"He Licks Everything — Walls, Windows, Even People"
It's Tuesday morning. Your son is licking the kitchen counter again. Yesterday it was the car window. Last week, a metal railing at the park. Other parents stared. You pulled him away, wiped his mouth, and felt that familiar wave of fear — germs, chemicals, judgment.
You've tried saying no. You've tried distraction. But his tongue keeps seeking surfaces you'd rather it didn't find. This is not defiance. This is not a habit you created. Your child's tongue is doing exactly what his nervous system is asking it to do — seeking intense sensory input through the most receptor-dense organ in the human body.
There is a name for this. There is a science behind it. And there are nine specific materials that redirect this need — safely, hygienically, and effectively. You are not failing. Your child's nervous system is speaking.
Technique A-120
Safe Oral-Gustatory Redirection
Pinnacle Blooms Consortium — OT • SLP • ABA • SpEd • NeuroDev
Reference: WHO Nurturing Care Framework (2018)
You Are Not Alone: The Numbers
You are among millions of families worldwide navigating this exact challenge. Object licking is one of the most commonly reported oral-sensory seeking behaviors across pediatric therapy clinics globally. The SPD Foundation confirms that the tongue provides dual sensory input — gustatory (taste) and intense tactile feedback — making it the nervous system's preferred tool for concentrated sensory exploration.
80%
Sensory Challenges
Of children with autism display sensory processing difficulties
PRISMA Systematic Review, 2024
60–70%
Oral-Sensory Seeking
Of children with SPD show oral-sensory seeking behaviors
Sensory Processing Measure data
1 in 36
ASD Identification
Children in the U.S. identified with ASD (CDC, 2024); India estimates 1 in 100 — 18M+ children
CDC MMWR / INCLEN Trust India
This isn't rare. This isn't strange. This is neurology.
Evidence: PMC11506176 • PMC10955541 • DOI: 10.12998/wjcc.v12.i7.1260

What's Happening in Your Child's Brain
The Neural Pathway
Your child's tongue has the highest concentration of tactile receptors of any organ in the human body. It contains over 10,000 taste buds plus mechanoreceptors that detect pressure, texture, temperature, and vibration simultaneously.
When your child licks a wall, their insular cortex — the brain's taste-processing center — is under-stimulated and actively seeking input. The tongue delivers more concentrated sensory data per square centimeter than the fingertips.
Multi-Modal Seeking
Object licking is multi-modal sensory seeking: taste + texture + temperature + pressure — all through one action. The nervous system is trying to regulate itself. It's seeking, not misbehaving.
Tongue Receptors
Taste buds and mechanoreceptors detect multiple inputs
Cranial Nerves VII, IX, X
Signals travel through cranial nerves to the brainstem
Gustatory/Somatosensory Cortex
Brain processes taste, texture, temperature, and pressure
Arousal Modulation
Nervous system uses input to regulate alertness and calm
"This is a wiring difference, not a behavior choice."
Frontiers in Integrative Neuroscience (2020): DOI: 10.3389/fnint.2020.556660 • SPD Foundation
Where This Sits in Development
Object licking that persists beyond the toddler years is a clinical signal — not a disciplinary problem. The developmental window for intervention is wide, and earlier implementation yields stronger redirection outcomes. "Your child is here. Here is where we're heading."
0–6 Months
Oral exploration normative — everything goes to mouth
6–18 Months
Mouthing peaks and begins to decline naturally
18–36 Months
Typical mouthing decreases significantly; persistence signals processing differences
3–5 Years
Persistent object licking — key clinical window for intervention
5–12 Years
Without intervention, licking may intensify or become socially limiting
Comorbidity Awareness: Oral-sensory seeking commonly co-occurs with tactile defensiveness, auditory sensitivity, and food selectivity. 60%+ of children who lick objects also show chewing/mouthing behavior. Nutritional deficiencies (zinc, iron) can amplify oral-seeking — medical screening recommended.
WHO Care for Child Development Package (2023) • PMC9978394 • UNICEF MICS indicators

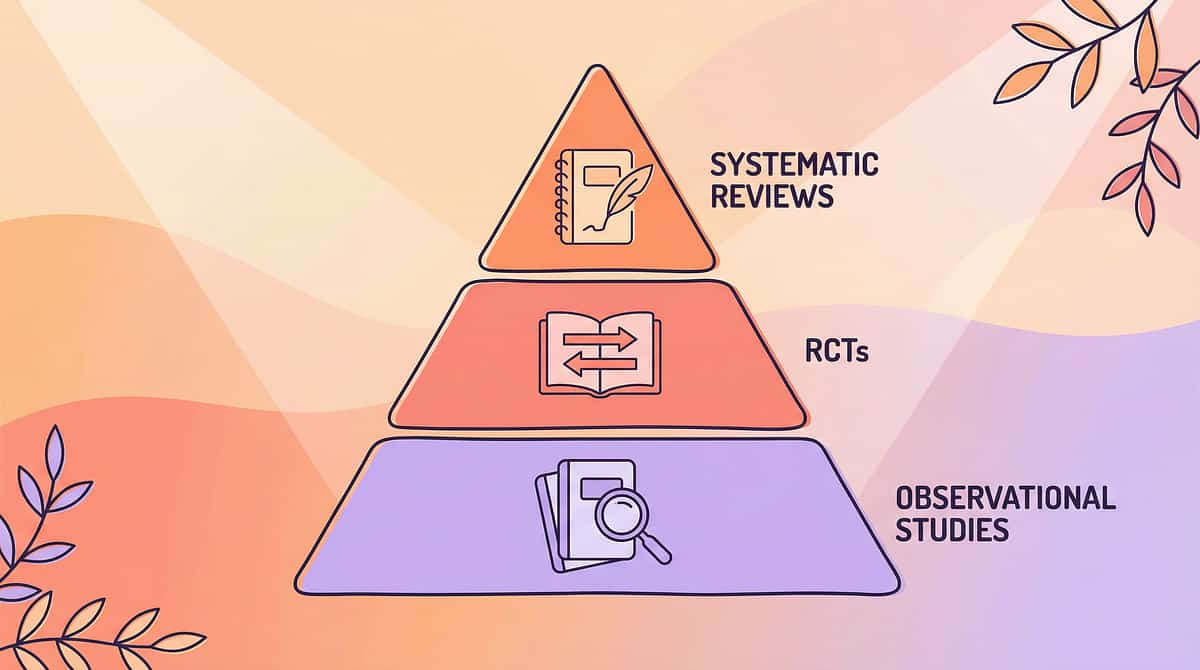
The Evidence Behind This Technique
Evidence Grade
Level II
Supported by systematic reviews, meta-analyses, and controlled studies
Confidence: 78%
"Clinically validated. Home-applicable. Parent-proven."
Key Research Findings
PRISMA Review (2024)
16 articles from 2013–2023 confirm sensory integration intervention meets evidence-based practice criteria for ASD
Meta-Analysis (2024)
Sensory integration therapy promotes adaptive behavior, sensory processing, and motor skills across 24 studies
Indian RCT (2019)
Home-based sensory interventions showed significant improvement in parent-administered sessions
NCAEP (2020)
Sensory integration classified as evidence-based practice for autism spectrum disorder
PMC11506176 • PMC10955541 • DOI: 10.1007/s12098-018-2747-4

Act II: Knowledge Transfer
The Technique: What It Is
Formal Name: Safe Oral-Gustatory Redirection Through Material Substitution
Parent-Friendly Alias: "Safe Licking Alternatives"
A structured sensory intervention that replaces unsafe object licking with clinically appropriate materials designed to deliver equivalent or superior gustatory (taste), tactile (texture), and thermal (temperature) input through the tongue. Rather than suppressing the licking behavior — which increases anxiety and redirects seeking to other potentially unsafe outlets — this technique honors the sensory need by providing nine categories of safe alternatives that satisfy the tongue's demand for concentrated sensory data.
Age Range
2–12 years
Duration
5–15 min per session
Frequency
2–3x daily + as needed
Protocol
8-week structured intro → maintenance
Sensory Processing (A)
Oral-Gustatory Processing
SEN-ORAL-GUST

Who Uses This Technique
"This technique crosses therapy boundaries because the brain doesn't organize by therapy type."
Occupational Therapy (OT)
Primary Lead. Assesses oral-sensory profile using standardized tools (Sensory Profile-2, Sensory Processing Measure). Designs the individualized oral-sensory diet incorporating safe licking alternatives. Calibrates material selection to match specific seeking patterns — flavor intensity, texture preference, temperature seeking.
Behavior Analyst (BCBA / ABA)
Develops functional behavior plan for licking redirection. Designs reinforcement schedule for choosing safe alternatives. Implements differential reinforcement of alternative behavior (DRA) and creates data collection systems for tracking redirection success.
Speech-Language Pathologist (SLP)
Addresses oral-motor function and tongue lateralization. Integrates licking alternatives into feeding therapy protocols. Monitors impact on oral-motor development and feeding readiness. Assesses tongue function beyond sensory seeking.
NeuroDev Pediatrician
Rules out nutritional deficiencies (zinc, iron) that amplify oral-seeking. Evaluates for pica vs. sensory-only licking. Monitors overall developmental trajectory and coordinates medication review if licking is anxiety-driven.
Adapted UNICEF/WHO Nurturing Care Framework for SLPs (2022) • DOI: 10.1080/17549507.2022.2141327

What This Technique Targets
Understanding exactly what this intervention addresses helps you measure real progress. The targets are organized from the core need outward, like rings on a bullseye — each building upon the one before.
Primary: Regulation
Child uses safe alternatives instead of environmental surfaces. Observable: unsafe licking decreases by 50%+ within 4 weeks.
Secondary: Safety & Social
Reduced pathogen exposure, less public embarrassment, child begins self-identifying sensory needs.
Tertiary: Growth
Oral-motor development strengthened, daily independence increased, caregiver stress significantly reduced.
PMC10955541: Meta-analysis confirms targets across social skills, adaptive behavior, sensory processing, and motor skills.

Materials Guide
What You Need: The 9 Materials
Each of these nine categories targets a specific dimension of oral-gustatory seeking. You don't need all nine to begin — start with Materials 1, 5, and 9 for an essential starter kit (₹300–1,500). Build out over time as you learn your child's preferences. Total comprehensive setup: ₹950–4,300.

1. Flavored Tongue Depressors & Licking Sticks
₹100–400 • Oral Motor Tools | Flavor-Based Sensory Tools
Safe, hygienic surfaces with varied tastes and textures for concentrated tongue input. Comes in fruit and sour flavors.

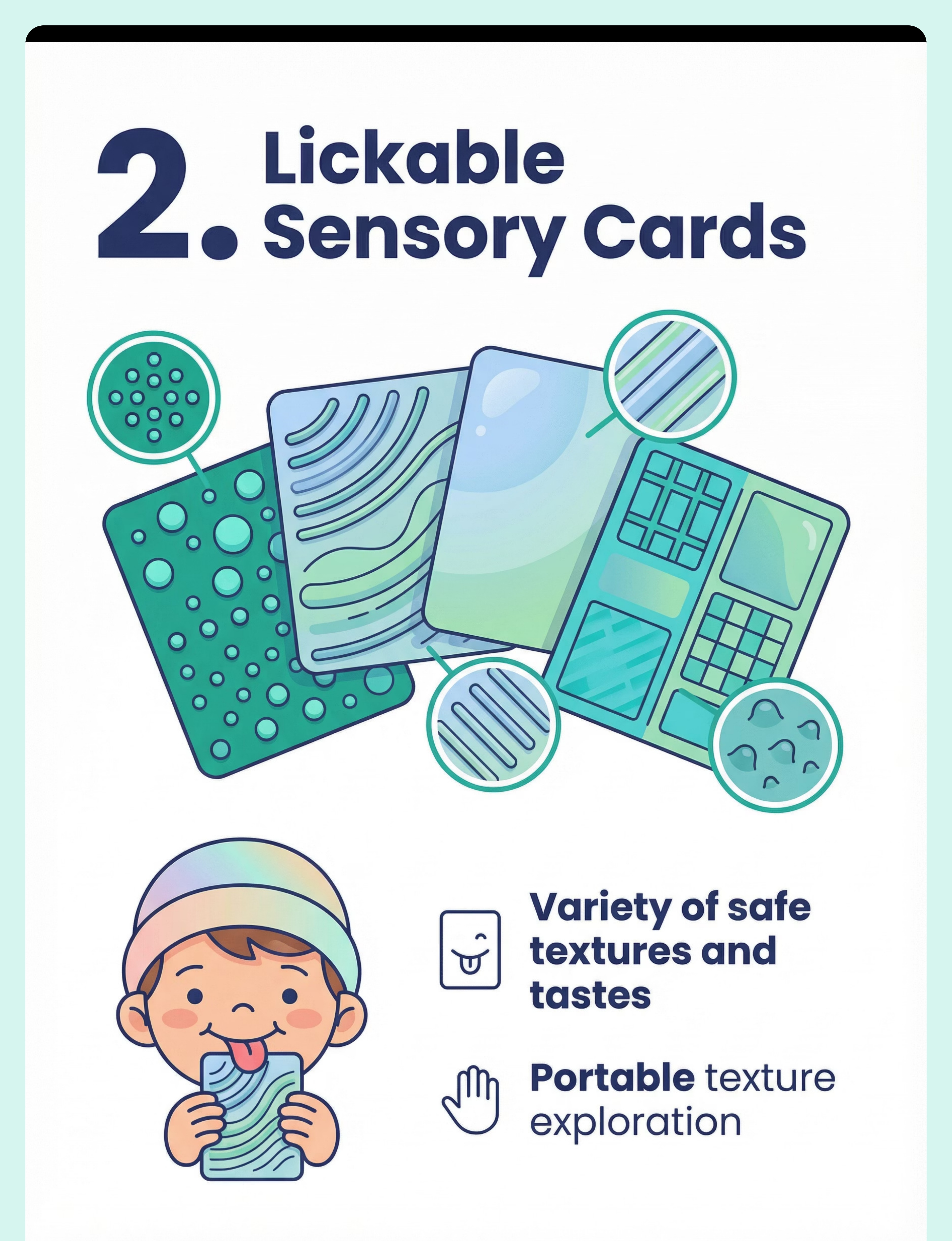
2. Lickable Sensory Cards & Surfaces
₹200–600 • Sensory Exploration Tools | Oral Motor Tools
Food-safe textured surfaces for portable tongue exploration. Vary in texture: bumpy, ridged, smooth, rough.
3. Frozen Treat Molds & Ice Options
₹100–500 • Sensory Regulation Tools | Temperature-Based Tools
Cold sensation + taste + texture = intense multi-sensory licking experience. DIY friendly with fruit juice.

4. Lollipops & Long-Lasting Licking Candy
₹50–300 • Flavor-Based Sensory Tools | Oral Motor Tools
Extended, socially acceptable licking with intense flavor delivery. Sour varieties provide especially strong input.
5. Food-Safe Silicone Licking Toys
₹200–800 • Oral Motor Tools | Sensory Chew/Lick Items
Washable, durable, designated safe licking objects with varied textures. Clinical-grade silicone is non-negotiable for aggressive seekers.

6. Edible Sensory Play Materials
₹100–500 • Sensory Play Tools | Multi-Sensory Integration
Licking incorporated into safe, playful exploration activities. Edible finger paints, taste-safe playdough, and sensory bins.

7. Lickable Flavor Sprays & Drops
₹100–400 • Flavor-Based Sensory Tools
Instant flavor on any safe surface — creates lickable opportunities anywhere. Sour, sweet, mint, and fruit varieties.

8. Metallic & Temperature-Varied Oral Tools
₹100–500 • Oral Motor Tools | Temperature-Based Tools
Stainless steel and temperature variation for material-specific seeking. Chill in fridge before offering.

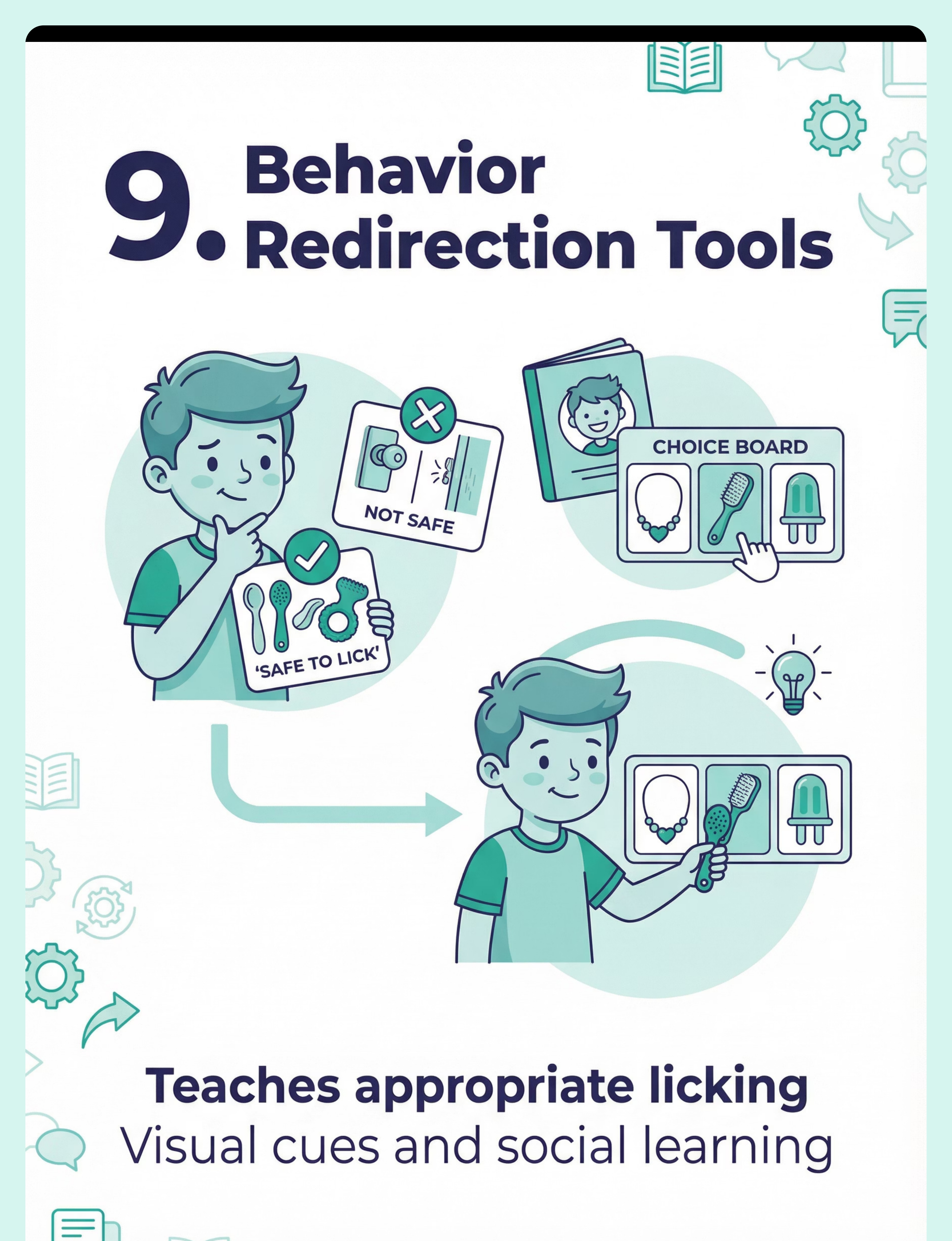
9. Licking Replacement Behavior Supports
₹0–300 • Visual Supports | Behavioral Tools
Visual cue cards, choice boards, and social stories for appropriate licking. Printable and DIY options available.

DIY & Substitute Options
"Not every family can order from Amazon. Not every village has same-day delivery. Here's how to start TODAY."
Buy This → Make This
- Flavored Sticks → Apply honey, jam, peanut butter, or yogurt to plain wooden tongue depressors or ice cream sticks from local shops.
- Sensory Cards → Adhere food-safe textured materials (silicone pot holders, textured placemats) to sturdy cardboard. Vary textures.
- Frozen Treats → Freeze fruit pieces (grapes, mango, berries). Make popsicles in kulfi molds or ice cube trays. Ice chips are free.
- Lollipops → Available at any local kirana store. Imli/tamarind for intense gustatory input. Sugar-free for frequent use.
- Silicone Toys → Repurpose food-safe silicone teething toys, ice cube trays with textures, or silicone baking molds.
More Zero-Cost Swaps
- Edible Play → Make edible finger paints from curd/yogurt with food coloring. Taste-safe playdough from besan flour or cooked rice.
- Flavor Sprays → Mix water with food-safe extracts (vanilla, rose, peppermint) in a small spray bottle. Nimbu pani for sour seekers.
- Metal Tools → Designate specific stainless steel baby spoons as personal "licking spoons." Chill in fridge 30 minutes before offering.
- Behavior Supports → Draw "safe to lick" vs. "not safe to lick" picture cards on paper. Write a simple social story on notebook pages.
Zero-Cost Version: Items 3 (ice), 4 (household spoons), 6 (kitchen ingredients), 8 (metal spoons), and 9 (hand-drawn cards) = ₹0
Caveat: For severe oral-sensory seeking or children who aggressively bite materials, clinical-grade silicone licking toys (Material #5) are non-negotiable for safety.
WHO Nurturing Care Framework (2018): equity-focused interventions • PMC9978394
Safety First: Before You Begin
Before offering any materials, run through this traffic-light safety check. Your child's safety always comes first — every single session.
🔴 DO NOT PROCEED IF
- Child is actively ingesting non-food items (may be PICA — requires immediate medical evaluation)
- Child has open sores, cuts, or infections in/around the mouth
- Child has known severe food allergies not cleared by physician
- Child has recently vomited or shown GI distress
- Materials haven't been verified for food-safety, choking hazard, or age-appropriateness
🟡 MODIFY & MONITOR IF
- Child has mild oral sensitivities alongside seeking (start with less intense options)
- Child is currently dysregulated or in meltdown (wait for baseline calm)
- Child has dental concerns (reduce sugary options, prioritize texture)
- Child tends to bite rather than lick (use only rigid, bite-resistant materials)
- Less than 30 minutes since a meal
🟢 PROCEED WHEN
- All materials verified as food-safe and age-appropriate
- Child is calm, alert, and in a regulated state
- Environment clean and free of competing sensory distractions
- Parent has selected 2–3 starting materials
- Allergies checked and cleared
🛑 Red Line Behaviors — STOP IMMEDIATELY: Child swallows non-food material • Tongue bleeding or injury • Severe gagging, choking, or breathing difficulty • Allergic reaction (swelling, rash, breathing changes) • Child becomes severely distressed and cannot be calmed within 5 minutes
DOI: 10.1007/s12098-018-2747-4: Indian Journal of Pediatrics RCT (2019) — home-based safety protocols
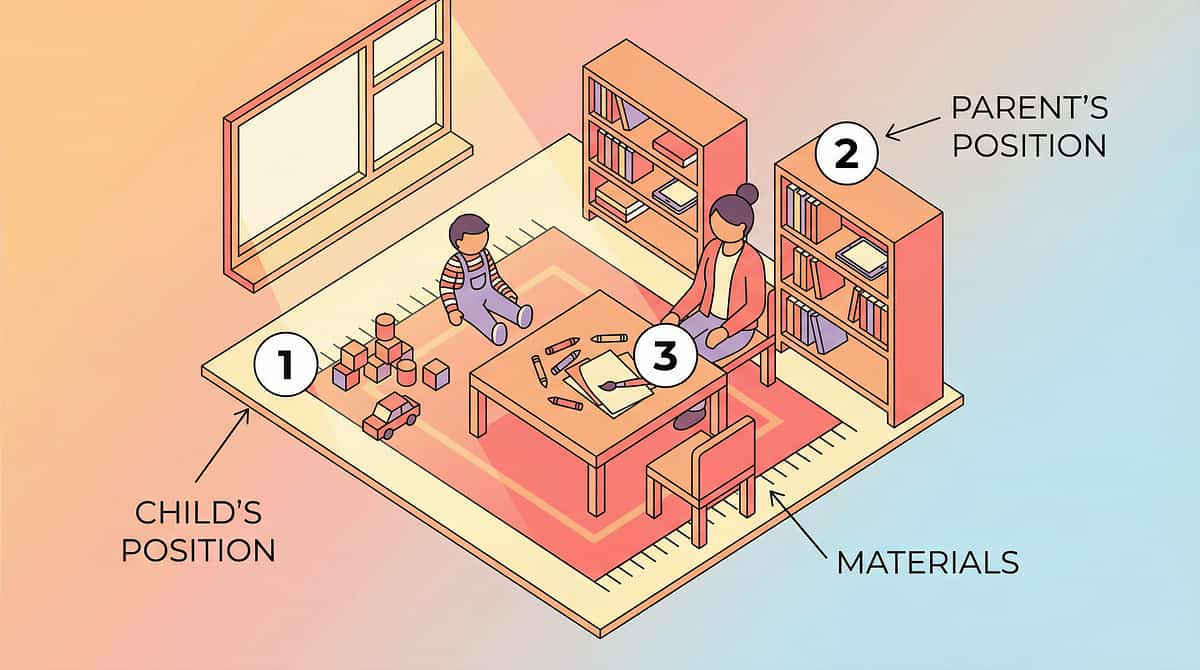
Set Up Your Space
A well-prepared environment is half the therapy. Here's how to arrange your session space for maximum effectiveness and safety.
Remove from Space
- Objects the child typically licks (cover or block access if possible)
- Competing sensory stimulation (TV, loud music, flashing lights)
- Other children who might distract or judge
- Cleaning chemicals or sprays near licking surfaces
Environment Settings
- Lighting: Natural or warm (avoid harsh fluorescent)
- Sound: Quiet or calm background music
- Temperature: Comfortable room temperature
- Surface: Clean, wipeable surface under materials
- Best time: Mid-morning or mid-afternoon (child alert, not hungry or tired)
- Avoid: Immediately after meals, during transitions, when dysregulated
PMC10955541: Structured 1:1 environment confirmed most effective • Ayres Sensory Integration Theory

Act III: The Execution
Is Your Child Ready? Readiness Check
"The best session is one that starts right." Before each session, run this 60-second pre-session assessment to determine if your child is in the right state to engage productively.
Fed Recently
Child has eaten within the last 2 hours (not hungry, not just finished eating)
Feeling Well
No signs of illness — no fever, nausea, or oral discomfort
Calm-Alert State
Not mid-meltdown, not drowsy, not hyperaroused. No meltdown in the last 30 minutes.
Materials Ready
At least 2 safe licking materials prepared. "Safe to Lick" visual card visible.
Parent Available
You are emotionally present — not rushed, not distracted, not frustrated
✅ All Green
Proceed to Step 1
🟡 1–2 Amber
Modify: offer one familiar safe option without structure
🔴 Any Red
Postpone: calming activity instead. Try again in 1–2 hours.

Step 1: The Invitation
Duration: 30–60 seconds
"Hey [child's name], I have something yummy/interesting for your tongue today! Want to see what's in the tray?"
Your Body Language
- Get down to child's eye level
- Use warm, playful tone — this is an invitation, not a demand
- Gesture toward materials tray with open palm (not pointing)
- Smile. Your energy sets the tone.
Reading the Response
✅ Acceptance: Child looks at tray, reaches toward materials, moves closer, or makes eye contact.
🟡 Hesitation: Child turns away → wait 10 seconds, try different wording. Child ignores → place most appealing material in their visual field.
🔴 Distress: Child becomes upset → postpone. This is not the right moment.
Already licking something unsafe? Calmly place safe alternative near the object being licked. Don't remove the unsafe object yet.
ABA Pairing Procedures: Establishing motivating operations before demand placement • OT "Just-Right Challenge" principle

Step 2: The Engagement
Duration: 1–3 minutes
Pick up one safe licking material. Hold it where the child can see it — about 30 cm from their face, slightly below eye level. Introduce it with enthusiasm and clarity.
"Look at this! This one tastes like [flavor/description]. Your tongue can explore this one. It's safe to lick!"
1
Present Slowly
Model first — lick the material yourself (if hygienic) or pretend with enthusiasm
2
Offer to Hand
Place in child's hand — don't put directly to their mouth. If hesitant, place on tray within reach.
3
Reinforce Instantly
The moment tongue touches safe material: "Yes! That's your licking stick! Your tongue loves that!"
✅ Engagement
Child takes material and begins licking — celebrate quietly ("You found it!")
🟡 Tolerance
Child holds material but doesn't lick yet — wait patiently, model again
🔴 Avoidance
Child pushes away or shows distress — try a different material; if all refused, postpone
PMC11506176: Structured material introduction meets evidence-based practice criteria

Step 3: The Therapeutic Action
Duration: 3–5 minutes
This is the therapeutic event — the tongue is receiving the concentrated sensory input it was seeking from unsafe objects, now through a safe channel. Allow the child to freely explore.
What to Do
- Sit quietly beside the child while they lick and explore
- Narrate occasionally: "Your tongue is finding bumpy parts!" / "That one is cold!"
- If child finishes one material, offer a second option from the tray
- If child reaches for unsafe object: "That one's not for licking. This one is!"
- Match the child's pace — brief or extended, both are valid
What NOT to Do
- Don't force the material into the child's mouth
- Don't remove the material if child is engaged (unless safety concern)
- Don't express disgust or discomfort with the licking
- Don't compare to "normal" behavior
- Don't restrict to one material if they want variety
Observe & Record
Note which materials preferred, duration of engagement, licking intensity, any unsafe attempts, and emotional state throughout.
Sensory Integration Theory (Ayres): Active, child-directed exploration produces superior outcomes vs. passive receipt • PMC10955541
Step 4: Repetition & Building
Duration: 2–5 minutes
Offer 2–3 different materials during each session. The variety is therapeutic — each material delivers different sensory data (flavor vs. texture vs. temperature), building a broader oral-sensory vocabulary.
1
Round 1: The Anchor
Child's preferred material — builds compliance and trust
2
Round 2: The Stretch
Introduce one new or less-preferred material — gentle challenge
3
Round 3: The Reward
Return to preferred material or child's choice — autonomy building
Mon: Taste + Temp
Flavored sticks + frozen treats
Tue: Texture Focus
Silicone toys + sensory cards
Wed: Multi-Sensory
Edible play + flavor sprays
Thu: Material + Flavor
Metal tools + lollipops
Fri: Child's Choice
Full collection — autonomy day
Progression Indicators: Child reaches for safe option before being prompted → PROGRESSING. Uses in new environment → GENERALIZING. Declines unsafe objects independently → SELF-MANAGING.

Step 5: Reinforce & Celebrate
Duration: 30–60 seconds
Reinforcement within 3 seconds of the desired behavior is the golden rule. Here's exactly what to say and do.
When Child Chooses Safe Material
"Amazing! You chose your licking stick! Your tongue knows what it needs!"
When Child Redirects
"You stopped and got your safe one! That was so smart!"
When Child Asks
"You told me what you need! Here's your licking tray!"
Reinforcement Menu
- Verbal praise (primary — use every time)
- High-five or preferred physical touch
- Extra time with preferred activity
- Sticker on a licking chart (visual tracker)
- Choice of next material to try
Token Economy (Ages 4+)
Each independent safe choice = 1 token. 5 tokens = small preferred reward. Track on a visual board near the materials tray.
"Celebrate the attempt, not just the success." If the child reached for the safe option — even if they changed their mind — that's progress worth acknowledging.

Step 6: The Cool-Down
Duration: 1–2 minutes
Transitions matter. A structured cool-down helps your child's nervous system shift gently from the sensory session back to daily life — and teaches them that sensory tools have a beginning and an end.
Transition Warning
"Two more licks, then we'll put the licking tray away."
Countdown & Close
"One more... and all done! Great licking session today!"
Cool-Down Activity
Offer water (transitions oral focus). Gentle face wipe with warm cloth. Deep breath: "Smell the flower 🌸... blow out the candle 🕯️"
Material Put-Away Ritual
"Let's put your licking tools back in their special box. You can use them again later." Child participates if able — builds routine and ownership.
Transition to Next Activity
"Your tongue got what it needed. Now let's [next activity]." If child resists: one more turn, then gently complete.
NCAEP (2020): Visual supports and transition strategies classified as evidence-based practices

Capture the Data: Right Now
"60 seconds of data now saves hours of guessing later." Within 60 seconds of session end, record these fields. Quick, simple, and essential for tracking what's working.
Field 1: Material Preference
Which material(s) did the child lick today? Check all that apply: Flavored Sticks • Sensory Cards • Frozen Treats • Lollipops • Silicone Toys • Edible Play • Flavor Sprays • Metal Tools • Behavior Supports
Field 2: Engagement Level
How long did the child engage? Less than 1 min • 1–3 min • 3–5 min • 5+ min
Field 3: Unsafe Attempts
How many unsafe licking attempts during session? 0 times • 1–2 times • 3–5 times • 5+ times
Bonus Field: Redirection success — when you offered the safe alternative after an unsafe attempt, did the child accept? Yes, immediately • Yes, after prompting • No, refused • N/A (no unsafe attempts)
BACB Guidelines + Cooper, Heron & Heward: Applied Behavior Analysis data collection standards

What If It Didn't Go as Planned?
Every unexpected outcome is data, not failure. Here are the most common challenges families face — and specific, research-informed fixes for each one.
Child refused all materials
Why: Materials may not match the specific sensory property being sought. Fix: Observe what the child IS licking. Cold surfaces → frozen treats and chilled metal. Rough surfaces → textured cards. Match the alternative to the seeking pattern.
Child licked once and went back to the wall
Why: Safe alternative wasn't intense enough. Fix: Increase intensity — stronger flavors (sour, spicy-safe), colder temperatures, multiple textures simultaneously. The alternative must be MORE satisfying.
Child became distressed during redirection
Why: Redirection felt like punishment. Fix: Place safe alternative NEAR the unsafe surface without removing the child. Let curiosity drive the transition. Never forcibly remove — replace, don't remove.
Child bites instead of licking
Why: Combined oral-motor needs. Fix: Add dedicated chewing tools alongside licking materials. Address both needs separately. See related technique A-96.
Family members think you're encouraging licking
Why: Misunderstanding the redirection principle. Fix: Share the family guide. "We're not encouraging licking — we're making it SAFE. The need exists whether we provide tools or not."
Child only wants one material
Why: Found their preferred sensory match. Fix: Celebrate it. One accepted alternative is infinitely better than zero. Introduce variety slowly over weeks, not days.
Licking increases at school or in public
Why: No access to safe alternatives in new environments. Fix: Create a portable licking kit (small pouch with 2–3 options). Coordinate with school/caregivers.
"Session abandonment is not failure — it's data."
Adapt & Personalize
No two children are the same, and this technique flexes to meet your child exactly where they are. Use these adaptation frameworks to calibrate the approach for your family's unique needs.
Easier Version
1 familiar material only. No redirection required — just availability. Parent initiates. No data tracking. For bad days, early stages, younger children.
Standard Version
2–3 materials in structured tray. Active redirection. Parent models and narrates. 3 data points tracked. 2–3 sessions daily + availability throughout day.
Advanced Version
Full 9-material collection. Child initiates independently. New environments (school, restaurants). Child teaches others. Data tracked by child with support.
By Seeking Intensity
Intense Seekers (licks constantly, across all surfaces): Increase flavor intensity — sour, mint. Use temperature extremes. Offer 4–5 sessions daily. Carry portable kit everywhere.
Moderate Seekers (specific surfaces or times): Match material to pattern. Focus around high-licking times. Standard intensity. 2–3 sessions daily.
By Age
- Ages 2–3: Parent-led entirely. Emphasis on frozen treats and edible play. Constant supervision.
- Ages 4–6: Introduce choice boards and visual supports. Begin self-selection.
- Ages 7–9: Portable kit independence. Social story focus. Peer awareness.
- Ages 10–12: Self-advocacy. Environmental management. Fade parental prompts.

Act IV: The Progress Arc
Week 1–2: What to Expect
25%
Progress
Awareness & Tolerance phase
What You'll See
- Child may initially reject safe alternatives — this is normal; novel items require adjustment
- By end of Week 1: Child tolerates at least 1 safe material without distress
- By end of Week 2: Child begins showing preference for specific material(s)
- Unsafe licking frequency may NOT decrease yet — you're adding, not yet replacing
Your Parent Milestones
- You've identified your child's primary seeking pattern (flavor? texture? temperature?)
- You've completed at least 10 structured sessions
- You're getting faster at setup and cleanup
- You're feeling less anxious when your child licks — because you have tools now
"I'm not sure this is working yet, but my child is at least holding the materials." — THAT IS PROGRESS. Neural pathways take time. 3–7 exposures for tolerance, 7–14 for preference.
Week 3–4: Consolidation
50%
Progress
Consolidation & Preference phase
This is the phase where neural pathways are strengthening. You'll begin to see the behavioral shifts that signal real change is happening beneath the surface.
Prompted Response
Child reaches for safe material when prompted within 5 seconds
Clear Preferences
Child shows hierarchy among materials (e.g., always picks frozen treats first)
Unsafe Licking Decreases
10–30% reduction in unsafe licking typical at this stage
Generalization Seeds
Child brings you a licking tool, points at or names the "licking tray," or shows materials to visitors
Adjust if needed: If unsafe licking hasn't decreased by Week 4 → increase to 4–5 sessions daily. If child shows boredom → introduce 2 new materials. If only one material works → that's fine; ensure it's always accessible.
"You may notice you're more confident too."

Week 5–8: Mastery Indicators
75%
Progress
Mastery & Generalization phase
Mastery isn't perfection — it's the point where your child's nervous system has built a reliable new pathway for meeting its oral-sensory needs safely. Here are the specific, observable criteria to look for.
Independent Selection
Child independently selects safe licking material at least 70% of the time when oral-seeking urge occurs
50%+ Reduction
Unsafe object licking has decreased by 50% or more from baseline
Multi-Setting Use
Child uses safe alternatives in at least 2 different settings (home + one other)
Sustained Engagement
Child maintains engagement with safe materials for 3+ minutes per session
Redirection Acceptance
80%+ success rate when prompted to use safe alternative
🏆 Mastery Badge: All 5 criteria met for 2 consecutive weeks = MASTERY UNLOCKED
If 3 of 5 met → continue 2 more weeks. Mastery in home but not other settings → focus on generalization. Full mastery → move to maintenance phase (tools available, sessions not structured).
PMC10955541: Mastery criteria derived from behavioral measurement standards • BACB mastery criteria

Celebrate This Win 🎉
"You did this. Your child grew because of your commitment."
You Identified
Your child's oral-sensory seeking as a neurological need, not a behavior problem
You Built
A structured environment with safe alternatives — over 40 sessions in 8 weeks
You Redirected
Without punishment, shaming, or frustration. With patience, tools, and love.
Your Child Has Tools
Literal, physical tools to meet their own sensory needs safely — everywhere they go
The germs concern is managed. The public embarrassment is reduced. Your child's nervous system is getting what it needs through channels you designed.
🎈Family Celebration Suggestion: Let your child choose a special activity today. Tell them: "Your tongue is so smart — it learned how to use its special tools! Let's celebrate!"
📸 Photo/Journal Prompt: Take a photo of your child with their preferred licking material. Write the date. In 6 months, you'll look back and see how far you've both come.

Red Flags: When to Pause
"Trust your instincts — if something feels wrong, pause and ask." Even as progress happens, stay vigilant for these specific warning signs that warrant professional attention.
🚩 Ingesting Materials, Not Just Licking
Pieces found in stools or child swallowing parts of tools. This may be PICA — stop non-food licking materials immediately. Consult pediatrician for nutritional screening (zinc, iron).
🚩 Tongue Injury or Mouth Sores
Bleeding, swelling, blisters, or persistent soreness. Material may be too rough or infection developing. Pause all licking activities for 48 hours. Consult if not improving.
🚩 Sudden Dramatic Increase in Licking
Unable to stop, licking during sleep, licking everything. May indicate medical issue, medication side effect, or severe anxiety. Contact NeuroDev Pediatrician before continuing.
🚩 Severe Distress During Redirection
Extreme meltdowns, self-injury, or aggression. Licking may serve an anxiety-regulation function. Pause structured redirection. Consult behavioral specialist for functional assessment.
🚩 No Progress After 8 Weeks
Zero acceptance of safe alternatives and no decrease in unsafe licking. Underlying function may differ. Request comprehensive oral-sensory evaluation from OT.
🚩 Unusual Accompanying Oral Behaviors
Excessive drooling, tongue thrusting, difficulty swallowing, or eating changes. May indicate oral-motor dysfunction or ENT issues. Refer to SLP + ENT.
📞Pinnacle Helpline: 9100 181 181 (FREE, 16+ languages, 24/7)
The Progression Pathway
This technique doesn't exist in isolation. It sits within a carefully mapped developmental journey. Here's where you are, what came before, and where you might go next based on your child's response.
Path A: Gustatory Seeking Persists
→ A-119: Seeks Strong Flavors
→ A-121: Food Texture Sensitivity
→ A-121: Food Texture Sensitivity
Path B: Other Oral-Motor Behaviors
→ A-96: Chews Non-Food Items
→ A-98: Puts Non-Food in Mouth
→ A-98: Puts Non-Food in Mouth
Path C: Anxiety-Driven
→ Behavioral Self-Regulation
→ Emotional Regulation Index
→ Emotional Regulation Index
Long-Term Goal: Child independently manages oral-sensory needs using self-selected safe tools across all environments, with zero unsafe object licking.

Related Techniques
Your child's oral-sensory journey connects to a broader ecosystem of techniques. Explore the ones most relevant to your family's needs.

A-96: Chews Non-Food Items
9 materials for safe chewing redirection when your child bites and chews objects beyond licking.

A-97: Mouths Objects
9 materials for oral exploration redirection when mouthing persists beyond typical developmental stages.

A-119: Seeks Strong Flavors
9 materials for intense gustatory seeking when your child craves extreme sour, spicy, or bitter experiences.

A-121: Food Texture Sensitivity
9 materials for expanding oral tolerance when food textures trigger avoidance or gagging.
Parent Support Techniques
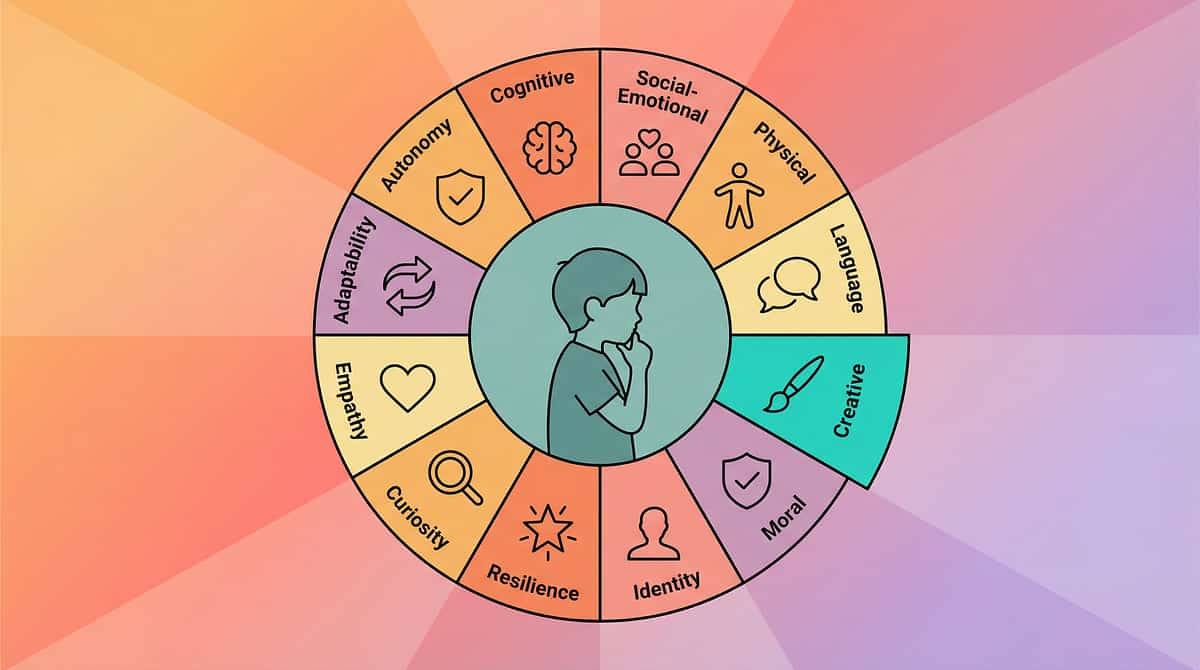
The Full Developmental Map
"This technique is one piece of a larger plan." Your child's development spans all 12 domains. Oral-sensory processing connects directly to communication, behavioral regulation, and daily living independence.
A — Sensory Processing ★
Current technique domain. Oral-Gustatory Processing sub-domain.
B — Communication
Oral-motor skills feed speech development directly.
C — Social Skills
Safe licking reduces social barriers and peer exclusion.
D — Behavioral Regulation
Self-managed seeking reduces dysregulation episodes.
H — Daily Living
Hygiene practices and independent sensory management.
K — Family Support
Caregiver confidence and reduced family stress.
WHO/UNICEF Nurturing Care Framework: Five components of nurturing care require holistic developmental monitoring
Act V: Community & Ecosystem
Families Who've Been Here
Arjun's Family — Hyderabad
Before:"Arjun (age 4) licked every metal surface — park railings, shopping cart handles, the kitchen sink. We were terrified of germs. We stopped going to parks."
After (Week 6):"We gave Arjun his own stainless steel 'licking spoon' and a pouch of flavored sticks. He carries his pouch everywhere. Last week, he reached for his pouch at the park instead of the railing. I cried."
Priya's Family — Bangalore
Before:"Our daughter (age 7) licked walls at school. Other children teased her. She was being excluded from group activities."
After (Week 8):"Her teacher reports she uses her silicone licking toy during class transitions. The teasing stopped because the tool looks like any other fidget. She was invited to a birthday party last month."
"Object licking redirection has one of the highest parent satisfaction rates among our sensory techniques. The shift from 'I can't stop him' to 'I gave him tools' transforms the family dynamic from fear to empowerment." — Senior Occupational Therapist, Pinnacle Blooms Network
Anonymized clinical narratives. Individual outcomes vary by child profile.

Connect with Other Parents
You're not navigating this alone. Thousands of families worldwide are on this same journey. Connecting with others who understand multiplies your resilience, your knowledge, and your hope.
Oral-Sensory Parent Group
WhatsApp community for families managing licking, mouthing, and chewing behaviors. Peer support, therapist Q&A, and material recommendations.
Pinnacle Parent Forum
Online discussion board with therapist moderation. Share wins, ask questions, find local resources.
Local Parent Meetups
Find your nearest Pinnacle center's parent support group for in-person connection and shared learning.
Peer Mentoring
Connect with an experienced parent who's been through this journey. Request through the helpline.
"Consistency across caregivers multiplies impact. Your experience helps others — consider sharing your journey."
WHO NCF: Community engagement is a core principle. Parent support networks improve intervention outcomes. PMC9978394
Professional Support: Find Your Team
Home implementation is powerful — and sometimes you need expert guidance to optimize, troubleshoot, or take the next step. Here's when and how to access professional support.
When to Bring In Support
- Tried this technique 8+ weeks with limited progress
- Red flags from the safety card are present
- You want a comprehensive oral-sensory evaluation
- You need an individualized sensory diet design
- You want your child's AbilityScore® assessment
Pinnacle Services Available
- ✅ Occupational Therapy — Sensory Integration focus
- ✅ Behavioral Therapy — Functional behavior assessment & DRA
- ✅ Sensory Integration Therapy — Oral-sensory diet design
- ✅ Parent Training — EverydayTherapyProgramme™
- ✅ AbilityScore® Assessment — Standardized baseline
📞 Free Helpline
9100 181 181
16+ languages, 24/7
16+ languages, 24/7
🌐 Find a Center
pinnacleblooms.org/centers
70+ locations
70+ locations
🗓️ Teleconsult
Book online
Free initial consultation
Free initial consultation
The Research Library
"Deeper reading for the curious parent." Every recommendation in this guide is grounded in peer-reviewed research. Here are the key studies that underpin this technique.
PRISMA Systematic Review (2024)
16 articles from 2013–2023 confirm sensory integration intervention as evidence-based for ASD.
PubMed: PMC11506176
PubMed: PMC11506176
Meta-Analysis (World J Clin Cases, 2024)
24 studies: Sensory integration therapy promotes social skills, adaptive behavior, sensory processing, and motor skills.
PubMed: PMC10955541
PubMed: PMC10955541
WHO Care for Child Development (2023)
Age-specific evidence-based recommendations for caregivers, implemented in 54 countries.
PubMed: PMC9978394
PubMed: PMC9978394
Indian RCT — Padmanabha et al. (2019)
Home-based sensory interventions demonstrate significant outcomes in parent-administered sessions.
DOI: 10.1007/s12098-018-2747-4
DOI: 10.1007/s12098-018-2747-4
Frontiers in Integrative Neuroscience (2020)
Comprehensive framework for evaluating sensory processing treatment in ASD.
DOI: 10.3389/fnint.2020.556660
DOI: 10.3389/fnint.2020.556660
Additional Sources: Dunn W. (1997) — Sensory processing impact on daily lives • Baranek GT. (2002) — Efficacy of sensory interventions • Schaaf RC & Lane AE. (2015) — Best-practice assessment protocol • SPD Foundation: spdfoundation.net
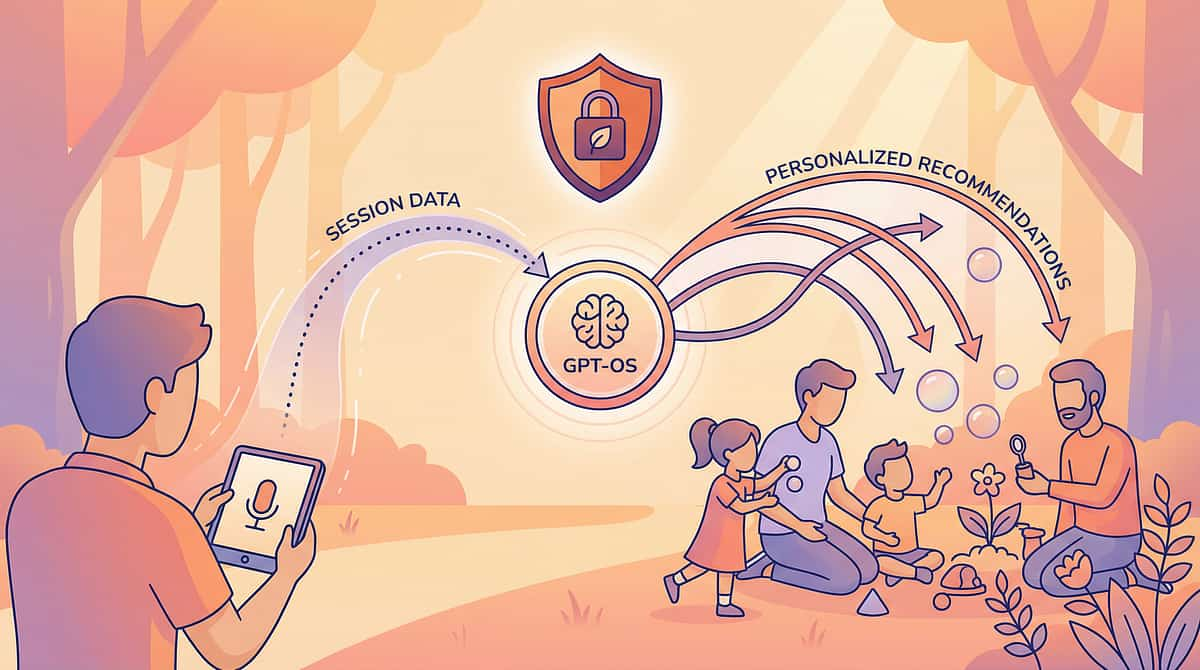
How GPT-OS® Uses Your Data
The session data you capture (from the data tracker) feeds into a powerful system that learns your child's unique patterns and optimizes recommendations over time. Here's how it works — and how your privacy is protected.
What GPT-OS® Learns
- Your child's oral-sensory preference profile (flavor, texture, temperature, material type)
- Optimal session timing and duration
- Redirection success patterns
- Progress trajectory relative to similar children
- When to recommend progression or adjustment
Privacy & Data Protection
- All data encrypted in transit and at rest
- HIPAA-equivalent privacy standards
- Data anonymized for population-level research
- Parent controls: view, download, or delete at any time
- No third-party sharing without explicit consent
"Your data helps every child like yours."
1. Awareness
Licking recognized as sensory need
2. Alternatives
Safe licking options introduced
3. Redirection
Child accepts alternatives when prompted
4. Self-Management
Child chooses safe options independently
5. Integration
Appropriate oral-sensory habits established

Watch the Reel
Episode 120
Sensory Solutions Series
A-120: "9 Materials That Help When Child Licks Objects"
Duration: 75 seconds | Domain: Sensory Processing → Oral-Gustatory Processing
Watch a Pinnacle senior occupational therapist demonstrate each of the 9 materials, showing safe licking techniques and real-time redirection strategies with a child.
🎬Video Embed: Reel A-120 — available on the Pinnacle Blooms Instagram, YouTube, and techniques portal.
Also Watch
A-96 Reel
9 Materials for Chewing Non-Food Items
A-97 Reel
9 Materials for Mouthing Objects
A-119 Reel
9 Materials for Seeking Strong Flavors
NCAEP (2020): Video modeling classified as evidence-based practice. Multi-modal learning improves parent skill acquisition.
Share This with Your Family
"If only one parent executes the technique, it's limited. Consistency across caregivers multiplies impact."
👴👵 Explain to Grandparents
"[Child's name] has a sensory need — their tongue seeks intense input. We've given them safe tools to satisfy this need. Offer these items when you see them licking walls or objects. Don't punish the licking — redirect to these tools. That's it!"
🏫 Teacher Communication Template
"Dear [Teacher], [Child's name] has an oral-sensory processing need that presents as object licking. We are working with Pinnacle Blooms on a structured redirection program. Please allow [child] to use their designated licking tools (stored in their bag) during transitions and free time. A visual cue card is included. Pinnacle Helpline: 9100 181 181."
📥Download: "Safe Licking Alternatives — A Quick Guide for All Caregivers" (1-page printable PDF)
PMC9978394: WHO CCD Package emphasizes multi-caregiver training for intervention generalization
Act VI: The Close & Loop
Frequently Asked Questions
Is licking objects dangerous?
Licking itself is a sensory behavior, not inherently dangerous. The risk comes from the surfaces — exposure to pathogens, chemicals, or toxic substances. Safe alternatives satisfy the need while eliminating the health risk.
Will providing licking tools make the behavior worse?
Research consistently shows the opposite. When sensory needs are met through appropriate channels, inappropriate seeking decreases. Providing tools isn't "encouraging" licking — it's managing it safely.
At what age should I be concerned?
Oral exploration is normative up to about 18 months. Licking that persists or intensifies beyond age 2, particularly if focused on specific surfaces, suggests processing differences. Intervention is most effective between ages 2–6 but works through age 12.
Should I stop my child or let them lick?
Neither — redirect. Stopping creates anxiety without addressing the need. Unlimited unsafe licking creates health risks. The Pinnacle approach: meet the need with safe alternatives while building awareness of safe vs. unsafe.
Could licking be a sign of pica?
Pica involves eating non-food items, not just licking. However, licking can progress toward ingestion. If your child swallows materials, consult a pediatrician immediately for nutritional screening and behavioral evaluation.
My child only licks cold or metal surfaces?
This indicates temperature-specific or material-specific seeking. Prioritize Materials 3 (Frozen Treats), 7 (Flavor Sprays on cold surfaces), and 8 (Metallic/Temperature Tools).
How long until I see results?
Most families see acceptance of at least one safe alternative within 1–2 weeks. Measurable decrease in unsafe licking begins around weeks 3–4. Full redirection (70%+ independent use) typically by weeks 5–8.
Can I use this without professional guidance?
Yes — this page provides everything for home implementation. Professional guidance is recommended if behavior is severe, pica signs are present, concurrent medical conditions exist, or no progress after 8 weeks. 📞 9100 181 181 (FREE).
Your Next Step: Start Now
You've read the science. You understand the need. You have the materials list. You know the protocol. The only step left is the first one.
Start This Technique Today
Scroll to the materials list — purchase or DIY your first 3 materials. Begin your first session tomorrow.
Book a Consultation
Schedule a free teleconsultation with a Pinnacle OT for personalized guidance. Or call: 9100 181 181
Explore Next Technique
A-119: 9 Materials for Seeking Strong Flavors, or browse all sensory techniques.
Validated by the Pinnacle Blooms Consortium — OT • SLP • ABA • SpEd • NeuroDev
Preview of 9 materials that help when child licks objects Therapy Material
Below is a visual preview of 9 materials that help when child licks objects therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.















Link copied!

The Pinnacle Promise
Pinnacle Blooms Consortium
"From fear to mastery. One technique at a time."
Every parent, everywhere, empowered with evidence-based, clinically validated intervention techniques — executed from home, powered by GPT-OS®, supported by the world's largest integrated pediatric therapy consortium.
Medical Disclaimer: This content is educational and informational. It does not replace assessment by a licensed occupational therapist, behavioral specialist, or pediatrician. Oral-sensory behaviors should be professionally assessed to rule out medical causes including nutritional deficiencies. Ensure all materials are food-safe and age-appropriate. Monitor for choking hazards. Individual results vary. Statistics represent aggregate outcomes across the Pinnacle Blooms Network.
Statutory Identifiers: © 2026 Pinnacle Blooms Network®, unit of Bharath Healthcare Laboratories Pvt. Ltd. All rights reserved.
CIN: U74999TG2016PTC113063 | DPIIT: DIPP8651 | MSME: TS20F0009606 | GSTIN: 36AAGCB9722P1Z2
CIN: U74999TG2016PTC113063 | DPIIT: DIPP8651 | MSME: TS20F0009606 | GSTIN: 36AAGCB9722P1Z2
🔗 All Techniques
📞 Free Helpline
9100 181 181
16+ languages, 24/7
16+ languages, 24/7
📧 Email
→ Next Technique