
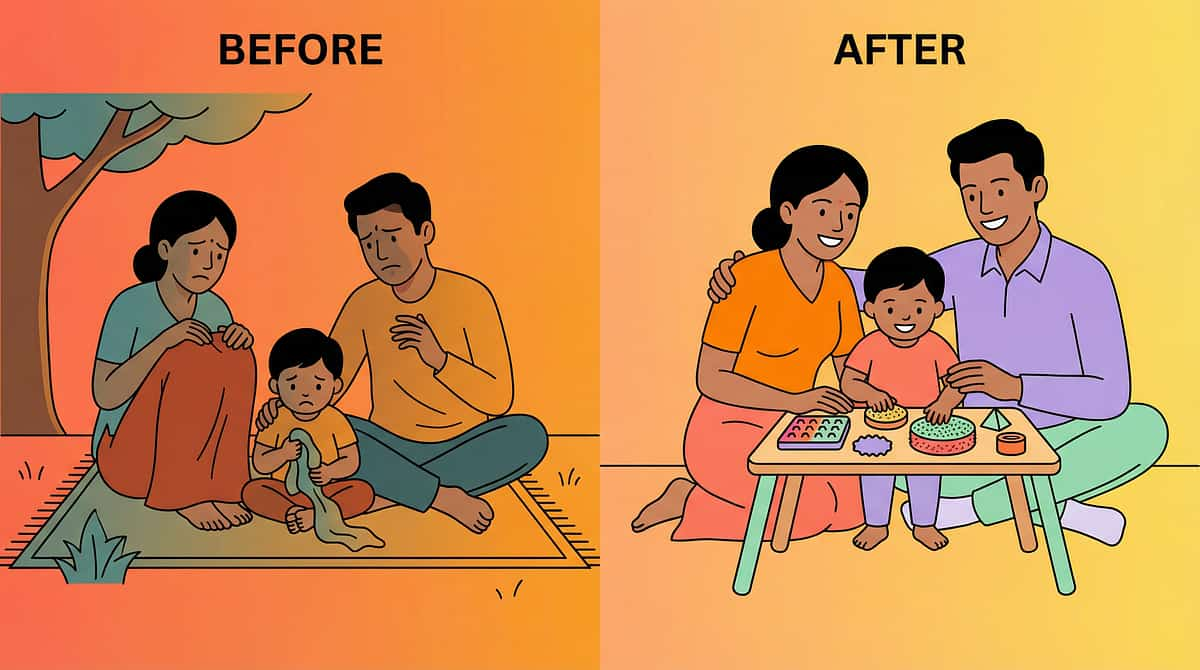
She carries everything. He never stops crashing. Their body is telling you something.
It's 7:30 AM and he's already moved the dining chairs twice — not because he's angry, but because he needed to push them. She insists on carrying every single grocery bag from the car — all at once, arms shaking — and when you try to take one, she has a meltdown. He crashes onto the couch like he's tackling a wrestling opponent, then looks up calm and regulated.
You are not failing. Your child's nervous system is speaking — loudly, persistently, and with great urgency. And today, you're going to understand exactly what it's saying.
A-106
Domain A: Sensory
Ages 3–12
Home Applicable
A-106 | 9 Materials That Help When Child Seeks Heavy Lifting
Proprioceptive Seeking — Sensory Regulation | Domain A | Ages 3–12
Proprioceptive Seeking — Sensory Regulation | Domain A | Ages 3–12

You are not the only parent Googling "why does my child crash into everything" at midnight.
The house is finally quiet, but your mind is racing. You’re sitting in the glow of your phone at 2:00 AM, deep in the rabbit hole of forums, parenting blogs, and YouTube videos. You've asked the questions that keep you awake: Why won’t the usual advice work for them? Is this my fault? Why does a simple trip to the store feel like navigating a storm? You feel like you're searching for a missing piece of a puzzle, desperate to help your child find the peace they can't seem to access.
Please, take a breath. You are doing an incredible job, and you are not alone in this search.
Is this my fault?
Why won't the usual parenting advice work?
Am I missing something the therapist isn't telling me?
Will my child ever feel calm in their own body?
Everything you have been experiencing—the crashes, the intensity, the confusion—has a name, a cause, and, most importantly, a path forward. Your child is speaking to you through their behavior, and you have finally found the place where that language is understood. Relief is not just a hope; it is within your reach.
A-106
Domain A: Sensory
Ages 3–12
Home Applicable

This is not disobedience. This is a wiring difference.
The Proprioceptive System — Your Child's Hidden Sixth Sense
Proprioception is the body's internal GPS — a continuous stream of signals from nerve endings called mechanoreceptors, embedded in every muscle, tendon, and joint capsule in your child's body. Every time your child pushes against a wall, carries a heavy bag, or crashes into a cushion, these mechanoreceptors fire electrical signals up the spinal cord to the brain. Under typical conditions, this system runs quietly in the background, keeping the body regulated, calm, and ready to learn.
What Goes Different in a Proprioceptive-Seeking Brain
In children with proprioceptive under-responsivity, the mechanoreceptor signals arrive at the brain's somatosensory cortex at lower-than-typical amplitude. The brain receives the signal — but it doesn't register with enough intensity to trigger the regulatory response the nervous system needs. The result: the child's arousal system stays dysregulated. Their reticular activating system (RAS) — the brain's on/off switch for alertness — stays stuck in a high-alert state. The child cannot self-calm through ordinary movement. They need more. Much more.
The Four Brain Regions Driving the Seeking Behavior
- Somatosensory Cortex (parietal lobe) — receives and maps proprioceptive input; under-responsive in heavy-work seekers
- Cerebellum — coordinates movement, balance, and motor planning; relies on proprioceptive feedback to function
- Reticular Activating System (brainstem) — regulates arousal, attention, and alertness; dysregulated when proprioceptive input is insufficient
- Insular Cortex — integrates body-state signals with emotional regulation; directly linked to meltdown thresholds
The Bathtub That Won't Stay Full
Here is the clearest way to understand your child's nervous system. Imagine a bathtub with a drain that runs 3× faster than normal. Every movement your child makes — walking to school, sitting at a desk, eating lunch — adds a little water. But for your child's brain, the drain empties it almost as fast as it fills. By mid-morning, the tub is nearly empty. The nervous system is running on fumes.
So the brain does the only logical thing: it sends an urgent signal. SEEK. CRASH. PUSH. CARRY. SQUEEZE. These are not tantrums. These are not attention-seeking. These are a nervous system placing an emergency order for the one input that fills the tub fast — deep proprioceptive pressure. When your child finally crashes into the sofa, carries the heavy laundry basket, or pushes against the wall, the tub fills. The RAS calms. The insular cortex settles. The child can breathe. Think. Connect.
This is why the technique in this guide works. It doesn't suppress the seeking behavior. It satisfies the neurological need that drives it — predictably, safely, and in a way that builds the brain's own regulatory capacity over time.
This is not a behavior to stop. This is a hunger to feed — safely and purposefully.
Frontiers in Integrative Neuroscience (2020): Comprehensive framework for evaluating sensory integration treatment in ASD establishes neurological basis for proprioceptive-based interventions. DOI: 10.3389/fnint.2020.556660

Your child is here. Here is where we're heading.
1
Ages 3–5: Emergence
Proprioceptive seeking intensifies as children enter environments requiring stillness (preschool, mealtimes). Seeking behaviors are at their most urgent and least socially navigable.
2
Ages 5–8: Peak Challenge ◄ YOUR CHILD
School demands seat-based learning. The seeking need doesn't decrease — but the acceptable outlets do. This is when families most often seek help. This technique is precisely designed for this window.
3
Ages 8–12: Channeling Phase
With consistent intervention and sensory diet, children begin to recognize their own seeking cues and navigate to appropriate outlets independently.
4
Adolescence → Adulthood
With proper support, most heavy-work seekers develop effective self-regulation strategies and channel proprioceptive needs into sports, fitness, manual work, and other socially valued activities.
Comorbidity Awareness: Proprioceptive seeking commonly co-occurs with ASD (80%), ADHD (60–70%), Sensory Processing Disorder (primary presentation), Developmental Coordination Disorder, and Anxiety where seeking serves as a coping mechanism.
Clinically validated. Home-applicable. Parent-proven.
Key Research Findings
Sensory Integration Works
PRISMA systematic review (Children, 2024): 16 studies confirm sensory integration intervention meets evidence-based practice criteria across sensory, behavioral, and regulatory outcomes. PMC11506176
Proprioceptive Input Reduces Seeking
Meta-analysis (World J Clin Cases, 2024): Across 24 studies, sensory integration therapy promoted social skills, adaptive behavior, and gross/fine motor skills. PMC10955541
Home-Based Delivery Works
Indian RCT (Padmanabha et al., 2019): Home-based sensory interventions administered by trained parents demonstrated significant measurable outcomes in Indian pediatric population. DOI: 10.1007/s12098-018-2747-4
"You are not experimenting on your child. You are implementing a technique backed by the same evidence that governs therapy in Pinnacle's 70+ clinical centers."

ACT II: KNOWLEDGE TRANSFER
The Technique: What It Is
Technique Identity
Formal Name: Proprioceptive Heavy Work Sensory Diet Protocol
Parent-Friendly Alias: "Feeding the Heavy-Work Hunger"
Technique Code: A-106
Canon Material Category: Proprioceptive / Sensory Equipment
Parent-Friendly Alias: "Feeding the Heavy-Work Hunger"
Technique Code: A-106
Canon Material Category: Proprioceptive / Sensory Equipment
What It Is
A structured approach to providing safe, appropriate, high-intensity proprioceptive input to children whose nervous systems are under-responsive to proprioception — meaning they need significantly more muscle-and-joint input than typical children to feel regulated, grounded, and calm.
What It Does
Redirects unsafe, uncontrolled seeking behavior (crashing into walls, carrying dangerously heavy items, squeezing too tight) into purposeful, safe heavy-work activities using 9 specific materials. When the proprioceptive hunger is met, seeking behaviors decrease organically — because the need is satisfied.
Who It's For
Children ages 3–12 who show proprioceptive under-responsivity — they carry everything, crash constantly, push against surfaces, roughhouse intensely, and are calmer after vigorous physical activity.
Domain A: Sensory
Ages 3–12
10–20 Min Sessions
3–6× Daily
Home + School + Outdoor

This technique crosses every therapy boundary — because the brain doesn't organize by therapy type.
Occupational Therapy (Primary Lead)
The OT is the clinical architect. OTs use standardized assessments (Sensory Processing Measure, Sensory Profile 2) to confirm proprioceptive under-responsivity, then design an individualized sensory diet integrated into the child's daily routine across home, school, and community.
Speech-Language Pathology
SLPs integrate proprioceptive input into oral-motor work. Children who seek proprioceptive input through the body often also seek it orally — chewing shirts and pencils. Chewy tubes (Material #9) address this oral seeking channel directly.
ABA / BCBA
Applied Behavior Analysts structure the heavy-work protocol using behavioral principles: antecedent modification (provide input before the child escalates), reinforcement scheduling, and data collection on seeking behaviors.
Special Education
SpEd specialists ensure the sensory diet extends into classroom settings. Chair bands, weighted lap pads, chewy necklaces, and classroom "jobs" (carrying books, stacking chairs) are embedded into the school day.
NeuroDev Pediatrics
NeuroDev pediatricians confirm differential diagnosis, co-manage any pharmacological considerations, and provide medical clearance for the intensity of heavy-work protocols used. They are the clinical authority when seeking behavior causes injury risk.
"At Pinnacle, no technique is owned by one discipline. A-106 is designed, delivered, and monitored by OT + ABA + SLP + SpEd + NeuroDev working as one converged team — because that is how real developmental change happens."

A precision tool. Not a random activity.
The primary target is clear: reduce unsafe, uncontrolled proprioceptive seeking behavior so the child learns their body's need CAN be met through specific, safe outlets rather than crashing into furniture. Observable indicator — seeking behaviors decrease in frequency and intensity following heavy-work input sessions.
Target | Before | After (4–8 weeks) | |
Seeking frequency | Crashes/pushes 20+ times daily | Seeks appropriate outlet, 5–8 times daily | |
Duration of dysregulation | 45–90 min meltdowns | 5–15 min episodes with faster recovery | |
Focused attention | <3 min seated task | 10–20 min seated task post-heavy work | |
Safe seeking | Crashes into furniture/people | Goes to crash pad, trampoline |

The 9 Materials
9 materials. One goal: feed the proprioceptive hunger safely.
Each of the 9 materials below targets the proprioceptive hunger through a different channel — impact, resistance, compression, oral, or functional heavy work. Together they form a complete sensory diet kit. Individually, even one is enough to begin today.
Weighted Wagon / Push Cart
Canon: Proprioceptive Equipment | ₹1,500–5,000 | DIY Available
Heavy pulling with purpose — the muscles work, the brain gets fed, and they have a job to do.
Heavy pulling with purpose — the muscles work, the brain gets fed, and they have a job to do.
Crash Pad / Giant Bean Bag
Canon: Proprioceptive / Crash Mat | ₹3,000–12,000 | DIY Available | ⭐ Highest Impact
Safe target for the crashing need — whole-body impact input, on demand.
Safe target for the crashing need — whole-body impact input, on demand.
Body Sock / Lycra Tunnel
Canon: Sensory Sack | ₹800–2,500 | DIY Available
Whole-body resistance they control — they push out, the fabric pushes back.
Whole-body resistance they control — they push out, the fabric pushes back.
Weighted Vest / Weighted Backpack
Canon: Weighted Equipment | ₹2,000–6,000 | ⚠️ OT Guidance Recommended
Constant input during activity — the weight does the work so they don't have to crash.
Constant input during activity — the weight does the work so they don't have to crash.
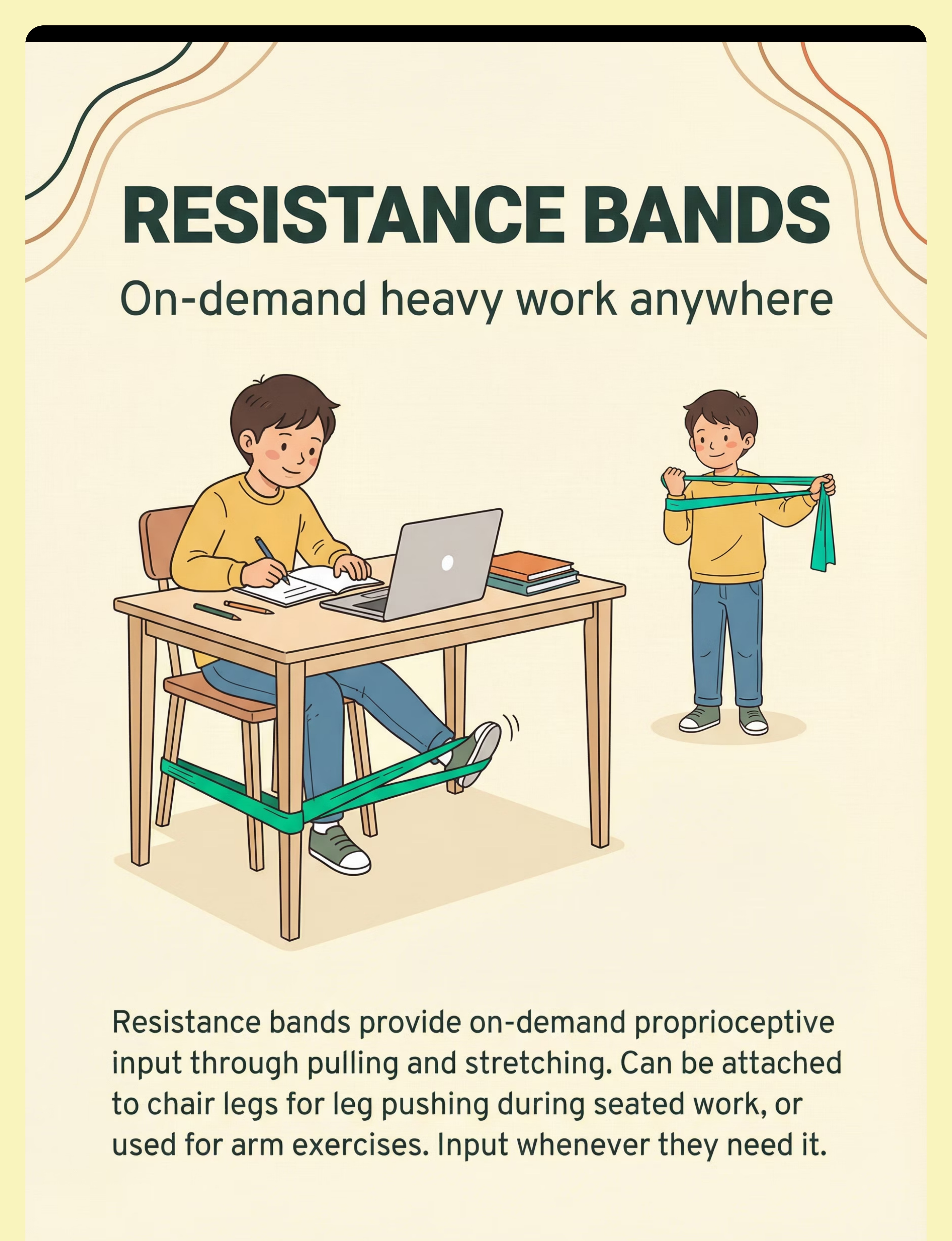
Resistance Bands / Therapy Bands
Canon: Resistance Equipment | ₹300–1,000 | DIY Available | 🏫 School-Friendly
On-demand heavy work anywhere — attach to chair for leg pressing during seated work.
On-demand heavy work anywhere — attach to chair for leg pressing during seated work.
Mini Trampoline / Indoor Bouncer
Canon: Proprioceptive / Vestibular | ₹2,000–6,000 | ⭐ Most Satisfying for Seekers
Jump, land, regulate, repeat — every landing sends proprioceptive signals to the brain.
Jump, land, regulate, repeat — every landing sends proprioceptive signals to the brain.
Compression Vest / Compression Clothing
Canon: Compression Equipment | ₹600–2,500 | DIY: Tight athletic wear
All-day baseline input — constant even pressure so they don't have to seek as intensely.
All-day baseline input — constant even pressure so they don't have to seek as intensely.
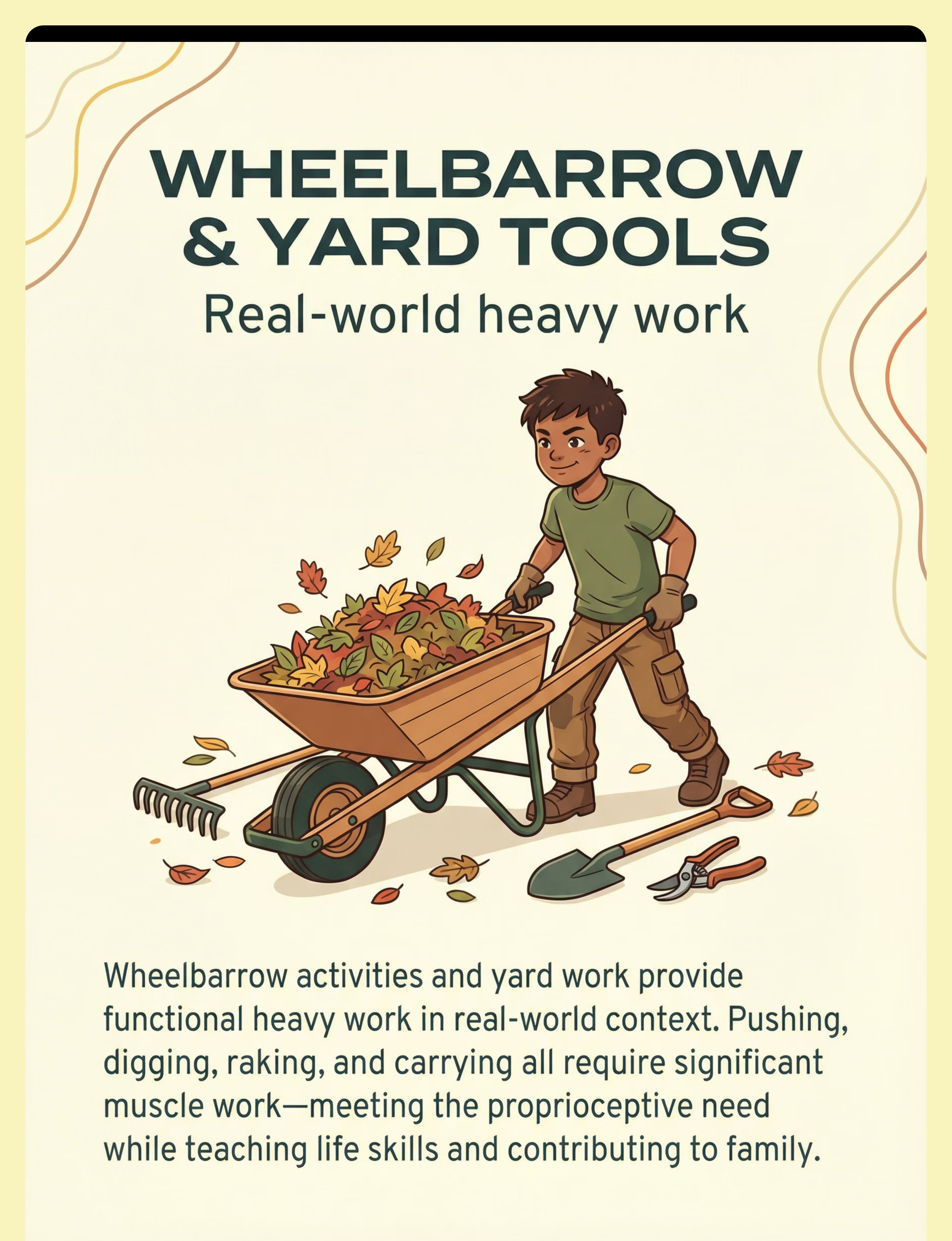
Wheelbarrow & Yard Tools
Canon: Heavy Work / Functional Tools | ₹800–3,000 | Mostly DIY
Real-world heavy work — pushing, digging, raking meets the need while teaching life skills.
Real-world heavy work — pushing, digging, raking meets the need while teaching life skills.
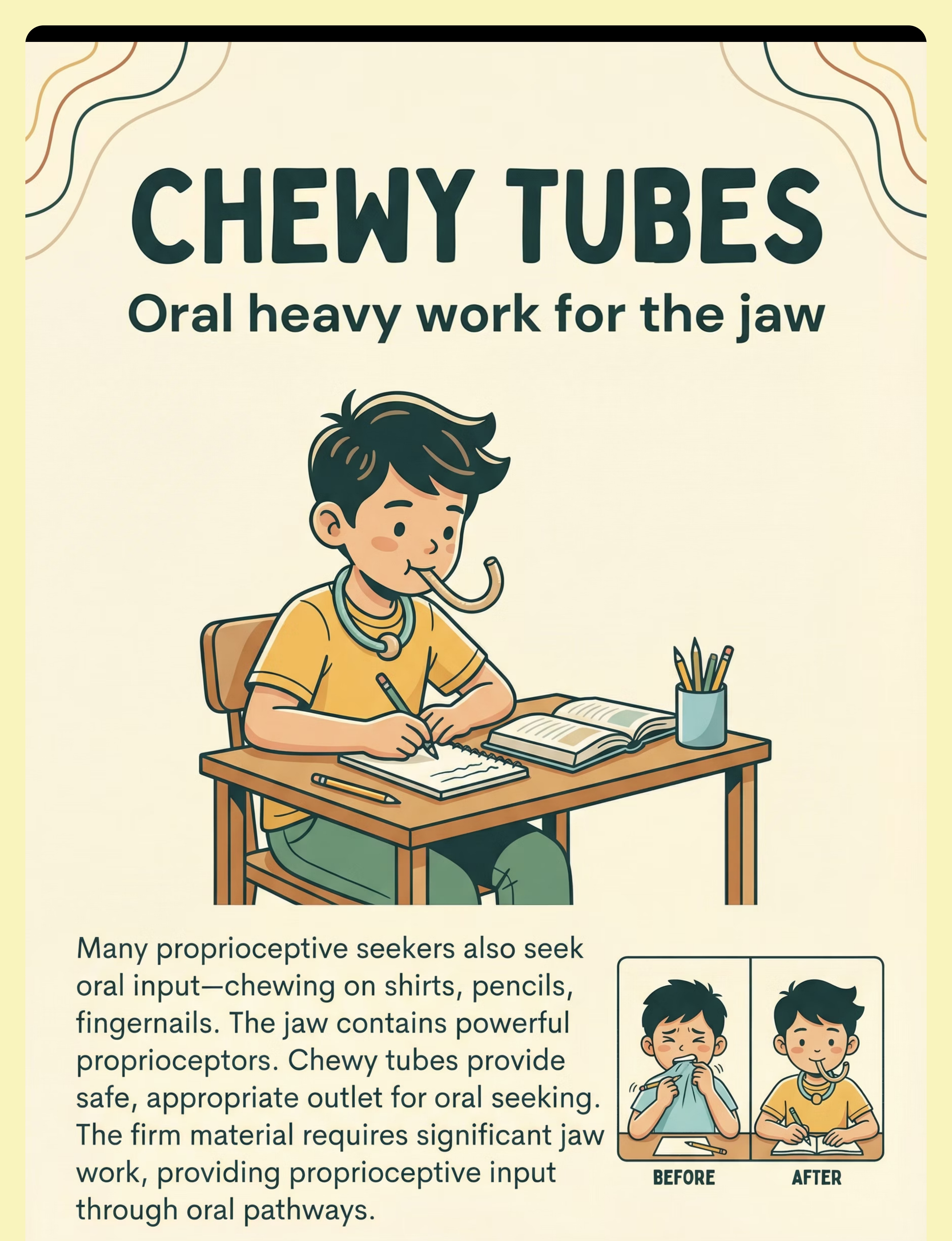
Chewy Tubes / Oral Motor Chews
Canon: Oral Motor Equipment | ₹300–1,200 | ⚠️ Safety-Critical — Purpose-Made Only
Oral heavy work for the jaw — if they chew shirts and pencils, give them the right thing.
Oral heavy work for the jaw — if they chew shirts and pencils, give them the right thing.
Starter Kit (₹4,000–5,000): Crash Pad/Beanbag (DIY stacked cushions) + Resistance Bands (chair band setup) + Chewy Tubes. These three address impact seeking, seated regulation, and oral seeking — the three most urgent channels.

Material 1: Weighted Wagon / Push Cart
Why It Works
The weighted wagon delivers sustained push-pull resistance directly through the muscles and joints of the arms, shoulders, and core. Every delivery trip is a targeted proprioceptive dose — the child gets a "job," a purpose, and a regulatory hit in one activity.
Commercial Option
DIY Version
Laundry basket + rope handle + books inside. The pushing and pulling resistance is physically identical to a commercial wagon — same muscles, same joints, same proprioceptive signals to the brain. Load to approximately 5–10% of the child's body weight to start.
How to Use It
- Give child a "delivery job" — take these books to the bedroom
- 3–5 delivery trips = standard session
- Add an uphill path or longer route to increase intensity
- Build to obstacle course variations as tolerance grows
Regulatory signal to watch for: Child slows push, walks normally after delivering — task-completion calm.

Material 2: Crash Pad / Giant Bean Bag
Why It Works
The crash pad is the single highest-impact material for proprioceptive seekers. Every crash, jump, and belly flop delivers a massive whole-body proprioceptive signal — the most intense, most immediate regulatory input available without leaving the house. Children who crash into furniture and people need exactly this — a safe, purposeful target for an urgent neurological need.
Commercial Option
DIY Version
Old mattress on floor OR 6+ couch cushions stacked in a corner. The same high-intensity impact proprioception — thickness absorbs and feeds the signal simultaneously. Minimum 6-inch thickness for jumping activities.
Safety Notes
- Place away from all walls, furniture, and hard surfaces
- Establish no-headfirst rule before first use
- One jumper at a time
- 5–15 crashes = typical regulatory dose
Regulatory signal: Child slows own pace, breathing deepens — they've met the need. They may sit quietly on the pad.

Material 3: Body Sock / Lycra Tunnel
Why It Works
The body sock provides whole-body resistive input that the child completely controls. They push out — the fabric pushes back. Every push in every direction fires proprioceptive signals from muscles and joints across the entire body simultaneously. It's immersive, self-directed, and deeply organizing to the nervous system.
Commercial Option
DIY Version
Large stretchy fitted sheet sewn into a sack with a head opening. The key is stretch — the fabric must resist the child's push while allowing full movement. Same resistive proprioceptive input when child pushes outward against fabric.
How to Use It
- Encourage star shape, ball shape, animal walks inside
- 5–10 minutes of active pushing provides significant input
- Do not rush — this is self-directed at child's pace
- Always ensure clear face/head opening
- Introduce gradually over 2–3 sessions if child is claustrophobic
Regulatory signal: Child finds a comfortable position and stops pushing — satiation.

Material 4: Weighted Vest / Weighted Backpack
Why It Works
The weighted vest delivers continuous proprioceptive input throughout an activity — the weight does the work so the child's nervous system receives a sustained regulatory signal without the child needing to crash or push. It's the most practical tool for bridging the gap between dedicated heavy-work sessions, reducing the intensity of seeking behavior during calm periods.
Commercial Option
DIY Version
Backpack with evenly distributed weight (books, water bottles) — maximum 5–10% body weight. Distribute weight symmetrically. Same continuous proprioceptive loading during activity.
Critical Safety Protocol
- Maximum 5–10% of body weight — never more
- 20–30 minutes on / 20–30 minutes off cycle
- Never use for sleeping
- Remove during high-intensity exercise
- Consult OT before beginning for individual calibration

Material 5: Resistance Bands / Therapy Bands
Why It Works
Resistance bands are the most versatile and school-friendly material in the A-106 kit. Attached to chair legs at ankle height, they provide constant on-demand heavy work during any seated activity. The child can press against the band at any moment — during drawing, eating, or listening — receiving proprioceptive input without interrupting any other activity.
Commercial Option
DIY Version
Exercise bands from any sports store. Tie around chair front legs at ankle height. Same on-demand resistance input for arms and legs.
How to Use It
- Tie band around chair front legs at ankle height
- Child pushes feet against band during any seated activity
- Runs during other activities — it is background input
- Switch to hand-held band for arm exercises during breaks
- Change band resistance level as child's strength grows
School note: This material is invisible, completely silent, and requires zero teacher intervention — perfect for classroom use.
Material 6: Mini Trampoline / Indoor Bouncer
Why It Works
The mini trampoline is one of the most satisfying materials for proprioceptive seekers — because every single landing delivers an intense, full-body proprioceptive signal. The repetitive, rhythmic nature of bouncing is inherently organizing to the nervous system. It addresses both the proprioceptive and vestibular seeking dimensions simultaneously.
Commercial Option
Safety Protocol
- One jumper at a time — always
- Handle bar for children under 6 or with coordination difficulties
- Check springs and mat surface regularly
- 1 meter clearance on all sides
How to Use It
- Free bouncing — child controls all intensity
- Add cognitive layer: count bounces, jump to music rhythm
- 5–10 minutes of sustained bouncing = significant regulatory dose
- Parent role: stand nearby for safety, not to direct
Regulatory signal: Bouncing becomes rhythmic, child may begin humming or singing.

Material 7: Compression Vest / Compression Clothing
Why It Works
Compression clothing provides constant, even proprioceptive pressure across the body throughout the entire day. Unlike the weighted vest (which is time-limited), compression clothing can be worn for extended periods as a baseline sensory support. It reduces the intensity of seeking behavior by maintaining a consistent low-level proprioceptive signal — the child doesn't feel as "empty."
Commercial Option
DIY Version
Tight-fitting athletic wear / rash guard worn under clothes. Key: snug, not restrictive. The child should be able to breathe normally and move freely. Same even compression proprioception — it's about sustained gentle pressure, not tightness.
How to Use It
- Wear under school uniform as an invisible sensory support
- Particularly effective in the hours after a heavy-work session
- Useful during transitions (car rides, waiting rooms) when other materials aren't available
- Can be worn during sleep if the child finds it calming

Material 8: Wheelbarrow & Yard Tools
Why It Works
Yard tools deliver the most "real-world" proprioceptive heavy work available — pushing, digging, raking, carrying, and hauling engage the full proprioceptive system through functional, purposeful activity. The additional benefit: the child is building life skills, contributing to the household, and earning genuine social recognition for strength that usually gets them in trouble indoors.
Commercial Option
DIY Version
Any bucket, bag, or container to fill and carry. Mopping, vacuuming, sweeping with genuine full-body effort. Carrying groceries, stacking firewood, watering plants with heavy cans. The principle is functional heavy work — same neurological input as commercial tools.
Indoor Alternatives
- Mopping the floor (full arm + shoulder engagement)
- Vacuuming with a full-size vacuum
- Moving furniture with parent supervision
- Carrying laundry baskets between rooms
- Stacking heavy books on shelves
Material 9: Chewy Tubes / Oral Motor Chews
Why It Works
The jaw is one of the most powerful proprioceptive organs in the body. Children who chew shirts, pencils, book corners, and collars are seeking oral proprioceptive input — their jaw is hungry for the same heavy-work input their body craves. Chewy tubes provide appropriate, safe, purpose-made targets for this oral seeking channel, replacing destructive chewing with a sanctioned outlet.
Commercial Option
⚠️ NO DIY — Safety Critical
Chewy tubes have no DIY equivalent. Food-safe, non-toxic, purpose-made materials are required. Improvised materials create significant choking and safety risk. This is the one material where purchase is non-negotiable.
How to Use It
- Offer immediately when child begins chewing clothing or objects
- Necklace-style chews for all-day access — breakaway clasps only
- Inspect before every use — replace when showing wear or teeth marks
- Never leave unattended with the chewy tube
- SLP coordination recommended for severe oral seekers

Every family can start today. Zero budget required.
The therapeutic principle — providing heavy proprioceptive input — does not require specific brand products. It requires the right physical forces. WHO Nurturing Care Framework: Effective early childhood interventions must be context-specific and equity-focused. Household items can deliver identical sensory input.
Material | Buy (₹) | DIY Version | Why It Works | |
Weighted Wagon | ₹1,500–5,000 | Laundry basket + rope + books inside | Same pushing/pulling resistance through muscles and joints | |
Crash Pad | ₹3,000–8,000 | Old mattress OR 6+ couch cushions stacked in corner | Same high-intensity impact proprioception | |
Body Sock | ₹800–2,500 | Large stretchy fitted sheet sewn into a sack | Same resistive input when child pushes outward against fabric | |
Weighted Vest | ₹2,000–6,000 | Backpack with evenly distributed weight — max 5–10% body weight | Same continuous proprioceptive loading during activity | |
Resistance Bands | ₹300–1,000 | Exercise bands from any sports store | Same on-demand resistance input for arms and legs | |
Compression Clothing | ₹600–2,500 | Tight-fitting athletic wear / rash guard under clothes | Same even compression proprioception — key is snug, not restrictive | |
Wheelbarrow | ₹800–3,000 | Any bucket/bag to fill and carry; mopping, vacuuming | Same functional heavy work principle | |
Chewy Tubes | ₹300–1,200 | NO DIY — safety-critical. Purchase only. | Food-safe, non-toxic, purpose-made required. Choking risk with improvised materials. |
"This is WHO/UNICEF equity in action. Proprioceptive regulation is a human right — not a premium product."

Read this before your first session. Every single time.
🔴 RED: Absolute Stop Signals
- Seeking causes injury to themselves or others (bruising, cuts)
- Cannot be redirected to safe outlets after multiple attempts
- Seeking intensity escalating week over week
- Child shows distress or pain during heavy-work activities
- Active injury, illness, or joint hypermobility (seek OT clearance)
- History of cardiac conditions, seizures, or neurological contraindications
🟡 AMBER: Proceed With Caution
- Weighted vest/backpack: max 5–10% body weight. Never for sleeping.
- Chewy tubes: inspect before every use. Replace at first sign of wear.
- Mini trampoline: one jumper at a time. Handle bar for under-6s.
- Crash pad: minimum 6-inch thickness. No headfirst rule established first.
- Body sock: always ensure clear face/head opening.
🟢 GREEN: Proceed When
- Child is fed and has had adequate sleep
- Child is in calm-alert or mildly dysregulated state
- Space is clear of hazards (setup complete)
- You have 10–20 uninterrupted minutes
- Child has no active illness or injury today
- You have reviewed the specific safety note for today's material
Emergency Protocol: If child becomes severely distressed during session — remove materials calmly, move to a neutral space, offer deep pressure (bear hug if accepted, or heavy blanket). Do not restrain. Document what preceded the distress for future session adjustment.

The right environment makes the technique work. Set this up once. Use it every day.
Room Layout
Clear floor zone: minimum 3m × 3m
Crash Pad / Mattress
Far corner — 1.5m clear on all sides
Trampoline
Center-left, 1m clearance all sides
Wagon / Push Cart
Entry point — clear path to walk through
Parent Position
Near doorway — full visual of entire space
Materials Shelf
Low shelf: body sock, bands, chews — accessible to child
What to Remove
- Glass items and fragile objects within reach
- Sharp furniture corners (cover with padding)
- Climbing temptations that lead to unsafe heights
- Screens and noise sources (first 3 sessions)
What to Add
- Visual schedule of today's heavy-work activities
- Visual hourglass or digital timer
- Water bottle — heavy work creates thirst
- Small reinforcement box (stickers, preferred items)
Sensory Environment
- Lighting: Natural or warm lamp — avoid harsh fluorescent
- Sound: Silence for first 2–3 sessions
- Temperature: Set 2°C cooler than usual — heavy work generates heat
Daily Setup Time: 5 minutes. After the first week, the child often helps set up — this itself is heavy work.

Ags 3–12
Home Applicable
60 seconds. Before every session. No exceptions.
A child's nervous system state shifts hour to hour. Starting a heavy-work session while your child is already dysregulated, hungry, or unwell can backfire, turning a therapeutic opportunity into a source of stress. This 60-second check is the critical difference between a productive, regulating session and a total meltdown.
You are the sensor. Your child cannot always tell you what they need. You have to read it.
🍽️ Fed?
Ensure the last meal was within 2 hours; heavy work on an empty stomach often causes irritability rather than regulation.
💧 Hydrated?
Offer water before starting, as intense proprioceptive input naturally increases body temperature.
😴 Rested?
If the child shows signs of being overtired, such as rubbing eyes or a glassy stare, shorten the session to 10 minutes maximum.
🤒 Unwell?
Check for fever, stomach complaints, or unusual sensory sensitivity; postpone the session if any are present.
🧠 Regulated?
Is the child in a "ready to engage" window? Look for eye contact and responsiveness, avoiding sessions when they are too hyper or fully shut down.
If 3 or more of these are "no" — postpone the session. A 20-minute delay is not a failure. Forcing a session when the child isn't ready teaches the nervous system that heavy work is stressful, not regulating.
Pro tip: Do this check out loud with your child. "Are you hungry? Are you thirsty?" — this builds interoceptive awareness over time.

Step 1: The Invitation
Step 1 of 6
⏱️ 30–60 seconds
Every session begins with an invitation, never a command. The child is brought into the heavy-work space through play-based, low-demand engagement. The goal is to access motivation, not compliance.
The Script
"Hey! I set up something for you. Want to come see? We're going to do some really STRONG work today."
OR for a child who loves the activity already:
"It's heavy-work time! The crash pad is waiting for you. Can you carry this [small item] to the mat?"
Body Language
- Get to the child's level (crouch or sit)
- Use excited, warm tone — not demanding
- Point toward the space, lead with movement, not words
Acceptance Cues (child is ready)
- Moves toward the space
- Begins touching or engaging with materials
- Increased body movement/energy (this is anticipation, not dysregulation)
- Vocalizes positively or signs "more" or "yes"
Resistance Cues (modify)
- Turns away → Wait 5 minutes, offer again with a different material
- Covers eyes or ears → Reduce to one material, quieter environment
- Begins self-stimulatory behavior → Offer most preferred heavy-work item directly
Pairing Principle (ABA): The first 3–5 sessions are about establishing the space as a rewarding place, not maximizing therapeutic input.

Step 2: The Engagement
Step 2 of 6
⏱️ 1–3 minutes
The child is now in the space. You introduce the first material — chosen based on today's readiness assessment and the child's current seeking signal.
If child is... | Start with... | Why | |
Crashing into things on arrival | Crash Pad | Channel the active crash need immediately into the safe outlet | |
Running and jumping | Mini Trampoline | Match the vestibular + proprioceptive mix they're already seeking | |
Pushing against walls/furniture | Weighted Wagon | Redirect push-seeking into purposeful resistance | |
Chewing on clothes/objects | Chewy Tube | Address oral seeking at entry point immediately | |
Generally restless/fidgety | Resistance Bands on chair | Gentle entry that works for moderate arousal |
"Look — this is the crash pad. This is YOUR place to jump and crash. Let me show you — watch me!" [Demonstrate first. Parent models the activity.]
Engagement
Immediately imitates, takes over the material, shows excitement → Let them lead.
Tolerance
Watches, approaches, touches tentatively → Narrate: "See, you can push it as hard as you want."
Avoidance
Moves away from specific material → Switch to a different material from the 9-material list.

Step 3: The Therapeutic Action
Step 3 of 6
⏱️ 8–12 minutes
The child engages in sustained, repetitive heavy-work input through the chosen material(s). The parent's role is now facilitation, not instruction. Keep the energy positive, the commentary minimal, and the redirection gentle.
🔴 Crash Pad Session
Child jumps/crashes from standing height (no furniture). 5–15 crashes = typical regulatory dose. Variations: forward, sideways, seated drop, belly flop. Regulatory signal: Child slows own pace, breathing deepens.
🔵 Weighted Wagon Work
Fill wagon with books/water bottles. Give child a "delivery job." 3–5 delivery trips = standard session. Variations: uphill path, longer route, obstacle course. Regulatory signal: Child settles after delivering — task-completion calm.
🟣 Body Sock Exploration
Child enters sock, pushes outward in all directions. Encourage star shape, ball shape, animal walks. 5–10 minutes of active pushing provides significant input. Regulatory signal: Child finds comfortable position and stops — satiation.
🟢 Trampoline Bouncing
Free bouncing — child controls all intensity. Add cognitive layer when established: count bounces, jump to music. 5–10 minutes = significant regulatory dose. Regulatory signal: Bouncing becomes rhythmic, child may begin humming.
🟠 Resistance Band Work
Tie band around chair front legs at ankle height. Child pushes feet against band during any seated activity. This material runs during other activities — it is background input.
Parent Coaching During Action: Use minimal words. Narrate what you see: "You're SO strong." | "Feel how heavy that is? Your muscles are working hard." | "Your body is getting exactly what it needs right now." Optimal duration: 10–15 minutes. Diminishing returns after 20 minutes.

Step 4: Repeat & Vary
Step 4 of 6
⏱️ 3–5 additional minutes
"3 good repetitions are worth more than 10 forced ones."
Material | Min. Effective | Optimal | Satiation Signal | |
Crash Pad | 5 crashes | 10–15 crashes | Child self-stops, sits calmly on pad | |
Wagon | 2 delivery trips | 4–5 trips | Child slows push, walks normally | |
Body Sock | 3 shape changes | 5–8 min exploration | Child curls up or removes sock calmly | |
Trampoline | 20 jumps | 50–100 jumps | Bouncing becomes rhythmic, pace decreases | |
Resistance Bands | 10 pushes | 20–30 reps | Child stops voluntarily |
Variation to maintain engagement: Introduce variations after the first 3–5 repetitions to prevent habituation. Crash Pad: vary jump height and direction. Wagon: change the cargo or route. Body Sock: try different shapes, add music. Trampoline: counting, catching a ball while bouncing.
Satiation Recognition: Spontaneous decrease in activity intensity + deeper, more rhythmic breathing + calmer facial expression + willingness to transition to non-seeking activities. When you see satiation — the hunger has been fed. This is the goal. This is success.

Step 5: Reinforce & Celebrate
Step 5 of 6
⏱️ Within 3 seconds
Reinforcement delivered within 3 seconds of the desired behavior determines whether that choice strengthens. Miss the window — the reinforcement still feels good but loses significant behavioral impact.
For going to crash pad:
"YES! You felt that feeling and you went to the crash pad! That was PERFECT. Your body knew what it needed and you found the right place!"
For completing wagon delivery:
"You carried ALL of that! Did you feel how strong your muscles were? That's exactly what your body was asking for!"
For choosing chewy tube over shirt:
"I saw you reach for your chewy — that was amazing. Your mouth needed that and you knew exactly what to do!"
Reinforcement Menu
⭐ Sticker on chart
🎯 Token toward preferred activity
🎮 1 extra minute of preferred screen time
🤝 High-five + specific verbal praise
🌟 "Superhero Strength" certificate
Celebrate the attempt, not just the success. If the child tries the crash pad but only manages 2 jumps — celebrate the 2 jumps. The first 2–4 weeks require the most deliberate reinforcement.

Step 6: The Cool-Down
Step 6 of 6
⏱️ 2–3 minutes
Abrupt session endings are a common cause of post-session dysregulation. The cool-down bridges back to baseline using calming proprioceptive input — deep pressure, slow heavy work, or quiet compression.
Transition Warning (give 2–3 minutes notice):"Two more jumps, then we're going to do our finishing squeeze." OR use a visual timer: set it for 3 minutes. Child watches it count down.
Option A: Deep Pressure Finish
Weighted blanket placed over child while seated. 2 minutes of quiet with heavy blanket input. No demands.
Option B: Squeeze & Release
Parent provides joint compressions (shoulder, hip) — 10 slow, firm compressions. Check OT guidance for correct technique. Deeply calming for most proprioceptive seekers.
Option C: Heavy Blanket Roll
Child lies on mat, parent rolls heavy blanket around them like a burrito. Child can request pressure increase. 2 minutes.
Option D: Slow Wagon Roll
End the session by very slowly pushing an empty wagon back to storage together. The slow heavy work transitions arousal down.
Material Put-Away Ritual: Child helps put away materials (this is more heavy work!). "Can you carry the crash pad to the corner? Can you put the chewy in the basket?" This builds routine and provides closing proprioceptive input.

60 seconds of data now saves hours of guessing later.
Most parents try to remember how a session went at bedtime. By then, the brain has already compressed, edited, and partially discarded the details. Research on retrospective recall in caregiving contexts shows that data captured within 60 seconds of session end is 10× more accurate than end-of-day recall. Over 4–8 weeks, even this simple four-field log generates a dataset powerful enough to identify your child's optimal session time, best-performing material, and average regulation window — the three variables that determine whether you scale up, hold steady, or modify the protocol.
You are not filling in a form. You are building your child's proprioceptive profile — a personalized map of what works, when it works, and how long it lasts. The GPT-OS® system reads this data and generates weekly protocol adjustments automatically. Your job is just to capture it honestly.
Field 1: Pre-Session Seeking Intensity
Unsafe Seeking Incidents (2 hours before session)
Count each incident separately: crashes into furniture, crashes into people, wall-pushing, floor-throwing, object-slamming. Do not count intentional play.
Tally: ○ 0 (calm baseline) ○ 1–3 (mild) ○ 4–7 (moderate) ○ 8–10 (high) ○ 10+ (crisis-level — consider session modification)
Tally: ○ 0 (calm baseline) ○ 1–3 (mild) ○ 4–7 (moderate) ○ 8–10 (high) ○ 10+ (crisis-level — consider session modification)
Field 2: Session Engagement Quality
How Present Was Your Child Today?
★★★★★ Self-directed — initiated activities, led transitions, minimal prompting
★★★★☆ Cooperative — followed all prompts, needed 1–2 redirections
★★★☆☆ Partial — completed 50–70% of planned activities with support
★★☆☆☆ Resistant — completed 1 activity, required significant coaxing
★☆☆☆☆ Refused — session not completed; log reason in notes
★★★★☆ Cooperative — followed all prompts, needed 1–2 redirections
★★★☆☆ Partial — completed 50–70% of planned activities with support
★★☆☆☆ Resistant — completed 1 activity, required significant coaxing
★☆☆☆☆ Refused — session not completed; log reason in notes
Field 3: Post-Session Regulation Window
How Long Did Calm Last After the Session Ended?
Start timing from the moment the cool-down ends. Stop when the first unsafe seeking behavior reappears or dysregulation is clearly visible.
○ Under 15 min (protocol needs review) ○ 15–30 min (building) ○ 30–60 min (on track) ○ 1–2 hours (strong response) ○ 2+ hours (optimal — note which material was used)
○ Under 15 min (protocol needs review) ○ 15–30 min (building) ○ 30–60 min (on track) ○ 1–2 hours (strong response) ○ 2+ hours (optimal — note which material was used)
Field 4: Today's MVP Material
Which Single Material Produced the Most Visible Regulation?
Circle one. If two materials tied, circle both and note the sequence.
[Crash Pad] [Weighted Wagon] [Body Sock] [Weighted Vest] [Resistance Bands] [Mini Trampoline] [Compression Vest] [Yard Tools / Wheelbarrow] [Chewy Tube]
Note: If a DIY alternative was used, write it in. All materials count.
[Crash Pad] [Weighted Wagon] [Body Sock] [Weighted Vest] [Resistance Bands] [Mini Trampoline] [Compression Vest] [Yard Tools / Wheelbarrow] [Chewy Tube]
Note: If a DIY alternative was used, write it in. All materials count.
Field 5: Parent Observation Note (Free Text)
One sentence. What stood out today?
This is the most underrated field in the tracker. A single sentence — written immediately after the session — captures the qualitative signal that numbers miss. Examples:
• "He asked to do it again — first time ever."
• "She settled within 3 minutes of the body sock. Faster than last week."
• "He refused the wagon but accepted the crash pad immediately."
• "Meltdown at school today — session was shorter but still helped."
• "She made eye contact during the cool-down. Didn't expect that."
These notes, read across 4–8 weeks, reveal the emotional and relational arc of your child's progress — the part no star rating can capture.
• "He asked to do it again — first time ever."
• "She settled within 3 minutes of the body sock. Faster than last week."
• "He refused the wagon but accepted the crash pad immediately."
• "Meltdown at school today — session was shorter but still helped."
• "She made eye contact during the cool-down. Didn't expect that."
These notes, read across 4–8 weeks, reveal the emotional and relational arc of your child's progress — the part no star rating can capture.
What Your Data Is Telling You: A Quick Interpretation Guide
Pattern | What It Means | What To Do | |
Regulation window under 15 min for 3+ sessions in a row | Protocol intensity is too low for this child's threshold | Increase session duration by 5 min or add a second daily session | |
Engagement drops to ★★☆☆☆ or below consistently | Child may be fatigued, overstimulated pre-session, or fighting illness | Check sleep quality, screen time in the 2 hours before sessions, and pre-session hunger | |
One material consistently outperforms all others | Child has a dominant proprioceptive preference channel | Lead every session with that material; use others as secondary or cool-down only | |
Regulation window growing week over week | Neural pathway consolidation is actively occurring | Stay the course — do not change the protocol, even if progress feels slow | |
Seeking incidents increasing despite consistent sessions | Sensory diet may need professional recalibration | Contact Pinnacle helpline immediately: 9100 181 181 (free, 18 languages) |

Session didn't go perfectly? That's not failure. That's data.
Child refused to enter the space at all
Why: Space or materials may feel new or overwhelming.
Next time: Bring one material to where the child already is. Start in familiar territory. Spend 3 sessions "just showing" materials without any demand.
Next time: Bring one material to where the child already is. Start in familiar territory. Spend 3 sessions "just showing" materials without any demand.
Child engaged for 2 minutes then walked away
Why: Session started too late in the dysregulation cycle. OR not enough preferred material variety.
Next time: Offer heavy work earlier — before they're escalated. Add their most-preferred material.
Next time: Offer heavy work earlier — before they're escalated. Add their most-preferred material.
Child kept seeking unsafely even after session
Why: Input intensity or duration was insufficient for this child's need level.
Next time: Increase session duration by 5 minutes. Add one more material rotation. Consider crash pad → trampoline sequence for higher intensity.
Next time: Increase session duration by 5 minutes. Add one more material rotation. Consider crash pad → trampoline sequence for higher intensity.
Child escalated immediately after the session
Why: Cool-down was insufficient, OR the transition to the next activity was abrupt.
Next time: Add 3–5 minutes to cool-down. Warn about the next activity during cool-down, not after. Offer compression clothing for the post-session period.
Next time: Add 3–5 minutes to cool-down. Warn about the next activity during cool-down, not after. Offer compression clothing for the post-session period.
Child started hurting siblings/parents during the session
Why: Seeking behavior directed at people is often proprioceptive seeking + social communication.
Next time: Provide crash pad immediately when social-seeking starts. Introduce: "Crash pad, not people." Repeat across 4–6 sessions consistently.
Next time: Provide crash pad immediately when social-seeking starts. Introduce: "Crash pad, not people." Repeat across 4–6 sessions consistently.
Child did great for two weeks then stopped wanting sessions
Why: Habituation — the same materials used the same way lose novelty.
Next time: Introduce one new variation or new material. Change the delivery job for the wagon. Add music to trampoline. Rotate materials weekly.
Next time: Introduce one new variation or new material. Change the delivery job for the wagon. Add music to trampoline. Rotate materials weekly.
No noticeable difference in seeking after 3 weeks
Why: Protocol may need adjustment. Child's sensory need may exceed what home protocol can address alone.
Action: Book a Pinnacle OT assessment → 9100 181 181
Action: Book a Pinnacle OT assessment → 9100 181 181

No two children need identical protocols. This one is built for yours.
The standard protocol in this guide is calibrated for a child aged 5–9, with moderate proprioceptive seeking, in a stable home environment. But your child is not average. Use the three-level intensity dial below to match the protocol to where your child actually is today — not where you hope they'll be next week.
Level 1 — Reduced Intensity
Use on: bad days, illness recovery, post-meltdown days, first week of protocol, high-anxiety periods, or any day the child woke dysregulated.
- One material only — crash pad or body sock preferred (both provide deep input with minimal demand)
- Session duration: 5 minutes maximum. Stop before the child wants to stop.
- No sequencing. No transitions between materials.
- Zero verbal demands during the session — no instructions, no questions, no praise language. Presence only.
- Environmental complexity: reduce to minimum. One light source. No music. No siblings in the room.
- Data note: Log this as a "Level 1 session" — do not compare regulation windows to standard sessions.
Level 2 — Standard Protocol
Use on: typical days when the child is rested, fed, and not post-meltdown. This is the default.
- Full 6-step protocol as written (Cards 14–19)
- Duration: 15–20 minutes
- 3–4 materials in rotation, sequenced: heavy work first → compression → oral motor last
- 3–6 sessions daily, spaced minimum 90 minutes apart
- Verbal reinforcement active throughout
- Data capture: all 5 fields within 60 seconds of cool-down
Level 3 — Elevated Intensity
Use when: child has completed 4+ weeks of standard protocol, regulation windows consistently exceed 90 minutes, and child is actively seeking more challenge.
- Begin outdoors: 10 minutes of yard work (wheelbarrow, digging, carrying) before indoor session
- Full crash pad + trampoline + wagon rotation — all three in one session
- Add cognitive challenge during trampoline: counting backwards, naming categories, answering questions mid-bounce
- End with 10-minute compression clothing wear during a calm preferred activity
- Introduce obstacle course format: sequence 4–5 heavy-work stations with 30-second transitions
- Data note: Log as "Level 3 session." Watch for signs of over-stimulation (increased aggression, refusal, crying post-session).
Age-Based Modifications
Ages 3–5: The Foundation Years
- Lead with the weighted wagon or push cart — it's functional, purposeful, and easy for young children to understand
- Sessions capped at 10 minutes. Young nervous systems saturate faster.
- Transitions between materials: use a visual schedule with pictures, not words
- Body sock: introduce over 3 separate sessions — first session, just touch it. Second, put feet in. Third, full entry.
- Reinforcement: immediate, physical, and specific. "You pushed SO hard!" beats "Good job."
- Sticker chart visible in the therapy space — child places sticker immediately after cool-down
Ages 6–8: The Awareness Window
- Full standard protocol appropriate from Week 1
- Begin teaching interoceptive awareness: "Does your body feel hungry for heavy work right now?"
- Trampoline counting (count jumps aloud) builds self-monitoring and number skills simultaneously
- Introduce the "body check" before and after sessions: child rates their body on a 1–5 calm scale using fingers
- Child begins to identify their own "early warning signs" of dysregulation — teach them the vocabulary: "I feel buzzy," "I feel crashy," "I feel tight"
- Start transitioning data capture to the child: they circle the star rating themselves
Ages 9–12: The Autonomy Transition
- Child begins self-scheduling heavy-work breaks — provide a visual menu of options, not a fixed timetable
- Introduce the concept of a "sensory diet": child co-creates their weekly schedule with parent as consultant
- Transition heavy-work channels to age-appropriate activities: martial arts (judo, wrestling), rock climbing, swimming, competitive sports
- Reduce parent-directed sessions to 1–2 per day; increase child-initiated sessions
- Child maintains their own simplified tracking log — one sentence per day
- Goal by end of this phase: child can identify dysregulation, select an appropriate heavy-work activity, execute it independently, and return to task without parent prompt

ACT IV: THE PROGRESS ARC
In the first two weeks: you are planting seeds, not harvesting fruit.
✅ Real Progress in Weeks 1–2
- Child enters the heavy-work space without significant resistance on 3+ of 7 days
- At least one session where child sustained engagement for 5+ minutes
- One instance of going to crash pad or trampoline without being prompted (even once — this is remarkable)
- Unsafe seeking behavior count stable or showing 10–15% reduction
- Parent completes at least 4 of 7 days of sessions
⚠️ What Is Not Progress Yet (expected, normal)
- Seeking behaviors still present — they won't vanish in 2 weeks
- Some sessions going poorly or being abandoned — this is expected and data
- Child not yet independently initiating heavy-work activities
- Post-session regulation window still short (15–30 minutes is success at this stage)
Week 2 is when most parents abandon — results feel too small. This is the critical commitment point. If your child tolerates the crash pad for 10 seconds longer today than last week — that is neural pathway formation. That is real. That is working.
Daily Goal: 1 session per day, any material, any duration. Consistency > intensity at this stage.
In weeks 3–4: the neural pathways are forming. Watch for these signs.
Protocol Progress
You are 40% of the way through the core intervention window
Seeking Reduction
Expected decrease in unsafe seeking incidents from Week 1 baseline by Week 3–4
Regulation Window
Post-session regulation window should be extending consistently by Week 4
🧠 Neural Pathway Formation Signs
Child anticipates the session — begins moving toward the heavy-work space when they see you setting up. Child requests a material by name, gesture, or leading you to the space. Child begins using appropriate outlet spontaneously — goes to crash pad without being told at least once.
📊 Behavioral Consolidation
Parent can predict when the child will need input (before mealtimes, after school, before homework). Child shows clear satiation signals after sessions. Fewer meltdowns specifically related to "prevented from seeking" scenarios.
👪 Parent Milestone
You may notice you're more confident, less anxious about the crashing. You have a tool. You understand what your child's body is communicating. This shift in parental understanding is clinically significant — it changes the entire interaction pattern.
When to increase frequency: If the regulation window is still under 30 minutes consistently in week 4 → Increase session frequency to 4–6 daily sessions (shorter each — 5–8 minutes). The total proprioceptive input needs to be higher.
By week 8: the child begins to become their own therapist.
75% Complete
🏆 Mastery Zone
Level 1 Mastery — Tool Use
Child independently goes to crash pad, trampoline, or wagon when experiencing seeking urge (without prompt from parent). Child can name or signal their preferred heavy-work activity. Session can run with minimal parent instruction — child leads.
Level 2 Mastery — Self-Awareness
Child shows early recognition of their own regulation state: fidgeting → self-initiates heavy work before escalating. Child can communicate (verbally or via AAC/gesture) that they "need" heavy work. Unsafe seeking incidents at 50%+ reduction from Week 1 baseline.
Level 3 Mastery — Generalization
Child uses appropriate heavy-work strategies in settings beyond the home (school, relatives' homes, public). Post-session regulation window consistently 2+ hours. Skill maintained even on days with disrupted routine.
"Mastery here doesn't mean the proprioceptive need disappears. It means the child has learned to meet it safely, independently, and appropriately. That is a life skill."

You did this. Your child grew because of your commitment.
You started with a child crashing into every surface, carrying everything to exhaustion, pushing against walls to feel something. You didn't punish it. You didn't try to stop it. You understood it. You built a protocol. You showed up — day after day — with a crash pad and a wagon and the patience of a thousand therapists.
And now your child goes to the crash pad. Now they carry the grocery bags with purpose and pride instead of panic. Now you see the regulatory window — those beautiful 2 hours of calm focus after a good heavy-work session.
Understand
Proprioceptive under-responsivity at a clinical level
Execute
A 6-step home-based heavy-work protocol
Track
Data and adapt the intervention in real time
Reduce
Unsafe seeking by 50%+ over 8 weeks
Document this: What does your child look like after a great heavy-work session? That regulated, calm, satisfied expression — that is 8 weeks of your work.

Even in the success zone: trust your instincts. These signs mean pause and call.
🔴 Red Flag 1 — Escalating Injury Risk
Seeking behaviors are causing more frequent or more severe injuries (bruising, cuts, others hurt) despite consistent protocol implementation. → Pause. OT assessment required.
🔴 Red Flag 2 — No Regulatory Effect Despite Protocol
Consistent weekly sessions for 4+ weeks with no measurable reduction in seeking frequency or improvement in regulation windows. → Book a formal sensory assessment.
🔴 Red Flag 3 — Extreme Distress Response
Child becomes severely distressed, self-injurious, or inconsolable when prevented from seeking — beyond what the protocol can manage at home. → Clinical-level intervention intensity needed.
🔴 Red Flag 4 — New or Worsening Comorbid Symptoms
Emergence or intensification of seizure activity, significant regression in communication, extreme sleep disruption, or new stereotyped behaviors. → NeuroDev pediatric consultation immediately.
🔴 Red Flag 5 — Safety of Other Children
Seeking behavior consistently endangers siblings, other children, or the child themselves. → Pinnacle center consultation. More structured therapeutic environment may be needed.
🔴 Red Flag 6 — Parent Distress
Managing the protocol is significantly impacting the family's mental health or daily functioning. → This is a red flag too. You matter. Call for support.
You are not done. You are exactly where you need to be on a much longer journey.
★ You Are Here: A-106 — Seeks Heavy Lifting
You have completed the foundational proprioceptive heavy-work protocol. Your child is feeding the hunger safely and purposefully.
Path 1 → A-107: Uses Too Much Force
Your child's heavy work is effective but their force grading is off — they break things, hurt without meaning to. A-107 is the natural next technique after A-106 mastery.
Path 2 → A-108: Oral Sensory Seeking
If chewing behaviors (Material #9 in A-106) are the most prominent presentation, A-108 provides an oral-motor-specific deep dive with additional techniques and materials.
Path 3 → A-109: Movement Seeking
If jumping and spinning are more prominent than heavy lifting, A-109 addresses the vestibular seeking dimension with its own targeted protocol and material set.
Path 4 → A-115: Full Sensory Diet
After mastering A-106, building a complete sensory diet integrates all modalities into a sustainable daily schedule. The long-term goal for every family using this series.

Already have the crash pad? These techniques use the same materials.
Technique | Code | Difficulty | Materials You Already Own | |
Clumsiness & Body Awareness | A-105 | 🟡 Core | Crash pad, body sock | |
Uses Too Much Force | A-107 | 🟡 Core | Resistance bands, weighted items | |
Oral Sensory Seeking | A-108 | 🟢 Intro | Chewy tubes | |
Movement Seeking (Vestibular) | A-109 | 🟡 Core | Trampoline, crash pad | |
Can't Sit Still | A-110 | 🟡 Core | Resistance bands, weighted vest | |
Building a Sensory Diet | A-115 | 🔴 Advanced | All materials from A-106 |
"You already own materials for all 6" ✅ Having completed A-106, your material kit covers all 6 related techniques. This is the Canon Material leverage principle — each technique deepens the value of materials already in your home.
ACT V: COMMUNITY & ECOSYSTEM
They started exactly where you are. Here's where they are now.
Arjun, Age 7 — Hyderabad
Before A-106 (Week 1): Arjun was crashing into furniture 25–30 times daily. At school, he was suspended twice for crashing into other children — not from aggression, but because his nervous system was on fire with unmet proprioceptive need. His parents had tried every behavioral strategy. Nothing worked.
After A-106 (Week 8): Arjun now has a crash pad corner in the living room that he goes to independently when he feels "the crash feeling" (his words). His school has a resistance band on his chair. Unsafe crashing incidents at school: 0 in the last 4 weeks.
"We stopped fighting his need and started feeding it. The bruises disappeared. Our couch survived. And Arjun started saying 'I need my crash pad' — those four words changed everything." — Arjun's father
Priya, Age 5 — Bengaluru
Before: Priya's hugs left marks on her little brother. Her teachers called every week because she was "too rough" with classmates. She insisted on carrying every single item from the car, and if her parents took anything from her hands, she'd melt down completely.
After 6 weeks: Priya has a weighted backpack she wears to school. She has "delivery jobs" around the house every evening. Her body sock is the last thing she uses before bed — 10 minutes of pushing outward, and she's asleep in 20 minutes. Her teacher called to say she hadn't been reported for roughness in 3 weeks.
"I felt so guilty thinking she was doing this to upset me. Understanding that her body was just hungry — that changed me as a parent. I stopped grieving her behavior and started feeding her need." — Priya's mother
"In my experience, A-106 produces some of the fastest visible changes of any sensory technique — because the seeking behavior is so clear and the corresponding relief from appropriate heavy-work input is so immediate. Parents see results in the first week. That early evidence of success sustains the commitment through the harder weeks." — Senior OT, Pinnacle Network
Preview of 9 materials that help when child seeks heavy lifting Therapy Material
Below is a visual preview of 9 materials that help when child seeks heavy lifting therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.









Link copied!

From fear to mastery. One technique at a time.
The Pinnacle Promise
Pinnacle Blooms Network® exists to transform every home into a proven, evidence-based, 24×7 therapeutic environment — making clinical-grade intervention accessible to every family in every village, city, and country on Earth. No child should miss the therapy their developing brain needs because it wasn't accessible, affordable, or understandable.
A-106 is one of 70,000+ techniques in the GPT-OS® library. Every technique page is a link in a chain — from fear to understanding, from chaos to protocol, from seeking to self-regulation.
Navigation
Medical Disclaimer
This content is educational and evidence-informed. It does not replace assessment, diagnosis, or treatment by a licensed occupational therapist, behavior analyst, speech-language pathologist, or medical doctor. Proprioceptive seeking behaviors that cause injury, significantly impair daily function, or are escalating in severity require professional evaluation. Individual results vary. Consult a qualified professional before implementing weighted equipment protocols for children with hypermobility, cardiac conditions, or neurological diagnoses.
Contact
"From fear to mastery. One technique at a time."
— The Pinnacle Blooms Consortium
— The Pinnacle Blooms Consortium
© 2025 Pinnacle Blooms Network® | All Rights Reserved | CIN: U74999TG2016PTC113063 | DPIIT: DIPP8651 | Powered by GPT-OS® | 70+ Centers | 20M+ Sessions | 70+ Countries