
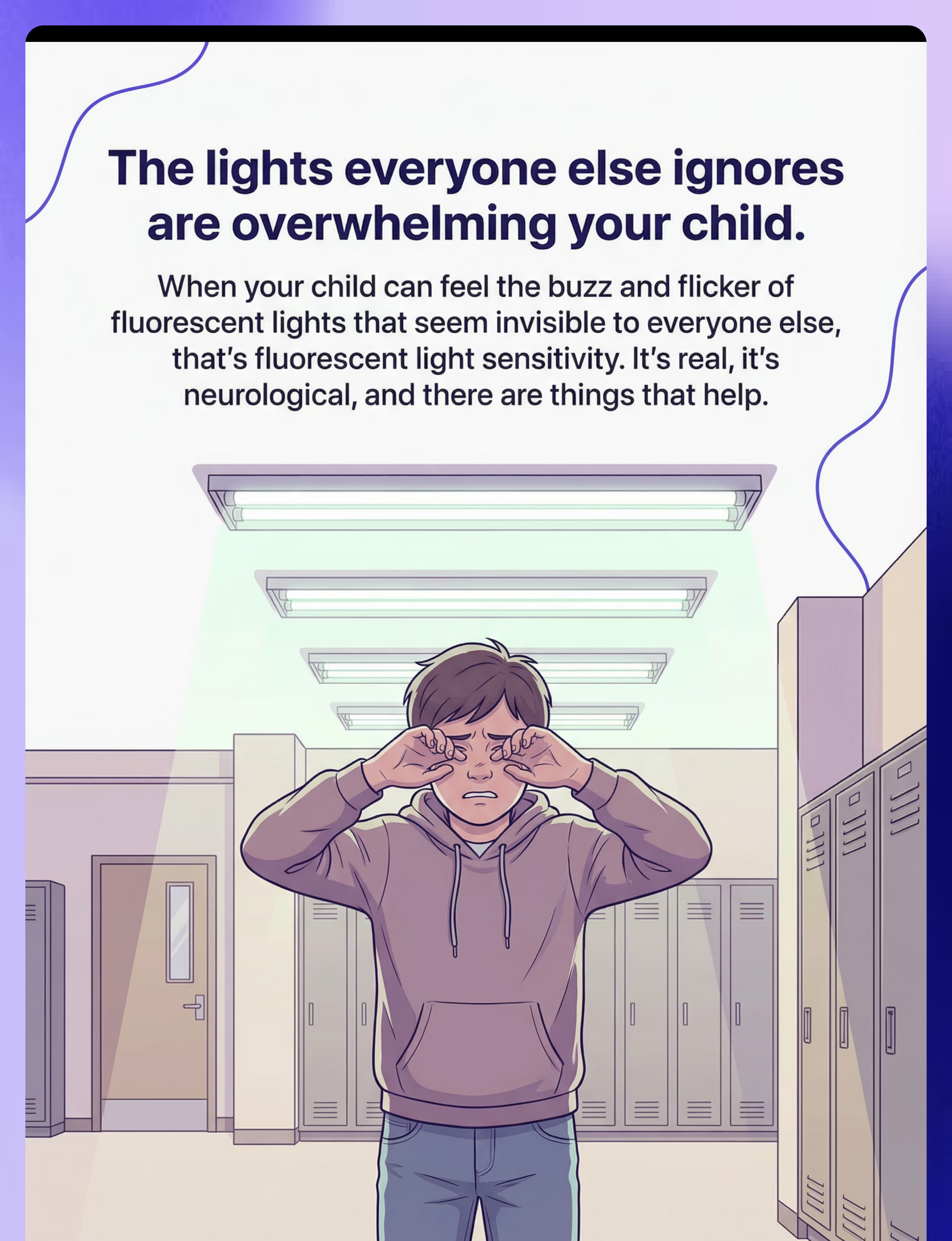
"The Lights Everyone Else Ignores Are Overwhelming Your Child."
When your child melts down in stores, can't focus at school, and covers their eyes in places that seem perfectly normal to everyone else — it's not behaviour. It's the lights.
Sensory Solutions Series — Episode A-059
Ages 3–12
Visual Processing + Light Sensitivity

"My son has always hated certain stores. He'd walk in, and within minutes he'd be covering his eyes, getting agitated, having what looked like tantrums but were actually meltdowns. For years I thought he was just being difficult about shopping — refusing to cooperate, making excuses not to run errands with me. Then I started paying attention to what these places had in common. Big box stores. His school. The doctor's office waiting room. The library. It wasn't the crowds, though those don't help. It wasn't the noise. It was the lights. Those long fluorescent tubes in the ceiling, the flat industrial fixtures, the buzzing glow that's everywhere in institutional spaces. He can feel something in those lights that I can't even perceive. He says they 'buzz' even when I can't hear anything. He says they 'flicker' even when they look perfectly steady to me. He says the light feels 'sharp' and 'wrong' in a way he can't fully explain but clearly experiences. Under fluorescent lights, he can't focus. He can't think clearly. He gets headaches within 20–30 minutes. He becomes irritable, then agitated, then explosive. His classroom has them — rows and rows of fluorescent tubes. The cafeteria has them. The gym has them. The hallways have them. He spends his entire school day under lights that are actively distressing him, draining his coping resources, and creating a constant low-level sensory assault — and then everyone wonders why he has behaviour problems by afternoon. At home, with our warm incandescent bulbs and lamps instead of overheads, he's a completely different child. Calm, focused, pleasant. It's not his behaviour — it's his environment."
— Parent Voice, Pinnacle Blooms Network. What actually helps when you can't escape fluorescent lighting? This guide answers that question — for every family, in every setting.
This Is More Common Than You Think.
Fluorescent light sensitivity is a recognised form of visual sensory over-responsivity. Your child is not being dramatic. They are not making it up. Their nervous system genuinely perceives characteristics of fluorescent light that most people filter out automatically. The same child who melts down at school may be perfectly regulated at home — the difference is often the lighting environment.
1 in 6
Children Affected
Children with autism experience clinically significant light sensitivity (visual sensory over-responsivity studies)
100–120Hz
Flicker Rate
The flicker rate of fluorescent lights. Most people can't perceive it. Some children's visual systems cannot filter it out.
70–90%
Classrooms
Of school classrooms in India and globally use fluorescent lighting as primary illumination
Up to 85%
Autistic Individuals
Report some form of sensory processing difference, with visual sensitivity among the most common (AOTA)
"If your child behaves differently in different environments, and the environments have different lighting — the lighting may be the variable that explains everything."
What's Actually Happening in Your Child's Brain
The Science
Fluorescent lights produce light in pulses — turning on and off 100–120 times per second. Most visual processing systems integrate these pulses into perceived steady light. But some children's brains — particularly those with autism, sensory processing differences, or migraine conditions — cannot filter out this flicker.
Additionally, fluorescent lights produce a discontinuous, spiky light spectrum rather than the smooth, continuous spectrum of sunlight. This spectral difference is perceived as harsher, sharper, and more uncomfortable by sensitive visual systems.
What This Means for Your Child
- They may literally SEE the lights flickering, even when they look steady to you
- They may HEAR the electrical buzz of the ballasts that you cannot detect
- The light quality feels genuinely "sharp," "wrong," or painful — not figuratively, but neurologically
- The distress builds cumulatively: tolerable for 10 minutes, uncomfortable at 30, unbearable by the afternoon
- This is a WIRING difference — not a behaviour choice, not an attitude problem, not an excuse
Key Insight: "This is a wiring difference, not a behaviour choice. The visual cortex is over-amplifying characteristics of fluorescent light that neurotypical brains automatically filter. The child's experience is as real as yours — just different." — Frontiers in Integrative Neuroscience (2020), DOI: 10.3389/fnint.2020.556660

Where Fluorescent Light Sensitivity Fits in Your Child's Development
Understanding when sensitivity typically emerges — and how it evolves — helps caregivers anticipate challenges and plan appropriate support at each stage.
Age 0–2
Sensory systems developing. Early light preferences may emerge. Infants may turn away from bright or flickering sources.
Age 2–4 ⟶ Sensitivity Becomes Noticeable
As children enter daycare, preschool, and public spaces with fluorescent lighting, behavioural patterns emerge — meltdowns in stores, difficulty in institutional settings, preference for home environments.
Age 4–7 ⟶ School Impact Peak
Full-day exposure to classroom fluorescents creates cumulative load. "Afternoon meltdown" pattern emerges. Behaviour problems attributed to the child rather than the environment.
Age 7–12 ⟶ Self-Awareness Develops
Children begin to verbalise what bothers them: "the lights buzz," "it hurts my eyes," "the light feels wrong." With appropriate supports, self-advocacy skills develop.
What Commonly Co-Occurs: Auditory sensitivity, general sensory processing differences, migraine conditions, visual processing challenges, and attention difficulties that worsen specifically under fluorescent lighting.
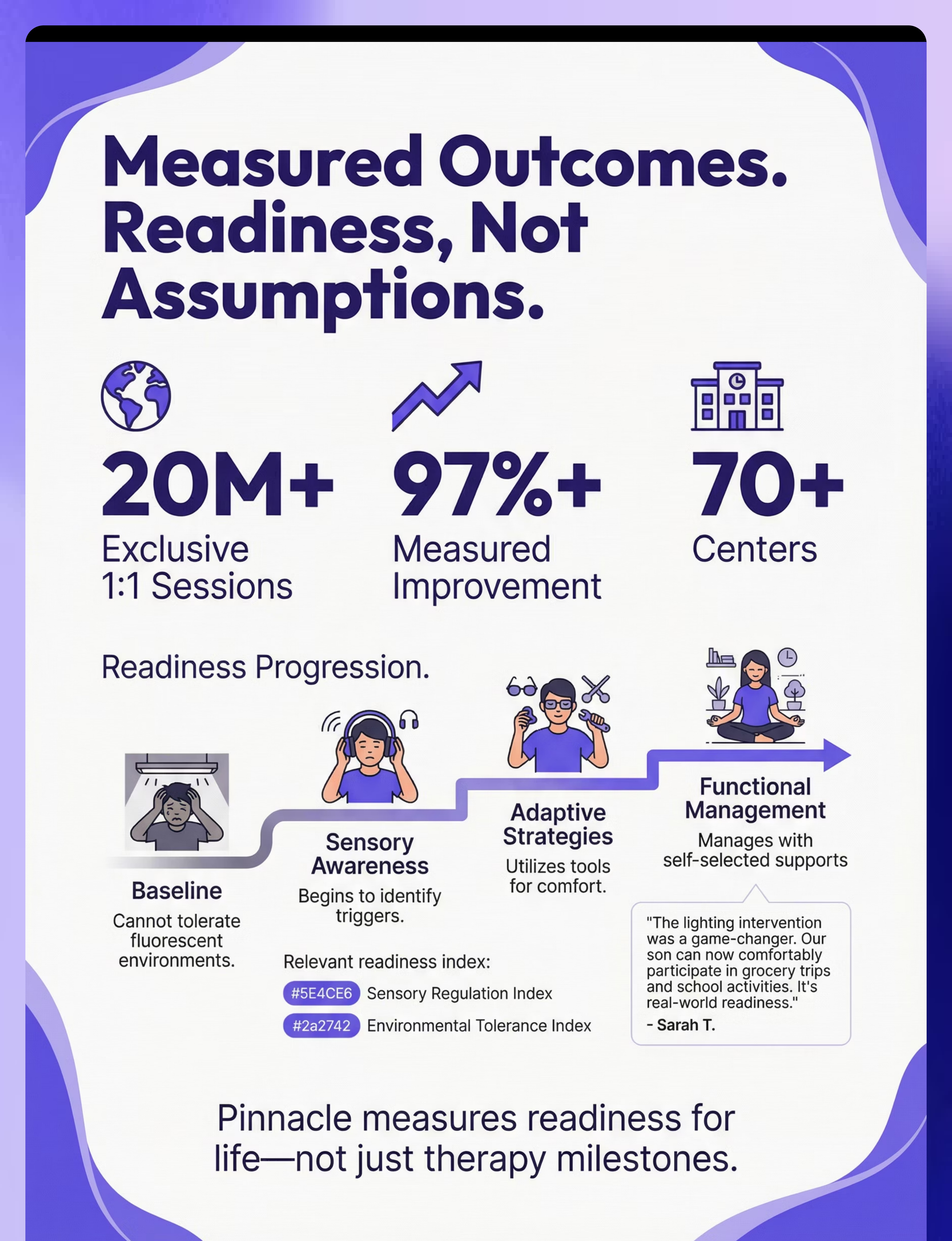
Your Child's Journey: From "cannot tolerate fluorescent environments" → to "manages with supports" → to "self-advocates and independently applies strategies." — WHO Care for Child Development Package, PMC9978394

The Evidence Supporting Environmental Light Intervention
This is not an experimental approach. Sensory integration and environmental modification for children with autism is supported by systematic reviews, meta-analyses, and clinical consensus from multiple independent research bodies.
PRISMA Systematic Review (Children, 2024)
16 articles from 2013–2023 confirm sensory integration intervention meets criteria to be considered evidence-based practice for children with ASD. Environmental modification is a core component. Ref: PMC11506176
Meta-Analysis (World J Clin Cases, 2024)
Sensory integration therapy across 24 studies effectively promoted adaptive behaviour, sensory processing, and functional skills. Individual treatment sessions were most effective. Ref: PMC10955541
FL-41 Lens Research
Studies demonstrate FL-41 tinted lenses reduce photophobia, light-triggered headaches, and visual discomfort in sensitive populations including children with autism and migraine.
Indian RCT (Indian J Pediatr, 2019)
Home-based sensory interventions demonstrated significant outcomes in Indian paediatric populations, establishing feasibility and safety of parent-administered environmental modifications. Ref: DOI: 10.1007/s12098-018-2747-4
Evidence Grade: Level II–III — Supported by systematic reviews, clinical consensus, and individual studies. "Clinically validated. Home-applicable. Parent-proven."

ACT II: THE KNOWLEDGE TRANSFER
Environmental Light Management for Fluorescent Light Sensitivity
Parent-Friendly Name: "Changing the Light, Not the Child"
Environmental Light Management is a multi-layered intervention approach that addresses fluorescent light sensitivity through a combination of personal protective tools (tinted glasses, hats), environmental modifications (light covers, alternative lighting), behavioural strategies (strategic positioning, scheduled breaks), and systemic advocacy (documentation, accommodation requests).
Rather than expecting the child to "get used to" lighting that their neurological system finds genuinely distressing, this approach modifies the environment and equips the child with tools to manage unavoidable exposure. It draws from Occupational Therapy sensory processing frameworks, Applied Behaviour Analysis environmental manipulation principles, and WHO/UNICEF nurturing care models.
Domain
Sensory Processing / Visual Processing (Domain A)
Age Range
3–12 years
Setting
School + Home + Public Spaces
Frequency
Daily environmental management + as-needed acute support
Duration
Ongoing — environmental management is continuous, not session-based

This Technique Crosses Therapy Boundaries
Light sensitivity is not siloed within a single professional domain. Its impact spans behaviour, sensory regulation, learning, and neurology — which is why the Pinnacle consortium approach involves multiple disciplines working in concert.
Occupational Therapist (OT) — Primary Lead
Evaluates sensory processing profile, identifies specific light sensitivity characteristics (flicker vs. brightness vs. spectral), recommends appropriate filters and environmental modifications, develops sensory diet incorporating light management, conducts school consultation for accommodation planning.
BCBA / ABA Analyst
Conducts functional analysis of behaviour patterns across environments with different lighting. Documents behavioural contrast between fluorescent and non-fluorescent settings. Develops data-driven accommodation requests and creates behavioural monitoring protocols to track intervention effectiveness.
Special Educator (SpEd)
Implements classroom modifications — seating arrangements, light cover installation, break schedules. Integrates lighting accommodations into IEP/individual plans. Monitors academic performance changes correlated with environmental modifications.
NeuroDevelopmental Paediatrician
Rules out underlying visual or neurological conditions. Provides medical documentation supporting accommodation requests. Evaluates for comorbid migraine or photophobia conditions. Coordinates referral to developmental optometrist if indicated.
"The brain doesn't organise by therapy type. Light sensitivity impacts behaviour, sensory regulation, learning, and neurological function. That's why the Pinnacle consortium approach works — no silos." — Adapted UNICEF/WHO Nurturing Care Framework (2022): DOI: 10.1080/17549507.2022.2141327

Your Fluorescent Light Management Toolkit — 9 Materials
A complete, evidence-informed toolkit ranging from zero-cost strategies to clinical-grade tools. Every family can start today — even with no budget at all.
Tinted Glasses & Precision Lenses
Rose, amber, or FL-41 tinted glasses that filter specific wavelengths of fluorescent light. The starting point for personal protection. ₹1,000–₹15,000
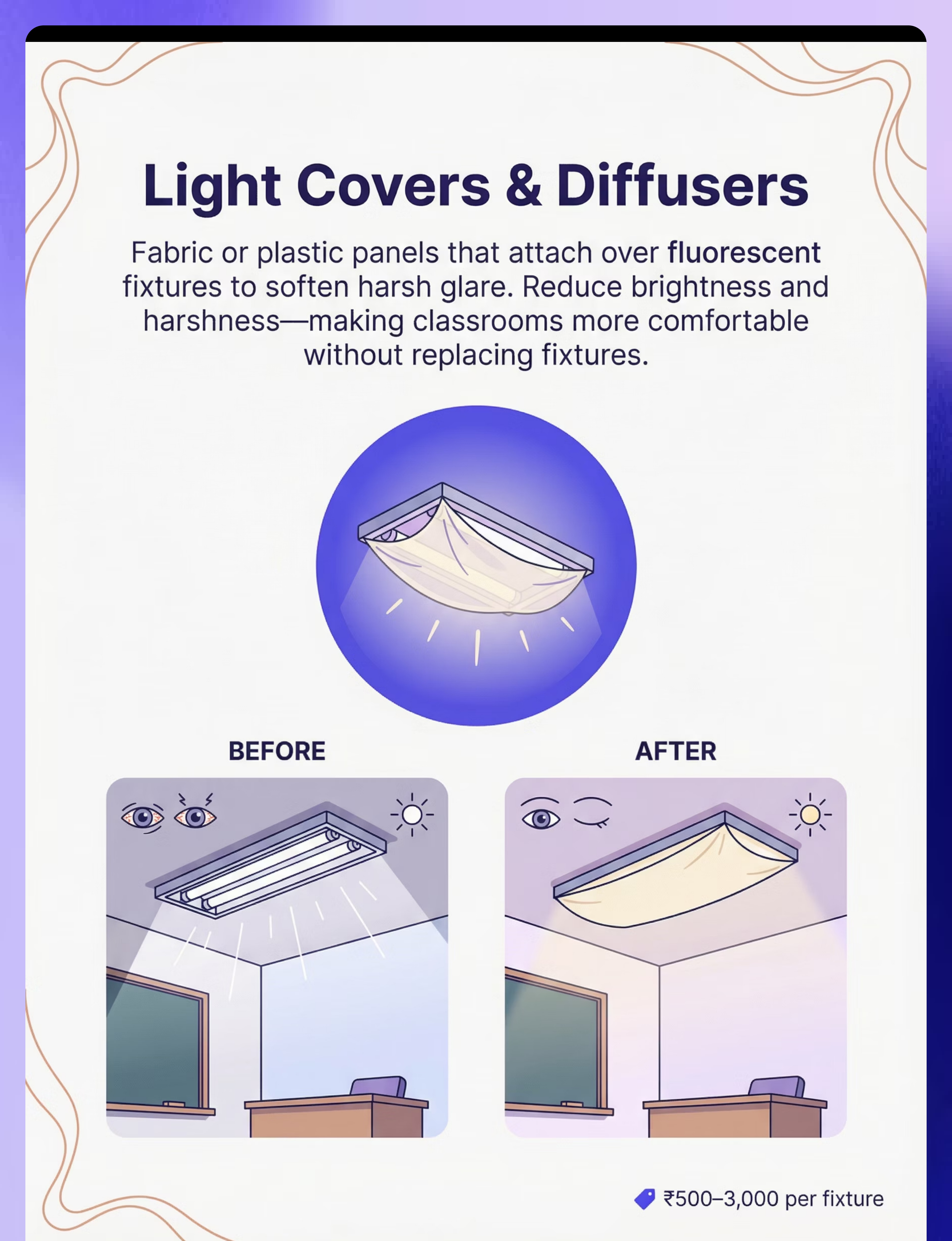
Light Covers & Diffusers
Fabric or plastic panels that attach over fluorescent fixtures to soften and diffuse harsh light. ₹500–₹3,000 per fixture
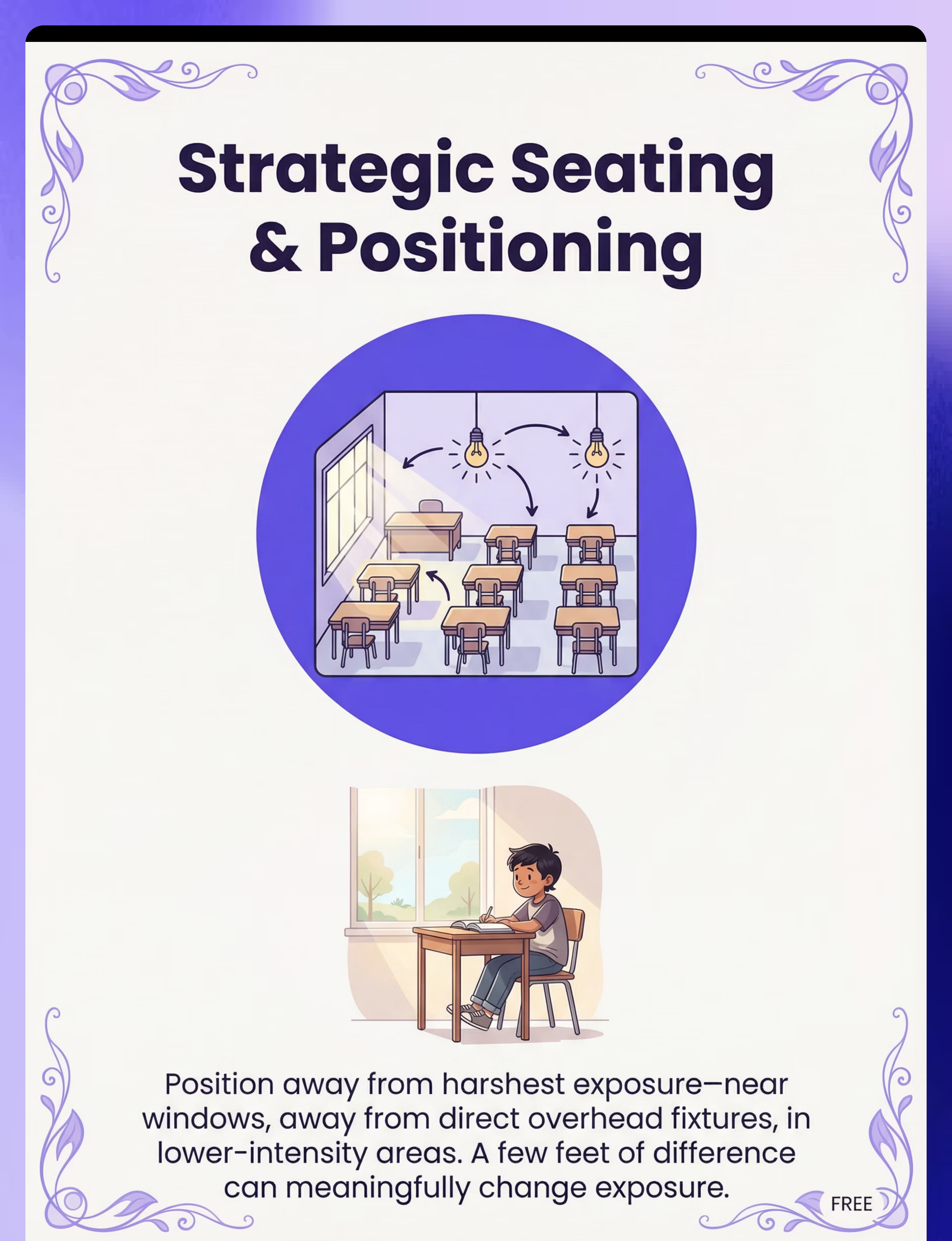
Strategic Seating Plan
Mapping optimal positions — near windows, away from direct overhead fixtures, in lower-intensity areas. FREE
Hat or Visor
Simple physical barrier to overhead fluorescent glare. Child-controlled, portable, and peer-normalised. ₹200–₹1,000
Natural Light Maximisation
Window positioning, blind management, and unnecessary fixture turn-off protocols. FREE
Alternative Lighting Sources
Quality flicker-free LED (2700–3000K), incandescent, or halogen desk/floor lamps providing warm-spectrum, continuous light. ₹500–₹5,000
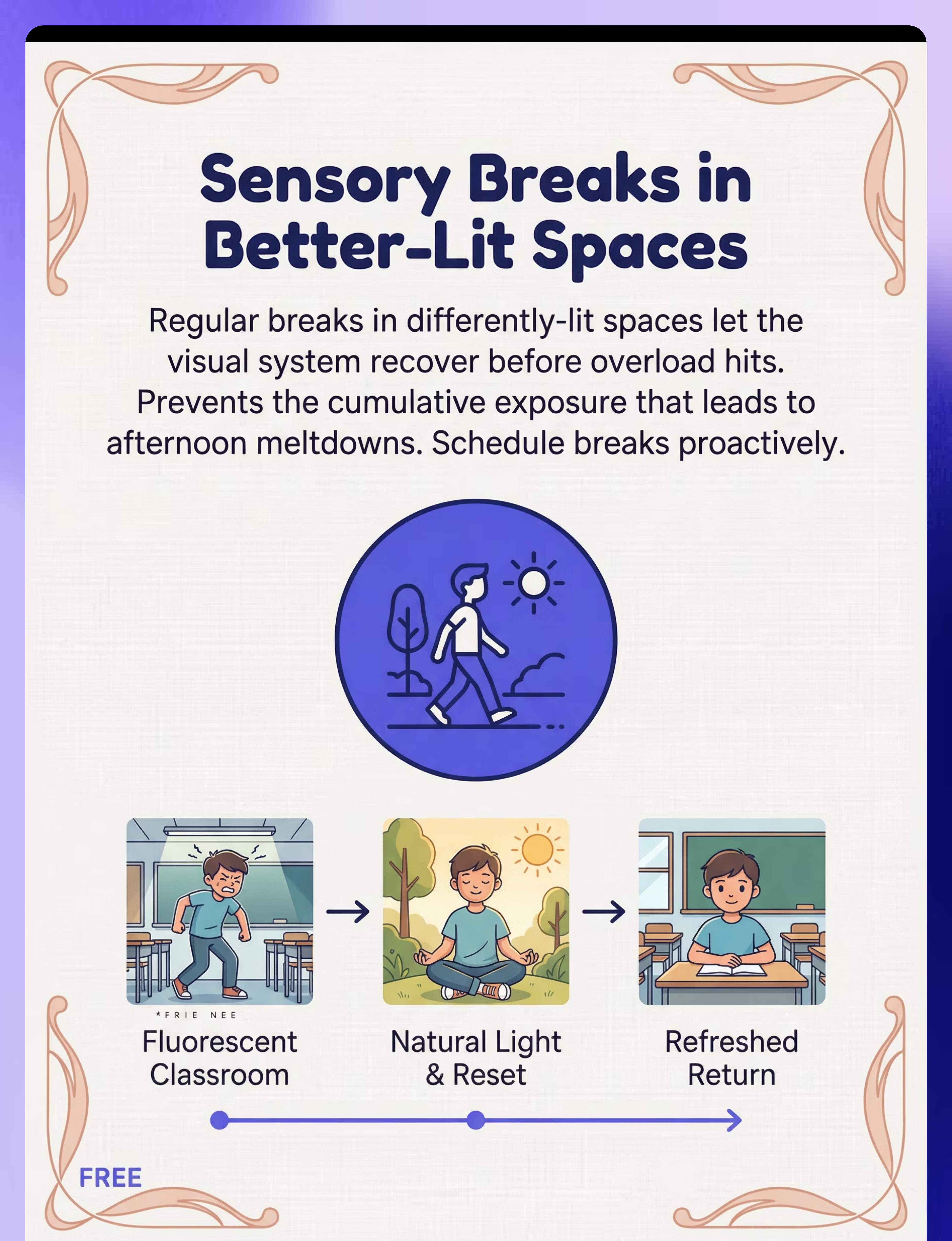
Sensory Break Schedule
Structured break protocol with identified recovery spaces — outdoor areas, differently-lit rooms, sensory corners. FREE
Portable Light Alternatives
Warm desk lamp for personal workspace, creating a comfortable light zone within a problematic environment. ₹1,000–₹5,000
Environmental Documentation & Advocacy Tools
Behaviour logs, professional evaluations, accommodation request templates, and comparison documentation. ₹0–₹2,000
Total Budget Range: ₹0 (free strategies only) to ₹15,000 (full toolkit). Essential Starters: Tinted glasses trial (₹1,000) + Strategic seating (FREE) + Breaks (FREE). Items validated through clinical use across 70+ Pinnacle centres.

Every Family Can Start Today — Zero-Cost Alternatives
Not every family can order from Amazon. Not every village has access to specialty lenses. This is the WHO/UNICEF equity principle in practice: every parent, regardless of economic status, can begin managing fluorescent light sensitivity TODAY with household items and free strategies.
Buy This | Make This / Do This | |
FL-41 Tinted Glasses (₹1,000+) | Start with any affordable tinted/coloured glasses from a local shop. Rose or amber sunglasses from a street vendor can provide an initial test of whether tinting helps before investing in clinical-grade lenses. | |
Commercial Light Covers (₹500+) | Translucent dupatta, muslin cloth, or thin cotton fabric draped carefully over fixtures. Ensure fire safety — maintain distance from bulbs. Use only with cool-running fixtures. | |
Quality LED Desk Lamp (₹1,000+) | Any table lamp with a warm incandescent or candle-type bulb. Even an appropriately covered mobile phone flashlight can provide warm focused light for brief homework sessions. | |
Formal Accommodation Letter (₹2,000) | Hand-written letter to teacher documenting specific behavioural differences in different lighting environments. Include dates, times, and observations. Even without professional letterhead, documented patterns are evidence. |
Free Strategies That Require Zero Materials
- Strategic seating near windows — just request it
- Natural light maximisation — open blinds
- Scheduled sensory breaks outdoors — build into routine
- Parent-documented behaviour comparison logs — notebook and pen
- Teaching the child to verbalise "the lights bother me" — communication practice
Important Caveat: If affordable tinted glasses help, professional evaluation for optimal prescription tint is worthwhile when resources allow. Developmental optometrists and Irlen screeners can identify the precise tint that provides maximum benefit. — WHO Nurturing Care Framework (2018), PMC9978394

Safety Considerations — Read Before Implementing
🟢 Green — Safe to Proceed
- Child has no history of seizure disorders triggered by light
- Tinted glasses allow adequate vision for safe movement and learning
- DIY light covers are fire-safe with appropriate materials maintained at distance from heat
- Hat/visor doesn't obstruct peripheral vision for safety
🟡 Amber — Proceed with Caution
- Very dark tints that significantly reduce vision may create safety hazards — start with lighter tints
- Some children are sensitive to ALL artificial light including LEDs — test alternatives before assuming they'll work
- Children with true photophobia need medical evaluation before environmental light strategies
- School accommodation requests may take time — prepare interim solutions
🔴 Red Line — Stop and Consult a Professional
- Light sensitivity suddenly appeared (was not always present) — could indicate neurological change requiring medical evaluation
- Child experiences visual aura, severe headaches with nausea/vomiting, or visual field changes — migraine or neurological evaluation needed
- Sensitivity is worsening rapidly — medical evaluation to rule out underlying conditions
- DIY light covers create any fire hazard risk — remove immediately
Environmental Requirements: Assess the specific fluorescent environments causing problems. Map light fixture locations, natural light availability, and optimal positioning in each space. Identify accessible recovery/break spaces with different lighting. — DOI: 10.1007/s12098-018-2747-4

Prepare Your Environments — The Setup That Prevents 80% of Problems
Home Environment Setup
- Audit your home lighting: Walk through every room. Identify any fluorescent or compact fluorescent (CFL) fixtures. These are the priority replacements.
- Replace fluorescents with warm alternatives: Quality LED bulbs (2700–3000K, flicker-free rated), incandescent, or halogen. Start with the homework space and bedroom.
- Create a recovery zone: The child's bedroom or a designated calm space should have ONLY warm, comfortable lighting. This is where the visual system resets after fluorescent exposure.
- Homework station lighting: Position a warm desk lamp as the primary work light. Turn off overhead fluorescents when the desk lamp is sufficient.
- Maximise natural light access: Open blinds during daytime. Position work areas near windows.
School Environment Setup
- Map the classroom: Identify all fluorescent fixture locations, window positions, and intensity variations.
- Identify optimal seat position: Near windows, away from direct overhead fixtures, in lower-intensity corners.
- Prepare accommodation documentation: Professional evaluation + behaviour comparison evidence + specific accommodation requests.
- Identify break spaces: Where can the child go for sensory recovery? Outdoor areas, differently-lit rooms, sensory corners.
Public Spaces Strategy
- Keep tinted glasses accessible — in bag, on person, ready for any fluorescent environment
- Plan store visits strategically: shorter visits, less crowded times
- Teach the child awareness: "When your eyes start feeling uncomfortable, tell me and we'll take a break."

ACT III: THE EXECUTION
Pre-Implementation Readiness Assessment
Before beginning Environmental Light Management, confirm you have the foundations in place. The best intervention starts when the environment is ready and the family is prepared.
✅ Environments Identified
You have identified which environments cause the most distress — school classroom, specific stores, medical offices, etc.
✅ Behavioural Contrast Observed and Documented
You have observed and recorded the difference in your child's behaviour between fluorescent-lit and non-fluorescent settings.
✅ Communication Baseline Established
Your child can communicate discomfort at some level — verbal, behavioural, pointing, or gestures.
✅ At Least One Tool Ready
Even if it's strategic seating — a completely free option — you have at least one tool ready to implement from Day 1.
✅ School Informed and Home Audit Complete
Teacher has been informed (even informally) about the lighting accommodation request. Home lighting audit is complete.
✅ GO
All checks passed → Proceed to implementation
⚠️ MODIFY
Some checks not ready → Start with free strategies while preparing others
🛑 POSTPONE
If light sensitivity appeared suddenly or is worsening rapidly → Medical evaluation first
Step 1: Introduce the Concept to Your Child
The Invitation
This is a conversation, not a therapy session. The goal is to validate the child's experience, name the cause, and introduce the idea of tools — without pressure. Allow 5–10 minutes and follow the child's lead.
For Ages 3–5
"I know the lights at school/store make your eyes feel bad. I have something that might help. Want to try these special glasses? They make the light feel softer."
For Ages 6–9
"You know how the lights at school bother you? That's because those lights flicker really fast — your eyes can see it even though most people can't. That's actually pretty amazing that your eyes are so sensitive. I have some tools that can help make those lights feel better. Let's try them together."
For Ages 10–12
"Your sensitivity to fluorescent lights is a real neurological thing — your visual system processes certain light frequencies differently. It's like having very sharp hearing but for light. There are specific tools and strategies that can help you manage fluorescent environments better. Let's figure out what works for you."
What Acceptance Looks Like
- Child is willing to try on tinted glasses
- Child participates in choosing seat position
- Child expresses interest in the "why" behind the sensitivity
What Resistance Looks Like — and What to Do
- Refuses to wear "weird glasses" → Let them choose the style/colour. Try a hat instead.
- Doesn't believe it will help → Start with free strategies that don't require their buy-in
- Embarrassed about looking different → "Lots of people wear glasses to help their eyes. These just have a special colour."

Step 2: Introduce Each Tool Systematically
The Engagement
Do NOT introduce all 9 materials at once. Start with ONE tool and add others progressively. Overwhelming a child with simultaneous changes reduces buy-in and makes it impossible to identify what's actually working.
Week 1: Strategic Seating
FREE, requires no child action, invisible to peers. Request seat near window / away from direct overhead fixtures. Document any behavioural change with the new position.
Week 2: Add Tinted Glasses Trial
Let child try rose, amber, or other tinted glasses at home first. Then try in a brief fluorescent exposure (quick store visit). Document: did the glasses change their comfort level?
Week 3: Add Sensory Breaks
Introduce scheduled breaks before the overload point. Identify recovery spaces (outdoor, differently-lit rooms). Practise the break request communication together.
Week 4: Add Environmental Modifications
Install light covers in classroom (if approved). Set up portable desk lamp for homework space. Begin formal accommodation documentation.
Child Response Guide: ENGAGEMENT (child asks for their glasses/requests breaks) → The tools are working. TOLERANCE (uses tools without enthusiasm) → Continue — comfort may be subtle at first. AVOIDANCE (refuses tools) → Don't force. Find THEIR tool from the 9 available options. — PMC11506176
Step 3: Active Environmental Light Management Protocol
The Therapeutic Action
This is not a single "session" — it's an ongoing environmental management protocol. The therapeutic action happens every day in every fluorescent-lit environment. It is multi-layered by design: no single strategy is sufficient on its own.
Layer 1 — Personal Protection
Tinted glasses on before entering any fluorescent environment. Hat/visor available as backup. This becomes as automatic as putting on shoes before going outside.
Layer 2 — Positioning
Sit in the optimal pre-identified position in every regular environment. Near windows. Away from direct fixtures. In lower-intensity zones.
Layer 3 — Environmental Modification
Light covers on classroom fixtures. Unnecessary fixtures turned off. Alternative lighting sources available. Natural light maximised.
Layer 4 — Exposure Management
Scheduled breaks before the cumulative overload point. The break happens BEFORE the meltdown, not after. If meltdowns typically happen after 2 hours, schedule breaks at 90 minutes.
Layer 5 — Advocacy
Formal documentation in place. School accommodations active. Teachers informed. Break protocol agreed upon. The system supports the child.
Execution Errors to Avoid
- Don't wait for a meltdown to implement strategies (reactive) — implement before exposure (proactive)
- Don't introduce all layers simultaneously — build progressively
- Don't force tinted glasses if the child hates them — try other tools
- Don't assume one strategy will solve everything — the power is in layering multiple approaches

Step 4: Build Consistency Across All Environments
Repeat & Vary
☀️ Morning (Before School)
- Glasses on before entering school building
- Remind child of their break schedule
- Confirm hat/visor is in bag as backup
🏫 School Day (Ongoing)
- Seated in optimal position
- Light covers in place on classroom fixtures
- Breaks taken at scheduled intervals
- Teacher monitors for early signs of light distress
🌇 After School (Recovery)
- Return to home environment with warm, comfortable lighting
- 15–30 minutes in recovery zone (no screens, no fluorescents)
- Outdoor time if available — natural light reset
🛒 Weekend / Public Spaces
- Glasses on for store visits
- Shorter visits planned to fluorescent environments
- Child practises requesting breaks: "My eyes need a break from the lights"
Variation Within the Protocol: Try different tinted glass colours periodically — sensitivity may change. Rotate between hat and glasses depending on environment. Gradually extend fluorescent exposure duration as tolerance builds (with supports).
Satiation Point: If the child is managing well with current strategies, don't add more. Success doesn't mean adding complexity — it means the current protocol is working. "3 consistent strategies > 10 inconsistent ones."

Step 5: Reinforce Self-Advocacy and Environmental Management
Reinforce & Celebrate
Reinforcement must be immediate (within 3 seconds), specific, and focused on the self-advocacy behaviour — not just the tolerance. The long-term goal is a child who manages their own needs, not a child who silently suffers.
Child puts on glasses independently
"Great job getting your glasses ready! You're taking care of your eyes."
Child requests a sensory break
"I'm proud of you for knowing what you need. Let's go take that break."
Child tells teacher "the lights are bothering me"
"That was brave and smart. You told someone what you needed."
Child tolerates longer fluorescent exposure than before
"You lasted the whole trip! Your strategies are working."
Reinforcement Menu
- Verbal praise — immediate, specific, not just "good job" but naming exactly what they did well
- Extra time in preferred activity
- Choice of next break activity
- Sticker/token for self-advocacy chart
- Natural consequence: "Because you used your glasses, you were comfortable for the whole shopping trip and we got everything done."

Step 6: Post-Exposure Recovery Protocol
The Cool-Down
After extended fluorescent exposure — a school day, a long shopping trip — the visual system needs recovery time. This is not optional. It is neurological recovery, as necessary as sleep after exertion.
Transition Script: "We're done with the bright lights for now. Let's go to your comfortable spot and let your eyes rest."
Signs of Adequate Recovery
- Facial tension releases
- Eye rubbing/squinting stops
- Irritability subsides
- Child re-engages with activities voluntarily
- "I feel better" or equivalent communication
If Recovery Takes Longer Than Expected
- Today may have had higher exposure than usual — note for future planning
- Review: were breaks adequate? Were glasses worn consistently?
- Consider: is the child's overall regulation state lower today (fatigue, illness, stress)?
- Adjust tomorrow's plan accordingly
60 Seconds of Data Now Saves Hours of Guessing Later
Consistent data tracking transforms guesswork into evidence — for accommodation requests, professional consultations, and refining your child's personalised protocol. Keep it simple: a tally you can complete in under a minute.
1. Fluorescent Exposure Duration
Approximate total hours in fluorescent-lit environments today
2. Tools Used
Circle: Glasses / Hat / Seating / Breaks / Light Covers / Lamp / None
3. Highest Distress Level (1–5)
1 = Comfortable | 2 = Mild, managed | 3 = Moderate, required breaks | 4 = Significant, early removal needed | 5 = Meltdown despite supports
4. Self-Advocacy Moment? (Y/N)
Did the child request a tool or break independently today?
Weekly Pattern Review (Every Sunday — 5 minutes): Average daily distress level trending down? Which tools used most and seem most effective? Any pattern to worst days? Self-advocacy frequency increasing?
"This data is your evidence. It drives accommodation requests, professional consultations, and your child's personalised protocol." — BACB Guidelines for behavioural data collection | Cooper, Heron & Heward, Applied Behaviour Analysis (8th ed.)
Troubleshooting — When Strategies Aren't Working
"Session abandonment is not failure — it's data. Every attempt teaches you something about your child's needs."
Problem: Child refuses to wear tinted glasses
Why: Self-consciousness, discomfort, sensory issue with frames on face, or doesn't believe it helps. What to do: Let them choose the style/colour. Try clip-on tints for existing glasses. Try a hat/visor instead. Let them observe the difference: "Try 5 minutes with, 5 minutes without — you tell me which feels better." Some children won't wear glasses but will accept every other strategy.
Problem: School won't install light covers or change seating
Why: Schools may not understand light sensitivity or may cite policies. What to do: Provide formal documentation from OT or physician. Present specific, feasible requests — not "change all the lights" but "may my child sit by the window and wear a hat." Escalate through formal accommodation channels. Contact Pinnacle for school consultation support.
Problem: Strategies help but child still struggles by afternoon
Why: Cumulative exposure exceeds tolerance even with supports. What to do: Add more frequent breaks earlier in the day. Layer additional strategies. Investigate whether specific activities (gym, cafeteria) have worse lighting. Consider discussing a modified schedule if needed.
Problem: Fine some days, melts down other days with same setup
Why: Sensory tolerance varies with overall state — fatigue, illness, stress, sleep quality all affect the threshold. What to do: Track co-factors. On low-tolerance days, implement maximum support proactively. Teach the child to recognise their own variable threshold: "Today is a hard day for your eyes — let's use extra support."
Problem: Can't afford tinted glasses or specialty items
Why: Financial constraints are real. What to do: The most effective strategies are FREE — strategic seating, natural light maximisation, breaks, and advocacy. Affordable tinted glasses (₹100–₹500 from local vendors) can provide initial testing. Prioritise documentation and accommodation requests, which create systemic solutions requiring no family cost.

Your Child Is Unique — Adapt the Protocol
No two children with fluorescent light sensitivity experience it identically. Intensity, triggers, and optimal strategies vary. Use this guide to calibrate the protocol to your child's specific profile and current capacity.
Advanced Version — Building Independence
Child self-manages tool selection and break timing. Extended fluorescent tolerance with supports. Active self-advocacy with teachers and peers. Minimal adult intervention for routine environments. Ages 10–12 lead strategy selection.
Standard Version — Moderate Sensitivity / Most Days
Strategic tool use across all regular environments. Structured break schedule every 60–90 minutes. Beginning self-advocacy — child requests tools and breaks. Mixed adult and child management. Tolerance for typical school day with supports.
Easier Version — High Sensitivity / Bad Days / Younger Children
Maximum environmental control — avoid fluorescent environments when possible. Heavy reliance on personal protection (glasses, hat). Frequent breaks every 30–45 minutes. Recovery time equal to exposure time. Adult-managed: parent handles all advocacy and tool management.
Sensory Avoider (Most Fluorescent-Sensitive Children)
Focus on filtering, reducing, and managing exposure. These children benefit most from glasses, covers, positioning, and breaks.
Sensory Seeker with Light Sensitivity (Less Common)
Focus on alternative light quality (warm, continuous spectrum) rather than light reduction. May benefit from visual sensory activities in comfortable lighting.

ACT IV: THE PROGRESS ARC
The First Two Weeks — Your Baseline Is Shifting
25%
Progress Milestone
Weeks 1–2 represent your first quarter of the progress arc — the baseline is actively shifting
If Tinted Glasses Help
The child may show immediate relief in fluorescent environments. Some children have a dramatic, visible response — relaxation, reduced squinting, improved focus. Others show subtle improvement that's easier to see in the data than in the moment.
Strategic Seating Impact
May produce the first behavioural data contrast: same classroom, different seat, different behaviour pattern. This is powerful early evidence for your accommodation documentation.
First Scheduled Breaks
May feel disruptive initially but prevent late-day meltdowns. The child may begin commenting on light differences they notice: "This room is better" or "I can see better now."
Early Self-Management Signals
You may notice the child reaching for their glasses or hat independently — this is early self-management emerging. Celebrate it immediately and specifically.
Parent Milestone: "You may notice that YOU start seeing fluorescent lights differently — noticing them in stores, offices, schools. You're developing awareness of what your child experiences." Data Point: Baseline distress level in Week 1 vs. distress level with initial strategies in Week 2. Any reduction confirms the approach is correct.

Weeks Three and Four — The Strategies Are Becoming Routine
50%
Consolidation Phase
Weeks 3–4 mark the halfway point — strategies are transitioning from deliberate effort to habitual action
At this stage, the most meaningful shift isn't dramatic behavioural change — it's the quiet normalisation of the tools. Strategy use is becoming habit.
Tool Use Becomes Habitual
Glasses on automatically before fluorescent environments. Break requests become self-initiated rather than parent-prompted.
Behavioural Contrast Becomes Clear
Supported vs. unsupported fluorescent exposure shows measurable difference in your data. School may begin reporting behavioural improvement — especially afternoon behaviour.
Language Develops
The child can explain their sensitivity: "Fluorescent lights flicker and it hurts my eyes." This verbal self-understanding is a significant developmental milestone.
Support Network Expands
Other teachers or caregivers may notice the strategies working and begin supporting them — expanding the child's protective environment beyond the immediate family.
Neural Pathway Formation: Repeated strategy use builds habitual response patterns. The brain is learning: fluorescent environment → deploy tool → manage successfully. This becomes automatic over time.
Mastery Phase — Your Child Is Managing Their Own Environment
75%
Mastery Milestone
Weeks 5–8 — the mastery badge unlocks when criteria below are consistently met
Mastery Criteria — Specific, Observable, Measurable
- ✅ Child independently uses at least 2 strategies across multiple environments
- ✅ Self-advocates for accommodations with adults (requests break, asks to move seat)
- ✅ Tolerates full school day in fluorescent classroom with supports in place
- ✅ Average distress level consistently at 1–2 compared to baseline
- ✅ Light-triggered meltdown frequency reduced by more than 50% from baseline
- ✅ Can identify and articulate triggers and tools: "I use my glasses because fluorescent lights flicker and it bothers my eyes"
- ✅ Functions in at least one previously-avoided public space (grocery store, library) with strategies
Mastery criteria met for 2+ consecutive weeks
→ Consider reducing support level to build independence
Mastery in some environments but not others
→ Focus on the challenging environments specifically
Mastery criteria not met by Week 8
→ Consider professional OT evaluation for additional support strategies
You Did This. Your Child Grew Because of Your Commitment.
Your child walked into school today wearing their glasses, sat in their window seat, took their scheduled break before the meltdown point, and came home regulated. Six weeks ago, that same school building was a sensory battleground. The lights that haven't changed are now manageable — because the approach has changed.
You did this. You observed. You documented. You advocated. You implemented. You adjusted when things didn't work. You celebrated the small wins. Your child is learning that they can manage challenging environments — not by suffering through them, but by understanding their neurology and deploying the right tools. That is a life skill that will serve them far beyond childhood.
"Document this milestone in your child's progress journal. Date it. Note which strategies made the difference. This becomes part of their story — not a story of disability, but a story of understanding and empowerment."
Family Celebration Suggestion: Take a family photo in a place that was previously avoided — the grocery store, the mall, the library. Let your child see themselves comfortable in a space that was once a source of distress. That photo is evidence of growth.
When to Pause and Seek Professional Guidance
🚩 Sensitivity Worsening Despite Strategies
If distress is increasing over time rather than decreasing or stabilising, this may indicate a changing condition requiring medical evaluation — not simply a protocol adjustment.
🚩 New Visual Symptoms Appear
Visual aura (spots, zigzag lines, tunnel vision), sudden visual field changes, or persistent visual disturbances beyond normal fluorescent sensitivity. These warrant prompt ophthalmological or neurological review.
🚩 Severe Headaches with Nausea or Vomiting
May indicate a migraine condition requiring specific medical management beyond environmental strategies. Do not manage with environmental tools alone.
🚩 Sensitivity Extends to ALL Light Sources
Broader photophobia including natural sunlight may require ophthalmological evaluation to rule out eye conditions beyond fluorescent sensitivity.
🚩 Behavioural Deterioration Despite Full Implementation
If all strategies are correctly in place but behaviour is worsening, other factors may be at play — consult the Pinnacle team for professional re-evaluation.
Your Child's Visual Sensory Journey — Where You Are and Where You're Going
Long-Term Developmental Goal: Independent environmental management — a child/adolescent/adult who understands their visual processing differences, carries appropriate tools, self-advocates for accommodations, and functions comfortably across diverse environments.

Explore Related Intervention Techniques
Same Cluster — Visual Sensory Challenges
- A-057: Sensitivity to Bright Light
- A-058: Visual Overstimulation in Busy Environments
- A-060: Screen Light Sensitivity
- A-061: Difficulty with Visual Transitions
Cross-Domain Related Techniques
- Auditory Sensitivity techniques (many children with light sensitivity also have sound sensitivity)
- General Sensory Regulation techniques
- Classroom Accommodation strategies
- Self-Advocacy skill building
Parent Support Resources
- K-980: Understanding Light Sensitivity
- K-985: Advocating for Lighting Accommodations at School
- K-990: Creating a Sensory-Friendly Home

This Technique Within the Full Developmental Landscape
Fluorescent Light Distress management sits within Domain A: Sensory Processing, specifically the Visual Processing sub-domain. But its impact ripples far beyond a single domain — visual comfort is foundational to almost everything a child does.
"Every technique is a thread in the larger tapestry of your child's development. Pulling this thread strengthens the entire fabric."
ACT V: THE COMMUNITY & ECOSYSTEM
From a Parent Who Walked This Path
"For years I didn't connect his afternoon meltdowns at school with the lighting. He was 'fine' in the morning — teachers said he was cooperative, engaged, focused. By 2pm he was a different child. Irritable, couldn't focus, would melt down during transitions. Our OT at Pinnacle asked about the lighting in his classroom. I hadn't even thought about it. She had us observe: all fluorescent tubes, blinds closed, no natural light. She suggested we try FL-41 glasses, request a seat by the window, and ask for scheduled outdoor breaks. Within two weeks, the afternoon meltdowns stopped. Not reduced — stopped. Same child, same classroom, same teacher, same curriculum. The only change was the lighting experience. His glasses filter the worst of the fluorescent light, his window seat gives him natural light supplement, and his outdoor break at 11am resets his visual system before the cumulative overload hits. Now he's in 4th grade. He puts his glasses on independently every morning, knows to ask for breaks when he needs them, and can explain to anyone why: 'Fluorescent lights flicker and my eyes can see it. These glasses help.' He went from 'behaviour problem child' to 'the kid who knows exactly what he needs.' That's not a small thing."
— Parent, Pinnacle Blooms Network. Note: Illustrative case; outcomes vary by child profile. Individual assessment recommended.
You Are Not Doing This Alone
Thousands of families across India are navigating exactly what you're navigating. The Pinnacle parent community is where strategies get refined — what works for one family may be the breakthrough for another. Connect, share, and grow together.
Parent Community
Join the Pinnacle Parent Community on WhatsApp/Telegram. Connect with parents managing light sensitivity in the Sensory Solutions group. Share wins, ask questions, get real-time peer support.
Social Media & Video
Follow @pinnacleblooms on Instagram for daily technique tips. Subscribe to Pinnacle's YouTube channel for video demonstrations of every technique in this series.
FREE National Autism Helpline
9100 181 181 — Available in 16+ languages, 24×7. For guidance, troubleshooting, referrals, and AbilityScore® assessments. Email: care@pinnacleblooms.org
When You Need Professional Support
Some children need more than home strategies and environmental modifications — especially when the sensory profile is complex, when accommodations require formal documentation, or when medical conditions are co-occurring.
Occupational Therapist
Comprehensive sensory processing evaluation, sensory diet development, school accommodation planning. The OT is your primary professional for light sensitivity management. Start here.
Developmental Optometrist
Visual processing evaluation, precision tinted lens prescription, ruling out visual conditions. Some children benefit from Irlen screening for custom tint selection.
NeuroDevelopmental Paediatrician
If migraines are suspected, sensitivity is worsening, or underlying neurological factors need evaluation. Provides medical documentation for accommodation requests.
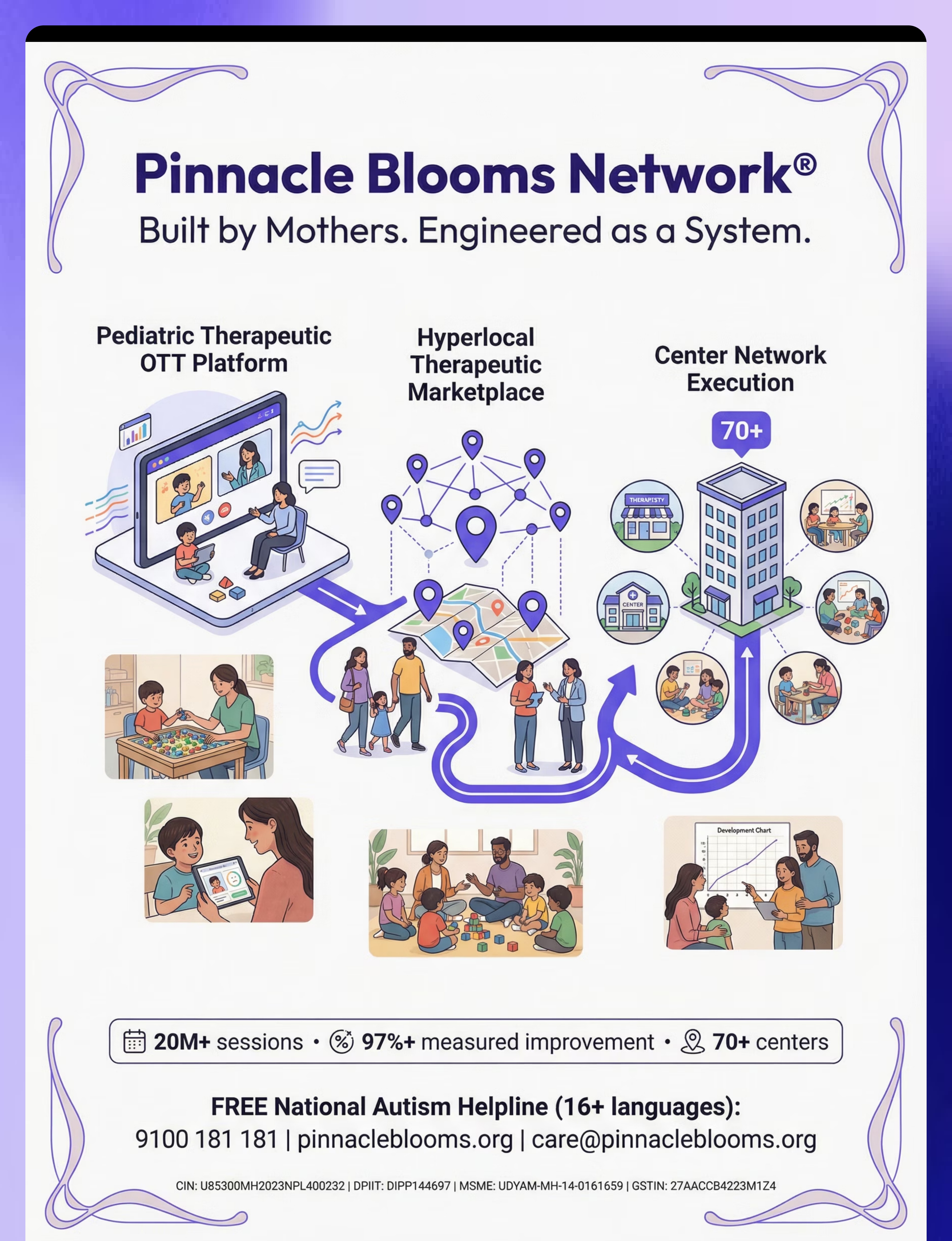
Pinnacle Centres Available Across: Andhra Pradesh, Telangana, Karnataka, Tamil Nadu, Maharashtra, and expanding nationally. 70+ centres. 20M+ therapy sessions delivered.
Deeper Reading for the Curious Parent
Every recommendation in this guide is grounded in peer-reviewed evidence. Below is the research library for parents, therapists, and programme leads who want to go deeper.
PRISMA Systematic Review (Children, 2024)
"Sensory integration intervention meets criteria to be considered evidence-based practice for children with ASD" — 16 articles, 2013–2023. Ref: PMC11506176
Meta-Analysis (World J Clin Cases, 2024)
Sensory integration therapy across 24 studies effectively promoted social skills, adaptive behaviour, sensory processing, and motor skills. Ref: PMC10955541
Indian RCT (Indian J Pediatr, 2019)
Home-based sensory interventions demonstrated significant outcomes in Indian paediatric populations. Ref: DOI: 10.1007/s12098-018-2747-4
WHO Care for Child Development (CCD) Package
Age-specific evidence-based recommendations. Implemented in 54 LMICs. Ref: PMC9978394 | WHO/UNICEF CCD Package (2023)
Frontiers in Integrative Neuroscience (2020)
Comprehensive framework for evaluating sensory integration/sensory processing treatment in ASD. Ref: DOI: 10.3389/fnint.2020.556660
NCAEP Evidence-Based Practices Report (2020)
Classification of visual supports and environmental modification as evidence-based practices for autism. FL-41 lens research also demonstrating benefit for photophobia, migraine, and light sensitivity conditions.
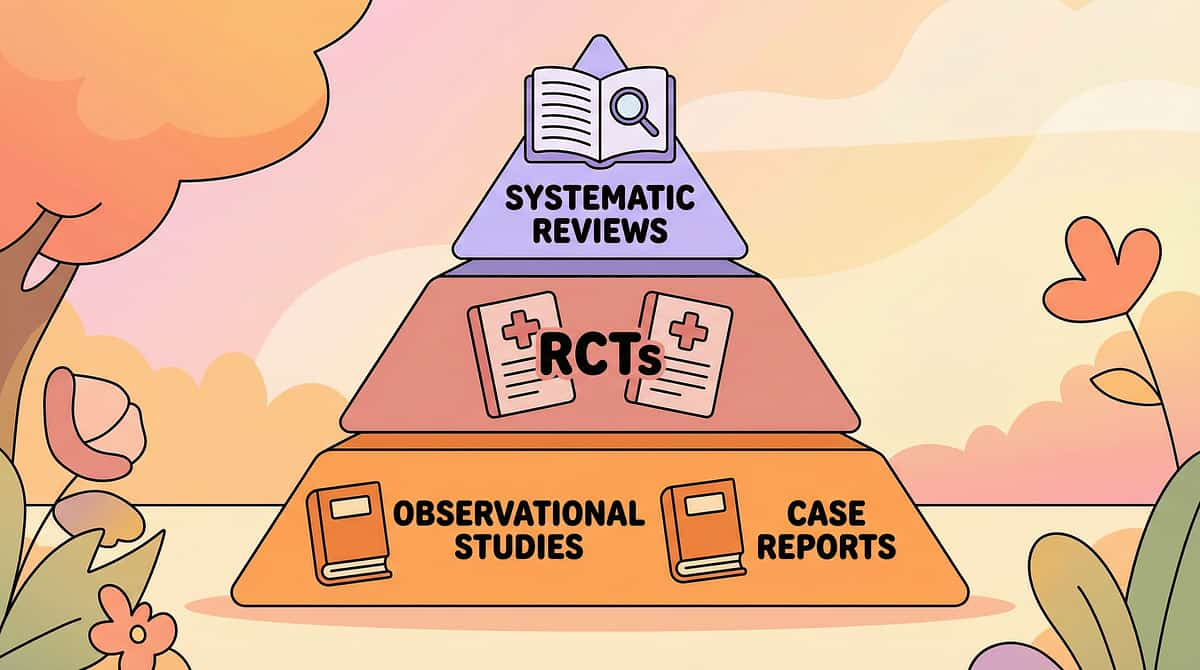
Evidence Pyramid: Systematic Reviews + Meta-Analyses → RCTs → Clinical Consensus → Case Studies. "Evidence-based means the research supports it. Parent-proven means families like yours have made it work."
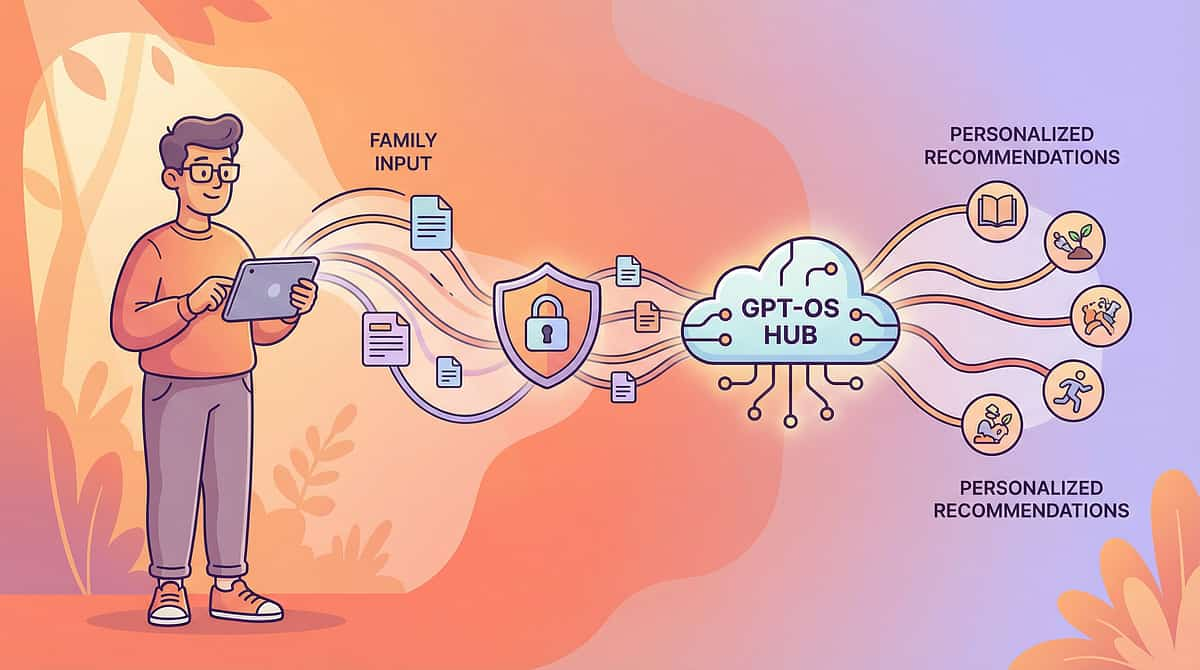
How GPT-OS® Personalises Your Child's Light Sensitivity Protocol
Your daily tracking data — distress levels, tools used, exposure duration, self-advocacy moments — feeds into the GPT-OS® Sensory Regulation Index and generates personalised recommendations specific to your child's evolving profile, not a generic template.
What GPT-OS® Generates for You
- Optimal break timing based on YOUR child's specific cumulative exposure tolerance
- Tool effectiveness ranking — which strategies are making the biggest difference
- Environmental priority mapping — which spaces need the most attention
- Alert triggers — when patterns suggest the need for professional re-evaluation
Your Data Helps Every Child Like Yours
When your tracking shows that FL-41 glasses reduced distress from Level 4 to Level 2 in a 7-year-old with a specific sensory profile — that data point helps GPT-OS® recommend FL-41 glasses sooner for the next family with a similar profile. Privacy is protected under Pinnacle's ISO/IEC 27001 certified information security framework.
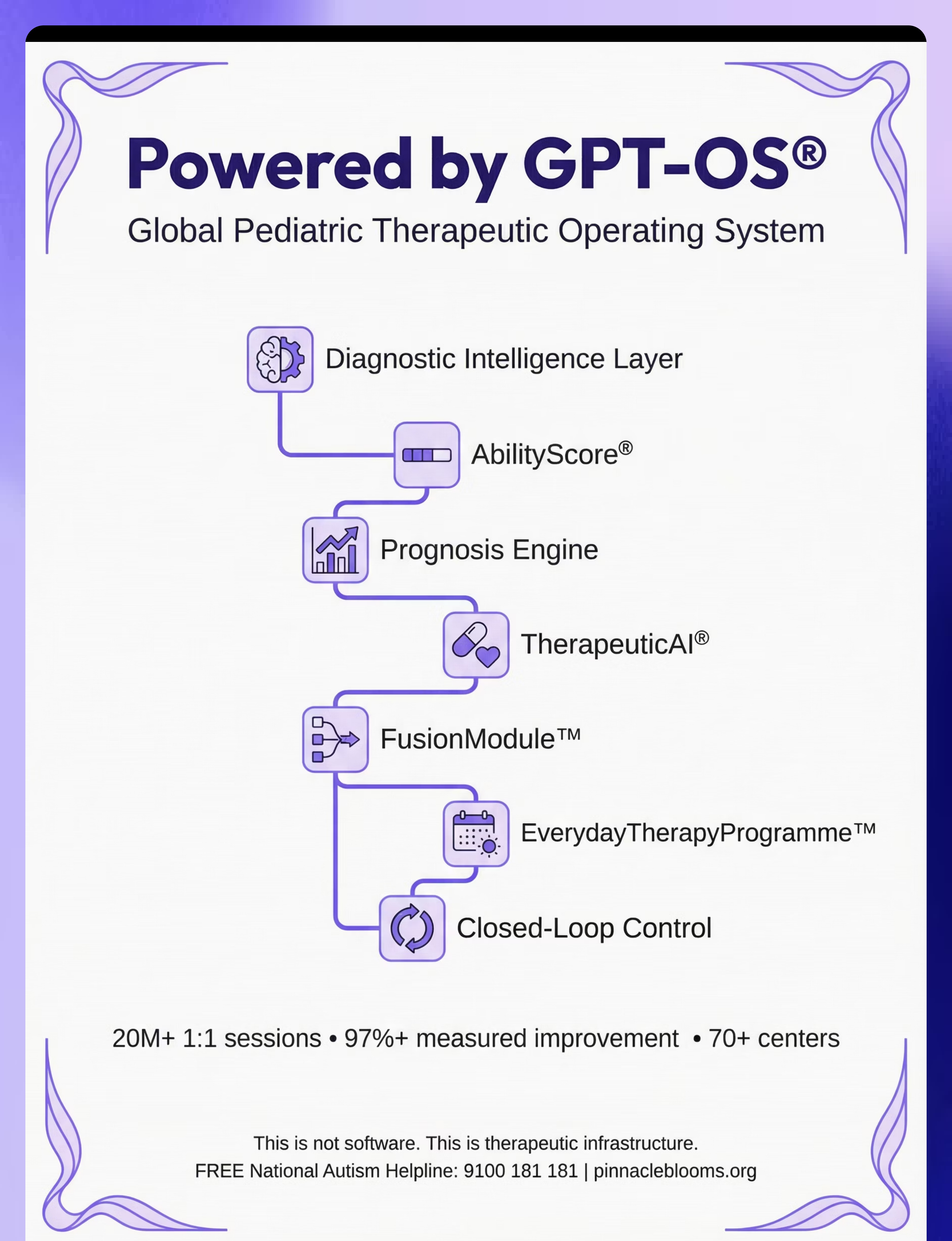
Powered by GPT-OS®: Diagnostic Intelligence Layer → AbilityScore® → Prognosis Engine → TherapeuticAI® → FusionModule™ → EverydayTherapyProgramme™ → Closed-Loop Control. 20M+ 1:1 sessions • 97%+ measured improvement • 70+ centres • Patents filed across 160+ countries. "This is not software. This is therapeutic infrastructure."

Watch the Reel: 9 Materials That Help With Fluorescent Light Distress
In 60 seconds, watch a Pinnacle therapist demonstrate each of the 9 materials — see what they look like, how they're used, and the immediate difference they make.
Reel ID: A-059 | Domain: Sensory Processing / Visual Processing | Series: Sensory Solutions Series — Episode 59
[Embed Reel A-059 video here]
This technique page is the deep-dive companion to Reel A-059. The Reel introduces the materials; this page gives you everything you need to implement them. This Reel is presented by the Pinnacle Blooms Occupational Therapy team — the same therapists who developed and validated these strategies across 70+ centres and 20M+ therapy sessions.
If Only One Person Implements This, It's Limited. Share It.
Consistency across caregivers multiplies impact. The more people in your child's life who understand their light sensitivity — and how to support it — the stronger the protective environment around them. — PMC9978394, WHO CCD Package
Share This Page
Download Resources
"Explain to Grandparents" Summary
"Your grandchild has sensitive eyes that can detect the flickering in fluorescent lights — the long tube lights in schools and stores. This flickering, which most people can't see, causes them real discomfort: headaches, eye pain, and behavioural distress. The tinted glasses/hat/seating near windows help filter or reduce this light. Please help by: keeping warm lighting at your home, supporting their use of glasses/hat, and allowing breaks from bright lights."
Teacher Communication Template
"Dear [Teacher], [Child's name] has documented visual sensory sensitivity to fluorescent lighting (documented by [OT/Physician]). This neurological sensitivity causes [specific symptoms]. Requested accommodations: [specific list]. These accommodations have been shown to significantly improve [child's] classroom participation and behaviour regulation. Thank you for your support. — [Parent name]"

ACT VI: THE CLOSE & LOOP
Your Questions, Answered
Will my child ever outgrow fluorescent light sensitivity?
Some children's sensitivity decreases as their nervous system matures and they develop coping strategies. Others maintain the sensitivity into adulthood but manage it effectively with tools. The goal is functional management, not necessarily elimination of the sensitivity. Many adults with light sensitivity manage it independently with tinted glasses and environmental awareness.
Are FL-41 glasses the same as regular sunglasses?
No. FL-41 is a specific pink tint developed to filter the wavelengths most associated with light sensitivity, photophobia, and migraine triggers. Regular sunglasses reduce all light equally; FL-41 selectively filters problematic wavelengths. However, some children respond better to rose, amber, or other tints — individual trial is necessary.
How do I convince the school to make changes?
Documentation is key. Get a formal letter from your child's OT or physician. Collect behaviour data showing contrast between environments. Present specific, feasible accommodation requests: seat by window, permission to wear hat, scheduled breaks. Frame accommodations as helping the child succeed, not as criticism of the school.
Do LED replacements solve the problem?
Some do, some don't. Quality LEDs with good drivers produce minimal flicker and may be well-tolerated. Cheap LEDs may have visible flicker (especially when dimmed) and can be as problematic as fluorescents. Key factors: no flicker, warm colour temperature (2700–3000K), and continuous spectrum. Test before committing.
Is this the same as photophobia?
Related but distinct. Photophobia is sensitivity to light in general, including bright sunlight. Fluorescent light sensitivity is specifically triggered by characteristics unique to fluorescent light — the flicker rate and spectral quality. Many children have both, but some are specifically sensitive to fluorescents while tolerating other light sources well.
How quickly will I see results?
Tinted glasses often show immediate effect — the child visibly relaxes when the problematic light is filtered. Strategic seating and breaks may take 1–2 weeks to show clear behavioural patterns. The full multi-layered protocol typically shows consistent improvement within 4–6 weeks. Data tracking makes the progress visible.
Can light sensitivity cause actual headaches?
Yes. Fluorescent light sensitivity can cause genuine headaches, eye strain, fatigue, nausea, and dizziness. These are real physiological responses, not imagined. If headaches are severe or frequent, evaluation for migraine condition is recommended.

You've Read the Science. You've Seen the Strategies. Now Act.
The difference between knowing and doing is starting. Your child doesn't need a perfect plan — they need a parent who begins today with what they have. Strategic seating is free. Natural light is free. A conversation with your child is free. Start there.
Validated by the Pinnacle Blooms Consortium: OT • SLP • ABA • SpEd • NeuroDev. Built by Mothers. Engineered as a System. "The difference between knowing and doing is starting. Start today."
Preview of 9 materials that help with fluorescent light distress Therapy Material
Below is a visual preview of 9 materials that help with fluorescent light distress therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.






Link copied!
The Pinnacle Promise
OT
Occupational Therapy
SLP
Speech-Language Pathology
ABA
Applied Behaviour Analysis
SpEd
Special Education
NeuroDev
Neuro Development
CRO
Clinical Research & Outcomes
"From fear to mastery. One technique at a time." — Pinnacle Blooms Network®
Medical Disclaimer: This content is educational. It does not replace assessment by a licensed occupational therapist, developmental optometrist, or healthcare provider. Persistent light sensitivity or photophobia should be evaluated to rule out underlying visual or neurological conditions and identify appropriate interventions. Individual results may vary. Statistics represent aggregate outcomes across the Pinnacle Blooms Network.
© 2025 Pinnacle Blooms Network®, unit of Bharath Healthcare Laboratories Pvt. Ltd. All rights reserved.
Statutory Identifiers: CIN: U74999TG2016PTC113063 | DPIIT: DIPP8651 (Govt. of India) | MSME: Udyog Aadhaar TS20F0009606 | GSTIN: 36AAGCB9722P1Z2
FREE National Autism Helpline (16+ languages): 9100 181 181 | pinnacleblooms.org | care@pinnacleblooms.org