
"He talks for an hour. She never notices they've walked away."
You are sitting at the dinner table. Your child has been explaining the exact speed specifications of the Shanghai Maglev for the fourteenth time this week. You have tried to respond. You have tried to change the subject. He doesn't notice. He doesn't pause. When you finally manage a word, he acknowledges it with the briefest nod — and continues exactly where he left off.
This is not rudeness. This is not selfishness. This is a genuine difference in how your child perceives conversation. And it can be taught.
🧠"You are not failing. Your child's brain processes conversation differently — and that difference has a name, a science, and a pathway forward." — Pinnacle Blooms Consortium, Speech-Language Pathology Division
Technique B-207
Domain B: Social Communication
Episode 207

You Are Among Millions of Families Navigating This.
Research published in the World Journal of Clinical Cases (2024), analyzing 24 studies, confirmed that pragmatic language difficulties — including one-sided conversation patterns — are among the most impactful and most intervention-responsive challenges in pediatric development.
1 in 36
Children Globally
Diagnosed with autism, for whom reciprocal communication difficulty is a defining feature.
70–80%
With ASD
Show significant pragmatic language impairment including reduced conversational reciprocity.
21M+
Therapy Sessions
Delivered by Pinnacle Blooms Network across India — many specifically targeting social communication.
In India, Padmanabha et al. (Indian Journal of Pediatrics, 2019) demonstrated that structured home-based communication interventions produce significant outcomes — meaning what you do at home matters enormously. Across Pinnacle's 70+ centers serving families from 70+ countries, reciprocal communication difficulty is one of the three most commonly addressed goals in the Social Communication domain. You are not alone. And this is not permanent.
PMC11506176
PMC10955541
Padmanabha et al. 2019
WHO NCF 2018

This Is a Wiring Difference. Not a Choice. Not a Character Flaw.
What's Different in Your Child's Brain
For many children with social communication differences, the background monitoring program that tracks conversation runs less automatically. The prefrontal cortex — responsible for social awareness and conversational self-regulation — processes social cues less intuitively. The Superior Temporal Sulcus, which reads facial expressions and body language in real time, may process listener disengagement more slowly or less reliably.
The Mirror Neuron System and the Theory of Mind network — the circuitry responsible for perspective-taking — show altered connectivity patterns. The result: your child genuinely may not notice that you've stopped listening — not because they don't care, but because their brain isn't automatically scanning for these signals.
What's Typically Happening
When most people converse, their brain automatically runs a "background program" that monitors: Is the listener still engaged? How long have I been talking? What did they just say that I should respond to? When is it their turn?
The good news: Neural pathways for social cognition are experience-dependent. Structured practice with explicit visual supports builds new pathways. This is neuroplasticity at work.
"The child who lectures isn't selfishly choosing monologue. They're navigating social interaction with a map that's missing the back-and-forth lane. Our job is to give them that map." — Pinnacle Blooms Consortium, NeuroDevelopmental Team
DOI: 10.3389/fnint.2020.556660
Your Child Is Here. Here Is Where We're Heading.
The WHO Care for Child Development (CCD) Package — implemented in 54 low- and middle-income countries including India — identifies reciprocal communication as a critical developmental milestone within responsive caregiving. When this milestone is delayed, structured intervention is the evidence-based pathway forward.
Age 2–3
Parallel play; simple parallel exchanges in familiar routines begin.
Age 3–4
Basic turn-taking in structured contexts; simple reciprocal exchanges emerging.
Age 4–6
Reciprocal conversation begins; perspective monitoring develops.
Age 6–9
Peer-level reciprocal dialogue; listener awareness becomes more automatic.
Age 9–14
Fully automatic listener monitoring; sophisticated conversational reciprocity with peers and adults.
⚠️Most children presenting with B-207 challenges are accessing skills from the earlier stages — even while their vocabulary and verbal ability may be far ahead. Typical age of presentation: 4–14 years.
Common co-occurring profiles: Autism Spectrum Condition, SPCD (Social Pragmatic Communication Disorder), high-functioning profiles with significant pragmatic language gaps, ADHD with impulsivity component. Research consistently shows: earlier is better, but never too late. The 8–12 week intervention window shows measurable outcomes in multiple systematic reviews.
PMC9978394
WHO CCD Package
UNICEF MICS

Clinically Validated. Home-Applicable. Parent-Proven.
Evidence Grade: Level I
Systematic Review + RCT
Confidence: HIGH — 90%
Based on PRISMA Systematic Reviews, Meta-Analyses, RCTs, and ASHA/NCAEP confirmed evidence-based practices — the strongest level of clinical evidence available.
Key Finding
Children who receive structured reciprocal communication intervention with visual supports and home practice show measurable improvement in conversation turn-taking, listener awareness, and peer interaction within 8–12 weeks.
Study | Finding | Population | |
PRISMA Systematic Review 2024 (PMC11506176) | 16 studies confirm pragmatic language intervention is evidence-based practice | Children 3–14, ASD | |
Meta-Analysis World J Clin Cases 2024 (PMC10955541) | Social communication intervention promotes social skills across 24 studies | Children with ASD, 24 RCTs | |
Padmanabha et al., Indian J Pediatr 2019 | Home-based structured interventions show significant outcomes in Indian children | Indian children 4–10 years | |
ASHA Practice Portal 2023 | Pragmatic language intervention: strong evidence base | Pediatric, varied diagnosis | |
NCAEP EBPs 2020 | Social narratives + visual supports: confirmed EBPs for autism | ASD, all ages |

Technique B-207: What It Is
🗣️ Formal Name
Reciprocal Communication Training (Pragmatic Turn-Taking Intervention)
Also known as: "The Two-Way Conversation Protocol" | "Tennis Match Talking"
Also known as: "The Two-Way Conversation Protocol" | "Tennis Match Talking"
📋 Session Parameters
Age Range: 4–14 years
Session: 15–25 minutes
Frequency: Daily practice, 3–5x/week
Setting: Home + School + Social contexts
Session: 15–25 minutes
Frequency: Daily practice, 3–5x/week
Setting: Home + School + Social contexts
🎯 Domain & Subdomain
Domain: B — Social Communication
Subdomain: B3 — Reciprocal Communication
Technique Code: B-207
Subdomain: B3 — Reciprocal Communication
Technique Code: B-207
Reciprocal Communication Training is a structured pragmatic language intervention that teaches children the explicit mechanics of two-way conversation: turn-taking, listener monitoring, question-asking, topic building, and proportionate speaking time. Unlike general communication therapy, this technique specifically targets the social-cognitive architecture of dialogue — the understanding that conversation is a shared, co-created exchange where both partners contribute, respond, and adjust.
The intervention uses visual maps, physical turn-taking objects, question scaffolds, listener cue training, and structured conversation games to make implicit conversation rules explicit and learnable. Evidence from ASHA, NCAEP, and multiple systematic reviews classifies these approaches as evidence-based practices for children with social communication differences.
Domain B: Social Communication
Subdomain: Reciprocal Communication
Turn-Taking Games

This Technique Crosses Therapy Boundaries — Because the Brain Doesn't Organize by Therapy Type.
Speech-Language Pathologist — PRIMARY
Pragmatic language evaluation and intervention; designs the conversation maps, scripts, and structured dialogue protocols. Assesses theory of mind and social cognition components.
ABA Therapist / BCBA — SECONDARY
Applies behavioral reinforcement principles to shape conversation turn-taking behavior; designs reinforcement schedules for question-asking and listener monitoring; runs discrete trial training for specific conversation components.
NeuroDev Pediatrician — OVERSIGHT
Assesses underlying social cognition profile; rules out or addresses co-occurring conditions (ADHD, anxiety); monitors overall developmental trajectory; provides family psychoeducation.
Special Educator — INTEGRATION
Implements conversation supports in academic and social contexts; designs classroom modifications; coordinates with school peers and teachers; runs social skills groups.
Parent / Family — HOME EXECUTION
The most critical role. Home practice 3–5x weekly multiplies clinic outcomes by 5–7x. Parents run the daily conversation protocols, maintain visual supports, track data, and create natural generalization opportunities.
"Reciprocal communication is not one therapist's territory. It requires the SLP to build the script, the BCBA to reinforce it, the SpEd to generalize it, the pediatrician to contextualize it, and the parent to live it daily. The Pinnacle FusionModule™ coordinates all five lanes simultaneously."
This Isn't a Random Activity. It's a Precision Tool.
Every component of B-207 targets a specific, measurable communication behavior — from the innermost core skill to the broader developmental gains that flow from it.
🎯 Primary Target
Reciprocal turn-taking in conversation — the child initiates turns, pauses for partner response, and waits before continuing.
Observable indicator: Child pauses after speaking and looks toward partner; average turn length decreases toward age-appropriate norms.
🎯 Secondary Targets
- Listener monitoring: Child checks listener's face/body for engagement cues
- Question-asking: Child asks at least 1–2 spontaneous questions per conversation
- Topic building: Child responds to what partner actually said before introducing new content
- Turn-length calibration: Child demonstrates awareness of proportionate speaking time
🎯 Tertiary Developmental Gains
- Peer friendship formation and maintenance
- Theory of mind development
- Reduced social isolation and rejection
- Academic participation in discussion-based learning
- Long-term: Adult relationship quality, vocational communication competence
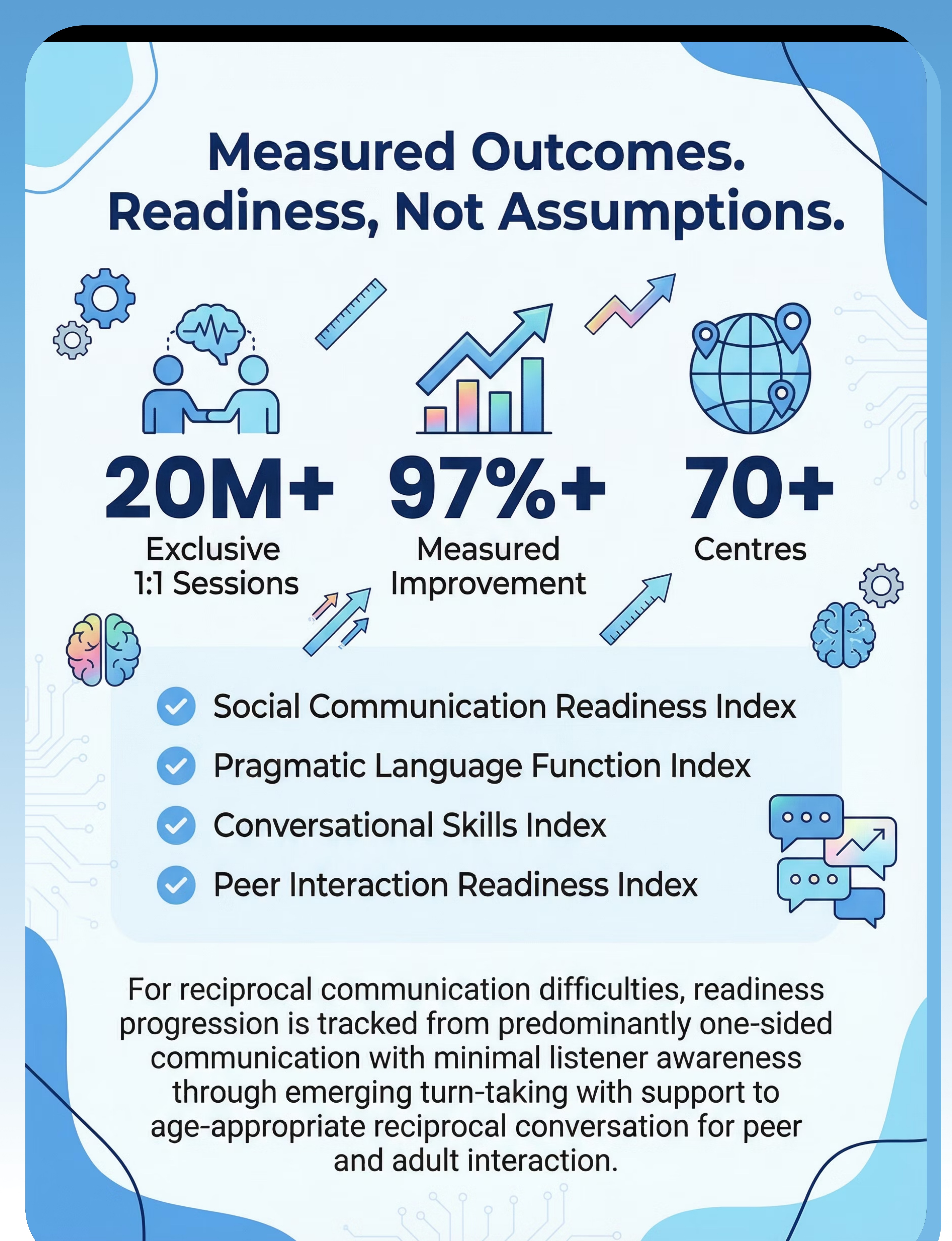
Progress Readiness Indexes (GPT-OS® Tracked)
✅ Social Communication Readiness Index
✅ Pragmatic Language Function Index
✅ Conversational Skills Index
✅ Peer Interaction Readiness Index
9 Materials. Each One Teaches a Different Piece of the Back-and-Forth.
Every material in the B-207 canon targets a distinct conversation skill. All have zero-cost DIY alternatives — no purchase is ever required to begin.
1
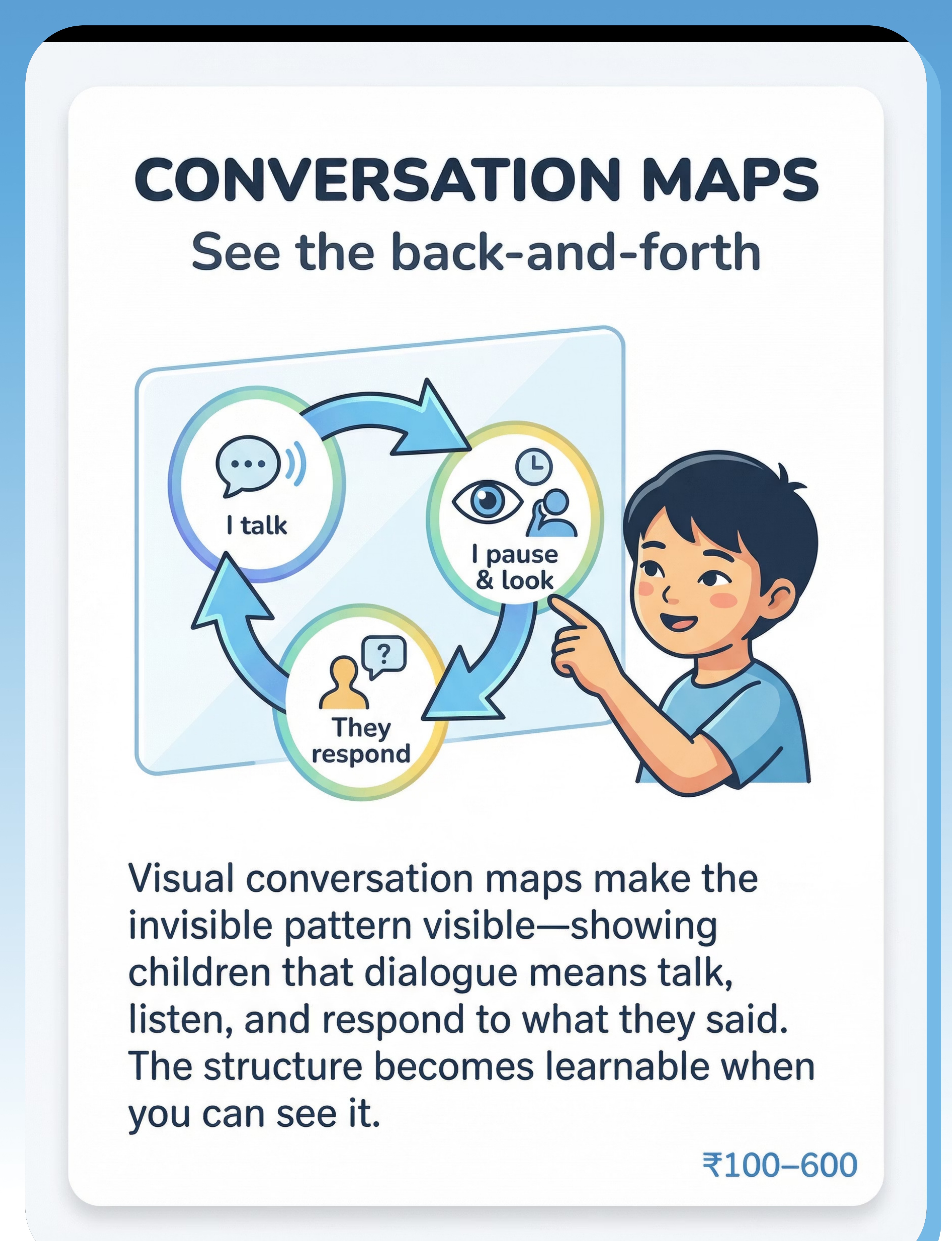
Visual Conversation Maps
Talk-Listen-Respond Charts that make the invisible conversation pattern visible. ₹100–600 | ✅ DIY: Zero-cost version available
2
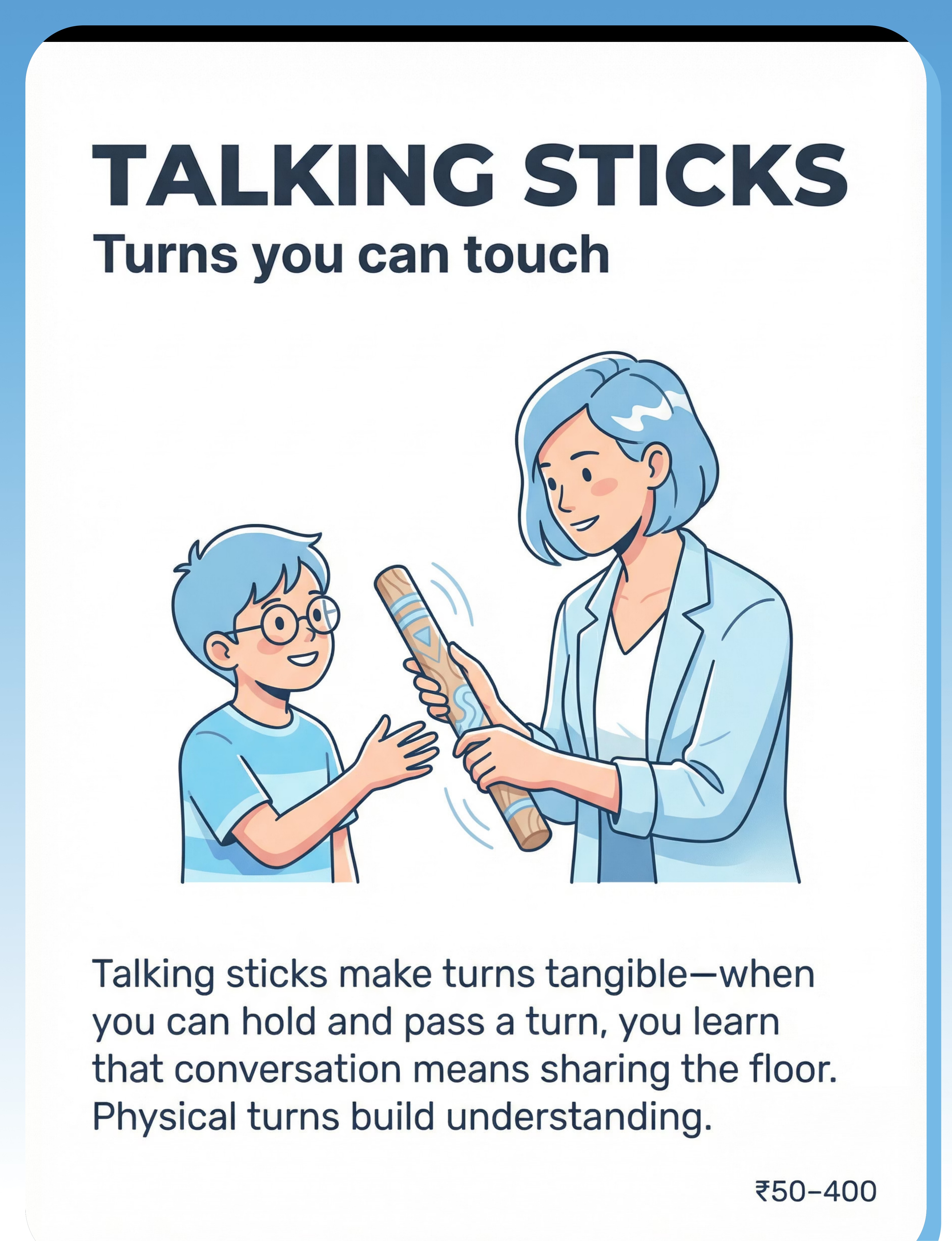
Talking Sticks & Turn-Taking Objects
Physical objects that make abstract turns tangible and holdable. ₹50–400 | ✅ Any passable object works
3
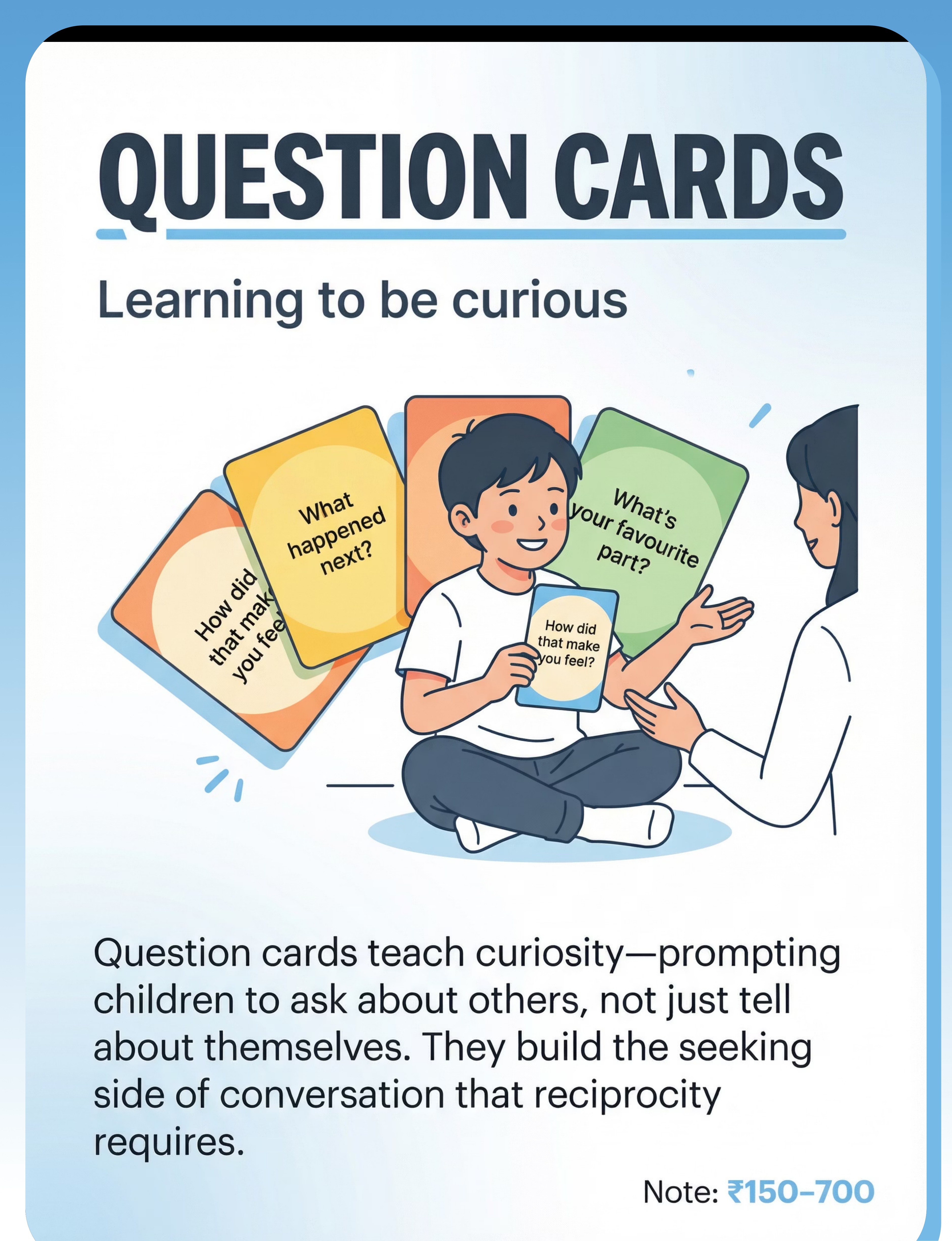
Question Cards & Curiosity Prompts
Structured prompts that build the question-asking half of reciprocity. ₹150–700 | ✅ Index card set
4
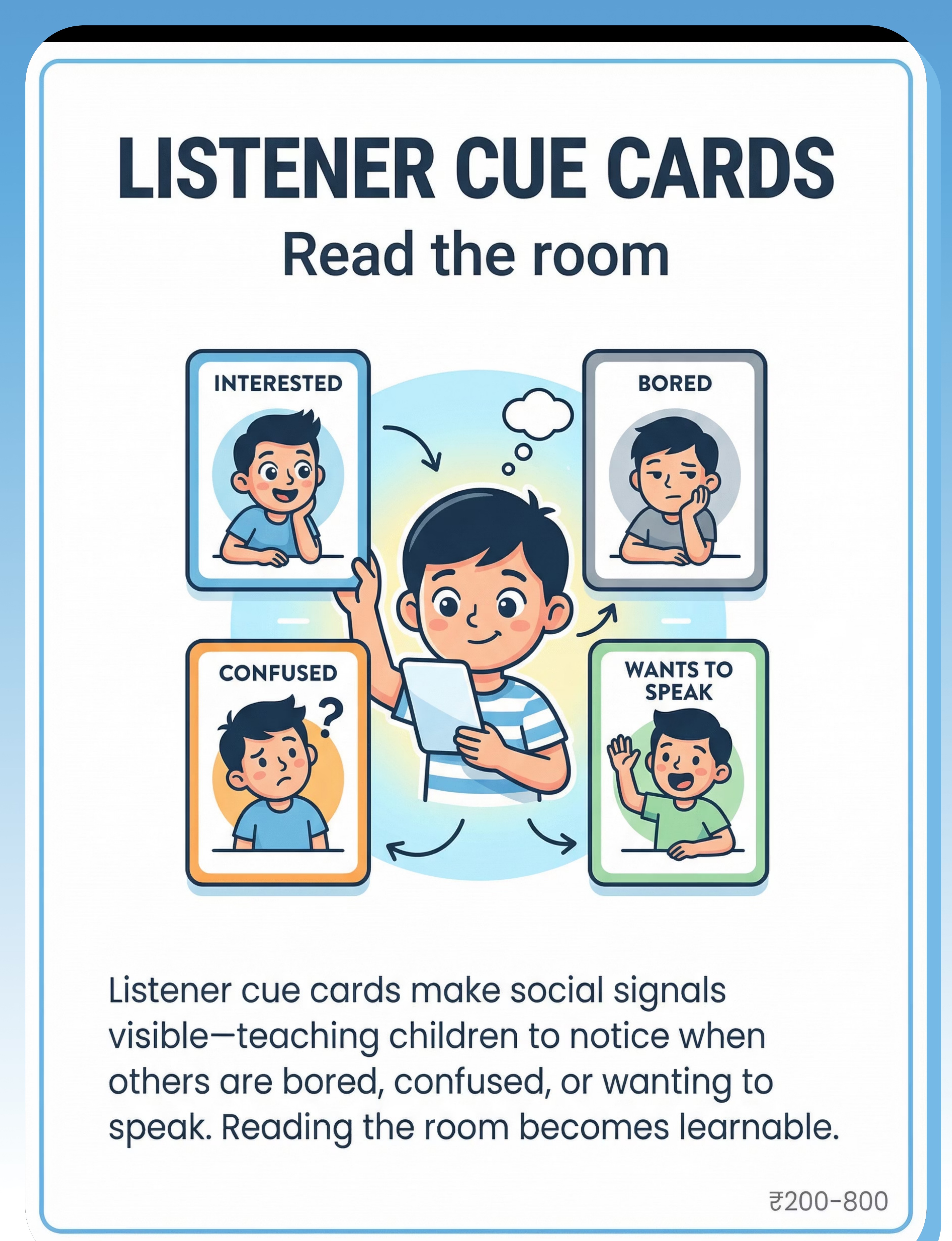
Listener Cue Cards
Visual guide to reading listener engagement, boredom, confusion, and desire to speak. ₹200–800 | ✅ Drawn/printed photo set
5
Conversation Timers
Sand timers and visual countdowns that build time awareness in conversation. ₹200–1,000 | ✅ Kitchen timer / phone timer
6
Topic Bridge Cards
Sentence starters like "That reminds me of…" connecting responses to what a partner said. ₹100–500 | ✅ Written on index cards
7
Social Stories
Stories told from two perspectives — speaker AND listener — building theory of mind. ₹200–900 | ✅ Write with your child
8
Video Recording & Playback Tools
Phone/tablet recording for children to see their own conversation patterns from outside. ₹0–5,000 (phone camera = ₹0) | ✅ Smartphone only needed
9
Structured Conversation Games
Board games, card games, and activity games that build reciprocal skills through play. ₹150–1,200 | ✅ Adapt any game with conversation rules
⭐Pinnacle Recommends Starter Set: If you can only start with 3 — Conversation Map (DIY) + Talking Stick (any object) + Question Cards (index cards). Total cost: ₹0.

Every Family Can Start Today. With What They Already Have.
Conversation Map — DIY
Draw a simple cycle on paper: "I TALK" → "I PAUSE + LOOK" → "THEY TALK" → "I LISTEN" → "I RESPOND." Alternatively: draw a tennis court. Ball on your side = your turn. Ball on other side = their turn. Zero cost.
Talking Stick — DIY
Any object your child finds special: a decorated wooden spoon, a favourite small toy, a smooth stone, a rolled paper tube. The magic is in the ritual, not the object. Only the holder speaks.
Question Cards — DIY
Write on 15–20 index cards: "What do YOU think about…?" / "How did that make you feel?" / "What happened next?" / "What's your favorite part?" / "Tell me more about that." / "What would you do if…?"
Listener Cue Cards — DIY
Print or draw four faces: INTERESTED (eye contact, nodding) | BORED (looking away, yawning) | CONFUSED (furrowed brow) | WANTS TO TALK (leaning forward). Label each with what to do: "Keep going!" / "Wrap up!" / "Explain again!" / "Stop and listen!"
Conversation Timer — DIY
Any kitchen timer, phone alarm, or sand timer. Set for 1–2 minutes. "Your turn to talk — when the timer rings, it's my turn."
Topic Bridge Cards — DIY
Write sentence starters on cards: "That reminds me of…" | "I also…" | "Something similar…" | "I agree because…" | "Tell me more about…" | "That makes me think…"
📖Social Story — DIY: Write a 1-page story with your child about a character (use a different name) who loves talking about their special interest. Include: what the speaker thinks, what the listener thinks, what happens to the friendship, and a better way the conversation could go. Draw simple illustrations together. Video Playback — DIY: Any smartphone. Record a 3-minute practice conversation. Watch together with a specific focus each time. Frame all review positively.
The WHO Nurturing Care Framework (2018) explicitly states that effective early intervention must be accessible regardless of family economic status. Every technique in the Pinnacle system has a zero-cost version.

Read Before Every Session. Non-Negotiable.
🔴 RED — STOP. Do Not Proceed If:
- Child is in active meltdown or severe dysregulation
- Child is unwell (fever, pain, significant illness)
- Child has shown aggressive behavior in last 30 minutes
- You (parent/caregiver) are overwhelmed or distressed — your regulation is contagious
- Conversation practice has triggered severe anxiety or shutdown in the last session without modification
🟡 AMBER — MODIFY. Proceed with Adjustments If:
- Child is mildly tired or hungry → shorten to 5 minutes, reduce complexity
- Child had a difficult day at school → use lighter game-based version, skip video review
- Child seems resistant → use choice: "Talking stick or Question cards first?"
- Parent has limited time → use dinner table talking stick only, 5-minute version
🟢 GREEN — GO. All Clear If:
- Child is fed, rested, and in baseline regulated state
- Environment is calm (low noise, no competing screens)
- You have 15–25 minutes without interruption
- Child has had a neutral to positive interaction in the last hour
Contraindications for Specific Materials
- Video Playback: Requires explicit child assent. Never review footage that caused distress. Focus on 1 skill per viewing only. Never criticism-oriented.
- Social Stories: Never present as "this is what you're doing wrong." Always: "This is a character learning something."
- Conversation Timers: If timers cause anxiety (common in OCD features), use visual sand timers only, or eliminate entirely.
- Talking Sticks: Ensure object is age-appropriate and not a choking/safety hazard for younger children.
🚨Red Line Protocol — Stop immediately if you observe: Severe crying/screaming or self-injurious behavior | Child completely shutting down | Aggressive behavior toward people or objects | Prolonged distress after session (>15 minutes). If these occur repeatedly: consult your Pinnacle SLP or call 9100 181 181.
Clinical Note: This content is educational and does not replace assessment by a licensed speech-language pathologist.
Clinical Note: This content is educational and does not replace assessment by a licensed speech-language pathologist.

Spatial Precision Prevents 80% of Session Failures.
Set Up Your Space
Room configuration:
Child and parent face-to-face, approximately 3 feet apart, at the same eye level. Materials on the table between both partners. Conversation Map posted on wall behind parent — visible to child during conversation. Timer at center of table. Cards on child's side. Game between both.
Child and parent face-to-face, approximately 3 feet apart, at the same eye level. Materials on the table between both partners. Conversation Map posted on wall behind parent — visible to child during conversation. Timer at center of table. Cards on child's side. Game between both.
Environmental settings:
Lighting: Warm, indirect — not fluorescent overhead.
Sound: Minimal background — no music, AC/fan quiet enough for voice.
Seating: Same height — not parent towering over child.
Lighting: Warm, indirect — not fluorescent overhead.
Sound: Minimal background — no music, AC/fan quiet enough for voice.
Seating: Same height — not parent towering over child.
Preparation Checklist
Remove from space:
- All screens (TV, tablets, phones — face-down is not enough)
- Toys that compete for attention, especially topic-interest items
- Siblings or competing noise sources
Prepare in space:
- Conversation Map posted at eye level
- Timer within both partners' view
- Talking stick placed between both partners
- Question cards fanned out visibly
- Listener Cue Cards near conversation map
- Data tracking sheet + pen ready
🏠Joint Family Note (Indian Context): In joint households, ensure privacy for the session. Other family members observing can distract or create performance pressure. If grandparents wish to participate: introduce them in Week 3–4 once your child has consolidated the basics. Consistency across caregivers multiplies outcomes — but sequence the introduction carefully.

The Best Session Is One That Starts Right.
Answer honestly before every session. This 60-second check determines whether you run a full session, a modified version, or postpone entirely — protecting your child's willingness to engage tomorrow.
Check | Target | If YES → | If NO → | |
🍽️ Child has eaten in the last 2 hours | Yes | Continue | Feed first, wait 20 min | |
😴 Child is not overtired | Yes | Continue | Postpone to tomorrow morning | |
🧘 Child is in baseline calm state | Yes | Continue | Use 5-min calming activity first | |
📅 No meltdown in last 2 hours | Yes | Continue | Modify to lightest version only | |
🏥 Child is not unwell | Yes | Continue | Skip — rest today | |
⏰ You have 20+ uninterrupted minutes | Yes | Continue | Use 5-minute dinner version instead | |
💚 You are regulated and patient | Yes | Continue | Take 5 minutes for yourself first |
ALL YES
→ Full Session (All phases)
3+ YES
→ Modified Session (Lighter game version only)
MAJORITY NO
→ Postpone (Do cool-down activity as standalone instead)
"Your regulation is the most important variable in every session. Children co-regulate with caregivers. If you are anxious, frustrated, or rushed — your child will feel it before the first word is spoken. 5 minutes of your own calming is worth more than 20 minutes of a session you're half-present for."

How You Begin Determines Whether the Session Actually Happens.
❌ Do NOT Say:
- "Time for conversation practice."
- "We're going to work on your talking today."
- "The therapist said we need to do this."
✅ For children motivated by games:
"Hey — want to play that conversation game? You got pretty good at question catch last time."
✅ For children motivated by their special interest:
"I want to hear about [trains/dinosaurs/Minecraft] for 2 minutes — but first let's do our talking game and then I'm all yours."
✅ For children motivated by video:
"We're going to record ourselves today and watch it back. You can be the director."
✅ For children who resist transitions:
"5 more minutes of what you're doing, then our conversation time. I'll set the timer."
✅ For teenagers:
"I read something interesting — want to try something for 10 minutes? It actually works on peer conversations."
"The invitation activates the Motivating Operation — the child's readiness to engage. Framing the activity as their idea, their interest, or their choice doubles completion rates and triples quality." — Pinnacle BCBA Division

2 Minutes of Shared Warmth Opens the Conversational Window.
Option A: "Tell Me One Thing"
Each person shares one thing about their day. No evaluation, just listening. Model exactly what you're teaching — pause, look, wait, respond to what they said.
Option B: Visual Map Review
Point to the conversation map together. "Today we're practising the [turn-taking/question-asking/bridge phrases] step. Which one do you want to focus on?" Child chooses = child invests.
Option C: Topic Menu
Offer 3 conversation topics on cards: child's interest + 1 shared + 1 about you. Child picks the topic. This pre-arranges success by using a topic they care about.
Option D: Joke or Riddle Exchange
Low-pressure reciprocal exchange using humor. Child tells joke. You respond. You tell joke. They respond. Same reciprocal structure — zero emotional loading.
What to Watch for in Warm-Up
- Child makes eye contact? → ↑ readiness for full session
- Child smiles or relaxes? → ↑ continue
- Child immediately begins monologue on preferred topic? → use talking stick immediately
- Child is silent and withdrawn? → move to lighter game option

The Core Back-and-Forth. The Engine of Change.
15–20 Minutes Total
4 Phases
Phase A: Structure (5 min) — Conversation Map + Talking Stick
Place the Conversation Map visible to both. Place the Talking Stick on the table between you. Say: "Whoever has the stick, talks. Then we pass it. Then we listen. Then we respond to WHAT THE OTHER PERSON SAID." Model one full cycle — share a sentence, place stick down, pause 3 seconds, look at child. Repeat 3–5 cycles. Target: 3 full exchanges per phase.
Phase B: Question Building (5 min) — Question Cards
Fan out Question Cards face-up between you. Each person picks a card and asks that question. Child picks card → reads question → you answer → you respond with follow-up. Gradually remove cards. Child prompted: "Pick your own question — ask me something without a card." Target: 2–3 spontaneous questions per session by Week 4.
Phase C: Cue Check (3 min) — Listener Cue Cards
Role-play: parent monologues for 90 seconds. Ask child: "What cue was I showing? Which card matches how I looked?" Reverse: child talks for 90 seconds; you show one of the four listener states. Child identifies your state. Most children need 3–4 weeks before independently spotting cues without prompts.
Phase D: Bridge Building (2 min) — Topic Bridge Cards
Practice 2–3 rounds: you make a statement → child uses a bridge card to connect their response → child adds their content. Example: You: "I had a really tiring day." Child: "That reminds me of… when I was tired after swimming." ✅ Bridge used.
Execution Error | Why It Happens | Fix | |
Child grabs stick and doesn't pass | Impulse control + habit | Put masking tape marker on table: "stick MUST cross this line before you take it" | |
Child reads question card but ignores answer | Still in information-delivery mode | Pre-teach: "Asking means WAITING for the answer and RESPONDING to it" | |
Child identifies wrong listener cue | Facial processing differences | Exaggerate expressions initially; add verbal cue: "I just yawned — what does that mean?" | |
Bridge cards feel mechanical | Early stage — normal | Fluency comes with practice; celebrate any use at all |

3 Good Reps Beat 10 Forced Ones. Every Time.
Repetition Guidance
Target frequency: 3–5 sessions per week
Target reps per phase: 3–5 exchange cycles — not more
Session length: 15–20 minutes. Never exceed 25 minutes without a break.
Signs of productive session: Child smiles, engages, asks at least 1 spontaneous question.
Signs of satiation: Child becomes silent, irritable, or seeks escape → end the phase, not the session.
Target reps per phase: 3–5 exchange cycles — not more
Session length: 15–20 minutes. Never exceed 25 minutes without a break.
Signs of productive session: Child smiles, engages, asks at least 1 spontaneous question.
Signs of satiation: Child becomes silent, irritable, or seeks escape → end the phase, not the session.
Variation Menu — Prevent Boredom Across Weeks
- Week 1–2: Structured talking stick + question cards (high scaffold)
- Week 3–4: Introduce conversation games as primary vehicle
- Week 5–6: Add video recording + playback review
- Week 7–8: Natural conversation with bridge card reminder only (low scaffold)
Topic Rotation
- Week 1: Their preferred topic (trains, Minecraft, dinosaurs)
- Week 2: Shared topic (family event, movie you both watched)
- Week 3: Parent's interest (child practices genuine curiosity)
- Week 4+: Novel topics drawn from life (age-appropriate news, community events)


Timing Matters More Than Magnitude. Celebrate the Attempt, Not Just the Success.
⏱️Within 3 seconds of desired behavior → specific, enthusiastic, genuine praise. After 10 seconds: the behavioral link fades. After 30 seconds: the child has no idea what you're praising.
When child pauses and waits:
"YES — you paused! You looked at me! That's the exact back-and-forth we're building!"
When child asks a spontaneous question:
"You just asked me a question WITHOUT the card! That's a real conversation move right there!"
When child uses a bridge phrase:
"You connected your answer to what I said — that's exactly what great conversationalists do!"
When child notices a listener cue:
"You caught that I was confused — and you explained it again. That's reading the room!"
When child passes the talking stick:
"You passed it. That's the whole game right there — sharing the floor."
Reinforcement Menu
Tier 1 — Natural
Extra 5 minutes of preferred activity. Child chooses next session's topic. Child leads dinner conversation for 3 minutes (earned).
Tier 2 — Token Economy
Conversation coin earned per full exchange cycle → 10 coins = agreed reward. Sticker chart visible on wall.
Tier 3 — Tangible
Small preferred item for weekly goal (e.g., 3 spontaneous questions in one week). Use sparingly — fade early.
Reinforce with: Rosette Imprint Reward Jar (₹589, amzn.in/d/02C5R9Jn) or 1800+ Reward Stickers (₹364, amzn.in/d/01wrHJWX)

No Session Ends Abruptly. The Exit Matters as Much as the Entry.
The cool-down ritual is itself embedded reciprocity practice — the closing exchange ("What was YOUR favorite part?") is a real question in a real moment, not a drill.
Warning (2 minutes before end): "Two more rounds, then we're done for today." Use visual timer with visible countdown.
Closing Exchange: Each person shares one sentence about the session. Child is prompted if needed: "What was YOUR favorite part?" — real reciprocity embedded in transition.
Material Put-Away Ritual: Child participates in packing away materials. This creates ownership and positive closure. "Talking stick in the [box/drawer]. Conversation map stays on the wall."
Bridge to Next Activity: Name what comes next: "After this, you have [10 minutes of trains/dinner/screen time]." Pre-naming reduces resistance at session end.
💡If child resists ending: Don't power-struggle — session success matters for next session's willingness. Use transition object: "The talking stick will be here tomorrow." Offer choice of cool-down activity. Never extend session as reward — this creates ending resistance habituation.

60 Seconds of Data Now Saves Hours of Guessing Later.
Fill this immediately post-session. Your data feeds into the AbilityScore® progression tracking and helps your Pinnacle therapist see exactly where your child is progressing and where to focus next.
📅 Session Basics
Date: _____________ | Session #: ____ | Duration: ____ min
🎯 Talking Stick Passes
Child passed stick without prompting: YES / NO / WITH PROMPT
Count of voluntary passes: ____
Count of voluntary passes: ____
❓ Questions Asked (by child)
Spontaneous (no card): ____ | With card: ____ | With verbal prompt: ____
👁️ Listener Cues Noticed
Noticed listener state: YES / NO
Which cue identified: _____________________
Which cue identified: _____________________
🌉 Bridge Phrases Used
Spontaneous: ____ | With card: ____ | With prompt: ____
⭐ Session Rating
Child engagement level: 😞 1 — 2 — 3 — 4 — 5 😊
Parent confidence level: 😞 1 — 2 — 3 — 4 — 5 😊
One-sentence observation: ________________________
Parent confidence level: 😞 1 — 2 — 3 — 4 — 5 😊
One-sentence observation: ________________________

Session Abandonment Is Not Failure. It's Data.
🔴 Child immediately launches into monologue, ignores all tools
Why: The habit of monologue is deeply reinforced. Materials feel like obstacles.
Fix: Use topic-entry strategy: "Tell me about [interest] for exactly 1 minute, then I ask you a question." Give the controlled monologue first, then transition.
Fix: Use topic-entry strategy: "Tell me about [interest] for exactly 1 minute, then I ask you a question." Give the controlled monologue first, then transition.
🔴 Child refuses to pass the talking stick
Why: Object attachment or hasn't internalized turn concept yet.
Fix: Put a physical boundary on the table. Reduce session to 3 exchanges only. Celebrate even 1 pass.
Fix: Put a physical boundary on the table. Reduce session to 3 exchanges only. Celebrate even 1 pass.
🔴 Child asks question from card but ignores the answer
Why: Still in information-delivery mode — question is social performance, not genuine curiosity.
Fix: Pre-teach: "Asking means waiting AND responding." After they ask, say: "Okay I'll answer — and then ask me what I think about that."
Fix: Pre-teach: "Asking means waiting AND responding." After they ask, say: "Okay I'll answer — and then ask me what I think about that."
🔴 Child gets anxious about video recording
Why: Self-consciousness; fear of criticism; sensory discomfort with camera.
Fix: Start by filming ONLY you (parent). Then watch together. Build trust. Never review footage that caused distress.
Fix: Start by filming ONLY you (parent). Then watch together. Build trust. Never review footage that caused distress.
🔴 Child melts down when timer rings ending their turn
Why: Timer is aversive; abrupt ending feels like interruption.
Fix: Switch to visual countdown only (no alarm sound). Give 30-second "wrap up" warning. Validate: "I know you have more to say. You can add one more sentence."
Fix: Switch to visual countdown only (no alarm sound). Give 30-second "wrap up" warning. Validate: "I know you have more to say. You can add one more sentence."
🔴 Progress plateaus — no improvement after 4 weeks
Why: May need professional assessment of underlying social cognition profile; or incorrect difficulty level.
Fix: Call 9100 181 181 or book a Pinnacle SLP session. Show your data tracker.
Fix: Call 9100 181 181 or book a Pinnacle SLP session. Show your data tracker.
🔴 Parent feels exhausted and doesn't want to do sessions
Why: Caregiver burnout is real. 20-minute sessions 5x/week is a significant commitment.
Fix: 3x/week is clinically sufficient. Use dinner table talking stick as embedded daily practice. Share this page with another caregiver. You don't have to do this alone.
Fix: 3x/week is clinically sufficient. Use dinner table talking stick as embedded daily practice. Share this page with another caregiver. You don't have to do this alone.
No Two Children Are Identical. Your Child Needs the Version That Fits Them.
1
Level 1 — Easier
Structured game with picture cards only. Maximum scaffolding, minimum pressure.
2
Level 2 — Core
Talking stick + question cards. Standard protocol as described.
3
Level 3 — Harder
Natural conversation with bridge cards only. Minimal scaffolding, maximum generalization.
Ages 4–6
- Session = 8–10 minutes maximum
- Use stuffed animals as partners (lower pressure)
- Talking stick = favourite toy
- 1 skill only per session
- Praise ratio: 5 celebrations per correction
Ages 10–14
- Frame as "social intelligence skill" not "therapy"
- Use real peer scenarios they care about
- Video review is often highly motivating for teens
- Let them choose the topic and format
- Peer practice: invite a trusted friend once/month
Co-occurring ADHD
- Very short sessions (10 minutes)
- High-energy game format (catch, movement-based)
- Frequent reinforcement: every exchange, not every few
- Allow movement during conversation
Co-occurring Anxiety
- Remove video recording entirely or indefinitely
- Use comfortable, familiar setting exclusively
- Lower threshold: 1 exchange per session = success in early weeks
- No timers; use visual count instead

In Weeks 1–2, You Are Building Awareness. Not Yet Skill.
15%
Awareness Phase
Weeks 1–2: Familiarity is the prerequisite of everything that follows.
What You May See — Real Progress, Even If It Doesn't Feel Like It
✅ Child tolerates talking stick without grabbing it back immediately
✅ Child acknowledges the conversation map and what it shows
✅ Child asks 1 prompted question (even with card)
✅ Monologue duration slightly shorter (even 30 seconds shorter is neural change)
✅ Child notices when they've been talking a while (even if they continue)
✅ Child sits for the full 15-minute session without escape attempts
What Is NOT Progress Yet (Do not expect in Weeks 1–2)
- ❌ Spontaneous turn-taking without tools
- ❌ Noticing listener boredom in natural conversation
- ❌ Asking questions without prompt
- ❌ Significant reduction in monologue frequency
"If your child tolerated the talking stick for 3 passes — that's real progress. If they asked one question from a card — that's neural pathway activation. If they sat through the session — you are building the habit that everything else depends on. Weeks 1–2 are not about skill. They are about familiarity. Familiarity is the prerequisite of everything."
Weeks 3–4: The Neural Pathway Is Forming. Watch for These Signs.
40%
Consolidation Phase
Weeks 3–4: The "neural pathway forming" signals most parents miss because they're looking for bigger changes.
Consolidation Indicators
Child Anticipates
✅ Child reaches for question card before being prompted — anticipating the activity.
Self-Correction Emerges
✅ Child pauses mid-monologue and self-corrects: "Oh — your turn."
Session Memory
✅ Child comments on a previous session: "Remember when I asked you about…?"
Real Life Reference
✅ Child references the conversation map in daily life: "We should use our talking stick!"
Fluid Handoffs
✅ Talking stick passes become more fluid — less friction at each handoff across all phases.
First Bridge Phrase
✅ Child uses one bridge phrase spontaneously — even once is a milestone worth celebrating.
"You may notice you're more confident too. You've learned to wait, to model, to reinforce at the right moment. Your own conversational patience has grown. That matters — because your patience is your child's scaffold."

Weeks 5–8: From Scaffolded Skill to Emerging Habit.
70%
Emergence Phase
Weeks 5–8: Skills are becoming habits. Scaffolds can begin to fade.
Mastery Emergence Indicators
✅ Child takes turns consistently across all three phases
✅ Child asks 2–3 spontaneous questions per session without card prompt
✅ Child uses bridge phrases without card reference ("That reminds me of…")
✅ Child notices obvious listener disengagement (boredom/confusion cues)
✅ Child adjusts topic when partner expresses interest in something different
✅ Session engagement level: consistently 4–5 / 5
Generalization Check at Week 6
Have a 5-minute casual dinner conversation with no materials. Count: spontaneous questions, pauses for partner, responses to what partner said. Compare to Week 1 baseline. Even 50% improvement = significant clinical progress.
When to Start Fading Scaffolds
- Remove question cards when child asks 2 spontaneous questions for 3 consecutive sessions
- Remove talking stick when child passes voluntarily for 5 consecutive exchanges
- Remove conversation map when child references it less than once per session
- Fade timer when turns are approximately equal without external measurement
Progress in Communication Is Progress in Belonging. Celebrate It Fully.
First Spontaneous Question
No card, no prompt. Celebration idea: Child picks dinner menu. Write it on the calendar: "The day [Name] asked their first real question."
First Time Noticing Listener Boredom
Celebration idea: Special dessert + tell the family: "Something amazing happened in conversation today."
First Natural Reciprocal Exchange
Without any tools — pure conversation. Celebration idea: Video record it (with permission). This is the moment to show at age 18.
3 Consecutive High-Quality Sessions
Celebration idea: Family outing of child's choice — they've earned it.
Friend Comments on Improvement
This is the real milestone. Generalization has occurred. Frame this on the wall. This is what it was all for.
"My son could talk for 45 minutes about trains without taking a breath. He never noticed when people walked away, never asked questions, never waited for responses. Last week, a classmate said, 'I like talking to your son now — he actually listens.' That's everything. He went from talking AT the world to talking WITH it." — Parent, Pinnacle Network
Illustrative case. Individual outcomes vary. Narrative represents composite experiences from Pinnacle families across India.

Home Intervention Has Boundaries. These Signs Mean It's Time for Clinical Support.
🚨 No progress after 8 weeks of consistent (3x+/week) home intervention
This suggests the intervention intensity or approach needs clinical calibration from a licensed SLP.
🚨 Child becomes significantly more distressed or anxious during/after sessions
Possible underlying anxiety, sensory sensitivity, or protocol modification needed — requires professional guidance.
🚨 Regression: Previously acquired skills disappearing
Rule out medical, environmental, or developmental changes requiring comprehensive assessment.
🚨 Child has never made eye contact or shown awareness of listener
Requires comprehensive social cognition assessment — theory of mind evaluation by a specialist.
🚨 Peer interactions completely absent or severely impaired
May indicate a broader social profile requiring multi-disciplinary assessment beyond home intervention.
🚨 School reporting significant impact on academic or social participation
IEP/IFSP goals may be indicated; school-based SLP referral recommended.
🚨 Family in crisis from communication challenges
Caregiver support is a clinical intervention. Pinnacle's family counseling services are available.
📞FREE National Autism Helpline: 9100 181 181
16+ languages | 24×7 | Available to all families navigating social communication challenges — diagnosis not required.
16+ languages | 24×7 | Available to all families navigating social communication challenges — diagnosis not required.
You Are Not Done. You Are on a Journey with a Clear Forward Path.
Every technique in Domain B builds on the one before it. B-207 is not an endpoint — it is the foundation for richer, more nuanced social communication skills that your child will develop in the months ahead.
B-208 Next If:
Listener awareness remains the primary gap — child still misses social cues in natural settings.
B-209 Next If:
Conversational breakdowns and misunderstandings are frequent — repair strategies needed.
B-210 Next If:
Dyadic skills are solid — ready to practice with a peer group setting.
Lateral options if B-207 isn't resonating after 8 weeks: B-212 Video Modeling Conversation Program (heavily video-based, different entry point) | B-220 Social Skills Group Protocol (peer-mediated approach).
Your Child's Conversation Skills Journey Doesn't End Here.
Every technique in Domain B: Social Communication shares materials, principles, and momentum. Here is where you can go next — and what you already own that will help you get there.
Technique | Code | Difficulty | Materials You Already Have? | |
Topic Maintenance Training | B-205 | 🟢 Intro | ✅ Yes — same materials | |
Literal Language Understanding | B-206 | 🟡 Core | Partial | |
Social Cue Recognition Training | B-208 | 🟡 Core | ✅ Yes — Listener Cue Cards | |
Conversational Repair Strategies | B-209 | 🔴 Advanced | Partial | |
Peer Conversation Skills | B-210 | 🔴 Advanced | ✅ Yes — Conversation Games | |
Greeting & Farewell Protocols | B-180 | 🟢 Intro | ✅ Yes — Question Cards |
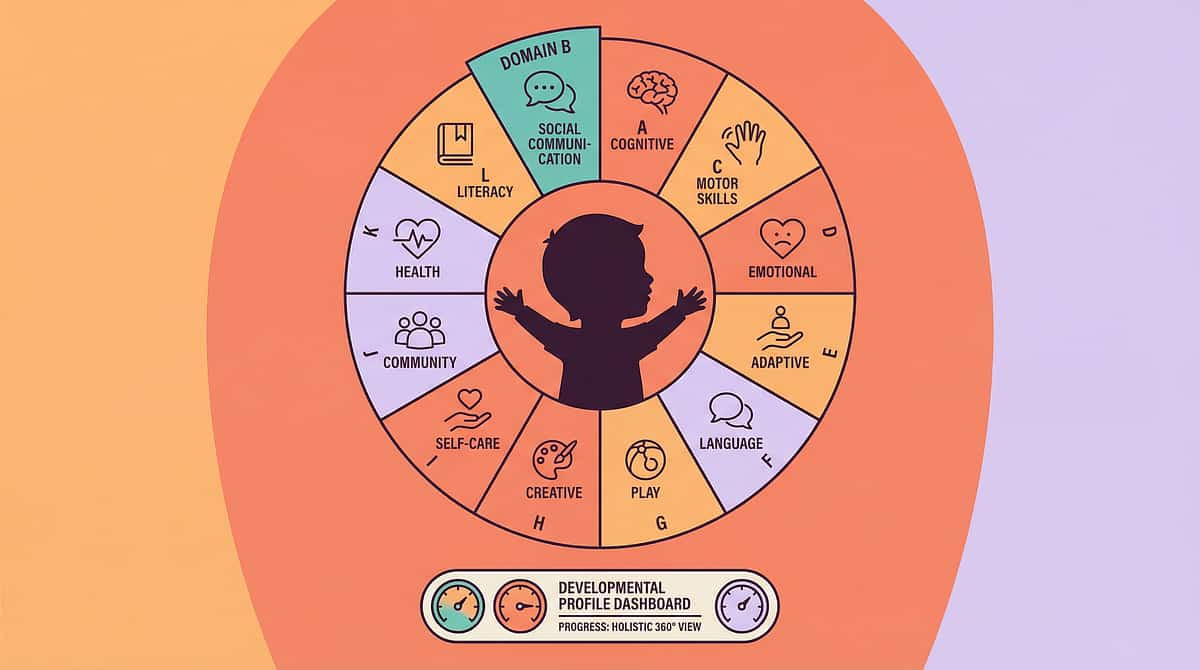
This Technique Is One Piece of a Larger Plan.
★ Currently Active Domain
B-207: Social Communication
Reciprocal Communication Training is your current focus within Domain B. The starred domain is where your child's greatest daily gains are happening right now.
Reciprocal Communication Training is your current focus within Domain B. The starred domain is where your child's greatest daily gains are happening right now.
WHO Nurturing Care Framework Alignment
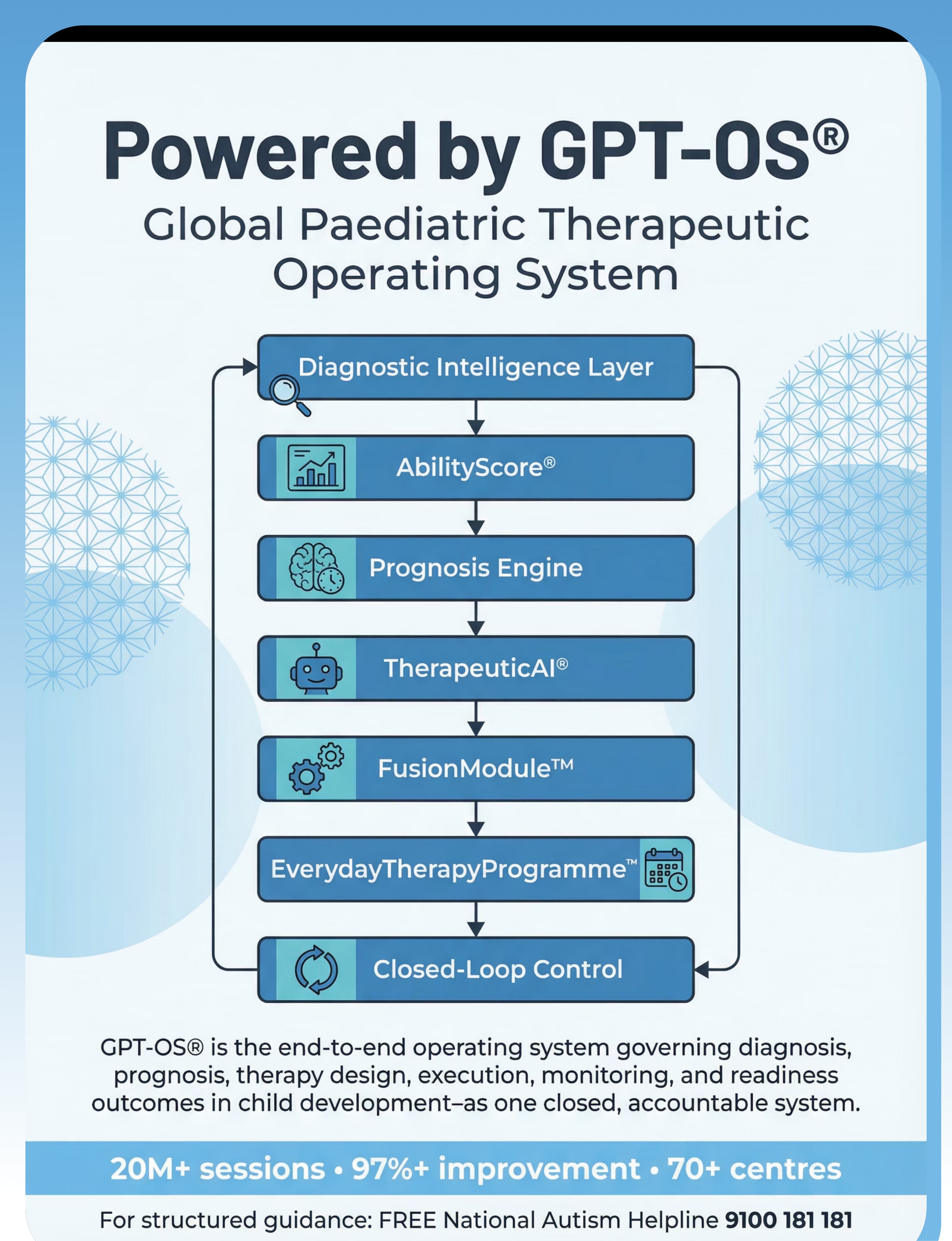
This technique directly serves the NCF component: Responsive Caregiving — sensitive, consistent caregiver-child interaction that builds communication, trust, and social cognition. GPT-OS® monitors all five NCF components: Health | Nutrition | Responsive Caregiving | Security/Safety | Early Learning.
"From 'He Just Doesn't Get It' to 'He Actually Listens Now.'"
The Before: Priya's son Arjun, age 9, Bengaluru. Every dinner table became a 45-minute lecture on cricket statistics. When cousins came over, Arjun would talk at them about Virat Kohli's batting average until they quietly disappeared into another room. He'd come to her confused — "Why didn't they want to play with me?" He had no idea his conversations were one-sided. He wasn't choosing it. He genuinely couldn't see it.
The Turning Point: Their Pinnacle SLP introduced the Conversation Map and the Talking Stick. At home, Priya started using the stick at dinner — not as a therapy exercise, but as a family ritual. The first week: Arjun grabbed it back every time. By week 3: he started passing it before being reminded. By week 5: he looked at her one evening and said, "Amma — you haven't talked yet. Here."
That was the moment.
Week 8. A cousin visits. Arjun asks: "What's your favorite part about your new school?" The cousin's face changes completely. A real conversation starts. It lasts 12 minutes. Both of them contribute. Both of them laugh.
"That question changed everything. He'd finally noticed that someone else had thoughts worth hearing."
Illustrative case. Individual outcomes vary. This narrative represents composite experiences from Pinnacle families across India.
You Don't Have to Navigate This Alone.
🇮🇳 Pinnacle Family Community
Connect with families across Pinnacle's 70+ center network navigating identical challenges. Moderated by licensed therapists. pinnacleblooms.org/community →
📱 WhatsApp Support Groups
Domain-specific groups: Social Communication families, ASD parent support, Teen social skills families. Request access: 9100 181 181
🌐 Global Parent Networks
Autism Society of India: autismsocietyindia.org
ASHA Parent Resources: asha.org/public
Autism Science Foundation: autismsciencefoundation.org
ASHA Parent Resources: asha.org/public
Autism Science Foundation: autismsciencefoundation.org
📺 Pinnacle Reels Community
Follow @PinnacleBlooms for daily parent-education reels across all 12 developmental domains. 1,000+ technique-specific reels published. B-207 Reel: "Monologue, Not Dialogue."
💬 Peer Parent Mentoring
Experienced Pinnacle parents available for 1:1 mentoring. Connect through your nearest Pinnacle center or helpline: 9100 181 181
Consistency Across Caregivers: A child who practices 20 minutes daily at home makes 7x more progress than one who only receives clinic sessions. If only one parent practices and the other doesn't, impact is halved. Share this page.
Home Intervention Is Powerful. Professional Assessment Makes It Precise.
Speech-Language Pathologist (SLP) — Primary
Pragmatic language evaluation, Social Communication Readiness Index assessment, structured intervention programming, generalization planning, caregiver coaching. Recommended: Full evaluation before beginning home intervention for best results.
NeuroDevelopmental Pediatrician
Social cognition profile assessment, autism/SPCD/ADHD diagnostic clarity, medical co-occurrences, medication considerations if indicated.
Psychologist / Child Psychiatrist
Theory of mind evaluation, social anxiety assessment, family systems support, cognitive-behavioral strategies for self-awareness development.
Special Educator
School-based implementation, IEP goal development, peer interaction facilitation, classroom social communication supports.
BCBA / ABA Therapist
Behavioral intervention design, reinforcement scheduling, discrete trial training for specific components, generalization programming.
How to Access Pinnacle Services
Call FREE Helpline: 9100 181 181 (16+ languages, 24x7) — assessment intake, no appointment needed
Request AbilityScore® Evaluation — establishes baseline across all 12 domains
GPT-OS® Personalized Plan — FusionModule™ coordinates all disciplines simultaneously
EverydayTherapyProgramme™ — home protocol designed specifically for your child
The Science Behind What You're Doing. For the Curious Parent.
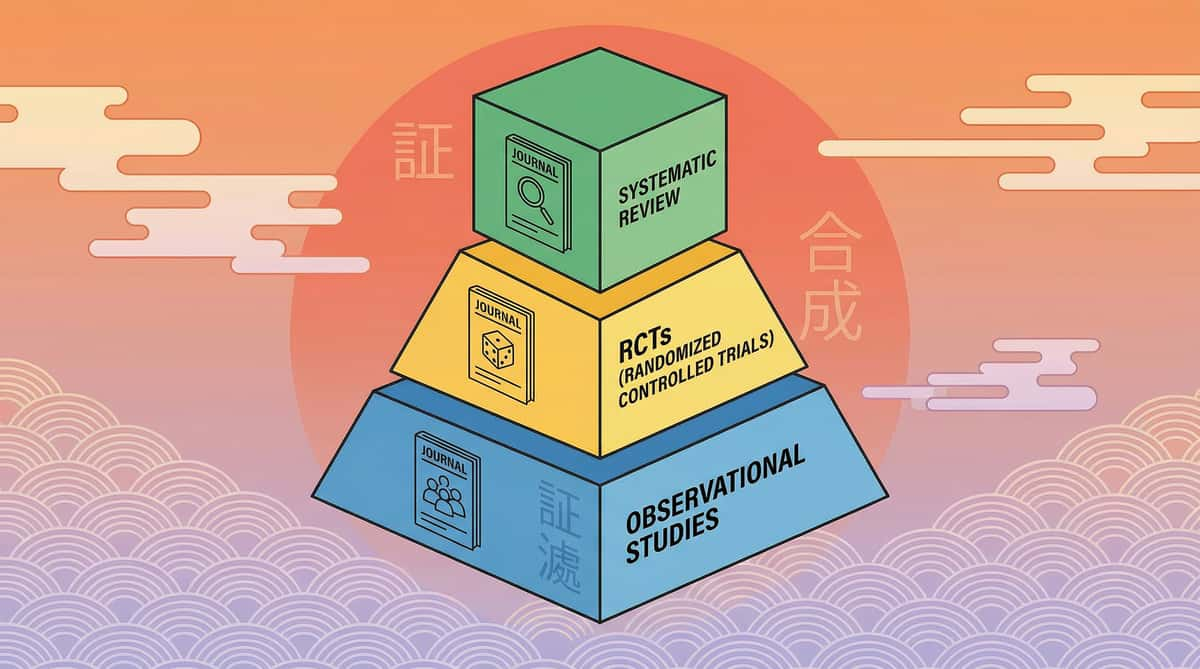
Evidence Pyramid
Level I — Systematic Reviews (Highest confidence)
Level II — Randomized Controlled Trials
Level III — Cohort Studies
Level IV — Case Studies
Level II — Randomized Controlled Trials
Level III — Cohort Studies
Level IV — Case Studies
B-207 is supported by Level I and Level II evidence — the strongest available in clinical science.
Key Studies for B-207
- PMC11506176 — PRISMA Systematic Review (2024): 16 articles confirming pragmatic language interventions are evidence-based practices for ASD. → PubMed
- PMC10955541 — Meta-Analysis World J Clin Cases (2024): 24 studies: social communication intervention effectively promotes social skills and peer interaction. → PubMed
- Padmanabha et al. 2019 — Indian RCT demonstrating home-based communication interventions show significant outcomes. → DOI
- NCAEP 2020 — Social Narratives + Visual Supports: confirmed evidence-based practices. → ncaep.fpg.unc.edu
- Frontiers in Integrative Neuroscience 2020 — Neurological framework for social communication differences in ASD. → DOI
- ASHA Practice Portal — Comprehensive clinical evidence for pragmatic language intervention. → asha.org
- WHO Nurturing Care Framework 2018 — Global evidence-base for caregiver-mediated responsive communication. → nurturing-care.org
Your Data Helps Your Child. And Every Child Like Yours.
What GPT-OS® Learns from B-207 Data
- Rate of talking stick adoption (proprioceptive vs. conceptual learning profile)
- Question frequency progression (theory of mind development rate)
- Listener cue recognition threshold (social cognition ceiling)
- Bridge phrase spontaneity timeline (language automatization rate)
- Session tolerance (regulatory profile interaction with social demand)
🔒 Privacy Assurance
Pinnacle operates under ISO/IEC 27001 (Information Security) and India's IT Act. Your child's data is never sold, never shared with third parties, and used exclusively for clinical improvement of their own pathway and anonymized population-level research.
"Your 60 seconds of daily data contributes to the largest pediatric social communication dataset in India. The insights generated help calibrate interventions for every child in the Pinnacle network. Your child's journey helps build the map for every family who comes after."
See the Materials in Action. Watch Once, Know What to Do.
🎬B-207: "9 Materials That Help When Child Talks At Not With"
Series: Social Communication & Pragmatic Language Solutions | Episode 207 | Duration: ~75 seconds
Series: Social Communication & Pragmatic Language Solutions | Episode 207 | Duration: ~75 seconds
This reel walks you through all 9 materials in 75 seconds — a therapist introduction, each material named with its one-line function, and a closing visual of what genuine reciprocal conversation looks like. Watch it before your first session. Share it with your child's school. Send it to grandparents.
Why Video Modeling Works
Research from NCAEP (2020) classifies video modeling as an evidence-based practice for autism. Seeing a skilled adult demonstrate correct technique creates neural priming that purely text-based learning cannot match. The combination of this page (text + protocol) + the Reel (visual demonstration) is a more powerful learning package than either alone.
Series Navigation
← B-206: "When Your Child Takes Words Too Literally"
→ B-208: "When Your Child Misses Social Cues"
Consistency Across Caregivers Multiplies Impact. This Page Is Shareable.
For Your Spouse / Partner
"Read this page — it's the protocol we're using for [Name]'s conversation skills. The most important part: we both need to use the talking stick at dinner. Takes 10 minutes. Big difference."
For Grandparents (Simplified)
"[Name] is learning to take turns in conversation. When [he/she] starts talking a lot about one topic — please wait, then ask a question about something YOU care about, then pass it back. A 'talking stick' helps. Ask us to show you."
For School Teachers
"[Child's name] is working on reciprocal conversation skills. In class discussions, [he/she] may need a visual cue when it's time to listen vs. speak. A question card on their desk helps prompt curiosity about classmates' ideas. We're happy to share materials."
For Other Family Members
"We're working on teaching [Name] that conversation goes both ways. The most helpful thing you can do: ask [him/her] questions AND wait for their question back before answering yours. It teaches reciprocity through modeling."
📊Caregiver Consistency Data: Children who receive consistent implementation across 3+ caregivers show 3x faster generalization than children with single-caregiver implementation. — WHO CCD Package Implementation Data (PMC9978394)

Questions Real Parents Ask. Answers from the Consortium.
Q1: My child is verbal and intelligent — can they really not understand turn-taking?
Yes, absolutely. Verbal ability and social cognition are processed by different brain networks. A child can have a vocabulary of 10,000 words and still have genuine difficulty with the social architecture of conversation. Intelligence does not inoculate against pragmatic language differences. In fact, highly verbal children often show more prominent one-sided conversation patterns precisely because they have so much to say.
Q2: We've tried telling him to let others talk. Nothing changes. Why?
Because instruction without skill-building doesn't work. Telling a child to "let others talk" is like telling them to "just read" without teaching phonics. The skill of noticing listener cues, pausing, asking questions, and building on others' comments requires explicit teaching, structured practice, and reinforcement — not just instruction. That's what this technique provides.
Q3: How long will we need to do this intervention?
Most families see meaningful change by 8–12 weeks with consistent home practice (3–5 sessions/week). Full naturalization — where reciprocal skills are automatic without tools — typically takes 4–6 months. Skills gained are generally maintained with periodic reinforcement practice.
Q4: My daughter is 12 — is it too late?
No. Pragmatic language intervention has been shown effective through adolescence and even into adulthood. The approach modifies slightly for teens — less game-based, more real-scenario practice, peer involvement — but the core principles apply. Earlier is always better, but 12 is not too late.
Q5: Should I tell my child this is "therapy"?
This depends on your child's age and self-awareness. For younger children (4–8): framing as "our special talking game" is usually better. For older children (9–14): many respond well to "this is a social intelligence skill that lots of people work on." Avoid any framing that implies they are doing something wrong. They are learning something new.
Q6: What if only one parent can do the sessions?
One committed parent + consistent home practice = significant progress. The ideal is 3+ caregivers. But one person doing it consistently beats two people doing it inconsistently every time.
Q7: My child has an active IEP/IFSP — should the school be doing this?
Yes, ideally. Social communication goals are frequently included in IEPs for children with ASD, SPCD, or related diagnoses. Share this page with your child's school SLP. Consistency between home and school is more powerful than either alone.
Q8: What is the difference between this and "social skills groups"?
Social skills groups provide peer practice in a supported setting — valuable for generalization. B-207 is individual home practice that builds the foundational skills children need before peer practice is productive. Sequence: individual B-207 skills first → then peer practice in groups. Many children who fail social skills groups haven't yet built the individual reciprocity foundation.
You Understand the Science. You Have the Materials. You Know the Protocol.
You arrived on this page searching for help. You have now read 40 cards of evidence-based guidance from India's largest pediatric therapy consortium — built from 20 million therapy sessions, 97%+ measured improvement, and the wisdom of thousands of families who walked this path before you.
The only thing left is to begin.
Begin with the DIY materials you can make in 15 minutes. No purchase required.
Speak with a licensed SLP. First assessment available within 48 hours at any of 70+ centers. Free, 24x7, 16+ languages.
🏆Validated by the Pinnacle Blooms Consortium
🗣️ SLP • 🧩 ABA • 🧠 NeuroDev • 📚 SpEd • 👨👩👧 Family • 🔬 CRO
"From fear to mastery. One technique at a time."
🗣️ SLP • 🧩 ABA • 🧠 NeuroDev • 📚 SpEd • 👨👩👧 Family • 🔬 CRO
"From fear to mastery. One technique at a time."
Preview of 9 materials that help when child talks at not with Therapy Material
Below is a visual preview of 9 materials that help when child talks at not with therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.







Link copied!

The Pinnacle Promise
"From fear to mastery. One technique at a time."
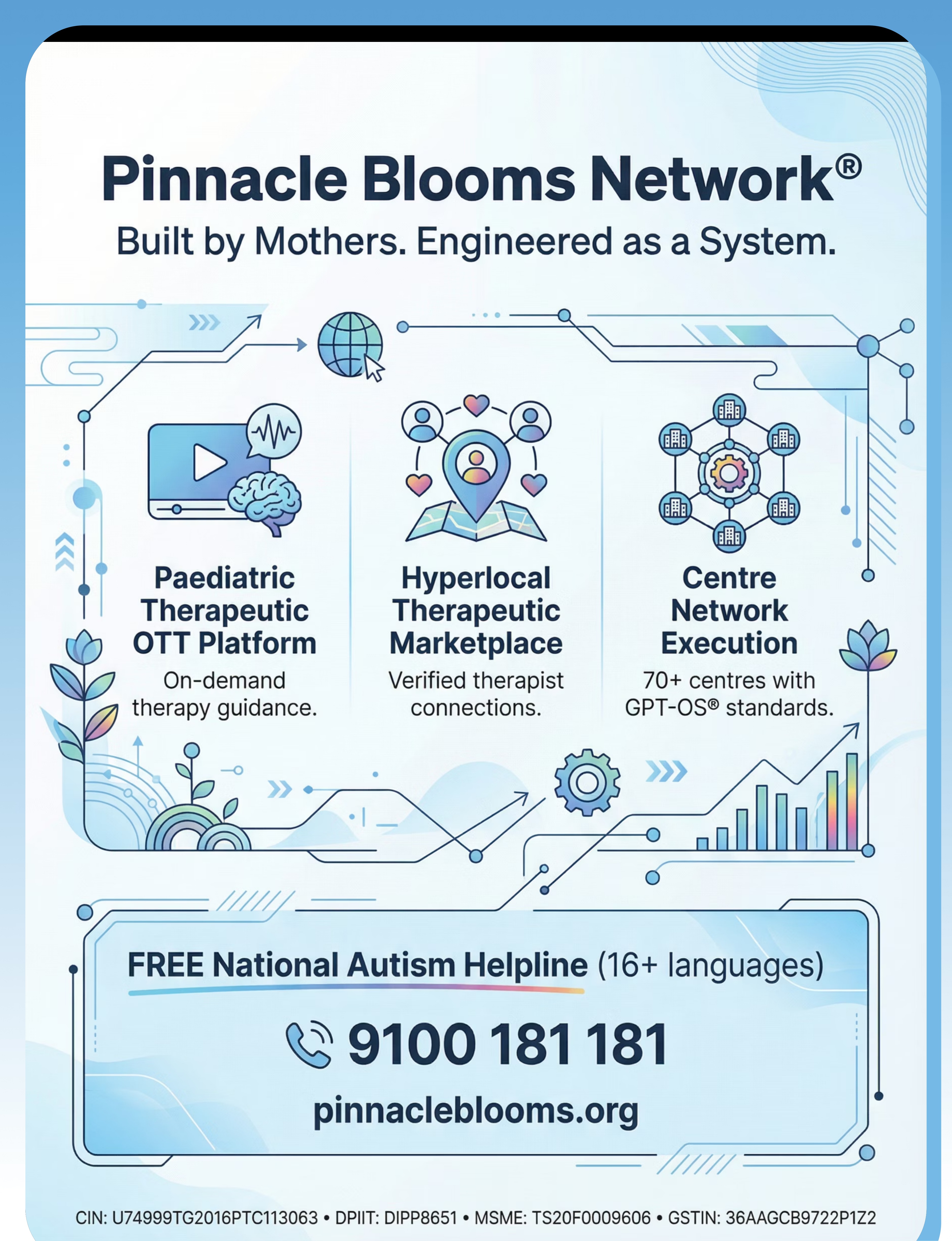
Pinnacle Blooms Network® is built by mothers, engineered as a system, and calibrated by the largest pediatric therapy data infrastructure in India. Every technique on this platform emerges from clinical practice across 70+ centers, 20M+ individual therapy sessions, and the daily lived experience of families navigating neurodevelopmental differences.
We believe every child deserves a home that functions as a 24×7, personalized, multi-sensory, evidence-based therapy environment. We believe every parent has the capacity to be their child's most powerful intervention partner. And we believe no family should navigate this alone. That is the Pinnacle Promise.
Clinical Disclaimer: This content is educational. It does not replace assessment by a licensed speech-language pathologist or healthcare provider. Significant or persistent social communication difficulties should be evaluated comprehensively. Individual results may vary. Statistics represent aggregate outcomes across the Pinnacle Blooms Network.
Statutory Identifiers
CIN: U74999TG2016PTC113063
DPIIT: DIPP8651 (Govt. of India)
MSME: Udyog Aadhaar TS20F0009606
GSTIN: 36AAGCB9722P1Z2
DPIIT: DIPP8651 (Govt. of India)
MSME: Udyog Aadhaar TS20F0009606
GSTIN: 36AAGCB9722P1Z2
Quality Standards
ISO 13485: Medical Device QMS
ISO/IEC 27001: Information Security
ISO/IEC 27001: Information Security
Proprietary Technology
GPT-OS® | AbilityScore® | TherapeuticAI® | FusionModule™ | EverydayTherapyProgramme™ are proprietary IP of Bharath Healthcare Laboratories Pvt. Ltd.
© 2025 Pinnacle Blooms Network®, unit of Bharath Healthcare Laboratories Pvt. Ltd. All rights reserved. | techniques.pinnacleblooms.org/social-communication/reciprocal-communication-b207