"One moment she's there — present, engaged, laughing at something her brother said. Then she's gone. Her eyes go flat, like someone pulled a curtain behind them. Her body goes still. Not tense. Empty. She stops responding to her name. To questions. To anything. I sit with her and I talk to her, softly, telling her I'm here, telling her she's safe. I don't know if she can hear me. I don't know if I'm helping or making it worse. How do I reach a child who has disappeared inside herself?" — Parent, Pinnacle Network

- Heart rate slows
- Sensory processing dampens
- Prefrontal cortex goes offline (no reasoning, no language)
- Metabolism shifts to conservation mode
- The body goes still — exactly like an animal "playing dead"
"This is a wiring difference, not a behaviour problem."


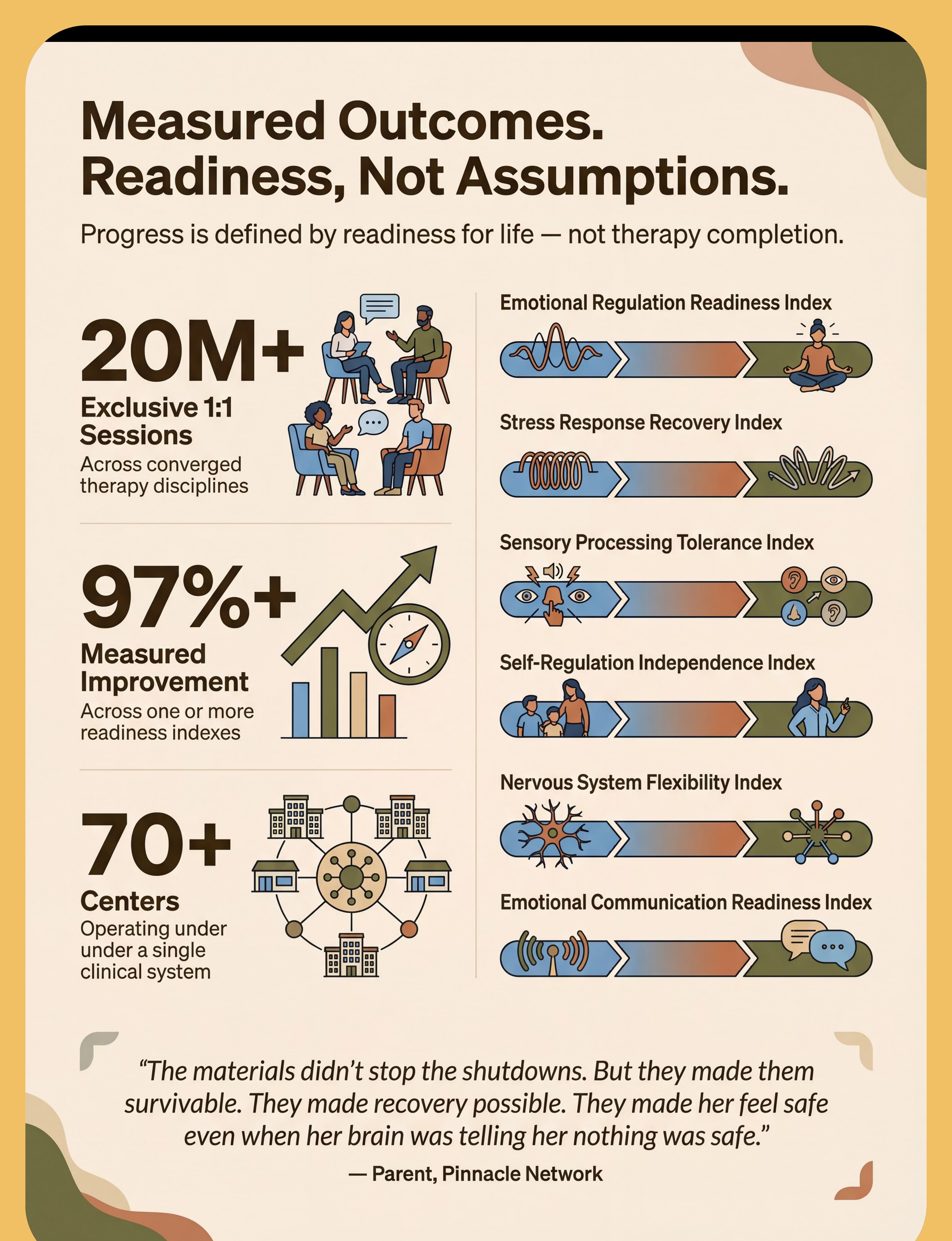
- Emotional Regulation Readiness Index
- Stress Response Recovery Index
- Self-Regulation Independence Index
- Nervous System Flexibility Index





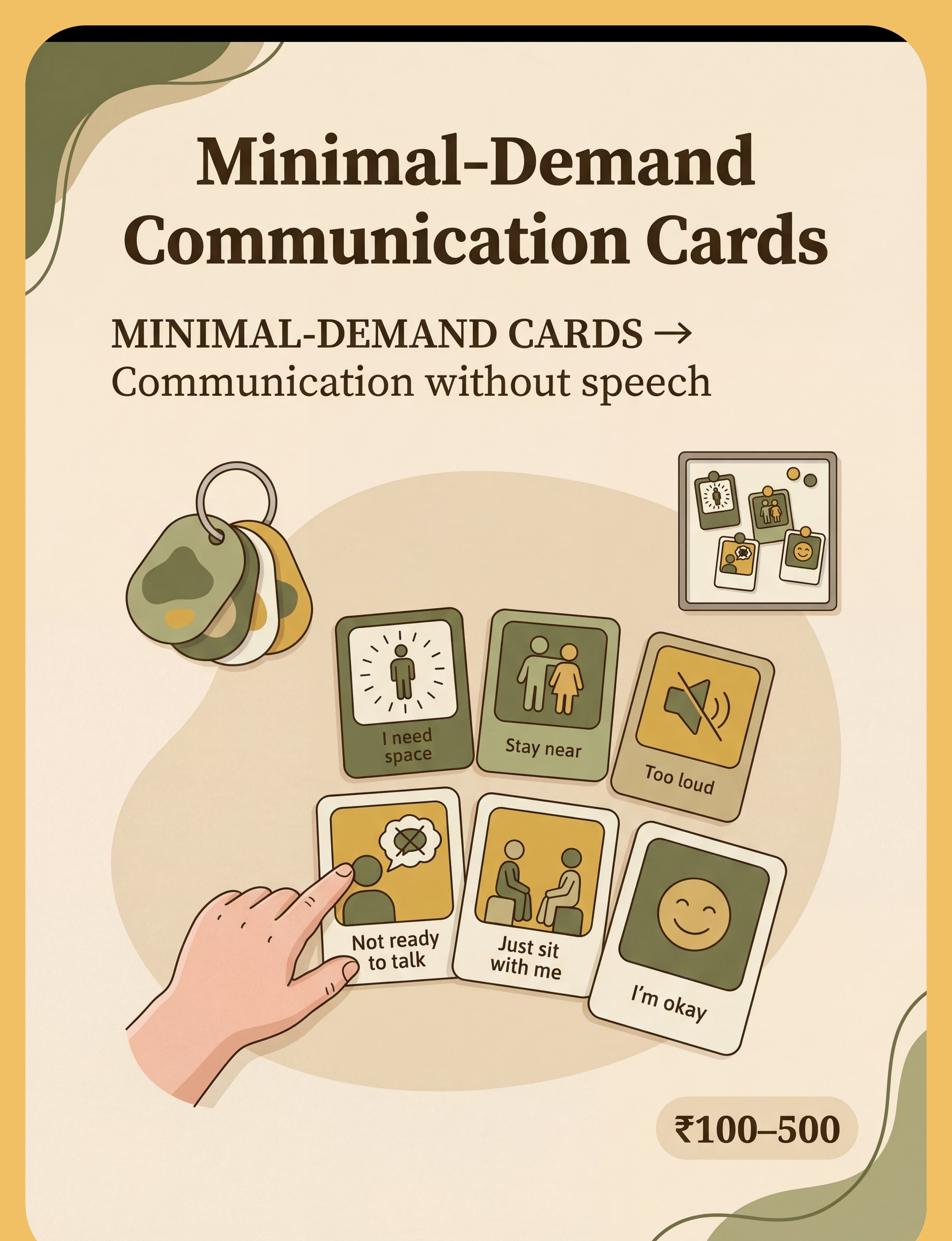
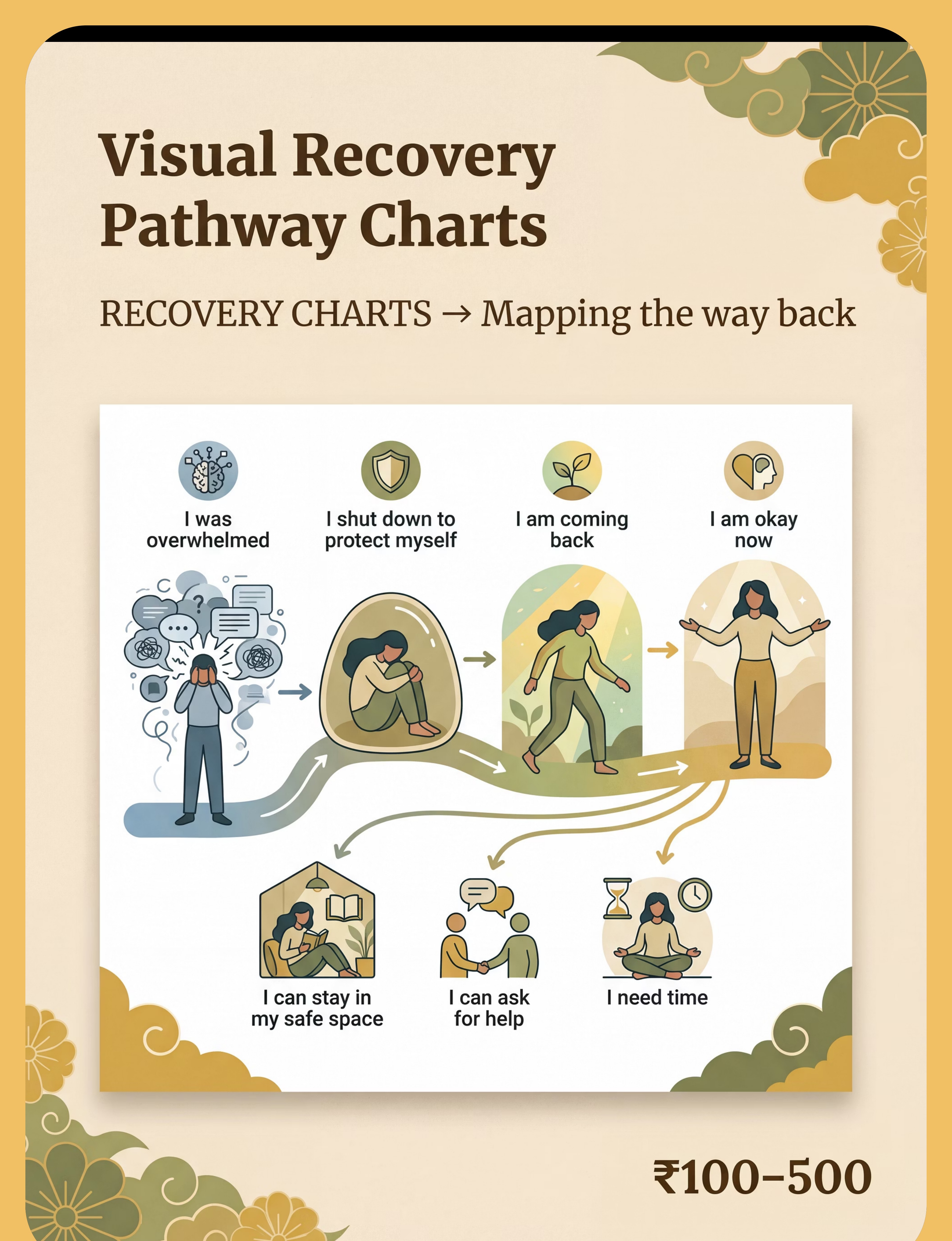
- "I'm okay"
- "I need space"
- "Stay near"
- "Too loud"
- "Water"
- "Not ready to talk"
- "Just sit with me"




🛒 Commercial Option | 🏠 DIY / Zero-Cost Alternative | |
Weighted blanket ₹1,500–8,000 | Layer 3–5 regular blankets; sew rice/bean pockets into fabric. Aim for ~10% body weight. | |
Noise-cancelling headphones ₹2,000–5,000 | Industrial ear defenders (construction/shooting range): ₹200–400 at hardware stores | |
Privacy tent ₹1,000–3,000 | Large cardboard box + cushions; table + draped blankets; corner with hung sari/dupatta | |
Light-filtering glasses ₹500–2,000 | Child's sunglasses; pull shades down; drape a light cloth over eyes | |
Laminated comm cards ₹200–500 | Paper cards in ziplock bag; drawn by parent; icons from Google Images + printed | |
Temperature tools ₹300–1,500 | Rice sock (microwave); wet cloth from fridge; warm water bottle wrapped in cloth | |
Sensory tent ₹2,000–6,000 | Old mosquito net hung in corner; bedsheet draped over chair backs | |
Water bottle with straw ₹100–300 | Any cup with straw; squeeze bottle | |
Recovery pathway chart ₹200–500 | Hand-drawn on paper with child; photos of child + arrow drawings; 5 images laminated |

- Child shows ANY new neurological symptoms (convulsive movements, incontinence, significant change in breathing) → Seek immediate medical evaluation
- Child is deeply unresponsive and cannot remove materials independently → Do NOT apply weighted items; do NOT put food near mouth (aspiration risk)
- Child shows distress signals while any material is applied → Remove immediately, no questions
- Enclosed space is locked, latched, or has inadequate ventilation → Never use; redesign before use
- Parent is in emotional dysregulation → Regulate YOURSELF first
- Weighted materials: Weight ≈ 10% body weight. NEVER exceed 15%
- Heat tools: Always test temperature. Never leave electric heating unattended
- Enclosed spaces: Child must always be able to exit independently
- Communication cards: Available, NEVER demanded
- Water/snacks: Position, do not offer. Do not place near mouth
- All materials introduced to child BEFORE an episode during a calm regulated period
- Child's preferences for each material are known
- Safe space established — child knows it's theirs and has been in it calmly
- All caregivers understand that shutdown is not behaviour
- Emergency contact (9100 181 181) saved in all caregivers' phones
- Safe space is set up and child knows it's theirs
- All 9 materials are in place and accessible
- Child has been in the safe space during calm times (not just during shutdown)
- Communication cards made WITH the child and known to them
- Recovery pathway chart created WITH child and displayed in space
- All regular caregivers briefed: shutdown = nervous system event, not behaviour
- Parent has practised own regulation during a non-crisis moment

"I'm here. You're safe. I'm not going anywhere. Take all the time you need."
- Move slowly and without urgency
- Position at an angle — not directly in front (less confrontational)
- Sit DOWN — lower eye level reduces perceived social demand
- Do not touch unless child initiates
- If child allows touch: firm, steady hold — not light stroking
- "What happened?" — cognitive demand
- "Can you tell me what's wrong?" — language demand
- "Look at me." — sensory/social demand
- "You're okay!" — contradicts their experience
- Any question at all — questions are demands

Offer the Materials — The Deployment Protocol
Step 3 of 6 Weighted Blanket Unfold near child. Do not drape on them unless invited or known preference. The option should be visible and within reach. Comfort Object Place near child's hand. Do not put in their hands unless they reach. Communication Cards Lay the keyring/board within visual range. No instruction. No invitation. No expectation. Water Bottle Place on floor within arm's reach. Straw forward. No "do you want?" — just present. Simple Snack Small bowl nearby. Available, not offered. No language attached. Temperature Item Warm blanket unfolded and available. Cool cloth placed nearby. After materials are placed: STEP BACK. Sit. Do not hover. Look nearby but not directly at the child. Being watched is a social processing demand. Reduce it. 🟢 Ideal Child moves to safe space, uses one or more materials, shows gradual softening in body posture 🟡 Acceptable Child stays where they are, no materials used, but sensory environment is modified and caregiver is calm and present 🔴 Concerning Child shows new physical symptoms, increased distress, or difficulty breathing → medical assessment required

"Waiting without demanding is active support. I am doing something by doing nothing. My presence communicates safety. My calmness is the therapy."
- Seated nearby (1.5–2m, in child's peripheral vision)
- Calm regulated breathing, relaxed posture, hands unclenched
- Available — if child reaches for you, respond immediately
- Silent — no commentary, no checking in, no narration
- Watching lightly — not staring, not looking away completely
- Slight shift in body posture
- Eyes begin to focus rather than glaze
- Small physical movements (fingers, toes)
- Reaching for water or comfort object
- Micro-expressions appearing on face
- Using a communication card
- "You're back! I was so worried!" → Emotional intensity adds demand
- "Do you want to tell me what happened?" → Processing demand too soon
- "See? You're okay!" → Invalidates the experience
- Big hug the moment they surface → Follow their lead only
- Keep environment unchanged (dim, quiet, contained)
- No demands whatsoever
- Offer water and simple food
- Stay nearby but not intrusive
- "We don't have anywhere to be. Rest."
- Gradual environmental brightening IF child tolerates
- Low-demand activities available
- 1–2 gentle, warm interactions — no processing questions
- Protect from school return, homework, sibling interaction
- If child wants to talk, let them lead
- "Sometimes your brain needs to rest from too much. That's okay. You're okay."
- Track what preceded it — without interrogating the child
Location: Home / School / Community / Car / Other
Preceding signs visible? Y/N | Severity (1–5): ___
Most helpful: ___ | Least helpful: ___ | Recovery quality (1–5): ___
- Patterns across 10+ episodes identify trigger clusters → preventable load
- Materials effectiveness data → personalises your protocol
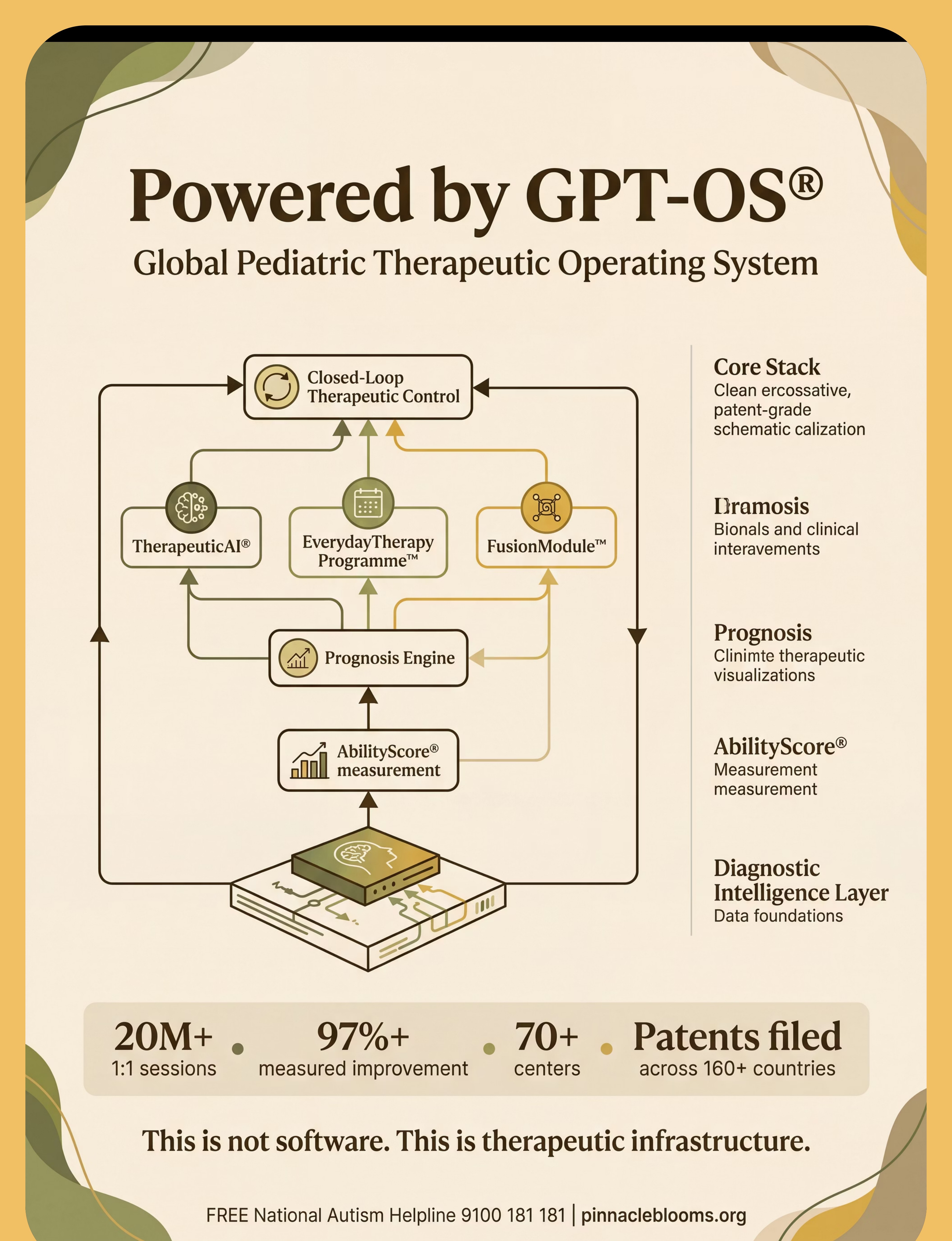
- GPT-OS® AbilityScore® tracks Stress Response Recovery Index over time
- At Pinnacle centres, this data informs FusionModule™ cross-disciplinary planning


- Weighted blanket: Use lighter weight or skip; heavy pressure may dysregulate
- Enclosed space: Keep fully open (tent with sides up, not closed)
- Touch: Minimal. Firm if offered; never light stroking
- Light: Go dimmer — consider blackout
- Sound: Go quieter — noise-cancelling, not just reducing
- Weighted blanket: Heavier weight often better; more proprioceptive input preferred
- Enclosed space: Tighter enclosure may be more regulating
- Rhythmic movement (rocking, swinging) during recovery may help
- Some predictable white noise may be preferred to complete silence
Age Group | Primary Approach | Key Notes | |
Ages 2–4 | Physical comfort primary; parent holding if tolerated; familiar objects essential | Recovery faster with close presence; safe space builds familiarity | |
Ages 5–10 | Safe space + materials; can begin using comm cards; visual chart becomes useful | Beginning self-direction; child involvement in designing protocol increases ownership | |
Ages 11–18 | Privacy CRITICAL; may resist being "managed"; peer awareness (school context) | Include them fully in protocol design; self-advocacy becomes the goal |
- Child has visited safe space during a non-crisis moment
- Child has touched or engaged with at least one material voluntarily
- Communication cards have been made WITH the child
- All household caregivers have been briefed
- First shutdown episode WITH the space available has occurred (data collected)
- Parent has stayed regulated during one shutdown — huge milestone
- Shutdown stopping completely (may still happen identically)
- Child independently using materials during shutdown
- Communication during shutdown (this comes much later)
- Shorter episodes necessarily (environment effect takes time to register as "safe")
- Child MOVES TOWARD safe space during a shutdown (instead of away or random)
- Child picks up comfort object during or immediately after shutdown
- Shutdown duration begins to shorten in familiar home environment
- Child's body posture shifts faster from rigid/still to relaxed within safe space
- Parent's protocol begins to feel automatic (not effortful)
- Siblings and other caregivers begin to respond appropriately without prompting

"The materials didn't stop the shutdowns. But they made them survivable. They made recovery possible. They made her feel safe even when her brain was telling her nothing was safe." — Parent, Pinnacle Network




Preview of 9 materials that help when child shuts down Therapy Material
Below is a visual preview of 9 materials that help when child shuts down therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.