sessions per day (morning and afternoon) and introduce one new material from the 9 materials list. You may notice you're more confident too.
Week 5–8: Mastery Indicators
Act IV: Progress Arc
Weeks 5–8
75%
Progress at Week 8
Mastery — self-regulation emerging
Independent Equipment Use
Child uses rotation equipment independently as a regulatory strategy — without parent prompting
60–80% Reduction
Uncontrolled spinning episodes reduced by 60–80% from baseline — measurable, observable, neurologically significant
Multiple Strategies
Child uses at least 2–3 different vestibular strategies — not just spinning. The repertoire has expanded.
Self-Monitoring
Child begins to self-monitor: shows awareness of body's movement needs — the precursor to full self-regulation
Maintenance Check: Does regulated behaviour persist on days without a formal session? If the child maintains reduced spinning and uses equipment/alternatives on unstructured days, the neural pathways are consolidating. 🎖️MASTERY UNLOCKED — when the child uses 3+ regulatory strategies independently and participation in activities is no longer significantly impacted.
🎉 Celebrate This Win
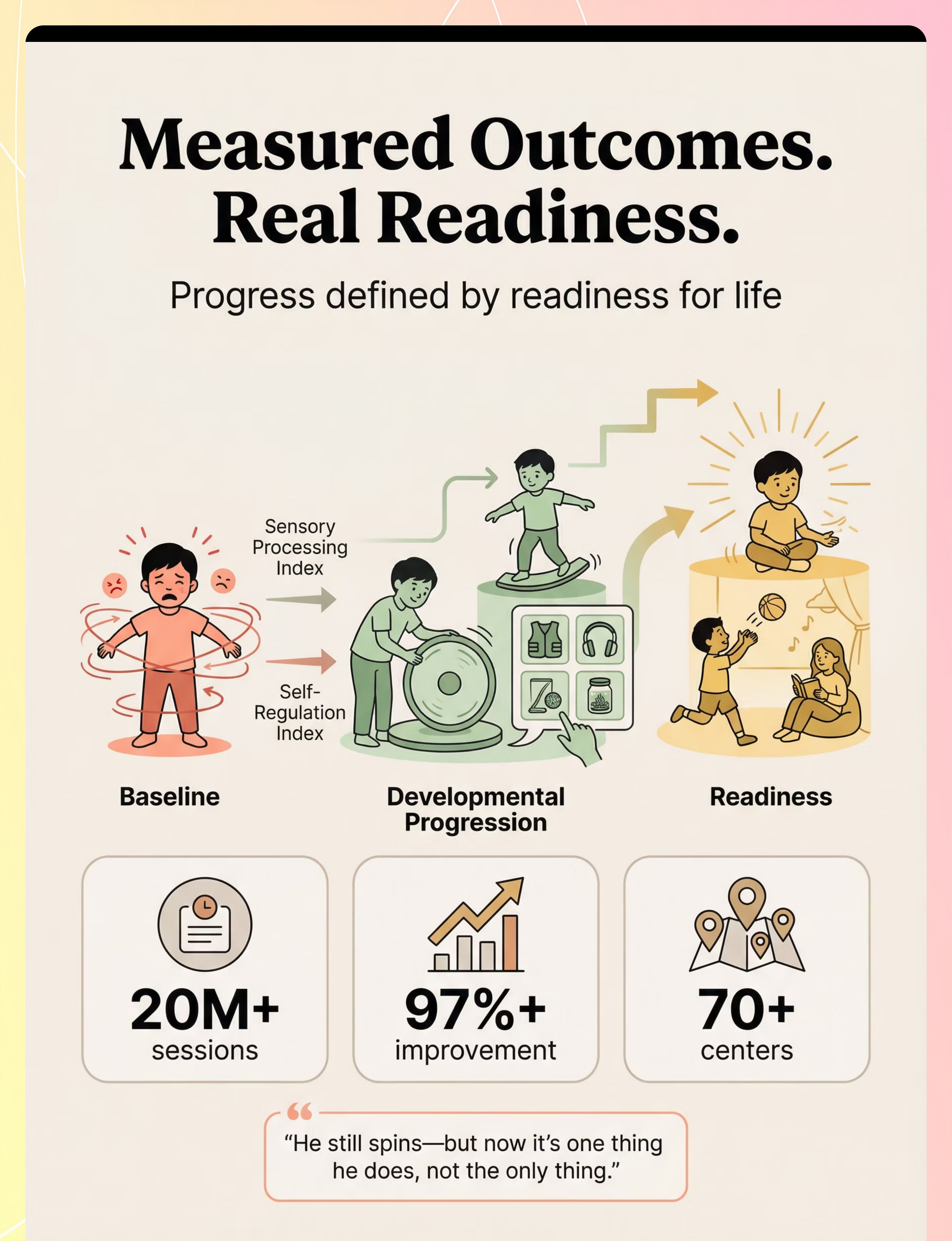
"He still spins — but now it's one thing he does, not the only thing he does."— Parent, Pinnacle Network
Five to eight weeks ago, you were watching your child spin in circles while the world stared. You were told to "just stop him." You were told it was a phase. You were told it was a behaviour problem. You knew it was something else. And you were right.
You provided safe rotation when the world said "just make him stop."
You added heavy work when the system needed grounding.
You introduced balance challenges when the system was ready to grow.
You built a schedule that fed the vestibular need before it became desperate.
Your child grew because of your commitment. Mark this milestone. Take a photo of your child on their balance board. Write in a journal what has changed. Tell your spouse, your parents, your child's teacher: "We did this together."
🚩 Red Flags — When to Pause
Trust your instincts — if something feels wrong, pause and ask. The following signs require professional consultation before continuing the protocol.
🚩 Spinning is INCREASING despite 4+ weeks
May indicate a more complex vestibular profile requiring clinical assessment. Do not increase protocol intensity without professional guidance.
🚩 New concerning behaviours emerge
Head banging, extreme self-injury during or after spinning → Seek immediate developmental paediatrician evaluation.
🚩 Regression in other developmental areas
Lost words, lost eye contact, lost skills → Urgent: contact your paediatrician and Pinnacle helpline immediately.
🚩 Repeated vestibular overload symptoms
Nausea, pallor, falling without recovery appearing repeatedly → Protocol intensity exceeds current capacity. Seek OT assessment.
🚩 Severe distress at sight of equipment
Equipment has become aversive. Stop using that specific material immediately and seek guidance on re-pairing.
01
Self-Resolve
Adjust protocol using troubleshooting and personalisation guidance
02
Teleconsult
Book a virtual consultation → pinnacleblooms.org/teleconsult
03
Clinic Visit
Find your nearest Pinnacle centre → pinnacleblooms.org/centers
04
Emergency
FREE National Autism Helpline → 9100 181 181 (16+ languages, all hours)
The Progression Pathway
This technique is one node in a structured developmental sequence. Understanding where it sits — and where it leads — helps you plan your child's full vestibular development arc.
Efficient vestibular processing → Self-regulated movement repertoire → Full participation across home, school, and community settings → Readiness for life. Each technique in this sequence builds the foundation for the next — a carefully engineered developmental staircase.
Related Techniques in This Domain
You already own materials for 4 of these techniques — your investment in this protocol opens the door to the entire vestibular domain.
Technique | Level | Key Materials | You Own | |
A-079: Child Is Always in Motion | Intro | Balance boards, sensory schedules | ✅ | |
A-080: Child Seeks Intense Movement | Intro | Weighted vest, resistance bands | ✅ | |
A-082: Child Crashes Into Everything | Core | Weighted vest, body sock, crash pad | Partial | |
A-083: Child Has Balance Difficulties | Core | Balance board, stepping stones | ✅ | |
A-084: Child Avoids Movement | Advanced | Gentle swing, weighted blanket | Partial | |
K-1015: Vestibular Processing Guide | Education | No materials needed | ✅ |
Your Child's Full Developmental Map
This technique is one piece of a larger plan. Vestibular regulation impacts not just sensory processing, but also motor coordination, attention regulation, emotional regulation, and social participation. When the spinning decreases and regulation improves, downstream improvements cascade across multiple domains.
Preview of 9 materials that help when child spins excessively Therapy Material
Below is a visual preview of 9 materials that help when child spins excessively therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.







Link copied!

Families Who've Been Here
Act V: Community & Ecosystem
Before: "Our 4-year-old son spun 20–30 times a day. In the kitchen, the grocery store, the playground. He'd spin until he fell over, get up, and spin again. His preschool teacher was at a loss — he'd spin instead of participating in everything. Other kids stared."
After (8 weeks): "We started with a sit-and-spin at home — scheduled times when spinning was available. Then added heavy work activities before transitions. Then balance board time in the morning. Slowly, the desperate quality of the spinning decreased."
"The spinning isn't gone. But the desperation is. And that changes everything."
Before: "My daughter would spin in circles at every family gathering. Relatives whispered. I felt judged. I didn't know what to do except hold her still, which made her scream."
After (6 weeks): "Now she has a 'movement bag' we bring everywhere — a wobble cushion, resistance band, and her regulation cards. At our last family dinner, she used her wobble cushion under the table and sat through the entire meal."
From the Therapist's Notes: One child's post-rotary nystagmus was initially absent (indicating severe vestibular under-responsivity). After 8 weeks of graded vestibular input, nystagmus became detectable — a neurological marker of improved vestibular processing capacity. Spinning episodes decreased from 25+/day to 5–7/day. Illustrative case; outcomes vary by child profile.