
When Your Child Crashes Into Everything — Walls, Furniture, People — and Nothing Seems to Hurt
He throws himself into walls. Not by accident — on purpose, over and over. He crashes into his little sister constantly — not to hurt her, but he just can't seem to stop himself. Teachers say he "invades personal space." Other kids avoid him. You've tried telling him to be gentle. He nods, says okay, and five seconds later he's slamming into something full-force again.
Your child's body is speaking. This is not defiance. This is not aggression. This is a nervous system that needs intense physical input to know where it is in space.
Sensory Solutions Series — Episode 82
Age Band: 2–10 Years
Evidence Grade: Level I–II

You Are Not Alone — The Numbers Are Staggering
If you've ever felt like you're the only parent dealing with this — the crashing, the wall-slamming, the bruises that don't seem to bother your child — you are not alone. Not even close. Across India and around the world, millions of families are navigating the exact same living room chaos you are right now.
1 in 6
Children experience sensory processing differences significant enough to affect daily life
72%
Of parents report feeling isolated and unsupported when their child's sensory needs are first identified
3+ Years
Average time families wait before receiving a clear explanation for their child's crashing behaviour
The hardest part isn't the crashing itself — it's the silence around it. The looks at the playground. The well-meaning relatives who say 'he just needs more discipline.' The teachers who send notes home. You've been carrying this alone, and you shouldn't have to.
What you're holding right now is what thousands of parents wished they'd had earlier — a clear, evidence-based explanation and a step-by-step plan built by occupational therapists, speech-language pathologists, ABA specialists, and special educators who work with children like yours every single day. You found this. That matters.
1
You're Not Imagining It
Your child's crashing is real, it's neurological, and it has a name: proprioceptive seeking behaviour.
2
You're Not Failing
This is not a parenting problem. This is a nervous system that needs a specific kind of input — and now you know how to provide it.
3
You're Not Alone
A growing community of Indian families is learning, sharing, and supporting each other through exactly this journey.
What's Happening Inside Your Child's Brain When They Crash
The Proprioceptive System — Your Child's Hidden Sense
Your child has a sense you've probably never heard of: proprioception. It's the system that tells your brain where your body is in space — without looking. It's why you can touch your nose with your eyes closed. Why you can walk up stairs in the dark.
This system runs on receptors buried in every muscle, every joint, every piece of connective tissue. They constantly send signals to the brain: here is your arm, here is your leg, this is how hard you're pressing, this is how fast you're moving.
In Your Child, These Signals Are Too Quiet
Your child's proprioceptive system has what clinicians call a high threshold — it requires much more intense input than typical to register. Normal activities don't produce enough signal. The brain's body map is fuzzy, incomplete.
So the nervous system does what any intelligent system does when it's not getting enough data: it seeks more. Crashing provides massive proprioceptive input. The impact loads every muscle and joint simultaneously with intense sensation. For a brief moment after a crash, your child's brain finally has a clear picture of where their body is.
This is a wiring difference, not a behaviour choice. Clinical name: Proprioceptive Seeking Behaviour / Under-Responsive Proprioceptive Processing.
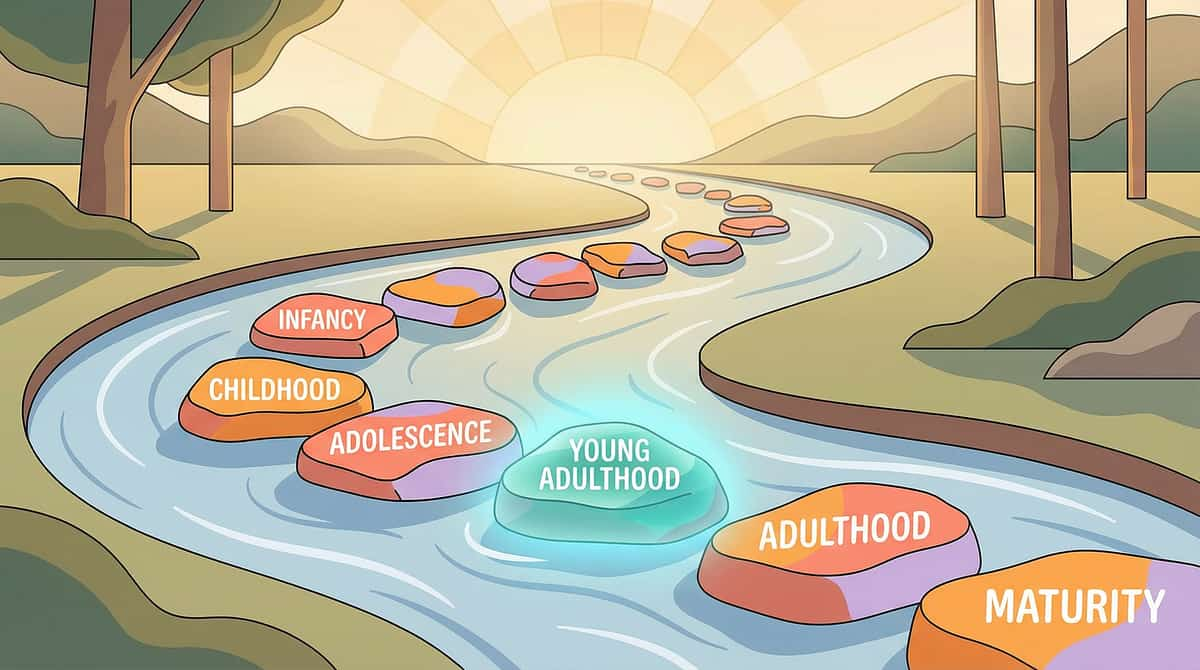
Where Crashing Behaviour Sits in Your Child's Development
Understanding the developmental timeline helps you see where your child is — and where intervention leads. The proprioceptive system matures through childhood, and targeted intervention during the peak window produces the most significant outcomes.
1
0–12 Months
Proprioceptive system begins developing through rolling, crawling, pushing up. Receptors calibrate through natural movement.
2
1–2 Years
Walking, climbing, jumping provide increasing input. Children naturally seek impact activities — typical proprioceptive development.
3
2–4 Years ★
Proprioceptive seeking patterns become visible. Intense crashing exceeds typical developmental patterns. Most parents first notice the difference here.
4
4–7 Years ✦
Peak intervention window. Nervous system is highly plastic. Appropriate proprioceptive input can reshape sensory processing patterns. Most responsive period.
5
7–10 Years
With intervention, proprioceptive regulation improves. Social consequences of crashing increase significantly without intervention.
Proprioceptive seeking rarely occurs in isolation. Your child may also show vestibular seeking (spinning, swinging), oral seeking (chewing, mouthing), tactile processing differences, motor planning challenges, and attention difficulties. A comprehensive sensory processing evaluation maps the full profile.

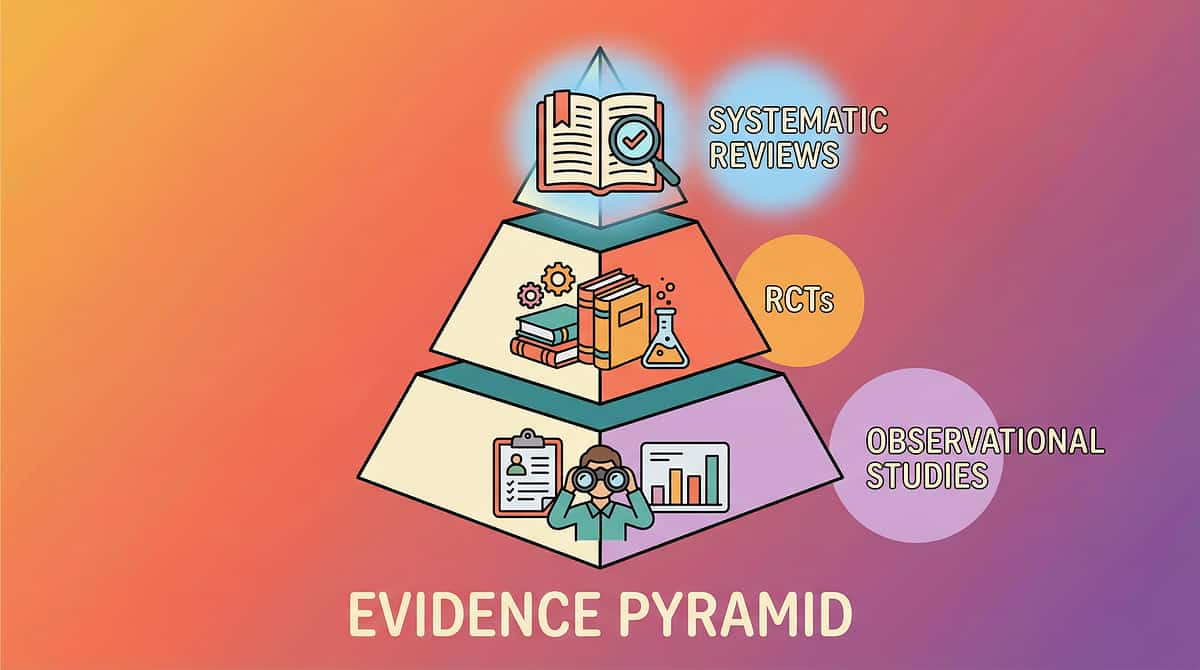
The Evidence Behind Proprioceptive Intervention — What the Research Confirms
Evidence Grade: Level I–II
Systematic Reviews + RCTs
PRISMA Systematic Review (2024)
16 articles from 2013–2023 analysed. Conclusion: Sensory integration intervention meets criteria to be considered an evidence-based practice for children with ASD. Proprioceptive-based interventions show consistent positive outcomes across sensory processing, motor skills, and adaptive behaviour.
Published in: Children (MDPI) | PMC11506176
Meta-Analysis Across 24 Studies (2024)
Pooled analysis confirms sensory integration therapy effectively promotes social skills, adaptive behaviour, sensory processing capacity, and gross/fine motor development. Sessions of approximately 40 minutes demonstrated optimal outcomes.
Published in: World Journal of Clinical Cases | PMC10955541
Indian RCT — Home-Based Intervention (2019)
Home-based sensory interventions demonstrated significant outcomes when parents were trained in structured protocols. Safety monitoring validated parent-administered proprioceptive intervention.
Published in: Indian Journal of Pediatrics | DOI: 10.1007/s12098-018-2747-4
Neurological Basis Framework (2020)
Comprehensive evaluation framework establishing the neurological basis for sensory-based interventions in ASD. Confirms proprioceptive processing differences as measurable neurological phenomena, not behavioural choices.
Frontiers in Integrative Neuroscience | DOI: 10.3389/fnint.2020.556660
Clinically validated. Home-applicable. Parent-proven. This is not experimental. This is established science implemented across 70+ Pinnacle centres with 21 million+ data points validating outcomes.

Proprioceptive Input Through Safe Impact Materials — What This Technique Is
Formal Definition
Proprioceptive Seeking Redirection Through Structured Heavy Work and Safe Impact Materials
Parent-Friendly Name: "Safe Crashing + Heavy Work — Giving the Body What It Needs Without the Danger"
Rather than attempting to stop the crashing (which addresses the symptom, not the need), this intervention channels the body's drive for impact into designated materials and activities that deliver equivalent or superior proprioceptive input without injury risk.
Technique Specifications
- Domain: Sensory Processing + Proprioception + Body Awareness
- Age Range: 2–10 years
- Session Duration: 10–20 minutes home sessions
- Frequency: 2–3× daily with heavy work throughout
- Setting: Home + School + Playground + Therapy
- Difficulty: Introductory to Core
Crash Pads
Body Socks
Weighted Materials
Heavy Work
Tunnels
Trampolines

Who Uses This Technique — The Consortium Disciplines
This technique crosses therapy boundaries because the brain doesn't organise by therapy type. Four disciplines combine to create a comprehensive, consistent intervention framework around proprioceptive seeking behaviour.
Occupational Therapy (Primary Lead)
OTs trained in Ayres Sensory Integration® are the primary clinicians. They assess the sensory processing profile, design the "sensory diet" (daily proprioceptive input schedule), select and grade materials, and train parents in execution. OTs understand why the body crashes and prescribe exactly how much input, through which channels, at what intensity.
Applied Behaviour Analysis (ABA)
BCBAs address the behavioural dimension: teaching the child WHERE crashing is appropriate (crash pad = yes, wall = redirect), reinforcing safe crashing choices, fading prompts as the child self-directs to safe targets, and collecting data on crashing frequency and location to measure intervention impact.
Special Education
Special educators adapt classroom and learning environments: movement breaks with heavy work, weighted lap pads during seated activities, seating modifications, and transition protocols that include proprioceptive input. They ensure the sensory strategy generalises beyond therapy into the educational setting.
NeuroDevelopmental Pediatrics
Pediatric neurologists and developmental pediatricians rule out medical conditions, assess pain perception, evaluate for broader developmental concerns, and provide the diagnostic framework that situates proprioceptive seeking within the child's complete neurological profile.
What This Technique Targets — Precision, Not Guesswork
This intervention targets three concentric layers of developmental outcomes. Progress moves outward from the neurological core to observable social behaviour — each layer building on the last.
🎯 Primary Target
Proprioceptive Processing and Body Awareness — registers body position accurately, reduces unsafe crashing frequency, improves internal body map
🔵 Secondary Target
Motor Regulation and Safety Awareness — grades force appropriately, navigates space without colliding, recognises impact on others' bodies
🟢 Tertiary Target
Social Body Skills and Self-Regulation — participates in physical play without excessive force, maintains appropriate personal space, independently seeks safe input

The 9 Materials That Channel the Crash Safely
These nine material categories span safe crash targets, constant pressure input, productive loading activities, alternative deep pressure, and controlled rhythmic impact. When the proprioceptive system receives adequate input through safe channels, the urgency of seeking through unsafe crashing typically decreases measurably.
1
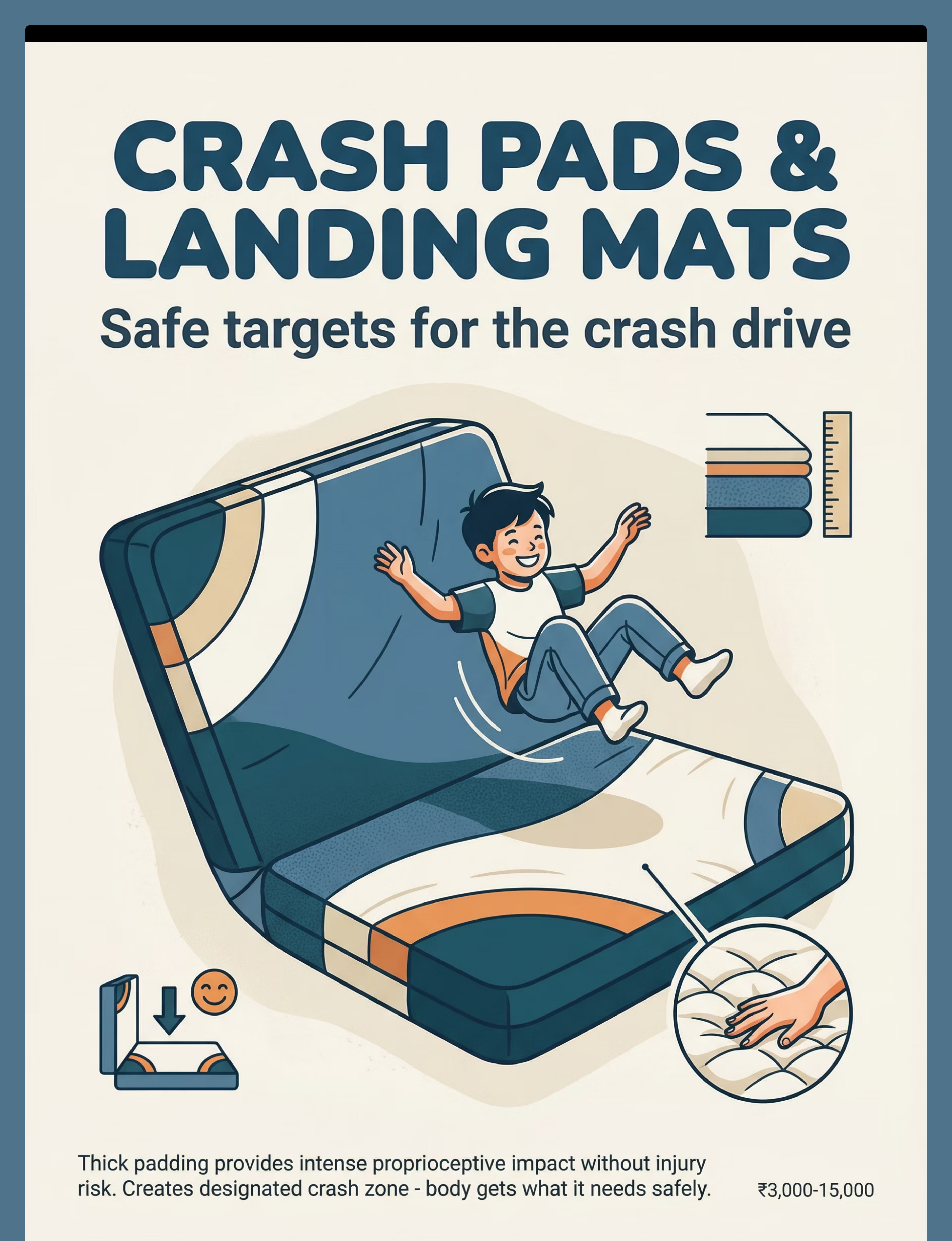
Crash Pads & Landing Mats
The essential safe crash target. Absorbs impact while providing resistance. ₹3,000–15,000 | Canon: Sensory Regulation Tools
2
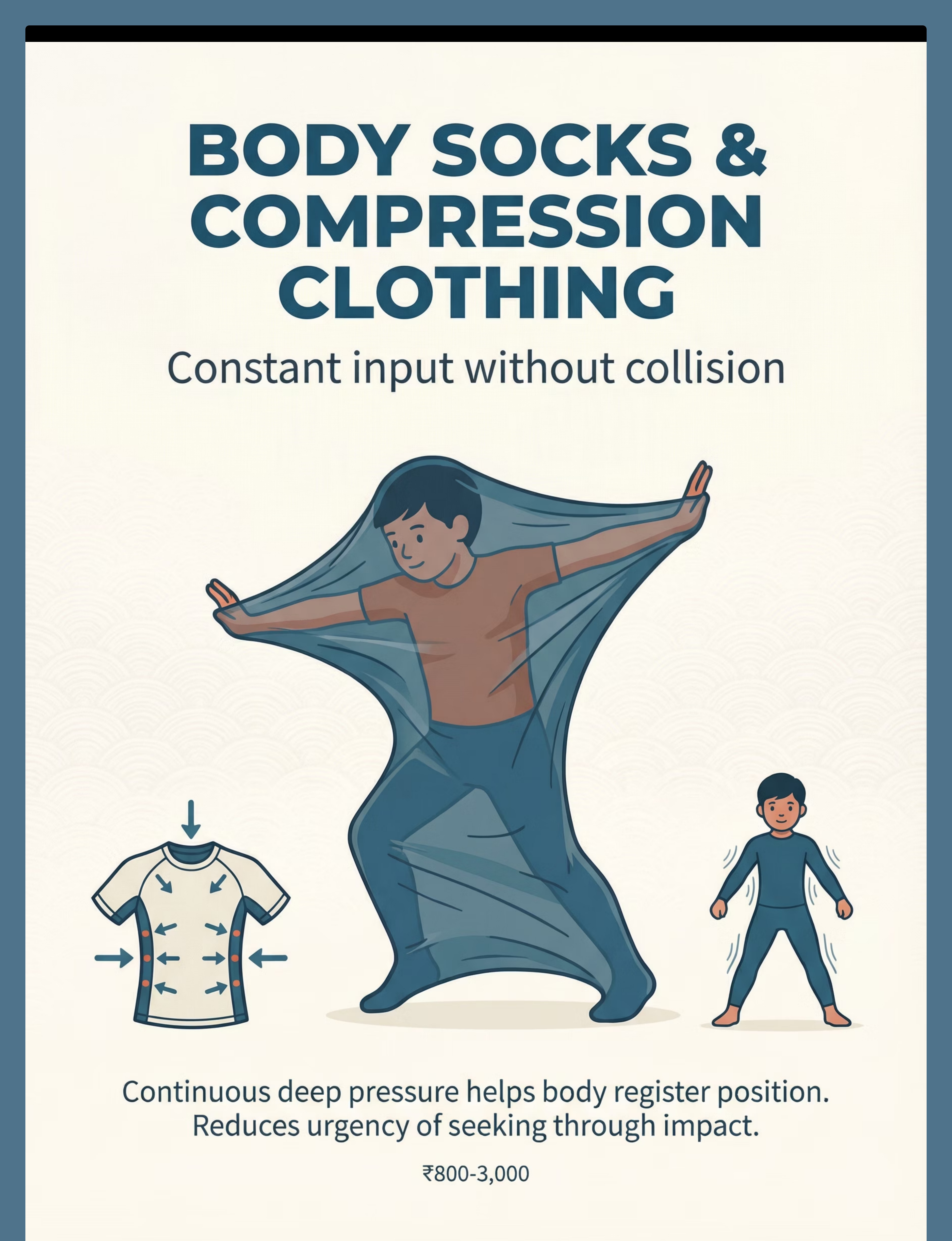
Body Socks & Compression Clothing
Constant input without collision. Continuous pressure against skin provides ongoing proprioceptive input. ₹800–3,000
3
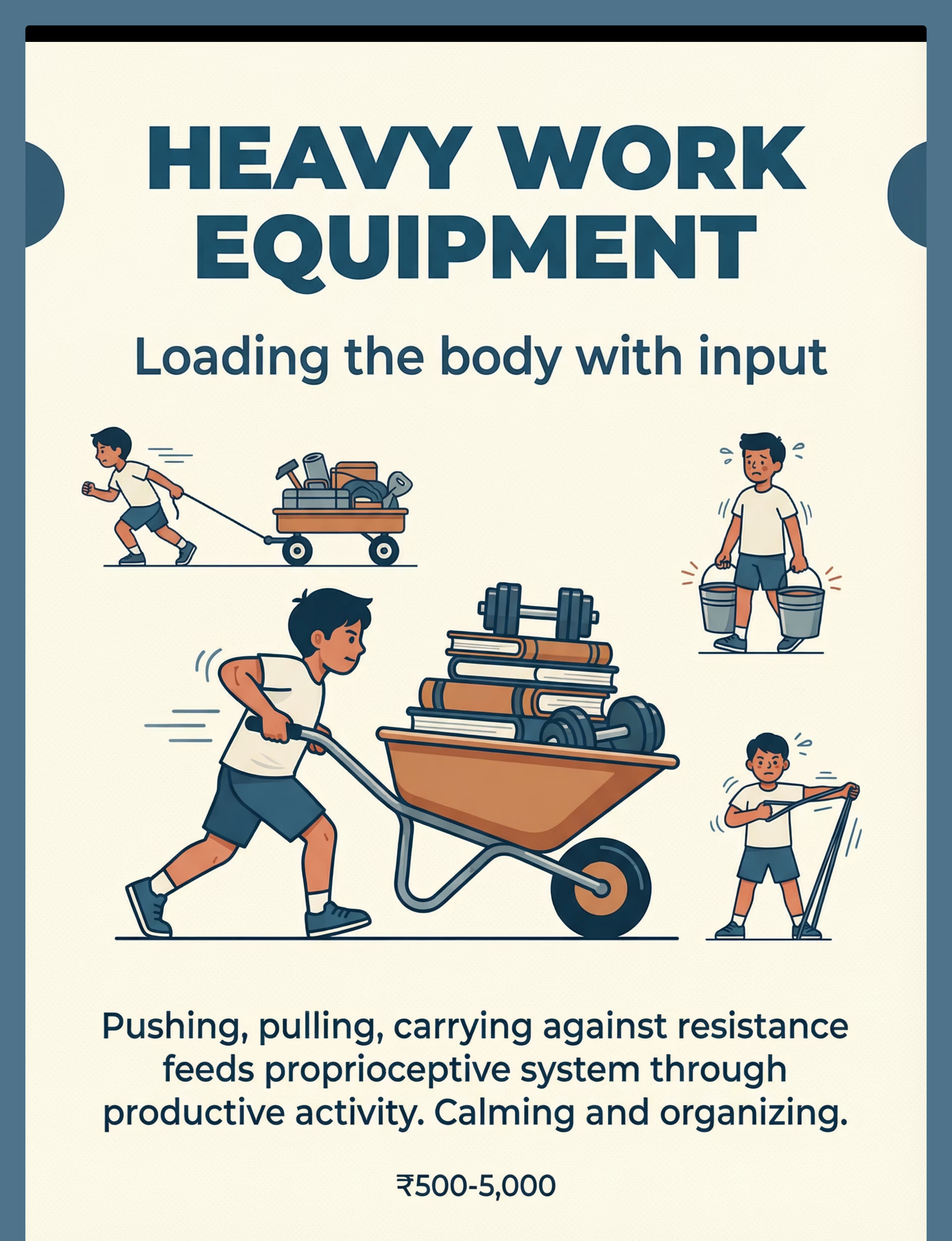
Heavy Work Activity Equipment
Loading the body with input. Wheelbarrows, wagons, weighted buckets, resistance bands. ₹500–5,000
4
Weighted Materials
Grounding input through pressure. Weighted blankets and lap pads provide proprioceptive information during calm activities. ₹1,500–6,000
5
Tunnels & Squeeze Machines
Controlled intense pressure. Resistance against the body during crawling delivers proprioceptive input through compression. ₹1,000–12,000
6
Trampolines & Bounce Equipment
Vertical impact, controlled and rhythmic. Repetitive impact through jumping loads joints rhythmically. ₹2,000–15,000
7
Therapy Balls & Steamrollers
Rolling and pressing deep input. Rolling pressure distributes deep proprioceptive input across the body surface. ₹800–3,000
8
Climbing & Hanging Equipment
Working hard against gravity. Muscles working against gravity produce intense proprioceptive input. ₹2,000–20,000
9
Rough-and-Tumble Play Structures
Structured crash and wrestle. Safe mats and rules transform roughhousing into therapeutic proprioceptive input. ₹1,500–8,000
Total Investment Range: ₹500–20,000. Start with essential starters: crash pad + heavy work activities, which can be DIY. See Card 10 for zero-cost alternatives.

DIY & Zero-Cost Alternatives — Start Today With What You Have
Not every family can order online. Not every village has same-day delivery. This card ensures you can start this afternoon with items already in your home. The WHO/UNICEF Nurturing Care Framework emphasises context-specific, equity-focused interventions. These DIY options are clinically valid.
Clinical Material | Household Substitute | Why It Works | |
Crash Pad (₹3,000–15,000) | Stack old mattresses, pile heavy cushions, bean bag chairs together. Cover with durable fabric. Place away from walls. | Same principle: absorbs impact while providing resistance. The body feels the crash without injury risk. | |
Body Sock (₹800–3,000) | Tight-fitting athletic compression clothing. Lycra fabric sewn into tube shape. Stretchy pillowcase for smaller children. | Continuous pressure against skin provides ongoing proprioceptive input. | |
Heavy Work Equipment (₹500–5,000) | Laundry baskets loaded with books. Buckets filled with water to carry. Push boxes across floor. Wall push-ups. Animal walks. Backpacks loaded with books. | Any activity requiring muscles to push/pull/carry against resistance loads the proprioceptive system. | |
Weighted Blanket (₹1,500–6,000) | Fabric pouches filled with rice or dried beans, sewn securely. Layer multiple heavy blankets. Weighted stuffed animals. | Weight pressing on the body provides constant proprioceptive information. Must be under 10% body weight. | |
Tunnel (₹1,000–12,000) | Large cardboard boxes with ends cut open. Blankets draped between furniture to crawl under. Couch cushion squeeze. Blanket "burrito roll." | Resistance against body during crawling = proprioceptive input through compression. | |
Trampoline (₹2,000–15,000) | Jump on mattresses (supervised). Hopscotch. Jump rope. Jumping jacks. Exercise ball bouncing. | Repetitive impact through jumping loads joints rhythmically. | |
Therapy Ball (₹800–3,000) | Any large, firm exercise ball. Couch cushions for rolling/pressing. Pillow steamroller (press firmly over limbs). | Rolling pressure distributes deep input across body surface. | |
Climbing Equipment (₹2,000–20,000) | Playground equipment. Safe furniture climbing (supervised). Tree climbing. Chin-up bar in doorframe with mat below. | Muscles working against gravity = intense proprioceptive input. | |
Rough Play Area (₹1,500–8,000) | Mattresses on floor. Established rules: safe zone only, stop means stop, no hitting. Supervised pillow fights. | Structure and rules make roughness safe and therapeutically valid. |
Safety First — Read This Before Starting Any Proprioceptive Activity
🔴 RED — Do Not Proceed If:
- Child has a recent injury to muscles, joints, or bones
- Child has a condition affecting connective tissue (Ehlers-Danlos, hypermobility) — consult physician first
- Child is severely distressed, in meltdown, or medically unwell
- Equipment shows wear, damage, or instability
- Child is under 2 years old for crash pad activities
- Weighted blanket exceeds 10% of child's body weight
- Any activity where child cannot exit freely
🟡 AMBER — Proceed With Modifications If:
- Child is mildly dysregulated — use calming input first
- First time using any new material — introduce gradually
- Child has co-occurring vestibular sensitivity — avoid spinning/bouncing initially
- Multiple children present — one at a time on equipment
- Child has had a recent meal — wait 30 minutes
🟢 GREEN — Safe to Proceed When:
- Child is alert, fed, and in a regulated or seeking state
- Equipment is appropriate for child's size and weight
- Supervising adult is present and attentive
- Environment is clear of hard surfaces near crash zones
- Child can communicate desire to stop
🛑 STOP IMMEDIATELY IF: Child shows distress, pain, fear, difficulty breathing, nausea, or any unexpected reaction. Session abandonment is not failure — it's data.
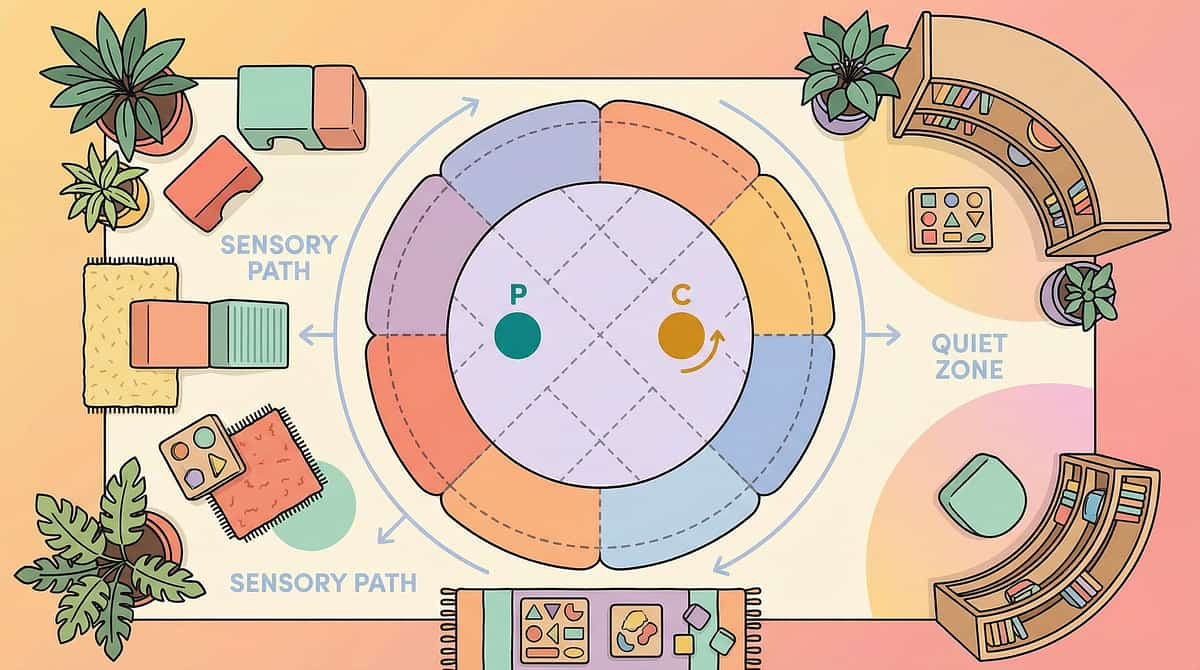
Set Up Your Space — The Physical Environment Matters
Spatial precision prevents 80% of session failures. A properly arranged space means safer crashes, more effective heavy work, and a clear signal to your child's nervous system that this is a designated space for proprioceptive input.
01
The Crash Zone (Centre of Room)
Place crash pad/cushion pile with at least 1 metre clearance from walls, furniture, and hard surfaces on all sides. The child needs running room AND safe overshoot space.
02
Heavy Work Station (Against Wall or Open Path)
Wheelbarrow/wagon/weighted items positioned for push/pull activities with a clear 3-metre path. Resistance bands anchored to stable furniture.
03
Compression Corner (Quiet Area, Soft Lighting)
Body sock, weighted blanket, and squeeze materials in a designated calming spot. This is where the child goes when they need input without impact.
04
Parent Position (Within Arm's Reach)
You need to see and reach the child at all times during impact activities. Position yourself where you can guide without blocking. Remove sharp-edged furniture, breakable items, and hard toys from the crash zone radius.

Is Your Child Ready? — The 60-Second Pre-Session Check
Starting a proprioceptive session when your child isn't ready reduces effectiveness and increases frustration for everyone. This quick readiness check takes 60 seconds and dramatically improves session outcomes.
✅ Full Readiness — All 7 Checked → 🟢 GO
- Child has eaten within the last 2 hours (not hungry)
- Child is not ill or in pain
- Child is awake and alert (not drowsy or just waking)
- No meltdown in the last 30 minutes
- Child shows signs of seeking (bouncing, crashing) OR is in a calm-alert state
- Environment is set up per Card 12
- Supervising adult is present and undistracted
🟡 5–6 Checked → MODIFY
- Skip crash pad activities; start with weighted blanket or compression
- Use heavy work at lower intensity
- Shorter session (5–7 minutes instead of 10–20)
🔴 4 or Fewer → POSTPONE
- Quiet compression activities (blanket burrito, gentle squeeze)
- Calm heavy work (carry one item, wall push-ups)
- Revisit when readiness indicators improve
The best session is one that starts right. A skipped session is better than a session started under the wrong conditions.

Step 1 — The Invitation (30–60 Seconds)
Every session begins with an invitation, not a command. The way you introduce the materials sets the emotional tone for everything that follows.
"Hey [child's name]! Look what we have today! Want to come CRASH on the big pad? Let's see how big a crash you can make!"Or, for heavy work entry: "I need your STRONG muscles! Can you help me push this heavy box? You're so strong — show me!"
Body Language That Works
- Get to child's eye level
- Use animated, energetic voice matching their energy
- Point to or touch the materials
- Model the activity briefly
What Acceptance Looks Like
- Child moves toward the materials
- Child's eyes light up
- Child begins the activity spontaneously
- Child laughs or vocalises excitedly
- Even just looking with interest
If Child Resists
- Ignores: Place materials in child's natural crash path
- Runs to wall: "Crash over HERE — the pad gives BIGGER crashes!"
- Not seeking now: Offer compression/weighted materials instead

Step 2 — The Engagement (1–3 Minutes)
The child is approaching the materials. Now deepen the interaction. Language, energy, and sequencing all matter here — your enthusiasm becomes their enthusiasm.
For Crash Pad Activities
"Ready... set... CRASH!" (Build anticipation with countdown)
"WOW! That was a huge crash! Want to do an even BIGGER one?"
"Can you crash like a bear? Like a frog? Like a cannonball?"
For Heavy Work Activities
"Push it alllll the way to the wall! You're SO strong!"
"Can you carry this big heavy book to the shelf? Your muscles are working so hard!"
"Let's do bear walks — hands and feet on the floor, walk like a big heavy bear!"
For Compression Activities
"Want to get in the body sock? Stretch it out as BIG as you can!"
"Let's make a burrito! I'm going to roll you up super tight!"
Child Response: Engaged
Actively using materials, smiling, requesting more, body relaxing into the input. Continue and celebrate!
Child Response: Tolerating
Using materials but not enthusiastically. Continue at current level — don't push for more intensity yet.
Child Response: Avoiding
Turning away, leaving the area, becoming distressed. Shift to a different material or a gentler approach.

Step 3 — The Core Therapeutic Action (3–8 Minutes)
This is the main event. The child's proprioceptive system is being fed. Three structured approaches address different aspects of proprioceptive need — combine them within a session based on your child's responses.
1
The Crash Protocol
Child runs and crashes onto crash pad — 3–5 crashes in sequence. Between crashes, insert heavy work: "Now push the big cushion back! Ready for another crash?" Vary crash types: running, jumping, backwards, rolling. After 3–5 crashes, transition to compression for 2–3 minutes.
2
The Heavy Work Circuit
Push a loaded wheelbarrow or box across the room (30 sec) → Carry weighted items to a destination (30 sec) → Animal walks across the room (1 min) → Wall push-ups: hands on wall, push hard 10 times (30 sec) → Repeat circuit 2–3 times.
3
The Compression Sequence
Body sock stretching and moving (2 min) → Weighted blanket or vest during calm activity (3–5 min) → Therapy ball steamroller: adult rolls ball firmly over child's back/legs (2 min).
Common Execution Errors: Don't stop the child mid-crash to correct form. Don't make it too structured — keep it playful. Don't be too gentle — these children need INTENSE input. Don't rush between activities — let each complete its input cycle.
Step 4 — Repeat & Vary (3–5 Minutes)
Therapeutic dosage: 3 good repetitions are worth more than 10 forced ones. Variety maintains engagement whilst ensuring the proprioceptive system receives adequate stimulation across different input channels.
Therapeutic Dosage
- Crash activities: 5–10 crashes per session
- Heavy work circuits: 2–3 complete circuits
- Compression activities: 2–5 minutes per activity
Crash Pad Variations
- Running crash vs. jumping crash vs. log-roll crash
- Crash with stuffed animals ("Your teddy wants to crash too!")
- Target crash: "Crash right HERE!"
- Countdown crash: "3... 2... 1... CRASH!"
- Slow-motion crash (builds body awareness and force grading)
Heavy Work Variations
- Change what's being pushed/pulled (different weights, items)
- Add pretend play: "You're a construction worker!"
- Include helping activities (carrying groceries, moving laundry)
- Partner heavy work (both push together, tug of war)
Satiation Indicators — Tank Is Full When:
- Interest drops — movements become listless
- Child voluntarily moves to a calming activity
- Body appears more relaxed and regulated
- Seeking behaviours have noticeably reduced
- Child initiates a different, calmer activity

Step 5 — Reinforce & Celebrate
The ABA Principle: Reinforce immediately, specifically, enthusiastically. Reinforcement delivered within 3 seconds of the desired behaviour is exponentially more powerful than praise given moments later.
For Safe Target Choice
"You crashed on the PAD! Not the wall — the PAD! That was so smart!"
For Heavy Work Effort
"Look how strong you are! You pushed that all the way across the room!"
For Regulation Outcome
"Your body is so calm now. You gave it what it needed. That's amazing."
What to Reinforce
- ✅ Crashing on the safe target (not wall, floor, or person)
- ✅ Going to the crash pad independently
- ✅ Completing heavy work activities
- ✅ Using body sock or compression when seeking input
- ✅ Any attempt to self-regulate through appropriate channels
- ✅ Telling you "I need to crash" (verbal self-advocacy)
Reinforcement Menu
- Verbal praise (always, immediately, specifically)
- Physical reinforcement: big bear hug, high-five, or deep pressure squeeze
- More crashing! (the activity itself is often the best reward)
- Preferred activity access after session completion
Celebrate the attempt, not just the success. A child who runs toward the crash pad but misses and hits the floor next to it tried. That's progress.

Step 6 — The Cool-Down (2–3 Minutes)
No session ends abruptly. The cool-down transitions from high-energy input to regulated calm — it signals to the nervous system that the feeding cycle is complete and it's time to consolidate.
The material put-away ritual is not just tidying — carrying the crash pad, moving the weighted items back to their place — this IS proprioceptive input during cool-down. The session ends with input, not absence of input.
"Your body got exactly what it needed. You did such a good job crashing safely. Now let's give your body a rest. The crash pad will be here for next time."
If the child resists ending: offer one more "bonus" crash, redirect to compression materials, use a visual timer, or remind: "The crash pad isn't going away. It will be here for you when you need it again."
Capture the Data — 60 Seconds, Right Now
Within 60 seconds of session end, record these 3 data points. Data transforms guesswork into precision — and your data contributes to the largest structured paediatric therapy outcomes database on Earth.
1
Crash Redirection Rate
How many times did the child crash on the safe target vs. unsafe surfaces? [Safe target crashes: ___] / [Unsafe crashes: ___] = ___% safe
2
Session Duration & Engagement
How long did the child stay engaged with the materials? [Minutes: ___] | Engagement level: [High / Medium / Low]
3
Post-Session Regulation
How was the child's regulation after the session compared to before? [Much calmer / Somewhat calmer / Same / More agitated]
4
Heavy Work Duration (Optional)
Total minutes of heavy work/compression activities: [___]
When your data enters GPT-OS®, it improves recommendations for every family navigating proprioceptive seeking. Your data helps every child like yours. And every child's data helps yours.

What If It Didn't Go As Planned? — Troubleshooting Guide
Every session is data. When things don't go as expected, the session hasn't failed — it has revealed something important about your child's current sensory state, material preferences, or timing needs.
Problem 1: "My child ignored the crash pad and crashed into the wall next to it."
Why: The crash pad is new; the wall is familiar. The body goes where it knows.
Fix: Make the crash pad more exciting — place it IN the child's natural crash path. Make crashing on it a game with countdowns, cheering, and celebration. Over time, the pad becomes the preferred target.
Fix: Make the crash pad more exciting — place it IN the child's natural crash path. Make crashing on it a game with countdowns, cheering, and celebration. Over time, the pad becomes the preferred target.
Problem 2: "My child got MORE wound up, not calmer."
Why: Some children need calming input BEFORE high-energy proprioceptive input. Starting with crash pad may dysregulate before it regulates.
Fix: Start with compression or weighted materials. Do heavy work (pushing, carrying) FIRST. Then introduce crash pad when the child is more organised.
Fix: Start with compression or weighted materials. Do heavy work (pushing, carrying) FIRST. Then introduce crash pad when the child is more organised.
Problem 3: "My child lost interest after 2 minutes."
Why: The activity may not have been intense enough, or the child's tank filled quickly today.
Fix: Increase intensity (bigger crashes, heavier work). Or accept that 2 minutes was enough — follow the child's lead. Some days are shorter sessions.
Fix: Increase intensity (bigger crashes, heavier work). Or accept that 2 minutes was enough — follow the child's lead. Some days are shorter sessions.
Problem 4: "My child crashed into ME instead of the pad."
Why: You may be the most familiar crash target. The child's body goes to what it knows.
Fix: Position yourself behind or beside the pad, not between the child and the pad. Redirect: "Crash on the PAD! I'll be right here cheering!"
Fix: Position yourself behind or beside the pad, not between the child and the pad. Redirect: "Crash on the PAD! I'll be right here cheering!"
Problem 5: "My child became aggressive/upset during the session."
Why: The child may have been overstimulated, or the activity triggered frustration rather than regulation.
Fix: Stop immediately. Offer calming compression. Do NOT push through distress. Try a gentler approach next session. Session abandonment is not failure — it's data.
Fix: Stop immediately. Offer calming compression. Do NOT push through distress. Try a gentler approach next session. Session abandonment is not failure — it's data.
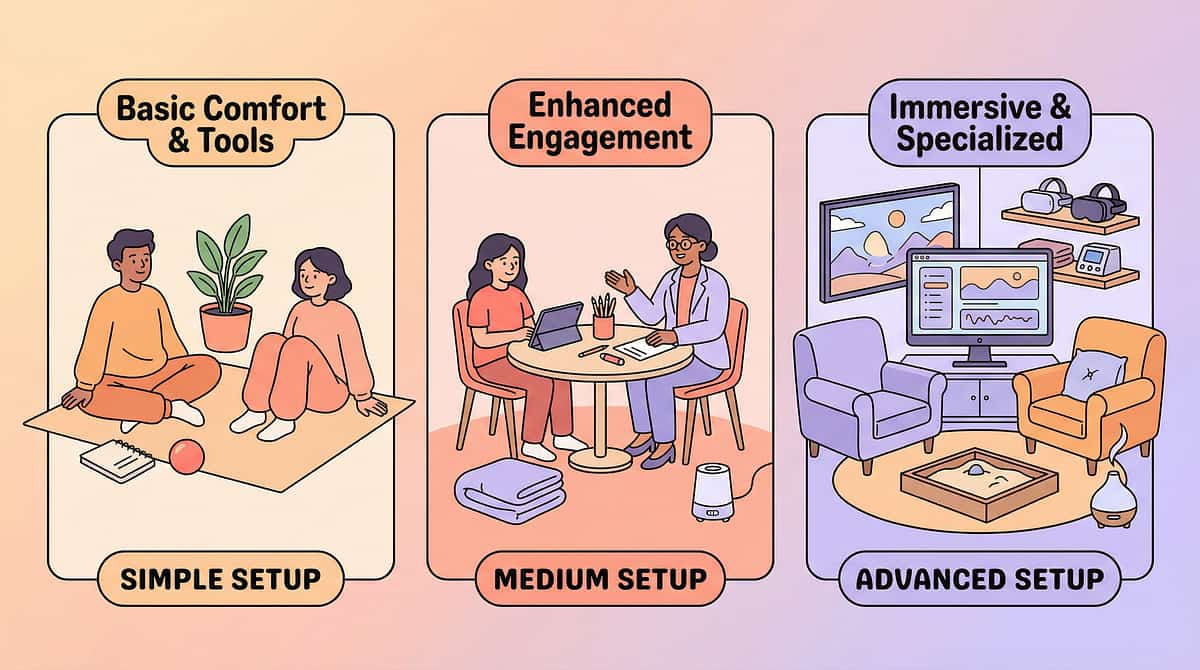
Adapt & Personalise — No Two Children Are Identical
The protocol described in Steps 1–6 is a starting point, not a rigid prescription. Every child presents with a unique sensory profile, age, threshold level, and co-occurring needs. Use these adaptations to match the intervention to your child.
1
Easier Version
For bad days, new children, or younger ages. Compression only (body sock, weighted blanket). Gentle heavy work (carrying one light item). No crash pad — only pressure activities. 5-minute session.
2
Standard Version
The protocol described in Steps 1–6. Crash pad + heavy work circuit + compression. 10–15 minute session. Varied activities. Data capture after every session.
3
Harder Version
For children who need more intensity or older children. Larger crash pad with running start. Weighted wheelbarrow. Climbing wall + hanging bar circuits. Resistance band heavy work. 15–20 minute sessions, multiple per day.
Ages 2–3
Shorter sessions, softer surfaces, constant supervision, play-based only.
Ages 4–6
Standard protocol, emerging self-direction, start teaching "I need to crash."
Ages 7–10
Longer sessions, more complex heavy work, social integration, self-advocacy skills.

ACT IV: The Progress Arc
Week 1–2: What to Expect — Setting Realistic Foundations
15%
Progress Point
You are at the beginning of the journey. Seeds are being planted.
4+
Sessions Target
Complete 4+ sessions in the first 14 days to establish the pattern.
What Progress Looks Like Now
- ✅ Child acknowledges the crash pad exists (looks at it, touches it)
- ✅ Child accepts one heavy work activity without refusing
- ✅ Child tolerates 30 seconds of compression
- ✅ One instance of crashing on the pad instead of the wall (even with prompting)
- ✅ You complete 4+ sessions in 14 days
What Is NOT Progress Yet (And That's Okay)
- ❌ Crash frequency has NOT significantly decreased
- ❌ Child does NOT independently seek the crash pad
- ❌ Force grading has NOT improved
- ❌ Peers are NOT yet safer around the child
If your child tolerates the crash pad for 3 seconds longer than last week — that's real progress. You're planting seeds, not harvesting. The neural pathways are forming beneath the surface.

Week 3–4: Consolidation Signs — Neural Pathways Forming
Something is shifting. You may not be able to see it clearly yet, but the nervous system is building new routes — safer, more organised pathways for proprioceptive input. Here's what to look for.
40%
Progress Point
Neural pathway formation is underway. The foundation is consolidating.
20-30%
Expected Reduction
Approximate decrease in unsafe crashing by end of weeks 3–4.
Consolidation Indicators
Child begins going to crash pad WITH prompting. Heavy work activities are now anticipated — child may seek them. Visible calming after proprioceptive input. Child may start communicating the need: pointing to crash pad, pulling you toward heavy work.
Behavioural Signals of Neural Change
Child hesitates before crashing into wall (awareness emerging). Child chooses crash pad some of the time without being told. Body appears more organised after sessions. Force grading begins improving in non-crash activities.
Parent Milestone
You may notice you're more confident too. You've started reading the crashing differently — not as destruction, but as communication. That shift in understanding IS the intervention working.

Week 5–8: Mastery Indicators — The Body Is Learning
Observable, measurable milestones signal that the proprioceptive system is developing new processing patterns. These are the moments parents describe as "something clicked." You'll know it when you see it.
75%
Progress Point
Mastery is unlocking. The body is learning to self-regulate.
50%+
Crash Reduction
Target reduction in unsafe crashing from baseline at mastery stage.
Mastery Criteria — Observable
- ✅ Child independently goes to crash pad when needing to crash
- ✅ Unsafe crashing reduced by 50%+ from baseline
- ✅ Heavy work used as self-regulation strategy
- ✅ Force grading improved: gentler touches, hugs that don't hurt
- ✅ Verbal or non-verbal communication of proprioceptive needs
Generalisation Indicators
- Skills appearing at school (movement breaks, weighted lap pad)
- Skills appearing with peers (slightly gentler play)
- Skills appearing in new settings (playground, grandparent's house)
When to Move to Next Level
If mastery criteria are consistently met for 2+ weeks → explore advanced techniques, reduce structured sessions, increase environmental integration.

Celebrate This Win — You Did This
You arrived on this page scared. Your child was crashing into walls, furniture, people. Bruises were accumulating — yours and theirs. Teachers were complaining. Other children were avoiding yours. You didn't know why your child needed to slam into everything, and you definitely didn't know what to do about it.
You Now Understand
This is proprioceptive seeking — a neurological need, not defiance.
You Now Have
9 categories of materials that channel the need safely.
You Now See
Your child going to the crash pad instead of the wall. Carrying heavy things with purpose. Calming under a weighted blanket. Using their body with emerging awareness.
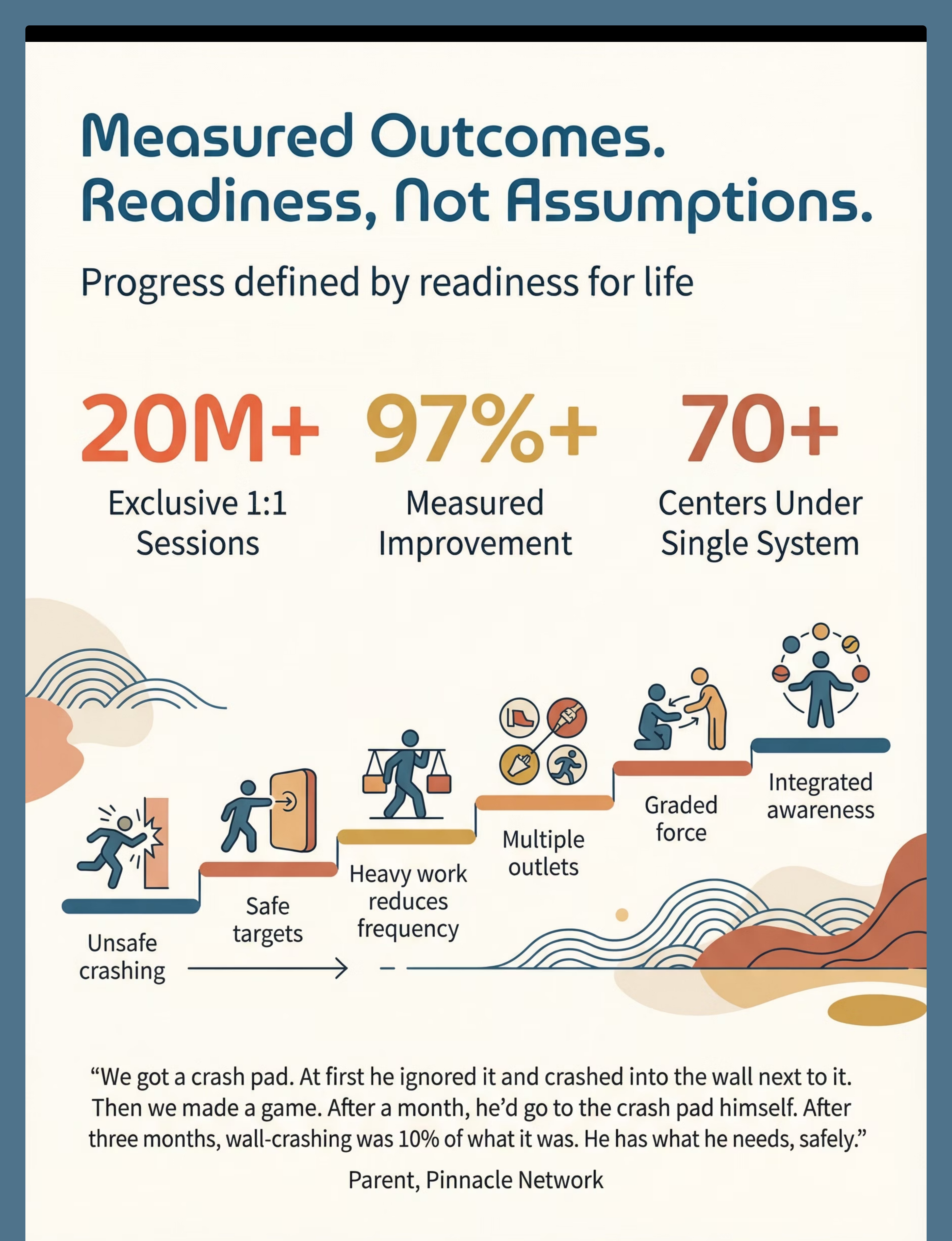
"Our son was a wall-crasher, furniture-launcher, human wrecking ball. We got a crash pad — just a basic one, put it in the living room. After a month, he'd go to the crash pad himself when he needed to crash. After three months, the wall-crashing was maybe ten percent of what it was. He still needs to crash — that hasn't changed. But now he knows WHERE to crash. The bruises are gone. The dread is gone."— Parent, Pinnacle Blooms Network
📸 Document this milestone. Photograph the crash pad with the wall untouched behind it. Write the date. This is evidence of transformation.
Red Flags — When to Pause and Seek Professional Guidance
Home intervention is powerful — and it works best within appropriate boundaries. These signals indicate that professional assessment is needed before continuing, or urgently.
🚩 Pause and Consult If:
- Crashing is causing significant injury to the child or others despite safe targets being available
- Crashing has NOT decreased at all after 8 weeks of consistent intervention
- Child crashes exclusively at people (not surfaces) — may have aggression component alongside sensory need
- Complete absence of pain response combined with other safety-unaware behaviours — needs medical evaluation
- Crashing combined with regression in other areas (speech, social engagement, self-care skills)
- Child becomes significantly more agitated after proprioceptive input (paradoxical response)
Escalation Pathway
Self-Resolve: Adjust technique using Card 22 modifications → Monitor 2 more weeks
Teleconsult: Book a virtual session with a Pinnacle OT → Professional guidance without travel
Clinic Visit: Comprehensive sensory processing evaluation → Full profile + individualised plan
📞 FREE National Autism Helpline: 9100 181 181 — 16+ languages, available 24/7. Trust your instincts — if something feels wrong, pause and ask. A professional evaluation is never wasted.
The Progression Pathway — Where You've Been, Where You're Going
This technique sits within a carefully designed sequence. Understanding the pathway before and after A-082 helps you see the bigger clinical logic — and plan your next steps with confidence.
Path A — Body Awareness Still Developing
→ A-085: 9 Materials That Help When Child Uses Too Much Force. Focus shifts from safe crashing to force grading and body control.
Path B — Child Also Seeks Spinning
→ A-083: 9 Materials That Help When Child Spins Constantly. Address vestibular seeking alongside proprioceptive needs.
Path C — Social Skills Need Work
→ Related social body techniques in the Social Domain. Gentle play skills, personal space awareness, peer interaction.
Related Techniques in Sensory Processing & Proprioception
If you've invested in materials for this technique, you're already equipped for several related interventions. The Canon material system is designed so that each purchase serves multiple therapeutic purposes across the sensory processing domain.
Technique | Difficulty | Materials You Already Own | Domain | |
A-080: Child Chews on Everything | Introductory | Body socks, compression clothing | Sensory Processing | |
A-081: Child Seeks Tight Squeezes | Introductory | Body socks, tunnels, weighted materials | Sensory Processing | |
A-083: Child Spins Constantly | Core | Trampolines, therapy balls | Sensory Processing | |
A-084: Child Has No Fear of Falling | Core | Crash pads, climbing equipment | Sensory Processing | |
A-085: Child Uses Too Much Force | Core | Heavy work equipment, weighted items | Sensory Processing | |
K-1055: Heavy Work Activities for Home | Introductory | All heavy work equipment | Motor Development |
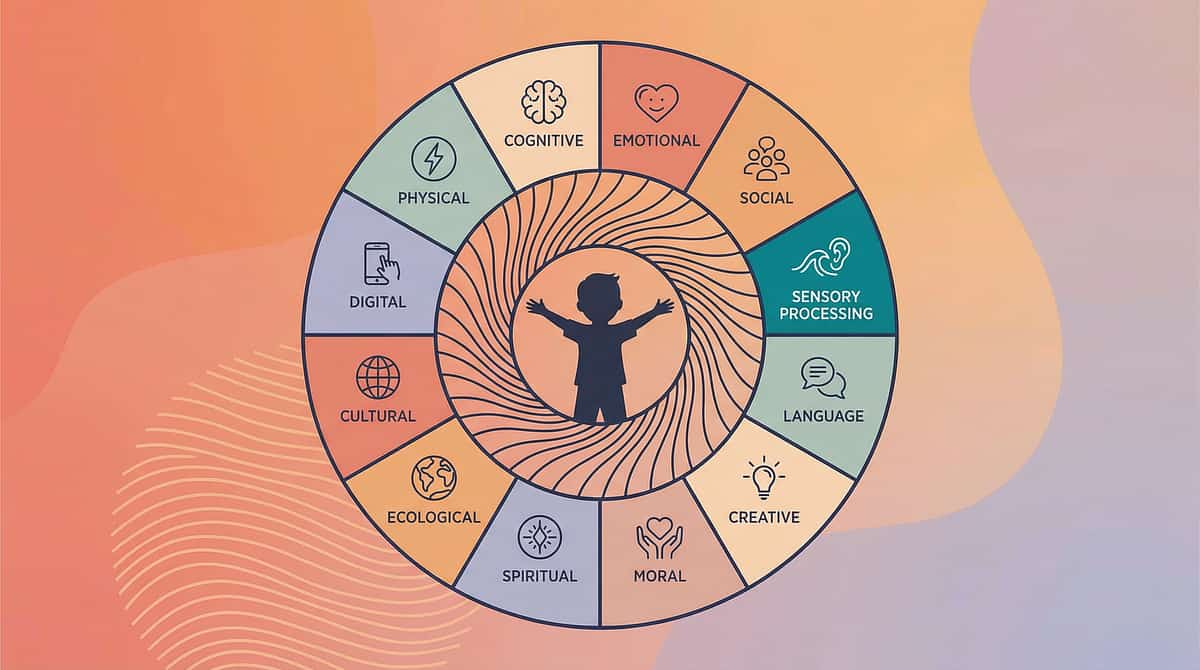
Your Child's Full Developmental Map — The Big Picture
This technique addresses the Sensory Processing domain — one of 12 developmental areas your child is growing across. Seeing the full map helps you understand where proprioceptive work sits within the broader picture of your child's development.
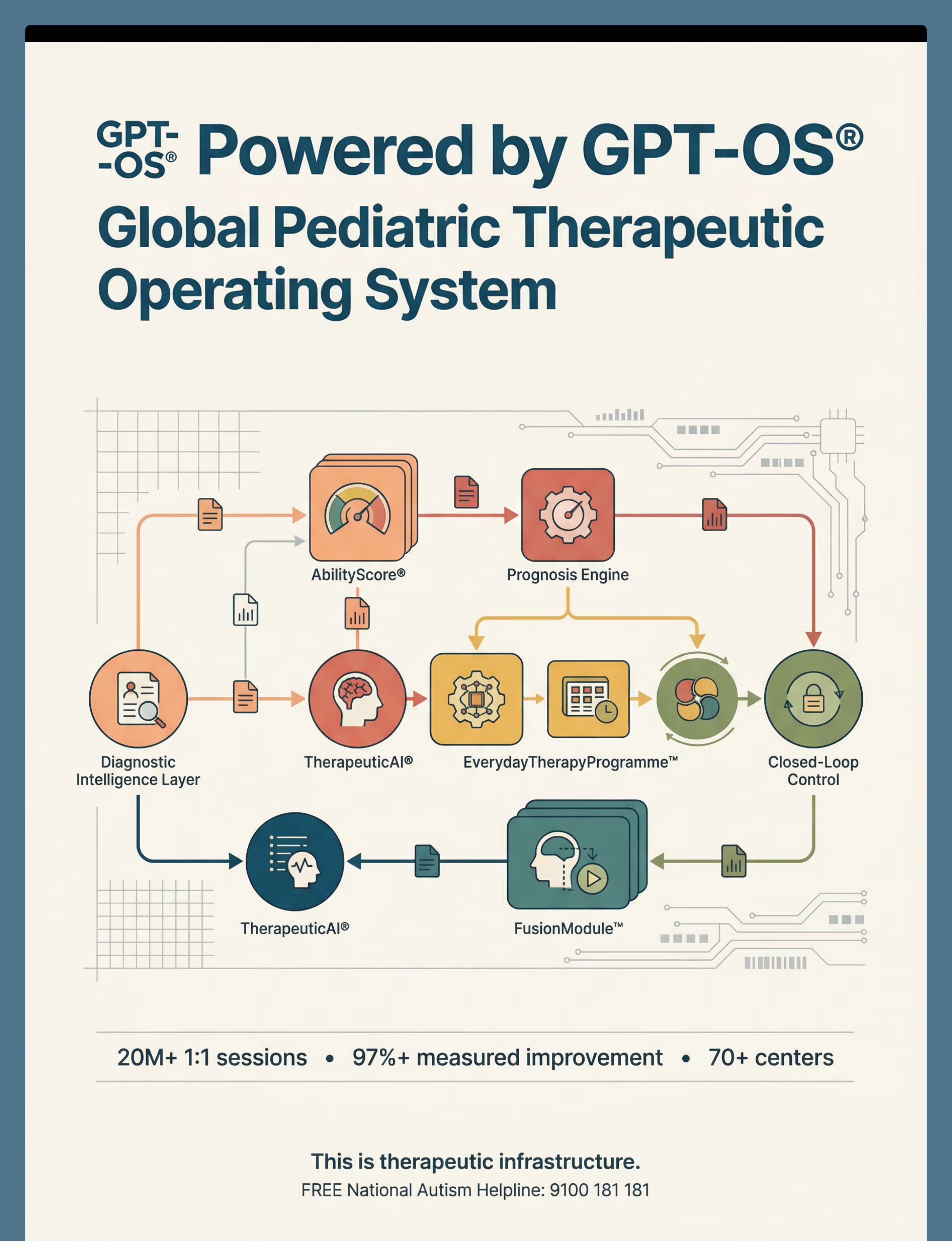
When you're ready, GPT-OS® can map your child's complete profile across all 12 domains and create a personalised intervention pathway that addresses multiple areas simultaneously through the FusionModule™.
ACT V: Community & Ecosystem
Families Who've Been Here — You're Not Walking This Alone
Family 1 — The Wall Crasher
Before: 4-year-old boy crashed into walls 15–20 times per hour. Bruises on forehead, shoulders. Teachers sending daily incident reports. Siblings refused to play near him.
After (12 weeks): Crash pad in living room, heavy work circuit before school, weighted vest at circle time. Wall crashing reduced to 1–2 times per day. Goes to crash pad independently.
"We went from dreading every minute to watching him run to his crash pad with a huge grin. Same kid. Same energy. Safe target."
Family 2 — The Human Wrecking Ball
Before: 6-year-old girl crashed into everything and everyone. Expelled from one school for "aggressive behaviour." No friends would come over. Parents exhausted and heartbroken.
After (16 weeks): Comprehensive sensory diet: crash pad, daily heavy work schedule, body sock for transitions, climbing wall in bedroom. Crashing into people reduced by 80%. Re-enrolled in school with accommodations. Two friends who enjoy rough play together (on mats, with rules).
"They called her aggressive. She wasn't. She was sensory starving."
From the Therapist's Notes:: "Both families saw the fastest progress when heavy work was scheduled throughout the day — not just during 'therapy sessions.' When the proprioceptive system gets fed continuously, the crisis crashes decrease."

Connect With Other Parents — Isolation Is the Enemy of Adherence
Families navigating proprioceptive seeking behaviours need each other. The parents who stick with intervention longest — and see the deepest outcomes — are almost always connected to a community of peers who understand.
Sensory Solutions WhatsApp Group
Join the Pinnacle Parent Community to connect with families navigating the same challenges. Share what works, ask what doesn't, and celebrate the wins together.
Pinnacle Parent Forum
The online forum at pinnacleblooms.org/community provides a searchable archive of parent experience, therapist contributions, and technique-specific threads — including a dedicated A-082 proprioceptive seeking thread.
Peer Mentoring Programme
Connect with an experienced parent who has already navigated crashing behaviours. They've been where you are. They can tell you what worked, what didn't, and when it started getting better.
Your Professional Support Team — Home + Clinic = Maximum Impact
Home-based intervention works best when supported by professional guidance. Think of it as a closed-loop system: your home sessions provide daily proprioceptive input, professional sessions provide assessment, guidance, and calibration.
Find Your Nearest Centre
70+ centres across India, each operating under GPT-OS® clinical standards. Matching your child's needs to the right clinical environment and therapist profile.
Therapist Matching
Get matched with an Occupational Therapist specialising in sensory integration and proprioceptive processing. Each match considers your child's age, profile, location, and goals.
Teleconsultation
Can't visit in person? Book a video session with a Pinnacle OT. Same clinical expertise, delivered to your living room — where the crash pad lives.
📞FREE National Autism Helpline: 9100 181 181 | 16+ languages | Available 24/7
The Research Library — For Parents Who Want to Go Deeper
Evidence for the curious parent. Ammunition for the school meeting. Validation for the sceptical grandparent. Every claim in this technique guide is anchored to peer-reviewed research — here is where to find it.
01
PRISMA Systematic Review (2024)
16 studies, 2013–2023. Confirms evidence-based practice status for sensory integration in ASD. → PMC11506176
02
Meta-Analysis — 24 Studies (2024)
Pooled analysis across social skills, adaptive behaviour, sensory processing, motor skills. → PMC10955541
03
Indian RCT — Home-Based Sensory Intervention (2019)
Padmanabha et al. Significant outcomes with parent administration. → DOI: 10.1007/s12098-018-2747-4
04
WHO Nurturing Care Framework (2018)
Global framework for early childhood development emphasising caregiver-delivered, equity-focused interventions. → nurturing-care.org
05
NCAEP Evidence-Based Practices Report (2020)
Classifies sensory integration as an evidence-based practice for autism. → ncaep.fpg.unc.edu

How GPT-OS® Uses Your Data — Transparency, Always
Every data point you record contributes to something larger than your individual child's progress. Transparency about how this works is not optional — it's a promise from Pinnacle Blooms Network.
What GPT-OS® Learns From A-082 Data
- Optimal crash pad introduction timing by age and sensory profile
- Heavy work scheduling patterns that produce fastest crashing reduction
- Which material combinations work best for different proprioceptive thresholds
- Progression velocity: how quickly children typically move through mastery stages
Privacy & Data Protection
- Your child's data is encrypted, anonymised for research, and never sold
- You own your data and can request deletion at any time
- Pinnacle Blooms Network® operates under Indian data protection regulations
- ISO/IEC 27001 Information Security standards applied
Your data helps every child like yours. And every child's data helps yours.
Watch the Reel — See the Materials in Action
Video modelling is classified as an evidence-based practice for autism by the National Clearinghouse on Autism Evidence and Practice (NCAEP, 2020). Multi-modal learning — visual + text + demonstration — improves parent skill acquisition significantly over text alone.
Crash Pad Techniques
Safe crashing guidance with running, jumping, and rolling variations demonstrated by a Pinnacle OT.
Body Sock Engagement
Strategies for introducing and maintaining engagement with body sock and compression materials.
Heavy Work Circuit
Complete heavy work circuit demonstration including animal walks, push/pull activities, and wall push-ups.
Steamroller + Climbing
Therapy ball steamroller technique and safe climbing/hanging demonstrations with safety guidance integrated.
Reel A-082 | Sensory Solutions Series — Episode 82 | Duration: 60–85 seconds
Share This With Your Family — Consistency Across Caregivers Multiplies Impact
If only one parent executes this technique, its impact is limited. When grandparents, spouses, school teachers, and nannies all understand the proprioceptive need and know the safe crash protocol, the child receives consistent intervention across every environment. WHO CCD Package research confirms multi-caregiver training as critical for intervention generalisation.
"Explain to Grandparents" Version
"[Child's name] crashes into things because their body needs intense physical input to know where it is in space. This is a neurological need called proprioceptive seeking, not bad behaviour. We've set up a crash pad — please direct all crashing to the pad. When [child] carries heavy things or wears the compression vest, that's therapy. Please support it."
Teacher/School Communication Template
"[Child's name] has proprioceptive seeking needs. They require: movement breaks with heavy work every 30–45 minutes, weighted lap pad during seated activities, designated crash space in the sensory corner, and patience with force grading — they're learning. These are evidence-based accommodations (see attached research summary). We would appreciate your partnership."
Frequently Asked Questions — From Parents Who've Been Where You Are
Q: Is crashing behaviour a sign of autism?
Proprioceptive seeking (including crashing) can occur in children with autism, sensory processing disorder, ADHD, and typical development. It is not diagnostic on its own. However, when combined with other developmental differences, it should be evaluated within a comprehensive assessment. Contact Pinnacle's FREE helpline (9100 181 181) for guidance.
Q: Will my child grow out of crashing?
The intensity of proprioceptive seeking may decrease with nervous system maturation, but the underlying processing pattern typically persists. With intervention, children learn to meet the need safely and functionally — the crashing doesn't disappear, but it transforms into healthy, regulated physical activity.
Q: How long before I see results?
Most families see initial signs of change within 2–4 weeks. Measurable reduction in unsafe crashing typically occurs by weeks 5–8. Full integration of safe proprioceptive strategies may take 3–6 months of consistent practice.
Q: Can I use a regular mattress instead of a crash pad?
Yes. Old mattresses, stacked cushions, and bean bags can serve as DIY crash zones. Commercial crash pads offer more durability and optimal density, but household alternatives work on the same principle. The key is having a designated, safe crash target.
Q: My child crashes more at school. What do I do?
Request a meeting to discuss sensory accommodations: movement breaks with heavy work, weighted lap pad, seating modifications, and designated proprioceptive input times. Share the research references from Card 34. Pinnacle can provide a professional letter supporting accommodations.
Q: Is this dangerous? Can heavy work or crash pads hurt my child?
When used according to the safety guidelines in Card 11, these materials and activities are safe. Crash pads absorb impact. Heavy work uses the child's own body weight. Weighted materials should follow the 10% body weight rule. Always supervise.
Q: My spouse thinks I'm encouraging bad behaviour by providing crash pads. How do I explain?
Share Card 03 (the neuroscience) and Card 37 (the grandparent version). Key message: providing safe outlets for a neurological need is no different than providing glasses for a child who can't see clearly. You're not encouraging crashing — you're channelling it safely whilst the nervous system develops.
Q: Should I stop my child from crashing completely?
No. Attempting to eliminate all crashing addresses the symptom, not the need, and often increases dysregulation. The goal is providing safe outlets (WHERE to crash) and additional proprioceptive input (heavy work, compression) that reduces the URGENCY of crashing.
Your Next Step — Start Now
You've read the science. You understand the need. You have the materials list and the protocol. The only thing left is to act — and every day you act is a day your child's nervous system gets the input it's been asking for.
🟢 Start This Technique Today
Download the session guide + tracking sheet + material checklist. Everything you need to run your first session this afternoon.
📞 Book a Consultation
Connect with a Pinnacle OT for personalised guidance. Or call FREE: 9100 181 181 (16+ languages, 24/7). Professional support, on your terms.
🔄 Explore the Next Technique
A-083: 9 Materials That Help When Child Spins Constantly. Continue building your child's sensory diet with the next technique in the series.
Validated by the Pinnacle Blooms Consortium
OT • ABA • SpEd • NeuroDev
Preview of 9 materials that help when child crashes into things Therapy Material
Below is a visual preview of 9 materials that help when child crashes into things therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.







Link copied!

The Pinnacle Promise
From fear to mastery. One technique at a time.
You arrived here scared, exhausted, and uncertain. Your child was crashing into everything, and you didn't know why or what to do. Now you understand the proprioceptive system. You have 9 evidence-based material categories, a clinical execution protocol, progress markers, and a community of families who've walked this path.
Your child's body will always need proprioceptive input. What changes is how that need gets met.
Pinnacle Blooms Network®
Built by Mothers. Engineered as a System.
20M+ sessions • 97%+ measured improvement • 70+ centres
OT • SLP • ABA • SpEd • NeuroDev • CRO • WHO/UNICEF-Aligned
20M+ sessions • 97%+ measured improvement • 70+ centres
OT • SLP • ABA • SpEd • NeuroDev • CRO • WHO/UNICEF-Aligned
Free Support
📞9100 181 181
FREE National Autism Helpline
16+ languages | 24/7
FREE National Autism Helpline
16+ languages | 24/7
Medical Disclaimer: This content is educational. It does not replace assessment by a licensed occupational therapist, sensory integration specialist, or healthcare provider. Persistent crashing behaviours, especially when combined with other developmental concerns, should be evaluated within a comprehensive sensory processing and developmental assessment. Individual results may vary. Statistics represent aggregate outcomes across the Pinnacle Blooms Network.
Legal: © 2025 Pinnacle Blooms Network®, unit of Bharath Healthcare Laboratories Pvt. Ltd. All rights reserved. CIN: U74999TG2016PTC113063 | DPIIT: DIPP8651 | MSME: TS20F0009606 | GSTIN: 36AAGCB9722P1Z2
Legal: © 2025 Pinnacle Blooms Network®, unit of Bharath Healthcare Laboratories Pvt. Ltd. All rights reserved. CIN: U74999TG2016PTC113063 | DPIIT: DIPP8651 | MSME: TS20F0009606 | GSTIN: 36AAGCB9722P1Z2