"She Cries for Everything. I'm Always Guessing What's Wrong."
If your child's every need arrives as a cry, a scream, or a meltdown — and you're exhausted from decoding what they actually want — you're not failing as a parent. Your child is using the only communication tool they currently have.

You Are Among Millions of Families Navigating This Exact Challenge
Across India — in homes in Chennai, Hyderabad, Delhi, Pune, Bengaluru — parents are waking up to this exact morning. The crying that means everything and nothing. The guessing. The exhaustion. The guilt that somehow you should understand your own child better. You should know: this is one of the most common challenges in pediatric development. And it is one of the most effectively addressed — when the right tools are introduced in the right order.
1 in 36
Children with ASD Globally
CDC, 2023. The majority experience delayed functional communication as a primary challenge.
80%
Rely on Crying as Primary Communication
Children with ASD who use crying, screaming, or challenging behaviour at some developmental stage. (PRISMA Review, PMC11506176, 2024)
97%+
Show Measurable Improvement
Children receiving structured FCT at Pinnacle centers improve their Communication Readiness Index within 8–12 weeks. (GPT-OS® Real-World Evidence, 20M+ sessions)

Why Crying Persists: The Neuroscience in Plain English
The Neurological Truth
When a child has not yet developed efficient cortical pathways for intentional communication, the limbic system (the brain's emotional core) activates faster than the prefrontal cortex (the brain's planning and language centre).
In plain terms: the feeling arrives before the words do. The body cries before the brain can form a request. This is a wiring difference, not a behaviour choice.
Carr & Durand's foundational FCT principle (JABA, 1985): Efficiency drives behaviour. Whichever communication method gets results fastest will be repeated. If crying gets faster results than pointing, the child will cry. If pointing reliably gets faster results — pointing wins.
The FCT Bridge
Functional Communication Replacement Training works by creating external scaffolding — picture cards, buttons, signs, objects — that gives the prefrontal cortex a shortcut.
A child who cannot yet form "I want juice" in spoken words CAN learn to hand a picture of a juice box. Same message. Same outcome. Less distress for everyone.
Key Research
Carr & Durand (1985) JABA | Mirenda P. (2003) Language, Speech, and Hearing Services in Schools | DOI: 10.3389/fnint.2020.556660 — Frontiers in Integrative Neuroscience
Your Child's Communication Journey: A WHO Developmental Map
Crying as primary communication is developmentally appropriate at 0–12 months. When the transition to intentional signalling is delayed — whether due to autism, speech delay, sensory processing differences, or motor challenges — crying remains the most efficient tool. This is not regression. This is an incomplete developmental transition. FCT addresses this transition directly.
6–9 Months
Cries to signal needs. Begins proto-declarative gestures.
12 Months
First signs emerge. Proto-imperative pointing develops.
18 Months
First words emerge (10–50 word vocabulary).
24 Months
Two-word combinations: "more juice," "help me."
36 Months
Sentences forming. FCT fully replaces crying as primary communication tool.
Common Co-occurring Challenges: Sensory processing differences (increase distress-based crying) | Limited joint attention (reduces incidental communication learning) | Motor planning difficulties (may delay gesture/sign emergence). WHO Care for Child Development (CCD) Package — implemented across 54 countries. PMC9978394

Clinical Confidence Rating: Level I Evidence
Finding 1 — FCT is the Gold Standard
Classified as Evidence-Based Practice by NCAEP (2020). Across 40+ years of research, FCT consistently shows that teaching an efficient alternative communication reduces problem behaviour — including crying — when the alternative is more effective and efficient than the problem behaviour.
Carr & Durand, 1985 | NCAEP EBP Report, 2020
Finding 2 — AAC Does Not Delay Speech
Multiple systematic reviews confirm the opposite of the common fear: AAC use supports, not replaces, speech development. Children who use AAC show equal or greater verbal communication development compared to those who do not.
Mirenda P, 2003 | ASHA Evidence Maps
Finding 3 — Indian Context Validated
Home-based communication interventions in Indian pediatric populations demonstrate significant outcomes when caregiver training is included. Parent-implemented FCT is both feasible and effective in Indian joint household contexts.
Padmanabha et al., Indian J Pediatr, 2019 | DOI: 10.1007/s12098-018-2747-4
Finding 4 — Pinnacle Real-World Evidence
97%+ of children receiving structured FCT under GPT-OS® governance at Pinnacle centers show measurable improvement in Communication Readiness Index within 8–12 weeks. Across 20M+ exclusive 1:1 sessions.
40+
Years of Research
Hundreds of peer-reviewed publications supporting FCT as the standard of care.
97%+
CRI Improvement
Children at Pinnacle centers show measurable progress within 8–12 weeks.

Functional Communication Replacement Training (FCT)
Technique B-137
Domain B — Social Communication
Parent-Friendly Alias:"From Tears to Tools" — Teaching Your Child to Ask Instead of Cry
What FCT Does
- Identifies what the crying is communicating (request, protest, help-seeking, emotion)
- Teaches a specific, achievable alternative signal for that function
- Ensures all caregivers honour the signal faster than they respond to crying
- Systematically generalises the signal across settings, people, and contexts
Who It's For
Children aged 12 months – 6 years (highest impact window) who:
- Cry as their primary means of requesting or protesting
- Have limited pointing, gesturing, signing, or verbal requests
- Show communication-based frustration or distress
Session Format
- Duration: 5–15 minute structured sessions
- Frequency: Daily — embedded in natural routines
- Age Range: 12 months – 6 years
Speech-Language Therapy
Primary lead for FCT design and AAC selection.
Applied Behaviour Analysis
Behavioural architecture and differential reinforcement.
Occupational Therapy
Sensory and motor support for signal execution.
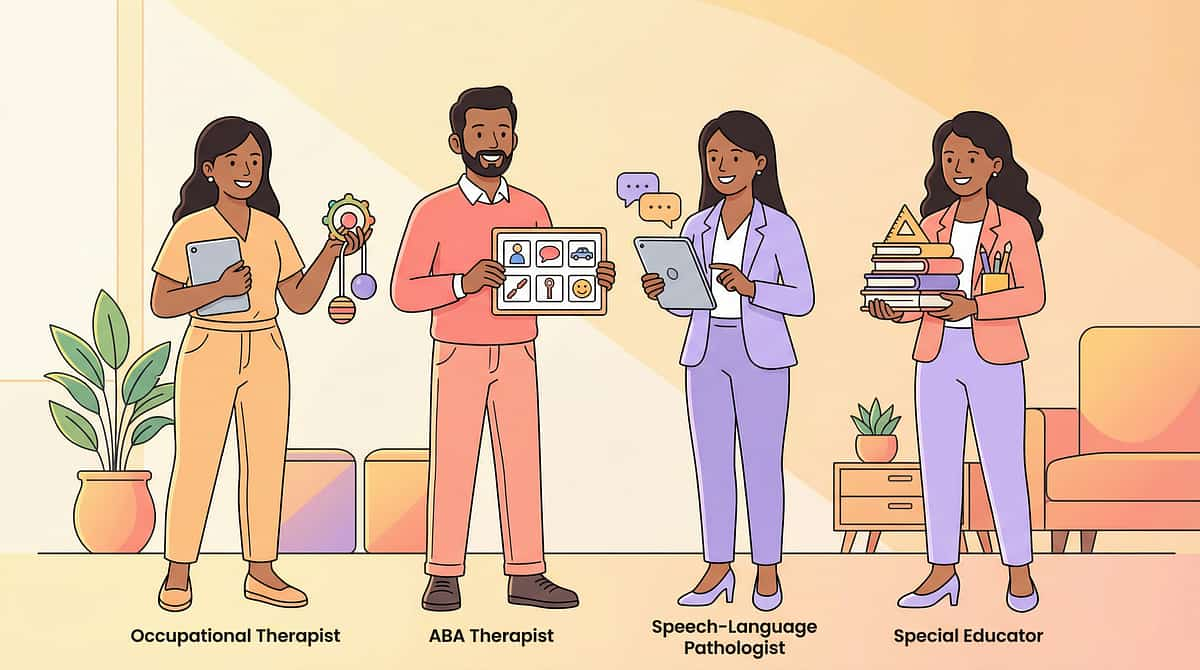
The Consortium Behind This Technique: 5 Disciplines, One Direction
"This technique crosses therapy boundaries because the brain doesn't organise by therapy type. A child communicating for the first time is simultaneously achieving a speech milestone, a behavioural goal, a sensory regulation success, and a social-emotional breakthrough." — Pinnacle Blooms Consortium
1
Speech-Language Pathologist (SLP)
Primary FCT Lead. Conducts communication function assessment, selects the initial AAC system or gesture, designs symbol vocabulary, and trains caregivers in responsive communication. At Pinnacle, SLPs hold clinical authority over all FCT programme design.
2
BCBA / ABA Therapist
Behavioural Architecture Lead. Analyses antecedents, behaviours, and consequences maintaining the crying pattern. Designs the differential reinforcement protocol ensuring the new signal consistently outcompetes crying for reinforcement. Manages extinction burst protocols.
3
Occupational Therapist (OT)
Sensory & Motor Support. Addresses underlying sensory processing and fine motor demands to ensure the child can physically execute the chosen signal — pressing a button, handing a card, making a sign.
4
Special Educator (SpEd)
Environmental Generalisation Lead. Ensures FCT signals are embedded in learning environments, school routines, and structured activities. Consistency across the educational setting is critical for generalisation.
5
Neuro-Developmental Paediatrician
Medical Clearance. Rules out medical causes of excessive crying (pain, GI distress, ear infection, dental issues, sleep deprivation). Medical clearance is the first step in any FCT programme.

Precision Targets: What FCT Is Actually Building
🎯 Primary Target
Functional Communication Signal Acquisition. The child learns at least one reliable, consistent signal to replace crying for their most frequent communication function — requesting preferred items, protesting non-preferred activities, seeking help.
Observable indicator: Child uses signal independently, without prompting, in at least 3 different contexts within 8 weeks.
🎯🎯 Secondary Targets
Reduction in Communication-Based Distress. As signals become efficient, crying for communication purposes decreases measurably. Note: emotional crying (genuine distress, pain, sadness) is expected to remain and is not targeted for reduction.
Signal Generalisation Across People. The signal works not just with the primary caregiver but across all household members. This requires caregiver training as a non-negotiable component.
Observable indicator: Frequency of communication-based crying decreases by 50%+ within 8–12 weeks.
🎯🎯🎯 Tertiary Targets
Foundation for AAC System Expansion. The first FCT signal is typically simple (one picture, one button, one sign). As reliability builds, the vocabulary expands.
Caregiver Confidence and Reduced Family Stress. When communication works, the entire family ecosystem de-stresses. Parents report significant reduction in household tension within 4–6 weeks.
Social Participation Increase. Children who can communicate their needs participate more fully in family meals, outings, play, and school activities.
9 Materials That Help Moving from Crying to Signals
Pinnacle 128 Canon Materials System
Clinically Validated

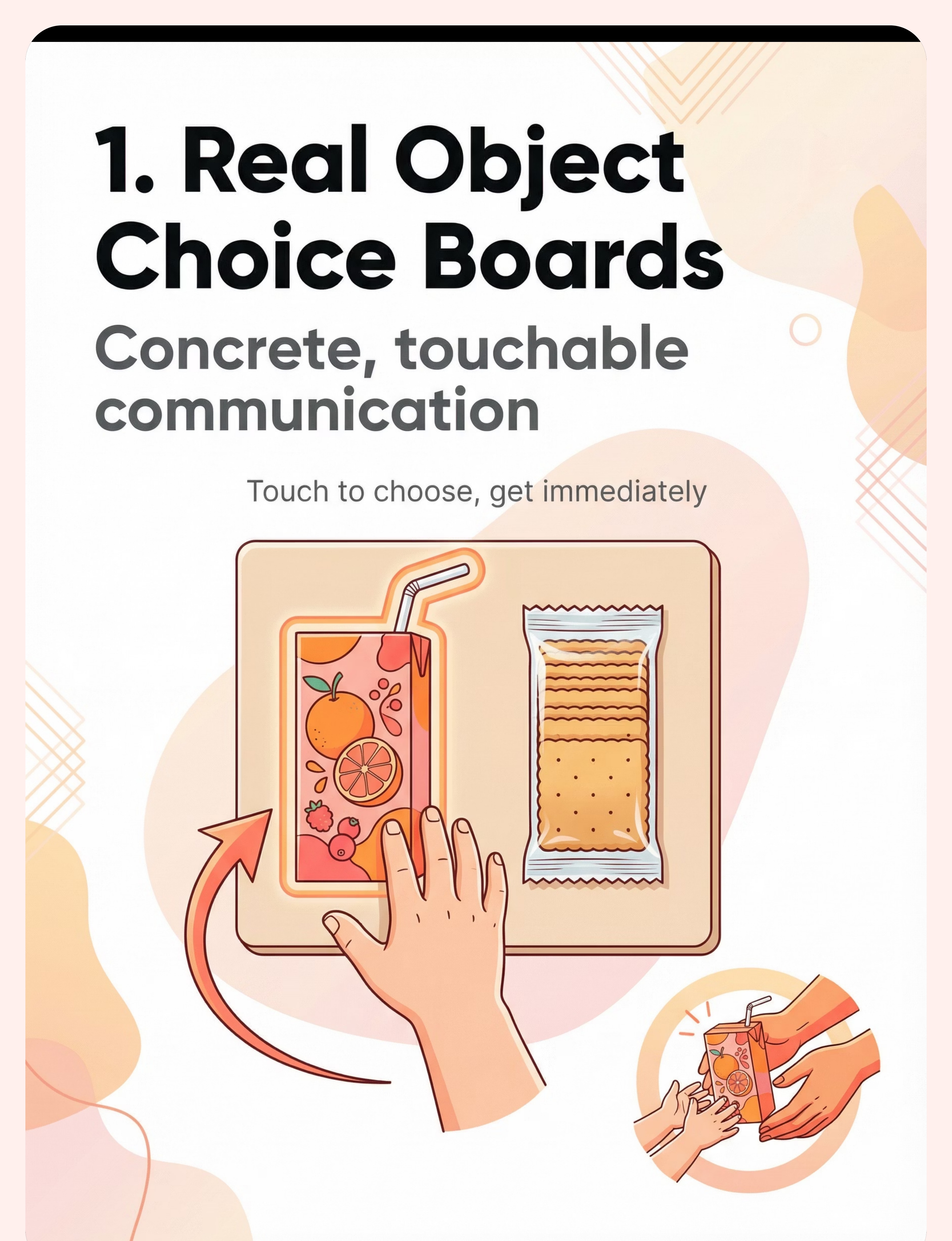
1. Real Object Choice Boards
Two real objects mounted on a tray or velcro board. Child touches what they want and receives it immediately. Why it works: Bypasses symbolic processing entirely. Maximum efficiency for earliest-stage learners. Price: ₹200–1,000 | DIY: Cookie sheet + velcro + real containers. Cost: ₹0–200.

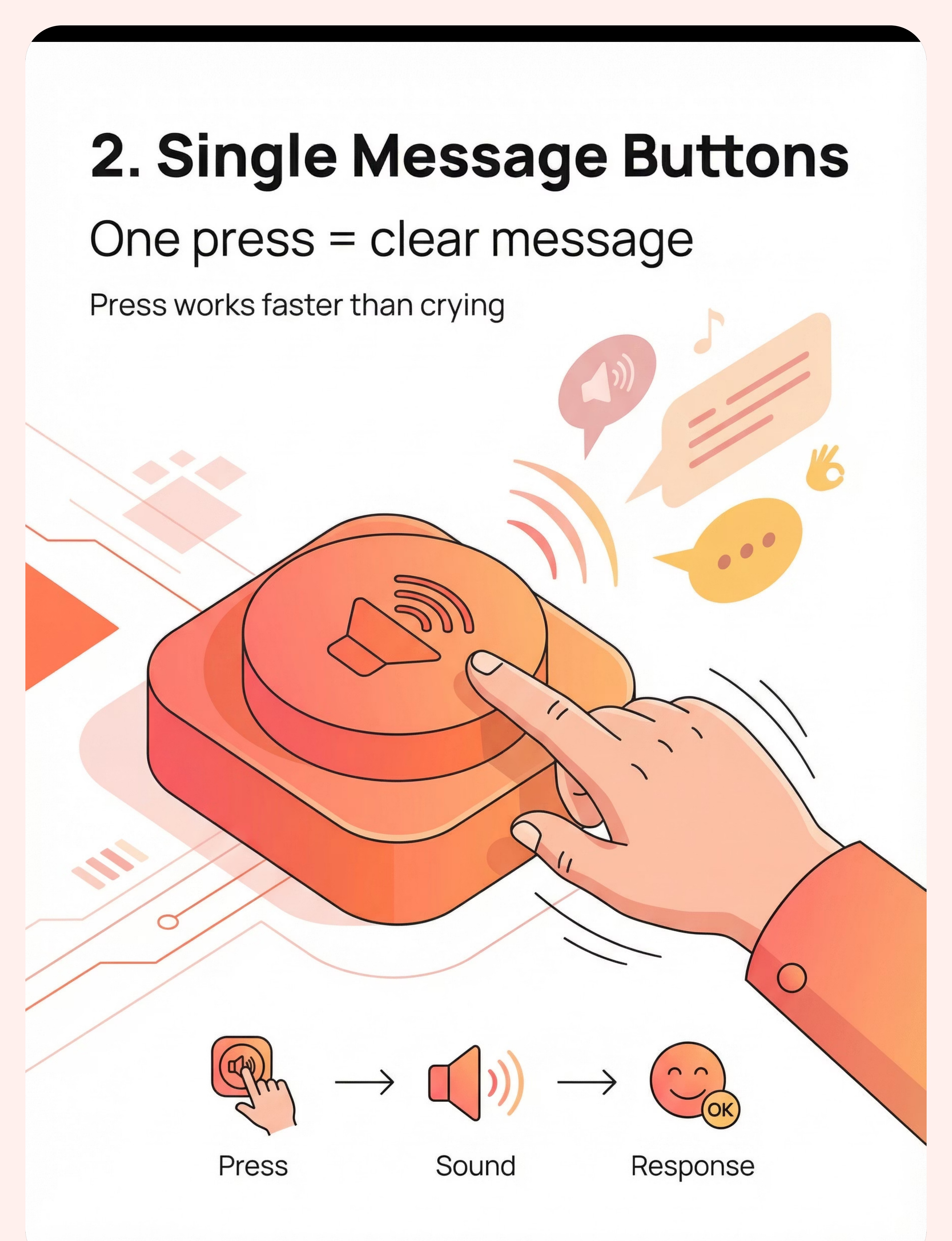
2. Single Message Buttons
One large button, pre-recorded with one message ("More please," "Help me," "I want"). Press = immediate, clear communication. Why it works: One motor action = one unambiguous message. Highest efficiency for single-function requests. Price: ₹1,500–6,000.

3. First Words Picture Cards
Laminated cards for core vocabulary: eat, drink, play, help, more, stop, no, all done, toilet. Child hands picture, receives referent. Why it works: PECS — 30+ years, Level I evidence. Price: ₹300–2,000 | DIY: Print + laminate. Cost: ₹150–300.

Materials 4–6: Signs, Emotions & Request Strips

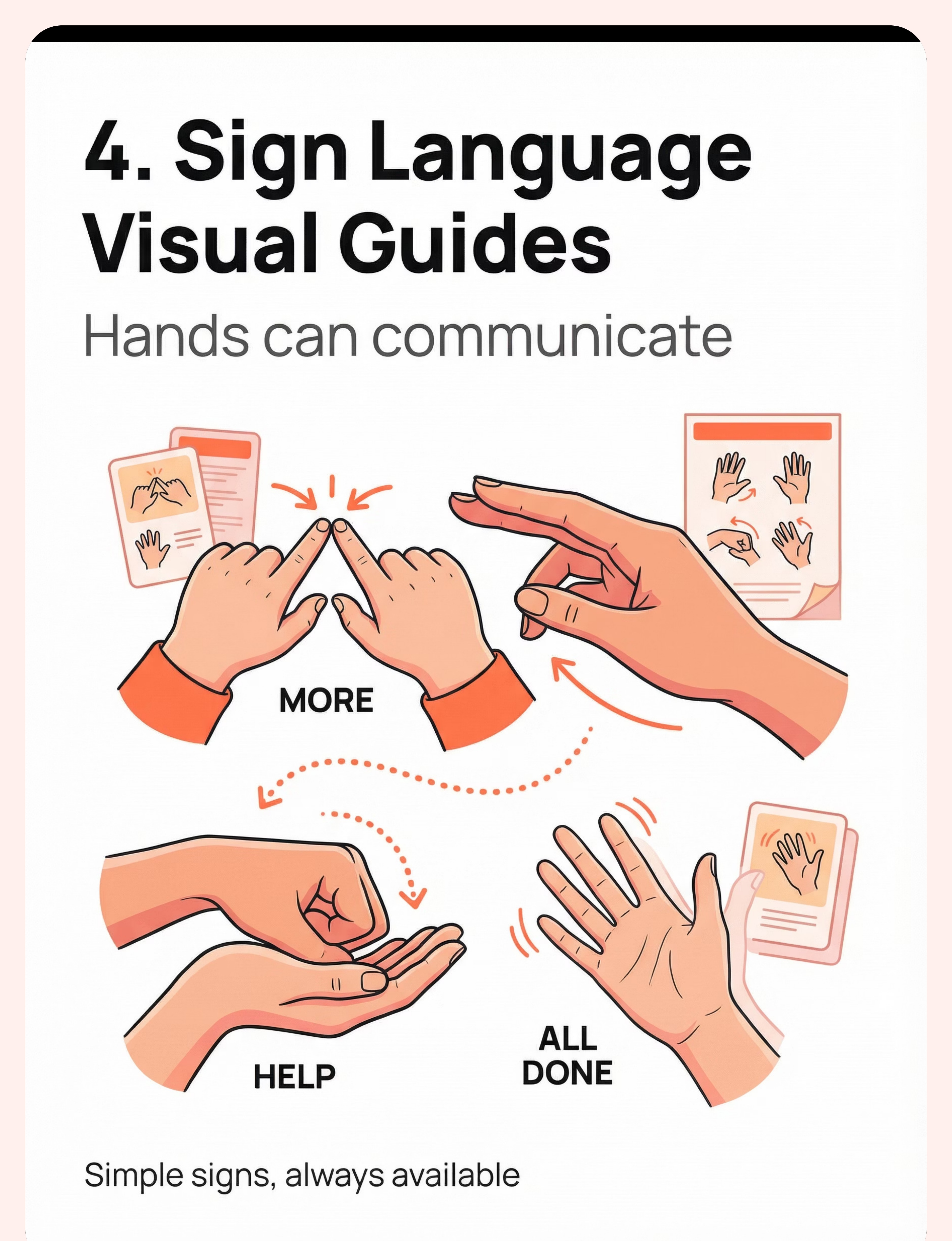
4. Sign Language Visual Guides
Poster or card set showing 5 core signs: MORE, HELP, EAT, DRINK, ALL DONE. Bodies can communicate before voices are ready. Why it works: No equipment needed. Always available. Motor approximations are accepted. Price: ₹200–1,500. Canon: Everything Sign Language Book (₹706).

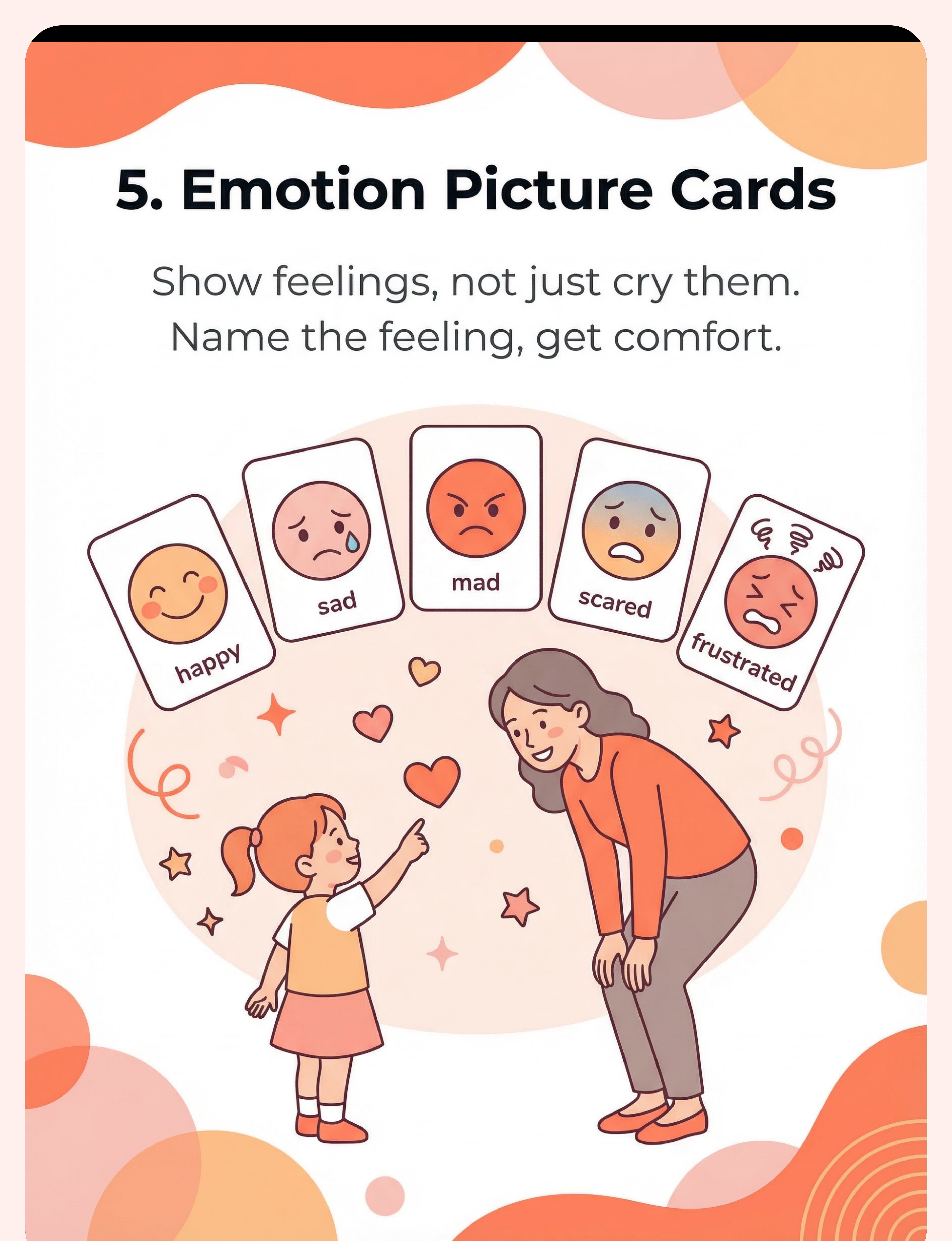
5. Emotion Picture Cards
Cards showing happy, sad, mad, scared, frustrated, tired. Child points to or presents card. Feelings get named, not just cried. Why it works: Separates emotional communication (feelings) from requesting communication (wants). Different FCT pathway, same principle. Price: ₹200–1,500 | DIY: ₹100–200.

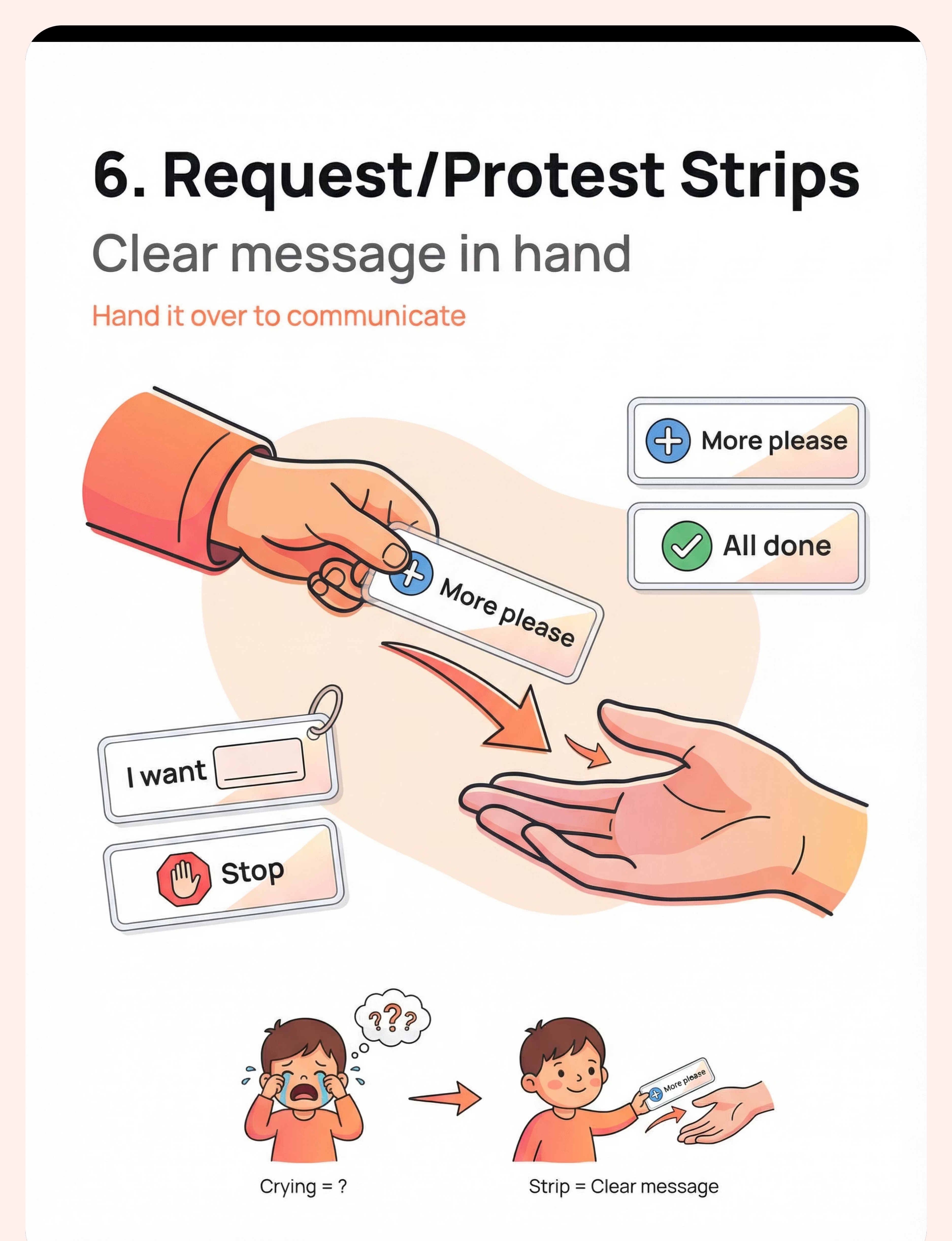
6. Request / Protest Strips
Portable laminated strips: "I want ___", "Stop please", "More", "All done", "No thank you". Child hands strip — crystal clear message. Why it works: Portable. Always available. Covers both requesting AND protesting functions in one system. Price: ₹200–1,000 | DIY: ₹150–300.

Materials 7–9: Help Cards, AAC Apps & Calm-Down Kits
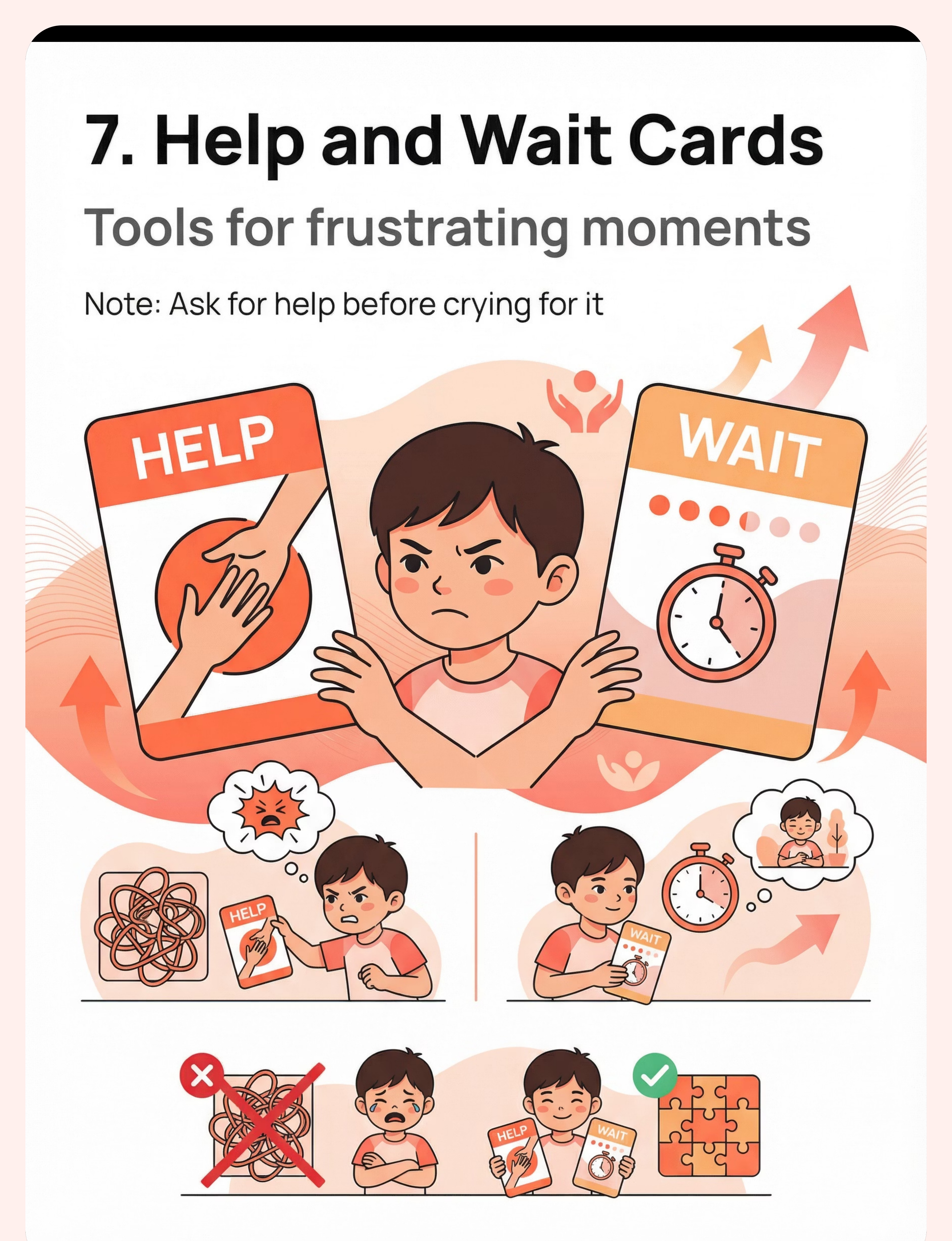
7. Help and Wait Cards
"HELP" card child hands to adult when stuck. "WAIT" visual timer/card for teaching delayed gratification without meltdown. Why it works: Targets two of the most common crying triggers: task difficulty and waiting. Gives child control over these moments. Price: ₹300–2,000.

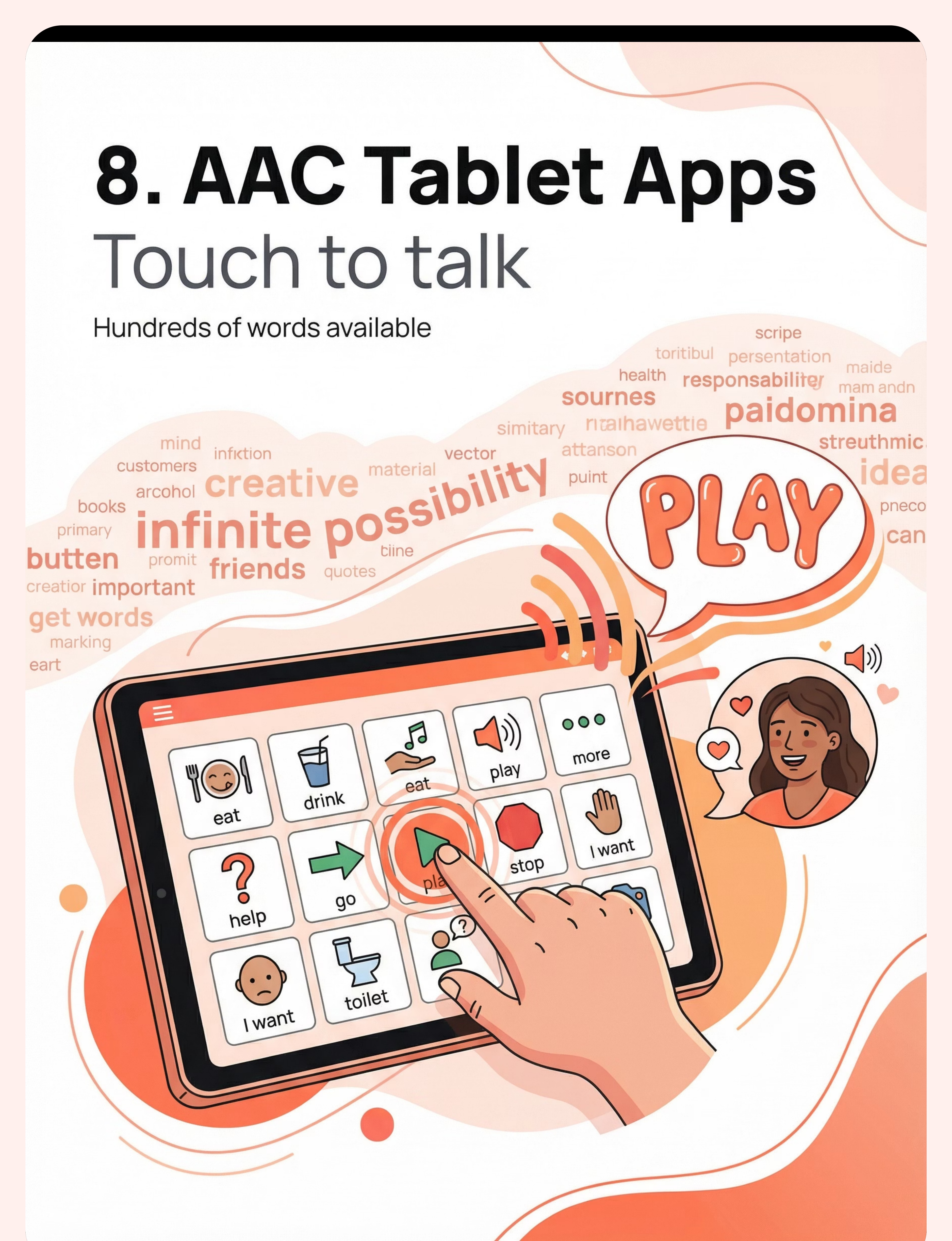
8. AAC Tablet Apps
Apps on phone/tablet that speak for the child. Touch picture → hear word. Whole vocabulary at fingertips. Why it works: Unlimited vocabulary potential. Bridges to speech development. Price: ₹0–15,000 (LetMeTalk: Free | Avaz AAC: ₹2,500/yr). Recommended: Avaz AAC — Indian company, Indian languages supported.
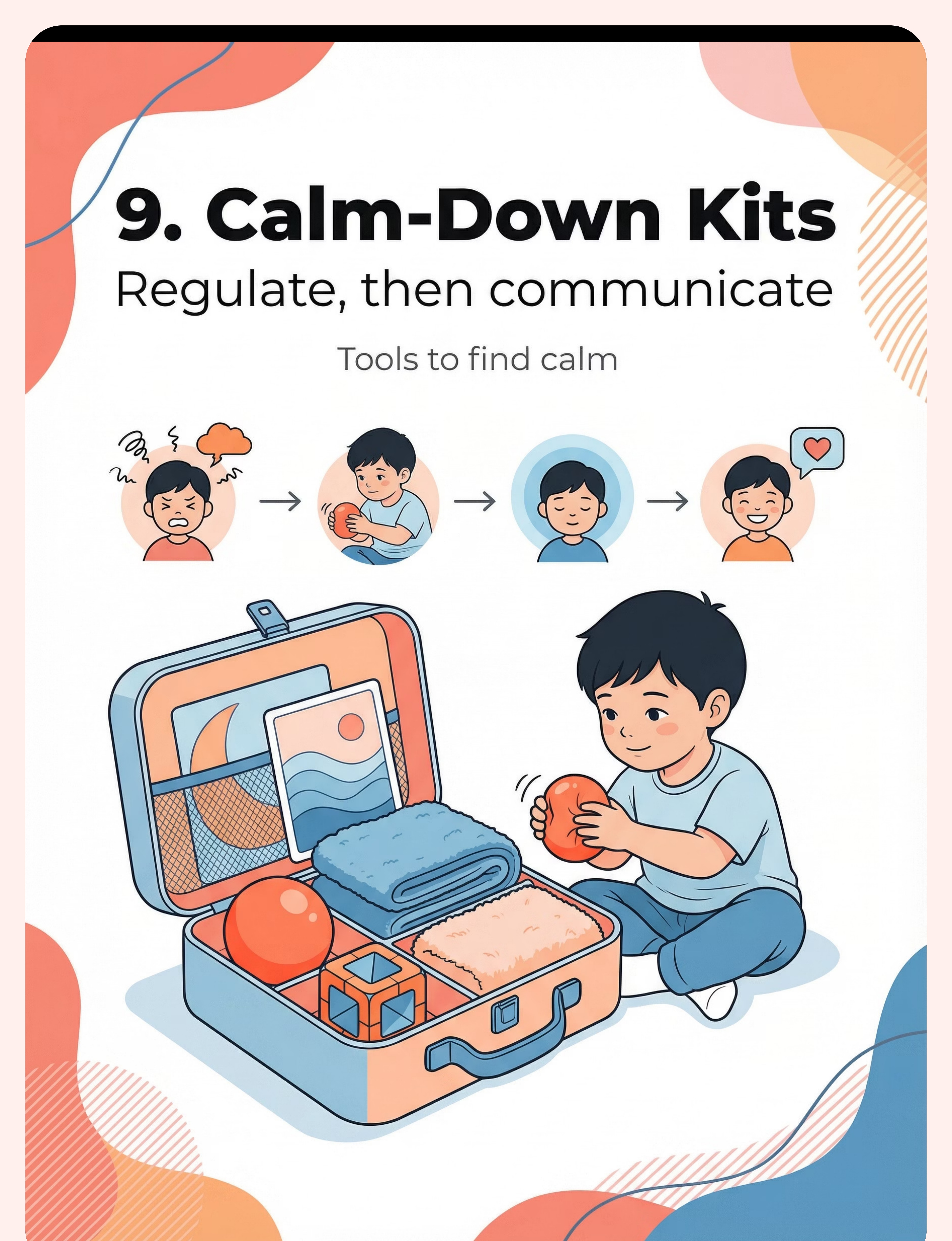
9. Calm-Down Kits
Portable kit: squeeze ball, weighted item, noise-cancelling headphones, calming visual. Why it works: Some crying is sensory distress, not communicative. Regulate FIRST, then communicate. A dysregulated nervous system cannot use FCT tools. Price: ₹500–3,000.
Every Family Can Start Today — Including Zero-Budget Families
WHO Equity Principle
Every intervention recommended by Pinnacle Blooms includes a zero-cost pathway. No family should be excluded from evidence-based care due to resource constraints. Why substitutes work: The therapeutic principle is the signal, not the specific material. A photograph of a juice box works as well as a professional PECS card if the child can identify it and the caregiver honours the exchange.
Material | DIY Version | Cost | |
Choice Board | Cookie sheet + velcro dots + actual snack containers | ₹0–200 | |
Message Button | Old mobile with voice memo app | ₹0 | |
Picture Cards | Print photos from phone + laminate pouches | ₹100–300 | |
Sign Language | Free printable ASL/ISL guides online | ₹0 | |
Emotion Cards | Print & cut emotion faces | ₹50–100 | |
Request Strips | Laminated A5 cards with velcro | ₹100–200 | |
Help/Wait Cards | Drawn clock face + sand timer from kitchen | ₹50–100 | |
AAC App | LetMeTalk (free) / JABtalk (free) | ₹0 | |
Calm-Down Kit | Stress ball (₹50) + soft fabric from home | ₹50–100 |
Total DIY Starter Kit: ₹350–1,100 for a complete FCT materials set. When the clinical-grade material is non-negotiable: Children with significant fine motor limitations may require purpose-built AAC devices with accessibility features. Consult a qualified SLP before substituting.

Pre-Session Safety Protocol — Read Before Starting
🔴 RED — STOP. Do Not Proceed
- Child shows signs of illness, fever, ear pain, or physical distress — crying may have a medical cause. Consult paediatrician before FCT.
- Child has had a severe meltdown within the past 30 minutes — the nervous system needs full recovery time.
- Any item in the materials kit is a choking hazard for your child's developmental age/oral stage.
- Child is sleep-deprived — tired children cry more; FCT over a fatigued child reinforces, not reduces, distress.
🟡 AMBER — MODIFY. Proceed with Caution
- Child appears mildly unsettled — use a simplified version (one choice only, no new skill introduction).
- Family environment is unusually chaotic today — delay formal session, embed signal practice in natural routines only.
- Grandparent or new caregiver present who has not been trained on honouring signals — do not start a session they will inadvertently undermine.
🟢 GREEN — GO. Session Conditions Met
- Child is fed, rested, and in a regulated state.
- At least one trained caregiver is fully present.
- Environment is reasonably calm.
- You have 10–15 uninterrupted minutes.
- You are yourself regulated — your anxiety transmits.
MEDICAL DISCLAIMER: Persistent or sudden-onset crying in a child who was previously communicating should always be medically evaluated. Crying can indicate ear infection, dental pain, GI distress, headache, or other pain. FCT does not address medically-caused crying. FREE HELPLINE: 9100 181 181

Stage Your Space in 3 Minutes — Before the Session Begins
Step-by-Step Setup
Position [1] — Child: Seated or on floor, comfortable, not restricted. Chair with table support if available. Child should be able to reach materials easily.
Position [2] — Caregiver: At child's eye level. Not towering over the child. Not across a room. Close enough to prompt, far enough to not overwhelm.
Position [3] — Materials: Lay out only the materials for today's session. If introducing a choice board, have exactly 2 options visible. Not the whole kit. Novelty overwhelms — familiarity teaches.
Remove From the Space
- Other toys the child may fixate on
- Screens (including your phone — it will distract you too)
- Other children for the structured session
- Excessive visual clutter from the wall behind you
Environment Settings
Lighting: Warm, not fluorescent. Natural light or warm lamp preferred. Many children with sensory differences are adversely affected by harsh overhead lighting.
Sound: Quiet. Low-volume background music (child's preferred calm music) is acceptable if already part of the child's regulatory routine.
Session Anchor
FCT is most powerful when embedded in natural routines — mealtime, snack time, play transitions, bath time. The setup is primarily for structured teaching sessions.
60-Second Readiness Assessment — Before Every Session
☐ The Checklist
- Child has eaten within the last 2 hours
- Child has slept adequately (no obvious fatigue)
- No fever, physical discomfort, or illness signs
- No severe meltdown in the past hour
- Child is in the room voluntarily (not resisting entry)
- You have 10–15 uninterrupted minutes
- Caregiver is calm and present
🟢 5–7 Checked: GO
Proceed to Step 1: The Invitation. All conditions are met for a structured session.
🟡 3–4 Checked: MODIFY
Simplified version only: one natural routine moment, no new skill introduction. Use snack time or a highly preferred routine to practise one already-known signal.
🔴 0–2 Checked: POSTPONE
Not today. Do one calming activity together. Reconnect. Attempt again tomorrow. Pushing through a non-ready child teaches the wrong lessons. "The best session is one that starts right."
Step 1 of 6
Every Session Begins With an Invitation, Not a Command
The Opening — Say This
"[Child's name], look — [show material with calm enthusiasm] — shall we try this?"
In Hindi: "[Name], dekho — chalein?"
In Telugu: "[Name], chooḍu — chesidāmā?"
Body Language
- Match child's physical level (sit down if they're on the floor)
- Make the material visually interesting — hold at child's eye level
- Smile. Your emotional tone is the first signal the child reads.
- Do NOT grab the child's hand or physically direct them at this stage.
What Acceptance Looks Like
- Child looks at material (even briefly) — this is enough. Begin.
- Child reaches toward material — excellent, follow their lead.
- Child moves toward you — proceed.
What Resistance Looks Like
- Child turns away — wait 5 seconds, try once more with a different object.
- Child walks away — follow gently, bring material to them.
- Child cries immediately — assess: return to Card 13 decision gate.
Timing
30–60 seconds. If the invitation is not accepted within 2 minutes, postpone.
ABA Principle: Pairing — establishing the caregiver and materials as motivating before demand placement. OT Principle: "Just-Right Challenge."

Step 2 of 6
The Child Is Now Engaged. Now You Introduce the Signal.
"Look — [hold up juice box] — juice. [hold up cracker] — biscuit. Which one?"
How to Present the Material
- Slow movement — bring material into view at child's pace, not yours
- Hold objects at child's eye level, approximately 30 cm from face
- Wait — a full 3-second pause after presenting. Resist the urge to fill the silence.
- The pause IS the teaching moment. The child's brain is processing.
Child Response Indicators
Engagement: Looks at objects, reaches, leans toward one — honour immediately, name what they chose: "Juice! You chose juice!"
Tolerance: Passive but not resisting — prompt gently: "Show me — which one?" (gesture toward objects)
Avoidance: Turns away, pushes objects — reduce to one item only, or transition to natural routine.
Reinforcement Cue
The moment the child makes any communicative gesture toward either object — however subtle — provide the item AND verbal praise immediately.
"YES! You SHOWED me! You said juice! Here is your juice!" (enthusiastic, specific, immediate)
Timing: 1–3 minutes from presentation to first exchange attempt.

Step 3 of 6
The Core Therapeutic Action — The Exact Moment the Signal Is Taught
Physical Exchange (Choice Board / Picture Cards)
Child approaches the choice board. Guide their hand (full physical prompt if needed) to the desired item, then immediately provide that item and enthusiastic praise. Fade the physical prompt as rapidly as the child can manage — from full hand-over-hand → light wrist touch → pointing gesture → no prompt.
Button Press
Position button within reach when the known motivation is present. Child presses → immediate delivery of the reinforcer + verbal affirmation. No delay. No "say the word first." The button IS the word.
Sign Teaching
Model the sign (MORE: tap fingertips together) while providing MORE. Then hand-over-hand prompt the child to make the sign before giving more. Accept all approximations. A flat hand patting the other hand is MORE if that's what the child can do today.
Common Execution Errors — Avoid::❌ Waiting for "better" communication before responding — respond to any attempt ❌ Requiring verbal approximation when AAC is the target modality ❌ Responding to crying faster than to the signal (this is the single most critical error) ❌ Multiple caregivers using different systems simultaneously. If signal use is not emerging after 4 weeks of daily practice → consult your Pinnacle SLP.

Step 4 of 6
Dosage and Variation — 3 Good Repetitions Beat 10 Forced Ones
Daily Repetition Targets
- Structured sessions: 3–5 clear signal opportunities per session
- Natural routine embedding: 8–15 incidental opportunities throughout the day
- Total daily signal opportunities: 10–20 (spread across routines)
How to Introduce Variation
- Same signal, different reinforcer: "More" crackers → "More" tickles → "More" blocks
- Same signal, different location: kitchen → bedroom → garden
- Same signal, different communication partner: Mummy → Daddy → Grandmother → Teacher
Satiation Indicators — When Your Child Has Had Enough
- Turns away from materials and does not return when invited
- Becomes floppy or unresponsive
- Lies down or moves to the edge of the space
- Looks through you rather than at you
⚠️ Extinction Burst Warning
When a new FCT programme begins, crying may temporarily increase before it decreases. This is an extinction burst — the child is testing whether the old strategy still works. It is a sign the protocol is working. Maintain consistency. Do NOT return to responding to crying.
Timing: 3–5 minutes of repetition with variations. Total session to this point: 8–12 minutes.

Step 5 of 6
Timing Is Everything — Reinforce Within 3 Seconds
The Reinforcement Rule
The moment the child uses the signal — any recognisable attempt — deliver:
- The requested item (within 3 seconds)
- Verbal praise (immediate, specific, enthusiastic)
- Emotional warmth (a smile, a touch, a moment of celebration)
Reinforcement Scripts — Say These
"YES! You SHOWED me! You said MORE! Here is MORE biscuit! I am SO proud of you!"
"You pressed the button! You said HELP! Mummy is coming! Here is the help!"
"You gave me the picture! You asked for JUICE! Here is your juice — you ASKED ME! That was amazing!"
The Cardinal Rule & Reinforcement Menu
Celebrate the attempt, not just the success. A hand-over-hand prompted exchange still gets genuine praise for participating.
Reinforcement Options: Natural reinforcers (the item itself — always preferred) | Social reinforcers (enthusiastic praise, high fives, a favourite song) | Token economy (star chart, sticker book — from ₹150) | Sensory reinforcers (a brief preferred sensory activity).
Within 3 seconds. Not "soon." Not "after I finish this sentence." Three. Seconds.

Step 6 of 6
End With Intention — No Session Ends Abruptly
"Two more, then all done. [Signal: hold up 2 fingers]. Two more chances — then we finish."
A child whose session ends abruptly may associate the session with distress. A child whose session ends with warmth and transition anticipates the next one.
If Child Resists Ending
- Use a visual timer so "all done" is visible, not just verbal
- Keep voice calm and warm — do not match escalation with urgency
- Offer a transition object from the calm-down kit
- If resistance is significant, assess: is the child signalling they want MORE of the positive interaction? (This is a success signal.)
Visual Timer
Time Timer or DIY countdown (sand timer, drawn clock) — NCAEP classifies visual timers as evidence-based practice for autism (2020).
Purpose
Preventing post-session dysregulation. The transition script and materials put-away ritual create a predictable, safe ending that the child begins to trust and anticipate.

60 Seconds of Data Capture. Right Now. Before You Forget.
Why Data Matters
Your daily observations are the engine of GPT-OS®. Without data, your child's therapist is working with anecdotes. With data, they are working with evidence. The difference is the precision of the programme.
The absence of data is the most common reason FCT programmes fail to reach their potential.
Where to Log
- GPT-OS® EverydayTherapyProgramme™ app (for enrolled families)
- Download printable FCT Daily Tracker (PDF): techniques.pinnacleblooms.org/B137/tracker
- WhatsApp summary to therapist: simply voice-note the 3 fields above
Key Metric: Signal-to-Crying Ratio over time — the Communication Readiness Index (CRI) used by Pinnacle to measure FCT progress.
The 3-Field Session Log
1. SIGNALS TODAY: How many times did child use signal independently?
□ 0 □ 1–2 □ 3–5 □ 5+
2. SIGNAL TYPE USED:
□ Object reach □ Picture exchange □ Button press □ Sign/gesture □ Vocalisation □ Combination
3. CRYING vs. SIGNAL RATIO (estimate):
□ All crying, no signal
□ Mostly crying, some signal attempts
□ Equal crying and signal use
□ Mostly signal, some crying
□ Signal dominant today

8 Common FCT Challenges — And What to Do About Them
Problem 1: Child throws the picture card instead of exchanging it
Solution: Return to Phase 1: hand-over-hand exchange with physical prompt. The card must visibly and immediately produce the desired item every time, with zero exceptions over the next 20 trials.
Problem 2: Signal was working last week; child has stopped
Solution: Three possibilities: (a) Reinforcer has lost value — change to a more preferred item. (b) Someone in the household is responding faster to crying again — audit caregiver consistency. (c) Child is ill or fatigued — return to readiness assessment.
Problem 3: Crying increased when we started FCT
Solution: This is an extinction burst — normal and expected. Maintain the protocol completely. Do NOT respond to the crying. The burst typically peaks within 3–5 days and then declines. If it continues beyond 2 weeks, consult your Pinnacle SLP or BCBA.
Problem 4: Child only uses signal with one caregiver
Solution: Generalisation is not yet complete — not failure. Train all caregivers using the same materials and scripts. Book a Pinnacle caregiver training session: 9100 181 181.
Problem 5: Child only signals for one item
Solution: Use natural deprivation. Present the choice board ONLY when the favourite item is not the only option available. Ensure other highly preferred items are available as alternative choices.
Problem 6: Grandparent gives in to crying "out of pity"
Solution: The grandparent needs to understand that responding to crying maintains the child's frustration long-term. Share this page with them. Use the Family Guide PDF (Card 37). Compassion and consistency are not opposites.
Problem 7: Child uses signal but cries when item takes 5 seconds
Solution: Reinforce faster. Within 3 seconds is the clinical standard. If physical setup prevents this, change the setup. The item must be already in your hand before the exchange begins.
Problem 8: Nothing is working after 4 weeks
Solution: Stop home programme and call Pinnacle: 9100 181 181. A formal communication function assessment by a qualified SLP + BCBA is needed. The child may have unidentified barriers requiring clinical investigation.

Every Child Is Different — Adapt the Protocol to Yours
12–24 Months
- Start with real objects only (no pictures yet)
- Maximum 2 choices at any time
- Sessions: 3–5 minutes maximum
- Natural routine embedding: every snack, every transition
2–4 Years
- Introduce photograph-based picture cards
- 2–4 choices possible
- Begin teaching "I want ___" sentence strip
- Sessions: 8–12 minutes
4–6 Years
- Introduce AAC app if not using speech
- Begin teaching spontaneous commenting, not just requesting
- Generalise across settings: home → school → community
Joint Household Adaptation (Indian Family Context): In joint families, 4–6+ adults may interact with the child daily. Each must be trained on the same signal system. Use the Family Guide PDF (Card 37) to standardise across all household members. Consistency across caregivers is the most powerful predictor of FCT success. Sensory Seeker: Make the exchange itself sensory — a high-five handover, exciting delivery. Sensory Avoider: Quiet, low-stimulation delivery. Whispered praise. Motor Planning Difficulties: Full physical prompting is appropriate longer. Accept larger approximations.

Week 1–2
Planting the Seed
Week 1–2: What to Expect
What You May See (All Progress)
- Child tolerates the material being present — this is progress
- Child makes eye contact with the choice board or button — this is progress
- Child makes one or two prompted exchanges (hand-over-hand) — this is progress
- Crying has not reduced yet — this is normal and expected
"Tiny Wins" to Celebrate
"She looked at the choice board before crying today. She looked at it."
"He pressed the button once when I hand-over-hand guided him. That's the neural pathway forming."
"She held the picture card for 3 seconds instead of throwing it. Something is registering."
Parent Reality Check
The most common reason FCT programmes fail in Weeks 1–2 is inconsistency driven by impatience. The protocol feels tedious. The child seems indifferent. The crying hasn't changed.
Persist. The research is unambiguous: FCT works. It takes 2–8 weeks for the signal to stabilise. You are in the foundation phase.
Session frequency target: 1–2 structured sessions per day, 8–12 minutes each. Natural routine embedding: every snack, transition, and play time.

Week 3–4
Neural Pathway Forming
Week 3–4: The Neural Pathway Is Forming
Consolidation Indicators — Look for These
- Child reaches toward the choice board before you present it — neural anticipation forming
- Child uses signal spontaneously in one context where they previously only cried — generalisation beginning
- Child attempts the signal before escalating to crying in at least some situations — signal preference emerging
- Caregivers report confidence in the exchange — the protocol is landing
What to Do Now
- Increase variety of choices presented (same signal, different items)
- Begin generalisation across people — introduce the board to a second caregiver this week
- Fade one level of prompting — if you've been doing full hand-over-hand, move to light wrist touch
Parent Milestone
"You may notice that you are more confident too. You're reading your child's pre-cry window and presenting the board before they escalate. This is co-regulation — your attunement growing alongside your child's skill."
30%
Signal Use Target
Signal-to-crying ratio shifts from 10:90 toward 30:70 in at least one context by end of Week 4.
2nd
New Caregiver
Introduce the board to a second caregiver this week to begin cross-person generalisation.

Weeks 5–8
Signal Starts Winning
Weeks 5–8: The Signal Starts Winning
What Mastery Looks Like
- Child uses signal independently (no prompt) in the primary context where it was taught
- Signal generalises to at least 2–3 different communication partners
- Crying frequency in the primary function category is measurably reduced
- Child corrects when a new caregiver doesn't understand — repeats signal, looks for comprehension
The "Correcting" Indicator
When a child repeats or modifies their signal when not understood — this is sophisticated communicative persistence. This is the exact behaviour pattern of a child who knows language works.Celebrate this loudly.
What to Add Now
- Expand vocabulary: add a second signal function (e.g., if request is mastered, begin protest signals)
- Begin community generalisation: practice during grocery run, grandparents' visit, playground
- Consider AAC vocabulary expansion if using a device
Signal-to-Crying Target: 70:30 ratio in primary context. 50:50 or better in secondary contexts.

Your Child Just Crossed a Milestone That Changes Everything
When your child uses a signal independently — without prompting, without hand-over-hand, without you presenting the material — and receives what they requested, and then uses it again the next day without being reminded: Your child has communicated intentionally. For perhaps the first time. This is enormous.
What This Means Neurologically
A new synaptic pathway has been created, strengthened, and retrieved. The child's brain has learned that they have agency — that something they do with their body produces a predictable, positive result in their environment. This is the foundation of all future language development.
What This Means for Your Family
The desperation of a child who can only cry to communicate is being replaced by a child who can be understood. The family stress curve, which peaks during high-communication-demand periods, has a new trajectory.
What This Means for You
You did this. Not the app. Not the materials. You — with consistency, with patience, with the willingness to hold the protocol on hard days. Take this in.
📹Document the Moment: Record the first independent signal exchange. Send it to your Pinnacle therapist. Send it to family. Save it. This is the video you will watch when the next challenge feels insurmountable.

These Are Your Signals to Call for Clinical Support
🔴 No signal emergence after 6 weeks of daily consistent practice
A formal communication function assessment is overdue. Something is blocking that we can identify clinically. Call Pinnacle immediately: 9100 181 181
🔴 Crying significantly increased after 3 weeks (sustained, not extinction burst)
The protocol may not match the child's communication function. A BCBA functional behaviour assessment is needed. Call Pinnacle immediately: 9100 181 181
🔴 Child shows self-injurious behaviour when crying is not responded to
This requires immediate professional consultation. Do not continue FCT without clinical guidance. Call: 9100 181 181
🔴 Parent/caregiver mental health is deteriorating significantly
You cannot pour from an empty cup. Call for caregiver support. Pinnacle offers parent counselling alongside child therapy. 9100 181 181
Orange Flags — Book a Consultation Within 2 Weeks: Signal not generalising after 8 weeks | Only one caregiver has been successfully trained | Child's crying is associated with apparent physical discomfort | Progress has plateaued at Week 4 and not resumed. FREE National Autism Helpline: 9100 181 181 | 16+ languages | 24x7 | pinnacleblooms.org/book-consultation
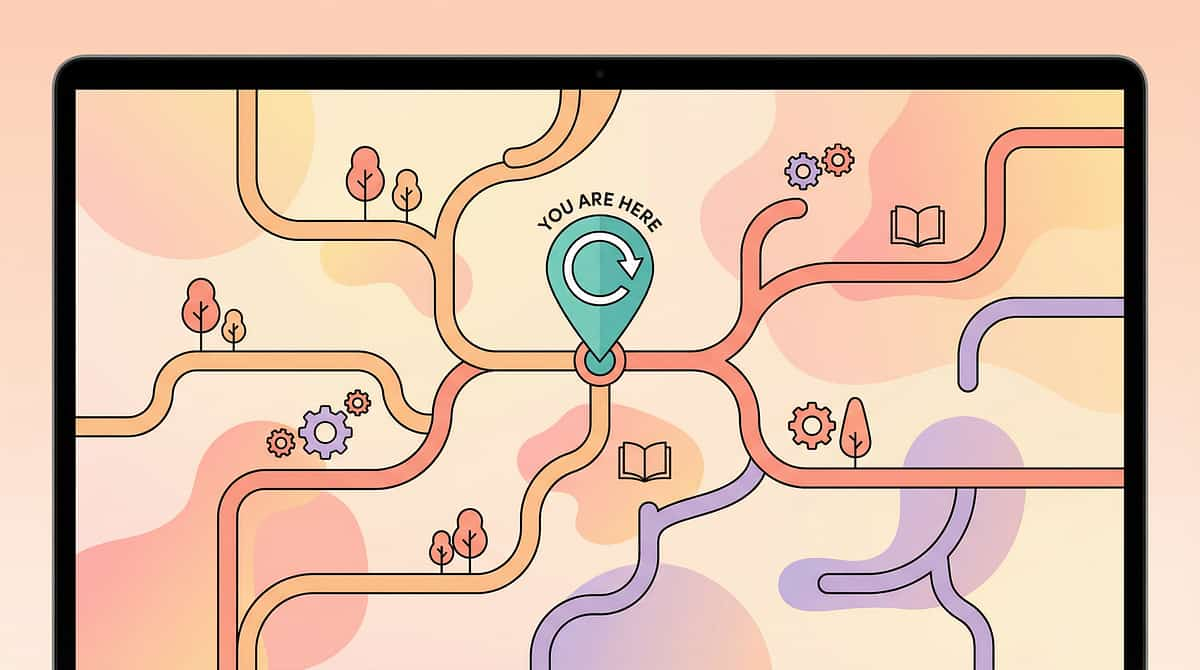
You Are Here. Here Is Where We Are Heading.
B-136
Teaching First Communication: Establishing communicative intent
B-137 ← YOU ARE HERE
Moving from Crying to Signals (FCT)
B-138
Teaching Requesting: Expanding FCT to structured mand training
B-141
Sentence Building with AAC: From single-word to multi-symbol communication
B-180
Social Communication: Full conversation and social interaction across all environments
Lateral Alternatives
B-120 — Joint Attention Strengthening: If communication intent is still inconsistent
B-097 — Sensory Regulation Foundation: If sensory dysregulation is the primary crying driver
Long-Term Developmental Goal
Independent, multi-modal functional communication — capable of requesting, protesting, commenting, greeting, and social interaction — across all natural environments.
Prerequisite Techniques
B-136 Teaching First Communication | B-134 Limited Communicative Intent | B-006 Limited Pointing: Building gestural communication foundation
Other Techniques in This Domain That Work Alongside FCT
B-136 — Teaching First Communication
Difficulty: Foundation | Materials: Object Choice + Picture Cards. Building communicative intent before FCT begins.
B-138 — Teaching Requesting
Difficulty: Core | Materials: PECS Phase III + AAC App. Structured mand training — requesting with expanding vocabulary.
B-141 — Building First Sentences
Difficulty: Intermediate | Materials: Sentence Strips + AAC App. Combining symbols: "I want + [item]."
B-160 — Teaching "All Done" and Protest
Difficulty: Core | Materials: All Done Card + Request Strips. The other side of FCT: communication as protest.
B-120 — Joint Attention Foundation
Difficulty: Foundation | Materials: Bubbles + Social Toys. The prerequisite that unlocks all communication.
B-097 — Sensory Regulation for Communication
Difficulty: Intermediate | Materials: Calm-Down Kit + Sensory Tools. When dysregulation blocks communication access.
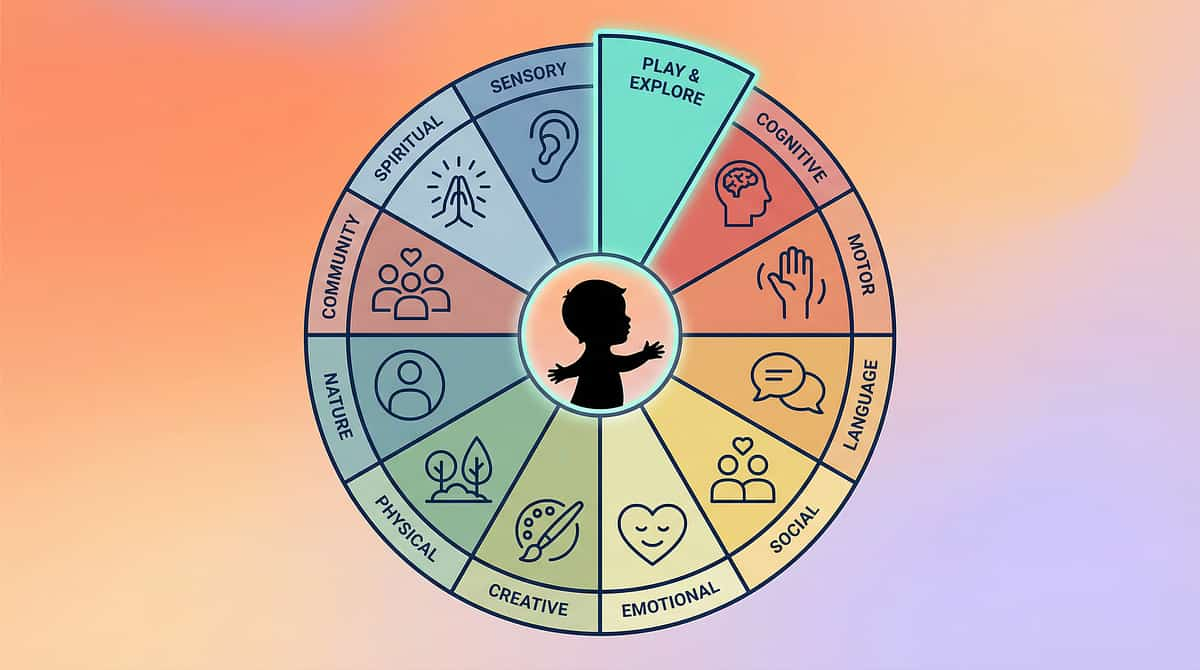
FCT Is One Piece. Here Is the Full Picture.
Why the Full Map Matters
A child making extraordinary progress in FCT (communication) may simultaneously experience sensory challenges (Domain A) that directly limit where FCT can generalise. Or motor planning difficulties (Domain E) that determine which AAC modality is physically accessible.
FCT does not exist in isolation. GPT-OS® tracks all 12 domains simultaneously, creating the FusionModule™ convergence that coordinates all disciplines toward a single developmental outcome.
Access Your Child's Full Map
→ pinnacleblooms.org/gpt-os
→ Or call: 9100 181 181
WHO/UNICEF Nurturing Care Framework — five components of nurturing care require holistic developmental monitoring. PMC9978394

Three Families. Three Turning Points. All Real.
Amrutha, Hyderabad — 4-year-old son
"Arjun was crying 25–30 times a day. We thought it would never end. Our SLP at Pinnacle started with just one object choice — juice or water at breakfast. Three weeks in, he reached for the juice box before a single sound. Five weeks in, he was handing picture cards. Eight weeks in, the crying for food and drink had dropped by 80%. We still have hard days. But now we know what he wants. That changes everything."
— Parent, Pinnacle Hyderabad | CRI improvement: 340 → 680 in 12 weeks
Priya, Chennai — 2.5-year-old daughter
"My mother-in-law was convinced the picture cards were 'making her lazy to talk.' We shared the Pinnacle research. She attended one session. She now uses the picture cards more consistently than anyone in the house. Riya started using two-picture combinations by Week 10. Her SLP said the AAC accelerated her verbal attempts. It did."
— Parent, Pinnacle Chennai | Note: Outcomes vary. Individual professional assessment required.
Suresh, Bengaluru — Child with ASD + Sensory Challenges
"We tried everything. Nothing worked until the calm-down kit and FCT were combined. The OT at Pinnacle showed us that Vishal was crying because of sensory overload first, communication failure second. Once we regulated the sensory, the FCT signal teaching worked within two weeks. The order of interventions matters."
— Parent, Pinnacle Bengaluru | Note: Illustrative case. Results vary.
All stories are illustrative. Results depend on individual child profile, caregiver consistency, co-occurring conditions, and professional guidance. Individual professional assessment required.
You Don't Have to Do This Alone
WhatsApp: Pinnacle Parents – FCT & Communication
A moderated community of parents implementing FCT across India. Share wins, troubleshoot challenges, support each other. Consistent caregiver support is one of the strongest predictors of FCT success.
→ Join: pinnacleblooms.org/parent-community
Instagram: @PinnacleBlooms
Daily evidence-based content. Parent Q&A. Therapist insights. FCT demos. → instagram.com/PinnacleBlooms
YouTube: Pinnacle Blooms Network
Full FCT tutorial series. Parent training videos. Therapy demonstrations. → youtube.com/PinnacleBlooms
Pinnacle Parent Circles
Monthly online parent group sessions facilitated by Pinnacle SLPs and BCBAs. Free for all enrolled families. → pinnacleblooms.org/parent-circles
"Consistency across caregivers multiplies impact." One parent implementing FCT correctly is powerful. An entire family implementing FCT consistently is transformative.
80+ Pinnacle Centers Across India — Expert FCT Support Near You
What to Expect at a Pinnacle Center
Communication Function Assessment (SLP): What is the crying communicating? Formal assessment identifies the primary communicative function and designs the FCT target hierarchy.
AbilityScore® Communication Baseline: A standardised score (0–1000) across 349 developmental skills. Your child's Communication Readiness Index baseline — so progress has a number, not just a feeling.
BCBA Functional Behaviour Assessment: Identifying antecedents, behaviours, and consequences maintaining crying as communication.
FusionModule™ FCT Programme: SLP + BCBA + OT coordinated programme — one converged plan, multiple disciplines.
EverydayTherapyProgramme™: Your home FCT protocol, designed by the clinical team, delivered through GPT-OS®.
Find Your Center
→ pinnacleblooms.org/centers
→ FREE: 9100 181 181 | 16+ languages | 24x7
Key Cities
Hyderabad | Chennai | Bengaluru | Mumbai | Delhi | Pune | Visakhapatnam | Vijayawada | Coimbatore | Kochi | and 70+ more
International Families
GPT-OS® teleconsultation available for families in the UAE, UK, USA, Singapore, Australia, and 60+ countries.
→ pinnacleblooms.org/teleconsultation
The Evidence Behind Every Word on This Page
FCT Foundation — Carr & Durand (1985)
JABA: Reducing behaviour problems through functional communication training. The landmark study establishing FCT. 40+ years of replication.
AAC and Speech — Mirenda (2003)
Language, Speech, and Hearing Services in Schools: AAC does not impede speech development; it supports it. Critical for addressing the "it will stop them talking" misconception.
NCAEP EBP Classification (2020)
FCT classified as Evidence-Based Practice for Autism. 27 studies reviewed. Consistent positive outcomes across populations.
Indian Home-Based Interventions — Padmanabha et al. (2019)
Indian Journal of Pediatrics: Home-based interventions in Indian pediatric populations — feasibility and outcomes. DOI: 10.1007/s12098-018-2747-4
PRISMA Review — PMC11506176 (2024)
16 articles confirming evidence-based practice criteria for communication interventions in ASD. Sensory + communication integration evidence.
Meta-analysis — PMC10955541 (2024)
World J Clin Cases: 24 studies demonstrating multi-domain improvements through structured communication intervention.
Your Session Data Is Therapy Infrastructure
What GPT-OS® Learns from Your FCT Data
- Signal acquisition rate (how quickly your child learns each modality)
- Generalisation patterns (which contexts the signal is most robust)
- Satiation patterns (which reinforcers lose value and when)
- Extinction burst duration (for population-level calibration)
Your Data Helps Every Child
When your child's data flows into GPT-OS®, it joins 20M+ sessions of real-world therapeutic data. The population-level patterns improve recommendations for every future family using this exact protocol.
Privacy Assurance
All data is de-identified, encrypted, and governed under ISO/IEC 27001 Information Security Management standards. DPIIT8651 regulatory compliance. Indian Data Protection Act compliant.
GPT-OS® Stack: AbilityScore® | TherapeuticAI® | FusionModule™ | EverydayTherapyProgramme™ | Prognosis Engine

The Reel That Surfaces This Challenge
Reel B-137 Details
Title: "9 Materials That Help Moving from Crying to Signals"
Reel ID: B-137 | Series: Functional Communication Series — Episode 137
Domain: B — Social Communication & Pragmatic Language
Runtime: 75 seconds
How to Use This Reel
- Share on WhatsApp to explain materials to joint family members
- Use as a training tool for grandparents, domestic helpers, and teachers
- The visual demonstration reduces setup errors
NCAEP (2020): Video modelling is classified as evidence-based practice for autism. Multi-modal learning (visual + text + demonstration) improves parent skill acquisition.
Watch the Series
← Previous: B-136 — Teaching First Communication
→ Next: B-138 — Teaching Requesting
All 999 Reels
→ pinnacleblooms.org/reels
→ instagram.com/PinnacleBlooms
→ youtube.com/PinnacleBlooms
Preview of 9 materials that help moving from crying to signals Therapy Material
Below is a visual preview of 9 materials that help moving from crying to signals therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.







Link copied!
Consistency Across Caregivers Multiplies Impact
If you implement FCT correctly but one other caregiver in the household responds faster to crying than to signals — the programme fails. Not because FCT doesn't work. Because inconsistency teaches the child that crying still works sometimes. Every adult who interacts with your child for more than 30 minutes per day must understand and implement the FCT protocol.
Share This Page
📲 WhatsApp | 📧 Email | 🔗 Copy link: techniques.pinnacleblooms.org/functional-communication/moving-from-crying-to-signals-B137
Download the Family Guide (1-page PDF): techniques.pinnacleblooms.org/B137/family-guide
Explain to Grandparents — Simplified
"Nana, when [child] hands you a picture or presses the button, give them what they want immediately. Don't wait. Don't ask them to say it. If you respond to the signal faster than to the crying, [child] will use the signal. If crying works faster, [child] will cry. It's that simple."
School Communication Template
"[Child's name] is currently using [picture exchange / button press / sign] to communicate their needs. Please honour this signal immediately when used. Please do not require verbal requests. Please contact us if you have questions: [parent contact]."