
9 Materials That Help With Communication Overall
Every Way They Try to Connect Counts — Building Bridges to Understanding
Communication & Understanding
Episode L-994
Ages 18 months–10 years
📞FREE National Autism Helpline: 9100 181 181 | 16+ Languages | 24×7

Act I — The Emotional Entry
The Recognition Moment
"He's four years old and I don't know how to explain what he needs to the world — because he can't tell me either. He pulls my hand, screams, throws himself on the floor in the grocery store. Not because he's spoilt. Because every single thing he wants to say is locked somewhere inside him and no door opens it. The speech therapist called it 'global communication delays.' I called it the most heartbreaking thing I've ever heard — because it wasn't just speech. It was everything. The not-pointing. The not-looking. The not-responding when I call his name. Where do I even begin?"
You are not failing. Your child's nervous system is navigating a world it was not yet wired to map. These materials build every bridge — not just words.
The WHO Nurturing Care Framework (2018) confirms that early identification and caregiver awareness during the critical window from birth to age 3 directly and measurably impacts neurodevelopmental outcomes. You found this resource at exactly the right moment.
SLP
Speech-Language Pathology
AAC
Augmentative Communication
OT
Occupational Therapy
ABA
Applied Behavior Analysis
SpEd
Special Education
You Are Among Millions of Families Navigating This Exact Challenge
1 in 36
Children with ASD
Diagnosed with autism spectrum disorder in the United States
80%
Experience Delays
Children with ASD experience global communication delays affecting ALL channels — not just speech
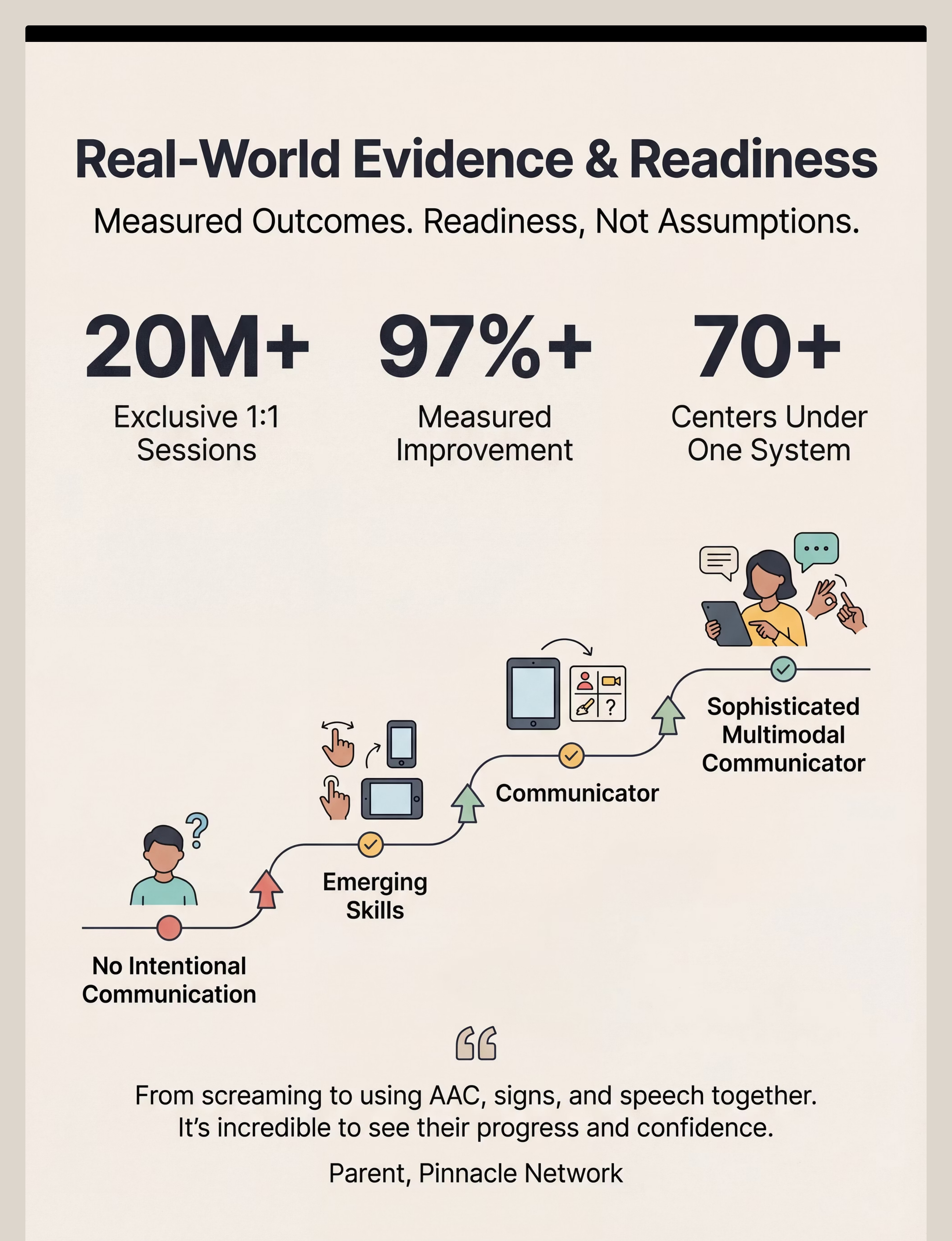
21M+
Sessions Delivered
Therapy sessions delivered by Pinnacle across 70+ centers, 97%+ measured improvement
Global communication delays affect tens of millions of families worldwide. India alone has an estimated 10–18 million children on the autism spectrum, and communication delays are the most common presenting concern across Pinnacle's 70+ clinical centers. The overwhelming majority of parents who sit exactly where you are sitting right now felt precisely what you feel: the isolation, the confusion, and the fierce love that drove them to find answers.
You are not an outlier. You are at the center of a movement. PRISMA systematic review (2024): 80% of children with autism display sensory and communication processing difficulties across multiple modalities simultaneously. References: PMC11506176 | PMC10955541
This Is a Wiring Difference. Not a Behavior Choice. Not Your Failure.
What's Happening in the Brain
Communication delays are rooted in atypical multi-region neural integration — not cognitive or motivational deficits. When your child screams instead of pointing, the neural pathway that converts "I want that" into a coordinated gesture-plus-eye-contact-plus-vocalization is not yet firing in integrated, sequential ways.
These materials work precisely because they build those neural pathways through structured, joyful, repeated practice — using the brain's own neuroplasticity.
Brain Region Breakdown
Brain Region | In Global Communication Delays | |
Auditory Cortex | May over- or under-filter spoken language | |
Wernicke's Area | Slower or atypical processing; understanding lags | |
Broca's Area | Motor speech planning difficulties despite knowing what to say | |
Prefrontal Cortex | Reduced drive to orient toward people as communication partners | |
Cerebellum | Affects gesture, signing, and motor-based AAC access |
Frontiers in Integrative Neuroscience (2020): Comprehensive neurological framework confirms global communication delays are rooted in atypical multi-region neural integration. Reference: DOI: 10.3389/fnint.2020.556660
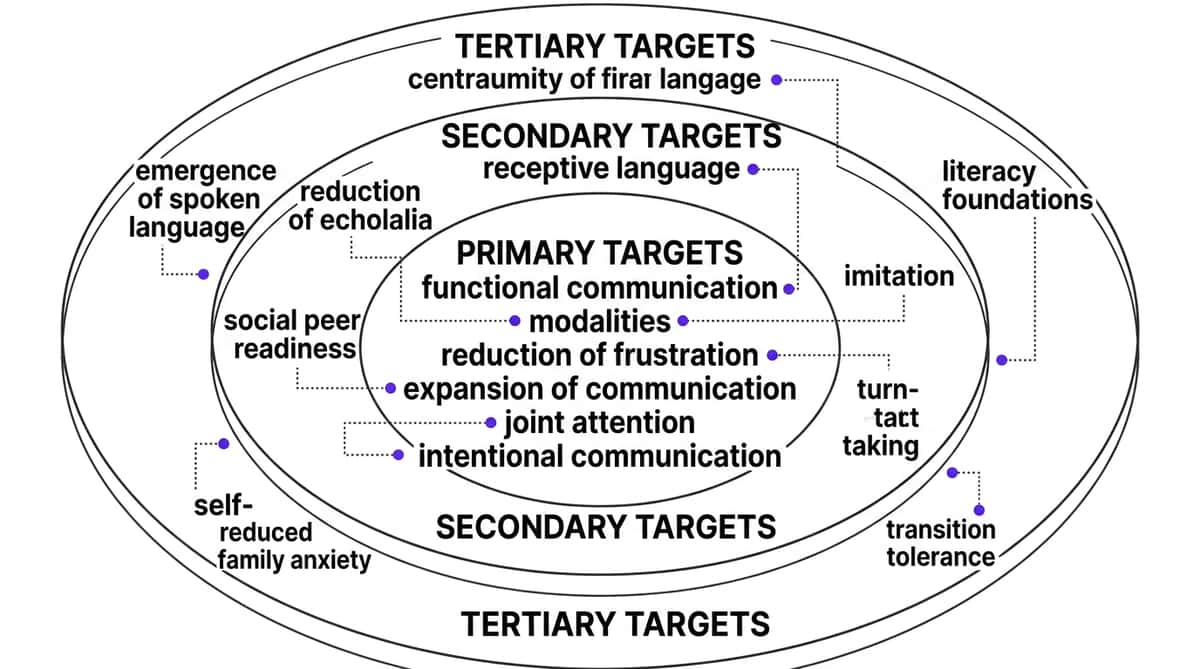
Your Child Is Here. Here Is Where We Are Heading.
Total communication intervention doesn't wait for speech to arrive. It builds every pathway simultaneously — because a child who cannot yet speak can still communicate through signs, pictures, gestures, and devices while speech skills continue to develop. The evidence is clear: multiple modalities support, not replace, the emergence of speech.
Prelinguistic Foundations
Joint attention, intentional communication, turn-taking, imitation (ages 6–12m typically)
Receptive Language
Understanding words, directions, and concepts (continuous development)
Expressive Communication
Vocalizations, gestures, signs, pictures, AAC, and speech (multi-modal)
Pragmatic Language
Requesting, commenting, social exchange (social use of communication)
Communication delays commonly co-occur with sensory processing differences (80%), attention challenges (60%), and motor planning difficulties (40%). This program addresses the intersection. References: PMC9978394 | WHO/UNICEF CCD Package 2023
Clinically Validated. Home-Applicable. Parent-Proven.
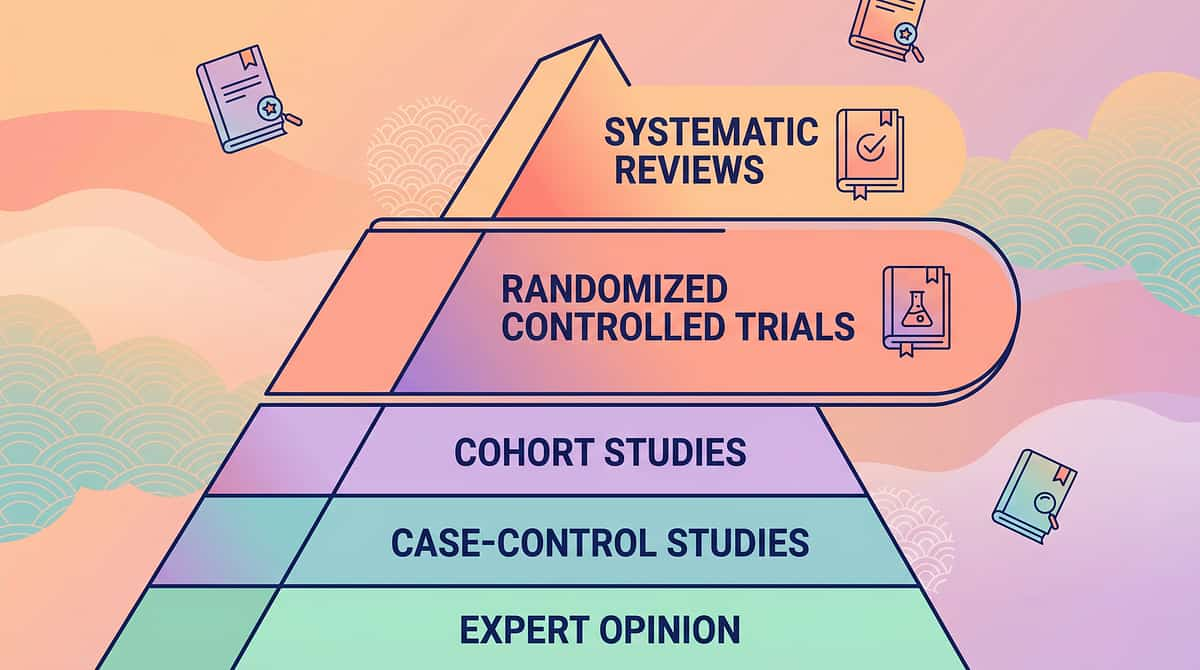
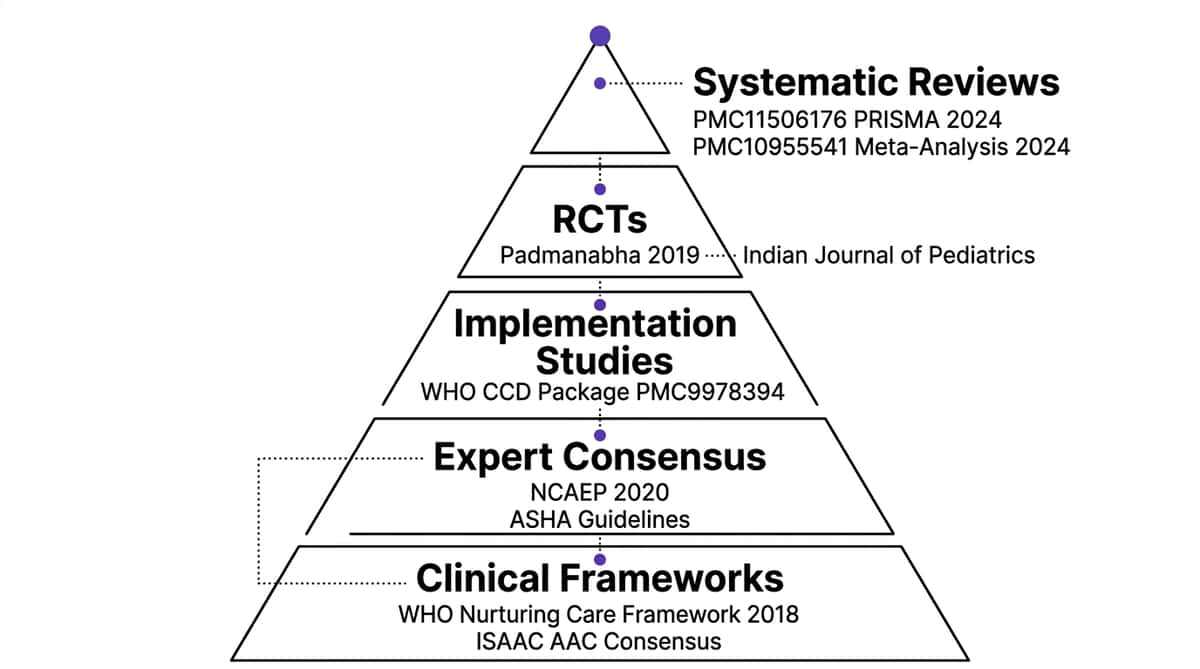
EVIDENCE LEVEL I — Systematic Review + Multi-RCT Meta-Analysis. The highest tier of clinical evidence supports every technique on this page.
Study | Finding | Source | |
PRISMA Systematic Review (2024), 16 studies 2013–2023 | Multimodal communication intervention meets evidence-based practice criteria for ASD | PMC11506176 | |
Meta-Analysis, World J Clin Cases (2024) | Multimodal approach effectively promotes social skills, adaptive behavior, expressive communication across 24 studies | PMC10955541 | |
WHO CCD Package Implementation (2023) | Home-based multimodal caregiver interventions show significant outcomes in 54 countries | PMC9978394 | |
Indian RCT, Padmanabha et al. (2019) | Home-based communication interventions demonstrated significant outcomes in Indian pediatric population | DOI:10.1007/s12098-018-2747-4 | |
NCAEP Evidence-Based Practices Report (2020) | AAC, picture exchange, sign language, and video modeling each independently classified as evidence-based practices | NCAEP 2020 |
"AAC does NOT prevent or delay speech development. Children who use augmentative communication often develop MORE verbal speech — because communication becomes successful and motivating." — Multi-systematic review consensus, International Society for AAC (ISAAC)

Act II — Knowledge Transfer
Total Communication / Multimodal Communication Material Suite
Parent-Friendly Name: "Every Bridge to Connection" — the 9 materials that build ALL communication pathways
Communication is far more than speech. It is the entire system through which human beings send, receive, and share meaning — encompassing prelinguistic foundations (joint attention, intentional communication, turn-taking), receptive language (understanding words and concepts), expressive communication (conveying needs through any modality), and pragmatic social communication (using communication in real social contexts).
When a child experiences global communication delays, multiple components are affected simultaneously. The total communication approach — endorsed by WHO, ASHA, and ISAAC — recognizes that speech is one modality among many, and that providing children with multiple pathways to communicate accelerates rather than impedes speech development.
Foundations
Joint attention, cause-and-effect understanding, turn-taking, sensory regulation
Expressive Modalities
Picture cards, AAC devices, sign language, core vocabulary
Language Development
Interactive books that combine all communication channels simultaneously
Ages: 18 months – 10 years
Session: 10–30 minutes
Frequency: Daily + 2–3 structured sessions/week

These Materials Cross Therapy Boundaries — Because the Brain Doesn't Organize by Therapy Type
🗣️ Speech-Language Pathologist
Primary lead discipline. Designs the total communication system; selects AAC devices; trains caregivers in PECS, core vocabulary, and multimodal strategies; monitors speech emergence.
🧠 ABA / BCBA
Secondary discipline. Establishes functional communication through verbal behavior programs; uses incidental teaching and reinforcement to build spontaneous communication across all modalities.
✋ Occupational Therapist
Supporting discipline. Addresses sensory regulation prerequisites; optimizes physical AAC access; supports fine motor skills for signing; creates sensory regulation protocols.
📚 Special Educator
Supporting discipline. Embeds communication strategies across academic settings; uses visual supports, core vocabulary, and AAC in learning contexts; coordinates with therapy team.
👶 NeuroDev Pediatrician / EI Specialist
Prescribing/coordinating discipline. Differential diagnosis; prescribes communication evaluation; coordinates multi-disciplinary team; monitors neurodevelopmental trajectory.
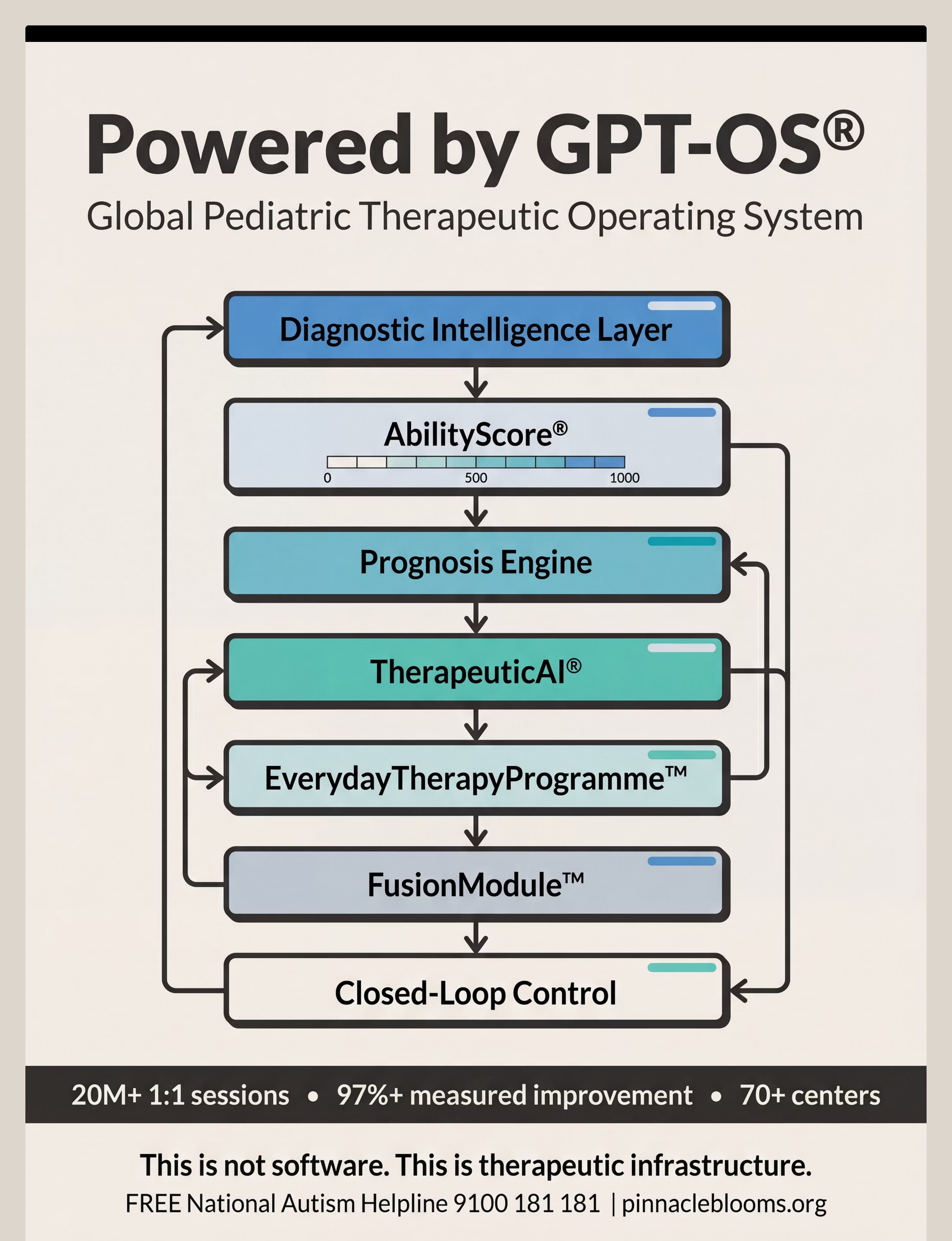
Pinnacle's FusionModule™ — the proprietary multi-disciplinary convergence system within GPT-OS® — ensures all five disciplines contribute to a single coordinated communication plan. No fragmented silos. One system, one plan, one child.
📞Need the full team? Call 9100 181 181 — Free multi-disciplinary assessment guidance, 24×7.

Precision Tools, Not Random Activities — Each Material Targets a Specific Developmental Layer
Observable Behavioral Indicators
Parents can measure progress through these 5 key signals:
- Number of spontaneous communication initiations per day
- Number of modalities used by the child
- Frequency of frustration meltdowns related to communication breakdown
- Response rate to familiar communication partner
- Length of shared interaction episodes
Research Evidence
Meta-analysis (World J Clin Cases, 2024): Multimodal communication intervention effectively promoted social skills (primary), adaptive behavior (secondary), and long-term developmental competencies (tertiary) across 24 independent studies.
Reference: PMC10955541

9 Materials. 9 Pathways. Every Bridge Your Child Needs.

1. Joint Attention & Engagement Toys
Builds the human-connection foundation before all other communication. Teaches that sharing experiences with people is rewarding. Bubble machine, pop-up toys, spinning light toys. ₹300–2,000

2. Picture Communication Cards & Boards
Makes abstract language concrete and visible — enables both receptive understanding AND expressive communication. PECS cards, choice boards, ARASAAC symbol sets. ₹500–3,000

3. AAC Devices & Apps
Gives children a functional voice NOW — while speech is developing. Research confirms AAC SUPPORTS speech emergence. CBoard (free), LetMeTalk (free Android), Proloquo2Go. ₹0–₹50,000+

Materials 4–6: Signs, Books & Cause-Effect

4. Sign Language Resources & Visuals
Hands communicate before mouths can — gross motor signs emerge before fine motor speech. Signs bridge to speech, not away from it. Indian Sign Language reference cards, key word signs. ₹200–1,500
5. Interactive Communication Books
Shared reading = shared language. Lift-flap, touch-and-feel, and sound books invite participation — building joint attention, vocabulary, and turn-taking simultaneously. Photo albums of child's own life. ₹300–1,500

6. Cause-and-Effect Communication Toys
"My actions create results" is the pre-communication insight. Switch toys and adapted devices teach agency and intentionality — prerequisites for purposeful communication. ₹500–3,000
Materials 7–9: Turn-Taking, Core Vocabulary & Sensory Tools

7. Turn-Taking Games & Materials
Conversation is fundamentally turn-based. Rolling a ball, stacking alternately, and simple games wire the back-and-forth exchange pattern that conversation requires. ₹200–1,500

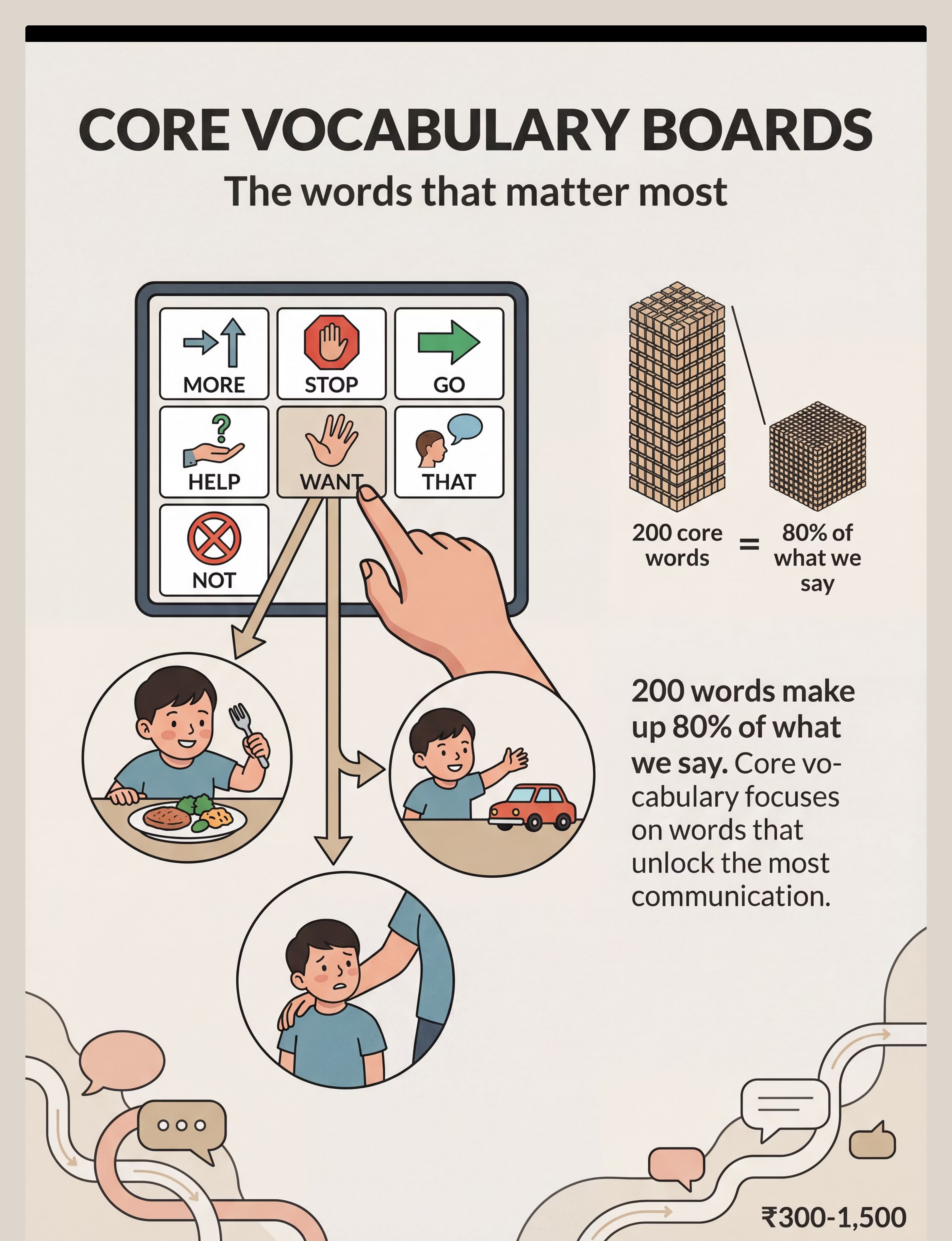
8. Core Vocabulary Communication Boards
200 words make up 80% of everything we say. Core vocabulary (WANT, MORE, STOP, GO, HELP, THAT) gives maximum communicative power with minimum learning investment. ₹300–1,500

9. Sensory Regulation & Attention Tools
A dysregulated child cannot communicate. Sensory tools create the calm, focused state where communication becomes possible — they are prerequisites, not accessories. ₹200–2,000
Total investment range: ₹2,500–₹65,000+ depending on AAC level chosen. Essential starter kit (under ₹3,000): Joint attention toy + printed picture cards + free AAC app + printed core board + basic sensory tool.
Every Parent Can Execute This — Regardless of Budget or Postcode
"Context-specific, equity-focused interventions must be accessible to ALL families." — WHO Nurturing Care Framework (2018)
Material | Clinical Version | DIY Substitute | ₹0 Version | |
1. Joint Attention Toys | Commercial cause-effect toys ₹300–2,000 | Tin can + pebbles shaker, sock puppet | Scarves for peek-a-boo, bubbles from soap + water | |
2. Picture Cards | PECS system, laminated sets ₹500–3,000 | Printed photos from phone, laminated with contact paper | Screenshot photos from phone, no lamination needed | |
3. AAC Device | Dedicated device ₹15,000–50,000+ | Tablet with free CBoard or LetMeTalk app installed | Free web-based CBoard.io on any internet device | |
4. Sign Language | Printed reference cards ₹200–1,500 | A4 printed signs from free ARASAAC downloads | YouTube sign language videos on phone | |
5. Interactive Books | Commercial lift-flap books ₹300–1,500 | Photo album of child's own life/family/routine | Magazine cut-outs in a notebook, handmade flap pages | |
6. Cause-Effect Toys | Switch toys ₹500–3,000 | Light switch (child-safe), any toy + dramatic parental reaction | Clap hands → adult does funny face. Simple, powerful. | |
7. Turn-Taking Games | Commercial games ₹200–1,500 | Ball rolled back and forth, block stacking alternately | Any two objects passed between parent and child | |
8. Core Vocabulary Board | Printed/laminated boards ₹300–1,500 | A4 printed from project-core.com, taped to table | Drawn by hand with marker on cardboard | |
9. Sensory Tools | Commercial fidgets, chewelry ₹200–2,000 | Clean damp cloth for chewing, homemade stress ball | Firm hand pressure, proprioceptive activities |
When clinical-grade is non-negotiable: AAC devices for children with motor access challenges (requires OT assessment); chewelry must be food-grade/non-toxic; weighted items require OT prescription for correct weight and duration.
Read This Before You Begin. Every Time.
🔴 CONTRAINDICATIONS — Do NOT proceed if:
- Child shows signs of illness, fever, or pain
- Child has had a severe meltdown in the last 30 minutes
- Child has not eaten in 3+ hours
- You are distressed, rushed, or cannot be fully present
- Weighted items: NO use without OT prescription
- Oral motor chewelry: ONLY food-grade, non-toxic items
🟡 MODIFY IF:
- Child is mildly tired → shorten to 5 minutes
- Child in unfamiliar environment → use portable materials only
- Child resists a specific modality → switch immediately, never force
🟢 SAFE TO PROCEED WHEN:
- Child is fed, rested, and regulated
- You are calm with 10–30 minutes uninterrupted
- All materials assembled and within reach
- Space is prepared per setup guide
STOP IMMEDIATELY if:
- Self-injurious behavior (head-banging, biting self)
- Extreme distress (inconsolable crying 3+ minutes)
- Physical aggression toward caregiver
- Signs of medical emergency
📞Safety question? Call 9100 181 181 — Free, 24×7

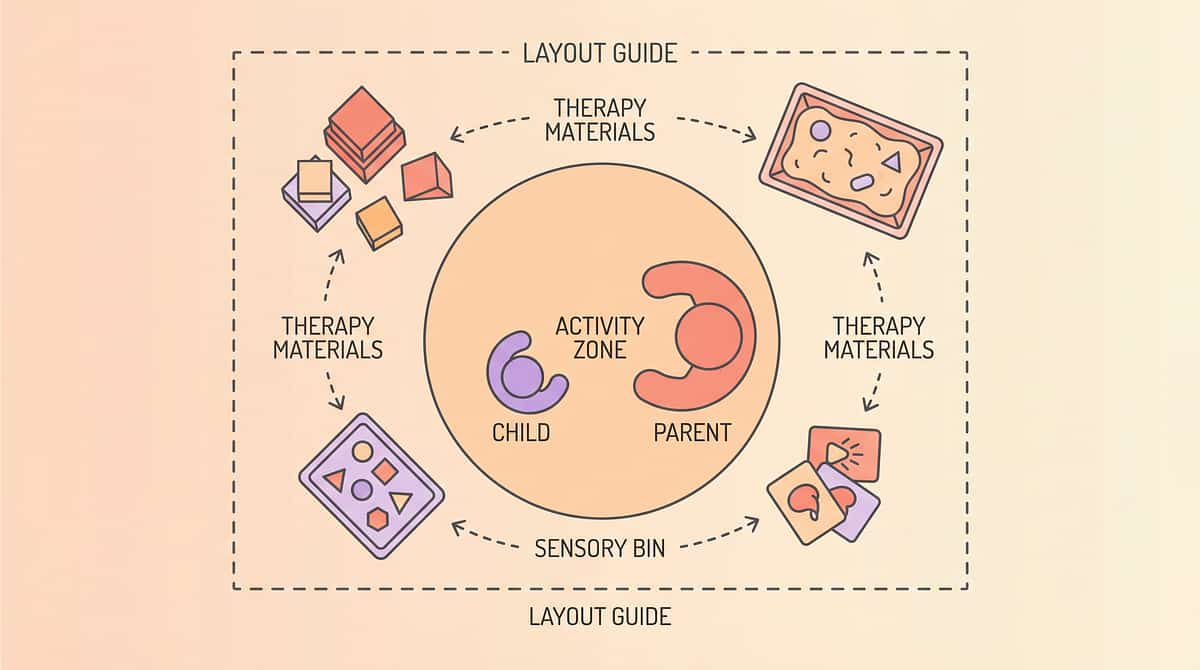
3 Minutes of Setup Prevents 80% of Session Failures
Remove From the Space
- Screens (TV off, unrelated tablets away)
- Auditory distractions (loud music, adjacent conversations)
- Competing toys not used in this session
- Other children if possible during initial learning phase
Position
- Parent at child's eye level (floor sitting, or kneeling at table)
- Child facing parent with materials accessible between them
- AAC device or picture board within child's reach
- Materials organized left-to-right in order of use
Environment Checklist
- Lighting: Natural or warm artificial — no harsh fluorescents
- Temperature: Comfortable — sensory-sensitive children highly affected by discomfort
- Noise: Quiet — no background TV, music, or competing voices
- Duration signal: Visual timer visible and facing child
The "Just Right" Environment
Calm ≠ sterile. This space should feel inviting, warm, and slightly exciting — not clinical. Your child should want to be here. Add one preferred visual item or comfort object to signal "this is a good place."

Act III — The Execution
The Best Session Is One That Starts Right. Take 60 Seconds to Check.
Indicator | ✅ GO | 🟡 MODIFY | 🔴 POSTPONE | |
Fed | Ate normally in last 2 hours | Ate lightly; have snack available | Not eaten in 3+ hours — feed first | |
Rested | Usual sleep, alert | Slightly tired — shorten to 10 min | Overtired — rest first | |
Regulated | Calm body, available eyes | Mildly activated — use sensory tool first | Dysregulated, in distress | |
Healthy | No signs of illness | Mild cold — gentle session only | Fever, pain, acute illness | |
Receptive | Responds to name, shows interest | Limited response — use highest motivator | Completely unresponsive | |
Post-event | No major incident in last hour | Minor difficulty, resolved | Severe meltdown in last 30 min | |
Caregiver | Calm, present, unhurried | Slightly rushed — still workable | Distressed, very rushed — reschedule |
All ✅
Full session — proceed to Step 1: The Invitation
Any 🟡
Modified session — 10 min, highest-preference material, lower demands
Any 🔴
Postpone — calming routine, reconnect tomorrow. No failure here.

Step 1: The Invitation — Every Protocol Begins With an Invitation, Not a Command.
Step 1 of 6
Duration: 30–60 seconds
Step 1 Goal: Bring the child into shared presence and anticipation without demand.
"[Child's name]... look what I have." [Pause. Hold preferred material at child's eye line. Wait 5 seconds.] "Should we try it together?" [Warm smile. Open body language. No demand.]
Body Language
- Get physically LOW — sit on the floor at child's level
- Lean slightly forward with open, inviting posture
- Hold the material out — let curiosity do the work
- You are the most interesting thing in the room
Reading Acceptance Cues
- ✅ Child looks at material or at you → proceed to Step 2
- ✅ Child moves toward material → proceed to Step 2
- ✅ Child vocalizes, reaches, or gestures → proceed immediately
- 🟡 Child continues current activity → animate material more
- 🔴 Child moves away → try from child's current location
AAC Variation
Hold device open to a motivating page. Model one press: "Look — [presses button] — ball!" Wait for child's response.
Sign Variation
Use the sign for the activity/object while showing it. MORE while showing a favorite snack. GO while showing a preferred toy. Pair consistently every time.

Step 3: The Therapeutic Action — What Actually Builds the Neural Pathway
Step 3 of 6
Duration: 5–15 minutes (core session)
Step 3 Goal: Execute the core therapeutic action specific to the selected material. This is where communication architecture is being built.
Joint Attention — Triple-Gaze Protocol
Activate toy → look at toy with exaggerated surprise → look at child for eye contact → look back at toy together → wait for child to look at YOU. That spontaneous eye contact in shared excitement = joint attention. Document it.
Picture Communication — Model-Expand-Respond Cycle
Hold up "WANT" card → model "I WANT..." → wait 5 full seconds (the pause IS the therapy) → child communicates in ANY modality → respond immediately as if perfect speech → expand one level.
AAC Device — Model with Natural Consequences
YOU press a button: "I WANT... BALL" → get the ball naturally → offer device to child (do not demand) → respond meaningfully to any button press → never correct mid-communication.
Sign Language — Sign-Speak-React Triplet
Make sign clearly → say word simultaneously → react to meaning as if spoken → accept approximations (30% handshape accuracy counts) → never withhold item until sign is "perfect."
Turn-Taking — Structured Exchange
Clear "MY turn" signal → take brief turn (under 5 seconds) → clear "YOUR turn" signal → wait 10 seconds → react to whatever child does as a successful turn.
Common execution errors: Asking "Can you say...?" → Replace with modeling + waiting. Rushing the 5-second wait → The pause IS the invitation. Correcting before responding → Respond first, always. Accepting only "perfect" communication → Any attempt = success.
Step 4: Repeat and Vary — 3 Good Repetitions Are Worth More Than 10 Forced Ones
Step 4 of 6
Duration: 3–5 minutes
Step 4 Goal: Build neural pathways through varied repetition without satiation.
Material | Target Reps | Signs of Satiation | Variation Strategy | |
Joint Attention Toys | 5–10 joint-gaze moments | Child stops looking at you after the effect | Switch toy, location, or reaction style | |
Picture Cards | 3–5 card exchanges | Child ignores cards, pushes away | Switch topic, card size, or core word | |
AAC Device | 5–8 modeled presses | Child closes device or moves away | Switch page, offer different category | |
Sign Language | 3–5 modeled + child attempts | Child turns away, stops imitating | Switch to a different sign, different context | |
Turn-Taking Games | 5–10 exchanges | Child takes materials and moves off | Accept naturally — celebrate the exchanges |
The Variation Principle: Same therapeutic target, different material. If AAC isn't landing today, switch to picture cards. The communication pathway is the target — the modality is the vehicle. Change vehicles freely.
Satiation Signals — Stop Here
- Child moves away repeatedly
- Child begins stereotypic play with the material (not interactive)
- Frustration or crying for 2+ minutes
- Completely distracted with no re-engagement after one attempt
Step 5: Reinforce and Celebrate — Timing Matters More Than Magnitude.
Step 5 of 6
Immediate. Specific. Enthusiastic.
The 3-Second Rule: Reinforcement delivered within 3 seconds of the target behavior is 10× more effective than reinforcement delivered at 10 seconds.
After ANY communication attempt: "YES! You said [word/sign/pressed button/pointed to picture]! You TOLD me! Here is [requested item]! AMAZING!"
Social Reinforcement
Big excited praise, tickle or physical play, animated facial expression, high five / fist bump
Token/Visual
Sticker chart, token board, points system, photo celebration
Natural Consequence
Get the requested item, chosen activity begins, person appears / song plays, communication partner responds
"Celebrate the ATTEMPT, not just the success. A child who reached for a picture card but didn't quite get it — celebrate the reach. A child who pressed the wrong AAC button — celebrate the pressing. Attempts are the seeds of skills."
📞Reinforcement system not working? Our BCBA team can help. Call 9100 181 181.

Step 6: The Cool-Down — No Session Ends Abruptly.
Step 6 of 6
Duration: 1–3 minutes
Step 6 Goal: Transition the child from therapeutic engagement back to baseline through a predictable, warm closure ritual. The cool-down prevents post-session dysregulation.
Warning (120 seconds before end)
"Two more turns, then all done." Hold up two fingers. Use a visual timer if available.
Final Exchange (60 seconds before end)
"One more — YOUR turn — beautiful! And... all done!" Use ALL DONE sign or picture card if using AAC/visual system.
Material Put-Away Ritual
Invite child to participate in putting materials away. "Ball goes here. Cards go here." Gives the session a clear ending and builds transition skills.
Transition Activity
Move immediately to a known preferred activity: bubbles, snack, outdoor time, favorite song. The transition should feel like a reward, not a loss.
Verbal Closure
"Great communicating today. I'm so proud of you. I love talking with you."
If child resists ending: Offer a choice ("Do you want to put the ball away, OR the cards?"). Use visual schedule if available. Allow 30 more seconds if needed, then natural close. Consistency of endings builds tolerance over time. NCAEP 2020

60 Seconds of Data Now Saves Hours of Guessing Later
Data transforms hope into strategy. Without measurement, you cannot know if an approach is working — or when to change it. GPT-OS® uses your session data to personalize future recommendations.
1. Communication Initiations
Count how many times the child independently initiated communication (any modality). Example: "3 times — 1 point, 1 button press, 1 reach"
2. Modalities Used
Which communication modes did the child use? Example: "Picture card + vocalization"
3. Session Response Quality
Simple 1–5 rating: 1=refused, 2=tolerated, 3=participated, 4=engaged, 5=led. Example: "Rating: 4 — child led last turn-taking exchange"
GPT-OS® In-App Tracker
Log in to pinnacleblooms.org/tracker — Your data feeds personalized weekly plan updates via TherapeuticAI®
Downloadable PDF Tracker
unknown link — Printable paper tracker for every session
Paper Backup
Date | Materials Used | Initiations | Modalities | Rating | Notes — simple and effective
Session Abandonment Is Not Failure — It's Data. Here's How to Read It.
❓ Child refused all materials and walked away
What happened: Readiness wasn't there — sensory state was off. Next session: Do a sensory regulation activity for 5 minutes first. Try highest-preference material only. Shorten to 5 minutes.
❓ Child used material non-functionally (threw cards, lined up AAC buttons)
What happened: Communication function not yet understood — child sees objects, not tools. Next session: Step back to cause-and-effect toys and joint attention. Build intentionality first.
❓ Child pointed at pictures but never used them to communicate
What happened: Receptive understanding without expressive use. Next session: Create a communication temptation — hold preferred item behind your back, present the picture, wait expectantly.
❓ Child used AAC for one session, then refused it entirely
What happened: If pressing buttons didn't reliably get results, motivation drops. Next session: Ensure EVERY button press gets an immediate, meaningful response. One press = one consequence. Always.
❓ Child won't maintain eye contact during joint attention activities
What happened: Direct eye contact may be neurologically aversive — common in autism. Adaptation: Stop requiring eye contact. Build joint attention through shared gaze at objects, not at you.
❓ Child only uses communication to request food/preferred items
What happened: Functional requesting is established — this is excellent! Next session: Celebrate this. Now expand: create opportunities to comment, reject, and seek social routine.
❓ Signs/pictures/AAC stopped working after 2 weeks
What happened: Habituation — child learned to get items without the tool. Next session: Increase waiting, add communication temptations, consult SLP for next vocabulary level.

No Two Children Are Identical. Here Is How to Make These Materials Fit Yours.
Level | Joint Attention | Picture / AAC | Turn-Taking | |
1 — Easiest (bad day) | Parent initiates all; any glance = success | One card, unlimited time, no demand | One exchange, any response accepted | |
2 — Starting | Two material choices; look at object = success | 2-card choice board, 10-sec wait | 3 exchanges, child takes turn when prompted | |
3 — Regular | Standard protocol per Steps 1–6 | 4–6 card board, 5-sec wait, model + expect | 5–7 exchanges, child initiates turn | |
4 — Strong day | Child-initiated joint attention moments | Child navigates 9+ word board independently | Child maintains game for 3+ minutes | |
5 — Advanced | Child directs parent's attention to show/share | Child combines 2+ symbols to communicate | Child repairs communication breakdowns |
Sensory Seeker (craves input)
- Add movement to all activities
- Provide proprioceptive input before communication work
- Use high-energy, animated interactions — be exciting
Sensory Avoider (over-responsive)
- Use quieter materials initially (picture cards vs. loud toys)
- Reduce physical proximity — give more personal space
- Softer voice, slower movements, low-demand invitation style

Act IV — The Progress Arc
Week 1–2: Progress Is Subtle. But It Is Unmistakably Real.
Foundation Building — 15% Progress
What You MAY See | What It Means | |
Child tolerates material 3 seconds longer than before | Neural pathway formation beginning — this is real data | |
Child looks at communication partner briefly during activity | Joint attention flickering — foundational progress | |
Fewer meltdowns during communication attempts | Reduced frustration as new modality begins to work | |
Child reaches toward or touches picture/AAC device | Object recognition preceding functional use — excellent sign | |
Child accepts session without resistance | Pairing successful — child associates tools with positive experience |
What is NOT expected yet in weeks 1–2: Spontaneous independent use of communication tools, consistent eye contact, clear readable signs or words, extended turn-taking exchanges, generalization to other settings.
Weeks 1–2 may feel invisible. You are doing deep work that won't yet show on the surface. The neural pathways are forming. The pairing is happening. Trust the process — and track the tiny wins.
Reference: PMC11506176

Week 3–4: The Turning Point. Neural Pathways Are Consolidating.
Consolidation Phase — 40% Progress
Anticipation
Child moves toward communication materials before session begins — they know what's coming and they want it.
Preference Signals
Child reaches for one modality over another — they are self-selecting their strongest communication channel.
Spontaneous Attempts
Unprompted reach toward picture board or AAC during NON-session times — the biggest early milestone.

Reduced Prompting Needed
You say and model less — child is initiating more. Prompting fading naturally is a sign of true learning.
Multi-Modal Combinations
Child begins combining two channels (points + vocalizes; presses AAC + looks at you). Communication complexity is growing.
Parent milestone: You may notice YOU are more confident. You are reading your child's communication attempts better. You are responding faster. This is the real transformation — you are becoming your child's most effective communication partner.

Week 5–8: Mastery Unlocked — The Skills Are Becoming Part of Who Your Child Is.
Mastery Phase — 75% Progress
Mastery Criterion | Benchmark | How to Assess | |
Functional requesting | Child spontaneously uses 1+ modality in 4/5 opportunities | Count over 3 consecutive sessions | |
Modality variety | Child uses 2+ distinct modalities (sign + vocalization, picture + gesture) | Observe in one 20-min session | |
Partner responsiveness | Child adjusts communication when first attempt not understood | Create intentional "communication breakdowns" and observe | |
Generalization | Communication skills appear in at least 2 settings | Report from secondary caregiver | |
Reduced frustration | Communication-related meltdowns reduced by 50%+ vs. baseline | Track frequency from Week 1 data |
Generalization Indicators
Child uses picture card at restaurant to point to food; makes AAC-related sounds at school; brings parent to picture board when frustrated — unprompted.
Ready for Next Level
Mastery on 4/5 criteria = ready to add complexity: expand vocabulary, introduce new modality, begin conversational turn-taking protocols.
📞Ready to progress? Your GPT-OS® team will guide the next step. Call 9100 181 181. Reference: PMC10955541
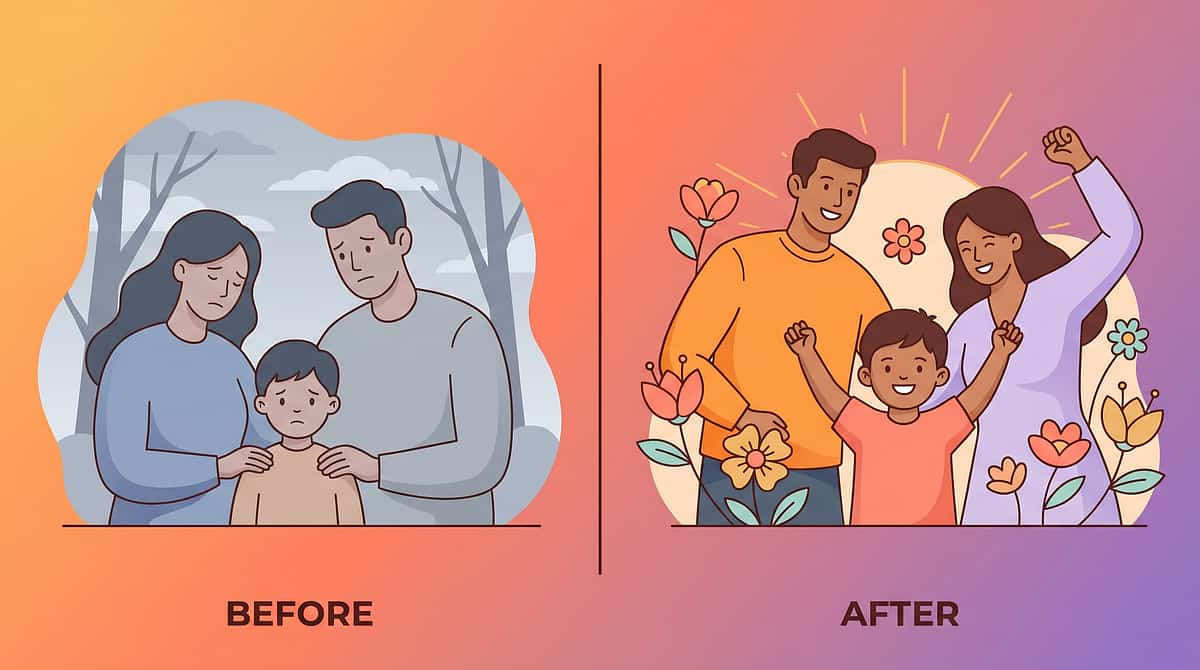
You Did This. Your Child Connected Because of Your Commitment.
You showed up — tired, uncertain, sometimes heartbroken — and you built bridges. Every picture card you held up, every sign you modeled, every AAC button you pressed, every turn you took and gave — it all compounded. And now your child communicates. Not like everyone else. In their own way, on their own terms, through pathways YOU helped build. That is everything.
✅ Functional Modality
Established at least one functional communication modality
✅ Reduced Frustration
Communication-driven frustration behaviors are down
✅ Joint Attention
Built the joint attention foundation for all future language learning
✅ Data Documented
GPT-OS® has baseline data for precision next steps
Journal prompt: Write one sentence: "Before, my child... Now, my child..." Capture this. Print it. Put it on your wall. These micro-victories ARE the milestones.
Share Your Story With Pinnacle Community → Your story helps another parent take the first step.
Trust Your Instincts. If Something Feels Wrong, Pause and Ask.
Red Flag | What It Looks Like | What To Do | |
Communication regression | Child loses previously established skills (was using 5 signs, now uses 0) | Teleconsult within 48 hours — regression can signal medical or sensory changes | |
Severe self-injury | Head-banging, biting self, scratching during communication activities | Stop immediately — functional behavior assessment needed | |
Complete material rejection | Child who previously tolerated sessions now refuses all approaches for 5+ days | Assessment for underlying sensory, medical, or psychological changes | |
No modality emerging at 6 months | No consistent use of any modality despite daily implementation | Comprehensive re-evaluation — AAC access assessment, motor evaluation | |
Increased aggression | Sessions are triggering aggression not present before | Stop structured sessions, consult ABA team — demands may be too high | |
Medical changes | New medications, illness, significant life changes with regression | Medical consultation first — always rule out physical factors |
Self-resolve
1–2 days rest
Teleconsult
Within 48 hours
Clinic Visit
Within 1 week
Emergency
Call 9100 181 181 immediately
📞FREE Helpline: 9100 181 181 | 24×7 | 16+ Languages | Locate Nearest Center
You Are Not Done — You Are on a Journey. Here Is Where You Go Next.
Based on your child's response profile, choose your next direction:
Joint Attention Gains Primary
AAC/Picture Primary Modality
Sensory Regulation Primary Need
Pragmatic/Social Emerging
Long-term developmental goal this feeds: Functional multimodal communication → social communication readiness → school participation → self-advocacy.
You Already Own Materials for Some of These — Keep Building.
Technique | Code | Difficulty | Materials You May Already Have | |
9 Materials for Expressive Communication | L-992 | Intro–Core | Picture cards, AAC from L-994 | |
9 Materials for Receptive Language | L-993 | Intro–Core | Interactive books, visual supports | |
Joint Attention Building Techniques | L-997 | Intro | Cause-effect toys from L-994 | |
Social Connection Materials | L-995 | Core | Turn-taking games from L-994 | |
Pragmatic Communication Skills | L-996 | Core–Advanced | AAC device from L-994 | |
Visual Communication Supports | L-934 | Intro–Core | Picture cards, core vocabulary from L-994 |
Materials you already own that work across techniques:✅ Joint attention toys → L-997 | ✅ Picture cards → L-992, L-993, L-934 | ✅ AAC device → L-992, L-995, L-996 | ✅ Turn-taking games → L-995, L-996 | ✅ Core vocabulary boards → L-992, L-995
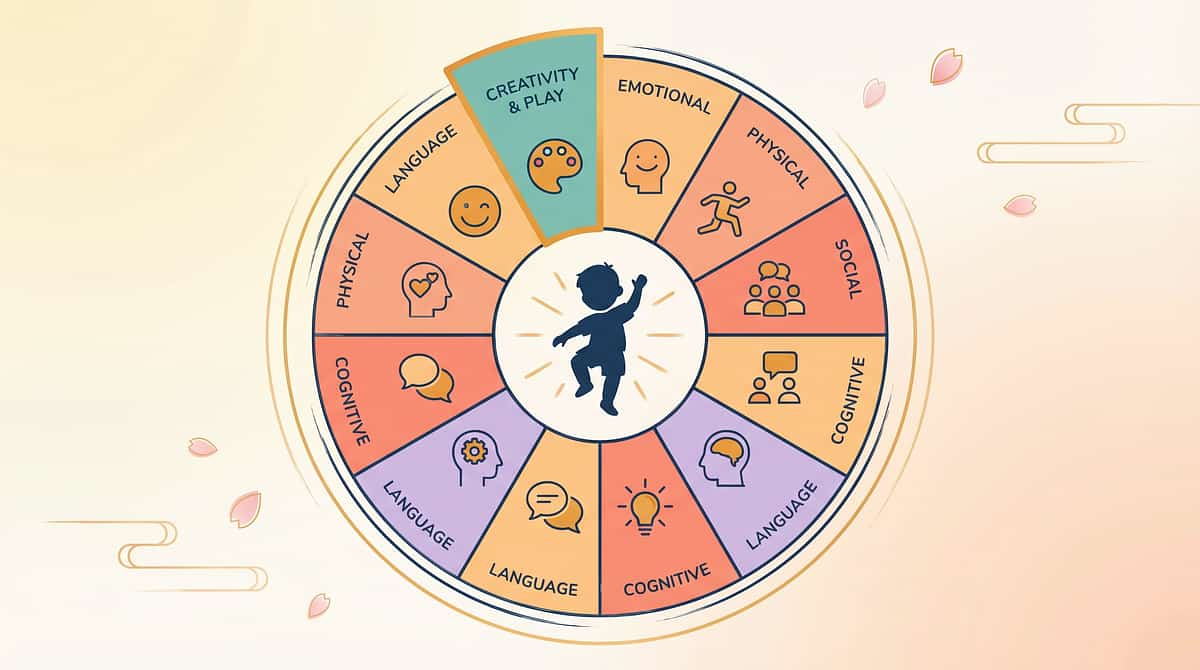
This Technique Is One Piece of a Larger Plan. Here Is the Whole Picture.
Your child's development spans 12 interconnected domains. Communication is the foundation that elevates every other domain — and every other domain feeds back into communication.
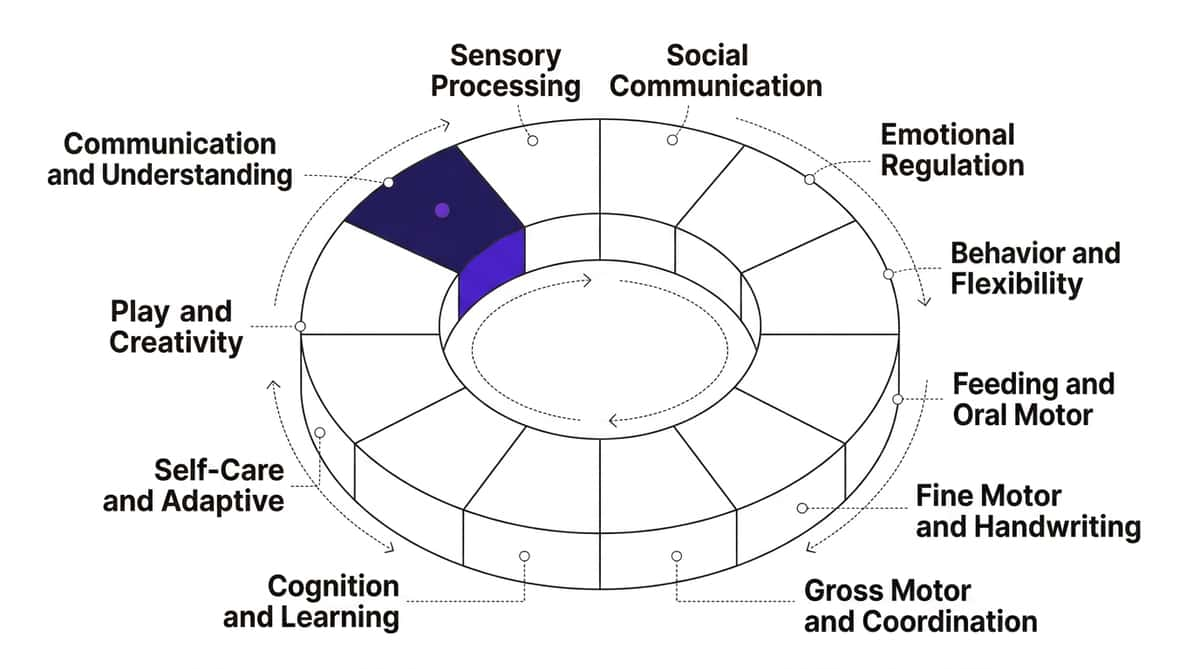
The greatest gains come when all 12 domains are addressed as a coordinated system — not in isolation. GPT-OS® is the system that coordinates them. Each domain's progress accelerates every other domain.
📞Get your child's full 12-domain AbilityScore® assessment. Call 9100 181 181. | Log in to GPT-OS® Dashboard
Reference: WHO Nurturing Care Framework (2018)
Act V — Community & Ecosystem
They Were Exactly Where You Are. Here Is Where They Are Now.
"He walks to his picture board at meal time. He presses 'WANT EAT' on the tablet. He signs 'MORE' for biscuits. The meltdowns are maybe one a week now — because he can TELL me. He's not fully verbal. But he is COMMUNICATING. And that changes everything." — Parent of Arjun, age 3.5, Chennai
Before (Week 0)
Arjun had five words, none consistent. He dragged his mother everywhere — to the fridge, the door, the TV — because he had no other way to communicate. Meltdowns 3–4 times a day. The family felt like his personal guessing machine.
Using L-994 for 8 weeks: Picture cards for meals (3 items), simple AAC app (free), daily bubble + joint attention sessions, 5 core signs.
After (Week 8+)
"She picks up the core vocabulary board and points to 'HELP SIT YOU.' Three words. She is telling me what she needs. I cried for an hour the first time she did it. I still cry sometimes. This was not nothing. This was everything." — Parent of Priya, age 5, Hyderabad
Therapist note: Within 6 weeks using 2 modalities consistently. Speech syllables emerged at week 9 — consistent with AAC-supported speech emergence research.
Individual outcomes vary. Case details anonymized. Statistics represent aggregate outcomes across the Pinnacle Blooms Network.

Isolation Is the Enemy of Adherence. You Are Not Alone in This.
WhatsApp Parent Group — Communication Overall
Connect with families navigating the same materials and techniques. Join Communication Support Group →
Pinnacle Online Community
Guided discussions, therapy tips, milestone celebrations. Moderated by Pinnacle clinical team. Join Community →
Local Parent Meetups
Organized by Pinnacle centers — meet face-to-face with families in your city. Find Local Meetup →
Peer Mentoring
Connect with an experienced parent matched by child's profile and location. Request Peer Mentor →
"My son's communication turned around when I joined the WhatsApp group. Another parent had tried exactly what wasn't working for me and found the fix. That's 2 weeks I didn't lose." — Parent, Pinnacle Hyderabad
A parent who connects with one other family navigating the same challenge is 3× more likely to maintain consistent home implementation. Community is therapeutic infrastructure, not optional support.

Home + Clinic = Maximum Impact. Professional Backing for Every Family.
Research consistently shows that children receiving both professional therapy AND structured home implementation achieve outcomes 2–4× superior to either approach alone. The clinic gives precision. The home gives frequency. Together, they transform.
Specialty | What They Offer | Book | |
Speech-Language Pathologist | Comprehensive communication assessment, AAC evaluation, PECS training, core vocabulary programming | ||
ABA/BCBA Therapist | Functional communication training, verbal behavior programs, reinforcement optimization | ||
Occupational Therapist | Sensory regulation assessment, AAC physical access, fine motor for signing | ||
Multi-Disciplinary Assessment | AbilityScore® evaluation + full team consultation | ||
Teleconsultation (Remote Families) | Video consultation with Pinnacle specialist team for families outside major cities |
📞FREE First Consultation: 9100 181 181 | 24×7 | 16+ Languages | Find Your Nearest Center
Reference: WHO NCF Progress Report (2023): Primary health care + family-based intervention as complementary, not competing, delivery platforms.
Every Claim on This Page Has a Source. Here Are the Sources.
# | Citation | Finding | Link | |
1 | PRISMA Systematic Review, Children (2024) | 16 studies confirm multimodal communication intervention is evidence-based practice | ||
2 | Meta-Analysis, World J Clin Cases (2024) | 24 studies: communication intervention effectively promotes social, adaptive, expressive outcomes | ||
3 | WHO CCD Implementation Study (2023) | Home-based multimodal intervention efficacy across 54 LMICs | ||
4 | Padmanabha et al., Indian J Pediatr (2019) | Indian RCT: home-based communication interventions, significant outcomes | ||
5 | NCAEP Evidence-Based Practices (2020) | AAC, PECS, sign language, video modeling: each independently evidence-based | ||
6 | WHO Nurturing Care Framework (2018) | Holistic early childhood development framework — foundational reference | ||
7 | ISAAC AAC Research Consensus | AAC supports rather than hinders speech development |

Your Data Helps Your Child. And Every Child Like Yours.
What GPT-OS® Learns from L-994 Data
- Which modalities are effective for this child's profile
- Which reinforcement categories drive highest engagement
- Session duration and tolerance patterns
- Progress velocity vs. 20M+ session population norms
- Optimal next technique sequencing
Privacy Assurances
- All data encrypted, GDPR and Indian PDPA compliant
- No personally identifying data shared with third parties
- Aggregate anonymized data improves recommendations for all families
- Your data is yours — export or delete at any time
Every session you log makes GPT-OS® more accurate for every family. 20 million sessions already. Each new session makes the prognosis engine more precise for the next child diagnosed today.

Watch How These 9 Materials Work — In Action, With Real Children.
Reel L-994
Series: Communication & Understanding — Episode 994
Domain: L | Communication
Duration: ~75 seconds
Domain: L | Communication
Duration: ~75 seconds
What You'll See in This Reel
- Child and adult using cause-and-effect toy with joint attention
- Picture card exchange in real time
- AAC device being modeled and responded to
- Sign language key words demonstrated
- Parent-child turn-taking interaction
- Core vocabulary board in use
Connection to this page: This Reel surfaces the challenge. This page gives you everything you need to address it. The Reel is the introduction — this page is the full program.
Consistency Across Caregivers Multiplies Impact
Share this page with every caregiver in your child's life. A child who receives consistent communication support from 3 caregivers achieves milestones in 40–60% less time than a child with only one consistent responder.
📥unknown link | 🏫unknown link
NCAEP (2020): Video modeling is classified as an evidence-based practice for autism. Multi-modal learning (visual demonstration + text + practice) improves parent skill acquisition and intervention fidelity.
Preview of 9 materials that help with communication overall Therapy Material
Below is a visual preview of 9 materials that help with communication overall therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.







Link copied!

Act VI — Frequently Asked Questions
The Questions Every Parent Asks. The Answers From the Consortium.
Q1: If I give my child a tablet with AAC, will they never learn to talk?
No. Multiple independent systematic reviews confirm that AAC users develop equal or more spoken speech than children for whom AAC is withheld. Communication success motivates further communication attempts, including speech. Withholding AAC to "force" speech is not evidence-based. Providing it is. → See Card 6: Evidence Grade
Q2: My child is only 18 months. Isn't it too early for picture cards and AAC?
No. Children as young as 9–12 months benefit from simple AAC and sign language introduction. The brain is most plastic in these early years. Waiting until age 3 or 4 means years of missed opportunity. Start now, in the simplest form. → See Card 5: Developmental Timeline
Q3: We've tried picture cards before and they didn't work. Why would it be different?
How picture cards are used matters far more than whether they're used. Most implementation failures occur because: (a) cards weren't motivating enough, (b) child wasn't shown how to USE them to get results, or (c) no one consistently responded to card-based communication. → See Cards 17–22 for the correct protocol.
Q4: Which material should I start with?
Start with the ONE material that creates the clearest, most immediate communication success for your child. Most families find cause-and-effect toys + simple picture cards are the easiest entry point. The modality they pick up fastest is their communication strength. → See Card 25: Adapt and Personalize
Q5: We don't have the budget for a dedicated AAC device. Can we still use these materials?
Absolutely. Every material has a ₹0 alternative. Free AAC apps (CBoard.io, LetMeTalk) work on any smartphone. Printed picture cards cost a few rupees. Core boards can be drawn by hand. Evidence shows DIY approaches achieve equivalent outcomes when implementation is consistent. → See Card 13: DIY Alternatives
Q6: My child uses pictures at home but won't use them at school or in public. Is this normal?
Yes. Generalization is a separate skill that needs to be explicitly taught. Use the same materials in multiple settings, with multiple people. Share the Family Guide with teachers. Generalization takes 2–4 additional weeks beyond home mastery. → See Card 28: Mastery Indicators
Q7: How many of these 9 materials should I use at once?
Start with 1–2. Add a second modality when the first is being used consistently. Add a third when the second is established. Overwhelming a child with too many systems creates confusion, not communication. → See Card 25: Implementation Sequence
Q8: My child has been using these materials for 6 weeks with no visible change. What do I do?
Six weeks of faithful implementation with no measurable change signals the approach needs adjustment or there is an underlying factor requiring professional assessment. Do not continue the same approach indefinitely. Contact our clinical team — this is exactly what teleconsultation is for. → See Card 30: Red Flags
📞Didn't find your answer? Call 9100 181 181 — our clinical team answers in 16+ languages, 24×7. | Ask GPT-OS® | Book Teleconsultation