"I haven't used the bathroom alone in three years. She follows me from room to room, screaming if I even close the kitchen door. School drop-off has become daily trauma for both of us. I love her completely — but I am drowning."
— Parent, Pinnacle Network, Hyderabad
Validated across 70+ centres | 21M+ therapy sessions | India's largest paediatric therapy network

PRISMA Systematic Review (2024): 80% of children with autism diagnosis display sensory processing and regulatory difficulties that directly impact separation tolerance. PMC11506176 | PMC10955541

In children with autism, the amygdala fires a full threat-response to separation even when there is no danger. Your leaving the room registers neurologically as you disappearing forever.
The prefrontal cortex (which processes "they'll be back in 10 minutes") is still maturing in all young children — and in autism, this maturation is significantly slower. Your child genuinely cannot conceptualise your return.
Your presence provides essential regulatory input: your voice's rhythm, your familiar scent, the proprioceptive weight of contact. The child's nervous system uses you as its external regulator. When you leave, regulation collapses.
Separation triggers a cascade of physical distress signals — racing heart, tight chest, churning stomach — that the child cannot identify or self-manage.

Study | Finding | Population | |
White & Roberson-Nay (2009) | Separation anxiety interventions in autism show significant behavioural reduction | ASD children 4–12y | |
Kerns et al. (2014) | Graduated exposure therapy reduces separation anxiety in ASD with 68% responder rate | 47 children ASD | |
NCAEP (2020) | Visual supports & social stories = evidence-based practice for autism anxiety | Systematic review | |
Bowlby (1988) | Graduated separation tolerance builds permanent attachment security | Foundational | |
Pinnacle Blooms (2025) | 97%+ measured improvement in Caregiver Dependence Reduction Index | 70+ centres, India |
PubMed: PMC11506176 | PMC10955541 | PMC9978394 | NCAEP 2020

- Age Range: 2–10 years
- Session Duration: 10–20 minutes/practice
- Frequency: Daily graduated practice
- Full Protocol: 8–12 weeks to significant tolerance

"The brain doesn't organise by therapy type. A child's separation anxiety has behavioural, sensory, communicative, and neurological roots simultaneously. This is why our consortium approach treats the whole child — not just the behaviour."
— Pinnacle Blooms Consortium Clinical Team









Material | Buy This | Make This (₹0) | Why It Works | |
Visual Return Timer | Sand timer ₹200 | Paper chain (1 link = 1 minute, child removes links until return) | Same visual countdown principle | |
Transitional Object | Comfort item ₹425 | Parent's worn T-shirt / scarf (carries scent) | Olfactory connection is neurologically equivalent | |
Separation Schedule | Printed board ₹150 | Photos printed/drawn, taped in sequence on cardboard | Predictability mechanism is identical | |
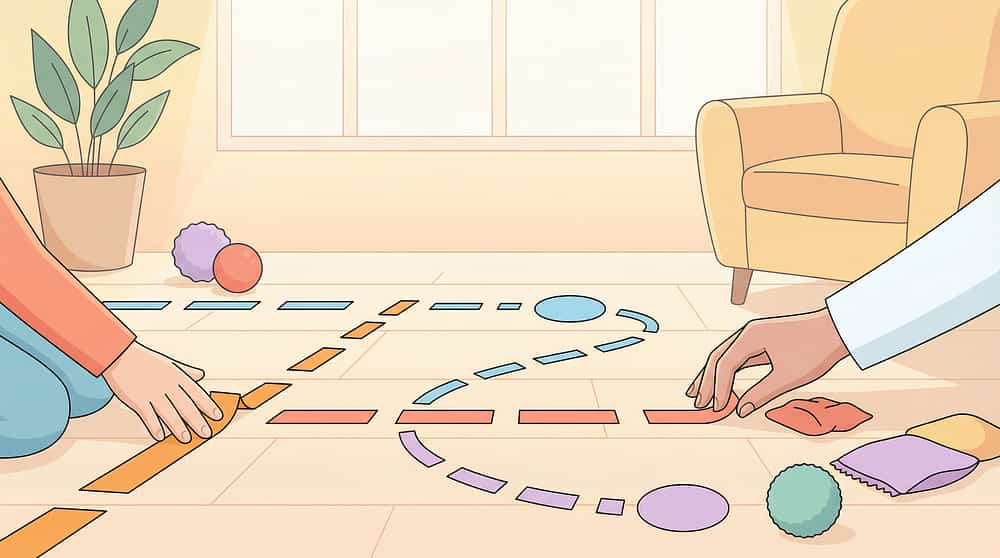
Graduated Distance Kit | Printed chart ₹100 | Masking tape distance markers on floor + notebook tally | Same graduated exposure principle | |
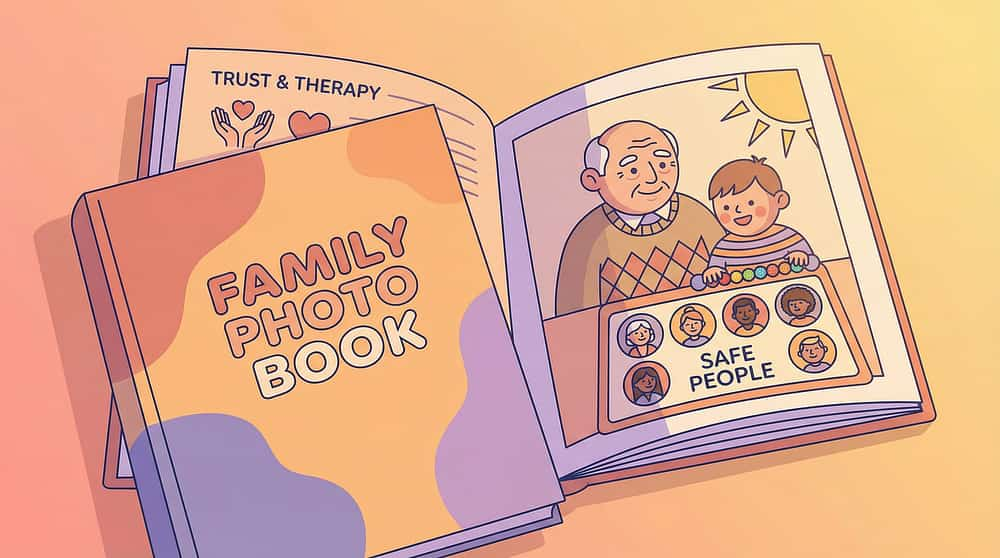
Caregiver Introduction | Photo book ₹100 | Laminated family photo card wallet | Visual anchor for safe people is the same | |
Independent Play Kit | Sensory bin ₹300 | Tupperware + rice/sand/dried beans + household small objects | Sensory absorption = same engagement | |
Calm-Down Kit | Kit ₹364 | Zip-lock bag: stress ball + feather + laminated breath card + small weight | Portable regulation tools work regardless of brand | |
Social Story Book | Book ₹150 | Handwritten A5 booklet with drawn/printed photos, 6–8 pages | Narrative schema is in the structure, not the production | |
Reunion Ritual Cards | Cards ₹100 | 3 movements of your secret handshake, practised until automatic | Ritual consistency is the therapy, not the material |

- Child is currently in acute meltdown or post-meltdown recovery (30-min window minimum)
- Child is ill, feverish, overtired, or hungry
- You are in a state of significant emotional distress
- You have recently broken an "I'll be back in X" promise — trust needs rebuilding first
- Child has experienced significant trauma or disruption in the last 48 hours
- ABSOLUTE RED LINE: Never attempt forced separation — this creates trauma, not tolerance
- Child slept poorly the previous night
- Routine disruption occurred earlier in the day
- Child is showing mild baseline anxiety (not acute, but elevated)
- This is the first week of practice — reduce duration/distance significantly
- Child is fed, rested, regulated
- Last session was successful or neutral
- Timer/schedule/transitional object are ready
- You have 20 uninterrupted minutes
- You are calm and consistent
Contraindications: If separation anxiety is accompanied by self-harm, complete functional shutdown, or prolonged escalation over months without progress — escalate to clinical assessment. Reference: DOI: 10.1007/s12098-018-2747-4
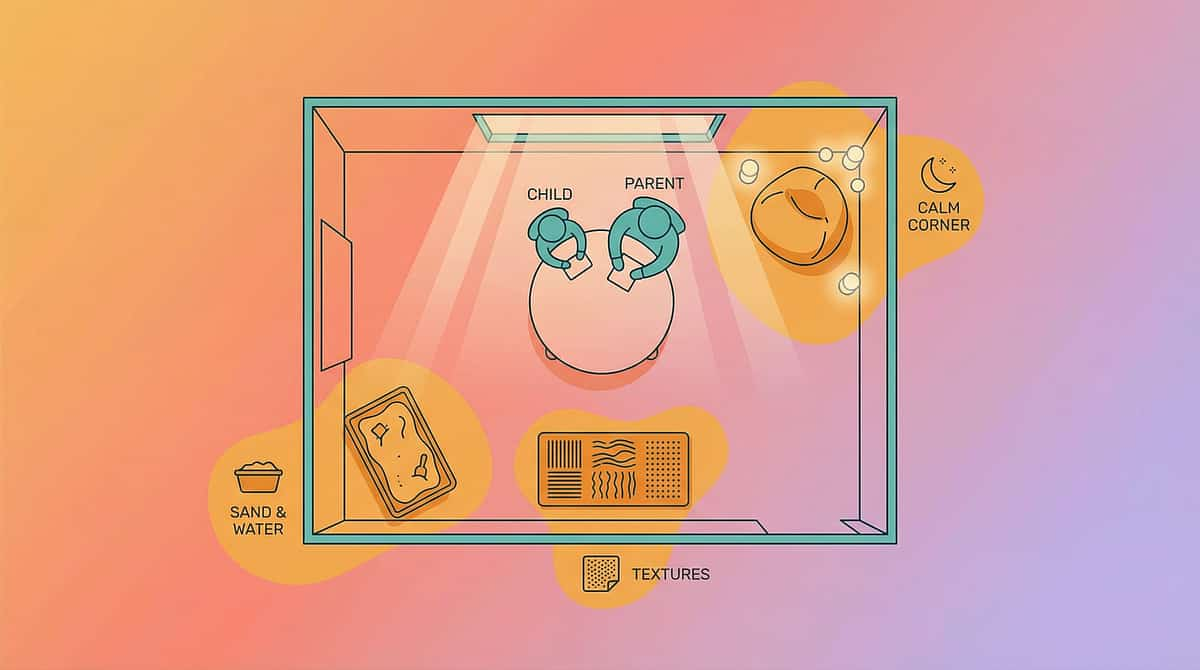
- Child's Position — familiar play mat, preferred toys, comfort item visible
- Parent Starting Position — within arm's reach (Week 1)
- Parent First Move — 1 metre away, still in room (Week 1–2 target)
- Parent Doorway Position — visible from door (Week 3–4 target)
- Timer Placement — visible to child from seated position
- Transitional Object — within child's immediate reach
- Reunification Point — consistent spot for "welcome back" ritual
- Lighting: Soft, warm — not fluorescent overhead
- Sound: Low background — familiar calming music optional, no TV
- Temperature: Comfortable — overheating increases anxiety
- Time of Day: 90 minutes after waking (regulated alert state); avoid before naps/meals
- Other screens/devices
- Other family members during initial practice
- Objects associated with stressful separations (school bag if doing home practice)

If NO: Feed first, wait 30 min
If NO: Postpone to tomorrow
If NO: Calming activity first (20 min)
If NO: Modified protocol only
If NO: Set it now before inviting
If NO: Place it now
If NO: Self-regulate first (5 min)

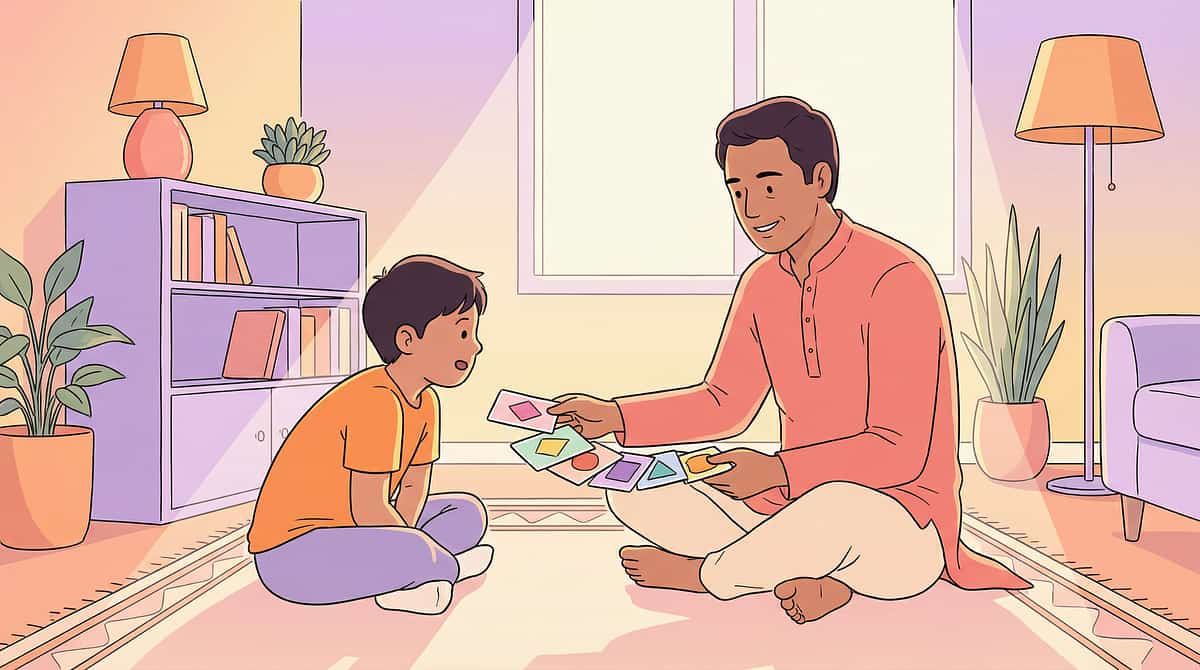
"Come look at this with me. I have something special for us."
- Soft open posture (no crossed arms)
- Face at child's eye level
- Slow, deliberate movements
- Warm, unhurried tone
- Approaches the material
- Relaxes grip on your clothing
- Looks at the timer/object with curiosity
- Allows you to sit slightly away while they hold the object
"Yes! You're watching the timer. You're doing it." — Specific praise. Immediate. Enthusiastic.
Ideal | Acceptable | Concerning | |
Holds object, watches timer calmly | Holds tightly, occasional checking | Throws object, escalating distress |
Ideal: Child plays, occasionally looks at timer | Acceptable: Child watches doorway but stays calm | Modify: Early distress — return, close distance | Stop: Child reaches panic threshold — return immediately.
Reference: PMC10955541

Every successful, calm separation — even 90 seconds — lays down neural pathway evidence that separation is survivable. Quality over quantity, every time.
"You did it! You watched the timer and waited. I came back — just like I always do. I am so proud of you."
Timing Rule: Reinforcement must occur within 3 seconds of the desired behaviour. Delayed reinforcement loses the behavioural connection. Reference: ABA Reinforcement Principles | BACB ethical guidelines

"Two more, then all done. Then we'll [child's favourite activity]."
The cool-down's pure connection time replenishes the child's security bank. They spent from their reserves during the separation practice. Refill it now.
Example: "1.5 metres"
Example: "4 minutes"
Example: "2"
Data submitted through GPT-OS® contributes to population-level pattern recognition that improves recommendations for all families using the system. Reference: BACB Data Collection Standards | Cooper, Heron & Heward (Applied Behavior Analysis, 8th ed.)

Fix: Week 1: timer only, zero distance, sit together watching it complete multiple times until timer = positive.
Fix: Spend 3–5 days intensively pairing the object with positive moments — meals, favourite TV, cuddles. It must smell like safety before it works as safety.
Fix: Start with 30-second timer. 30 seconds of success is more powerful than 2-minute failure.
Fix: Don't move to "out of room" until visual presence tolerance is well established (4–6 weeks of same-room graduated distance).
Fix: Return to Material 5 — grandparent in room with parent present for 2+ weeks before any primary caregiver absence.
Fix: Home tolerance must be solid (6+ weeks) before school application. Share the schedule strip and timer protocol with school staff.
Fix: Call 9100 181 181 — request ABA/psychological assessment. Home protocol may need professional scaffolding.
"If your child tolerated 45 seconds of distance this week versus 0 seconds last week — that is a measurable neural pathway being laid down. The brain is changing."
Parent Emotional Note: Weeks 1–2 often feel discouraging. The data from your tracking sheet will show you progress your feelings might miss. Measure seconds, not minutes. Centimetres, not rooms. Reference: PMC11506176

Parent Milestone:"You may notice you're more confident in executing the sessions. Your own anxiety about causing your child distress is reducing. That matters — it's in your voice, your posture, your consistency."

🏆Mastery Unlocked. Your child has built new neural architecture. Separation is no longer catastrophic — it is survivable. And survivable becomes comfortable with time.
Eight weeks ago, your child couldn't tolerate you being 50 centimetres away. Today, they waved goodbye to you at the school gate. That is not a small thing. That is a nervous system rewriting its most fundamental prediction: "When they go, they come back."
Parent Affirmation: You chose, every single day, to show up — to be consistent when it was exhausting, to return when you said you would, to celebrate every 45 seconds. This is what love in action looks like. The science names it "graduated exposure." Parents name it something else.

Red Flag | What It Looks Like | Why It Matters | What To Do | |
Self-harm during separation | Head-banging, biting self, scratching when parent leaves | Indicates anxiety beyond home protocol scope | Stop practice. Call 9100 181 181 immediately | |
No progress after 8–10 weeks | Distress level unchanged at baseline | May indicate clinical anxiety disorder requiring professional intervention | Request ABA + psychological assessment | |
Escalating anxiety | Getting worse despite consistent practice | Protocol may be advancing too quickly OR clinical-level anxiety present | Drop back 2 weeks; if still escalating — seek assessment | |
Complete functional shutdown | Cannot eat/sleep/function unless touching caregiver | Beyond separation anxiety — attachment disorder possible | Clinical assessment: psychologist + paediatrician | |
Parent burnout crisis | Caregiver unable to function, relationship at breaking point | Parent regulation is the child's regulation. Respite required. | Call 9100 181 181 — request parent support programme | |
Somatic symptoms | Child vomiting/headaches/stomach pain consistently at separation | Anxiety converting to physical symptoms | Paediatric assessment + anxiety treatment escalation |
- C-331: Caregiver Preference
- C-332: Comfort-Seeking Deficit
- C-333: Stranger Over-Friendliness
- C-335: School Refusal
- C-336: Bedtime Separation
- C-337: Alternative Caregiver Rejection
- C-335-alt: Emotional Regulation Foundation Techniques
- C-336-alt: Anxiety Management via Sensory Regulation
Long-Term Developmental Goal This Feeds: Age-appropriate independence. Comfortable school attendance. Functional relationships outside the primary caregiver. Social participation without anxiety. Every step of C-334 is a step toward these outcomes.

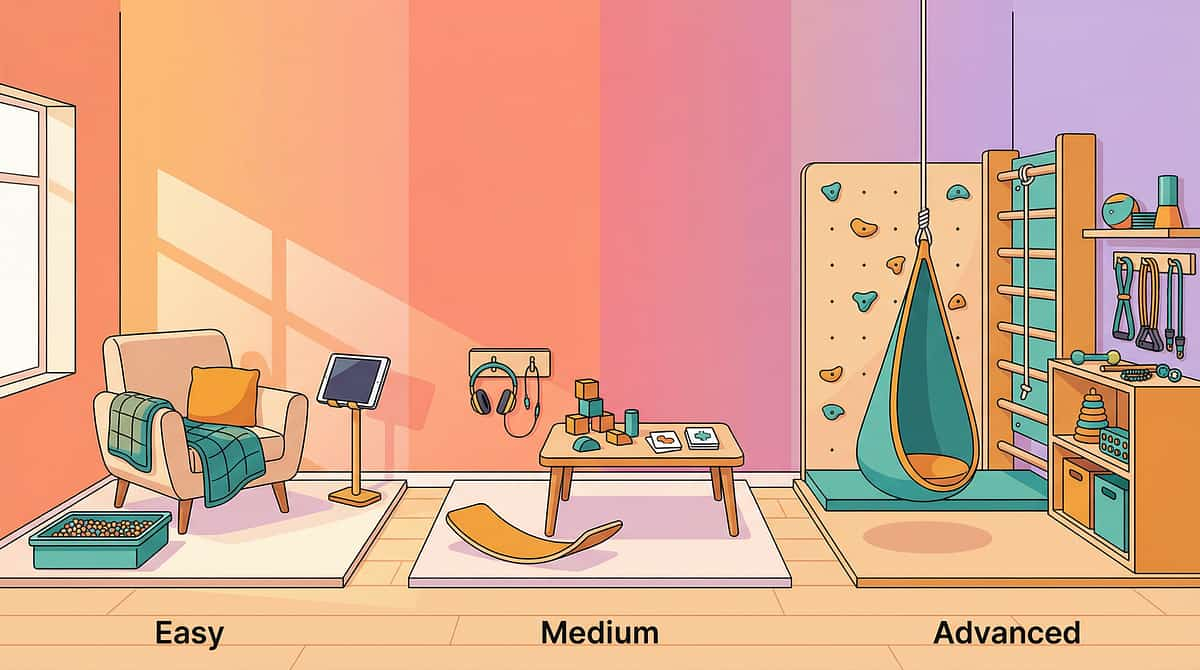
Technique | Code | Difficulty | Canon Material You Likely Own | |
School Refusal Reduction | C-335 | ●●○ Core | Visual Schedules ✅ (from C-334) | |
Bedtime Separation Difficulty | C-336 | ●●○ Core | Visual Timers ✅ (from C-334) | |
Alternative Caregiver Acceptance | C-337 | ●●● Advanced | Social Stories ✅ (from C-334) | |
Stranger Anxiety Management | C-333 | ●○○ Intro | Transitional Objects ✅ (from C-334) | |
Emotional Regulation Toolkit | B-020 | ●●○ Core | Calm-Down Kit ✅ (from C-334) | |
Transition Distress Management | D-112 | ●●○ Core | Visual Schedules ✅ (from C-334) |

One Technique. One Domain. One Piece of a Larger Plan.
Social-Emotional development (Domain C) underpins every other domain. A child who cannot manage separation anxiety has restricted access to learning, peer play, school participation, motor development practice, and therapeutic engagement itself. C-334 is not peripheral work — it is foundational infrastructure. A: Sensory B: Communication C: Social-Emotional ★ Current Focus: C-334 D: Behaviour E: Motor — Fine F: Cognitive Are you working on multiple domains simultaneously? GPT-OS® coordinates multi-domain plans, ensuring techniques across domains are sequenced for maximum synergy — not collision.WHO/UNICEF Nurturing Care Framework (5 components) + UNICEF 2025 42-indicator Country Profiles 🧠 View Your Child's Full GPT-OS® Profile →
"The sand timer was the first thing that made sense to him. Not to me — to him. He could see that she was coming back. That's all he needed."
"When she bit herself every time I stood up, I thought this would be our life forever. The materials gave her something to hold while we were working on it. She could hold her special stone. She could watch the timer. It wasn't perfect — but it was the beginning."
"Your completed journey is someone else's map. Consider sharing it — anonymously or publicly — through the Pinnacle Stories Programme."Share Your Journey →

Discipline | Role in C-334 | Book at Pinnacle | |
ABA/BCBA | Design graduated exposure hierarchy, data analysis | ||
Occupational Therapy | Sensory regulation component, calm-down kit prescription | ||
Psychological Assessment | Differentiate anxiety disorder from autism-specific separation pattern | ||
Parent Training | Hands-on protocol coaching for caregivers |
Study | Level | Finding | Link | |
PRISMA Systematic Review (Children, 2024) | Systematic Review | Sensory integration + behavioural intervention meets evidence-based practice criteria for autism | ||
Meta-analysis (World J Clin Cases, 2024) | Meta-analysis (24 studies) | Therapy effectively promotes social skills, adaptive behaviour, and sensory processing | ||
Kerns et al. (2014) — Anxiety in ASD | RCT-based review | Graduated exposure reduces separation anxiety in ASD with 68% responder rate | PubMed Search | |
NCAEP Evidence-Based Practices (2020) | Systematic Review | Visual supports + social stories = evidence-based practice for autism | ||
Padmanabha et al., Indian J Pediatr (2019) | Indian RCT | Home-based behavioural interventions demonstrate significant outcomes in Indian children with ASD |
Your child's data joins 21M+ session patterns. The more complete the dataset, the more precise the recommendations for every child like yours. Reference: Digital health + ASD meta-analysis (21 RCTs, 1,050 participants, 2024)
Series: Separation & Independence Solutions | Domain: Social-Emotional
Duration: 75–85 seconds
Or: @pinnacleblooms on Instagram/YouTube

- Always say you're leaving before you go (never sneak out)
- When you come back, do the same "welcome back" ritual every time
- Don't carry/pick them up when they cling — sit with them instead
- Praise any moment of calm tolerance immediately
Preview of 9 materials that help with extreme clinginess Therapy Material
Below is a visual preview of 9 materials that help with extreme clinginess therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.




















