
She doesn't know her own strength.
And she tries. You can see her trying. Something goes wrong between her brain and her hands — every single time. This is not a behavior problem. It's a calibration challenge. And calibration can be corrected.

A-097 | Sensory Processing
You Are Not Failing. Your Child Is Not Being Aggressive.
The Scene
She's six years old. This morning she tried to pet the cat — gently, you saw her try — and the cat ran away scratching. At breakfast she set her glass down and it shattered. She wasn't throwing it. She was placing it. Her placing is everyone else's slamming.
At school her teacher pulled you aside again: "She needs to learn to be gentle." You've been telling her to be gentle her whole life. Gentle hands. Soft touch. Easy, easy. She knows. She tries.
The Validation
Between her brain saying gentle and her hands actually being gentle, something goes wrong every single time. You are not failing. Your child is not being aggressive.
Her proprioceptive system — the sense that tells her brain how hard her muscles are working — is not giving accurate feedback. She cannot feel how hard she's pushing. This is a calibration problem. And calibration can be corrected.
🔬 Technique A-097
Age 2–12 years
10–20 min/session
Act I — Recognition
You Are Among Millions of Families Navigating This Exact Challenge.
80%
Sensory Difficulties
Of children diagnosed with ASD experience significant sensory processing difficulties including force modulation challenges
1 in 36
Worldwide ASD
Children worldwide are diagnosed with autism — the population this affects most severely
4–8M
In India
Children in India estimated to live with significant sensory processing challenges affecting daily functioning
Force modulation difficulty — using too much force without feeling it — is one of the most common and least understood challenges in sensory processing. It affects children with autism, sensory processing disorder, developmental coordination disorder (DCD), ADHD, and hypermobility. It is not aggression. It is not carelessness. It is a proprioceptive system that is not providing accurate feedback about force output. This is one of the most navigable challenges in pediatric therapy — when approached correctly.
Act I — The Science
This Is a Wiring Difference. Not a Behavior Choice.
The Proprioceptive System
Proprioception is your child's sixth sense — the internal GPS that tells the brain where body parts are in space, how much force muscles are generating, and how to calibrate movement in real time.
Proprioceptive receptors in muscles (muscle spindles), tendons (Golgi tendon organs), and joints fire continuously during movement. Their signals travel to the cerebellum and somatosensory cortex to create real-time feedback about force production.
When this system is under-responsive: Proprioceptive thresholds are elevated — the brain needs MORE force to register "force is happening." The child applies more force because lighter force doesn't register as "enough." They do not feel the difference between soft and firm.
Parent Translation
Imagine trying to adjust a volume knob while wearing thick gloves. You know you need to turn it up a little — but you can't feel the knob properly, so you turn it too much. That's your child's proprioceptive system.
She knows she should press gently. But her hands aren't getting clear feedback about how hard they're already pressing. So the volume always comes out too loud.
Clinical Term: Force Modulation Difficulty / Proprioceptive Processing Dysfunction — The inability to accurately grade and regulate force output in motor actions due to insufficient or inaccurate proprioceptive feedback. Distinct from intentional aggression or deliberate roughness.

Act I — Development
Your Child's Journey. Here Is Where You're Going.
0–2 Years
Proprioceptive system develops through movement, handling, and sensory play
2–4 Years
Force modulation begins developing — children learn "gentle" through feedback and social response
4–7 Years
Social consequences of force miscalibration become prominent at school and in peer play
You Are Here
Without intervention, difficulties often intensify social isolation — with structured intervention, significant improvement is achievable
With Intervention
Functional force calibration across contexts — gentle hugs, unbroken crayons, friendships intact
What commonly co-occurs: Sensory Processing Disorder (SPD), Autism Spectrum Condition (ASD), Developmental Coordination Disorder (DCD), ADHD, Hypermobility/EDS, and low muscle tone (hypotonia). Recognizing these co-occurrences helps target the right intervention approach from the start.

Act I — Evidence
Clinically Validated. Home-Applicable. Parent-Proven.
🏆 Level I Evidence
Systematic Review + Meta-Analysis Grade
92% Strong Evidence Base
The proprioceptive-based materials and force-grading approaches on this page are supported by Level I systematic review evidence and validated across Indian home-based settings.
Key Studies
- PRISMA Systematic Review (2024): 16 studies confirm sensory integration is evidence-based practice for ASD. Proprioceptive input is a validated core component. PMC11506176
- Meta-Analysis, World J Clin Cases (2024): SI therapy significantly improves gross/fine motor skills, adaptive behavior, and social skills. PMC10955541
- Padmanabha et al., Indian J Pediatr (2019): Indian RCT confirms home-based sensory intervention programs produce significant developmental outcomes when parent-administered with proper training.
- WHO NCF (2018): Sensory-motor stimulation as an essential component of nurturing care globally.

Act II — The Technique
A-097: Proprioceptive Input & Force Modulation Training
"Teaching the Body to Feel Its Own Strength"
What It Does
- Provides intense proprioceptive input that "calibrates" an under-responsive system
- Creates external feedback loops that supplement unclear internal feedback
- Builds conscious force-grading skills through structured, playful practice
- Transfers force awareness into social touch, writing, object handling, and daily activities
What It Is NOT
- A behavioral intervention — this is sensory, not punitive
- A quick fix — proprioceptive change happens over weeks to months
- A replacement for OT assessment — this is home extension of clinical programming
Domain A: Sensory Processing
Age 2–12 years
Daily or 3–5×/week
1. Theraputty
2. Weighted Materials
3. Heavy Work
4. Force-Grading Games
5. Writing Tools
6. Sensory Fidgets
7. Compression Clothing
8. Feedback Systems
9. Social Touch Practice

Act II — Disciplines
This Technique Crosses Therapy Boundaries — Because the Brain Doesn't Organize by Therapy Type.
🔵 Occupational Therapy (Primary Lead)
OTs design the sensory diet — the scheduled proprioceptive input plan that runs throughout the day. They assess the proprioceptive system formally (SPM, Sensory Profile 2, EASI) and prescribe intensity, frequency, and material progression. The techniques on this page emerge directly from sensory integration OT practice.
🟢 ABA / BCBA (Behavioral Support Layer)
ABA therapists structure the reinforcement schedule that makes force-grading practice motivating and repeatable. They address behavioral consequences of force miscalibration and use data collection to track force modulation progress objectively. Session structure principles here follow ABA methodology.
🟡 Special Education (School & Learning Layer)
SpEd specialists translate force modulation interventions into classroom accommodations: weighted lap pads during seat work, resistance bands on chair legs, writing tool modifications, and movement breaks before fine motor tasks. They communicate proprioceptive needs to teachers and build school-based sensory diets.
🟠 NeuroDev Pediatrics (Medical Authority)
NeuroDev physicians rule out medical contributors (hypermobility, hypotonia, neurological conditions) and provide the diagnostic framework. They validate the intervention approach from a medical evidence standpoint and coordinate with OT for integrated care. Escalation decisions go through this lens.

Act II — Targets
What We're Working Toward — Precisely.
Not "be gentler." Specific, observable, measurable targets.
Proprioceptive Awareness
Child begins to feel the difference between heavy force and light force. Measurement: Can squeeze theraputty to different marked levels on request? Can identify "harder" vs "softer" squeeze?
Writing Pressure Calibration
Child maintains writing pressure that does not tear paper and produces legible marks. Mechanical pencil lead does not break in normal use. Measurement: Writing sessions without paper tears; pencil lead intact for 5+ minutes.
Object Handling
Child sets down objects without slamming. Opens and closes doors/drawers without force. Handles fragile items without breaking them. Measurement: No accidental breakage across 3+ daily contexts.
Calibrated Social Touch
Child can hug without hurting. High-fives without leaving marks. Holds hands without squeezing too hard. Measurement: Social touch without negative feedback in 80%+ of opportunities.
Automatic Calibration
Force modulation occurs without conscious effort or external reminders — across novel contexts and social settings. Measurement: 6+ weeks of consistent appropriate force use.

Material 1 of 9
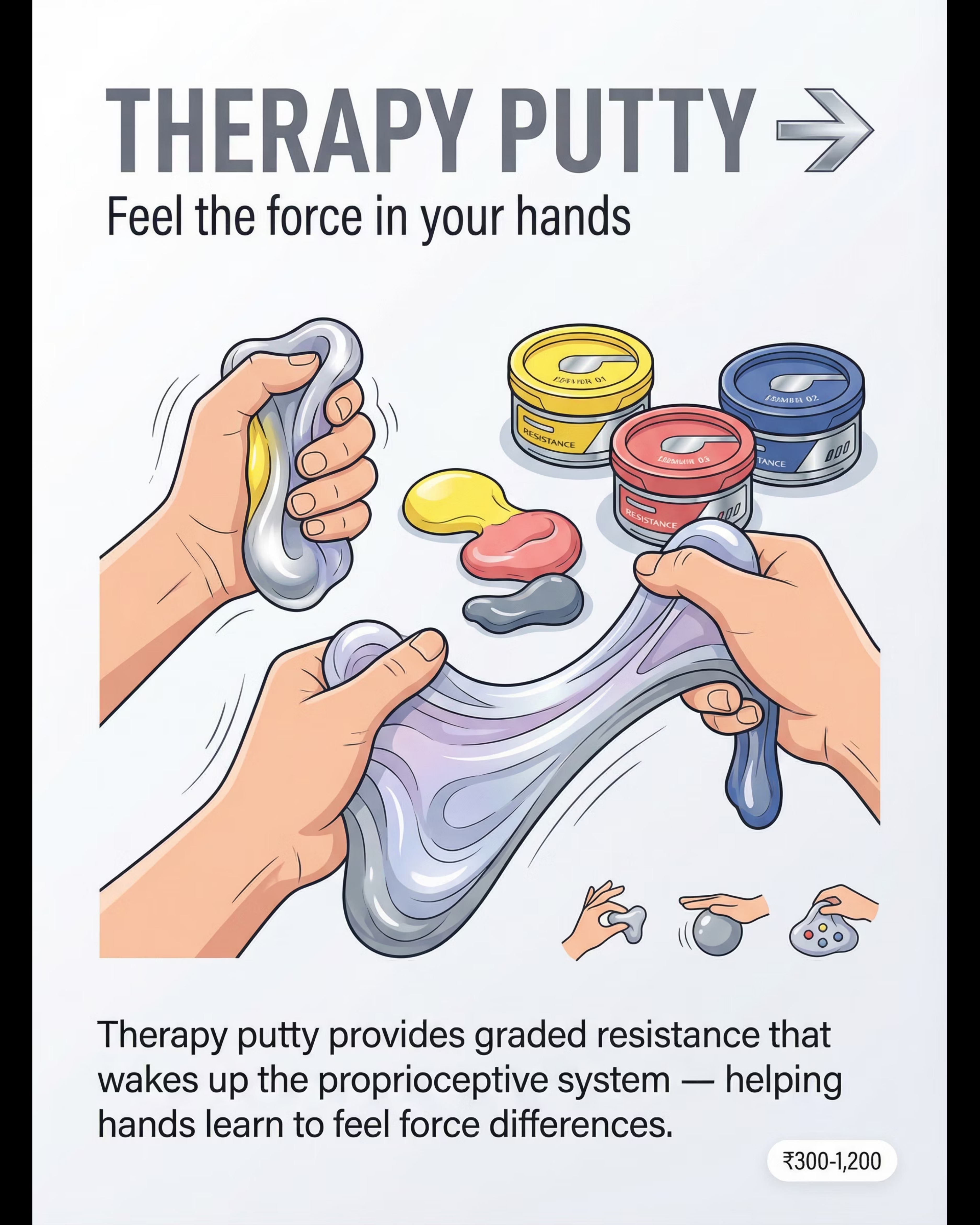
Theraputty & Resistance Putty
Feeling force through resistance
Why It Works
Color-coded graded resistance putty creates direct proprioceptive feedback through the hands. The child squeezes, pinches, and rolls — feeling how much force they're generating in real time. Different resistance levels build force discrimination skills progressively.
Clinical use: Start with soft (yellow/tan), progress to firm (green), then extra-firm (blue/purple) as calibration improves. The graded progression matches the proprioceptive system's developing sensitivity.
How to Use It
- Squeeze as hard as you can (3 seconds) — then squeeze just a tiny bit (3 seconds)
- Roll into a ball slowly — feel how it pushes back
- Pinch into a thin ribbon without breaking it
- Match a "squeeze level" — can you make it the same as last time?
DIY Alternative ₹0
Stiff bread dough or thick chapati dough. Knead with increasing firmness. Different dough hydrations = different resistance levels.
₹400–1,500
Canon: Resistance/Fine Motor

Material 2 of 9
Weighted Materials
Lap Pads, Wrist Weights, Weighted Vests — Grounding body awareness

Weighted Lap Pads
Placed on the child's lap during seated tasks, a weighted lap pad provides consistent deep proprioceptive input that helps the nervous system regulate and organize. The constant sensory input grounds the child and reduces force miscalibration during fine motor tasks like writing.
DIY: Pillowcase filled with 1kg of rice, sewn shut. Use 5–10% of child's body weight only.

Weighted Vests & Wrist Weights
Weighted vests distribute proprioceptive input across the torso — calming and organizing for children who seek intense sensory input. Wrist weights add resistance during fine motor activities, making force production more conscious and detectable.
Important: Consult OT for appropriate weight before purchasing. Generally 5–10% body weight for vests. Never leave weighted items on unsupervised.
₹800–4,000
Canon: Weighted Sensory Materials
Material 3 of 9
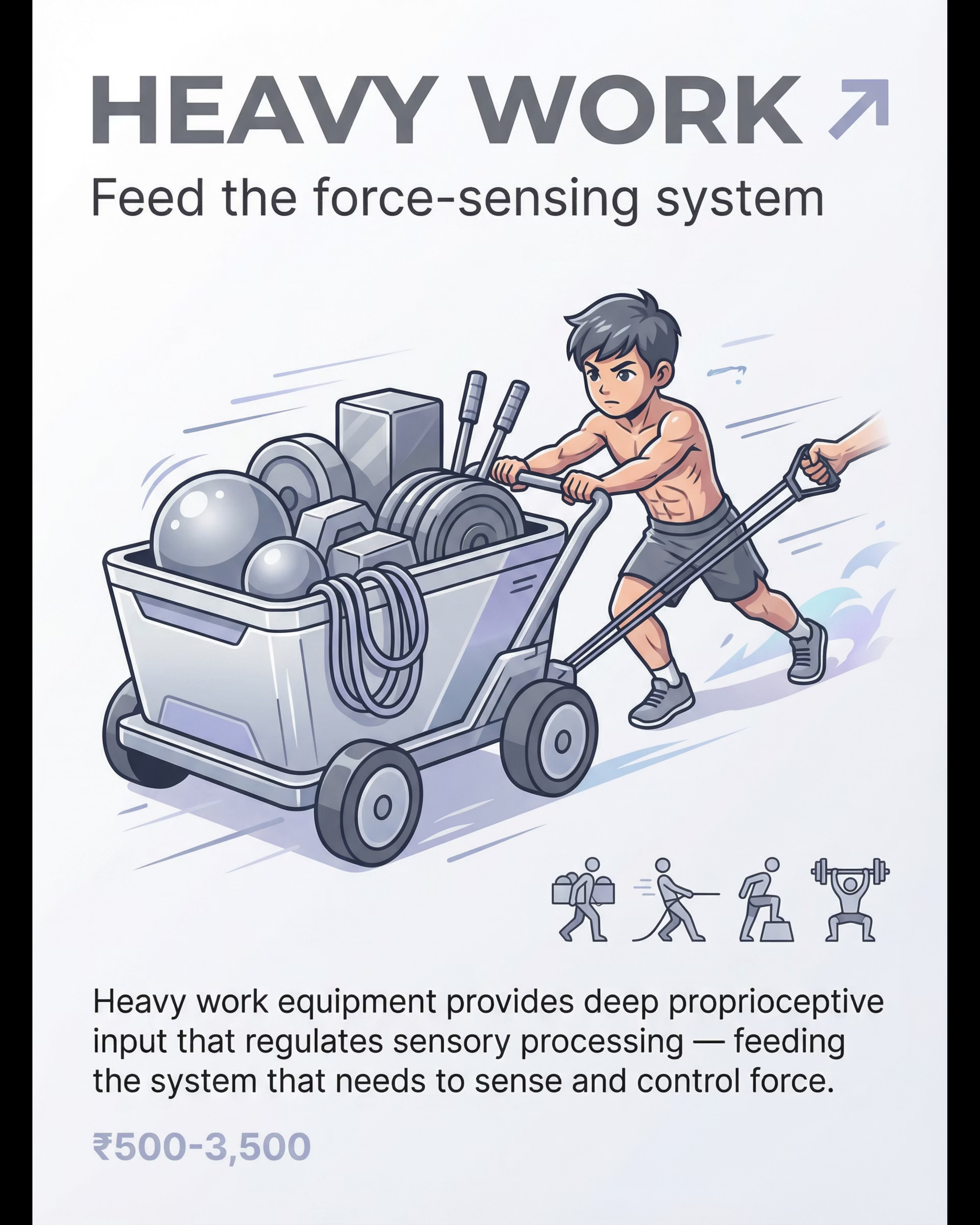
Heavy Work Equipment
Crash Pads, Medicine Balls, Push/Pull — Intense calibration input
Why Heavy Work First
Heavy work activities — pushing, pulling, carrying, jumping — provide the most intense proprioceptive input available. They "wake up" and calibrate the proprioceptive system before any fine motor or force-grading practice. This is Phase A of every session and is not optional.
The muscle spindles and Golgi tendon organs receive rich, clear input during heavy work — filling the proprioceptive "tank" before you ask the nervous system to perform precise force discrimination.
Heavy Work Activities
- Wall push-ups: Palms on wall at shoulder height, 10 slow push-aways
- Animal walks: Bear walk, crab walk across the room
- Carrying: Backpack with 500g–1kg, walk to another room and back
- Crash pad: 5 controlled supervised jumps/crashes onto padded mat
- Push/pull: Laundry basket full of heavy items across the room
DIY Alternative ₹0
Stack of folded blankets for jumping. Filled laundry basket for pushing. Gallon jug with handle for carrying.
₹1,000–6,000
Canon: Heavy Work Equipment

Material 4 of 9
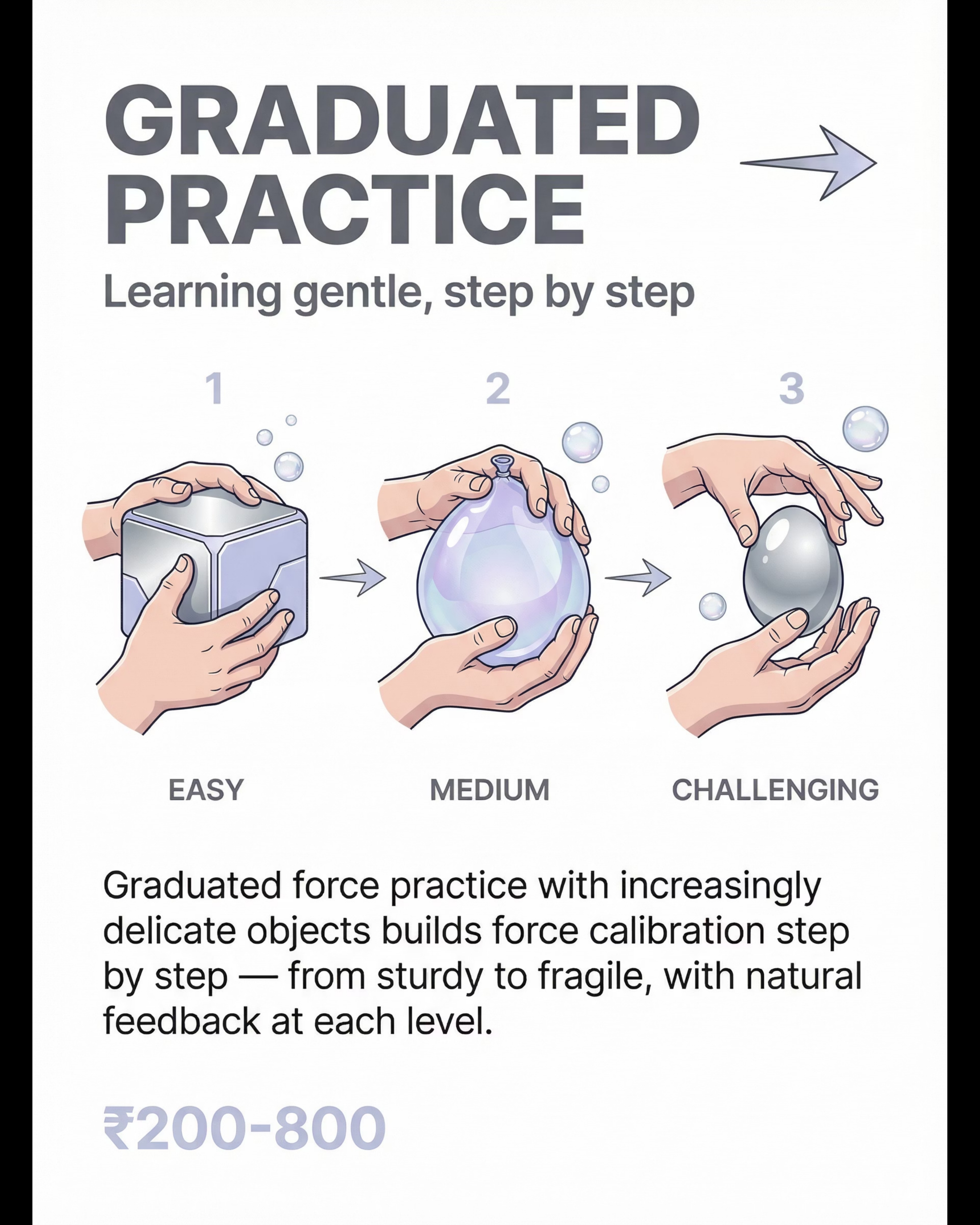
Force-Grading Games & Activities
Egg & Spoon, Stacking, Jenga, Balloons — Practice that teaches calibration
Egg & Spoon Walk
Walking across a room balancing an egg (or ball) on a spoon requires constant, real-time force calibration. Too much grip on the spoon = tilting. The natural consequence teaches proprioceptive discrimination without any adult correction needed.
Stacking & Jenga
Stacking cups or playing Jenga requires extremely precise force gradation — remove a block too forcefully and the tower falls. The game itself is the biofeedback. Children learn force calibration as a side effect of wanting to win.
Balloon Tapping
Keeping a balloon aloft with the gentlest possible taps is one of the most effective force-grading activities. Too much force sends the balloon to the ceiling; too little and it falls. The "just-right" zone becomes physically felt.
Tower Building
Stack 10 cups without knocking — a precise, highly engaging activity that builds force awareness and hand steadiness simultaneously. Begin with larger cups and progress to smaller ones as calibration improves.
₹200–1,500
Canon: Fine Motor Games

Material 5 of 9
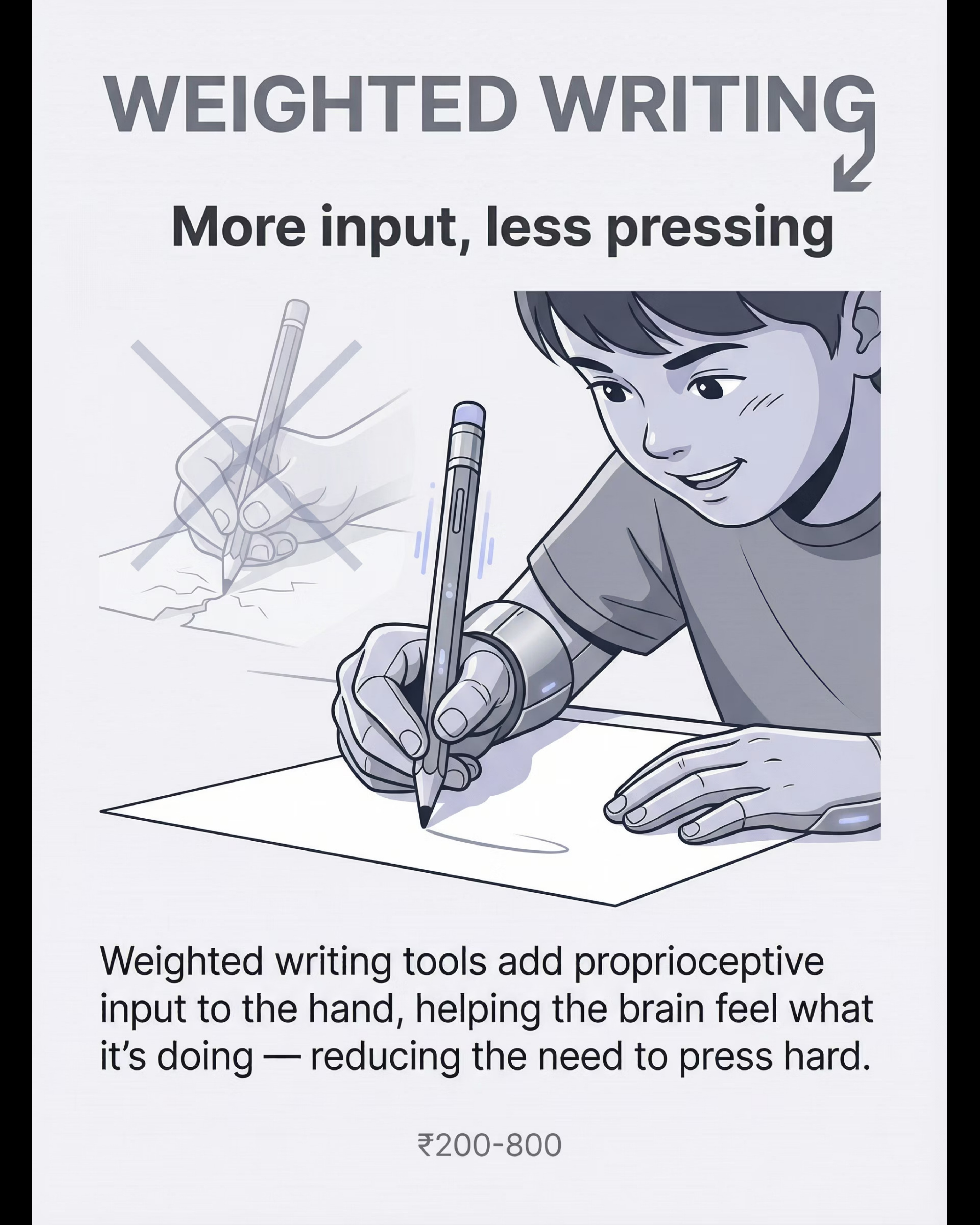
Writing Pressure Tools
Mechanical Pencils, Carbonless Paper, Grips — Making pressure visible
Why Writing Pressure Matters
For many children with force modulation difficulty, writing is where the challenge becomes most visible — and most academically impactful. Torn paper, broken pencil tips, and illegible pressed-down marks signal proprioceptive miscalibration in the hand.
Writing pressure tools make invisible force visible — giving the child immediate, objective feedback about how hard they're pressing, without any adult needing to say a word.
Tool Applications
- Mechanical pencil: Lead snaps immediately when too much pressure is applied — instant, non-punishing feedback that trains calibration rapidly
- Carbonless NCR paper: Stack of sheets reveals how deeply pressure transfers — should go through 1–2 sheets only
- Pencil grips: Textured grips provide tactile-proprioceptive information about grip pressure
DIY Alternative ₹15
Basic mechanical pencil. Stack 5–10 sheets of regular paper. Check impression depth after writing practice.
Sequencing note: Introduce writing pressure tools only after 2–3 weeks of proprioceptive loading. Premature use creates frustration before calibration exists.
₹100–800
Canon: Fine Motor / Writing Materials
Material 6 of 9
Sensory Feedback Fidgets
Pop Tubes, Resistance Fidgets, Stress Balls — Feedback through manipulation
How Fidgets Build Proprioception
Sensory fidgets provide continuous, accessible proprioceptive feedback throughout the day — at the desk, in the car, during circle time. They are not toys for distraction; they are sensory tools that keep the proprioceptive system active and regulated.
Pop tubes provide resistance in both directions (pull and push). Resistance fidgets require graded squeezing. Stress balls provide variable compression feedback. Together, they create a portable sensory diet that extends the session into everyday life.
Fidget Selection by Goal
- Force discrimination: Graded resistance stress ball set (different firmness levels)
- Sustained input: Pop tube — child pulls and pushes repeatedly during listening tasks
- Fine motor precision: Small resistance fidget that requires fingertip-specific pressure
- Oral seekers: Chewable fidget necklace — proprioceptive input through jaw and neck
DIY Alternative ₹0
Balloon partially filled with flour or rice = DIY stress ball with variable firmness. Sand-filled balloon = extra resistance.
₹100–600
Canon: Sensory Fidget Materials

Material 7 of 9
Compression & Proprioceptive Clothing
Shirts, Vests, Shorts, Body Socks — Constant proprioceptive input
Why Compression Works
Compression garments provide constant, gentle deep pressure across the body — a low-level proprioceptive signal that keeps the nervous system regulated throughout the day. Unlike a single therapy session, compression clothing delivers hours of continuous input during school, meals, and play.
For children who are proprioceptive under-responders (need more input to register sensation), compression clothing significantly reduces the sensory "noise" that drives overforce — because the system is already receiving the input it needs.
How to Use Compression Garments
- Begin with a snug-fitting sports undershirt layered under school uniform
- Should feel snug but not restrictive — child should be able to take a deep breath comfortably
- Start with 1–2 hours during most challenging periods (writing time, recess)
- The nervous system habituates to constant input — strategic use beats all-day wear
- Body socks (lycra full-body) provide intense input and are excellent for home use
DIY Alternative ₹0
Snug-fitting sports undershirt already in wardrobe. Layer under school uniform. Should feel comfortably tight.
₹500–2,500
Canon: Compression Clothing
Material 8 of 9
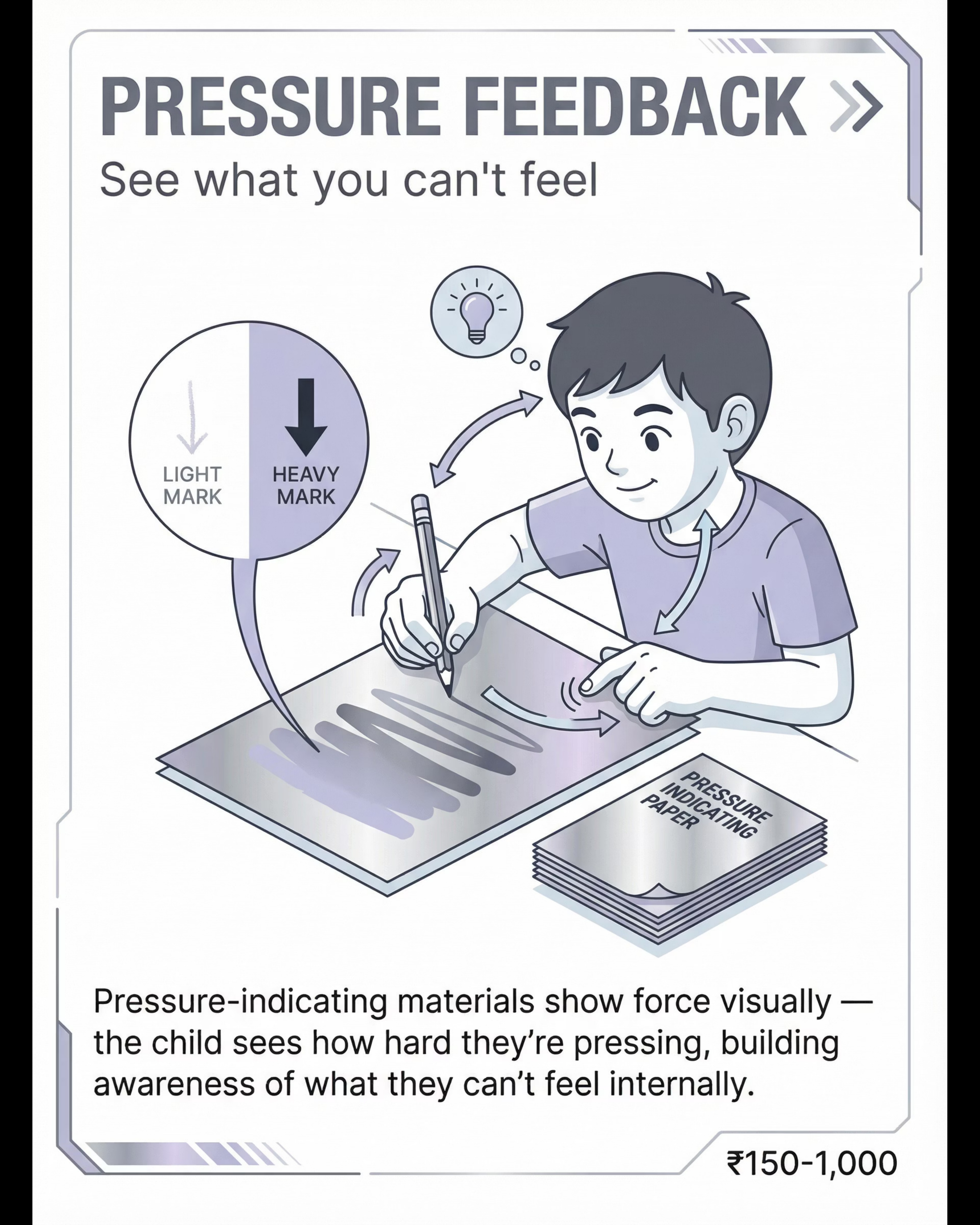
Visual & Auditory Force Feedback Systems
External cues for internal calibration
Why External Feedback Matters
When the internal proprioceptive system is not providing accurate force data, external feedback systems create a supplementary signal — visible, objective, and immediate. They help the child understand what their body is doing from the outside while the internal system is developing accuracy.
A digital bathroom scale is the most accessible force feedback tool available in any home. The child presses, sees a number, and can practice matching a target number — making invisible force completely visible.
Feedback System Applications
- Bathroom scale (₹500–800): Child presses palms on scale surface and reads force in kg — set target numbers to match. Practice making the number go lower and lower.
- Pressure-sensitive apps: Tablet apps that respond to touch pressure show force as color intensity or sound — immediate visual feedback for hand force
- Auditory feedback: Activities where too much force = a loud sound (alarm, bell) naturally train force reduction
- Video feedback: Recording and watching back — child sees their own force level from the outside
DIY Alternative ₹500
Bathroom scale from any general store. Digital display provides immediate numeric force output for practice.
₹500–5,000
Canon: Biofeedback / Visual Feedback

Material 9 of 9
Social Touch Practice Materials
Stuffed Animals, Dolls, Practice Partners — Learning gentle connection
Why Practice Safe Touch
Social touch is the ultimate transfer target — the moment when proprioceptive calibration becomes human connection. But children cannot practice calibrated touch with peers before they can calibrate it at all. Stuffed animals and practice partners create a safe, zero-consequence environment to develop gentle touch skills before they're needed in real social contexts.
The progression is deliberate: stuffed animal → self-squeeze comparison → family member (parent/sibling) → peers. Each step requires demonstrated calibration before advancing.
Practice Sequence
- Stuffed animal baseline: "Hug teddy so gently he doesn't squish" — observe and discuss
- Graduated pressure: "Now hug him at a 3 out of 10 — now a 7 — now back to 2"
- Self-comparison: Child squeezes their own arm gently, then more firmly — feels the difference
- Family member practice: Gentle high-five, soft handshake, calibrated hug with parent
- Social integration: Practiced touch in real peer contexts with supervision
₹300–1,500
Canon: Transition Objects

Act II — Investment
9 Materials. Evidence-Backed. Available Today.
Sourced from the Pinnacle 128 Canon Materials system. Every item on this page has a ₹0 DIY alternative — start with what you have.
Material | Price Range | DIY Alternative | |
1. Theraputty & Resistance Putty | ₹400–1,500 | Stiff chapati/bread dough | |
2. Weighted Materials | ₹800–4,000 | Rice-filled pillowcase (consult OT for weight) | |
3. Heavy Work Equipment | ₹1,000–6,000 | Laundry basket, household items (free) | |
4. Force-Grading Games | ₹200–1,500 | Balloon (₹5), plastic cups, plastic eggs | |
5. Writing Pressure Tools | ₹100–800 | Mechanical pencil ₹15, stacked paper | |
6. Sensory Feedback Fidgets | ₹100–600 | Flour-filled balloon stress ball | |
7. Compression Clothing | ₹500–2,500 | Snug sports undershirt (existing wardrobe) | |
8. Visual Feedback Systems | ₹500–5,000 | Bathroom scale ₹500–800 | |
9. Social Touch Materials | ₹300–1,500 | Stuffed animal you already own |
Essential Starter Kit: Heavy work activities (free/household) + Theraputty (₹400) + Force-grading games (₹200) = ₹600 to start. Full sensory diet kit: up to ₹6,000. The neurological mechanism is identical whether you use clinical-grade theraputty or stiff chapati dough.

Act II — Safety
Read This Before Every Session. Non-Negotiable.
🔴 ABSOLUTE STOP
- Child is unwell, feverish, or has acute pain anywhere
- Open skin wounds, rashes, or skin sensitivity in area of material contact
- Significant meltdown or emotional crisis in the past 2 hours
- Child shows severe distress at sight of materials — do not force proceed
- Medical Stop: Confirmed cardiac conditions, seizure disorder, or significant hypermobility with joint instability — consult doctor before weighted materials or heavy work
🟡 MODIFY & PROCEED
- Child is tired but not dysregulated — shorten to 5 minutes, lighter intensity
- Mild hypermobility — avoid joint compression; focus on muscle-based proprioception
- First time using weighted materials — start at minimum weight (500g) and observe 10 minutes
- Under 3 years — all activities floor-level, fully supervised, mouth-safe putty only
🟢 GO CONDITIONS
- Child is calm, alert, and has eaten within the past hour
- No meltdown in past 2 hours
- Materials inspected — no broken pieces, no choking hazards
- 15–20 uninterrupted minutes available
- You have reviewed the session protocol at least once
Weight Guidelines: Lap pads 0.5–1.5 kg (max 10% body weight). Weighted vests 5–10% body weight for maximum 20–30 minutes. Never leave weighted items on unsupervised. Stop immediately if: skin color changes, severe distress, vomiting, joint pain, or refusal escalating to crisis.

Act II — Environment Setup
The Right Environment Prevents 80% of Session Failures.
Setup Checklist
- ✅ Floor mat / non-slip surface for movement activities
- ✅ Materials within child's arm's reach — no reaching across
- ✅ Distractions removed: screens off, toys put away, siblings in another room
- ✅ Phone on silent
- ✅ Visual timer visible to child — supports session transitions
- ✅ Water and preferred snack available post-session
Materials Pre-Positioned
- Putty/resistance materials on table
- Heavy work equipment at floor level
- Writing tools with paper stack on table
- Fidgets in accessible bin/basket
- Stuffed animals for social touch practice at floor level
Environment Specifications
Factor | Recommendation | |
Lighting | Natural or warm light. Avoid harsh fluorescent. | |
Sound | Quiet or low background music. No television. | |
Temperature | Comfortable. Compression clothing works better when not overheated. | |
Space | Minimum 2m × 2m clear floor space for movement activities | |
Surfaces | Non-slip mat for floor work. Stable table/chair for fine motor work. |
Parent position: alongside the child (not behind). Get to the child's physical level — floor or low chair. The environment communicates safety before a single word is spoken.

Act III — Readiness
60-Second Pre-Flight Check. Do This Before Every Session.
"The best session is one that starts right. A 5-minute perfect session builds more than a 20-minute forced one."
Error: table is too large to display. Please roll back to an earlier version using Version History.
All Green → GO
Proceed to Step 1: The Invitation
1–2 Amber → MODIFY
Shorten session to 8 minutes. Lower-intensity materials only (fidgets, stuffed animals). Skip heavy work.
Any Red → POSTPONE
Do a short calming activity and try again tomorrow. Postponing is always the right call.

Step 1 of 6
🖐 The Invitation
"Come play with me — not 'we're doing therapy now'"
The Opening Script:"Hey [name], I found something really cool. Want to come see what this stuff does?"
(Hold up the theraputty or fidget — don't hand it over yet.)
Body Language
- Get to the child's physical level (floor or low chair)
- Relaxed, open posture — no urgency, no performance pressure
- Neutral to warm facial expression — not overly enthusiastic (can feel pressuring)
- Materials in your hands, not pushed toward the child
Acceptance Cues (child is ready)
- Moves toward you or the material
- Asks "what is that?"
- Makes eye contact or glances at material with interest
- Reaches toward material
Resistance Cues (modify)
- Moves away or turns body away
- Pushes material away
- Covers eyes or face
- Verbal refusal ("no" / "I don't want to")
If Resistance Occurs
Don't push. Say: "Okay, I'll just leave this here. You can touch it if you want." Leave material nearby. Wait 2–3 minutes. Try once more with a different material. If still resistant → Postpone session.
Timing: 30–60 seconds. A rushed or pressured invitation undermines the entire session.

Step 2 of 6
🤲 The Engagement
"Introducing the material — following the child's lead"
Child Response Indicators
- Engagement: Actively manipulating, vocalizing, maintaining contact — proceed with session
- Tolerance: Holding material but not interacting much — normal start, maintain gentle encouragement
- Avoidance: Dropping, shaking off, distress signals — see troubleshooting (Card 30)
Reinforcement Cue
When child actively engages: "Yes! I can see your hands working so hard."Specific. Immediate. Genuine.
Timing: 1–3 minutes. Follow the child's pace — do not rush to demonstrate force discrimination before genuine engagement is established.

Step 3 of 6
⚙️ The Therapeutic Action
"The active ingredient — proprioceptive input through graded force practice"
1
Phase A: Proprioceptive Loading (3–4 min)
Purpose: "Wake up" and calibrate the proprioceptive system through intense input — heavy work FIRST, always.
- Wall push-ups: 10 slow push-aways, palms at shoulder height
- Animal walks: Bear walk 2 lengths, crab walk back
- Carrying: Backpack with 500g–1kg to another room and back
- Crash pad: 5 controlled supervised jumps
2
Phase B: Graded Resistance Practice (3–4 min)
Purpose: Build force discrimination through resistance feedback. The goal is range, not strength.
- "Squeeze as hard as you can — go!" (3 seconds)
- "Now squeeze... just a tiny little bit." (3 seconds — compare deformation)
- "Roll it slowly — feel how it pushes back"
- "Pinch it into a thin ribbon without breaking it"
3
Phase C: Force Feedback Transfer (3–4 min)
Purpose: Transfer proprioceptive awareness to a functional task. Choose ONE:
- Writing: Mechanical pencil on 5 sheets — impression should go through 1–2 sheets only
- Object handling: "Set this glass down so quietly I can't hear it" — repeat 5×
- Social touch: "Hug teddy so gently he doesn't squish"
- Force-grading game: Egg-and-spoon walk or 10-cup tower
Common Error: Rushing Phase A. Heavy work is not optional — it calibrates the proprioceptive system for Phases B and C. Skipping it reduces effectiveness significantly.

Step 4 of 6
🔁 Repeat & Vary
"3 good reps > 10 forced reps. Dosage matters."
Therapeutic Dosage
- Phase A (Heavy Work): 1 complete sequence per session. Repeat every session.
- Phase B (Resistance): 3–5 putty cycles per session (each cycle = 3 squeeze variations)
- Phase C (Transfer): 3–5 repetitions of chosen transfer task
Satiation Indicators — Child Has Had Enough
- Drops or puts material down voluntarily
- Begins seeking distraction — looks away, reaches for other objects
- Quality of engagement decreasing (going through motions)
- Yawning or physically settling
When you see satiation: Don't push for "one more." Move immediately to Step 5. A session that ends on the child's voluntary terms maintains motivation for tomorrow.
Variation Options (across sessions)
Variation Type | Example | |
Material swap | Rotate: putty, dough, stress ball, pop tubes | |
Activity swap | Egg-and-spoon, balloon tap, Jenga, stacking cups | |
Heavy work swap | Bear walk → wheelbarrow → carrying → crash pad | |
Force level game | "Can you set it down at a 2 out of 10 force?" | |
Partner variation | Practice social touch with different family members |

Step 5 of 6
🌟 Reinforce & Celebrate
"Within 3 seconds of the behavior. Specific. Enthusiastic. Real."
For Force Modulation Success
"That was SO gentle — I felt nothing when you put it down! That's exactly it."
For Effort (Even If Not Perfect)
"I saw you trying to be gentle. Your brain is working so hard to learn this."
For Heavy Work Completion
"Those bear walks were AMAZING — your whole body worked so hard!"
Type | Example | When to Use | |
Verbal praise | "Incredible force control — your hands are learning!" | Every correct response, immediately | |
Token/sticker | 1 token per session → 5 tokens = preferred reward | Daily tracking | |
Natural reward | "You set that down so gently — now you get to hold it yourself" | Object handling tasks | |
Physical play | Post-session rough-and-tumble (supervised) as reward | High motor-seeking children | |
Preferred activity | 5 minutes of chosen screen/game post-session | Session completion |
Key ABA Principle: Celebrate the attempt, not just the success. The child who tries to be gentle and still squeezes too hard is showing neurological effort — that effort deserves recognition. The calibration will follow the effort.

Step 6 of 6
🌙 The Cool-Down
"No session ends abruptly. Transitions are therapeutic."
Transition Warning Script
"Two more, then we're all done."
(Show 2 fingers. Point to visual timer if available.)
If Child Resists Ending
- Acknowledge: "I know you want to keep going — that means you're enjoying it!"
- Firm but warm: "We're finishing for today. Same time tomorrow."
- Offer bridge: "You can carry the putty to the shelf — that's your special job."
Post-Session
Child should feel organized, calm, not overstimulated. 10–15 minutes of free play is the ideal transition activity after a session — let the nervous system integrate what it just learned.
Joint compressions: Gently press down through child's shoulders for 10 seconds. This is calming and organizing proprioceptive input — the nervous system's equivalent of a deep breath.
Act III — Data
60 Seconds of Data Now Saves Hours of Guessing Later.
Record These 3 Data Points Immediately Post-Session
1. Engagement Level
1 (refused) — 2 (tolerated) — 3 (engaged) — 4 (enthusiastic)
1 (refused) — 2 (tolerated) — 3 (engaged) — 4 (enthusiastic)
2. Force Modulation Observation
A. No awareness — same force as baseline
B. Aware but inconsistent — some calibration moments
C. Calibrating with reminders/feedback
D. Spontaneous force modulation observed
A. No awareness — same force as baseline
B. Aware but inconsistent — some calibration moments
C. Calibrating with reminders/feedback
D. Spontaneous force modulation observed
3. Notable Moment (1 sentence)
"Today [child name] [what happened]"
Example: "Today Priya set her cup down quietly — no slam — first time."
"Today [child name] [what happened]"
Example: "Today Priya set her cup down quietly — no slam — first time."
Why This Data Matters
Proprioceptive change is gradual and not always visible in daily life before it shows up in session data. Tracking engagement level gives you a leading indicator — improvement in engagement consistently precedes improvement in force modulation by 1–3 weeks.
If engagement hasn't improved after 6 weeks of consistent sessions, that is the signal to consult an OT — not to continue pushing the same approach. Data tells you which fork in the road to take.
📥 Download: A-097 Weekly Progress Tracker — 8-week sheet at pinnacleblooms.org/trackers/A-097

Act III — Troubleshooting
Session Abandonment Is Not Failure. It's Data.
These are the 7 most common problems with A-097. Every one has a fix.
Problem 1: Child Refuses to Touch the Putty
Why: Tactile defensiveness often co-exists with proprioceptive under-responsivity. Fix: Start with indirect proprioception — heavy work (carrying, wall push-ups) before any hand material. Introduce putty inside a plastic bag first — same resistance, no direct skin contact.
Problem 2: Child Uses Putty for 30 Seconds Then Throws It
Why: Short attention + novelty wearing off. Normal in early sessions. Fix: Reduce session length. Add a "mission" — "Can you squeeze it until the crack disappears?" Rotate materials more frequently.
Problem 3: Good in Therapy, Unchanged Everywhere Else
Why: Skill hasn't generalized yet — normal and expected. Transfer takes time and practice in each specific context. Fix: Practice at the actual dinner table, with the actual pencil at the actual desk, not only during "therapy time."
Problem 4: Heavy Work Makes Child MORE Dysregulated
Why: Some children are sensory avoiders — heavy work intensifies their overload. Fix: Switch to calming proprioceptive input — slow joint compressions, firm hugs, weighted blanket. Consult OT to determine sensory profile.
Problem 5: Child Breaks Things and Seems Satisfied
Why: The proprioceptive feedback loop is working — they got the input they needed. Fix: Celebrate the force briefly (heavy work), then immediately pivot: "Now let's see how GENTLE you can be." The contrast is the lesson.
Problem 6: Writing Tools Create Frustration and Tears
Why: Breaking pencil leads is punishing data before calibration exists. Too early for this tool. Fix: Return to foundational proprioceptive loading for 2–3 more weeks before reintroducing writing pressure tools. Sequence matters.
Problem 7: No Visible Progress After 3 Weeks
Why: Proprioceptive system changes take 6–12+ weeks. Three weeks is normal "no visible change" territory. Fix: Review data — is engagement improving even if force modulation isn't? Engagement is the prerequisite. If engagement also hasn't improved, consult OT.
Act III — Personalization
No Two Children Are Identical. This Is Your Child's Version.
Easier Modifications
For bad days or early sessions
- Putty in plastic bag (no direct skin contact)
- Lap pad only (no vest)
- Household heavy work only — no equipment
- 5 minutes total instead of 15
- Focus on Phase A only — skip B and C initially
- Stuffed animal only for social touch
Standard Protocol
As written in Steps 1–6
- Standard putty grades and resistance levels
- Full Phase A-B-C sequence
- 15–20 minute sessions
- 3–5 repetitions of transfer task
- Standard reinforcement schedule
Harder Modifications
For good days or advanced stages
- Firmer resistance putty grade
- Wrist weights added to writing tasks
- Force-grading game with timer
- Biofeedback (bathroom scale reading)
- Transfer to peer social touch practice
- Self-monitoring: "Tell me — was that gentle or too hard?"
By Sensory Profile
Sensory Seeker | Mixed Profile | Sensory Avoider | |
Lead with crash pad + heavy work | Lead with moderate putty + brief heavy work | Lead with joint compressions + weighted blanket | |
Use firmest putty | Standard putty grades | Softest putty; putty-in-bag option | |
More reps, longer Phase A | Standard repetitions | Fewer reps; longer cool-down |
By Age
- 2–4 years: Entirely play-based. Heavy work = pushing toy cart, carrying books. Putty = dough play. Force-grading = "touch the bubble without popping it."
- 5–7 years: As written above. Add writing pressure targets.
- 8–12 years: Self-monitoring layer. Child rates own force level 1–10. Biofeedback tools appropriate. Social touch practice with peers.
Act IV — Progress Arc
Weeks 1–2: Building the Foundation. Not Mastery Yet — Awareness.
Progress: 15%
What "progress" looks like in Weeks 1–2:
- ✅ Child tolerates theraputty for 2 minutes without refusal (even if force is unmodulated)
- ✅ Child completes heavy work activity with engagement
- ✅ Any brief moment of spontaneous gentle action — one door closed quietly, one set-down without slam
- ✅ Parent has completed 5+ sessions — consistency is the real win at this stage
What Is Not Progress Yet — And That's Fine
- ❌ Consistent force modulation across daily life — not expected yet
- ❌ Spontaneous self-correction — not expected yet
- ❌ Transfer to writing or social touch — not expected until Week 4+
- ❌ Peers noticing a difference — too early
Parent Emotional Preparation
In weeks 1–2, you may see increased seeking behavior (child wants more heavy work) before improvement. This is the proprioceptive system "waking up" — it's a good sign. You may also see increased awareness of failure: the child notices when they slam, which they didn't notice before. Awareness before control is the correct sequence.
Data target: Engagement level scoring 3 or 4 on at least 60% of sessions → on track.

Act IV — Week 3–4
Weeks 3–4: Neural Pathways Are Forming. Look for These Signs.
🧠 Child Begins to Anticipate Sessions
Child asks for putty or heavy work unprompted. This signals that the proprioceptive system has begun to recognize and seek the input it needs — a fundamental shift in sensory awareness.
🧠 Spontaneous Self-Correction Emerges
In at least 2–3 instances, child recalibrates after a slam — pauses, tries again more gently. This is the beginning of conscious force modulation. It will become automatic over the following weeks.
🧠 Writing Pressure Measurably Improves
Pencil impressions going through fewer sheets of paper. Pencil lead breaking less frequently. These are objective, trackable indicators of fine motor force calibration developing.
🧠 Parent Confidence Milestone
"I felt more confident running the session this week." This matters enormously — parent competence and consistency are the single strongest predictors of therapeutic outcome in home-based programs.
When to increase intensity: Child requests sessions consistently, completing them at engagement level 4, and showing at least 2 consolidation indicators above. Upgrade to firmer putty grade, add wrist weights to writing tasks, extend Phase B from 3 to 5 cycles.

Act IV — The Breakthrough
Weeks 5–8: This Is When It Becomes Real. Watch for These Moments.
🌟 The Quiet Door
A door closes quietly — without prompting. Child looks at their own hand, surprised. This is the proprioceptive system reporting accurately for perhaps the first time.
🌟 The Unbroken Crayon
Writing produces no torn paper in an entire session. Crayons survive a full art class. These are not small victories — they are neurological milestones.
🌟 The Hug That Doesn't Hurt
A hug doesn't hurt — and someone says so. Child lights up. The same child who used to squeeze so hard kids cried is now giving the gentle embrace their nervous system could never find before.
🌟 The Self-Instruction
Child uses the word "gentle" as a self-instruction — internalizing the concept as felt experience, not just a heard word. This is the moment "gentle" moves from instruction to identity.
🌟 Peers Notice
"Hey, you're not as rough anymore." The cat doesn't run away. These are social confirmations that the nervous system has genuinely recalibrated — not just in therapy, but in the world.
This is neurological change. The muscle spindles and Golgi tendon organs are firing more appropriately. The cerebellum is recalibrating motor output based on accumulated sensory experience. This is not behavior management. This is nervous system development.

Act IV — Celebrate
Your Child's Nervous System Just Learned Something New. That Deserves to Be Marked.
Document It
Photo document the first week with no broken crayons. Write it down: "On [date], [name] petted the cat gently for the first time." These records become part of your child's story of growth.
Milestone Reward
When 3 breakthrough indicators are consistently present → a special celebration (child's choice, not therapy-related). Let the child pick the reward. Their sense of agency amplifies the neurological reinforcement.
Tell the Teacher
Send a brief note — "We're seeing improvement in force calibration at home. Here's what we're doing." Teachers who understand the neurological basis respond very differently than those told to just watch for "aggression."
Share in Community
Share in the Pinnacle parent community. Your milestone encourages families who are still in weeks 1–2 that the breakthrough they're working toward is real. Your story is someone else's hope.
Don't say "finally" — it implies it should have happened sooner. Don't make the celebration about the past difficulty. Just celebrate the current achievement. The child is doing something genuinely hard — their nervous system is literally rewiring.
Act IV — Red Flags
Home-Based Intervention Is Powerful — and It Has Limits. Know When to Call.
🚩 Escalate to Professional OT Assessment If:
- No engagement improvement after 6+ weeks of consistent sessions (5×/week)
- Force modulation difficulties are causing injury to self or others
- Child develops new aversion to touch or physical contact during intervention
- Significant joint pain or hypermobility observed during heavy work
- Child is showing signs of other sensory processing difficulties not addressed here
- School is considering exclusion or restriction due to force-related incidents
🚩 Escalate to NeuroDev Pediatrician If:
- Force modulation difficulties accompanied by significant motor incoordination (falling, bumping into things constantly)
- No formal diagnosis yet and multiple areas of developmental concern
- Force difficulties accompanied by regression in other developmental areas
Your Escalation Path
Home-Based A-097 → OT Assessment → Sensory Profile 2 + EASI → FusionModule™ integrated plan → EverydayTherapyProgramme™ home extension
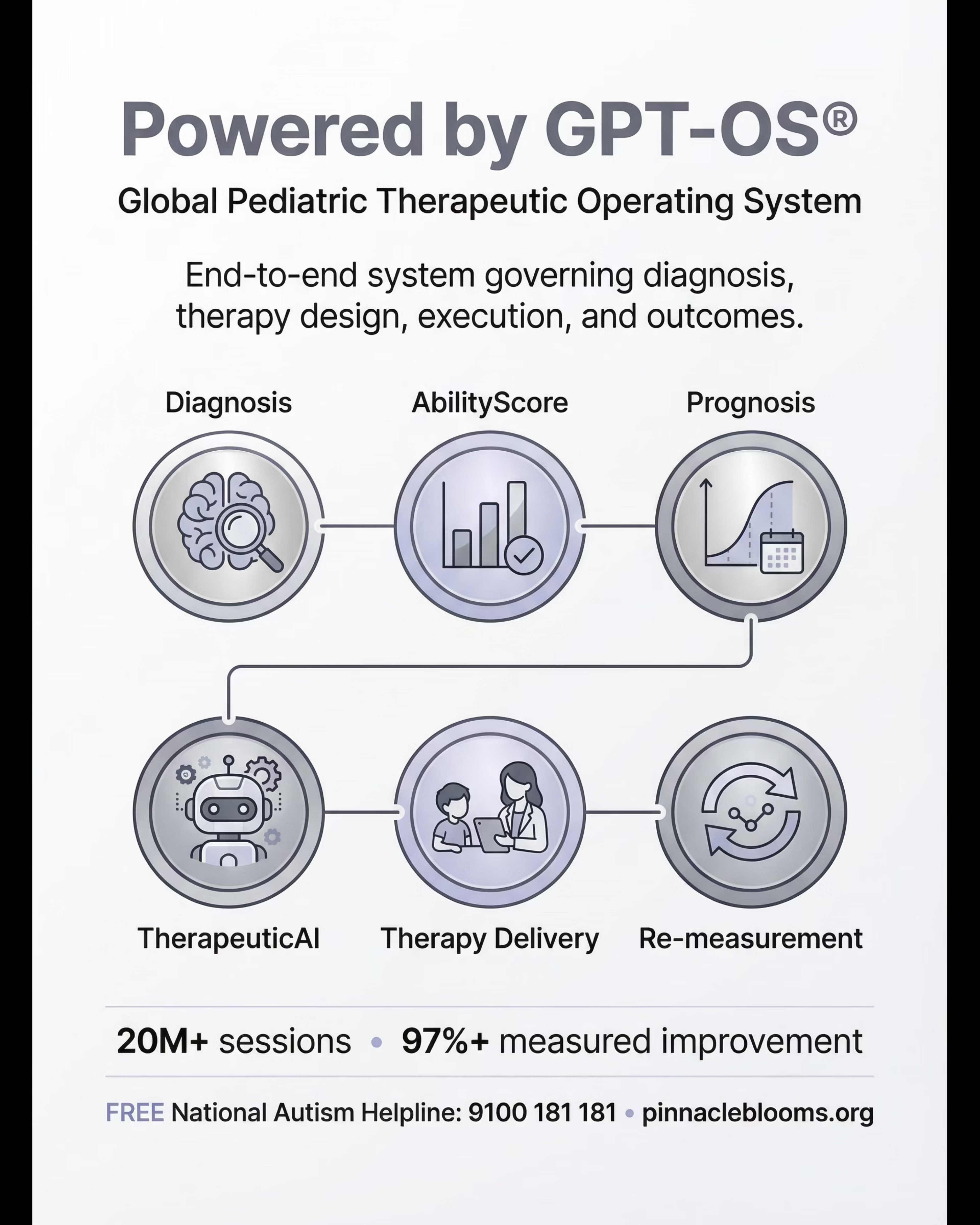
📞National Autism Helpline: 9100 181 181 — FREE, 16+ languages, 24×7. Hindi, Telugu, Tamil, Kannada, Malayalam, Marathi, Bengali, Gujarati, Punjabi, Odia, Urdu, English + regional dialects.
Act IV — Pathway
You Are Here. Here Is Where This Leads.
Why This Sequence
Force modulation (A-097) is foundational to the entire proprioceptive-motor sequence. A child who cannot calibrate force cannot effectively develop body awareness (A-099) or motor planning (A-100). Resolving A-097 — even partially — creates the proprioceptive foundation for everything that follows.
Lateral Connections
- K-1100: Understanding Proprioception (parent education)
- K-1105: Sensory Diet Basics
- K-1110: Heavy Work Activities at Home
Act V — Community
She Learned to Feel Her Own Strength. Here Is That Story.
"My daughter broke everything she touched. Not on purpose — she just couldn't feel how hard she was squeezing, pushing, pressing. Hugs hurt. High-fives left marks. Friends stopped wanting to play with her. She wasn't aggressive. She was just a kid whose body didn't give her accurate feedback.We started with heavy work activities — lots of pushing, pulling, carrying. Then theraputty for her hands. Force-grading games. Compression clothing during school. The OT worked on proprioception constantly.It took time — this wasn't a quick fix. But around month six, I noticed she was closing doors without slamming. She could pet the cat gently. Her writing didn't tear the paper anymore.Last month, a friend told her she gives 'the best hugs.' The same child who used to squeeze so hard kids cried. She learned to feel her strength. Her body finally speaks a language she can understand."
— Parent, Pinnacle Network | Illustrative case. Outcomes vary by child profile.
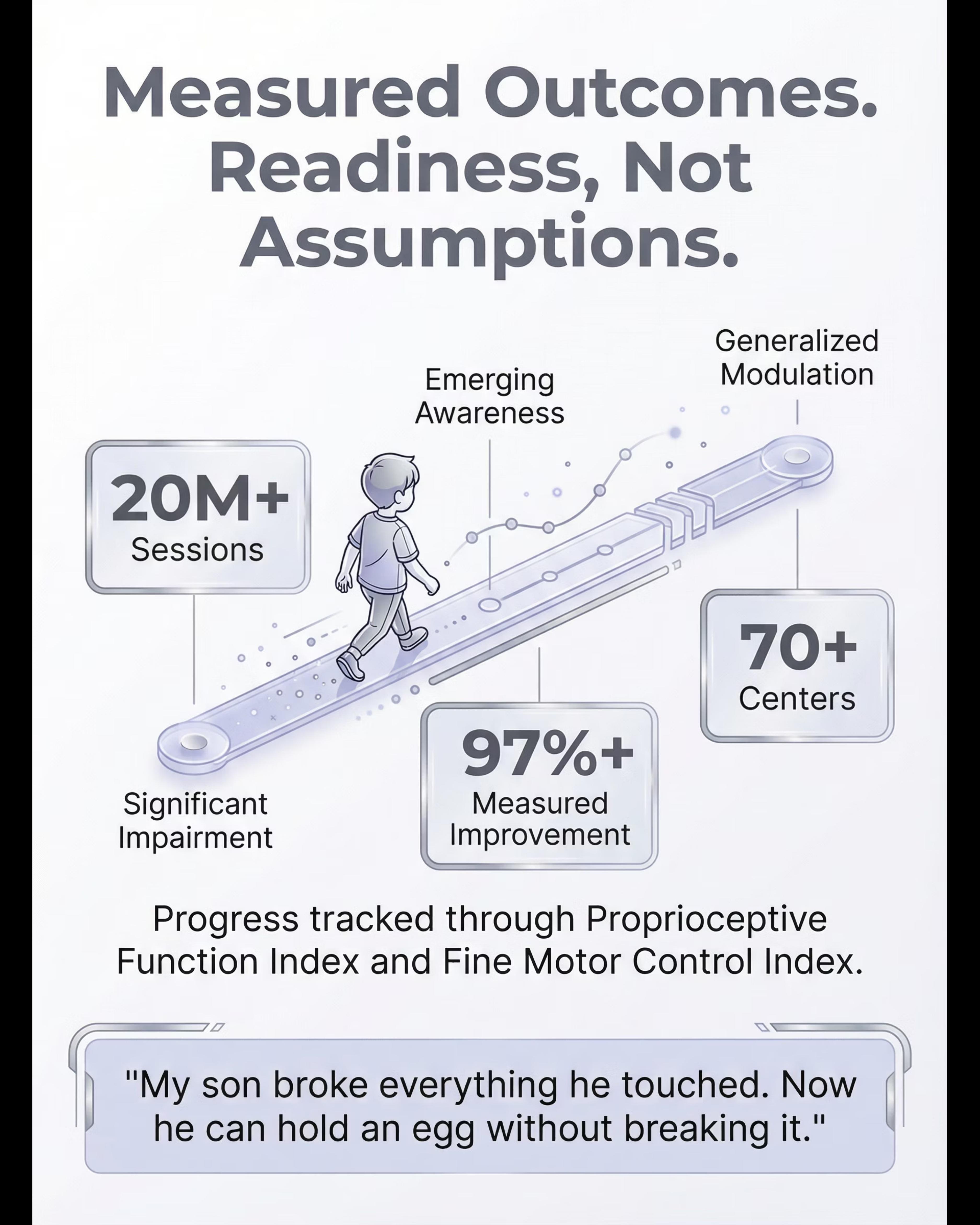
GPT-OS® Readiness Progression (this family): Stage 1 (Significant force miscalibration) → Stage 6 (Functional force calibration across contexts) | Timeline: 24 weeks

Act V — Connect
You Don't Have to Navigate This Alone. 70 Countries. Millions of Families.
📱 WhatsApp Community — Force Modulation Circle
Connect with parents whose children are navigating the same proprioceptive challenges. Share what's working. Ask what isn't. Real conversations, real strategies, real empathy from families who understand exactly where you are right now.
💬 Pinnacle Online Forum — Domain A: Sensory Processing
Active threads, OT Q&A, parent-to-parent advice, and weekly live sessions with Pinnacle OTs. Join a conversation or start one — your question is someone else's answer waiting to happen.
🤝 Peer Mentoring Program
Connect with a Pinnacle parent who has navigated force modulation with their child and emerged on the other side. Real stories. Real strategies. Real support — not clinical advice, but lived experience from someone who has walked this exact road.
📍 Local Parent Meetup
Pinnacle hosts monthly in-person parent gatherings in 70+ cities across India. Find your nearest group. There is something profoundly different about sitting in a room with other parents who truly understand — no explaining required.
Preview of 9 materials that help with force modulation Therapy Material
Below is a visual preview of 9 materials that help with force modulation therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.





Link copied!
Act VI — FAQ
Your Questions. Answered by the Consortium.
How do I know if this is force modulation — or aggression?
Force modulation difficulty and aggression have one critical difference: surprise. Children with force modulation difficulties are genuinely surprised when things break or people say "ow." They do not feel the force they're using. Aggressive behavior is intentional and purposeful. If your child is consistently surprised by force consequences — this is proprioceptive, not behavioral.
How long before I see real improvement?
Early awareness signs emerge in weeks 2–4. Functional improvement (consistent force calibration in daily activities) typically takes 8–16 weeks of consistent intervention. Social improvement (peers noticing) often takes 12–24 weeks. Proprioceptive change is gradual — not linear, but real.
Can I do this without a formal OT assessment first?
You can begin home-based heavy work and sensory diet activities immediately — they are safe and beneficial for virtually all children. However, for therapeutic precision (correct material intensity, correct sequence, monitoring for contraindications), a formal OT assessment is strongly recommended. Call 9100 181 181 for a free guidance call.
My child also avoids touch — can A-097 and A-098 be done together?
Yes, with care. Establish heavy work and proprioceptive loading (A-097 Phase A) first, as this is calming and organizing, before introducing tactile-specific materials for A-098. Do NOT force both material types simultaneously in the same session.
My child uses too much force AND sometimes too little — is that normal?
Yes — this is poor force discrimination rather than pure under-responsivity. The child cannot accurately feel force gradations in either direction. The same approach applies, but external feedback tools (biofeedback, carbonless paper) become particularly important to provide the discrimination signal the system isn't producing.
How much heavy work is too much?
For most children, 30–60 minutes of distributed heavy work throughout the day is beneficial and safe. Regular, scheduled, and distributed is better than one intense burst. Signs of too much: significant fatigue, increased dysregulation 30+ minutes after heavy work, or joint pain complaints.
Should compression clothing be worn all day at school?
Most OTs recommend starting with 1–2 hours during the most challenging periods (writing time, recess) rather than all day. The nervous system habituates to constant input — strategic use is more effective than constant use. Consult your OT for a school-specific wearing schedule.
Is there a connection between force modulation and autism specifically?
Force modulation difficulties appear in up to 80% of children with ASD because proprioceptive processing differences are a core feature of sensory processing in autism. However, force modulation difficulty also appears in DCD, ADHD, hypermobility, and as a standalone sensory processing challenge. The therapeutic approach is the same regardless of diagnostic category.