

Solitary play is the starting point of all play development — not the failure point. Every child begins here. The question is not whether your child prefers solo play, but whether they have the capacity for both. That capacity can be built, systematically, at home.
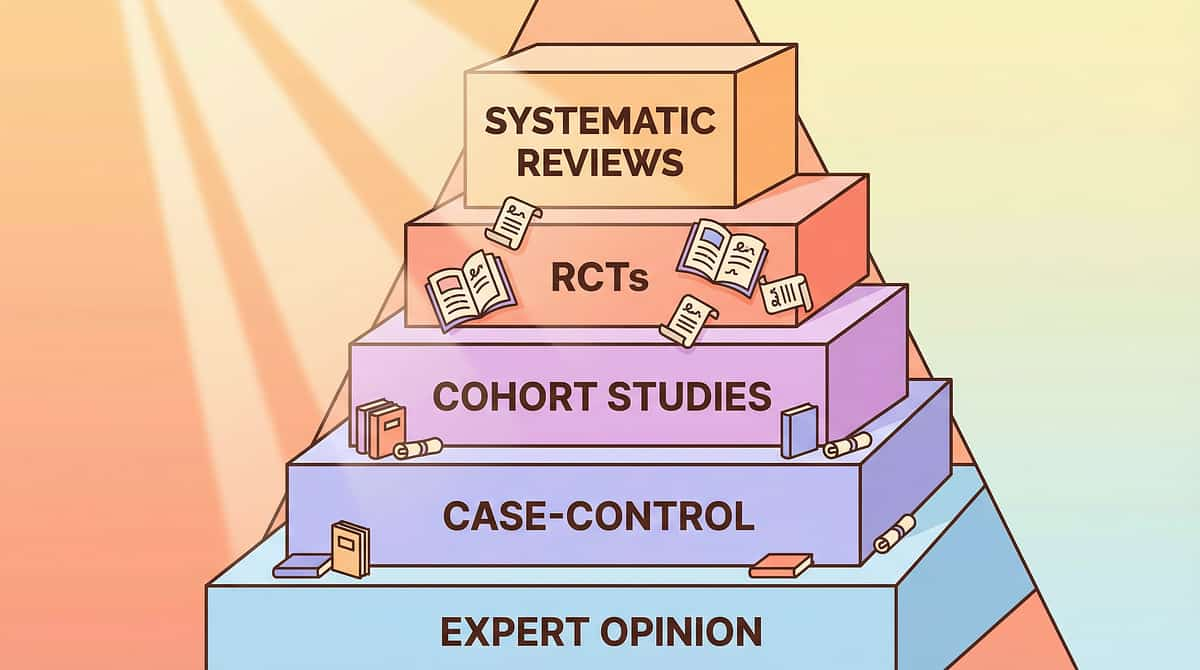
Of children with autism, per PRISMA Systematic Review, 2024
As their primary play mode — Wolfberg, Teachers College Press (2009)
Analyzing play development via Pinnacle GPT-OS® Real-World Evidence
"Social play difficulties affect the majority of children diagnosed on the autism spectrum. They are addressable. They are not permanent." — Pinnacle Consortium Clinical Team (OT + ABA + SLP + SpEd)
Citations: PMC11506176 | PMC10955541 | Wolfberg, P. (2009). Play and Imagination in Children with Autism.
For many children with autism or sensory differences, group play activates the brain's threat-detection system. The unpredictability of other children's movements, sounds, and intentions creates neurological overwhelm — not rudeness, not rejection. The nervous system says: "Too much. I'll do this alone where I'm safe."
- Mirror neuron system — lower activation during peer observation
- Amygdala — heightened threat response to unpredictable peer behavior
- Prefrontal cortex — limited theory of mind processing
- Sensory cortex — overwhelm from group play's multi-sensory chaos
- 🔊 Sensory overload — group play is too loud and chaotic
- 😰 Social anxiety — other children feel unpredictable or threatening
- 🔒 Rigid play patterns — others "ruin" how things should be done
- 🧩 Theory of mind gaps — difficulty reading others' play goals
- 💬 Communication challenges — can't negotiate play effectively
- 😞 Previous rejection — avoidance after social failure
- ❓ Play skill deficits — doesn't know HOW to play with others
Citation: Frontiers in Integrative Neuroscience (2020) | DOI: 10.3389/fnint.2020.556660 | Parten, M.B. (1932)

The WHO Care for Child Development Package, implemented in 54 countries, identifies responsive caregiving and structured play opportunities as the two most powerful drivers of social development progression. Understanding where your child sits on this trajectory is the first step to building the bridge forward.
Birth–12M | Normal
18M–2Y | Normal
2Y–3Y | Normal
3Y–4Y | Bridge Zone
4Y–5Y | Target
6Y+ | Life Goal
Citation: PMC9978394 | WHO/UNICEF CCD Package (2023) | WHO Developmental Milestones Framework

This technique carries Evidence Grade I — the highest tier, supported by Systematic Reviews, RCTs, and Meta-Analyses. Below are the four key pillars of evidence that underpin every session you'll run at home.
16 articles (2013–2023) confirm social skills intervention meets EBP criteria for ASD. Positive effects on peer interaction in 14/16 studies.
PubMed: PMC11506176
Across 24 studies, structured play interventions effectively promoted social skills (d=0.62), adaptive behavior (d=0.58), and sensory processing.
PMC10955541 | World J Clin Cases 2024
Home-based structured interventions by trained parents showed significant developmental outcomes comparable to clinic-based delivery.
DOI: 10.1007/s12098-018-2747-4 | Padmanabha et al.
Multi-caregiver training in structured play across 197 countries shows consistent gains in social participation indices.
PMC9978394 | WHO/UNICEF CCD 2023
Parent-Friendly Alias: "Building Bridges to Play Together"
A structured multi-material intervention that systematically builds a child's capacity for social play — starting from their existing solo play strengths and gradually introducing peer engagement using materials that reduce threat, increase predictability, and make social play structurally inviting. This is not about eliminating solo play — it's about expanding play repertoire so the child has both options.
15–20 min/session | 3–5×/week
8–12 weeks to measurable progression
2–8 years
OT • SLP • ABA • SpEd • NeuroDev
Cluster position:C-301 Parallel Play Only ← C-302 THIS TECHNIQUE → C-303 No Imaginative Play

The brain doesn't organize therapy by discipline. This child needs sensory safety, behavioral support, language scaffolding, and environmental structure — simultaneously. Pinnacle's FusionModule™ coordinates all five disciplines into one converged pathway.

Designs the sensory environment for shared play, assesses sensory triggers driving avoidance, and structures the physical environment for safe peer proximity. Leads sensory table setup and parallel play progressions.
Designs reinforcement systems for social play attempts, uses prompting hierarchies to build play initiations, implements data collection on peer play engagement, and programs reinforcement fading as intrinsic motivation develops.

Develops play scripts and role cards providing explicit language for joining and sustaining play. Targets pragmatic language: play invitations, turn-taking language, negotiating roles, and responding to peer bids.

Structures cooperative play for inclusion settings, adapts materials for classroom peer play, and trains school staff in supporting parallel-to-cooperative progressions.

Assesses underlying mechanisms (sensory processing, theory of mind, anxiety) driving solitary play preference. Guides pharmacological support if anxiety is significant. Monitors developmental trajectory.
Citation: DOI: 10.1080/17549507.2022.2141327 | Int J Speech-Lang Pathol (2022) | WHO NCF (2018)

Every session you run targets observable, measurable behaviors organized across three tiers. Primary targets are your session-by-session goals; secondary and tertiary targets are the broader developmental gains that accumulate with consistency.
Avoids all peer play — starting point
Can be near others without distress
Plays alongside peer with same materials
Interacts during play, some sharing
Shared goals, true collaboration
Moves between solo and social by choice
Citation: PMC10955541 | Meta-analysis: 24 studies on social skills, adaptive behavior, sensory processing outcomes

Clinically selected by the Pinnacle OT•SLP•ABA•SpEd•NeuroDev Consortium | Ages 2–8 | Home-deployable | Evidence-mapped
🎯 Solo play literally impossible — the activity requires a partner. Catch sets, partner puzzles, two-person balance activities. The toy itself requires partnership.
₹300–800 | DIY: soft ball catch | SHINETOY Shut The Box — ₹428 →
🎯 Predictable structure for shared play — making rules visible. Sand timers, visual turn-taking boards, whose-turn spinners. Concrete rules reduce overwhelm.
₹200–500 | DIY: "whose turn" cards, water bottle timer
🎯 Gradual transition from solo to shared. Art supplies at a shared table, modular building materials, connectable train tracks. Start side-by-side, gradually introduce sharing.
₹400–900 | DIY: shared art table with individual supplies
🎯 Concrete language for play participation. Visual cards: "Can I play?" "What are we building?" "Your turn!" When play language doesn't come naturally, scripts provide the words.
₹150–400 | Hospital Activity Sticker Book — ₹199 →
🎯 Sensory engagement creates natural proximity. Large sensory bins (rice, sand, water) big enough for two. Sensory focus reduces social demand — connect through senses first.
₹500–1,500 | DIY: large plastic bin with rice/water
🎯 Shared creation builds shared investment. Large block sets, team construction kits — projects that benefit from multiple builders. Scale up solo builders to shared construction.
₹600–2,000 | DIY: large cardboard box fort building
🎯 Role-based play creates structural need for partners — doctor needs patient. Doctor/patient sets, restaurant dramatic play, shop/customer scenarios.
₹400–1,200 | DIY: simple household props for two-person scenarios
🎯 Team versus game — removes competitive threat entirely. All players work toward shared goal. No winners/losers. Peer becomes ally, not opponent.
₹500–1,500 | Dyomnizy Memory Game — ₹519 →
🎯 External motivation builds the social play habit. Token boards, sticker charts for peer play attempts. When internal motivation is low, external rewards build the habit until intrinsic motivation develops.
₹100–400 | Reward Stickers 1800+ — ₹364 → | Reward Jar — ₹589 →
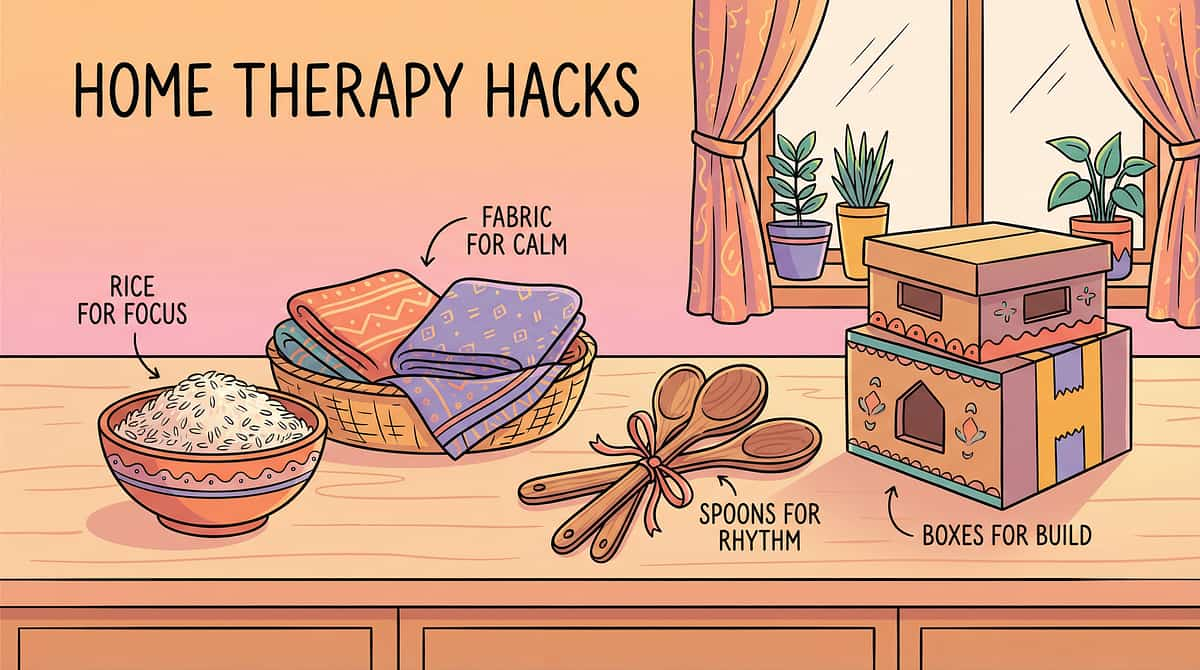
The WHO Nurturing Care Framework demands equity. No family should be excluded from evidence-based intervention due to cost. The therapeutic mechanism is not in the product — it's in the interaction structure the material creates. A cardboard box fort and a ₹2,000 building set activate the same shared creation neurology.
Material | 🛒 Commercial | 🏠 DIY Free Version |
Two-Player Games | Partner catch set ₹300–800 | Soft ball + rolled-up socks; balance beam from tape on floor |
Turn-Taking Visuals | Sand timer set ₹200–500 | Paper arrow card ("My Turn" / "Your Turn"), water bottle timer |
Parallel-Coop Materials | Modular building set ₹400–900 | Shared drawing paper, duplo/lego already owned, cardboard boxes |
Play Scripts | Printed card set ₹150–400 | Handwritten index cards with "Can I play?" phrases |
Sensory Materials | Sensory bin kit ₹500–1,500 | Large plastic tub + uncooked rice or sand from garden |
Building Sets | Cooperative block set ₹600–2,000 | Cardboard boxes + tape; large fort project |
Pretend Props | Doctor/restaurant set ₹400–1,200 | Household items: cups for restaurant, toy as patient |
Cooperative Games | Board game ₹500–1,500 | Modified card game: "Can we collect all cards together?" |
Reinforcement System | Token board kit ₹100–400 | Paper chart + stickers from any stationery shop |
Citation: PMC9978394 | WHO NCF Handbook (2022) — equity-focused intervention in 54 LMICs

- Child is in active meltdown or post-meltdown recovery (wait minimum 30 min)
- Child shows signs of illness, fever, or physical discomfort
- Peer partner is aggressive, unpredictable, or known trigger
- Child experienced a significant negative social event today
- You are highly stressed or emotionally depleted
- Child is tired but calm → shorter session, easier material level
- Child seems "revved up" → begin with sensory calming first
- Peer partner is unfamiliar → start with parent as partner
- Space is noisy or chaotic → use calmer corner, reduce scope
- Child is well-rested, fed, and in regulated state
- Environment is predictable and prepared
- 20 minutes of uninterrupted family time available
- Preferred reinforcer identified and ready
📞 If you observe concerning behaviors: 9100 181 181 | FREE 24×7
Citation: DOI: 10.1007/s12098-018-2747-4 | Padmanabha et al., Indian J Pediatr (2019)
Before a single material is introduced, the space itself must communicate safety. A well-prepared environment reduces sensory load, gives the child psychological control, and positions the parent as a calm anchor — not a hovering presence. Follow this checklist before every session.
Peer play requires full attention — no competition from TV or tablets
No setup during the session — the environment is ready, not chaotic
Psychological safety requires a visible escape — never a trapped feeling
We are expanding, not replacing — child's safe solo materials stay present
Available, not intrusive. Side, not above. Present, not staring.
Citation: PMC10955541 — 1:1 structured environment meta-analysis confirmation

The best session is one that starts right. A good 10-minute session beats a forced 30-minute struggle every time. Your child's nervous system will remember how play felt — make sure it feels safe. Run through all 7 indicators before proceeding.
# | Readiness Indicator | ✅ Yes — Proceed | ⚠️ No — Action |
1 | Child has been fed in last 2 hours | Go | Feed first, wait 15 min |
2 | Child is in regulated baseline state | Go | 5-min calming activity first |
3 | No meltdown in past 30 minutes | Go | Wait full 30 min minimum |
4 | Child shows no sign of illness | Go | Postpone until healthy |
5 | Preferred reinforcer identified | Go | Select reinforcer now |
6 | Play partner is calm and available | Go | Change partner or use adult |
7 | You (parent) are calm and present | Go | Take 5 deep breaths first |
Proceed to Step 1: The Invitation
Simplified version: parallel only, no peer, 10 min max
Calming activity today, try tomorrow

Children who prefer solitary play often feel ambushed by peer play demands. The invitation changes this. It positions social play as an option — not a requirement. The child retains control. Control reduces threat. Reduced threat enables approach.
Parent script (exact words):
"Hey, I've set up something that needs TWO people to work — do you want to try it with [peer name]?"
Wait 5–10 seconds. Accept any form of approach — even looking at the setup — as a "yes."
Show the game is "broken" without two players — demonstrate the incompleteness yourself. "See, I tried but I need someone."
Begin playing in the bin yourself, invite by proximity. "There's so much room in here."
Start building something clearly too large for one person. "This is going to need another builder."
Place the "Can I play?" card in child's hand before approaching peer — the card does the work.
📞 FREE play skills guidance: 9100 181 181
Parten's (1932) foundational research established the progression: Solitary → Parallel → Associative → Cooperative. You cannot skip steps. Attempting to force cooperative play before parallel play is like expecting a child to run before walking. We start with parallel — same space, same materials, own activity.
Both in play space with same type of materials. NO requirement to interact — each builds/creates their own.
"Arjun is building a tower! Priya is making a road!" Comment on proximity positively: "Two builders in the same space!"
Spontaneous glances, comments, or material reaching — these ARE connection attempts. Celebrate them quietly.
Child remains in shared space ≥3 minutes | Glances at peer's creation | Adjusts own play in response to peer | Vocalizes during parallel play (to self, parent, or peer)
Citation: Parten, M.B. (1932) | Wolfberg, P. (2009) Integrated Play Groups model

The specific therapeutic moment is when the material structurally requires or gently invites peer engagement. The parent's role is to position the material so cooperation is the path of least resistance — not forced, but architecturally inevitable.
Position catch set between both children. Demonstrate throwing to yourself doesn't work. The physics of catch creates the social structure. Duration: 5–10 throws = successful exposure.
Place timer/board in clear view. Parent runs first 2–3 turns to model. "Look — it's [child's name]'s turn!" Celebrate the wait as much as the turn.
At minute 3–4 of parallel play, place one shared element between them. "This track piece could connect both your buildings — who wants to try?"
Give child the script card right before peer opportunity. Whisper: "Want to try asking to join?" Support without forcing. Script reduces cognitive load of improvised social language.
Allow natural proximity. If child reaches across peer's space, narrate positively. Support child to respond to peer's questions (even with gesture).
Child actively engages with peer using material
Child tolerates peer, engages with material independently
Child leaves space, shows distress, refuses all contact
Duration of therapeutic exposure: 5–12 minutes core action phase | Citation: PMC10955541
Sensory integration and social skill research consistently shows: quality of exposure > quantity of trials. A child who genuinely tolerates 3 brief peer interactions has made more neurological progress than one who endures 15 forced, distress-filled ones.
Material | Target Reps | Each Rep Duration | Total Time |
Two-Player Games | 5–10 exchanges | 10–30 seconds | 3–5 min |
Turn-Taking | 3–5 turns each | 1–2 min each | 5–10 min |
Parallel Play | 1 sustained session | 5–10 min | 5–10 min |
Cooperative Building | 1 shared structure | 10–15 min | 10–15 min |
Sensory Bin | 1 shared session | 5–10 min | 5–10 min |
Play Scripts | 2–3 script uses | 30 sec each | 2–3 min |
Change the peer partner (sibling, same-age friend, adult) | Change the play theme within the same material | Change the physical location (indoors → outdoors) | Increase material complexity as tolerance builds
Decreased engagement with material | Increased physical distance from peer | Verbal "done/finish" signals | Repetitive behaviors increasing (self-regulation signal) → At any of these: move to cool-down

Reinforcement must be immediate (within 3 seconds), specific (what exactly you're celebrating), and enthusiastic (the energy signals importance). Reinforcement delivered 10 minutes later has almost zero behavioral impact.
"YES! You stayed right there with [peer name] — that was amazing!" + immediate preferred activity or sticker
"Did you just ask to play? That's incredible! That was so brave!" + token or verbal praise + preferred item
"You waited your whole turn! That's really hard and you did it!" + sticker on chart
"You said 'Can I play?' — that worked! Look, they said yes!" + celebrate jointly with peer
Always — the foundation of every reinforcement
30 sec of preferred solo activity as earned reward

Abrupt session endings create anticipatory anxiety for the next session. A child whose nervous system was activated by peer play proximity needs a structured return to baseline. The cool-down is not optional — it's the difference between a child who looks forward to the next session and one who dreads it.
Deep pressure: firm hug or weighted blanket (30 sec) | Proprioceptive: push hands against wall, 5 "elephant stomps" | Vestibular: 2 min of rocking or swinging | Visual: 2 min of preferred visual activity | Sensory: return to preferred solo play space
Use "first/then": "First we finish peer play, THEN you get your [preferred solo activity]." Avoid debate — the structure is the message.
Citation: NCAEP Evidence-Based Practices 2020 | Visual timer evidence for autism

ABA data collection standards require measurement of the behaviors targeted in each session. Without data, you cannot know if the intervention is working, what to adjust, or when to escalate. This is not bureaucracy — it is the foundation of evidence-based home therapy.
DATE: ___________
MATERIAL USED: _____________
DURATION: ___ min
1. Peer Proximity Tolerance
○ Left space immediately
○ Tolerated 1–3 min
○ Tolerated 3–5 min
○ Tolerated 5+ min
2. Social Play Engagement
○ No peer interaction
○ Brief glance/acknowledgment
○ Parallel play alongside peer
○ Initiated or responded to play
3. Distress Level
0 — Calm throughout
1 — Brief resistance, recovered
2 — Moderate distress, modified
3 — Significant distress, stopped
Your session data feeds the GPT-OS® Social Participation Index — tracking progression from exclusive solo play to flexible cooperative play. After 4 weeks of data, TherapeuticAI® generates a personalized progression recommendation.
This is your child's play development under clinical-grade surveillance, at home. When 50,000+ families record session data, GPT-OS® identifies which material sequences produce fastest progression for which child profiles.
Citation: BACB Guidelines | Cooper, Heron and Heward (Applied Behavior Analysis, 8th ed.)

When a session doesn't go as planned, that information is clinically valuable. Every challenge points to a specific mechanism — and every mechanism has a targeted fix. Use this troubleshooting guide before concluding that the intervention isn't working.
🔍Why: Peer felt too threatening too soon. Fix: Remove peer, use adult as partner for 2 more weeks. Ensure parallel phase before any peer introduction.
🔍Why: Still in parallel phase — this is normal and correct. Fix: Record as "parallel play achieved" — this IS the goal for early sessions. Don't push to cooperative yet.
🔍Why: Rigid play patterns + Theory of Mind gap. Fix: Use own-space building sets where each child has distinct territory. Cooperative building requires separate ownership zones first.
🔍Why: Reinforcer preference not accurately identified. Fix: Run a preference assessment — offer 5 items and observe which child approaches first.
🔍Why: Peer also needs preparation. Fix: Brief peer partner coaching: "If they come to you, say yes and show them what you're doing."
🔍Why: May need formal assessment. Action:📞9100 181 181 — speak to Pinnacle clinical team for AbilityScore® play skills assessment
Every child's solitary play preference is driven by a different underlying mechanism. Matching the intervention to the child's profile — rather than applying a one-size-fits-all approach — is what separates good outcomes from great ones.
Avoids group play due to sensory overwhelm (noise, movement, unpredictability)
- Start with sensory-compatible materials (bin, building sets)
- Quieter spaces, smaller peer groups (one peer)
- Longer parallel play phase before any cooperative expectation
Avoids group play due to social anxiety or previous negative experiences
- Start with adult as play partner — build confidence without peer risk
- Play scripts are especially important — reduce improvisation demands
- Cooperative games (shared winning) reduce competitive anxiety
- Ages 2–3: Focus on Materials 5 (sensory) and 1 (incomplete games) — language not yet available for scripts
- Ages 4–5: Add Material 4 (scripts) and 3 (parallel-to-cooperative progressions)
- Ages 6–8: All 9 materials applicable; emphasize Materials 7 (pretend) and 8 (cooperative games)
- Easier: Parent as partner; no peers yet; familiar home; preferred solo materials present
- Standard: One known peer; structured material; parallel phase first
- Harder: Two peers; less structured material; school or park setting
- Bad day: 5-minute session, parallel only
- Average day: 15–20 min full protocol
- Great day: 20–30 min, try next progression level
"If your child stayed in the shared space for 30 seconds longer than last session — that's real, measurable, neurological progress. The brain is forming new associations: 'peer presence = safe.' This takes repetition. Honor the small wins."
- Child enters shared play space without immediate distress
- Child tolerates peer's presence for ≥2 minutes
- Child engages with material while peer is present (even without interaction)
- Transition from session to next activity is smoother than week 1
- Spontaneous peer interaction
- Child-initiated play invitations
- Sustained cooperative play
- Comfortable peer play without adult facilitation
Session frequency: 3–5 sessions/week, 10–15 minutes each | Citation: PMC11506176 — 8–12 week outcome timelines

Weeks 3 and 4 mark the emergence of reliable, repeatable behavior patterns. The brain is beginning to encode "peer play = safe and possible." Watch for these consolidation indicators — they are the neurological green light to begin increasing session intensity.
The anticipatory dread is dissolving — this is significant neural change
Tolerance for peer proximity is becoming automatic, not effortful
The first seeds of genuine social interest — celebrate this moment
Language for social play is becoming available and accessible
Objective data confirms what you're already sensing: it's working
You may also notice:"You feel more confident too — your hands shake less, you laugh more during sessions. That's therapeutic competence developing. You are becoming your child's most important play therapist."

This is the phase where the work becomes visible to everyone — teachers, grandparents, neighbors. The neural architecture for social play is now established. What follows is the flowering of capacity built session by session over the preceding weeks.
Sustains parallel play 10+ minutes without distress | Independently enters shared space | Spontaneous vocalizations toward peer | Shares materials when offered
Engages in brief back-and-forth interaction | Responds to peer bids ("look at this!") | Play scripts becoming more fluid and less scripted-sounding | Occasionally initiates material sharing spontaneously
Participates in cooperative game following rules | Accepts shared victory/defeat without major distress | First instances of genuine collaborative play toward a shared goal

Behavioral science confirms: celebrating milestones is not sentimentality — it's reinforcement. When a parent celebrates progress, they reinforce their own intervention behavior AND the child's play development simultaneously.
Create a "Play Journey" visual board — photograph each material as it was mastered. "Look how far you've traveled from playing alone to playing together."
You have delivered evidence-based therapeutic intervention at home, consistently, across 8 weeks. That is clinical-grade dedication. Pinnacle's 97%+ improvement rate depends on parents exactly like you.
Call 9100 181 181 and share your outcome — Pinnacle's clinical team documents real-world results that drive research and help future families worldwide.
A child who moves from exclusive solitary play to sustained parallel or early associative play has demonstrated measurable neural plasticity. The Social Participation Index has moved. This is documented, trackable improvement.
The home programme is powerful — but it has a ceiling. Knowing when to escalate is not a sign of failure; it's a sign of clinical wisdom. Use this guide to make confident, informed decisions about next steps.
- Complete distress at ANY peer proximity (not improving after 4 weeks)
- Regression from previously achieved social play skills
- Aggressive response to peer play attempts (hitting, biting, throwing)
- No play engagement at all — unusual shutdown in both solo and social
- Play content involving concerning themes (persistent re-enactment of injury/harm)
- Signs of significant anxiety (sleep disruption, eating changes, excessive stimming)
- No measurable progress after 8–10 weeks of consistent 3–5×/week sessions
- Child plateauing at parallel play with no movement toward associative
- Child tolerates sessions but shows no generalization to natural settings
- Slow but consistent progress visible in session data
- Child shows any generalization (one spontaneous peer interaction outside sessions)
- Parent confidence improving and sessions feeling more natural
📞FREE National Autism Helpline: 9100 181 181 | 24×7 | AbilityScore® assessment available at all 70+ centers
C-302 sits at the core of the Social Development pathway — connecting the foundational work of parallel play with the more advanced skills of imaginative, sharing-based, and group play. Understanding where you are helps you navigate what comes next.
Foundation level — building awareness of other children
Playing alongside others without interaction
Bridging from exclusive solo play to social play
Building pretend and symbolic play with others
Advanced peer play integration and flexibility

If you have the C-302 materials, you already own everything needed for most related techniques. The Pinnacle 128 Canon Materials System is designed for maximum cross-technique efficiency — buy once, use across the entire domain.
Technique | Code | Level | Materials Overlap |
No Interest in Peers | C-300 | Intro | ✅ Same sensory materials |
Parallel Play Only | C-301 | Intro | ✅ Same all 9 materials |
THIS: Plays Alone | C-302 | Core | — |
No Imaginative Play | C-303 | Core | ✅ Same pretend props (Material 7) |
Can't Share During Play | C-304 | Core | ✅ Same cooperative games (Material 8) |
Can't Join Ongoing Play | C-305 | Advanced | ✅ Same scripts (Material 4) |

Your child's play development does not exist in isolation. It connects directly to language, sensory processing, emotional regulation, and behavioral self-regulation. GPT-OS® monitors all 12 developmental domains simultaneously so no area is left behind.
🎯 Active technique: C-302 Plays Alone
📊 Social Participation Index: Being tracked
🔗 Related techniques: Confirm via AbilityScore®
When you log session data (Card 20), it feeds the Social Participation Index. After 4 weeks of data, TherapeuticAI® assesses readiness for the next progression level across all 12 domains simultaneously — so no domain is left behind.
📞 FREE guidance: 9100 181 181

"She asked another child if they wanted to build together. I had to sit down. That's never happened before. She said 'Can I help?' with the card in her hand — and the other child said yes. Eight weeks of patience. Worth every session."
— Parent, Pinnacle Hyderabad Network | Child: 5 years | Diagnosis: ASD Level 1
"My son's solo play was magnificent — he'd build entire cities. I didn't want to take that away. These materials didn't. He still builds his cities. But now sometimes he lets his sister add a building. And occasionally he even asks her to."
— Parent, Pinnacle Bangalore Network | Child: 7 years | Diagnosis: ASD Level 2
"The sensory bin was the breakthrough. He'd never voluntarily get near another child. But when we both had our hands in the rice — he looked at her. That was the first look. From that look, everything grew."
— Parent, Pinnacle Chennai Network | Child: 4 years | Diagnosis: SPD + ASD features
Illustrative cases. Individual outcomes vary based on diagnosis, intervention intensity, and family participation. | 🏥 Pinnacle Blooms Consortium | 20M+ sessions | 97%+ measured improvement

WHO CCD Package implementation data across 54 countries shows that interventions delivered consistently by multiple caregivers produce 2.3× better outcomes than single-caregiver delivery. Community is not just support — it's a therapeutic multiplier.
50,000+ families navigating similar journeys across India and 70+ countries. Join the Play Skills Support Group for daily encouragement, material tips, and shared breakthroughs.
Evidence-based discussion moderated by Pinnacle consortium clinicians. Ask questions, share data, and get clinical-grade guidance from the community.
Monthly live sessions: "Using Play Materials at Home" by OT + ABA + SLP teams. Practical, real-time guidance from the clinicians who designed these protocols.
Follow @PinnacleBlooms for daily therapeutic content, material demonstrations, and family stories. #PinnacleBlooms #SolitaryPlay #PlaySkills #AutismParents
Citation: PMC9978394 | WHO CCD Package — caregiver community as protective factor for child development
- ✅ Steady progress visible in session data (4+ weeks)
- ✅ Child generalizing to at least one natural setting
- ✅ Parent confidence in protocol execution
- 🎯 AbilityScore® baseline — know exactly where child sits across all 12 domains
- 🎯 OT assessment — rule out sensory processing disorder
- 🎯 ABA assessment — behavior function analysis for severe peer avoidance
- 🎯 SLP assessment — pragmatic language evaluation
- 🎯 NeuroDev pediatrician — assess for ASD, anxiety, or other diagnoses
📞FREE National Autism Helpline: 9100 181 181 | 24×7 | 16+ languages
Andhra Pradesh | Telangana | Karnataka | Tamil Nadu | Maharashtra | Delhi NCR | And more
Can't reach a center? Pinnacle offers teleconsultation with licensed OT + SLP + ABA clinicians. Access clinical-grade guidance from home, on your schedule.
CIN: U74999TG2016PTC113063 | DPIIT: DIPP8651
Every material, every protocol step, and every timing guideline in C-302 is anchored in peer-reviewed evidence. For clinicians, researchers, and evidence-conscious parents, the full research base is transparent and accessible.
16 articles (2013–2023) confirm play-based and social skills interventions meet EBP criteria for ASD. Positive effects on peer interaction in 14/16 studies. PubMed: PMC11506176 →
24 studies. Social skills d=0.62, Adaptive behavior d=0.58. Structured intervention promotes social skills, sensory processing, and motor development. PubMed: PMC10955541 →
Home-based parent-administered intervention shows significant improvement in social responsiveness and adaptive behavior. Validates home delivery model. DOI: 10.1007/s12098-018-2747-4 →
Teachers College Press. Foundational evidence-based framework for guiding children with autism from solitary to cooperative play via structured peer support.
Joint attention and symbolic play in young children with autism. J Child Psychol Psychiatry. Targeted intervention significantly improves social play engagement.
Every session you log contributes to an adaptive intelligence system that gets smarter with every family that participates. Your child's data helps your child — and every child like them.
Comprehensive baseline across all 12 domains
Personalized progression recommendations
OT+ABA+SLP coordinated in one pathway
Daily home protocol auto-adjusted to child profile

The C-302 reel brings all 9 materials to life in under 90 seconds. Developed by the Pinnacle Consortium OT + SLP team, it demonstrates each material in real peer play scenarios — exactly as you'll implement them at home.
9 materials demonstrated with peer play scenarios, step-by-step parent guidance
Watch previous reel
Watch next reel
Citation: NCAEP EBP 2020 — Video modeling: evidence-based practice for autism | Multi-modal learning improves parent skill acquisition
WHO CCD Package implementation data across 54 countries: interventions delivered by multiple caregivers (both parents, grandparents, teachers) produce 2.3× better outcomes than single-caregiver delivery. Share this page with everyone who cares for your child.
📱 Share on WhatsApp
📧 Send by Email
🔗 Copy Page Link
URL: techniques.pinnacleblooms.org/social-development/child-plays-alone-C-302
"This child plays alone. That's okay — it's their comfort zone. We're helping them learn to also play with others, not instead of alone. These materials help. Please don't force them to play with others — let them approach when ready. Celebrate even tiny steps: 'You stayed near that child for 2 minutes — wonderful!'"
Download the Letter to School Teacher template — C-302 Play Programme Carryover. Plain language, visual format, ready to hand to any educator.
📞 Share this helpline with anyone supporting this child: 9100 181 181
Citation: PMC9978394 | WHO CCD Package — multi-caregiver training as intervention multiplier

No. Solitary play is developmentally normal through early toddlerhood and remains healthy in moderation. Concern arises with exclusive solitary play + active peer avoidance. This can reflect ASD features, sensory differences, social anxiety, or developmental delay. A formal assessment differentiates these. 📞 9100 181 181
Absolutely not. We're expanding their repertoire, not replacing it. The goal is a child who can play alone when they choose AND play with others when they choose. Their solo play skills are strengths — we're adding to them.
Observable changes in weeks 1–2: increased tolerance of shared space. Parallel play consolidation: weeks 3–4. Early associative play: weeks 5–8. Full cooperative play: 8–16 weeks with consistent intervention.
Match the material to the challenge: Sensory overwhelm → Material 5 (sensory bin) | Language barrier → Material 4 (scripts) | No interest → Materials 1 and 6 (incomplete games, cooperative building)
No. Essential starters: Materials 1, 2, and 5. These three cover the most common entry points. Add others as the child progresses and tolerance builds.
Essential. Never remove solo play opportunities. The programme requires maintaining solo play spaces alongside introducing shared play. Expanding the repertoire means preserving what exists.
Peer facilitation is half the intervention. Brief coaching for the peer: "When they come to you, say yes and show them what you're doing." For young children, adult as partner for the first 2–4 weeks is entirely appropriate.
Yes. These materials are beneficial for any child showing solitary play preference, regardless of diagnosis. If concern is significant, consult a developmental pediatrician. 📞 9100 181 181 for guidance.

Every material you've discovered, every session step you've learned, every safety check you'll run — it all leads to one moment: your child choosing to play with someone else. That moment is coming. You are the bridge builder.
Use the 6-step protocol (Cards 13–20) to run your first C-302 session. Everything you need is already in this guide.
Find your nearest Pinnacle center for AbilityScore® assessment and professional support across all 12 developmental domains.
C-303: No Imaginative Play — the natural next step for children who have mastered the social play bridge.
📞FREE National Autism Helpline: 9100 181 181 | Available 24×7 | 16+ Languages | Assessment | Guidance | Support
Preview of 9 materials that help when child plays alone Therapy Material
Below is a visual preview of 9 materials that help when child plays alone therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.





















"From fear to mastery. One technique at a time."
— Pinnacle Blooms Network® Consortium
India's largest autism and child development therapy chain. 70+ centers. 20M+ exclusive 1:1 therapy sessions. 97%+ measured improvement across Social, Sensory, Communication, Behavioral, Motor, and Cognitive domains. Empowering children from 70+ countries through GPT-OS® — the world's first Global Pediatric Therapeutic Operating System.
Medical Disclaimer: This content is educational and informational in nature. It does not constitute medical advice and is not a substitute for assessment by a licensed developmental pediatrician, psychologist, or occupational therapist. Solitary play preference may reflect autism spectrum disorder, social anxiety, sensory processing differences, developmental delay, or healthy introversion — each requiring different professional approaches. Some solitary play is developmentally normal and healthy. Results vary based on individual factors including underlying diagnosis, intervention intensity, and family participation. Consult qualified professionals for personalized guidance.
Statutory Identifiers: CIN: U74999TG2016PTC113063 | DPIIT: DIPP8651 (Govt. of India) | MSME: TS20F0009606 | GSTIN: 36AAGCB9722P1Z2
© 2025 Pinnacle Blooms Network® Pvt. Ltd. All Rights Reserved. GPT-OS®, AbilityScore®, TherapeuticAI®, FusionModule™, EverydayTherapyProgramme™ are proprietary marks of Pinnacle Blooms Network®.
🔄 Return to Top | ← C-301: Parallel Play Only | → C-303: No Imaginative Play | 🏠 Browse All Techniques
📞FREE National Autism Helpline: 9100 181 181 | pinnacleblooms.org | care@pinnacleblooms.org
While other children build together, negotiate, share — yours builds something magnificent. Alone. When anyone tries to join... they move away. 9 Materials That Bridge Solitary and Social Play. You are not failing as a parent. Your child's play is not broken — it's incomplete. The bridge can be built.