
They Play Beside Other Children. But Never Truly With Them.
"He plays alongside other kids at every birthday party, every playdate, every school recess — but the play never becomes shared. He stays in his world while they build theirs."
"You are not failing. Your child's social brain is navigating a system that doesn't yet have all its wiring in place. This is teachable. This is reachable. You are exactly where you need to be."
— Pinnacle Blooms Consortium | OT + SLP + ABA + SpEd + NeuroDev
— Pinnacle Blooms Consortium | OT + SLP + ABA + SpEd + NeuroDev
You've watched it happen dozens of times. The other children form a circle, negotiate a game, assign each other roles, laugh at something in the shared story they're creating together. Your child is three feet away — and three worlds apart. Playing beside them, not with them.
This is called cooperative play skill deficit — and it is not isolation, stubbornness, or indifference to friendship. It is an unmet developmental need that the brain can learn to meet, with the right materials and the right approach.
Social Play Solutions Series
Episode C-316
Age 3–10 years
1 in 36 Children Has Autism. Most Struggle With Cooperative Play.
The challenge you're watching is not rare — it's one of the most common developmental frontiers in paediatric therapy worldwide. Every number below represents a family that knows this exact morning, this exact playdate, this exact heartache — and every number also represents a child who found their way to shared play with the right support.
1 in 36
ASD Diagnosis Rate
Children diagnosed with autism globally (CDC 2023)
80%
Social Play Difficulty
Of children with ASD who experience cooperative play challenges
21M+
Therapy Sessions
Delivered by Pinnacle Blooms Network® across this exact challenge
97%+
Improvement Rate
Measured across Pinnacle's social skills interventions via GPT-OS®
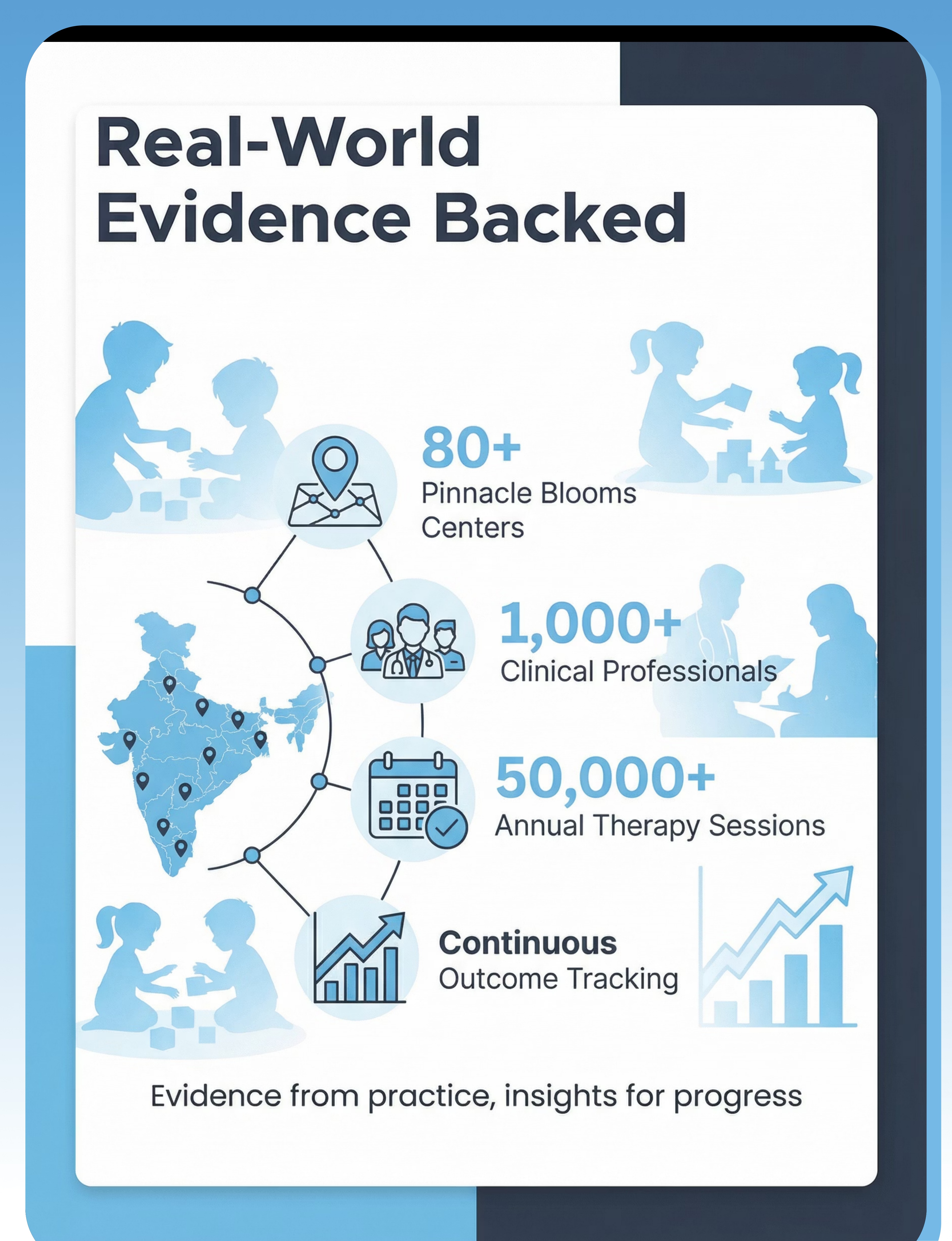
India is home to an estimated 8–10 million children with autism spectrum disorder and an additional 12 million children with developmental delays that affect social participation. Cooperative play deficit is among the top-three presenting concerns at all 70+ Pinnacle Blooms Network® centres.
Sources: PRISMA Systematic Review (2024): PMC11506176 | Meta-analysis, World J Clin Cases (2024): PMC10955541 | WHO/UNICEF CCD Package: PMC9978394 | Lancet India (2019)
Cooperative Play Is One of the Most Complex Things the Human Brain Does
What looks like "just playing together" requires six separate neural systems working in concert. When your child plays cooperatively, their brain must simultaneously manage all of the following — in real time, with another unpredictable human being.
1
Prefrontal Cortex
Executive function, turn-taking regulation, impulse control — wait, it's not your turn
2
Mirror Neuron System
Perspective-taking, imitation, reading others' intentions — what are they trying to do?
3
Limbic System
Emotional regulation during unpredictable peer interaction — don't melt down
4
Superior Temporal Sulcus
Social cue processing, joint attention — what does their face mean right now?
5
Cerebellum + ACC
Timing and sequencing of social responses, conflict monitoring — now it's my turn
This is a system, not a choice. Cooperative play deficits occur when neural architecture is under-connected, over-sensitive, or differently organised. Therapy creates new pathways. Materials are the training ground. You are the coach.
Play Develops in Stages. Your Child Is at a Waypoint, Not a Dead End.
The foundational science of play stages — first documented by Mildred Parten in 1932, confirmed across 90 years of developmental research — shows that cooperative play is the final destination of a developmental journey, not a starting point.
Chronological age does not equal developmental play stage. A 7-year-old may developmentally be at the parallel play stage — this is not regression, it's a starting point. Intervention meets the child at their current stage, not their birthday.
ASD
Autism Spectrum Disorder
ADHD
Impulse control challenges
SPD
Sensory Processing Differences
DLD
Developmental Language Disorder
Anxiety
Around social unpredictability
Children who struggle with cooperative play may be navigating one or more of the above — all are welcome here, all are reachable.

Clinically Validated. Home-Applicable. Parent-Proven.
The cooperative play materials on this page are drawn from evidence-based practice research spanning 90 years of developmental science and 21 million therapy sessions. This is not anecdote — it is Level I evidence in your hands.
Study | Key Finding | Source | |
PRISMA Review (2024) | 16 studies confirm structured cooperative play is EBP for ASD | PMC11506176 | |
Meta-analysis (2024) | 24 studies: promotes social skills + adaptive behaviour | PMC10955541 | |
JASPER RCT, Kasari (2012) | Significant cooperative play gains via joint attention + symbolic play | J Child Psychol Psychiatry | |
Padmanabha et al. (2019) | Home-based structured interventions: significant outcomes in India | DOI: 10.1007/s12098-018-2747-4 |
Key finding in one sentence: Structured cooperative play intervention using specific materials, delivered consistently by informed caregivers, produces measurable improvements in social participation within 6–12 weeks.

Cooperative Play Facilitation Through Structured Material Scaffolding
Parent-Friendly Alias: "Building Bridges Through Play" — The 9-Material Toolkit
Cooperative play is not a single skill — it is a complex orchestra of at least six cognitive and social capacities working simultaneously: perspective-taking, flexible thinking, impulse control, communication, emotional regulation, and theory of mind. When any of these is underdeveloped, cooperative play breaks down.
This technique uses nine strategically chosen material categories to scaffold each component independently, then together. Used consistently in structured home sessions, they create the neural pathways, behavioural patterns, and social confidence that make genuine peer collaboration accessible.
🎯 Domain
Social Play & Peer Interaction (SOC-PLY)
👶 Age Range
3–10 years
⏱️ Session Duration
15–30 minutes
📅 Frequency
3–5 × per week
💪 Evidence Grade
Level I — Systematic Reviews + RCTs
🏠 Setting
Home (primary), Centre (supported)

Five Therapy Disciplines. One Child. Completely Convergent.
The Pinnacle Blooms Consortium delivers this technique across all disciplines simultaneously through the FusionModule™ — because cooperative play is not an OT problem or an ABA problem. It is a whole-brain problem that needs a whole-consortium solution.
ABA/BCBA — Primary Lead
Designs the structured reinforcement schedule, task analysis of cooperative play steps, data collection system, and behavioural shaping sequence. BCBA defines mastery criteria and prompting hierarchy.
Occupational Therapist
Assesses sensory processing contributions to cooperative play avoidance. Addresses proprioceptive and tactile tolerance required for physical proximity during play.
Speech-Language Pathologist
Teaches the specific language of cooperative play: "Can I play too?", "My turn", "Let's make…". Addresses pragmatic language — understanding unwritten social communication rules.
Special Education Teacher
Creates visual scripts, social narratives, and rule-based structures that reduce the cognitive load of cooperative play. Supports executive function through predictable play frameworks.
NeuroDevelopmental Paediatrician
Monitors overall developmental trajectory, medication management if applicable, and provides AbilityScore® baseline and progression benchmarks.
"When your OT, SLP, ABA, and SpEd all deliver consistent language, consistent structure, and consistent materials — the brain integrates. Siloed therapy fragments. FusionModule™ converges." — Pinnacle Blooms Consortium Clinical Advisory
Precision Intervention: Every Material Has an Exact Target
This is not "activities to try." This is a clinical targeting map — nine materials, six skill domains, one convergent outcome: your child playing truly, joyfully, with another person.
Primary Target | Observable Behaviour Indicator | Timeline | |
Turn-Taking | Child waits without grabbing or melting down | 2–4 weeks | |
Shared Goal Coordination | Contributes to joint project without hijacking | 4–8 weeks | |
Role Negotiation | Accepts and maintains a role assigned by peers | 4–8 weeks | |
Collaborative Problem-Solving | Suggests solutions rather than quitting | 6–10 weeks | |
Joining Ongoing Play | Initiates joining peers with appropriate language | 6–12 weeks | |
Managing Disappointment | Recovers from loss or plan-change within 2 minutes | 4–8 weeks |

Material 1: Cooperative Board Games
Structured Cooperation
₹800–2,000
Primary Target: Shared Goals + Emotional Regulation
What They Are
Games where everyone is on the same team — working together against the game itself. Examples: Hoot Owl Hoot, Outfoxed, Race to the Treasure, Stone Soup, Mermaid Island, Cauldron Quest. Win together or lose together.
Clinical Function
Eliminates competition anxiety while building all cooperative play components. Shared winning creates positive emotional associations with collaboration. The brain experiences teamwork as rewarding — not threatening.
Material 2: Multi-Builder Construction Sets
Natural Collaboration Necessity
₹1,500–4,000
Primary Target: Shared Goal Coordination + Physical Interdependence
What They Are
Projects too big for one person: fort building kits, giant cardboard construction, large-scale LEGO projects (70+ pieces), team marble run builders, multi-person structure kits.
Clinical Function
Creates ecological demand for cooperation. When one child must hold while another connects, cooperation is structurally required — not asked for. Child experiences the neurological reward of shared creation without the abstract demand to "be cooperative."
DIY Version (₹0)
Blanket + chairs + pillows fort that requires 2 people to build. Cardboard boxes for a castle. The principle — not the product — is the active ingredient.

Material 3: Complementary Role-Play Sets
Natural Interdependence Through Roles
₹600–1,500
Primary Target: Role Negotiation + Perspective-Taking
What They Are
Doctor/hospital sets, restaurant/kitchen sets with customer role, veterinarian + pet owner sets, store/shopping with seller and buyer roles. Dramatic play where each role requires the other — a doctor without a patient is playing alone.
Clinical Function
Social scripts embedded in roles reduce the cognitive load of cooperative play. The child accesses social language through the character, not directly. The structure of the scenario guides collaboration organically.
DIY Version (₹0)
Rolled-paper stethoscope, cardboard medicine boxes, a teddy bear as patient. Shoe box as restaurant counter. The role structure drives cooperation — props are triggers, not the technique.

Material 4: Team Challenge and Relay Kits
Physical Cooperation with Immediate Feedback
₹500–1,500
Primary Target: Physical Cooperative Action + Concrete Feedback
What They Are
Parachute activity sets, team relay equipment, cooperative challenge cards, group movement games. Physical activities where children instantly see how their cooperation affects outcomes — collaboration becomes concrete and visible.
Clinical Function
Embodied cooperative learning. Children who struggle with abstract social demands often succeed when cooperation is physically experienced and immediately visible. The body teaches what the mind cannot yet access.
DIY Version (₹0)
Old bedsheet held by 4 corners — roll a ball across it together. Balloon keep-up game. Human chain obstacle course. Physical cooperation demand is identical regardless of equipment quality.

Material 5: Visual Turn-Taking Systems
Structure That Removes Conflict
₹200–600
Primary Target: Turn-Taking + Impulse Control
Sand timers show exactly how long a turn lasts. Turn tokens pass from child to child. The system decides — not the children, not the adults. Conflict disappears because no one can argue with a timer.
What They Are
Sand timer sets (1, 2, 3, 5-minute options), turn token systems, My Turn / Your Turn cards, sharing wheels, visual turn schedules with photo cards.
Clinical Function
Externalises executive function demands. The child's prefrontal cortex doesn't have to hold turn-sequencing in working memory — the system holds it. This is the most clinically powerful material for impulse control and turn-waiting.
DIY Version (₹0)
Phone timer + visual countdown drawn on paper. Popsicle sticks with names for turn order. "My Turn" card cut from cardboard. The externalised turn-structure is the clinical active ingredient.

Material 6: Cooperative Play Social Stories
Making Unwritten Rules Explicit
₹200–500
Primary Target: Joining Play + Communication Scripts
What They Are
"How to Join Play That's Already Happening" story, "Taking Turns" illustrated books, "Sharing and Cooperation" narrative guides, play problem-solving story books.
Clinical Function
Social stories make the unwritten rules of cooperative play explicit. How do you ask to join? What if someone has a different idea? Stories provide scripts for situations that previously produced shutdown. Read the story 50 times — the script becomes automatic.
DIY Version (₹0)
Parent-drawn 4-panel comic: "When I want to play, I say 'Can I play too?'" Photos of your child with caption cards. Personalisation with photos of your child is actually MORE effective than published stories.

Material 7: Collaborative Art Projects
Creative Cooperation + Shared Ownership
₹300–800
Primary Target: Contribution Without Dominance + Shared Pride
What They Are
Long paper rolls for group murals, pass-around collaborative drawing sets, collective collage kits, round-robin story creation cards, mosaic tile collaboration sets. Creative projects designed for multiple contributors — where everyone adds their part to create something no one could make alone.
Clinical Function
Shared ownership creates positive emotional valence around cooperative effort. The child experiences the joy of co-creation — a feeling that becomes the intrinsic motivator for future cooperative attempts. The result belongs to everyone.
DIY Version (₹0)
Old newspaper + poster paint: giant group painting on floor. Pass-around drawing — 30 seconds each, pass the paper. Shared creation principle requires only paper and imagination.

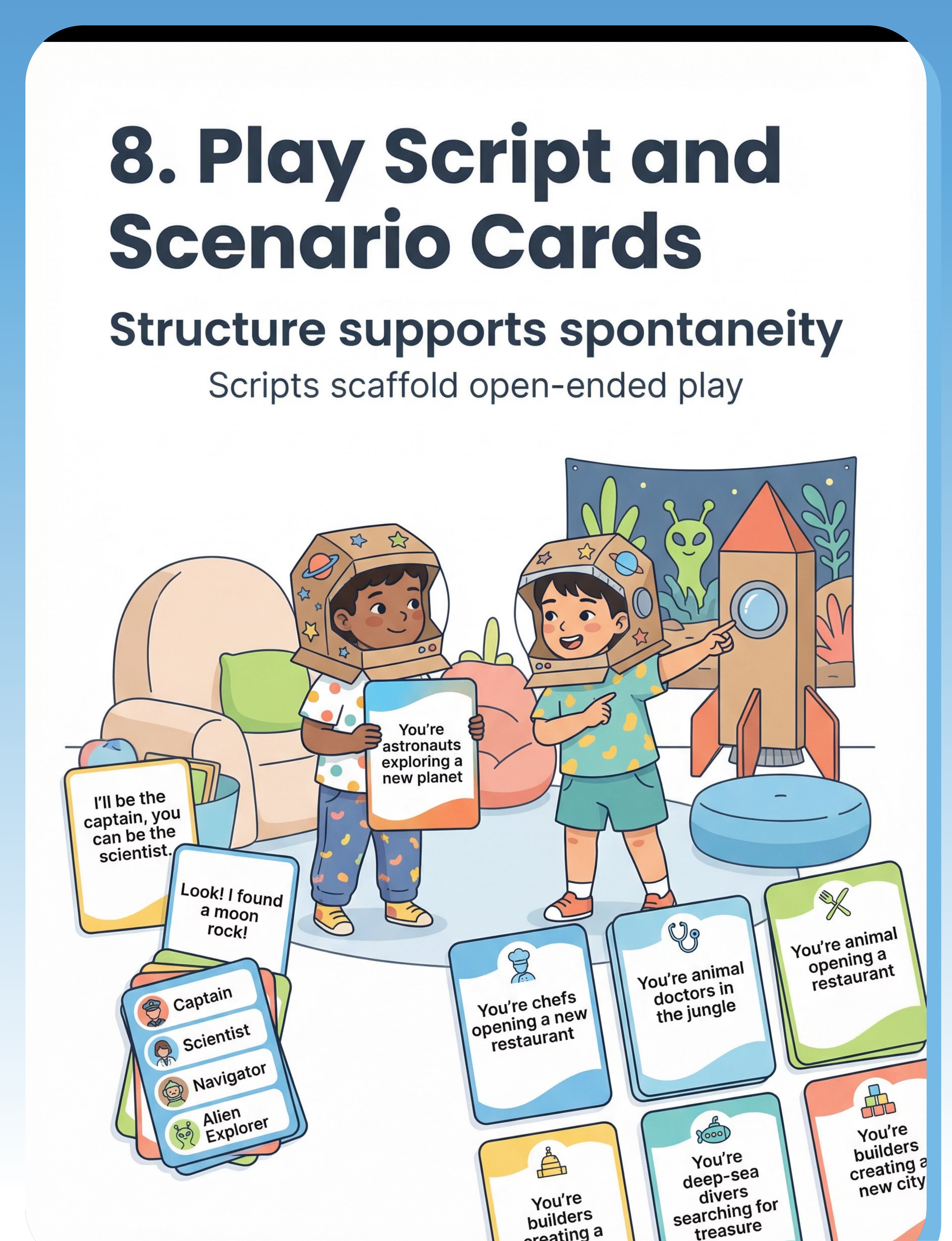
Material 8: Play Script and Scenario Cards
Structure Supporting Spontaneity
₹200–500
Primary Target: Reducing Cognitive Load of Open-Ended Play
What They Are
Play scenario prompt cards ("You're astronauts on a new planet"), dialogue starter cards ("I'll be the captain, you be the scientist"), role assignment cards, story starter cards, play theme card decks.
Clinical Function
Reduces executive function demands at play initiation. Most cooperative play breakdowns happen in the first 30 seconds. Cards eliminate the blank-page paralysis — the cards carry the initiation burden while the child carries the relationship.
DIY Version (₹0)
Cut paper slips: write 10 scenarios. "You're pirates finding treasure." "You're chefs making a cake." Laminate with tape. Your child's preferred scenarios work BETTER than generic cards.

Material 9: Partner and Two-Player Games
Dyad Before Group
₹400–1,200
Primary Target: Foundational Cooperative Experience
What They Are
Two-player cooperative games, partner puzzle sets (each player holds half the pieces), two-person challenge activities, cooperative seesaw toys, partner building challenges.
Clinical Function
Collaboration starts with one person. A dyad is cognitively simpler than a group. Once the child experiences successful partnership with one peer, group cooperation becomes achievable. Graduated exposure to cooperative demands: fewer competing intentions, simpler turn sequencing, lower emotional regulation demand.
DIY Version (₹0)
Partner puzzle: cut any A4 picture into 2 — each person holds half and must cooperate to complete it. Dyadic cooperation structure costs ₹0.

Every Material on This Page Has a ₹0 Version
WHO/UNICEF Equity Principle: evidence-based intervention must be available to every family regardless of income. The clinical outcome of household-material sessions is comparable when the therapeutic principle is applied correctly.
Zero-cost starter session — TONIGHT: Take a ball, a bowl, and a sibling or parent. "Let's see how many times we can pass it without dropping it. We're a TEAM." You've just delivered a Level I evidence-based cooperative play intervention with materials you already own.
Material | Commercial Version | Household DIY Version | Why It Works | |
Cooperative Board Games | Hoot Owl Hoot (₹1,200) | Modify any competitive game: "Let's ALL try to beat our BEST score together" | Same shared goal structure | |
Multi-Builder Sets | Fort building kit (₹2,000) | Blanket + chairs + pillows fort requiring 2 people to build | Scale creates cooperation necessity | |
Role-Play Sets | Doctor kit (₹800) | Rolled-paper stethoscope, cardboard boxes, teddy bear as patient | Role structure drives cooperation | |
Team Challenge Kits | Parachute set (₹1,000) | Old bedsheet held by 4 corners — roll a ball across together | Physical cooperation demand is identical | |
Visual Turn-Taking | Sand timer (₹400) | Phone timer + popsicle sticks with names for turn order | Externalised structure is the active ingredient | |
Social Stories | Published book (₹350) | Parent-drawn 4-panel comic with photos of YOUR child | Personalisation is MORE effective | |
Collaborative Art | Art supply kit (₹600) | Old newspaper + poster paint on floor; pass-around drawing | Shared creation requires only paper + imagination | |
Play Script Cards | Card deck (₹400) | Cut paper slips with 10 child-preferred scenarios, laminated with tape | Preferred scenarios work better than generic | |
Partner Games | Commercial game (₹800) | Cut any A4 picture into 2 — each person holds half | Dyadic cooperation costs ₹0 |
The Pre-Session Safety Gate: Read Before Every Session
These protocols are derived from Pinnacle's clinical safety standards across 70+ centres and 21 million therapy sessions. Safety is not a box to tick — it is the foundation of every therapeutic interaction.
🚫 RED: ABSOLUTE STOP — Do Not Proceed
• Child is in active meltdown or has not recovered within the last 30 minutes
• Child is showing signs of illness (fever, lethargy, pain)
• Child has expressed clear distress about playing with the peer partner today
• The peer partner is significantly older, more dominant, or has been unkind recently
• Session environment is chaotic, crowded, or has recent conflict energy
• You (the facilitating parent) are in significant distress
• Child is in active meltdown or has not recovered within the last 30 minutes
• Child is showing signs of illness (fever, lethargy, pain)
• Child has expressed clear distress about playing with the peer partner today
• The peer partner is significantly older, more dominant, or has been unkind recently
• Session environment is chaotic, crowded, or has recent conflict energy
• You (the facilitating parent) are in significant distress
⚠️ AMBER: MODIFY — Proceed with Adjustments
• Child is mildly dysregulated → Switch to dyad session with parent as play partner
• Child is tired → Shorten to 10 minutes, use highest-motivation material only
• Child had a difficult school day → Begin with 5 minutes of preferred solo play first
• Peer partner is less familiar → Use highly structured material only
• Child had a cooperative play failure recently → Use Partner Game or Team Art to rebuild confidence
• Child is mildly dysregulated → Switch to dyad session with parent as play partner
• Child is tired → Shorten to 10 minutes, use highest-motivation material only
• Child had a difficult school day → Begin with 5 minutes of preferred solo play first
• Peer partner is less familiar → Use highly structured material only
• Child had a cooperative play failure recently → Use Partner Game or Team Art to rebuild confidence
✅ GREEN: PROCEED — Safety Gate Passed
• Child is calm, alert, and fed
• No recent significant emotional event (within 90 minutes)
• Peer partner is familiar, similar age, and positively associated
• Environment is prepared · Parent is regulated and present
• Child is calm, alert, and fed
• No recent significant emotional event (within 90 minutes)
• Peer partner is familiar, similar age, and positively associated
• Environment is prepared · Parent is regulated and present
📞If in doubt: FREE Helpline 9100 181 181 — 24×7, 18+ languages. Stop the session if child becomes physically aggressive, shows extreme distress, or self-injurious behaviour.

The Right Space Makes Cooperation 3× More Likely
Research confirms that environmental setup directly determines session success. Spatial precision prevents 80% of session failures before they begin.
Remove Distractors
All screens off. Distracting toys out of sight. Door closed if possible. Visual clutter increases cognitive load.
Define the Play Zone
Use a rug, a low table, or taped boundary on the floor. Children need to know "we play HERE."
Position Materials Between Children
Not in front of one child — in the centre, equally accessible to both. This prevents territorial claiming.
Parent Behind and to the Side
Never between the children. The goal is peer interaction, not adult-child interaction. You are the coach, not the player.
Visual Schedule + Timer Visible
Even a simple 3-icon schedule (Start → Play → Finish) reduces anxiety. Both children must see the timer — removes "but it's MY turn" debates.
Reinforcement Ready but Hidden
Reward stickers/tokens nearby but not IN the play area — revealed upon achievement, not before.
Environmental settings: Natural light preferred · Quiet to low-level background, no TV · Comfortable temperature · Minimal clutter. Sensory Integration Theory (Ayres): structured environment is a core therapeutic principle. PMC10955541

60-Second Pre-Flight Check: Go, Modify, or Postpone?
The best cooperative play session is one that starts right. This 60-second assessment determines whether to proceed, adapt, or wait for a better window. There is no shame in postponing — it is clinical wisdom.
✅ Check These Now
□ Child ate a meal or snack within the last 2 hours
□ Child has slept reasonably well
□ No meltdown in the past 60 minutes
□ Child seems regulated (not shutdown or stimming for distress)
□ Play partner is present and in good mood
□ Child has not been recently punished about play
□ Parent has 20–30 minutes of unhurried attention
□ Child has slept reasonably well
□ No meltdown in the past 60 minutes
□ Child seems regulated (not shutdown or stimming for distress)
□ Play partner is present and in good mood
□ Child has not been recently punished about play
□ Parent has 20–30 minutes of unhurried attention
🟢 7/7 — GO
Begin protocol as designed
🟡 5-6/7 — MODIFY
Shorten to 10 min, use simplest material
🟠 3-4/7 — SIMPLIFY
Parent-child dyad only, 5–10 minutes
🔴 0-2/7 — POSTPONE
Not today. Preferred calming activity instead. No guilt.
If POSTPONE: Choose a preferred solo activity — sensory play, favourite book, movement break. Tell the child: "We'll play together tomorrow. Today we're taking care of your body first." This is therapeutic, not avoidance.

Step 1: The Invitation — Begin With Curiosity, Not Commands
Step 1 of 6
"Hey! I found something really cool. Want to come see? It's a game that NOBODY can win alone — you have to have a partner. Can you two be partners today?"
What you're doing neurologically: You are activating the child's approach motivation system (dopaminergic curiosity pathway) before introducing any cooperative demand. The brain moves toward novelty. The cooperation comes after engagement, not before.
Parent Body Language
Crouch to child's level · Genuine smile · Hold the material, don't open it yet · Slight lean toward the other play partner
Acceptance Signals
Child moves toward the material · Eye glance at other child · Any verbal response · Body orientation shifts toward activity
Resistance Responses
"I don't want to" → "You can just watch." · Continues current activity → Leave it; wait 3 minutes. · Meltdown beginning → Postpone.
⏱️ Timing: 30–60 seconds for invitation sequence.

Step 2: The Engagement — Introduce the Material With Wonder
Step 2 of 6
"Look — this game has [describe material simply]. Here's the rule: we're ALL on the same team. We either ALL win together, or we ALL try again together. There's no 'I lose.' Ready to try?"
For Cooperative Board Games
"Let me show you both how this works. We're all trying to [win condition]. Here's what each person does…" Demonstrate one turn yourself first.
For Multi-Builder Construction
"This structure needs one person to HOLD and one person to CONNECT. I wonder who wants which job?" Let children choose roles — agency reduces resistance.
For Turn-Taking System
"This timer is our team referee. When it rings, the item passes. The timer decides — not me, not you — the timer." Externalising authority removes the adult-child power dynamic.
Reinforcement cue: Within 3 seconds of ANY cooperative gesture (looking at each other, handing a piece, saying "your turn") → "YES! That's what teamwork looks like."
⏱️ Timing: 1–3 minutes for engagement establishment.

Step 3: The Therapeutic Action — The Cooperative Play Session
Step 3 of 6
This is where the neural pathway is being built. The core therapeutic action depends on the material in use.
Cooperative Board Games
Each player takes turns. Parent narrates cooperation: "That was brilliant teamwork." Do NOT take over — let the team fail together and try again. The failure IS the therapy.
Multi-Builder Construction
Assign roles: Holder, Connector, Director. Rotate every 5 minutes. Narrate contribution: "The whole structure exists because you needed each other."
Role-Play
Enter the scenario yourself first to model, then step back. Prompt only with questions: "What does the doctor say now?" — never with commands.
Visual Turn-Taking
Start the timer. Do NOT intervene during the wait. The waiting IS the therapeutic dose. When the timer rings: "The timer said it's [name]'s turn! Great waiting!"
Common execution errors: Taking over when children struggle (step back — let them navigate) · Talking too much (use 5-word maximum prompts: "Whose turn is it?") · Stopping when conflict begins (small conflicts ARE the training) · Praising one child more (balance praise equally).
⏱️ Duration: 10–20 minutes for therapeutic action phase.

Step 4: Repeat & Vary — Dosage Is Everything
Step 4 of 6
"3 deeply cooperative repetitions are worth more than 10 forced ones. Your child's nervous system learns from quality engagement, not quantity of exposure."
Material | Target Cooperative Exchanges Per Session | Mastery Marker | |
Cooperative Board Games | 1 full game (5–15 turns per player) | Completes game without quitting | |
Construction Sets | 3 complete build-hold-connect cycles | Accepts partner's role assignment | |
Role-Play | 3–5 role exchanges without script prompting | Initiates interaction within role | |
Turn-Taking | 6–10 full turn sequences | Waits without protest for 2 full turns | |
Art Collaboration | 3–5 contribution cycles | Adds to partner's section without objecting |
Easy Variation
Same material, parent joins as third player to reduce peer-to-peer demand
Standard Variation
Material as designed, minimal prompting
Challenge Variation
Add one new rule or role to the established activity
Novel Variation
Switch to a different material category in week 3–4
Satiation Indicators — When to Stop: Increased redirecting, silly/disruptive behaviour, requests to stop, physical withdrawal. These mean the cooperative learning window is closing. End before meltdown, not after.
Step 5: Reinforce & Celebrate — The Timing Is Everything
Step 5 of 6
ABA Reinforcement Principle: Reinforcement delivered within 3 seconds of the target behaviour increases the likelihood of that behaviour recurring. Immediate, specific, enthusiastic reinforcement teaches everything.
For Turn-Taking
"YOU WAITED! You let [partner] have their turn and you WAITED. That is exactly what teammates do. High five!"
For Shared Building
"Look what you TWO built! Neither of you could have made that alone. You needed each other — and look what happened!"
For Conflict Resolution
"You both wanted to be the doctor. You worked it out. You BOTH found a way. That is incredibly grown-up teamwork."
Reinforcement Type | Examples | Use When | |
Verbal (most common) | Specific praise + name of skill demonstrated | Every cooperative exchange | |
Physical | High five, fist bump, thumbs up (child-chosen) | Mastery moments | |
Token/Sticker | Reward Stickers ₹165 in Reward Jar ₹695 | Session completion | |
Natural | "Look — you made something amazing TOGETHER." | Always |
Celebrate the attempt, not just the success. A child who waited 8 seconds instead of 2 — that is progress. Celebrate the 8 seconds.

Step 6: The Cool-Down — No Session Ends Abruptly
Step 6 of 6
Why This Matters: Post-session dysregulation (meltdowns 5–10 minutes after a session) is often caused by abrupt endings without transition support. The cool-down is not optional — it is clinical.
1
2-Minute Warning
"Two more turns, and then we're going to put things away. Two more!" Hold up two fingers — verbal AND visual transition warning.
2
1-Minute Warning
"One more turn, and then you each pick ONE thing to put away. Who's going first?" Child participation in cleanup creates ownership and reduces session-ending grief.
3
Material Put-Away Ritual
Each child puts away one item. "You both played, you both help put away. That's the team rule." Shared ending, not unilateral stopping.
4
Cool-Down Activity (2 minutes)
Choose ONE: Hand squeeze game (5 squeezes each) · "Name one thing you liked" · Three big breaths together · Child's preferred calming sensory input.
If the child resists ending:"The timer means all done today. The game will be HERE tomorrow. I promise. You can see it before bed if you want to check." (Transition object principle — the game's presence tomorrow is guaranteed.)

60 Seconds of Data Now Saves Hours of Guessing Later
Within 60 seconds of session end, record these data points. This is the difference between guessing at your child's progress and knowing it.
📋 C-316 COOPERATIVE PLAY SESSION LOG
Date: _______ · Time: _______ · Duration: _____ min · Play Partner: _____________ · Material Used: _____________
DATA POINT 1 — TURN-TAKING
□ No turn-taking (grabbed immediately every time)
□ Attempted but required prompting every turn
□ Waited 1–2 turns independently
□ Waited 3+ turns independently ← MASTERY MARKER
DATA POINT 2 — COOPERATIVE EXCHANGES
How many moments of genuine cooperation occurred? _____ (tally)
DATA POINT 3 — EMOTIONAL REGULATION
□ Significant meltdown (session ended early)
□ Frustration expressed but managed
□ Mild frustration, self-recovered
□ No significant frustration ← IDEAL
OVERALL SESSION RATING:
□ Difficult · □ Mixed · □ Good · □ Excellent ← TARGET
Notes — What worked? What didn't? Any breakthrough moment? ________________________
Date: _______ · Time: _______ · Duration: _____ min · Play Partner: _____________ · Material Used: _____________
DATA POINT 1 — TURN-TAKING
□ No turn-taking (grabbed immediately every time)
□ Attempted but required prompting every turn
□ Waited 1–2 turns independently
□ Waited 3+ turns independently ← MASTERY MARKER
DATA POINT 2 — COOPERATIVE EXCHANGES
How many moments of genuine cooperation occurred? _____ (tally)
DATA POINT 3 — EMOTIONAL REGULATION
□ Significant meltdown (session ended early)
□ Frustration expressed but managed
□ Mild frustration, self-recovered
□ No significant frustration ← IDEAL
OVERALL SESSION RATING:
□ Difficult · □ Mixed · □ Good · □ Excellent ← TARGET
Notes — What worked? What didn't? Any breakthrough moment? ________________________

Session Didn't Go Perfectly? Good. That's Data.
"Session abandonment is not failure — it's information. Every difficult session tells the clinician something that a perfect session cannot." Here are the 7 most common challenges and exactly what to do.
🔴 Child Grabbed Every Time
Turn-taking demand exceeded current impulse control. Next session: Shorten turns to 30 seconds. Add physical token for every successful wait — make waiting VISIBLE.
🟠 Child Dominated or Withdrew Entirely
Group demand is currently above threshold. Next session: Switch to dyad (parent as play partner). Master parent-child cooperation first. Peer reintroduced in week 2–3.
🟡 Peer Partner Quit
Insufficient attention to peer's experience. Next session: Brief peer coaching first: "Your job is to be patient AND to have fun. You're the expert player."
🟡 Fixated on Winning Despite Cooperative Game
Rigid thinking — "games have winners." Next session: Avoid all game-format materials. Switch to Collaborative Art or Multi-Builder — no win/lose structure at all.
🟢 Session Lasted 3 Minutes
This IS the baseline — not a failure. Next session: Set a 3-minute TARGET. Get 3 clean cooperative exchanges in 3 minutes and END THERE with celebration. Build from this foundation.
🔴 Parent Anxiety Disrupted Session
Children regulate to the adult's nervous system. Next session: 5 minutes of calm solo activity before facilitating. Regulate yourself, then facilitate.
🚨 Child Severely Distressed
Cooperative play not yet accessible at this demand level. Do not retry for 3 days. 📞 Call 9100 181 181 — consult with your Pinnacle therapist via teleconsultation.
No Two Children Are Identical. Here's How to Customise.
Weeks 1–2
10 minutes maximum. Ends before satiation. Parent as primary play partner.
Weeks 3–4
15–20 minutes if weeks 1–2 were positive. Introduce one peer partner.
Weeks 5–8
20–30 minutes. Introduce novel peer partners. Begin fading parental support.
After Week 8
Natural play opportunities. Facilitated support withdrawn gradually. Real-world generalisation.
Individualised intervention is a core principle across OT (sensory profile), ABA (function-based), and SLP (communication profile) clinical practice. Adjust for the child in front of you — not the profile on a page.

Weeks 1–2: Planting the Seed (Don't Expect the Flower Yet)
Progress Arc — Phase 1
15% of Journey
✅ These ARE Progress in Weeks 1–2
- Child tolerates the cooperative activity for 3 more seconds than the first session
- Child makes eye contact with the play partner even once during the activity
- Child uses the turn-taking system without a meltdown — even if they didn't like waiting
- Child asks "is it my turn yet?" (even impatiently) — they're tracking the turn system
- Child smiles or laughs during even one moment of cooperative play
❌ NOT Expected Yet in Weeks 1–2
- Fluid, spontaneous cooperative play
- Sharing without prompting
- Managing disappointment gracefully
- Initiating play with peers independently
"Weeks 1 and 2 will feel like you're pushing a boulder. The boulder isn't moving yet — but you are changing the ground beneath it. Neural pathways are being created with every session. The visible change comes later. The invisible change is happening NOW."
📅 Session frequency this phase: 3–5 sessions per week, 10–15 minutes each. Source: PMC11506176
Weeks 3–4: The Pathways Are Forming — Watch for These Signals
Progress Arc — Phase 2
40% of Journey
🔵 Anticipation Signals
Child starts asking about the cooperative play session before you initiate it. They remember it. They want it.
🟢 Preference Emerging
Child shows a preferred material or preferred role. This is personalisation — the cooperation is becoming theirs.
🟡 Reduced Resistance
The first 2 minutes of sessions are calmer. Onboarding is faster. The cooperative activity is now associated with positive emotion.
🟠 Spontaneous Generalisation Seeds
Child uses a phrase from role-play or cooperative game in an unrelated context. The learning is transferring.
🔴 Self-Monitoring Emerging
When the child grabs instead of waits, they sometimes catch themselves — or immediately look at the timer. Self-monitoring is emerging.
Parent milestone: You may notice that YOU are more confident too. You know what to say, what to watch for, what's working. This confidence transfers to your child through every co-regulatory interaction.

Weeks 5–8: Mastery Unlocking — Look for the Badge Indicators
Progress Arc — Phase 3
75% of Journey
Mastery Criterion | Definition | Observable Evidence | |
Turn-Taking Independence | Waits for 3+ turns without prompting | No grab attempts; may ask "is it my turn?" verbally | |
Shared Goal Maintenance | Contributes to group project without redirecting | Adds to the shared creation, doesn't start solo project | |
Role Acceptance | Accepts assigned role for 5+ minutes | Stays in character even when it's not "the best" role | |
Conflict Navigation | Manages in-play disagreement without meltdown | Verbally negotiates or accepts resolution within 2 minutes | |
Generalisation | Cooperative play demonstrated with a NEW peer | Skills transfer without needing full protocol scaffolding |
4–5/5 Criteria Met
Progress to C-317 (Imaginative Play) or C-318 (Joining Ongoing Play)
3/5 Criteria Met
Strengthen current level with novel materials and new peer partners
1–2/5 Criteria Met
Return to Act III. Consider clinic consultation. Call 9100 181 181.
Source: PMC10955541 — mastery criteria derived from behavioural measurement standards and social participation index benchmarks.

You Did This. Your Child Plays with Others Because You Showed Up Every Day.
For 6–8 weeks, you set up the space while also managing the rest of family life. You invited cooperation when it would have been easier to let them play alone. You sat through the difficult sessions without giving up. You watched your child struggle — and supported instead of rescuing.
And your child? They discovered that playing with someone else feels good. They built the neural infrastructure for friendship. They learned to wait, even when waiting was hard. They experienced the joy of shared creation.
📸 Capture a moment of your child in genuine cooperative play. Write one sentence: "Before this journey, [this was hard]. Now, [this is possible]." This is your family's evidence-based success story.
Family Celebration Suggestion: Plan a special cooperative activity — a family game night, a shared cooking project, a collective art piece. Make the cooperative play principle the celebration itself.
Even in Progress, Know These Signals
These are specific thresholds — not vague concerns. If you observe these, pause and seek consultation. Trust your instincts. They are clinical instruments.
🚨 Pause and Consult If:
• No interest in peers at all — different from lacking skills; complete indifference to other children's presence
• Aggression is the primary response to any peer interaction despite 4+ weeks of consistent intervention
• Complete inability to share any item under any conditions after 4 weeks
• Significant regression from previously achieved cooperative play skills
• Extreme distress in any social situation — anxiety may be the primary issue
• No interest in peers at all — different from lacking skills; complete indifference to other children's presence
• Aggression is the primary response to any peer interaction despite 4+ weeks of consistent intervention
• Complete inability to share any item under any conditions after 4 weeks
• Significant regression from previously achieved cooperative play skills
• Extreme distress in any social situation — anxiety may be the primary issue
📞 Pinnacle Helpline: 9100 181 181 — 24×7, 18+ languages, FREE. "Trust your instincts. If something feels wrong, pause and ask."
You Are Here. Here Is Where You're Going.
Cooperative play does not exist in isolation — it sits within a carefully sequenced developmental GPS. Every technique before and after C-316 is mapped to your child's exact progress.
What Comes Next: Your 5 Possible Pathways
Based on your child's strongest emerging skills, one of five next-level techniques will be recommended. Each child's path is unique — the GPT-OS® system analyses your session data to suggest the most appropriate next step.
C-317: Imaginative Play
Best if your child has strong language and enjoys pretend scenarios
C-318: Joining Ongoing Play
Best if your child shows strong initiation but struggles to enter existing games
C-319: Turn-Taking in Structured Games
Best if your child can cooperate but needs rule-following support
C-320: Managing Sharing Challenges
Best if sharing objects remains the primary friction point
C-321: Playdate Planning
Best if your child is ready for real-world peer interaction outside the home
What You've Already Unlocked
Before arriving at C-316, your child has already demonstrated mastery of foundational skills. These are not small wins — they are the neurological scaffolding that makes cooperative play possible.
C-314: Understanding Personal Space
Your child can regulate proximity to peers without prompting
C-315: Appropriate Touching
Your child understands and respects physical boundaries in play
C-316: Cooperative Play (Current)
You are here. Building shared goals, shared materials, shared joy.
💡 Pro Tip: Don't rush to the next technique. Mastery at C-316 means your child can sustain cooperative play for 10+ minutes across 3 different materials with 2 different partners. Depth before breadth.
If You Need to Step Back: Supportive Techniques
C-305: Parallel Play Enhancement
If peer readiness is lower than expected
C-308: Joint Attention Activities
If shared attention is the bottleneck
C-311: Imitation Games
If mirroring and modelling is the foundation needed

Real Families. Real Play. Real Change.
Illustrative cases drawn from Pinnacle centre outcomes. Individual results vary. All identifying details anonymised.
Arjun, 6 years — Hyderabad
"Three weeks ago, he called a neighbor boy to the window and said 'Do you want to build something? I need your help.' He needed his help. He knew he needed someone else. For us, that was everything."
Therapist's note: Arjun's transition from parallel to cooperative play was driven by the construction set's ecological demand for collaboration. When the structure was too big for one person, his brain found the motivation to connect.
Meera, 5 years — Bangalore
"She walked up to a girl at the park and said 'I'll be the teacher and you can be the student.' The other girl said yes. They played for 20 minutes. I stood there and didn't cry. Almost."
Therapist's note: Meera's social stories gave her the language. The play script cards gave her the scenario. The materials had given her the words to take the first step.
Rohan, 7 years — Chennai
"He waited for 3 full turns in a board game last week. THREE. I know that sounds like nothing. But for Rohan, that was him climbing Everest."
Therapist's note: Three turns of independent waiting represents multiple neural circuits cooperating: impulse control, working memory, emotional regulation, and trust in the turn system. Rohan climbed Everest.

You Are Not Navigating This Alone
"Isolation is the enemy of adherence. Community is the multiplier of progress." Every family in the Pinnacle network is navigating a version of what you're navigating. Connection accelerates everything.
📱 WhatsApp Parent Group
Parents navigating social play development. Share what works. Ask what doesn't. Get peer support from families 4 weeks ahead of you.
Message "COOPERATIVE PLAY GROUP" to wa.me/919100181181
Message "COOPERATIVE PLAY GROUP" to wa.me/919100181181
💻 Pinnacle Parent Forum
Online forum for the Social Play & Peer Interaction domain. Moderated by Pinnacle clinical team.
pinnacleblooms.org/community/social-play
pinnacleblooms.org/community/social-play
🤝 Peer Mentoring Programme
Connect with a parent who has successfully navigated cooperative play with their child.
pinnacleblooms.org/peer-mentoring
pinnacleblooms.org/peer-mentoring
📍 Local Parent Meetups
Pinnacle centres across 70+ cities host monthly parent support groups. Find yours:
pinnacleblooms.org/centers
pinnacleblooms.org/centers
📞FREE National Autism Helpline: 9100 181 181 — 24×7 · 18+ languages · Completely free. Immediate guidance. AbilityScore® assessment booking. Nearest centre referral.

Your Questions, Answered
Generated from real parent queries at Pinnacle centres and the cooperative play parent community.
Q1: My child is 8 years old and still in parallel play. Is it too late?
No. Play stage development is not locked to chronological age — it is locked to neural readiness. An 8-year-old receiving consistent, evidence-based intervention can develop robust cooperative play skills. The 6–12 week timeline applies regardless of age.
Q2: How do I get my child to share without forcing them?
You don't force — you structure. The Visual Turn-Taking System removes the sharing decision from both the child AND you. The timer decides. Children respond to systems much better than to emotional appeals. Start with 1-minute turns.
Q3: My child plays beautifully with me but not with other children. Why?
Parent-child cooperative play is neurologically simpler. Use the Parent-Child Dyad as the training foundation, then gradually introduce a peer as third participant, then step back. This progression is part of the clinical protocol.
Q4: We tried cooperative board games and it ended in meltdown. Should we stop?
Don't stop — simplify. Switch to Visual Turn-Taking or Partner Games (lower demand), build tolerance there, and reintroduce the board game in week 3–4. See the Troubleshooting card for the complete guide.
Q5: How do I know if my child needs clinic-based therapy vs. home sessions?
If after 6 weeks of consistent home sessions (4× per week) you are not seeing ANY week 3–4 consolidation indicators, seek professional evaluation. When uncertain — call 9100 181 181.
Q6: Can siblings be the play partner?
Yes — siblings often make excellent initial partners. However, peer partners (same-age, unfamiliar children) are important for generalisation, even if siblings work well for initial sessions.
Q7: How many of the 9 materials should I buy?
Start with 3: Cooperative Board Games + Visual Turn-Taking System + Partner Games. These cover the broadest range at the lowest cost. Add materials as mastery develops. You do not need all 9 simultaneously.
Q8: My child's school won't provide support. What do I tell them?
Use this framing: "Cooperative play is a neurological skill, not a social choice. The supports that help include: visual turn sequence during group activities, role assignment before play begins, and specific verbal reinforcement for cooperative behaviours." Download the Teacher Template from the Share card.
Preview of 9 materials that help with cooperative play Therapy Material
Below is a visual preview of 9 materials that help with cooperative play therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.










Link copied!

Cooperative Play Is Learnable. Start Today.
You now have the evidence, the protocol, the materials, and the 6-step execution guide. The only remaining step is starting. Every session plants a seed. Every reinforced cooperative moment builds a neural pathway. Every wait, every shared creation, every "your turn" is your child building the infrastructure for friendship — for life.
📞 FREE National Autism Helpline: 9100 181 181
24×7 · 18+ Languages · Completely Free
Immediate guidance · AbilityScore® assessment booking · Nearest centre referral
24×7 · 18+ Languages · Completely Free
Immediate guidance · AbilityScore® assessment booking · Nearest centre referral
🏛️ PINNACLE BLOOMS NETWORK®
OT • SLP • ABA/BCBA • SpEd • NeuroDev Paediatrics • CRO
WHO-Aligned • UNICEF-Compatible • Evidence-Based
"From fear to mastery. One technique at a time."
OT • SLP • ABA/BCBA • SpEd • NeuroDev Paediatrics • CRO
WHO-Aligned • UNICEF-Compatible • Evidence-Based
"From fear to mastery. One technique at a time."
21M+
Therapy Sessions Delivered
97%+
Measured Improvement Rate
70+
Centres Across India
70,000+
Technique Library
Technique Code: C-316 | Domain: Social Play & Peer Interaction | Series: Social Play Solutions, Episode 316 | Published: 2025 | Version: 1.0
Medical Disclaimer: This content is educational in nature and does not constitute medical advice, diagnosis, or treatment. It does not replace assessment by a licensed developmental specialist, occupational therapist, speech-language pathologist, behavioural therapist, or physician. Cooperative play difficulties may relate to autism spectrum disorder, ADHD, social anxiety, developmental delays, language disorders, sensory processing differences, or other conditions requiring comprehensive professional assessment. Individual results vary. If concerned about your child's developmental progress, consult a qualified healthcare professional.
Bharath Healthcare Laboratories Pvt. Ltd. | Unit: Pinnacle Blooms Network®
CIN: U74999TG2016PTC113063 | DPIIT Recognition: DIPP8651 | MSME: TS20F0009606 | GSTIN: 36AAGCB9722P1Z2
Registered Office: Hyderabad, Telangana, India
© 2025 Pinnacle Blooms Network®. All rights reserved. GPT-OS®, AbilityScore®, TherapeuticAI®, FusionModule™ are proprietary trademarks of Bharath Healthcare Laboratories Pvt. Ltd.
CIN: U74999TG2016PTC113063 | DPIIT Recognition: DIPP8651 | MSME: TS20F0009606 | GSTIN: 36AAGCB9722P1Z2
Registered Office: Hyderabad, Telangana, India
© 2025 Pinnacle Blooms Network®. All rights reserved. GPT-OS®, AbilityScore®, TherapeuticAI®, FusionModule™ are proprietary trademarks of Bharath Healthcare Laboratories Pvt. Ltd.