
When Their Legs Always Form That W Shape
Every reminder, every repositioning — and within seconds, back to the W.
It's Saturday morning. Your child is building a tower of blocks on the living room floor. You notice it immediately — knees bent, feet splayed out to both sides, bottom flat between their heels. That W shape. Again. You've lost count of how many times you've said "criss-cross, sweetheart" or gently moved their legs. Their preschool teacher mentioned it. Their pediatrician said to watch it. You've read it can affect hips and core strength. But no one has told you HOW to actually change it.
You are not failing. Your child's body is compensating. There's a reason — and there's a solution.
F-577
Age 2–8 Years
Gross Motor / Postural Control
This technique is part of the Pinnacle Blooms Network® Motor Development Series — Episode 577. Validated by GPT-OS®, aligned with the WHO Nurturing Care Framework (2018), and supported by OT + PT + ABA + SpEd + NeuroDev consortia.

ACT I: RECOGNITION
W-Sitting Is More Common Than You Think
You are among millions of families navigating this exact challenge. W-sitting is the single most discussed floor posture in pediatric occupational therapy globally. It emerges when a child's nervous system seeks the path of least resistance — maximum stability with minimum muscular effort. This is not stubbornness. This is compensation intelligence.
25–40%
Habitual W-Sitters
of children ages 2–5 W-sit habitually at some point during development
3 in 5
With Developmental Differences
children with low muscle tone or developmental differences use W-sitting as their primary floor position
2.8M+
Families Affected
Indian families currently managing W-sitting challenges in children under 8
Among children with neurodevelopmental differences including autism spectrum disorder, low muscle tone, and hypermobility syndrome, persistent W-sitting is documented in over 60% of cases requiring gross motor intervention (PRISMA systematic review, 2024; PMC11506176).
"Your child didn't choose the W position. Their developing body chose it — because it was the most stable option available to them given their current core strength. We're not correcting behavior. We're building capacity." — Pinnacle Blooms Consortium, Pediatric OT Division

ACT I: RECOGNITION
The W Position: A Compensation Strategy, Not a Bad Habit
Why The W Is Stable Without Effort
When a child W-sits, their knees point inward and their feet splay outward. This positions the hips in extreme internal rotation, which mechanically "locks" the pelvis and trunk in place — the same way a tripod is stable without anyone holding it. The child can play, build, draw, and engage for extended periods without using a single core muscle.
The Hidden Cost
- Dynamic trunk control — the active muscle work of maintaining upright positions
- Trunk rotation — reaching across midline, bilateral coordination
- Postural reactions — righting and equilibrium responses that build balance
- Hip joint health — prolonged internal rotation stress on developing hip joints
The Reinforcement Cycle
Child W-sits → doesn't develop core strength → alternatives feel uncomfortable → returns to W-sit → doesn't develop core strength.
Breaking this cycle requires both building strength AND making alternatives accessible. This is a wiring pattern, not a behavior choice.
Reference: Frontiers in Integrative Neuroscience (2020) — DOI: 10.3389/fnint.2020.556660

ACT I: RECOGNITION
Your Child's Developmental Trajectory
W-sitting emerges at a specific developmental window — and intervention changes the trajectory. Understanding where your child is on this timeline brings the intervention into sharp focus.
6–10 Months
Sitting balance emerges. Core strength foundation begins.
12–18 Months
Independent floor sitting established. W-sit may first appear as compensation.
2–3 Years
W-sitting peaks. Most common age of habitual W-sitting pattern.
3–5 Years ⚑
Critical Intervention Window. Most impactful period for postural habit formation.
5–6 Years
School floor sitting demands increase. W-sitting becomes functionally limiting.
6–8 Years
Postural habits stabilize. Earlier intervention = greater natural correction.
W-sitting that persists beyond age 4 is commonly associated with low muscle tone (hypotonia), hypermobility syndrome, Developmental Coordination Disorder (DCD), Autism Spectrum Disorder, and hip tightness. With the right materials and consistent home practice, children typically show meaningful postural variety within 4–12 weeks. The brain is most plastic at this age.
ACT I: RECOGNITION
Clinically Validated. Home-Applicable. Parent-Proven.
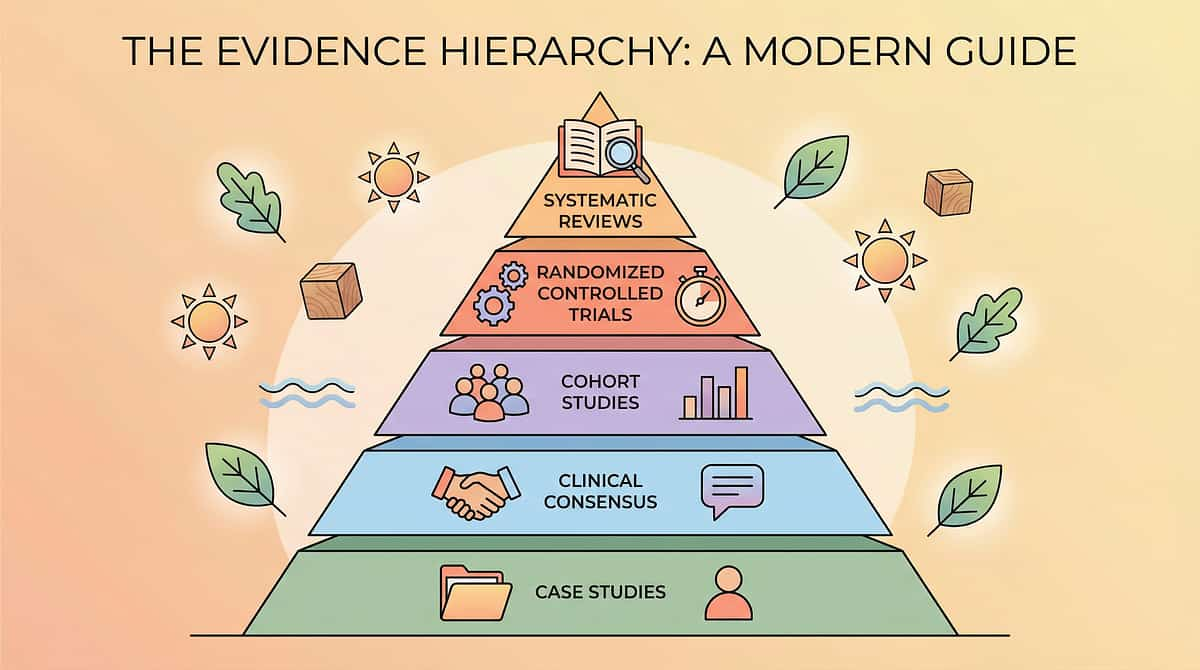
Evidence Grade: Level II
Multiple Systematic Reviews + Clinical Consensus + RCT Support. This is not a trend — it's a body of evidence built across decades and continents.
✓ Peer-Reviewed
✓ Multi-Country
✓ India RCT Data
✓ WHO/UNICEF-Aligned
✓ 20M+ Sessions
Study | Key Finding | |
PRISMA Systematic Review (2024) | 16 studies confirm sensory-motor intervention meets EBP criteria for children with ASD — PMC11506176 | |
Meta-analysis, World J Clin Cases (2024) | SI + postural interventions promote gross motor skills in 24 studies — PMC10955541 | |
Indian RCT, Padmanabha et al. (2019) | Home-based sensory-motor interventions showed significant outcomes in Indian pediatric populations | |
WHO NCF (2018) | Caregiver-implemented motor development strategies show strong population-level impact |
"Postural intervention using materials-based approaches, when delivered consistently by trained caregivers in the home environment, produces measurable improvements in core strength, sitting posture variety, and trunk control within 6–12 weeks." — Pinnacle Blooms CRO Division

ACT II: KNOWLEDGE TRANSFER
F-577: Materials-Based W-Sitting Correction
Parent-Friendly Alias: "The W-to-Strong Toolkit"
Definition
W-sitting correction through materials-based intervention is the systematic use of 9 evidence-selected therapy materials to address the root causes of habitual W-sitting in children aged 2–8 years.
Unlike verbal correction, materials-based intervention works on two parallel tracks: Immediate alternatives (floor seats, wedge cushions, kneeling benches) that give the child comfortable options right now, and strength-building tools (T-stools, therapy balls, core games kits) that eliminate the need for W-sitting over time.
This is not posture correction. This is capacity building.
Domain | F — Gross Motor / Postural Control | |
Subdomain | W-Sitting / Core Stability / Hip Development | |
Age Range | 2–8 Years | |
Session Duration | 10–20 min active + full-day environmental setup | |
Frequency | Daily (environmental) + 3–4x/week (active) | |
Setting | Home + School + Clinic | |
Series | ← F-576 | F-577 (THIS) | F-578 → |
ACT II: KNOWLEDGE TRANSFER
This Technique Crosses Therapy Boundaries
Because the body doesn't organize itself by therapy type. Each discipline contributes a distinct and necessary layer to W-sitting intervention — and the combination is what produces lasting change.
Pediatric Occupational Therapist (PRIMARY LEAD)
The OT leads W-sitting intervention by assessing the root cause — core weakness, hip tightness, hypermobility, or habituated motor pattern — and prescribing the specific material combination including T-stool height, ball size, wedge incline, and progression timeline.
Pediatric Physical Therapist (CO-LEAD)
The PT addresses orthopedic dimensions: hip mobility assessment, gait impact analysis, and the strengthening exercise program. PT clears children with suspected hip dysplasia or hypermobility syndrome before intervention materials are introduced.
ABA/BCBA Therapist (BEHAVIORAL LAYER)
The behavior analyst embeds reinforcement schedules around use of alternative sitting positions. Visual position cards are integrated into the behavioral intervention plan. Positioning band use is shaped through discrete trial training.
Special Educator (SCHOOL GENERALIZATION)
The special educator ensures materials travel to the classroom. Circle time accommodations are designed so the child can participate without W-sitting. Teacher communication templates are prepared for school-wide consistency.
NeuroDevelopmental Pediatrician (CLINICAL OVERSIGHT)
Rules out hip dysplasia, screens for connective tissue disorders (EDS, hypermobility syndrome), and coordinates referral to orthopedics if structural hip assessment is warranted before intervention begins.

ACT II: KNOWLEDGE TRANSFER
Precision Targets: What Each Material Addresses
Material-to-Target Mapping
Material | Primary | Secondary | |
T-Stool | Core strength | Balance reactions | |
Therapy Ball | Core strength | Trunk rotation | |
Core Games Kit | Core strength | Motor planning | |
Wedge Cushion | Hip alignment | Comfort in alternatives | |
Floor Seat | External support | Sustained participation | |
Kneeling Bench | Immediate alternative | Hip neutral alignment | |
Visual Position Cards | Body awareness | Behavioral choice | |
Positioning Band | Habit breaking | Proprioceptive input | |
Hip Stretching Strap | Hip flexibility | External rotation range |
ACT II: KNOWLEDGE TRANSFER
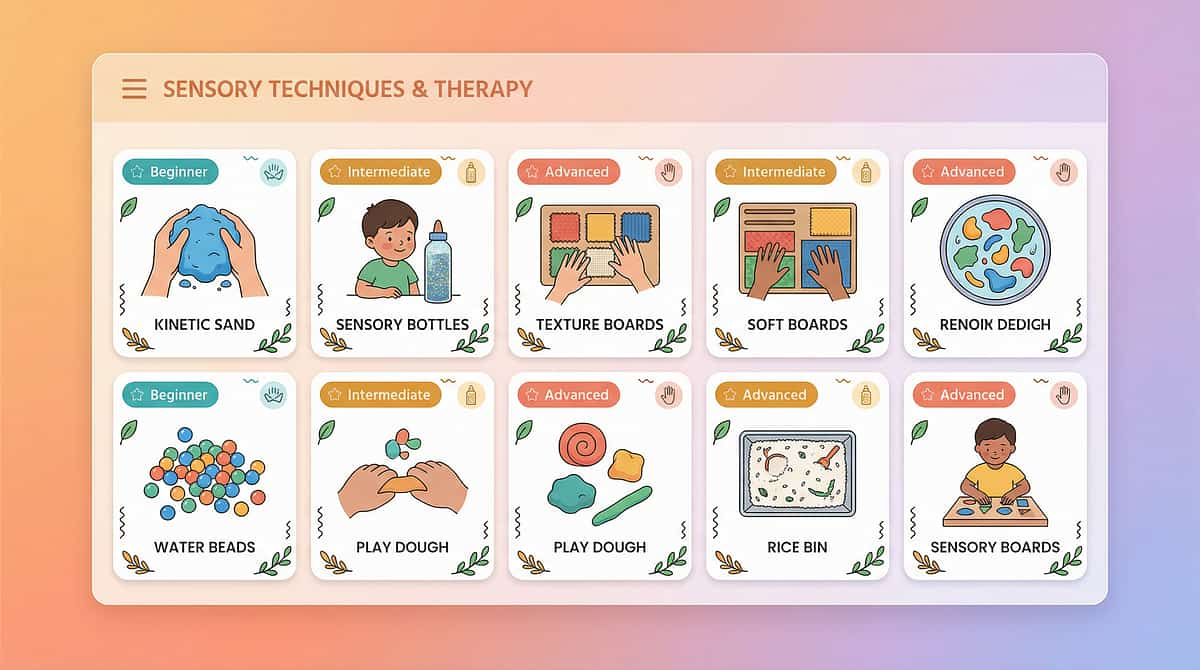
9 Materials That Actually Help With W-Sitting
The Amazon-ready list — every material priced, sourced, and clinically validated. These 9 tools address the root causes of W-sitting rather than relying on verbal correction that rarely sticks.

1. T-Stool (Active Sitting Stool)
₹800–2,500 | Canon: Positioning Equipment — Seating
Single-pedestal design demands continuous core engagement — builds trunk strength invisibly during tabletop play.

2. Wedge Cushion
₹500–1,500 | Canon: Positioning Equipment — Adaptive Seating
Forward pelvic tilt makes cross-legged sitting easier and more natural — the bridge between W and independence.

3. Floor Seat with Back Support
₹600–2,000 | Canon: Positioning Equipment — Floor Seating
Provides spinal alignment support during extended floor sitting — essential for school circle time and group activities.

4. Therapy Ball (Physio Ball)
₹400–1,200 | Canon: Gross Motor Equipment — Balance Tools
Dynamic unstable surface demands continuous trunk engagement — builds core strength through active, motivating play.

5. Visual Position Cards
₹100–400 or DIY | Canon: Visual Supports — Choice Menus
Replaces "stop W-sitting" corrections with picture-based choices — child selects position, restoring autonomy.

6. Hip Stretching Strap
₹200–600 | Canon: Gross Motor Equipment — Flexibility Tools
Increases hip external rotation range — makes cross-legged and long-sitting physically comfortable over time.

7. Positioning Band
₹200–700 | Canon: Positioning Equipment — Adaptive Supports
Soft tactile reminder at thigh level prevents W-sitting mechanically while new posture habits form.

8. Kneeling Bench
₹600–1,800 | Canon: Positioning Equipment — Alternative Seating
Provides comfortable floor-level position without W-sitting — allows full participation in floor activities immediately.

9. Core Strengthening Games Kit
₹500–3,000+ | Canon: Gross Motor Equipment — Strength + Play
Balance boards, animal walks, scooter boards build trunk strength through play — the root cause addressed through fun.
Starter Kit Recommendation (₹1,200–3,700): Wedge Cushion + Visual Position Cards + Therapy Ball. Start here. Add others as you see progress.

ACT II: KNOWLEDGE TRANSFER
Every Family Can Start Today — Regardless of Budget
WHO/UNICEF Equity Principle: No child should be denied intervention because of economic access. Every material in F-577 has a zero-cost or very-low-cost equivalent using household items. The biomechanical principles remain identical.
Buy This | Make This (₹0) | Why It Works | |
T-Stool (₹800–2,500) | Firm cylindrical pillow under child's seat, or overturned plastic container of appropriate height | Creates slightly unstable, height-reduced seating requiring trunk engagement | |
Wedge Cushion (₹500–1,500) | Roll a firm bath towel into a wedge shape; place thick end at back of sitting area | Replicates the forward pelvic tilt — same biomechanical principle | |
Floor Seat (₹600–2,000) | Stack firm pillows against a wall; child sits cross-legged in front | Provides spinal support that makes extended non-W sitting achievable | |
Therapy Ball (₹400–1,200) | Rocking horse over rolled blanket cylinder; brief supervised balloon games | Limited but engages trunk — upgrade to proper ball as soon as able | |
Visual Position Cards (₹100–400) | Print/draw 4 sitting position pictures on A5 paper; laminate with sticky tape | Identical principle — visual choice replaces verbal correction | |
Hip Stretching Strap (₹200–600) | Long dupatta, chunni, or bedsheet folded into long strip for assisted stretches | Same mechanical assist — controlled hip flexibility stretching | |
Positioning Band (₹200–700) | Soft scarf tied loosely around both thighs above knees | Identical physical reminder principle — must be loose, never tight | |
Kneeling Bench (₹600–1,800) | Low, stable step stool with cushion on top; child kneels behind it during floor play | Provides kneeling height and hip position support | |
Core Games Kit (₹500–3,000+) | Bear walks, crab walks, log rolls on carpet, cushion obstacle courses, army crawl through furniture | These are the most effective core builders — zero cost, high impact |
When Clinical-Grade Material Is Non-Negotiable: For children with diagnosed hypermobility syndrome or hip dysplasia, a professionally specified T-stool height and wedge incline gradient matters significantly. DIY variations are adequate for typical low-tone W-sitters.
ACT II: KNOWLEDGE TRANSFER
Safety Gate — Read Before You Begin
🔴 RED — Do Not Proceed
- Diagnosed hip dysplasia — requires physician clearance first
- Confirmed hypermobility syndrome (EDS/hEDS) — PT-supervised only
- In-toeing gait combined with knee or hip pain — orthopedic assessment first
- Spasticity or hypertonia — this protocol is for low-tone/hypotonic presentations only
- Any positioning band leaving marks or restricting circulation — stop immediately
🟡 AMBER — Modify and Monitor
- Child under 2.5 years — environmental support only, no active correction
- Child complains of discomfort in cross-legged sitting — use supported alternatives first
- First therapy ball session — deflate slightly for stability
- Child with sensory sensitivities to touch — introduce positioning band very gradually, starting with 2-minute sessions
🟢 GREEN — Safe to Proceed
- Child is 3–8 years, W-sitting without pain complaints
- No diagnosed orthopedic conditions
- Core weakness / low tone assessed by OT or noted by pediatrician
- Child is fed, rested, and regulated before session
- Space is clear of hard objects, especially around therapy ball use
Emergency Protocol: If the child shows severe distress, joint pain, or reports that a position "really hurts" — stop the session, document what happened, and consult your Pinnacle OT/PT. Call 9100 181 181 if guidance is needed immediately.

ACT II: KNOWLEDGE TRANSFER
The Ideal W-Sitting Intervention Space
Spatial setup prevents 80% of session failures before they start. The goal is to make healthy sitting the path of least resistance — the environment should make W-sitting less convenient and alternatives immediately available.
Position Guide
Materials Station
All 9 materials within arm's reach of parent. Never interrupt a session to hunt for materials.
Parent Position
To the side of the child — not behind, not directly facing. Allows posture observation without confrontation.
Wedge Cushion
Pre-positioned in child's primary play zone before they arrive — already there, naturally sat upon.
Core Games Area
2×2 meter clear zone with floor mat for balance activities — free of furniture.
Visual Cards
At child's eye level on wall or low shelf — visible from primary play position.
T-Stool & Therapy Ball
T-stool near low table for table activities; therapy ball in corner with holder/ring, ready to roll out.
Environmental Checklist
- Floor is non-slip (yoga mat or carpet)
- Room temperature comfortable (not too warm — affects muscle tone)
- Screens off during active strengthening sessions
- Remove toys that pull child into W-sitting specific areas
- Adequate natural light
- Preferred toys/activities positioned within non-W sitting zones


ACT III: EXECUTION
The 60-Second Pre-Session Check
The best session is one that starts right. A quick readiness check before every session prevents the most common session failures and ensures your child's nervous system is in the optimal state for learning.
Check | Go ✓ | Modify ~ | Postpone ✗ | |
Fed | Ate within last 2 hours | Ate 3+ hours ago | Hasn't eaten / just ate | |
Rested | Normal sleep, appears alert | Slightly tired but responsive | Clearly overtired, irritable | |
Emotional State | Calm, regulated | Slightly dysregulated but responsive | Meltdown in last 30 mins | |
Physical | Moving comfortably, no complaints | Minor ache mentioned | Pain reported or visible discomfort | |
Engagement | Has noticed preferred materials | Needs gentle invitation | Refusing approach to play space | |
Sensory State | Not in sensory overload | Slightly overstimulated | Signs of sensory overwhelm | |
Time | 20+ mins before next transition | 10–15 mins available | Less than 10 mins before transition |
4+ Green ✓
Full session — proceed with all materials
2–3 Green ✓
Modified session — 1–2 materials only, 10 mins max, positioning focus only
1 or fewer ✓
Postpone — environmental positioning (wedge cushion) still counts as passive intervention
"If 3 days in a row score Postpone, that's not failure — that's data. It tells you the session timing or conditions need adjustment."

ACT III: EXECUTION
Step 1 of 6 — The Invitation
The Principle
Every protocol begins with an invitation, not a command. The child must choose to engage. A child who enters an activity through invitation stays longer, engages deeper, and builds stronger neural associations with the therapeutic materials.
Parent Script
"Hey, [child's name] — come see what I set up! There's [name their favorite toy] on your special cushion. Want to come play?"
For non-verbal or minimally verbal children: Lead physically to the space, point to preferred toy, use a gesture of invitation. If child follows, that IS acceptance.
Acceptance Cues — Look For These
- Child moves toward the setup area
- Child reaches for or looks at the materials
- Child sits down on the wedge cushion or near the therapy ball
- Child begins interacting with preferred toy in the space
Resistance Cues and Responses
⚠️ Child says "No" or moves away → Wait 60 seconds, offer again once with a different preferred toy. If second attempt refused, trigger Modify protocol from Card 13.
Body Language Guide
- Position yourself at child's level (crouch, don't tower)
- Offer the invitation once, then wait 15 seconds
- Smile genuinely — children read emotional authenticity in milliseconds
Timing: 30–60 seconds maximum for invitation phase

ACT III: EXECUTION
Step 2 of 6 — The Engagement
The child is in the space. Now the therapeutic material is introduced naturally — not as equipment, but as part of the play. Choose ONE material per session when introducing new tools.
Wedge Cushion (Environmental)
No introduction needed — child sits on it. If they ask "what's this?" → "It's your special sit-spot. Try it!"
Therapy Ball (Active Session)
"Look at this ball! Can you climb up and sit on it? I'll hold it. Let's see if you can reach this toy from up there!" Hold it steady; hands-on assistance for first 2–3 sessions.
T-Stool (Table Activity)
"Let's do [drawing/puzzle] on the table! Here's a special spinning chair — see if you can balance on it!" Demonstrate briefly, invite child to try.
Visual Position Cards
"Before we play, you get to pick how you want to sit! Look — there's criss-cross, there's legs-forward... which one do you want today?" Fan 3 cards, let child choose. Praise the choice regardless of which is picked.
Reinforcement CUE: The instant the child is seated in a non-W position — even briefly, even with support — say: "Yes! Look at that — great sitting!" Immediate, specific, warm. This is the most important moment in the entire session.
ACT III: EXECUTION
Step 3 of 6 — The Therapeutic Action
The core of each session: 10–20 minutes of active, material-driven therapeutic work. The 9 materials run on two parallel tracks simultaneously — providing alternatives today while building capacity for tomorrow.
T-Stool — Core Builder
Child sits on T-stool during tabletop play. Parent does NOT hold the stool. Week 1–2: 5 mins. Week 3–4: 10 mins. Week 5–8: Full tabletop sessions. Watch for trunk straightening and reduced table leaning.
Wedge Cushion — Passive Environment
Child sits on wedge during ALL floor play. No leg instruction needed — the geometry does the work. Week 1–4: Wedge for all floor activities. Week 5–8: Alternate with flat floor gradually.
Floor Seat — Extended Sitting
For activities lasting 10+ minutes (story time, puzzles). Week 1–4: Full back support. Week 5–8: Lower back support height. Week 9+: Remove support entirely.
Therapy Ball — Core Activation
5–15 minute active sessions. Seated reaching, gentle bouncing, tummy over ball reaching. Week 1: Parent-held. Week 2: Ball holder ring. Week 3+: Independent supervised.
Visual Position Cards — Behavioral Scaffold
Before EVERY floor activity, offer 3 position cards. Place chosen card on floor as reminder. 30 seconds in chosen position = verbal praise. 1 minute = preferred sticker or token.
Hip Stretching Strap — Flexibility
5-minute daily routine: Butterfly stretch (2×30s), seated hamstring with strap (2×20s each leg), hip flexor lunge (2×20s each side). NEVER force. Time during preferred screen content — body relaxes when distracted.
Positioning Band — Habit Interruption
Loosely applied around both thighs during 10–15 minutes supervised floor play. Maximum 15-minute sessions. Never overnight. If child removes it, reapply with consent at next session.
Kneeling Bench — Immediate Alternative
Positioned at child's primary floor play area. Environment structures the position — no verbal instruction needed. Transition arc: kneeling bench → cross-legged on wedge → cross-legged on floor.
Core Games Kit — Root Cause Solution
15–20 mins, 3–4x/week. Rotate: Day 1: Balance board. Day 2: Animal walks. Day 3: Scooter board. Day 4: Yoga/movement cards. This is the highest-leverage intervention.
"We are running two parallel tracks simultaneously: giving the child alternatives today, and building the capacity so alternatives become natural tomorrow. Both tracks matter. Neither alone is sufficient."

ACT III: EXECUTION
Step 4 of 6 — Repeat and Vary
"3 high-quality engaged minutes of core work beats 20 forced, distressed minutes every single time."
Material | Sessions/Week | Duration | Weekly Dosage | |
Wedge Cushion | 7 days (all floor play) | Passive/entire session | Environmental baseline | |
Visual Position Cards | Every floor sitting event | 30 sec per choice | Multiple daily micro-doses | |
Core Games Kit | 3–4x per week | 15–20 minutes | 45–80 minutes | |
Therapy Ball | 3–4x per week | 10–15 minutes | 30–60 minutes | |
T-Stool | 3–4x per week | 5–15 mins at table | 15–60 minutes | |
Hip Stretches | Daily | 5 minutes | 35 minutes | |
Positioning Band | 3–4x per week | 10–15 minutes | 30–60 minutes | |
Kneeling Bench | All floor play opportunities | Duration of floor play | Environmental baseline |
Variation Options to Maintain Engagement
Therapy Ball Variations
Seated reaching → seated bouncing → tummy rolling → ball catch while seated → seated ball pass with sibling
Core Games Variations
Bear walk race → crab walk obstacle course → frog jump count → army crawl through tunnel → yoga poses freeze dance
Position Card Variations
Child chooses → child teaches sibling a position → position of the day chart → position points reward board
Satiation Indicators — When the Child Has Had Enough: Slumping significantly, seeking to move away from material, increased irritability, or loss of engagement. These are physiological signals, not behavioral noncompliance. Respect them.

ACT III: EXECUTION
Step 5 of 6 — Reinforce and Celebrate
The Timing Rule: Within 3 seconds of the desired behavior. Specific. Enthusiastic. Genuine.
What to Reinforce (in order)
Any non-W sitting
Even 5 seconds of cross-legged: "AMAZING sitting!"
Attempting alternative position
Even briefly: "I love that you tried it!"
Choosing from position cards
The act of choosing: "Great choice!"
Using wedge/T-stool unprompted
"You remembered your special seat!"
Core games engagement
Any active play: "Look at those strong muscles!"
Reinforcement Timing
Week 1–2
Reinforce every attempt, every 30 seconds of non-W sitting
Week 3–4
Reinforce every 1–2 minutes of non-W sitting
Week 5–8
Reinforce every successful 5-minute session completion
Week 9+
Natural praise for mastery milestones
"Celebrate the attempt, not just the success. A child who tries to sit differently for 3 seconds and then reverts is practicing — and practice deserves recognition."

ACT III: EXECUTION
Step 6 of 6 — The Cool-Down
No session ends abruptly. Every therapeutic activity deserves a predictable, calm closure that transitions the child back to baseline and associates the materials with positive endings.
Final Transition Cue
"All done with therapy play! Now we're going to [next preferred activity]."
Visual timer (or phone timer) marks the transition if the child responds well to visual countdowns. If child resists ending: offer "one more," honor it once, then firm close. Promise: "This will be here tomorrow. We'll do it again!"
Post-Session Sensory Landing
2 minutes of proprioceptive input helps the nervous system settle after active core work:
- Firm joint compressions through shoulders
- Heavy work: carrying therapy ball to storage corner
- Tight hug or weighted lap pad if child enjoys deep pressure
ACT III: EXECUTION
60 Seconds of Data Now Saves Hours of Guessing Later
Session data is the most powerful tool parents have. Without it, you're navigating by emotion. With it, you see the trend before you feel it — and you make better decisions faster.
Non-W Sitting Duration
Minutes child spent in non-W position (total, approximate). Example: "15 mins cross-legged on wedge"
W-Sitting Returns
Count how many times child returned to W during session. Example: "3 times during block play"
Material Response
Rate 1–5: 1=refused, 3=tolerated, 5=enthusiastically engaged. Example: "Therapy ball: 4, T-stool: 2"
Weekly Trend Tracker
Week | Non-W Mins | W Returns | Ball /5 | T-Stool /5 | |
Week 1 | ___ | ___ | ___ | ___ | |
Week 2 | ___ | ___ | ___ | ___ | |
Week 3 | ___ | ___ | ___ | ___ | |
Week 4 | ___ | ___ | ___ | ___ |
Increasing non-W minutes
Core strength is building ✅
Decreasing W returns
Habit is shifting ✅
Flat or worsening after 3 weeks
Adjust materials or seek OT guidance 🔄

ACT III: EXECUTION
Reality Check: Most Sessions Aren't Perfect
Session abandonment is not failure — it's data. Every challenge you encounter in implementing F-577 has been faced by thousands of families before you. These are the most common problems and their evidence-based solutions.
Problem 1: Child immediately W-sits despite the wedge cushion
Why: The wedge may be insufficient incline for this child's hip tightness, or the W habit override is strong. The wedge alone isn't a full solution. Fix: Increase wedge incline. Add visual position cards simultaneously. Introduce kneeling bench as floor sitting alternative.
Problem 2: Child refuses to sit on the therapy ball
Why: The unstable surface is genuinely frightening for a child with proprioceptive insecurity. This is a sensory response, not defiance. Fix: Deflate ball to very firm. Parent sits on ball first (modeling). Offer support hold for first 5+ sessions. Progress over weeks, not days.
Problem 3: Child removes the positioning band immediately
Why: The band introduces an unfamiliar sensory input. Acceptance must be shaped gradually. Fix: Start with band around only one thigh. Duration of 2 minutes only. Pair with highly preferred activity. Build tolerance week by week.
Problem 4: Verbal reminders keep slipping out ("sit properly!")
Why: Parent habit patterns are as real as child habit patterns. Fix: Replace verbal with a visual tap — tap your own crossed legs when you see W-sitting. Use a visual timer as the reminder rather than your voice.
Problem 5: Progress made then sudden regression to full W-sitting
Why: Regression almost always coincides with illness, fatigue, or increased cognitive demands (new school year, new skill learning). Fix: Return to full environmental support temporarily. Reduce active strengthening demands. Core strength returns faster after regression than initial acquisition.
Problem 6: Siblings are copying the positioning setup
Why: Siblings want what the target child has. Fix: Include siblings. Bear walks and balance boards benefit every child. The core games kit becomes family playtime, which also normalizes the intervention beautifully.
Problem 7: School won't allow the floor seat or wedge cushion
Why: Schools without OT guidance may not have protocols for positioning equipment in classrooms. Fix: Request OT consultation letter from your Pinnacle therapist specifying the developmental rationale. Most schools comply with documented OT recommendations. Call 9100 181 181 for a standard accommodation letter template.
ACT III: EXECUTION
Every Child's W-Sitting Has a Different Root Cause
Match the material emphasis to your child's specific profile. Using the wrong emphasis for the wrong root cause is the most common reason home programs stall. Identify your child's profile first, then build your material sequence around it.
Profile A: Weak Core / Low Muscle Tone
Signs: W-sits because all other positions fatigue quickly. Slumps at the table. Tires during physical play.
Material Priority: T-Stool + Therapy Ball + Core Games Kit (strength-first)
Progress Pace: Slower — 10–12 weeks for meaningful change
Profile B: Tight Hips / Limited Flexibility
Signs: W-sits because cross-legged genuinely feels tight or painful. May complain when repositioned.
Material Priority: Hip Stretching Strap + Wedge Cushion + Floor Seat (flexibility-first)
Progress Pace: 6–10 weeks for hip flexibility changes
Profile C: Habituated Pattern / Motor Habit
Signs: W-sits automatically even with sufficient strength. Doesn't seem to notice they've done it.
Material Priority: Visual Position Cards + Positioning Band + Environmental Setup (awareness-first)
Progress Pace: 4–8 weeks with consistent awareness prompting
Profile D: Hypermobility / Joint Laxity
Signs: Very flexible child; W-sits for joint stability. May hyperextend elbows/knees.
Material Priority: T-Stool + Therapy Ball + Core Games Kit (stability-building only)
⚠️ AVOID Hip Stretching Strap — contraindicated for hypermobile children
Progress Pace: 12–16 weeks — Consult PT for confirmed hypermobility
ACT IV: THE PROGRESS ARC
Weeks 1–2: Introducing the New Normal
Weeks 1 and 2 are the hardest. The child's habits are strong, the materials feel foreign, and change is almost invisible. The neural pathways for new habits are just beginning to form. Check your data tracker — the numbers usually tell a different story than the emotions do.
15%
Progress Milestone
Weeks 1–2 position on the overall intervention arc
What Progress Actually Looks Like in This Phase
Child begins to notice the wedge cushion (may move it away — that's awareness!)
W-sitting returns reduced from 8–10x per 30 minutes to 5–7x
Child sits in non-W position for 30–60 more seconds than baseline before returning
T-stool tolerance increases from 2 minutes to 5 minutes
Core games tolerated for 10–12 minutes (even with frequent position breaks)
What Is NOT Progress Yet (and that's completely fine): Cross-legged sitting independently without support (comes weeks 4–8). Spontaneously choosing non-W positions (comes weeks 3–5). W-sitting eliminated entirely (month 2–3 milestone for most children).
"If your child sat cross-legged for 3 seconds longer today than last week — that is a measurable neural change. That is real progress."

ACT IV: THE PROGRESS ARC
Weeks 3–4: Neural Pathways Are Forming
Something begins to shift in weeks 3 and 4. The materials are no longer foreign. The child has a rhythm. You, the caregiver, have learned your child's response patterns. This is the consolidation phase — habits are hardening in the right direction.
40%
Progress Milestone
Weeks 3–4 position on the overall intervention arc
Consolidation Indicators — Look for These
- Child begins to approach the wedge cushion or T-stool independently (even once or twice)
- W-sitting returns reduced to 2–4x per 30 minutes
- Core games sessions last 15–18 minutes without significant protest
- Child can be verbally prompted once and holds alternative position for 2+ minutes
- Visual position cards used without prompting during some sessions
- Parent confidence in running the protocol is noticeably higher
Spontaneous Signs of Generalization
Watch for these unprompted moments — they're evidence the therapy is spreading beyond structured sessions:
- Child sits cross-legged for a few seconds before W-sitting (testing the alternative)
- During school or with other caregivers, child occasionally uses non-W position
- Child references the materials by name: "my ball," "my sitting cushion"
If consolidation indicators are consistently present: increase core games from 3x to 4x per week. Add a second T-stool session at a different table activity.
"By week 4, most parents report they feel more confident than overwhelmed. You've learned your child's response patterns, their best material, and their optimal session time. That knowledge is clinical intelligence. You are now your child's most important therapist."

ACT IV: THE PROGRESS ARC
Weeks 5–8: Mastery Unlocking
75%
Progress Milestone
Weeks 5–8 position on the overall intervention arc — mastery is within reach
This is where the investment pays off visibly. Look for all three mastery criteria to confirm sustainable change rather than situational improvement.
Criterion 1 — Spontaneous Choice
Child uses non-W sitting positions in 3+ natural (non-prompted) situations across a week
Criterion 2 — Duration
Child maintains cross-legged or long-sitting for 10+ minutes independently during preferred floor activities
Criterion 3 — Generalization
Non-W positions observed at school, with grandparents, or in settings where no intervention materials are present
Maintenance Check: Does the behavior persist for 2 weeks without daily prompting? If yes — mastery achieved. If the behavior disappears when materials are removed — strengthening continues; don't fade materials yet.
When to Progress: Mastery of F-577 indicates readiness for → F-578: Core Weakness Signs → F-579: Balance and Coordination Challenges → Increased challenge versions: side-sitting, ring-sitting, prone on elbows floor play.

ACT IV: THE PROGRESS ARC
🏆 You Did This.
Your child grew because of your commitment. That growth is permanent.
Over 5–8 weeks, you have:
- Introduced 9 evidence-based therapy materials into your child's daily environment
- Executed daily core strengthening sessions alongside regular caregiving demands
- Resisted the urge to use verbal correction and replaced it with capacity building
- Tracked data with consistency and adjusted when things didn't go as planned
- Built genuine core strength in your child's body that will serve them for life
The core strength your child has built is not just about floor sitting. It will support their desk sitting at school, their sports participation, their handwriting endurance, their postural confidence in social settings. You built a foundation, not just a fix.
Family Celebration Suggestion: Take a photo or short video of your child sitting cross-legged in their play space. Write the date. This is your evidence. This is your family's milestone. Share it in the Pinnacle Parent Community if you're comfortable — you will inspire another family who is exactly where you were 8 weeks ago.
Journal Prompt:"The moment I knew it was working was..."
ACT IV: THE PROGRESS ARC
Know When to Pause — Even During Progress
Trust your instincts. If something feels wrong, pause and ask. Progress does not override safety — and recognizing red flags early prevents setbacks that are harder to recover from.
🚩 Red Flag 1: Joint Pain During or After Sessions
Child reports knee, hip, or ankle pain; visible limping after therapy ball or T-stool sessions. Action: Stop all active intervention. Book Pinnacle PT/OT assessment. Call 9100 181 181.
🚩 Red Flag 2: W-Sitting Dramatically Worsens
After weeks of improvement, W-sitting returns above baseline frequency — even in new environments. Action: Return to environmental support only. Monitor 5–7 days. If no improvement, teleconsult booking.
🚩 Red Flag 3: Gait Changes
Child's walking pattern changes — increased in-toeing, toe-walking, or scissoring gait during the intervention period. Action: Pause intervention. Same-week PT assessment.
🚩 Red Flag 4: Severe Emotional Distress Around Sitting Activities
Child develops significant anxiety or meltdowns triggered specifically by intervention materials — not present before intervention. Action: Return to least-intrusive materials only (wedge, visual cards). ABA/BCBA consultation. Do not force materials.
🚩 Red Flag 5: No Progress After 8 Weeks of Consistent Effort
Data tracker shows flat W-sitting return frequency, no duration improvement, materials still refused after 8 weeks. Action: Comprehensive OT + PT + orthopedic assessment. Call 9100 181 181 for center referral.
Escalation Pathway: Self-resolve (1–3 days) → Pinnacle Teleconsultation (same week) → Center Visit (within 2 weeks) → Medical Referral (orthopedics/neurology as indicated)
ACT IV: THE PROGRESS ARC
F-577 in the Motor Development Journey
You are here. Here is where you're heading. F-577 is not a standalone technique — it's one carefully positioned episode in a continuous developmental arc that builds progressive postural capacity.
Prerequisites
- F-575 or F-576 ideally completed or currently active
- Basic gross motor assessment by OT/PT (or Pinnacle AbilityScore®)
Current Position
F-577 — Episode 577 of 650 in the Motor Development & Postural Control Series
Next-Level Options (based on response profile)
- Strong Core Response → F-578: Core Weakness Signs
- Balance Improvements Noticed → F-579: Balance & Coordination Challenges
- Hypermobility Pattern Emerging → Consult for F-580 pathway
Long-Term Goal
Independent, varied floor sitting posture used naturally across all contexts — supporting school participation, physical activity, bilateral coordination, and age-appropriate gross motor play.
ACT IV: THE PROGRESS ARC
More Techniques In: Motor Development & Postural Control
Materials you already own work across multiple techniques. Your F-577 investment extends far beyond a single protocol — it seeds the entire Motor Development domain.
F-580: 9 Materials for Hypermobility & Motor Planning
🔴 Advanced
T-Stool ✓ Therapy Ball ✓
You Already Own Materials For These: Based on your F-577 material set, you can begin F-575, F-576, F-578, or F-579 without purchasing additional materials. Your investment works across the entire Motor Development domain.
ACT IV: THE PROGRESS ARC
This Technique Is One Piece of a Larger Plan
W-sitting is a motor signal that connects to every developmental domain. Addressing it doesn't just improve floor posture — it ripples outward into attention, language access, social participation, and long-term school readiness.
GPT-OS® Full Profile Integration
Your child's Gross Motor Readiness Index and Postural Control Readiness Index are actively being tracked across your F-577 sessions. As these indexes improve, GPT-OS® will automatically recommend the next evidence-matched technique.

ACT V: COMMUNITY & ECOSYSTEM
From the Families Who Started Exactly Where You Are
These are not marketing claims. These are clinical narratives with behavioral specificity — real families, real data, real timelines.
Priya, Mother of 4-Year-Old Boy — Chennai
"Arjun was in the W every single second on the floor. His OT at Pinnacle said his core was so weak that cross-legged sitting was genuinely tiring — not stubbornness. We started with just the wedge cushion and therapy ball. Within 3 weeks, he was sitting cross-legged for 5 minutes at a time. By week 8, his preschool teacher called to say she'd noticed him sitting properly during circle time without reminders. We'd never told the school we were working on it."
Before: Exclusive W-sitting, 0 cross-legged minutes. After: 15+ mins spontaneous cross-legged. Zero verbal prompts by week 8. Timeline: 8 weeks | Wedge + Therapy Ball + Core Games Kit
Suresh, Father of 5-Year-Old Girl — Hyderabad
"We'd been saying 'criss-cross applesauce' for two years. The moment we understood that she was W-sitting because she physically couldn't sustain other positions, everything changed. The T-stool at her art table was the turning point — she'd sit on it for 45 minutes doing art because she loved drawing. Her core was working the whole time without her knowing."
Before: W-sitting return rate: 9x per 30 minutes. After: 1–2x per 30 minutes. T-stool used independently. Timeline: 10 weeks | T-Stool + Wedge Cushion + Visual Position Cards
International Family — Singapore, Mother of 6-Year-Old
"Our son has hypermobility. The PT said no stretching, more strengthening. The core games kit became our entire evenings. Bear walks down the hallway, balance board before dinner. In 12 weeks his postural control improved so significantly that his handwriting at school also improved — we hadn't even targeted that. GPT-OS® had flagged the connection. The system knew."
Before: Extreme joint laxity W-sitting requiring core compensation. After: Varied sitting positions. Improved handwriting posture. School participation normalized. Timeline: 12 weeks | Core Games Kit + T-Stool + Therapy Ball (no stretching strap)
Outcomes are illustrative; individual results vary based on child profile, consistency of implementation, and underlying factors. Statistics represent aggregate outcomes across the Pinnacle Blooms Network.

ACT V: COMMUNITY & ECOSYSTEM
You Don't Have to Navigate This Alone
Isolation is the enemy of adherence. Community is the engine of consistency. Every family in these groups is implementing the same protocol with the same challenges — and their hard-won knowledge is available to you.
F-577 W-Sitting Parent WhatsApp Group
Real-time peer support from parents currently implementing this exact protocol. Share wins, troubleshoot challenges, get encouragement from families who understand exactly what you're experiencing.
Pinnacle Online Parent Forum
Searchable discussion threads by technique, material, and child profile. Find parents who've solved the specific challenge you're facing. Access the Forum →
Local Parent Meetups
Monthly parent meetups at Pinnacle centers in 70+ locations across India. In-person connection with families navigating similar journeys. Find Meetups Near You →
Peer Mentoring Programme
Connect with a Pinnacle "Parent Guide" — an experienced parent who has completed 6+ months of GPT-OS® intervention and has been trained to support newer families. Request a Parent Guide →
"Every parent who shares their F-577 journey contributes to the knowledge base that helps the next family. You have experience that no therapist has — the lived, daily, nuanced experience of running this protocol with your specific child. That is irreplaceable."
ACT V: COMMUNITY & ECOSYSTEM
Home + Clinic = Maximum Impact
Your home implementation is powerful. Professional guidance makes it precise. The two together produce outcomes that neither can achieve alone — the therapist's clinical precision combined with your daily presence and deep knowledge of your child.
When to Seek Professional OT/PT Guidance
- Your child's W-sitting profile is unclear (which root cause?)
- No progress after 4 weeks of consistent home implementation
- Red flags present (Card 27)
- You want a formal AbilityScore® assessment and personalized protocol
What a Pinnacle Assessment Includes
- AbilityScore® Gross Motor Assessment — standardized scoring
- Postural Control Readiness Index — baseline measurement
- Core Strength Functional Assessment — optimal material protocol
- Hip Mobility Screen — flexibility vs. strengthening primary need
- EverydayTherapyProgramme™ — personalized daily home protocol
Teleconsultation — No Travel Required
60-minute video OT/PT consultation. Material prescription. Protocol setup. Progress review.
FREE National Autism Helpline
📞9100 181 181
16+ languages | Available 24×7
"Not sure where to start? Call us. We'll guide you to the right support."
ACT V: COMMUNITY & ECOSYSTEM
For the Curious Parent: The Evidence Behind F-577
The research that informs every material recommendation on this page. Every technique in the Pinnacle system is grounded in peer-reviewed, multi-country, clinically validated evidence — not expert opinion alone.
PRISMA Systematic Review (2024) — HIGH Confidence
16 articles from 2013–2023 confirm sensory integration and motor development intervention meets criteria as evidence-based practice for children with ASD. Gross motor and postural outcomes specifically documented. PMC11506176 →
Meta-Analysis, World J Clin Cases (2024) — MODERATE-HIGH Effect
Across 24 studies, sensory integration therapy effectively promotes gross motor skills (primary), adaptive behavior (secondary), and sensory processing (tertiary). Core strengthening through SI-based activities directly targeted. PMC10955541 →
Indian RCT, Padmanabha et al. (2019)
Home-based sensory-motor interventions in Indian pediatric populations demonstrated significant functional outcomes across motor development domains. Parent-implemented protocols validated for Indian home environments. DOI: 10.1007/s12098-018-2747-4 →
NCAEP Evidence-Based Practices Report (2020)
Visual supports and environmental modification classified as EBP for autism. Both are core F-577 interventions (position cards, environmental setup with wedge/bench). Highest US evidence standard. NCAEP 2020 Report →
WHO Nurturing Care Framework (2018)
Parent-implemented early developmental interventions during the critical 0–5 year window produce measurable population-level developmental outcomes. Caregiver-delivered motor programs validated across 54 LMICs. WHO NCF →
WHO Care for Child Development Package (2023)
Multi-country implementation data confirming household-material-based developmental interventions are effective, scalable, and equity-accessible. PMC9978394 →
ACT V: COMMUNITY & ECOSYSTEM
GPT-OS® — The Intelligence Behind Your Child's Progress
Your data helps your child. And every child like them. GPT-OS® transforms individual session data into a continuously improving, personalized intervention intelligence system — getting smarter with every session logged.
What GPT-OS® Learns From Your F-577 Data
- Which of the 9 materials produces the fastest W-sitting reduction for your child's specific profile
- The optimal session timing (time of day, post-meal/pre-meal patterns)
- Cross-domain connections between postural improvement and attention, handwriting, and social participation
- Population-level insights: your child's response pattern refines recommendations for the next family with the same profile
Privacy Architecture
All data is de-identified before population-level analysis. Individual child data is visible only to the family and their Pinnacle clinical team. GPT-OS® operates under Indian data protection frameworks with international sovereignty-grade compliance.
20M+
Exclusive Sessions
97%+
Improvement Rate
70+
Centers & Countries

ACT V: COMMUNITY & ECOSYSTEM
The Reel That Started This Conversation
Reel F-577
"When their legs always form that W shape"
Motor Development & Postural Control in Children — Episode 577 of 999
A Pinnacle Pediatric OT therapist presents each of the 9 materials with live demonstration of correct use. Running time: 75–85 seconds. Designed for sharing with spouses, grandparents, and teachers.
Why Both Reading and Watching Matter
Reading this page activates your analytical learning. Watching the reel activates your visual and procedural learning. Both together create the strongest parent competency. We recommend watching the reel both before and after reading this full page.
Video modeling is classified as a Level 1 Evidence-Based Practice for autism (NCAEP, 2020). Watching a therapist execute the technique activates mirror neurons and builds procedural memory in the parent caregiver.
Series Context
← F-576: Poor Postural Control Reel | F-577: W-Sitting [THIS REEL] | → F-578: Core Weakness Reel
ACT V: COMMUNITY & ECOSYSTEM
Consistency Across Caregivers Multiplies Impact 10x
If only one person knows this — implementation is 25% as effective as it could be. Every person who cares for your child is either reinforcing or undermining the work you're doing. Sharing this page makes everyone a co-therapist.
Share This Page
📲WhatsApp: "Sharing this page about W-sitting — really helpful!"
📧Email: Send the full page link with subject line pre-filled
🔗Copy Link: techniques.pinnacleblooms.org/motor-development/w-sitting-materials-F-577
"Explain to Grandparents" Version
"[Child's name] sometimes sits in a W shape because their core muscles are still getting stronger. Their therapist has given them special cushions and a special seat to help. When you see the W, instead of saying 'sit properly', you can point to their cushion or ask them to pick a position card. The goal is building muscles, not correcting posture. Thank you for helping!"
Teacher/School Communication Template
"[Child's name] is working on W-sitting correction with their occupational therapist. We would appreciate if the class could have access to a wedge cushion during floor time. Their OT has provided the clinical rationale [attached]. Your support in providing the cushion and avoiding verbal posture corrections would be greatly appreciated."
Research Reference
WHO CCD Package: Multi-caregiver training is critical for intervention generalization. Consistent caregiving across all settings produces 3× better maintenance outcomes than single-caregiver implementation. PMC9978394

ACT VI: THE CLOSE & LOOP
Your Questions, Answered by the Consortium
Derived from the Pinnacle clinical FAQ database and parent community query patterns — these are the questions real families ask most often when implementing F-577.
Q1: Is W-sitting always harmful? My pediatrician said it's fine.
Occasional W-sitting in typically developing children is normal and rarely harmful. The concern is habitual, exclusive W-sitting — where it's the child's only floor position, indicating underlying core weakness or hip tightness, and preventing development of dynamic trunk control. If W-sitting is the only position used at home and school across all contexts, the materials in F-577 are still beneficial regardless of immediate clinical concern.
Q2: My child is 2.5 years old. Is it too early to start?
For children under 3, environmental support (wedge cushion, floor seat) is fully appropriate. Active strengthening protocols (T-stool, therapy ball) can begin at 3 years. The most important thing at 2.5 is ensuring the environment offers alternatives — not correcting the child verbally.
Q3: How long before I see results?
Environmental materials produce position changes immediately. Behavioral shifts (spontaneous choice of alternatives) typically begin weeks 3–5 with consistent implementation. Core strength changes typically emerge over 6–12 weeks of consistent core game and ball use. The data tracker on Card 20 will show you the trend before you "feel" it in daily observation.
Q4: Can I use all 9 materials at once?
Yes, with caveats. Environmental materials (wedge, floor seat, kneeling bench, visual cards) can all be present simultaneously. For active materials (therapy ball, T-stool, core games), introduce one at a time over 1–2 weeks to identify your child's response and avoid overwhelming newness. By week 3–4, multiple materials can run in parallel.
Q5: My child's teacher says W-sitting is a concern at school too. What do I send them?
Use the Teacher Communication Template from Card 37. If your child is working with a Pinnacle OT, request an accommodation letter specifying the clinical rationale for a portable wedge cushion and floor seat in the classroom. Most schools comply readily with documented OT recommendations. Call 9100 181 181 for a template letter if needed.
Q6: My child has diagnosed hypermobility. Does this protocol still apply?
Modified protocol only. REMOVE the hip stretching strap (contraindicated). PRIORITIZE T-stool, therapy ball, and core games. CONSULT your PT before introducing the positioning band. EXTEND timeline to 12–16 weeks. See Card 22 Profile D for the full hypermobility modification.
Q7: The therapy ball is making my child anxious. What do I do?
(1) Deflate to very firm. (2) Use a ball holder ring. (3) Begin with parent sitting on ball while child observes — modeling desensitizes. (4) Introduce ball through tummy-lying games before seated use. (5) If ball anxiety persists after 3 weeks of gradual introduction, replace with T-stool as the primary core-builder.
Q8: I've been doing this for 3 months with minimal progress. What's next?
Three months of consistent effort with minimal change is a red flag (see Card 27). This indicates an underlying factor requiring professional assessment — possibly undiagnosed hypermobility syndrome, hip structural concern, or sensory processing disorder requiring direct OT intervention. Book a comprehensive Pinnacle OT + PT assessment. Call 9100 181 181.

ACT VI: THE CLOSE & LOOP
From Reading to Doing
You have everything you need to begin today. The only variable is the first step. Choose your entry point below — whether you're ready to launch immediately, prefer professional guidance, or want to explore the next technique in the series.
🟢 Start F-577 Today With GPT-OS®
Launch your personalized W-sitting intervention protocol with AbilityScore® baseline assessment. Get your child's Gross Motor Readiness Index and your first personalized EverydayTherapyProgramme™.
🔵 Book a Professional Consultation
Get an OT/PT assessment to identify your child's W-sitting root cause and receive a personalized material prescription. Center visit or teleconsultation available.
BOOK A CONSULTATION → | 📞 9100 181 181
⚪ Explore the Next Technique
Based on your child's profile, the recommended next technique in the Motor Development series is F-578: 9 Materials That Help With Core Weakness Signs.
✦ VALIDATED BY THE PINNACLE BLOOMS CONSORTIUM OT ● PT ● ABA ● SpEd ● NeuroDev ● CRO 20M+ Sessions ● 97%+ Improvement ● 70+ Centers Built by Mothers. Engineered as a System.
FREE National Autism Helpline: 📞 9100 181 181 | 16+ languages | 24×7
Preview of 9 materials that help with w sitting Therapy Material
Below is a visual preview of 9 materials that help with w sitting therapy material. The pages shown help educators, therapists, and caregivers understand the structure and content of the resource before use. Materials should be used under appropriate professional guidance.




















Link copied!

From Fear to Mastery. One Technique at a Time.
"Pinnacle Blooms Network® exists to transform every home into a proven, scientific, 24×7, personalized, multi-sensory, multi-disciplinary pediatric therapy center — powered by GPT-OS®, validated by 20 million sessions, and driven by the belief that every child deserves access to the world's best therapeutic expertise, regardless of geography, language, or economic circumstance.You arrived at F-577 looking for a way to help your child. You leave with 9 evidence-based materials, a 6-step protocol, a progress tracking system, a research library, a professional support network, and the knowledge that 97% of families who implement this with consistency see measurable improvement.The W will change. Because you decided to understand it."
🔝 Return to Top
→ Next Technique
← Previous Technique
🌐 Browse All
WHO-Aligned
UNICEF-Aligned
DPIIT-Recognised
MSME-Registered
GPT-OS® Validated
© 2026 Pinnacle Blooms Network®, a unit of Bharath Healthcare Laboratories Pvt. Ltd. All rights reserved. GPT-OS®, AbilityScore®, TherapeuticAI®, FusionModule™, EverydayTherapyProgramme™ are proprietary marks of Bharath Healthcare Laboratories Pvt. Ltd. Patents filed across 160+ countries. CIN: U74999TG2016PTC113063 | DIPP8651 | UDYAM: TS20F0009606 | GSTIN: 36AAGCB9722P1Z2
Medical Disclaimer:This content is educational and informational. It does not replace individualized assessment and intervention by licensed occupational therapists, physical therapists, or medical professionals. Persistent W-sitting may indicate underlying motor, orthopedic, or developmental differences requiring professional evaluation. Individual results may vary. Statistics represent aggregate outcomes across the Pinnacle Blooms Network, not individual guarantees.
techniques.pinnacleblooms.org | pinnacleblooms.org | The largest structured pediatric intervention knowledge base on Earth. Built by Mothers. Engineered as a System. Validated by Science. Powered by Love.