
He was potty trained. Then one automatic flush changed everything.
You're in a restaurant. Your three-year-old needs to use the bathroom. He sees the toilet — his body goes rigid, hands fly to his ears, and he's already screaming before anyone has flushed anything. Eight months ago, he used the toilet independently. Then one automatic flush at a hotel went off while he was sitting. Now every toilet is the enemy. He's back in pull-ups. He holds his poop for days. Your pediatrician says constipation is becoming a medical issue.
You are not failing. Your child's nervous system is speaking.
Pinnacle Blooms Consortium® | Sensory Solutions Series — Episode A-037
You Are Among Millions
Toilet flush fear is a documented manifestation of auditory over-responsivity — where the brain's sound processing system registers a sudden, loud, unpredictable sound as a genuine threat. The flush sound — sudden onset, 70–85 decibels in an enclosed bathroom, low-frequency rumble combined with rushing water — is one of the most commonly reported auditory triggers in pediatric sensory literature. You are among millions of families navigating this exact challenge. And there is a clear, evidence-backed path forward.
80%
ASD & Sensory Difficulty
of children with ASD experience sensory processing difficulties including auditory over-responsivity (PRISMA Systematic Review, 2024)
1 in 6
Worldwide
children worldwide experience developmental delays where sensory challenges are a primary barrier to daily functioning
40-60%
Toileting Regression
of toilet-trained children with sensory processing differences experience some degree of toileting regression following traumatic sensory events
Research Citation: PRISMA systematic review (2024): 80% of children diagnosed with autism display sensory processing difficulties. Meta-analysis: Sensory integration therapy effectively promotes social skills, adaptive behavior, and sensory processing (World J Clin Cases, 2024). References: PMC11506176 | PMC10955541

This Is Wiring, Not Willpower
The Neuroscience
When your child hears a toilet flush, their auditory cortex processes the sound. In a typically-wired brain, the amygdala stays calm — the sound is "loud but harmless." In your child's brain, the auditory cortex over-amplifies the signal. The flush arrives at the amygdala coded as "DANGER — SUDDEN, LOUD, UNPREDICTABLE." The amygdala triggers a full fight-or-flight response: adrenaline surges, heart rate spikes, muscles tense for escape. Your child is not choosing fear. Their nervous system is experiencing a genuine threat response to a sound their brain cannot yet process as safe.
What This Means for You
Your child saying "I know it can't hurt me but I'm still scared" is neurologically accurate. Cognitive understanding (cortex) and sensory-emotional response (amygdala) operate on different pathways. You cannot reason away an amygdala response. You can, however, systematically retrain it through controlled exposure, protection, and neural pathway rebuilding — which is exactly what this protocol does.
The traumatic automatic flush — sudden activation while your child was seated, vulnerable, pants down — encoded as a genuine threat event. The brain now treats ALL toilets as potential sources of that threat. This is a wiring difference, not a behavior choice.
Your Child's Challenge on the Developmental Map
Understanding where toilet flush sensitivity sits in your child's developmental journey helps you respond with both urgency and patience. The peak vulnerability window spans ages 2–6 — precisely when children are building toileting independence. A disruption here has cascading effects, but also a clear rehabilitation pathway.
18–24 Months
Toilet awareness begins — child notices elimination, may show interest in toilet
Age 2–3
Active toilet training begins — most children start using toilet with support
⚠️ Age 2–6: PEAK VULNERABILITY
Prime window for auditory-sensory toilet events and toileting regression following trauma
Age 4–5
Expected: independent toileting including flushing and public restroom use
Age 7–10
Full toileting independence including nighttime and unfamiliar environments; residual sensitivities managed
Comorbidity Awareness: Toilet flush fear commonly co-occurs with sensitivity to hand dryers, vacuum cleaners, fire alarms, and general auditory defensiveness. Addressing this specific trigger builds the foundation for broader auditory tolerance. References: WHO/UNICEF CCD Package (2023) | PMC9978394

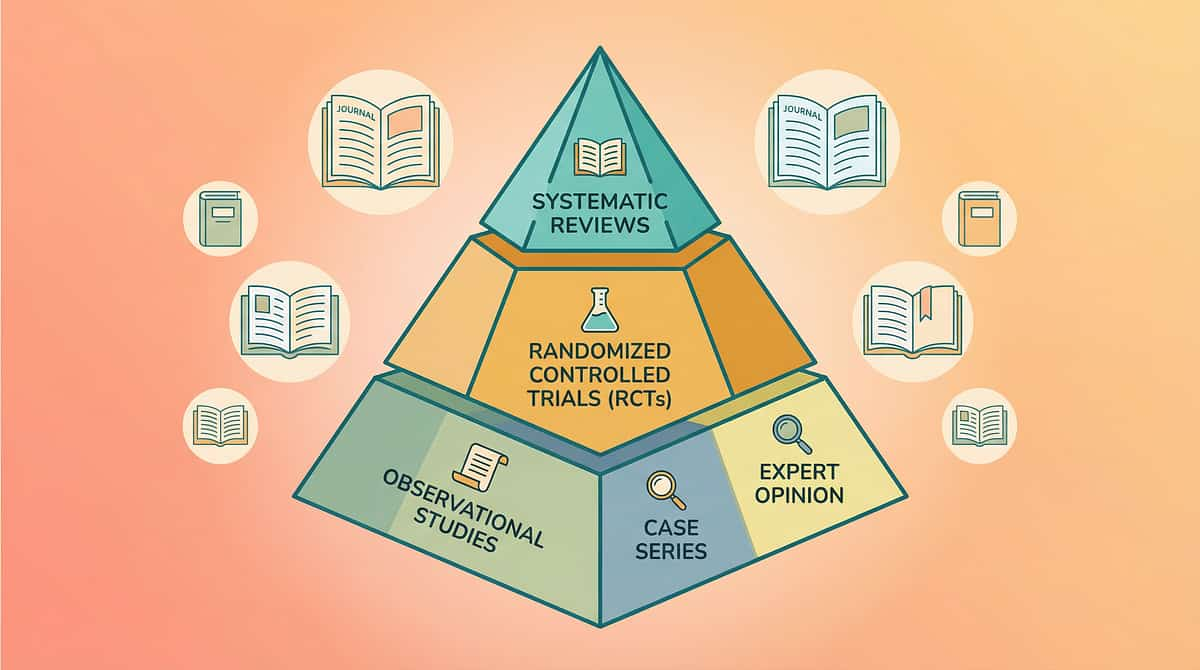
Evidence Grade: Level II — Systematic Review + Clinical Consensus Supported
This desensitization protocol is not guesswork. It is built on a robust, multi-source evidence base spanning systematic reviews, meta-analyses, randomized controlled trials, and real-world outcomes across 20M+ therapy sessions.
🛡️ Systematic Review (2024)
A PRISMA-model review of 16 articles (2013–2023) confirms sensory integration intervention meets evidence-based practice criteria for children with ASD. Auditory processing interventions using graduated exposure demonstrate measurable outcomes. PMC11506176
📊 Meta-Analysis (2024)
24 studies confirm sensory integration therapy effectively improves sensory processing, adaptive behavior, and daily living skills. Home-based protocols demonstrate significant outcomes when parent-administered with professional guidance. PMC10955541
🔬 Indian RCT (2019)
Home-based sensory interventions administered by trained parents in Indian pediatric populations demonstrated significant outcomes, establishing feasibility and efficacy in the Indian context. Padmanabha et al., Indian J Pediatr, 2019
🏥 Pinnacle Real-World Evidence
20M+ exclusive 1:1 therapy sessions across 70+ centers with 97%+ measured improvement rate — including Toileting Independence Index and Auditory Processing Index domains within GPT-OS®.
Clinically validated. Home-applicable. Parent-proven. AOTA, SPD Foundation, and NCAEP classify systematic desensitization and environmental modification as evidence-based practices for auditory over-responsivity.

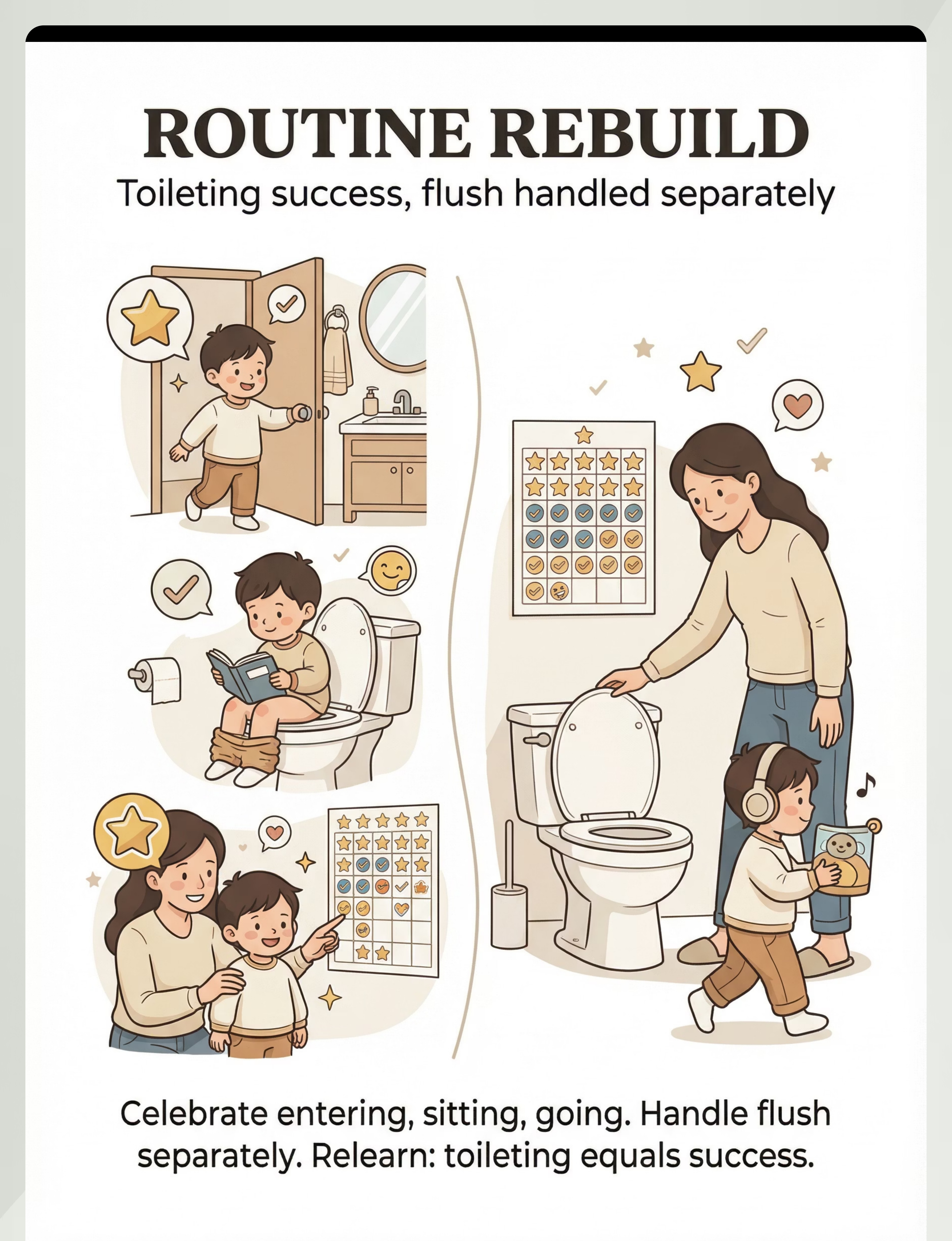
Toilet Flush Fear Desensitization Protocol
Parent-Friendly Name: "The Flush Safety Rebuild"
Technique ID: A-037
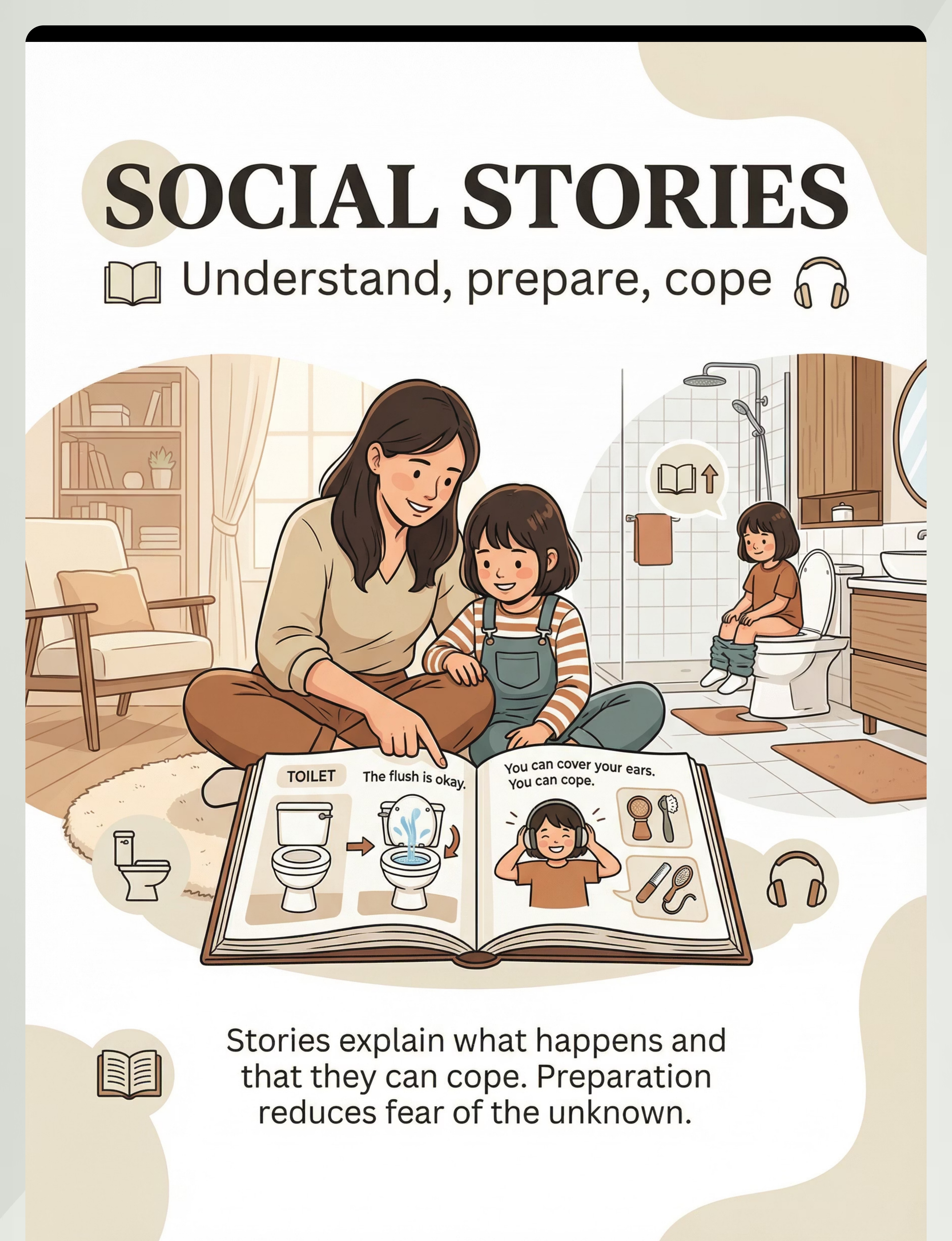
A structured, multi-material intervention protocol that restores functional toileting in children who have developed fear of toilet flushing sounds — particularly following traumatic automatic toilet experiences. The protocol combines immediate protective accommodations (sensor covers, noise-canceling headphones, countdown systems) with systematic graduated exposure to rebuild auditory tolerance and toileting confidence.
Unlike forced exposure approaches that worsen fear, this protocol prioritizes: Protection → Control → Gradual Tolerance → Independence.
Domain
Sensory Processing — Auditory | Sensory Regulation | Emotional & Behavioral Regulation | Daily Living & Self-Care
Age Range
2–10 years
Session Duration
5–15 min/session (graduated)
Frequency
Daily — integrated into natural toileting routine

Your Child's Multidisciplinary Team
Toilet flush fear sits at the intersection of sensory processing, behavior, communication, and medicine. No single discipline owns this problem — which is exactly why a team approach produces the best outcomes. Here's who does what and why each role matters.
Occupational Therapist (PRIMARY LEAD)
Assesses the child's sensory processing profile, designs the individualized desensitization protocol, and monitors auditory tolerance progression. The OT understands WHY the flush sound is neurologically threatening and designs graduated exposure to work WITH the nervous system.
Board Certified Behavior Analyst (BCBA)
Designs reinforcement systems, builds the positive toileting routine, implements systematic desensitization using ABA principles, and structures data collection for objective progress tracking. The BCBA ensures each step is reinforced and the child's behavior tells us what's working.
Speech-Language Pathologist (SLP)
Supports social stories and narrative comprehension. Develops communication scripts for the child to express fear and request accommodations. Essential when co-occurring communication challenges make expressing fear difficult.
NeuroDevelopmental Pediatrician
Monitors medical complications from toileting avoidance — constipation, encopresis, UTIs, bladder dysfunction. Assesses whether the anxiety component requires pharmacological support and validates the neurological basis of the fear response.
"This technique crosses therapy boundaries because the brain doesn't organize by therapy type."
Precision Targeting — Not a Random Activity
Every element of this protocol is designed to hit specific, measurable outcomes. Understanding the targets helps you recognize progress even when it feels invisible — and confirms you're working on the right things in the right order.
Observable behavior indicators of success include: child enters bathroom without distress signals, sits on toilet without pre-emptive ear covering, remains seated during flush (with or without protection), initiates flush independently, uses unfamiliar toilets with accommodation support, and stool/urine holding behavior is eliminated with a regular elimination pattern restored.

Your 9-Material Toolkit — Everything You Need
This protocol uses nine categories of materials — most of which cost nothing or next to nothing. Every family, everywhere, can implement the core protocol today. Items marked ESSENTIAL STARTER are the highest priority.
Toilet Sensor Covers / Flush Blockers
Canon: Toileting Visuals & Supports | Cost: ₹0–300
Post-it notes work perfectly. Purpose-made reusable silicone sensor covers available online. 🏷️ ESSENTIAL STARTER
Post-it notes work perfectly. Purpose-made reusable silicone sensor covers available online. 🏷️ ESSENTIAL STARTER
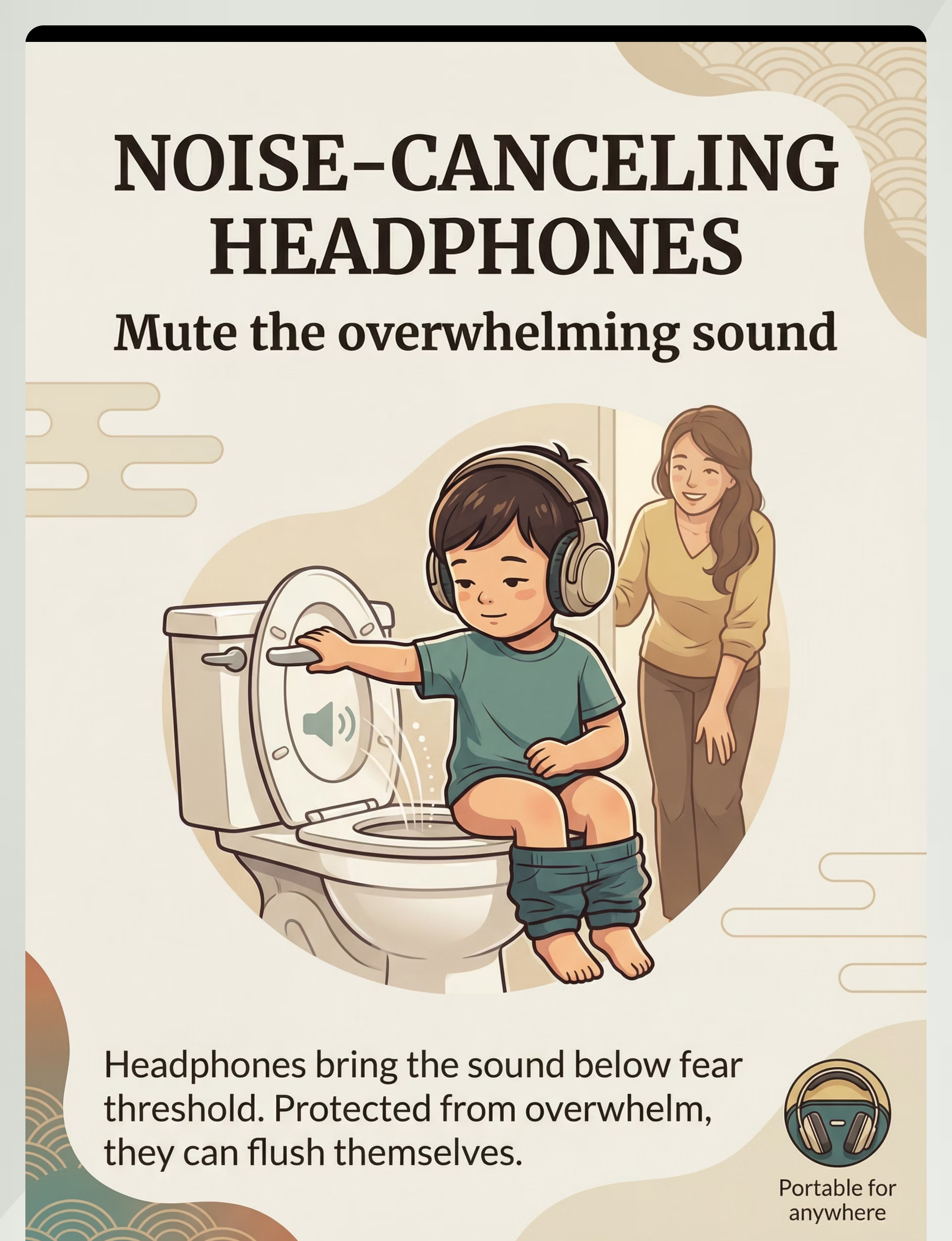
Noise-Canceling Headphones / Ear Defenders
Canon: Noise-Reducing Headphones/Ear Defenders | Cost: ₹1,500–8,000
🏷️ ESSENTIAL STARTER
🏷️ ESSENTIAL STARTER
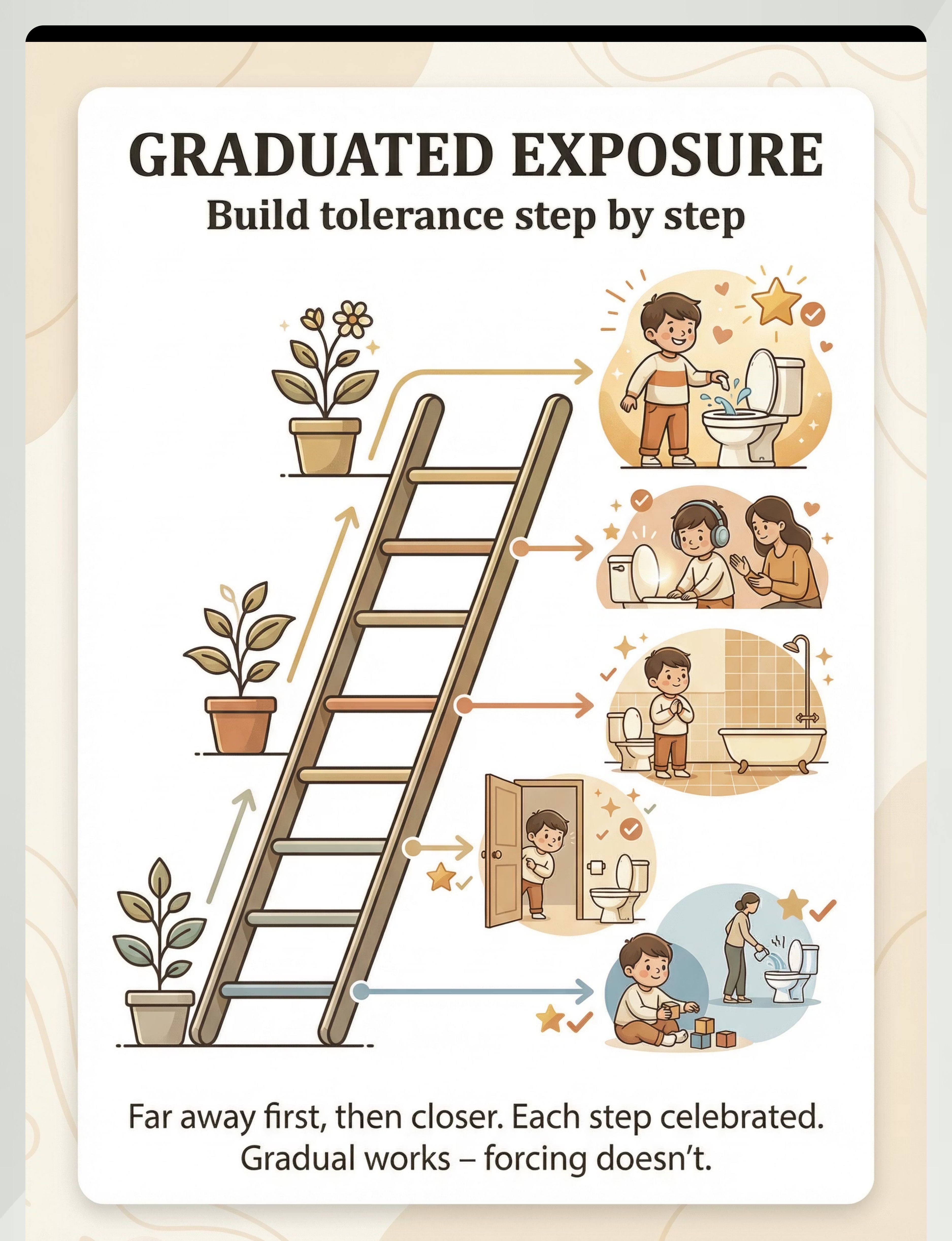
Graduated Exposure Protocol Materials
Canon: Visual Schedule System | Cost: ₹0 (printable)
Visual ladder chart + sticker reward system
Visual ladder chart + sticker reward system
Social Stories About Toilets and Flushing
Canon: Social Stories/Narrative Supports | Cost: ₹0–500
🏷️ Pinnacle Recommends
🏷️ Pinnacle Recommends
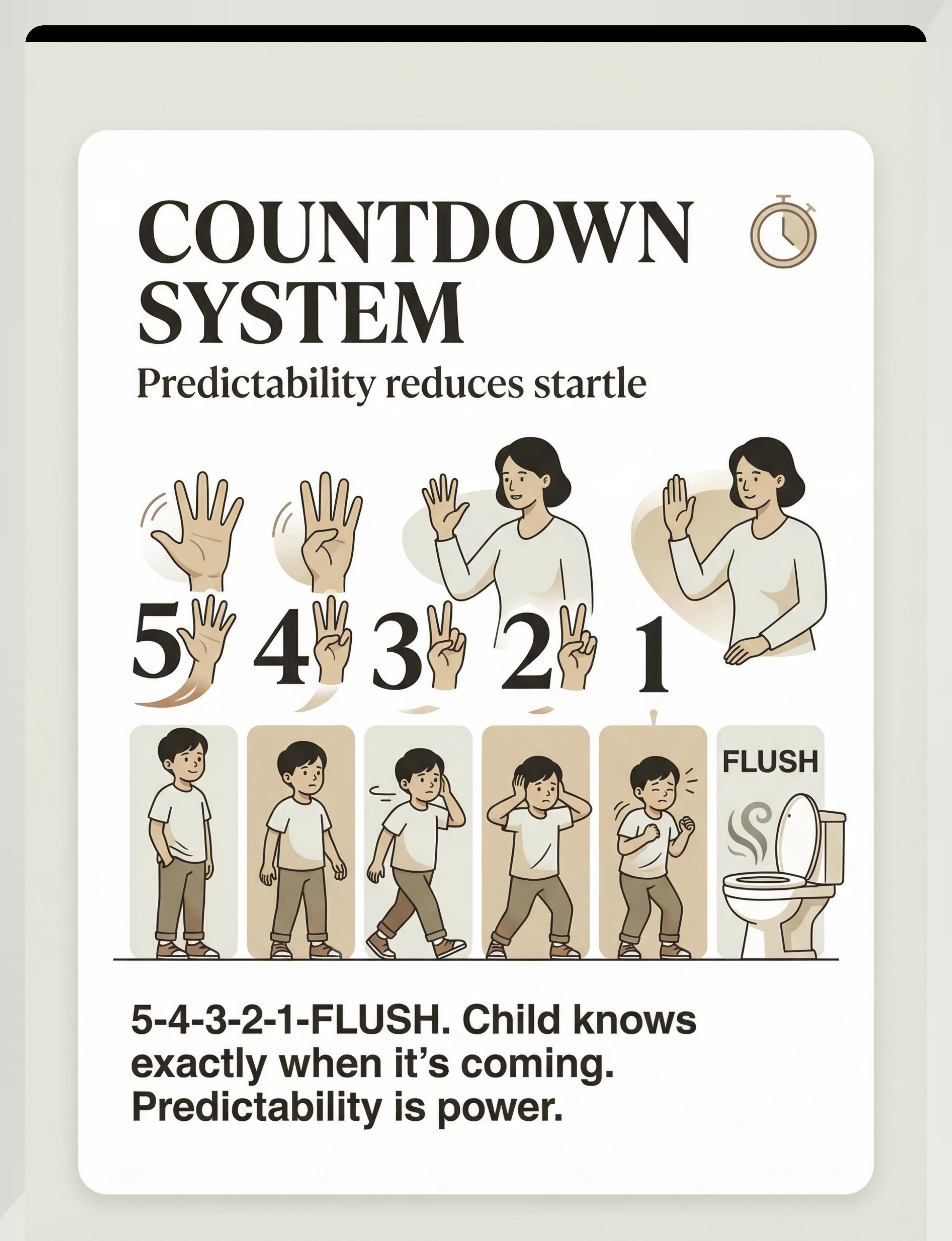
Countdown and Warning System
Canon: Transition Warning Cards/Cues | Cost: ₹0 (finger counting) – ₹200 (visual cards)
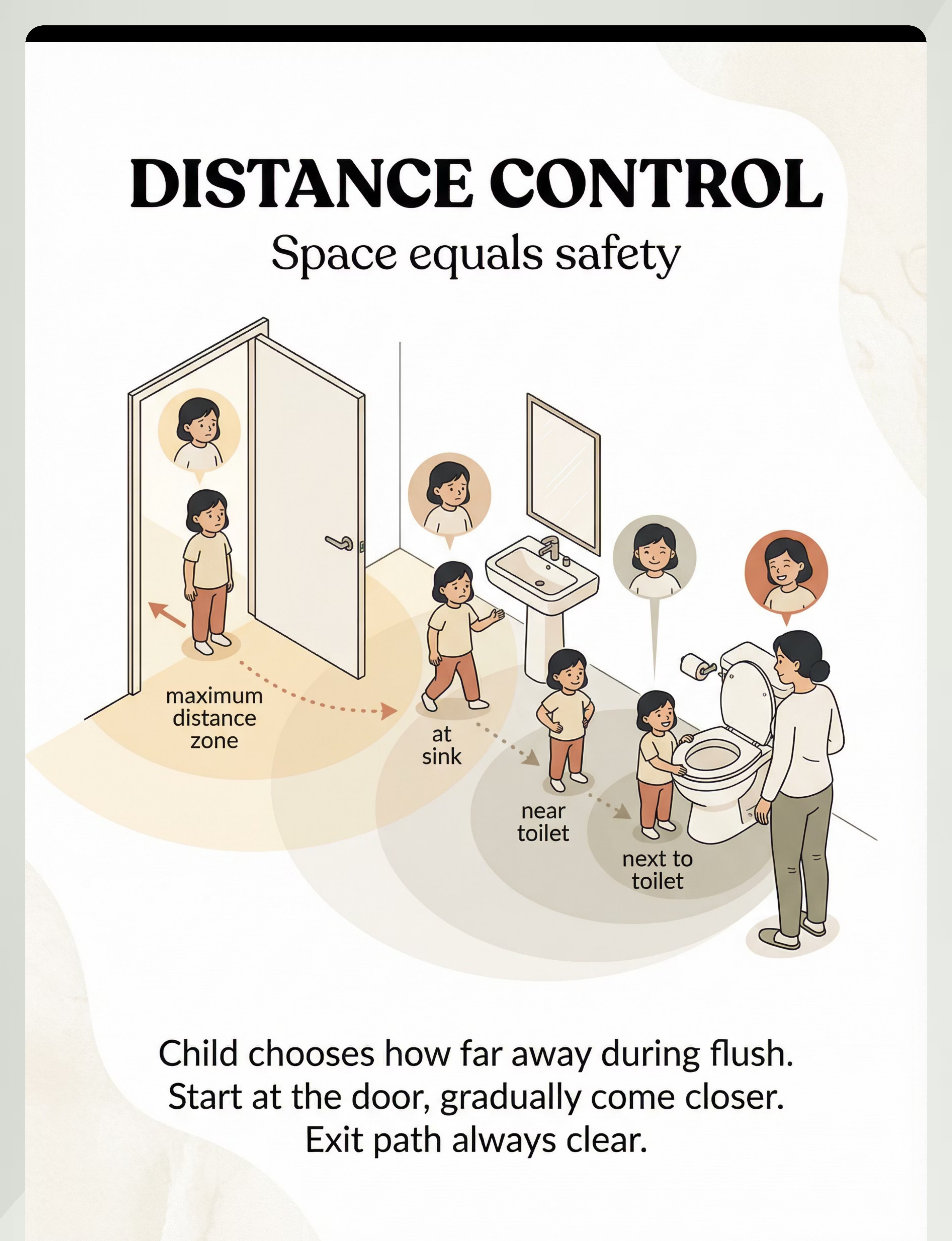
Distance and Exit Control Markers
Canon: Visual Supports | Cost: ₹0
Painter's tape for floor markers works perfectly
Painter's tape for floor markers works perfectly
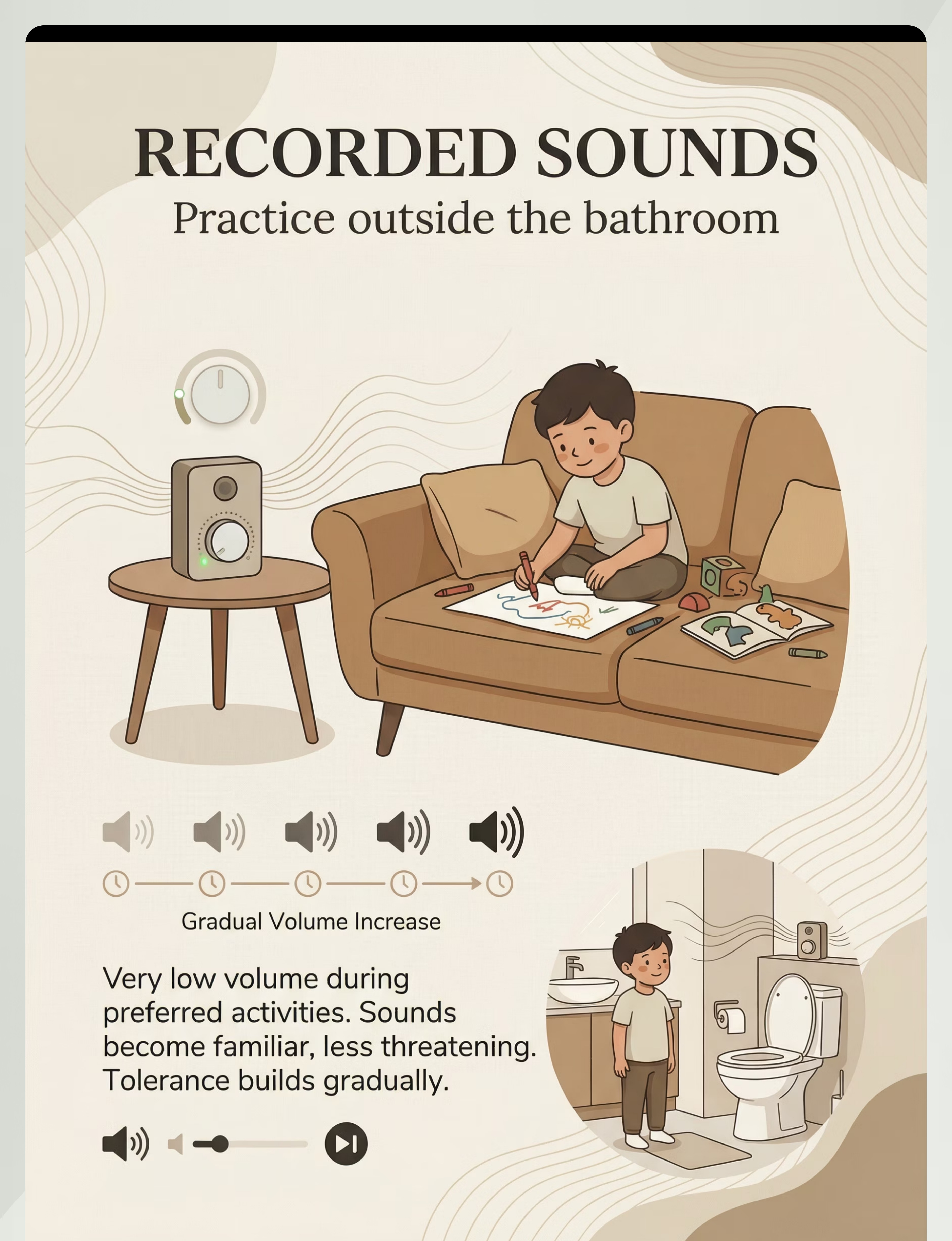
Recorded Flush Sounds (Controlled Exposure)
Canon: Sensory Calming Apps + Audio Resources | Cost: ₹0–500
YouTube recordings + Bluetooth speaker
YouTube recordings + Bluetooth speaker
Positive Toileting Routine Rebuild Kit
Canon: Reward Charts/Token Systems | Cost: ₹0–500
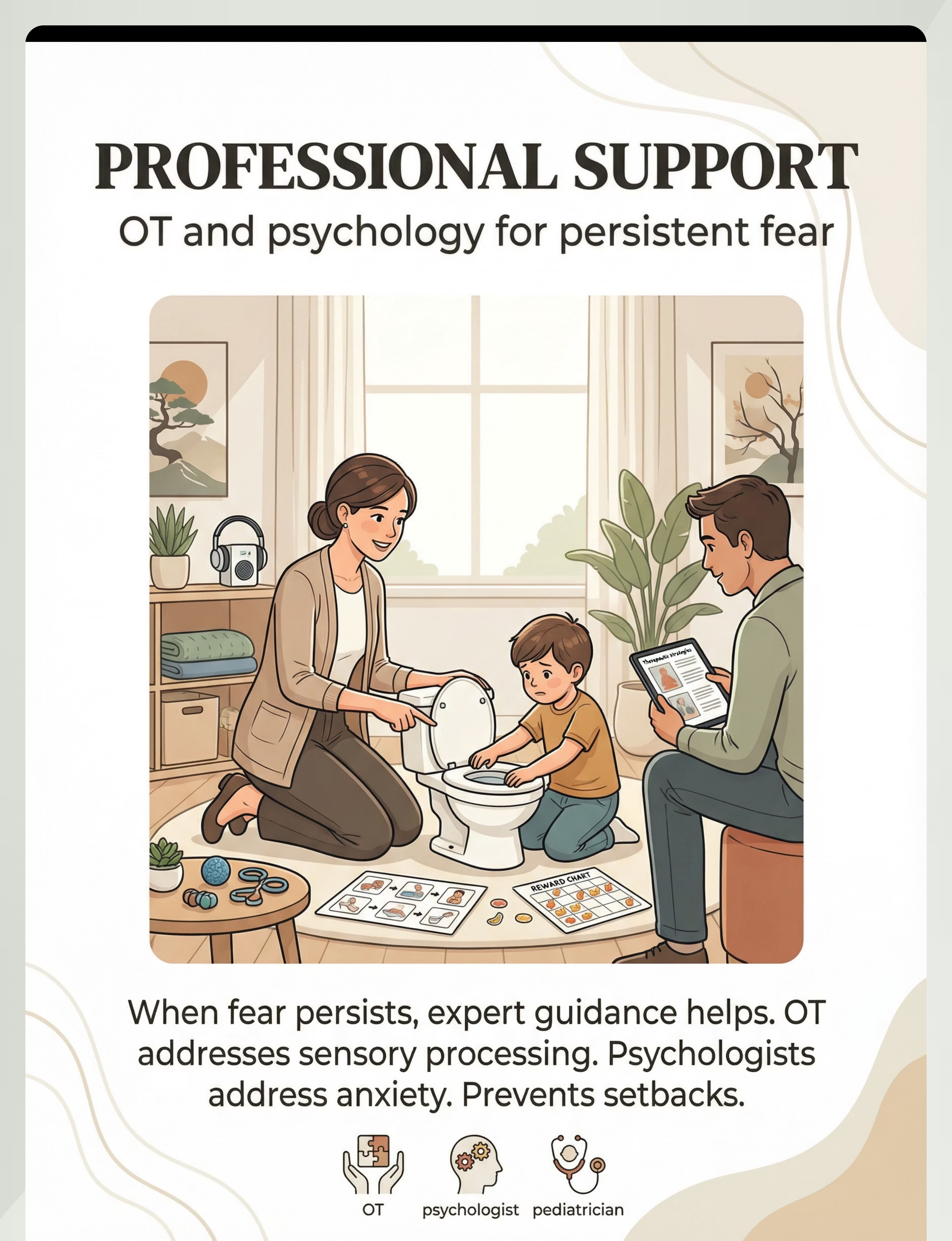
Professional Therapeutic Support
Canon: OT Assessment + Psychology | Cost: ₹1,500–5,000/session
For persistent cases: pinnacleblooms.org
For persistent cases: pinnacleblooms.org
Total Toolkit Cost: ₹0–8,000+ — most essential items cost nothing. Every family, everywhere, can start this protocol today.

Every Parent Can Start Today — Regardless of Budget
The WHO/UNICEF Nurturing Care Framework emphasizes equity-focused, context-specific interventions. This protocol is designed for every home, every village, every family. Here is the complete zero-cost version of every material.
Material | Buy This | Make This (Free) | |
Sensor Covers | Reusable silicone covers (₹200–300) | Post-it notes, sticky notes, painter's tape, washi tape — any opaque material that covers the sensor. Keep a pad in your bag. | |
Headphones | Kid-sized noise-canceling (₹1,500–8,000) | Industrial hearing protection earmuffs from hardware store (₹300–600). Or tightly-fitting over-ear headphones the child already owns. Some children respond to hands over ears with parent counting down. | |
Exposure Ladder | Printed visual hierarchy chart (₹100) | Hand-drawn steps on paper, numbered 1–12. Stick on bathroom wall. Child colors in each step as mastered. Use star stickers from any stationery shop. | |
Social Story | Commercial social story book (₹300–500) | Homemade laminated pages using photos of YOUR child's bathroom, YOUR child's headphones, YOUR child's coping tools — more effective because it's personalized. | |
Countdown System | Visual countdown cards (₹200) | Your fingers. Your voice. "5-4-3-2-1-FLUSH" costs nothing and works immediately. | |
Recorded Sounds | Sound app (₹0–500) | YouTube — search "toilet flush sound effects." Play through phone speaker at lowest volume. Free and available immediately. | |
Reward System | Sticker chart (₹100–300) | Hand-drawn chart on paper with star drawings or tick marks. The reward can be a hug, a high-five, or 5 minutes of preferred activity. |
Zero-Cost Version Total: ₹0. Every family, everywhere, can start this protocol today.

Safety Gate — Read Before Proceeding
Before beginning any desensitization work, review these clear guardrails. Following them protects your child and your progress. When in doubt, pause and seek professional guidance.
🔴 RED LINES — DO NOT PROCEED IF:
• Child shows signs of severe anxiety beyond toileting (generalized panic, sleep disruption, refusing to leave home) → Seek professional assessment FIRST
• Child has medical emergency from holding — impacted stool, severe abdominal pain, blood in stool or urine → See pediatrician IMMEDIATELY
• Child experienced recent trauma unrelated to toileting → Professional support needed first
• Child is under active anxiety treatment that may conflict → Consult treating professional
• Child has medical emergency from holding — impacted stool, severe abdominal pain, blood in stool or urine → See pediatrician IMMEDIATELY
• Child experienced recent trauma unrelated to toileting → Professional support needed first
• Child is under active anxiety treatment that may conflict → Consult treating professional
🟡 PROCEED WITH MODIFICATION IF:
• Child has co-occurring sensory challenges → Modify environment for multi-sensory comfort
• Child is on anxiety medication → Proceed with medical team awareness
• Child has significant communication limitations → Adapt social stories and warning systems
• Multiple caregivers involved → Ensure ALL caregivers follow identical protocol — inconsistency is dangerous
• Child is on anxiety medication → Proceed with medical team awareness
• Child has significant communication limitations → Adapt social stories and warning systems
• Multiple caregivers involved → Ensure ALL caregivers follow identical protocol — inconsistency is dangerous
🟢 CLEAR TO PROCEED WHEN:
• Fear is specifically toilet-flush related (not generalized bathroom phobia)
• Child is physically healthy enough for toileting activities
• At least one caregiver can commit to consistent daily implementation
• Home bathroom is available for controlled practice
• Child is physically healthy enough for toileting activities
• At least one caregiver can commit to consistent daily implementation
• Home bathroom is available for controlled practice
CRITICAL SAFETY PRINCIPLES: NEVER force exposure. NEVER punish accidents. NEVER surprise-flush. NEVER block the exit. ALWAYS follow the child's pace. MONITOR for constipation, UTIs, encopresis — consult pediatrician if holding persists beyond 2–3 days.

Preparing the Bathroom — Your Therapeutic Stage
The environment you create directly shapes your child's nervous system response. A thoughtfully prepared bathroom reduces sensory load, increases predictability, and communicates safety before a single word is spoken.
Physical Environment
• Bathroom clean, well-lit, and warm — cold bathrooms add sensory discomfort
• Fan/ventilator OFF during early sessions — reduces additional sound input
• Door OPEN during early sessions — reduces feeling of being enclosed
• Clear exit path — nothing between child and door
• Toilet lid up (if applicable) — familiar position
• Fan/ventilator OFF during early sessions — reduces additional sound input
• Door OPEN during early sessions — reduces feeling of being enclosed
• Clear exit path — nothing between child and door
• Toilet lid up (if applicable) — familiar position
Remove from Space
• Other sound-making devices (don't attempt hand dryer simultaneously)
• Strong scents — air freshener adds sensory load
• Clutter that restricts movement or escape
• If bathroom echoes, place a towel on the floor to reduce sound reverberation
• Strong scents — air freshener adds sensory load
• Clutter that restricts movement or escape
• If bathroom echoes, place a towel on the floor to reduce sound reverberation
Materials Positioned
• Headphones accessible on bathroom counter or designated hook
• Sticky notes/sensor covers in parent's pocket for any outing
• Visual countdown cards on wall at child's eye level
• Reward chart visible in bathroom
• Sticker stars/markers ready and within reach
• Sticky notes/sensor covers in parent's pocket for any outing
• Visual countdown cards on wall at child's eye level
• Reward chart visible in bathroom
• Sticker stars/markers ready and within reach
Lighting & Sound
• Bright enough to see comfortably — not harsh fluorescent
• Background silence — no music or TV; we're working on ONE sound
• All background sound sources minimized so the flush is the only variable
• Background silence — no music or TV; we're working on ONE sound
• All background sound sources minimized so the flush is the only variable
Environmental setup is a core principle of Sensory Integration Theory (Ayres). A structured environment maximizes session effectiveness. (PMC10955541)

Pre-Session Readiness Assessment (60 Seconds)
Check these indicators before every single session. A session that starts wrong almost always ends badly — and a failed session can temporarily set back progress. Sixty seconds of assessment now saves hours of recovery later.
✅ Child is fed and hydrated
Hungry or thirsty children are already dysregulated — their nervous system has less capacity to handle challenges.
✅ Child is rested and calm-alert
Not overtired, not post-meltdown, not mid-tantrum, not mid-stimming episode. Calm-alert is the optimal learning state.
✅ No recent negative toilet experience (same day)
Fear must not be freshly activated. If there was a bad bathroom event earlier today, postpone.
✅ No illness or physical discomfort
Stomach aches, fever, ear infection — all add sensory load and reduce the child's capacity to engage.
✅ Parent is calm and patient
Children read parent anxiety with extraordinary precision. If you're stressed today, postpone the session.
✅ Time is available — no rushing
"We need to leave in 5 minutes" creates pressure that collapses the therapeutic space entirely.
All ✅ → GO
Proceed with full protocol
1–2 ❌ → MODIFY
Use simplified version: protective elements only (headphones + countdown) without exposure challenge
3+ ❌ → POSTPONE
Alternative calming activity. No session is better than a failed session.

Step 1 — The Invitation (Not a Command)
⏱️ Timing: 30–60 seconds
The session begins with an invitation that gives your child agency, signals safety, and frames what's about to happen as a game — not a medical procedure. Your body language and tone communicate more than your words.
"Hey [child's name], let's go play our bathroom game! Remember, we have your special headphones and your stickers. You get to be the boss of when things happens. Ready to earn some stars?"
Body Language Essentials
• Relaxed posture — do NOT show anxiety about going to the bathroom
• Playful tone — this is a game, not a medical procedure
• Hold headphones visibly — the protection IS the invitation
• Have sticker chart ready — the reward is visible before you begin
• Playful tone — this is a game, not a medical procedure
• Hold headphones visibly — the protection IS the invitation
• Have sticker chart ready — the reward is visible before you begin
What Acceptance Looks Like
• Child walks toward bathroom (even hesitantly) ✅
• Child reaches for headphones ✅
• Child asks about stickers/reward ✅
• Child says "okay" or nods ✅
• Child reaches for headphones ✅
• Child asks about stickers/reward ✅
• Child says "okay" or nods ✅
What Resistance Looks Like & How to Respond
• Immediate "no" or crying → "That's okay. We can try later. No pressure."
• Body stiffening, pulling away → "I see you're not ready. Let's do [preferred activity] instead."
• "I'm scared" → "I know. That's why we have your special headphones. You're the boss. You say when."
• Body stiffening, pulling away → "I see you're not ready. Let's do [preferred activity] instead."
• "I'm scared" → "I know. That's why we have your special headphones. You're the boss. You say when."
CRITICAL: If the child refuses, ACCEPT IT. Do not bribe, threaten, or negotiate. Simply return to the invitation at another time. Pressure creates resistance. Patience creates progress.

Step 2 — Establishing Protection and Control
⏱️ Timing: 1–3 minutes
Before any flush occurs, your child needs to feel protected and in control. This step runs two parallel tracks simultaneously — physical protection and spatial autonomy. Both communicate the same message: you are safe and you are in charge.
Track A — Protection Setup (Every Session)
1. Child puts on headphones (or parent helps)
2. Parent: "Your headphones are on. The loud sound can't bother you now."
3. If using automatic toilet: parent places sensor cover while child watches
4. Parent: "See? I covered the sensor. It won't flush until WE say so."
5. Child acknowledges protection is in place
2. Parent: "Your headphones are on. The loud sound can't bother you now."
3. If using automatic toilet: parent places sensor cover while child watches
4. Parent: "See? I covered the sensor. It won't flush until WE say so."
5. Child acknowledges protection is in place
Track B — Distance Establishment
1. Parent: "Where do you want to stand? By the door? By the sink? You choose."
2. Child selects their comfort distance
3. Parent: "Perfect. That's your spot. You're in charge of your spot."
4. Mark the spot if helpful — tape on floor
2. Child selects their comfort distance
3. Parent: "Perfect. That's your spot. You're in charge of your spot."
4. Mark the spot if helpful — tape on floor
Engagement ✅
Child participates in protection setup, chooses distance, shows curiosity — proceed normally
Tolerance ⚠️
Child allows setup but shows mild anxiety — proceed slowly, reduce demands
Avoidance 🔴
Child refuses to enter bathroom — retreat to Step 1, try later today or tomorrow
Reinforcement Cue: "Great job putting on your headphones! That's one star already!" — immediate, specific praise delivered the moment the child complies.

Step 3 — The Flush Event (Protected, Controlled, Predicted)
⏱️ Timing: 1–2 minutes including countdown
This is where healing happens. The child experiences a toilet flush — but THIS time, it is on THEIR terms, with THEIR protection, at THEIR predicted moment. The therapeutic power lies in the gap between what happened before (sudden, uncontrolled, terrifying) and what happens now (announced, controlled, safe).
Confirm Protection
"Headphones on? ✅ Sensor covered? ✅ Standing where you want? ✅"
Announce Intention
"I'm going to flush. Remember, you're wearing your headphones. You're at your spot. You're safe."
Begin Countdown
"Ready? 5… 4… 3… 2… 1… FLUSH!" Use a consistent, calm voice. Hold up fingers for a visual count simultaneously.
Execute Flush
Parent flushes EXACTLY at the "FLUSH" moment — not before, not after. Predictability is the medicine.
Immediate Acknowledgment
"You did it! The flush happened and you were SAFE! You're amazing! How was that? Too loud? Just right?"
The flush lasts 3–5 seconds. That is the entire therapeutic exposure. Quality over quantity — one calm, controlled, predicted flush does more healing than ten forced ones.

Step 4 — Therapeutic Dosage: How Many, How Different
⏱️ Timing: 3–5 minutes total
Target: 2–3 flushes per session
Repetition builds neural pathways. But more is not better — 3 good flushes beats 10 forced ones every time. Introduce variation across sessions (not all at once) to build generalization while maintaining the safety of predictability.
Weeks 1–2
Same toilet, same distance, same full protection, same countdown. Build reliability and trust. Parent always flushes.
Weeks 3–4
Slightly closer distance. Child's hand on flush handle (parent presses with them). Countdown shortened to "3-2-1-FLUSH."
Weeks 5–8
Child flushes independently (with headphones). Child tries lighter protection. Different toilet in the house. Child leads the countdown.
Satiation Indicators — When the Child Has Had Enough:
- Distraction, wandering attention during session
- Asking to leave or saying "I'm done"
- Mild irritability emerging
- Gestural signals of disengagement
When you see these signals, end the session gracefully and celebrate what was accomplished. Never push past satiation — a willing child tomorrow is worth more than a forced session today.
Step 5 — Reinforcement: The Moment That Cements Progress
⏱️ Within 3 seconds of successful flush
Reinforcement is the mechanism by which the brain learns that the bathroom is now associated with success, not danger. Timing is everything — the reinforcement must be immediate, specific, and enthusiastic.
"You did it! You stayed while the toilet flushed! That was SO brave! You earned your star!" ⭐
Social Reinforcement
High-five, hug, verbal praise, clapping — immediate, warm, and genuine. The most powerful reinforcer for most children.
Token Reinforcement
Star on sticker chart, token toward a bigger reward. 1 star = session participation. 3 stars = independent flush with headphones. 5 stars = independent flush without headphones. 10 stars = bigger reward.
Activity Reinforcement
5 minutes of preferred activity after the session. The session ends with something wonderful, cementing a positive association with the whole bathroom experience.
Tangible Reinforcement
Small toy, special snack — use sparingly and as backup. Social reinforcement should be the primary driver.
CRITICAL PRINCIPLE: "Celebrate the ATTEMPT, not just the success." A child who entered the bathroom and watched from the door has made real progress. A child who put on headphones but couldn't stay for the flush has made real progress. Reinforce every step forward.

Step 6 — Transition Back to Baseline
⏱️ Timing: 1–2 minutes
How a session ends matters as much as how it begins. A thoughtful cool-down closes the therapeutic loop, returns your child to regulation, and signals that the bathroom experience is complete — not ongoing. Always end on a high note.
If Child Resists Ending (Great Progress!)
"I love that you want to keep going! We'll do more tomorrow. You're going to have so many stars!" End on a high note. Always end on success — leaving the child wanting more is the ideal outcome.
If Child Escalated During Session
No formal cool-down needed — the session ended when distress appeared. Comfort the child: "I know that was hard. You're safe. We'll try differently next time." No punishment. No visible disappointment. The session was data, not failure.
Material Put-Away Ritual: Child helps hang headphones on designated hook. Child places sticker on chart (the final reinforcement). Bathroom returns to "normal" — not a therapy space — until next session.
60 Seconds of Data — Capture It Now
Within 60 seconds of every session ending, record three simple data points. This information transforms your work from intuition-based to evidence-based — helping you recognize progress that's invisible to daily observation and make smarter decisions about pacing.
1. Distance Tolerance
Where did your child stand during the flush?
□ Outside bathroom □ At door □ At sink □ Near toilet □ Next to toilet □ Flushing self
□ Outside bathroom □ At door □ At sink □ Near toilet □ Next to toilet □ Flushing self
2. Protection Level Required
□ Full headphones + sensor cover + countdown + parent flush
□ Headphones + countdown + parent flush
□ Countdown + parent flush
□ Child flush with headphones
□ Child flush with hands over ears
□ Child flush independently
□ Headphones + countdown + parent flush
□ Countdown + parent flush
□ Child flush with headphones
□ Child flush with hands over ears
□ Child flush independently
3. Distress Level (0–5)
0 = Calm, engaged | 1 = Mild unease | 2 = Noticeable anxiety, stayed
3 = Significant anxiety, completed with support | 4 = High distress, session shortened | 5 = Panic, session abandoned
3 = Significant anxiety, completed with support | 4 = High distress, session shortened | 5 = Panic, session abandoned
📄 PDF Tracker
Downloadable tracking sheet — print and fill daily. Simple table format any caregiver can use.
📱 GPT-OS® Tracker
Digital in-app tracker with auto-graphed progress over time. Syncs with your child's developmental profile.
"60 seconds of data now saves hours of guessing later."

When Sessions Don't Go Perfectly (Most Won't — That's Normal)
Non-linear progress is the rule, not the exception in sensory desensitization work. Here are the most common challenges families encounter, why they happen, and exactly what to do about each one.
"My child refused to enter the bathroom."
Why: Anticipatory anxiety is at peak. The bathroom itself has become a threat cue.
Fix: Start OUTSIDE the bathroom. Play near the bathroom with the door open. Read the social story. Let flush occur while child is in another room — exposure begins before formal sessions.
Fix: Start OUTSIDE the bathroom. Play near the bathroom with the door open. Read the social story. Let flush occur while child is in another room — exposure begins before formal sessions.
"My child screamed when I flushed."
Why: Sound was above their current tolerance threshold.
Fix: Increase distance. Add headphones if not using. Reduce flush volume (partially close lid to muffle). Return to recorded sounds at very low volume.
Fix: Increase distance. Add headphones if not using. Reduce flush volume (partially close lid to muffle). Return to recorded sounds at very low volume.
"My child was fine for 3 days then suddenly regressed."
Why: Neural pathway building is non-linear. Stress, tiredness, illness, or an unexpected flush elsewhere can temporarily reset progress.
Fix: This is normal. Return to the protection level that felt safe. Do not push forward. Progress will resume.
Fix: This is normal. Return to the protection level that felt safe. Do not push forward. Progress will resume.
"My child won't wear the headphones."
Why: Some children have tactile sensitivity to head/ear pressure.
Fix: Try different styles — headband type, ear-loop defenders, loose-fitting over-ear. Try headphones during preferred activities first so they become associated with pleasure, not the bathroom.
Fix: Try different styles — headband type, ear-loop defenders, loose-fitting over-ear. Try headphones during preferred activities first so they become associated with pleasure, not the bathroom.
"Great at home, panics in public restrooms."
Why: Public restrooms add multiple sensory assaults — echoing, hand dryers, strangers, unfamiliar smells. Generalization takes longer.
Fix: Master home first. Then add one public variable at a time. Always carry sensor covers + headphones for public outings.
Fix: Master home first. Then add one public variable at a time. Always carry sensor covers + headphones for public outings.
"Session abandonment is not failure — it's data."
No Two Children Are Identical — Adapt This Protocol
The protocol described across the previous cards is a framework, not a rigid script. Your child's unique sensory profile, age, communication level, and co-occurring challenges should shape how you implement each step. Here is how to calibrate.
Ages 2–3
Primarily sensory protection (headphones + distance) and simple reward. Social stories can be picture-only. Countdown = 3 count (not 5). Sessions shorter — 1–2 flushes maximum. Language is simple and reassuring.
Ages 4–6
Full protocol as described. Social stories with text. Self-countdown emerging. Token economy highly effective. Child can begin to verbalize about the experience.
Ages 7–10
More cognitive engagement. Explain the neuroscience in age-appropriate terms. Child can help design their own exposure ladder. Greater autonomy over pace and protocol choices.
Sensory Profile Modifications:
Sensory Avoider (most flush-fear children)
Extra protection layers, slower pace, more distance, longer at each step. Headphones are essential, not optional. Never rush the ladder.
Co-occurring Tactile Sensitivity
Use headband-style ear defenders, not over-ear. Soften bathroom lighting if visual sensitivity is also present. Use visual cues (finger counting, picture cards) instead of verbal countdown if communication is limited.

Weeks 1–2: Building the Foundation
Progress Bar: ~15%
The first two weeks are the hardest — not because nothing is happening, but because most of what's happening is invisible. Your child's brain is building new neural associations: bathroom + headphones + countdown + parent = SAFE. This pathway is being laid right now, even if behavior hasn't dramatically changed. Think of it like a seed under soil: growth is happening before the sprout appears.
What "Progress" Looks Like at This Stage
• Child enters bathroom without full panic (even if reluctant)
• Child allows headphones to be placed
• Child watches parent flush from a safe distance — even from the door
• Child hears recorded flush sounds at low volume without distress
• Accidents decrease slightly as fear of the bathroom environment reduces
• Child begins to participate in the "bathroom game" routine
• Child allows headphones to be placed
• Child watches parent flush from a safe distance — even from the door
• Child hears recorded flush sounds at low volume without distress
• Accidents decrease slightly as fear of the bathroom environment reduces
• Child begins to participate in the "bathroom game" routine
What Is NOT Progress Yet (And That's Okay)
• Child is NOT flushing independently
• Child is NOT using public restrooms comfortably
• Child may still need reminders about headphones
• Accidents may still occur, especially at school or public places
• Child is NOT using public restrooms comfortably
• Child may still need reminders about headphones
• Accidents may still occur, especially at school or public places
"If your child tolerates being in the bathroom while a flush occurs — even at maximum distance with full protection — that's real progress."
Patience is not passive. Patience is active protection of your child's healing timeline.

Weeks 3–4: Neural Pathways Forming
Progress Bar: ~40%
By weeks three and four, the protocol is no longer new — it's becoming a ritual. And rituals are exactly what anxious nervous systems need. You may begin to see the first spontaneous signs that your child's brain is genuinely revising its threat assessment of the bathroom.
Consolidation Indicators
• Child anticipates the "bathroom game" — may initiate or ask about it
• Countdown becomes familiar — child may count WITH you
• Distance from toilet during flush is decreasing (moving from door toward sink)
• Headphone usage becoming automatic — child reaches for them independently
• Sticker chart generating genuine pride — child shows it to family members
• Fewer accidents at home — child using toilet with protection reliably
• Countdown becomes familiar — child may count WITH you
• Distance from toilet during flush is decreasing (moving from door toward sink)
• Headphone usage becoming automatic — child reaches for them independently
• Sticker chart generating genuine pride — child shows it to family members
• Fewer accidents at home — child using toilet with protection reliably
Spontaneous Progress Signs
• Child counts "5-4-3-2-1" in other contexts — generalization of the coping tool
• Child points out toilets without panic ("look, a toilet!")
• Child asks to try without one layer of protection ("can I do it without headphones today?")
• Social story becomes a preferred book — child requests it at bedtime
• Child points out toilets without panic ("look, a toilet!")
• Child asks to try without one layer of protection ("can I do it without headphones today?")
• Social story becomes a preferred book — child requests it at bedtime
When to Increase Intensity: When the child's distress level is consistently 0–1 for three consecutive sessions at the current level → move to the next step on the exposure ladder. Never move forward based on schedule alone — let the data guide the pace.
"You may notice you're more confident too. Parental self-efficacy grows alongside your child's tolerance."
Weeks 5–8: Independence Emerging
🏆 Mastery Zone
Progress Bar: ~75%
By weeks five through eight, the protocol begins to dissolve into independence. The structure that was once necessary scaffolding starts to feel unnecessary because your child's nervous system has built a new, safer relationship with the flush sound.
Consecutive Days
of independent home flushing = mastery achieved for home environment
Week Accident-Free
No accidents for 7 consecutive days confirms functional toileting restoration
Mastery Criteria (Observable, Measurable):
- Child uses home toilet independently — sitting, eliminating, flushing ✅
- Child flushes with minimal protection (countdown only, or hands over ears — no headphones) ✅
- Accident frequency back to baseline or better ✅
- Stool holding eliminated — regular elimination pattern restored ✅
- Child can verbalize coping strategy: "I count to 5 and then flush" ✅
- Fear rating consistently 0–1 during home flushing ✅
When to Stay vs. Progress: If child still needs headphones — THAT'S FINE. Functional toileting with accommodation IS mastery for now. Move forward when the child says "I don't need headphones anymore" — follow their lead, not a schedule.

You Did This. Your Child Grew Because of Your Commitment.
Remember Card 01? That child in the doorway, hands pressed to ears, terrified of a sound that most children never notice? Look at them now.
You spent weeks — maybe months — doing the same countdown, placing the same sensor covers, putting on the same headphones, celebrating the same small victories. You resisted the urge to force it. You resisted the urge to say "it can't hurt you." You protected, you controlled, you were patient, and you let your child's nervous system heal on its own timeline.
That is not ordinary parenting. That is therapeutic parenting. That is what the Pinnacle Blooms Consortium trains for.
🎉 Family Celebration Suggestion
Mark this milestone. A special meal. A family outing — to a restaurant where your child uses the public restroom! A photo of them proudly flushing the toilet (if they consent). This is their achievement. Honor it.
📓 Photo/Journal Prompt
Document this milestone. Write down the date. Take a photo. Describe where you started and where you are now. You will want to remember the moment your child's fear became their strength.

Clinical Guardrails — Even After Celebration
Celebrating progress and staying clinically alert are not in conflict — they coexist. Even children who have achieved mastery at home can develop complications, and some fears signal something that needs professional attention. Trust your instincts.
🔴 Seek Medical Help IMMEDIATELY If:
• Constipation requiring intervention — child hasn't had a bowel movement in 3+ days with abdominal pain
• Suspected encopresis — soiling in underwear despite toilet training
• Recurrent UTIs — burning, frequency, fever
• Blood in stool or urine
• Severe abdominal distension or pain
• Suspected encopresis — soiling in underwear despite toilet training
• Recurrent UTIs — burning, frequency, fever
• Blood in stool or urine
• Severe abdominal distension or pain
🟡 Seek OT/Psychology Within 2 Weeks If:
• Fear persists unchanged beyond 2–3 months of consistent home protocol
• Anxiety is generalizing beyond toilets — new fears emerging
• Child showing shame, self-blame, mood changes ("I'm stupid," "I'm a baby")
• Multiple auditory sensitivities worsening
• School significantly impacted — holding all day, refusing to attend
• Anxiety is generalizing beyond toilets — new fears emerging
• Child showing shame, self-blame, mood changes ("I'm stupid," "I'm a baby")
• Multiple auditory sensitivities worsening
• School significantly impacted — holding all day, refusing to attend
🟢 Normal Variation — Continue Protocol:
• Occasional regression after illness, stress, or routine change — return to previous step
• Non-linear progress ("two steps forward, one step back") is completely normal
• Child needs headphones for public restrooms even when home is mastered — THIS IS FINE
• Child prefers to exit before parent flushes — functional, acceptable
• Non-linear progress ("two steps forward, one step back") is completely normal
• Child needs headphones for public restrooms even when home is mastered — THIS IS FINE
• Child prefers to exit before parent flushes — functional, acceptable
📞 Pinnacle Blooms FREE National Autism Helpline: 9100 181 181 — available in 16+ languages for guidance at any stage of the protocol.
Your Developmental GPS — Where You've Been, Where You're Going
Toilet flush fear desensitization doesn't exist in isolation — it's one node in a larger therapeutic network. Understanding the full pathway helps you see where this work fits and what comes next, no matter which direction your child's development takes you.
Whatever path your child's progress reveals, the skills built in this protocol — graduated exposure, sensory protection, countdown systems, positive reinforcement — transfer directly to every adjacent challenge. One toolkit, many doors.
Explore More Auditory Sensory Techniques
Your headphones, social stories, countdown system, and reward charts apply to every one of these techniques. The toolkit you've built here is a platform — not a single-use tool. You already own the materials for all of these.
A-036: Hand Dryer Fear ⭐⭐
Core materials overlap: Headphones ✅ Countdown ✅ Graduated Exposure ✅. Often the next fear to address after flush mastery.
A-038: Vacuum Cleaner Distress ⭐⭐
Core materials overlap: Headphones ✅ Recorded Sounds ✅ Distance Control ✅. High prevalence in sensory-sensitive children.
A-039: Fire Alarm Anxiety ⭐⭐⭐
Advanced. Headphones ✅ Social Stories ✅ Countdown ✅. School safety is a key driver for this intervention.
A-040: Multiple Auditory Sensitivities ⭐⭐⭐
Advanced. Full toolkit applies. For children with broad auditory defensiveness across many sound types.
K-901: Understanding Auditory Over-Responsivity ⭐
Introductory. Educational — no materials needed. The knowledge foundation for all auditory sensitivity work.
K-910: When Potty Training Regresses ⭐
Introductory. Toileting supports ✅. The prerequisite knowledge for understanding why regression happens.
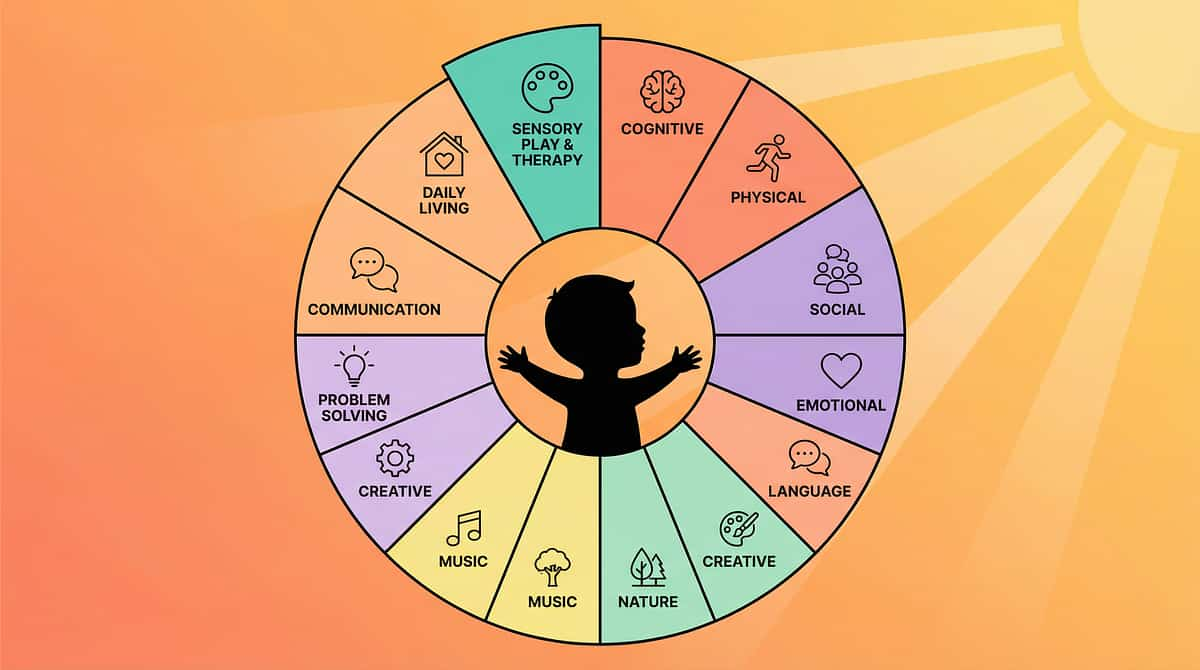
This Technique Is One Piece of a Larger Plan
Every child's development spans twelve interconnected domains. Toilet flush fear desensitization addresses a specific node — but the ripples extend far beyond auditory processing. Understanding your child's full developmental map helps you see both the specificity of this intervention and its broader impact.
PRIMARY Impact
Domain A — Sensory Processing (Auditory)
SECONDARY Impact
Domain F — Daily Living (Toileting Independence)
TERTIARY Impact
Domain J — Community Participation (Public bathroom access)
"This technique is one piece of a larger plan — and every piece matters."
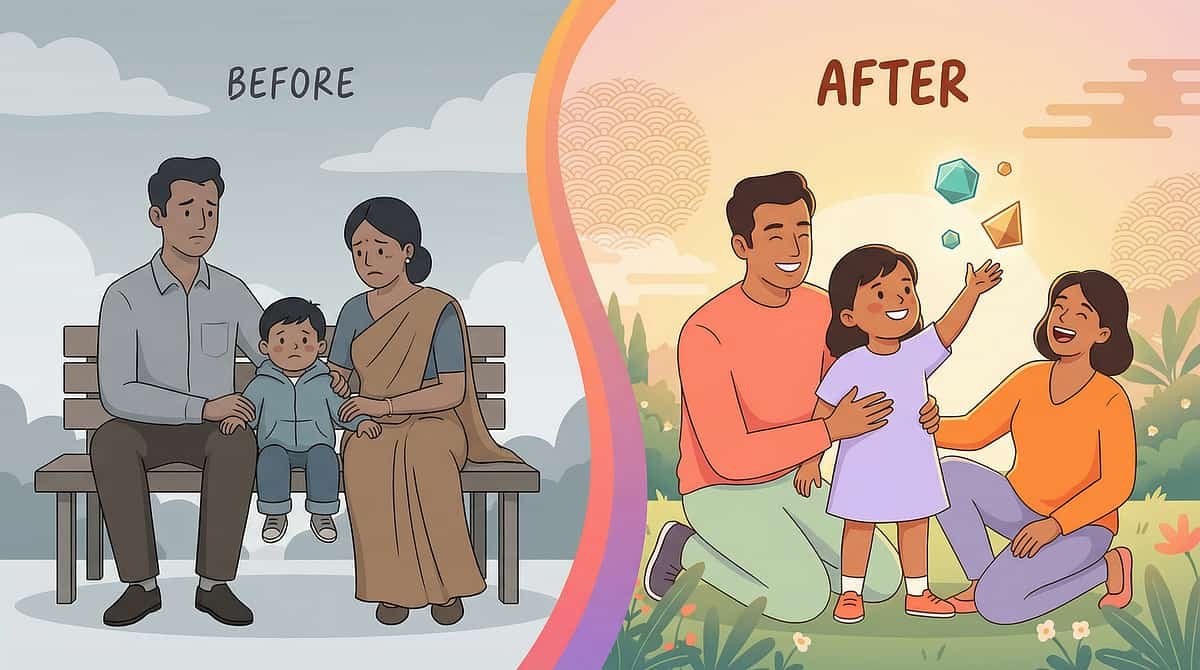
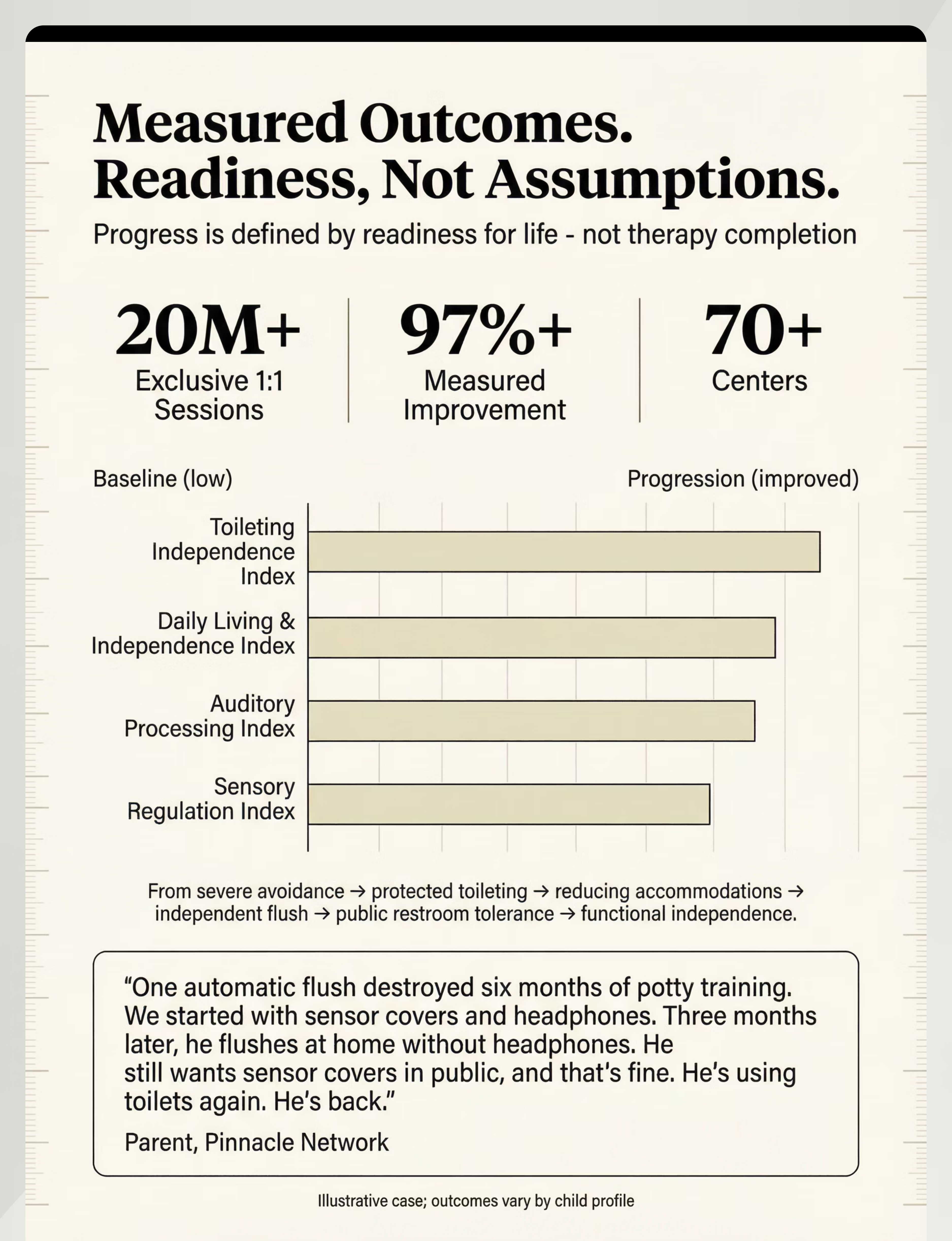
From Severe Avoidance to Independent Flushing
These are anonymized, illustrative accounts drawn from the experience of families navigating this exact protocol. Outcomes vary by child profile — but the trajectory is one of the most gratifying in all of sensory processing work.
Family Story 1 — 3 Months
Before: "One automatic flush destroyed six months of potty training. He was back in pull-ups, holding his poop for days, terrified of every bathroom."
Protocol: Sensor covers + headphones → countdown system → graduated distance → child-initiated flush
After: "He flushes at home without headphones. He still wants me to cover the sensor in public, and that's fine. He's using toilets again. We're not fighting constipation anymore."
Protocol: Sensor covers + headphones → countdown system → graduated distance → child-initiated flush
After: "He flushes at home without headphones. He still wants me to cover the sensor in public, and that's fine. He's using toilets again. We're not fighting constipation anymore."
Family Story 2 — 4 Months
Before: "She refused to use the school bathroom for four months. She held it all day. She had UTIs three times. The school said she needed a pull-up."
Protocol: Social stories + recorded sounds → home flush mastery → school consultation for manual-flush access → gradual school bathroom reintroduction
After: "She uses the nurse's bathroom at school now. She's working on the regular bathroom with a friend. No more UTIs. No more pull-ups."
Protocol: Social stories + recorded sounds → home flush mastery → school consultation for manual-flush access → gradual school bathroom reintroduction
After: "She uses the nurse's bathroom at school now. She's working on the regular bathroom with a friend. No more UTIs. No more pull-ups."
"Toilet flush fear has one of the most gratifying recovery trajectories in sensory processing work. The protocol, when followed with consistency and patience, works. Most families see functional improvement within 4–8 weeks." — Pinnacle Blooms Therapist
Illustrative cases; outcomes vary by child profile.

You Are Not Navigating This Alone
The loneliness of parenting a sensory-sensitive child can be profound — especially around something as invisible and misunderstood as toilet flush fear. Other parents get it. They've been in the car with wet pants. They've held a screaming child in a restaurant bathroom. They know. Find them.
Toileting & Sensory Parent Group
WhatsApp community of parents working through auditory sensory challenges and toileting regression. Share tips, celebrate wins, and ask questions at 2am when you need it most.
Pinnacle Parent Community Forum
Online forum organized by challenge type. Find parents working on the exact same technique — and see what has worked for children like yours.
Local Pinnacle Parent Meetup
Your nearest Pinnacle center hosts monthly parent meetups. Meet families in your city navigating similar journeys, with therapist facilitation.
Peer Mentoring
Connect with an experienced parent who has successfully completed this protocol. Real advice from someone who has been exactly where you are right now.
"Your experience helps others — consider sharing your journey once you've reached mastery."
Home + Clinic = Maximum Impact
The home protocol you've been following is powerful — but professional support can compress the timeline, address co-occurring challenges, manage medical complications, and provide the individualized precision that a general protocol cannot. For persistent cases, clinic is not optional — it's essential.
Find Your Nearest Pinnacle Center
🗺️ 70+ Centers Across India
Therapist Matching for This Technique
• PRIMARY: Occupational Therapist — Sensory Integration Specialist
• SUPPORT: Child Psychologist — Anxiety/Phobia Specialist
• MEDICAL: NeuroDevelopmental Pediatrician — Toileting Complications
• SUPPORT: Child Psychologist — Anxiety/Phobia Specialist
• MEDICAL: NeuroDevelopmental Pediatrician — Toileting Complications
What Professional Support Adds
- Comprehensive sensory processing evaluation — is this only auditory, or broader?
- Individualized desensitization protocol — faster and more precise than a general approach
- Medical monitoring for holding and constipation complications
- School consultation and accommodation planning (IEP/IDP support)
- Parent support and caregiver stress management
Teleconsultation for Remote Families
The Evidence — For the Curious Parent
You deserve to know exactly what the science says about the approach you're trusting with your child's wellbeing. This protocol draws from Level I–II evidence — the highest standard available in behavioral health research.
📚 PRISMA Systematic Review (2024)
"Sensory Integration Intervention as Evidence-Based Practice for ASD" — 16 articles, 2013–2023. Confirms SI intervention meets evidence-based practice criteria for children with ASD. Auditory processing interventions demonstrate measurable outcomes across controlled studies.
PubMed: PMC11506176
PubMed: PMC11506176
📚 Meta-Analysis (World J Clin Cases, 2024)
"Efficacy of Sensory Integration Therapy for ASD" — 24 studies. Demonstrates improvement in sensory processing, adaptive behavior, social skills, and motor skills. 1:1 individual sessions showed maximum effectiveness.
PMC10955541 | DOI: 10.12998/wjcc.v12.i7.1260
PMC10955541 | DOI: 10.12998/wjcc.v12.i7.1260
📚 Indian Pediatric RCT (2019)
Padmanabha et al. — Home-based sensory interventions by trained parents in Indian pediatric populations. Demonstrates significant outcomes, establishing feasibility and efficacy specifically in the Indian context.
DOI: 10.1007/s12098-018-2747-4
DOI: 10.1007/s12098-018-2747-4
📚 WHO Nurturing Care Framework (2018)
Foundation for equity-focused, home-implementable interventions. Implemented across 54 LMICs. Establishes evidence base for household-material-based intervention delivery.
PMC9978394 | nurturing-care.org
PMC9978394 | nurturing-care.org
📚 Frontiers in Integrative Neuroscience (2020)
Comprehensive framework for evaluating sensory integration/sensory processing treatment in ASD, establishing the neurological basis for sensory-based interventions.
DOI: 10.3389/fnint.2020.556660
DOI: 10.3389/fnint.2020.556660
📚 NCAEP Evidence-Based Practices Report (2020)
Classifies visual supports and systematic desensitization as evidence-based practices for autism. Provides the clinical consensus layer underpinning this protocol's design.
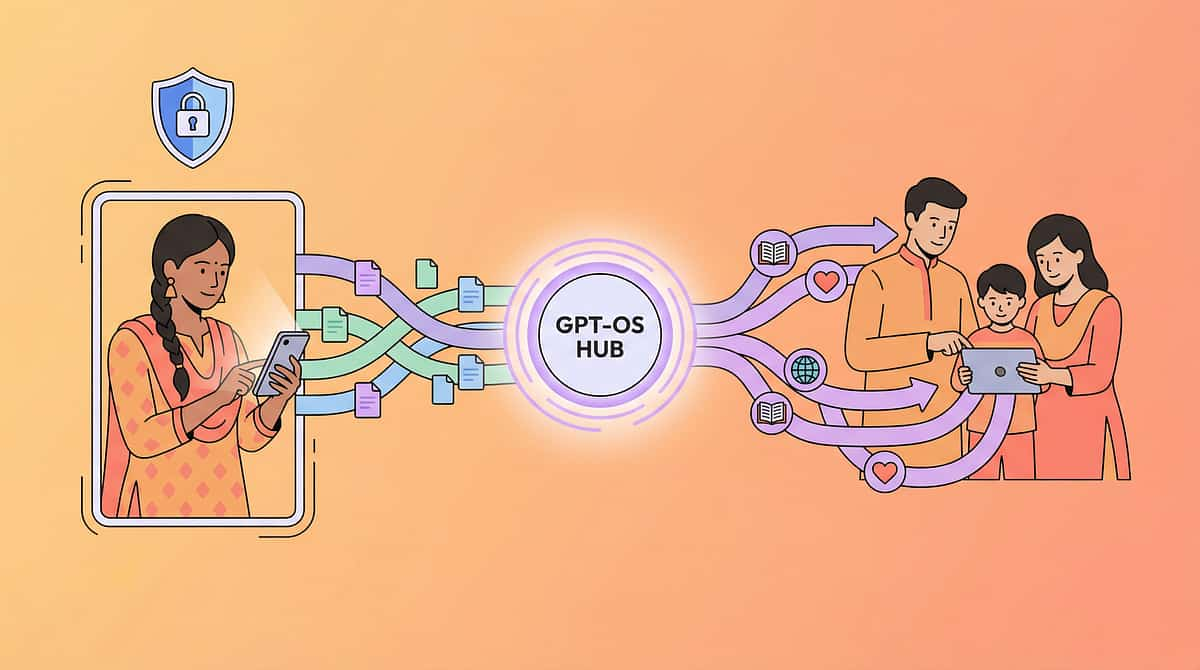
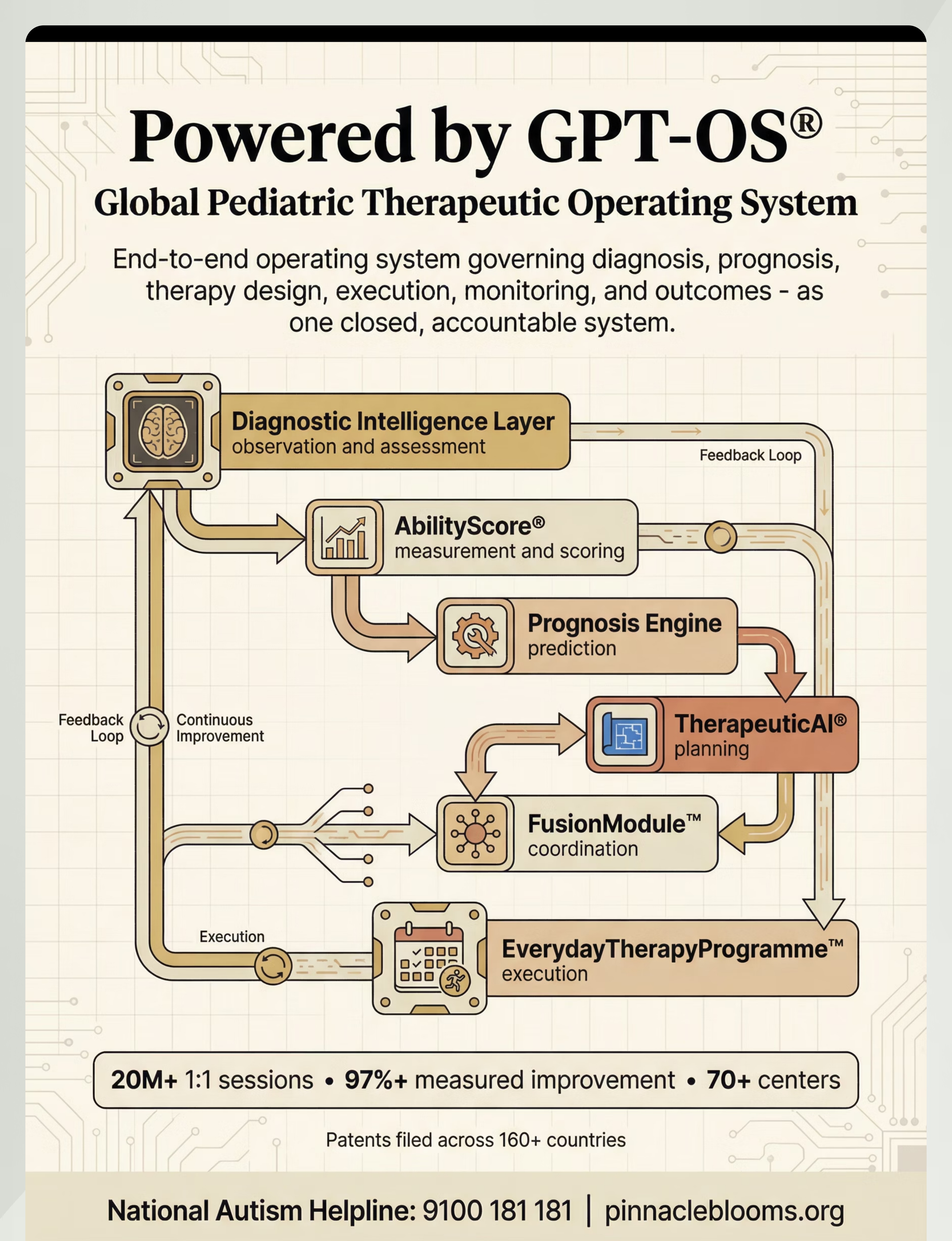
Powered by GPT-OS® — Your Data Drives Personalized Improvement
Every data point you record becomes part of a learning system built from 20M+ therapy sessions. GPT-OS® doesn't just store your child's progress — it uses it to predict pacing, flag thresholds, and recommend next steps with a precision no single therapist can replicate alone.
🔒 Encrypted In Transit & At Rest
All session data protected with industry-standard encryption protocols.
🔒 No External Sharing
No individual child data is shared outside the system. Parent controls access and deletion.
🔒 DPDPA 2023 Compliant
Compliant with Indian IT Act, Digital Personal Data Protection Act 2023, and ISO/IEC 27001 standards.
"Your data helps every child like yours. The more families contribute, the more precise GPT-OS® becomes for all."
20M+ 1:1 sessions • 97%+ measured improvement • 70+ centers • Patents filed across 160+ countries

Watch: 9 Materials That Help When Child Fears Toilet Flush
Reel ID: A-037
Series: Sensory Solutions — Episode 37
Duration: 75–85 seconds
This Reel was developed by the Pinnacle Blooms Consortium — a multidisciplinary team of Occupational Therapists, BCBAs, Speech-Language Pathologists, Special Educators, and NeuroDevelopmental Pediatricians. Every material shown is drawn from the 128 Canon Materials system and validated across 20M+ therapy sessions.
Toilet Sensor Covers / Flush Blockers
Noise-Canceling Headphones / Ear Defenders
Graduated Flush Exposure (At Home)
Social Stories About Toilets and Flushing
Countdown and Warning System
Distance and Exit Control
Recorded Flush Sounds (Controlled Exposure)
Positive Toileting Routine Rebuild
Therapeutic Support (OT/Psychology)
Video modeling is classified as an evidence-based practice for autism (NCAEP, 2020). Multi-modal learning — reading, watching, and doing — significantly improves parent skill acquisition and implementation fidelity.

Consistency Across Caregivers Multiplies Impact
One caregiver doing the protocol perfectly while others work against it — through surprise flushes, pressure, or dismissal — can undo weeks of hard-won progress. Share this page with everyone in your child's life who interacts with them around bathrooms.
📱 WhatsApp / Text
Send this page link to your spouse, grandparents, and nanny. Include the one-page Family Guide PDF for those who won't read a full protocol page.
📧 Email to Therapist / Pediatrician
Forward to your child's OT, BCBA, and pediatrician so they can align their clinic work with your home protocol.
"Explain to Grandparents" Script: "[Child's name] has a neurological sensitivity to loud, sudden sounds — especially toilet flushing. This is NOT a behavioral choice and cannot be fixed by reasoning or punishment. Please: (1) Always warn before flushing, (2) Let [child] use headphones in the bathroom, (3) Cover automatic flush sensors with sticky notes, (4) Never surprise-flush, (5) Celebrate every bathroom success."
Teacher/School Script: "Dear [Teacher], [Child's name] is working through a clinically-guided desensitization protocol for toilet flush sensitivity. Please allow: access to a non-automatic toilet, use of ear defenders during bathroom visits, and extra time for bathroom trips. A Pinnacle Blooms therapist can consult with school staff if helpful."

Your Questions, Answered
How long will this take?
Most families see meaningful improvement within 4–8 weeks of consistent daily protocol. Full independence including public restrooms may take 3–6 months. Some children retain mild sensitivity managed with simple accommodations long-term — and that is a successful outcome.
"I know it won't hurt me but I'm still scared." What does that mean?
Your child has intact cognitive understanding but their amygdala overrides their cortex. This is neurologically normal. You cannot reason away an amygdala response. You retrain it through safe, repeated, predicted exposure — which is exactly what this protocol does.
Is it okay to just let my child avoid flushing?
Short-term accommodation (parent flushes later) is therapeutically appropriate during the early phase. Long-term complete avoidance leads to constipation, UTIs, and dependency. The goal is functional independence with acceptable accommodations — not zero accommodation.
What about school? They can't accommodate my child.
Most schools can provide access to a non-automatic toilet (nurse's office, staff restroom), allow ear defenders, and provide extra bathroom time. In India, children with developmental support needs are entitled to reasonable accommodation under the RPwD Act, 2016. Document the need through your pediatrician or therapist.
Will my child always need headphones?
Many children transition: headphones → hands over ears → countdown only → independent flush. Some retain a preference for sensor covers in public restrooms indefinitely. Functional toileting is the goal — not zero accommodation — forever.
My child's constipation is getting worse. Should I continue?
See a pediatrician FIRST. Medical management of constipation runs in parallel with the desensitization protocol. The fear protocol addresses the CAUSE of holding; the pediatrician manages the CONSEQUENCE. Both are necessary.
Is this only for children with autism?
No. Toilet flush fear occurs in neurotypical children, children with sensory processing differences without autism, and children with anxiety disorders. The protocol works regardless of diagnosis. Children with autism may benefit from additional OT assessment for co-occurring sensory challenges.
Can I use this for hand dryers and other loud sounds?
Yes. The core principles (protection → control → graduated exposure → independence) apply to all auditory sensitivities. Specific protocols for hand dryers (A-036), vacuum cleaners (A-038), and fire alarms (A-039) are available with tailored material recommendations.

One Step. Today. That's All It Takes.
You have the knowledge. You have the materials — many of which cost nothing. You have the evidence. You have a community of families who have walked this road before you. The only thing left is to begin.
🟢 Start This Technique Today
Begin with sensor covers and a countdown. Print the tracking sheet. Read the social story tonight. Your first session can happen tomorrow morning. You already have everything you need.
📞 Book a Consultation
Talk to a Pinnacle OT about your child's specific sensory profile for a personalized, faster pathway.
FREE National Autism Helpline: 9100 181 181
FREE National Autism Helpline: 9100 181 181
🔗 Explore the Next Technique
A-038: 9 Materials That Help With Vacuum Cleaner Distress — your headphones and countdown system already apply.
Validated by the Pinnacle Blooms Consortium
🧠 Occupational Therapy • 🗣️ Speech-Language Pathology • 📋 Applied Behavior Analysis • 📚 Special Education • 👨⚕️ NeuroDevelopmental Medicine
Preview of 9 materials that help when child fears toilet flush Therapy Material
Below is a visual preview of 9 materials that help when child fears toilet flush therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.








Link copied!

From Fear to Mastery. One Technique at a Time.
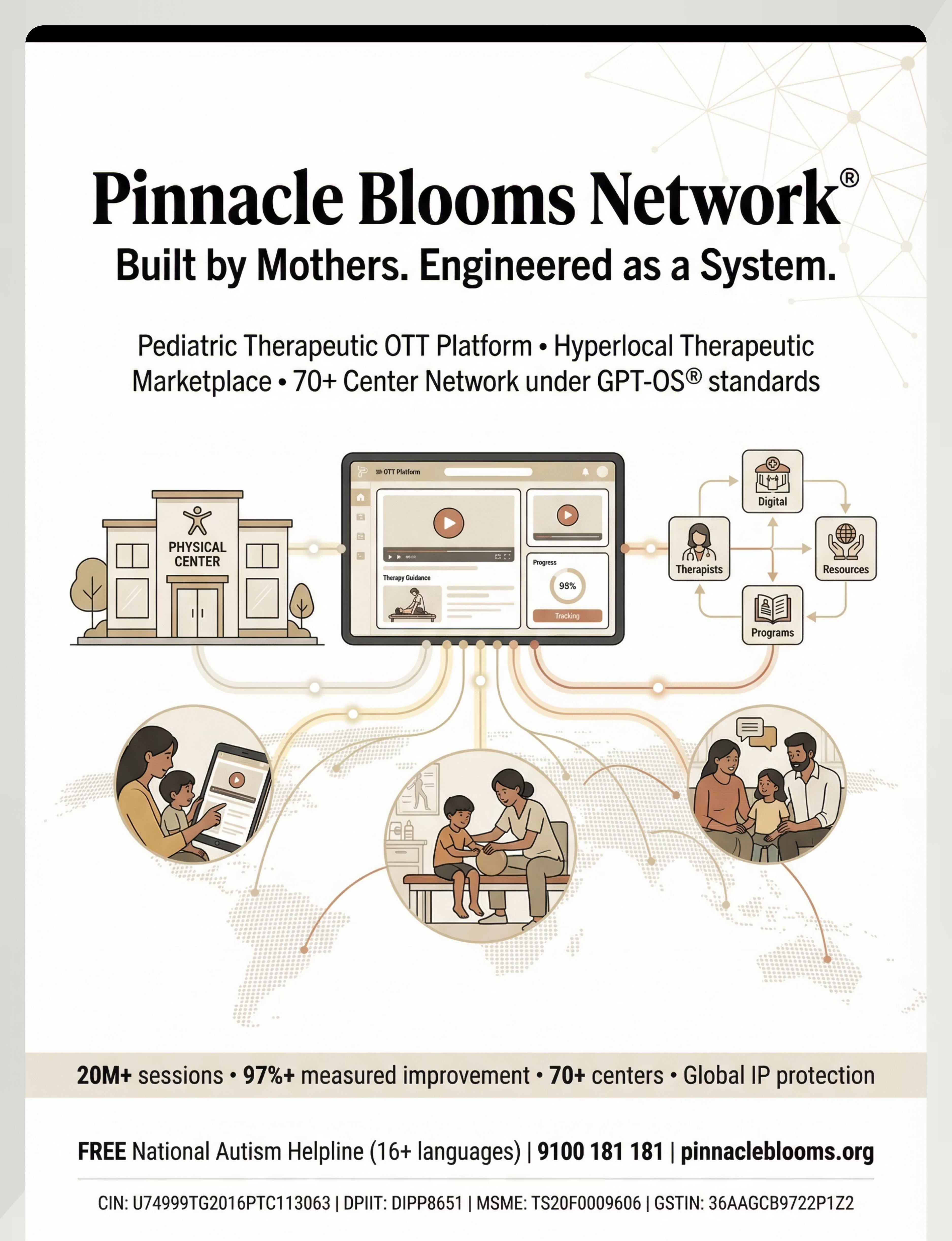
🧠 Pinnacle Blooms Network®
Built by Mothers. Engineered as a System.
Occupational Therapy • Speech-Language Pathology • Applied Behavior Analysis • Special Education • NeuroDevelopmental Medicine
Occupational Therapy • Speech-Language Pathology • Applied Behavior Analysis • Special Education • NeuroDevelopmental Medicine
🌍 Our Mission
Every child deserves to use a toilet without fear. Every parent deserves the tools and knowledge to help their child get there. This page — one of 70,000+ evidence-linked technique pages — exists because a consortium of thousands of therapists, researchers, and families decided no parent should navigate this alone.
Medical Disclaimer: This content is educational and does not replace assessment by a licensed occupational therapist, psychologist, or healthcare provider. Significant toileting regression may require comprehensive evaluation and professional intervention. If your child's toilet avoidance is causing medical concerns — prolonged holding, constipation, encopresis, UTIs — consult a pediatrician promptly. Individual results may vary. Statistics represent aggregate outcomes across the Pinnacle Blooms Network. Toilet flush fear recovery timelines vary significantly between children.
🔗 Explore More Techniques
➡️ Next Recommended
A-038: Vacuum Cleaner Distress Protocol
📞 FREE Helpline
9100 181 181 | 16+ languages
pinnacleblooms.org
pinnacleblooms.org
© 2026 Pinnacle Blooms Network®, unit of Bharath Healthcare Laboratories Pvt. Ltd. All rights reserved. CIN: U74999TG2016PTC113063 | DPIIT: DIPP8651 | MSME: TS20F0009606 | GSTIN: 36AAGCB9722P1Z2
techniques.pinnacleblooms.org — The largest structured pediatric intervention knowledge base on Earth.