
Their Brain Won't Stop Listening — Even in Sleep.
Your daughter wakes at everything. The refrigerator cycling on. A car passing outside. Her sister turning over in the next room. Sounds you don't even register jolt her fully awake. Getting her back to sleep takes an hour. She's 7 years old and it's been like this since infancy. You're exhausted. She's exhausted. You are not failing — her nervous system is speaking.
"You are not failing. Your child's nervous system is speaking. And there are 9 evidence-based materials that help."
🧠 Pinnacle Blooms Consortium
🎯 Sensory Solutions Series — Episode A-052
👶 Ages 2–12
⏱ Auditory Processing + Sleep Regulation

You Are Among Millions.
Sound-triggered sleep disruption affects millions of families worldwide. When a child's brain cannot gate environmental sounds during sleep, the entire family's health deteriorates. This is not rare. This is not a phase. This is a documented neurological pattern — and it responds to intervention.
80%
Sensory Difficulties
of children diagnosed with autism display sensory processing difficulties (PRISMA Systematic Review, 2024 — PMC11506176)
86%
Sleep Disturbance
of children with ASD experience clinically significant sleep disturbance, with auditory sensitivity as a primary contributor (Frontiers in Neuroscience, 2020)
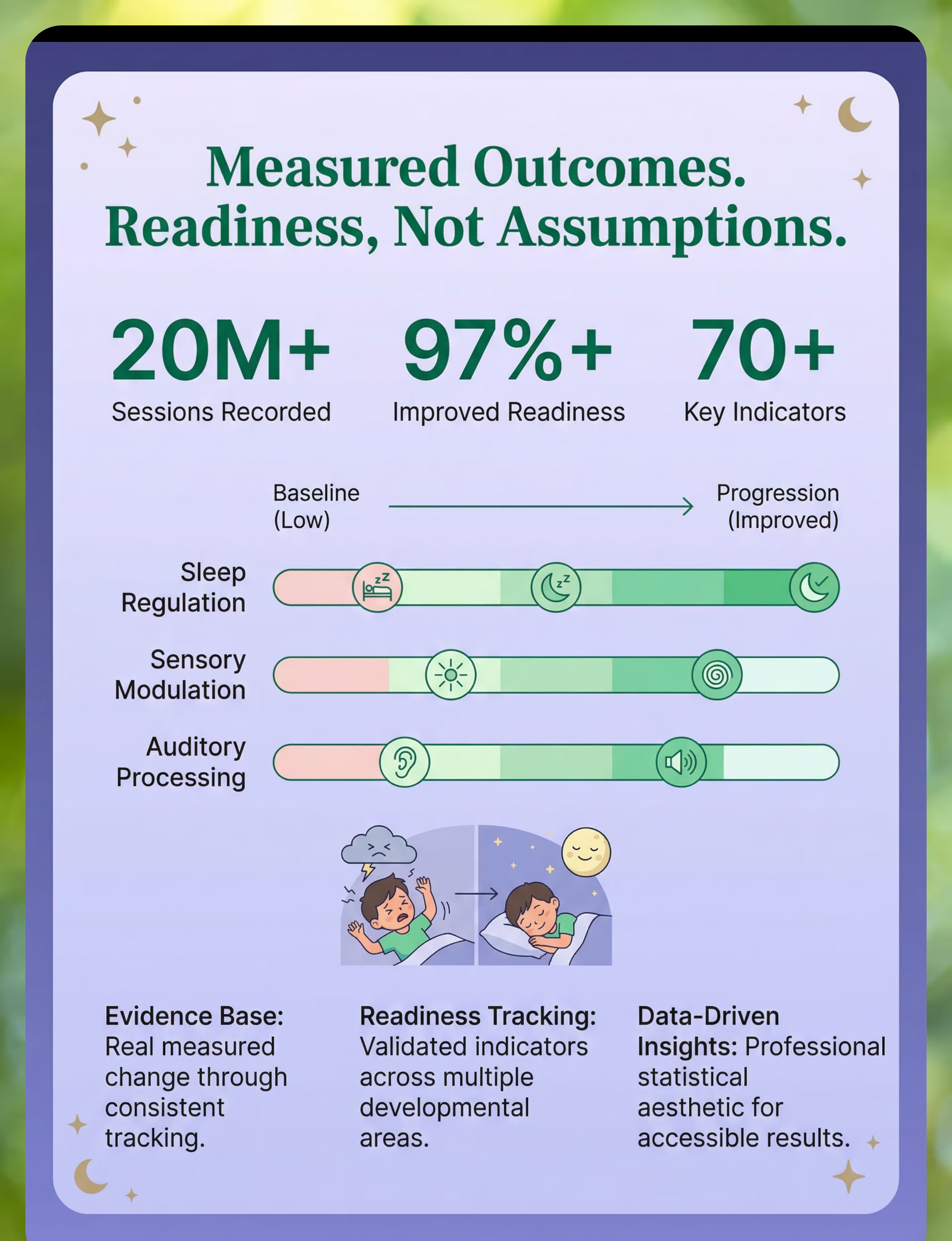
20M+
Therapy Sessions
delivered by the Pinnacle Blooms Network — the largest dataset of pediatric intervention outcomes on Earth
In India alone, an estimated 2–3 million children experience sensory-based sleep disruption. Pinnacle Blooms Network serves families across 70+ centers and from 70+ countries through GPT-OS® guided intervention.
Sources: PMC11506176 | PMC10955541 | DOI: 10.12998/wjcc.v12.i7.1260 | WHO Nurturing Care Framework (2018)

The Neuroscience: Why Their Brain Won't Filter Sound at Night
The Sound Gate
During typical sleep, a part of the brain called the reticular activating system acts as a gatekeeper. It decides which sounds are "safe" (the refrigerator humming, a car passing) and which need attention (a fire alarm, your name being called). Safe sounds get blocked before they reach conscious awareness. Your child sleeps through them.
When the Gate Stays Open
For children with auditory over-responsivity or sensory processing differences, this gating is less effective. Sounds that should be filed as "safe background" instead pass through the gate and trigger arousal. The brain treats a door closing the same as an alarm. The child wakes — not because they're being difficult, but because their brain is wired to stay vigilant.
A Wiring Difference, Not a Behavior Choice
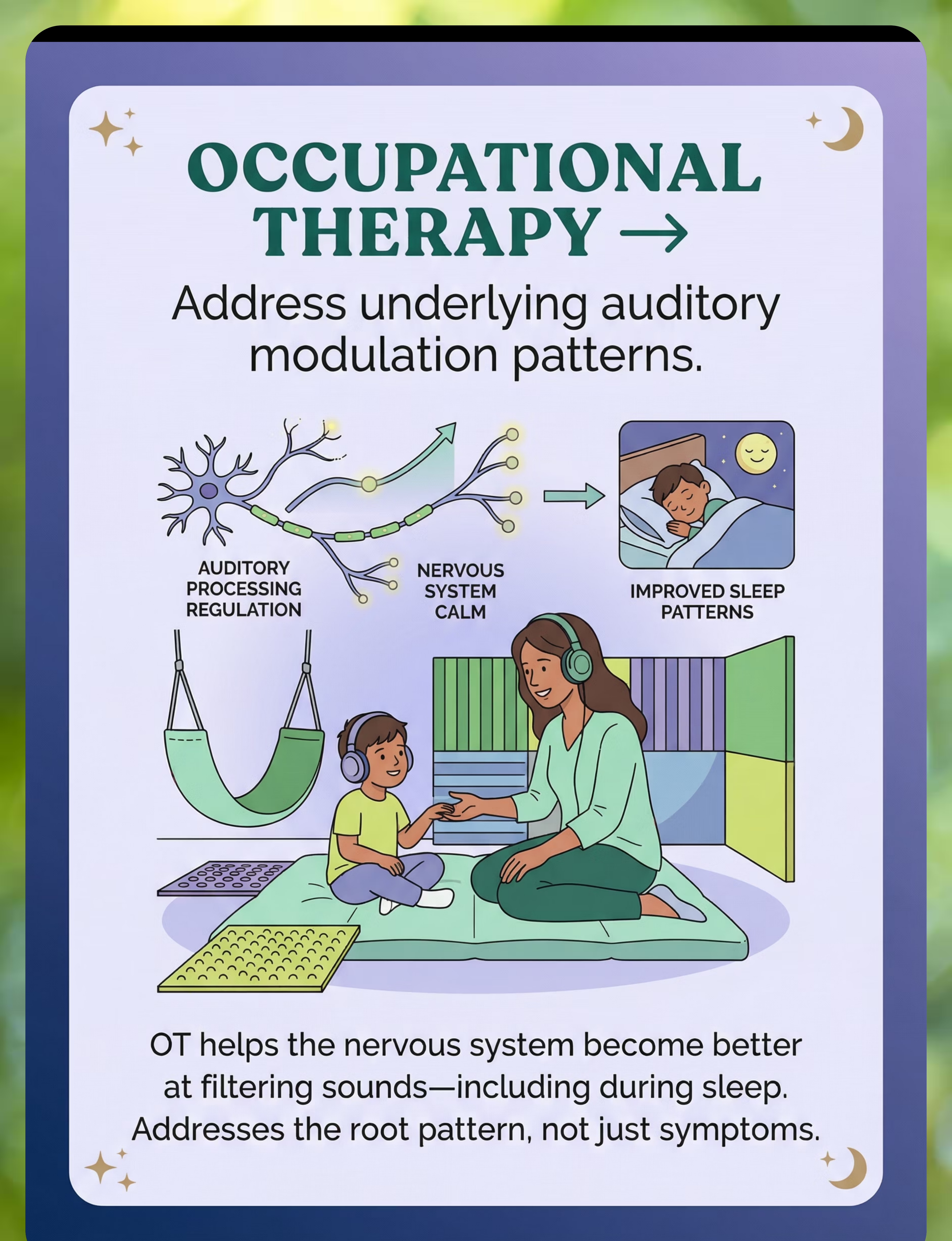
This pattern is neurological. It involves differences in how the auditory cortex processes input during sleep states and how the thalamus modulates arousal thresholds. It is documented in peer-reviewed research and responds to structured, multi-layered intervention.
Frontiers in Integrative Neuroscience (2020) — DOI: 10.3389/fnint.2020.556660 | Sensory Integration Theory (Ayres, 1972)
Developmental Context: Sound-Triggered Sleep Disruption
0–6 Months
Startle reflex to loud sounds is typical. Sleep cycling developing.
6–18 Months
Sound gating during sleep begins to mature. Habituation to household sounds emerges.
18 Months–3 Years
Most children sleep through typical household sounds. Persistent waking = earliest red flag.
3–5 Years ⬅ Common Intervention Window
Auditory gating should be well-established. Sound-triggered sleep disruption strongly correlates with sensory processing differences.
5–8 Years ⬅ Critical Intervention Window
Without intervention, the pattern becomes entrenched. Secondary anxiety about sleep may develop.
8–12 Years
Child may develop compensatory strategies or the pattern may generalize. OT for auditory modulation shows strong evidence at this stage.
Comorbidity Awareness: Sound-triggered sleep disruption commonly co-occurs with daytime auditory sensitivity, tactile defensiveness, anxiety, ADHD-presentation symptoms (often driven by chronic sleep deprivation), and general sensory over-responsivity patterns.
Your child is here — on a developmental timeline with a clear forward path. These 9 materials target the mechanisms that keep the sound gate open.
WHO Care for Child Development (CCD) Package | PMC9978394 | UNICEF MICS developmental monitoring indicators across 197 countries

Clinically Validated. Home-Applicable. Parent-Proven.
Evidence Grade: Level I–II
This intervention approach is supported by systematic reviews, meta-analyses, randomized controlled trials, and large-scale clinical outcome data.
PRISMA Systematic Review (2024)
16 articles from 2013–2023 confirm sensory integration intervention meets criteria to be considered evidence-based practice for children with ASD. (PMC11506176)
Meta-Analysis — World J Clin Cases (2024)
Sensory integration therapy effectively promotes social skills, adaptive behavior, sensory processing, and motor skills across 24 studies. (PMC10955541)
Indian RCT — Padmanabha et al. (2019)
Home-based sensory interventions demonstrated significant outcomes for parent-administered sessions. (DOI: 10.1007/s12098-018-2747-4)
WHO CCD Package (2023)
Age-specific evidence-based recommendations for caregivers, implemented in 54 low- and middle-income countries. (PMC9978394)
Pinnacle Network Real-World Evidence
20M+ exclusive 1:1 sessions with 97%+ measured improvement across readiness indexes — the largest integrated pediatric therapy outcome dataset globally.
85%
Evidence Confidence
Strong evidence for multi-layered sensory-based sleep intervention. Individual material evidence ranges from strong (environmental modification, sensory calming) to emerging (specific sound masking protocols).

🌙🔇 Multi-Layered Sound Management for Sleep
Parent-Friendly Name: "Helping Your Sound-Sensitive Child Sleep Through the Night"
A structured, multi-layered intervention protocol combining 9 categories of materials and strategies to address sound-triggered sleep disruption in children with auditory processing differences. Rather than relying on a single solution, this approach creates overlapping layers of intervention — environmental sound reduction, active sound masking, direct ear protection, nervous system regulation, and underlying auditory processing intervention — that together reduce the frequency and severity of sound-triggered sleep disturbance.
Each layer addresses a different mechanism. Families implement layers progressively based on the child's specific profile and tolerance. The cumulative effect is far greater than any single intervention alone.
Domain
Sensory Processing + Sleep Regulation (Domain A — Sensory)
Age Range
2–12 years
Frequency
Daily (nightly)
Duration
Ongoing with progressive modification

This Technique Crosses Therapy Boundaries — Because the Brain Doesn't Organize by Therapy Type
At Pinnacle Blooms Network, these disciplines operate under a single converged system — GPT-OS® FusionModule™ — ensuring that the OT's sensory recommendations, the ABA specialist's behavioral protocols, and the pediatrician's medical oversight operate as one coordinated plan, not four separate opinions.
Precision Targets — This Is Not a Random Activity
🎯 Primary Target
Auditory gating during sleep. Observable: Reduced frequency of sound-triggered night wakings from 4–5 per night toward 0–1. Reduced time to fall asleep in non-silent environments.
🎯 Secondary Targets
Sleep onset latency under 30 minutes. Sleep maintenance with consolidated blocks. Parasympathetic shift enabling sleep readiness. Daytime auditory tolerance improvement.
🎯 Tertiary Targets
Cognitive function (memory, attention, learning). Emotional regulation. Family functioning. Long-term developmental trajectory. Observable: Improved daytime behavior, attention, and emotional regulation.
Reference: PMC10955541 (Meta-analysis: sensory integration therapy targets across multiple developmental domains)

Your Materials Kit — Everything You Need
Pinnacle Recommends: Start with Material #7 (free household fixes) + #8 (bedroom audit) + #1 (gradual noise introduction). These three layers cost little and provide the foundation.
# | Material | Canon Category | Price Range | Purchase | |
1 | White/Pink Noise Machine (LectroFan, Yogasleep, Hatch) — variable volume, multiple sound profiles | White Noise & Sound Machines | ₹500–5,000 | 🛒 Amazon.in | |
2 | Soft Sleep-Safe Ear Protection (Mack's Pillow Soft silicone, CozyPhones sleep headband) | Noise-Reducing Headphones & Ear Defenders | ₹300–3,000 | 🛒 Amazon.in | |
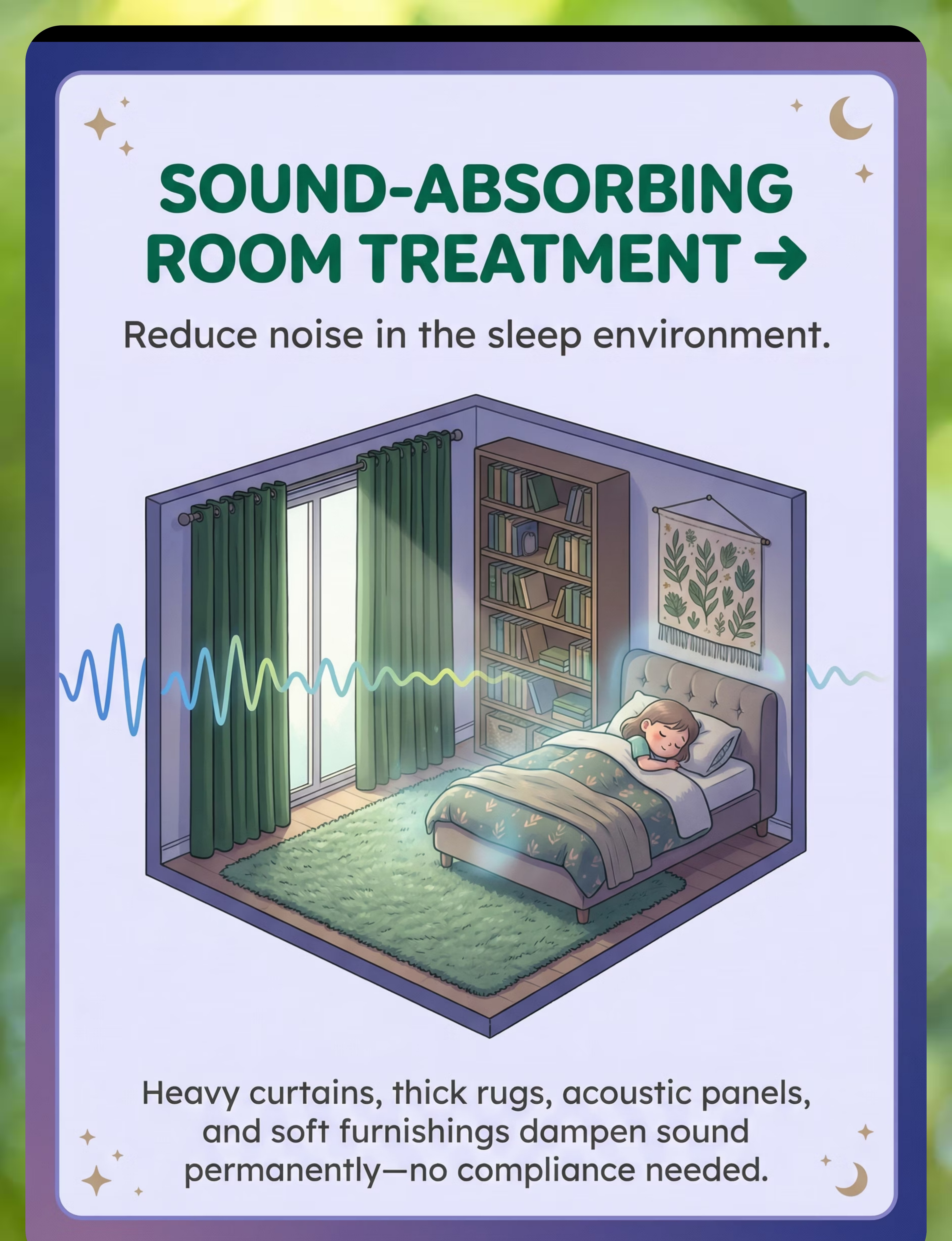
3 | Sound-Absorbing Room Treatment (Heavy blackout curtains, thick rug, acoustic panels, fabric wall hangings) | Specialty Bedding & Sleep Environment | ₹2,000–30,000 | 🛒 Amazon.in | |
4 | Consistent Sleep Sound Ritual Kit (Calm/Moshi sleep story app, Bluetooth speaker, timer) | Sleep Routine Supports | ₹0–2,000 | 🛒 Amazon.in | |
5 | Sensory Calming Tools (Weighted blanket max 10% body weight, compression pajamas, massage lotion, dim red night light) | Weighted Blankets & Compression Vests | ₹500–8,000 | 🛒 Amazon.in | |
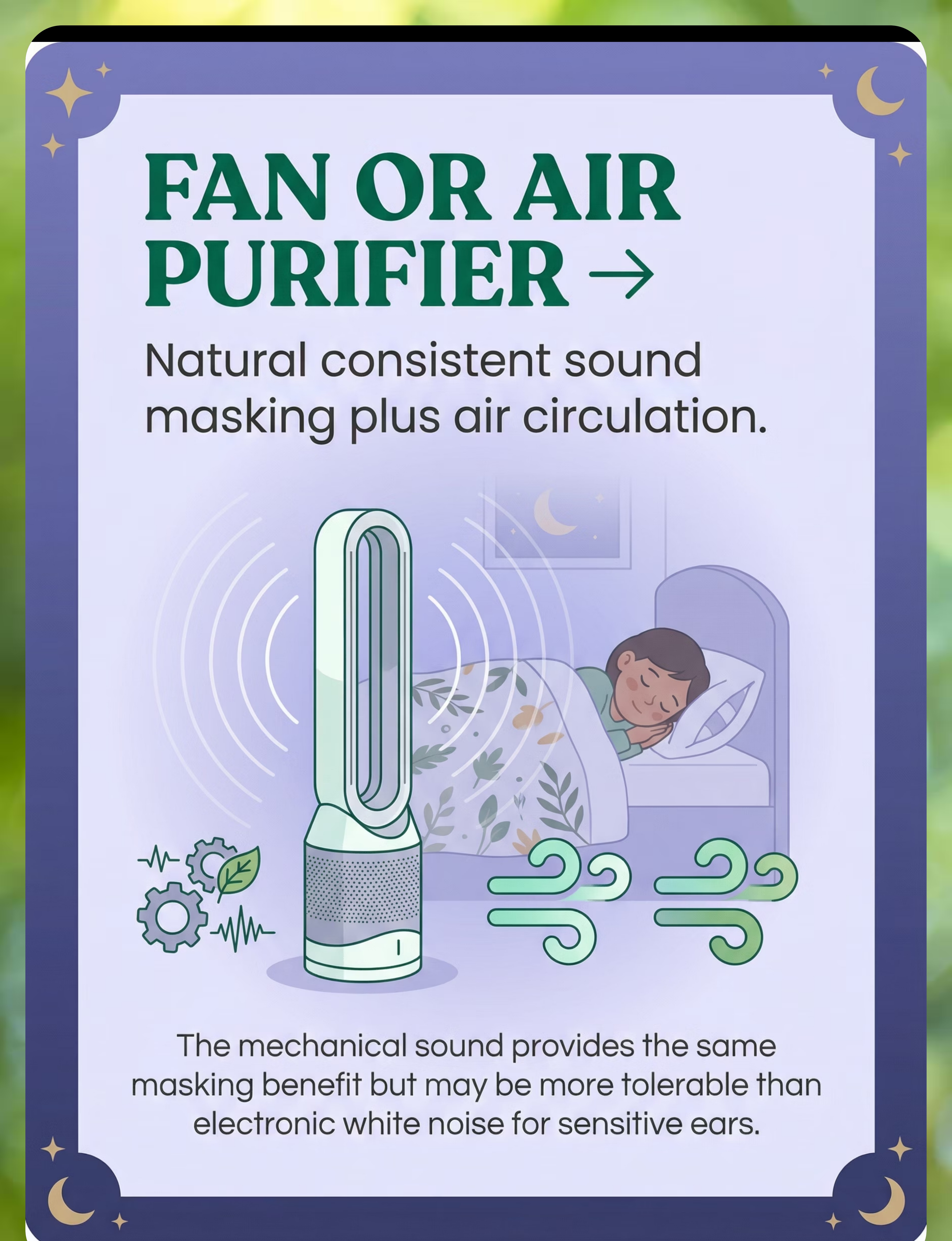
6 | Sound-Masking Fan or Air Purifier (Tower fan, HEPA air purifier — dual function) | White Noise & Sound Machines | ₹1,500–10,000 | 🛒 Amazon.in | |
7 | Household Sound Management Kit (Door hinge lubricant, soft-close dampers, felt furniture pads, draft stoppers) | General Home Environment | ₹0–2,000 | 🛒 Amazon.in | |
8 | Bedroom Layout Optimization (Room assessment, bed repositioning, furniture barriers) | Sleep Environment | ₹0–5,000 | DIY — see Card 10 | |
9 | Occupational Therapy for Auditory Modulation (Professional OT evaluation + home program) | Professional Services | ₹1,000–3,000/session | 📞 9100 181 181 |
Total Investment Range: ₹0–30,000+ (many strategies are zero-cost)

Every Family Can Start Tonight — Regardless of Budget
WHO/UNICEF Equity Principle: Not every family can order from Amazon. These zero-cost and ultra-low-cost alternatives use the same sensory and acoustic principles as clinical-grade materials. The CCD Package implemented across 54 low- and middle-income countries demonstrates that household-material-based interventions deliver measurable outcomes.
💰 Buy This
Clinical or commercial product options
🛠 Make This
Zero-cost or ultra-low-cost household alternatives
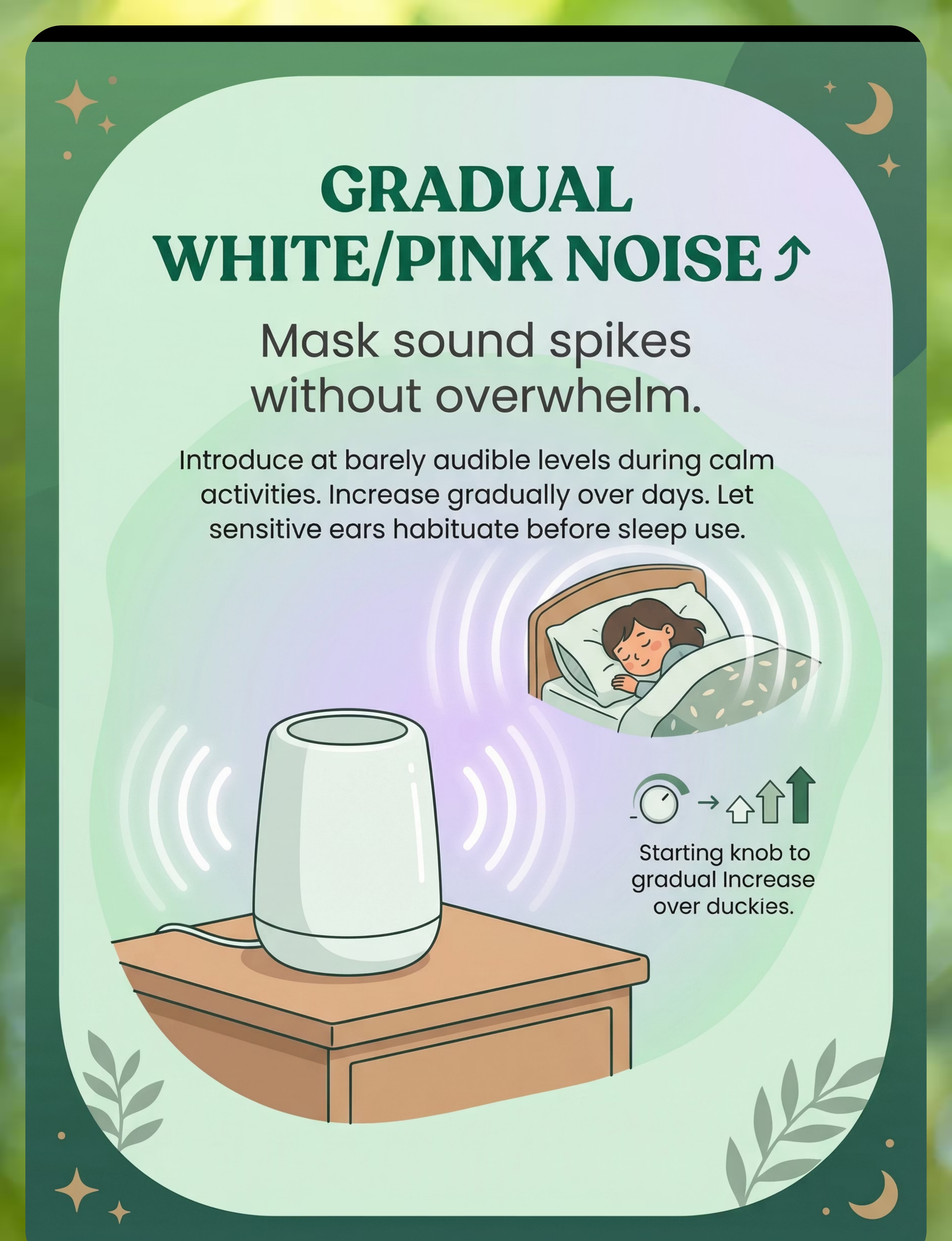
Material 1 — White/Pink Noise
Buy: Dedicated sound machine (₹500–5,000)
DIY: Free smartphone app (myNoise, White Noise Lite, Rain Rain). Try pink or brown noise — often more tolerable for sensitive ears. Start barely audible. Increase 5% every 2–3 days.
DIY: Free smartphone app (myNoise, White Noise Lite, Rain Rain). Try pink or brown noise — often more tolerable for sensitive ears. Start barely audible. Increase 5% every 2–3 days.
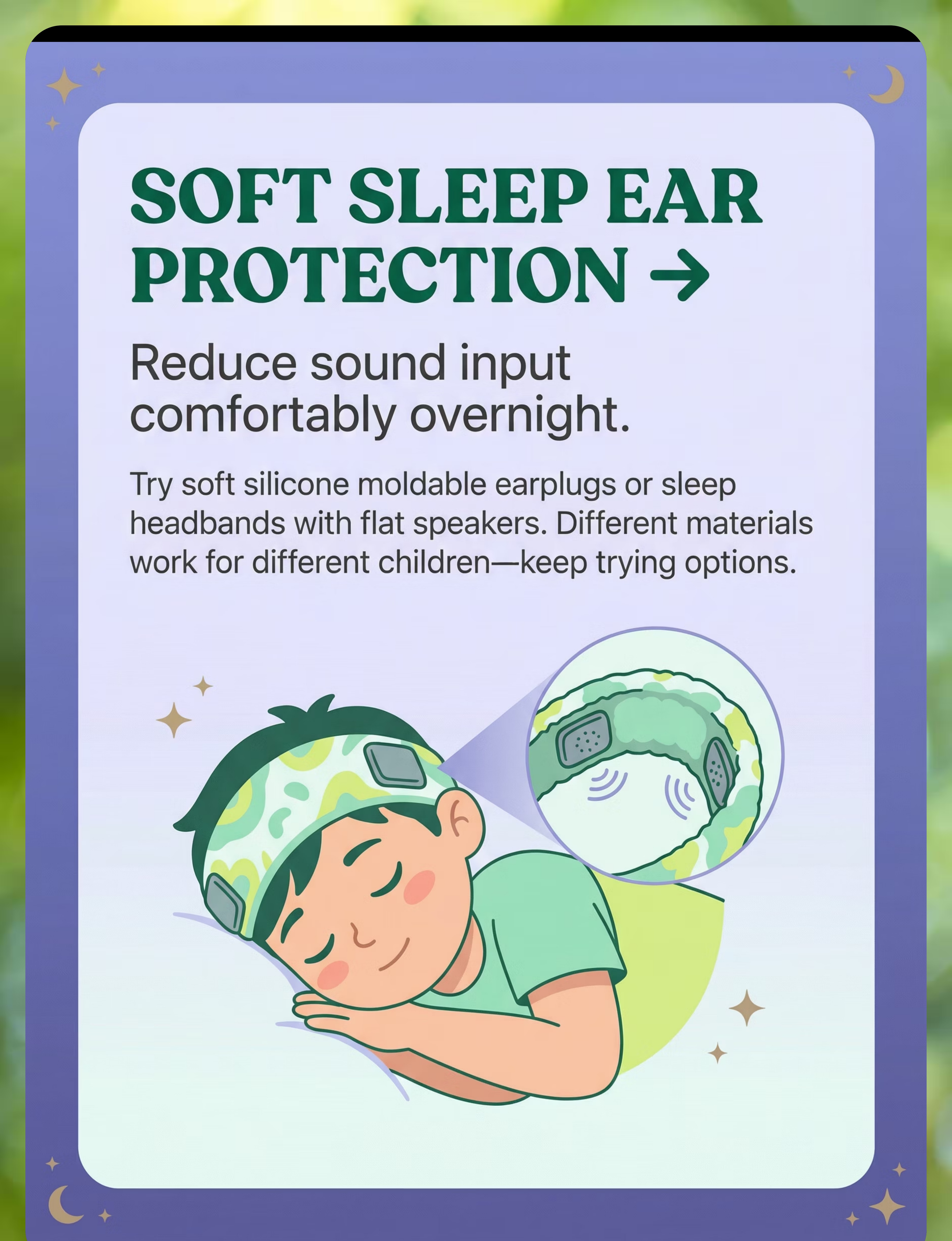
Material 2 — Ear Protection
Buy: Silicone putty earplugs or sleep headband (₹300–3,000)
DIY: For older children, soft cotton balls loosely placed (NOT inserted into ear canal). Sleep headband from soft stretchy fabric with flat pocket for flat earbuds. Reduces ambient sound and provides mild compression.
DIY: For older children, soft cotton balls loosely placed (NOT inserted into ear canal). Sleep headband from soft stretchy fabric with flat pocket for flat earbuds. Reduces ambient sound and provides mild compression.
Material 3 — Room Sound Treatment
Buy: Acoustic panels and heavy curtains (₹2,000–30,000)
DIY: Hang thick blankets or quilts on walls facing noise sources. Place filled bookshelves against shared walls. Lay thick duvets as floor rugs. Stuff door gaps with rolled towels.
DIY: Hang thick blankets or quilts on walls facing noise sources. Place filled bookshelves against shared walls. Lay thick duvets as floor rugs. Stuff door gaps with rolled towels.
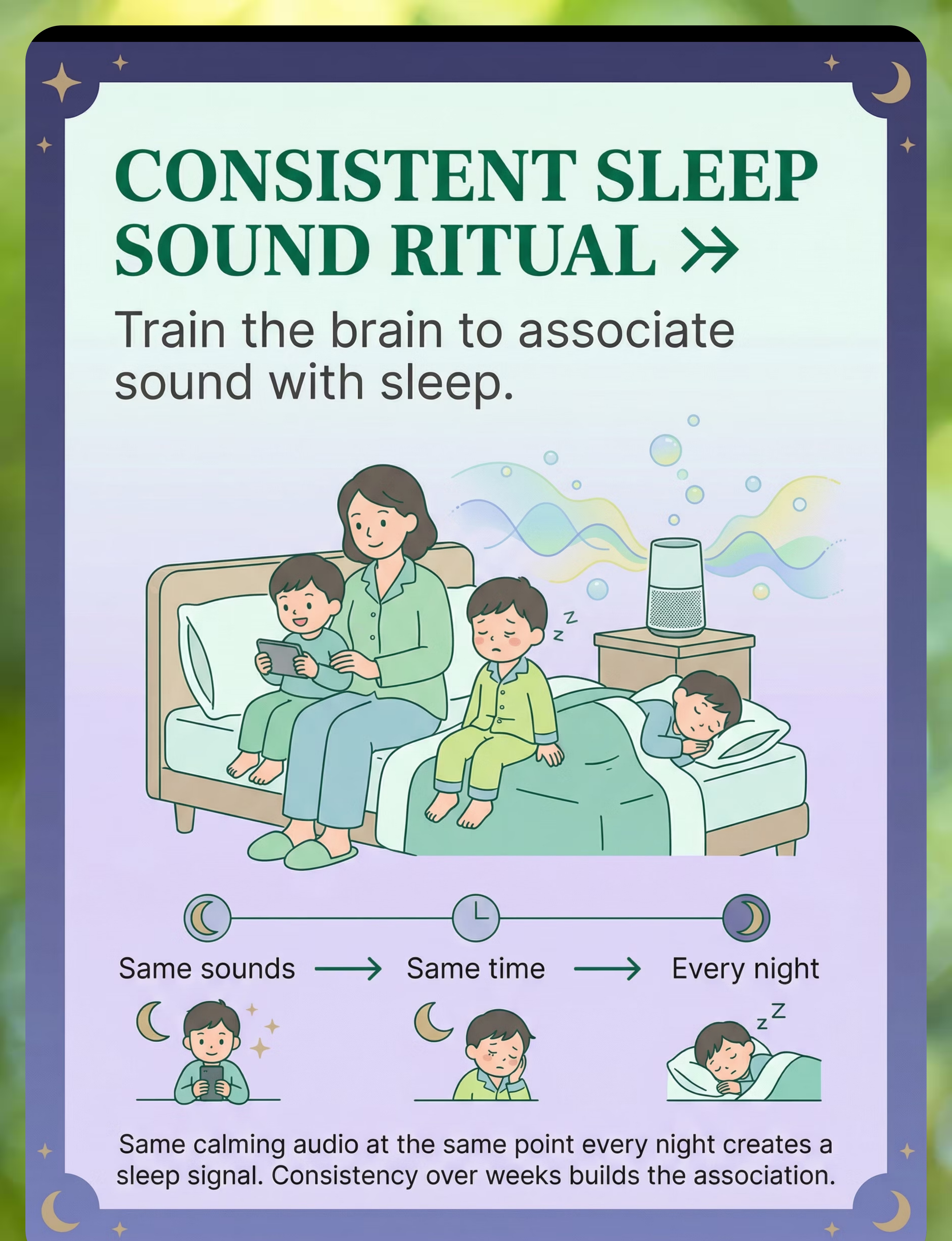
Material 4 — Sleep Sound Ritual
Buy: Sleep story app subscription (₹0–500/month)
DIY: Parent reads the same story at the same time every night in the same calm voice. Free YouTube playlists of rain/ocean sounds (screen off, audio only). Record your own voice — its familiarity may outperform any app.
DIY: Parent reads the same story at the same time every night in the same calm voice. Free YouTube playlists of rain/ocean sounds (screen off, audio only). Record your own voice — its familiarity may outperform any app.
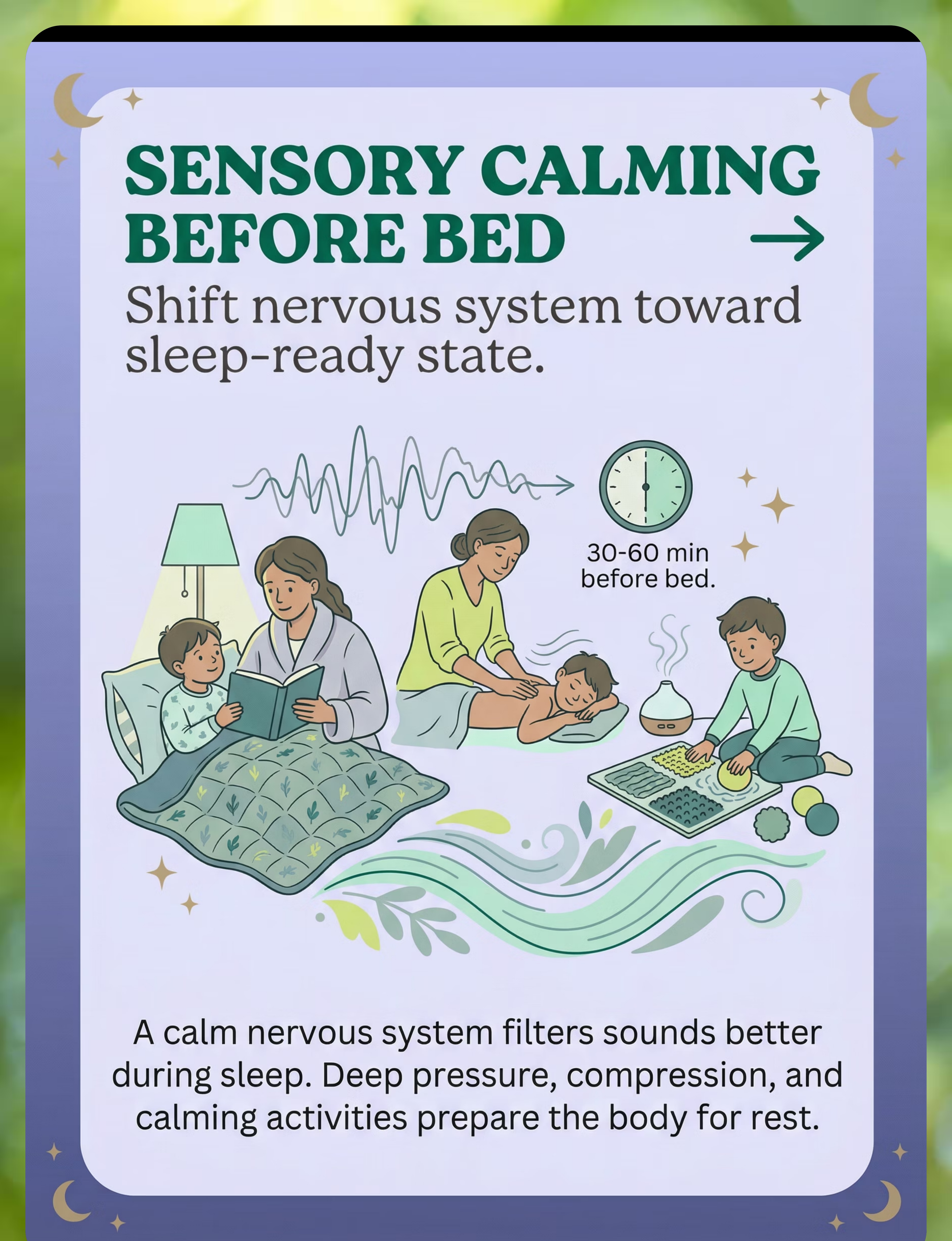
Material 5 — Sensory Calming
Buy: Weighted blanket, compression pajamas (₹500–8,000)
DIY: "Burrito roll" — wrap child firmly in a regular blanket. Firm slow massage with any lotion. Warm bath before bed. Stack two regular blankets for gentle distributed weight during reading time.
DIY: "Burrito roll" — wrap child firmly in a regular blanket. Firm slow massage with any lotion. Warm bath before bed. Stack two regular blankets for gentle distributed weight during reading time.
Material 6 — Fan/Air Purifier
Buy: Tower fan or HEPA purifier (₹1,500–10,000)
DIY: Any existing household fan positioned for sound benefit rather than air direction. Ceiling fan or old table fan placed away from the bed provides masking.
DIY: Any existing household fan positioned for sound benefit rather than air direction. Ceiling fan or old table fan placed away from the bed provides masking.
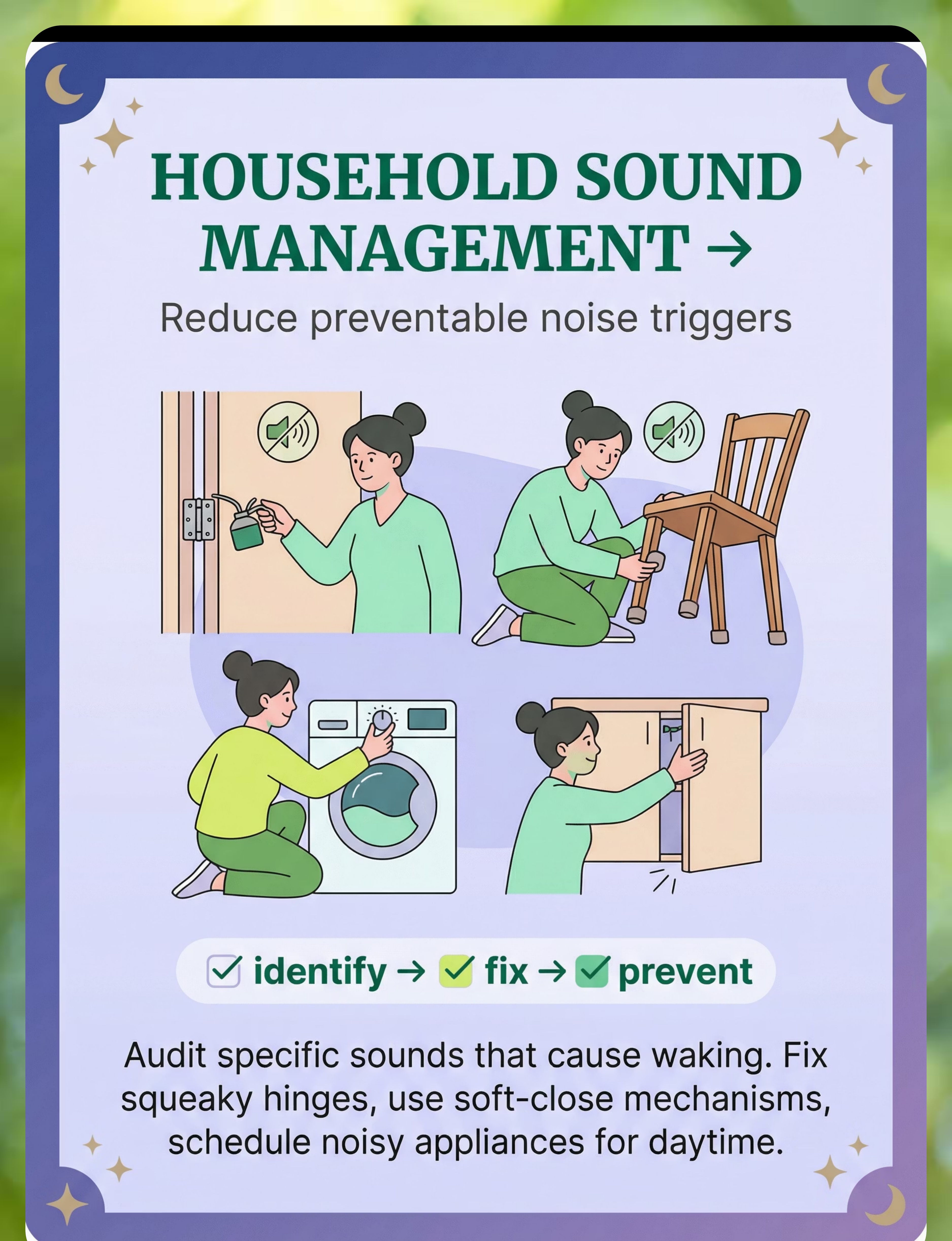
Material 7 — Household Sound Fixes
Buy: Soft-close dampers and felt pads (₹200–2,000)
DIY: Cooking oil on squeaky hinges. Old socks cut as furniture leg pads. Folded paper in rattling cupboard doors. Schedule noisy appliances for daytime only. Create a family "quiet hours" agreement poster.
DIY: Cooking oil on squeaky hinges. Old socks cut as furniture leg pads. Folded paper in rattling cupboard doors. Schedule noisy appliances for daytime only. Create a family "quiet hours" agreement poster.
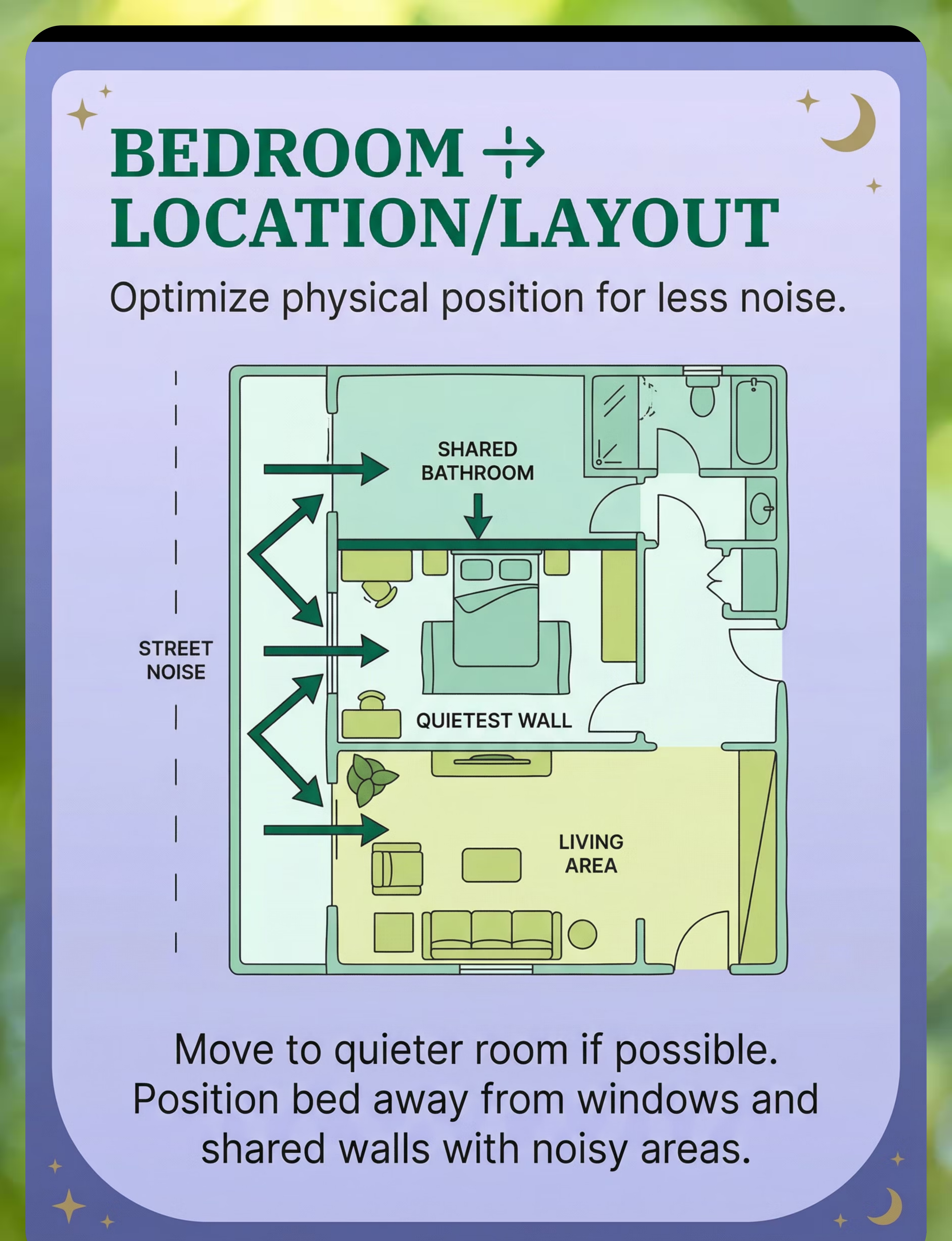
Material 8 — Bedroom Layout
Buy: Nothing required
DIY: Walk through your home during the child's sleep time. Note every sound source. Move the bed to the quietest wall. Place heaviest furniture between the bed and the noise source. If possible, swap rooms.
DIY: Walk through your home during the child's sleep time. Note every sound source. Move the bed to the quietest wall. Place heaviest furniture between the bed and the noise source. If possible, swap rooms.
Material 9 — OT Support
Buy: OT evaluation sessions (₹1,000–3,000/session)
Access: FREE initial consultation via Pinnacle National Autism Helpline — 9100 181 181. Teleconsultation available for remote families.
Access: FREE initial consultation via Pinnacle National Autism Helpline — 9100 181 181. Teleconsultation available for remote families.
Reference: WHO NCF Handbook (2022) | PMC9978394 (CCD Package equity-focused interventions across 54 LMICs)

Safety Gate — Read This Before Starting
🔴 DO NOT PROCEED IF:
• Child has known hearing loss or suspected hearing abnormality — see audiologist first
• Child has a medical sleep disorder diagnosis (sleep apnea, seizure-related disruption, severe restless leg syndrome)
• Child is under 3 years old and earplugs or small objects are being considered — choking hazard
• Weighted blankets are being considered for a child under 2 or who cannot independently remove the blanket
• Child shows signs of ear infection, ear pain, or recent ear surgery
• Child has a medical sleep disorder diagnosis (sleep apnea, seizure-related disruption, severe restless leg syndrome)
• Child is under 3 years old and earplugs or small objects are being considered — choking hazard
• Weighted blankets are being considered for a child under 2 or who cannot independently remove the blanket
• Child shows signs of ear infection, ear pain, or recent ear surgery
🟡 PROCEED WITH MODIFICATION IF:
• Child has anxiety about sleep or the dark — introduce new materials during daytime first, never force at bedtime
• Child has tactile defensiveness — ear protection may be rejected; use gradual introduction
• Family lives in a genuinely noisy environment — expect longer timeline
• Child is on medication affecting sleep — coordinate with prescribing physician
• Child has tactile defensiveness — ear protection may be rejected; use gradual introduction
• Family lives in a genuinely noisy environment — expect longer timeline
• Child is on medication affecting sleep — coordinate with prescribing physician
🟢 CLEAR TO PROCEED WHEN:
• Child is generally healthy with no active ear infections
• Sleep disruption pattern matches sound-triggered profile
• Family can commit to at least 2 weeks of consistent implementation
• Environment allows for some degree of modification
• Sleep disruption pattern matches sound-triggered profile
• Family can commit to at least 2 weeks of consistent implementation
• Environment allows for some degree of modification
Critical Safety Notes: Alarm awareness — ensure any ear protection or sound masking still allows the child to hear smoke alarms. White noise should stay under 65 dB at pillow position. Weighted products: no more than 10% of child's body weight, and many experts recommend against unsupervised overnight use for young children.
Reference: DOI: 10.1007/s12098-018-2747-4 (Indian RCT safety protocols for home-based sensory interventions)

The Sleep Environment Blueprint
Bedroom Setup: Numbered Positions
1. Bed position: Against the quietest (interior) wall, farthest from street. Head against solid wall, not under window.
2. Sound machine: 1–2 meters from bed, aimed toward primary noise source (window or door).
3. Fan/air purifier: Opposite side of room from bed — not blowing directly on child.
4. Heavy curtains: Covering all windows completely, extending 10–15 cm beyond frame on each side.
5. Rug: Large area rug covering most of the hard floor — the larger and thicker, the better.
6. Bookshelf/furniture barrier: Against any shared wall with a noisy room.
7. Door treatment: Draft stopper at base. Soft-close damper or felt pad on frame.
8. Night light: Dim red or amber only (not blue/white — suppresses melatonin). Low to ground.
2. Sound machine: 1–2 meters from bed, aimed toward primary noise source (window or door).
3. Fan/air purifier: Opposite side of room from bed — not blowing directly on child.
4. Heavy curtains: Covering all windows completely, extending 10–15 cm beyond frame on each side.
5. Rug: Large area rug covering most of the hard floor — the larger and thicker, the better.
6. Bookshelf/furniture barrier: Against any shared wall with a noisy room.
7. Door treatment: Draft stopper at base. Soft-close damper or felt pad on frame.
8. Night light: Dim red or amber only (not blue/white — suppresses melatonin). Low to ground.
What to REMOVE
- Hard, reflective surfaces (mirrors, glass frames adjacent to bed)
- Ticking clocks
- Electronics with audible hums or notification sounds
- Items that might fall or rattle in the night
Lighting & Temperature
- Temperature: 18–22°C is optimal for sleep
- Blackout curtains + dim red night light if needed
- No screens for 30–60 minutes before bed
Reference: PMC10955541 (Sensory Integration Theory — environmental setup as core principle; structured environments most effective)

Pre-Session Readiness: The 60-Second Check
Before implementing any new sleep material or strategy tonight, run through this checklist. The best session is one that starts right.
Child Health Check
Child is not currently ill (no fever, ear infection, stomach upset)
Regulation State
Child has not had a significant meltdown or dysregulation event in the past 2 hours
Nutrition
Child has eaten an appropriate evening meal (not hungry, not overly full)
Daytime Familiarization
The new material has been introduced during DAYTIME first — child has seen, touched, and is familiar with it
Environment Ready
Bedroom environment changes are complete (curtains hung, rug placed, sound machine positioned)
Safety Verified
All safety items checked (alarm audibility, weighted blanket weight, earplug size)
Caregiver Regulated
Parent/caregiver is emotionally regulated — your stress transmits. If you're anxious about tonight, that's data, not failure.
✅ All Checked → GO
Begin the bedtime protocol tonight with the first layer of intervention.
🟡 1–2 Unchecked → MODIFY
Introduce only environmental changes tonight. Save child-worn materials for a night when the child is fully regulated and familiar with the items.
🔴 3+ Unchecked → POSTPONE
Tonight is not the night. Do the daytime familiarization work this week. Plan for implementation when conditions are right.
"Forcing a new sleep strategy on a bad night creates negative associations. Patience tonight pays dividends for years."

STEP 1 OF 6
The Invitation
Timing: During the daytime, 3–7 days BEFORE first bedtime use
The Principle: Every new sleep material begins with a daytime invitation, not a bedtime demand. A child who is first asked to tolerate something new at their most vulnerable time (bedtime, in the dark, when tired) will almost certainly reject it. Introduce during calm, controlled daytime moments.
Parent Script (say these words): "Look what I found! This is a [sound machine / special pillow headband / new blanket]. It makes a really gentle sound. Want to hear it? We're not using it for sleep yet — I just want you to know what it is."
For white/pink noise machines specifically: Place it in the living room during a calm activity (drawing, building blocks). Turn it on at the lowest possible volume — barely audible. Let the child notice it on their own. No pressure. No "this is for bedtime." Just presence.
✅ What Acceptance Looks Like
- Child ignores the machine (neutral = good)
- Child asks questions about it
- Child wants to touch or control it
- Child continues their activity normally
⚠️ What Resistance Looks Like & What to Do
- "Turn it off" → Immediately comply. "Okay! We'll try another time." No persuasion.
- Child covers ears → Volume is too high. Next time, start even lower.
- Child becomes anxious → Remove completely. Try again in 2–3 days with item visible but off.

STEP 2 OF 6
The Engagement
Timing: Days 3–7 of introduction, still during daytime
The Principle: Gradually increase the child's exposure to each material while the child maintains regulation. This is the habituation phase — the brain needs repeated, low-threat exposure to classify the new sensory input as "safe."
Sound Machine / Fan
Days 3–4: Sound machine on during calm play, volume one small notch up from introduction.
Days 5–6: Sound machine on during meals or family time — multiple contexts.
Day 7: Sound machine on during pre-bedtime routine (reading, calming activities). NOT yet during actual sleep.
Days 5–6: Sound machine on during meals or family time — multiple contexts.
Day 7: Sound machine on during pre-bedtime routine (reading, calming activities). NOT yet during actual sleep.
Ear Protection
Days 3–4: Child wears headband or holds earplugs during play. No requirement to put them in.
Days 5–6: Child tries wearing the headband during a quiet activity for 5–10 minutes.
Day 7: Child wears the headband during the pre-bedtime routine for 15–20 minutes.
Days 5–6: Child tries wearing the headband during a quiet activity for 5–10 minutes.
Day 7: Child wears the headband during the pre-bedtime routine for 15–20 minutes.
Weighted Blanket / Compression
Days 3–4: Weighted blanket draped over legs during screen time or reading.
Days 5–6: Weighted blanket used during family time on the couch.
Day 7: Weighted blanket used during bedtime story in the bedroom.
Days 5–6: Weighted blanket used during family time on the couch.
Day 7: Weighted blanket used during bedtime story in the bedroom.
✅ Engagement
Child seeks out or asks for the material → proceed
🟡 Tolerance
Child allows it without complaint but doesn't seek it → continue at this level 2 more days
🔴 Avoidance
Child actively avoids or asks to remove → step back one level, maintain for 3–4 more days
"I notice you're really comfortable with the [sound machine / headband]. You're getting so good at this."
Reference: PMC11506176 (Sensory integration — structured material introduction meets evidence-based criteria)

STEP 3 OF 6
The Therapeutic Action: First Bedtime Implementation
Timing: Night 1 of active bedtime use (typically Day 8–10 of overall protocol)
Tonight, for the first time, the materials the child has been gradually introduced to will be present during actual sleep. This is the moment the layers begin working together.
60 Minutes Before Bed — Environmental Layers
Room treatment already in place (curtains, rug, acoustic panels — permanent). Bedroom layout already optimized. Household sound management active (family aware of quiet hours, squeaky fixes done).
30 Minutes Before Bed — Sensory Calming Layer
Begin the sensory wind-down: warm bath → dim lights → weighted blanket over legs during story time → gentle massage or compression. Start the consistent sleep sound ritual: same calming audio, same volume, same time.
At Bedtime — Sound Masking Layer
Turn on white/pink noise machine or fan at the habituated level. If using ear protection, offer it: "Want your special headband tonight?" — do NOT insist on first night.
Critical: Only implement layers the child has successfully habituated to. The first night is data collection, not a test. If the child is distressed by a new element, calmly remove it: "That's okay, we'll try again another time."
Ideal
Child falls asleep with new layers in place. Even one layer working = success.
Acceptable
Child takes longer to fall asleep but eventually does. Novelty may extend sleep onset on Night 1.
Concerning (Not Failure)
Child cannot fall asleep with new element and asks for removal. Remove calmly. This is information — the habituation phase needs more time.
STEP 4 OF 6
Repeat & Vary
Timing: Nights 2–14 of active bedtime implementation
The Dosage Principle: Consistency is the active ingredient. The brain needs 7–14 consecutive nights of the same conditions to begin associating these environmental cues with sleep safety. Changing sounds, rotating materials, or skipping nights resets the habituation clock.
Nightly Repetition Protocol
- Same time, same order, same materials, same volumes, same routine — every night for 14 consecutive nights
- If one layer isn't tolerated, continue without it but keep everything else identical
- Add one new layer only after current layers are well-established (usually after Week 2)
Variation Options Within the Same Principles
- Sound variety: Shift from white noise to pink or brown, or try nature sounds (rain, ocean)
- Volume micro-adjustments: Increase sound masking by 5% increments if sounds still cause wakings
- Sensory calming variations: Alternate between compression, deep pressure, and vestibular (slow rocking)
Satiation Indicators: If the sensory calming routine extends bedtime by more than 30 minutes, the child may be using it as a delay tactic. Tighten the routine to 15–20 minutes with clear "last activity" signals.
"3 good nights > 10 forced nights." If the child is clearly distressed by a material, 3 calm nights without it produce better long-term outcomes than 10 resistant nights with it.

STEP 5 OF 6
Reinforce & Celebrate
Timing: Every morning after implementation nights
The ABA Reinforcement Principle: Within the first interaction after waking, acknowledge what went well — even if the night wasn't perfect. Timing matters: immediate, specific, enthusiastic.
If the child slept through (even partially)
"You slept so well last night! Your body did such a good job resting. I'm so proud of you."
If the child woke but settled faster
"I noticed you woke up once last night but you went right back to sleep. That's amazing progress!"
If the night was rough but materials were tolerated
"You kept your headband on all night — that takes real bravery. Your body is learning."
Reinforcement Menu
Sticker Chart
Sticker on a visual sleep chart the child participates in tracking
Special Breakfast
A preferred breakfast item the morning after a good sleep night
Bonus Time
Extra 5 minutes of preferred morning activity
Sleep Hero Badge
"Sleep hero" badge or stamp on their hand — celebrate the attempt, not just the success
Critical: Celebrate the attempt, not just the success. A child who tolerates a new headband for 2 hours before removing it has shown enormous bravery. A child who sleeps to 4am instead of waking at midnight has achieved measurable progress.

STEP 6 OF 6
The Cool-Down: The Morning Transition
Timing: Within 15 minutes of waking
The Principle: Just as the bedtime routine transitions the child INTO sleep, the morning routine should consciously transition them OUT. Children with sensory processing differences benefit from predictable transitions in both directions.
What to Do If the Child Reports Discomfort
"The sound was too loud" → Reduce volume by 10% tonight
"My ears hurt" → Ear protection type needs changing; try a different material
"I couldn't sleep" → Check whether the child is reporting genuine difficulty or morning forgetfulness (ask about specific wakings vs. general feeling)
"I don't want that thing anymore" → Respect the refusal for tonight. Reintroduce during daytime in 2–3 days.

60 Seconds of Data Now Saves Hours of Guessing Later
Every morning, record these 3 essential data points. This discipline transforms guesswork into engineering.
1
Number of Sound-Triggered Wakings
Count only wakings where a sound trigger was identified. Bathroom trips or nightmare wakings don't count. Even an estimate is valuable data.
2
Sleep Onset Time
How many minutes from lights-out to sleep? An estimate is fine. Track whether this improves, worsens, or stays stable over time.
3
Materials in Use Last Night
Check all that applied: White/pink noise machine · Fan/air purifier · Ear protection · Weighted blanket · Sleep sound ritual · Room treatment · Bedroom layout optimization
Optional Bonus Data Points
- Specific sound that caused waking (if known)
- Child's self-reported sleep quality (1–5 scale, for children 5+)
📋 Downloadable Tracking Sheet
Printable PDF grid — dates as rows, the 3 data points as columns
📱 GPT-OS® In-App Tracker
Automatically feeds into your child's Sleep Regulation Index within AbilityScore®
📝 Simple Notebook
Draw a grid with dates as rows and the 3 data points as columns — works perfectly
This data feeds directly into GPT-OS® pattern recognition. After 14 nights, the system identifies which layers are working and recommends specific modifications. Without data, you're guessing. With data, you're engineering.
Most Nights Won't Be Perfect. Here's Your Troubleshooting Guide.
"Session abandonment is not failure — it's data."
Problem 1: "White noise is 'annoying' or 'too loud'"
Reset to barely audible — the child should almost not notice it. Try pink noise (lower frequency, softer) or brown noise (even lower). Try nature sounds: rain, ocean waves, wind. Some children tolerate mechanical fan sound better than electronic noise.
Problem 2: "Earplugs come out during sleep"
Try silicone putty earplugs that mold to ear shape. Try a sleep headband instead — it can't be unconsciously removed as easily. If no ear coverage works, strengthen other layers (sound masking, room treatment) to compensate.
Problem 3: "Good for 3 nights then regresses"
This is normal. The brain cycles through habituation. Continue the protocol unchanged for a full 14 nights before concluding anything. Regression around Night 4–5 is so common it has a name: the "extinction burst." Things get worse before they stabilize.
Problem 4: "Room treatment didn't help"
Audit the specific sounds causing wakings. Room treatment absorbs mid-to-high frequency sounds (voices, TV) but does less for low-frequency sounds (traffic rumble, bass from neighbors). Low-frequency problems need denser materials or sound masking to address.
Problem 5: "Child won't do the sensory calming routine"
The routine may be too long or too structured. Simplify: warm bath + one calming activity + the sleep sound. Let the child choose from 2–3 calming options rather than following a fixed script.
Problem 6: "3 weeks and nothing has improved"
After 3 weeks of consistent implementation with no measurable change, this is a signal to seek professional assessment. Call the Pinnacle National Autism Helpline: 9100 181 181.
Problem 7: "Other family members won't follow quiet hours"
Rather than demanding silence, focus on layers the family CAN control: sound masking, ear protection, room treatment. These reduce the impact of sounds you can't eliminate. A family meeting with a visual "quiet hours" poster helps, but the strategy should not depend on perfect silence.
No Two Children Are Identical — Personalize the Protocol
← Easier
For younger children, higher sensitivity, early stages. Environmental layers only. White noise barely perceptible or absent. Sensory calming shortened to 10 minutes. No data tracking burden.
Standard
Ages 4–8, moderate sensitivity, second week onward. Environmental layers + sound masking + sensory calming. Sleep sound ritual established. 3 daily data points. Layer additions every 7–10 days.
→ Advanced
Older children, milder sensitivity, maintenance phase. All 9 layers active. Child participates in own data tracking. Gradual reduction of sound masking volume over weeks, building adaptive capacity.
For the Sensory Avoider (Most Common)
- Prioritize environmental modification OVER body-worn items
- Introduction pace: slower (10–14 days of daytime familiarization)
- Start with natural sounds (rain, wind) rather than electronic noise
- Headband-style ear protection preferred over in-ear
For the Sensory Seeker Who Is Also Auditory-Sensitive
- May actively want the weighted blanket and seek compression
- Sound masking may need to be richer (layered sounds rather than single tone)
- May respond well to vestibular calming (rocking, hammock swing) before bed
1
Ages 2–3
Environmental layers only. No ear protection (choking risk). Weighted blanket supervised only. Parent co-regulation is the primary sensory calming tool.
2
Ages 4–6
All layers available. Child begins participating in the ritual. Visual sleep chart introduced.
3
Ages 7–12
Child takes ownership. Can learn to adjust their own sound machine. Self-monitoring becomes part of the protocol.

Weeks 1–2: Tolerance, Not Mastery
15%
Progress at This Stage
You are building the foundation. Visible results are still ahead — the neurological work is invisible but essential.
What Progress ACTUALLY Looks Like
- Child tolerates the sound machine being on (even if they don't love it yet)
- Sleep onset may initially INCREASE as the child adjusts — this is normal
- The child stops commenting on or complaining about the new elements (habituation emerging)
- Child mentions the sound machine without negativity ("the rain sound is on")
- Bedtime resistance decreases — the sensory calming routine makes transitions smoother
What Is NOT Progress Yet (Manage Expectations)
- You will probably NOT see dramatic sleep improvement in Week 1
- The child will probably NOT sleep through the night yet
- The child may still request removal of new elements some nights
- Sound-triggered wakings may not yet decrease — you're building the foundation
Parent Emotional Preparation: This is the hardest phase because effort is high and visible results are low. You are doing invisible neurological work. The brain is learning to categorize these new sounds as "safe background" — a process that takes repetition and time, not intensity.
"If your child tolerates the sound machine for one hour longer than last week — that's real progress."

Weeks 3–4: The Neural Pathways Are Forming
40%
Consolidation Phase
Sound-triggered wakings are beginning to decrease. The child is starting to request elements of the routine. Neural habituation is taking hold.
Consolidation Indicators
Sound-triggered wakings begin to decrease (from 4–5/night toward 2–3/night). The child falls asleep faster with the established routine. Morning reports shift from "I heard everything" to "I don't remember waking up."
Behavioral Changes Signaling Neural Pathway Formation
Child's daytime auditory sensitivity may slightly improve. Bedtime anxiety decreases. Child begins associating the routine with safety rather than struggle. Child sleeps through sounds that previously caused full arousal.
When to Increase Intensity
If the child is comfortable with current layers and wakings have decreased by 30%+, consider adding the next layer: environment only → add sound masking → add sensory calming → consider ear protection.
"You may notice you're more confident too. You're no longer dreading bedtime. You have a system. The anxiety of 'will tonight be terrible?' is being replaced by 'we have a protocol.'"

Weeks 5–8: Functional Sleep Is Emerging
75%
Mastery Phase
Sound-triggered wakings reduced to 0–1 per night. Sleep onset under 30 minutes. Child begins self-regulating when they wake. Functional sleep is here.
🏆 Sleep Regulation — Functional Level
Mastery Criteria — Observable & Measurable
Sound-triggered wakings reduced to 0–1 per night (from baseline 4–5). Sleep onset under 30 minutes with established routine. Child self-regulates if they wake — may register sound and return to sleep WITHOUT parent intervention.
Generalization Indicators
Child can nap in moderately noisy environments (car, living room). Sleep quality improves at relatives' homes when portable elements travel with them. Daytime auditory tolerance shows measurable improvement.
Maintenance Check
If you turn off the sound machine for one night, does the child still sleep reasonably? (Some regression is expected; catastrophic regression suggests dependency rather than neural change.) Is the child sleeping through 4–5 nights out of 7?
When to Move to the Next Level
If mastery is achieved with all 9 layers, begin gradually reducing the most intrusive layers (ear protection first, then sound masking volume reduction) while maintaining environmental layers permanently.
"Mastery unlocked: When the child consistently achieves 5+ nights per week of functional sleep (≤1 waking, ≤30 min onset, restorative quality) — this technique has achieved its primary target."

You Did This. Your Family Is Sleeping.
You arrived at this page exhausted. Maybe desperate. Your child was waking 4–5 times every night. Bedtime was a war. Sleep was a fragmented, anxious, painful experience for the entire family.
You learned the neuroscience. You set up the environment. You introduced materials with patience and persistence. You tracked the data. You troubleshot the failures. You adapted the protocol to your specific child.
And now — your child sleeps.
"Your commitment changed your child's neurological reality. The brain learned to filter. The nervous system learned to trust the night. You engineered that."
Family Celebration Suggestion: Mark this milestone. Take a photo of your child sleeping peacefully. Write the date on your tracking sheet. Tell your child: "You are such a brave sleeper now." If comfortable, share your journey with other families on the Pinnacle parent community. Your experience is the evidence that gives another exhausted parent hope.

Clinical Guardrails — Recognize These Signs
Even in the mastery phase, these signs mean pause and consult your clinical team immediately.
🔴 Flag 1: Sleep Disruption Worsens After 3+ Weeks
More wakings, not fewer. Longer sleep onset, not shorter. This is not the typical "extinction burst" — that resolves by Week 2. Do: Stop adding new layers. Maintain only environmental modifications. Contact Pinnacle for professional assessment.
🔴 Flag 2: New Anxiety About Sleep Emerges
Crying at bedtime, fear of the bedroom, refusal to go to bed. Different from initial resistance to materials. Do: Remove all recently added materials. Return to pre-intervention routine. Seek consultation — sound sensitivity may be secondary to an anxiety condition.
🔴 Flag 3: Child Reports Ear Pain or Hearing Change
Pulling at ears, asking "what?" more frequently, complaints of ringing or buzzing. Do: Stop all ear protection immediately. Stop sound masking. Consult pediatrician and request audiology referral.
🔴 Flag 4: Snoring, Gasping, or Unusual Breathing
Audible breathing difficulties, pauses in breathing, mouth breathing with arched neck. This may indicate sleep apnea. Sound management will not address this. Do: Contact pediatrician immediately.
🔴 Flag 5: Daytime Behavior Deteriorates Despite More Sleep
Child sleeps more hours but behavior worsens — increased aggression, emotional dysregulation, cognitive decline. Sleep quality may not be improving even though quantity appears to. Medical sleep study may be indicated.
"Trust your instincts — if something feels wrong, pause and ask."
Your Child's Sleep Journey — Where You Are and Where You're Going
Path A — Deepen Sound Management
A-052-DD-01: Gradual White Noise Introduction — Complete Protocol
A-052-DD-02: Sensory Calming Bedtime Routines for Sound-Sensitive Children
A-052-DD-02: Sensory Calming Bedtime Routines for Sound-Sensitive Children
Path B — Daytime Auditory Sensitivity
A-048: Covers Ears Constantly
A-053: Fear of Loud Sounds
A-044: Sensitivity to Specific Sounds
A-053: Fear of Loud Sounds
A-044: Sensitivity to Specific Sounds
Path C — Broader Sleep Challenges
S-120: General Sleep Difficulties
S-122: Difficulty Falling Asleep
S-122: Difficulty Falling Asleep
Long-term developmental goal: Consolidated, restorative sleep → Improved daytime sensory regulation → Enhanced cognitive function → Better learning outcomes → Higher quality of life for child and family.

More Techniques in Sensory Processing + Sleep
If you've implemented A-052, you already own materials — sound machines, heavy curtains, weighted blankets, and sensory calming tools — that directly apply to these related techniques.
A-048: Covers Ears Constantly
Sensory Regulation | Intro Level
Materials: Noise-Reducing Headphones, Ear Defenders
techniques.pinnacleblooms.org
Materials: Noise-Reducing Headphones, Ear Defenders
techniques.pinnacleblooms.org
A-053: Fear of Loud Sounds
Sensory Regulation | Intro Level
Materials: Sound Exposure Tools, Calming Kits
techniques.pinnacleblooms.org
Materials: Sound Exposure Tools, Calming Kits
techniques.pinnacleblooms.org
A-044: Sensitivity to Specific Sounds
Auditory Processing | Core Level
Materials: Therapeutic Listening, Sound Tools
techniques.pinnacleblooms.org
Materials: Therapeutic Listening, Sound Tools
techniques.pinnacleblooms.org
S-120: General Sleep Difficulties
Sleep Regulation | Intro Level
Materials: Sleep Environment, Routine Supports
techniques.pinnacleblooms.org
Materials: Sleep Environment, Routine Supports
techniques.pinnacleblooms.org
S-122: Difficulty Falling Asleep
Sleep Regulation | Core Level
Materials: Calming Tools, Routine Supports
techniques.pinnacleblooms.org
Materials: Calming Tools, Routine Supports
techniques.pinnacleblooms.org
K-980: Creating a Sensory-Friendly Bedroom
This Technique Is One Piece of a Larger Plan
Cross-Domain Impact of Improved Sleep
When sleep improves, every other domain benefits. Research consistently shows that restorative sleep directly impacts cognitive function (Domain F), emotional regulation (Domain E), behavioral regulation (Domain J), motor coordination (Domains B–C), and language processing (Domain D).
Fixing sleep is not just a sleep intervention — it's a whole-child developmental accelerator.
GPT-OS® Integration
When you track data through the GPT-OS® system, your child's progress feeds into their AbilityScore® — a comprehensive developmental score across all 12 domains. This allows the system to identify which techniques across ALL domains will produce the greatest gains for YOUR specific child.

Real Families. Real Sleep. Real Change.
Parent, Pinnacle Network
"For five years, our son woke 4–5 times every single night at sounds — the fridge, cars outside, doors in the hall. We were all chronically exhausted. Nothing we tried worked. We finally worked with an OT who understood sensory sleep issues. We did a complete bedroom sound audit, introduced pink noise gradually over three weeks, added heavy curtains and a rug, fixed every squeaky hinge, and started a sensory calming routine before bed. He still wakes sometimes, but now it's once or twice a week instead of 4–5 times a night. Everyone is sleeping. Finally."
Illustrative case; outcomes vary by child profile.
Parent, Pinnacle Network
"Our daughter, age 4, had never slept through the night. Her pediatrician said she'd outgrow it. At 4, we were still waiting. The bedroom layout change alone — moving her to the quietest room and positioning her bed against the interior wall — reduced wakings from nightly to 2–3 times a week. Adding the fan as sound masking got us to 1 waking most nights. It wasn't one magic fix. It was layers."
Illustrative case; outcomes vary by child profile.
Senior Occupational Therapist, Pinnacle Blooms Network
"What parents often don't realize is that the child who 'hates white noise' may have been introduced to it incorrectly — too loud, too sudden, at bedtime when anxiety is highest. When we restructure the introduction to be gradual, low-volume, and during calm daytime periods, the majority of previously-resistant children can habituate within 2–3 weeks."

You're Not Alone in This — Join Families on the Same Journey
Isolation is the enemy of adherence. Families implementing sleep interventions report higher consistency and better outcomes when they're part of a supportive community. You deserve both a system and a community.
Sleep Solutions Parent Community
WhatsApp group for parents implementing sound-management sleep strategies. Share tips, troubleshoot, celebrate milestones. Request to join at pinnacleblooms.org/community
Pinnacle Parent Forum
Online discussion board organized by challenge type. Find threads on auditory sensitivity, sleep disruption, and sensory processing. pinnacleblooms.org/forum
Local Parent Meetups
Pinnacle centers across 70+ locations host monthly parent support meetings. Find your nearest center at pinnacleblooms.org/centers
Peer Mentoring
Connect with a parent who has successfully implemented this protocol and can guide you through the early weeks. Request a peer mentor by calling 9100 181 181.
"Your experience helps others — consider sharing your journey."
Home + Clinic = Maximum Impact
Find Your Nearest Pinnacle Center
Pinnacle Blooms Network operates 70+ centers across India. For A-052 (Sound-Triggered Sleep Disruption), the primary discipline lead is Occupational Therapy — Sensory Integration Specialty.
Request a therapist with specific expertise in: Sensory processing evaluation (SPM-2, Sensory Profile) · Sleep-specific sensory intervention · Auditory modulation and desensitization · Parent training for home-based sensory strategies
Teleconsultation for Remote Families
Not near a center? Pinnacle offers teleconsultation in 16+ languages. A qualified OT can review your child's profile, assess the sleep challenge, and design a personalized implementation plan — all via video.
📞Book a teleconsultation: 9100 181 181 (FREE National Autism Helpline)
Assessment Pathway
AbilityScore® Assessment
Comprehensive baseline across all developmental domains
Sensory Processing Evaluation
Detailed auditory, tactile, vestibular, proprioceptive profiling
Sleep Regulation Assessment
Specific sleep pattern analysis within GPT-OS® framework
Personalized Intervention Plan
Technique selection, material recommendations, and home program design
Ongoing Tracking
Sleep Regulation Index + Sensory Modulation Index progression monitoring
Deeper Reading for the Curious Parent
PRISMA Systematic Review (2024) — PMC11506176
"Sensory Integration Intervention for Children with Autism Spectrum Disorder." 16 articles from 2013–2023 confirm SI intervention meets evidence-based practice criteria.
Meta-Analysis — World J Clin Cases (2024) — PMC10955541
"Effects of Sensory Integration Therapy on Children with ASD." 24 studies. Effective promotion of social skills, adaptive behavior, sensory processing, and motor skills. DOI: 10.12998/wjcc.v12.i7.1260
Indian RCT — Padmanabha et al. (2019)
Home-Based Sensory Interventions. Demonstrated significant outcomes for parent-administered sessions with established safety protocols. DOI: 10.1007/s12098-018-2747-4
WHO CCD Package (2023) — PMC9978394
Care for Child Development. Age-specific evidence-based recommendations for caregivers. Implemented across 54 LMICs.
Frontiers in Integrative Neuroscience (2020)
Framework for Evaluating SI/SP Treatment in ASD. Comprehensive neurological basis for sensory-based interventions. DOI: 10.3389/fnint.2020.556660
WHO Nurturing Care Framework (2018) + NCAEP (2020)
Five components of nurturing care. 111 country contributors. Foundation for global ECD policy. NCAEP classifies visual supports and sensory strategies as evidence-based practice for autism.
Pinnacle Network Real-World Evidence: 20M+ exclusive 1:1 sessions • 97%+ measured improvement across readiness indexes • Ongoing outcomes data contributing to the largest integrated pediatric therapy evidence base globally.

Your Data Powers Better Outcomes — For Your Child and Every Child Like Yours
What GPT-OS® Learns From A-052 Data
- Which sound masking frequencies are most effective for specific auditory sensitivity profiles
- Optimal introduction pace by age band
- Which layer combinations produce the fastest results
- Regional environmental factors (urban vs. rural noise profiles) and their impact on strategy selection
Privacy and Data Protection
- All session data encrypted in transit and at rest
- Personal identifiers separated from clinical data in the analytics layer
- Your data contributes to population-level insights only when anonymized
- You maintain full ownership and can request deletion at any time
- Compliant with Indian DPDP Act (2023) and global data protection standards
"Your data helps every child like yours. The more families contribute, the smarter the recommendations become for everyone."
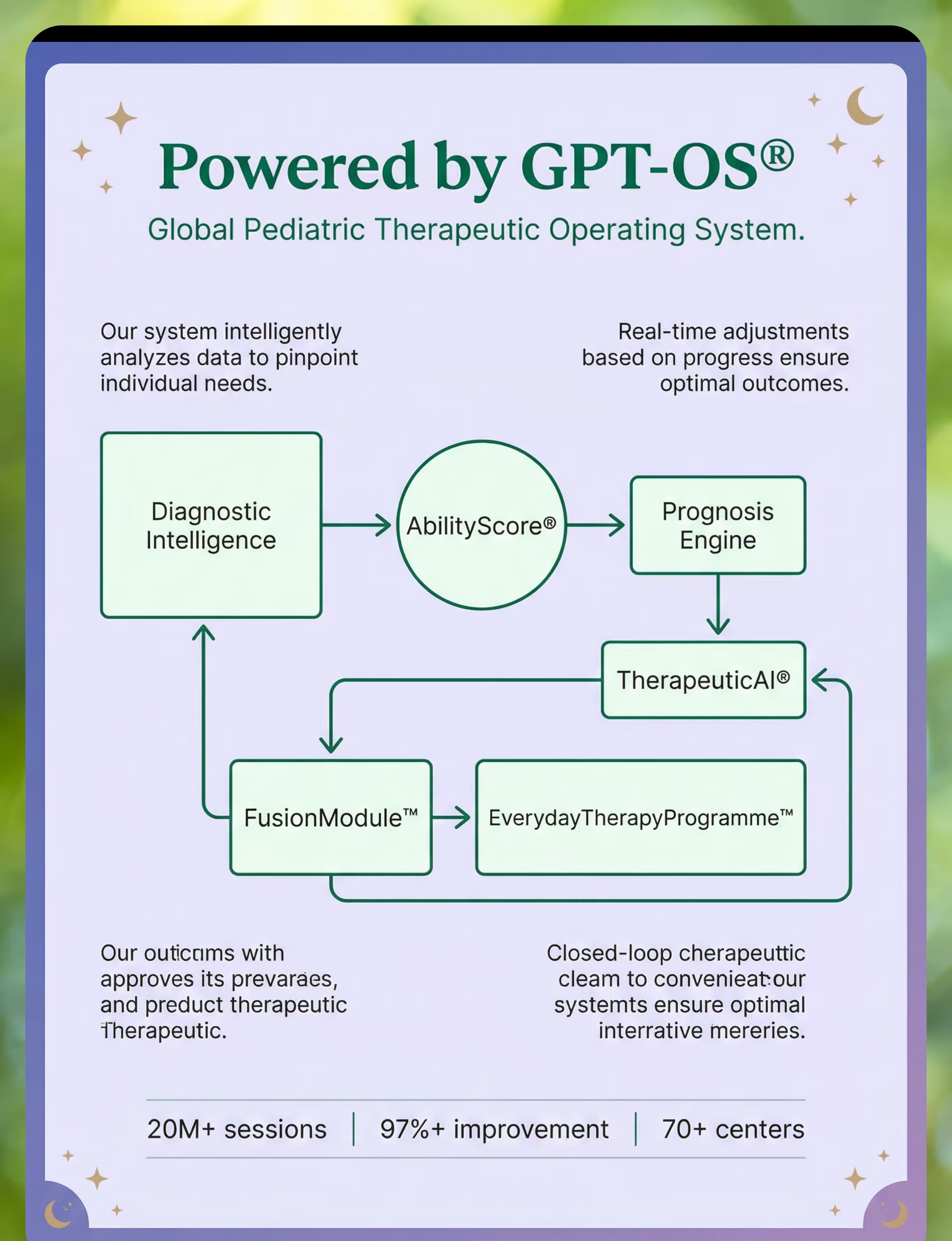
GPT-OS® Stack: Diagnostic Intelligence → AbilityScore® → Prognosis Engine → TherapeuticAI® → FusionModule™ → EverydayTherapyProgramme™ → Closed-Loop Control

Watch: 9 Materials That Help When Sounds Disrupt Sleep
Reel ID: A-052
~75 seconds
Sensory Solutions Series — Episode 52
This Reel summarizes the 9 materials in a 75-second visual format. Watch a Pinnacle consortium therapist introduce each material, demonstrate the key concepts, and show real-world implementation.
Multi-modal learning matters: You've read the detailed protocol across these cards. Now watch it demonstrated. Research shows that combining text instruction with video demonstration significantly improves parent skill acquisition and implementation fidelity. (NCAEP Evidence-Based Practices Report, 2020)
Share This Reel
📱 Instagram
📱 Facebook
💬 WhatsApp
🔗 Copy Link

If only one parent executes this protocol, it's limited. When spouses, grandparents, school staff, and nannies all understand and support the approach, the child experiences consistency — and consistency is the active ingredient.
WhatsApp
Send this page to your spouse, parent group, or caregiver. Link: techniques.pinnacleblooms.org/sensory-processing/sounds-disrupt-sleep
Family Guide (1-Page PDF)
Simplified summary of the 9 materials, the bedtime protocol, and the morning tracking checklist. Print and tape to the refrigerator.
"Explain to Grandparents" Version
Plain-language summary without clinical terminology. Focuses on: what to do, what not to do, and why this matters. Designed for extended family who want to support without clinical jargon.
Teacher/School Communication Template
Letter explaining the child's sleep challenges and home intervention, with requests for school-based support — quiet rest area, understanding about fatigue, auditory accommodations in classroom.
Reference: PMC9978394 (WHO CCD Package — multi-caregiver training as critical for intervention generalization)

Your Questions, Answered
Q: Will my child become dependent on white noise and never sleep without it?
Many adults use fans or sound machines their entire lives — this is not pathological dependency. Over time, as auditory gating matures (especially with OT support), many children naturally reduce their need for sound masking. The goal is functional sleep NOW while building underlying capacity over months and years.
Q: Is it safe to have a sound machine running all night?
Yes, when volume is kept under 65 dB at pillow position (about conversation level). The AAP recommends placing sound machines as far from the sleeping area as possible and using the lowest effective volume. All-night use at safe volumes is well-established practice.
Q: My child hates anything touching their ears. Is there any hope for ear protection?
Absolutely. In-ear options are just one category. Sleep headbands provide sound reduction without ear insertion. Some children tolerate a soft hood or beanie. And if no ear coverage works, strengthening other layers (sound masking, room treatment) can compensate.
Q: We rent our apartment. Can we do room treatment without permanent changes?
Yes. Removable adhesive hooks hold heavy curtains and tapestries. Thick rugs sit on floors without installation. Freestanding bookshelves serve as sound barriers. Draft stoppers are fully removable. No holes or permanent modifications required.
Q: How do I know if this is sensory processing or an anxiety disorder?
Key differentiator: sensory-based sleep disruption is triggered by SPECIFIC SOUNDS the child can identify. Anxiety-based disruption involves WORRY about sleep or generalized fear unrelated to specific sensory triggers. Many children have both — professional assessment clarifies, and both components can be addressed simultaneously.
Q: My pediatrician says my child will "grow out of it." Should I wait?
Some children do develop better auditory gating over time. However, chronic sleep deprivation during developmental years causes cumulative harm to cognition, emotional regulation, and learning. Intervening now — even with simple environmental modifications — reduces harm while waiting for maturation.
Q: Can these strategies help adults with sound-sensitive sleep too?
Yes. The same principles apply to adolescents and adults with auditory processing differences. This page focuses on pediatric implementation, but the science is universal.
Q: How long before I should contact a professional if I don't see improvement?
After 3 weeks of consistent implementation with no measurable change in any metric, seek professional assessment. Call the FREE Pinnacle National Autism Helpline: 9100 181 181.
Didn't find your answer? → Ask GPT-OS® at pinnacleblooms.org → Book a teleconsultation: 9100 181 181

From Reading to Action — Your Child's Better Sleep Starts Tonight
🟢 START THIS TECHNIQUE TODAY
Launch the GPT-OS® guided session for A-052. Receive personalized material recommendations, step-by-step prompts, and daily tracking integrated into your child's AbilityScore® profile.
📞 BOOK A FREE CONSULTATION
Speak with a Pinnacle specialist who can assess your child's specific sleep profile and design a personalized implementation plan.
Call 9100 181 181 (FREE National Autism Helpline — 16+ languages, available nationwide)
🔄 EXPLORE THE NEXT TECHNIQUE
Ready for more? Continue your journey through the sensory processing domain or explore the progression pathway.
✅Validated by the Pinnacle Blooms Consortium — OT • SLP • ABA • SpEd • NeuroDev • CRO
Preview of 9 materials that help when sounds disrupt sleep Therapy Material
Below is a visual preview of 9 materials that help when sounds disrupt sleep therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.





Link copied!

The Pinnacle Promise
"From fear to mastery. One technique at a time." — The Pinnacle Blooms Consortium
About Pinnacle Blooms Network®
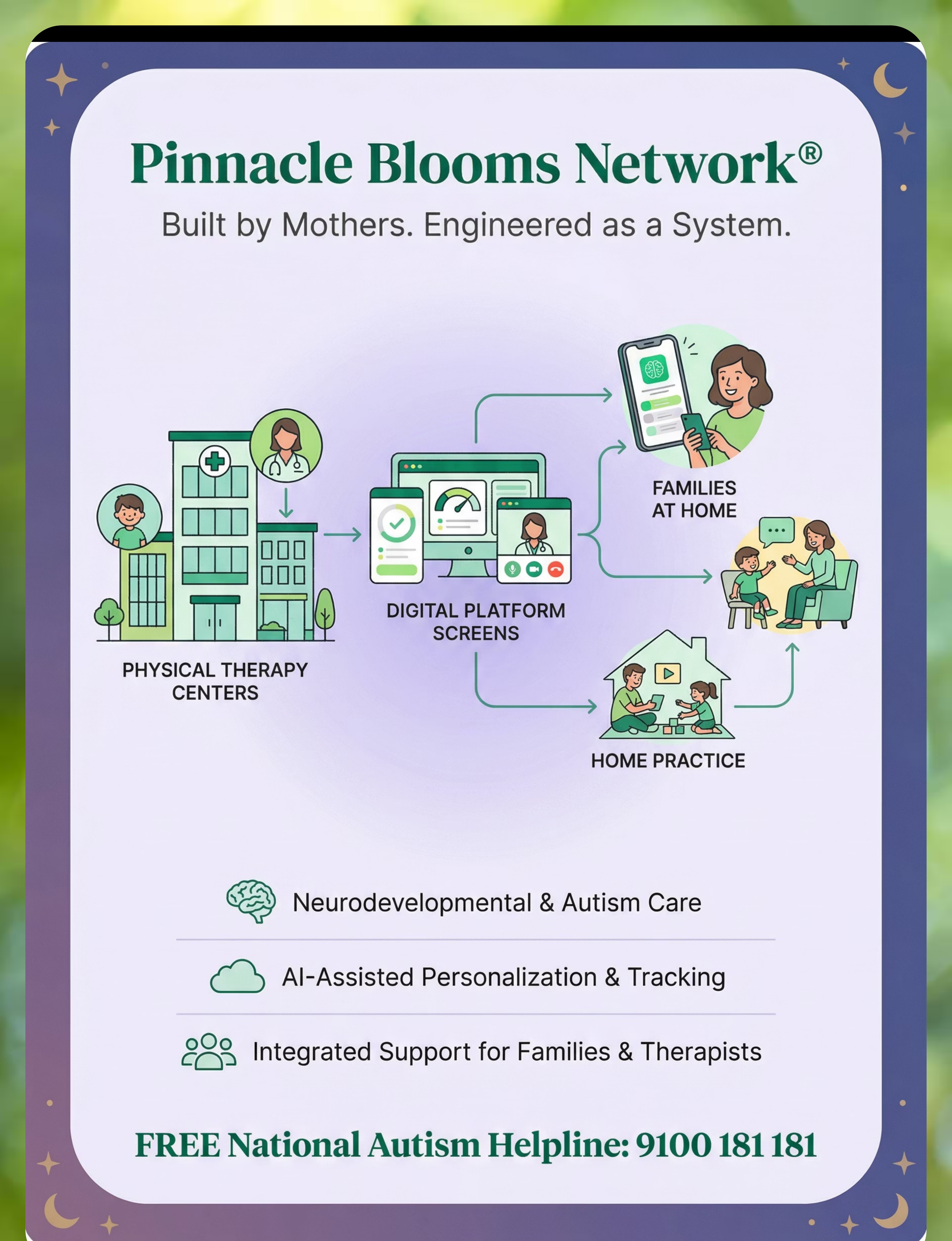
Built by Mothers. Engineered as a System. Pinnacle is the execution layer of GPT-OS® — delivering therapy, daily programs, digital continuity, and marketplace access at population scale.
70+
Centers
Across India
500+
Therapists
On the network
20M+
Sessions
Exclusive 1:1 therapy sessions delivered
97%+
Improvement
Measured improvement across readiness indexes
Serving families from 70+ countries
Patents filed across 160+ countries
📞 FREE National Autism Helpline
9100 181 181
Available 24/7 | 16+ languages | Nationwide
Available 24/7 | 16+ languages | Nationwide
Medical Disclaimer
This content is educational. It does not replace assessment by a licensed occupational therapist, sleep specialist, or healthcare provider. Persistent sleep disruption may indicate underlying medical conditions requiring evaluation. Individual results may vary. Statistics represent aggregate outcomes across the Pinnacle Blooms Network.
Copyright & Attribution
© 2025 Pinnacle Blooms Network®, unit of Bharath Healthcare Laboratories Pvt. Ltd. All rights reserved.
CIN: U74999TG2016PTC113063 | DPIIT: DIPP8651 | MSME: TS20F0009606 | GSTIN: 36AAGCB9722P1Z2
CIN: U74999TG2016PTC113063 | DPIIT: DIPP8651 | MSME: TS20F0009606 | GSTIN: 36AAGCB9722P1Z2
Explore More Techniques
Return to Top
↑ Card 01 — Their Brain Won't Stop Listening
Next Recommended Technique
Pinnacle Home