
When They Can't Feel What Their Body Is Telling Them
It's 2pm. He's been playing for three hours. Suddenly he's running — sprinting — to the bathroom, hands pressed against himself, face desperate. He barely makes it. He's eight years old. And when I ask "Did you not feel the need to go?" he looks at me completely genuinely confused. Not embarrassed. Confused. Like I've asked him something in a foreign language.
Body Signal Recognition Training — teaching your child to hear what their body has been saying all along. You are not failing. Your child's interoceptive system processes internal signals differently. This is neuroscience, not neglect.
Interoception
Body Awareness
Self-Regulation
Toileting
Emotional Regulation
🏥Pinnacle Blooms Consortium — OT · ABA · SLP · SpEd · NeuroDev · CRO
📞FREE National Autism Helpline: 9100 181 181

You Are Not Alone: The Numbers
Interoceptive differences are among the most common — and least discussed — challenges in children with neurodevelopmental conditions.
80%
Interoceptive Differences
of children with autism show interoceptive processing differences
1 in 36
Children in India
diagnosed annually with autism — interoception rarely assessed
Millions
Families Worldwide
navigate this exact challenge silently — without the vocabulary to name it
Interoception — the brain's ability to detect and process signals from inside the body — is atypical in autism, ADHD, and sensory processing disorder. Most parents have never heard the word. Most children have never been assessed for it. Yet it underlies toileting accidents, unexplained meltdowns, dysregulated eating, and emotional explosions that appear to come from nowhere.
You are among millions of families navigating this. The silence around it is not because it's rare. It's because the word hasn't reached you yet.
Research: PRISMA Systematic Review (2024) — 80% of children with ASD display sensory processing difficulties (PMC11506176). Meta-analysis, World Journal of Clinical Cases (2024) — sensory integration therapy shows measurable outcomes across 24 studies (PMC10955541).
📞9100 181 181 | FREE in 16+ languages

What's Happening in Your Child's Brain
This is not a behaviour problem. It is a sensory processing difference in the brain's internal communication system.
The Neuroscience
Interoception is processed primarily through the insular cortex — the region responsible for detecting and interpreting signals from internal organs, muscles, and bodily states. In children with autism and sensory processing differences, the insular cortex may receive dampened signals, fail to prioritise them, or lack the neural pathways connecting sensation to conscious awareness.
The body is sending messages. The receiving station isn't processing them at full strength.
What This Means for Your Child
- Their bladder fills — but the signal doesn't reach awareness until it's urgent
- Their stomach empties — but "hunger" stays below the threshold of notice
- Their emotions escalate in the body — but they don't consciously register the buildup
- Their heart races, fists clench — but they don't know they're getting angry until they already are
"This is a wiring difference, not a choice. And wiring can be trained."
Research: Frontiers in Integrative Neuroscience (2020) — comprehensive neurological basis for sensory-based interventions in ASD (DOI:10.3389/fnint.2020.556660). Kelly Mahler's interoception research demonstrates explicit interoception teaching improves neural pathway connectivity.
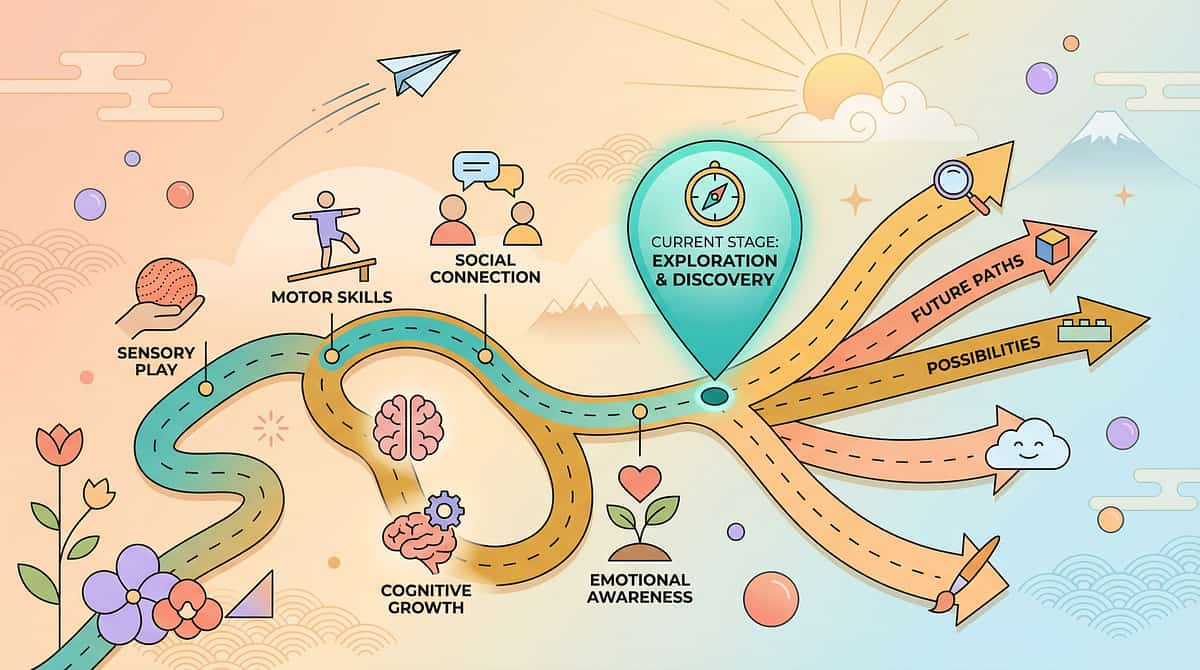
Where This Sits in Development
Your child is not behind forever. They are at a waypoint. Here is the map forward.
Age 1–2
Basic hunger and fullness awareness begins
Age 2–3
Toilet training readiness develops
Age 3–4
Bladder cues develop reliably in most neurotypical children
Age 4–8
Emotion-body signals emerge reliably — many children with ASD plateau here
Age 8–14+
Advanced interoception mastery and self-regulation independence
Most neurotypical children develop reliable interoceptive awareness gradually, through experience and gentle parental cueing. For children with neurodevelopmental differences, this automatic development stalls — not because they lack the hardware, but because the software needs explicit installation.
Autism
ADHD
SPD
DCD
Anxiety
"Your child is here. Here is where we are heading."
The Evidence Behind Interoception Training
Interoceptive awareness is teachable. Systematic, structured practice produces measurable change. This is not hope — it is documented outcome.
Evidence Grade: LEVEL II — Strong Clinical Evidence
Systematic Review — 2024
PMC11506176 — 16 studies, 2013–2023. Sensory integration intervention = evidence-based practice for ASD. Effect sizes: moderate to strong.
Meta-Analysis — 2024
PMC10955541 — 24 studies across multiple countries. SI therapy improves adaptive behaviour, social skills, sensory processing, emotional regulation.
India RCT — 2019
DOI: 10.1007/s12098-018-2747-4 — Home-based sensory interventions: significant outcomes. Parent-administered protocols validated.
NCAEP 2020
Body awareness + visual supports = evidence-based practices for autism. Multi-modal approaches improve parent skill acquisition and child outcomes.
"Clinically validated. Home-applicable. Parent-proven. Consortium-endorsed."

The Technique: What It Is
E-506 | Episode 506 of 999
Formal Name: Interoceptive Awareness Training through Structured Material-Based Practice
Parent-Friendly Alias: "Teaching Your Child to Hear Their Body"
Body Signal Recognition Training is a structured, multi-material approach to building interoceptive awareness — the ability to notice, name, and respond to internal body signals including hunger, thirst, bladder fullness, bowel urgency, tiredness, pain, temperature, and the physical sensations of emotions. For children whose interoceptive systems do not develop automatically, this training provides explicit, scaffolded practice across multiple daily contexts. It works by creating conditions where signals occur, directing conscious attention to them, building vocabulary to name them, and establishing routines that make body-checking habitual.
Domain E
GI & Toileting
Domain C
Emotional Regulation
Domain A
Sensory Processing
Self-Regulation
Body Awareness
Session Specifications
- Duration: 5–15 minutes per practice session
- Frequency: 2–5x daily (embedded in routines)
- Age Range: 4–14 years
Setting & Lead
- Setting: Home · School · Daily life
- Lead: Parent/Caregiver (with OT guidance)

Who Uses This Technique
Interoception training crosses every therapy boundary. Because the body doesn't organise by therapy type.
Occupational Therapy — Primary Lead
The architect of interoception training. OTs assess interoceptive processing, design structured activity sequences, calibrate sensory input intensity, and build the home practice protocols parents follow.
ABA / BCBA
Designs the reinforcement structures, data collection systems, and behavioural prompting hierarchies that make interoception practice consistent and measurable. Tracks toilet schedule adherence and body-check frequency.
Speech-Language Pathology
Builds the sensation vocabulary — the words children need to name what they feel. Without language for internal states, awareness cannot become communication.
Special Education
Integrates body check-in routines into school schedules, classroom transitions, and IEP goals. Ensures interoception strategies generalise from home to school.
Neurodevelopmental Paediatrics
Rules out medical contributors to interoceptive differences, coordinates interdisciplinary planning, and monitors overall developmental progress through GPT-OS® readiness indexes.
"When your OT teaches body check-ins, your ABA therapist measures consistency, and your SLP builds the vocabulary — they're all working the same system from different angles. That convergence is what GPT-OS® coordinates."
📞9100 181 181

9 Materials: An Overview
Nine materials. Clinically selected. Home-executable. Every price point covered. Below is a complete overview — each material is explored in detail on the cards that follow.
1
Interoception Curriculum
Structured body signal teaching system — ₹2,000–8,000
2
Body Check-In Visual Charts
Visual prompts for systematic internal scanning — ₹200–1,000
3
Sensation Vocabulary Cards
Words for what the body feels — ₹200–800
4
Scheduled Toileting Timer
External cue system when internal cues fail — ₹300–2,500
5
Hunger-Fullness Rating Scale
Makes invisible signals visible — ₹100–500 or free printable
6
Emotion-Body Connection Maps
Where feelings live in the body — ₹200–1,000 or free printable
7
Biofeedback Tools
See what you can't yet feel — ₹500–3,000
8
Movement & Body Awareness Activity Cards
Create sensations to notice — ₹0–2,000
9
Daily Routine Signal Pairing Toolkit
Practice at natural body-signal moments — ₹0 (strategy-based)
Starter Kit (Minimum Viable Set — ₹500 total): Body check-in chart (printable ₹0) + Sensation vocabulary cards (₹200–300) + Timer (phone app ₹0) + Hunger-fullness scale (printable ₹0)

Material 1: Interoception Curriculum
Pinnacle Recommends ✓
Canon: Interoception & Body Awareness Materials
The Interoception Curriculum is the most comprehensive structured body signal teaching system available for children with neurodevelopmental differences. Developed primarily through Kelly Mahler's pioneering research, this curriculum provides a sequenced, explicit programme for building the eight interoceptive signal pathways — from body-state awareness through to emotional regulation.
What It Includes
- Structured lesson sequences for each body signal type
- Age-adapted activities from 4 through to adolescence
- Parent and therapist implementation guides
- Progress monitoring built into the curriculum structure
How to Use It
Follow the curriculum sequence beginning with the loudest, most detectable signals (heart rate post-movement, obvious hunger) and progressively build toward subtler detection. Use 1–2 lessons per week alongside daily embedded check-ins. Your OT can calibrate the pace to your child's sensory profile.
Price: ₹2,000–8,000 | Search on Amazon.in
Free Starting Point: Download free body awareness worksheets and follow Kelly Mahler's free articles at kelly-mahler.com before investing in the full curriculum.

Material 2: Body Check-In Visual Charts
Canon: Visual Supports / Body Awareness Charts
₹200–1,000
Body check-in visual charts are structured visual prompts that guide a child to systematically scan their internal landscape — from head to toe — at scheduled intervals throughout the day. They work by externalising the internal scanning process, making the invisible visible and the habitual intentional.

How It Works
A body outline with labelled areas (head, chest, tummy, bladder, legs) prompts a structured internal scan. The child either points to the area they notice a sensation in, or rates each area on a simple scale.

Where to Place It
Post the chart at the child's eye level — beside the dining table for mealtime check-ins, near the bathroom for toileting prompts, and at the child's calm-down space for emotional regulation entry.
DIY Alternative (₹0): Draw a body outline on A4 paper. Add head/chest/tummy/legs labels. Laminate with sticky tape. Attach to wall at child's eye level. The homemade version works as well as the commercial one — the practice is the active ingredient.
Material 3: Sensation Vocabulary Cards
Canon: Emotion/Sensation Language Cards
₹200–800
Without words for internal states, awareness cannot become communication. Sensation vocabulary cards provide the precise language children need to bridge the gap between a body signal and a spoken report. They are the SLP component of interoception training made concrete and portable.
Core Vocabulary Set
- FULL / EMPTY
- TIGHT / LOOSE
- BUZZY / CALM
- URGENT / WAITING
- HEAVY / LIGHT
How to Introduce
Start with 5 words only. Add 5 more every 2 weeks as the child demonstrates recognition. Use during check-ins: lay 2–3 cards face up and ask "Does it feel like any of these?" Accept any selection — there is no wrong answer.
Progression
Week 1–4: 5 words. Week 5–8: 10 words. Week 9+: full vocabulary spectrum. Eventually, child begins using words spontaneously without cards present — this is the target behaviour.
DIY Alternative (₹20): Write 20 sensation words on index cards with simple drawings. "FULL" "EMPTY" "TIGHT" "BUZZY" "URGENT" "CALM" — drawn in the child's presence creates immediate ownership of the vocabulary.

Material 4: Scheduled Toileting Timer
Canon: Visual Timers / Scheduled Prompting Tools
₹300–2,500
When internal cues fail to reach conscious awareness, an external cue system becomes the bridge. The scheduled toileting timer provides a reliable, non-judgmental external signal that replaces the missing internal one — and over time, through consistent pairing, begins to train the internal pathway it temporarily substitutes for.
The Core Principle
The timer is not a permanent crutch — it is a scaffold. By pairing timer prompts with bladder check-in practice ("Timer went off — let's check your bladder before we go"), the external cue gradually builds the internal awareness pathway. The scaffold comes down as the pathway strengthens.
Timer Protocol
- Starting interval: Every 60–90 minutes
- When accidents reduce: Extend to every 2 hours
- Child goes independently: Timer becomes optional check only
- Vibrating wrist timer: Ideal for school settings — discreet and non-disruptive
Price: ₹300–2,500 | Search on Amazon.in
DIY Alternative (₹0): Set phone alarm every 90 minutes labelled "Bathroom Check." Any phone or smart speaker can serve this function at zero cost.

Material 5: Hunger-Fullness Rating Scale
Canon: Emotion/Body Rating Scales
₹100–500 | Free printable available
The hunger-fullness rating scale makes the invisible visible. It externalises an internal continuum — from "completely empty" to "uncomfortably full" — giving the child a concrete, visual reference point for a signal that was previously below conscious detection. This is one of the most powerful single materials in the E-506 toolkit.
1
1–3: Empty
Tummy feels hollow, empty, growling. Body needs food now.
2
4–6: Just Right
Comfortable. Eating is a good idea. Not urgent, not full.
3
7–8: Full
Tummy is satisfied. Food can stop.
4
9–10: Too Full
Uncomfortably full. Body signalling to stop eating.
How to Use: Before every meal, ask the child to point to their number. After the meal, ask again. Over time, the child begins pointing without being asked. That moment is a measurable interoceptive milestone. Post the scale on the dining table at child's eye level.
Safety Note: If a child begins restricting eating or showing disordered eating behaviours around scale use, discontinue immediately and seek professional guidance. See Card on Red Flags.
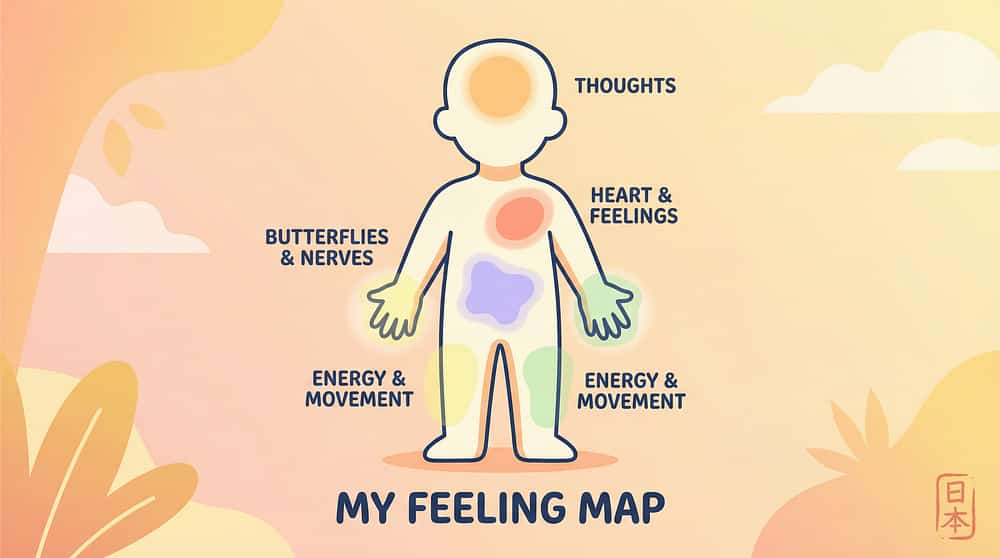
Material 6: Emotion-Body Connection Maps
Canon: Emotion Recognition / Body Mapping Materials
₹200–1,000 | Free printable available
Emotion-body connection maps are visual body outlines on which children (with adult support) identify where different emotions live in their body. This material directly builds the bridge between interoceptive signal detection and emotional awareness — the foundation of self-regulation. They work because emotions generate physical sensations before they generate conscious emotional awareness.

How to Build the Map
Sit with the child after a clear emotional moment. "That was exciting — where did you feel the excitement in your body? In your chest? Your tummy? Your legs?" Use colours: red for anger, yellow for excitement, blue for calm, purple for worry.
How to Use the Map Daily
Reference the map during check-ins: "Yesterday you showed me that worry lives in your tummy — is your tummy feeling like that now?" The map transforms abstract emotional states into concrete, nameable body locations.
If child becomes distressed during body-emotion mapping: Skip emotion mapping temporarily. Focus on physical signals only (hunger, bladder, tiredness). Seek OT guidance if distress persists. Possible trauma history may require professional support before this material is appropriate.

Material 7: Biofeedback Tools
Canon: Biofeedback & Body State Monitoring Tools
₹500–3,000
Biofeedback tools — primarily pulse oximeters and simple heart rate monitors — show children what they cannot yet feel. They create an external, objective data point that bridges the gap between internal signal and conscious awareness. When a child cannot reliably detect their own heart racing, seeing the number rise on a device provides immediate, undeniable evidence that something is happening inside their body.
The Bridge Principle
The device is the training wheel. You use it not because the child will always need it, but because it demonstrates that the body is always sending signals — even when the child says "I don't feel anything." Over weeks of practice with biofeedback, children begin detecting the sensation that the device has been showing them exists.
Practical Protocol
- Jump 20 times → check pulse oximeter → notice heart rate rise
- "Your heart is at 110. Can you feel it beating in your chest?"
- Rest 2 minutes → check again → "Now it's at 75. Notice the difference?"
- Over time, child reports sensation before checking device
Safety: Non-invasive, medical-grade consumer devices — safe for children 4+. Price: ₹500–3,000 | Amazon.in
DIY Alternative (₹0): Use resting hand-on-chest method to notice heartbeat. Jump 20 times, then notice heart rate change through hand pressure. The experience of the sensation — not the number — is the clinical target.

Material 8: Movement & Body Awareness Activity Cards
Canon: Movement & Proprioceptive Activity Resources
₹0–2,000
Movement is the fastest way to create loud interoceptive signals. Activity cards provide structured yoga poses, stretching sequences, jumping activities, and proprioceptive exercises — each paired with narrated body-awareness prompts that direct conscious attention to the sensations being generated. You cannot practise noticing a signal that isn't there; movement creates the signal first.
Yoga & Stretching
Slow, deliberate stretches create sustained proprioceptive signals. "Notice your legs stretching — feel the pull? That's your muscles talking to you." Cosmic Kids Yoga (YouTube, free) is ideal for ages 4–10.
Jumping & Cardio
10–20 jumping jacks immediately before a check-in amplifies heart rate, breathing, and muscle sensation — making quiet signals loud enough to detect. Ideal for sensory under-responders.
Heavy Work Activities
Pushing, pulling, carrying — proprioceptive "heavy work" creates deep body awareness signals. Wall push-ups, carrying books, pushing a laundry basket. These ground the body before a check-in session.
Key Principle: Always narrate the sensation during the activity. "Notice your heart — is it fast or slow? Notice your legs — are they heavy or light?" The narration is what links movement to interoception.
Material 9: Daily Routine Signal Pairing Toolkit
₹0 — Strategy-Based
Canon: Routine-Based Intervention Supports
The most powerful interoception tool costs nothing. The daily routine signal pairing toolkit is a structured strategy for embedding brief body-signal check-ins into the natural moments when body signals predictably occur — mealtimes, bathroom times, morning wake-up, evening wind-down, and transitions. Consistency at natural signal moments builds the neural habit faster than any scheduled session.
Before Eating
"Before we eat — how does your tummy feel? Empty? Full? Something in between?" — 10 seconds. No pressure. Accept any answer including "I don't know."
Before Bathroom Trips
"Timer went off. Let's check your bladder — any pressure there at all?" — Pair the external timer with internal checking until the internal signal emerges independently.
Before Bed
"Let's check your body before sleep — any tired feelings? Heavy legs? Heavy eyes?" — Evening tiredness signals are often the most accessible for children to detect.
After Exciting Activities
"That was exciting! Where do you feel the excitement? In your chest? Tummy? Legs?" — Post-activity emotional signals are louder and more accessible for emotional-body mapping.
The active ingredient is consistent, structured attention to internal signals — not the specific material. Practice drives neural pathway development, not paper quality.

DIY & Substitute Options
Every family can start today. Zero-cost versions exist for every material on this list.
Clinical Grade | DIY / Household Substitute |
Interoception Curriculum ₹2,000–8,000 | Free body awareness worksheets + Kelly Mahler's free articles at kelly-mahler.com |
Body Check-In Chart ₹200–1,000 | Draw body outline on A4. Add labels. Laminate with tape. Cost: ₹0 |
Sensation Vocabulary Cards ₹200–800 | 20 sensation words on index cards with simple drawings. Cost: ₹20 |
Vibrating Timer Watch ₹1,500–2,500 | Phone alarm every 90 minutes labelled "Bathroom Check." Cost: ₹0 |
Hunger-Fullness Scale ₹100–500 | Draw 1–10 number line. Tape to dining table. Cost: ₹0 |
Emotion-Body Map ₹200–1,000 | Print body outline. Draw with child where feelings live. Cost: ₹0 |
Pulse Oximeter ₹500–3,000 | Hand-on-chest method. Jump 20 times, notice heart rate change. Cost: ₹0 |
Movement Cards ₹0–2,000 | Cosmic Kids Yoga on YouTube. Jumping jacks. Stretching with narration. Cost: ₹0 |
Routine Pairing Toolkit | "Before eating — how does your tummy feel?" Practised consistently. Cost: ₹0 |
The active ingredient is consistent, structured attention to internal signals — not the specific material. A homemade hunger scale works as well as a printed one because the practice drives neural pathway development, not the paper quality.

Safety First: Before You Begin
Most interoception training is gentle and safe. Know the signals that mean pause, modify, or stop.
1
🟢 Green — Safe to Proceed
- Child is calm, rested, and fed before structured sessions
- Activities are presented as playful exploration, never interrogation
- Check-ins are brief (30–60 seconds), not extended examinations
- "I don't know" is a valid and informative answer — never correct it
- Practise during calm moments, never during active meltdown
2
🟡 Amber — Modify
- Child shows mild resistance → reduce frequency, try different framing
- Child fixates on biofeedback numbers → limit device use
- Child overwhelmed by vocabulary → start with 5 words only
- Child has had a difficult day → use shorter check-ins
3
🔴 Red — Stop & Seek Guidance
- Child severely distressed by body-focused activities
- Eating restriction appears to develop around hunger-fullness scales
- Child shows signs of medical illness requiring physical assessment
- Pain under-responsiveness presents as safety risk
- No progress after 3 months of consistent effort
Red Line: Stop if your child shows signs of severe anxiety, self-harm, or persistent refusal to eat related to scale use. Seek professional evaluation immediately.
📞9100 181 181
Set Up Your Space
Interoception practice doesn't need a therapy room. It needs a consistent, calm space where checking in feels normal.
Body Check-In Chart
Posted on wall at child's eye level — the visual anchor for every session
Sensation Vocabulary Cards
5–10 cards displayed and accessible — rotate sets to maintain novelty
Hunger-Fullness Scale
Near the dining area — prompts mealtime check-ins naturally
Yoga Mat or Calm Spot
Floor space for movement-based signal creation before check-ins
Timer
Phone or visual timer preset to scheduled intervals — non-negotiable for toileting programme
Environmental Settings
- Noise: Low — interoception requires inward attention
- Lighting: Natural or soft — calm supports body awareness
- Screens: Off during structured check-in (30–60 seconds)
- Temperature: Comfortable — temperature is itself an interoceptive signal
Key Principle
Body check-ins at the same time, in the same place, with the same words build the neural habit of internal attention faster than sporadic sessions. Parent position: beside the child, not opposite — collaborative, not evaluative.

Is Your Child Ready? Pre-Session Check
60 seconds before you begin. The best session is the one that starts right.
Physical Readiness
- Child has eaten in last 2 hours
- No signs of illness (fever, lethargy, pain)
- No major meltdown in last 30 minutes
- Not extremely fatigued
Emotional Readiness
- Regulation level: Calm to Alert (not Distressed)
- No major transition within last 10 minutes
- No known triggers active in environment
Environment Readiness
- Quiet space available (even briefly)
- Materials ready and visible
- Timer set if using scheduled prompting
All Green ✓ → GO
Full session, standard practice
3+ Amber ⚠️ → MODIFY
Shorten to 1 check-in only, no new vocabulary
Any Red ✗ → POSTPONE
30-minute wait, then re-check, or skip today
If POSTPONE: Try a passive version — simply say once during a natural moment: "Before we eat, let's check: how does your tummy feel?" Then drop it, no pressure.

Step 1 of 6
Step 1: The Invitation
Don't interrogate the body. Invite it. The framing in the first 10 seconds sets the tone for everything that follows.
For Beginners
"Let's do something interesting. We're going to try to listen to what your body is telling us. Your body sends little messages all day — let's see if we can hear any."
For Ongoing Practice
"Time for our body check-in. Let's see what your body is saying today."
For Mealtime Routine
"Before we eat — quick body check. Let's see if we can feel your tummy."
For Movement-Based Entry
"Let's jump 10 times. Then we're going to notice what your heart feels like."
What NOT to Say
❌ "Are you hungry? You should be hungry." — presumptive and invalidating
❌ "Tell me what you feel." — too open, too abstract for children with interoceptive differences
❌ "Why don't you know?" — shaming and counterproductive
❌ "Just check in quickly" — urgency defeats the purpose of internal attention
The invitation establishes body awareness as curious, safe exploration — not a test, not a performance. The child's answer is never wrong. "I don't know" is excellent data.
📞9100 181 181

Step 2 of 6
Step 2: Create the Signal
You cannot practise noticing a signal that isn't there. First, create the signal. Then notice it.
1
Heart Rate / Breathing
Jump 10 times → stop → hand on chest → "Feel your heart beating? Is it fast or slow right now?"
2
Hunger (Mealtime)
Wait until just before meal → "Before we eat, let's check your tummy. Is it empty? Full? Something in between?"
3
Bladder (Schedule)
At 90-minute timer → "Let's check your bladder. Any pressure? Any feeling there at all?"
4
Emotions (Natural Moment)
After exciting activity → "Where do you feel the excitement? In your chest? Tummy? Legs?"
5
Tiredness (Evening)
After dinner, before bath → "Any heavy feeling? Do your legs feel tired?"
6
Muscles (Post-Movement)
After yoga or exercise → "Notice your legs. Do they feel tight? Warm? Stretched?"
Key Principle: Start with loud signals (heart racing after jumping, obvious hunger) before quiet ones (mild bladder filling, subtle fatigue). Loud signals build the neural pathway that later detects quiet ones.

Step 3 of 6 — The Core Technique
Step 3: The Therapeutic Action
The active ingredient: directed internal attention + vocabulary + connection to meaning. Repeat daily.
Step A — Direct Attention (5–10 seconds)
"Stop what you're doing. Put your hand on your tummy/chest/forehead. Notice what you feel there. Don't say anything yet. Just notice." Give 5–8 seconds of actual silence. Resistance is normal. Wait.
Step B — Offer Vocabulary (10–15 seconds)
Show sensation vocabulary cards. "Does it feel like any of these? EMPTY? FULL? TIGHT? BUZZY? WARM? CALM? URGENT?" Accept any word. Accept "none of those." Accept "I don't know."
Step C — Connect to Meaning (10 seconds)
"That empty feeling? That's your body saying it needs food — that's hunger." "That pressure? That's your bladder — your body saying it's time to go." "Those butterflies? That's your body getting ready for something new."
Step D — Connect to Action (5 seconds)
"So what does your body need right now?" Hunger → food soon. Bladder pressure → bathroom now. Fatigue → rest. Emotional signal → name emotion, use regulation tool.
Common error: Rushing. The silence in Step A is doing clinical work. Protect it. Total duration: 2–5 minutes. If the child is severely distressed or refuses all body-focused attention, do not push — note as data and consult your OT.
Step 4 of 6
Step 4: Repeat & Vary
3 good check-ins beat 10 forced ones. Dosage is quality, not quantity.
Week 1–2
2 check-ins per day — mealtime + bedtime
Week 3–4
3 check-ins per day — add bathroom schedule
Week 5–8
4–5 micro check-ins embedded in transitions
Week 8+
Child-initiated check-ins begin to appear
Variation to Maintain Engagement
Variation | How |
Change the anchor signal | Hunger one day, heart rate next, tiredness the day after |
Change the vocabulary set | Rotate 5-word sets so novelty maintains attention |
Change the format | Cards one day, body outline drawing next, verbal only third |
Change the position | Standing, seated, or lying-down body scan |
Add biofeedback layer | Pulse oximeter visual data alongside sensation awareness |
Satiation Indicators — when the child has had enough today: Active avoidance of the check-in format. Perseverative, automatic answers. Visible frustration. "I already know" — celebrate this! It is a sign of growing competence. Rule: 3 authentic, attended check-ins = excellent session.

Step 5 of 6
Step 5: Reinforce & Celebrate
Reinforce the attempt. Reinforce the noticing. Not just the correct answer.
What to Reinforce
✅ Stopping what they were doing to check in — the attention itself
✅ Any use of sensation vocabulary, even approximations
✅ Tolerating the check-in without distress
✅ Connecting a sensation to meaning
✅ Initiating a body signal response ("I need to go to the bathroom")
"You stopped and listened to your body! That is exactly what we're practising — brilliant!"
"You said 'empty' for your tummy — you NAMED what your body felt. That's huge."
"You went to the bathroom when the timer went off. Your body and the timer are working together — excellent."
Reinforcement Options
- Verbal praise (always — immediate and specific)
- Reward Stickers 1800+ ₹364 — 1 sticker per successful check-in
- Reward Jar ₹589 — token economy for body awareness milestones
- Natural reinforcement: preferred activity because body-need was recognised and met
ABA Principle
Timing > Magnitude. Immediate, specific praise within 3 seconds outperforms large delayed rewards every time. The reinforcer closest in time to the behaviour is the most powerful.
📞9100 181 181

Step 6 of 6
Step 6: The Cool-Down & Transition
Every body-awareness session ends with a return to ease. The transition is part of the technique.
This structured close prevents abrupt endings that can dysregulate some children — particularly when emotional content has been surfaced during the session.
If Child Resists Ending
Some children become engaged by body awareness activities and resist stopping. This is a good sign. Acknowledge: "You want to keep checking in — that's wonderful. We'll do more tomorrow."
Post-Session Dysregulation Prevention
If the session surfaced emotional body signals (anxiety, frustration), spend 60 seconds with a calming sensory activity before transitioning — deep breathing, gentle joint compression, or a transition object. Avoid ending sessions abruptly when emotional content has been stirred.
Capture the Data — Right Now
60 seconds of data now saves hours of guessing later. Record before you forget.
Daily Body Signal Log — E-506
Date: ___________
Check-in Location: □ Mealtime □ Bathroom □ Transition □ Other
Signal Type: □ Hunger □ Bladder □ Emotion □ Fatigue □ Other
Child Response: □ No response □ Tolerated □ Identified word □ Self-initiated
Spontaneous signal noticed today: ___________
Toileting accidents today: ___ | Self-initiated: ___
Track Over Time
- Frequency of spontaneous body signal reports (week by week)
- Toileting accident frequency (trend line over 8 weeks)
- Vocabulary used — which words is the child using spontaneously?
- Self-initiation rate — is the child checking in without prompting?
GPT-OS® Tracking
Data entered through GPT-OS® EverydayTherapyProgramme™ feeds directly into the Interoceptive Awareness Readiness Index — giving your OT real-time progress data at each session.

What If It Didn't Go As Planned?
Session abandonment is not failure. It is data. Here are the 7 most common difficulties — and exactly what to do.
Problem 1: Child says "I don't know" to every check-in
Cause: Genuine interoceptive difficulty — this IS the challenge you're addressing.
Fix: Celebrate "I don't know" as honesty. Add biofeedback visual to show external data. Reduce vocabulary options to 2 words only.
Fix: Celebrate "I don't know" as honesty. Add biofeedback visual to show external data. Reduce vocabulary options to 2 words only.
Problem 2: Child resists or avoids check-ins
Cause: Body awareness feels unfamiliar or anxiety-provoking.
Fix: Reduce to 1 check-in/day in the least-pressured context. Use more playful framing. "Detective game — let's search for a signal."
Fix: Reduce to 1 check-in/day in the least-pressured context. Use more playful framing. "Detective game — let's search for a signal."
Problem 3: Toileting accidents continue despite timer
Cause: 90-minute interval may be too long; or child isn't sitting on toilet when timer sounds.
Fix: Reduce timer interval to 60 minutes. Confirm child actually sits on toilet at each alarm.
Fix: Reduce timer interval to 60 minutes. Confirm child actually sits on toilet at each alarm.
Problem 4: Child names the same sensation word regardless of context
Cause: Echolalia / preference for a familiar word.
Fix: Remove verbal answer option temporarily. Use pointing only. Show 2 very different cards (EMPTY vs. TIGHT) and ask which is more true.
Fix: Remove verbal answer option temporarily. Use pointing only. Show 2 very different cards (EMPTY vs. TIGHT) and ask which is more true.
Problem 5: Parent finds it hard to maintain consistency
Cause: Check-in feels like an extra task, not yet a habit.
Fix: Attach one check-in to a non-negotiable routine — the meal doesn't happen without the 15-second check-in first. One habit anchors the system.
Fix: Attach one check-in to a non-negotiable routine — the meal doesn't happen without the 15-second check-in first. One habit anchors the system.
Problem 6: Child becomes distressed by emotion-body maps
Cause: Body-emotion connection may surface uncomfortable memories or anxiety.
Fix: Skip emotion mapping temporarily. Focus on physical signals only. Seek OT guidance if distress persists.
Fix: Skip emotion mapping temporarily. Focus on physical signals only. Seek OT guidance if distress persists.
Problem 7: No progress after 6 weeks
Cause: May need individualised OT assessment; underlying processing differences may require clinical-grade intervention.
Fix: Call 9100 181 181. Request OT evaluation. Continue routine pairing while assessment is scheduled.
Fix: Call 9100 181 181. Request OT evaluation. Continue routine pairing while assessment is scheduled.
Adapt & Personalise
No two children are identical. Here is how to adjust for yours.
← Easier
- Single signal focus (hunger only, for weeks)
- 2-word vocabulary (EMPTY / FULL)
- Biofeedback visual only (sees heart rate number)
- Timer every 60 minutes (very frequent prompting)
- Adult-guided check-in (full script each time)
Harder →
- Multi-signal sessions (hunger + bladder + emotion)
- 20-word vocabulary (full spectrum cards)
- Internal perception only (no device, pure sensation)
- Timer every 2 hours (building independence)
- Child-initiated check-in (adult present but silent)
Sensory Under-Responder
Start with loud signals. Use jumping/exercise to amplify heart rate before checking. Use cold water on face to create clear temperature signal. Use biofeedback device as bridge.
Sensory Over-Responder
Focus on calming and normalising body sensations. "Your heart beating fast is normal." Build tolerance, not alarm.
Nonverbal / Minimally Verbal
Use picture-point response only. Body check-in chart with emoji faces. No verbal response required — pointing to a picture is full participation.
Younger Children (4–6)
"Where is your tummy?" body touch as first step. 2 options maximum. Very short (30 seconds). Game format always.
Older Children / Adolescents (10+)
Greater autonomy. Self-monitoring journal. Biofeedback app on their own phone. Ownership language: "Your body, your data."

ACT IV: The Progress Arc
Week 1–2: What to Expect
In the first two weeks, you are building a habit. The child is building awareness of a new internal channel. Neither happens overnight.
15%
Progress at Week 2
Foundation-laying phase — the neural habit is forming
Week 1–2 Observable Indicators (these ARE progress)
✓ Child tolerates body check-ins without severe resistance
✓ Child makes eye contact or pauses when check-in language is used
✓ Child selects a vocabulary word even if not perfectly accurate
✓ Child goes to bathroom when timer sounds (even without sensing the need)
✓ Parent has established a consistent routine anchor
"If your child tolerated a body check-in for 15 seconds without avoidance — that is a real neural pathway event. You cannot see the brain wiring, but it is happening."
What is NOT progress yet at this stage (normal): Child self-initiating check-ins (weeks 6–8 target). Reduction in toileting accidents (weeks 4–6 target). Spontaneous hunger reporting (weeks 4–8 target). Emotional signal awareness (weeks 6–12 target).
📞9100 181 181

Week 3–4: Consolidation Signs
40%
Progress at Week 4
Consolidation phase — neural pathways strengthening
Weeks 3–4: The neural pathways are strengthening. Look for these early consolidation signals.
✓ Child anticipates check-ins at routine moments (before meal, before bathroom)
✓ Child uses 2–3 sensation words with consistency and apparent accuracy
✓ Timer-prompted toileting has fewer accidents between prompts
✓ Child tolerates check-ins in 2+ different contexts (home + school)
✓ Child occasionally reports a signal before being asked ("My tummy is saying something")
✓ Child refers to hunger-fullness scale without prompting at mealtimes
What This Means Neurologically
The insular cortex is beginning to route interoceptive signals to conscious awareness more reliably. This is not imagination — it is measurable neural consolidation through repeated, attended practice.
Parent Milestone
"You may notice you're more confident too. The check-in language feels natural. That's because it is now a genuine communication channel between you and your child about their internal world."
When to Increase Frequency: If consolidation indicators appear before week 4, add one more daily check-in context and expand vocabulary from 5 to 10 words.

Week 5–8: Building Independence
65%
Progress at Week 8
Independence-building phase — scaffolding begins to fade
Weeks 5–8: The goal shifts. From parent-prompted to child-initiated. Begin fading the scaffolding.
✓ Child self-initiates bathroom trips in response to internal sensation (at least occasionally)
✓ Child uses hunger-fullness scale vocabulary spontaneously at mealtimes
✓ Child reports a physical sensation without being asked (pain, discomfort, tiredness)
✓ Emotional meltdowns show earlier warning: "I'm feeling tight" or "I need a break"
✓ Toileting accident frequency measurably reduced from Week 1 baseline
✓ Child applies body awareness in novel contexts (school, extended family visits)
Key Indicator to Watch: Does the child now check in with their body during moments you haven't prompted? Even once per day spontaneously is a major milestone. Record it immediately.
Celebrate the Milestones
Progress in interoception is invisible to the world. You see it. Name it. Celebrate it.
🏅 Milestone 1: First Signal Word
Child uses a sensation vocabulary word unprompted for the first time. "My tummy is empty." Celebrate with maximum enthusiasm. This is neural pathway evidence.
🏅 Milestone 2: Timer Trust
Child goes to bathroom at timer prompt without arguing for 7 consecutive days. "Your body and the timer are working as a team now."
🏅 Milestone 3: First Self-Initiation
Child goes to bathroom (or asks for food, or says "I'm tired") based on internal signal, without timer or prompt. This is the entire point. Mark this day.
🏅 Milestone 4: Emotion-Body Link
Child names a body sensation during an emotional moment before exploding. "My chest feels tight." Foundational self-regulation emerging. Enormous.
🏅 Milestone 5: Cross-Context Generalisation
Body awareness behaviour appears in a new setting without prompting — school, grandparent's house, restaurant. The learning has transferred. It is now part of the child.
You did this. Every check-in you showed up for. Every "I don't know" you accepted without correction. Every timer you set and followed through. This child's growing awareness is the direct result of your consistency. That is measurable science.
📞9100 181 181

Red Flags: When to Escalate
Most children progress steadily. Know the signs that call for professional evaluation.
🚨 No Measurable Progress After 8–10 Weeks
Underlying sensory processing differences may require clinical-grade OT assessment and specialised intervention beyond home practice. Do not continue without professional guidance if no change is observed after consistent daily effort.
🚨 Pain Under-Responsiveness Creates Safety Risk
Child is not noticing significant injuries, burns, or illness signs. Medical evaluation needed to rule out neuropathy or other physical contributors. This is a safety concern — act promptly.
🚨 Interoceptive Hypervigilance Develops
Child becomes obsessively focused on body sensations. Can indicate anxiety disorder. Psychological evaluation recommended before continuing interoception training.
🚨 Eating Restriction Develops Around Scale Use
Immediately discontinue scale use. Consult a paediatric dietitian and psychologist. Do not wait to see if it resolves on its own.
🚨 Severe Distress During Body-Awareness Activities
Possible trauma history or severe anxiety. Seek psychological evaluation before continuing any body-awareness work.
🚨 Toileting Accidents Increasing Despite Timer
Medical evaluation needed — urological or gastroenterological contributors possible. Do not assume this is behavioural.
What to tell the professional: "My child has interoceptive processing differences. We've been doing home-based interoception training for [X weeks] using [materials]. Here is what we've observed: [data from the tracking log]."
📞9100 181 181 — FREE in 16+ languages
Your Progression Pathway
Body Signal Recognition is one technique in a complete interoception and self-regulation progression. Here is your map.
← E-504: Toilet Training Resistance
Before this technique — establishing the behavioural foundation
← E-505: Independent Wiping Skills
Immediate predecessor in the toileting cluster
★ E-506: Body Signal Recognition
YOU ARE HERE — building interoceptive awareness across all signal types
→ E-507: Public Bathroom Avoidance
Builds directly on bladder signal recognition developed here
→ E-508: Constipation & Withholding
Bowel signal awareness is the foundation needed for this technique
GPT-OS® Readiness Progression Stages
1
Stage 1: No awareness — external cues only (where most start)
2
Stage 2: Emerging detection — signals identified when prompted
3
Stage 3: Developing interpretation — connecting signals to meaning
4
Stage 4: Advancing response — growing spontaneous awareness
5
Stage 5: Mastery — reliable interoception supporting independence

Related Techniques
Interoception connects to every domain of your child's development. Here are the techniques that work alongside E-506.
E-507
Public Bathroom Avoidance — builds directly on bladder signal recognition developed in E-506
E-508
Constipation & Withholding — bowel signal awareness developed in E-506 is the essential foundation
C-254
Emotional Meltdown Prevention — emotion-body signals from E-506 become the regulation tools here
A-Series
Sensory Processing — interoception is the eighth sensory system, foundational to the entire A-domain
K-5580
Understanding Interoception — deeper parent knowledge base for this domain
E-506-DD-01
Interoception Curriculum Deep-Dive Guide — full Kelly Mahler curriculum implementation support
Interoception doesn't exist in isolation. A child who learns to notice bladder pressure (E-506) uses the same neural pathway development to notice emotional buildup (C-254). The vocabulary built for hunger signals transfers to anger and anxiety signals. This is why consistent interoception practice creates cascading improvements across domains.
The Full Developmental Map
This technique is one precision instrument in a complete developmental system. Here is the whole picture.
Current Technique's Domain
E — Gastrointestinal & Toileting (with cross-domain impact on C: Emotional Regulation, A: Sensory Processing, and L: Adaptive Behaviour)
GPT-OS® Whole-Child View
Body signal recognition is foundational infrastructure for multiple developmental domains. When a child cannot detect internal signals, deficits appear across toileting (E), emotional regulation (C), feeding (G), adaptive behaviour (L), and social participation (B). Improving interoception is high-leverage development work.
"This technique is one piece of a larger plan. GPT-OS® sees the full picture."
Powered by GPT-OS®
What guides these materials is not a content team. It is a therapeutic operating system governing 20 million clinical sessions.
Diagnostic Intelligence Layer
591+ structured observations → 349 skills → 79 abilities → Standardised diagnostic clarity across all developmental domains
AbilityScore® (Patented)
Universal developmental score 0–1000. Comparable across time, therapists, and centres. The first standardised measure of its kind in paediatric therapy.
Prognosis Engine
Developmental trajectory prediction from 20M+ session data. Real-time forecasting calibrated to your child's specific profile.
TherapeuticAI®
Therapy focus + intensity + sequencing + reinforcement logic. Always executed under licensed human clinical authority.
FusionModule™
OT + SLP + ABA + SpEd + Medical → Single converged pathway. Every discipline working from the same data, toward the same goals.
EverydayTherapyProgramme™ ← You Are Using This Now
Clinical plans → daily home-executable micro-interventions. Closed-loop: Observe → Score → Plan → Execute → Re-measure → Adapt.
20M+
1:1 Sessions
Clinical data powering every recommendation
97%+
Measured Improvement
Across the Pinnacle Blooms Network®
70+
Centres
Patents filed across 160+ countries
"This is not software. This is therapeutic infrastructure."
📞 FREE National Autism Helpline: 9100 181 181 | 🌐 pinnacleblooms.org
Preview of 9 materials that help with body signal recognition Therapy Material
Below is a visual preview of 9 materials that help with body signal recognition therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.




















Link copied!
The Pinnacle Promise
✦ Pinnacle Blooms Network® ✦
Built by Mothers. Engineered as a System.
OT · SLP · ABA/BCBA · Special Education · NeuroDev Paediatrics · CRO
OT · SLP · ABA/BCBA · Special Education · NeuroDev Paediatrics · CRO
"From fear to mastery. One technique at a time."
We exist to transform every home into a proven, scientific, 24×7, personalised, multi-sensory paediatric therapy centre — for every child, at every income level, in every language, on every continent. Powered by 20M+ clinical sessions. Validated by 97%+ measured improvement. Governed by GPT-OS®.
20M+
Clinical Sessions
97%+
Measured Improvement
70+
Centres
70+
Countries Served
Technique E-506 is part of the Gastrointestinal & Toileting Challenges series — Episode 506 of 999. Part of the Pinnacle 70,000+ technique library at techniques.pinnacleblooms.org
This content is educational. It does not replace individualised assessment and intervention planning with licensed occupational therapists, psychologists, and healthcare professionals. Persistent interoceptive differences may indicate underlying sensory processing, neurological, or developmental conditions requiring professional evaluation. Seek professional help for concerns. Individual results may vary. Statistics represent aggregate outcomes across the Pinnacle Blooms Network®.
CIN: U74999TG2016PTC113063 | DPIIT: DIPP8651 (Govt. of India Startup India) | MSME: Udyog Aadhaar TS20F0009606 | GSTIN: 36AAGCB9722P1Z2
© 2025 Pinnacle Blooms Network®, unit of Bharath Healthcare Laboratories Pvt. Ltd. All rights reserved.
© 2025 Pinnacle Blooms Network®, unit of Bharath Healthcare Laboratories Pvt. Ltd. All rights reserved.
📞 FREE National Autism Helpline: 9100 181 181 | 16+ languages | 24×7
🌐 pinnacleblooms.org | 📧 care@pinnacleblooms.org
🌐 pinnacleblooms.org | 📧 care@pinnacleblooms.org