

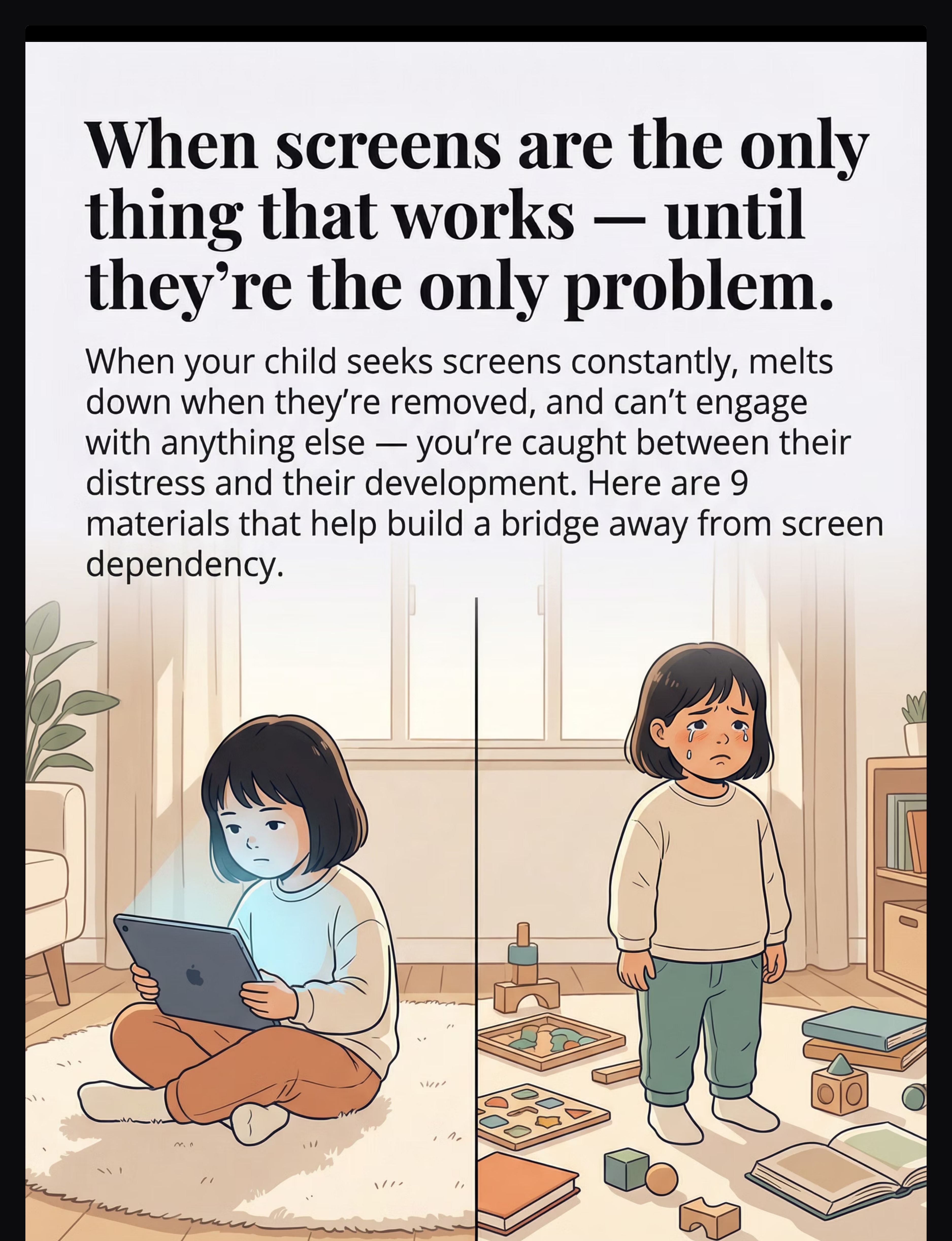
"The brain that seeks screens intensely is often the same brain that, with the right support, becomes intensely focused on music, art, science, or storytelling."


Study | Finding | Source | |
PRISMA Systematic Review (2024) | Sensory integration intervention is evidence-based practice for ASD across 16 studies (2013–2023) | PMC11506176 | |
Meta-analysis (World J Clin Cases, 2024) | Sensory integration effectively promotes social skills, adaptive behaviour, and sensory processing across 24 studies | PMC10955541 | |
Indian RCT (Padmanabha, 2019) | Home-based sensory interventions showed significant measurable outcomes in Indian paediatric population | DOI: 10.1007/s12098-018-2747-4 | |
NCAEP (2020) | Visual supports and behavioural strategies classified as evidence-based practices for autism | National Clearinghouse on Autism | |
WHO/UNICEF CCD Package | Age-specific caregiver interventions across 54 LMICs show measurable developmental outcomes | PMC9978394 |

"You are not building a screen-free child. You are building a child for whom screens are one option among many."
# | Material | What It Replaces | Price Range | |
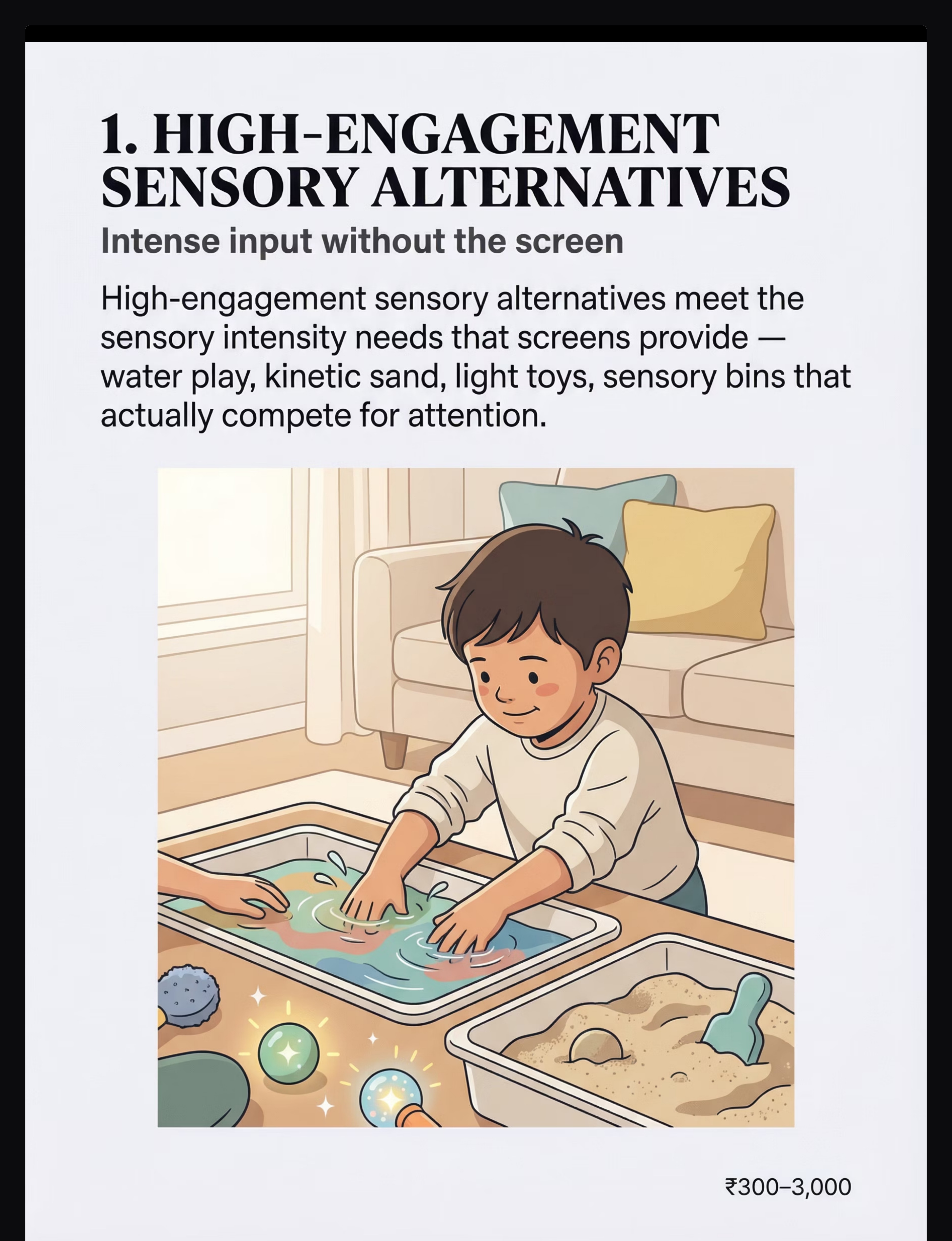
1 | High-Engagement Sensory Alternatives | The sensory intensity screens provide | ₹300–3,000 | |
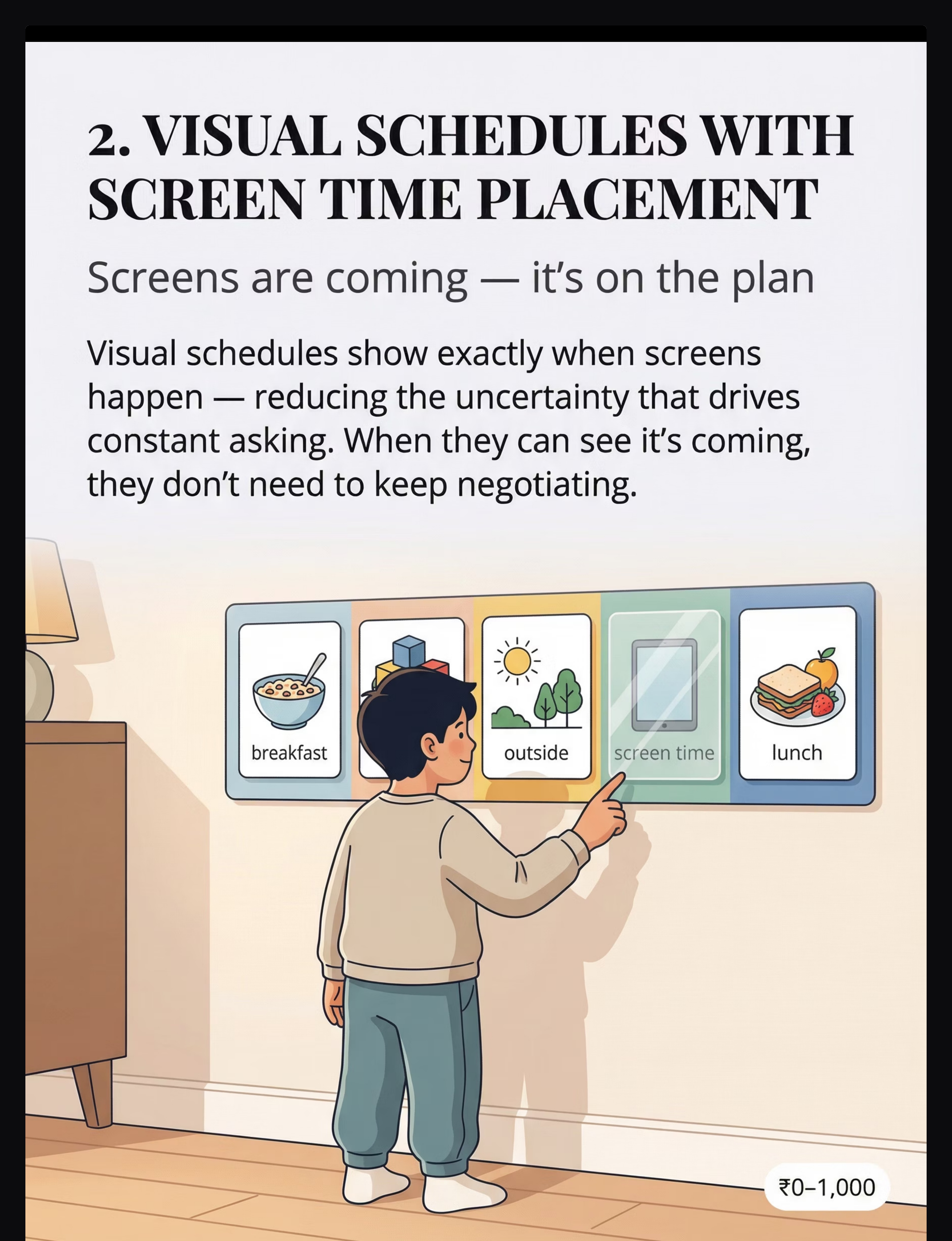
2 | Visual Schedules with Screen Time Placement | The uncertainty that drives constant asking | ₹0–1,000 | |
3 | Transition Supports & Timers | The meltdown when screens end | ₹500–2,000 | |
4 | Interactive Physical Play Equipment | Passive screen absorption | ₹2,000–20,000 | |
5 | Cause-and-Effect Toys & Games | The immediate feedback loop | ₹500–3,000 | |
6 | Special Interest Materials (Non-Screen) | The screen as content delivery | ₹300–5,000 | |
7 | Social & Interactive Games | Solitary screen engagement | ₹300–2,000 | |
8 | Emotional Regulation Toolkit | Screens as the only calming tool | ₹300–2,000 | |
9 | Parent-Child Connection Activities | What screens can never provide | ₹0 |

Material | Buy This | Make This (Free/Low Cost) | |
Sensory Alternatives | Kinetic sand, light-up toys | Water basin + food colouring, rice sensory bin, mud kitchen outside | |
Visual Schedule | Velcro schedule board | Printed photos on cardboard, drawn symbols on paper | |
Transition Timer | Time Timer visual clock | Phone timer propped visibly, hand-drawn countdown chart | |
Physical Play | Mini trampoline | Couch cushion obstacle course, dance party, outdoor park | |
Cause-Effect Toys | Marble run, light-up buttons | Light switches (supervised), kitchen timer, ball-in-box drops | |
Special Interest | Commercial figurines, books | Library books, printed pictures for collage, themed sensory bin | |
Social Games | Board games, card games | Hide and seek, building with household objects, cooking together | |
Regulation Toolkit | Calm-down jar kit | DIY glitter jar (water + glitter glue), pinwheel, heavy blanket | |
Connection Time | N/A — this is time, not a product | 15 minutes of fully present, child-led play daily |
- Child's meltdowns are self-injurious (head-banging, biting self, extreme aggression)
- Screen removal has triggered dangerous behaviours (running away, throwing objects at others)
- Sleep is severely disrupted (under 6 hours per night for extended period)
- Child has stopped eating adequately or regressed significantly in toileting
- You suspect underlying autism, ADHD, or anxiety not yet professionally diagnosed
- Meltdowns regularly last over 30 minutes
- Child has been using screens 8+ hours/day for over 6 months
- Only one parent is implementing (inconsistency reduces effectiveness)
- Other major stressors in the family (moving, new sibling, school change)
- Child is under age 2 — immediate OT consultation recommended
- Child is 2–12 years old
- Screen-seeking is intense but not dangerous
- Child has some capacity for alternative engagement with support
- Both caregivers can implement with some consistency

The Right Environment Prevents 80% of Session Failures
Remove from Space All screens (including parent's phone — put it away visibly) Screen-adjacent items (remotes, chargers, tablet stands) Distracting background noise (TV off, music off unless planned) Other children if they have their own screen access Add to Space Prepared sensory alternative (already set up, not in packaging) Visual schedule displayed at child's eye level Timer already running or visible Transition activity ready for session end Regulation toolkit within reach 5 Key Positions Position 1: Sensory bin — within child's reach Position 2: Visual schedule — at child's eye level on wall Position 3: Timer — visible to both child and parent Position 4: Regulation toolkit — within arm's reach Position 5: Next activity — already set up before session ends Parent State Check Are you regulated? Anxious or frustrated parents escalate situations. Do you have 20–30 minutes? Don't start if you'll be interrupted. Is this a reasonable time of day? Avoid hungry, tired, or ill states. PMC10955541 Sensory Integration Theory — Ayres

Indicator | GO ✓ | MODIFY ⚠️ | POSTPONE ✗ | |
Child is fed (within 2 hours) | Full meal | Snack only | Hungry | |
Child is rested | Normal sleep | Slightly tired | Overtired | |
Child is physically well | Healthy | Mild symptoms | Sick | |
Child's arousal level | Calm-alert | Slightly elevated | Already dysregulated | |
Recent screen time | None in 1 hr | 30 min ago | Just ended | |
Recent stressor | None | Minor upset | Major meltdown today | |
Parent availability | Full 20–30 min | 10–15 min | Less than 10 min |
"Never push through when the child isn't ready. A poor session teaches that the activity is aversive."

"Hey, I set up something really cool. Want to come see?"
(Do NOT explain what it is. Mystery creates intrigue. Let the sensory appeal speak.)




□ Sensory Alternative □ Visual Schedule
□ Transition Timer □ Physical Play
□ Cause-Effect □ Special Interest
□ Social Game □ Regulation Toolkit
□ Connection Time
□ 1 — Refused completely
□ 2 — Brief engagement (under 3 min)
□ 3 — Engaged with support (5–10 min)
□ 4 — Engaged independently (10+ min)
□ 5 — Led the activity (initiated or extended)
□ Major meltdown (30+ min recovery)
□ Significant protest (15–30 min)
□ Moderate protest (5–15 min)
□ Minor protest (under 5 min)
□ Accepted calmly

- Child explores new materials briefly before asking for screens again
- Visual schedule reduces some negotiation (not all)
- Transition timer acknowledged but doesn't yet prevent meltdowns
- Some days are worse than the day before — this is normal (extinction burst)
- Occasional 3–5 minute engagement without prompting
- Independent extended play
- Meltdown-free transitions
- Spontaneous choice of non-screen activities
- Consistent engagement across materials
"Parent Milestone — Week 1–2: You successfully offered an alternative at least 5 times this week. That's the entire goal. Not mastery — offering."
"Parent Milestone — Weeks 3–4: You maintained consistency through the hardest phase. You noticed and celebrated at least 3 specific positive behaviours this week. The relationship is strengthening."

- First time child engaged with a non-screen activity for 5+ minutes
- First time child checked the visual schedule independently
- First time a transition went without a full meltdown
- First time child reached for a regulation tool independently
- First time child initiated a non-screen activity without prompting
- First time child said "okay" to "not right now" about screens
- First time screens were just one part of the day, not the whole day
- First week you consistently implemented the visual schedule
- First session where you genuinely enjoyed playing with your child
- First day where you didn't feel like every moment was a screen battle
- Screen removal consistently triggers self-injury (head-banging, biting, hitting self)
- Child's sleep has reduced to under 6 hours/night persistently
- Child has stopped eating adequately or shown significant weight change
- Meltdowns have escalated in frequency or intensity after 4 weeks of consistent intervention
- Child shows signs of significant anxiety or depression unrelated to screen times
- 8 weeks of consistent implementation with no observable change
- Screen use is escalating despite structured limits
- Child's development appears to be regressing in language, motor, or social skills
- Parent is experiencing burnout that prevents consistent implementation
- You suspect autism, ADHD, or sensory processing disorder not yet diagnosed





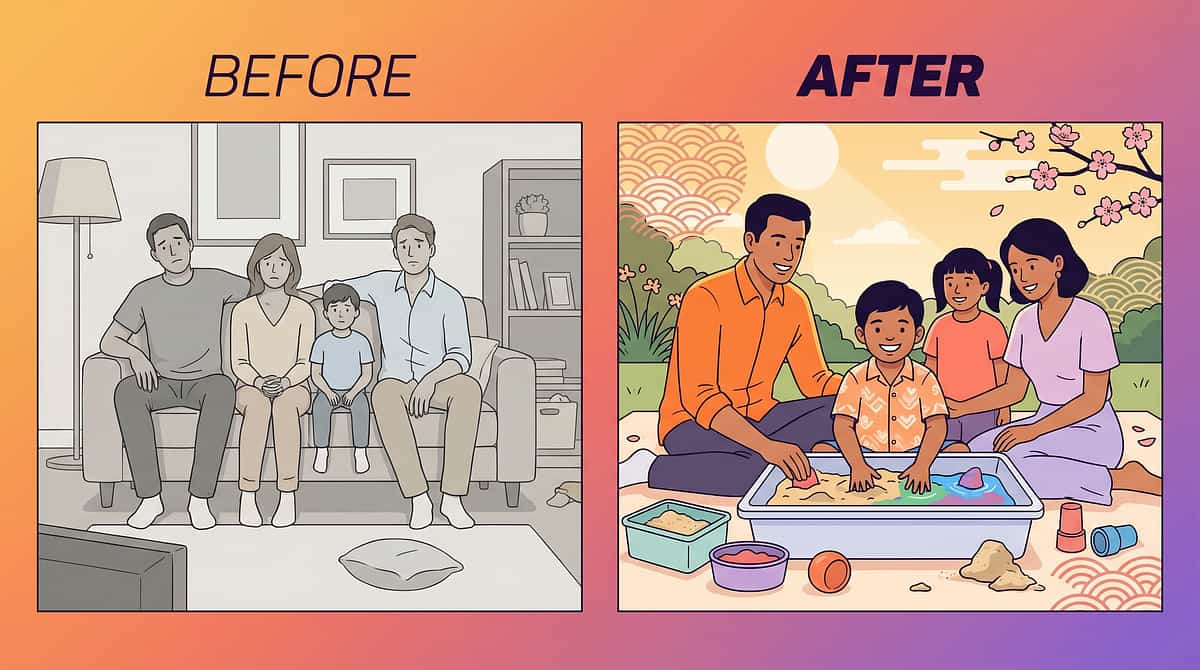
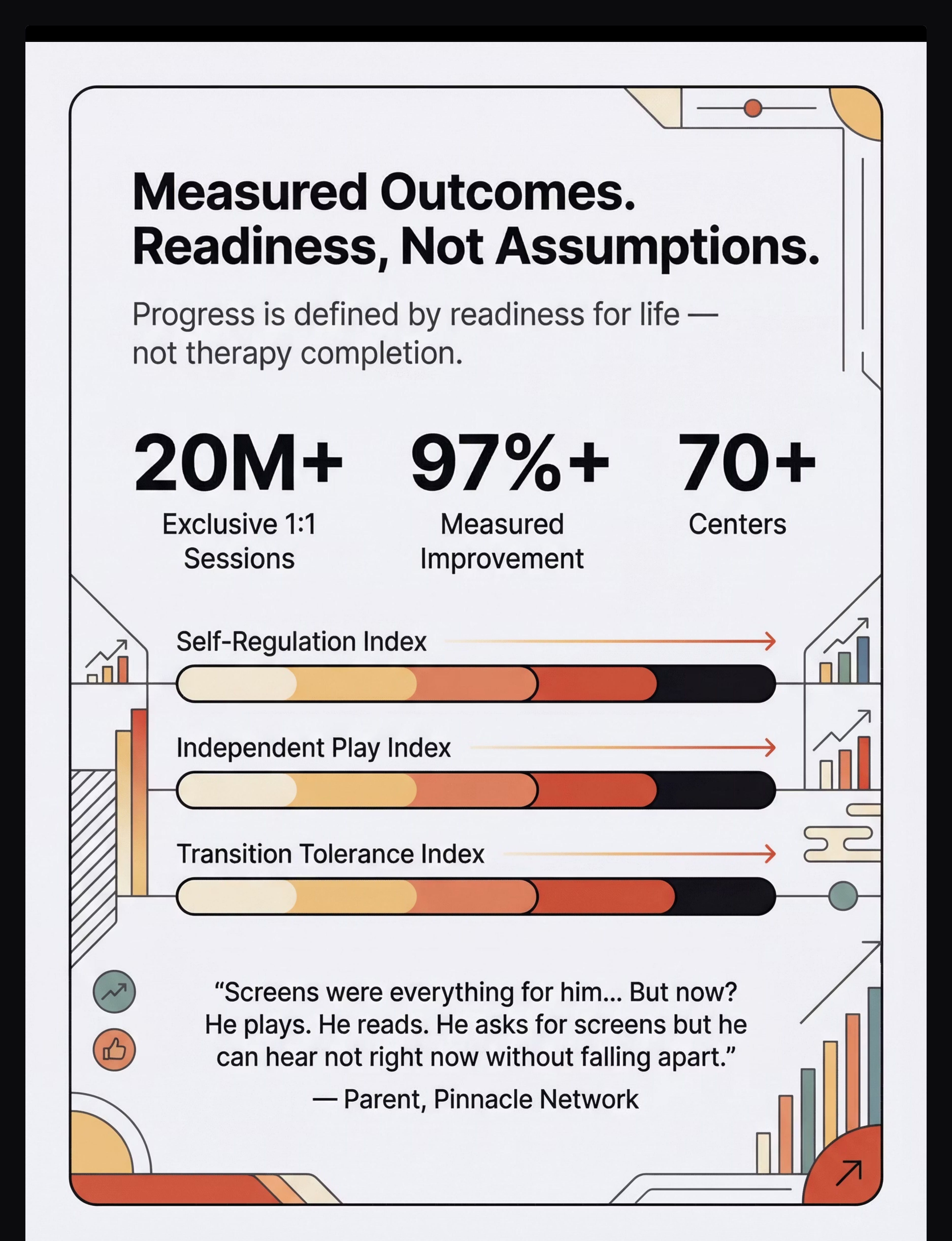
"He plays. He reads. He asks for screens but he can hear 'not right now' without falling apart. He has other things that matter to him now. Screens are still part of his life — but they're not the only thing anymore."
— Parent, Pinnacle Network (Hyderabad Centre)
"What these families discovered — and what we see consistently — is that the goal isn't restriction. It's expansion. When the world becomes more interesting and more predictable, screens become less of an obsession and more of an activity."
— Senior OT, Pinnacle Blooms Network

"Your experience — even now, in the middle of it — helps other families who are just beginning. Consider sharing your journey."


- Your spouse or co-parent
- Grandparents who care for your child
- Your child's teacher or school counsellor
- Domestic help or nanny
- Other family members who may provide screen access

"Your child's brain is plastic. The window is open. Every day of consistent support is a day of neural pathway building that compounds over time."
Preview of 9 materials that help with excessive screen seeking Therapy Material
Below is a visual preview of 9 materials that help with excessive screen seeking therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.








We do not publish strategies we have not deployed. We do not cite research we have not validated. We do not make promises our data does not support.
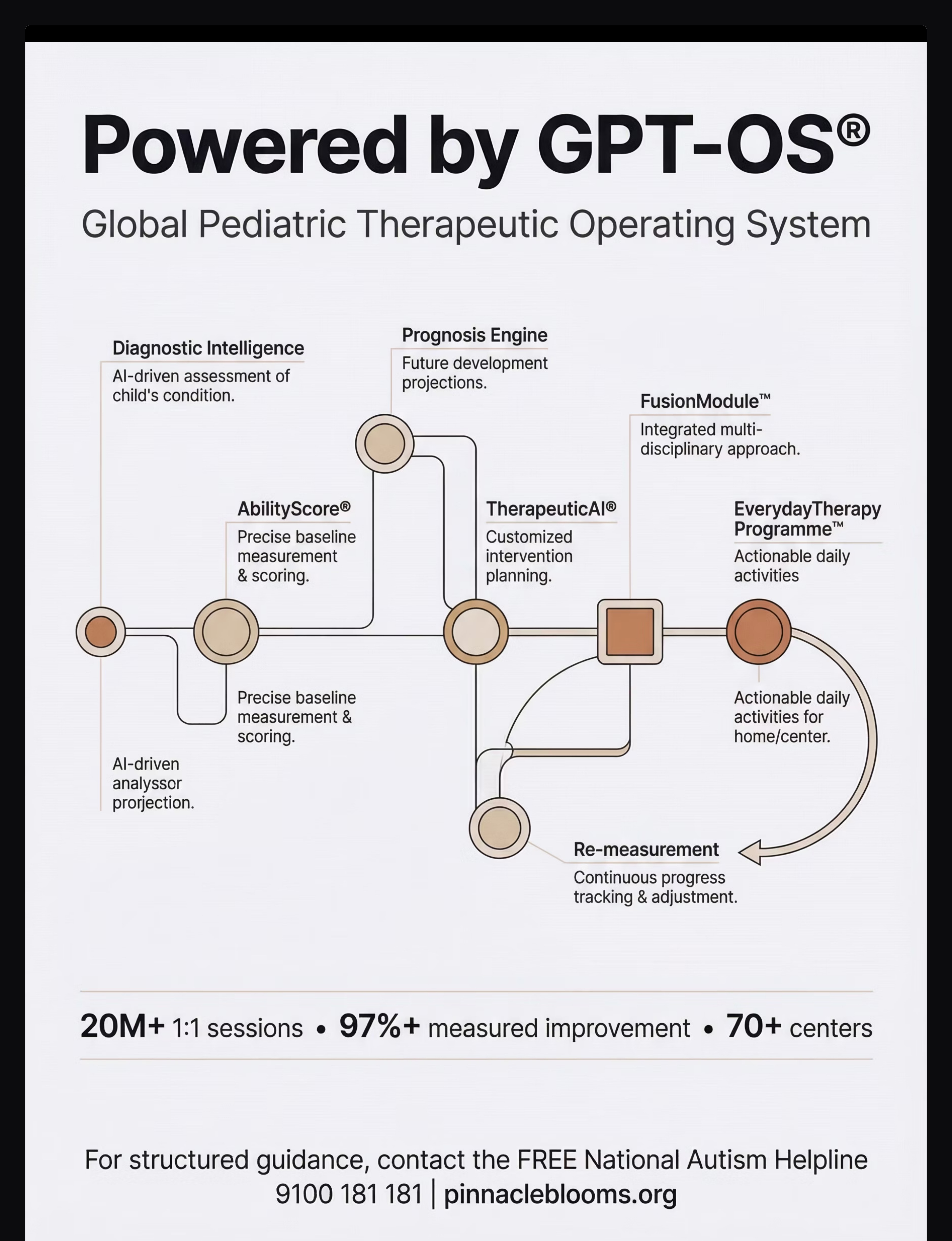
20M+ sessions. 97%+ measured improvement. 70+ countries. This is not aspiration. This is our operating record.
A-065: Difficulty Transitioning Between Activities
techniques.pinnacleblooms.org/sensory-behavioral/transition-difficulties-A-065
You already own the Transition Timer and Visual Schedule — you're halfway there.
For families in India and 70+ countries — always free, always available
© 2026 Pinnacle Blooms Network®, unit of Bharath Healthcare Laboratories Pvt. Ltd. All rights reserved.
CIN: U74999TG2016PTC113063 | DPIIT: DIPP8651 | MSME: TS20F0009606 | GSTIN: 36AAGCB9722P1Z2