
"Every birthday party is the same story. He arrives. He finds a corner. The other kids are laughing together — and he's watching from twenty feet away."
You've whispered "go play with the kids" a hundred times. You've guided him gently toward the group. And every time, he drifts back to the edge. At school, it's the circle time floor, the fence perimeter at recess, the table corner during group projects. He's watching. He's aware. You can see he wants to belong.
9 Materials That Help With Group Participation
From the edge to the circle — with the right tools, it's a learnable journey.
From the edge to the circle — with the right tools, it's a learnable journey.
You are not failing. Your child is not broken. Group participation is a skill constellation — and skill constellations can be built.
FREE National Autism Helpline: 9100 181 181 | 24×7 | 16+ languages
FREE National Autism Helpline: 9100 181 181 | 24×7 | 16+ languages
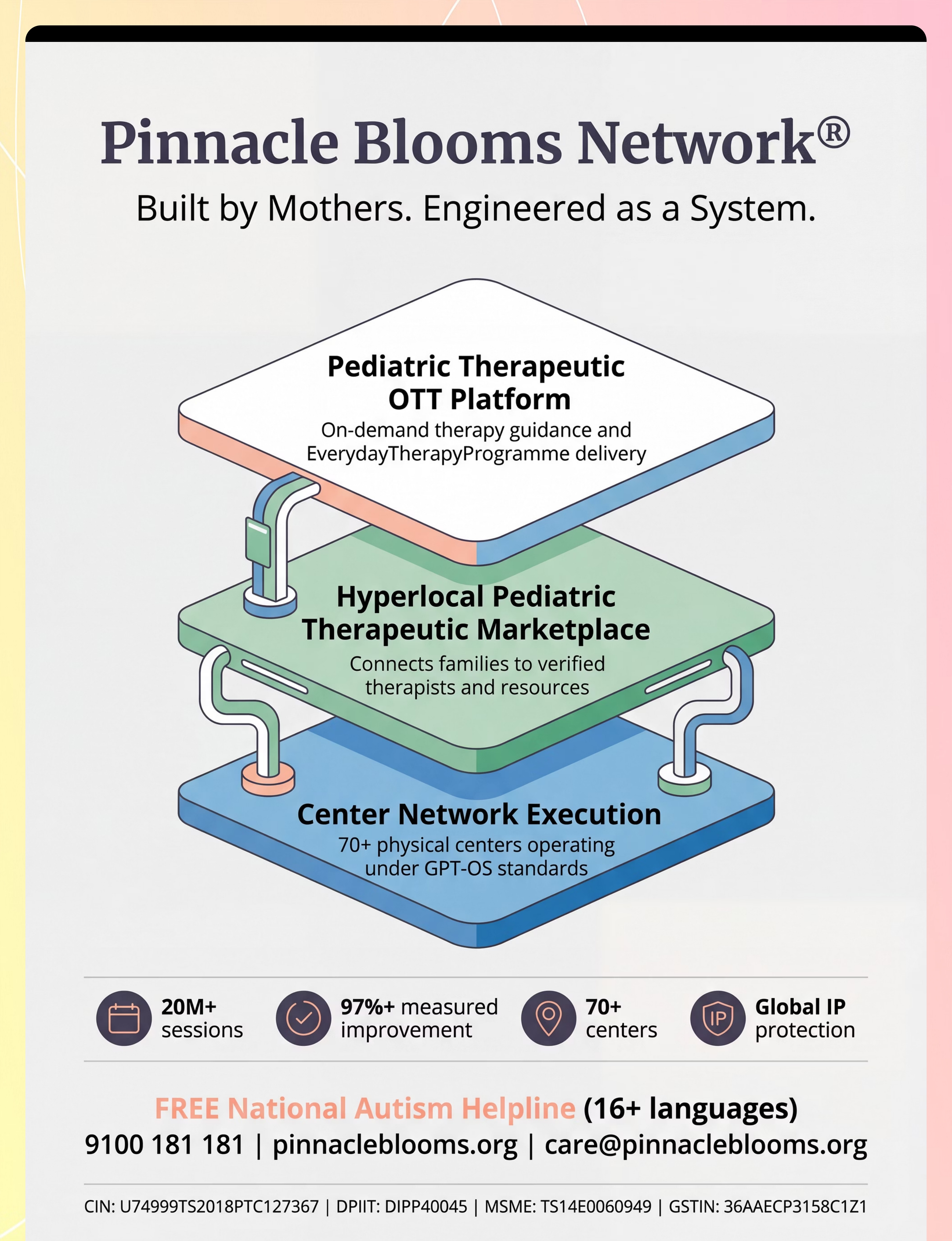
Pinnacle Blooms Network®
OT • SLP • ABA/BCBA • SpEd • NeuroDev • Pediatrics

ACT I — WHY
The Numbers
You Are Among Millions of Families Navigating This Exact Challenge
Group participation difficulty is not a character flaw. It is a documented, measurable challenge affecting millions of children across autism spectrum, ADHD, social anxiety, developmental delay, and language differences worldwide. Across 70+ Pinnacle centers operating under GPT-OS® clinical standards, group participation consistently ranks among the top 5 parent-reported challenges at initial intake.
80%
Experience Group Difficulty
Of children with ASD experience significant social participation difficulties in group contexts (PRISMA, 2024)
1 in 36
Children Have Autism
In the US (CDC, 2023); India estimates 1–1.5% of pediatric population
21M+
Therapy Encounters
At Pinnacle Blooms Network® — real data, real families navigating this exact challenge
You are not the only parent watching your child stand at the edge of a birthday party, longing for inclusion that feels unreachable. You are among a global community — and there is a proven, structured path forward.

ACT I — WHY
The Neuroscience
This Is a Wiring Difference. Not a Behaviour Choice.
The Neuroscience
Group environments activate multiple brain systems simultaneously:
- Prefrontal Cortex: Executive control for turn-taking, rule-following, impulse regulation
- Superior Temporal Sulcus: Social cue reading — tracking multiple faces, voices, movements
- Amygdala: Threat detection — in sensory-sensitive children, groups can trigger low-level threat responses
- Mirror Neuron System: Imitation and social learning — critical for "reading" group norms
- Anterior Cingulate Cortex: Prediction & error detection — groups are unpredictable, this cortex works overtime
What This Means for Your Child
When your child stands at the edge of a group, their brain is not being defiant. It may be:
- Overwhelmed — processing 8 simultaneous social channels when the capacity is 2
- Confused — unable to decode the invisible "rules" that neurotypical children absorb passively
- Dysregulated — the sensory complexity of groups pushes them into survival mode
- Under-scripted — genuinely not knowing what to do, when to speak, how to enter, what role to take
The 9 materials in this page address each of these brain-level barriers directly.

ACT I — WHY
Development Timeline
Your Child's Development in Context — A WHO/UNICEF Framework
Children with autism, ADHD, developmental delay, or social communication differences often "stall" at earlier developmental stages — engaging in parallel play (playing alongside peers, not with them) when their neurotypical classmates have moved to cooperative play (shared goals, defined roles, coordinated action). This is not a permanent state. It is a developmental waypoint with a clear forward path.
12–18 Months
Parallel Play — watches peers, plays independently alongside others
2–3 Years
Associative Play — shares loosely, loose interaction with peers
3–5 Years
Early Cooperative — shared goals begin to emerge
6–8 Years
Complex Group — rules + roles, coordinated action
8–12 Years
Peer Group Mastery — social politics, independent navigation
← Common Intervention Zone for Group Participation → Ages 3–7 years. Common co-occurring challenges: sensory processing difficulties, executive function delays, pragmatic language differences, emotion regulation. The WHO Care for Child Development (CCD) Package — implemented in 54 countries — specifically includes peer interaction and group participation as developmental monitoring indicators.

ACT I — WHY
Evidence Grade
Clinically Validated. Home-Applicable. Parent-Proven.
⭐⭐⭐⭐ LEVEL I EVIDENCE
Systematic Reviews + Randomized Controlled Trials
These are not theories. These are peer-reviewed findings, replicated across populations, validated in Indian clinical contexts, and operationalized through 21 million Pinnacle therapy sessions.
Key Evidence Sources
Study | Finding | |
PRISMA Systematic Review (2024) | 16 studies confirm structured material-based intervention is evidence-based practice for ASD — PMC11506176 | |
Meta-analysis, World J Clin Cases (2024) | 24 studies: structured intervention promotes social skills, cooperative behavior, peer interaction — PMC10955541 | |
Indian RCT, Indian J Pediatr (2019) | Home-based structured intervention with parent delivery showed significant outcomes in Indian pediatric population | |
NCAEP Evidence-Based Practices (2020) | Social stories, video modeling, visual supports classified as evidence-based practices for autism | |
WHO NCF (2018) | Responsive caregiving with structured play and social opportunities is core to nurturing care globally |
For personalized assessment: 9100 181 181

ACT II — WHAT
The Technique
9 Materials That Support Group Participation
Parent-Friendly Name: The Group Toolkit
Formal Definition: Group participation is the complex, multi-layered skill of successfully engaging as a member of a social group — whether structured (circle time, team sport, classroom project) or unstructured (birthday party, playground, family gathering). It encompasses: reading and entering group activities, understanding group norms and rules, taking turns in multi-person sequences, coordinating actions with multiple people simultaneously, managing the sensory and emotional demands of group contexts, and flexibly adapting to group dynamics.
The 9 materials in this page address the nine most common functional barriers to group participation, each grounded in a distinct evidence base from occupational therapy, applied behavior analysis, speech-language pathology, and special education.
Social Skills Development
Group Dynamics & Peer Interaction
Ages 3–12
Home + Clinic + School settings
Multi-Disciplinary
OT + SLP + ABA + SpEd
H-707
Social Skills Series Episode 707

ACT II — WHAT
Who Uses This
This Is a Multi-Disciplinary Toolkit — Because the Brain Doesn't Organize by Therapy Type
🟣 Occupational Therapist (Primary Lead)
Addresses the sensory regulation barrier. Uses sensory diet, regulatory tools, environmental modification, and activity grading to help the child tolerate and thrive in group sensory environments.
🔵 Speech-Language Pathologist
Addresses the social communication barrier. Works on social stories, script training, pragmatic language for group entry ("Can I play?"), conversational turn-taking, and reading group communication cues.
🟢 ABA / BCBA Therapist
Addresses the behavioral skill deficit barrier. Uses video modeling, social skills group training, reinforcement systems, and graduated exposure protocols.
🟡 Special Educator
Addresses the hidden curriculum barrier. Creates visual rule cards, role assignment systems, structured group activities, and classroom accommodation plans.
🔴 NeuroDev Pediatrician
Evaluates underlying neurological contributors — sensory processing disorder, executive dysfunction, social anxiety comorbidities — and coordinates medical management where relevant.
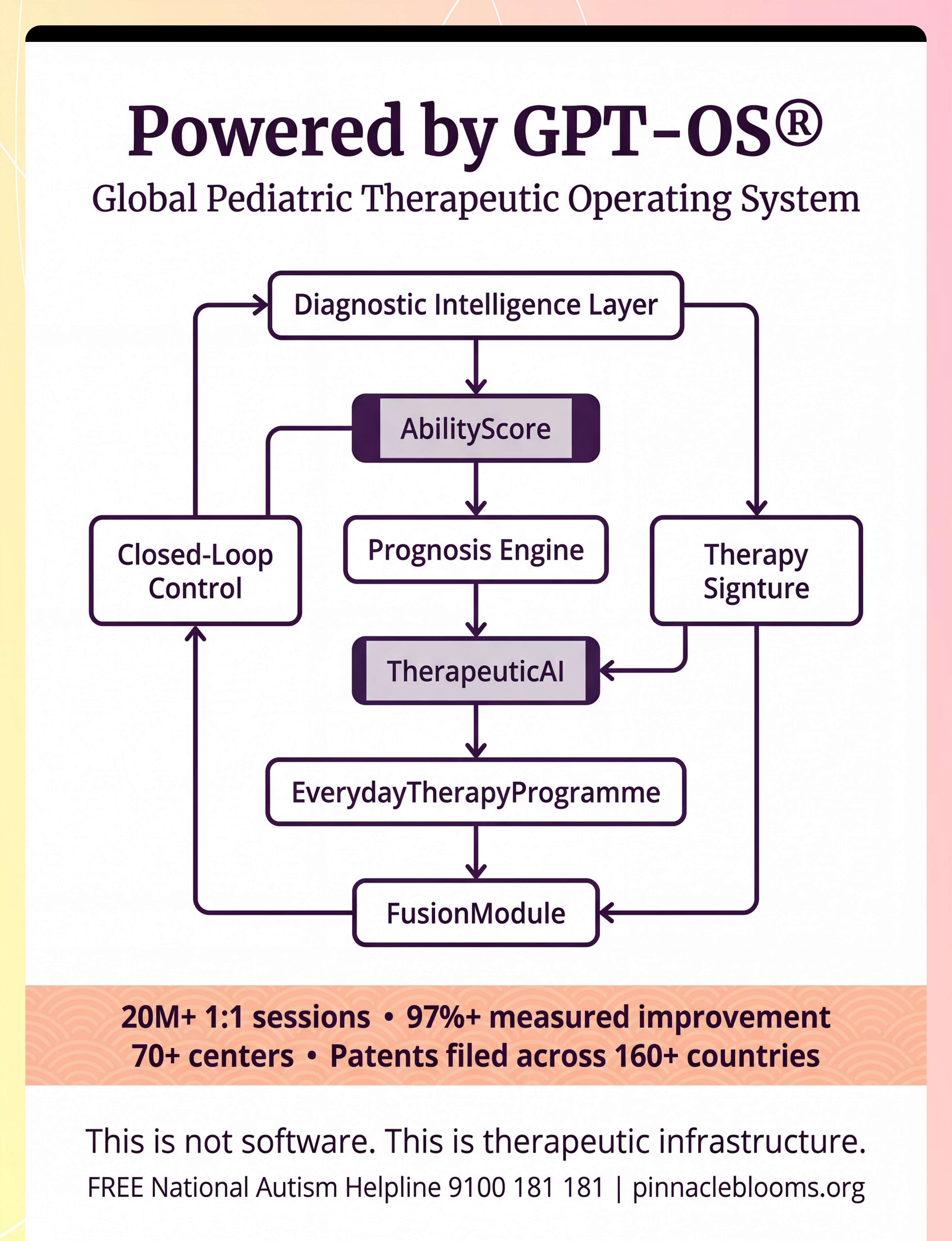
At Pinnacle Blooms Network®, all five disciplines contribute to a single FusionModule™ plan. Group participation goals are set once, tracked across all therapy hours, and reported through a unified GPT-OS® dashboard.

ACT II — WHAT
What This Targets
Precision Targeting — What These 9 Materials Build
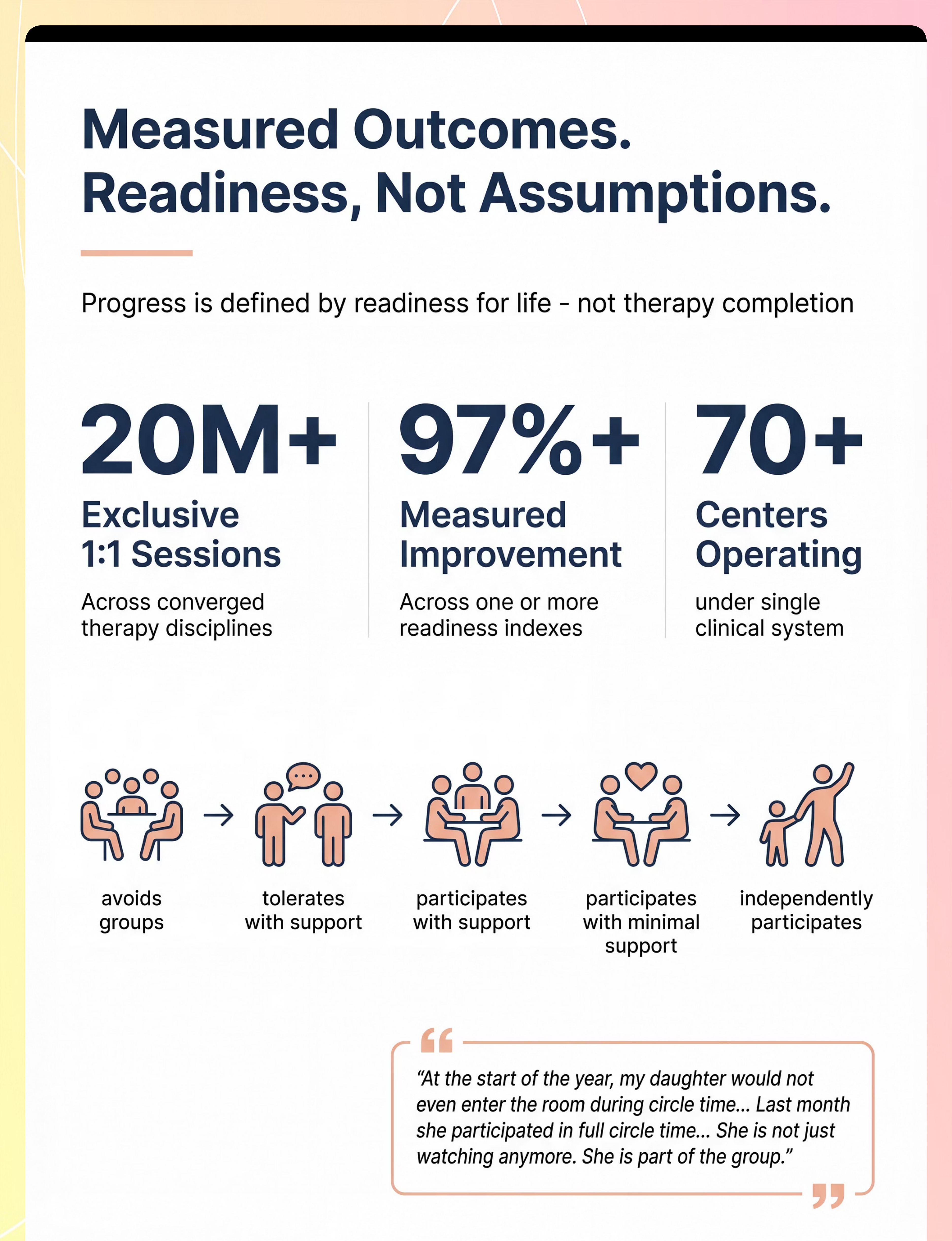
Observable behavior indicators range from Avoidance (refuses groups, flees, covers ears) → Tolerates (stays near group, watchful) → Participates (supported) (joins with adult guidance) → Participates (minimal support) (initiates entry, stays for duration) → Independent (joins, navigates, contributes, maintains — independently). Research confirms social skills, adaptive behavior, and sensory regulation as primary, secondary, and tertiary targets for structured material-based intervention (PMC10955541).

ACT II — WHAT
Materials 1–4
The 9 Group Participation Materials — Canon-Validated (Part 1)

Material 1 — Cooperative Board Games
₹800–2,500 | Examples: Hoot Owl Hoot, Outfoxed, Forbidden Island, First Orchard
Why it works: Makes invisible group rules visible — shared goals, clear turns, cooperative structure.

Material 2 — Visual Turn-Taking Cues
₹100–800 | Examples: Talking stick, turn spinner, photo sequence board, My Turn/Wait cards
Why it works: Externalizes who-goes-when for children who can't track it internally.

Material 3 — Social Stories & Group Scripts
₹200–1,500 | Examples: "Joining a Game," "Circle Time," "Birthday Party" stories
Why it works: Provides the hidden curriculum of groups in explicit, readable form.

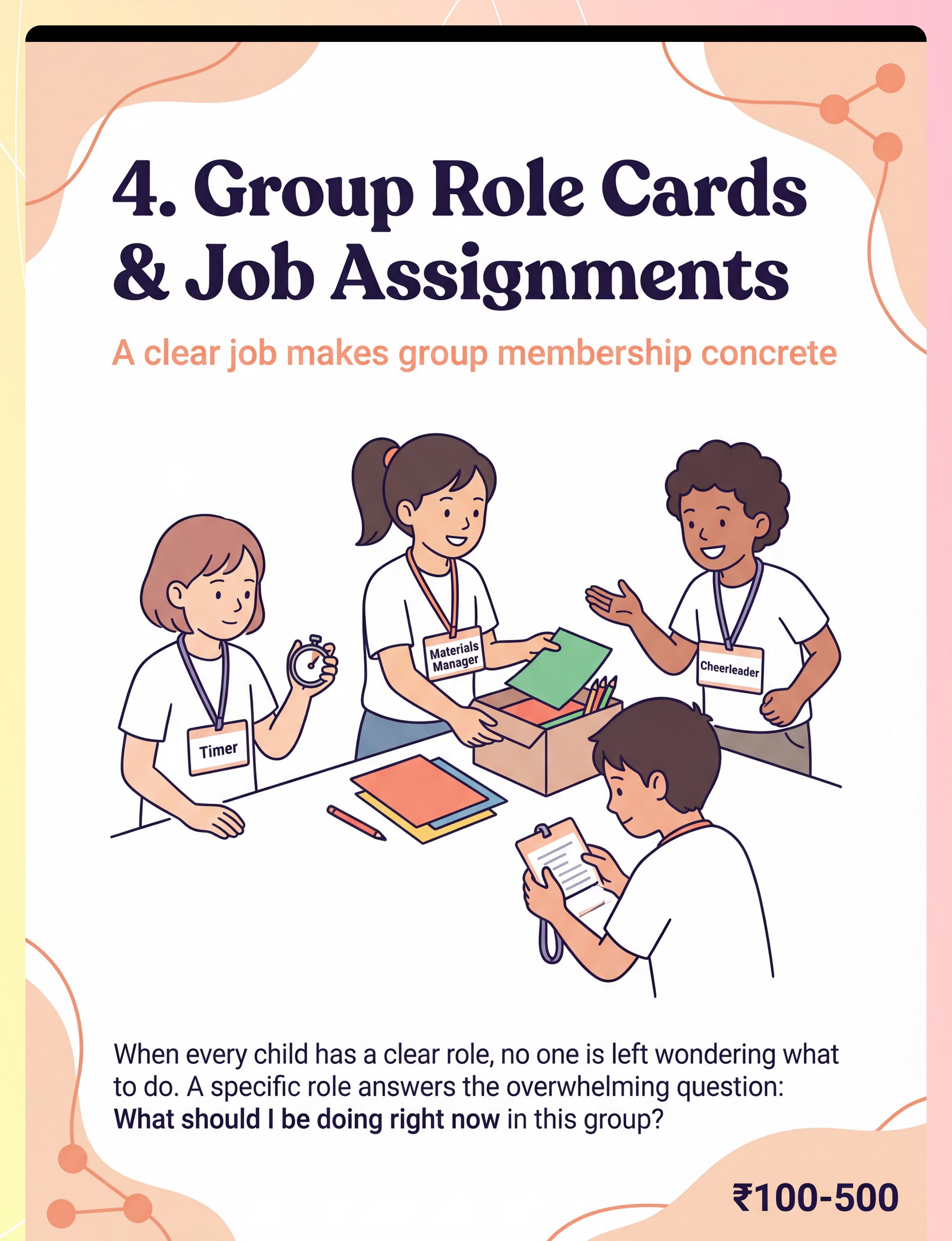
Material 4 — Group Role Cards & Job Assignments
₹100–500 (mostly DIY) | Examples: Timer card, Materials Manager, Cheerleader, Reporter
Why it works: Gives the child a concrete anchor — "I know exactly what I'm supposed to do."

ACT II — WHAT
Materials 5–9
The 9 Group Participation Materials — Canon-Validated (Part 2)

Material 5 — Play Parachute
₹500–2,000 | Sensory / Gross Motor / Cooperative Play Equipment
Why it works: Physically requires coordination — the parachute only rises when everyone lifts together.

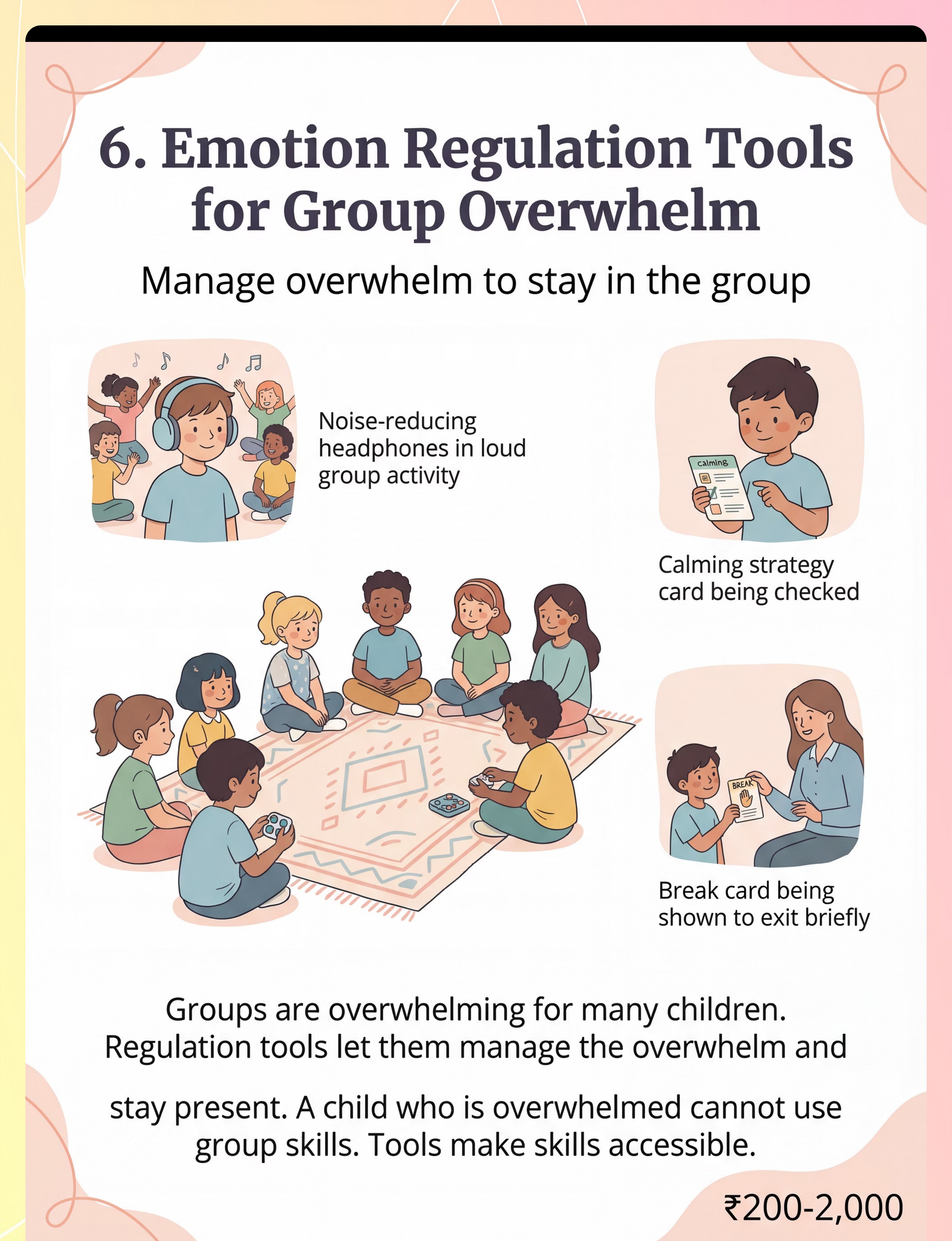
Material 6 — Emotion Regulation Tools
₹200–2,000 | Examples: Quiet fidgets, noise-reducing headphones, break cards, calming cards
Why it works: Groups are dysregulating — regulation tools keep the child present and accessible.

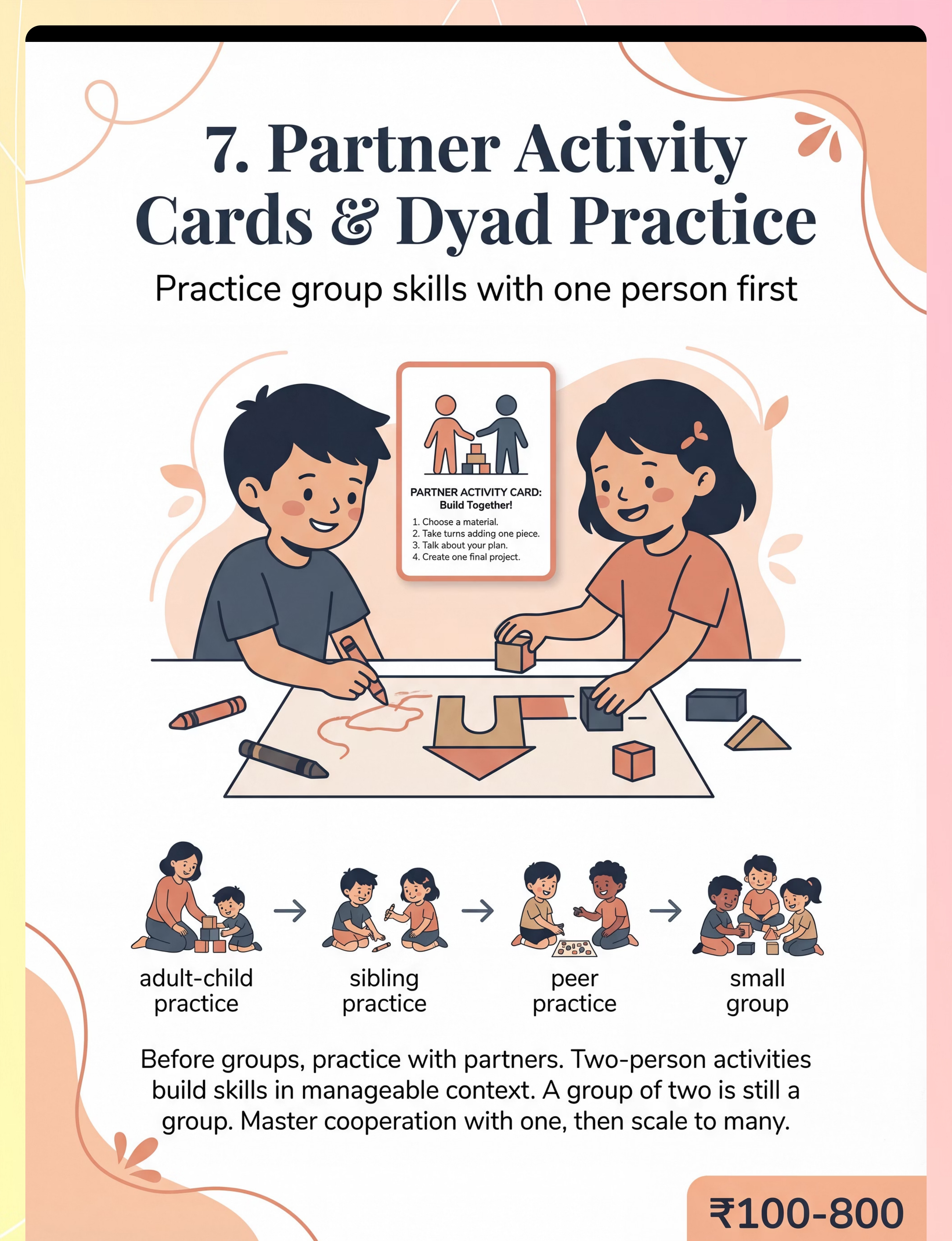
Material 7 — Partner Activity Cards (Dyad Practice)
₹100–800 | Examples: Cooperative drawing cards, interview question cards, two-person building activities
Why it works: Group skills need stepping stones — mastery with one person before navigating many.

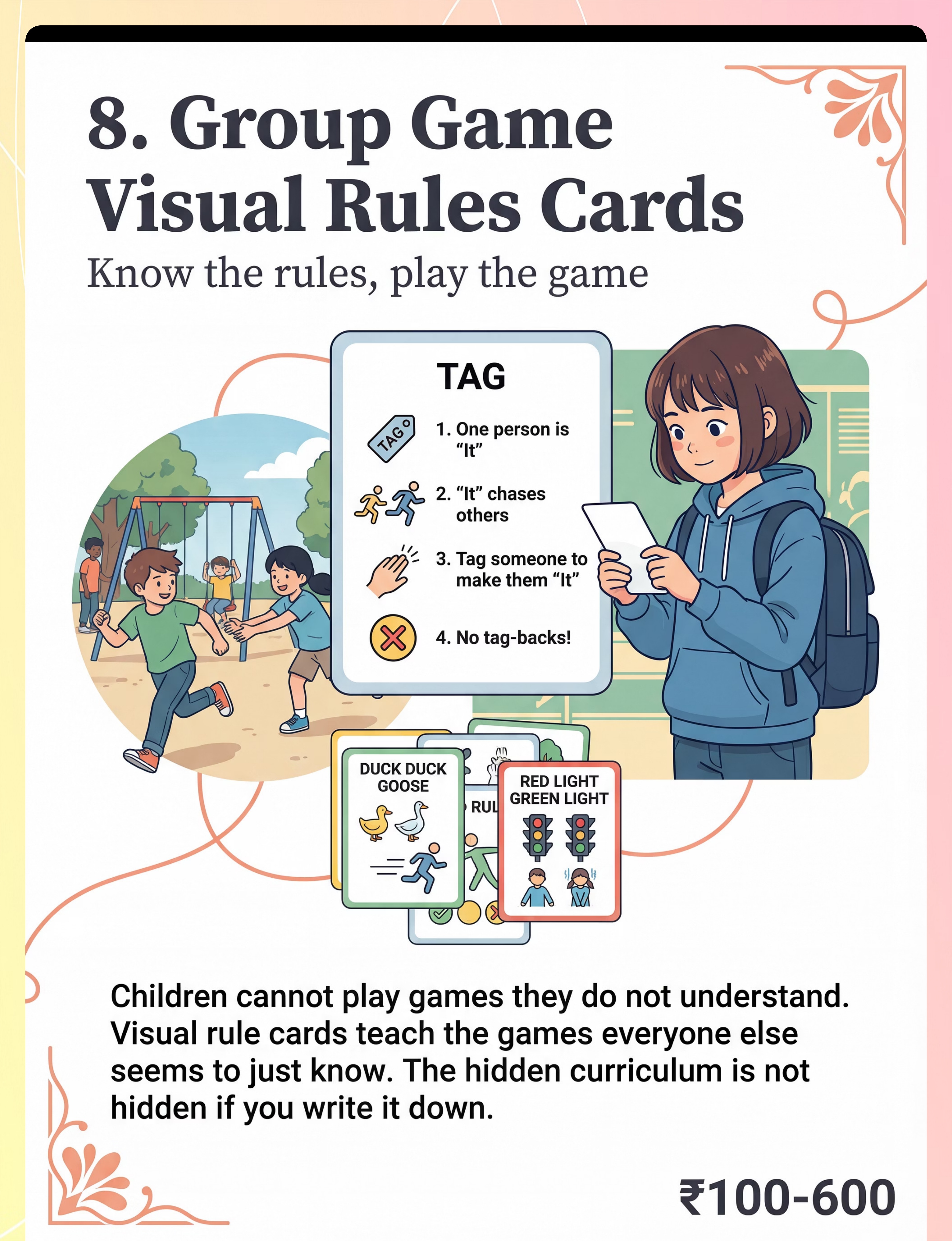
Material 8 — Group Game Visual Rules Cards
₹100–600 (DIY) | Examples: Tag rules card, Red Light Green Light card, Duck Duck Goose card
Why it works: Children can't play games they don't understand — visual rules unlock participation.

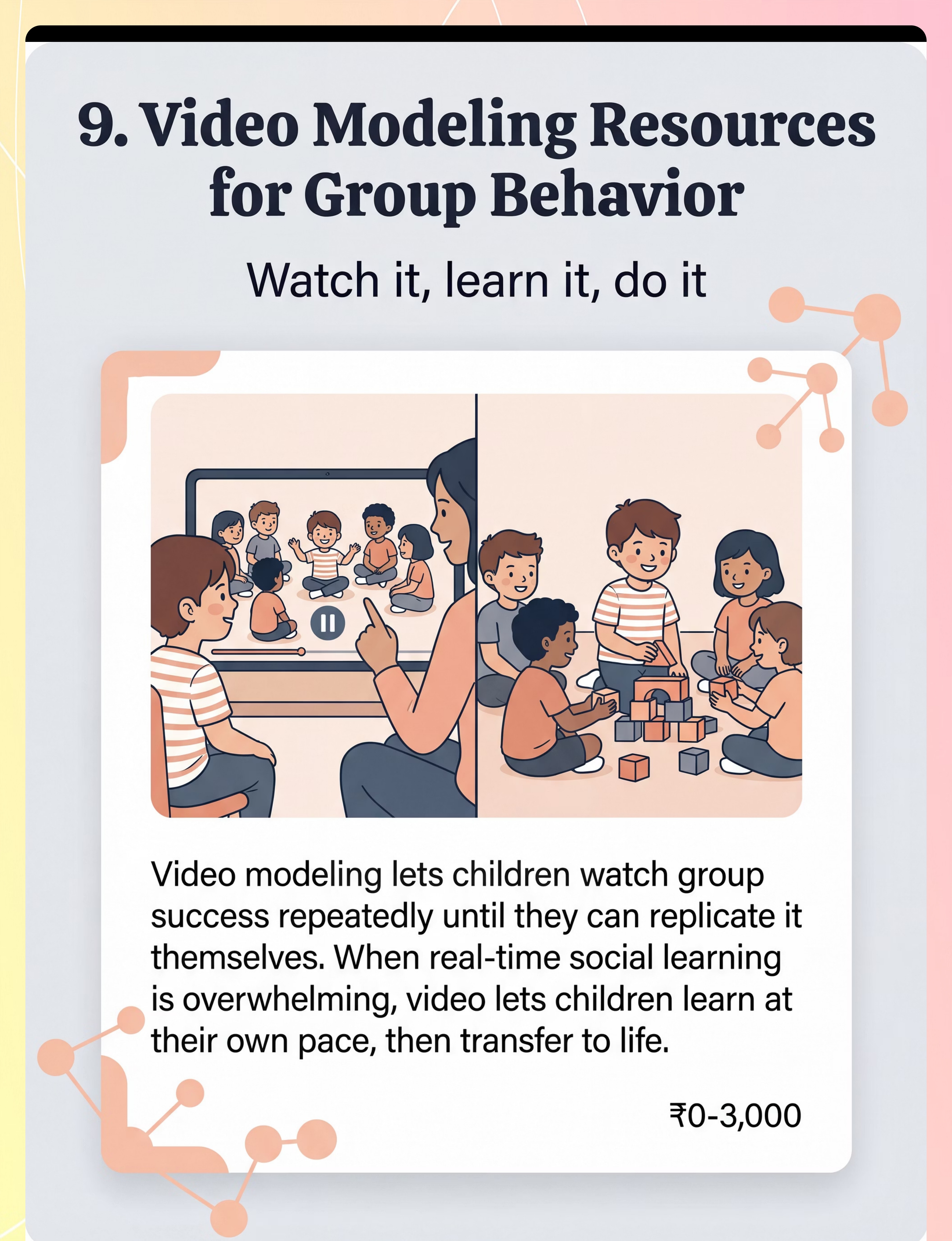
Material 9 — Video Modeling Resources
₹0–3,000 | Examples: Model Me Kids, YouTube social skills channels, custom family videos
Why it works: Children can watch group success repeatedly at their own pace before attempting it live.

ACT II — WHAT
DIY & Zero-Cost Alternatives
Every Family Can Start Today — Zero Cost Required
WHO Nurturing Care Framework Principle: Effective intervention must be accessible across all economic contexts. Every material in this page has a household alternative that preserves the therapeutic mechanism.
Material | Clinical Version | ₹0 Household Version | |
Cooperative Board Game | Hoot Owl Hoot ₹800+ | Modify any card game to "all vs. the deck" — team goal with house rules | |
Visual Turn Indicator | Commercial spinner ₹300 | Write names on paper plates, use clothespin as pointer | |
Social Story | Printed book ₹200+ | A4 paper, drawn scenes, handwritten in child's language | |
Role Cards | Laminated cardstock ₹100 | Index cards, hand-drawn roles, safety-pin to shirt | |
Parachute | Commercial ₹800 | Large bedsheet — same cooperative physics, zero cost | |
Regulation Fidget | Therapy putty ₹200 | Rice in sealed zip-lock bag; rolled fabric scrap | |
Break Card | Printed card ₹50 | Green/red index card — green = stay, red = need break | |
Game Rules Card | Printed/laminated ₹100 | Hand-drawn on A4, folded to pocket size | |
Video Modeling | Commercial program ₹1500+ | Record sibling/family member on phone; free YouTube |
Important: For children with significant sensory sensitivities, noise-reducing headphones genuinely improve group tolerance. When one purchase is possible, this is the Pinnacle clinical team's highest-priority recommendation.

ACT II — WHAT
Safety First
Read Before Every Session — Non-Negotiable Safety Gate
🔴 DO NOT Proceed If:
- Child is showing signs of illness (fever, pain, physical distress)
- Child experienced significant trauma or extreme dysregulation within past 2 hours
- Using a group with peers who have previously bullied or rejected this child
- Sensory overwhelm is already present before the session begins
- Child is communicating "no" through consistent refusal — honour this, then re-approach
🟡 MODIFY Approach If:
- Child is tired (after school, post-nap) — choose lower-demand activities
- Child had a difficult day — use regulation tools proactively, not reactively
- Group size feels large — start with dyad before full group
- New environment — preview the space first, social story about the new location
🟢 SAFE to Proceed:
- Child is fed, rested, in calm baseline state
- Environment is set up and distractions removed
- Regulation tools ready before they're needed
- Group members are safe, familiar, and supportive
- Clear exit/break plan available
Material Safety: Talking sticks — no sharp edges. Lanyards for role cards — breakaway safety clasps ONLY. Parachute — lightweight, breathable. Fidgets — no small parts for under-3. Video screens — 10–15 min max. 🛑 STOP IMMEDIATELY IF child shows acute distress, physical self-harm, or severe emotional dysregulation. "Session abandonment is not failure — it is good clinical judgment."
Clinical support: 9100 181 181
Clinical support: 9100 181 181

ACT II — WHAT
Set Up Your Space
The Right Space Prevents 80% of Session Failures
The Group Zone
- Carpet or rug defines the boundary — children know "in circle = in group"
- Circle or facing arrangement — all participants visible to each other
- Adult positioned WITHIN the group, not outside watching
- Group size: start with 2–3 children for initial sessions
Materials Station
- All materials within adult reach, not child's impulsive reach
- Role cards prepared and labeled before group starts
- Visual turn indicator set up and visible to all
The Break Corner (Non-Negotiable)
- Designated quiet spot, visible from group but separate
- 2–3 calm-down items available (book, fidget, sensory toy)
- MUST be established BEFORE group starts — not improvised mid-session
Environment Checklist
- Noise: reduce background noise; turn off television, music
- Lighting: natural or warm light preferred; avoid harsh fluorescent
- Temperature: comfortable, not hot
- Remove toys that might attract more interest than the group activity

ACT III — HOW
Readiness Check
The Pre-Flight Check — 60 Seconds Before Every Session
Run this quick checklist before every session to determine whether to proceed, modify, or postpone.
Indicator | ✅ GO | ⚠️ MODIFY | 🛑 POSTPONE | |
Fed in last 2 hours? | Yes | Not recently | Hungry/stomach upset | |
Rested? | Yes | Slightly tired | Very tired/just woke | |
Regulated? | Calm, alert | Some excitement | Dysregulated/post-meltdown | |
Recent illness/pain? | None | Mild, managed | Sick today | |
Willing to engage? | Shows interest | Neutral | Active refusal | |
Group peers safe? | Familiar, friendly | Mixed | Recent conflict with peers |
5–6 GOs ✅
Proceed to Step 1: The Invitation
2–4 GOs ⚠️
Modify — use dyad instead of group; reduce group size; shorter duration
Any POSTPONE 🛑
Rest today — brief 1:1 preferred activity. No demands. Return tomorrow.

ACT III — HOW
Step 1 of 6
Step 1: The Invitation
Duration
30–60 seconds
Principle
ABA Pairing + OT "Just-Right Challenge"
The Opening Script:
"Hey, we're going to play a really fun game together. It's called [game name]. You're going to be on my team — we play together, not against each other. Want to see what it looks like?"For younger/lower-demand:
"Look what I found! Want to see this? Come sit with me for a second…"
Parent Body Language
- Seated or kneeling at child's eye level
- Open posture, no hovering
- Relaxed, unhurried — if YOU feel rushed, the child will feel rushed
- Material visible but not pushed toward child
Acceptance Cues to Watch For
- Makes eye contact with the material
- Moves toward you or the material
- Asks a question about the game
- Sits near you without being asked
Resistance Responses
- Walks away → Follow playfully, don't demand. Try again in 5 min.
- Says "no" → Honour it. Offer a lower-demand activity.
- Ignores → Try playing with sibling/parent first to generate interest.

ACT III — HOW
Step 2 of 6
Step 2: The Engagement
Duration
1–3 minutes
Principle
Gradual exposure, visual scaffolding first
For Cooperative Board Game
"See these pieces? We each have a role. When the spinner says it's your turn, that arrow points to YOU. Then we move together toward the goal. I'll show you first — watch." → Model one complete turn yourself, narrating aloud.
For Visual Turn-Taking Cue
"This stick is the talking stick. Only the person holding it speaks. I hold it → I talk. You hold it → you talk. Let me show you how it goes." → Demonstrate the pass. Let child hold the stick first.
For Parachute
"Let's both grab an edge. Ready? When I count to 3, we both lift. Ready — 1, 2, 3… LIFT! Did you feel that? We made it rise TOGETHER!" → Start with just 2 people. Feel the cooperative physics first.
Reinforcement Cue: When the child makes ANY positive engagement gesture → immediate, specific praise within 3 seconds: "YES! That's exactly it. You held the stick and waited — perfect turn-taking!"

ACT III — HOW
Step 3 of 6
Step 3: The Therapeutic Action
Duration
5–15 minutes (core session time)
Principle
Evidence-based material deployment with specific therapeutic targets
Cooperative Board Game
Play 1–3 rounds. Narrate cooperation: "When WE all contribute, WE win." Celebrate group process, not individual performance. Target: Shared goal pursuit, rule-following, turn-taking in sequence.
Visual Turn-Taking Cues
Circle activity with consistent turn indicator: "Now the arrow is on Maya. Maya's turn. Now it's coming to YOU — ready?"Target: Turn-taking comprehension, waiting regulation, sequence tracking.
Social Story
Read BEFORE the group activity (not during). Then: "What does the story say to do when you want to join? Right — walk up and say 'Can I play?' Let's practice that right now."Target: Group norm comprehension, script for entry/participation.
Role Cards
Assign roles before group begins. Point to card when their role is relevant: "You're the Timer. When the sand runs out, say STOP." Celebrate: "You did your Timer job perfectly — the whole group needed that!"Target: Group contribution identity, structured participation anchor.
Parachute Play
Progress through: waves → coordinated lifts → mushroom → games with balls. Narrate: "Look — when we ALL lift together, it flies! If one person drops their edge, it falls. We NEED each other."Target: Physical cooperative action, felt interdependence, group cohesion.

ACT III — HOW
Step 4 of 6
Step 4: Repeat & Vary
Duration
3–5 minutes total
Principle
Therapeutic dosage + satiation monitoring
Material | Target Reps | Variation to Maintain Engagement | |
Cooperative Game | 2–3 complete rounds | Change roles across rounds | |
Turn-Taking Cues | 5–8 turn sequences | Change the topic/content of each turn | |
Social Story | 3–5 times across the week | Role-play after reading instead of reading again | |
Role Cards | Full group activity (15–20 min) | Rotate roles in next session | |
Parachute | 3–5 cooperative activities | Progress from waves → mushroom → ball games |
Satiation Indicators (Child Is Done): Loses interest, looks away repeatedly; introduces off-topic behavior; asks to do something else; increased physical fidgeting or body language withdrawal.
"3 genuinely cooperative repetitions are worth more than 10 forced ones." — Pinnacle Clinical Dosage Principle
"3 genuinely cooperative repetitions are worth more than 10 forced ones." — Pinnacle Clinical Dosage Principle
What to Vary: Group composition (add or change one member) · Activity complexity · Your narration (highlight different cooperative elements each round) · Reinforcement type (praise → token → natural consequence of group success)

ACT III — HOW
Step 5 of 6
Step 5: Reinforce & Celebrate
Principle
ABA reinforcement — immediate, specific, enthusiastic
The Formula
Within 3 seconds + Specific behavior named + Enthusiastic delivery = MAXIMUM IMPACT
For turn-taking: "YES! You waited for Maya's turn AND took your turn when the arrow pointed to you. That is EXACTLY how groups work. Incredible!"
For cooperative contribution: "Look what happened when you held your edge — the parachute FLEW! Your contribution made that happen. Every person in this group needed you."
For group entry: "You walked up, you said 'Can I play?' — that was the exact right thing to say. You DID it. I am so proud of you."
For staying in the group: "You stayed for the whole game. You stayed in the circle even when it felt hard. That is growing, and I see it."
"You tried to join the group today. Even though it felt hard, you TRIED. That is the whole thing. That is growth." — Celebrate the attempt, not just the success.
Questions about reinforcement strategies? 9100 181 181

ACT III — HOW
Step 6 of 6
Step 6: The Cool-Down
Duration
2–3 minutes
Principle
Regulated ending prevents post-session dysregulation
This structured transition prevents abrupt endings that can cause dysregulation. Involve the child in tidy-up — contributing to the close of a shared activity is itself a group skill. "You were Timer today — can you be Cleanup Captain too?"
If Child Resists Ending
- Offer a time-visual: "When this sand runs out, we finish."
- Offer a bridge: "We can play this again tomorrow/Saturday."
- Never abruptly remove materials — gradual withdrawal.
Visual Supports for Cool-Down
- Visual timer (sand timer, digital countdown)
- "All Done" card
- First-Then visual: [tidy up] THEN [snack/preferred activity]

ACT III — HOW
Data Capture
60 Seconds of Data Now Saves Hours of Guessing Later
Field 1 — Duration in Group (minutes)
How many minutes did the child remain engaged in the group activity? Even 2 minutes longer than last week is measurable progress.
Field 2 — Support Level Required
0 = Independent | 1 = Verbal prompt only | 2 = Gestural prompt | 3 = Physical guidance needed. Record the highest support level required during the session.
Field 3 — Group Entry Attempt
Did the child initiate group entry themselves? YES / NO / PARTIAL. "Partial" = moved toward group but stopped; parent completed the entry.
Why This Data Matters: Your daily 60-second entries aggregate into GPT-OS® readiness scores. After 4 weeks: GPT-OS® generates a Group Participation Readiness Index update → your therapist receives a progress summary automatically → technique recommendations adjust based on your child's actual response pattern.
Access tracker at: pinnacleblooms.org/track | Download 4-week PDF: pinnacleblooms.org/resources/H-707-tracker
Access tracker at: pinnacleblooms.org/track | Download 4-week PDF: pinnacleblooms.org/resources/H-707-tracker

ACT III — HOW
Troubleshooting
Real Sessions Don't Go Perfectly — Here's What To Do
Child refused to join the group at all
Why: Group anxiety, previous negative group experience, or current dysregulation.
Do next time: Start smaller — dyad with parent only. No peers until child is comfortable in 2-person structure. Read "Joining a Game" social story for 3 days before attempting group again.
Do next time: Start smaller — dyad with parent only. No peers until child is comfortable in 2-person structure. Read "Joining a Game" social story for 3 days before attempting group again.
Child joined but left after 2 minutes
Why: Sensory overwhelm, duration beyond current capacity, or interest dropped.
Do next time: 2-minute participation IS a WIN if previous baseline was 0. Celebrate it. Next session aim for 3 minutes. Build duration in 1–2 minute increments. Use regulation tools proactively.
Do next time: 2-minute participation IS a WIN if previous baseline was 0. Celebrate it. Next session aim for 3 minutes. Build duration in 1–2 minute increments. Use regulation tools proactively.
Child tried to control the entire game
Why: Rigidity, anxiety about unpredictability, or insufficient understanding of shared control.
Do next time: Pre-assign roles before the game begins (role cards). Practice "you decide, then I decide" in dyad first.
Do next time: Pre-assign roles before the game begins (role cards). Practice "you decide, then I decide" in dyad first.
Child became dysregulated during group
Why: Sensory overwhelm or emotional escalation triggered by group dynamics.
Do next time: Introduce break cards BEFORE the next session. Practice using the break card in calm state. Proactively offer fidget at session start.
Do next time: Introduce break cards BEFORE the next session. Practice using the break card in calm state. Proactively offer fidget at session start.
Social story didn't transfer to real situation
Why: Story was read too long before the event, or situation differed from story.
Do next time: Read social story within 30 minutes of the group activity. Do a brief role-play of the specific scenario immediately after reading.
Do next time: Read social story within 30 minutes of the group activity. Do a brief role-play of the specific scenario immediately after reading.
Parachute caused sensory overwhelm instead of regulation
Why: Too loud, too fast, or too unpredictable for this child's sensory profile.
Do next time: Start with slow waves only. Add noise-reducing headphones. Build up to complex activities across multiple sessions.
Do next time: Start with slow waves only. Add noise-reducing headphones. Build up to complex activities across multiple sessions.
"Session abandonment is not failure — it is data." — Pinnacle Blooms Clinical Standard

ACT III — HOW
Adapt & Personalize
No Two Children Are Identical — Adjust Until It Fits
Sensory-Seeking Children
Parachute play first (intense input → then calm for social activity). Movement-based cooperative activities. Active fidget tools. Louder, more energetic group contexts tolerated better.
Sensory-Avoiding Children
Start with visual supports and games (low sensory demand). Noise-reducing headphones as standard. Smaller groups (2–3) before expanding. Break card practiced before needed. Dim lighting preferred.
High Anxiety Profile
More social story preparation. Higher predictability — same game, same group, same location for first 4 sessions. Video self-modeling using footage of child's own successful moments. More incremental exposure steps.
Age | Priority Focus | Group Size | Key Materials | |
3–5 years | Basic turn-taking, staying in circle | 2–3 | Cooperative simple games, parachute, role cards | |
5–8 years | Game rules, joining strategies, emotional regulation | 3–5 | Visual game rules, social stories, regulation toolkit | |
8–12 years | Complex dynamics, self-advocacy, group roles | 4–8 | Advanced cooperative games, video modeling, social scripts |

ACT IV — PROGRESS
Weeks 1–2
The First Two Weeks: Tolerance, Not Mastery
✅ Signs You Are On Track
- Child tolerates the group structure longer than baseline (even 60 seconds more)
- Any positive interaction with group material (looks at game, touches piece, accepts role card)
- Reduced intensity of resistance (less refusal, even if participation is minimal)
- Any curiosity about the activity from a distance
- Physical participation in family cooperative activity (parachute with siblings)
⏸️ What Is NOT Expected Yet
- Spontaneous group entry without prompting
- Following all game rules independently
- Sustained 15-minute group participation
- Peer-level social interaction within the group
- Transferring skills to school/public settings
Parent Milestone
The changes at weeks 1–2 are neurological (tolerance window expanding) and behavioral (baseline shifting). They are real and measurable — even when they feel invisible.
"If your child stayed in the group for 3 minutes today versus 1 minute last week — that is a 200% improvement. That is real progress in a real nervous system."

ACT IV — PROGRESS
Weeks 3–4
Weeks 3–4: The Neural Pathway Is Forming
Child begins to anticipate the group activity
Asks "when are we doing the game?" — the prefrontal cortex has encoded the sequence. This is a clinically significant moment most parents miss because it isn't dramatic enough to celebrate.
Spontaneous use of a group skill
Picks up talking stick without being told. When a child uses a skill spontaneously, it means the behavior has become automatic enough to transfer. Celebrate this.
Beginning to generalize
Uses "can I play?" phrase in a non-practiced context. Visible preference for cooperative game over solo play at times. Peer interaction increases, even if brief and supported.
When to Increase Intensity: Child breezing through current group size → add one more participant. Turn-taking is fluent with current indicator → reduce visual prominence slightly. Social story fully internalized → try the situation without pre-reading.
"You may notice you're running the session with less effort. Your intuition is getting calibrated to your child's group readiness signals. That's parent skill development happening alongside child development."
"You may notice you're running the session with less effort. Your intuition is getting calibrated to your child's group readiness signals. That's parent skill development happening alongside child development."

ACT IV — PROGRESS
Weeks 5–8 Mastery
Weeks 5–8: Mastery Indicators
🏆GROUP PARTICIPATION MILESTONE — Week 5–8 Mastery Level
✅ Core Mastery Criteria
- Independently enters familiar group activity (asks to join, waits, joins appropriately) at least 3 out of 5 opportunities
- Participates in structured group activity for 15+ minutes with minimal adult support
- Turn-taking (gives AND receives) in group of 3+ without explicit prompting
- Uses group skill in a novel context (generalization)
- Shows positive affect — enjoyment, not just compliance
🌐 Generalization Indicators
- Uses "can I play?" at playground without prompted rehearsal
- Participates in circle time at school with reduced adult support
- Cooperates in family game night without role cards as supports
➡️ When to Move Forward
- → H-708: Playground Friendship (applying group skills in unstructured peer contexts)
- → Increase group size, reduce structure progressively
- → Introduce competitive elements alongside cooperative skills
Maintenance Check: After 2 weeks without formal practice, does the skill persist? Yes → mastered. No → needs distributed practice in more varied contexts, not more intensity in a single context.

ACT IV — PROGRESS
Celebrate This Win
You Did This. Your Child Grew Because of Your Commitment.
There was a day, not long ago, when you stood at a birthday party and watched your child walk to the corner of the room. When circle time meant floor tantrums. When "group activity" meant your child at the perimeter, watching.And now — your child is in the circle. Your child held the talking stick and waited. Your child lifted the parachute edge with the group and felt it rise. Your child used words to join a game.You created that. Week by week, session by session, with patience that most people will never understand.That is not a small thing. That is a transformation.
From
Unable to participate in group activities without significant distress or avoidance
To
Active, supported, growing group participant with measurable skill progression
Timeline
5–8 weeks of consistent, evidence-based home practice
Family Celebration Suggestion: Celebrate with a special family cooperative activity of the child's choosing — they get to design the group game this time. 📸 Document a photo or video of a successful group participation moment. Share with your GPT-OS® therapist via the dashboard.
Share your child's progress with us: 9100 181 181

ACT IV — PROGRESS
Red Flags
These Signs Mean: Pause and Seek Professional Consultation
🔴 Behavioral Regression
Significant decrease in group tolerance despite consistent practice — worse than baseline after 4+ weeks. May indicate an unaddressed sensory, anxiety, or communicative need.
🔴 Extreme Distress Responses
Meltdowns increasing in frequency, duration, or intensity specifically in response to group activities — beyond what you'd expect for the learning curve.
🔴 Peer Victimization
Any indication the child is being bullied, excluded, or mocked in group settings. Group participation practice in unsafe peer environments can cause setbacks, not progress.
🔴 Self-Injurious Behavior
Any instance of self-harm in response to group activity demands. Stop all group practice immediately and contact your BCBA/therapist.
🔴 No Progress at Week 6
Absolutely no measurable progress after 6 weeks of consistent practice indicates technique mismatch or unidentified barrier. Professional evaluation required.
"Trust your instincts. If something feels wrong, pause and ask. Your child's safety is more important than any week's practice quota."

ACT IV — PROGRESS
Progression Pathway
Your Child's Developmental GPS — You Are Here
Long-Term Developmental Goal: Independent peer group participation → Community inclusion → Social confidence → Lifelong belonging capacity.
Parachute/Movement was strongest
→ H-720: Team Sport Participation
Social stories resonated most
→ H-715: Circle Time Mastery → H-708: Playground Friendship
Emotion regulation was primary blocker
→ Domain C techniques: Emotional Regulation foundations first
Group size was primary limiter
→ Continue H-707, gradually increase group size → then H-708

ACT IV — PROGRESS
Related Techniques
Explore the Social Skills Domain — Techniques You Can Work On In Parallel

H-705: Making Friends
Difficulty: INTRO | Social Communication
Materials you already own from H-707 will transfer here. → techniques.pinnacleblooms.org/…/making-friends-H-705
Materials you already own from H-707 will transfer here. → techniques.pinnacleblooms.org/…/making-friends-H-705

H-706: Conversation Skills with Peers
Difficulty: CORE | Pragmatic Language + Turn-Taking
The talking stick from H-707 is a direct prerequisite material. → techniques.pinnacleblooms.org/…/conversation-skills-H-706
The talking stick from H-707 is a direct prerequisite material. → techniques.pinnacleblooms.org/…/conversation-skills-H-706

H-708: Playground Friendship
Difficulty: CORE → ADVANCED | Unstructured Peer Interaction
Next recommended technique after H-707 mastery. → techniques.pinnacleblooms.org/…/playground-friendship-H-708
Next recommended technique after H-707 mastery. → techniques.pinnacleblooms.org/…/playground-friendship-H-708

H-715: Circle Time Participation
Difficulty: CORE | Classroom Group Skills
Social stories and role cards from H-707 apply directly. → techniques.pinnacleblooms.org/…/circle-time-H-715
Social stories and role cards from H-707 apply directly. → techniques.pinnacleblooms.org/…/circle-time-H-715

H-720: Team Sport Participation
Difficulty: ADVANCED | Cooperative Physical Activity
Parachute play from H-707 is the primary bridge technique. → techniques.pinnacleblooms.org/…/team-sport-H-720
Parachute play from H-707 is the primary bridge technique. → techniques.pinnacleblooms.org/…/team-sport-H-720

ACT IV — PROGRESS
Full Developmental Map
One Technique. One Domain. One Piece of a Whole Child.
Group participation is not an isolated skill. H-707 simultaneously builds Language development (pragmatic language in group contexts), Emotional regulation (managing group emotions), Executive function (rules, turns, flexible thinking), Academic readiness (classroom group work is a prerequisite for learning), and Community inclusion (the ultimate long-term goal).
Your child's GPT-OS® profile shows which domains need the most support and how H-707 connects to the whole picture.
→ See Your Child's Full Developmental Profile:pinnacleblooms.org/ability-score
Request a free AbilityScore® assessment: 9100 181 181
→ See Your Child's Full Developmental Profile:pinnacleblooms.org/ability-score
Request a free AbilityScore® assessment: 9100 181 181

ACT V — COMMUNITY
Family Stories
These Are Real Families. Real Children. Real Outcomes.
Story 1 — "From the Door to the Circle"
Before (Week 1): Arjun, age 6, stood at the classroom door during circle time every morning — not entering, watching from outside. Birthday parties were 10-minute arrivals followed by requests to leave.
The Approach: Social stories read each morning before school. Role card as "Bell Ringer" for circle time. Parachute play with siblings on weekends.
After (Week 7): Arjun enters circle time independently 4 out of 5 days. He knows his role. At his cousin's birthday party — he played two organized games.
"He's not just watching anymore. He's IN it. I cried at that birthday party. He was laughing with the other kids. That was my whole goal — just laughing with other kids."
Story 2 — "The Parachute Moment"
Before: Priya, age 5, played alongside peers but never with them. Parallel play at 5 years in a preschool setting where classmates were doing cooperative projects.
The Approach: Parachute play at home with parents and older sibling. Cooperative board game three times per week. Visual turn indicator for family game nights.
After (Week 6): Priya initiates "her turn" in family games without prompting. At school, her teacher reports she joined a small group activity and held her section of a shared art project — for the first time.
"When she held the edge and felt the whole thing rise because everyone lifted together — she got it in her body. She understood cooperation before she understood it with words."
Outcomes vary by child profile, intervention intensity, and developmental factors. Illustrative of typical progress trajectories under Pinnacle GPT-OS® protocols. To hear more stories: 9100 181 181

ACT V — COMMUNITY
Connect With Parents
You Are Not a Solo Operator — You Are Part of a Global Parent Community
WhatsApp Group — Group Participation Support
Join parents specifically working on group participation skills. Share what's working, ask for advice, celebrate milestones together.
Online Forum — Social Skills & Peer Interaction
Moderated by therapists. Ask clinical questions, share strategies, access monthly webinars on social skills development.
Local Parent Meetup
Pinnacle centers host monthly meetups by challenge area. Group Participation Support meetups connect local families for structured playdates and shared learning.
Peer Mentoring
Connect 1:1 with an experienced Pinnacle parent who has navigated group participation challenges. Matched by child age and challenge profile.
"Your experience helps other parents who are in the place you were six months ago. Consider sharing your journey." — WHO/UNICEF NCF Community Engagement Principle

ACT V — COMMUNITY
Professional Support
Home + Clinic = Maximum Impact
70+ Pinnacle Blooms centers operating under GPT-OS® clinical standards across India, serving families from 70+ countries via teleconsultation. Remote families access the same GPT-OS® clinical standard via teleconsultation.
Need | Specialist | Book | |
Sensory regulation assessment | Occupational Therapist | pinnacleblooms.org/book-ot | |
Social communication evaluation | Speech-Language Pathologist | pinnacleblooms.org/book-slp | |
Behavioral intervention planning | ABA/BCBA Therapist | pinnacleblooms.org/book-aba | |
Classroom inclusion support | Special Educator | pinnacleblooms.org/book-sped | |
Comprehensive developmental assessment | NeuroDev Pediatrician | pinnacleblooms.org/book-neuro |
📞 FREE Helpline
National Autism Helpline
9100 181 181 | 24×7 | 16+ languages
9100 181 181 | 24×7 | 16+ languages
🌐 Teleconsultation
Remote families in 70+ countries
pinnacleblooms.org/teleconsult
pinnacleblooms.org/teleconsult
💰 Insurance/Funding
Our team helps navigate funding options
pinnacleblooms.org/insurance-guide
pinnacleblooms.org/insurance-guide

ACT V — COMMUNITY
Research Library
The Science Behind These 9 Materials — Deeper Reading for the Curious Parent
PRISMA Systematic Review (2024)
16 studies (2013–2023): Structured material-based social skills intervention qualifies as evidence-based practice for children with ASD. Confirms efficacy across cooperative games, social stories, and video modeling. → PubMed: PMC11506176
Meta-analysis, World J Clin Cases (2024)
24 studies: Sensory integration and structured social intervention effectively promotes social skills, adaptive behavior, and peer interaction in pediatric populations. → PubMed: PMC10955541
Indian RCT, Indian J Pediatr (2019)
Home-based structured intervention with parent delivery: significant outcomes in Indian pediatric autism population. Validates the home execution model entirely. → DOI: 10.1007/s12098-018-2747-4
NCAEP Evidence-Based Practices Report (2020)
Social stories, video modeling, visual supports all classified Level 1 Evidence-Based Practices for autism intervention. → NCAEP 2020 Full Report
WHO Care for Child Development Package (2023)
Multi-country evidence base for caregiver-delivered structured intervention. Peer interaction and group skills as monitored developmental indicators in 54 LMICs. → PMC9978394

ACT V — COMMUNITY
GPT-OS® Technology
Your Sessions Are Not Just Practice — They Are Evidence That Improves Every Child Like Yours
What GPT-OS® Learns from H-707 Sessions
- Which of the 9 materials shows fastest tolerance growth for your child's sensory profile
- Optimal group size progression rate for your child's anxiety/regulation baseline
- Whether dyad-first or group-first introduction produces better outcomes
- Transfer rate from structured to unstructured group contexts for your age/profile group
Privacy Assurance
- All personal data encrypted per Indian IT (Amendment) Act 2008 standards
- Data used for clinical improvement only — never shared commercially
- Parent controls data visibility settings via GPT-OS® dashboard
- DPIIT DIPP8651 registered | CIN U74999TG2016PTC113063
"Your data helps every child like yours. Every session contributes to the largest structured pediatric intervention database ever built — 21 million sessions and growing."

ACT V — COMMUNITY
Share This Page
Consistency Across All Caregivers Multiplies Impact — Share This Page
WHO Care for Child Development Package research confirms that multi-caregiver training is critical for generalization of skills. When grandparents, teachers, and other caregivers use consistent language and supports, your child's progress accelerates significantly.
📱 Share via WhatsApp
Pre-filled message: "This page has practical materials for group participation challenges in children. Sharing because it helped us: techniques.pinnacleblooms.org/social-skills/group-participation-materials-H-707"
📄 Explain to Grandparents
"The child is learning group participation step by step. The tools: a cooperative game (everyone works together), a turn indicator (shows whose turn it is), and role cards (gives the child a specific job in the group)."
🏫 Teacher Communication Template
"Our child is working on group participation skills. Current targets: turn-taking, group entry scripts, role assignment. Visual supports at home: talking stick / role cards / social story. Could we align on consistent language at school?"

ACT VI — CLOSE
FAQ
Questions Every Parent Asks — Answered by the Pinnacle Consortium Team
My child does fine one-on-one but falls apart in groups. Is this a separate skill?
Yes — this is one of the most common presentations. 1:1 and group social skills are genuinely different skill sets. Groups add: multi-person turn-tracking, ambient noise regulation, unpredictable dynamics, and the cognitive load of coordinating with multiple people simultaneously. Start with Material 7 (dyad partner activities) and use those as a stepping stone.
At what age should I be worried about group participation difficulties?
By age 5–6, cooperative play (shared goals, basic coordination) should be emerging. Significant difficulty at 5+ years — especially affecting school circle time — warrants professional evaluation. However, intervention can begin at any age. Earlier is better, but "later" is not too late. Contact us: 9100 181 181.
Should I tell the other children about my child's challenges?
Age-appropriate peer awareness is generally positive. For young children (3–6): simple language — "Maya learns turns in a different way — this talking stick helps everyone." For older children (7–12): with the child's awareness and consent, a brief, non-stigmatizing explanation. Avoid labels in peer contexts unless the child chooses to share. Our SLP team can advise: 9100 181 181.
The social stories aren't working — my child reads them but doesn't use the skills.
This is called a "generalization gap." Solutions: (1) Read within 30 minutes of the situation, not the night before. (2) Role-play the story scenario immediately after reading. (3) Brief verbal rehearsal right before the group event. (4) First real-world applications often need an adult verbal prompt: "Remember the story? What did the story say?"
What's the ideal group size to start with?
Start with 2 people (adult + child) → then 3 (adult + child + sibling or familiar peer) → then 4–5. Only expand group size when the child shows comfort at the current size: spontaneous participation, minimal prompting, positive affect. Rushing group size is the most common parent mistake.
Can these materials be used at school too?
Yes — and home-school coordination is one of the strongest predictors of outcome. The visual turn indicator, role cards, social stories, and break card system all transfer directly to school settings. Download the Teacher Template (Card 37) and share with your child's teacher. Your child's IEP goals for group participation can directly reference these materials.
How long should each group practice session be?
Start with the child's current tolerance window + 2–3 minutes. If baseline is "refuses group activities," start with a 5-minute cooperative activity with just one other person. Build in 1–2 minute increments. The 15-minute cooperative session is a 5–8 week goal, not a week-1 starting point.
Didn't find your answer? → Ask GPT-OS®: pinnacleblooms.org/ask → Book a 15-minute teleconsultation → Call: 9100 181 181

ACT VI — START
Your Next Step
Your Child Can Learn to Belong.
The path from the edge to the circle starts with one material, one session, one today.
✅ Validated by the Pinnacle Blooms Consortium
OT • SLP • ABA/BCBA • SpEd • NeuroDev • Pediatrics • CRO • WHO/UNICEF Aligned
21M+ sessions • 97%+ improvement • 70+ centers • Patents: 160+ countries
21M+ sessions • 97%+ improvement • 70+ centers • Patents: 160+ countries
9100 181 181 | FREE | 24×7 | 16+ languages | pinnacleblooms.org
Preview of 9 materials that help with group participation Therapy Material
Below is a visual preview of 9 materials that help with group participation therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.






Link copied!

Pinnacle Blooms Network®
H-707 | SOC-GRP Domain
The Pinnacle Promise
"From fear to mastery. One technique at a time."Every parent who arrives on this page scared and leaves empowered — every child who moves from the edge of the group to the centre of it — every technique that transforms a home into a 24×7 personalized therapy environment —This is why Pinnacle Blooms Network® exists.
Consortium Disciplines
Occupational Therapy | Speech-Language Pathology | Applied Behavior Analysis (BCBA) | Special Education | NeuroDevelopmental Pediatrics | Clinical Research Organization
Standards & Scale
WHO/UNICEF Aligned | GPT-OS® Governed | 70+ Centers | 70+ Countries Served | 21M+ sessions
Contact
FREE National Autism Helpline (16+ languages): 9100 181 181
Email: care@pinnacleblooms.org
Web: pinnacleblooms.org
Techniques: techniques.pinnacleblooms.org
Email: care@pinnacleblooms.org
Web: pinnacleblooms.org
Techniques: techniques.pinnacleblooms.org
This content is educational and does not replace individualized assessment and intervention from licensed speech-language pathologists, occupational therapists, behavioral specialists, or social skills professionals. Group participation challenges may reflect underlying developmental differences requiring comprehensive evaluation. Intervention should be tailored to each child's specific profile, needs, and goals. Individual results may vary. Statistics represent aggregate outcomes across the Pinnacle Blooms Network® under GPT-OS® clinical standards.
© 2025–2026 Pinnacle Blooms Network®, unit of Bharath Healthcare Laboratories Pvt. Ltd. All rights reserved. Content generated under GPT-OS® Content Engine. Reel H-707 | SOC-GRP Domain | CIN: U74999TG2016PTC113063 | DPIIT: DIPP8651 | MSME: Udyog Aadhaar TS20F0009606 | GSTIN: 36AAGCB9722P1Z2