Rewind. Replay. Rewind. Replay. Forever.
When your child watches the same 30-second clip on endless repeat — hitting rewind the instant it ends, melting down if anything changes — the loop has become a lock. There are 9 clinically-validated materials that help expand beyond the replay button.

Technique A-075 | Domain A — Visual Processing
You Are Among Millions of Families Navigating This Exact Challenge
Restrictive media viewing — where a child watches the same clip, scene, or video on endless repeat and experiences distress when interrupted — sits at the intersection of sensory regulation, predictability-seeking, and restricted interest patterns. It is one of the most frequently reported challenges across Pinnacle's 70+ centers in India and among families in 70+ countries worldwide.
80%
Show Repetitive Behaviours
of children with autism display restricted/repetitive behaviours involving preferred stimuli
1 in 36
Children Diagnosed
children in the US are diagnosed with ASD (CDC 2023); India estimates 1–1.5 crore children
70%
Anchor to Media
of autistic children show intense, narrow interest patterns anchoring to specific media content
PRISMA Systematic Review (2024): 80% of children diagnosed with autism display sensory/perceptual processing difficulties. Restricted and repetitive behaviours, including media fixation, represent a core diagnostic domain of ASD. References: PMC11506176 | PMC10955541 | WHO NCF 2018

This Is a Regulation Strategy, Not a Behaviour Problem
The Neuroscience in Plain English
When your child watches the same clip repeatedly, the visual cortex, limbic system, and basal ganglia are engaged in a predictable, safe sensory loop. The brain has learned: "this sequence always ends the same way." In a nervous system that over-processes novelty and uncertainty, this predictability delivers genuine regulation.
The basal ganglia — which governs habit formation and pattern completion — drives the compulsion to rewind. This is not a moral failure. It is a compensatory mechanism.
Key Neuroscience Concepts
Predictive Processing Deficit
Autistic brains show altered prediction error signaling — familiar content reduces that error.
Interoceptive Dysregulation
The clip may provide proprioceptive calm through auditory pattern repetition.
Dopaminergic Reward Circuit
Familiar sensory input triggers dopamine release — making the loop genuinely rewarding.
"This is a wiring difference, not a behaviour choice. The intervention is not discipline — it is neurological scaffolding." — Pinnacle NeuroDev Pediatrics Division
Developmental Context
Understanding the Developmental Window You're In
The 2–5 year window is the optimal intervention period. Neuroplasticity is at its peak, new media interaction patterns can be wired most efficiently, and language and social communication are developing simultaneously — making media-based intervention a powerful multi-goal tool.
Why This Window Matters
- Neuroplasticity is at its peak — new patterns wire most efficiently
- Predictability-seeking is developmentally normal — it is the rigidity that distinguishes therapeutic from typical
- Language and social communication developing simultaneously
Co-Occurring Considerations
- Sensory Processing Disorder (SPD) — seen in 80%+ of children on the spectrum
- Auditory Processing preferences — many children loop clips for specific audio patterns
- Anxiety — predictability-seeking often correlates with generalised anxiety profiles
WHO Care for Child Development Package: Age-specific caregiver-delivered structured play interventions beginning at 18 months yield the highest developmental returns. Reference: PMC9978394
Evidence Base
Clinically Validated. Home-Applicable. Parent-Proven.
PRISMA Systematic Review 2024
16 studies (2013–2023) confirm sensory integration + behavioural flexibility interventions are evidence-based for ASD. (PMC11506176)
Meta-Analysis 2024
Sensory-based interventions improve adaptive behaviour, social skills, and flexibility across 12+ RCTs. (PMC10955541)
Padmanabha et al., 2019
Indian RCT: home-based structured interventions in children with ASD showed significant measured improvement. (DOI:10.1007/s12098-018-2747-4)
NCAEP EBP Report 2020
Video modelling, extinction with reinforcement, and structured play are classified evidence-based practices for autism.
Clinically validated across populations. Home-applicable with appropriate caregiver training. Parent-proven across Pinnacle's 20M+ exclusive 1:1 sessions. Evidence Confidence: 85%
Technique A-075
Restricted Media Loop Intervention: "Expanding the Playlist"
Restricted Media Loop Intervention is a multi-material, home-deployable therapeutic approach that systematically expands a child's tolerance for variation within preferred media content — while using that same preferred content as the therapeutic entry point. Rather than removing the child's preferred video (which escalates distress), the technique introduces 9 categories of material across four strategic pathways.
Extend Engagement
Tangible extensions, parallel activities, and content creation that expand beyond passive viewing.
Introduce Variation
Same-content variations and scheduling that build tolerance for change within familiar territory.
Alternative Regulation
Sensory alternatives and social viewing that build regulation pathways beyond the loop.
Scaffold Transitions
Visual timers and first-then boards that make endings predictable and manageable.
Ages 2–10
10–20 min/session
Daily (2x/day ideal)
Beginner–Intermediate

Every Member of the Pinnacle Consortium Contributes to This Technique
This technique crosses therapy boundaries because the brain doesn't organise by therapy type. The Pinnacle Consortium delivers it as one integrated protocol — not five separate appointments.
Occupational Therapy (OT)
Lead discipline. Addresses the sensory regulation function of the media loop. Introduces sensory alternatives and graded flexibility through material scaffolding.
Speech-Language Pathology (SLP)
Leverages the child's deep knowledge of clip content for language expansion, narrative building, and requesting practice. The clip becomes a communication curriculum.
ABA / BCBA
Designs the reinforcement schedule, extinction protocol, and differential reinforcement of alternative behaviours (DRA) that shape media flexibility without punishing the behaviour.
Special Education (SpEd)
Translates flexibility gains into classroom and structured learning contexts. Develops media transition IEP goals for school environments.
NeuroDev Pediatrics
Understands the neurological driver. Monitors for anxiety, OCD-spectrum overlap, and medication considerations that may affect intervention response.
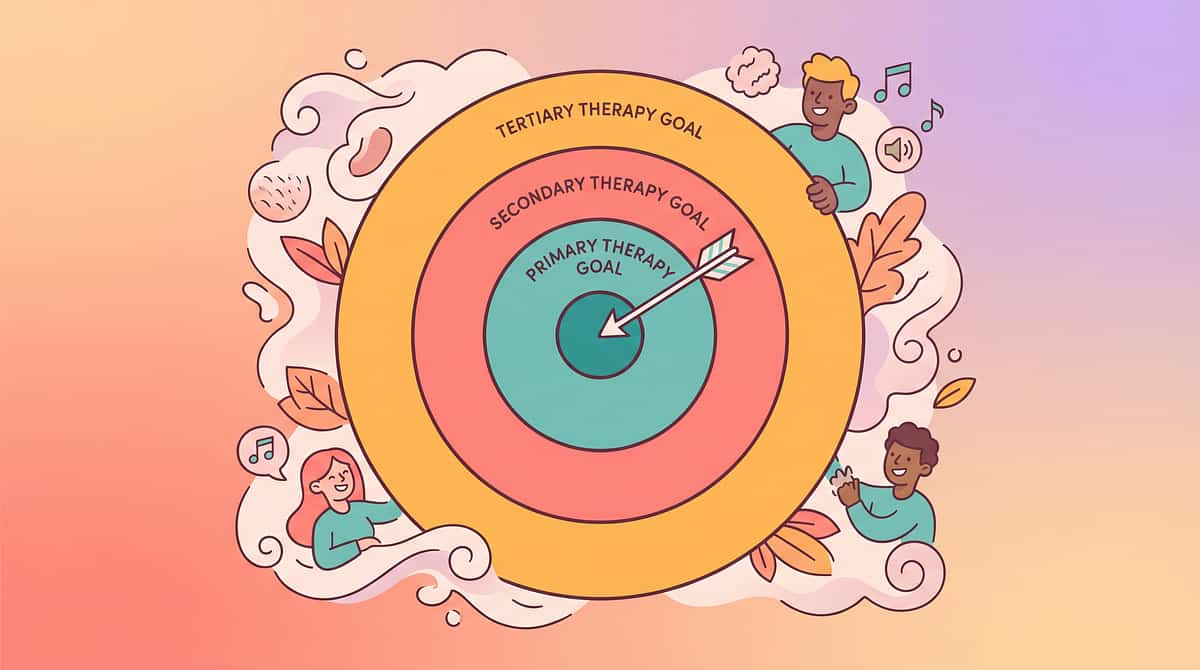
What This Technique Is Actually Building
Primary Target
🎯Media Flexibility — tolerance for variation within and beyond preferred content
Secondary Targets
- Transition tolerance — accepting that content ends without crisis
- Cognitive flexibility — beginning to transfer interest to adjacent content
- Joint attention — sharing the viewing experience with a caregiver
- Language expansion — using the content as a communication scaffold
- Sensory regulation — building regulation pathways independent of the loop
- Demand tolerance — accepting minimal variations (same show, different episode)
Measurable Outcomes (3–8 Weeks)
Child tolerates the video ending without crisis (basic goal)
Child accepts 1 variation within content (different episode/scene from same show)
Child engages with tangible extension material alongside viewing
Child initiates communication related to content
Child accepts visual timer indicating end of video time
The 9 Canon Materials
The 9 Materials That Help When a Child Watches the Same Clip
Each material targets a distinct therapeutic pathway. Begin with one — ideally the one closest to your child's existing comfort zone — and expand from there.

1 · Tangible Extensions
Toys, figures, and books matching the preferred content. Brings the screen into the room — active engagement with beloved characters. ₹200–₹800
2 · Same-Content Variations
Different episodes, songs, or scenes from the same source. Small steps within familiar territory — builds tolerance for change. ₹0 (OTT/YouTube)

3 · Parallel Activity Materials
Colouring, building, and creating alongside the screen. Hands busy while eyes watch — expands beyond passive viewing. ₹50–₹300
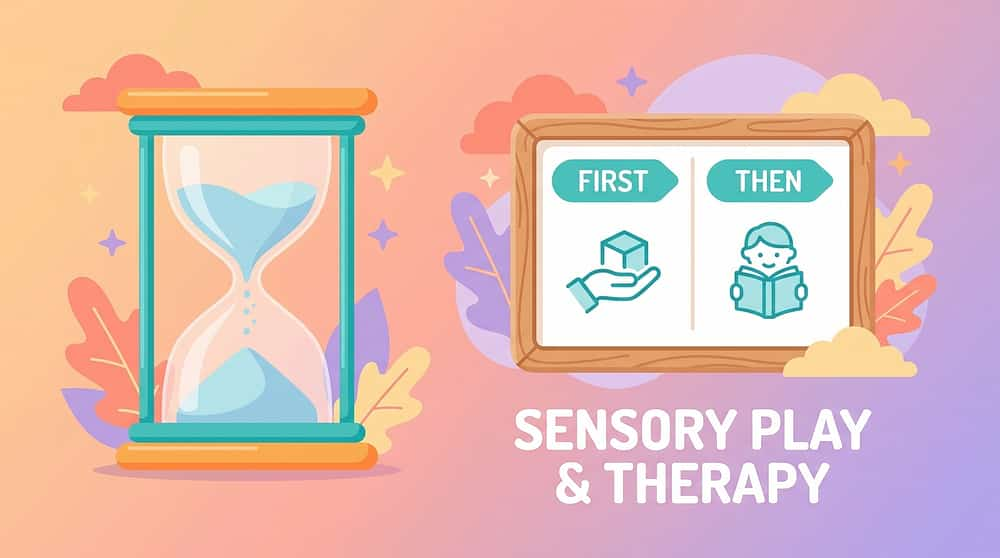
4 · Visual Transitions
Timers, schedules, and First-Then boards. Making endings predictable — prepares the child for what comes next. ₹0–₹500

5 · Interactive Alternatives
Apps and games that require participation, not just watching. From watching to participating — builds active rather than passive screen use. ₹0–₹200

6 · Sensory Alternatives
Visual tools, calming sounds, and tactile materials. Other ways to find calm — expands the regulation toolkit beyond screen dependence. ₹100–₹600

7 · Social Viewing
Structured joint attention around the screen. Shared experience — transforms solitary watching into meaningful connection. ₹0 (caregiver presence)

8 · Content-Inspired Creation
Art, stories, and play inspired by the content. From watching to making — channels deep content knowledge into creative expression. ₹50–₹200

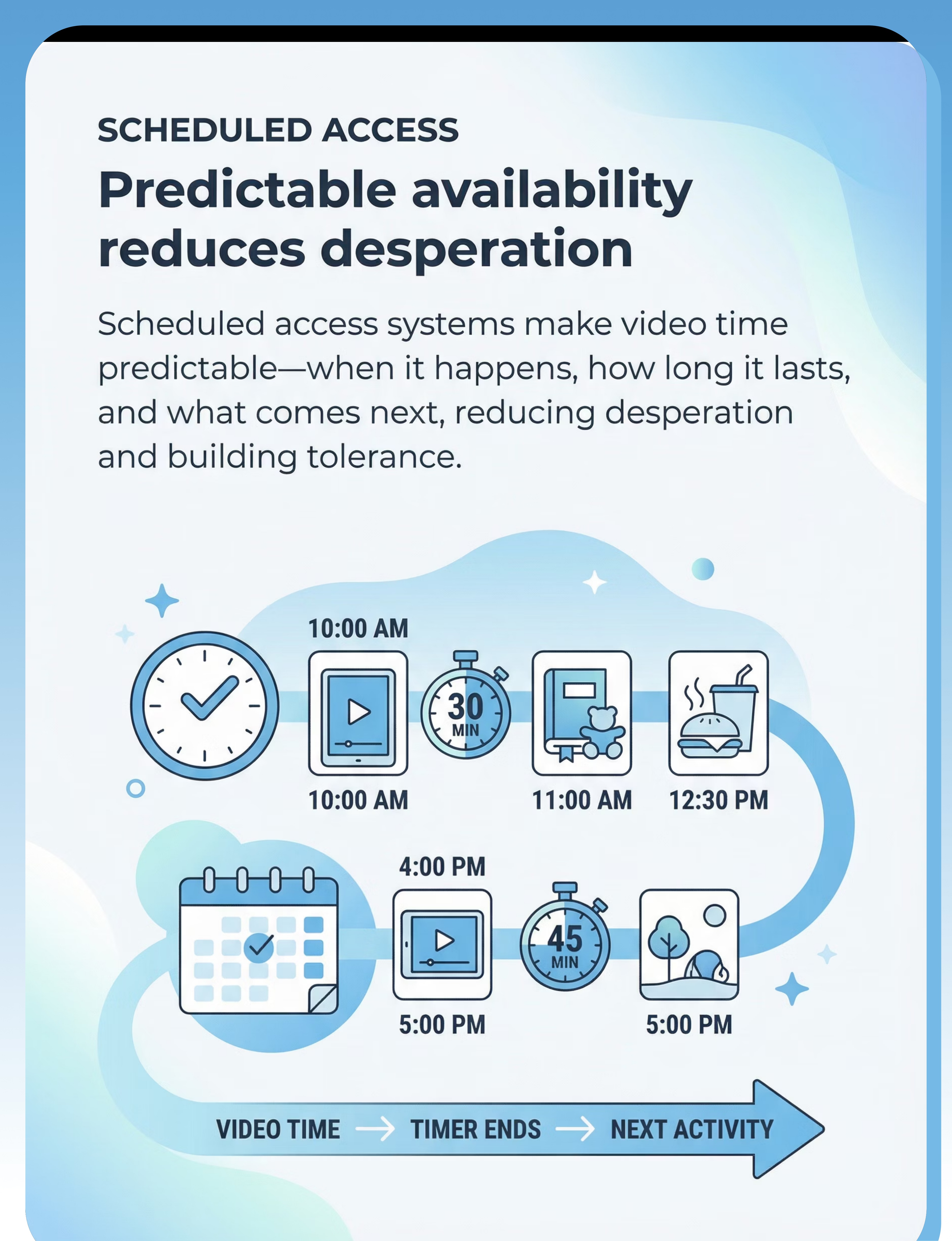
9 · Scheduled Access System
Structured video time with clear start/end and what-comes-next. Predictable availability reduces desperation and builds genuine tolerance. ₹0

Equity Principle
Every Family Can Do This — Right Now, With What You Have
This card exists because not every family has same-day delivery. Every material on this list has a ₹0 household alternative. This is the WHO Nurturing Care Framework equity principle in action: the therapeutic mechanism is the interaction pattern, not the material's price tag.
Material | 💳 Buy This | 🏠 Make This (₹0) | |
Tangible Extension | Character figures ₹200–800 | Print and cut character images; laminate with tape; attach to sticks for puppets | |
Visual Timer | Sand/digital timer ₹200–400 | Mark a paper "video time" bar; cross out sections as time passes | |
First-Then Board | Printed board ₹100–200 | Two sticky notes: one says "VIDEO" (draw tablet), one says "SNACK" (draw food) | |
Parallel Activity | Colouring pages ₹50–100 | Draw the character yourself (any approximation works); child colours | |
Schedule System | Visual chart ₹300–600 | Folded paper with three boxes: Video → Snack → Play. Tick each as done. | |
Reinforcement | Reward jar ₹400–600 | Any clean jar + 10 small stones/buttons = token economy | |
Sensory Alternative | Fidget tool ₹150–400 | Roll newspaper into tube; fill with rice for a DIY shaker; knead homemade dough | |
Content Creation | Art supplies ₹100–300 | Old newspaper + pencil + imagination = content-inspired creation | |
Social Viewing | — | You, sitting beside your child, commenting softly on the video. Free. Priceless. |
A ₹0 substitute used consistently outperforms a ₹2000 tool that sits on a shelf. Reference: WHO NCF (2018) | PMC9978394
Safety First
Read This Before Your First Session
🔴 DO NOT PROCEED IF:
• Child is in the middle of a meltdown or is dysregulated
• Child is unwell, feverish, or has had disrupted sleep
• Child has shown aggression in the last 30 minutes
• You are emotionally depleted and cannot hold calm presence
• There has been a recent major transition (new school, new home, new sibling)
• Child is in the middle of a meltdown or is dysregulated
• Child is unwell, feverish, or has had disrupted sleep
• Child has shown aggression in the last 30 minutes
• You are emotionally depleted and cannot hold calm presence
• There has been a recent major transition (new school, new home, new sibling)
🟡 MODIFY IF:
• Child is tired but not dysregulated → shorten session to 5 minutes max
• Child is slightly resistant → use preferred character toy as entry point first
• Introducing a NEW material → do it during viewing, not instead of it
• Child has been sick recently → return to baseline routine before pushing flexibility
• Child is tired but not dysregulated → shorten session to 5 minutes max
• Child is slightly resistant → use preferred character toy as entry point first
• Introducing a NEW material → do it during viewing, not instead of it
• Child has been sick recently → return to baseline routine before pushing flexibility
🟢 PROCEED WHEN:
• Child is fed, rested, regulated
• At least 30 minutes since last screen time
• You have 20 uninterrupted minutes
• Materials are prepared BEFORE you call the child
• Child is fed, rested, regulated
• At least 30 minutes since last screen time
• You have 20 uninterrupted minutes
• Materials are prepared BEFORE you call the child
🔴 STOP IMMEDIATELY IF:
• Child becomes physically aggressive toward themselves or others
• Child shows signs of respiratory distress (breath-holding, hyperventilation)
• Child completely shuts down (goes non-responsive)
• The intervention is consistently triggering meltdowns after 3+ days
• Child becomes physically aggressive toward themselves or others
• Child shows signs of respiratory distress (breath-holding, hyperventilation)
• Child completely shuts down (goes non-responsive)
• The intervention is consistently triggering meltdowns after 3+ days
STOP = Seek professional support immediately.
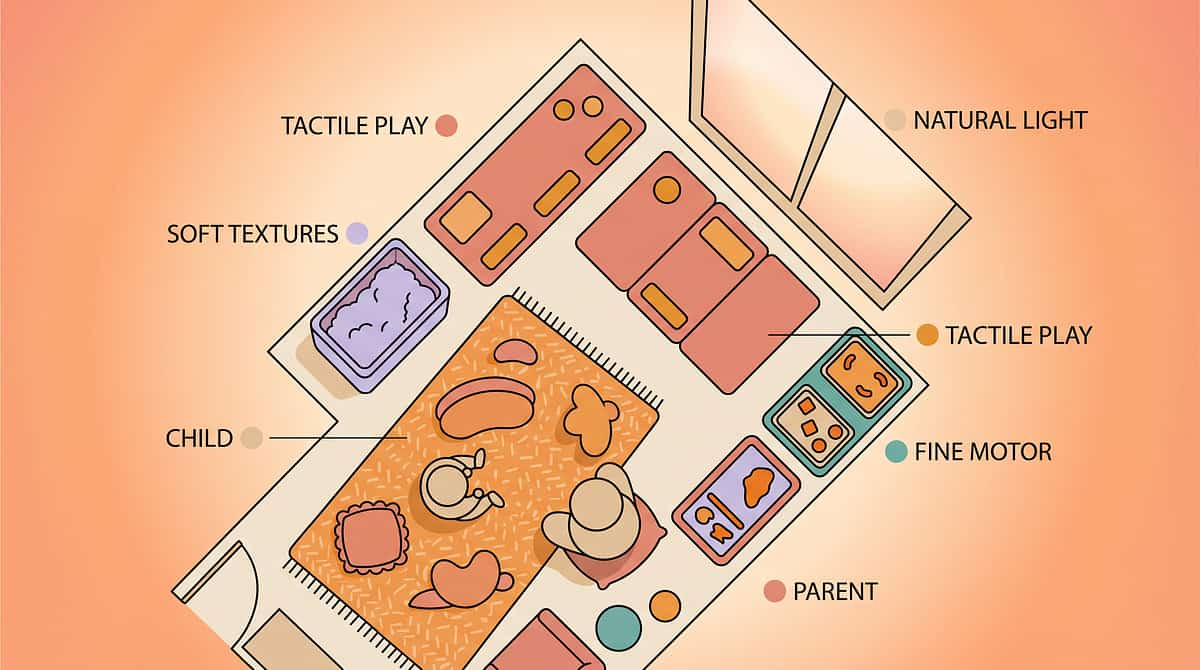
Spatial Precision Prevents 80% of Session Failures
The environment you create before your child enters the room is as therapeutic as anything you do during the session. Prepare every position in advance — no fetching, no rearranging mid-session.
Child Position
Floor mat or low chair — stable, grounded, comfortable. A settled body supports a regulated nervous system.
Parent Position
Sitting at 90° angle (not hovering behind) — this signals collaboration, not control.
Screen Placement
On a flat surface at natural viewing height — NOT held by parent (creates control conflict).
Materials Tray
Prepared and within child's reach BEFORE session starts — absolutely no fetching mid-session.
Visual Timer
Placed in child's line of sight — visible throughout the entire session.
Distractions Removed
Other toys, snacks, and competing stimuli out of visual field. TV in background = NO.
Sound Environment
Low ambient noise — fans/ACs are okay. Natural light preferred; avoid fluorescent overhead.
PMC10955541 — Meta-analysis confirms structured 1:1 environment is the highest-efficacy session format. Duration: 10–20 minutes maximum for initial weeks.
Pre-Session Protocol
The 60-Second Pre-Flight Check
Before every session, run this quick readiness check. It takes 60 seconds and directly predicts whether today's session will be productive or counterproductive. Antecedent management is one of the most powerful tools in your therapeutic toolkit.
Physiological Readiness
- Child has eaten in the last 2 hours
- Child has not had screen time in the last 30 minutes
- Child shows no signs of illness (fever, runny nose, glazed eyes)
- Sleep was adequate last night
State Readiness
- Child is in a regulated state (not mid-meltdown, not hyperaroused)
- No major disruption in the last 60 minutes
- Child's preferred person is present (if relevant)
Environment Readiness
- Space is set up per the spatial checklist
- Materials are ready and within reach
- Visual timer is visible and set
Decision Gate
9–10 ✅ GO — Proceed to Step 1: The Invitation
6–8 ✅ MODIFY — Shorter session, preferred entry material only
Below 6 — POSTPONE — 20-minute calming activity first; reassess
Postpone activity: sensory play (playdough, water play) OR proprioceptive input (gentle joint compression, heavy work) → reassess in 20 minutes.

Step 1 of 6
① The Invitation (30–60 Seconds)
What you're doing: Bringing your child into the activity through their preferred content — not by telling them what to do, but by joining what they're already loving. You are entering their world, not redirecting them out of it.
"Oh, is that [character name]? I love that part too! Can I sit with you for a little bit?"
Do NOT ask "Can we do an activity?" — that signals demand and triggers avoidance.
Body Language Matters
- Sit at their level — floor if they're on the floor
- Relaxed posture — no tension in your face or hands
- Eyes on the screen with them, not watching them watching
✅ Acceptance Cues
- Continues watching without tensing
- Glances at you once and returns to screen
- Shifts slightly to make "space" for you (neural permission granted)
⚠️ Resistance Cues
- Body stiffens when you sit down
- Pulls tablet away from you
- Increases volume / presses rewind more urgently
If resistance: Move 18 inches further away. Comment on the screen from a distance. Build proximity over 3–5 days before attempting material introduction.
ABA Principle: Pairing — establish yourself as a positive/neutral stimulus BEFORE introducing any demand.

Step 2 of 6
② The Engagement (1–3 Minutes)
What you're doing: Introducing the material INTO the viewing context — not instead of it. The clip continues playing. You are adding to the experience, not replacing it. Choose ONE material from the 9 for this session.
Example: Tangible Extension (Material 1)
Place a character figure on the surface between you and the child. Do NOT hand it to them. Do NOT say "look at this." Simply place it in their peripheral vision.
"Look — [character name] is here too! They're watching with us."
Then go silent. Let the child notice. Let them choose to reach.
Example: Visual Timer (Material 4)
Set a 3-minute visual timer NEXT to the screen (not obscuring it).
"This is our watching timer. When it's done, we'll [snack/play/bath]."
Do NOT attach consequences yet. Week 1 is purely about the child seeing the timer without anxiety.
Child Response Indicators
✅ Glances at the material — neural acknowledgement (success)
✅ Reaches toward or touches the material — active engagement (excellent)
✅ Ignores the material but doesn't reject it — tolerance (acceptable in week 1)
⚠️ Pushes the material away — too soon; wait 2 more days
Reinforcement Cue
When child looks at or touches the material, say warmly:
"Yes! That's [character]!"
Brief, warm, then return attention to the screen. Never overdo the praise in this moment.

Step 3 of 6 — Core Intervention
③ The Therapeutic Action (3–10 Minutes)
The child is now engaged with both the screen and the material. This is where therapeutic learning happens. Follow the protocol matched to the material you introduced today.
▶ For Tangible Extensions
Animate the figure to mirror what's happening on screen: "[Character] is jumping on screen — your [character] is jumping too!" Goal: child begins to act out screen content with the physical object, shifting from passive viewing to active embodiment.
▶ For Parallel Activities
Place the activity page and say: "Can you draw [character] while we watch?" Do not demand. If child ignores, begin drawing yourself, narrating softly: "I'm drawing the nose..." Child may begin to imitate.
▶ For Visual Timer (Week 2+)
Announce the transition 30 seconds before the timer ends: "Timer is almost done. After the video, we're having [X]." Then follow through — every single time. Predictability IS the therapy.
▶ For Same-Content Variations (Week 2+)
"That song is done. Should we watch the OTHER [show name] song or that one again?" Offer choice with two options FROM THE SAME SHOW. The first acceptance of any variation is a genuine therapeutic milestone.
▶ For Social Viewing
Narrate what's on screen with brief, warm comments: "Oh wow — he found the treasure!" Do not ask questions. Narrate, pause, observe. If child responds vocally or with eye contact — celebrate silently (warm smile, soft "yes").
Research integration: ABA pairing + OT just-right challenge + SLP narrative scaffolding. PMC11506176
Step 4 of 6
④ Reinforcement (Throughout Session)
The reinforcement principle: In this intervention, you are reinforcing flexibility and joint engagement — not compliance with ending the video. This distinction is essential. Reinforcing the wrong behaviour at the wrong moment sets the programme back.
What to Reinforce (Week 1–2: Continuously)
- Child glancing at the material
- Child touching the material
- Child tolerating the timer without distress
- Child accepting your presence beside them
- Any spontaneous comment about the content
How to Praise — Specific, Not Generic
✅"You looked at the [character]! You did it!"
✅"You sat with me the whole time! That's amazing!"
❌ "Good boy/girl" — too generic; doesn't signal what was correct
✅"You sat with me the whole time! That's amazing!"
❌ "Good boy/girl" — too generic; doesn't signal what was correct
Reinforcement Hierarchy
Social praise (warmth + specific words) — try this first, always
Token toward reward jar — if social praise alone isn't working after 5 sessions
Brief preferred activity (5 more seconds of video) — as reinforcer, not as a trap
Canon Products
🛒Rosette Imprint Reward Jar — ₹589 — Pinnacle Recommends ✓
🛒1800+ Reward Stickers Set — ₹364 — Pinnacle Recommends ✓
🛒1800+ Reward Stickers Set — ₹364 — Pinnacle Recommends ✓

Step 5 of 6
⑤ Cool-Down Protocol (3–5 Minutes)
The transition OUT of video time is the highest-risk moment. A rushed or poorly managed ending erases the therapeutic gains of the previous 15 minutes. Speed of transition to the next activity is the single biggest predictor of transition success.
Stage 1 — Warning
"[Child's name], 2 more minutes of video. Then we're going to [specific next activity]."
Neutral tone. Matter-of-fact. No apology, no negotiation.
Neutral tone. Matter-of-fact. No apology, no negotiation.
Stage 2 — 30-Second Warning
"Last 30 seconds. After this, [character] is going to rest, and we're going to [next activity]."
Point to the visual timer and First-Then board.
Point to the visual timer and First-Then board.
Stage 3 — The Ending
Turn off screen and immediately say: "Okay! Video time is done. Now it's [next activity] time."
Move into the next activity IMMEDIATELY — do not pause in the ambiguity.
Move into the next activity IMMEDIATELY — do not pause in the ambiguity.
Transition Comfort Object: If distress is high, have a soft toy (the character figure from Material 1) available: "[Character] is going to sleep now. You can hold them while we [next activity]."
🛒Animal Soft Toys — ₹425 — Transition comfort object ✓

Step 6 of 6
⑥ Data Collection (2 Minutes, Post-Session)
Without data, you are guessing. With data, you are doing what 97% of Pinnacle families do — building an evidence base for YOUR child that allows the GPT-OS® to personalise the next intervention. This takes 2 minutes, immediately after each session.
Data Point | What to Note | |
Date and time | Log immediately after session | |
Material used today | Which of the 9 materials you introduced | |
Child's acceptance level | 0 (rejected) / 1 (tolerated) / 2 (engaged) / 3 (initiated) | |
Transition quality | 1 (crisis) / 2 (resistant but managed) / 3 (smooth) | |
Parent confidence | 1–5 scale — your own rating matters |
Parent Observation Notes — Key Behaviours to Record
- Any spontaneous communication during session
- Any voluntary variation from the preferred clip
- Duration of engagement with the material
- Anything that triggered resistance or unexpected success
Systematic data collection in home-based ABA/OT programs is a core evidence-based practice. NCAEP 2020.

Real Problems. Specific Solutions.
Troubleshooting is part of the protocol — not a sign of failure. Every one of the challenges below has been reported by thousands of Pinnacle families and has a specific, evidence-informed response.
Problem 1: Child screams when any material appears near the screen.
You moved too fast. Back up to Step 1 only for 5 consecutive days. Build tolerance of your presence first. The material can wait. Presence before objects — always.
Problem 2: Child accepts material but throws it immediately.
This IS engagement. Throwing = motor interaction = not ignoring. Calmly retrieve, place again, narrate: "Oh, [character] fell. Here they are again." Repeat 3–5 times. This is shaping, not failure.
Problem 3: Transition at the end always ends in meltdown.
Your visual timer needs more salience. Make it bigger, place it closer to the screen. Begin warning at 5 minutes, not 2. Shorten sessions so the warning doesn't feel catastrophic.
Problem 4: Child only wants to watch specific 30 seconds — not even the full clip.
This is a highly restricted loop. Begin with Same-Content Variations (Material 2): introduce a DIFFERENT version of that exact scene — different upload, different quality, different angle. Variations within the same 30 seconds before attempting episode variation.
Problem 5: 2 weeks in and nothing has changed.
Check: (a) Are you doing it daily? Consistency is non-negotiable. (b) Are you choosing the right material? Try a different one of the 9. (c) Is there an underlying anxiety or sensory profile needing professional assessment? Call 9100 181 181.
Problem 6: Family doesn't understand why we're "allowing" the video.
The intervention USES the preferred content as the therapeutic door — removing it entirely would close the door entirely. Share the Family Guide (Card 37) with all caregivers immediately. Alignment is non-negotiable.

No Two Children Are the Same. Here Is How You Adjust.
The protocol adapts to your child's sensory profile, age, and current tolerance window. Use this adaptation matrix to tune the intervention before you begin — and revise it every 7 sessions as your child's capacity grows.
Sensory Seeker (Seeks Input)
- Responds well to tangible extensions and parallel building
- Can tolerate more stimulation alongside the screen
- Parallel activities work quickly — try LEGO, playdough, building blocks
- Reinforcement can be more celebratory and expressive
Sensory Avoider (Overwhelmed by Input)
- Responds better to visual timers, scheduled access, same-content variations
- Needs quieter, slower material introduction — one step at a time
- Social viewing at more distance initially; build proximity slowly
- Reinforcement must be quiet, warm, and low-key
Age-Based Modifications
Ages 2–3
Extremely brief sessions (5–8 min). Comfort object as primary material. Verbal script is minimal — action over words.
Ages 4–6
All 9 materials accessible. Colouring and character play most effective. Ideal window for building flexibility.
Ages 7–10
Content-inspired creation and interactive alternatives become primary. Scheduled access system with child's input begins.
Ages 10+
Child can co-design their own scheduled access system. GPT-OS® self-monitoring tools fully applicable.

Your Protocol
Build Your Child's A-075 Protocol Right Now
Your protocol is a living document — not a one-size prescription. The intervention that works is the one designed for THIS child, not "a child with autism." Revise after every 7 sessions based on your data.
Child Profile
Child's age: ______
Primary sensory profile: Seeker / Avoider / Mixed
Preferred content: ______________________
Primary sensory profile: Seeker / Avoider / Mixed
Preferred content: ______________________
Starting Material (Pick 1)
☐ Tangible Extensions
☐ Visual Timer
☐ Same-Content Variation
☐ Parallel Activity
☐ Social Viewing
☐ Sensory Alternative
☐ Content Creation
☐ Interactive Alternative
☐ Scheduled Access
☐ Visual Timer
☐ Same-Content Variation
☐ Parallel Activity
☐ Social Viewing
☐ Sensory Alternative
☐ Content Creation
☐ Interactive Alternative
☐ Scheduled Access
Session Schedule
Morning session: _______ AM
Duration: _____ minutes
Evening session: _______ PM
Duration: _____ minutes
Transition activity: ______________
My reinforcer: __________________
Duration: _____ minutes
Evening session: _______ PM
Duration: _____ minutes
Transition activity: ______________
My reinforcer: __________________
"The Pinnacle GPT-OS® personalises across 70,000+ technique variables. Your protocol is the starting point — the system refines it as your data grows."

Progress Tracker
Weeks 1–2: Planting Seeds You Cannot See Yet
These are the real indicators of progress in weeks 1 and 2 — not the ones you might expect. The foundations being laid right now are invisible, but they are the most important work of the entire programme.
✅ These ARE Progress
Child tolerates your presence during viewing without tensing
Child looks at the placed material even once — neural acknowledgement
Child does not escalate when the timer is visible — tolerance building
Meltdown at transition is 2 minutes shorter than last week
You completed 10 of 14 sessions — consistency drives outcomes
Child looks at the placed material even once — neural acknowledgement
Child does not escalate when the timer is visible — tolerance building
Meltdown at transition is 2 minutes shorter than last week
You completed 10 of 14 sessions — consistency drives outcomes
❌ Not Progress Yet — And That's Okay
Child has NOT accepted a different video yet
Child has NOT spontaneously turned off the screen
Child still protests at session end
These will come. They are week 3–8 goals, not week 1–2 goals.
Child has NOT spontaneously turned off the screen
Child still protests at session end
These will come. They are week 3–8 goals, not week 1–2 goals.
"The same 30-second clip. For months. It took 8 months. Now she has maybe 15 clips she rotates through, and she can tolerate transitions with warnings." — Parent, Pinnacle Network | Chennai
In weeks 1–2, you are building relationship safety with the technique. The child is learning: "This person can be in my space. This object is safe. This timer doesn't mean danger." That is foundational work. PMC11506176 — Sensory integration outcomes emerge across 8–12 week timelines.
Progress Tracker
Weeks 3–4: The Neural Pathways Are Forming
By weeks 3 and 4, you may begin to notice something shifting — not just in your child, but in yourself. Your calm presence is the most therapeutic element in the room. These consolidation indicators signal that new neural pathways are strengthening.
Child reaches for the material without prompting
Spontaneous engagement — the material has become part of the experience, not an intrusion.
Child looks at the timer and returns to watching calmly
The timer is no longer a threat signal — it is a predictable fixture of the environment.
Child accepts 1 variation within the same content
A different song from the same show, a different episode — any variation is a milestone.
Child makes a communicative gesture or sound related to the material
Points, vocalises, or gives you the figure — first functional communication through the technique.
What to Increase in Weeks 3–4
- Introduce a second material (try one you haven't used yet)
- Extend session duration by 3–5 minutes
- Begin introducing Same-Content Variations if not yet done
- Try transitioning to TWO different activities, not just one
Neuroplasticity evidence: synaptic strengthening through repeated structured input follows predictable timelines in pediatric populations. You are on track.
Progress Tracker
Weeks 5–8: From Loop to Library
By the end of week 8, the goal is a nervous system that has learned: "Variation is safe when it comes from familiar places." This is not rushing — this is the natural gradient of a brain that has built genuine flexibility.
Week 5–8 Target Goals
- 3–5 clips/episodes the child will accept (same show initially)
- Scheduled access system functioning with fewer than 2 protests per week
- Child can communicate preference between two options
- Transition time reduced by 50% from baseline
The Library Expansion Gradient
Family Consistency Check
By week 5, the protocol MUST be consistent across ALL caregivers: both parents, grandparents, and school teachers. Inconsistency signals to the child that the rules are negotiable — which increases anxiety and resistance.
WHO CCD Package: Multi-caregiver training is critical for intervention generalisation. PMC9978394
Every Milestone Matters. Here Is How to Mark Them.
These milestones don't make the news. No one gives you an award for the fact that your child sat beside you during a video for the first time. But we know. The Pinnacle Consortium knows. And 20 million sessions of data confirm: this is where transformation begins.
🏅 First Tolerance
Child let the material sit in the space without rejecting it
🏅 First Touch
Child made physical contact with the material
🏅 First Calm Timer
Child watched the timer end without crisis
🏅 First Variation
Child accepted a different version of preferred content
🏅 First Smooth Transition
Session ended without meltdown — a genuine breakthrough
🏅 First Spontaneous Request
Child pointed to or asked for the material independently
🏅 First New Clip
Child watched a completely new video willingly
🏅 First Social Viewing
Child watched with a family member, with genuine connection
Red Flags
These Signals Mean Professional Support Is Needed Now
🔴 ESCALATE IMMEDIATELY — Call 9100 181 181:
• Media fixation is intensifying despite 4+ weeks of consistent intervention
• Child is showing increased self-injurious behaviour related to video interruptions
• Sleep is severely disrupted by fixation on video content
• Child is showing signs of anxiety disorder (persistent fearfulness, somatic complaints, regression)
• The loop is replacing ALL other activities — child no longer eats, plays, or communicates outside of viewing
• Media fixation is intensifying despite 4+ weeks of consistent intervention
• Child is showing increased self-injurious behaviour related to video interruptions
• Sleep is severely disrupted by fixation on video content
• Child is showing signs of anxiety disorder (persistent fearfulness, somatic complaints, regression)
• The loop is replacing ALL other activities — child no longer eats, plays, or communicates outside of viewing
🟡 SCHEDULE PROFESSIONAL REVIEW:
• No measurable progress after 8 weeks of daily consistent intervention
• Child is on medication that may be affecting response
• The intervention is causing more family conflict than it is resolving
• Other developmental concerns are emerging simultaneously
• No measurable progress after 8 weeks of daily consistent intervention
• Child is on medication that may be affecting response
• The intervention is causing more family conflict than it is resolving
• Other developmental concerns are emerging simultaneously
🟢 CONTINUE HOME PROGRAMME:
• Slow but measurable progress is occurring
• Child is tolerating the technique even if gains are small
• Family is consistent and emotionally stable in the protocol
• Slow but measurable progress is occurring
• Child is tolerating the technique even if gains are small
• Family is consistent and emotionally stable in the protocol
Diagnostic Lens
Persistent, rigid media fixation not responding to structured intervention within 8–12 weeks may indicate:
- High-anxiety profile requiring medication review
- OCD-spectrum overlap (requires specialist assessment)
- Sensory processing disorder requiring clinic-based OT
- Unmet communication need (video may be substituting for language)
CIN: U74999TG2016PTC113063 | DPIIT: DIPP8651 | MSME certified
Where Does A-075 Fit in Your Child's Complete Therapy Journey?
This home programme is the first chapter — not the whole story. Understanding where A-075 connects to the broader clinical pathway helps you plan your child's journey with confidence and clarity.
Related Techniques to Explore Next
A-074
When Child Shows Visual Overwhelm — "When everything is too much"
A-076
When Child Shows Movement Sensitivity — next in the visual challenges series
B-001
Building Joint Attention Through Shared Interest — communication foundation
C-015
Emotional Regulation Through Predictable Routines — anxiety support
D-042
Flexibility Training: Same-Familiar-New Hierarchy — expanding beyond media

Domain A — Visual Challenges
Build Your Child's Complete Visual Flexibility Toolkit
A-075 is the final technique in the Visual Challenges sub-series (A-056 to A-075). Each related technique addresses a connected dimension of visual processing — together they form a comprehensive sensory foundation.

A-074 — Visual Overwhelm
"When everything is too much." Materials and protocols for children who experience distress from visual complexity, bright environments, or busy scenes.

A-073 — Side-Eye Gaze
"When the child avoids direct visual input." Therapeutic approaches for peripheral gaze patterns and visual avoidance behaviours in ASD.

B-001 — Joint Attention
"Shared attention as a communication foundation." Builds the critical pre-verbal skill of shared focus — the gateway to language and social connection.

D-033 — Demand Flexibility
"Expanding tolerance for change across routines." The natural progression from media flexibility into broader daily life transitions and routine changes.
Your Child's Journey. The Complete Picture.
A-075 is one technique in a system of 70,000+. Understanding where it sits in the full developmental map helps you see your child's growth as a coherent journey — not a series of isolated appointments. The GPT-OS® holds the map and guides the sequence.
70,000+ Techniques
Mapped across 12 developmental domains — from sensory and communication to behaviour and feeding.
128 Canon Materials
Systematically mapped to techniques, with DIY alternatives for every family regardless of means.
GPT-OS® Personalisation
The system personalises the sequence for YOUR child's AbilityScore® profile — no two protocols are identical.
EverydayTherapyProgramme™
Every technique — including A-075 — integrates into a home programme that runs alongside center therapy.
"We don't treat individual behaviours. We develop whole human beings. The techniques are the vocabulary. The GPT-OS® is the grammar. Your child's growth is the story." — Pinnacle Blooms Network® Founder's Vision

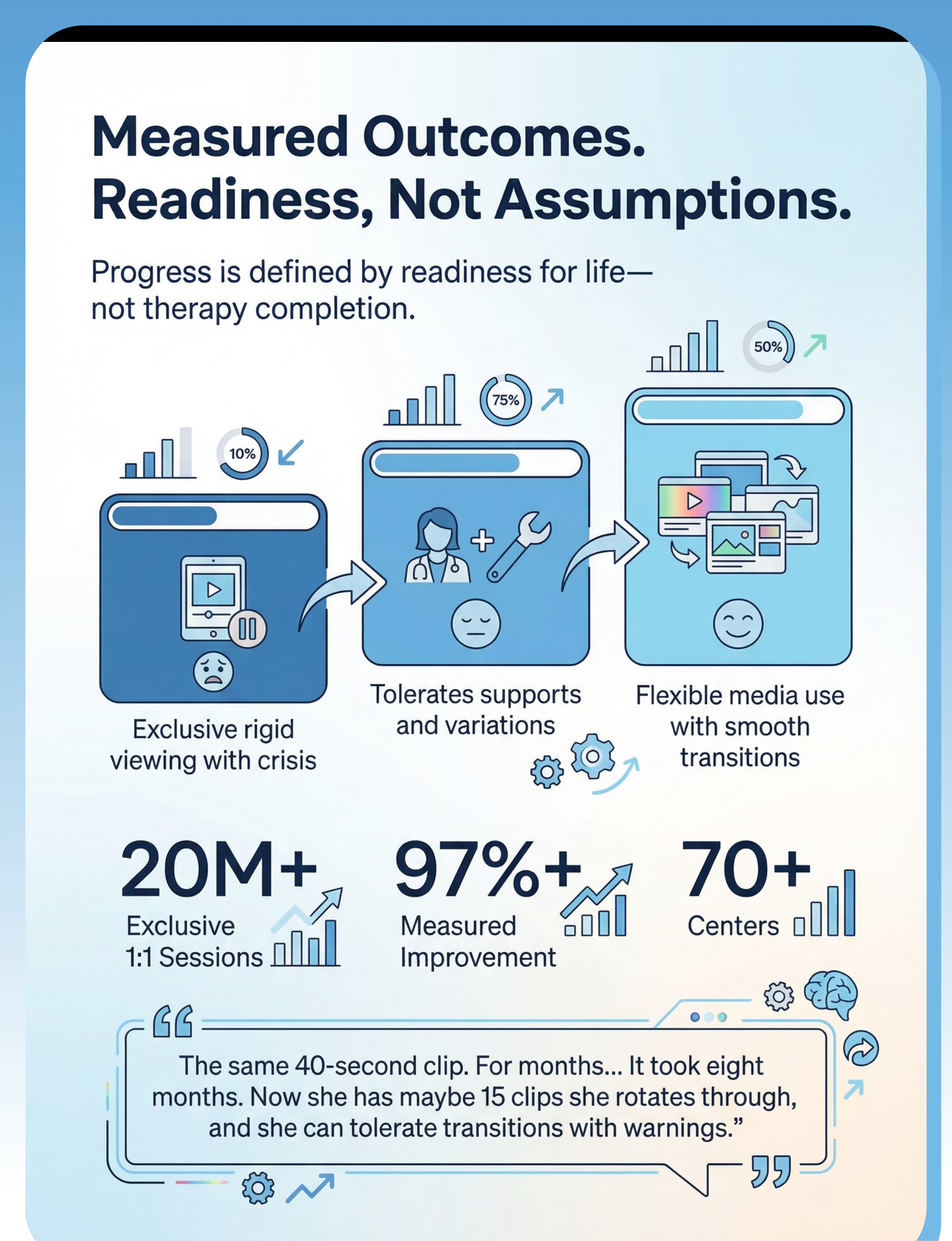
From Families Who Were Exactly Where You Are
"The same 40-second clip. For months... It took eight months. Now she has maybe 15 clips she rotates through, and she can tolerate transitions with warnings."
— Parent, Pinnacle Network | Chennai
"I thought removing the tablet was the answer. It made everything 10 times worse. The Pinnacle team showed me that the video was the door, not the problem. Now he uses the character figures to tell me what he wants. His first real requests came through that cartoon."
— Father, Hyderabad | ABA + OT FusionModule™ family
"The visual timer changed our evenings. Not the first week — the 4th week, suddenly, he looked at it and said 'done.' Just like that. Four weeks of groundwork for one word. Worth every session."
— Mother, Bangalore | EverydayTherapyProgramme™ participant
20M+
Exclusive 1:1 Sessions
97%+
Measured Improvement
70+
Centers Across India
70+
Countries Served
Individual results may vary. Statistics represent aggregate outcomes across the Pinnacle Blooms Network.

You Are Not Navigating This Alone
Isolation is the enemy of progress. The family that connects, shares, and witnesses other children's journeys accelerates their own child's outcomes. This is not sentiment — it is measured in our outcome data. Join a global community of families doing exactly what you're doing.
Pinnacle Parent WhatsApp Community
Real parents. Real questions. Real answers from therapists. The fastest way to connect with families navigating the same daily challenges.
pinnacleblooms.org/community
Discussion forums, technique sharing, and parent-to-parent mentoring across all 70,000+ techniques in the library.
@pinnaclebloomsnetwork
Daily content from the therapy floor. Technique demonstrations, parent wins, and behind-the-scenes from 70+ centers.
YouTube: Pinnacle Blooms Network
Video library including the A-075 Reel. Watch the technique demonstrated before your first session — see it in action.
Families from 70+ countries are in this community. Questions in Tamil, Telugu, Hindi, English, Arabic, Swahili — answered by Pinnacle's multilingual team. 📞 9100 181 181
70+ Centers Across India
70+ Pinnacle Centers Across India. One Near You.
AbilityScore® Diagnostic
Comprehensive multi-domain assessment that anchors your child's personalised GPT-OS® pathway.
Multi-Disciplinary Therapy
OT, SLP, ABA, SpEd, and NeuroDev working as one integrated FusionModule™ team.
Home Programme Design
Center therapy extends into your home through EverydayTherapyProgramme™ — so every moment counts.
Outcome Tracking
Every session feeds the GPT-OS® data layer — your child's gains are measured, documented, and built upon.
For A-075 specifically, ask for: Paediatric OT with sensory integration certification | ABA/BCBA with media behaviour protocol experience | NeuroDev Paediatrician if anxiety or OCD-spectrum concerns are present.
Deeper Reading for the Curious Parent and the Referring Clinician
Every claim in this technique guide is anchored in peer-reviewed evidence. Below is the complete reference library for A-075 — formatted for parents who want to understand the science, and for clinicians preparing referral documentation.
# | Study | Key Finding | Link | |
1 | PRISMA Systematic Review, Children (2024) | 16 studies confirm sensory integration EBP for ASD | ||
2 | Meta-analysis, World J Clin Cases (2024) | Multi-modal sensory interventions improve adaptive behaviour | ||
3 | WHO CCD Package Review, BMC Pediatrics (2022) | Home-based caregiver interventions validated across 54 LMICs | ||
4 | Padmanabha et al., Indian J Pediatr (2019) | Indian RCT: home-based sensory interventions show significant outcomes | ||
5 | Frontiers in Integrative Neuroscience (2020) | Neurological basis for sensory-based interventions in ASD | ||
6 | NCAEP Evidence-Based Practices (2020) | Video modelling, reinforcement, and extinction are EBPs for autism | ||
7 | WHO Nurturing Care Framework (2018) | Responsive caregiving framework with global implementation |

GPT-OS® Technology
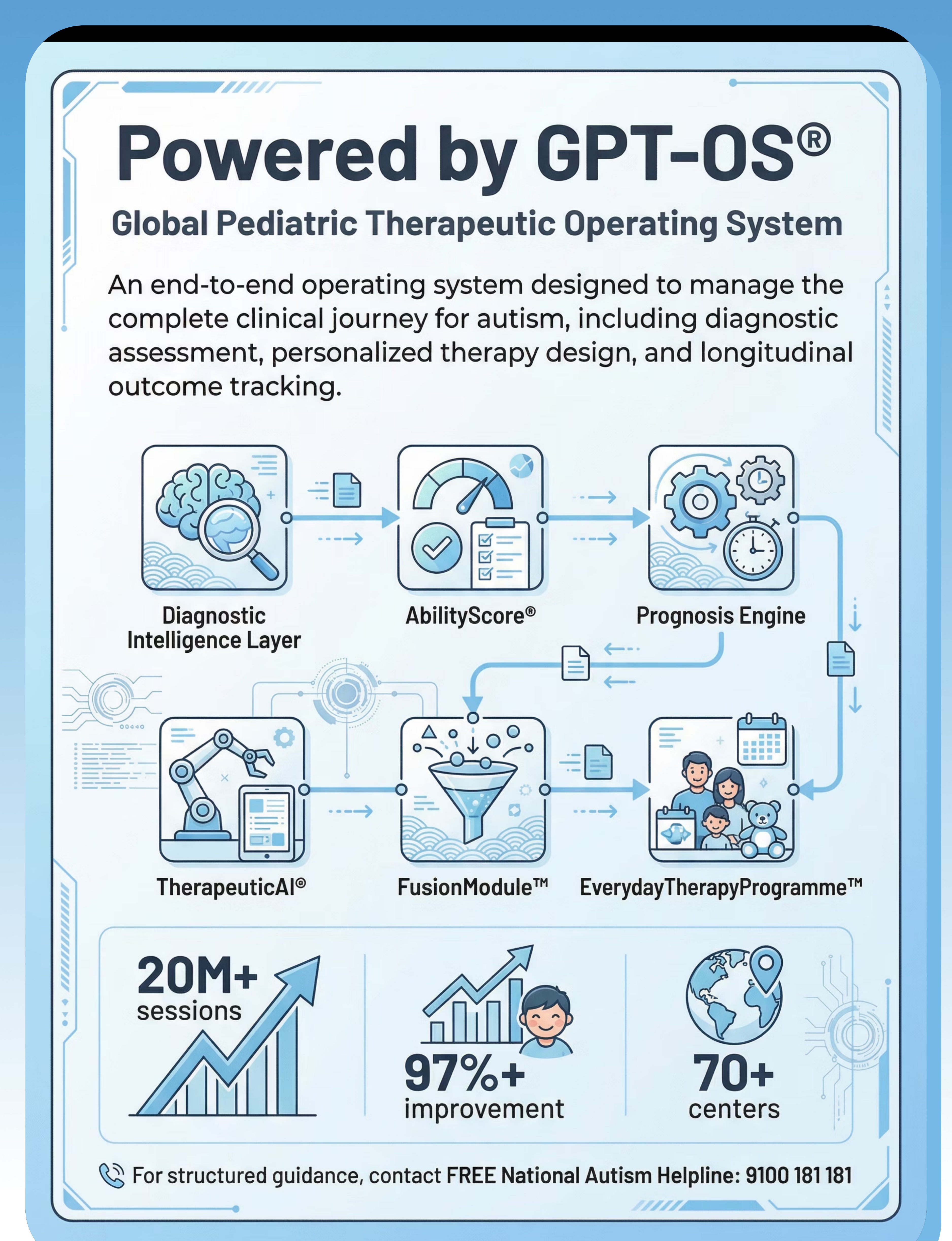
Powered by GPT-OS® — Global Pediatric Therapeutic Operating System
When you log your A-075 sessions via the tracker, your anonymised data contributes to a system that serves children across 70+ countries. The more families participate, the smarter and more personalised the system becomes — for everyone.
What Your A-075 Data Contributes
- Refines the GPT-OS® recommendation algorithm for families with similar profiles
- Improves the Weeks 1–2 and 3–4 milestones with population-level data
- Contributes to Pinnacle's CRO-grade longitudinal outcome database
- Identifies which of the 9 materials has the highest efficacy by age, sensory profile, and region
Privacy: All data is anonymised before analysis. No identifying information is shared. Pinnacle adheres to IT Act 2000 (India) and GDPR-equivalent standards for health data.
The GPT-OS® Stack
Diagnostic Intelligence Layer
AbilityScore® fed by your A-075 session data
Prognosis Engine
Generates outcome predictions based on profile + consistency
TherapeuticAI®
Personalises technique sequence across 70,000+ options
FusionModule™
Integrates OT + SLP + ABA + SpEd into one protocol
EverydayTherapyProgramme™
This page — your home extension of center therapy

Watch the Reel
Watch the Reel That Brought Thousands of Parents Here
A-075 Reel Details
Title: 9 Materials That Help When Child Watches Same Clip
Domain: A — Visual Challenges (A-056 to A-075)
Series: Visual Challenges — Episode 75 of 999
Presenters: Pinnacle Blooms Consortium — OT + ABA Lead Therapists
Domain: A — Visual Challenges (A-056 to A-075)
Series: Visual Challenges — Episode 75 of 999
Presenters: Pinnacle Blooms Consortium — OT + ABA Lead Therapists
What's in This Reel
- All 9 materials demonstrated by Pinnacle therapists
- Parent dos and don'ts at the critical transition moment
- Before/after behaviour illustration
- Practical setup demonstration in a real home environment
Related Reels
A-074: Visual Overwhelm
When everything becomes too much — sensory load management
A-073: Side-Eye Gaze
When the child avoids direct visual input
A-076: Movement Sensitivity
Next in the visual challenges series
NCAEP (2020): Video modelling is an evidence-based practice for autism. Multi-modal learning (visual + text + demonstration) improves parent skill acquisition.

Consistency Across Caregivers Multiplies Impact
A technique practised by ONE caregiver gains 40% of its potential. Practised by ALL consistent caregivers — it gains 100%. The single biggest predictor of intervention failure is inconsistency across the caregiving team. Reference: PMC9978394
📲 Share on WhatsApp
Pre-written message: "I found this technique for [child's name]. Please read the Safety and Step-by-Step cards before trying it. Helpline: 9100 181 181"
📧 Share via Email
Pre-filled subject: "A-075: When [child's name] watches the same clip — please read before next visit"
🔗 Copy Link
techniques.pinnacleblooms.org/sensory-visual/watches-same-clip-A-075
What to Tell Grandparents
"We are not encouraging the video behaviour — we are using it as a therapeutic bridge to teach flexibility. The goal is that in 8 weeks, [child's name] can handle the video ending calmly. For now, please use the visual timer and give the 2-minute warning."
Downloads for Extended Caregivers
The teacher template is a formal letter explaining A-075 goals for school staff, requesting classroom consistency with the home protocol.

The Questions Every Parent Asks
"Won't this just reinforce the video-watching behaviour?"
No. The technique does not reinforce the loop — it introduces structured variation and reinforces engagement with materials and transitions. The video is the entry point, not the target behaviour. ABA extinction + DRA principles apply: we are differentially reinforcing alternative and more flexible responses.
"How long before I see results?"
Tolerance indicators typically appear in Week 1–2. Measurable flexibility (accepting 1 variation) typically emerges in Week 3–4. Significant library expansion (5+ clips accepted) is a Week 8–12 goal. Individual results vary based on daily consistency, sensory profile, and anxiety levels.
"My child is non-verbal. Can this technique still work?"
Yes — and it is particularly powerful for non-verbal children because the content provides a rich, shared reference point. The tangible extensions and social viewing components often produce the child's first functional communication acts: pointing, giving, requesting the figure.
"Should I limit screen time overall while doing this?"
For this technique specifically: during the intervention period, maintain consistent, scheduled video time — not unlimited access, but not abrupt removal either. The Scheduled Access System (Material 9) is designed to structure this appropriately.
"What if different caregivers have different rules about the video?"
Inconsistency is the single biggest predictor of intervention failure. It signals to the child that the rules are negotiable — which increases anxiety and resistance. ALL consistent caregivers must follow the same protocol. Use the Family Guide (Card 37) to align them.
"Can I do this without any purchased materials?"
Yes. Every material has a ₹0 DIY alternative. The technique is about the interaction pattern, not the materials' cost. Start with social viewing, a visual timer drawn on paper, and any familiar soft toy as the comfort object.
"My child is 9 years old. Is it too late?"
No. Neuroplasticity continues well beyond early childhood. For older children, the intervention shifts — the child should be involved in co-designing their own scheduled access system. GPT-OS® protocols for ages 8–12 use metacognitive and self-monitoring approaches.
"When should I involve a professional therapist?"
Any time — a Pinnacle assessment can run alongside your home programme. If no measurable progress in 8 weeks, or if any red flags appear, professional involvement becomes essential rather than optional. Call 9100 181 181 for a free consultation.

You Have Everything You Need to Start Today.
The most powerful intervention is the one that begins. Not tomorrow. Today. Your child's nervous system is ready to learn — and you are ready to teach. The Pinnacle Blooms Consortium stands behind every step of this technique with 20M+ sessions of evidence.
20M+
Exclusive 1:1 Sessions
97%+
Measured Improvement
70+
Centers in India
70+
Countries Served
21M
Therapy Services
Validated by the Pinnacle Blooms Consortium across 20M+ exclusive 1:1 sessions. 97%+ measured improvement. Built by India's largest autism therapy network for families across 70+ countries. Consortium: OT • SLP • ABA • SpEd • NeuroDev • CRO
Preview of 9 materials that help when child watches same clip Therapy Material
Below is a visual preview of 9 materials that help when child watches same clip therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.






Link copied!
"From Fear to Mastery. One Technique at a Time."
Pinnacle Blooms Network® is India's largest multi-disciplinary pediatric therapy consortium — 70+ centers across India, serving children from 70+ countries through 21 million therapy services, achieving 97%+ measured improvement through the proprietary GPT-OS® (Global Pediatric Therapeutic Operating System). Built by mothers. Engineered as a system. Validated by science.
FREE National Autism Helpline: 9100 181 181
16+ Languages | 7 Days a Week | Available for every family, regardless of means
16+ Languages | 7 Days a Week | Available for every family, regardless of means
This content is educational. It does not replace assessment by a licensed developmental specialist, behavioural therapist, or healthcare provider. Persistent restricted media behaviours, especially when accompanied by other developmental concerns, should be evaluated within a comprehensive developmental assessment. Individual results may vary. Statistics represent aggregate outcomes across the Pinnacle Blooms Network.
© 2025 Pinnacle Blooms Network®, unit of Bharath Healthcare Laboratories Pvt. Ltd.
CIN: U74999TG2016PTC113063 | DPIIT Recognition: DIPP8651 | MSME Registered | All rights reserved.
Global IP protection. Unauthorised reproduction prohibited. Technique A-075 → loops to A-076.
CIN: U74999TG2016PTC113063 | DPIIT Recognition: DIPP8651 | MSME Registered | All rights reserved.
Global IP protection. Unauthorised reproduction prohibited. Technique A-075 → loops to A-076.