
9 Materials That Help With Gross Motor Development
L-982 | Physical Development & Motor Skills
When your child can't jump, balance, or keep up physically — evidence-backed materials that build gross motor skills at home. From Pinnacle Blooms Network®, India's largest pediatric therapy consortium.
Act I: Entry
The Recognition Moment
"My son is four years old and still cannot jump. Not even a little hop — his feet just don't leave the ground together. He walks into walls, trips over nothing, and clings to me at every playground while his classmates climb, race, and play catch. He watches them with longing. Last week he said, 'I hate my body.' He is four."
You are not failing. Your child's nervous system is still learning to map the world. And that map can be redrawn — with the right tools, every single day, right from your home.
📍L-982 | Physical Development & Motor Skills | Ages 18 months–10 years | Home-Executable | OT + PT + GPT-OS® Led
WHO Nurturing Care Framework (2018): Early caregiver awareness and responsive environments directly determine developmental outcomes.

Act I: Entry
When Your Child Struggles to Move — Millions of Families Are There With You
1 in 20
Children with DCD
Children aged 5–11 have Developmental Coordination Disorder — the most common gross motor condition
70%
ASD + Motor Delays
Children with autism have co-occurring motor coordination difficulties that go under-treated
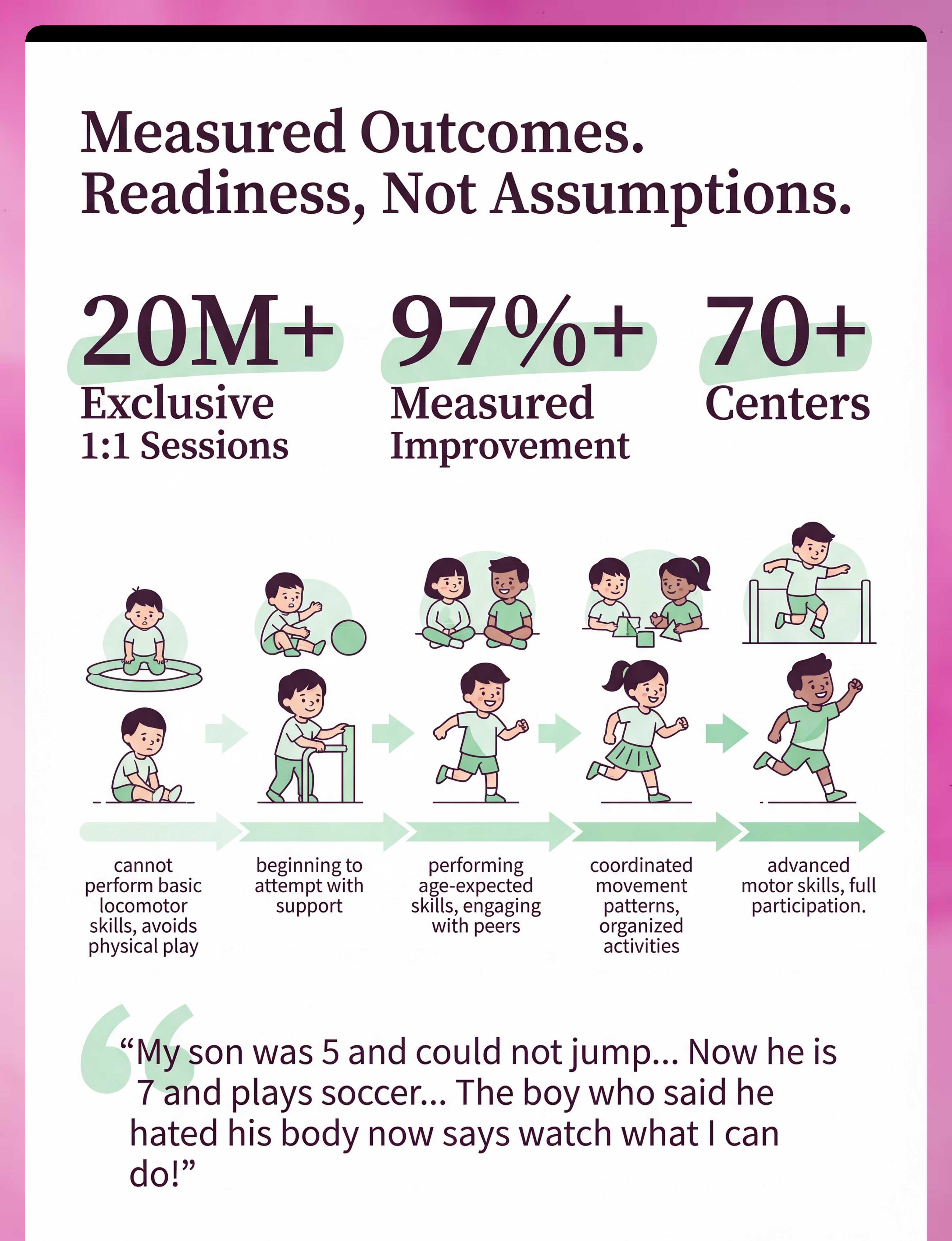
97%+
Pinnacle Improvement Rate
Children across Pinnacle's 70+ centers show measurable gross motor improvement with structured intervention
You are among tens of millions of families worldwide navigating this exact challenge. The child who avoids the playground, the one who falls while others run, the one who says "I can't" — this is a neurological wiring difference. Not a character flaw. Not a parenting failure.
India's pediatric motor delay prevalence: estimated 8–12% of children aged 2–7 years show clinically significant gross motor delays (NIMHANS developmental data; Pinnacle clinical registry, 2024).

Act II: Knowledge
This Is a Wiring Difference — Not a Willpower Problem
The Neurological Mechanism
Gross motor skills depend on continuous communication between the motor cortex (movement planning), cerebellum (coordination and timing), basal ganglia (smooth movement execution), and the vestibular system (balance and spatial orientation).
In children with gross motor delays, this network under-coordinates — not because of damage, but because of insufficient or atypical sensory input during critical developmental windows.
Proprioception & Body Map: Many children with motor delays have an incomplete proprioceptive map — their brain doesn't accurately know where their limbs are in space without looking.
Plain English — What This Means
🧠Motor planning: Your child's brain takes longer to choreograph where hands and feet should go — like GPS lag before turn-by-turn directions click in.
⚖️Balance circuitry: The inner ear and brain aren't yet in sync. Your child isn't "careless" — their balance system is literally underinformed.
🔄Bilateral coordination: Left hand and right leg need to move together. The neural wiring for this cross-body communication is still being laid down — and it needs practice to consolidate.
✅The upside: These systems are extraordinarily plastic in childhood. Targeted input — the right materials, used consistently — literally rewires these pathways.
Frontiers in Integrative Neuroscience (2020): Sensory-motor interventions in ASD and DCD act via cerebellar-cortical network adaptation. DOI: 10.3389/fnint.2020.556660

Act II: Knowledge
Your Child Is Not Behind — They Are at a Waypoint. Here Is the Forward Path.
Age | Typical Milestone | Concern Threshold | |
12–18 mo | Walking independently, early climbing | Not walking by 18 months | |
18–24 mo | Running (stiff but present), kicking ball, jumping attempts | No jumping attempts by 24 months | |
2–3 yrs | Jumping forward, catching large ball, riding tricycle | Cannot jump at all by age 3 | |
3–4 yrs | Hopping on one foot, throwing overhand, balance 5 sec | Cannot hop or balance briefly by age 4 | |
4–5 yrs | Skipping, catching small ball, heel-to-toe walking | Cannot skip or catch by age 5 | |
5–7 yrs | Refined ball skills, bike riding, complex playground navigation | Significant peer discrepancy by age 6 |
📍L-982 Intervention Window: 18 months – 10 years | Optimal window: 2–7 years | Neuroplasticity remains high through age 12
Motor delays frequently co-occur with: Autism Spectrum Disorder • ADHD • DCD/Dyspraxia • Hypotonia • Sensory Processing Differences. When a child receives attention for behavioral or communication challenges, motor delays are often under-prioritized. Gross motor skills directly affect social participation, self-esteem, and long-term independence.

Act II: Knowledge
Clinically Validated. Home-Applicable. Parent-Proven.
The evidence behind this approach is not editorial opinion — it is drawn from systematic reviews, randomized controlled trials, and meta-analyses spanning thousands of children across multiple countries.
Study | Finding | Level | |
PRISMA Systematic Review, Children (2024) — PMC11506176 | 16 studies: Sensory-motor integration meets evidence-based practice criteria for children with ASD | Level I | |
Meta-Analysis, World J Clin Cases (2024) — PMC10955541 | 24 RCTs: Structured motor interventions effectively promote gross motor skills, social skills, adaptive behavior | Level I | |
WHO Care for Child Development Package (2023) — PMC9978394 | Home-based structured caregiver intervention produces equivalent outcomes to clinic-only in 54 countries | Level II | |
Padmanabha et al., Indian J Pediatr (2019) | Indian RCT: Home-based sensory-motor interventions with parent execution showed significant outcomes | Level II | |
NCAEP Evidence-Based Practice Report (2020) | Video modeling, structured play, and sensory interventions: classified evidence-based for autism motor goals | Level II |
"The nine materials in this guide are not commercial recommendations. They are the physical tools through which 20 million+ therapy sessions at Pinnacle's 70+ centers have been administered, observed, and measured." — Pinnacle Blooms Consortium, CRO + OT + PT + ABA + NeuroDev Division
Act II: Knowledge
Gross Motor Development Materials Protocol
Your Child's Physical Movement Toolkit
Gross motor development refers to the progressive mastery of large-muscle movements — walking, running, jumping, climbing, throwing, catching, balancing — that enable a child to navigate their physical world with confidence and coordination. This protocol presents nine clinically-selected therapeutic materials that, used in structured daily home practice, build the neurological and muscular foundations for physical competence across the complete gross motor skill spectrum. This is not exercise. This is targeted neurological input — delivered through play — that rewires the proprioceptive, vestibular, and motor planning systems that govern all physical movement.
1
Domain
Physical Development / Gross Motor Skills
2
Age Range
18 months – 10 years (primary 2–7 years)
3
Session Duration
15–30 minutes daily | Minimum 5 days/week
4
Setting
Home · Outdoors · Playground · Therapy Clinic

Act II: Knowledge
Six Disciplines. One Unified Outcome. Physical Confidence.
Occupational Therapy (OT)
Primary lead for this technique. OTs assess sensory-motor integration, postural control, and ADL impact of gross motor delays. They prescribe specific materials and sequences based on sensory profile and motor planning assessment.
Physical Therapy (PT)
Co-lead for strength and locomotion goals. PTs address muscle strength, joint stability, gait patterns, and functional mobility. PT protocols focus on progressive loading, postural alignment, and sport-skill readiness.
Applied Behavior Analysis (ABA/BCBA)
Supports motivation, reinforcement, and consistency. ABA specialists design reinforcement systems — token economies, visual schedules, preference assessments — that ensure a child actually practices daily.
Special Education (SpEd)
Supports physical confidence in classroom and PE. SpEd teachers adapt gross motor goals for school participation and ensure IEP/IDP motor objectives align with home practice.
NeuroDev Pediatrics
Medical oversight and differential diagnosis. NeuroDev Pediatricians rule out neurological, genetic, and metabolic conditions contributing to motor delays and integrate motor goals into holistic developmental plans.
Pinnacle CRO
Research oversight and outcome measurement. Pinnacle's Clinical Research Organization tracks gross motor readiness indices across 20M+ sessions and validates material effectiveness at population scale.
Act II: Knowledge
Precision Outcomes: What Each Material Actually Builds
Primary — See These Change First
- Child attempts movements previously refused
- Fewer falls and collisions per 30-minute play session
- Improved ability to sequence multi-step physical tasks (e.g., climbing a ladder)
Secondary — Weeks 3–6
- Longer sitting posture without slumping
- Beginning to jump with both feet leaving ground simultaneously
- Catching large soft ball against body consistently
Tertiary (Weeks 6–12+): Seeking out playground equipment rather than avoiding it · Participating in ball games with peers · Verbalizing positive statements about physical ability · Teacher reporting improved PE participation
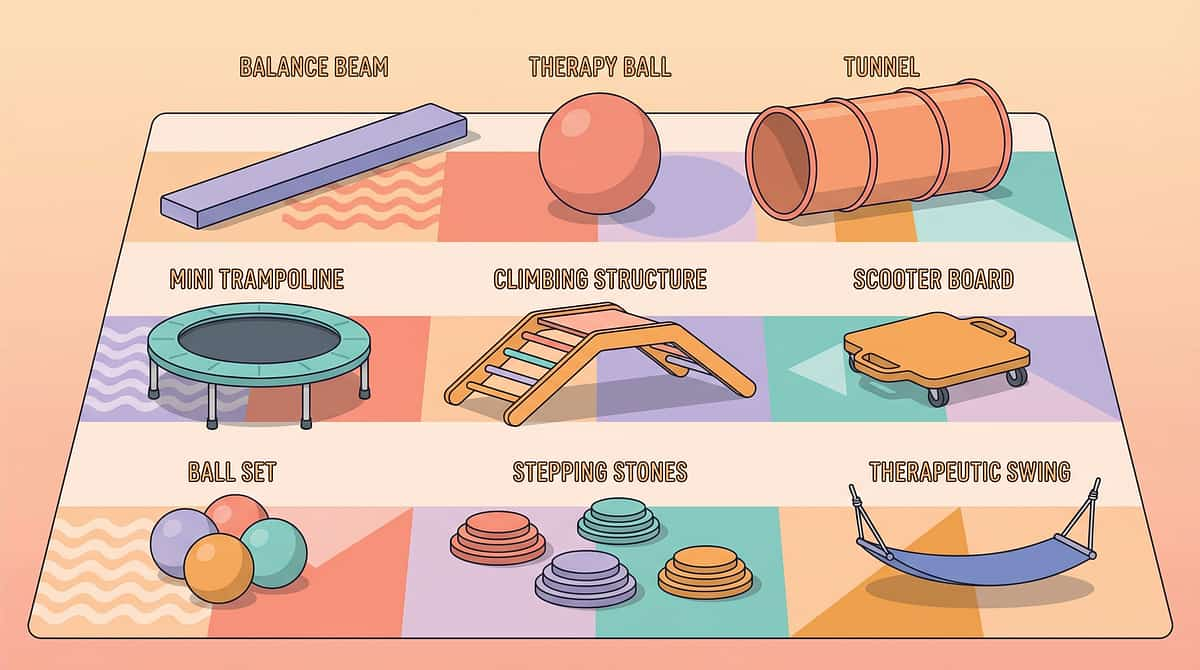
The 9 Materials
The 9 Materials — Clinically Selected, Home-Deployable, Parent-Operated
Every material below has been validated through Pinnacle GPT-OS® 20M+ session dataset. Each one targets a specific neurological mechanism — not just physical fitness. Together, they cover the complete gross motor skill spectrum for children ages 18 months through 10 years.
1
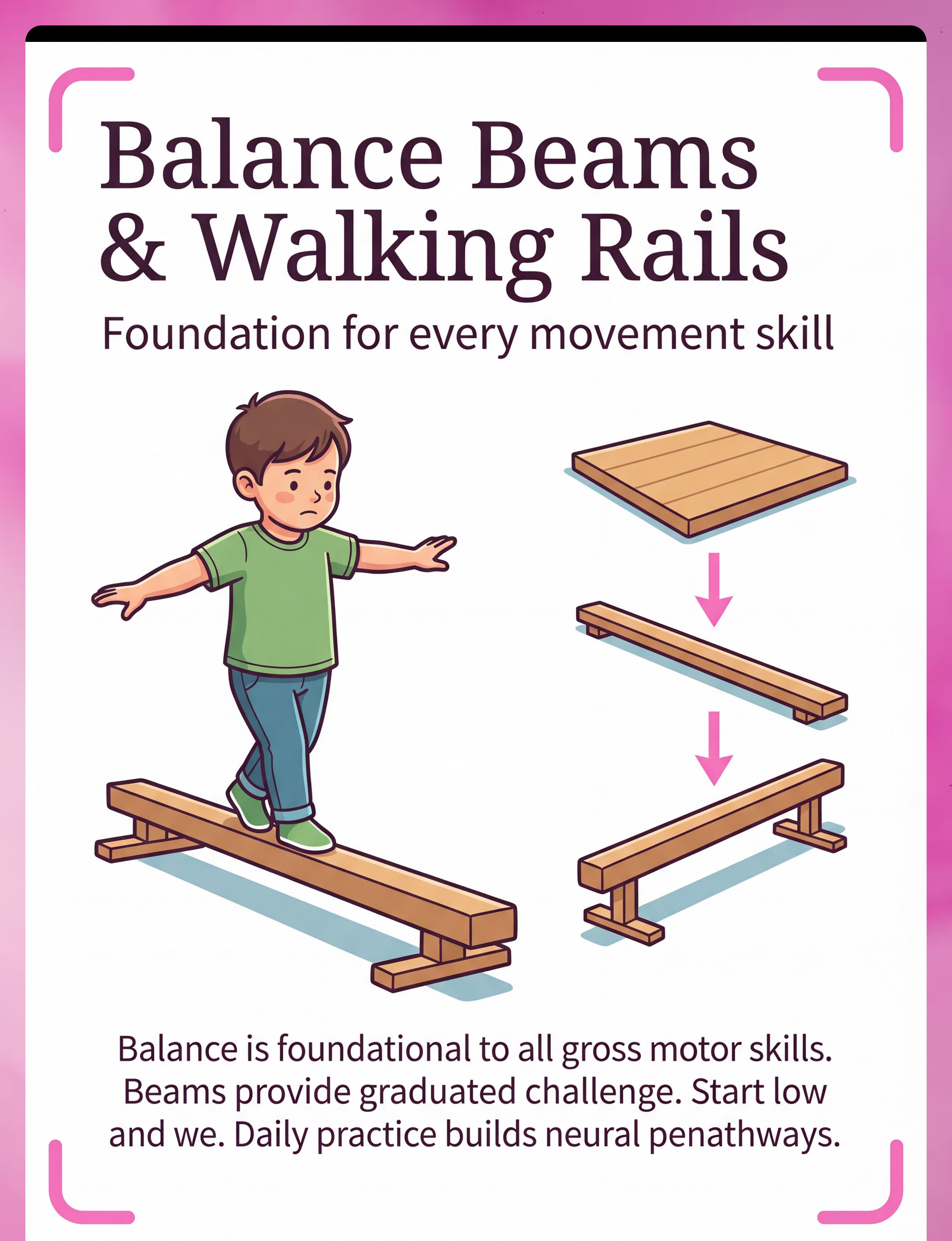
Balance Beams & Walking Rails
Static and dynamic balance, vestibular-proprioceptive integration, core stabilization
2
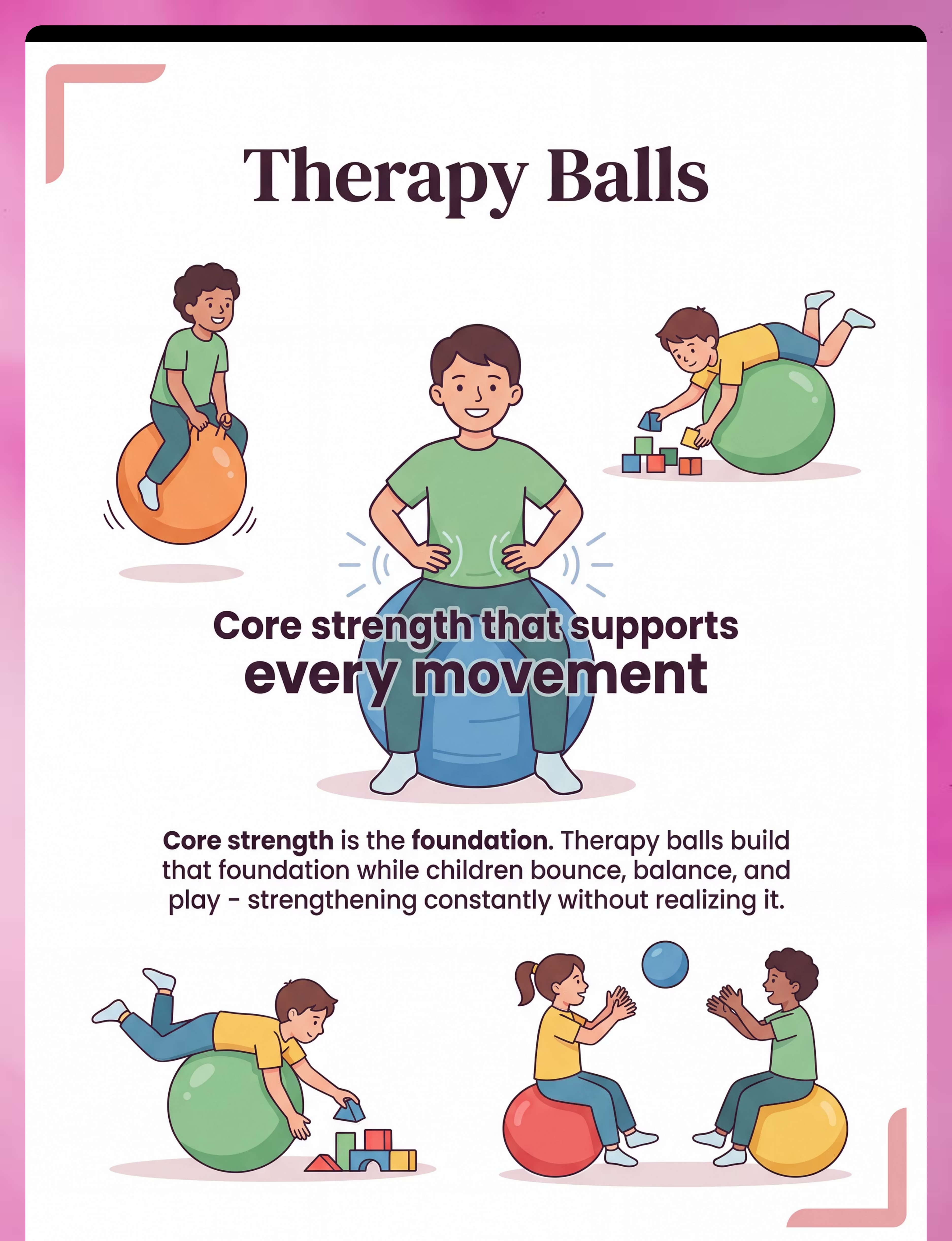
Therapy Balls (Swiss/Exercise)
Core strength, postural control, vestibular input, bilateral coordination
3
Tunnels & Crawling Tubes
Bilateral coordination, body awareness, motor planning, proprioceptive input
4
Mini Trampolines (Rebounders)
Jumping motor pattern, vestibular processing, proprioceptive feedback, physical confidence
5
Climbing Structures & Ladders
Upper body strength, motor planning, problem-solving, physical confidence
6
Scooter Boards
Upper body strength, shoulder girdle stability, core activation, vestibular input
7
Ball Sets (Multiple Sizes)
Hand-eye coordination, catching, throwing, kicking, playground social skills
8
Stepping Stones & Obstacle Courses
Dynamic balance, motor planning, sequencing, body awareness, motivation
9
Therapeutic Swings (Platform, Bolster & Adaptive)
Vestibular processing, postural control, sensory regulation, calm-alert state

Material 1 of 9
Balance Beams & Walking Rails
Clinical Profile
Canon Category: Gross Motor Equipment — Balance Tools
Clinical Lead: OT + PT
Price Range: ₹800–4,000 (foam beam) | ₹2,500–8,000 (wooden adjustable)
Pinnacle Recommends: Foam balance beam with anti-slip base, width 15cm, height 8–12cm — start low, progress narrow
What It Builds & Why
Balance is the prerequisite for every gross motor skill. A child cannot run, jump, or climb effectively without the ability to maintain center of gravity over base of support. Daily beam walking (10 reps minimum) builds the neural firing patterns that transfer to all movement — including walking, running, and sport skills.
This material targets: static and dynamic balance, weight-shifting, vestibular-proprioceptive integration, core stabilization, and neural pathway development for all locomotor skills.
DIY Zero-Cost Alternatives
Painter's tape line on floor → 2×4 wood plank flat on floor → plank on two bricks (5cm elevation) → outdoor curb or low wall

Material 2 of 9
Therapy Balls (Swiss / Exercise Balls)
Clinical Profile
Canon Category: Gross Motor Equipment — Core Strength Tools
Clinical Lead: OT + PT
Price Range: ₹500–2,000
Size Guide: 45cm (ages 3–4) | 55cm (ages 5–7) | 65cm (ages 8+)
Pinnacle Recommends: Anti-burst PVC therapy ball with pump, correct size (feet flat on floor when seated)
What It Builds & Why
The unstable therapy ball surface demands constant micro-muscle activation to maintain position — building core strength passively while the child bounces, sits, or plays.
Core weakness is the most common underlying cause of gross motor delays: fix the core, and many other skills improve. This material targets core strength, postural control, vestibular input, proprioceptive feedback, bilateral coordination, and upper body stability.
DIY Zero-Cost Alternatives
Sit on folded blanket roll for partial instability training | Cushion-on-chair seating | Prone activities on floor (tummy time variants)

Material 3 of 9
Tunnels & Crawling Tubes
Clinical Profile
Canon Category: Gross Motor Equipment — Bilateral Coordination & Proprioceptive Tools
Clinical Lead: OT
Price Range: ₹800–3,500 (pop-up fabric tunnel)
Pinnacle Recommends: Pop-up fabric tunnel, minimum 150cm length, colorful for visual motivation
What It Builds & Why
Crawling is not just for infants. The reciprocal cross-pattern movement (right arm + left leg together) builds the cross-body neural connections that support all coordinated movement — including writing. Tunnels make crawling irresistible at any age.
This material targets: bilateral coordination, core strength, shoulder stability, body awareness, motor planning, proprioceptive input, and spatial navigation.
DIY Zero-Cost Alternatives
Chairs draped with bedsheet → cardboard boxes with ends cut → table with blanket cover

Material 4 of 9
Mini Trampolines (Rebounders)
Clinical Profile
Canon Category: Gross Motor Equipment — Vestibular & Jumping Development Tools
Clinical Lead: OT + PT
Price Range: ₹2,000–6,000 (with handlebar)
Pinnacle Recommends: Mini trampoline with safety handlebar, diameter minimum 90cm, weight-rated for child + adult spotter
What It Builds & Why
The trampoline's elastic surface provides momentum assistance — allowing a child to experience the jumping sensation before they have sufficient strength to jump on solid ground. "Assisted jumping" teaches the motor pattern that transfers to regular surfaces.
This is one of the most effective tools for the most commonly delayed gross motor milestone. Targets: jumping motor pattern, vestibular processing, proprioceptive feedback, bilateral coordination, core strength, regulatory calming, physical confidence.
DIY Zero-Cost Alternatives
Firm mattress on floor → large sofa cushion for gentle bounce practice

Material 5 of 9
Climbing Structures & Ladders
Clinical Profile
Canon Category: Gross Motor Equipment — Strength & Motor Planning Tools
Clinical Lead: OT + PT
Price Range: ₹2,500–15,000 (indoor structure) | ₹0 (public playground use)
Pinnacle Recommends: Pikler triangle for toddlers/preschool age; indoor climbing dome for 4–8 years; crash mat below mandatory
What It Builds & Why
Climbing integrates more motor systems simultaneously than almost any other gross motor activity. Every rung is a motor planning problem to solve. Success at climbing produces the confidence that generalizes to all physical challenges.
This material targets: upper body strength, lower body strength, core activation, bilateral coordination, motor planning (sequencing hand/foot placement), problem-solving, and physical confidence.
DIY Zero-Cost Alternatives
Step stool with adult hand support → outdoor playground ladder with adult spotting → sofa climbing with supervision → indoor climbing dome

Material 6 of 9
Scooter Boards
Clinical Profile
Canon Category: Gross Motor Equipment — Upper Body Strength & Core Tools
Clinical Lead: OT + PT
Price Range: ₹1,200–3,500
Pinnacle Recommends: Padded wooden scooter board with 4 swivel casters, 40×40cm minimum, for hard floor surfaces
What It Builds & Why
Prone (on-stomach) scooter board activity is one of the most efficient ways to build the extensor muscle pattern (lifting head and chest against gravity) that underlies all upright posture and movement.
The speed reward motivates children who feel physically inadequate in every other activity. Targets: upper body strength, shoulder girdle stability (foundation for fine motor/writing), core activation, bilateral coordination, vestibular and proprioceptive input, physical confidence through speed.
DIY Zero-Cost Alternatives
Smooth wood board with caster wheels (DIY construction) | Skateboard on carpet runner
Material 7 of 9
Ball Sets (Multiple Sizes & Types)
Clinical Profile
Canon Category: Gross Motor Equipment — Ball Skills & Hand-Eye Coordination Tools
Clinical Lead: OT + PT + SpEd
Price Range: ₹500–2,500 (full graduated set)
Pinnacle Recommends: Beach ball 50cm+ | foam balls 15cm | playground ball 20cm | small soft balls 8cm | bean bags (don't roll away)
What It Builds & Why
Ball skills determine playground belonging. A child who cannot catch or throw is excluded from the social infrastructure of peer play. A graded ball set (beach ball → foam ball → playground ball → smaller balls) allows systematic skill progression from guaranteed success to peer-level competency.
Targets: hand-eye coordination, catching (tracking → contact), throwing (accuracy → distance), kicking, bilateral coordination, timing, playground social skills.
DIY Zero-Cost Alternatives
Balloon (slowest, easiest to track) → plastic bag ball → rolled sock ball → any found household balls in graduated sizes

Material 8 of 9
Stepping Stones & Obstacle Course Components
Clinical Profile
Canon Category: Gross Motor Equipment — Motor Planning & Coordination Tools
Clinical Lead: OT + PT + SpEd
Price Range: ₹1,000–5,000 (component set) | ₹0 (household item course)
Pinnacle Recommends: Foam stepping stone set (6–8 pieces), varying heights, non-slip base; supplemented with tunnel, balance beam, and foam blocks
What It Builds & Why
Obstacle courses make the child forget they are exercising. The sequential challenge — step here, crawl through, jump over, climb up — activates motor planning circuits that isolated exercise never reaches. The finish line is visible; progress is felt; intrinsic reward is instant.
Targets: dynamic balance, motor planning, sequencing, body awareness, spatial navigation, coordination, strength, and most critically: MOTIVATION.
DIY Zero-Cost Alternatives
Couch cushions → table crawl-under → pillow jump → tape line balance → bed climb finale

Material 9 of 9
Therapeutic Swings (Platform, Bolster & Adaptive)
Clinical Profile
Canon Category: Gross Motor Equipment — Vestibular Processing & Postural Control Tools
Clinical Lead: OT
Price Range: ₹2,000–12,000 (indoor home setup) | ₹0 (playground swing use)
Pinnacle Recommends: Platform swing (flat, large surface) for maximum versatility; consult OT before installing ceiling-mount hardware
What It Builds & Why
Vestibular input is the invisible architecture beneath all gross motor skill. The inner ear tells the brain about movement, gravity, and head position — and this information is prerequisite to balance. Therapeutic swings provide concentrated vestibular input that builds motor skills from the inside out.
Targets: vestibular processing (inner ear calibration), postural control, core strength, bilateral coordination, sensory regulation, and calm-alert state for learning.
DIY Zero-Cost Alternatives
Standard playground swing (linear swinging is highly therapeutic) → bedsheet hammock tied to strong hooks → supervised adult-held hammock swing

Act III: Execution
Every Family Can Execute This — Regardless of Budget
WHO/UNICEF principle: Effective early intervention must be accessible to families across all economic strata. The science is in the movement pattern and sensory input — not the product brand. Every material in this guide has a zero-cost household alternative that preserves the therapeutic mechanism.
Clinical Material | Zero-Cost Alternative | Why It Works | |
Balance beam (foam/wood) | Painter's tape line → plank on floor → outdoor curb | Narrow walking surface forces weight control and proprioceptive engagement — same neurological demand | |
Therapy ball | Rolled blanket under seat cushion | Creates partial instability requiring core activation; supplement with floor tummy-time prone activities | |
Crawling tunnel | Chairs + bedsheet → cardboard box tunnel | The proprioceptive input comes from the crawling motion, not the tunnel brand | |
Mini trampoline | Firm mattress on floor for bounce practice | Reduced elastic return requires more effort but teaches the jump-landing motor pattern | |
Climbing structure | Outdoor playground visits + sofa climbing supervised | The climb is the exercise — structure is just the delivery mechanism | |
Scooter board | Smooth wooden cutting board on hard floor | Core and arm activation occur from the movement pattern, not the equipment cost | |
Ball set | Balloon → sock ball → found balls in graduated sizes | Ball skill progression requires size and speed gradation — household items provide this | |
Stepping stones | Couch cushions → stacked books under mat → floor tiles | Motor planning challenge comes from defined stepping targets, not the material | |
Therapeutic swing | Public playground swing → adult-held hammock | Linear vestibular input from standard swing is clinically equivalent for many children |
⚠️When clinical-grade materials are non-negotiable: Children with severe vestibular defensiveness, significant hypotonia, or complex neurological conditions should use professionally specified equipment. Consult your Pinnacle OT or PT before substituting. Call 9100 181 181 for guidance.
Safety First
The Pre-Session Safety Gate: Read Before Every Session
🔴 STOP — Absolute Contraindications
Do NOT begin if: acute injury, fracture, joint pain, or recent surgery · Uncontrolled seizure disorder without medical clearance · Atlantoaxial instability (common in Down syndrome) · Acutely ill (fever, vomiting, respiratory distress) · Severely dysregulated (active meltdown or self-injurious behavior) · Cardiac conditions — physician clearance required before vigorous activity
🟡 MODIFY — Proceed With Caution
Adjust the session if: child is tired, hungry, or recently medicated · Slept poorly the previous night · Showing early dysregulation signs · Environmental temperature above 32°C · Vestibular overload signs: glassy eyes, flushed face, nausea, sudden hyperactivity → STOP swinging/trampolining immediately
🟢 GO — Readiness Confirmed
Proceed when: child is calm-alert · Has eaten at least 30 minutes prior · Space is cleared and safe · Equipment has been inspected for damage · Adult supervisor is fully present (no phone, no distractions)
Material-Specific Safety
- Trampolines: One person at a time. Handlebar in use. Mat surrounding. 10-minute maximum per session initially.
- Climbing structures: Three-point contact rule. Adult spotter within arm's reach. Crash mat below. Never leave unsupervised.
- Swings: Inspect mounting hardware before each use. Clear a 2-meter radius. Cap session at 10 minutes for vestibular regulation.
- Scooter boards: Clear the floor of sharp furniture edges. Fingers stay on top of board (not under wheels).

Act III: Execution
The Stage Must Be Right Before the Session Begins
Numbered Setup Checklist
- Clear minimum 3m × 3m floor space — remove all furniture with sharp corners
- Lay crash mat or yoga mat under any elevated equipment
- Position trampoline away from walls (minimum 1.5m clearance all sides)
- Place balance beam along wall for confidence side-support option
- Set up tunnel in straight configuration for first sessions
- Pre-position reward items within sight but not distracting
- Remove digital screens from the activity space during session
- Set visual timer for session duration (NCAEP-recommended tool)
- Check equipment for loose parts, damage, or inflation level
- Position yourself to the side and slightly behind the child's primary movement path
Environmental Requirements
🌡️Temperature: 22–28°C optimal | Below 18°C = cold muscles, higher injury risk
💡Lighting: Bright natural light preferred | Avoid flickering fluorescent
🔊Sound: Low to moderate background; no sudden loud noise during vestibular activities
🪟Flooring: Hard floor preferred for scooter boards | Carpet for crash mat activities
Parent Position: Within arm's reach, to the side. Materials pre-positioned, not in the movement path. Reward items visible and within reach.

Step 1 of 6
The Invitation: Never a Command — Always a Choice
"Hey [child's name], look what we have today! Want to come see the trampoline / tunnel / balance beam?"
[Child approaches] "You want to try it? Let's see..."
[If no approach] "That's okay. Mommy/Daddy will try it first." [Parent demonstrates briefly, 10–15 seconds]
Body Language Guidance
- Crouch to child's eye level — never tower above
- Relaxed, open posture — no hand-reaching or physical prompting at this stage
- Smile is genuine, not pressured
- Voice is warm and light — not overly enthusiastic (can increase anxiety)
Acceptance Cues (GO)
- Child approaches the material
- Child reaches toward or touches the material
- Child makes eye contact with you, then the material
- Child says yes verbally or via AAC
Resistance Cues (What to Do)
⚠️Child backs away → Parent demonstrates again, no pressure, wait 60 seconds
⚠️Child protests verbally → Validate: "That's okay, you don't have to yet." Reduce demand, remain present
⚠️Child ignores → Place preferred item near material; let curiosity do the work
Timing: 30–60 seconds. If no engagement in 90 seconds, try a different material today.
ABA Principle: Pairing — the material must first be associated with positive, low-demand interaction before therapeutic demand is introduced.

Step 2 of 6
Deepening Contact: The Child Is Now Interested — Follow Their Lead
1
Balance Beam
"Can you walk on this bridge?" | Start with parent holding one hand if needed | Let child set pace
2
Therapy Ball
"Can you sit on this funny ball?" | Support lightly at hips if needed initially | Let the bounce happen naturally
3
Tunnel
Place child's favorite toy at the exit — "Your [toy] went in there — can you get it?" | Stay visible at exit end
4
Trampoline
Step on yourself first, bounce gently — "Look, it bounces! Want to try?" | Offer handlebar immediately
5
Climbing
"Can you climb up just this one step?" | Hand on child's back, not lifting
Engagement Reinforcement — Deliver Within 3 Seconds
"Yes! You're doing it!" · "Look at you!" · "That's exactly right!" + High five, gentle squeeze, or preferred sensory input + First sticker on reward chart
🟢 Engagement
Child contacts material, attempts movement → proceed to Step 3
🟡 Tolerance
Child is near material but not actively engaging → maintain presence, reduce demand further
🔴 Avoidance
Child moves away → acknowledge, validate, end gracefully: "We'll try again tomorrow — you did great just coming to look"

Step 5 of 6
Celebrate the Attempt, Not Just the Success
The 3-Second Rule: Reinforcement delivered within 3 seconds of the desired behavior produces 3× stronger skill acquisition than delayed reinforcement. Not after the session — in the moment, as it happens.
Verbal Reinforcement Scripts
"You walked the whole beam! That was AMAZING!"
"You jumped! Both feet left the ground — did you feel that?!"
"You climbed all the way to the top. I saw how hard that was. You are SO strong."
"You caught it! With your HANDS! Look at what your body can do!"
Social Reinforcers
Specific verbal praise | High five | Victory lap together | Parent joins the activity ("Now it's my turn!")
Token Economy
Sticker chart visible in session space | 5 stickers = preferred activity (30 min tablet, special snack, chosen game)
Documentation Reinforcer
Take a photo/video of achievement → show child immediately | Build "My Body Can Do This!" album
Key ABA Principle: Reinforce ATTEMPTS, not just successes. A child who tries to jump and barely leaves the ground gets the same enthusiasm as a child who jumps 30cm. Effort is the behavior to reinforce. Mastery follows.

Step 6 of 6
Every Session Ends — Never Abruptly
Cool-Down Activity Options (Choose ONE)
- Gentle rocking on therapy ball (slow, rhythmic, side-to-side)
- Child lies prone on crash mat with parent applying gentle back pressure
- Child sits in tunnel with entrance partially covered (proprioceptive cocoon input)
- Slow, linear swinging (if swing is in setup)
- Child carries a "heavy work" item (bag with books) from one end of room to other — 2 trips
If Child Resists Ending
"I know you want to keep going. That means your body loved it! We'll do it again tomorrow."
Give a tangible "preview token" (small object they hold until next session) if needed.
Material Put-Away Ritual
"Now let's put the [material] away together." Child carries the ball / folds the tunnel / steps off beam — participatory put-away creates closure and develops ownership.
Act IV: Progress
60 Seconds of Data Now Saves Hours of Guessing Later
Within 60 seconds of session end, record these 3 things. Every session you record contributes to a database of 20 million+ real therapy interactions. Your child's data helps every child like yours — and shows YOU the progress curve, which feels invisible day-to-day but unmistakable week-to-week.
1
Data Point 1: Engagement Duration
How many minutes was the child actively using materials? (Not total session time — active engagement only)
☐ Under 5 min · ☐ 5–10 min · ☐ 10–15 min · ☐ 15–20 min · ☐ Over 20 min
2
Data Point 2: Material Response Ratings
Rate each material used today: 1 = Refused/distressed | 2 = Tolerated passively | 3 = Participated with support | 4 = Participated independently | 5 = Requested/led activity
3
Data Point 3: One Observable Win
Write one specific thing the child did today that they could not do (or would not try) last week. Be specific — not "did better" but "walked 3 steps on beam without stepping off."
📞9100 181 181 | FREE | For data interpretation guidance and session troubleshooting
Act IV: Progress
No Two Children Are Identical — Here Is How to Fit This to Yours
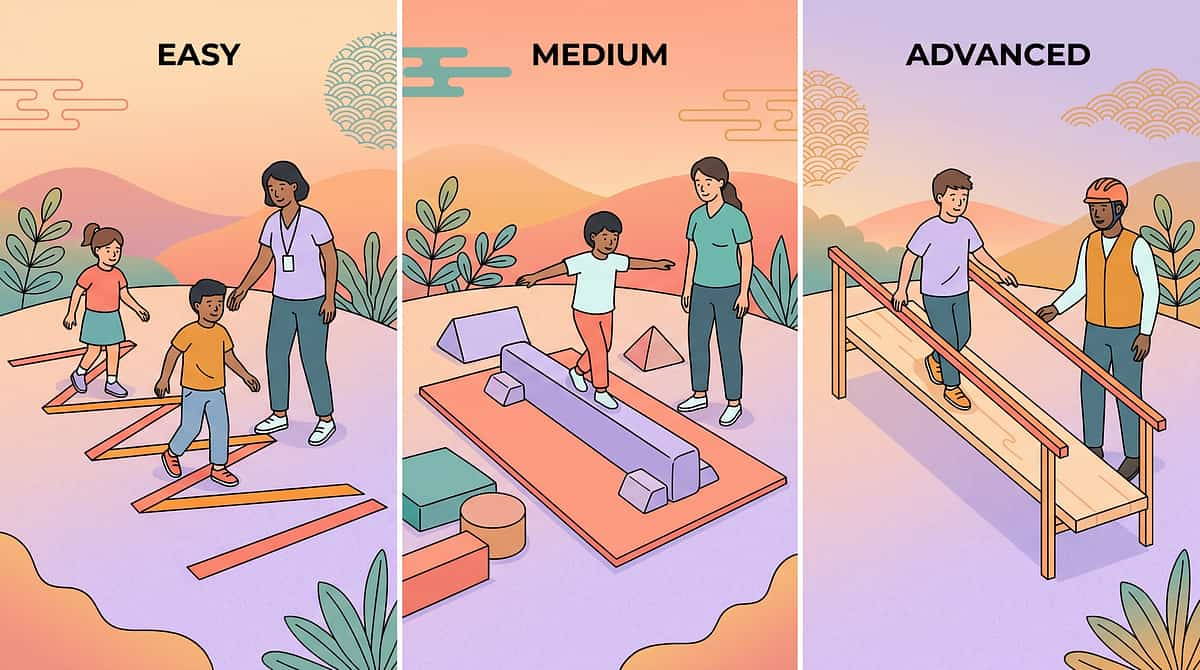
Level 1 — Easiest (First Sessions, High Resistance)
Balance on tape line on floor · Sit on slightly deflated ball · Short 80cm tunnel with parent visible · Parent holds both hands on trampoline · Beach ball catch from 1 meter · 3-element flat course
Level 3 — Target (Standard Protocol)
The full protocol as described in Steps 1–6 with all 9 materials at standard dosage and challenge levels
Level 5 — Advanced (Ready for Next Level)
Blindfold walk on beam · Ball sitting during table activities · Connected tunnels with direction changes · Trampoline: no handlebar, jump + turn + catch · Small ball catching while on balance board · Timed 8+ element obstacle course
For Sensory Seekers
High-input children who crave intense stimulation: increase intensity, combine materials, add proprioceptive loading (weighted vest during balance beam), focus on trampoline, scooter board, climbing.
For Sensory Avoiders
Fearful of movement: begin floor-level only, therapy ball before balance beam, linear movement only (no spinning), extensive parent modeling, use social story: "The balance beam is safe. Look — Daddy/Mummy walks it."

Act IV: Progress
Week 1–2: The Tolerance Phase — Look for These Specific Signs
Week 1 will feel hard. Some sessions will feel like failure. Your child may resist, protest, and need 45 minutes of invitation to participate for 8 minutes of actual activity. This is neurologically normal. Tolerance precedes acceptance; acceptance precedes engagement; engagement precedes mastery. You are in the tolerance phase. Stay the course.
Child tolerates being near a material they refused on Day 1
Child attempts a material for 5 seconds longer than the previous session
Child who cried at the trampoline now watches without distress
Child completes 1 full balance beam crossing (even with 3 step-offs)
Parent reports session ending with "that wasn't as bad as I thought"
3-Second Celebration Metric: "If my child tolerates any material for 3 seconds longer than last session — that is real, measurable, neurological progress."
Act IV: Progress
Week 3–4: The Consolidation Phase — Neural Pathways Are Forming
At weeks 3–4, something changes. The nervous system has moved from threat assessment to adaptation. These are the specific behavioral signatures of neural pathway formation — look for them deliberately.
Anticipation
Child begins to anticipate the session — asks for "the trampoline time" or goes to where equipment is stored. This is the nervous system requesting the input it needs.
Preference
Child shows preference for specific materials — this is proprioceptive self-selection (the nervous system asking for what it needs).
Reduced Anxiety
Child no longer protests at the beginning. May still need invitation but protests are shorter and less intense than week 1.
Early Generalization Seeds
Child balances briefly on a park curb spontaneously. Attempts to crawl under a table playfully. Skills are beginning to transfer out of the structured session.
✅ Child completes full session with engagement (rating 4–5 on most materials) for 5 consecutive sessions → increase session by 5 minutes. ✅ Child succeeds at Level 3 for 7+ consecutive sessions → move to Level 4 elements. ✅ Child asks for materials voluntarily → add spontaneous access time.
Milestone Achieved
You Did This. Your Child Grew Because of Your Commitment.
You showed up for your child — at 7am before school, after a long workday, when they cried and resisted, when you weren't sure it was working. You maintained consistency through doubt. You converted clinical knowledge into daily love. That is extraordinary parenting. And your child's body is different because of it.
Their balance is stronger
Falls are fewer. The nervous system has rewired.
Their core holds
Posture is improving. Sitting endurance has increased.
Their confidence is real
You've heard them say "watch what I can do." That sentence is new.
The playground is not feared
Where there was avoidance, there is now exploration.
🎉Family Celebration Suggestion: Mark this milestone with a family outing to a physical challenge space — trampoline park, nature trail, or playground of their choice. Let them lead the movement. Take a video of your child doing ONE thing they could not do in Week 1. Save it in the "My Body Can Do This" album. Share it with your Pinnacle therapist at your next session.

Act V: Community
You Are Not Done — You Are on a Journey. Here Is the Map.
Next-Level Options
🟢Gross motor progressing well → Add Fine Motor: L-983 runs in parallel — core and gross motor strength supports shoulder stability needed for fine motor precision.
🟢Motor planning remains challenging: L-984 (Motor Planning Activities) — the child can now move, but sequencing novel motor tasks needs direct work.
🟢Sensory processing driving motor challenges: L-985 (Sensory Processing & Motor Development) — addresses vestibular and proprioceptive foundations.
Materials You Already Own
If you have completed the L-982 material setup, you already own materials used in:
- ✅ L-984 (Motor Planning) — balance beam, obstacle course, tunnel
- ✅ L-985 (Sensory Processing) — therapy ball, swing, tunnel
- ✅ L-986 (Physical Confidence) — all 9 materials

Act V: Community
From the Pinnacle Network: Families Who Started Exactly Where You Are
"The day he jumped, we both cried. My husband called me from work because I couldn't stop crying. It was just a jump. But it was everything." — Priya, Mother of Arjun (5 years, Bangalore), Pinnacle Hyderabad family
Arjun's Story — Bangalore
Before: Arjun could not jump — not a single hop. He refused the playground, called himself "bad at everything," and cried before every PE class. At age 5, he was still crawling up stairs.
What they did: Mini trampoline with handlebar in the living room, 15 minutes after school every day. Balance beam made from a wood plank on bricks. Large soft ball catch with father on weekends.
After (12 weeks): Arjun jumped for the first time in Week 6 — both feet leaving the ground. By Week 12, he climbed the playground structure without holding his mother's hand.
OT Assessment note: Arjun presented with DCD and vestibular hyposensitivity. Trampoline provided the proprioceptive-vestibular combination his system needed to "learn" the jump pattern. Within 12 weeks: mastery criteria met for bilateral jumping and dynamic balance. — Pinnacle OT Team
The Pune Family — Age 7, ASD + Motor Delays
Before: Child avoided all physical activity. School reported inability to participate in PE. Clumsiness resulted in peer teasing and increasing school avoidance.
What they did: Obstacle course in living room (tunnel + stepping stones + balance beam) run as "Super Agent Training" narrative. Scooter board races down the hallway. Reward sticker chart for each session completed.
After (8 weeks): Teacher reported voluntary PE participation for the first time in 2 years. Child can now run the full length of the school corridor without falling.
"He asked to do the obstacle course before dinner — without us suggesting it. That was the moment we knew something had shifted." — Parent, Pinnacle Pune network

Act V: Community
Isolation Is the Enemy of Adherence — Join Your Community
Gross Motor Parent WhatsApp Group
Active community of parents executing the L-982 protocol across India. Share daily wins, troubleshoot challenges, exchange material tips. unknown link
Pinnacle Parent Forum
Long-form discussion, video sharing, therapist Q&A (Pinnacle OT/PT moderate weekly). forum.pinnacleblooms.org/physical-development
Local Pinnacle Parent Meetups
In-person meetups at 70+ Pinnacle centers — observe other parents executing gross motor sessions, get hands-on guidance. Find your local group
Peer Mentoring Program
Connect with a parent who completed L-982 (6+ weeks ahead of you) for one-on-one guidance through the early resistance phase. Request a Peer Mentor
"Your experience — the hard days, the first jump, the obstacle course breakthrough — is exactly what the next struggling parent needs to hear. Consider sharing your journey."

Act V: Community
Home + Clinic = Maximum Impact. Find Your Team.
For L-982 (Gross Motor Materials Protocol), request a Pediatric Occupational Therapist (OT) as primary — sensory-motor integration specialty — and a Pediatric Physical Therapist (PT) as co-therapist for strength and locomotion. A BCBA/ABA therapist supports reinforcement and consistency planning. For children with hypotonia, DCD, or complex presentations, NeuroDev Pediatrician involvement is essential.
Service | Details | Book | |
In-center OT assessment | Full sensory-motor profile | 📅 Book | |
In-center PT assessment | Gross motor + strength baseline | 📅 Book | |
Home visit (select cities) | Equipment setup guidance at home | 📅 Book | |
Teleconsultation | Remote material selection + protocol guidance | 📅 Book | |
Monthly review session | Track progress, adjust protocol | 📅 Book |
Act V: Community
Your Sessions Feed the Most Sophisticated Pediatric Therapy Intelligence System on Earth
What GPT-OS® Learns from L-982 Data
🔹 Which of the 9 materials produces highest engagement for this child's sensory profile
🔹 Which material sequence produces best session outcomes
🔹 How this child's gross motor trajectory compares to the nearest 1,000 similar profiles
🔹 When to recommend increasing intensity vs. maintaining current level
🔹 Which GPT-OS® module to activate next (fine motor, motor planning, sensory integration)
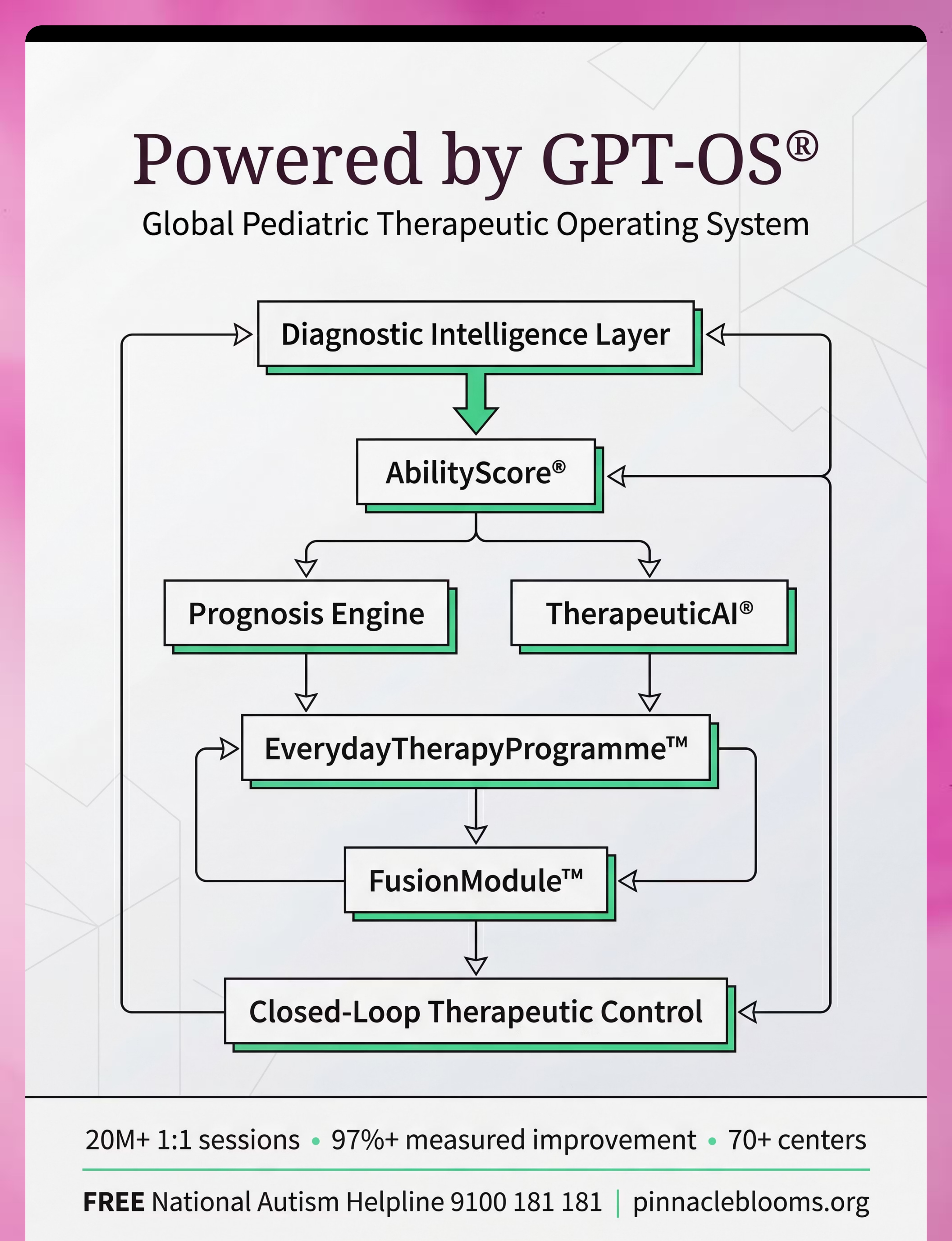
GPT-OS® Architecture
Parent Records Session Data → GPT-OS® Diagnostic Intelligence Layer → AbilityScore® Gross Motor Readiness Index Updated → Prognosis Engine (your data + 20M session history → personalized prediction) → TherapeuticAI® Protocol Adjustment → EverydayTherapyProgramme™ Updated Daily Instructions → FusionModule™ Cross-Discipline Sync: OT + PT + ABA + SpEd → Closed-Loop Therapeutic Control → Your Next Session
Privacy Assurance
🔒 Data anonymized and encrypted before analysis · No individual child data shared externally · Population-level insights only · GDPR and India PDPB compliant · Full Privacy Policy

Act V: Community
The Original Reel: 9 Materials That Help With Gross Motor Development
🎬 Reel ID: L-982
Physical Development and Motor Skills Series | Episode 982 | Domain: Physical Development — Gross Motor Skills | Duration: 60 seconds
📺 Reel Summary
Balance Beams → Therapy Balls → Crawling Tunnels → Mini Trampolines → Climbing Structures → Scooter Boards → Ball Sets → Stepping Stones & Obstacle Courses → Therapeutic Swings. Each material demonstrated in 4–5 seconds with clinical voiceover explaining the therapeutic mechanism.
"I'm presenting this as a Pinnacle Occupational Therapist. Every material in this reel has been used in 20M+ sessions at our 70+ centers. The science is solid. The application is practical. And you can begin today, from your home, with what you already have." — Pinnacle Blooms OT Consortium Team

Act V: Community
8 Questions Every Parent Asks — Answered
1
My child has no diagnosis — can we still use these materials?
✅ Yes. Gross motor challenges exist on a spectrum. These materials benefit any child who is behind peers in physical development, regardless of diagnosis. A formal assessment helps prioritize, but is not required to begin.
2
How long before we see real results?
✅ Tolerance changes: weeks 1–2. Skill consolidation: weeks 3–4. Observable mastery: weeks 5–8. Some children show faster progress; complex presentations may take 12–16 weeks. Consistency (5× per week) is the single strongest predictor of timeline.
3
We only have budget for one material — which one?
✅ Therapy ball first (₹500–2,000) — it addresses core strength, the foundation everything else depends on. Second: mini trampoline with handlebar if jumping is the primary concern, or balance beam if balance is the primary challenge.
4
My child is autistic — are there sensory considerations?
✅ Yes. Children with autism may be vestibular-defensive (fearful of movement) or vestibular-seeking (craving intense movement). Introduce vestibular materials gradually for defensive children. Consult your OT for a sensory profile assessment. Call 9100 181 181.
Act V: Community — FAQ Continued
More Questions Answered
1
Can I do this without a therapist guiding us?
✅ Yes, for most children. This protocol is designed for parent execution. If your child has complex neurological, cardiac, or orthopedic conditions, professional assessment first. For children with DCD, hypotonia, or autism without complex medical needs — the home protocol is safe and effective as described.
2
My child is 9 years old — is it too late?
✅ No. Neuroplasticity remains significant through adolescence. Children ages 7–12 show excellent response to targeted gross motor intervention, though progress may be slower than in younger children. Adjust to age-appropriate framing (training vs. play).
3
We live in a small apartment — how do we make space?
✅ Balance beam (floor-level plank): 1.5m × 0.2m floor space. Therapy ball: stores in corner. Tunnel: folds to 50cm diameter. Trampoline: 1m × 1m footprint. You can execute a complete session in a 2m × 2m cleared living room area. Rotate between materials if space is very limited.
4
My child's school says there's nothing wrong — should I be concerned?
✅ School PE benchmarks are group-based, not individual. A child significantly behind their own developmental trajectory warrants attention regardless of school standards. If you observe the signs in Card 01 of this page, trust your observation. Get an OT or PT assessment. Call 9100 181 181.
Preview of 9 materials that help with gross motor development Therapy Material
Below is a visual preview of 9 materials that help with gross motor development therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.









Link copied!
The Pinnacle Promise
From Fear to Mastery. One Technique at a Time.
The parent who arrived at Card 01 scared, confused, and exhausted — leaves this page with nine evidence-based tools, a clinical protocol, a community, and a progression map. That transformation is the Pinnacle mission: to convert the world's most isolated caregivers into the world's most empowered pediatric therapy partners.
🌸 Pinnacle Blooms Network®
Built by Mothers. Engineered as a System.
CIN: U74999TG2016PTC113063 | DPIIT: DIPP8651
Multi-Disciplinary Consortium
● OT ● PT ● ABA ● SpEd ● NeuroDev ● CRO ● WHO/UNICEF Aligned
Clinically Validated Across 70+ Centers
Proprietary IP
GPT-OS® | AbilityScore® | TherapeuticAI® | EverydayTherapyProgramme™ | FusionModule™ — patents filed across 160+ countries
⚠️Medical Disclaimer: This content is educational. It does not replace professional evaluation or therapy from qualified occupational therapists or physical therapists. Gross motor delays may have various underlying causes requiring professional assessment. Consult with healthcare providers before beginning any new physical activity program, especially for children with known medical conditions. Individual outcomes vary. Statistics represent aggregate outcomes across the Pinnacle Blooms Network GPT-OS® platform.
© 2025–2026 Pinnacle Blooms Network®, unit of Bharath Healthcare Laboratories Pvt. Ltd. All rights reserved. MSME: Udyog Aadhaar TS20F0009606 | GSTIN: 36AAGCB9722P1Z2