When Your Child's Hands Can't Do What Their Heart Wants To
It is 7:42 in the morning. Your child is standing at the closet, fully dressed in their mind — but the zipper has defeated them for the fourth time in five minutes. You step in, zip it yourself, and the morning proceeds. But that look on their face stays with you all day.
Fine Motor for Self-Care
F-617
Ages 3–10
ACT I — EMOTIONAL ENTRY
You Are Not Failing Your Child. Their Hands Are Still Learning.
Fine Motor for Self-Care is a precisely staged neurological process — and when it lags, it lags for reasons that have nothing to do with intelligence, effort, or parenting. Building the hand skills that make independence possible — one button, one zipper, one tied shoe at a time.
🏥 Pinnacle Blooms Consortium®
India's most experienced pediatric therapy network
👐 Pediatric OT
Occupational therapy — the lead clinical discipline
🎯 Ages 3–10
The critical window for self-care skill building
✅ Evidence-Based
Level I evidence — systematic reviews and RCTs
WHO Nurturing Care Framework (2018): Early caregiver awareness and targeted intervention directly shape developmental trajectories. The period from birth through middle childhood is the critical window for building self-care independence.
ACT I — THE NUMBERS
Millions of Families Wake Up to This Same Morning
You are among an estimated 8–12 million families in India navigating fine motor self-care challenges right now. In your child's classroom of 30, statistically 4–6 children are struggling with the same buttons, zippers, and containers — most silently, most without targeted help.
1 in 6
Children Affected
Children in India experience fine motor delays affecting daily function
47%
ASD Overlap
Of children with ASD show clinically significant fine motor difficulties impacting self-care
3–7
Critical Years
The window when self-care fine motor skills should consolidate — and when delays are most treatable
"My child isn't broken. Their hands are still developing the specific skills that buttons and zippers demand. That gap is closeable." — Parent, Pinnacle Network

ACT I — NEUROSCIENCE
The Neuroscience of Buttons and Zippers
Self-care tasks like buttoning, zipping, and tying shoes are among the most neurologically complex activities a young child attempts. Each fastener demands the simultaneous coordination of six distinct neural systems. When a child's hands fumble, it is a developing nervous system executing an extraordinarily complex multi-system coordination task — often before all six systems have matured sufficiently. This is a wiring-in-progress situation, not a willpower problem.
Somatosensory Cortex
Tactile discrimination — feeling the button without looking
Motor Cortex
Finger isolation commands — index and thumb working independently
Cerebellum
Precision timing and force calibration — how hard to push
Prefrontal Cortex
Motor planning — what sequence of movements to execute
Visual Cortex
Visuomotor integration — aligning button to buttonhole
Proprioceptive System
Body-position sense — knowing where fingers are without looking

ACT I — DEVELOPMENTAL TIMELINE
Your Child's Developmental Waypoint — Not Their Destination
Every child moves through a predictable self-care milestone arc. Knowing where your child sits on this timeline transforms the challenge from a judgment into a navigation point. Fine motor self-care delays frequently co-occur with ASD, DCD, ADHD, low muscle tone, and SPD — and all of these respond to targeted intervention.
1
Age 2–3
Removes clothing independently; participates in hand washing
2
Age 3–4
Large buttons attempted; spoon with minimal spill; undresses independently
3
Age 4–5
Buttons shirt; manages separating zipper; fork and spoon well; brushes teeth
4
Age 5–6
All fasteners managed; shoe-tying emerging; adequate independent grooming
5
Age 6–7+
Shoe-tying mastered; all clothing independent; knife and fork together
Your child is here — and this page is your bridge forward. With the right materials and consistent practice, the trajectory forward is clear, achievable, and supported by 20 million therapy sessions of real-world evidence from Pinnacle centers.
ACT I — EVIDENCE
Clinically Validated. Home-Applicable. Parent-Proven.
The 9 materials presented in this guide are selected from a corpus of peer-reviewed occupational therapy literature, Montessori practical life research, and Pinnacle Network's 20M+ session database. They are not trends. They are clinically validated tools backed by Level I evidence.
PRISMA Systematic Review (2024) — PMC11506176
16 studies (2013–2023) confirm fine motor and sensory integration intervention meets criteria for evidence-based practice in ASD. Effect sizes: moderate-to-large across motor skill outcomes.
Meta-Analysis — World Journal of Clinical Cases (2024)
24 studies confirm sensory integration + fine motor intervention promotes adaptive behavior, motor skills, and social participation. Fine motor for ADLs shows highest consistency of positive outcomes.
Indian RCT — Indian Journal of Pediatrics (2019)
Home-based fine motor and sensory interventions delivered by trained parents demonstrated significant improvement in self-care functional outcomes in Indian pediatric populations.
NCAEP Evidence-Based Practices Report (2020)
Fine motor skill instruction and task analysis classified as evidence-based practice for autism, applicable across dressing, feeding, and grooming domains.

ACT II — KNOWLEDGE TRANSFER
Fine Motor for Self-Care: The Formal Definition
Formal Name
Fine Motor Skills for Activities of Daily Living (ADL Fine Motor Intervention)
Parent-Friendly Alias
"Building Independent Hands"
Badge
Domain: OT-FMSC | Ages: 3–10 | Sessions: 10–20 min daily | Setting: Home + School
What It Encompasses
Fine motor skills for self-care encompass the hand and finger abilities required for independent daily living: dressing (managing fasteners, orienting clothing), feeding (using utensils, opening containers), grooming (brushing teeth and hair, washing), and personal hygiene management.
These tasks require integration of: pinch strength, finger isolation, bilateral coordination, motor planning, tactile discrimination, and proprioceptive feedback. Children with fine motor self-care delays know what they want to do — the gap is between cognitive intent and physical execution. That gap is closeable.
ACT II — THE CONSORTIUM
The Consortium Behind This Technique
This technique doesn't belong to one therapy type. Independence belongs to the whole child — and the whole consortium works to get them there.
Pediatric Occupational Therapy (Lead)
Primary architect of self-care fine motor programs. OTs conduct ADL assessments, identify component skill deficits, prescribe materials, and design progressive practice hierarchies.
Pediatric Speech-Language Pathology
SLPs address oral motor self-care components and provide language scaffolding for multi-step sequences: "First soap, then rub, then rinse."
ABA / BCBA
ABA provides reinforcement architecture, task analysis, backward chaining protocols, and the data systems that make self-care skill acquisition systematic and measurable.
Special Education
SpEd teachers carry self-care goals into school environments — coat hooks, lunch containers, bathroom routines. Generalization across settings is critical for lasting independence.

ACT II — TARGETS
Precision Targets: What These 9 Materials Are Building
✅ Primary (Observable at Home)
- Independent dressing: buttons, zippers, snaps, lacing, shoe-tying
- Feeding independence: utensil use, container opening, food preparation
- Grooming independence: toothbrushing, hair brushing, hand washing
🎯 Secondary (Weeks 4–8)
- Bilateral hand coordination (both hands in simultaneous different roles)
- Motor memory (executing tasks automatically without thinking)
- Finger isolation and proprioceptive calibration
Within 6–8 weeks of consistent practice, expect your child to initiate dressing attempts rather than wait for help, show reduced frustration during fastener tasks, and persist longer before abandoning.
ACT II — THE 9 MATERIALS
The 9 Materials That Build Independent Hands
Every material below is clinically mapped to a specific fine motor component. This is not a shopping list — it is a therapeutic toolkit.

Material 1
Dressing Frames & Fastener Boards
Canon: Dressing / Fastener Practice
Wooden or fabric frames mounted with individual fastener types — buttons, zipper, snaps, buckles, laces — for isolated, pressure-free practice.
Why OT Prescribes It
Eliminates the complexity of dressing on a moving body. The child practices the motor skill at the optimal viewing angle, on a stable surface, with time pressure completely removed. Muscle memory formed here transfers directly to clothing.
- Ages: 3–8 | Price: ₹400–₹1,500
- Pinnacle Recommends ✅

Material 2
Button Snakes & Threading Buttons
Canon: Dressing / Fastener Practice
A ribbon with a large button at one end, threaded through buttonholes in sequential felt pieces — often themed as a caterpillar, train, or garden.
Why OT Prescribes It
Provides dozens of button-through-buttonhole repetitions in a single play session. The pinch → push → pull motion is repeated until automatic. Graduated hole sizes allow progressive challenge, so the task grows with your child's skill.
- Ages: 2–6 | Price: ₹150–₹400

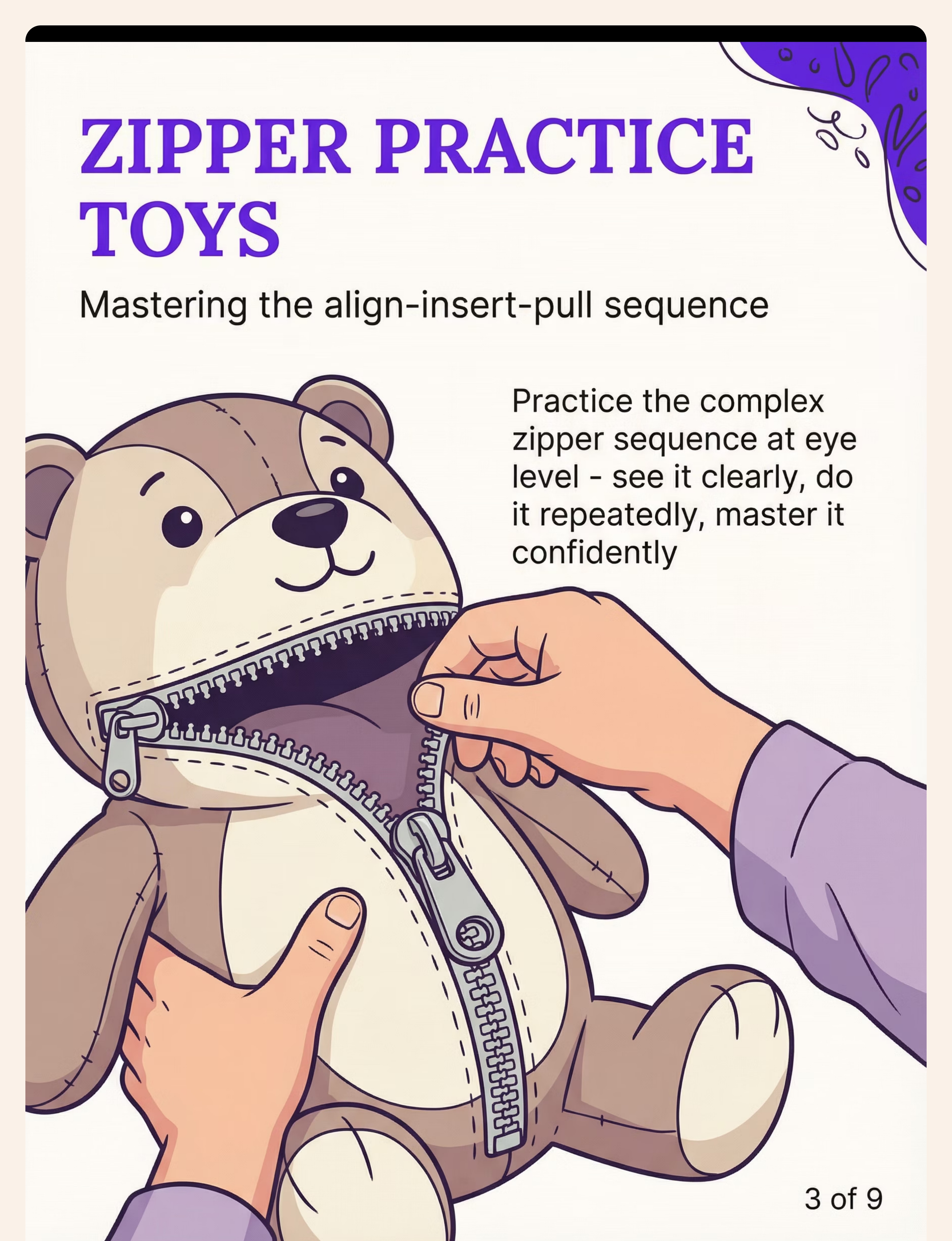
Material 3
Zipper Practice Toys & Boards
Canon: Dressing / Fastener Practice
Stuffed animals with zipper mouths, busy boards with zippers, and zipper pouches with large pull tabs designed for little hands.
Why OT Prescribes It
Zippers require a 4-step motor sequence: align → insert pin → hold bottom → pull up. Practicing on an external object lets the child see the mechanism clearly. Large pull tabs build confidence before standard zippers — a critical scaffolding step that most home practice misses.
- Ages: 3–7 | Price: ₹200–₹600

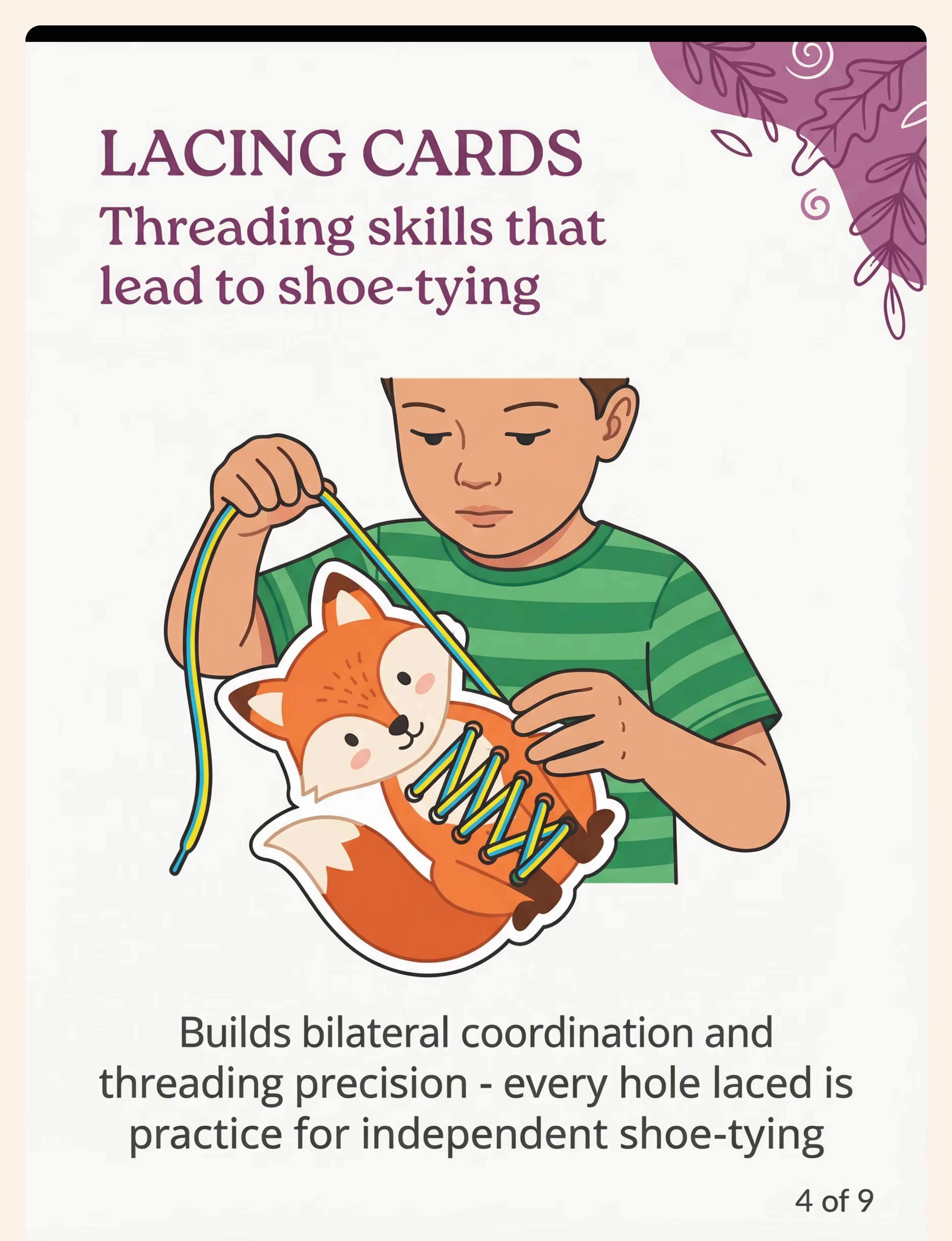
Material 4
Lacing Cards & Lacing Activities
Canon: Fine Motor / Pre-Writing
Cardboard or foam shapes with punched holes, threaded with shoelaces or yarn — progressing to shoe-shaped lacing boards.
Why OT Prescribes It
Builds bilateral coordination and threading precision — the exact motor foundation shoe-tying demands. Every hole threaded is practice for independent footwear management. The bilateral coordination developed here also activates writing readiness pathways, making this one of the highest-yield materials in the toolkit.
- Ages: 3–7 | Price: ₹100–₹350
Material 5
Pinch & Grasp Strengthening Tools
Canon: Strengthening / Resistive Materials
Clothespins, therapy putty (multiple resistance levels), spring tweezers, squeeze balls, and dropper sets.
Why OT Prescribes It
Weak pinch strength makes fasteners physically impossible regardless of technique knowledge. These tools build the baseline strength that all dressing and container tasks require. Think of this as the foundation layer — without adequate pinch and grasp, even the best technique fails. Therapy putty provides progressive resistance that strengthens as the child improves.
- Ages: 3–10 | Price: ₹100–₹500

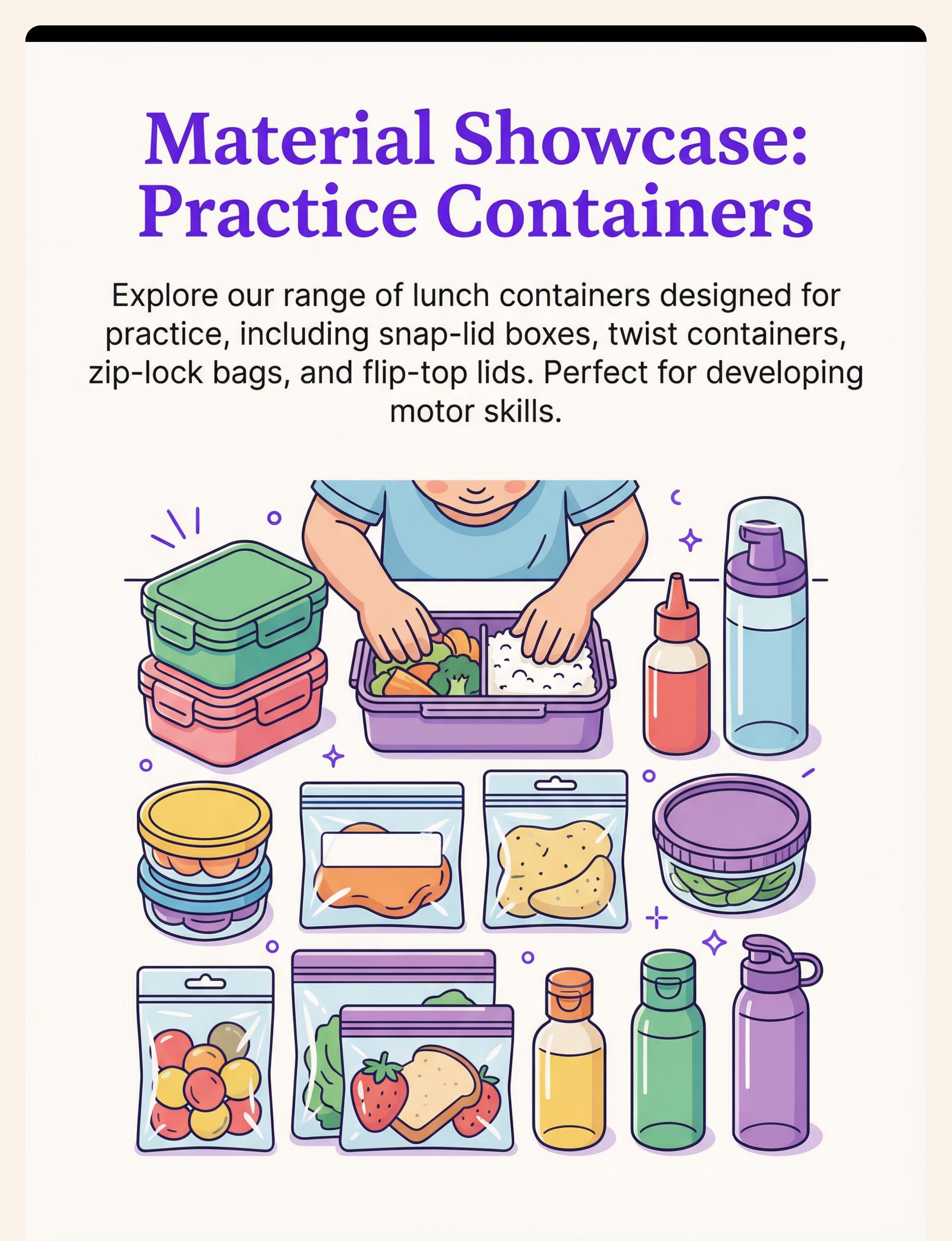
Material 6
Practice Food Containers & Packaging
Canon: Feeding Skills / Container Practice
Varied container types: snap-lid boxes, zip-lock bags, twist containers, flip-top lids, straw-poke juice boxes — assembled as a home practice kit.
Why OT Prescribes It
Lunchtime container management is a primary source of school-based difficulty and embarrassment. Practicing with actual containers during non-meal times builds automatic skill before the pressure of a school lunch environment. One child came home for weeks with an untouched lunch — not because she wasn't hungry, but because she couldn't open her dabba. That is exactly what this material addresses.
- Ages: 4–9 | Price: ₹0–₹300
- ✅ DIY — Use household containers. No purchase required.

Material 7
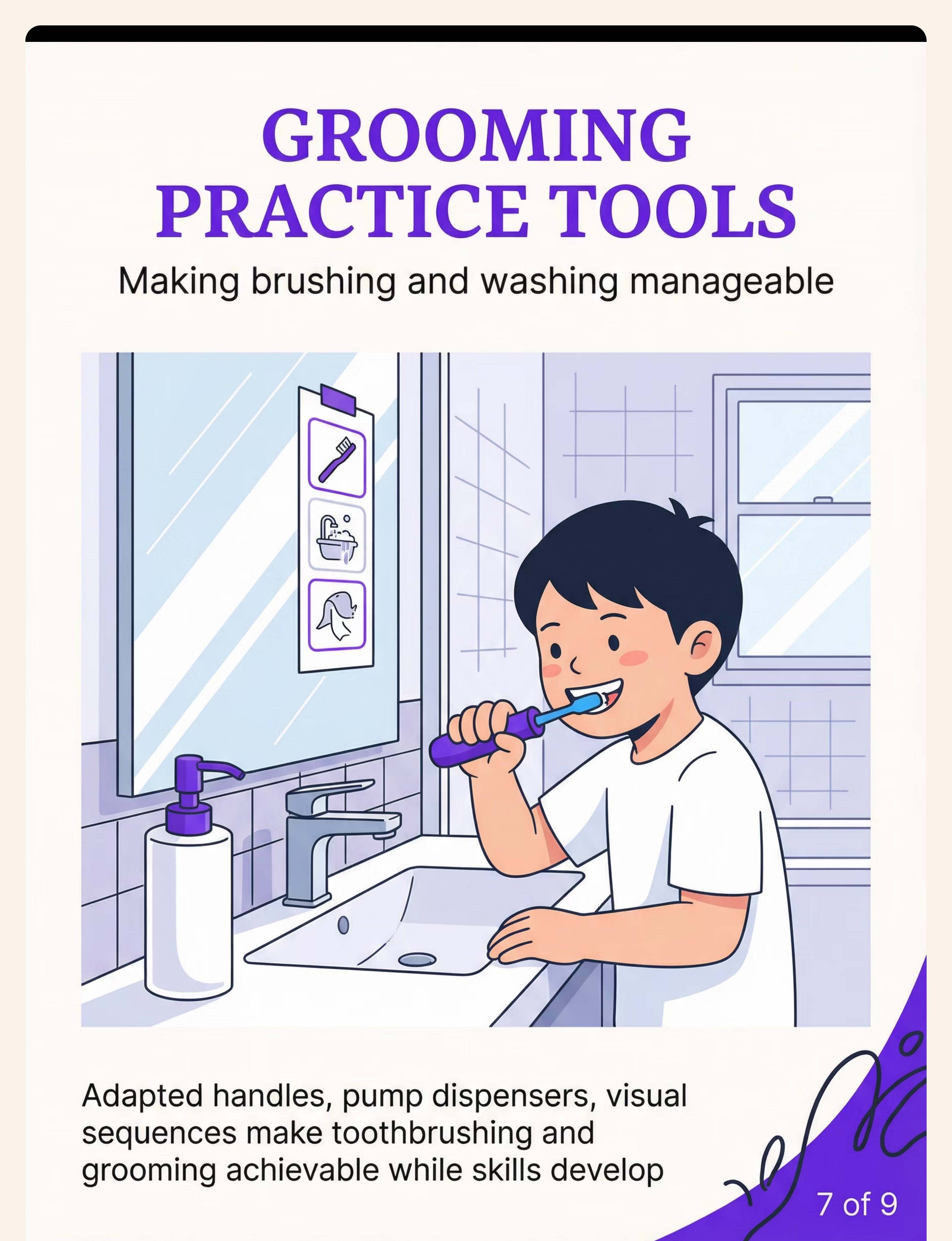
Grooming Practice Tools (Adapted)
Canon: Grooming / Personal Hygiene
Built-up handle toothbrushes, toothpaste pump dispensers, visual sequence charts, electric toothbrush, detangling brushes.
Why OT Prescribes It
Adapted tools enable grooming independence while underlying fine motor skills develop — a parallel strategy. Toothpaste pumps eliminate squeezing demands. Visual sequence charts address motor planning gaps by breaking the routine into visible steps. Electric toothbrushes provide a success experience that builds confidence and reduces morning resistance, making the whole routine more sustainable.
- Ages: 3–8 | Price: ₹150–₹600
Material 8
Utensil Skill Builders & Adaptive Utensils
Canon: Feeding Skills / Adaptive Utensils
Built-up handle forks and spoons, angled utensils, weighted utensils, safety training knives, training chopsticks with connector.
Why OT Prescribes It
Feeding independence affects every meal, every social situation, every school day. Adapted utensils enable success now; skill-building practice closes the underlying gap over time. Together they build both functional independence and long-term capability — a two-track strategy that keeps the child engaged and succeeding even while the harder skills develop.
- Ages: 3–9 | Price: ₹200–₹700
Material 9
Shoe-Tying Practice Boards
Canon: Dressing / Shoe-Tying Materials
A mounted shoe or shoe-shaped board at table height with color-coded laces (two colors to track lace movement) and a visual sequence card.
Why OT Prescribes It
Shoe-tying at foot level is one of the hardest fine motor tasks — awkward angle, limited visibility, thin laces. A shoe-tying board brings the task to eye level, making the sequence visible and learnable before transfer to actual shoes. The two-color lace system is a breakthrough: when both laces are the same color, the child cannot track which lace is doing which action. Two colors make the choreography of tying visible.
- Ages: 4–8 | Price: ₹200–₹500

ACT II — DIY OPTIONS
Zero-Cost Versions That Work Just as Well
The science is in the practice, not the product. A ₹30 clothespin builds the same pinch strength as a ₹500 therapy tool. A homemade button snake produces the same neural pathway development as a commercial Montessori frame. Your household is already a therapy center. Every family, every economic reality, every geography — these techniques work.
Material | Buy This | Make This (₹0) | |
Dressing Frame | Wooden Montessori frame ₹400–1,500 | Stretch fabric over picture frame. Sew 3–4 large shirt buttons. Add a separating zipper. | |
Button Snake | Commercial set ₹150–400 | Ribbon + button from any shirt. Cut 8–10 circles from old felt. Make holes with scissors. | |
Zipper Practice | Commercial toy ₹200–600 | Sew a jacket zipper onto any fabric pouch. Stuff with small treasures for motivation. | |
Lacing Cards | Commercial cards ₹100–350 | Cardboard + hole punch + shoelace. Cut animal shapes. Punch holes around edges. | |
Pinch Tools | Therapy putty + clothespins ₹100–500 | Household clothespins (₹30/pack). Play-dough for putty. Tweezers from kitchen. | |
Container Practice | Specialty containers ₹0–300 | Use your own household dabbas, zip bags, and bottles. | |
Grooming Aids | Adapted tools ₹150–600 | Wrap foam around toothbrush handle. Use pump soap. Draw visual sequence chart on paper. | |
Adaptive Utensils | Commercial adapted set ₹200–700 | Wrap rubber bands around spoon handle for grip. Bend spoon slightly for angle. | |
Shoe-Tying Board | Commercial board ₹200–500 | Tie an old shoe to a board with wire. Use two-colored laces (mark both laces differently). |

ACT II — SAFETY
Safety Gate: Read This Before Every Session
🔴 DO NOT PROCEED IF:
Child has open wounds on hands • Active meltdown or severe distress • Sensory overload within 1 hour • Signs of illness, fever, or extreme fatigue • Any material poses choking risk • Signs of pain or self-injurious behavior
🟡 MODIFY IF:
Child is mildly dysregulated (shorter session, simpler material) • It's a "bad day" (reduce expectations, increase reinforcement) • Time pressure is high — skip the session entirely. Rushed practice builds frustration, not skill.
🟢 PROCEED WHEN:
Child is fed, rested, calm-alert • Session is during low-pressure, non-rushed time • Materials prepared and within reach • Parent is calm and unhurried • Reinforcers are ready
The Prime Rule: A session that ends well — even if short — is infinitely more therapeutic than a session pushed to completion that ends in distress. Stop before frustration. Never push through.
ACT II — SETUP
Your Home Fine Motor Practice Station
Environment is a therapeutic variable — not just a backdrop. The right setup measurably improves session outcomes. Poor posture alone reduces fine motor precision by approximately 30%. These details matter clinically.
Position the Child
Table height at elbow level. Feet flat on floor or footrest — no dangling. Core stability directly supports hand function. Child's trunk upright, not slumped.
Lighting & Sound
Natural light from the side (not behind child — avoids shadow). Soft background music at 60–70 BPM. Avoid TV audio. Cold hands significantly reduce dexterity — keep room comfortable.
Prepare Materials
One material out at a time — choice overload disrupts attention. Practice material staged in neutral position. Difficulty set to child's current level, not aspirational. Reinforcer box nearby but not visible yet.
Session Duration
Maximum 15 minutes for ages 3–5. Up to 20 minutes for ages 6–10. Stop at first sign of genuine fatigue — every time, without exception.

ACT III — EXECUTION
60-Second Pre-Flight Check
The best session is one that starts right. Two minutes of readiness assessment saves twenty minutes of frustration. If postponing a session: it is not failure. It is intelligent therapeutic scheduling.
Indicator | ✅ GO | ⚠️ Modify | 🔴 Postpone | |
Fed? | Normal meal within 2 hrs | Snack needed first | Hungry — feed first | |
Rested? | Normal sleep last night | Mildly tired — shorten | Overtired — rest day | |
Regulated? | Calm, alert, engaged | Slightly elevated — warm up first | Meltdown — postpone | |
Interest? | Approaches materials | Neutral — stronger motivator | Active avoidance — try tomorrow | |
Physical? | Hands comfortable, no injury | Minor discomfort — monitor | Pain or injury — postpone |
5–6 GO Indicators
→ Proceed to Step 1
3–4 GO Indicators
→ Modified session: simpler material, shorter time
0–2 GO Indicators
→ Postpone. Record in data log. Return tomorrow.
📞FREE Helpline: 9100 181 181 — 16+ languages | 24×7

STEP 1 OF 6
Step 1 — Invite, Don't Command
STEP 01
Duration: 30–60 seconds
ABA Principle: Pairing + Motivating Operation
The Script
"Hey — want to see something? I have this cool snake today — look how many pieces it has. Want to put one on?"
"This bear has a secret pocket — but only you can open it. Want to try?"
Body Language Matters
Sit beside the child, not across from them. Beside = collaborative. Across = test. Keep materials visible but not yet pushed toward them. Use a warm, curious tone — not an instructional tone.
Acceptance Cues
- Eye contact toward materials
- Body orientation toward table
- Reaching toward materials
If Resistance
"That's okay — we can just look at it." Place in view without expectation. Wait 2 minutes. Offer again with a stronger motivator.

STEP 2 OF 6
Step 2 — Introduce the Material
The Introduction Protocol
- Place the material at child's midline on the table
- Demonstrate the action ONCE, slowly, without commentary: "Watch me first"
- Offer to child: "Now you try" — no further instruction yet
- Observe what they attempt naturally — this is baseline data
Key Principles
Speed: Deliberately slow — give child time to track visually. Angle: Tilted toward child for optimal view of the mechanism. Hands: Keep yours visible and still while child works — resist the urge to help immediately.
Any attempt — any engagement with the material — earns immediate, specific praise: "You picked it up — that's exactly right." The attempt, not the success, is reinforced at this stage.
STEP 02
Duration: 1–3 minutes
OT Principle: Material Introduction + Sensory Familiarization
Child Response Guide
Attempts immediately → Let them try independently
Watches, then attempts → Wait quietly, encourage with "go ahead"
Touches but doesn't attempt → Model once more, then offer
Ignores material → Tie to interest: "the button opens to find a dinosaur"
STEP 3 OF 6
Step 3 — The Core Therapeutic Action
Duration: 5–12 minutes | The Active Ingredient. This is where neural pathway formation actually happens. The specific execution varies by material — here is how to run each one effectively.
Dressing Frames
Teach one fastener type per session. For buttons: "Fold the fabric so the button can peek through. Push it from behind. Pull it forward." Hand-over-hand only after 3 independent attempts.
Button Snake & Lacing Cards
Count aloud together. Celebrate each piece. 5–8 pieces per session, not speed. For lacing: always the same consistent direction — in from front, out from back, pull through.
Zipper Practice
Teach verbally AND physically: "Pin in the box → Hold the bottom → Pull up high." Repeat this same phrase every time. Consistency of language builds the motor program.
Shoe-Tying Board
Backward chaining: parent completes steps 1–4, child pulls tight (step 5) for first 3 sessions. Then gradually child takes over from the end backward, session by session.
Utensils & Containers
Practice cutting play-dough before food. One utensil type per session. For containers: open, close, open, close — repetition is the point. Time how long opening takes — it will shorten week over week.
STEP 4 OF 6
Step 4 — Dose the Practice
Repetition Targets by Material
- Dressing Frames: 3–5 complete fastener cycles
- Button Snake: 5–10 pieces threaded
- Zipper Practice: 4–6 complete open-close sequences
- Lacing Cards: 1 complete card (all holes)
- Pinch Tools: 10–15 clothespin clips or 5 putty retrievals
- Containers: 3–5 opens per container type
- Grooming: Full routine sequence × 1 (timed)
- Utensils: 10 fork stabs, 8 spoonfuls, or 5 cuts
- Shoe-Tying: 3–5 complete tie attempts
The Prime Dosage Rule
3 good repetitions > 10 forced repetitions. A rep completed with appropriate form, appropriate pressure, and self-correction is worth 3 rushed reps. Quality beats volume, every time.
Satiation Indicators — Stop When You See:
- Increasing errors when earlier reps were correct
- Reduced force or effort on the task
- Increased body movement, wiggling, looking away
- Verbal protests increasing
→ At first satiation sign: one more rep, then celebrate and stop.
STEP 5 OF 6
Step 5 — Catch Them Succeeding
Duration: Continuous throughout session | ABA Principle: Contingent Reinforcement + Behavior-Specific Praise. The rule: child completes attempt → within 3 seconds → specific, enthusiastic praise.
💬 Social (Free, Always)
"You pushed that button through — did you see your fingers do that?!" • High five, fist bump • Victory dance (child's choice) • "Call grandma to tell her what you just did"
⭐ Token Economy
One sticker per completed session. Five stickers = chosen reward. Use Pinnacle Reward Sticker Set — 1,800+ stickers, ₹364 Amazon.in →
🏆 Tangible (Use Sparingly)
Small preferred edible after full session (not mid-session). Access to preferred toy for 5 minutes post-session. Pinnacle Reward Jar for token economy — ₹589 Amazon.in →
Celebrate the attempt, not just the success. Success: "You did it — your hands know how to do that now." Attempt: "You tried the whole sequence — your hands are learning."
STEP 6 OF 6
Step 6 — Close the Session Well
STEP 06
Duration: 1–2 minutes
Why It Matters: Abrupt session endings cause dysregulation spill-over into the next activity. The cool-down is therapeutic, not optional.
Transition Warning Sequence
5 min before → "We have 5 more minutes."
2 min before → "Two more buttons, then all done."
1 min before → "Last one — make it your best."
End → "All done! You practiced [X]. High five."
Cool-Down Activity (Choose One)
- Proprioceptive: Push both palms flat on table for 10 seconds
- Tactile: Run hands through a small bowl of dry rice or sand
- Cognitive: "Pick three materials to put away first"
Material Put-Away Ritual
Child participates in put-away — this is itself a fine motor activity. Placing materials in containers, closing boxes, returning lacing cards: additional practice with zero additional demand.
If Child Resists Ending
"I know. You're getting really good at this. We'll do it again tomorrow — same time. Now let's put it away together." Do not extend past planned end — resistance must never earn more time.

ACT III — DATA
60 Seconds of Data Now = Weeks of Progress Visibility
"60 seconds of data now saves hours of guessing later. One data point means nothing. 40 data points tell a developmental story." — Log your session immediately after cool-down, while observations are fresh.
Which Material?
Dressing Frame / Button Snake / Zipper Toy / Lacing Cards / Pinch Tools / Containers / Grooming Tools / Utensils / Shoe-Tying Board
How Many Successful Reps?
Count completed without hand-over-hand assistance. Track week-over-week increase — this number should trend upward.
Session Energy Level
Child's state overall: 1 = Very Difficult → 5 = Excellent. A decreasing resistance trend over weeks is a clear success indicator.
ACT III — TROUBLESHOOTING
Reality Check: Most Sessions Have Rough Moments
"Session abandonment is not failure. It is data. The child told you something important about what needs to change."
Child refuses to touch the material
Why: Tactile sensitivity, task demand too high, or motivation insufficient. Fix: Hide material in favorite toy. Reduce demand to "just touch it." Try a different material from the 9.
Child attempts but immediately gives up
Why: Task difficulty exceeds current skill level. Fix: Make it easier — larger buttonhole, larger zipper pull tab. Pre-teach the first sub-step only. Celebrate immediately on first contact.
Skill doesn't transfer to real clothing
Why: Transfer hasn't occurred yet — normal in weeks 1–4. Fix: Practice on actual clothing during low-pressure times (never morning rush). Start with one garment they love.
Progress plateaus after initial gains
Why: Natural acquisition plateau, or task has become too easy. Fix: If too easy — increase difficulty. If plateau despite correct difficulty: consult OT. GPT-OS® plateau alerts will notify you.
Sessions cause significant emotional distress
Why: Task demand too high, or environmental factors. Fix: Reduce all demands. Make it purely play. Seek OT consultation — this level of resistance may indicate sensory factors needing professional assessment.
ACT III — PERSONALIZATION
Your Child. Your Version. Your Timeline.
No single protocol fits every child. Effective fine motor intervention is individually calibrated — sensory profile, age, frustration tolerance, and motivation all shape how the technique is delivered. Here is how to tune it precisely.
Sensory-Sensitive Child
Soft, non-scratchy fabrics on dressing frames. Warm therapy putty before use. Avoid metallic buckles — use plastic. Allow tactile exploration before any demand. More breaks, shorter sessions.
Sensory-Seeking Child
Textured items hidden inside therapy putty. Add vibration element (electric toothbrush exploration). More physical input in reinforcement (deep pressure high fives). Heavier materials preferred.
Low Frustration Tolerance
Shrink the task — one button only for the entire session. Make materials extremely motivating. Increase reinforcement density. Shorten sessions to 5–7 minutes.
Ages 3–4 (Younger)
All materials at maximum large size. Sessions 5–8 minutes maximum. Heavy play framing throughout. 1–2 repetitions per session, not 5–10.
Ages 8–10 (Older)
Involve child in selecting which material. Self-monitoring data sheets. Add speed challenge. Connect to real-world goals: "When you master this, you won't need help with your school uniform."
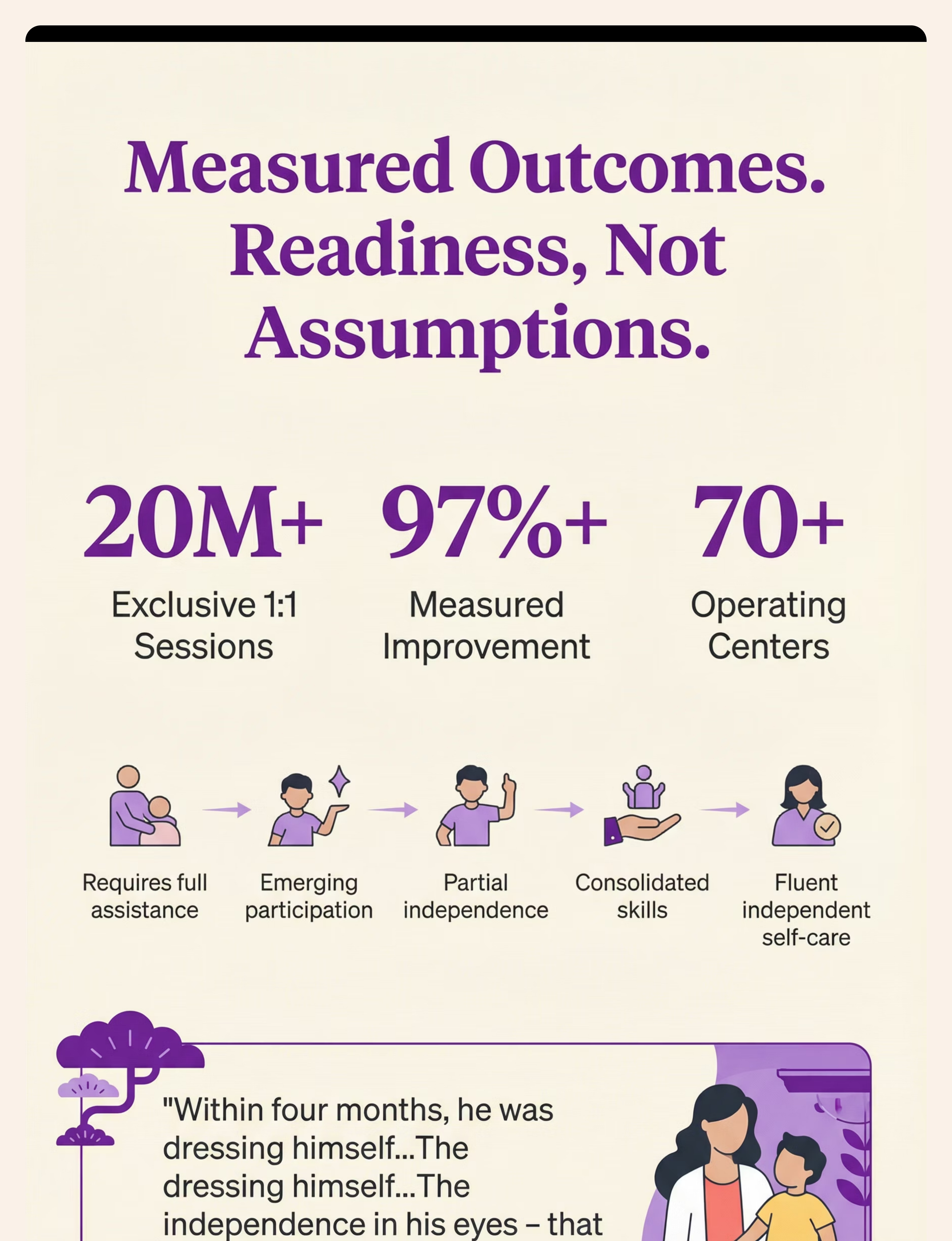
ACT IV — PROGRESS ARC
Weeks 1–2: Tolerance, Not Mastery
Foundation Phase
You are building the neural foundation. Progress is real but invisible.
Tolerance Growth
Session tolerance doubles on average from Day 1 to Day 14
Measurable Win
A child who tolerates the material 3 seconds longer than last week has had a therapeutic win
What progress looks like in weeks 1–2: child tolerates the material longer than Day 1 ✅ — reduced resistance at session start ✅ — at least one independent attempt, even if unsuccessful ✅ — session ends without distress ✅. What is NOT expected yet: independent fastener completion, transfer to real clothing, or spontaneous practice. That is all completely normal — and completely on track.
📞 FREE Helpline — 9100 181 181 — Call if you have questions about early-phase progress
ACT IV — PROGRESS ARC
Weeks 3–4: The Neural Pathways Are Forming
Consolidation Phase
Synaptic strengthening is underway. Behavioral consistency is emerging.
Consolidation Indicators
- Child anticipates the session — fetches material, asks for it ✅
- Consistent technique on the same material (muscle memory forming) ✅
- Reduced verbal prompting needed per rep ✅
- First glimpses of transfer: child attempts buttons on actual shirt ✅
- Frustration duration decreases — still frustrated, but recovers faster ✅
What Parents Typically Notice
"He started going to the dressing board himself before I even suggested it. He's not faster yet — but he's trying."
"She threaded 6 pieces on the button snake in one go. Two weeks ago she got through 2."
Week 3–4 Upgrade
What you witness in weeks 3–4 is synaptic strengthening. The behavior change you see is the output of brain-level restructuring. Consider: increasing to 5 sessions/week, moving one step up on difficulty, or adding a second material from the 9.

ACT IV — PROGRESS ARC
Weeks 5–8: Mastery Is Arriving
Mastery Phase
Skills are consolidating into automatic, transferable independence
Skill Area | Mastery Indicator (Observable, Measurable) | |
Buttoning | 3+ buttons independently without verbal prompt in under 2 minutes | |
Zipping | Separating zipper completed independently (3/3 attempts) | |
Lacing | Full card laced independently using consistent technique | |
Shoe-Tying | Complete bow tied independently on practice board | |
Containers | Opens 4/5 container types independently at school lunch | |
Utensils | Fork and spoon used appropriately without adapted handle | |
Grooming | Full brushing/washing sequence without step prompts |
🏅Independence Badge — Fine Motor for Self-Care — Awarded by the Pinnacle Blooms Consortium to children and families who committed to the process.

ACT IV — MILESTONE
You Did This. Your Child Grew Because of You.
Weeks ago, a zipper defeated your child before the school day began. Buttons were a morning war. Lunchboxes were things other children opened. Today, those are different stories. Not because your child was fixed — because your child was met with patience, with the right tools, and with a parent who showed up and did the work.
That commitment built these hands. You built these hands.
📷 Photo Prompt
Capture [Child's name] zipping their own jacket. Date: ___. Time from attempt to success: ___. Their face when they did it: ___.
📖 Journal Prompt
Write down what they couldn't do 8 weeks ago and what they can do today. Keep it. This is a clinical milestone worth honoring.
🎉 Family Celebration
Let the child demonstrate their new skill to grandparents — the pride in showing off matters therapeutically. The emotional reward reinforces the neurological investment.

ACT VI — CLOSE
Your Questions, Answered
From the most common questions at Pinnacle centers and parent communities across India.
My child is 9 — is it too late to build these skills?
No. Fine motor self-care skills are learnable across the entire childhood span. Older children often learn faster because their cognitive understanding of the task is stronger. Several Pinnacle families have achieved fastener independence in children ages 9–12 using exactly these materials. The approach remains the same — the language and motivation simply adjust to the child's age.
We've tried buttons before and it always ends in meltdown. Why would this be different?
The difference is context and sequence. Previous attempts were likely during real dressing — high demand, time pressure, natural frustration. This approach separates practice from the real task: dressing frames and button snakes during calm times, never morning rush. The strength and readiness work (Materials 4 and 5) also prepares the hands before the skill is demanded.
How many of the 9 materials should we use at once?
Start with ONE — the most important material for your child's current primary difficulty. Master that material over 3–4 weeks before adding a second. Multiple materials simultaneously fragment attention and make progress harder to measure. More is not better. Depth is better.
My child can button at home but not at school. Why?
This is skill generalization — the skill learned in one context needs explicit practice in new contexts. Schedule one practice session at school (after hours if possible), or ask the teacher to provide a brief opportunity. Transfer to the school environment needs to be deliberately practiced, not assumed.
More Frequently Asked Questions
Do I need to buy all 9 materials?
No. Start with the DIY versions from the zero-cost guide — they are clinically equivalent. Only purchase commercial materials if the DIY version is impractical to make, or if the child responds better to a commercial design. The skill acquisition happens in the practice, not the product.
My child's OT says we need formal therapy first. Can I still use this guide?
Yes — this guide is designed to complement professional therapy, not replace it. Many Pinnacle OTs send parents to this page as the home practice companion to clinical sessions. If your child is in formal OT: share this page with their therapist. Use it for the home practice that extends the therapy session into daily life.
How do I know if my child has sensory processing issues needing separate treatment?
Signs include: extreme resistance to materials (not just typical frustration), tactile defensiveness (avoiding certain textures), significant distress beyond frustration level. If these signs are present, an OT sensory assessment at a Pinnacle center is recommended before proceeding independently. 📞9100 181 181
Progress is very slow. Should I be worried?
Slow but consistent progress is not concerning — it is neurotypical skill acquisition at a slower developmental rate. What warrants concern is zero progress after 6–8 weeks of consistent, correct practice. If you are seeing any improvement at all — any — continue. Slow steady progress is still progress.
Didn't find your answer? Ask GPT-OS®: pinnacleblooms.org | Still need help? 📞9100 181 181

ACT VI — CALL TO ACTION
From Fear to Mastery.
Start This Technique Today.
Your child's hands are ready to learn. The materials are accessible. The evidence is clear. The six-step protocol is in your hands. The only remaining ingredient is the first session.
20M+
Sessions Delivered
Real-world evidence base from Pinnacle centers
97%+
Measured Improvement
Across children who completed the full protocol
70+
Centers in India
Professional support available near you
70
Countries Served
Pinnacle Blooms Consortium® global reach
Preview of 9 materials that help with fine motor for self care Therapy Material
Below is a visual preview of 9 materials that help with fine motor for self care therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.










Link copied!
ACT VI — THE PROMISE
The Pinnacle Blooms Consortium® Stands Behind This
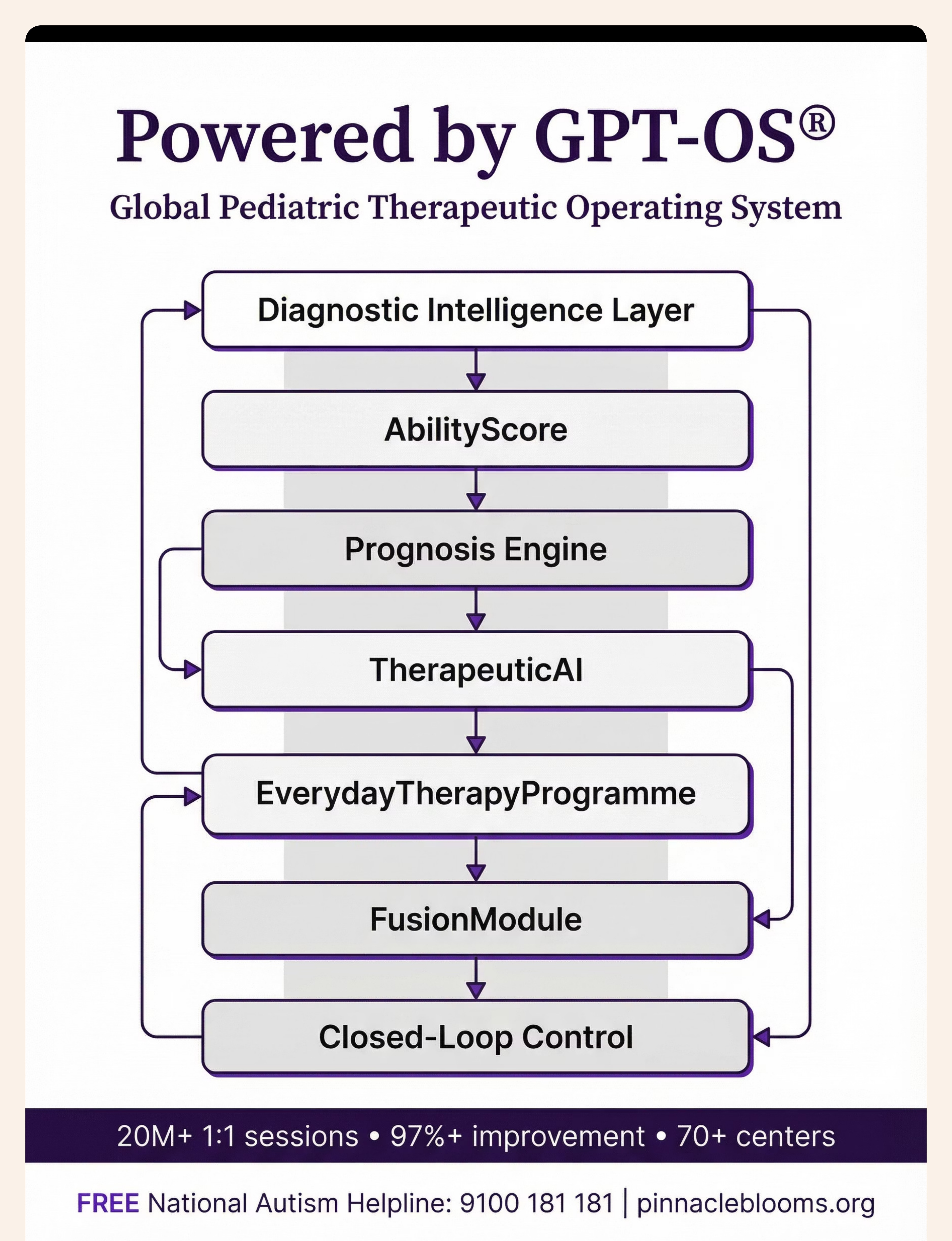
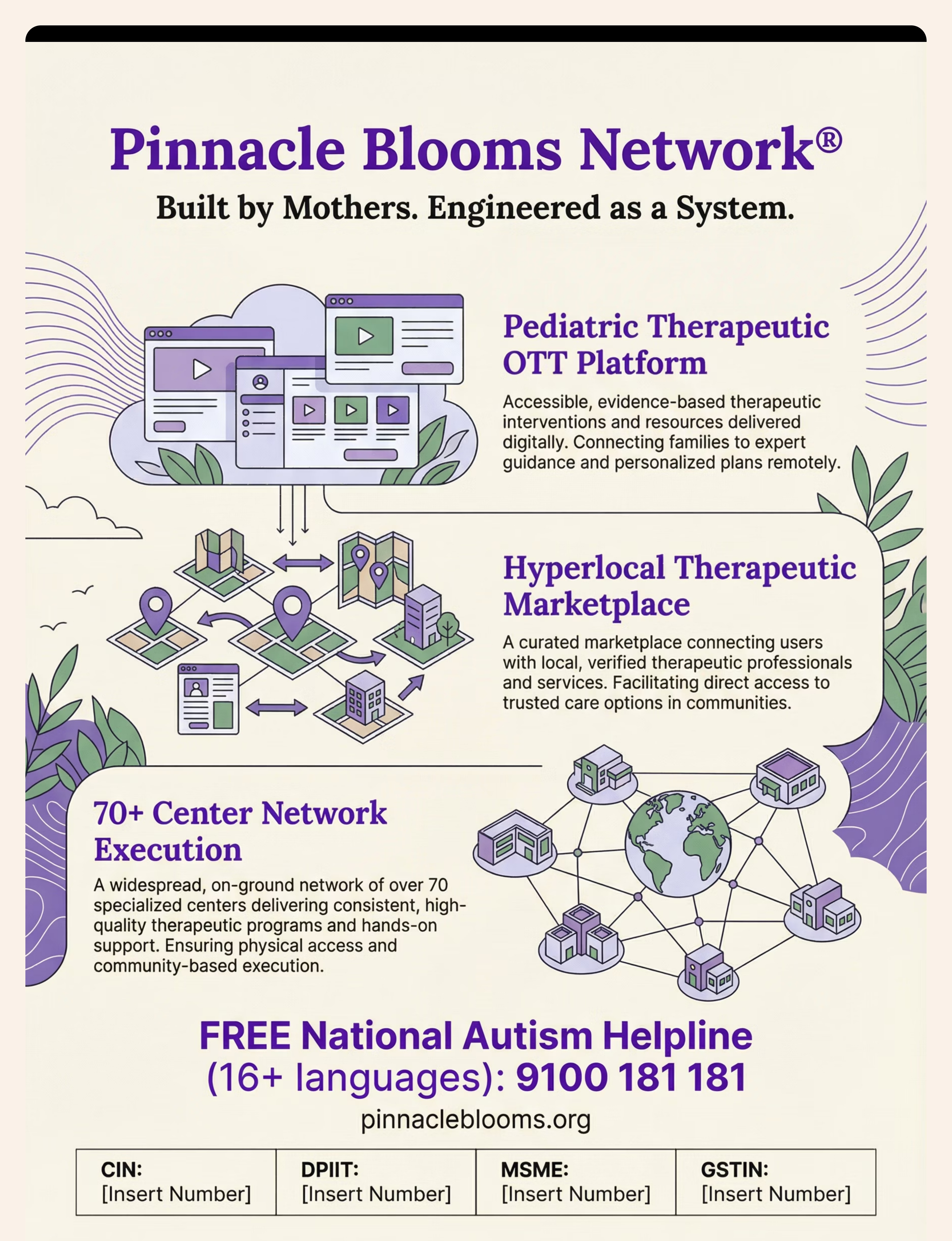
PINNACLE BLOOMS NETWORK®
Built by Mothers. Engineered as a System.
OT • SLP • ABA • SpEd • NeuroDev • CRO
70+ Centers • 70 Countries
20M+ Sessions • 97%+ Improvement
"From fear to mastery. One technique at a time."
Our Mission
Pinnacle Blooms Network® exists to transform every home in India — and globally — into a proven, scientific, 24×7, personalized, multi-sensory, multi-disciplinary pediatric therapy environment. Run on GPT-OS®. Built by the world's most experienced consortium of pediatric therapy specialists.
Navigate
📞 FREE National Autism Helpline: 9100 181 181 | 16+ languages | 24×7 | pinnacleblooms.org
This content is educational and informational only. It does not constitute medical advice and does not replace evaluation by licensed healthcare providers. Fine motor delays affecting self-care may indicate underlying developmental conditions — including DCD, ASD, low muscle tone, or sensory processing disorders — requiring professional assessment. Always consult your child's healthcare team before beginning any home intervention program. Stop any activity that causes distress and seek professional guidance. Individual results may vary. Progress timelines are population-level estimates and do not predict individual outcomes.
CIN: U74999TG2016PTC113063 | DPIIT: DIPP8651 | MSME: TS20F0009606 | GSTIN: 36AAGCB9722P1Z2
© 2025 Pinnacle Blooms Network®, unit of Bharath Healthcare Laboratories Pvt. Ltd. All rights reserved. GPT-OS®, AbilityScore®, TherapeuticAI®, EverydayTherapyProgramme™, FusionModule™ are proprietary marks of Bharath Healthcare Laboratories Pvt. Ltd.