

"The teachers tell me she's a model student. Every parent-teacher conference is glowing — focused, polite, follows directions. She's a pleasure to have in class, they say. And then she gets in the car — and it's like a different child entirely. Before we're even out of the parking lot, she's screaming. Crying. Kicking the seat. By the time we get home, it's a full meltdown. Homework is impossible. Dinner is a battle. Everything I say is wrong. I used to think she was choosing to behave at school and misbehave at home — saving her worst for the people who love her most. But now I'm starting to understand: she's not choosing anything. She's spent all day holding herself together. And by 3:00 PM, there's nothing left."



Study | Finding | Population | |
PRISMA Systematic Review (2024) — PMC11506176 | Sensory integration intervention is evidence-based practice for ASD | 16 studies, 2013–2023 | |
Meta-analysis (World J Clin Cases, 2024) — PMC10955541 | SI therapy promotes social skills, adaptive behaviour, sensory processing | 24 studies | |
Indian RCT (2019) — DOI: 10.1007/s12098-018-2747-4 | Home-based sensory interventions: significant measurable outcomes | Indian paediatric population | |
NCAEP Evidence-Based Practices (2020) | Visual supports, parent-implemented interventions: EBP for autism | National clearinghouse | |
WHO CCD Package — PMC9978394 | Caregiver-implemented home interventions: efficacy in 54 LMICs | Global implementation |





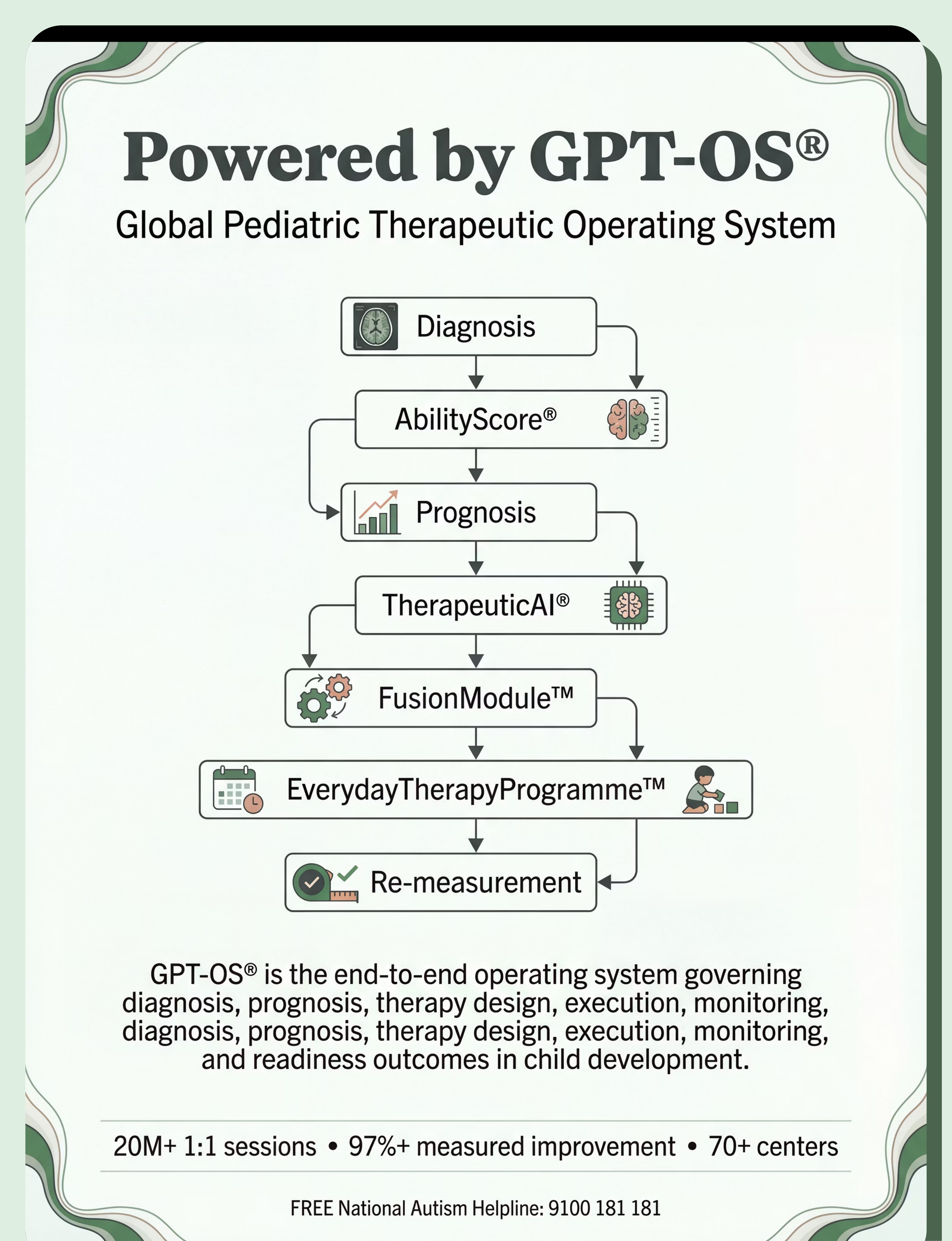
"The brain doesn't organize by therapy type. After-school collapse involves sensory systems, behavioral systems, emotional systems, and academic systems — simultaneously. That's why one discipline alone is never sufficient." — Pinnacle Blooms Consortium Clinical Advisory

What You'll See | When | What It Means | |
Child walks to decompression space | Week 1–2 | Environmental support working | |
Child says "I need space" | Week 3–4 | Self-awareness emerging | |
Recovery under 30 min | Week 5–8 | Regulatory capacity building | |
Child uses kit independently | Month 2–3 | Self-regulation developing |


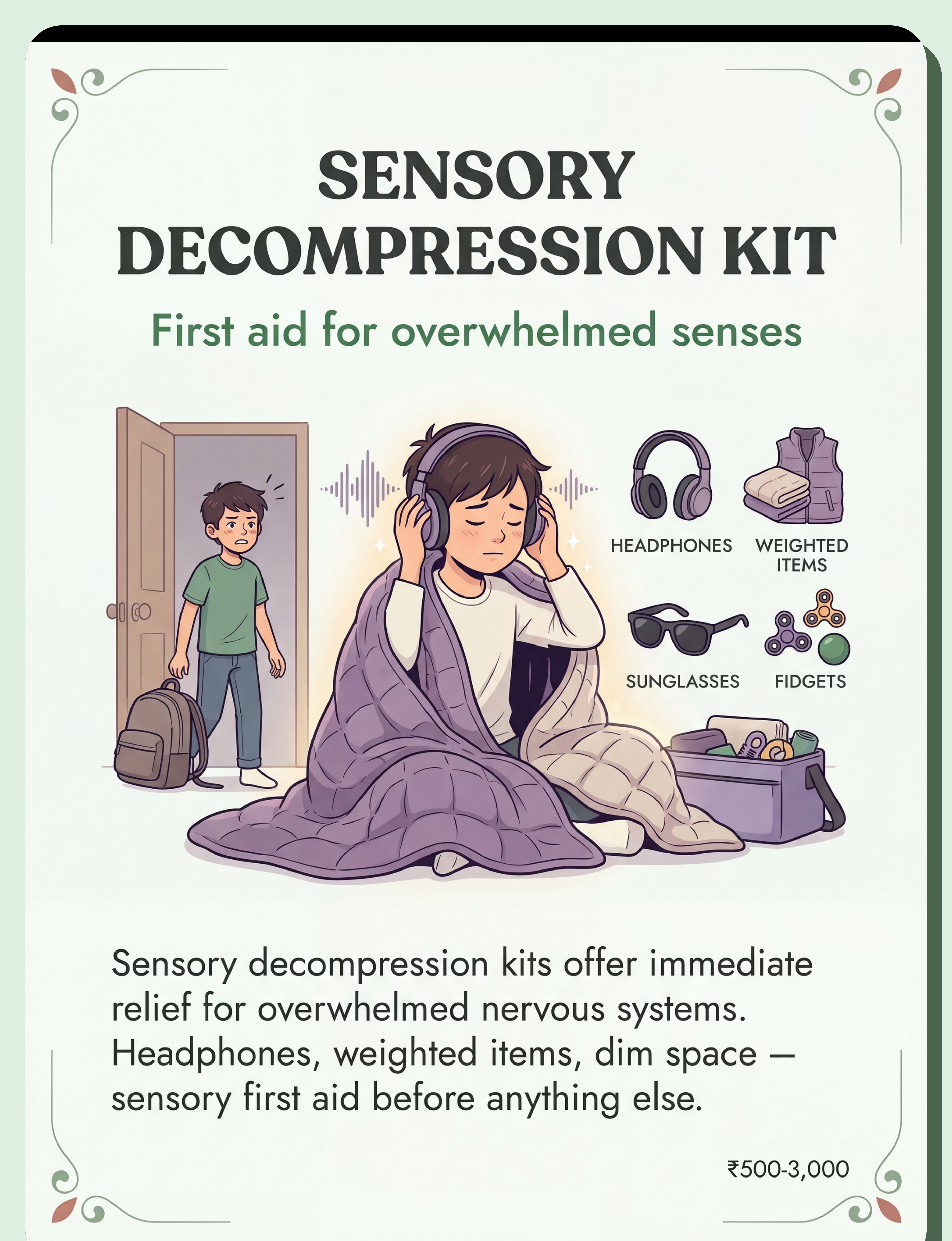
- Noise-canceling headphones or ear defenders
- Sunglasses or tinted glasses
- Weighted lap pad
- Compression vest
- Preferred fidgets
- Calming aromatherapy
- Chewy tube

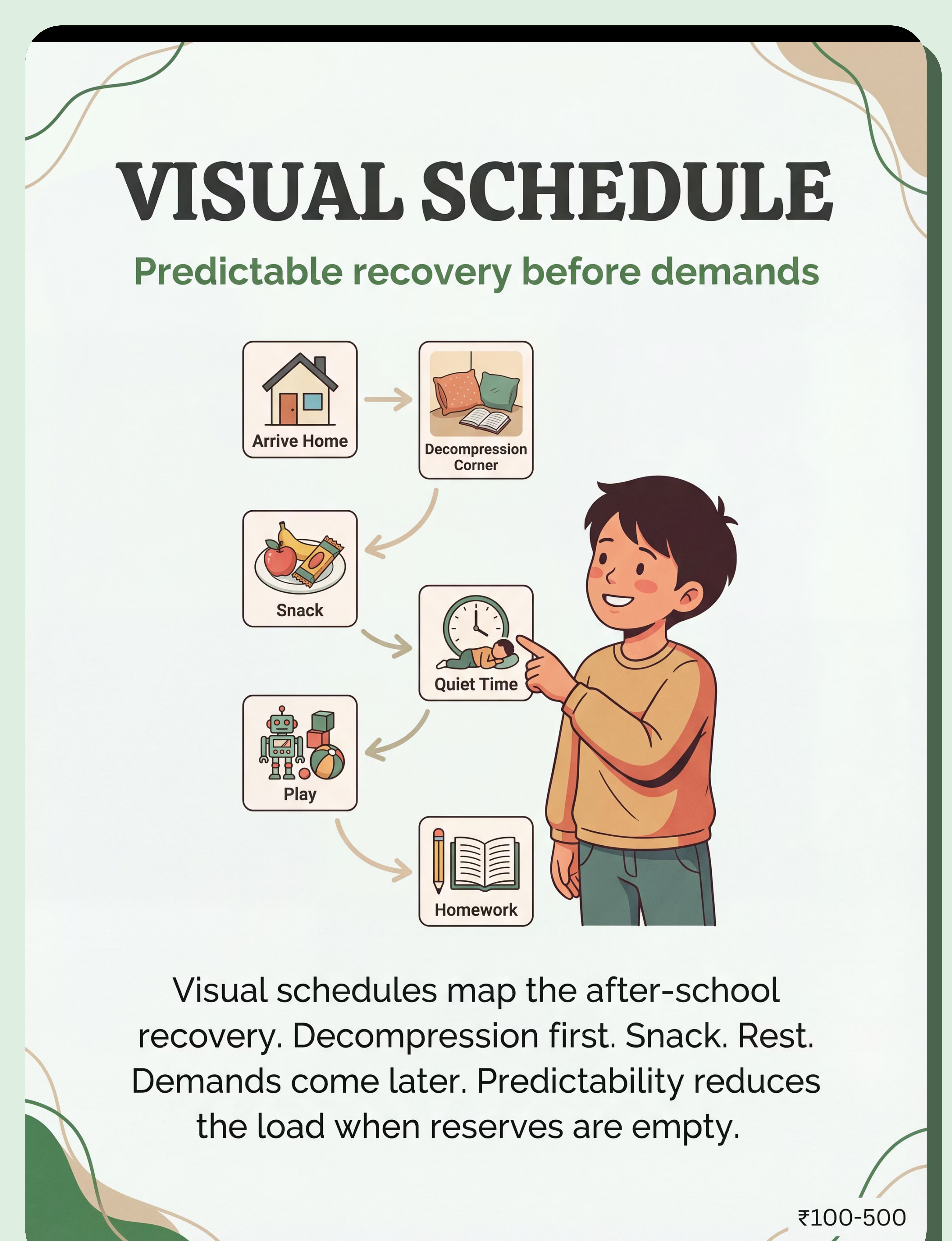
- Printed or velcro visual schedule cards
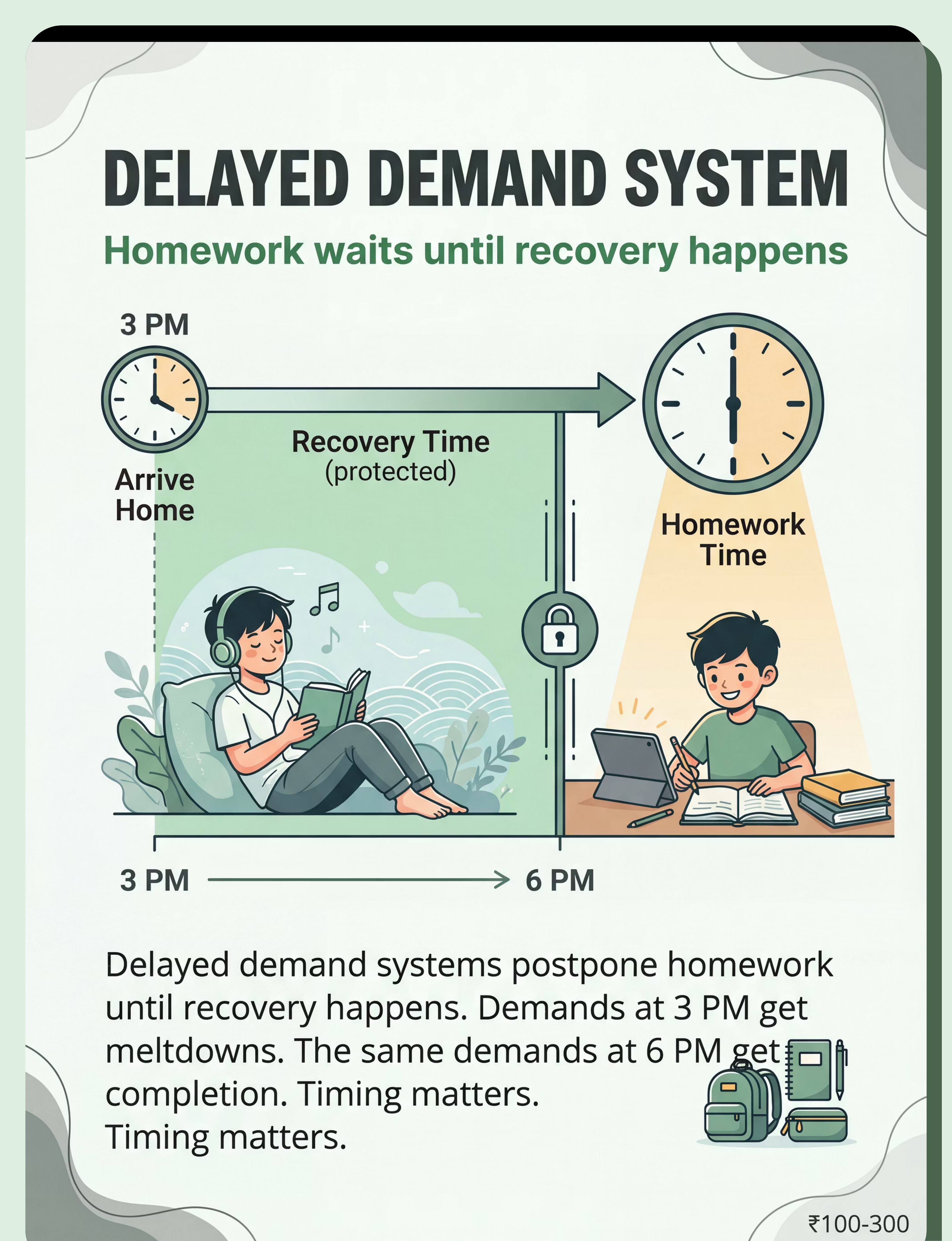
- After-school sequence: Arrive → Decompress → Snack → Rest → Play → (later) Homework
- First/Then board for immediate transitions


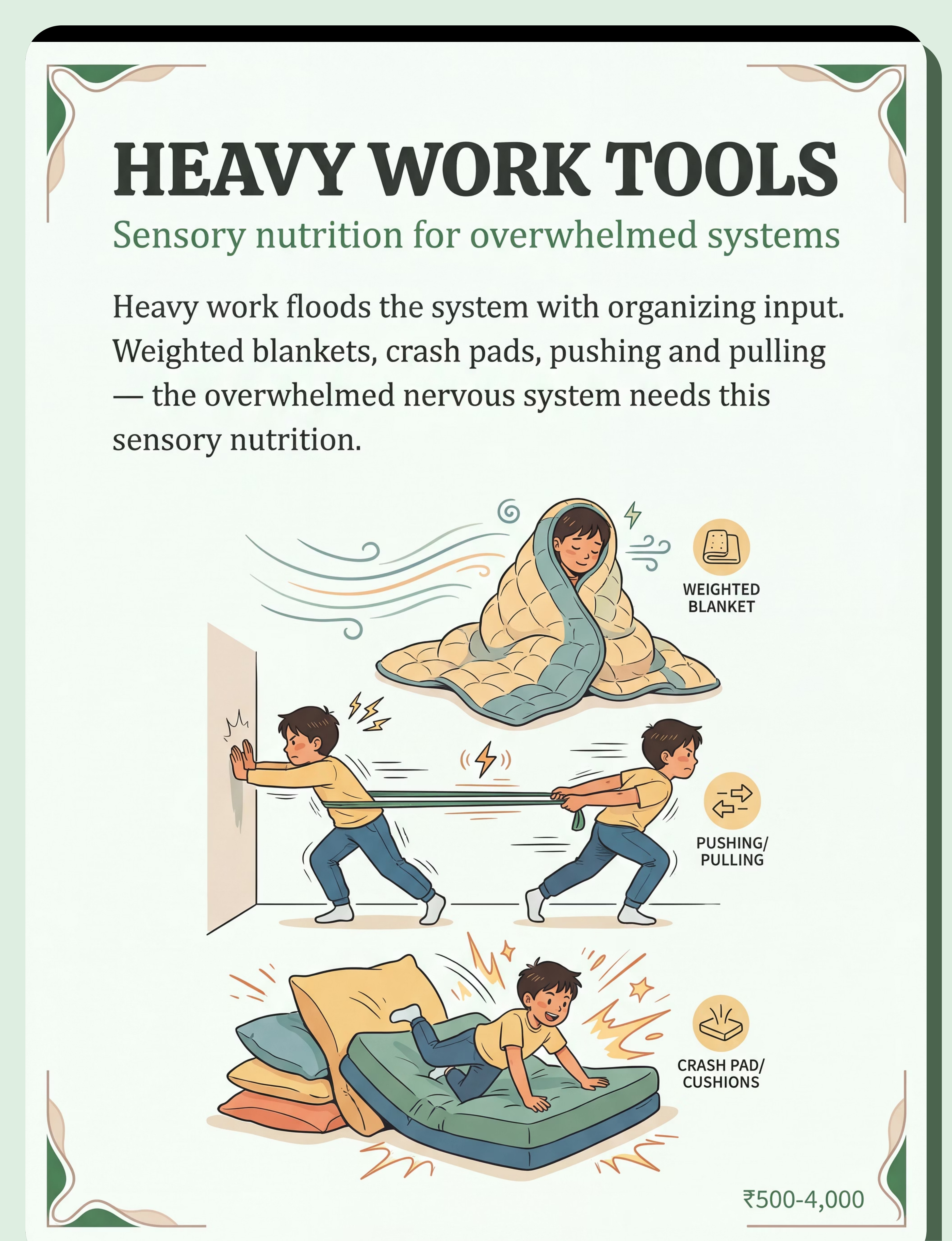
- Weighted blanket (10% child body weight)
- Weighted lap pad
- Crash pad or thick cushions
- Resistance bands
- Body sock or compression tunnel
- Mini trampoline

- Agreed-upon connection ritual (your child helps design it)
- Visual "no questions zone" reminder
- Timer for protected connection time
- Comfort items for shared moment

- Visual homework time marker
- Timer showing protected recovery time
- Homework station (set up for later — not visible from decompression corner)
- Written family agreement on homework timing


Material | Buy Option | DIY/Free Version | Why It Works | |
Sensory Decompression Kit | ₹500–3,000 | Earmuffs (airport/hardware) + sunglasses + heavy quilt + stress ball from kitchen | Same sensory principles — reduces auditory, visual, proprioceptive overload | |
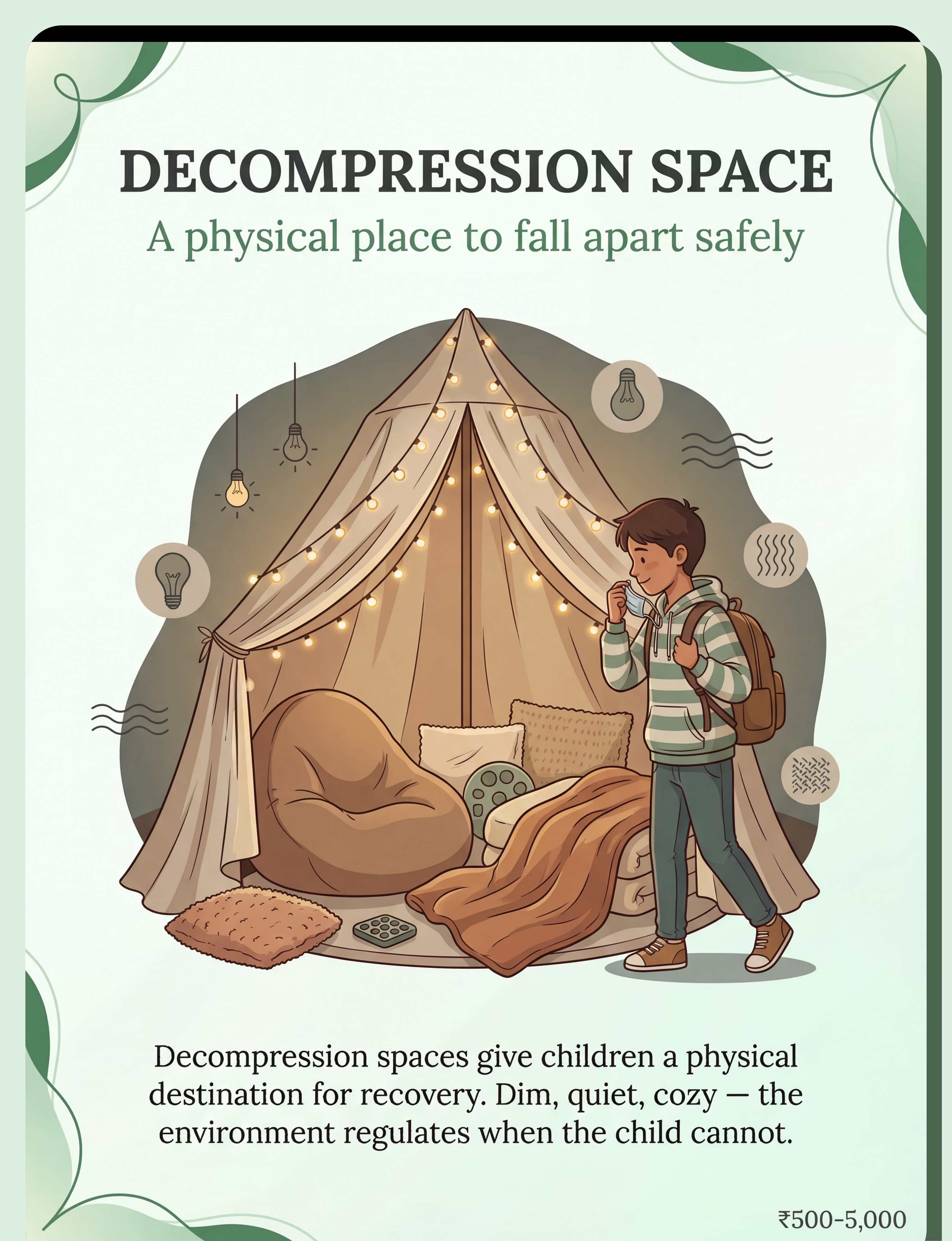
Decompression Space | ₹500–5,000 | Blanket draped over 2 chairs + fairy lights + pillows from bedroom | Enclosed feeling + dim light = parasympathetic activation | |
Visual Schedule | ₹100–500 | Hand-drawn cards on A4 paper + clothespins on string | Predictability works regardless of production quality | |
Heavy Work Tools | ₹500–4,000 | Heavy backpack walks, laundry basket pushing, pillow squishing, wall push-ups | Proprioceptive input is the goal — tools are delivery mechanisms | |
Snack Station | ₹100–300 | Any protein + preferred crunchy/chewy item + water — prepared before pickup | Physiological restoration requires food — not special food | |
Movement Outlets | ₹500–5,000 | Running in the street, jumping on mattress, obstacle course of household furniture | Cortisol discharge via movement — any vigorous safe movement works | |
Parent Regulation | ₹0–500 | 4-7-8 breathing, mantra card on the fridge, texting a friend during crisis | Co-regulation requires a regulated adult — zero cost to regulate yourself |

- Child is currently mid-meltdown and in an unsafe physical state (hitting, biting, self-harm) — Wait for the acute episode to pass
- You are in a dysregulated state yourself — You cannot co-regulate from dysregulation
- Collapse includes self-harm, aggression with injury potential, or dangerous property destruction
- Child is unwell, feverish, or in physical pain — address medical needs first
- Child is in the 0–15 minute acute collapse window — Use passive support only (silent presence, offer sensory kit without demands, no questions)
- Weighted items feel distressing — never apply weighted tools against the child's resistance
- Child refuses decompression space — Offer, never force; the space works only when voluntary
- Child has moved past the acute peak (first 15–20 minutes)
- Environment is prepared and materials are accessible
- You (parent) are regulated and can provide calm presence
- Child is not hungry (snack first if needed)
- Decompression kit assembled and accessible (by door or in space)
- Snack prepared and waiting — no preparation needed on arrival
- Decompression space: dim lights on, weighted blanket set out, fidgets accessible
- Homework station visible but distant from decompression area
- Television and audio off or minimal
- Bright overhead lights off, lamps on low
- YOUR regulation: take 3 breaths before leaving for pickup
- 🚪 Decompression kit meets child at the door
- 🛋️ Decompression corner: dim, enclosed, quiet — primary destination
- 🍎 Snack station in kitchen — waiting, no prep required
- ✏️ Homework station: set up but not visible from decompression corner
- 📺 TV off | 🔊 Music off | 🌟 Bright lights reduced
60-Second Readiness Check — Run This Every Afternoon
ACT III — Execution Before beginning the protocol, spend 60 seconds assessing the conditions. The best session is one that starts right. A 10-minute supported recovery beats a 30-minute forced protocol every time. ALL GREEN → Proceed Full 6-step protocol — Card 14 (Arrival Invitation) SOME AMBER → Simplify Decompression space + snack only. No active steps 3–6. ANY RED → Wait Passive support only. Call 9100 181 181 if persistent.



- Weighted blanket wrapping (10% body weight, 20-min max)
- Wall push-ups (10–15 reps)
- Carrying heavy items (grocery bags, laundry basket)
- Animal walks: bear walk, crab walk, wheelbarrow walk

- Mini trampoline jumping (5–10 minutes)
- Running circuit in garden or hallway
- Crash pad diving (supervised)
- Resistance band pulling/pushing against doorframe
- Pillow pile crashing

- Gentle swinging (indoor or outdoor swing)
- Rocking on beanbag
- Back-and-forth movement in chair
🟢 Read alongside each other
🟢 Physical proximity — same room, occasional light touch if welcome
🔴 NOT: "Tell me about your day. What happened?"


Standard: Typical collapse day — Full 6-step sequence.
Expanded: During transitions (new school year, testing) — Extend all phases by 50%, defer homework entirely.

- Child walks toward decompression space without being guided (even once)
- Child accepts headphones when offered without throwing them
- Collapse DURATION shortens by even 10–15 minutes
- Physical aggression reduces in frequency even if not in intensity
- Child seems to anticipate snack or decompression (shows routine awareness)
- One afternoon that was "better than usual" — that's real progress
- Independent self-regulation (this takes months, not days)
- Happy, cooperative homework completion
- "Normal" afternoons
- Complete elimination of collapse



- ✓ Self-initiated recovery: Child reaches for decompression kit without being offered it
- ✓ Self-awareness: "I'm overstimulated" or "I need heavy work"
- ✓ Reduced duration: Typical recovery under 20 minutes
- ✓ Functional evening: Dinner, essential tasks, bedtime without crisis
- ✓ Relationship intact: Collapse episodes don't dominate the relationship narrative
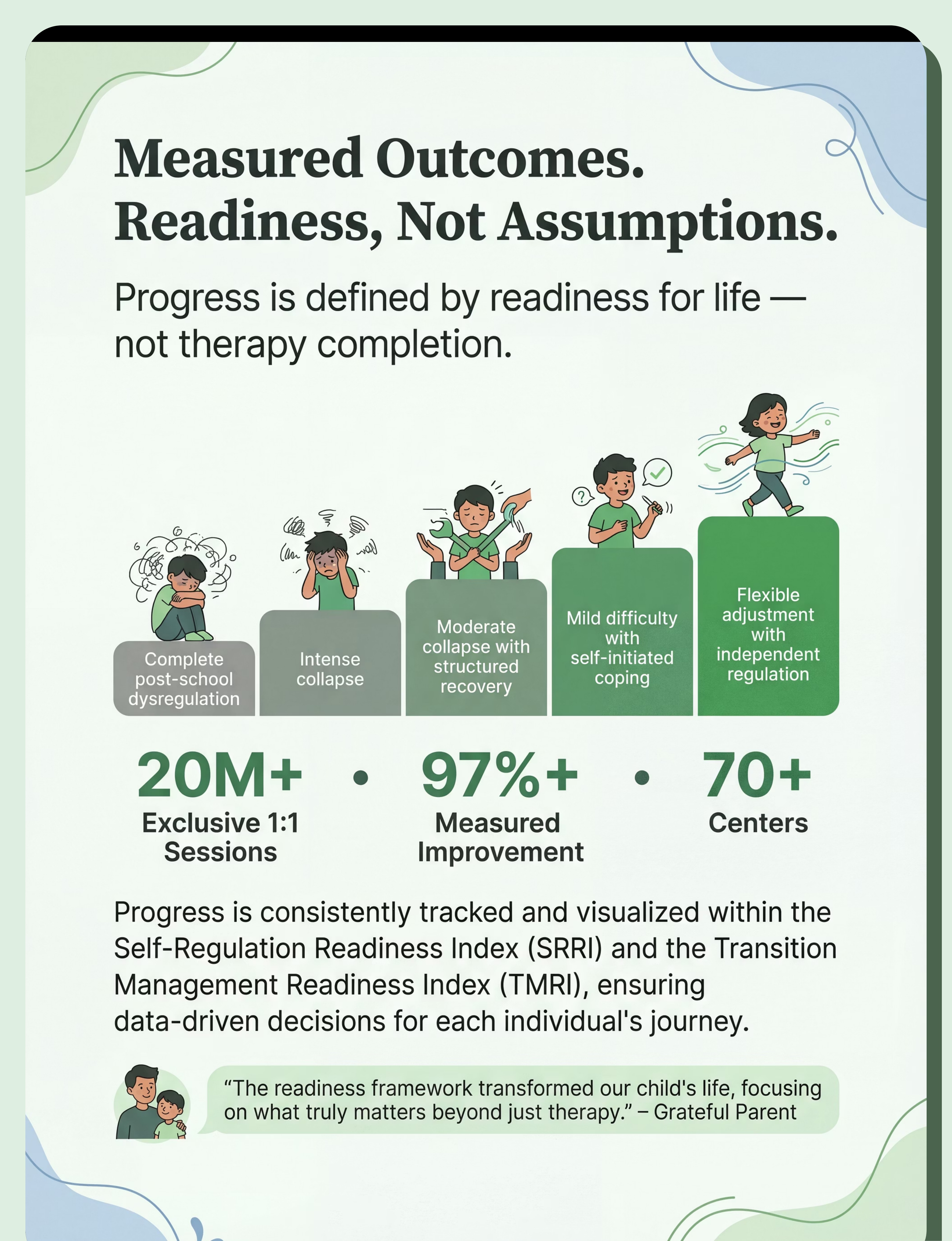
- ✓ Data trend: Self-Regulation Readiness Index showing consistent progression across 12 weeks
- After-school collapse regularly includes self-harm (head-banging, scratching, hitting self)
- Collapse includes aggression causing injury to parents, siblings, or property
- Child expressing thoughts of not wanting to be alive or hopelessness about school
- Collapse accompanied by school refusal — child cannot attend school
- Meltdowns last 3+ hours daily despite 4+ weeks of consistent protocol
- Parent experiencing daily crisis affecting their own mental health
- Protocol shows zero improvement after 4 consistent weeks
- New behaviours emerging (regression in other developmental areas)
- School is unresponsive to concerns about the academic/social load
- Child's collapse is affecting sibling development at a crisis level
- Child expresses strong negative feelings about school beyond typical resistance
Technique | Code | Difficulty | Materials You Have | |
Managing Big Emotions | C-251 | 🟡 Core | ✓ Same kit | |
After-School Collapse | C-252 | 🟡 Core | ✓ THIS PAGE | |
Morning Routine Struggles | C-253 | 🟡 Core | ✓ Same visual tools | |
Transition Meltdowns | C-265 | 🟠 Advanced | ✓ Most materials overlap | |
Zones of Regulation | C-272 | 🟠 Advanced | + Emotion cards needed | |
All Transitions | I-781 | 🟢 Intro | ✓ Same kit |
Preview of 9 materials that help with after school collapse Therapy Material
Below is a visual preview of 9 materials that help with after school collapse therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.







Every technique page in the Pinnacle network is developed by a consortium of licensed clinicians across occupational therapy, speech-language pathology, applied behaviour analysis, special education, and neurodevelopmental paediatrics. Every claim is referenced. Every recommendation is grounded in evidence. Every material suggestion serves the child, not a commercial interest. This is what it means to transform a home into a proven, scientific, 24×7 therapy centre for your child — not by replacing professional care, but by extending it into every moment of every day.
16+ Languages — 24×7 — FREE
© 2025 Pinnacle Blooms Network®, unit of Bharath Healthcare Laboratories Pvt. Ltd.